cyclosporine: immunology, pharmacology and therapeutic uses
TRANSCRIPT

SURVEY OF OPHTHALMOLOGY VOLUME 31 . NUMBER 3. NOVEMBER-DECEMBER 1986
THERAPEUTIC REVIEW JOEL MINDEL AND SAIICHI MISHIMA, EDITORS
Cyclosporine: Immunology, Pharmacology Therapeutic Uses
ROBERT B. NUSSENBLATT, M.D., AND ALAN G. PALESTINE, M.D.
and
Abstract. Human and animal investigations since the mid- 1970s have demonstrated thr ellec- tiveness of qclosporine (Cs,\) as an immunosuppressive agent. In the area of transplantation immunity, it has been shown to enhance success of renal, hone marrow. and li\,er transplanta- tion. Moreover. certain models of autoimmune disease have heen effectively treated with CL\. and a number of studies have reported encouraging results \vith CsA therapy for ocular inflam- matory disorders. notably BehCet’s disease. The most serious side effects of CsA are nephrotosi- city and hypertension; thus. conservative dosages of the drug and careful monitoring of renal function during treatment are recommended. The purpose of this review is to provide clinicians and researchers with a clear perspective of both the potential benefits and shortcomings of this .tgent (Surv Ophthalmol 31:159-169, 1986)
Key words. cyclosporine l cornea1 transplantation l immunoloqy l
immunosuppressive agents l ocular inflammatory disorders
Cyclosporine (CA) has presented the clinician
and researcher with a twofold opportunity, opening
the possibility of new treatments for ocular inflam- matory disorders and providing a new tool for prob-
ing the immune system. Cyclosporine’s story begins in 1969-70 in the Microbiology Department of San-
doz, Ltd., in Basel, Switzerland, when two new strains of fungi imperfecti were isolated from soil
samples taken from Wisconsin and Norway.12 The fungal extracts showed a narrow spectrum of anti- fungal activity and were low in toxicity. Because of
these observations, compound 24-556 entered into a screening program. In <January 1972, Jean Bore1 discovered the marked immunosuppressive effects of this metabolite, and so began a most interesting saga. This review summarizes current information concerning this agent, so that the ophthalmic re-
searcher and clinician can better put into perspec-
tive its great potential as well as its shortcomings.
Pharmacology and Metabolism
Cvclosporinc (Fig. 1) is a cyclic peptide contain-
ing eleven amino acids with a total molecular weight
of 1202.“,!“’ Uncharged at physiologic pH and in-
soluble in water, it is soluble in ethanol or it can be
dissolved in olive or sesame oil at 60°C:. It will then
remain in solution at room temperature. These solu-
bility characteristics substantially influence the
clinical use of this drug. The oral preparation is an
olive oil solution with 12.5% ethanol which must be
dispersed in juice or milk before ingestion.“” Conse-
quently, oral absorption is variable and slow. Ap-
proximately 30% of the oral dose is absorbed, with a
peak blood level 2-4 hours after ingestion.’ “I How-
159

160 Surv Ophthalmol 3 l(3) November-December 1986 NUSSENBLATT, PALESTINE
C”39
!
C”3\ ,C”3 H’ \cH2 I
f” C”3 C”3 HO CH
7”2 f”3 ‘$ \/\
CH3 F” C”3
CHj- ~-CH-CO-N-CH-C-~-CH-CO-
C”3, co
C”3
,CH-CH2-iH
CH3 : I
Ii
OC-CH - N-CO-CH-ti-CO-CH-N-
iH3 ii LH*
CH3 CH3
b
i-C”3
ti I
ii-CH-k-CO-C”
,tH CH3 ‘CH3
iH2
tH
c& ‘cti3
Fig. I. Structure of cyclosporine A, a cyclic peptide.
ever, the absorption may vary between 4% and 60%, and it appears to improve after extended use
in some patients. A single 600 mg oral dose will
produce a peak plasma concentration of 240 to 1250 ng/ml (mean 538 ng/ml).6 Therefore, absorption
varies among individuals as well as over time in a
single patient. The variability in oral drug availabil-
ity is one of the factors which influences individual adjustment of the dose for each patient. A relation-
ship of absorption to meals has not been reliably
established,3gJ5 but bile and the enterohepatic circu-
lation do affect absorption. An intravenous formula-
tion containing ethanol and polyoxyethylated castor oil is available, but is rarely needed in the treatment
of autoimmune diseases. ‘O No commercially avail-
able topical cyclosporine formulation is currently
available. Although this has potential use in oph- thalmology, the lipid solubility and uncharged na-
ture of the molecule make ocular penetration difli-
cult and prevent the use of the usual ophthalmic vehicles.
A radioimmune assay is available to measure
nannogram concentrations of CsA, which, in the blood, is largely bound to erythrocytes.50 This bind- ing is temperature-dependent and can markedly in-
fluence the results of a plasma CsA concentration assay. CsA leaves the erythrocyte as the tempera- ture decreases.5* It is therefore important to either assay whole blood CsA concentrations or to always allow the blood to equilibrate at 25°C for two hours prior to plasma separation so that the plasma con- centration consistently reflects the “true” blood concentration. At 25”C, the blood concentration is approximately live times the measured plasma con- centration. 6’ Erythrocyte CsA binding is saturated
above 5000 nglml, which is considerably above the therapeutic range. There is a biphasic decrease in
blood and tissue concentrations of CsA; the mean elimination half-lives are 1.2 hours and 27 hours in
normal individuals.‘j An elevated serum bilirubin
and associated liver dysfunction will prolong the
half-life, and the elimination of CsA is not affected
by renal disease. The clearance of the drug is 6-7 ml/min/kg.83J4
CsA is most highly concentrated in lipid contain-
ing tissues. The highest concentrations are in the
fat, breast, pancreas, liver, kidney and lymphoid
tissue whereas the lowest concentrations are in brain and muscle.‘J8 The concentration in the fat is
approximately 10 times the plasma concentration.
Hence, a large reserve of drug is present. The con-
centration in the aqueous humor in patients with chronic flare is 40% of the plasma concentration.
