damping capacity assessment versus resonance frequency ... · damping capacity assessment versus...
TRANSCRIPT

_____________________________Sebastian Soicu et al 109
orIgInal arTIClES
Damping CapaCity assessment versus resonanCe FrequenCy ananlysis in the Determination oF Dental implant stability
Sebastian Soicu1, Dorin Bratu2, Ioan Borsanu3
reZumatAcest articol îşi propune să facă o trecere în revistă a studiilor clinice referitoare la rolul capacităţii de amortizare (tehnica Periotest) şi analizei frecvenţei de rezonanţă (tehnica RFA) în determinarea stabilităţii implantelor dentare şi în detectarea celor cu risc de mobilizare. Ambele tehnici de investigare sunt metode de testare intraorală non-invazivă şi sunt influenţate de parametri ca densitatea oaselor maxilare, inserarea implantelor la maxilar sau mandibulă, lungimea stâlpului implantar sau înălţimea porţiunii supracrestale a implantului. Rezultatele studiilor sugerează că valori ridicate înregistrate prin tehnica RFA şi scăzute înregistrate prin tehnica Periotest indică implante dentare cu o evoluţie favorabilă, în timp ce valorile scăzute/în scădere ale tehnicii RFA sau valorile ridicate/în creştere ale tehnicii Periotest indică pierdere de os marginal periimplantar. Totuşi, măsurătorile singulare, folosind oricare dintre cele două tehnici, au o valoare clinică limitată. Datorită volumului limitat al cercetării ştiinţifice pe acest subiect, este nevoie de mai multe studii clinice care să investigheze valoarea de prognostic a tehnicilor RFA şi Periotest, în detectarea pierderii în timp a stabilităţii implantare.Cuvinte chieie: stabilitate implantară, Periotest, analiza frecvenţei de rezonanţă, interfaţa implant-os
abstraCtThis paper presents a review of the clinical literature on the damping capacity assessment (Periotest technique) and resonance frequency analysis (RFA technique) in the determination of dental implant stability and the prognostic value of each technique to detect implants at risk for failure. Both techniques are non-destructive intraoral testing methods and seem to be influenced by factors such as bone density, implant insertion on upper or lower jaw, abutment length and supracrestal implant length. Data suggest that high RFA and low Periotest values indicate successfully integrated implants and that low/decreasing RFA and high/increasing Periotest values indicate marginal bone loss. However, single readings using any of the techniques are of limited clinical value. Due to the limited number of clinical reports found, the prognostic value of the RFA and Periotest techniques in predicting loss of implant stability has yet to be established in more clinical studies.Key words: implant stability, Periotest, resonance frequency analysis, implant-bone interface
Received for publication: Dec. 13, 2009. Revised: Jan. 17, 2010.
1Dental Medicine Clinique „Exces Image” Pitesti.2Department of Prostodontics, Faculty of Dental Medicine, Victor Babeş Timişoara, Roamania3Dental Medicine Clinique „Prof. Dr. Bratu” Timişoara.
Correspondence to:Sebastian SoicuClinica de Medicină Dentară „Exces Image” Bd. Republicii Nr. 150, Piteşti, jud. Argeş, România, cod 110177;Tel: 0248221240, 0723545847, 0788500654;Fax 0248221240E-mail address: [email protected]
introDuCtion
The resonance frequency analysis (RFA – using the Osstell™ device) and the damping capacity assessment (Periotest™ technique) are the non-destructive intraoral testing methods for assessing implant stability. Another technique – the insertion torque measurements – only assess conditions at the time of implant insertion.1
One of the most important parameters for the short- and long-term clinical functioning of an implant is considered to be the development of a firm implant-bone interface.2 The contact between bone and implant surface and its characteristics are influenced by the different implant geometries and surfaces as well as various host site conditions.2

_____________________________110 TMJ 2010, Vol. 60, No. 1
Although the technical approach to implant stability of each device (OsstellTM and PeriotestTM
instruments) differs substantially, both methods seem to be useful in the long-term follow-up of dental implant integration.3 From the peri-implant bone loss point of view, it can be stated that the techniques are both suitable to detect a decrease in implant stability.1,4
Today, RFA is frequently used in clinical research to monitor implant stability. The RFA technique may detect bone loss earlier than Periotest™ method.4,5 Due to its higher reproducibility, RFA has replaced, in some cases the Periotest™ technique, which has been developed for a similar purpose.3,4 It is known that, at this moment, it is not recommended to entirely rely on Periotest™ or RFA measurements against radiographic diagnosis of the peri-implant bone situation follow-up.4
The destructive methodologies, such as removal torque assessment, pullout and pushout techniques, may be of value as research techniques, but they are of limited value in clinical use, owing to ethical concerns associated with the invasive nature of such methodology.6
The aim of this article is to define and characterize the RFA and Periotest™ techniques as methods for testing the implant/bone interface and to analyze their validity, clinical significance and prognostic value for assessing implant stability.
