cy 2017 final rule summary for radiation oncology · cy 2017 final rule summary for radiation...
TRANSCRIPT

CY 2017 Final Rule Summary for
Radiation Oncology
November 15, 2016
Presented for ACRO Members
Revenue Cycle Inc.

Contact Information
Revenue Cycle Inc.
1817 W. Braker Lane
Bldg. F, suite 200
Austin, Texas 78758
www.revenuecycleinc.com
(512) 583-2000

Presenters
Teri Bedard, BA, RT(R)(T), CPC
Director of Corporate Consulting
Amanda Klun, MBA, MSHA, RTT
Consultant

Housekeeping
• Everyone is muted
• If you have any questions please post under Q&A
• If you have an additional question that was not answered
during the webinar, please email us at
[email protected] and let us know you listened to
the ACRO final rule webinar
• Everyone who requests a pdf copy of presentation will be
emailed one

Disclaimer
This presentation was prepared as a tool to assist attendees in learning about documentation, charge
capture and billing processes. It is not intended to affect clinical treatment patterns. While reasonable
efforts have been made to assure the accuracy of the information within these pages, the responsibility
for correct documentation and correct submission of claims and response to remittance advice lies with
the provider of the services. The material provided is for informational purposes only.
Efforts have been made to ensure the information within this document was accurate on the date of
presentation. Reimbursement policies vary from insurer to insurer and the policies of the same payor
may vary within different U.S. regions. All policies should be verified to ensure compliance.
CPT® codes, descriptions and other data are copyright 2016 American Medical Association (or such
other date of publication of CPT®). All Rights Reserved. CPT® is a registered trademark of the
American Medical Association. Code descriptions and billing scenarios are references from the AMA,
CMS local and national coverage determinations (LCD/NCD).and standards nationwide.

Objectives of this Presentation
Basic Review of Reimbursement Settings
Discuss the Highlights HOPPS Final Rule Items
Discuss the MPFS Final Rule Items
Review MPFS Reimbursement Impact for 2017
Discuss the Quality Payment Program Final Rule per MACRA

HOPPS and MPFS Payment Systems
HOPPS
• Hospitals and ASCs
• Payments based on costs
• Adjusted by a wage index
• Grouped in APCs
• Example : Tx Plans
– 77295 & 77301
• Historically the same
payment rate under HOPPS
MPFS
• Physicians and Office Settings
• Codes have RVUs
• CF is applied to all RVUs
• GPCI’s
• Codes can be split into Global, TC,
26 payment
• Example: Tx Devices
– 77332, 77333, 77334
• Historically different payment
rates under MPFS

Federal Register
• Document actions of Federal agencies and forum for public
review and comment
• Publications include: Presidential Documents, Rule &
Regulations, Proposed Rules and Notices
Hospital Outpatient Prospective Payment
System (HOPPS)
Medicare Physician Fee Schedule
(MPFS)

Proposed vs. Final Rule
Proposed Rule:
• CMS plans, goals, solutions to
problems and proposed
rulemaking
• Opportunity for public to make
comments
Final Rule:
• Final legal effect after
consideration of comments
FINAL RULE
Consideration of Comments
+ Proposed
Rules

HOPPS Final Rule CY 2017
https://www.federalregister.gov/documents/2016/11/14/20
16-26515/medicare-program-hospital-outpatient-
prospective-payment-and-ambulatory-surgical-center-
payment

HOPPS 2017 Final Rule Highlights
• Increase in payments of 1.7%
• Changes to APCs, several codes are moving around and
reimbursements are adjusting
• Provider-based departments (PBDs)
– Excepted & Nonexcepted off-campus PBDs set
– Bill on UB04, paid at 50% of HOPPS fee & use G-codes
for treatments and IGRT
• Hospital Outpatient Quality Reporting (OQR) Program
– OP-33: External Beam Radiotherapy for Bone
Metastases

2016-2017 Hospital Outpatient Prospective Payment System National Average Course Example Impacts
Type HOPPS 2016 Course
Medicare Allowable
HOPPS 2017
Course Medicare
Allowable
2016 - 2017 Final
Rule Variance
2016- 2017
Final Rule %
Change
2D - 10 fxs $3,885.92 $4,060.50 $174.58 4.49%
3D - w/ imaging (33 fxs) $11,402.99 $11,850.26 $447.27 3.92%
3D - w/out imaging (33 fxs) $11,712.48 $12,238.06 $525.58 4.49%
IMRT - Simple 44 fxs $26,345.47 $26,042.12 ($303.35) -1.15%
IMRT - Complex 30 fxs $18,623.93 $18,415.06 ($208.87) -1.12%
SRS- Linac $9,180.54 $9,373.93 $193.39 2.11%
SRS- Cobalt Frame/Frameless (Same Day) $8,888.77 $9,062.50 $173.73 1.95%
SRS- Cobalt Frameless $9,180.54 $9,373.93 $193.39 2.11%
SBRT Linac 3 Fractions $11,499.46 $11,766.06 $266.60 2.32%
SBRT Linac 5 Fractions (Brain) $15,135.05 $15,378.67 $243.62 1.61%
SBRT - Cobalt 5 Fractions (Brain) $15,135.05 $15,378.67 $243.62 1.61%
Proton - 25 Fractions $31,611.91 $27,760.94 ($3,850.97) -12.18%
Prostate - HDR $11,490.68 $12,247.25 $756.57 6.58%
Prostate - LDR $9,442.13 $9,467.79 $25.66 0.27%
GYN - T&O - HDR $12,623.80 $13,464.05 $840.25 6.66%
GYN - Cylinder 1 Chan- HDR $5,445.00 $5,503.85 $58.85 1.08%
GYN - Cylinder Multi Chan - HDR $5,629.37 $5,697.75 $68.38 1.21%
APBI Single Channel - HDR $12,790.60 $12,638.10 ($152.50) -1.19%
APBI Multi Channel - HDR $12,974.97 $12,832.00 ($142.97) -1.10%
MPFS Final Rule CY 2017
https://www.federalregister.gov/documents/2016/11/15/2016-
26668/medicare-program-revisions-to-payment-policies-under-
the-physician-fee-schedule-and-other-revisions