CsA is in extremely low and non-therapeutic con-
centrations in the cerebrospinal fluid.77 CsA metabolism involves oxidative alterations by
the cytochrome P-450 microsomal enzymes of the
liver.5J3 The ring structure remains intact during metabolism. A number of the side-chains of the ami- no acids are hydroxylated or N-demethylated; over 15 metabolites of CsA have been identified. Only
0.1% of the CsA is excreted unchanged.25,g8 Excre- tion occurs primarily through the bile and intes- tines, although a small amount (6%) of the drug and its metabolites are excreted in the urine.25
The pharmacology ofCsA relates to possible drug interactions. The recommended clinical plasma concentration was initially 100-300 ng/ml. How- ever, in view of side-effects such as nephrotoxicity, this has been lowered to 50-100 ng/ml. Drugs such
CYCLOSPORINE
as phenobarbital or phenytoin, which increase the
activity of the hepatic microsomal enzymes, will in-
crease the rate of metabolism of the drug, thereby lowering plasma concentrations.“.” Isoniazid, ri-
fampin, and intravenous sulpha/trimethoprim have
also been reported to decrease circulating GSA con- centrations.‘“.‘” Ketoconazole is an inhibitor of the
hepatic microsomal enzymes and therefore will in-
crease the plasma GSA concentration when admin-
istered concomitantly.” Cimetidine and erythromy-
tin may also increase the plasma concentration.“’ CsA has an additive toxic effect with known nephro-
toxic drugs. Renal toxicity is the major clinical side-
effect of cyclosporine and drugs such as gentamicin,
amphotericin B, co-trimoxazole, and nonsteroidal
antiinflammatory agents will markedly enhance
CsA induced nephrotoxicity.“H.q” These drugs may
be clinically necessary at times, but should be avoid-
ed if alternate compounds are clinically acceptable.
Mechanism of Action of Cyclosporine
CsA has been an effective immunologic probe which has been used to dissect the immune rc-
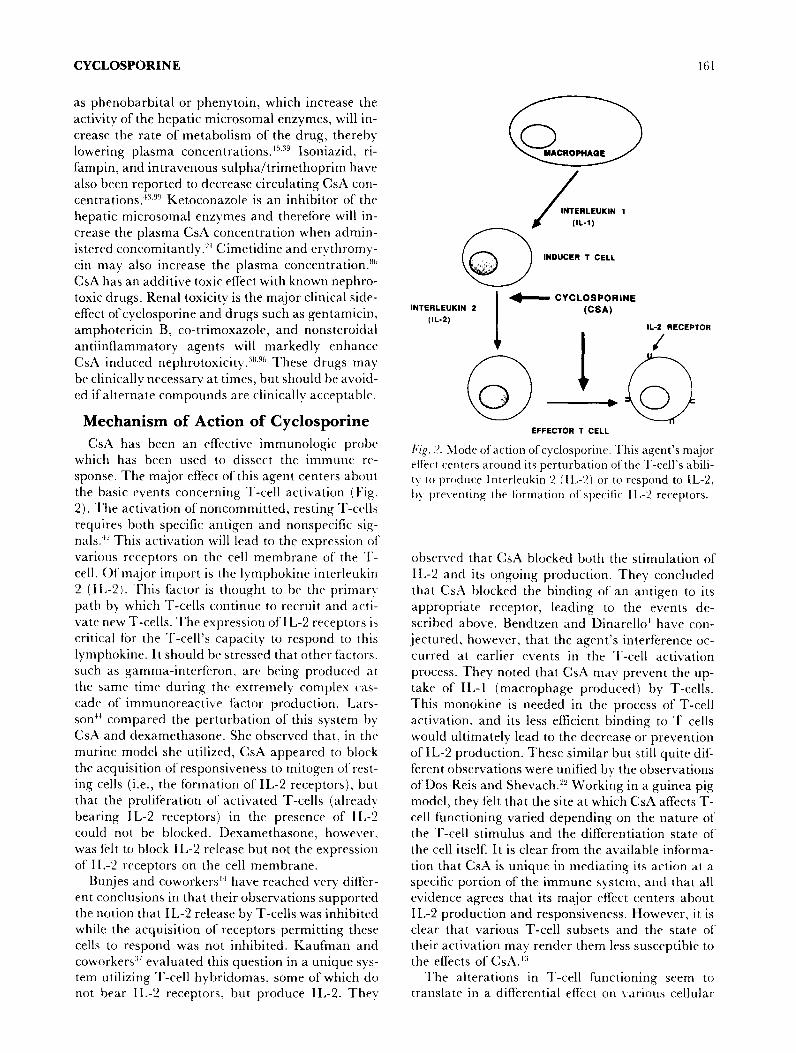
sponse. The major effect of this agent centers about the basic events concerning T-cell activation (Pig.
2). The activation of noncommitted, resting T-ccalls
requires both specific antigen and nonspecific sig-
nals.” This activation will lead to the expression 01‘ various receptors on the cell membrane of the T-
cell. Of major import is the lymphokine interlrukin 2 (IL-2). This factor is thought to be the primar).
path by which T-cells continue to recruit and acti-
vate new T-cells. The expression of IL-2 receptors is
critical for the T-cell’s capacity to respond to this
lymphokine. It should be stressed that other factors, such as gamma-interferon, are being produced at the same time during the extremely complex (‘as-
cadc of immunoreactive f’actor production. Lars-
son” compared the perturbation of this system b)
CsA and dexamethasone. She observed that, in the
murine model she utilized, CsA appeared to block
the acquisition of responsiveness to mitogen of rest- ing cells (i.e., the formation of IL-2 receptors), but
that the proliferation of activated T-cells (already
bearing IL-2 receptors) in the presence of IL-2 could not be blocked. Dexamethasone, howeLTer.
was f‘elt to block IL-2 release but not the expression
of IL-2 receptors on the cell membrane. Bunjes and coworkers” have reached very ditI’er-
ent conclusions in that their observations supported the notion that IL-2 release by T-cells was inhibited while the acquisition of receptors permitting these cells to respond was not inhibited. Kaufman and
coworkers3’ evaluated this question in a unique sys- tem utilizing T-cell hybridomas, some of which do not bear IL-2 receptors. but produce IL-2. They
161
a 0 YACROPtlAQE
INTERLEUKIN I
INDUCER T CELL
IL-2 RECEPTOR
/
+ CYCLOSPORINE INTERLEUKIN 2 t-4
(IL-2)
. EFFECTOR T CELL
Fig. 2. Mode of action of’cyclosporine. This agent’s major effect centers around its perturbation ofthe T-cell’s abili- ty to produce Interleukin 2 (11,-Z) or to rrspond to IL-2, hy prevrnting the formation of specific I L-2 receptors.
observed that CsA blocked both the stimulation of
IL-2 and its ongoing production. They concluded
that CsA blocked the binding of an antigen to its
appropriate receptor, leading to the events de-
scribed above. Bendtzen and Dinarello’ have con-
jectured, however, that the agent’s interference oc-
curred at earlier events in the T-cell activation
process. They noted that Cspl may prevent the up- takr of IL-1 (macrophage produced) by T-cells. This monokine is needed in the process of T-cell
activation, and its less efficient binding to T cells
would ultimately lead to the decrease or prevention of IL-2 production. These similar but still quite dif-
ferent observations were unified by the observations of DOS Reis and Shevach.‘LY Working in a guinea pig
model, they felt that the site at which CsA affects T- cell functioning varied depending on the nature of
the T-cell stimulus and the differentiation state of the cell itself: It is clear from the available informa-
tion that CsA is unique in mediating its action at a specific portion of the immune system, and that all evidence agrees that its major effect centers about IL-2 production and responsiveness. However, it is clear that various T-cell subsets and the state of’ their activation may render them less susceptible to
the effects of CsA.” The alterations in T-cell functioning seem to
translate in a differential effect on various cellular

162 Surv Ophthalmol 3 l(3) November-December 1986 NUSSENBLATT, PALESTINE
components of the immune system. The presence of CsA has a variable effect on B-cell functioning. Lil-
lehoj et a15’ found that CsA had no effect on B-cell
proliferation to T-cell independent antigens, nor did
it inhibit the expression of B-cell activation markers. In the S-antigen model for uveitis, Chan and col-
leagues9 noted that specific antibody production
was not inhibited by GSA administration, but rather
that the time needed to reach peak levels was some- what longer than that needed in control animals.