resonance Frequency analysisResonance frequency analysis (RFA) is a non-
invasive and non-destructive quantitative measurement of implant integration by assessing changes in implant stability over time. RFA measurements have documented healing changes along the implant–bone interface by measuring the increase/decrease in stiffness of the implant/bone interface. RFA also has been used to determine whether implants are sufficiently stable to receive the final restoration or to be loaded and to identify ‘‘at-risk’’ implants.7-9
RFA was first proposed by Meredith et al. (1996).10 The original electronic11 technique used an L-shaped transducer that was screwed to an implant or its abutment and a direct connection (wire) between the transducer and the resonance frequency analyzer. The transducer beam was then excited over a range of frequencies, from 5 to 15 kHz. A frequency response analyzer subsequently analyzed the response of the beam. At the first flexural resonance of the beam, there was a marked change in amplitude and in phase of the received signal. The resonance frequency can thus be identified in a plot of frequency (Hz) against amplitude (V).2,11
At the beginning, prototype instruments used in a number of studies indicated the results in Hz. One
disadvantage of the technique is the fact that each transducer has its own genuine RF and that the RF of the same implant varies between transducers. A linear relation was found between abutment length and RF, and measurements with different transducers and implants with different abutment lengths have to be calibrated before submitting the data to statistical analysis.
The first commercial version of the RFA technique (Osstell™, Integration Diagnostic AB, Göteborg, Sweden) used transducers that were calibrated by the manufacturer. Before performing RFA, a registration of the implant length was needed. RF measurements were now expressed as the implant stability quotient (ISQ) with values from 1 to 100. These are based on the underlying and calibrated RF of the transducer used.
More recently, the commercial instrument was modified; it is now wireless and makes use of a magnetic peg – Smartpeg – attached to an implant or abutment (Mentor™, Integration Diagnostic AB, Göteborg, Sweden) (Fig. 1). The peg is excited and the RF is expressed electromagnetically as ISQ units (the magnetic pulse technique).2,11
Figure 1. RF measurement using Osstell™ Mentor™ device, with the magnetic peg attached to one implant.
Damping capacity assessment (Periotest™ technique)
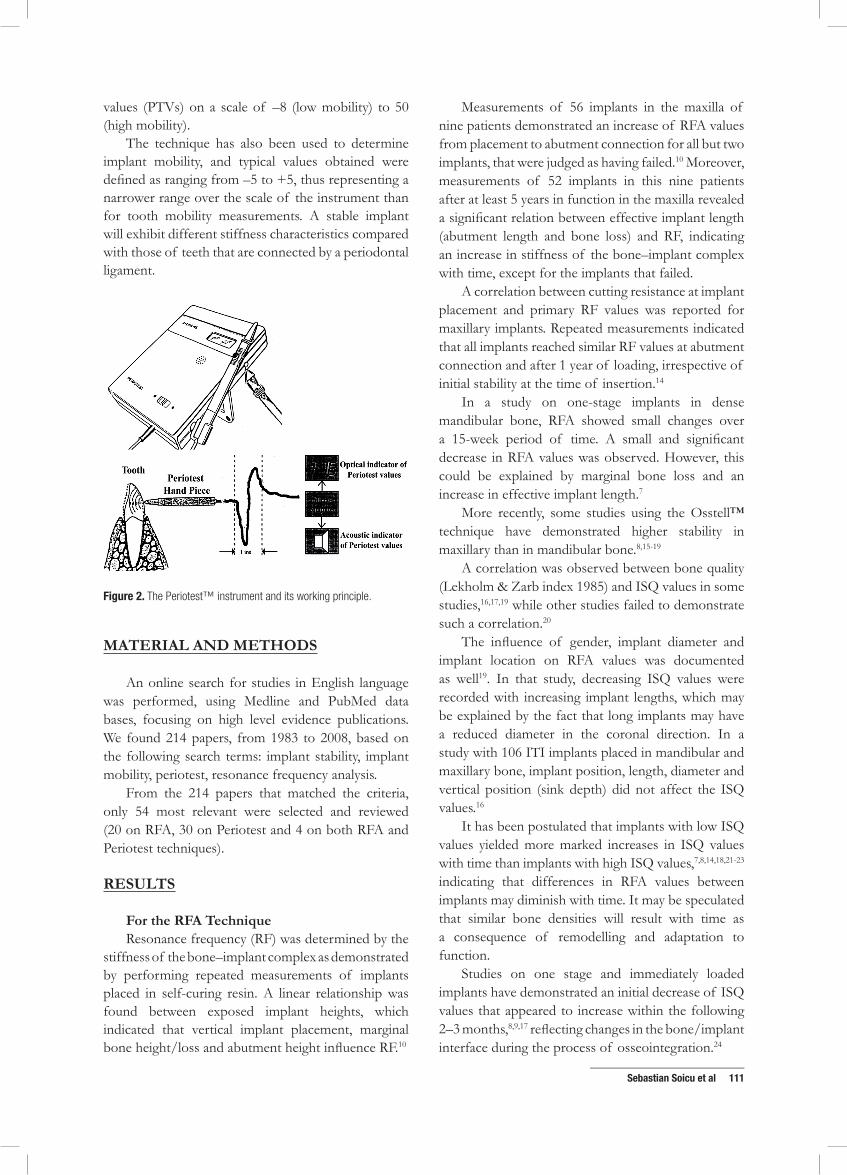
Periotest™ (Gulden-Medizintechnik, Bensheim an der Bergstrasse, Germany) is an electronic instrument (Fig. 2), originally designed to perform quantitative measurements of the damping characteristics of the periodontal ligament surrounding a tooth, thereby establishing a value for its mobility.12,13
The Periotest™ instrument comprises a hand piece containing a metal slug that is accelerated towards a tooth by an electro-magnet. The contact duration of the slug on the tooth is measured by an accelerometer. The software in the instrument is designed to relate contact time as a function of tooth mobility. The result is displayed digitally and audibly as Periotest™
_____________________________Sebastian Soicu et al 111
values (PTVs) on a scale of –8 (low mobility) to 50 (high mobility).
