data submission manual - maryland state...
TRANSCRIPT

COMAR 10.25.06
Data Submission Manual
Formatted for 2002 Medical Care Data Base due June 30, 2003
Maryland Health Care Commission 4160 Patterson Avenue
Baltimore, Maryland 21215 410-764-3574
www.mhcc.state.md.us
2-14-03

TABLE OF CONTENTS
I. Introduction.........................................................................................................1
II. File Documentation...............................................................................................5
III. Special Instructions for Financial Data Elements......................................................11
IV. Data Element Documentation ................................................................................14
APPENDICES A. File Layouts .....................................................................................................26
B. Media Information............................................................................................33
C. Data Dictionary: Encounter, Pharmacy, and Provider Reports...............................34
D. Explanation of Practitioner Specialty ..................................................................43
E. Explanation of Coverage Type ..........................................................................47
F. Maryland County Zip Code Crosswalk .................................................................49
G. 2002 MCDB Payers and Payer ID Numbers .........................................................57

1
Section I
Introduction
Important Updates for 2002 MCDB Submission: 1. Reporting Period defined as “Claims adjudicated from January 1, 2002 through April 30, 2003 with a
start date of January 1, 2002.” 2. Covered Lives – Percentage of covered lives deleted from table. Table revised to request
breakdown of covered lives by delivery system for all Maryland counties. (p 9) 3. Billing & Reimbursement Information for Encounter & Pharmacy – Imbedded “+” or “-” signs will
not be allowed. If coded correctly, bill type will identify debit or credit. (p 12-13) 4. Pharmacy Billing & Reimbursement Information – Billed Charge, Patient Liability, and
Reimbursement Amount must be represented using two implied decimal places. Two zeros may be used if cents are not provided. (p 13)
5. Modifiers – AMA and HCPCS modifiers may be used to distinguish services that have been altered by a
specific condition. Payers using homegrown codes must provide documentation mapping homegrown codes to AMA modifiers or HCPCS Level II National Modifiers. (bottom p 15)
6. Place of Service codes updated according to CMS-HIPAA standards. New! Urgent Care Facility,
Value 20, added to Place of Service reporting. Urgent Care Facility defined as: Location, distinct from a hospital emergency room, an office, or a clinic, whose purpose is to diagnose and treat illness or injury for unscheduled, ambulatory patients seeking immediate medical attention. (p 17-19)
7. Type of Bill Options – Option 1 is preferred. Both options will be allowed for the 2002 MCDB
collection. Option 2 will be deleted for the 2003 MCDB collection due June 30, 2004. (p 24) 8. Pharmacy File Layout – Item 12. Date Filled is now 8 characters (instead of 10) resulting in a shorter
file length of 104. (p 31) 9. Encrypted PATIENT ID – Encryption of patient IDs on encounter & pharmacy layouts must be consistent
in order to link across files. 10. Provider Directory Report – Practitioner Last Name and Practitioner First Name must be entered
separately according to format specifications. (p 32) 11. Provider Directory Report – DEA# is a required field in this format. Please cross reference
DEA #s on Pharmacy & Provider Directory layouts. (p 32) 12. Zip Code crosswalk updated. (Appendix F, p 49)
13. 2002 MCDB reporting Payers & payer ID #s listed. (Appendix G, p 57)
For 2002 data due June 30, 2003

2
DATA SUBMISSION MANUAL Purpose: The Data Submission Manual is designed to provide payers with guidelines of technical specifications, layouts, and definitions necessary for filing the reports specified under COMAR 10.25.06.01D. The file documentation (see Section II) and data element documentation (see Section IV) must accompany all data submissions. This manual is available in electronic form on the Commission’s website at www.mhcc.state.md.us and payers are encouraged to download for use in completion of this project.
Payer ID # Please see Appendix G for a list of 2002 MCDB payers and assigned ID numbers. Please use this identifier on all submission media and documentation. Questions regarding the information in this manual should be directed to:
Ms. Sharon Gruel Maryland Health Care Commission
4160 Patterson Avenue Baltimore, Maryland 21215
Phone 410-764-3574 FAX 410-358-1236 [email protected] (e-mail)
Please direct data processing inquiries to:
Ms. Sophie Nemirovsky Social & Scientific Systems, Inc. 8757 Georgia Avenue, 12th Floor
Silver Spring, MD 20910 Phone 301-628-3264 FAX 301-628-3201
[email protected] (e-mail)
All requests for exceptions to the filing formats must be sent to the Commission on or before April 30th according to COMAR 10.25.06.11.
The data base contractor is not authorized to grant exceptions.

3
Data Set Glossary
Reporting Period Claims adjudicated from January 1, 2002 through April 30, 2003 with a start date of January 1, 2002.
Encounter Report Fee-for-service encounters and specialty care capitated encounters provided by health care practitioners and office facilities (i.e., HCFA 1500 claims). This does not include hospital facility services documented on UB 92 claims forms. The following medical services must be included:
• Physician services • Non-physician health care professionals • Freestanding Office Facilities (radiology centers, ambulatory surgical
centers, birthing centers, etc.) • Durable Medical Equipment (DME) • Prescription Drug (in a separate file) • Dental – if services are provided under a medical benefit package. • Vision - if services are provided under a medical benefit package.
Pharmacy Report These data detail prescription drugs only. Provider Directory Report These data detail all health care practitioners and suppliers who provided services to enrollees during the reporting period. Each encounter submission should be accompanied by a Provider Directory Report. In instances where the data comes from different sources, a separate Provider Directory Report must be provided (with a crosswalk of every practitioner ID listed in the Encounter Report) for each health care practitioner or supplier who provided services. Reporting Deadline June 30, 2003 # of Services Any health or medical care procedure or service rendered by a health care practitioner documented by CPT, HCPCS or locally defined code (i.e., homegrown medical procedure code). In a VARIABLE FORMAT one service is equal to one line item, multiple line items can appear on a single record (claim). In FIXED FORMAT one service corresponds to one record (service). If service includes more than one unit, it is still counted as one service. # of Claims Number of claims in VARIABLE FORMAT is equal to the number of HCFA 1500 encounters (bills) submitted. In the FIXED FORMAT, claims are also equal to the number of HCFA 1500 encounters originally received. This number would not conform with the number of records submitted using the fixed format because multiple services are sometimes submitted on one claim.

4
Payer Submission and Documentation Checklist Please use this checklist as a guideline for your data submission. Item Page #
Encounter Report layout 27
Pharmacy Report layout 31
Provider Directory Report layout 32
Media Format Information 33
Code media & documentation with your payer ID# 57 Did you include the necessary documentation in order to read your data?
File Documentation
Copies of File Layouts
Coverage Type Mapping
Delivery System Mapping
Modifier Mapping
Practitioner Specialty Mapping Place of Service Mapping Type of Bill Mapping Zip Code Crosswalk
DATA WITHOUT PROPER DOCUMENTATION WILL BE RETURNED!

5
Section II
File Documentation
• Encounter
• Pharmacy
• Provider Directory
www.mhcc.state.md.us
For 2002 data due June 30, 2003

6
MARYLAND HEALTH CARE COMMISSION MCDB Documentation Form
Payer Name (s):____________________________________________________________
Payer ID #________ (See Appendix G for a complete list of 2002 MCDB payers & Payer ID #s).
Encounter/Provider Directory Data Contact: ______________________________________
Pharmacy Data Contact: ____________________________________________________
Name/Title: _______________________________________________________________
Address: __________________________________________________________________
Telephone Number: ________________________________________________________
Facsimile Number: _________________________________________________________
E-mail Address: ____________________________________________________________
ENCOUNTER IBM 3480 Cartridge IBM 3490 or 3490E Cartridge 9-Track Reel Media Type: 4mm, 8mm Tape DLT Tape IV IBM Comp. 3.5 diskette CD-Rom CR-R Number of Media: ____________________Number of Claims: ________________________________ Blocking Factor: ____________________ Number of Services: _______________________________ Logical Record Length: ____________________________ Fixed Format Variable Format Computer Operating System: __________________________ Recording Format: ASCII EBCDIC
PROVIDER IBM 3480 Cartridge IBM 3490 or 3490E Cartridge 9-Track Reel Media Type: 4mm, 8mm Tape DLT Tape IV IBM Comp. 3.5 diskette CD-Rom CR-R Number of Media: ____________________Number of Records: ________________________________ Blocking Factor: ____________________ Logical Record Length: _____________________________ Computer Operating System: __________________________ Recording Format: ASCII EBCDIC
PHARMACY IBM 3480 Cartridge IBM 3490 or 3490E Cartridge 9-Track Reel Media Type: 4mm, 8mm Tape DLT Tape IV IBM Comp. 3.5 diskette CD-Rom CR-R Number of Media: ____________________ Number of Prescriptions:_____________________________ Blocking Factor: ____________________ Logical Record Length:______________________________ Computer Operating System: __________________________ Recording Format: ASCII EBCDIC
Please forward media and accompanying documentation to:
Mrs. Sophie Nemirovsky Social & Scientific Systems, Inc. 8757 Georgia Avenue, 12th Floor Silver Spring, MD 20910

7
ENCOUNTER DATA SUBMISSION DOCUMENTATION
1. Encounter Control Total Verification
Please complete the following table by indicating the number of covered lives and number of services by delivery system type for the time period January 1, 2002 through April 30, 2003. Use the average number of covered lives (the average number of insured individuals and their dependents) per year as the basis for your determination of enrollment. In addition, specify the total payment information for all delivery system types.
Payment Information
Delivery System Type
Covered Lives
# Services
Total Billed
Amount
Total Allowed Amount
Total Patient Liability
Total Reimburse
Amount HMO, (non-Medicaid), HMO/POS include policies with “opt out” provision in this category
PPO-POS (Point of Service Indemnity Plan)
PPO or Other Managed Care
Indemnity Care
Other (specify)
Total
$ $ $ $
Comments:__________________________________________________________________ 2. Service From Date Frequency
Please complete the table below using the month and year segments for Service From Date (data element number 27 on the encounter fixed file layout). This table will provide an assessment of your data submission. Service From Date
Month/Year #
Claims #
Services Service From Date
Month/Year #
Claims #
ServicesJan 2002 Sept 2002 Feb 2002 Oct 2002 Mar 2002 Nov 2002 Apr 2002 Dec 2002 May 2002 Jan 2003 Jun 2002 Feb 2003 Jul 2002 Mar 2003 Aug 2002 Apr 2003

8
3. Procedure Code Aggregation
Please complete the following table with claims totals according to the ranges listed. Provide a total for HCPCS and all non-coded procedures. All remaining procedure code totals should be summed into “Homegrown.”
Procedure Code Range
(data element #25 variable format) (data element #34 fixed format)
Total Allowed Charges
# Services
CPT: 99201-99499 CPT: 00100-01999 99100-99140
CPT: 10040-69979 CPT: 70010-79999 CPT: 80002-89399 CPT: 90701-99099 99141-99199
HCPCS: A0000-V5399 Not Coded (Blank) Homegrown *(please include a list of homegrown medical procedure codes and their definitions.)*
All other fields.
TOTAL
Comments____________________________________________________________________________________________________________________________________________