Conversion Factor (CF) Update
• The Medicare Access and CHIP Reauthorization Act of 2015
(MACRA) put into law April 16, 2015
– CF to increase 0.5% each year through 2019
– CF 0% increase 2020 – 2025, additional payments based on
Quality Payment Program (MIPS)
– 2026 and beyond payments on participation in APMs
• 0.75% update for qualifying APMs
• 0.25% update for non-qualifying APMs
• Conversion Factor for 2017 = $35.8887
– Increase from 2016
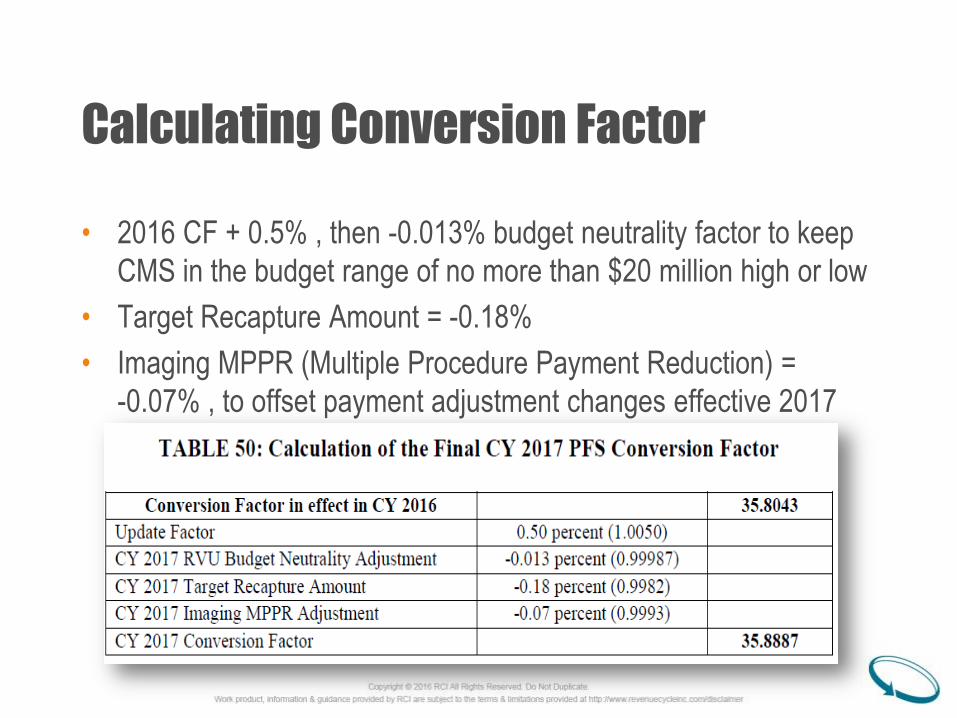
Calculating Conversion Factor
• 2016 CF + 0.5% , then -0.013% budget neutrality factor to keep
CMS in the budget range of no more than $20 million high or low
• Target Recapture Amount = -0.18%
• Imaging MPPR (Multiple Procedure Payment Reduction) =
-0.07% , to offset payment adjustment changes effective 2017

MPFS Payment
• Work: Relative time and intensity of service
• Practice Expense (PE): Costs of maintaining practice, i.e. rent, supplies,
equipment
• Malpractice (MP): Costs of malpractice insurance
• Geographic Practice Cost Index (GPCI): Adjusts for geographic variation
in costs
• Conversion Factor (CF): Converts to dollar amount

MPFS Payment Impact Table
TABLE 52: CY 2017 PFS Estimated Impact on Total Allowed Charges by Specialty*
(A)
Specialty
(B) Allowed
Charges (mil)
(C)
Impact
of Work
RVU
Changes
(D)
Impact
of PE
RVU
Changes
(E)
Impact
of MP
RVU
Changes
(F)
Combined
Impact**
Radiation Oncology $1,726 0% 0% 0% 0%
Radiation Therapy Centers $44 0% 0% 0% 0%
** Column F may not equal the sum of columns C, D, and E due to rounding.

Geographic Practice Cost Index (GPCI)
• Factor applied to the reimbursement equation to account for
geographic location of provider and variation in costs of
furnishing services in the particular location
• Required to be reviewed and if necessary adjusted every 3
years
• Per MACRA the Work GPCI floor of 1.0 extended thru
12/31/17
• CY 2017 reviews completed and few items to address
– Frontier States 1.0 PE GPCI
– Fee Schedule Adjustments for State of California

Frontier States PE GPCI
• Frontier States include
– Montana, Wyoming, North Dakota, South Dakota and
Nevada
• Due to population/size of each state
– At least 50% of counties are considered frontier and
population per square mile is less than 6
– CMS is capping the PE (Practice Expense) GPCI at 1.0
for the Frontier States even if the value would be lower
than the “floor value”

