cushing's syndrome
DESCRIPTION
An essay on Cushing's SyndromeTRANSCRIPT
Iqra Mumal
17/04/14
The Feedback Mechanism of Cortisol and Its Use in Screening Tests to Help
Diagnose Cushing’s Syndrome
1. Introduction
Cortisol, also known as the “stress hormone”, is a steroid hormone produced
by the zona fasciculata of the adrenal cortex . The release of cortisol can be triggered
by a variety of stresses. This includes physical stress such as infection, de-‐hydration
or thermal exposure but it can also be physiological stresses such as fear and
anticipation. Its function is to regulate metabolism and the body’s reaction to stress
and inflammation. This is achieved by increasing blood sugar, suppressing the
immune system and aiding in metabolism.1
2. The Regulation and Feedback Mechanism of Cortisol
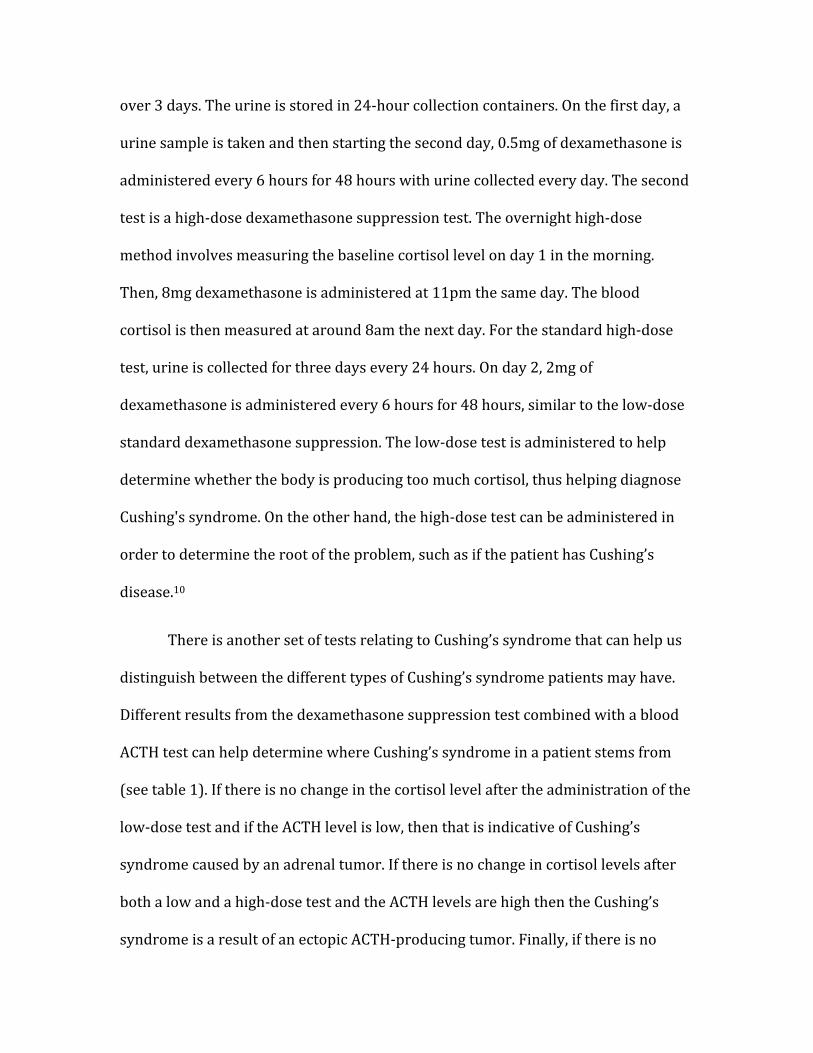
Cortisol secretion is controlled by the hypothalamic-‐pituitary-‐adrenal axis
(HPA) (see fig. 1). Corticotropin-‐releasing hormone (CRH), secreted by the
hypothalamus, is released into the hypophyseal portal blood vessels. CRH then acts
on the anterior pituitary and causes the release of ACTH (adreno-‐corticotropic
hormone). Finally, ACTH stimulates the adrenal gland, which produces and secretes
cortisol. After synthesis, cortisol diffuses into blood plasma where it is absorbed by
different tissues and implements its regulatory functions as a hormone. Eventually,
the liver metabolizes the cortisol in the blood plasma.2
Cortisol, like many of the other hormones regulated by the hypothalamus,
regulates its own secretion by negative feedback inhibition (see fig. 1) Cortisol is
able to do this by binding to the receptors on the hypothalamus and the anterior
pituitary and inhibiting the secretion of CRH and ACTH. Since cortisol is produced
by the action of both CRH and ACTH, a reduction in those will inevitably lead to a
reduction in cortisol levels. This allows the body to remain in a hormonal
homeostasis.3 This is an incredibly important system in our body and any
imbalances in the degree of hormone secretion can lead to a variety of disorders.