The technique has also been used to determine implant mobility, and typical values obtained were defined as ranging from –5 to +5, thus representing a narrower range over the scale of the instrument than for tooth mobility measurements. A stable implant will exhibit different stiffness characteristics compared with those of teeth that are connected by a periodontal ligament.
Figure 2. The Periotest™ instrument and its working principle.
material anD methoDs
An online search for studies in English language was performed, using Medline and PubMed data bases, focusing on high level evidence publications. We found 214 papers, from 1983 to 2008, based on the following search terms: implant stability, implant mobility, periotest, resonance frequency analysis.
From the 214 papers that matched the criteria, only 54 most relevant were selected and reviewed (20 on RFA, 30 on Periotest and 4 on both RFA and Periotest techniques).
results
For the rFa techniqueResonance frequency (RF) was determined by the
stiffness of the bone–implant complex as demonstrated by performing repeated measurements of implants placed in self-curing resin. A linear relationship was found between exposed implant heights, which indicated that vertical implant placement, marginal bone height/loss and abutment height influence RF.10
Measurements of 56 implants in the maxilla of nine patients demonstrated an increase of RFA values from placement to abutment connection for all but two implants, that were judged as having failed.10 Moreover, measurements of 52 implants in this nine patients after at least 5 years in function in the maxilla revealed a significant relation between effective implant length (abutment length and bone loss) and RF, indicating an increase in stiffness of the bone–implant complex with time, except for the implants that failed.
A correlation between cutting resistance at implant placement and primary RF values was reported for maxillary implants. Repeated measurements indicated that all implants reached similar RF values at abutment connection and after 1 year of loading, irrespective of initial stability at the time of insertion.14
In a study on one-stage implants in dense mandibular bone, RFA showed small changes over a 15-week period of time. A small and significant decrease in RFA values was observed. However, this could be explained by marginal bone loss and an increase in effective implant length.7
More recently, some studies using the Osstell™ technique have demonstrated higher stability in maxillary than in mandibular bone.8,15-19
A correlation was observed between bone quality (Lekholm & Zarb index 1985) and ISQ values in some studies,16,17,19 while other studies failed to demonstrate such a correlation.20
The influence of gender, implant diameter and implant location on RFA values was documented as well19. In that study, decreasing ISQ values were recorded with increasing implant lengths, which may be explained by the fact that long implants may have a reduced diameter in the coronal direction. In a study with 106 ITI implants placed in mandibular and maxillary bone, implant position, length, diameter and vertical position (sink depth) did not affect the ISQ values.16
It has been postulated that implants with low ISQ values yielded more marked increases in ISQ values with time than implants with high ISQ values,7,8,14,18,21-23 indicating that differences in RFA values between implants may diminish with time. It may be speculated that similar bone densities will result with time as a consequence of remodelling and adaptation to function.