Adjustments to CA GPCIs
• Per MACRA, beginning CY 2017 fee schedule areas for CA
must be Metropolitan Statistical Areas (MSAs) as defined by
the Office of Management and Budget (OMB) as of
December 31 of the previous year
• All areas not located in an MSA must be treated as a single
rest-of-state fee schedule area
• Change from 9 current localities to 32 in CY 2017
• Values to be implemented gradually over 6 year period in
increments of 1/6 each year
– 58 counties in CA, 50 in transition in 2017

Valuation of Specific Codes
• Codes evaluated on annual basis, the RUC recommends values by February
10th of each year in order to be considered, if late then put off until next year
– CMS evaluates recommendations and also reviews claims data, review
of medical literature, comparative databases, comparison to other codes
and discussion with physicians and other healthcare professionals before
deciding whether or not to accept the RUC’s recommendations or
establish different values
• CY 2017 Rad Onc code changes
– G6011
– 77332, 77333 and 77334
– 77470
– 77778 and 77790

PE RVUs for G6011
• Per PAMA (Patient Access and Medicare Protection Act) signed into
law 12/18/15 G-codes used for Tx & IGRT must maintain assigned
definitions, inputs and values for CY 2017 and CY 2018
• Code G6011 (complex treatment up to 5 MeV energy) decrease in non-
facility PE for 2017
• Due to claims data – from 2 specialties
– Data to set rate in 2016 showed 51% billed by dermatology & 43%
by radiation oncology
– Most recent data 85% radiation oncology & ~6% dermatology
• Can’t revalue code as norm, so adjusted PE due to specialty indirect
PE values assigned to rad onc vs. dermatology
– Change in Indirect PE impacts overall PE RVU for code

Valuation of 77332, 77333 & 77334
• Identified through high expenditure specialty screening tool
– RUC recommended no changes
– CMS believes current RVUs overstate work involved in furnishing
service of treatment devices
• Based on research, CMS found 34% decrease in total time to provide
service for code 77332
– RUC did not incorporate time into recommended value
• Due to incremental increase in work value (simple, intermediate and
complex) the intermediate (77333) and complex (77334) codes change
as well
• Code 77332 down $15.23 & 77334 down $21.17, but 77333 up $44.63!

Valuation of 77470
• Identified through high expenditure specialty screening tool
• Accepted value recommended by RUC for 2017
• Believe description of code and vignette describe different
and unrelated treatment being performed by the physician
and clinical staff for a typical patient
– Disparity between work RVUs and PE RVUs
• Work RVU for 2017 is 2.03 down from 2.09
• CMS expressed serious concerns how 77470 is valued and
coded

Valuation 77778 & 77790
• CY 2015 definition for 77778 did not include handling and
loading
– CY 2016 it was added to definition of 77778, but Work
RVU was not adjusted to account for it
• CY 2016 Interim work RVU for 77778 = 8.00 & 77790 = 0
• Discrepancies between the RUC and specialty society as to
what is included in 77778
– Pre-service time is not calculated same between groups
• Work RVU for 2017 set at 8.78 and PE RVU raised, an
increase in payment of $47.44

TABLE 27: Finalized CY 2017 Work RVUs for New, Revised and Potentially Misvalued Codes
HCPCS
code Long Descriptor
CY 2016
Work RVU
Proposed
CY 2017
Work RVU
Final CY
2017 Work
RVU
CMS Work
Time
Refinement
77332 Treatment devices, design and construction;
simple (simple block, simple bolus) 0.54 0.45 0.45 No
77333
Treatment devices, design and construction;
intermediate (multiple blocks, stents, bite
blocks, special bolus)
0.84 0.75 0.75 No
77334
Treatment devices, design and construction;
complex (irregular blocks, special shields,
compensators, wedges, molds or casts)
1.24 1.15 1.15 No
77470
Special treatment procedure (eg, total body
irradiation, hemibody radiation, per oral or
endocavitary irradiation)
2.09 2.03 2.03 No
77778
Interstitial radiation source application,
complex, includes supervision, handling,
loading of radiation source, when performed
8.00 8.00 8.78 No
77790 Supervision, handling, loading of radiation
source 0.00 0.00 0.00 No

Sedation Values Removed from Codes
• Trend in which sedation for certain procedures is performed
by different physician than endoscopy
– Resource costs are not incurred by endoscopic
procedure, need to change values to reflect this
• Separate sedation codes created by CPT Editorial
Committee – based on age of patient and if provider did
both the procedure & sedation or just one or other
• Several placement codes & hyperthermia treatments with
0.25 work RVU decrease due to removal of sedation from
value