9
4. Regional Data Information In the following table, please indicate the total number of covered lives based on enrollee’s county of residence for claims adjudicated between January 1, 2002 through April 30, 2003). Enrollment should be based on the average number of covered lives, i.e., total number of insured individuals and their dependents across all delivery systems. If this estimation approach cannot be used, please attach documentation to indicate the approach used to develop the proportions by county.
County Breakdown of Covered Lives by Delivery System
Maryland Counties
(refer to Zip Code crosswalk in Appendix F)
Covered
Lives (across all delivery
systems)
HMO, (non-Medicaid), HMO/POS,
PPO-POS
PPO or Other
Managed Care
Indemnity Care
Other (please specify)
Allegany
Anne Arundel
Baltimore City
Baltimore
Calvert
Caroline
Carroll
Cecil
Charles
Dorchester
Frederick
Garrett
Harford
Howard
Kent
Montgomery
Prince George’s
Queen Anne’s
St. Mary’s
Somerset
Talbot
Washington
Wicomico
Worcester TOTAL (all eligible
enrollees for reporting cycle)

10
PHARMACY DATA SUBMISSION DOCUMENTATION
1. Date Filled Frequency (Pharmacy)
Please complete the table below using the month and year segments for Date Filled (data element number 12 on the file layout). This table will provide an assessment of your data submission.
Month/Year # Prescriptions
Month/Year # Prescriptions
Prior to Jan 2002 Sep 2002 Jan 2002 Oct 2002 Feb 2002 Nov 2002 Mar 2002 Dec 2002 Apr 2002 Jan 2003 May 2002 Feb 2003 Jun 2002 Mar 2003 Jul 2002 Apr 2003
Aug 2002 2. National Drug Code (NDC)
Please complete the table below with totals from your pharmacy claims data. Provide a total for NDC and all non-coded drugs. All remaining drug code totals should be summed under “Not National Drug Codes.”
Code Range Total Reimbursement
Amount (data element #15)
# Prescriptions
NDC Not Coded Not National Drug Codes TOTAL
Comments____________________________________________________________________________________________________________________________________________

11
Section III
Special Instructions for Financial Data Elements
www.mhcc.state.md.us
For 2002 data due June 30, 2003

12
Billing and Reimbursement Information ENCOUNTER FILE
Each of the following financial fields must be recorded by line item. The value represented by each field must be rounded to whole dollars (i.e., no decimals) on the encounter file. Financial information includes:
• Billed Charge • Allowed Amount • Patient Liability • Reimbursement Amount
The financial format must be consistent for all financial fields. Imbedded “+” or “-” signs are not allowed. If bill type is correctly coded, it will identify debit and credit. For CAPITATED SERVICES: billed charge, allowed amount, and reimbursement amount should be equal to –999. All financials should be either numeric format (ASCII or EBCDIC) or signed overpunch.
Examples of text format which must be consistent for all financial fields include:
• 1997 • 1998 • 1999
• - 1997 • - 1998 • - 1999
Examples of signed overpunch format which must be consistent for all financial fields include: POSITIVE • 199{ = 1990 • 199B = 1992 • 199D = 1994 • 199F = 1996 • 199H = 1998 • 199A = 1991 • 199C = 1993 • 199E = 1995 • 199G = 1997 • 199I = 1999 NEGATIVE • 199{ = -1990 • 199K = -1992 • 199M = -1994 • 199O = -1996 • 199Q = -1998 • 199J = -1991 • 199L = -1993 • 199N = -1995 • 199P = -1997 • 199R = -1999
FINANCIAL INFORMATION GLOSSARY
FOR ENCOUNTER FILE
Line Item: A single line entry on a bill/claim for each health care service rendered. The line item contains information on each procedure performed including modifier (if appropriate), service dates, units (if applicable), and practitioner charges. The line item also includes allowed amount, patient liability, and reimbursement amount by line item. Billed Charge: Dollar amount as billed by the practitioner for health care services rendered. Each line item of a claim/bill must include the practitioner’s billed charges rounded to whole dollars (i.e., no decimals).
Allowed Amount: The retail amount for the specified procedure code. Each line item must include the payer’s retail amount rounded to whole dollars (i.e., no decimals). Patient Liability: The amount that the patient is required to pay for a particular service (i.e., coinsurance, copayment and deductible). Each line item must include the patient’s liability rounded to whole dollars (i.e., no decimals).
Reimbursement Amount: The amount paid to a practitioner, other health professional, or office facility. Each line item on the claim should have a reimbursement amount rounded to whole dollars (i.e., no decimals).

13
Billing and Reimbursement Information PHARMACY FILE
Each of the following financial fields must be recorded by line item. The value of financial field must be represented using two implied decimal places. Use 2 zeros - .00 - if cents are not provided. Financial information includes:
• Billed Charge • Patient Liability • Reimbursement Amount
The financial format must be consistent for all financial fields. Imbedded “+” or “-” signs are not allowed. If bill type is correctly coded, it will identify debit and credit. All financials should be either numeric format (ASCII or EBCDIC) or signed overpunch.
Examples of text format which must be consistent for all financial fields include:
• 1997 • 1998 • 1999
• - 1997 • - 1998 • - 1999
Examples of signed overpunch format which must be consistent for all financial fields include: POSITIVE • 199{ = 1990 • 199B = 1992 • 199D = 1994 • 199F = 1996 • 199H = 1998 • 199A = 1991 • 199C = 1993 • 199E = 1995 • 199G = 1997 • 199I = 1999 NEGATIVE • 199{ = -1990 • 199K = -1992 • 199M = -1994 • 199O = -1996 • 199Q = -1998 • 199J = -1991 • 199L = -1993 • 199N = -1995 • 199P = -1997 • 199R = -1999
FINANCIAL INFORMATION GLOSSARY FOR PHARMACY FILE
Line Item: A single line entry on a PRESCRIPTION SERVICE. The line item contains information on each PRESCRIPTION filled, including date filled, drug quantity and supply. This line item also includes billed charge, patient liability, and reimbursement amount for each prescription. Billed Charge: PRESCRIPTION retail price USING 2 IMPLIED DECIMAL POINTS, including ingredient cost, dispensing fee, tax, and administrative expenditures. Patient Liability: The amount that a patient is required to pay per prescription (i.e., coinsurance, copayment and deductible). Each line item of a prescription service must include the patient’s liability USING 2 IMPLIED DECIMAL POINTS. Reimbursement Amount: The amount paid to the pharmacy by the payer. Each line item of a pharmacy service should list the reimbursement amount USING 2 IMPLIED DECIMAL POINTS.

14
Section IV
Data Element Documentation
www.mhcc.state.md.us
For 2002 data due June 30, 2003

15
Coverage Type
Coverage Type: A data field that indicates type of insurance coverage (i.e., individual, Medigap, self-insured, employee sponsored, etc.). Instructions: Please identify your enrollee’s type of insurance coverage as mapped to the COMAR defined coverage types. Also, indicate the number of services (or rows) in your data set. See Appendix E for additional explanation of coverage type.
COMAR Information Payer Information
Coverage Type Value Description (describe values mapped from payer system)
# Claims
# Services
Medicare Supplemental (i.e. Individual, Group, WRAP)
1
Individual Plan 2 Private Employer Sponsored, Fully Self-Insured
3
Private Employer Sponsored, Insured
4
Public Employee (federal/FEHBP, state, county, local/municipal government and public school teachers)
5
Comprehensive Standard Health Benefit Plan (Private or Public Employee) The CSHBP applies to small businesses (i.e., public or private employers) with 2 to 50 eligible employees or a self-employed individual.
6
Medicare+Choice Services provided by a Medicare HMO under contract with the Centers for Medicare and Medicaid Services (CMS)
7
Unknown
9
Using Modifiers
Modifier: A discriminate code used by health care practitioners to indicate that a service was altered in some way from the stated CPT descriptor without changing the definition. Instructions: MHCC accepts national standard modifiers approved by the American Medical Association as published in the 2002 Current Procedure Terminology. Modifiers approved for Hospital Outpatient Use: Level 1 (CPT) and Level II (HCPCS/National) modifiers. Payers are required to use the following Level II (HCPCS) modifiers to identify Nurse Anesthetist services:
• QX – Nurse Anesthetist service; under supervision of a doctor • UZI – Nurse Anesthetist service, without the supervision of a doctor

16
Delivery System Type
Delivery System Type: A data field that indicates the payer’s product line (i.e., HMO, Indemnity, POS, etc. – see definitions in Text Box below). Instructions: Please identify how your product line is mapped to the COMAR defined delivery system types. Also, indicate the number of services (or rows) in your data set. COMAR delivery system types include:
COMAR Information Payer Information
Delivery System Types Value Description (describe values mapped from payer system)
# Claims
# Services
HMO (non-Medicaid, Includes Medicare+Choice)
1
PPO-POS 2 PPO or Other Managed Care 3 Indemnity Care 4 HMO-POS Rider 5 Not Coded 9
DELIVERY SYSTEM TYPE DESCRIPTION
Health Maintenance Organization (HMO)
• HMOs provide members care using specific doctors, hospitals and other health care providers that make up a coordinated system of patient care called a “network.”
• HMOs require recipients to choose a primary care provider (PCP) from a list of network providers.
• A referral is required from a member’s PCP for specialty care.
Point-of-Service (POS)
• POS products are much the same as HMOs when members receive services within the plan’s network.
• At additional cost, members can use out-of-network providers without getting a referral.
Preferred Provider Organization (PPO)
• The PPO health plan is similar to traditional fee-for-service health insurance.
• Members choose a provider, but pay less out of pocket if the provider participates in the network.
• Out-of-pocket expenses are higher if a practitioner is chosen from out-of-network.
Indemnity Care • Members independently select providers. • Insurance reimburses the provider and member
on a fee-for-service basis after the patient has satisfied any applicable deductible.
HMO-POS Rider • HMO Point-of-Service health insurance coverage allows members to see out-of-network providers. Coinsurance and deductibles usually apply to this type of coverage.