These disorders can result from both hypercortisolism (hypersecretion of cortisol)
or adrenal insufficiency, which is the hyposecretion of cortisol. Hyposecretion of
cortisol can lead to Addison’s disease while hypersecretion of cortisol leads to
Cushing’s syndrome.2,4
3. Cushing’s syndrome
Cushing’s syndrome develops as a result of high cortisol levels in the body for a
long time. Symptoms have been known to develop gradually so the diagnosis may
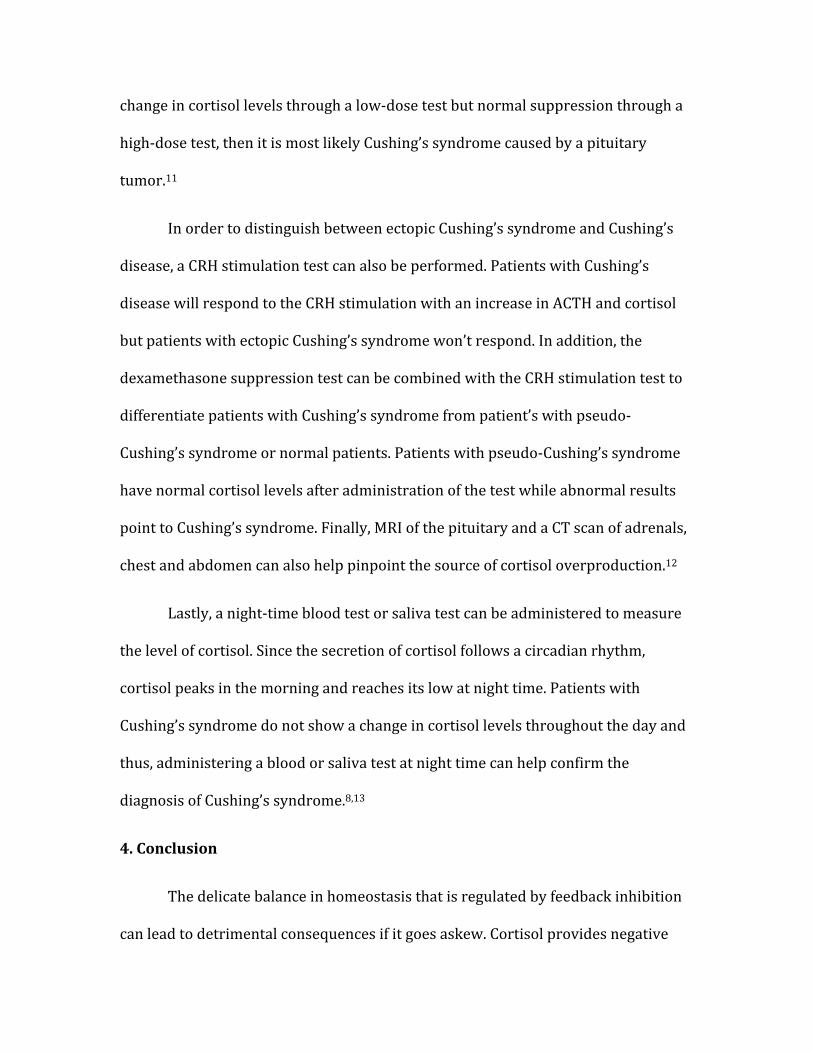
not be clear for some time. There is a wide range of symptoms that characterize a
patient with Cushing’s syndrome (see fig. 2). Symptoms include obesity,
characterized by fat around the main body area, facial puffiness, diabetes, high
blood pressure, muscle weakness, tiredness, aches and pains, mood swings, lack of
sex drive, osteoporosis, excess thirst and increased susceptibility to infections.4
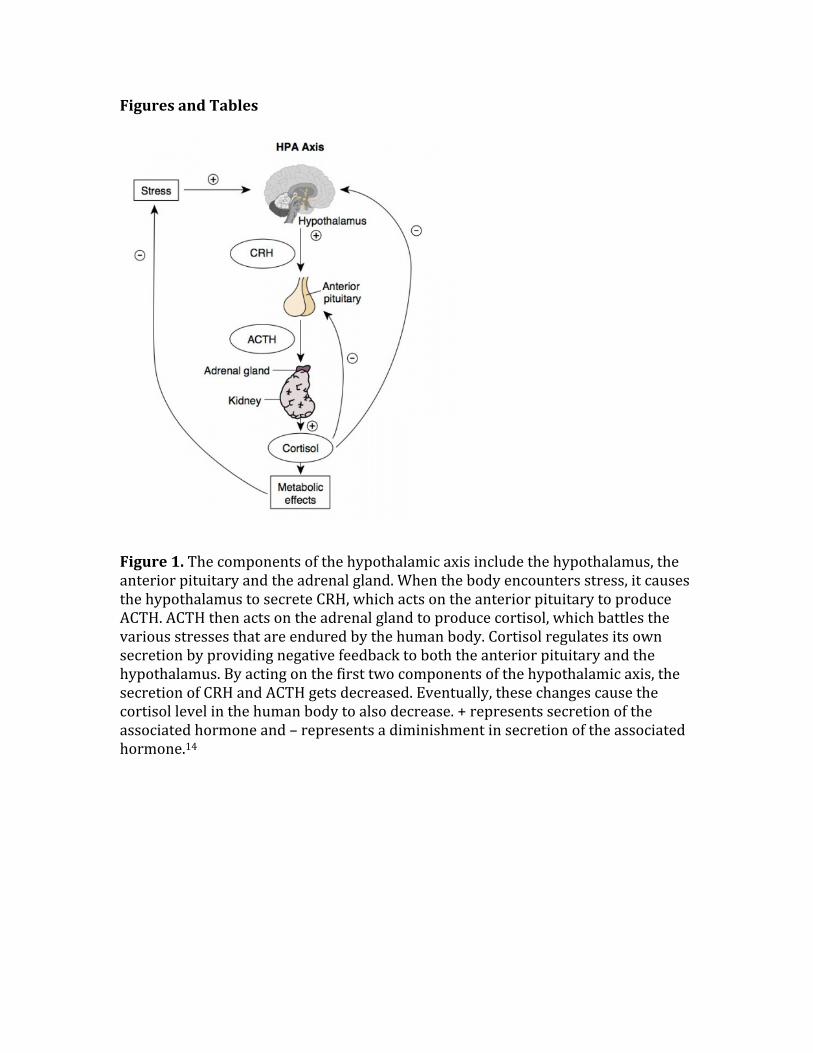
There are four main causes that can lead to the overproduction of cortisol. The
most common endogenous cause is a pituitary adenoma, which occurs about 70-‐
80% of the time. This is a benign or non-‐cancerous tumor of the anterior pituitary,
which results in the production of too much ACTH and leads to high volumes of
cortisol (see fig. 3). This form of Cushing’s syndrome is known as Cushing’s disease
and is characterized by high ACTH and cortisol levels.5
Another tumor that can lead to the overproduction of cortisol is a tumor in the
adrenal gland, which occurs about 10-‐20% of the time. This tumor can either be
benign, such as adrenal adenoma or micronodular hyperplasia, or malignant, such
as adrenal carcinoma. When this is the cause of Cushing’s syndrome, increased
negative feedback inhibition has the effect of decreasing the secretion of tropic
hormones. However, cortisol will remain high as negative feedback inhibition will