TABLE 26: Valuations for Services Minus Moderate Sedation
CPT code CY 2016 Work RVU CY2017 Final Work RVU
Use HCPCS code
G0500 to Report
Moderate
Sedation
(Y/N)
19298 6.00 5.75 N
31626 4.16 3.91 N
32553 3.80 3.55 N
43253 4.83 4.73 Y
49411 3.82 3.57 N
57155 5.40 5.15 N
77600 1.56 1.31 N
77605 2.09 1.84 N
77610 1.56 1.31 N
77615 2.09 1.84 N
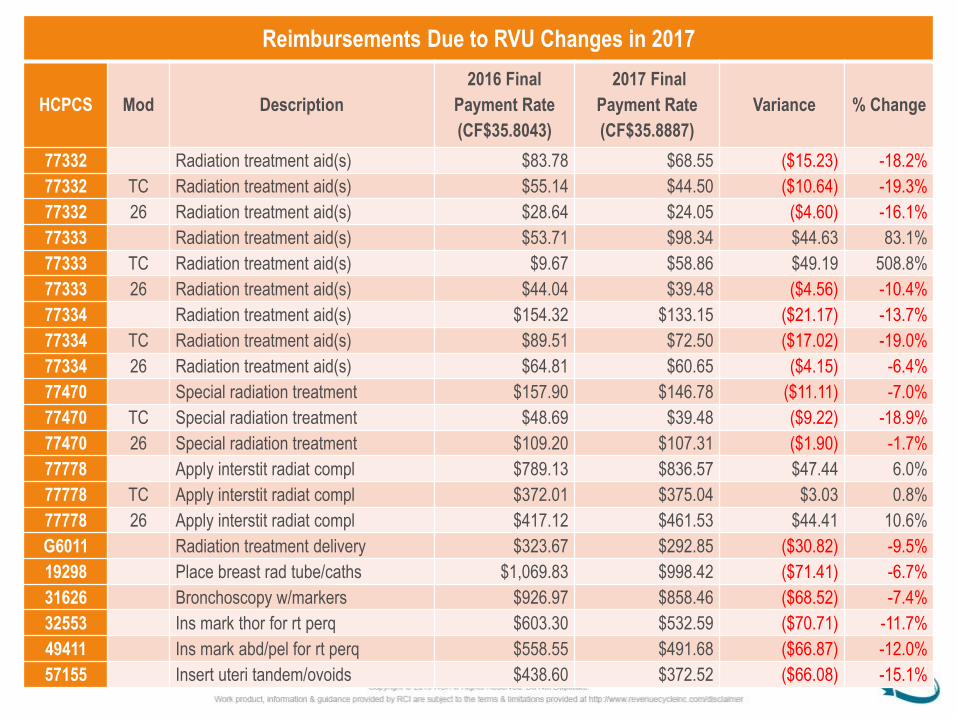
Reimbursements Due to RVU Changes in 2017
HCPCS Mod Description
2016 Final
Payment Rate
(CF$35.8043)
2017 Final
Payment Rate
(CF$35.8887)
Variance % Change
77332 Radiation treatment aid(s) $83.78 $68.55 ($15.23) -18.2%
77332 TC Radiation treatment aid(s) $55.14 $44.50 ($10.64) -19.3%
77332 26 Radiation treatment aid(s) $28.64 $24.05 ($4.60) -16.1%
77333 Radiation treatment aid(s) $53.71 $98.34 $44.63 83.1%
77333 TC Radiation treatment aid(s) $9.67 $58.86 $49.19 508.8%
77333 26 Radiation treatment aid(s) $44.04 $39.48 ($4.56) -10.4%
77334 Radiation treatment aid(s) $154.32 $133.15 ($21.17) -13.7%
77334 TC Radiation treatment aid(s) $89.51 $72.50 ($17.02) -19.0%
77334 26 Radiation treatment aid(s) $64.81 $60.65 ($4.15) -6.4%
77470 Special radiation treatment $157.90 $146.78 ($11.11) -7.0%
77470 TC Special radiation treatment $48.69 $39.48 ($9.22) -18.9%
77470 26 Special radiation treatment $109.20 $107.31 ($1.90) -1.7%
77778 Apply interstit radiat compl $789.13 $836.57 $47.44 6.0%
77778 TC Apply interstit radiat compl $372.01 $375.04 $3.03 0.8%
77778 26 Apply interstit radiat compl $417.12 $461.53 $44.41 10.6%
G6011 Radiation treatment delivery $323.67 $292.85 ($30.82) -9.5%
19298 Place breast rad tube/caths $1,069.83 $998.42 ($71.41) -6.7%
31626 Bronchoscopy w/markers $926.97 $858.46 ($68.52) -7.4%
32553 Ins mark thor for rt perq $603.30 $532.59 ($70.71) -11.7%
49411 Ins mark abd/pel for rt perq $558.55 $491.68 ($66.87) -12.0%
57155 Insert uteri tandem/ovoids $438.60 $372.52 ($66.08) -15.1%

Physician in PBDs
• Physicians working in provider-based departments
(excepted and nonexcepted) will continue to bill on
CMS1500 claim form
• Continue to report POS 19 (off-campus outpatient hospital)
code when services are performed at the PBD location
• Physicians will be reimbursed under MPFS facility rates
regardless if work is at an excepted or nonexcepted location
– CMS originally proposed to be paid per non-facility rates,
this was not finalized
– Both PBDs are considered facilities

CMS Recoupment of Overpayments
• Historically when an overpayment by CMS to a provider
occurred, CMS would use the National Provider Identifier
(NPI) to recoup overpayments from Medicare providers and
suppliers
– When not paid in full, referred to Department of Treasury
for further collection and CMS paid a fee for each referral
• Per ACA, CMS or MACs can now collect overpayments
without using the Treasury
• Now collections will be taken from TIN when collection from
NPI directly is unsuccessful

Example for Collecting Overpayment
“For example, a health care system may own a number of hospital
providers and these providers may share the same TIN while having
different NPI or Medicare billing numbers. If one of the hospitals in
this system receives a demand letter for a Medicare overpayment,
then that hospital (Hospital A) will be considered the obligated
provider while its sister hospitals (Hospitals B and C) will be
considered the applicable providers. This authority allows us to
recoup the overpayment of the obligated provider, Hospital A,
against any or all of the applicable providers, Hospitals B and C,
with which it, Hospital A, shares a TIN.”
Notification of Overpayment by CMS
• Notification provided in writing by CMS or Medicare
contractor – both NPI & TIN will not receive letter
• CY 2017 MPFS Final Rule, Medicare Financial
Management Manual, demand letters and MLN Matters
transmittals to provide updates and info on recoupment of
overpayments
• Prior to January 1, 2017 CMS will release information about
new process for recouping overpayments to Medicare
providers about the implementation through Medicare
Learning Network (MLN) or MLN Connects Provider eNews
article(s)