17
Place of Service
Place of Service: The location where health care services are rendered. Definitions provided on pages 18 & 19. Instructions: In the description column, please describe the values as mapped from your system and indicate the number of services (or rows) in your encounter data set.
CMS/HIPAA Information Payer Information Place of Service Value Description
(describe values mapped from payer system) #
Claims #
ServicesProvider’s Office 11 Patient’s Home 12 Urgent Care Facility 20 Inpatient Hospital 21 Outpatient Hospital 22 Emergency Room, hospital portion 23 Ambulatory Surgical Center 24 Birthing Center 25 Military Treatment Facility 26
Nursing Facility 32 Custodial Care Facility 33 Hospice 34 Ambulance – Land 41 Ambulance – Air or Water 42 Inpatient Psychiatric Facility 51 Psychiatric Facility, Partial Hospitalization 52 Community Mental Health Center 53
Intermediate Care Facility/Mentally Retarded
54
Residential Substance Abuse Treatment Facility
55
Psychiatric Residential Treatment Center 56
Comprehensive Inpatient Rehabilitation Facility
61
Comprehensive Outpatient Rehabilitation Facility
62
End Stage Renal Disease Treatment Facility
65
State or Local Public Health Clinic 71 Independent Laboratory & Imaging 81 Other Place of Service 99

18
Place of Service Codes for Professional Claims
Centers for Medicare & Medicaid Services
CMS –Code(s) Place of Service Description
11 Office Location, other than a hospital, skilled nursing facility (SNF), military treatment facility, community health center, state or local public health clinic, or intermediate care facility (ICF), where the health professional routinely provides health examinations, diagnosis, and treatment of illness or injury on an ambulatory basis.
12 Home Location, other than a hospital or other facility, where the patient receives care in a private residence.
20 Urgent Care Facility Location, distinct from a hospital emergency room, an office, or a clinic, whose purpose is to diagnose and treat illness or injury for unscheduled, ambulatory patients seeking immediate medical attention.
21 Inpatient Hospital A facility, other than psychiatric, which primarily provides diagnostic, therapeutic (both surgical and nonsurgical), and rehabilitation services by, or under, the supervision of physicians to patients admitted for a variety of medical conditions.
22 Outpatient Hospital A portion of a hospital which provides diagnostic, therapeutic (both surgical and nonsurgical), and rehabilitation services to sick or injured persons who do not require hospitalization or institutionalization.
23 Emergency Room – Hospital
A portion of a hospital where emergency diagnosis and treatment of illness or injury is provided.
24 Ambulatory Surgical Center A freestanding facility, other than a physician’s office, where surgical and diagnostic services are provided on an ambulatory basis.
25 Birthing Center A facility, other than a hospital’s maternity facilities or a physician’s office, which provides a setting for labor, delivery, and immediate postpartum care as well as immediate care of newborn infants.
26 Military Treatment Facility A medical facility operated by one or more of the Uniformed Services Military Treatment Facility (MTF) also refers to certain former U.S. Public Health Service (USPHS) facilities now designated as Uniformed Service Treatment Facilities (USTF).
31 Skilled Nursing Care Use code 32.
32 Nursing Facility A facility which primarily provides to residents skilled nursing care and related services for the rehabilitation of injured, disabled, or sick persons, or, on a regular basis, health-related care services above the level of custodial care to other than mentally retarded individuals.
33 Custodial Care Facility A facility that provides room, board and other personal assistance services, generally on a long-term basis, and which does not include a medical component.
34 Hospice A facility, other than a patient’s home, in which palliative and supportive care for terminally ill patients and their families are provided.
41 Ambulance – Land A land vehicle specifically designed, equipped and staffed for lifesaving and transporting the sick or injured.
42 Ambulance – Air or Water An air or water vehicle specifically designed, equipped and staffed for lifesaving and transporting the sick or injured.

19
51 Inpatient Psychiatric Facility
A facility that provides inpatient psychiatric services for the diagnosis and treatment of mental illness on a 24-hour basis, by or under the supervision of a physician.
52 Psychiatric Facility Partial Hospitalization
A facility for the diagnosis and treatment of mental illness that provides a planned therapeutic program for patients who do not require full time hospitalization, but who need broader programs than are possible from outpatient visits to a hospital-based or hospital-affiliated facility.
53 Community Mental Health Center
A facility where outpatient mental health services are provided in individual or group therapy settings by mental health care professionals, such as physicians, psychologists, social workers, nurse psychotherapists, licensed clinical professionals, and licensed marriage and family therapists.
54 Intermediate Care Facility/Mentally Retarded
A facility which primarily provides health-related care and services above the level of custodial care to mentally retarded individuals but does not provide the level of care or treatment available in a hospital or SNF.
55 Residential Substance Abuse Treatment Facility
A facility, which provides treatment for substance (alcohol and drug) abuse to live-in residents who do not require acute medical care. Services include individual and group therapy and counseling, family counseling, laboratory tests, drugs and supplies, psychological testing, and room and board.
56 Psychiatric Residential Treatment Center
A facility or distinct part of a facility for psychiatric care that provides a total 24-hour therapeutically planned and professionally staffed group living and learning environment.
60 Mass Immunization Center A location where providers administer pneumococcal pneumonia and influenza virus vaccinations and submit these services as electronic media claims, paper claims, or using the roster billing method. This generally takes place in a mass immunization setting, such as, a public health center, pharmacy, or mall but may include a physician office setting.
61 Comprehensive Inpatient Rehabilitation Facility
A facility that provides comprehensive rehabilitation services under the supervision of a physician to inpatients with physical disabilities. Services include physical therapy, occupational therapy, speech pathology, social or psychological services, and orthotics and prosthetics services.
62 Comprehensive Outpatient Rehabilitation Facility
A facility that provides comprehensive rehabilitation services under the supervision of a physician to outpatients with physical disabilities. Services include physical therapy, occupational therapy, and speech pathology services.
65 End Stage Renal Disease Treatment Facility
A facility other than a hospital, which provides dialysis treatment, maintenance, and/or training to patients or caregivers on an ambulatory or home-care basis.
71 State or Local Public Health Clinic; Local Health
Department
A facility maintained by either state or local health departments that provides ambulatory primary medical care under the general direction of a physician.
72 Rural Health Clinic Use code 71.
81 Independent Laboratory A laboratory certified to perform diagnostic and/or clinical tests independent of an institution or a physician’s office.
99 Other Place of Service Other place of service not identified above.

20
Practitioner Specialty
Practitioner Specialty: The health care field in which a physician, licensed health care professional, dental practitioner, or office facility has been certified. Instructions: In the description column, please list the payer specialty description(s) mapped to the COMAR defined specialties (more than one specialty can map to a COMAR defined specialty). Please indicate the number of services (or rows) in your encounter data set that links to those specialties in the Provider Directory file. See Appendix D for examples of practitioner specialty expansions and/or consolidations. Physicians: ♦LISTED ALPHABETICALLY & NUMERICALLY.
COMAR Information
Practitioner Specialty ValueDescription
(payer specialty descriptions mapped to COMAR defined specialties)
# Claims
# Services
General Practice 001 General Surgery 002 Allergy & Immunology 003 Anesthesiology 004 Cardiology 005 Dermatology 006 Emergency Medicine 007 Endocrinology Medicine 008 Family Practice 009 Gastroenterology 010 Geriatrics 011 Hand Surgery 012 Hematology 013 Internal Medicine 014 Infectious Disease 015 Multi-Specialty Medical
Practice ♦
101
Nephrology 016
Neonatology ♦ 100 Neurology 017 Nuclear Medicine 018
Obstetrics/Gynecology ♦ 039

21
COMAR Information
Practitioner Specialty ValueDescription
(payer specialty descriptions mapped to COMAR defined specialties)
# Claims
# Services
Oncology 019 Ophthalmology 020 Orthopedic Surgery 021 Osteopathy (include Manipulations)
022
Otology, Laryngology, Rhinology, Otolaryngology
023
Pathology 024 Pediatrics 025 Peripheral Vascular Disease or Surgery
026
Plastic Surgery 027 Physical Medicine and Rehabilitation
028
Proctology 029 Psychiatry 030 Pulmonary Disease 031 Radiology 032 Rheumatology 033 Surgical Specialty Not Listed Here
034
Thoracic Surgery 035 Urology 036 Other Specialties not listed (public health, industrial medicine)
037
Physician w/o Specialty Identified & Specialty not listed here
038
Obstetrics/Gynecology ♦ 039
Neonatology ♦ 100 Multi-Specialty Medical
Practice ♦
101
♦ LISTED ALPHABETICALLY & NUMERICALLY.

22
Other Health Care Professionals:
COMAR Information
Practitioner Specialty ValueDescription
(payer specialty descriptions mapped to COMAR defined
specialties)
# Claims
# Services
Acupuncturist 040 Alcohol/Drug Detox Services 041 Ambulance Services 042 Audiologist/Speech Pathologist 043 Chiropractor 044 Freestanding Clinic (Not a Government Agency)
045
Day Care Facility (Medical, Mental Health)
046
Dietitian/Licensed Nutritionist 047 Home Health Provider 048 Mental Health Clinic 102 Advanced Practice Nurse: Anesthetist
049
Advanced Practice Nurse: Midwife
050
Advanced Practice Nurse: Nurse Practitioner
051
Advanced Practice Nurse: Psychotherapist
052
Nurse – Other than Advanced Practice
053
Occupational Therapist 054 Optometrist 055 Podiatrist 056 Physical Therapist 057 Psychologist 058 Clinical Social Worker 059 Public Health or Welfare Agency (federal, state and local gov)
060
Respiratory Therapist 063 Voluntary Health Agency 061 Other Specialty Not Listed Above 062

23
Dental:
COMAR Information
Practitioner Specialty Value Description
(payer specialty descriptions mapped to COMAR defined specialties)
# Claims
# Services
General Dentist 070 Endodontist 071 Orthodontist 072 Oral Surgeon 073 Pedodontist 074 Periodontist 075 Prosthodontist 076
Office Facilities:
COMAR Information
Practitioner Specialty Value Description
(payer specialty descriptions mapped to COMAR defined specialties)
# Claims
# Services
Freestanding Pharmacy (includes grocery)
080
Mail Order Pharmacy 081 Independent Laboratory 082 Independent Medical Supply Company
083
Optician/Optometrist (for lenses and eye glasses)
084
Please specify whether using professional services or supplier codes for the following:
All Other Supplies 085 Freestanding Medical Facility
090
Freestanding Surgical Facility
091
Freestanding Imaging Center
092
Other Facility 093

24
Type of Bill Type of Bill: The data field that describes payment and adjustment status. NOTE: Capitated services on the Encounter File are identified as services where at least three financial variables (billed charge, allowed amount, and reimbursement amount) are equal to –999. USE ONLY ONE OF THE TWO OPTIONS LISTED BELOW.
Option 1 - PREFERRED
Value Label Definition 1 Final Bill Total adjusted amount of all credits and debits paid for a
claim by the insurance company to the provider.
8 Capitated Services
Set of predefined services provided by the provider to the plan’s enrollees under contract with an insurance company or managed care plan in exchange for a fixed and guaranteed monthly payment for each enrollee assigned to the provider.
Option 2
Value Label Definition 1 Debit Total amount per claim paid by the insurance company to
the provider.
2 Credit
Total amount per claim credited to the insurance company by the provider due to overpayment, paying the wrong provider, or paying for additional services that were denied.
3 Partial Debit
Partial amount per claim paid by the insurance company to the provider.
4 Partial Credit
Partial amount per claim credited to the insurance company by the provider due to overpayment, paying the wrong provider, or paying for additional services that were denied.
8 Capitated Services
Set of predefined services provided by the provider to the plan’s enrollees under contract with an insurance company or managed care plan in exchange for a fixed and guaranteed monthly payment for each enrollee assigned to the provider.
Instructions: Identify type of bill in the column provided. Please indicate the number of services (or rows) in your data set.
Type of Bill Description Bill Type # Claims
# Services