not have an effect on the adrenal gland.6
Another cause of Cushing’s syndrome can be ectopic or paraneoplastic Cushing’s
syndrome. This refers to tumors that are present outside the normal pituitary-‐
adrenal system and produce ACTH. Small cell lung carcinoma is an example of such
a tumor.7 Finally, the most common type of Cushing’s syndrome is iatrogenic
Cushing’s syndrome, which usually stems from treatment with corticosteroids for a
long time.2
3. Screening Test for Cushing’s syndrome
There are various reasons why the body can produce too much cortisol and
there are complex tests that have been generated to find the root cause of the excess
cortisol. Due to the fact that the level of cortisol varies depending on the time of the
day, a simple blood test is not enough to diagnose Cushing’s syndrome.8
The first thing to do is to determine whether there is an excess of cortisol in
the patient’s body (see fig. 4). The first test that is generally administered is the 24-‐
hour urine free cortisol level test, which is a test to measure the amount of cortisol
that is passed in urine. The way this test works is that the patient needs to collect all
the urine that is passed over 24 hours into a plastic container. The urine is then sent
to a laboratory to measure the cortisol levels. Since the secretion of cortisol
normally follows a circadian rhythm, patients with abnormal patterns of secretion
can be identified and diagnosed with Cushing’s syndrome.9
In addition, an alternative test that can be administered is a blood or urine
test that can be arranged after the patient takes a drug called dexamethasone. This
drug suppresses the amount of cortisol the body is supposed to make as
dexamethasone is a human made steroid that is similar to cortisol. Normally, it
should reduce the level of ACTH and subsequently cortisol. Thus, if the amount of