Medicare Advantage Program
• Providers and suppliers must be enrolled in Medicare with “approved
status” in order to render services to enrollees of Medicare Advantage
program
• Approved Status = enrolled and not revoked from Medicare
• Following plans must be enrolled, MA-PD plans, FDRs, PACE, Cost
HMOs or CMPs, demonstration programs, pilot programs, locum
tenens suppliers and incident-to suppliers
• Assists CMS in ensuring providers or suppliers are appropriate to
receive reimbursement
• If an organization or program does not ensure providers & suppliers
comply with requirements, possible sanctions or termination by CMS

Physician Self-Referral Law Updates
• Designated Health Services (DHS) are updated annually
• Four categories of services
– Clinical Laboratory Services;
– Physical Therapy, Occupational Therapy and Outpatient Speech-
Language Pathology Services;
– Radiology and certain other imaging services and
– Radiation Therapy Services and supplies
• No new codes added to Radiation Therapy service and supplies for 2017, 2
codes were removed
– 0019T, extracorporeal shockwave and A9545, I-131 tositumomab
• Full list at, https://www.cms.gov/Medicare/Fraud-and-
Abuse/PhysicianSelfReferral/List_of_Codes.html.

Office Space & Equipment Rental
• A physician cannot refer a Medicare beneficiary to another
entity with which that physician has a financial relationship
with and that entity cannot bill Medicare (or another
individual, entity or third party payer) or the beneficiary for
the referred services
• Concerns that per-click lease arrangements incentivize
referring physicians to over-refer & over-utilize services to a
lessee through which may or will receive revenue
– CMS proposed and finalized changes for CY 2017
Changes to Per-Click Arrangements
• CMS finalized that rental charges cannot be determined using a
formula based on per-unit of services charges in which the
services provided to patients are referred by the lessor to the
lessee
• Limits set-ups where the “lessor generates the payment from the
lessee through a referral to the lessee for a service to be
provided in the rented office space or using the rented
equipment”
• Arrangements are allowed when the referral for the service
provided in the rented office space or using the rented equipment
was not by the lessor

CY2017 Final Rule MPFS Global Non-Facility Course Compare
Type 2016 Global Course
CF = $35.8043
2017 Global Course
CF = $35.8887
2016 - 2017 Variance
Global Global %
Change
2D 10 fxs $5,099.61 $5,068.92 -$30.69 -1%
3D w/IGRT 33 fxs $17,266.62 $17,284.00 $17.37 0%
3D - w/out IGRT 33 fxs $13,663.64 $13,640.94 -$22.70 0%
IMRT 44 fxs $24,912.99 $25,095.53 $182.54 1%
IMRT 30 fxs $19,489.35 $19,614.25 $124.90 1%
SRS - Linac $5,743.01 $5,506.76 -$236.25 -4%
SBRT Linac 5 Fractions $12,079.65 $11,907.15 -$172.50 -1%
APBI Single Cath $7,214.92 $7,260.64 $45.72 1%
APBI MultiCath $10,065.30 $10,136.05 $70.74 1%
Prostate - HDR $7,212.06 $7,239.11 $27.05 0%
Prostate - LDR $3,157.94 $3,209.17 $51.23 2%
GYN T&O - HDR $5,309.42 $5,128.14 -$181.28 -3%
GYN Cyl 1 Chan HDR $3,535.32 $3,550.11 $14.79 0%
GYN Multi Chan HDR $4,430.78 $4,453.43 $22.65 1%

$-
$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
77280 77280-TC 77280-26 77285 77285-TC 77285-26 77290 77290-TC 77290-26
MPFS Simulation
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

$-
$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
77332 77332-TC 77332-26 77333 77333-TC 77333-26 77334 77334-TC 77334-26 77338 77338-TC 77338-26
MPFS Treatment Devices
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

$1.00
$10.00
$100.00
$1,000.00
$10,000.00
MPFS Dosimetry
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

$-
$20.00
$40.00
$60.00
$80.00
$100.00
$120.00
$140.00
$160.00
$180.00
77300 77300-TC 77300-26 77331 77331-TC 77331-26 77336 77370 77470 77470-TC 77470-26
MPFS MU Calcs, Special Dosimetry, Physics & Special Trmt Procedure
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

$-
$50.00
$100.00
$150.00
$200.00
$250.00
$300.00
$350.00
$400.00
77401 G6004 G6008 G6012 G6013 G6015 G6016
MPFS Treatment Delivery - EBRT & IMRT
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

$-
$20.00
$40.00
$60.00
$80.00
$100.00
$120.00
$140.00
77014 77014-TC 77014-26 G6001 G6001-TC G6001-26 G6002 G6002-TC G6002-26 G6017
MPFS Image Guidance
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