25
APPENDICES

26
Appendix A
File Layouts
www.mhcc.state.md.us
For 2002 data due June 30, 2003

27
File Layout
Encounter Data Report Submission This report details fee-for-service and specialty-care capitated encounters provided by health care practitioners and office facilities from January 1, 2002 through April 30, 2003. Please provide information on all health care services provided to Maryland residents whether provided by a practitioner or office facility located in-state or out-of-state. COMAR specifies that the Encounter Data Report file layout can be either fixed or variable. The two file layouts are as follows. Option 1, FIXED FORMAT: (preferred) Using the fixed format, it is possible that multiple services will be reported for each claim. Count each reported health care service even though documented on a single claim. For example, if a single claim contains 3 procedures then 3 services are documented as one line item.
Field Name LengthType
A=alphanumeric N=numeric
Dec Start End
1. Patient ID (encrypted) 12 A 1 12 2. Patient Date of Birth
(CCYYMM00) 8 N 13 20
3. Patient Sex 1 N 21 21 4. Filler (space fill) 1 A 22 22
5. Patient Zip Code 5 N 23 27 6. Patient Covered by Other
Insurance 1 N 28 28
7. Coverage Type (this field must be mapped –see pg. 15)
1 N 29 29
8. Delivery System Type (this field must be mapped –see pg. 16)
1 N 30 30
9. Claim Related Condition 1 N 31 31 10. Practitioner Federal Tax ID 9 A 32 40 11. Participating Provider Flag 1 N 41 41 12. Type of Bill (this field must be
mapped –see pg. 26) 1 A 42 42
13. Claim Control Number (Include on each record as this is the key to summarizing service detail to claim level)
23 A 43 65
14. Claim Paid Date (CCYYMMDD) 8 N 66 73 15. Number of Diagnosis Codes 2 N 74 75 16. Number of Line Items 2 N 76 77 17. Diagnosis Code 1 Remove
imbedded decimal points. 5 A 78 82
18. Diagnosis Code 2 5 A 83 87
19. Diagnosis Code 3 5 A 88 92 20. Diagnosis Code 4 5 A 93 97 21. Diagnosis Code 5 5 A 98 102 22. Diagnosis Code 6 5 A 103 107 23. Diagnosis Code 7 5 A 108 112 24. Diagnosis Code 8 5 A 113 117 25. Diagnosis Code 9 5 A 118 122 26. Diagnosis Code 10 5 A 123 127

28
Field Name Length
Type A=alphanumeric
N=numeric Dec Start End
27. Service From Date (CCYYMMDD)
8 N 128 135
28. Service Thru Date (CCYYMMDD)
8 N 136 143
29. Filler 2 A blank blank 30. Place of Service 2 N 146 147 31. Service Location Zip Code 5 A 148 152 32. Service Unit Indicator 1 N 153 153 33. Units 3 N 154 156 34. Procedure Code 6 A 157 162 35. Modifier I (this field must be
mapped –see pg. 17) 2 A 163 164
36. Modifier II (this field must be mapped –see pg. 18)
2 A 165 166
37. Servicing Practitioner ID 11 A 167 177 38. Billed Charge (line item
amounts required – see pg. 12) 9 N 178 186
39. Allowed Amount (line item amounts required – see pg. 12)
9 N 187 195
40. Reimbursement Amount (line item amounts required – see pg. 12)
9 N 196 204
41. Patient Liability (line item amounts required – see pg. 12)
9 N 205 213
Please provide detailed documentation with your data submission
Detailed documentation can consist of a map to data statistics on financial variables or any supportive references to assist SSS in assessing programmed data.
The Encounter data must link to Pharmacy data by PATIENT ID.
If the files do not link, MHCC will return the file for correction.
Encryption of Patient ID must be consistent to encryption of Patient ID in Pharmacy File.

29
Encounter Data Report Submission Option 2, VARIABLE FORMAT: Count each reported service as a health care claim even though the claim may contain multiple services. For example, if a claim documents 3 services then 3 occurrences in the line item section must be reported.
Field Name Length
Type A=alphanumeric
N=numeric Dec Occurs Start End
1. Patient ID (encrypted) 12 A 1 12 2. Patient Date of Birth
(CCYYMM00) 8 N 13 20
3. Patient Sex 1 N 21 21 4. Filler (space fill) 1 A 22 22 5. Patient Zip Code 5 N 23 27 6. Patient Covered by Other
Insurance 1 N 28 28
7. Coverage Type (this field must be mapped –see pg. 15)
1 N 29 29
8. Delivery System Type (this field must be mapped –see pg. 16)
1 N 30 30
9. Claim Related Condition 1 N 31 31 10. Practitioner Federal Tax ID 9 A 32 40 11. Participating Provider Flag 1 N 41 41 12. Type of Bill (this field must be
mapped –see pg. 26) 1 A 42 42
13. Claim Control Number (This is the key to summarizing service detail to claim level & must be included on each record.)
23 A 43 65
14. Claim Paid Date (CCYYMMDD) 8 N 66 73 15. Number of Diagnosis Codes 2 N 74 75 16. Number of Line Items 2 N 76 77
End of Fixed Record Portion:
Field Name Length
Type A=alphanumeric
N=numeric Dec Occurs Start End
4 Items 17-32 represent line items only. Repeat format 18-32 for each additional line item.
82 26 128
17. Diagnosis (Field will hold up to 10 diagnosis codes. Leave fields blank if not available.) Remove imbedded decimal points.
5 A 10 78 127
18. Service From Date (CCYYMMDD)
8 N
19. Service Thru Date (CCYYMMDD)
8 N
20. Filler 2 A blank blank 21. Place of Service 2 N 22. Service Location Zip 5 A 23. Service Unit Indicator 1 N 24. Units 3 N 25. Procedure Code 6 A 26. Modifier I (this field must be
mapped –see pg. 17) 2 A

30
Field Name Length
Type A=alphanumeric
N=numeric Dec Occurs Start End
27. Modifier II (this field must be mapped –see pg. 18)
2 A
28. Servicing Practitioner ID 11 A 29. Billed Charge (line item
amounts required – see pg. 12) 9 N
30. Allowed Amount (line item amounts required – see pg. 12)
9 N
31. Reimbursement Amount (line item amounts required – see pg. 12)
9 N
32. Patient Liability (line item amounts required – see pg. 12)
9 N
Please provide detailed hard copy documentation with your data
submission.
The Encounter data must link to Pharmacy data by PATIENT ID.
If the files do not link, MHCC will return the file for correction.
Encryption of Patient ID must be consistent to encryption
of Patient ID in Pharmacy File.

31
File Layout Pharmacy Data Report Submission
This report details all prescription drug encounters for your enrollees filled from January 1, 2002 through April 30, 2003. Please provide information on all prescription drugs provided to Maryland residents whether provided by a pharmacy located in-state or out-of-state. Do not include pharmacy supplies or prosthetics. COMAR specifies the Pharmacy Report be submitted separately from the Encounter Report. Fixed Format:
Field Name Length
Type A=alphanumeric
N=numeric Dec Start End
1. Patient ID (encrypted) 12 A 1 12 2. Patient Sex 1 N 13 13 3. Patient Zip Code 5 N 14 18
4.
Patient Date of Birth (CCYYMM00)
8 N 19 26
5. NCPDP Number 7 N 27 33 6. Pharmacy Zip Code (location
where prescription was filled and dispensed)
5 N 34 38
7. Practitioner DEA # (left justified field, for many payers the last 2 positions on the right will be blank)*
11 A 39 49
8. NDC Code 11 N 50 60 9. Drug Compound 1 N 61 61
10. Drug Quantity 5 N 62 66 11. Drug Supply 3 N 67 69 12. Date Filled (CCYYMMDD) 8 N 70 77 13. Patient Liability (line item
amounts required – see pg. 13) 9 N 2 78 86
14. Billed Charge (line item amounts required – see pg. 13)
9 N 2 87 95
15. Reimbursement Amount (line item amounts required – see pg. 13)
9 N 2 96 104
• Please note which of the following you are using to link the Pharmacy Data
Report with the Provider Directory Report:
DEA (Drug Enforcement Agency) #
Practitioner Federal Tax ID
Combination of both of the above
The Pharmacy data must link to Encounter data by PATIENT ID.
If the files do not link, MHCC will return the file for correction.
Encryption of Patient ID must be consistent to encryption of Patient ID in Encounter File.

32
File Layout Provider Directory Report Submission
This report details all health care practitioners (including other health care professionals, dental/vision services covered under a medical plan, and office facilities) who provided services to your enrollees from January 1, 2002 through April 30, 2003. Please provide information on all in-state practitioners as well as those out-of-state who served Maryland residents. COMAR 10.25.06 specifies the file layout for the Provider Directory Report be an 100 byte fixed format. The file layout is as follows:
Field Name Length
Type A=alphanumeric
Dec Start End
1. Servicing Practitioner ID 11 A 1 11 2. Practitioner Federal Tax ID 9 A 12 20 3. Practitioner Last Name * 40 A 21 60
4. Practitioner First Name * 20 A 61 80
5. Practitioner Specialty – 1 3 A 81 83 6. Practitioner Specialty – 2 3 A 84 86 7. Practitioner Specialty – 3 3 A 87 89 8. Practitioner DEA # 11 A 90 100
REMINDER
• Are the Practitioner First and Last names in their separate
fields? • Does the Practitioner DEA# match the Pharmacy File
DEA#?