cortisol in the blood is still high after taking this drug then a diagnosis of Cushing’s
syndrome can be confirmed. There are two different kinds of dexamethasone
screening tests that are administered to patients suspected of Cushing’s syndrome.
Both of these dexamethasone suppression tests can be done either overnight or a
standard (3-‐day) way.10
The first is a low-‐dose dexamethasone suppression test. For the overnight
low-‐dose method, 1mg of dexamethasone is administered at 11 pm. The next day,
the patient’s blood cortisol level is measured at 8 am. The standard low-‐dose
method is different in that the cortisol level is measured in urine which is collected
over 3 days. The urine is stored in 24-‐hour collection containers. On the first day, a
urine sample is taken and then starting the second day, 0.5mg of dexamethasone is
administered every 6 hours for 48 hours with urine collected every day. The second
test is a high-‐dose dexamethasone suppression test. The overnight high-‐dose
method involves measuring the baseline cortisol level on day 1 in the morning.
Then, 8mg dexamethasone is administered at 11pm the same day. The blood
cortisol is then measured at around 8am the next day. For the standard high-‐dose
test, urine is collected for three days every 24 hours. On day 2, 2mg of
dexamethasone is administered every 6 hours for 48 hours, similar to the low-‐dose
standard dexamethasone suppression. The low-‐dose test is administered to help
determine whether the body is producing too much cortisol, thus helping diagnose
Cushing's syndrome. On the other hand, the high-‐dose test can be administered in
order to determine the root of the problem, such as if the patient has Cushing’s
disease.10
There is another set of tests relating to Cushing’s syndrome that can help us
distinguish between the different types of Cushing’s syndrome patients may have.