Cytotoxic cells have been noted to be affected by CsA administration, apparently preventing the in-
duction of this T-cell subset.‘O’ We have noted that
the number of inducer T-cells in the draining lymph
node of the site of antigen immunization was mark-
edly diminished by CsA therapy.@ Of interest has
been the sparing of suppressor cells by CsA. Leap- man and coworkers4’ felt that in humans, while oth-
er subpopulations were inhibited, suppressor cells
were spared but not induced when CsA was added
in vitro. Hutchinson and colleagues”” noted a spar-
ing of donor-specific suppressor cells in rats receiv-
ing heart allografts. Others, however, have suggest-
ed that CsA administration may induce suppressor
cells, Wang and colleagues”’ felt that this mecha-
nism explained the longlasting unresponsiveness
seen in CsA-treated mice immunized vsith target
cells, which usually induce highly cytolytic cells.
Further, Hess and coworkers, studying human cells,
observed a nylon-wool adherent suppressor cell
which was induced by CsA administration30
The molecular basis for these effects has only re- cently begun to be elucidated. The evidence to date
would not suggest that a specific CsA receptor exists on T-cell membranes. 48 However, Merker and
Handschumacher 54 have reported a cytoplasmic macromolecule that does appear to bind with CsA.
It is clear that CsA’s effect is not just at the mem-
brane. CsA has been shown to inhibit lymphokine- specific mRNA and new protein synthesis.“‘,R’
Animal Studies
Calm and White,” as well as Green and Allison,‘8 noted the extensive prolongation of renal allografts
with CsA therapy, while others have shown similar results with cardiac allografting.~g,4’ In experimen-
tal lung transplantation in dogs, the addition ofCsA
leads to longterm normal lung function and no evi-
dence of rejection in some animalsg7 CsA treatment was also most effective in altering graft-versus-host
and host-versus-graft responses in rats-j2
An area ofgreat interest has been the basic under-
lying perturbations of the immune system which Iead to the clinical entity recognized as an autoim-
mune condition. Experimental allergic encephalo-
myelitis (EAE), induced by immunization with cen-
tral nervous system derived basic protein, a
paralytic condition, has been studied extensively. Bore1 and coworkers” demonstrated that CsA effec-
tively prevented the expression of EAE. Several re-
searchers have confirmed these observations, with
dosages usually at 15 mglkgfday. Cs.4 has also been noted to have a beneficial effect even when adminis-
tered with a delay of several days after immuniza-
tion,” and the agent was effective in preventing the
adoptive transfer of EAE with activated lympho-
cytes.’
The effect of CsA on the naturally occurring lu- pus-like disorder in certain mice has also been inves-
tigated. CsA treatment of NZB/W mice appears to
suppress anti-DNA titers normally noted in these
animals as they develop disease. Jones and Harris””
have also reported that CsA therapy improved the survival of NZB/W mice. A most important area of
investigation was carried out by Laupacis and col- leagues,+j who evaluated BB Wistar rats for their
spontaneous development ofdiabetes. In this study,
75% of control animals developed insulin-depen-
dent diabetes between 60 and 120 days of age while none of the 40 CsA treated rats became diabetic.
While control rats developed partial or complete
destruction of their islets of Langerhans by lympho- cytic infiltration, CsA-treated rats had normal pan-
creases.
Two major areas of investigation revolve around
the effects of CsA administration on transplantation models and those of autoimmunity, both induced and naturally occurring. This discussion will deal separately with the nonocular and ocular observa- tions.
NONOCU~R ANIMAL STUDIES
It should be emphasized that some models of pu-
tative autoimmune disease were not effectively treated with CsA; such an example is the spontane- ous autoimmune thyroiditis seen in the obese strain
of chickens. Wick and colleagues’02 observed that CsA therapy led to the development of much more severe disease as well as higher titers of thyroglobu-
lin autoantibodies. Transplantation immunity has been an area in-
fluenced greatly by CsA. Bore1 and coworkers” OCULAR ANIMAL STUDIES _ _,
early on demonstrated the effectiveness of CsA in The usefulness of CsA in preventing cornea1 graft delaying skin graft rejection in mice and graft-ver- rejection has been extensively evaluated. Coster and sus-host disease in mice and rats. Organ transplant Shepherd and their colleagues’0,g3 treated one group studies are too numerous to fully list. However, of outbred Dutch rabbits with 25 mg/kg/day of CsA

CYCLOSPORINE
after 6 mm penetrating grafts. Another group re-
ceived a 1 O/O CsA eye drop five times a day. Addi-
tionally, skin grafts were performed to ensure rejec- tion. In this study, prolongation ofthe cornea1 grafts were seen in all animals receiving systemic therapy.
This observation was confirmed by Bell and col- leagues.’ However, the topically applied CsA did
not appear to prolong cornea1 graft survival, but this was thought to he related to the need for skin graft-
ing to initiate the rejection. Salishury and Geh-
hardt’“’ gave a single retrobulbar injection ofCsA to
New Zealand white rabbits at the end of kerato-
plasty. Four (45%) of nine allografts treated with
Csi4 survived more than 70 days, while all untreated eyes rttjcctchd within 40 days. They observed that
CsA was less effective in suppressing allograft rqjec-
tion in heavily vascularized, inflamed graft sites.
Hunter and coworkers,” reported that a 1% CsA solution in arachis oil given topically five times dail)
significantly prolonged graft survisal. Kana and as-
sociates, using both a subconjunctival and topical route, confirmed the above observations? Roussel
and colleagues”’ took the novel approach of’deli\.cr-
ing a L 9’0 CM solution locally to the cornea bl- using
a polypropylene tube connected to a subcutaneous
osmotic pump. This method delivered CsA to the cornea1 surface at a continuous rate of 2.5 &%r (2.5
~gihr) fbr 28 day-s. This approach signi~ca~ltl~ de-
layed graft re_jection compared to controls. Addi-
tionally. this topical s!‘stem, when delivering a markedly higher CM dose (500 pgihr) appeared to
reverse cornea1 graft rcjrction after it began.“” How-
ever, because of‘thr relatively large ocular surface in the rabbit. systemic absorption can occur. thcrch)
making these results difficult to interpret without
systemic. blood levels, w*hich were not performed. An important consideration has been the ocular
penetration of local Cs/\ administration. Mosteller
and colleaguesi” observed that a 10% GSA ointment
preparation could obtain a peak of900 ng/ml in the cornea three hours after administration. Relatively-
low lrvc~ls were measured in the aqueous humor.
suggesting a cornea1 strctmal pooling of this hydro- phobic agent. Wiederhott and coworkers”” felt that therapeutic levels could be found in the aqueous
humor as well as the u\:ea/retina. \Ve”’ have noted,
as have Mosteller and colleagues,‘” that relativel)
low levels or‘ C&A penetrated intraocularly, and not at a therapeutically cfiactive dose.