Studies on one stage and immediately loaded implants have demonstrated an initial decrease of ISQ values that appeared to increase within the following 2–3 months,8,9,17 reflecting changes in the bone/implant interface during the process of osseointegration.24

_____________________________112 TMJ 2010, Vol. 60, No. 1
A relation between marginal bone loss and RFA was observed for mandibular implants, and changes in ISQ values were reported between implant insertion and a 6-month follow-up, but not between the 6- and the 12-month follow-up.25
results for the periotest techniqueInter-operator and inter-instrument variability
has been studied extensively.26-30 A linear relationship between contact time and PTVs resulted for implants assessed in vitro and in vivo, indicating the robustness of the instrument.31-33
Both in vitro and in vivo studies indicated a linear relationship between the vertical distances from the striking point to the first bone contact on the PTVs. It was, therefore, concluded that single Periotest™ measurements do not allow any prognosis for the stability of an implant, but that an individual implant may and should be measured repeatedly during follow-up.29,33,34
A mathematical model illustrating the effect of various geometric and clinical parameters on the PTV was developed. This model was validated in an in vitro experiment.35 The results showed that PTVs were sensitive to the position on which the Periotest™ impacted on the abutment and hence, depended on the angulations of the hand piece. A change in position of 1 mm in striking height may produce a difference in PTVs between 1 and 2.26,36-38 As the outcome of Periotest™ measurements is influenced by the distance from the striking point to the first bone contact, it is evident that the placement of the implant in vertical dimension, abutment height, the level of marginal bone loss and the striking position on the abutment-implant are critical factors for accuracy and/or reproducibility. Clinical studies using various implant systems have demonstrated significantly lower PTVs in mandibular than in maxillary bone, indicating higher stability in the former than in the latter location.36,39-41
Based on measurements of 2212 implants of various designs, the lowest PTVs were characteristic for very dense bone (Class 1: Lekholm & Zarb 1985). However, no linear correlation between the degree of bone density and PTVs was established.42,43 An inverse correlation between insertion torque values and PTVs as well as between bone density around implants in fresh bovine ribs and PTVs was demonstrated in an in vitro study.38 Also, a relationship between number of engaged cortical layers (no cortical bone, mono and bicortical anchorage) and PTVs was established. For TPS bicortical screws, lower PTVs were observed than for ITI implants,40,41 while, in another study and evaluating very similar ITI implants, no correlation could be detected between PTVs and bone density
determined histologically in bone core biopsies from implant sites in the mandible.44
Regarding the effect of implant length on PTVs, contradictory results have been reported. While a correlation was postulated by some authors,40 others only described this for the maxilla26,36,37,41 and another group of authors did not find any correlations.38,44,45
Evaluating four different implant surfaces in an animal model, neither a correlation between PTVs and marginal bone height nor between PTVs and bone contacts as determined histologically was found.46
A comparison between screw-shaped implants subjectied to excessive occlusal load and implants subjected to plaque accumulation in primates led to the result that some, but not all excessively loaded implants showed signs of clinical mobility while all implants with plaque accumulation were stable after 18 months. The PTVs correlated with the marginal bone loss and degree of bone–implant contact. However, for the clinically stable implants, no correlation could be demonstrated.47
The Periotest™ instrument was also evaluated to measure implant mobility in a controlled in vitro model.48 The range of mobility as determined by the Periotest™ instrument in vivo was –6 to +2. The authors concluded that clinically stable implants were not completely immobile as revealed by PTVs, but yielded a range of mobility.
Time elapsed since implant insertion appears to influence implant stability. This is sustained by the fact that lower PTVs are usually encountered with increasing time of follow-up.26,37,38,40,44,49,50 Decreasing PTVs were observed up to the fifth year of follow-up for 213 mandibular implants used for the retention of overdentures. This was interpreted as ongoing remodelling and stiffening of the interface following implant placement.40
DissCutions
rFa techniqueTo monitor the outcome of implant insertion and
determine the prognostic value of RFA in predicting loss of implant stability, 75 one-stage implants in the edentulous mandible were evaluated over time.7 One implant showed decreasing ISQ values from 2 to 15 weeks, the observation time at which clinical mobility was evident. Another patient within the same study yielded three of five implants that showed a dramatic decline in ISQ values from 2 to 6 weeks postoperatively, when the implants were loaded with a relined denture. Unloading of these implants resulted in recovery of two and maintained stability of one implant. Hence,

_____________________________Sebastian Soicu et al 113
the results seemed to indicate that RFA might identify the loss of implant stability.