Different results from the dexamethasone suppression test combined with a blood
ACTH test can help determine where Cushing’s syndrome in a patient stems from
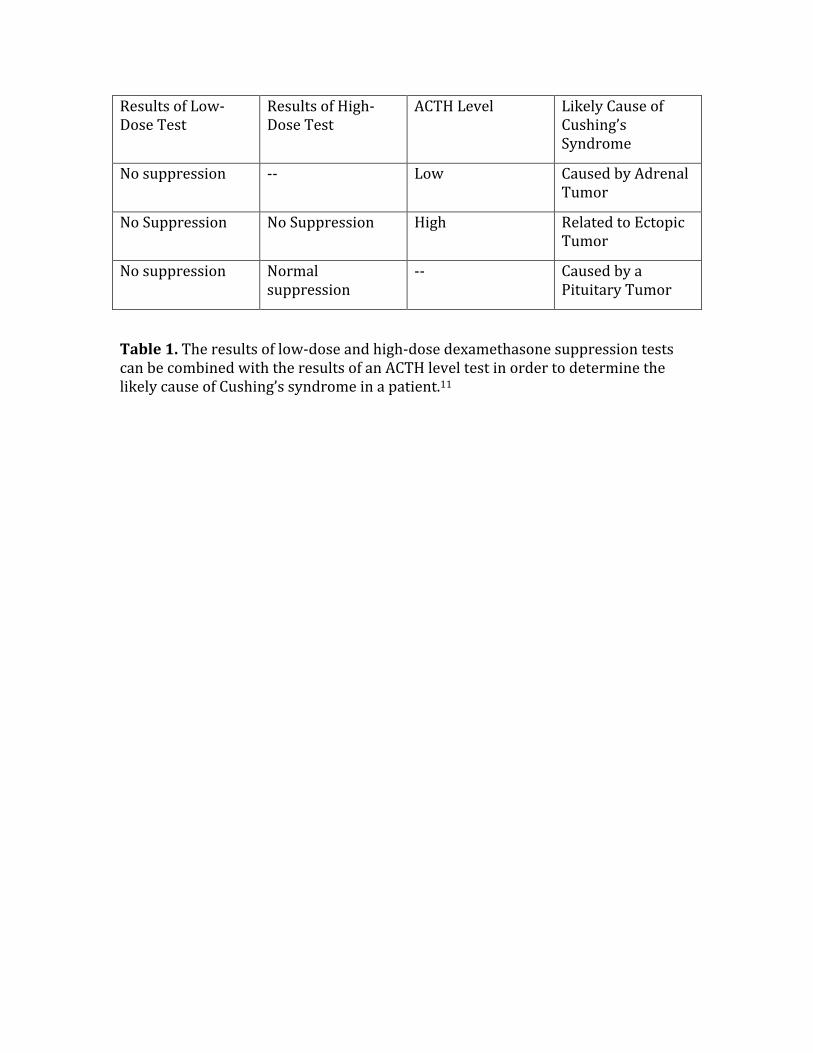
(see table 1). If there is no change in the cortisol level after the administration of the
low-‐dose test and if the ACTH level is low, then that is indicative of Cushing’s
syndrome caused by an adrenal tumor. If there is no change in cortisol levels after
both a low and a high-‐dose test and the ACTH levels are high then the Cushing’s
syndrome is a result of an ectopic ACTH-‐producing tumor. Finally, if there is no
change in cortisol levels through a low-‐dose test but normal suppression through a
high-‐dose test, then it is most likely Cushing’s syndrome caused by a pituitary
tumor.11
In order to distinguish between ectopic Cushing’s syndrome and Cushing’s
disease, a CRH stimulation test can also be performed. Patients with Cushing’s
disease will respond to the CRH stimulation with an increase in ACTH and cortisol
but patients with ectopic Cushing’s syndrome won’t respond. In addition, the
dexamethasone suppression test can be combined with the CRH stimulation test to
differentiate patients with Cushing’s syndrome from patient’s with pseudo-‐
Cushing’s syndrome or normal patients. Patients with pseudo-‐Cushing’s syndrome
have normal cortisol levels after administration of the test while abnormal results
point to Cushing’s syndrome. Finally, MRI of the pituitary and a CT scan of adrenals,
chest and abdomen can also help pinpoint the source of cortisol overproduction.12
Lastly, a night-‐time blood test or saliva test can be administered to measure
the level of cortisol. Since the secretion of cortisol follows a circadian rhythm,
cortisol peaks in the morning and reaches its low at night time. Patients with
Cushing’s syndrome do not show a change in cortisol levels throughout the day and
thus, administering a blood or saliva test at night time can help confirm the
diagnosis of Cushing’s syndrome.8,13
4. Conclusion
The delicate balance in homeostasis that is regulated by feedback inhibition
can lead to detrimental consequences if it goes askew. Cortisol provides negative

feedback inhibition to both the anterior pituitary and adrenal gland, which allows a
decrease in the production of cortisol. When this system is altered, for example, due
to the presence of a tumor in the anterior pituitary or adrenal gland, then that can
lead to Cushing’s syndrome. Screening tests such as the 24-‐hour urine free cortisol
test or dexamethasone suppression tests can not only help confirm a diagnosis of
Cushing’s syndrome but also figure out where the pathology of the disease lies.