The effects of CS~~ on an experimental herprtic
stromal keratitis model \vas investigated by Boisjol) and colleagues.’ They noted that the severity of stro- ma1 disease was significantly decreased in eyes treatt%d with a comhiIlation GSA/steroid topical preparation. but the incidence and duration of posi- tive cultures was increased in this group as com-
2.6
“‘~,~~ f??
10.0
9.0
6.0
70
6.0
~~
5.0
40
3.0
2.0
10
10 11 12 13 14
Blood
Daily Therapy
W Oil
M CsA
Lymph Node
Davs Post immunization
Fig. 3. In vitro prol%erative responses to the S-Ar: of lym- phocytes iiom lymph node and blood frnm Lewis rats
receiving rither CsA or oil. Significant proliferative IT-
sponses to this antigen were seen onI>- in the blood of rats rcvG\-.ing oil injections. (Reprinted from Nussenhlatt RB et al”’ with permission from Inll Arch ;1lI~1;gv Appr hmunol-
OgY)
pared to controls. A combination of systemic and
intravitreal CsA therapy also proved effective in suppressing secondary herpes simplex uveitis, a
condition thought to be due to an interaction be- tween herpes antigen as well as various components of the immune system.”
The effect of &A on retinal S-antigen induced experimental autoimmune uveitis (EAU) has been investigated extensively. This agent prevented the expression of EAU when S-antigen-immunized rats were treated with 10 mgikgiday CsA when begun on day 0, and at 40 m,g/k,q when CsA was begun on

164 Surv Opht~lmol 3 l(3) November-December 1986 NUSSENB~~, PALESTINE
day 7 after immunization.6g Similar observations
have been recently noted by Striph and associatesg” Neither cell-mediated nor antibody responses were
abrogated, but a delay in the time needed to obtain
peak responses was observed. Additionally, lym-
phocytes carrying immune memory for the S-Ag were not observed in the circulation in those ani-
mals receiving CsA’O (Fig. 3). At higher dosages of
the agent, some rats were noted not to develop EAU
even when evaluated weeks (4-5) after the abroga-
tion of therapy. 68 The transfer of EAU to naive rats
by cells from S-Ag-immunized donors could be sup- pressed by daily injections of CSA.~” The topical
application of GSA did not prove to be effective in preventing EAU as long as circulating CsA levels
could not be measured, suggesting that effect ofCsA is mediated through systemic mechanisms.~’ How-
ever, when su~ciently high amounts of the drug are
placed into the vitreous, the eye can be protecred
from EAU, while the contralateral, untreated eye
will express disease.
Human Studies
NONOCULAR HUMAN STUDIES
The usefulness of CsA in almost all aspects of
transplantation immunology has been extensively evaluated. Calne and colleagues’7 reported the use-
fulness of CsA in patients receiving renal allografts
from cadaver donors. In a European multicenter trial, renal transplant survival was superior in pa-
tients immunosuppressed with CsA as opposed to the standard azathioprine and steroid prophylax-
is.87 GSA has been used to prevent graft-versus-host disease in humans after allogeneic bone marrow
transplantation. ” Although toxic side effects were
noted, the agent appeared effective in preventing serious complications, The era of liver transplanta-
tion has perhaps undergone the most dramatic change with the use of CsA. As Starzl and col-
leagues wrote, “The purgatory in which liver trans- plantation was mired has ended in the cyclosporine era.“g4 Starzl reported that of the first 67 recipients
in the CsA series in its first two years, 42 passed the
one-year mark. This was almost as many patients as survived the one-year mark for the 17 years prior to
CsA therapy. Comparing the 66 patients undergo- ing cardiac transplantation at Stanford University
who received CsA to the 99 receiving azathioprine, the incidence of rejection was not significantly dif- ferent between the two groups. However, since re- jection episodes were less severe, mortality related to these episodes was reduced to near zero in the CsA group and therefore afforded distinct improve- ments in terms of survival, rehabilitation, and hos- pital costs.‘”
The use of CsA in a multitude of auto~mrnLine
diseases has begun in order to investigate its poten-
tial usefulness in some very problematic diseases. As of this writing, most studies are pilot in nature, with
randomized studies just getting started or projected.
Amor and Dougados’ have reported their experi-
ence in an open trial utilizing CsA in the treatment of rheumatoid arthritis. Their impression, using
several clinical and laboratory parameters, was that
the drug was a beneficial agent for this disorder. A
pilot study in the treatment of recently diagnosed
Type 1 diabetes mellitus patients with CsA resulted
in the observation that this therapy enhanced or
preserved endogenous secretion of insulinZ3 and
that results from a recently completed randomized study will support this observation (Dr. Beat von
Graffenreid, personal communication). It should be emphasized that controlled clinical trials are still
needed to fully evaluate these and other observa-
tions.
OCULAR HUMAN STUDIES
Experimental cornea1 transplantation data would
suggest that CsA may be a logical therapeutic agent for the enhancement of graft survival. Hoffman and
Wiederholt”2 have reported their experience in util-
izing a 2% CsA castor oil eye drop solution com- bined with dexamethasone drops as a therapeutic
regimen for 25 patients. In this open, nonrandom-
ized study, 21125 grafts remained clear with a mean follow-up period of ten months. They noted that all
patients on this regimen developed a punctate kera- titis and a slight conjunctivitis. A masked random-
ized study using systemic CsA is presently under-
way in the United States.