33
Appendix B Media Format Information
Instructions: Data must be provided on one of the following media using either the ASCII or EBCDIC recording format. Please label all media & documentation with your payer ID #. CD (preferred) Record Type: Fixed (preferred) or Variable length records Recording Format: ASCII or EBCDIC CR-R Record Type: Fixed (preferred) or Variable length records Recording Format: ASCII or EBCDIC IBM 3480/3480E or 3490/3490E Cartridge (preferred) Block Size: 16,000 bytes minimum, 32,760 bytes maximum Record Type: Fixed (preferred) or Variable length records
Recording Format: ASCII or EBCDIC Labels: Standard IBM labels preferred Media: 3480/3480E or 3490/3490E Cartridge Density: 3480/3480E or 3490/3490E Cartridge – default density 9 Track Magnetic Tape Reels Block Size: 16,000 bytes minimum, 32,760 bytes maximum Record Type: Fixed (preferred) or Variable length records Recording Format: ASCII or EBCDIC Labels: Standard IBM labels preferred Media: 9 Track Tape Density: 1600 or 6250 BPI 4 mm or 8 mm Tape Block Size: 16,000 bytes minimum, 32,760 bytes maximum Record Type: Fixed (preferred) or Variable length records Recording Format: ASCII or EBCDIC Media: 4mm or 8mm tape using dd or TAR commands Density: 1600 BPI DLT Tape IV Block Size: 16,000 bytes minimum, 32,760 bytes maximum Record Type: Fixed (preferred) or Variable length records Recording Format: ASCII or EBCDIC Media: DLT using dd or TAR commands Density: 1600 BPI IBM-compatible 3.5 inch diskette Block Size: N/A Record Type: Fixed (preferred) or Variable length records Recording Format: ASCII or EBCDIC Labels: N/A Media: IBM-compatible 1.44 Mbyte, 3.5-inch diskette PKZIP compressed

34
Appendix C
Data Dictionary
www.mhcc.state.md.us

35
Dat
a D
icti
onar
y –
EN
CO
UN
TER
Fi
eld
Nam
e C
OM
AR
D
escr
ipti
on
Fiel
d C
onte
nts
Pa
tient
ID
10
.25.
06.0
6.D
1 Pa
tient
’s u
niqu
e id
entif
icat
ion
num
ber,
as
sign
ed b
y th
e pa
yer
and
encr
ypte
d.
Patie
nt D
ate
of B
irth
10.2
5.06
.06.
D2
Dat
e of
pat
ient
’s b
irth
usin
g 00
inst
ead
of
day.
CCYY
MM
00
Patie
nt S
ex
10.2
5.06
.06.
D3
Sex
of t
he p
atie
nt.
1 M
ale
2 Fe
mal
e 3
Not
Cod
ed
Fi
ller
10.2
5.06
.06.
D4
Spac
e fil
ler.
Patie
nt Z
ip C
ode
10.2
5.06
.06.
D5
Zip
code
of
patie
nt’s
res
iden
ce.
Pa
tient
Cov
ered
by
Oth
er
Insu
ranc
e 10
.25.
06.0
6.D
6 In
dica
tes
whe
ther
pat
ient
has
add
ition
al
insu
ranc
e co
vera
ge.
0 N
o 1
Yes,
oth
er c
over
age
is p
rimar
y 2
Yes,
oth
er c
over
age
is s
econ
dary
9
Not
Cod
ed
Cove
rage
Typ
e 10
.25.
06.0
6.D
7 Pa
tient
’s t
ype
of in
sura
nce
cove
rage
. 1
Med
icar
e Su
pple
men
tal (
i.e.,
Indi
vidu
al,
Gro
up,
WRA
P)
2 In
divi
dual
Pla
n 3
Priv
ate
Empl
oyer
Spo
nsor
ed F
ully
Sel
f-
I
nsur
ed
4 Pr
ivat
e Em
ploy
er S
pons
ored
, In
sure
d 5
Publ
ic E
mpl
oyee
(fe
dera
l/FEH
BP,
stat
e, c
ount
y,
loca
l/mun
icip
al g
over
nmen
t an
d pu
blic
sch
ool t
each
ers)
6
Com
preh
ensi
ve S
tand
ard
Hea
lth B
enef
it Pl
an (
a se
lf em
ploy
ed in
divi
dual
or
smal
l bus
ines
ses
(pub
lic o
r pr
ivat
e em
ploy
ers)
with
2-5
0 el
igib
le e
mpl
oyee
s 7
Med
icar
e+Ch
oice
ser
vice
s pr
ovid
ed b
y a
Med
icar
e H
MO
un
der
cont
ract
with
the
Cen
ters
for
Med
icar
e an
d M
edic
aid
Serv
ices
(CM
S)
9 U
nkno
wn
Del
iver
y Sy
stem
Typ
e 10
.25.
06.0
6.D
8 Ty
pe o
f del
iver
y sy
stem
ren
derin
g se
rvic
e.
1 H
MO
(no
n-M
edic
aid,
incl
udes
Med
icar
e)
2 PP
O-P
OS
3 PP
O o
r O
ther
Man
aged
Car
e 4
Inde
mni
ty C
are
5 H
MO
-PO
S Ri
der
9 N
ot C
oded

36
Fiel
d N
ame
CO
MA
R
Des
crip
tion
Fi
eld
Con
ten
ts
Clai
m R
elat
ed C
ondi
tion
10.2
5.06
.06.
D9
Des
crib
es c
onne
ctio
n, if
any
, bet
wee
n pa
tient
’s c
ondi
tion
and
empl
oym
ent,
au
tom
obile
acc
iden
t, o
r ot
her
acci
dent
.
0 N
on-a
ccid
ent
1 W
ork
2 Au
to A
ccid
ent
3 O
ther
Acc
iden
t 9
Not
Cod
ed
Prac
titio
ner
Fede
ral T
ax I
D
10.2
5.06
.06.
D10
Em
ploy
er T
ax I
D o
f the
pra
ctiti
oner
, pra
ctic
e or
offi
ce f
acili
ty r
ecei
ving
pay
men
t fo
r se
rvic
es.
Part
icip
atin
g Pr
ovid
er F
lag
10.2
5.06
.06.
D11
Id
entif
ies
paye
r or
igin
of p
ract
ition
er,
prac
tice
or o
ffice
fac
ility
rei
mbu
rsem
ent
unde
r an
HM
O, p
refe
rred
pro
vide
r or
oth
er
man
aged
car
e co
ntra
ctua
l agr
eem
ent.
1 Ye
s 2
No
3 N
ot C
oded
Type
of
Bill
10.2
5.06
.06.
D12
D
escr
ibes
pay
men
t an
d ad
just
men
t st
atus
of
a cl
aim
. A
djus
tmen
ts in
clud
e pa
ying
a c
laim
m
ore
than
onc
e, p
ayin
g ad
ditio
nal s
ervi
ces
that
may
hav
e be
en d
enie
d or
cre
ditin
g a
prov
ider
due
to
over
paym
ent
or p
ayin
g th
e w
rong
pro
vide
r.
Clai
m C
ontr
ol N
umbe
r 10
.25.
06.0
6.D
13
Inte
rnal
pay
er c
laim
num
ber
used
for
trac
king
.
Clai
m P
aid
Dat
e 10
.25.
06.0
6.D
14
The
date
a c
laim
was
aut
horiz
ed fo
r pa
ymen
t.
CCYY
MM
DD
Num
ber
of D
iagn
osis
Cod
es
10.2
5.06
.06.
D15
Th
e nu
mbe
r of
dia
gnos
is c
odes
, up
to
ten.
1
thro
ugh
10.
Max
imum
is 1
0.
Num
ber
of L
ine
Item
s 10
.25.
06.0
6.D
16
If u
sing
Var
iabl
e Fo
rmat
, the
# o
f lin
e ite
ms
com
plet
ed in
the
var
iabl
e po
rtio
n (d
ata
elem
ents
22-
32)
mus
t m
atch
the
val
ue
ente
red
for
this
dat
a el
emen
t, m
axim
um
valu
e fo
r th
is d
ata
and
# o
f lin
e ite
ms
is 2
6.
Dia
gnos
is C
odes
10
.25.
06.0
6.D
17-D
26
The
prim
ary
ICD
-9-C
M D
iagn
osis
Cod
e fo
llow
ed b
y a
seco
ndar
y di
agno
sis
(up
to 9
co
des)
, if a
pplic
able
at
time
of s
ervi
ce.
R
emov
e im
bedd
ed d
ecim
al p
oint
.
Serv
ice
From
Dat
e 10
.25.
06.0
6.D
27
Firs
t da
te o
f se
rvic
e fo
r a
proc
edur
e in
thi
s lin
e ite
m.
CCYY
MM
DD
37
Fiel
d N
ame
CO
MA
R
Des
crip
tion
Fi
eld
Con
ten
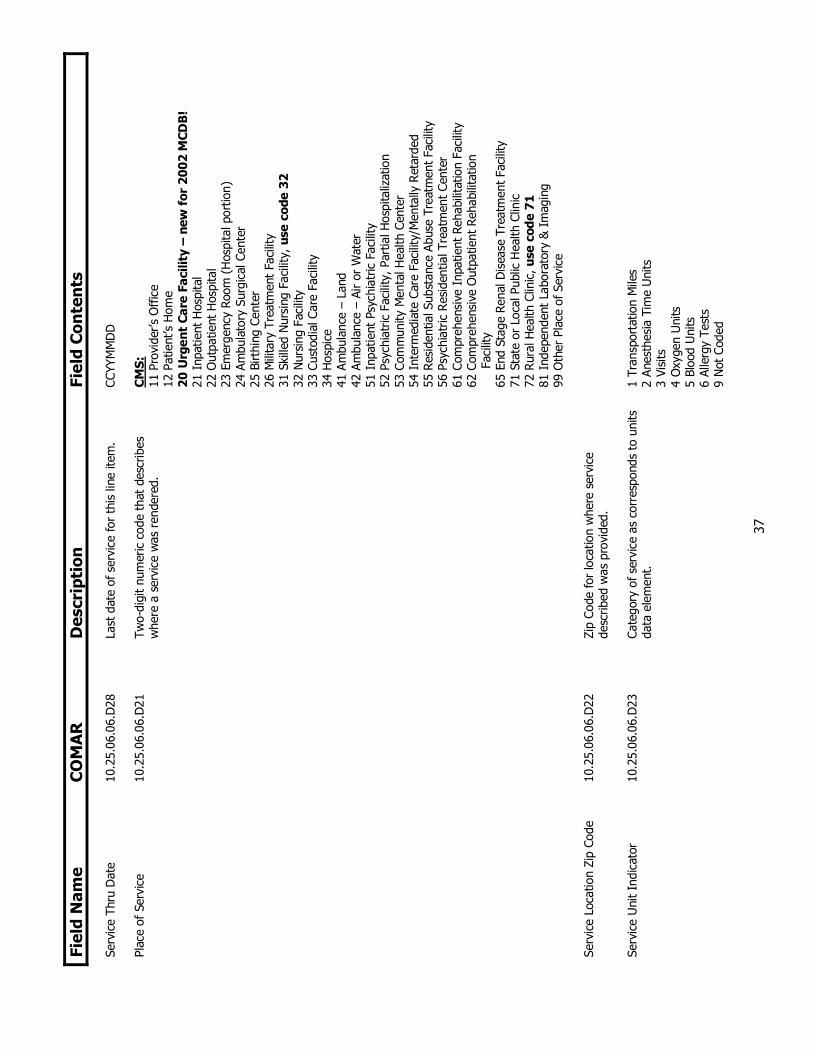
ts
Serv
ice
Thru
Dat
e 10
.25.
06.0
6.D
28
Last
dat
e of
ser
vice
for
this
line
item
. CC
YYM
MD
D
Plac
e of
Ser
vice
10.2
5.06
.06.
D21
Tw
o-di
git
num
eric
cod
e th
at d
escr
ibes
w
here
a s
ervi
ce w
as r
ende
red.
C
MS:
11
Pro
vide
r’s O
ffic
e 12
Pat
ient
’s H
ome
20 U
rgen
t Ca
re F
acili
ty –
new
for
200
2 M
CDB
! 21
Inp
atie
nt H
ospi
tal
22 O
utpa
tient
Hos
pita
l 23
Em
erge
ncy
Room
(H
ospi
tal p
ortio
n)
24 A
mbu
lato
ry S
urgi
cal C
ente
r 25
Birt
hing
Cen
ter
26 M
ilita
ry T
reat
men
t Fa
cilit
y 31
Ski
lled
Nur
sing
Fac
ility
, us
e co
de 3
2 32
Nur
sing
Fac
ility
33
Cus
todi
al C
are
Faci
lity
34 H
ospi
ce
41 A
mbu
lanc
e –
Land
42
Am
bula
nce
– Ai
r or
Wat
er
51 I
npat
ient
Psy
chia
tric
Fac
ility
52
Psy
chia
tric
Fac
ility
, Par
tial H
ospi
taliz
atio
n 53
Com
mun
ity M
enta
l Hea
lth C
ente
r 54
Int
erm
edia
te C
are
Faci
lity/
Men
tally
Ret
arde
d 55
Res
iden
tial S
ubst
ance
Abu
se T
reat
men
t Fa
cilit
y 56
Psy
chia
tric
Res
iden
tial T
reat
men
t Ce
nter
61
Com
preh
ensi
ve I
npat
ient
Reh
abili
tatio
n Fa
cilit
y 62
Com
preh
ensi
ve O
utpa
tient
Reh
abili
tatio
n
F
acili
ty
65 E
nd S
tage
Ren
al D
isea
se T
reat
men
t Fa
cilit
y 71
Sta
te o
r Lo
cal P
ublic
Hea
lth C
linic
72
Rur
al H
ealth
Clin
ic, u
se c
ode
71
81 I
ndep
ende
nt L
abor
ator
y &
Im
agin
g 99
Oth
er P
lace
of S
ervi
ce
Serv
ice
Loca
tion
Zip
Code
10
.25.
06.0
6.D
22
Zip
Code
for
loca
tion
whe
re s
ervi
ce
desc
ribed
was
pro
vide
d.
Serv
ice
Uni
t In
dica
tor
10.2
5.06
.06.
D23
Ca
tego
ry o
f ser
vice
as
corr
espo
nds
to u
nits
da
ta e
lem
ent.
1
Tran
spor
tatio
n M
iles
2 An
esth
esia
Tim
e U
nits
3
Visi
ts
4 O
xyge
n U
nits
5
Bloo
d U
nits
6
Alle
rgy
Test
s 9
Not
Cod
ed