Figures and Tables
Figure 1. The components of the hypothalamic axis include the hypothalamus, the anterior pituitary and the adrenal gland. When the body encounters stress, it causes the hypothalamus to secrete CRH, which acts on the anterior pituitary to produce ACTH. ACTH then acts on the adrenal gland to produce cortisol, which battles the various stresses that are endured by the human body. Cortisol regulates its own secretion by providing negative feedback to both the anterior pituitary and the hypothalamus. By acting on the first two components of the hypothalamic axis, the secretion of CRH and ACTH gets decreased. Eventually, these changes cause the cortisol level in the human body to also decrease. + represents secretion of the associated hormone and – represents a diminishment in secretion of the associated hormone.14
Figure 2. This figure outlines the various different symptoms that can be associated with Cushing’s syndrome. The range and generality of many of these symptoms make it hard to diagnose Cushing’s syndrome.15
Figure 3. The presence of a tumor in the anterior pituitary, also known as a pituitary adenoma, make up for 70-‐80% of endogenous Cushing’s syndrome.6
Results of Low-‐Dose Test
Results of High-‐Dose Test
ACTH Level Likely Cause of Cushing’s Syndrome
No suppression -‐-‐ Low Caused by Adrenal Tumor
No Suppression No Suppression High Related to Ectopic Tumor
No suppression Normal suppression
-‐-‐ Caused by a Pituitary Tumor
Table 1. The results of low-‐dose and high-‐dose dexamethasone suppression tests can be combined with the results of an ACTH level test in order to determine the likely cause of Cushing’s syndrome in a patient.11
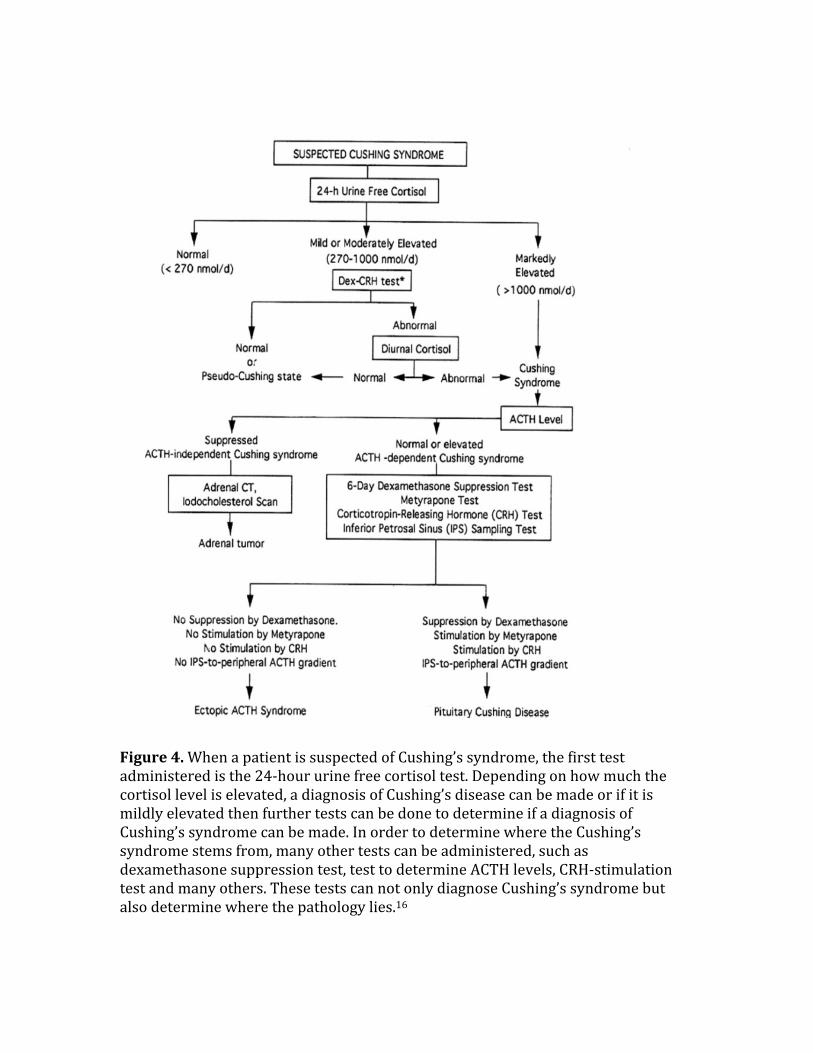
Figure 4. When a patient is suspected of Cushing’s syndrome, the first test administered is the 24-‐hour urine free cortisol test. Depending on how much the cortisol level is elevated, a diagnosis of Cushing’s disease can be made or if it is mildly elevated then further tests can be done to determine if a diagnosis of Cushing’s syndrome can be made. In order to determine where the Cushing’s syndrome stems from, many other tests can be administered, such as dexamethasone suppression test, test to determine ACTH levels, CRH-‐stimulation test and many others. These tests can not only diagnose Cushing’s syndrome but also determine where the pathology lies.16
References
1. Dickerson, Sally S., and Margaret E. Kemeny. "Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research." Psychological bulletin 130.3 (2004): 355.