We have reported the beneficial effects of CsA on patients with severe, sight-threatening intermediate
and posterior uveitis.“2.67 An initial sixteen patients ranged in age from 20 to 67 years and all had pre- viously received systemic corticosteroids and/or cy-
totoxic agents. These individuals, who had not had a positive therapeutic effect or intolerable side ef-
fects to these agents, were treated with CsA. Of the
16 patients, 15 had positive clinical responses to CsA therapy. Ofinterest, patients with cystoid mac-
ular edema demonstrated an improvement in visual acuity before the resolution of their edema could be demonstrated by fluorescein angiography. Resoiu- tion was, however, seen later in the therapeutic course (Fig. 4).62 While vitreal cells appear to linger, vitreal haze tends to dissipate more rapidly and can
be quantified.“.’ In longterm follow-up study of 52 patients treated with CsA, 41 of 52 patients (79%) were considered therapeutic successes at three months, and 63% (22 of 35) of those with one year’s follow-up were considered successfully treated as well.“’ Graham and associates” have noted similarb
CYCLOSPORINE
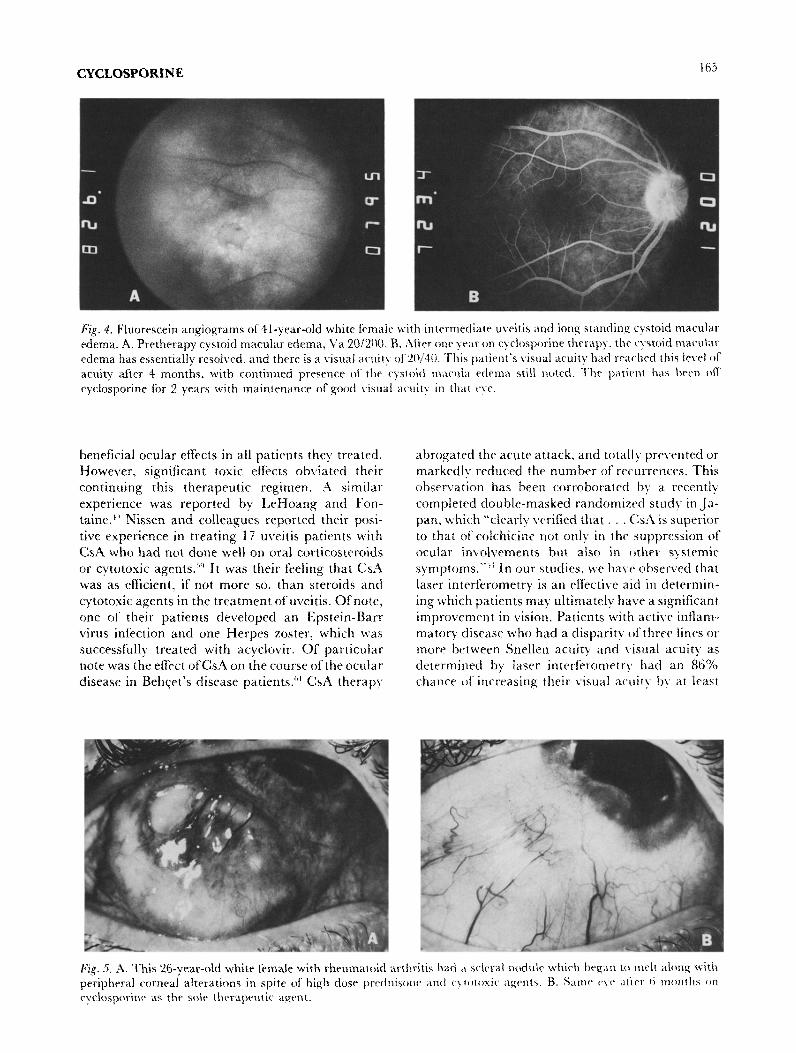
Fig. 4. Fluorescein angiograms of 41-year-old white female with intermediate uvcitis and long standing cystoid madar
edema. A. Pretherapy cystoid macular edema. I’a ~~/20(~. B. After one year on cyclosporine therapy. the cystoid ~~~cu~~~
edema has essentially resolved, and there is a visual acuity of 20/M. ‘I‘his patient’s visual acuity had reached this level of acuity after S months, with continued presence of the cystoid macula edema still noted. ‘I%P patient hx been ofi
cyclosporine for 2 years with li~aintenance of good visual acuity in that eye.
beneficial ocular effects in all patients they treated. abrogated the acute attack, and totally pre\.ented or However, significant toxic effects obviated their markedly reduced the number of recurrences. This
continuing this therapeutic regimen. A sirnilal observation has been corroboratrd by a recently
experience was reported by LeHoang and Fon- complctcd double-masked randomized study in .Ja- taine. !” Nissen and colleagues reported their posi- pan, which “clearly verified that . . Ck4 is superior tive experience in treating 17 uveitis patients with to that of colchicine not only in the suppression of
CsA who had not done well on oral corticostcroids ocular in\~o~ven~~ilts but also in other systemic
or cytotoxic agents.“’ It was their feeiing that CsA symptoms. “” In our studies, we ha\,e observed that was as efficient, if not more so, than steroids and laser interferometry is an effective aid in determin-
cytotoxic agents in the treatment of uveitis. Of note, ing which patients may ultinlatel~ have a significant one of’ their patients developed an Epstein-Barr improvrment in vision. Patients with active inflam- virus infection and one Herpes zoster, which was matory disease who had a disparity of three lines or
successfully treated with acyclovir. Of particular more between Snellen acuity and visual acuity as note was the efTect of&A on the course of the ocular detrrmined by laser interferometry had an 86%
disease in Behqet’s disease patients.h’ CsA therap) chance of increasing their visual acuity bx at least

166 Surv Ophthalmol 3 l(3) November-December 1986 NUSSENBLATT, PALESTINE
three lines with CsA therapy.74 Of interest as well
has been the excellent clinical response to CsA of a
patient with a severe scleral melt that was unrespon-
sive to cytotoxic agents (Fig. 5).
Toxicity and Side Effects
Although cytosporine has a relatively specific ef-
fect on the immune system, its use is associated with
a number of subjective side effects.45*76 Mild numb-
ness and tingling of the extremities as well as tem-
perature hypersensitivity are noted within several
days of starting on CsA by 90% of the patients.
Nausea and gastrointestinal distress beginning with
the first dose are noted in 2O%, but only in rare
individuals does this alter the patient’s ability to use the drug. This adverse reaction is responsive to a
decrease in dose. Increased hair growth is another
commonly observed side effect. It is usually noted
during the first several months of therapy. Gingival hyperplasia similar to phenytoin toxicity is noted in
25% of patients within the first several months of
therapy. Its severity is exacerbated by poor oral
hygiene and can largely be controlled by careful
attention to periodontal disease. Rarely, periodon-
tal surgery has been necessary. A fine hand tremor occurs in the early months of treatment, but this will
frequently improve during therapy. Oechslin et al”
reported cotton wool exudates in three bone marrow
recipients treated prophylactically with CsA for graft-versus-host disease. However, these aiter- ations were not noted in renal transplant patients
receiving CsA.”
Although CsA is not a cytotoxic drug and does
not cause leukopenia, a normochromic, normocytic
anemia is noted in 25% of patients. The hematocrit
rarely falls below 30%. It is important to rule out other causes of anemia. The cause of this anemia is
not known. Another unexplained side-effect is an increase in the erythrocyte sedimentation rate. A
significant increase is seen in 40% of patients in spite of an apparent clinical improvement in the underlying in~ammatory disease. This increase
may complicate treatment of diseases in which the sedimentation rate is an important clinical param- eter. Hepatic toxicity has not been a serious adverse reaction. Mild, dose-dependent elevations of serum transaminases and serum bilirubin have been noted.