A more recent study (2007) assessed ISQ values at the time of implant insertion of ITI implants (Straumann, Basel, Switzerland) and at 1, 2, 3, 4, 5, 6, 8 and 12 weeks thereafter24. One implant lost clinical stability after 3 weeks. At this time, the ISQ had declined significantly from 70, 69 and 68 to 45. However, the loss of clinical stability was coincidental to the low ISQ, but not to be predicted by RFA. In the remaining 16 implants of identical length, sink depth and diameter in nine patients, the ISQ at the time of placement did not correlate with a micro-CT analysis of the bone density or the bone trabecular connectivity of the parent jawbone. ISQ values decreased slightly after 2–4 weeks and increased thereafter to the levels of the time at implant insertion or higher, reflecting the changes observed at the bone/implant interface during the process of osseointegration.51 It has to be noted that in the reported study24, the numerical value of the implant having lost stability after 3 weeks (ISQ=45) was only marginally outside the range of the ISQ values reported for all the other implants at all observation periods.
In a longitudinal study on immediate loading, RFA was performed on 72 stable implants and compared with nine implants that had lost stability during a period of 1 year.9 Both groups of implants showed a high degree of initial stability documented by an ISQ=70. The implants losing stability showed a continuous decrease in ISQ values until clinical failure was evident. The mean ISQ value was statistically lower for the group with implants having lost stability (ISQ=52) than for the group with stable implants (ISQ=68). The lower the ISQ value was after 1 month of immediate loading, the higher was the risk for future loss of stability. The risk for loss of stability was 18.2%, if ISQ values were between 49 and 58.
In a study on implant stability in grafted maxillae, only a tendency towards lower initial ISQ values was found for 17 implants that lost stability during the study (ISQ=54.6) compared with 195 implants that remained stable (ISQ=62).23
Comparing immediately loaded ITI implants with implants loaded after 3 months of healing, the RFA technique was judged to be an unreliable methodology for the identification of mobile ITI implants.22 However, implant stability was reliably determined for implants with an ISQ>47. The insensitivity of detecting unstable implants was explained by the nature of the RFA technique, which appears to determine stability as a function of stiffness. Mobile implants display extremely low stiffness and hence, the first resonance frequency may not be identifiable, resulting
in false increased ISQ values, that may correspond to the second resonance frequency.31,32
A prospective pilot study was done in order to investigate differences in changes in implant stability and crestal bone height, between loaded and unloaded dental implants, at four months after placement.52 In the test group, 20 implants were placed in the anterior region of the mandible, in 10 patients. They were connected with a Dolder bar within 10 days and placed into function immediately. In the control group, 21 implants were placed in the anterior region of the mandible, in a 2-stage procedure, in 12 pacients. In both groups, measurements of the RF were made at the time of placement and repeated 4 months after placement.
In the early loading group, the mean change of ISQ was –0.08 ± 0.77 and the mean bone loss was 0.69±0.15 mm. In the unloaded group, the mean change in ISQ was 1.33 ± 1.65 and the mean bone loss was 0.53 ± 0.18 mm. There was no statistically significant difference accros the 2 treatment groups. When gender was included as a factor, the changes in stability and bone loss were statistically smaller among female than among male patients.
The absence of differences in implant stability founded between the 2 treatment groups or over the 4-month period within either group is inconsistent with other studies,7,14 where a slight decrease in stability for the majority of 75 machined Brånemark implants, placed in anterior mandibles with high bone density was found. When using 127 implants in 20 patients, it was showed that, when the primary stability is high at placement, the ISQ is more likely to be stable over time. These differences may be a result of different types and designs of implant used, or may simply reflect the small sample size that was used in each study.52
The lack of published normative values or baseline data for ISQ makes comparisons difficult. However, it is useful to compare changes in bone-implant interface stiffness over time. The ISQ values provided by the Osstell™ instrument are determined by the stiffness of the bone-implant interface and by the distance from the transducer to the first bone-implant contact (reflecting any change in bone level). Consequently, to know whether a change of ISQ over time is the result of bone loss, a change in the bone-implant interface or a mixture of both, the change in bone height needs to be known. However, since there is no published standard or ratio between bone loss and ISQ, it is not possible to know if the changes in ISQ are the result of bony crest changes or of a change in the interface stiffness. Thus, the only conclusion that can be drawn from this study is that

_____________________________114 TMJ 2010, Vol. 60, No. 1
early loading does not adversely affect the stability of dental implants placed in dense bone.52
periotest techinqueEvaluating PTVs of eight implants that lost