2. Dinan, Timothy G., and Lucinda V. Scott. "Anatomy of melancholia: focus on hypothalamic–pituitary–adrenal axis overactivity and the role of vasopressin." Journal of anatomy 207.3 (2005): 259-‐264.
3. Yehuda, Rachel, et al. "Alterations in cortisol negative feedback inhibition as examined using the ACTH response to cortisol administration in PTSD." Psychoneuroendocrinology 31.4 (2006): 447-‐451.
4. Reincke, Martin. "Subclinical Cushing’s syndrome." Endocrinology and metabolism clinics of North America 29.1 (2000): 43-‐56.
5. Lagerquist, Lynn G., et al. "Cushing’s disease with cure by resection of a pituitary adenoma: Evidence against a primary hypothalamic defect." The American journal of medicine 57.5 (1974): 826-‐830.
6. Kirschner, Marvin A., Ralph D. Powell JR, and Mortimer B. Lipsett. "Cushing’s syndrome: nodular cortical hyperplasia of adrenal glands with clinical and pathological features suggesting adrenocortical tumor." The Journal of Clinical Endocrinology & Metabolism 24.10 (1964): 947-‐955.
7. Dimopoulos, Meletios A., et al. "Paraneoplastic Cushing’s syndrome as an adverse prognostic factor in patients who die early with small cell lung cancer." Cancer 69.1 (1992): 66-‐71.
8. Imai, Yutaka., et al. "Altered circadian blood pressure rhythm in patients with Cushing’s syndrome." Hypertension 12.1 (1988): 11-‐19.
9. Yehuda, Rachel, et al. "Relationship between 24-‐hour urinary-‐free cortisol excretion and salivary cortisol levels sampled from awakening to bedtime in healthy subjects." Life sciences 73.3 (2003): 349-‐358.
10. Johnson, Gordon F., et al. "Dexamethasone suppresion test (DST) and plasma dexamethasone levels in depressed patients." Psychiatry research 13.4 (1984): 305-‐313.
11. Fang, Victor S., et al. "Plasma ACTH and cortisol levels in depressed patients: relation to dexamethasone suppression test." Life Sciences 29.9 (1981): 931-‐938.
12. Nieman, L. K., et al. "The ovine corticotropin-‐releasing hormone (CRH) stimulation test is superior to the human CRH stimulation test for the diagnosis of Cushing’s disease." The Journal of Clinical Endocrinology & Metabolism 69.1 (1989): 165-‐169.
13. Yaneva, Maria, et al. "Midnight salivary cortisol for the initial diagnosis of Cushing’s syndrome of various causes." Journal of Clinical Endocrinology & Metabolism 89.7 (2004): 3345-‐3351.
14. Tsigos, Constantine, and George P. Chrousos. "Hypothalamic–pituitary–adrenal axis, neuroendocrine factors and stress." Journal of psychosomatic research 53.4 (2002): 865-‐871.

15. Ross, E. J., and D. C. Linch. "Cushing's syndrome—killing disease: discriminatory value of signs and symptoms aiding early diagnosis." The Lancet 320.8299 (1982): 646-‐649.
16. Nieman, Lynnette K., et al. "The diagnosis of Cushing's syndrome: an endocrine society clinical practice guideline." Journal of Clinical Endocrinology & Metabolism 93.5 (2008): 1526-‐1540.