38
Fiel
d N
ame
CO
MA
R
Des
crip
tion
Fi
eld
Con
ten
ts
Uni
ts
10.2
5.06
.06.
D24
Q
uant
ity o
f se
rvic
es o
r nu
mbe
r of
uni
ts fo
r a
serv
ice.
Proc
edur
e Co
de
10.2
5.06
.06.
D25
D
escr
ibes
the
hea
lth c
are
serv
ice
prov
ided
(i.
e., C
PT-4
, HCP
CS o
r N
atio
nal D
rug
Code
).
Mod
ifier
I
10.2
5.06
.06.
D26
D
iscr
imin
ate
code
use
d by
pra
ctiti
oner
s to
di
stin
guis
h th
at a
hea
lth c
are
serv
ice
has
been
alte
red
[by
a sp
ecifi
c co
nditi
on]
but
not
chan
ged
in d
efin
ition
or
code
. A
mod
ifier
is a
dded
as
a su
ffix
to
a pr
oced
ure
code
fiel
d.
MH
CC a
ccep
ts n
atio
nal s
tand
ard
mod
ifier
s ap
prov
ed b
y th
e Am
eric
an M
edic
al A
ssoc
iatio
n as
pub
lishe
d in
the
200
2 Cu
rren
t Pr
oced
ure
Term
inol
ogy.
M
odifi
ers
appr
oved
for
Hos
pita
l Out
patie
nt U
se:
Lev
el I
(CP
T) a
nd L
evel
II
(HCP
CS/N
atio
nal)
mod
ifier
s.
Mod
ifier
II
10.2
5.06
.06.
D27
Sp
ecifi
c to
Mod
ifier
I.
Se
rvic
ing
Prac
titio
ner
ID
10.2
5.06
.06.
D28
Pa
yer-
spec
ific
iden
tifie
r fo
r th
e pr
actit
ione
r re
nder
ing
heal
th c
are
serv
ice(
s).
Bille
d Ch
arge
10
.25.
06.0
6.D
29
A pr
actit
ione
r’s b
illed
cha
rges
rou
nded
to
who
le d
olla
rs –
DO
NO
T U
SE D
ECIM
ALS
Allo
wed
Am
ount
10
.25.
06.0
6.D
30
Tota
l pat
ient
and
pay
er li
abili
ty.
D
O N
OT
USE
DEC
IMA
LS
Rei
mbu
rsem
ent
Amou
nt
10.2
5.06
.06.
D31
Am
ount
pai
d to
Em
ploy
er T
ax I
D #
of
rend
erin
g ph
ysic
ian
as li
sted
on
clai
m.
D
O N
OT
USE
DEC
IMA
LS
Patie
nt L
iabi
lity
10.2
5.06
.06.
D32
Th
e am
ount
tha
t th
e pa
tient
is r
equi
red
to
pay
for
a pa
rtic
ular
ser
vice
(i.e
., co
insu
ranc
e, c
opay
men
ts a
nd d
educ
tible
s).
DO
NO
T U
SE D
ECIM
ALS

39
Dat
a D
icti
onar
y –
PH
AR
MA
CY
Fi
eld
Nam
e C
OM
AR
D
escr
ipti
on
Fiel
d C
onte
nts
Pa
tient
ID
10
.25.
06.0
7.C1
Pa
tient
’s u
niqu
e id
entif
icat
ion
num
ber,
ass
igne
d by
the
pay
er a
nd e
ncry
pted
.
Patie
nt S
ex
10.2
5.06
.07.
C2
Sex
of P
atie
nt.
1 M
ale
2 Fe
mal
e 3
Not
cod
ed
Patie
nt Z
ip C
ode
10.2
5.06
.07.
C3
Zip
code
of
patie
nt’s
res
iden
ce.
Pa
tient
Dat
e of
Birt
h 10
.25.
06.0
7.C4
D
ate
of p
atie
nt’s
birt
h us
ing
00 in
stea
d of
day
. CC
YYM
M00
N
CPD
P N
umbe
r 10
.25.
06.0
7.C5
U
niqu
e 7
digi
t nu
mbe
r as
sign
ed b
y th
e N
atio
nal
Coun
cil f
or P
resc
riptio
n D
rug
Prog
ram
(N
CPD
P).
Phar
mac
y Zi
p Co
de
10.2
5.06
.07.
C6
Zip
Code
of
phar
mac
y w
here
pre
scrip
tion
was
di
spen
sed.
DEA
#
10.2
5.06
.07.
C7
Dru
g En
forc
emen
t Ag
ency
num
ber
assi
gned
to
an in
divi
dual
reg
iste
red
unde
r th
e Co
ntro
lled
Subs
tanc
e Ac
t.
ND
C Co
de
10.2
5.06
.07.
C9
Nat
iona
l Dru
g Co
de 1
1 di
git
num
ber.
Dru
g Co
mpo
und
10.2
5.06
.07.
C10
Indi
cate
s a
mix
of d
rugs
to
form
a c
ompo
und
med
icat
ion.
1
Non
-com
poun
d 2
Com
poun
d
Dru
g Q
uant
ity
10.2
5.06
.07.
C11
Num
ber
of u
nits
dis
pens
ed.
D
rug
Supp
ly
10.2
5.06
.07.
C12
Estim
ated
num
ber
of d
ays
of d
ispe
nsed
sup
ply.
Dat
e Fi
lled
10.2
5.06
.07.
C13
Dat
e pr
escr
iptio
n fil
led.
CC
YYM
MD
D
Patie
nt L
iabi
lity
10.2
5.06
.07.
C14
The
amou
nt t
hat
the
patie
nt is
req
uire
d to
pay
fo
r a
part
icul
ar s
ervi
ce (
i.e.,
coin
sura
nce,
co
paym
ents
and
ded
uctib
les )
. M
US
T IN
CLU
DE
2 I
MP
LIED
DEC
IMA
L P
LAC
ES.
Bille
d Ch
arge
10
.25.
06.0
7.C1
5 R
etai
l am
ount
for
drug
incl
udin
g di
spen
sing
fe
es a
nd a
dmin
istr
ativ
e co
sts.
M
UST
IN
CLU
DE
2 I
MP
LIED
DEC
IMA
L P
LAC
ES.
Rei
mbu
rsem
ent
Amou
nt
10.2
5.06
.07.
C16
Amou
nt p
aid
to t
he p
harm
acy
by p
ayer
. D
o no
t in
clud
e pa
tient
cop
aym
ent
or s
ales
tax
. M
UST
IN
CLU
DE
2 I
MP
LIED
DEC
IMA
L P
LAC
ES.

40
D
ata
Dic
tion
ary
– P
RO
VID
ER
Fi
eld
Nam
e C
OM
AR
D
escr
ipti
on
Fiel
d C
onte
nts
Se
rvic
ing
Prac
titio
ner
ID
10.2
5.06
.08.
D1
Paye
r-sp
ecifi
c id
entif
ier
for
a pr
actit
ione
r,
prac
tice,
or
offic
e fa
cilit
y re
nder
ing
heal
th
care
ser
vice
(s).
Prac
titio
ner
Fede
ral T
ax I
D
10.2
5.06
.08.
D2
Empl
oyer
Tax
ID
# o
f the
pra
ctiti
oner
, pr
actic
e or
offi
ce f
acili
ty r
ecei
ving
pay
men
t fo
r se
rvic
es.
Prac
titio
ner
Last
Nam
e 10
.25.
06.0
8.D
3 Pr
actit
ione
r’s la
st n
ame.
Prac
titio
ner
Firs
t N
ame
10.2
5.06
.08.
D4
Prac
titio
ner’s
firs
t na
me.
Prac
titio
ner
Spec
ialty
10.2
5.06
.08.
D5
The
heal
th c
are
field
in w
hich
a p
hysi
cian
, lic
ense
d he
alth
car
e pr
ofes
sion
al,
dent
al
prac
titio
ner,
or
offic
e fa
cilit
y ha
s be
en
cert
ified
. U
p to
3 c
odes
may
be
liste
d.
Phy
sici
ans:
00
1 G
ener
al P
ract
ice
002
Gen
eral
Sur
gery
00
3 Al
lerg
y &
Im
mun
olog
y 00
4 An
esth
esio
logy
00
5 Ca
rdio
logy
00
6 D
erm
atol
ogy
007
Emer
genc
y M
edic
ine
008
Endo
crin
olog
y M
edic
ine
009
Fam
ily P
ract
ice
010
Gas
troe
nter
olog
y 01
1 G
eria
tric
s 01
2 H
and
Surg
ery
013
Hem
atol
ogy
014
Inte
rnal
Med
icin
e 01
5 In
fect
ious
Dis
ease
10
1 M
ulti-
Spec
ialty
Med
ical
Pra
ctic
e 01
6 N
ephr
olog
y 10
0 N
eona
tolo
gy
017
Neu
rolo
gy
018
Nuc
lear
Med
icin
e 03
9 O
bste
tric
s/G
ynec
olog
y 01
9 O
ncol
ogy
020
Oph
thal
mol
ogy
021
Ort
hope
dic
Surg
ery
022
Ost
eopa
thy
(incl
udes
man
ipul
atio
ns)
023
Oto
logy
, La
ryng
olog
y, R
hino
logy
, Oto
lary
ngol
ogy