stability after prosthesis placement, six of eight implants showed PTVs of +4 or higher as determined at the time of abutment connection. All eight implants demonstrated PTVs from +13 to +30 at the time of loss of stability. Nine other implants with high initial PTVs (+3 to +8) were left unloaded for at least 4 months. This resulted in a decrease of PTVs (final measurements were from 0 to +5). In addition, two cases demonstrated high PTVs at the time of loss of implant stability. Derived from single case reports, the data suggest that high PTVs at abutment connection may indicate questionable osseointegration and may suggest increased risk for loss of stability if loaded. However, the level of evidence remains anecdotal and precludes the prognostic value of the Periotest™.36
When evaluating PTVs of four different implant systems after an average of 22.5 months after placement, 14 of 204 implants lost stability, with all those yielding positive PTVs. Also, significantly higher PTVs were found than for stable implants, except for the ITI implants in the maxilla.41
In a sequential study on 40 patients, evaluating PTVs after implant abutment connection, prosthetic impression, placement of the prosthesis and 6 and 12 months after occlusal loading, The Periotest™ instrument was able to identify 64% of the non-integrated implants at abutment connection and 12 months after occlusal loading. However, PTVs recorded at abutment connection failed to predict loss of implant stability at 12 months of functional loading.53
In an attempt to validate PTVs and other clinical and radiographic parameters for the detection of alveolar bone loss around 32 cylindrical implants in 16 patients, it was demonstrated that radiographs disclosed pathological loss of alveolar bone at the bone–implant contact area, while other parameters including Periotest™ assessments did not.54
ConClusions
1. Although extensively used in clinical research as one parameter to monitor implant stability, it has to be realized that RFA is affected by factors such as bone tissue characteristics and implant sink depth, diameter and surface characteristics.
2. Research indicates that implants yielding high ISQ values during follow-up appear to maintain
stability. Low or decreasing ISQ values may indicate a developing instability.
3. No established normative range of ISQ values is available as yet. Consequently, a single determination of the ISQ value does not define bone/interface characteristics or provide a quantitative evaluation of bone tissue integration.
4. At the present time, the prognostic values for developing implant instability and the validity and relevance of RFA for clinical use have to be questioned. Further research is needed to establish threshold ranges for implant stability and for implants at risk for losing stability, for different implant systems.
5. Although the Periotest™ instrument has been extensively evaluated in experimental and clinical research, prognostic value to detect loss of implant stability cannot be documented. A variety of factors, such as the striking position (abutment length, supracrestal implant length) and location within the jaw (mandible/maxilla), have been shown to influence the PTVs.
6. It is evident that negative PTVs indicate stability of implants, while high and positive PTVs may suggest loss of stability. Such increases in PTVs are often realized after the fact, indicating a high specificity of the Periotest™, but a low sensitivity.
7. Owing to a variety of factors, the reproducibility of assessments is questionable. Single readings of Periotest™ determinations are of limited clinical value and have not been demonstrated to reflect the nature of the bone/implant interface. By performing repeated measurements of the same implant over time, implant stability may be confirmed.
8. The Osstell instrument seems to be more precise than Periotest, whose values appear to be more susceptible to clinical conditions.
reFerenCes
1. Atsumi M, Park SH, Wang HL. Methods used to assess implant stability: Current status. Int J Oral Maxillofac Implants 2007;22:743-54.
2. Aparicio C, Lang NP, Rangert B. Validity and clinical significance of biomechanical testing of implant/bone interface. Clin Oral Imp Res 2006;17(Suppl. 2):2-7.
3. Zix J, Hug S, Kessler-Liechtl G, et al. Measurement of dental implant stability by resonance frequency analysis and damping capacity assessment: comparison of both techniques in a clinical trial. Int J Oral Maxillofac Implants 2008;23:525-30.
4. Lachmann S, Jager B, Axmann D, et al. Resonance frequency analysis
_____________________________Sebastian Soicu et al 115
and dampening capacity assessment. Part 2: peri-implant bone loss follow-up. Clin Oral Implants Res 2006;17:80-4.
5. Lachmann S, Jager B, Axmann D, et al. Resonance frequency analysis and dampening capacity assessment. Part 1: an in vitro study on measurement reliability and a method of comparison in the determination of primary implant stability. Clin Oral Implants Research 2006;17:75-9.
6. Brunski J. Push-out (pull-out), tensile, and reverse-torque tests of bone–implant interfaces. Clin Oral Implants Research 2006;17:in press.
7. Friberg B, Sennerby L, Linden B, et al. Stability measurements of one-stage Branemark implants during healing in mandibles. A clinical resonance frequency analysis study. I J Oral Maxillofac Surg 1999;28:266-72.
8. Barewal RM, Oates TW, Meredith N, et al. Resonance frequency measurement of implant stability in vivo on implants with a sandblasted and acid-etched surface. Int J Oral & Maxillofac Implants 2003;18:641-51.