Nephrotoxicity and hypertension have been the two major serious clinical toxicities of CsA therapy. Depending on the definition of renal toxicity, 75% or more of patients have some degree of renal func- tional change.26,76,78 A significant rise in the serum creatinine can be noted in treated patients. This is accompanied by a corresponding fall in glomerular filtration.‘” Initially this toxicity appears to be dose-
dependent and reversible; lowering of the dose will lead to a normalization of renal function within 4-6
weeks. However, chronic alterations in renal mor-
phology consisting of interstitial fibrosis and tubu-
lar atrophy have been noted in a large percentage of heart transplant patients treated for one year in
whom the serum creatinine was permitted to remain markedly elevated for extended periods of time.” In
our experience, this has also occurred in a patient
population where the dose of CsA was continually lowered to maintain a serum creatinine of less than
double the pretreatment serum creatinine.75 How-
ever, the initial dose of cyclosporine was 10 mg/kg and many patients received higher doses during
their treatment. It appeared that patients had more histologic evidence of renal toxicity if their serum creatinine was 50% above baseline for longer than
four months. Clinical monitoring of renal toxicity
does not fully reflect the underlying pathology. The patients in this study had a mean creatinine of 1.5
mg/dL in spite of the significant morphologic
changes.7” The significant irreversible renal toxicity
has led to recommendations of lower CsA doses and
the addition of other immunosuppressive drugs such as corticosteroids. It is further recommended
that creatinine not rise more than 20-30% above
the pretherapy level during CsA therapy. It is not
yet clear whether CsA nephrotoxicity is due to a
direct tubular toxic effect of the drug or whether it is due to decreased renal blood flow from an effect on
the sympathetic nervous system or on prostacyclin synthesis.7’
Systemic hypertension occurs in 25% of pa-
tients,7H more frequently in those patients with clini- cal alterations in renal function. It is responsive to
dose-reduction and to treatment with antihyperten-
sive regimens such as hydrochlorothiazide/alpha-
methyl dopa in combination with beta blocking
agents or prazosin. Reports of lymphoma caused initial concern
about the use of CsA.’ Lymphoma occurs no more frequently in organ transplant recipients receiving
CsA and prednisone than in similar patients treated
with other immunosuppressive agents. Forty-nine lymphomas occurred in 5000 transplant recipients followed for five yearsg’ Most of these deveiop in the first several months of therapy, and discontinuation
of therapy results in regression of the lymphoma. The incidence of lymphoma in patients receiving this drug for autoimmune disease is probably less than the above statistic, and to date we have seen none in our patients, nor are we aware of any reported.
Current Status The guidelines for the use of CsA in ocular in-

CYCLOSPORINE
flammatory diseases are undergoing modification as
new information concerning the mechanism of ac-
tion and the toxicity becomes available. Currently, CsA appears to be effective in diseases such as Beh- Get’s syndrome and in spite of the apparent nephro-
toxicity, probably has fewer severe side effects than
cytotoxic agents. In other inflammatory conditions, it is still a drug to be considered primarily in pa-
tients who have done poorly on high-dose cortico-
steroids or who cannot tolerate an effective mainte- nance dose of corticosteroids. In view of the
alterations in renal function, we have decreased the
starting dose of CsA to 6 mgfkglday and we contin-
ue the patient on low-dose corticosteroids. Renal
function should be carefully monitored by serum
creatinine and inulin or creatinine clearances. The amount of acceptable alteration in renal function
has not yet been determined; however, our current
guidelines suggest no more than a 30% increase in serum creatinine. CsA represents a first generation
drug of agents that will be effective on subsets of the immune system. In spite of its toxicity, organ trans-
plant survival has been dramatically improved.
Succeeding generations of CsA derivatives may of-
fer more specific action with less toxicity. For exam- ple, initial evaluation of Cyclosporine G has shown
that the nephrotoxicity is considerably less with this
drug, while the efficacy is only slightly reduced.“-b” In addition, an improved understanding of the
nephrotoxicitv may lead to the use ofvasodilators or
other drugs to decrease this side effect without af-
fecting the immunosuppressive action. Lastly. it
may be possible to reduce the required dose of CsA
by enhancing its effectiveness through the co-ad- ministration of other drugs. The final goal is the
control of immune-mediated inflammatory disease with minimal adverse effects.
References
Amor B. Dougados M: Ciclosporin in rheumatoid arthritis. Open trials with different dosages, in Schindler R (ed): &lo- $orin in Autoimmune Diseasec. Springer-Verlag, Berlin, 1985. pp 283-287 Atkinson K, Boland J. Britton K, et al: Blood and tissue distri- bution ofcyclosporine in humans and mice, in Kahan BD (ed): L~vclo@rine. Orlando FL. Grune and Stratton, 1983, pp 214- 217 Bell TAG. Easty DL. McCullagh: A placebo-controlled blind tr-ial of cyclosporine-A in prevention of cornea1 graft rejection in rabbits. BrJ Ophthalmol 66:303-308, 1982 Bendtwn K. Dinarello CA: LIechanism ofaction ofcyclospor- inr .I. Stand J Immunol 20:43-51. 1984 Beveridge 7’: Pharmacokinetics and metabolism of Cyclo- sperm A. m White DIG (cd): C,srlosporin A. I\lew York, Elsevier Biomedical Press. 1982, pp 35-44 Beveridge 1‘. Gratwohl A, Michot F, et al: Cyclosporin A: Pharmacokinetics after a sinqle dose in man and serum levels ., after multiple dosing in recipients of allogeneic bone-marro\\ crafts. Curr Ther Res 30:5-~18. 1981 Belwidge 7‘. Krupp P. SIcKibbin C: Lymphomas and lym-
8.
9.
10.