41
Fiel
d N
ame
CO
MA
R
Des
crip
tion
Fi
eld
Con
ten
ts
Prac
titio
ner
Spec
ialty
(co
n’t.
)
024
Path
olog
y 02
5 Pe
diat
rics
026
Perip
hera
l Vas
cula
r D
isea
se o
r Su
rger
y 02
7 Pl
astic
Sur
gery
02
8 Ph
ysic
al M
edic
ine
and
Reh
abili
tatio
n 02
9 Pr
octo
logy
03
0 Ps
ychi
atry
03
1 Pu
lmon
ary
Dis
ease
03
2 R
adio
logy
03
3 R
heum
atol
ogy
034
Surg
ical
Spe
cial
ty N
ot L
iste
d H
ere
035
Thor
acic
Sur
gery
03
6 U
rolo
gy
037
Oth
er S
pec
Not
Lis
ted
(pub
lic h
ealth
,indu
stria
l med
icin
e)
038
Phys
w/o
Spe
c Id
entif
ied
& S
pec
Not
Lis
ted
039
Obs
tetr
ics/
Gyn
ecol
ogy
Oth
er H
ealt
h C
are
Pro
fess
iona
ls:
040
Acup
unct
uris
t 04
1 Al
coho
l/Dru
g D
etox
Ser
vice
s 04
2 Am
bula
nce
Serv
ices
04
3 Au
diol
ogis
t/Sp
eech
Pat
holo
gist
04
4 Ch
iropr
acto
r 04
5 Fr
eest
andi
ng C
linic
– N
ot a
Gov
ernm
ent
Agen
cy
046
Day
Car
e Fa
cilit
y: M
edic
al,
Men
tal H
ealth
04
7 D
ietit
ian/
Lice
nsed
Nut
ritio
nist
04
8 H
ome
Hea
lth P
rovi
der
102
Men
tal H
ealth
Clin
ic
049
Adva
nced
Pra
ctic
e N
urse
: An
esth
etis
t 05
0 Ad
vanc
ed P
ract
ice
Nur
se:
Mid
wife
05
1 Ad
vanc
ed P
ract
ice
Nur
se:
Nur
se P
ract
ition
er
052
Adva
nced
Pra
ctic
e N
urse
: Ps
ycho
ther
apis
t 05
3 N
urse
– O
ther
Tha
n Ad
vanc
ed P
ract
ice
054
Occ
upat
iona
l The
rapi
st
055
Opt
omet
rist
056
Podi
atris
t 05
7 Ph
ysic
al T
hera
pist
05
8 Ps
ycho
logi
st
059
Clin
ical
Soc
ial W
orke
r 06
0 Pu
blic
Hea
lth o
r W
elfa
re A
genc
y (f
eder
al,
stat
e, a
nd
loca
l gov
ernm
ent)
06
3 R
espi
rato
ry T
hera
pist
06
1 Vo
lunt
ary
Hea
lth A
genc
y 06
2 O
ther
Spe
cial
ty N
ot L
iste
d Ab
ove

42
Fiel
d N
ame
CO
MA
R
Des
crip
tion
Fi
eld
Con
ten
ts
Prac
titio
ner
Spec
ialty
(co
n’t.
)
Den
tal:
07
0 G
ener
al D
entis
t 07
1 En
dodo
ntis
t 07
2 O
rtho
dont
ist
073
Ora
l Sur
geon
07
4 Pe
dodo
ntis
t 07
5 Pe
riodo
ntis
t 07
6 Pr
osth
odon
tist
Off
ice
Faci
litie
s:
080
Free
stan
ding
Pha
rmac
y (i
nclu
des
groc
ery)
08
1 M
ail O
rder
Pha
rmac
y 08
2 In
depe
nden
t La
bora
tory
08
3 In
depe
nden
t M
edic
al S
uppl
y Co
mpa
ny
084
Opt
icia
n/O
ptom
etris
t (f
or le
nses
& e
ye g
lass
es)
085
All O
ther
Sup
plie
s 09
0 Fr
eest
andi
ng M
edic
al F
acili
ty
091
Free
stan
ding
Sur
gica
l Fac
ility
09
2 Fr
eest
andi
ng I
mag
ing
Cent
er
093
Oth
er f
acili
ty
D
EA #
10
.25.
06.0
7.C7
D
rug
Enfo
rcem
ent
Agen
cy n
umbe
r as
sign
ed
to a
n in
divi
dual
reg
iste
red
unde
r th
e Co
ntro
lled
Subs
tanc
e Ac
t.

43
Appendix D
Explanation of Practitioner Specialty
www.mhcc.state.md.us

44
Practitioner Specialty Expansions/Consolidations
Practitioner Specialty: The health care field in which a physician, licensed health care professional, dental practitioner, or office facility has been certified. The following table shows examples where a practitioner specialty may encompass other services. For illustrative purposes only.
Practitioner Specialty Value Specialties Not Specifically IdentifiedGeneral Practice 001 General Surgery 002 Allergy & Immunology 003 Pediatric Allergy & Immunology Anesthesiology 004 Cardiology 005 Pediatric Cardiology Dermatology 006 Dermatopathology Emergency Medicine 007 Endocrinology Medicine 008 Pediatric Endocrinology Family Practice 009 Gastroenterology 010 Pediatric Gastroenterology Geriatrics 011 Hand Surgery 012 Hematology 013 Pediatric Hematology/Oncology Internal Medicine 014 Adolescent Medicine Infectious Disease 015 Pediatric Infectious Disease Multi-Specialty Medical Practice 101 Use this code only where provider-specific
identifiers are not available for physicians practicing as a group with varying specialties.
Nephrology 016 Pediatric Nephrology Neonatology 100 Neurology 017 Pediatric Neurology
Nuclear Medicine 018 Obstetrics/Gynecology 039 Oncology 019 Gynecological Oncology Ophthalmology 020 Pediatric Ophthalmology Orthopedic Surgery 021 Pediatric Orthopedic Surgery Osteopathy 022 Include manipulations Otology, Laryngology, Rhinology, Otolaryngology
023
Pathology 024 Forensic Pathology Oral Pathology
Pediatrics 025 Peripheral Vascular Disease/Surgery 026 Plastic Surgery 027 Reconstructive Surgery
Cosmetic Surgery Physical Medicine and Rehabilitation 028 Rehabilitative Sports Medicine Proctology 029 Colon & Rectal Surgery Psychiatry 030 Pediatric Psychiatry Pulmonary Disease 031 Pediatric Pulmonary Medicine Radiology 032 MRI
Nuclear Radiology Pediatric Radiology

45
Practitioner Specialty Value Specialties Not Specifically IdentifiedRheumatology 033 Surgical Specialty Not Listed Here 034 Abdominal Surgery
Head and Neck Surgery Maxillofacial Surgery Neurological Surgery Pediatric Surgery Vascular Surgery
Thoracic Surgery 035 Cardiovascular Surgery Thoracic Surgery
Urology 036 Urology Pediatric Urology
Other Specialties Not Listed
037 Public Health Industrial Medicine
Physician without a Specialty Identified and Specialty Not Listed Here
038 • Addiction Medicine • Algology/Pain
Management • Aerospace Medicine • Critical Care Medicine • Genetics • Infertility
• Multiple Specialty Physician Group
• Occupational Medicine • Preventative Medicine • Reproductive
Endocrinology • Urgent Care Medicine
Other Health Care Professionals: Practitioner Specialty Value Other Services Included Acupuncturist 040 Alcohol/Drug Detox Services 041 Ambulance Services 042 Audiologist/Speech Pathologist 043 Chiropractor 044 Freestanding Clinic (Not a Government Agency) 045 Day Care Facility 046 Medical
Mental Health Dietitian/Licensed Nutritionist 047 Home Health Provider 048 Home Infusion Therapy Mental Health 102 Use this code only where provider-specific identifiers
are not available for facilities where mental health services are provided by a psychiatrist, psychologist, or social worker.
Advanced Practice Nurse: Anesthetist 049 Nurse Anesthetist/Certified Registered Nurse Anesthetist (CRNA)
Advanced Practice Nurse: Midwife 050 Nurse Midwife Advanced Practice Nurse: Nurse Practitioner 051 Nurse Practitioner Advanced Practice Nurse: Psychotherapist 052 Nurse Psychotherapist Nurse – Other than Advanced Practice 053 Occupational Therapist 054 Optometrist 055 Podiatrist 056 Physical Therapist 057 Psychologist 058 Clinical Social Worker 059 Public Health or Welfare Agency 060 Federal, state, and local government Voluntary Health Agency 061 Planned Parenthood Other Specialty Not Listed Above 062 Hypnosis Respiratory Therapist 063

46
Dental:
COMAR Practitioner Specialty Value Other Services Included General Dentist 070 Endodontist 071 Orthodontist 072 Oral Surgeon 073 Pedodontist 074 Periodontist 075 Prosthodontist 076
Office Facilities:
COMAR Practitioner Specialty Value Other Services Included Freestanding Pharmacy 080 Includes grocery Mail Order Pharmacy 081 Independent Laboratory 082 Independent Medical Supply Company 083 Durable Medical Equipment
Prosthetic Devices Vision Products Blood
Optician/Optometrist 084 For lenses & eye glasses All Other Supplies 085 Freestanding Medical Facility 090 Freestanding Surgical Facility 091 Freestanding Imaging Center 092 Other Facility 093 Dialysis Center
Birthing Center

47
Appendix E
Explanation of
Coverage Type
www.mhcc.state.md.us

48
Coverage Type
Coverage Type: A data field on the tape that indicates type of insurance coverage (i.e., individual, Medigap, self-funded, etc.). The following table lists COMAR Coverage Types and provides a column of mapping examples.
COMAR Coverage Type Value Examples of Coverage Type
Medicare Supplemental (i.e. Individual, Group, WRAP)
1 Medigap
Individual Plan 2 • Conversion High • Conversion Standard • Direct Pay High • Direct Pay Standard • Student Health
Private Employer Sponsored, Fully Self-Insured
3 Use this category if your company is providing administrative services (your company assumes no risk) only to an employer under a health benefit contract.
Private Employer Sponsored Insured
4 Standard insurance policy in which your company assumes risk: • Commercial Basic • Commercial High • Commercial Standard • Preferred Provider Option • Triple Option • HMO • Point-of-Service • Triple Option HMO • Indemnity • Triple Option POS • Triple Option PPO
Public Employee 5 Federal, state, local, or school system
Comprehensive Standard Health Benefit Plan
6 Participating Carriers: • Aetna Life Insurance Co. • Aetna US Healthcare Inc. • CareFirst Blue Choice, Inc. • CareFirst of MD, Inc. • Cigna Healthcare Mid-Atlantic,
Inc. • Coventry Health Care DE, Inc. • Fidelity Insurance Company • Graphic Arts Benefit Corp. • Guardian Life. Ins. Co. of
America
• Kaiser Foundation Health Plan
of Mid-Atlantic States, Inc. • MEGA Life & Health Insurance
Company • Mid-West National Life Ins.
Co. of TN • Optimum Choice, Inc. • PHN-HMO, Inc. • Principal Life Ins. Co. • United Healthcare Insurance
Company
Medicare+Choice (services provided by a Medicare HMO under contract with CMS)
7 • Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc.