$-
$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
$700.00
77427 77431 77432 77435
MPFS Physician Treatment Management
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)
$-
$50.00
$100.00
$150.00
$200.00
$250.00
$300.00
$350.00
$400.00
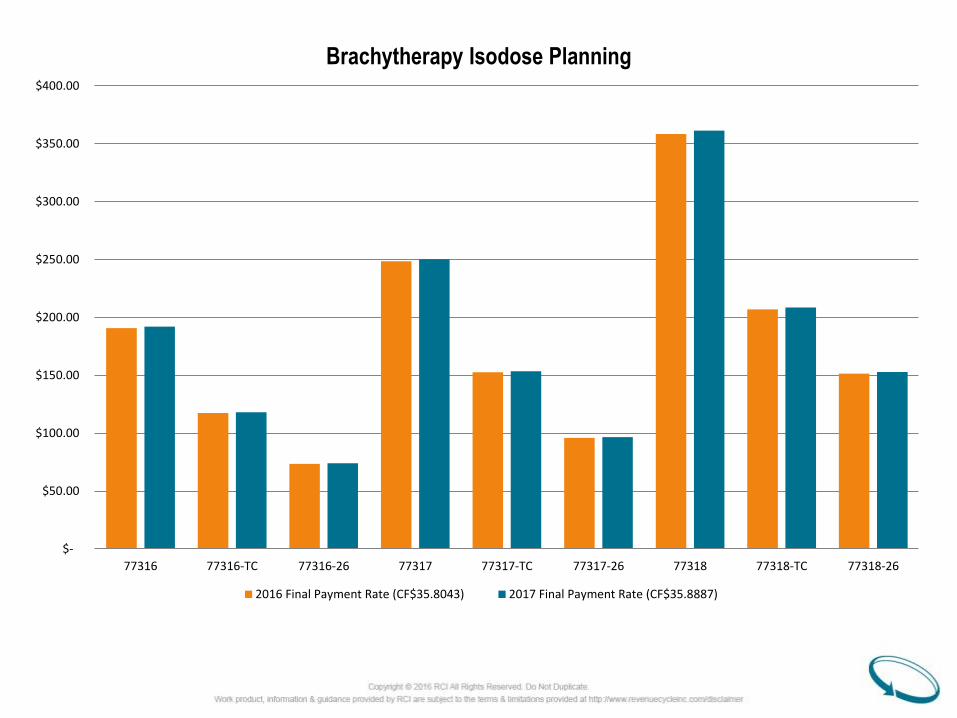
77316 77316-TC 77316-26 77317 77317-TC 77317-26 77318 77318-TC 77318-26
Brachytherapy Isodose Planning
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

$-
$200.00
$400.00
$600.00
$800.00
$1,000.00
$1,200.00
$1,400.00
$1,600.00
77372 77373
MPFS Stereotatic Treatment Delivery - SRS & SBRT
2016 Final Payment Rate (CF$35.8043) 2017 Final Payment Rate (CF$35.8887)

QUALITY PAYMENT PROGRAM
MACRA Final Rule CY 2017

https://www.federalregister.gov/documents/2016/11/04/201
6-25240/medicare-program-merit-based-incentive-
payment-system-and-alternative-payment-model-
incentive-under
Quality Payment Program Final Rule

Final Rule Response to “MACRA”
• Addresses changes to Physician Fee Schedule as signed
into law April 16, 2015 as part of Medicare Access and
CHIP Reauthorization Act of 2015 (MACRA)
• Released October 14, 2016
– Addresses provisions for changes to MPFS per MACRA
– Establishes Merit-based Incentive Payment System
(MIPS)
– Transition away from volume-based to value-based care
A Few Provisions of MACRA
• Repealed the Sustainable Growth Rate (SGR)
– No more proposed significant reductions to conversion factor (CF) each
year
• Established a timeline of payment factors going forward
– 2016 – 2019 CF raised 0.5% each year
– 2020 – 2025 CF update 0%, reimbursement based on MIPS reporting
– 2026 and beyond all about APMs & type of participation
• Qualifying APM = 0.75% update to CF
• Non-qualifying APM = 0.25% update to CF
• Develop Merit-based Incentive Payment System
– Reporting of measures beginning in 2017 for payment adjustments in
2019

Quality Payment Program (QPP)
• Beginning in 2017 reporting measures will determine
payment adjustments (+, - or neutral) in 2019
• QPP rewards values and outcomes through 2 means
– Advanced Alternative Payment Models (Advanced
APMs)
– Merit-based Incentive Payment System (MIPS)
• Only Eligible Clinicians will be able to participate
• Can participate individually or as a group
• Exemptions will apply as well

Who is an Eligible Clinician?
• Physicians
– MD, DO, Dentist, Chiropractor, Podiatrist & Optometrist
• Physician Assistant
• Nurse Practitioner
• Clinical Nurse Specialist
• Certified Registered Nurse Anesthetist
• Group that includes such professionals
• Hospital-based clinician who furnishes 75% or more of covered
pro services under POS 21(inpt) , 22 (opt) or 23 (ER)

Individual or Group
• MIPS eligible clinicians can report as individual or group
• Use TIN/NPI identifier for all 4 categories regardless of how
assessed
• Group reporting assessed as part of single TIN
– Which includes 2 or more eligible clinicians and 1 must
be a MIPS eligible clinician identified by an NPI and
Medicare billing rights are assigned to the TIN
– Data aggregated across the TIN
– Group must maintain status at all times during
performance period

Low-Volume Threshold
• Above threshold = eligible clinician
• Below threshold = exclusion from MIPS program
• Low-volume threshold criteria
– Medicare Part B charges < $30,000 or provides care to 100
or fewer Part B enrolled Medicare beneficiaries for a year
• Low-volume threshold applies to eligible clinicians practicing
under APMs
– If APM is Advanced APM the QA designation is not affected
• Groups can include low-volume threshold EC’s, performance
score applied across TIN, they will not receive any MIPS
payment adjustments

Four Participation Options in QPP
90-Consecutive Days Only
• Pick any 90-consecutive days & report measures
Partial Year
• Minimum 90- consecutive days AND
• Report more than one quality measure, improvement activity OR more than required measures in advancing care information
Full Year
• Report one measure in quality; one activity in improvement activities performance category OR report required measures in advancing care information performance category
Participate in Advanced APM
• 5% Bonus payment in 2019
Any eligible clinician chooses not to report any measures or
activities in 2017, -4% payment adjustment applied to every
claim in 2019!