9. Glauser R, Sennerby L, Meredith N, et al. Resonance frequency analysis of implants subjected to immediate or early functional occlusal loading. Successful vs. failing implants. Clin Oral Implants Res 2004;15:428-34.
10. Meredith N, Alleyne D, Cawley P. Quantitative determination of the stability of the implant-tissue interface using resonance frequency analysis. Clin Oral Implants Res 1996;7:261-7.
11. Valderrama P, Oates TW, Jones AA, et al. Evaluation of two different resonance frequency devices to detect implant stability: a clinical trial. J Periodontol 2007;78:262-72.
12. Schulte W, d’Hoedt B, Lukas D, et al. Periotest - a new measurement process for periodontal function. Zahnärztliche Mitteilungen 1983;73:1229–30,1233-6,1239-40.
13. Schulte W, Lukas D. Periotest to monitor osseointegration and to check the occlusion in oral implantology. J Oral Implant 1993;19:23-32.
14. Friberg B, Sennerby L, Meredith N, et al. A comparison between cutting torque and resonance frequency measurements of maxillary implants. A 20-month clinical study. Int J Oral and Maxillofac Surg 1999;28:297-303.
15. Balleri P, Cozzolino A, Ghelli L, et al. Stability measurements of osseointegrated implants using Osstell in partially edentulous jaws after 1 year of loading: a pilot study. Clinic Implant Dent & Related Res 2002;4:128-32.
16. Bischof M, Nedir R, Szmukler-Moncler S, et al. Implant stability measurement of delayed and immediately loaded implants during healing. Clin Oral Implants Res 2004;15:529-39.
17. Balshi SF, Allen FD, Wolfinger GJ, et al. A resonance frequency analysis assessment of maxillary and mandibular immediately loaded implants. Int J Oral & Maxillofac Implants 2005;20:584-94.
18. Becker W, Sennerby L, Bedrossian E, et al. Implant stability measurements for implants placed at the time of extraction: a cohort, prospective clinical trial. J Perio 2005;76:391-7.
19. Östman PO, Hellman M, Wendelhag I, et al. Resonance frequency analysis measurements of implants at placement surgery. Int J Prosth 2006;19:77-83.
20. Zix J, Kessler-Liechti G, Mericske-Stern R. Stability measurements of 1-stage implants in the maxilla by means of resonance frequency analysis: a pilot study.
21. Int J Oral & Maxillofac Implants 2005;20:747-52.22. Olsson M, Urde G, Andersen JB, et al. Early loading of maxillary
fixed cross-arch dental prostheses supported by six or eight oxidized titanium implants: results after 1 year of loading, case series. Clin Implant Dent & Related Res 2003;5(Suppl. 1):81-7.
23. Nedir R, Bischof M, Szmukler-Moncler S, et al. Predicting osseointegration by means of implant primary stability. Clin Oral Implants Res 2004;15:520-8.
24. Sjöström M, Lundgren S, Nilson H, et al. Monitoring of implant stability in grafted bone using resonance frequency analysis. A clinical study from implant placement to 6 months of loading. Int J Oral &
Maxillofac Surg 2005;34:45-51.25. Huwiler M, Pjeturson BE, Bosshardt DD, et al. Resonance Frequency
Analysis (RFA) in relation to jaw bone characteristics during early healing. Clinical Oral Implants Rese 2007;18:275-80.
26. Turkyilmaz I, Sennerby L, Tumer C, et al Stability and marginal bone level measurements of unsplinted implants used for mandibular overdentures. A one-year randomized prospective study comparing early and conventional loading protocols. Clin Oral Implants Res 2006;17:501-5.
27. Teerlinck J, Quirynen M, Darius P, et al. Periotest: an objective clinical diagnosis of bone apposition toward implants. Int J Oral & Maxillofac Implants 1991;6:55-61.
28. Manz MC, Morris HF, Ochi S. An evaluation of the Periotest system. Part I: examiner reliability and repeatability of readings. Implant Dent 1992;1:142-6.
29. Manz MC, Morris HF, Ochi S. An evaluation of the Periotest system. Part II: reliability and repeatability of instruments. Implant Dent 1992;1:221-6.
30. Chai JY, Yamada J, Pang IC. In vitro consistency of the Periotest instrument. J Prosth 1993;2:9-12.
31. Derhami K, Wolfaardt JF, Faulkner G, et al. Assessment of the Periotest device in baseline mobility measurements of craniofacial implants. Int J Oral & Maxillofac Implants 1995;10:221-9.
32. Meredith N. A review of nondestructive test methods and their application to measure the stability and osseointegration of bone anchored endosseous implants. Critical Reviews in Biomedical Engineering 1998;26:275-91.