II.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
167
phoproliferative lesions developing under cvclosporin therapy. Lancet i:788, 1980 Boisjoly HM, \Voog JJ, Pavan-Langston D. et al: Prophylactic topical Cyclosporine in experimental herpetic stromal krrati- tis. Arch Ophthalmol 102:1804-1807. 1984 Bolton C, Allsopp G. Cuzntr ML: The effect ofCyclosporin A on thr adoptive transfer of experimental encephalomyelitis in the Lewis rat. C/in Exp lmmunol 47:127-132. 1982 Bolton C, Borel.JF, Cuzner ML. et al; lmmunosuppression b) (:yclosporin A of experimental allrrqic cncephalomyelitis. ,/ ,Veurol Sci X6:147-153. 1982 Bore1 ,JF, Fewer C. Gubler HU. et al: Biological effects of Cyclosporin A: A new antilymphocytic agent. .4gents and Actions 6:468-475, 1976 Bore1 JF: The history of cyclosporine A and its significance. in White DJG (ed): Cyclosporine A. Elsevicr Biomedical Press. Amsterdam 1982, pp >8 Bore1 JF, Lafferty KJ: Cyclosporine: Speculation about its mechanism of action. Transplant Proc Z:i:1881-1885. 1983 Bunjes D. Hardt C. Rollingheff M, et al: Cyclosporin A medi- ates immunosuppression of primary cytotoxic T-cell responses by impairing the release ofinterleukin I and intrrlcukin 2. Eur _] Immunol 12:657-661. 1981 Burckart GJ, Venkataramanan R, Griffith B, et al: Cyclo- sporin A blood concentrations in a child after intravenous and oral therapy (abstracted). Drug Intel/ C/in Pharm 17:446, 1983 Calm RY. White DJG: Cyclosporin A - A powrrful immuno- suppressant in dogs with renal allografts. IRCS .Med Sci 5:595, 1977 Calnc RY. White DJG. Thiru S. et al: Cyclosporin A in pa- tients receiving renal allografts from cadaver donors. Lancet fi:1323-1327. 1978 Chan CC, Mochizuki M. Palestine AG. et al: Kinetics of T- lymphocyte subsets in the eyes ofLewis rats with experimental autoimmune uveitis. Cell Immunol %:430-434, 1985 Chan CC, Palestine .4G. Xussenblatt RB: C)-closporine-in- duced alterations ofhumoral rrsponse in experimental autoim- mune uveitis. Inrest Ophthalmol l’ir Sci 25:867-870. 1984 Caster DJ. Shepherd U’FI. Chin Fook ‘I‘. et al: Prolonged survival of cornea1 allografts in rahhits trcatrd with cyclo- sporin A. Lancet ii:688-689, 1979 Dieperink H. Moller J: Ketoconazole and cyclosporin (letter). Lanrct ii:12li. 1982 DosReis GA, Shevach EM: Efrect of Cyclosporin A on T-cell function in vitro: The mechanism of suppression of T cell proliferation depends on the nature of the T cell stimulus as well as the differentiation state of the responding T cell. J Immunol 12X.2360-2367. 1982 Dupre J. Stiller CR, Gent M, et al: Effects of Ciclosporin on insulin secretion in recent onset type 1 diabetes mellitus. in Schindler R (ed): C’iclosporin in .4utoimmunr Direuser. Berlin, Springer-Verlag, 1985. pp 120-127 Elliott JF. Lin Y, Mizel SB, et al: Induction of interleukin 2 messenger RNA inhibited by Cyclosporin .\. Sczence. I)ec 21:1439-1441. 1984 Fcrguson RM, Sommer BG: Cyclosporine (CsA1 in renal transplantation: a single institution experience. .4mJKidncrDis j:296-306, 1985 Flechner Shf. Van Buren C, Kerman RH. et al: The nephro- toxicity of c)-closporine in renal transplant recipients. Tmns- plnnf Proc 15:2689-2694, 1983 Graham FM, Sanders MD. James DG, Pt al: Cvclosporin A in the treatment of posterior uveitis. Tram Ophthalmol Sor C’K 1@:146-151. 1985 Grcrn CJ. Allison AC: Extensive prolongation of rabbit kidney alloqaft survival after short term Cyclosporin .4 treatment. Lancet i: 1182-l 183. 1978 Hall BM, Jelbart ME. Dorsch SE: Suppressor ‘1‘ cells in rats with prolonged cardiac allograft survival after treatment with Cyclosporine. Transplantation 37:59.?-600. 1984 Hess AD, Tutschka PJ, Santos G\V: ElIect ofCvclosporin A on human lymphocyte responses in vitro. II. Induction ofspecific alloantigrn unresponsiveness mediated by a nylon wool adher- ent suppressor cell. J Immunol 1X:961-968. 1’181

168 Surv Ophthalmol 3 l(3) November-December 1986 NUSSENBLATT, PALESTINE
31. Hiestand PC, Gunn HC, Gale JM, et al: Comparison of the pharmacological profiles of cyclosporine, (NVA”)-cvclospor- ine and (VAI,‘) Dihydro-cyclosporinc. Immunologv 55:249-255. 1985
32. Hoffmann F, Wiederholt M: Lokale Behandlung des hornhaut Transplantates b&m Menscheu mit Cyclosporin A, &Xn .%rx- at&l Augenheilkd 187:92-96, 1985
33. Hunter PA, Wilhelmus KR, Rice XX, et al: Cyclosporin .4 applied topically to the recipient eye inhibits cornea1 graft rejection. Qin Erp Immunof 4.5:173-l 77. 1981
34. Hutchinson IF, Shadur CA, Duarte JSA, et al: Cyclosporin A spares selectively lymphocytes with donor specific suppressor characteristics. Transplantation 32t210-216. 1981
35. Jones M, Harris G: Prolongation of life in female NZB/NZW (Fi) hybrid mice by ciclosporin 4. C/in &.YP Immunol .???: l-9. 1985
36. Kana JS, Hoffman F, Buchen R. et al: Rabbit cornea1 allograft survival following topical administration of cyclosporin A. In- vest Ophthalmol ?‘is Sci 22:686-690, 1982
37. Kaufman Y, Chang AE, Robb RJ, et al: Mechanism of action of Cyclosporin ‘4: Inhibition of iympttokine secretion studied with antigen-stimulated T-ccl1 hybridomas. ./ Immunol I.??‘: 3107-3111, 1984
38. Kennedy MS, Deeg HJ, Siegel Xl, et al: .4cutc renal toxicity with combined use of amphotericin B and c\closporinr after marrow transplantation. Trun~~~ff~~~~~~~ 35:21 l-215. 1983
39. Keown PA, Stiller CR, Laupacis AI,, et al: The effects and sidr effects ofcyclosporine: Relationship to drug pharmacokinetirs. Transplant Proc Il(No. 4):652)-661. 1982
4-o. Keown P*4, Stiller CR, Sinclair NR, et al: The clinical rel- evance of cyclosporine blood levels as measured by radioim- munoassay. Transplant Proc 15 (suppl to :\‘o.l):2438-2441. 1983
41. Kostakis AJ, White DJC, Calne RY: prolongation of rat heart allograft survival by Cyclosporin .4. IRCS Meed Sri .i:280. 1977
42. Lafferty K.J, Andous I.. Prowse S.J: Role of lymphokinc and antigen in the control of specific ‘T-cell rrsponstx Immunol Rei 51:279, 1980