Performance Categories
• Quality
• Improvement Activities
• Advancing Care Information
• Cost = 0% value in 2017 (transition year) for everyone

Full Participation vs. Threshold
• Full participation means
– Quality category 6 quality measures OR 1 specialty-specific
or subspecialty-specific measure set.
– Advancing Care Information 5 measures reported
– Improvement Activities up to 4 activities are reported
• Meeting Threshold means
– Any eligible clinician reports 1 out of 6 Quality measures,
attests to at least one Improvement Activity or reporting on
required measures in Advancing Care Information will meet
the MIPS threshold of 3 points and receive neutral payment
adjustment

Integrated Performance Categories
• Quality - 2017 category weight = 60%
– Replaces PQRS
– Report up to 6 quality measures, including an outcome
measure, for minimum of 90 consecutive day period
– Groups using Web interface will report 15 quality
measures for the full year
– Groups in APMs will report measures through APM
– General Oncology (19 measures) and Radiation
Oncology (4 specific measures) – Rad Onc under
Oncology per comments received

24b. Radiation Oncology
Title Prostate Cancer: Avoidance of Overuse of Bone Scan for Staging Low Risk
Prostate Cancer Patients
NQF#/Quality #: 0389/102
Description:
Percentage of patients, regardless of age, with a diagnosis of prostate cancer at
low (or very low) risk of recurrence receiving interstitial prostate brachytherapy, OR
external beam radiotherapy to the prostate, OR radical prostatectomy, OR
cryotherapy who did not have a bone scan performed at any time since diagnosis
of prostate cancer
Measure Steward: Physician Consortium for Performance Improvement Foundation (PCPI)
Measure Type: Process
Measure Domain: Efficiency and Cost Reduction
Data Submission
Method: Registry, EHR

24b. Radiation Oncology
Title Oncology: Medical and Radiation - Pain Intensity Quantified
NQF#/Quality #: 0384/143
Description:
Percentage of patient visits, regardless of patient age, with a diagnosis of cancer
currently receiving chemotherapy or radiation therapy in which pain intensity is
quantified
Measure Steward: Physician Consortium for Performance Improvement Foundation (PCPI)
Measure Type: Process
Measure Domain: Person and Caregiver Centered Experience and Outcome
Data Submission
Method: Registry, EHR

24b. Radiation Oncology
Title Oncology: Medical and Radiation – Plan of Care for Pain:
NQF#/Quality #: 0383/144
Description:
Percentage of visits for patients, regardless of age, with a diagnosis of cancer
currently receiving chemotherapy or radiation therapy who report having pain
with a documented plan of care to address pain.
Measure
Steward: American Society of Clinical Oncology
Measure Type: Process
Measure Domain: Person and Caregiver Centered Experience and Outcome
Data Submission
Method: Registry

24b. Radiation Oncology
Title Oncology: Radiation Dose Limits to Normal Tissues:
NQF#/Quality #: 0382/156
Description:
Percentage of patients, regardless of age, with a diagnosis of breast, rectal,
pancreatic or lung cancer receiving 3D conformal radiation therapy who had
documentation in medical record that radiation dose limits to normal tissues
were established prior to the initiation of a course of 3D conformal radiation for
a minimum of two tissues
Measure Steward: American Society of Clinical Oncology
Measure Type: Process
Measure Domain: Patient Safety
Data Submission
Method: Claims, Registry

Integrated Performance Categories
• Improvement Activities - 2017 category weight = 15%
– New category
– 93 activities to select from in eight subcategories
• Achieving Health Equity, Behavioral and Mental Health, Beneficiary
Engagement, Care Coordination, Emergency Response & Preparedness,
Expanded Practice Access, Patient Safety & Practice Assessment and
Population Management
– Attest to completing up to 4 improvement activities, for minimum of 90 consecutive
day period
– Groups with fewer than 15 participants, attest completing up to 2 improvement
activities, for minimum of 90 consecutive day period
– Groups in APMs will automatically receive points based on requirements through
participation in the APM and will be assigned full credit for current APMs
– Eligible clinicians in any other APM will automatically earn half credit and can
report more activities to increase score

Integrated Performance Categories
• Advancing Care Information - 2017 category weight = 25%
– Replaces Meaningful Use
– Fulfill required measures for minimum of 90 consecutive day period
• Security Risk Analysis
• E-Prescribing
• Provide Patient Access
• Send Summary of Care
• Request/Accept Summary of Care
– Choose to submit up to 9 measures for minimum of 90 consecutive day period OR
– If measures do not apply, then no reporting necessary (ex. hospital-based eligible
clinicians)
– The EHR edition used to submit data will determine which set of measures to
select from, link on CMS website at https://qpp.cms.gov/measures/aci can help
determine which edition an eligible clinician uses

Integrated Performance Categories
• Cost
– Replaces Value-Based Modifier
– No data submission required
– Calculated per adjudicated claims
– Will be counted starting in 2018