33. Meredith N. Assessment of implant stability as a prognostic determinant. Int J Prosth 1998;11:491-501.
34. Meredith N, Friberg B, Sennerby L, et al. Relationship between contact time measurements and PTV values when using the Periotest to measure implant stability. Int J Prosth 1998;11:269-75.
35. Haas R, Bernhart T, Dortbudak O, et al. Experimental study of the damping behaviour of IMZ implants. J Oral Rehabilit 1999;26:19-24.
36. Faulkner MG, Giannitsios D, Lipsett AW, et al. The use and abuse of the Periotest for 2-piece implant/abutment systems. Int J Oral & Maxillofac Implants 2001;16:486-94.
37. Olivé J, Aparicio C. Periotest method as a measure of osseointegrated oral implant stability. Int J Oral & Maxillofac Implants 1990;5:390-400.
38. Tricio J, Laohapand P, van Steenberghe D, et al. Mechanical state assessment of the implant-bone continuum: a better understanding of the Periotest method. Int J Oral & Maxillofac Implants 1995;10:43-9.
39. Tricio J, van Steenberghe D, Rosenberg D, et al. Implant stability related to insertion torque force and bone density: an in vitro study. J Prost Dent 1995;74:608-12.
40. Buser D, Weber HP, Lang NP. Tissue integration of non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. Clin Oral Implants Res 1990;1:33-40.
41. van Steenberghe D, Tricio J, Naert I, et al. Damping characteristics of bone-to-implant interfaces. A clinical study with the Periotest device. Clin Oral Implants Res 1995;6:31–9.
42. Salonen MA, Raustia AM, Kainulainen V, et al. Factors related to Periotest values in endosseal implants: a 9-year follow-up. Journal of Clinical Periodontology 1997;24:272-7.
43. Truhlar RS, Lauciello F, Morris HF, et al. The influence of bone quality on Periotest values of endosseous dental implants at stage II surgery. Journal of Oral and Maxillofacial Surgery 1997;55(Suppl. 5):55-61.
44. Truhlar RS, Morris HF, Ochi S. Stability of the bone–implant complex. Results of longitudinal testing to 60 months with the Periotest device on endosseous dental implants. Annals/Journal of Periodontology 2000;5:42-55.
45. Mericske-Stern R, Milani D, Mericske E, et al. Periotest measurements and osseointegration of mandibular ITI implants supporting overdentures. A one-year longitudinal study. Clinical Oral Implants Research 1995;6:73-82.
46. Haas R, Saba M, Mensdorff-Pouilly N, et al. Examination of the

_____________________________116 TMJ 2010, Vol. 60, No. 1
damping behavior of IMZ implants. International Journal of Oral & Maxillofacial Implants 1995;10:410-4.
47. Caulier H, Naert I, Kalk W, et al. The relationship of some histologic parameters, radiographic evaluations, and Periotest measurements of oral implants: an experimental animal study. International Journal of Oral & Maxillofacial Implants 1997;12:380-6.
48. Isidor F. Mobility assessment with the Periotest system in relation to histologic findings of oral implants. International Journal of Oral & Maxillofacial Implants 1998;13:377-83.
49. Chavez H, Ortman LF, DeFranco RL, et al. Assessment of oral implant mobility. Journal of Prosthetic Dentistry 1993;70:421-6.
50. Naert I, Alsaadi G, van Steenberghe D, et al. A 10-year randomized clinical trial on the influence of splinted and unsplinted oral implants retaining mandibular overdentures: peri-implant outcome. International Journal of Oral & Maxillofacial Implants 2004;19:695-702.
51. Tawse-Smith A, Perio C, Payne AG, et al. One-stage operative
procedure using two different implant systems: a prospective study on implant overdentures in the edentulous mandible. Clinical Implant Dentistry & Related Research 2001;3:185-93.
52. Abrahamsson I, Berglundh T, Linder E, et al. Early bone formation adjacent to rough and turned endosseous implant surfaces. An experimental study in the dog. Clinical Oral Implants Research 2004;15:381-92.
53. Brochu J-F., Anderson JD, Zarb GA. The influence of early loading on bony crest height and stability: a pilot study; International Journal of Prosthodontics 2005;18:506-11.
54. Drago CJ. A prospective study to assess osseointegration of dental endosseous implants with the Periotest instrument. International Journal of Oral & Maxillofacial Implants 2000;15:389-95.
55. Verhoeven JW, Cune MS, de Putter C. Reliability of some clinical parameters of evaluation in implant dentistry. Journal of Oral Rehabilitation 2000;27:211-6.