43. Langhoff E, &$adsen S: Rapid metabolism of cT!losporine and prednisone in kidney transplant patients rrcenmg tuhcrculo- static treatment (letter). Lancat zi:1031. 1983
44. Larsson EL: Cyclosporin A and dexamrthasone suppress T- cell responses by selectively acting at distinct sites of the trig- gering mechanism. J Immunol 124:282%2X33. 1980
45. Laupacis A: Complications of cyclosporine therapy-a com- parison to azathropine, in Kahan BD ied): ~)lrlo.~p~y~ne. Orian- do, FL, Grune and Stratton, 1984, pp 532-537
46. Laupacis A, Stiller CR, Garde11 C, et al: Cyclosporin prevents diabetes in BB Wistar rats. Lancet i: 10-12. 1983
47. Leapman SB, Filo RS, Smith EJ, et al: In vitro effects of Cyclosporin A on lymphocyte subpopulations. Tran.~pl~Rtutjffn 30:404-408. 1980
48. LeGrue SJ? Friedman A\%‘. Kahan BI3: Binding ofCyclospor- ine by human lymphocytes and phospholipid vesicles. ,J Im- munol 131:712-718, 1983
49. LeHoang P, Fontaine X Treatment of noninfectious inllam- matory disorders of the rye with Ciclosporin, in Schindtcr R (ed): Ciclosporin in Autoimmune Diseases. Berlin. Springrr \‘erlag? 1985, pp 137-138
50. Lemaire M, Tillement JP: Role of lipoproteins and erythro- cytes in the in vitro binding and distribution ofcyclosporin A in the blood. J Pharm Phannacol34:715-718, 1982
51. Lillehoj HS, Malek TR, Shevach EM: Differential effect of cyclosporin A on the expression ofT and B lymphocyte activa- tion antigens. J Immunol 133:244-250, 1984
52. Markwick JR, Chambers JD, Hobb JR, et al: Timing ofcyclo- sporin A therapy for abrogation of HVG and GVH responses in rats. Lancet ii: 1037-1039, 1979
53. Masuda K, Najakima A: A double masked study of Ciclo- sporin treatment in BehFet‘s disease, in Schindler R (ed): &lo- sporin in Autoimmune L&ares. Berlin. Springer Verlag, 1985, 162-164
54. Mercker M, Handschumacher RE: Uptake and nature of the intracellular binding of Cyclosporin A in a murine thymoma cell line, BW5147. J Immunol 132;3064-3070. 1984
55. Mochizuki M, Xussenblatt RB, Kuwabara T, et al: Eflects of Cyclosporine on thr efferent limb of the immune response. Transplant Pror l!i(Suppl 1):2364-2366, 1983
56. Mosteller MW, Gebhardt BM, Hamilton Ahi, et al: Penetra- tion of topical Cyclosporine into the rabbit cornea, aqueous humor, and serum. drch ~pkt~almol IM: 101-102, 1985
57. hfyers BD, Ross .J, Newton I., et al: Cyciosporine-associated chronic nephropathy. N Engl J .Cled 321;699-705, 1984
58. Niederberger N., Lrmaire M, ,qaurer G. et al: Distribution and binding of cyclosporine in blood and tissues, in Kahan BD (ed): C~i’rl~~pff~~n~. Clrlando, FL, Grune and Stratton, 1984, pp 203.-205
59. Nissen C, Bendtzen K, T\ede N, et al: The treatment of pre- sumed non-infective uveitis with Ciclosporin ‘4. Acta Opbhal- mologica 1~3(suppl~:?2-73~ 1985
60. Xussrnhlatt RB, Caspi RR, Dinning WJ, et al: .4 comparison ofthe effectiveness ofcyclosporine A, 13. and G in the treatment of experimental autoimmune uveitis in rats. ,/ Zmmunopharmacol (in press)
61. Nussenblatt RB. Dinning WJ. Fujikawa LS, et al: Local Cycio- sporine therapy for experimental autoimm~lne uveitis in rats. .irch Ophthalmoi 103:1559-1562, 1985
62. Nusscnblatt RB. Palestine AG, Chan CC: Cyclosporin A ther- apy in the treatment ofintraocular inflammatory disease resis- tant to systemic corticosteroids and cytotoxic agents. dm f Op~t~alrn~l X.275-282, 1983
63. Nussenblatt RB, Palestinc 4G, Chan CC: Cyclosporine tber- spy for uveitis: long-term followup. J Ocular Pharmacol lt369- 381. 1985
64. Nussenblatt RB, Pairstine AG, Ghan CC, Ct al: Effectiveness of Cyclosporin therapy for Behqet’s disease. drthritis Rheim 28: 671-679. 1985
65. Nussenblatt RB, Palestine AG, Chan CC, et al: Standardiza- tion ol‘vitrcal inflammatory activity in intermediate and postc- rior usritis. Opht~~alrnola.~~ g-7.467.-47 1. 1985
66. Sussrnhlatt RB. Schcr I: Effects of C&A in T-cell subsets in experimental autoimmune uveitis. Incest Ophthalmol 1% Sci X:10-Il. 1985
67. Nussenblatt RB, Palestine AG, Rook AH. et al: Treatment of
intraocular inflammatorv disease with Cyclosporin ‘4. Lnncet ii:235-238, 1983
68. Nussenblatt RB. Rodrizues MM. Salinas-Carmona MC, et al: Xlodulation of axperi&ntal autoimmune uveitis with Cycle- sporin A. .-lrch Ophthalmol 100: 1146-l 149, 1982
69. Nussenblatt RB. Rodrigues Mkf: Wacker WB, et al: Cycle-
sporin A: Ii~hibition of cxperimcntaf aut[)immune uveitts in Lewis rats. ,I Clin Inzest 6’7:1228-1231. 1981
70. Nussenblatt RB, Salinas-Carmona MC, bt’aksman BH, et al: Cyctosporin A: Cellular immune alterations in S-antigen in- duced raperimcntal autoimmune uvcitis. Int drch Allergy Im- munal 7#:289-294. 1983
71. Occhsiin hf. Thirl G, Landmann J. et al: Cotton-wool PXU-
dates not observed in recipients of renal transplants treated with cyclosporine. Transplantation 41:60-62, 1986
72. OhJO. ,\linasi P. Grabner G, rt al: Suppression of secondary hrrpes simplex uvritis by Cyclosporine. Iwest OphthQlmol I ‘i.rSri Zrf:194-500, 1985
73. Oycr PE, Stinson EB. ,Jamieson SW, et al: Cyclosporinc in cardiac transplantation: Q 2% year followup. Transplant Proc 15(Suppl):2546-2552, I983
74. Palestine AG, r\lter GJ, Ghan CC, et al: Laser interferometry and visual prognosis ‘in uveitis. Ophthalmology 92; 1567-1569, 1985
75. Palestine .4G, Austin HA, Batow JE, et al: Renal histopatho- logic z&rations in patients treated with cyclosporine for uvei- tis. N EzgiJ Med 318:1293-1298, 1986
76. Palestine AG. Austin HA, Nussenblatt RB: Cyclosporine in- duced nephrotoxicity in patienrs with autoimmune uveitis. Transplant Proc 17(~h. 4, Suppl 1):209-214, 1985
77. Palestine AG, Nussrnblatt RB. Chan CC: Cyclosporine pene- tration into the anterior chamber and cerebrospinal fluid. Am] Ophthalmot 99:210-211, 1985
78. Palestine AG, Nussrnblatt RB, Ghan CC: Side effects of sys- temic cyclosporine in patients not undergoing transplantation.

CYCLOSPORINE