TABLE 3: Data Submission Mechanisms for MIPS Eligible Clinicians Reporting Individually as TIN/NPI
Performance Category/Submission
Combinations Accepted Individual Reporting Data submission Mechanisms
Quality Claims, QCDR, Qualified registry, EHR
Cost Administrative claims (no submission required)
Advancing Care Information Attestation, QCDR, Qualified registry, EHR
Improvement Activities Attestation, QCDR, Qualified registry, EHR
TABLE 4: Data Submission Mechanisms for Groups
Performance Category/Submission
Combinations Accepted Group Reporting Data submission Mechanisms
Quality
QCDR, Qualified registry, EHR, CMS Web Interface (groups of 25 or more), CMS-
approved survey vendor for CAHPS for MIPS (must be reported in conjunction with
another data submission mechanism.) and Administrative claims (For all-cause
hospital readmission measure - no submission required)
Cost Administrative claims (no submission required)
Advancing Care Information Attestation, QCDR, Qualified registry, EHR, CMS Web Interface (groups of 25 or more)
Improvement Activities Attestation, QCDR, Qualified registry, EHR, CMS Web Interface (groups of 25 or more)

Potential Payment Adjustments
More information about the Quality Payment Program
available at https://qpp.cms.gov/
Graphic courtesy of CMS.gov

Payment Adjustments
• Meet threshold of 3.0 points, no adjustment for CY 2019
– Considered neutral
• Qualifying payments not made in lump sum, applied as an
adjustment factor on a per claim basis
• Applied to any Medicare Part B payments for any items and
services furnished by MIPS eligible clinician
• Years 2019 – 2024 additional bonus payments available
– Only if final score is above additional criteria established
each year
– Additional payment % determined by Secretary

Alternative Payment Models (APMs)
• Transitioning eligible clinicians to APMs is overall goal
– Moves healthcare from volume-based to value-based
• Two types of APMs were finalized
– Advanced APMs
– Other Payer Advanced APMs
• Specific criteria for each to be considered
• New APMs will be available in 2017 and 2018

Advanced APMs Criteria
• To qualify must meet all of the following criteria:
– The APM must require participants to use CEHRT;
– The APM must provide for payment for covered
professional services based on quality measures
comparable to those in the quality performance category
under MIPS and;
– The APM must either require that participating APM
Entities bear risk for monetary losses of a more than
nominal amount under the APM, or be a Medical Home
Model expanded under section 1115A(c) of the Act.

Other Payer Advanced APM Criteria
• Arrangement with a commercial payer or Medicaid & must meet all
criteria
– The payment arrangement must require participants to use
CEHRT;
– The payment arrangement must provide for payment for covered
professional services based on quality measures comparable to
those in the quality performance category under MIPS and;
– The payment arrangement must require participants to either bear
more than nominal financial risk if actual aggregate expenditures
exceed expected aggregate expenditures; or be a Medicaid
Medical Home Model that meets criteria comparable to Medical
Home Models expanded under section 1115A(c) of the Act.

Advanced APMs for CY 2017
• Released by CMS on 10/25/16
– Comprehensive ESRD Care Model (Large Dialysis
Organization (LDO) arrangement)
– Comprehensive ESRD Care Model (non-LDO arrangement)
– Comprehensive Primary Care Plus CPC+
– Medicare Shared Savings Program ACOs - Track 2
– Medicare Shared Savings Program ACOs - Track 3
– Next Generation ACO Model
– Oncology Care Model (two-sided risk arrangement)

Anticipated Advanced APMs for 2018
• Re-opening applications for new practices and payers in CPC+ &
Next Generation ACO Model
• CMS anticipates incentive payments may be available through
following models in 2018
– ACO Track 1+
– New voluntary bundled payment model
– Comprehensive Care for Joint Replacement Payment Model
(Certified Electronic Health Record Technology (CEHRT)
track)
– Advancing Care Coordination through Episode Payment
Models Track 1 (CEHRT track)

Qualifying Participants (QP)
• Eligible clinicians participating in Advanced APMs who have sufficient % of
patients or been paid sufficient amount of payments through APM
• 5% bonus payment beginning 2019 – 2024
• Even services provided in CAHs, RHCs and FQHCs will be counted
• Thresholds will be set to become a QP
– Medicare APM
• Based on Part B payments or # of patients who had services under
Part B
– All Payer Combination Option (uses Medicare APM & Other Payer
Advanced APMs option) – first payment in 2021
• Must participate in Advanced APM under Medicare & submit info to
CMS to determine is thresholds are met

QP Identifier
• Eligible clinicians will be identified by:
– Unique APM participant identifier
– APM entity
– TIN/NPI combinations
• If eligible clinician participates in multiple Advanced APMs
but does not meet threshold in a single one, will be
assessed across combined participation
• CMS will accelerate timeline to let eligible clinicians are
excluded from MIPS prior to need for info submitted

TABLE 14: APM Entity Submission Method for Each MIPS Performance Category
MIPS
Performance
Category
APM Entity Eligible Clinician Submission Method
Quality The APM Entity group submits quality measure data to CMS as required under
the APM.
Cost No data submitted by APM Entity group to MIPS.
Improvement
Activities
No data submitted by APM Entity group to MIPS unless the assigned score at the
MIPS APM level does not represent the maximum improvement activities score,
in which case the APM Entity may report additional improvement activities using a
MIPS data submission mechanism.
Advancing
Care
Information
Shared Savings Program ACO participant TINs submit data using a MIPS data
submission mechanism. Next Generation ACO Model and other MIPS APM
eligible clinicians submit data at either the individual level or at the TIN level using
a MIPS data submission mechanism.

Questions?