49
Appendix F
Maryland County Zip Code Crosswalk
www.mhcc.state.md.us
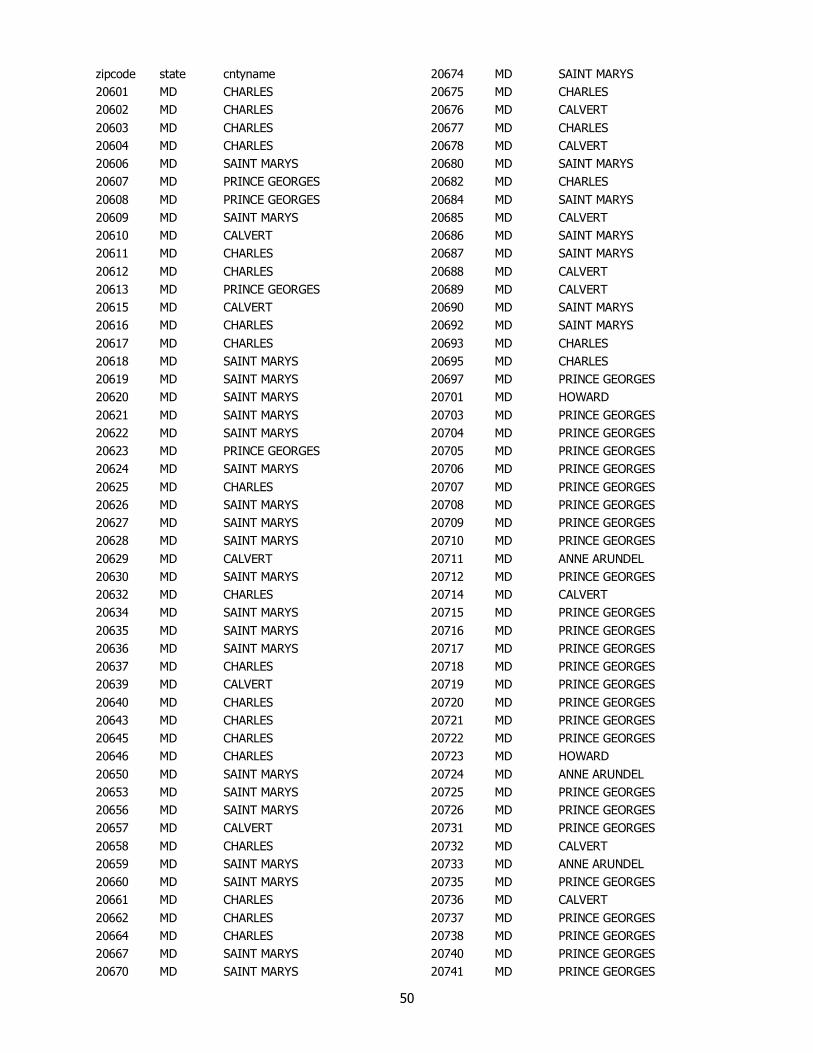
50
zipcode state cntyname 20601 MD CHARLES 20602 MD CHARLES 20603 MD CHARLES 20604 MD CHARLES 20606 MD SAINT MARYS 20607 MD PRINCE GEORGES 20608 MD PRINCE GEORGES 20609 MD SAINT MARYS 20610 MD CALVERT 20611 MD CHARLES 20612 MD CHARLES 20613 MD PRINCE GEORGES 20615 MD CALVERT 20616 MD CHARLES 20617 MD CHARLES 20618 MD SAINT MARYS 20619 MD SAINT MARYS 20620 MD SAINT MARYS 20621 MD SAINT MARYS 20622 MD SAINT MARYS 20623 MD PRINCE GEORGES 20624 MD SAINT MARYS 20625 MD CHARLES 20626 MD SAINT MARYS 20627 MD SAINT MARYS 20628 MD SAINT MARYS 20629 MD CALVERT 20630 MD SAINT MARYS 20632 MD CHARLES 20634 MD SAINT MARYS 20635 MD SAINT MARYS 20636 MD SAINT MARYS 20637 MD CHARLES 20639 MD CALVERT 20640 MD CHARLES 20643 MD CHARLES 20645 MD CHARLES 20646 MD CHARLES 20650 MD SAINT MARYS 20653 MD SAINT MARYS 20656 MD SAINT MARYS 20657 MD CALVERT 20658 MD CHARLES 20659 MD SAINT MARYS 20660 MD SAINT MARYS 20661 MD CHARLES 20662 MD CHARLES 20664 MD CHARLES 20667 MD SAINT MARYS 20670 MD SAINT MARYS
20674 MD SAINT MARYS 20675 MD CHARLES 20676 MD CALVERT 20677 MD CHARLES 20678 MD CALVERT 20680 MD SAINT MARYS 20682 MD CHARLES 20684 MD SAINT MARYS 20685 MD CALVERT 20686 MD SAINT MARYS 20687 MD SAINT MARYS 20688 MD CALVERT 20689 MD CALVERT 20690 MD SAINT MARYS 20692 MD SAINT MARYS 20693 MD CHARLES 20695 MD CHARLES 20697 MD PRINCE GEORGES 20701 MD HOWARD 20703 MD PRINCE GEORGES 20704 MD PRINCE GEORGES 20705 MD PRINCE GEORGES 20706 MD PRINCE GEORGES 20707 MD PRINCE GEORGES 20708 MD PRINCE GEORGES 20709 MD PRINCE GEORGES 20710 MD PRINCE GEORGES 20711 MD ANNE ARUNDEL 20712 MD PRINCE GEORGES 20714 MD CALVERT 20715 MD PRINCE GEORGES 20716 MD PRINCE GEORGES 20717 MD PRINCE GEORGES 20718 MD PRINCE GEORGES 20719 MD PRINCE GEORGES 20720 MD PRINCE GEORGES 20721 MD PRINCE GEORGES 20722 MD PRINCE GEORGES 20723 MD HOWARD 20724 MD ANNE ARUNDEL 20725 MD PRINCE GEORGES 20726 MD PRINCE GEORGES 20731 MD PRINCE GEORGES 20732 MD CALVERT 20733 MD ANNE ARUNDEL 20735 MD PRINCE GEORGES 20736 MD CALVERT 20737 MD PRINCE GEORGES 20738 MD PRINCE GEORGES 20740 MD PRINCE GEORGES 20741 MD PRINCE GEORGES

51
20742 MD PRINCE GEORGES 20743 MD PRINCE GEORGES 20744 MD PRINCE GEORGES 20745 MD PRINCE GEORGES 20746 MD PRINCE GEORGES 20747 MD PRINCE GEORGES 20748 MD PRINCE GEORGES 20749 MD PRINCE GEORGES 20750 MD PRINCE GEORGES 20751 MD ANNE ARUNDEL 20752 MD PRINCE GEORGES 20753 MD PRINCE GEORGES 20754 MD CALVERT 20755 MD ANNE ARUNDEL 20757 MD PRINCE GEORGES 20758 MD ANNE ARUNDEL 20759 MD HOWARD 20762 MD PRINCE GEORGES 20763 MD HOWARD 20764 MD ANNE ARUNDEL 20765 MD ANNE ARUNDEL 20768 MD PRINCE GEORGES 20769 MD PRINCE GEORGES 20770 MD PRINCE GEORGES 20771 MD PRINCE GEORGES 20772 MD PRINCE GEORGES 20773 MD PRINCE GEORGES 20774 MD PRINCE GEORGES 20775 MD PRINCE GEORGES 20776 MD ANNE ARUNDEL 20777 MD HOWARD 20778 MD ANNE ARUNDEL 20779 MD ANNE ARUNDEL 20781 MD PRINCE GEORGES 20782 MD PRINCE GEORGES 20783 MD PRINCE GEORGES 20784 MD PRINCE GEORGES 20785 MD PRINCE GEORGES 20787 MD PRINCE GEORGES 20788 MD PRINCE GEORGES 20790 MD PRINCE GEORGES 20791 MD PRINCE GEORGES 20792 MD PRINCE GEORGES 20794 MD HOWARD 20797 MD PRINCE GEORGES 20799 MD PRINCE GEORGES 20810 MD MONTGOMERY 20811 MD MONTGOMERY 20812 MD MONTGOMERY 20813 MD MONTGOMERY 20814 MD MONTGOMERY
20815 MD MONTGOMERY 20816 MD MONTGOMERY 20817 MD MONTGOMERY 20818 MD MONTGOMERY 20824 MD MONTGOMERY 20825 MD MONTGOMERY 20827 MD MONTGOMERY 20830 MD MONTGOMERY 20832 MD MONTGOMERY 20833 MD MONTGOMERY 20837 MD MONTGOMERY 20838 MD MONTGOMERY 20839 MD MONTGOMERY 20841 MD MONTGOMERY 20842 MD MONTGOMERY 20847 MD MONTGOMERY 20848 MD MONTGOMERY 20849 MD MONTGOMERY 20850 MD MONTGOMERY 20851 MD MONTGOMERY 20852 MD MONTGOMERY 20853 MD MONTGOMERY 20854 MD MONTGOMERY 20855 MD MONTGOMERY 20857 MD MONTGOMERY 20859 MD MONTGOMERY 20860 MD MONTGOMERY 20861 MD MONTGOMERY 20862 MD MONTGOMERY 20866 MD MONTGOMERY 20868 MD MONTGOMERY 20871 MD MONTGOMERY 20872 MD MONTGOMERY 20874 MD MONTGOMERY 20875 MD MONTGOMERY 20876 MD MONTGOMERY 20877 MD MONTGOMERY 20878 MD MONTGOMERY 20879 MD MONTGOMERY 20880 MD MONTGOMERY 20882 MD MONTGOMERY 20883 MD MONTGOMERY 20884 MD MONTGOMERY 20885 MD MONTGOMERY 20886 MD MONTGOMERY 20889 MD MONTGOMERY 20891 MD MONTGOMERY 20892 MD MONTGOMERY 20894 MD MONTGOMERY 20895 MD MONTGOMERY 20896 MD MONTGOMERY

52
20897 MD MONTGOMERY 20898 MD MONTGOMERY 20899 MD MONTGOMERY 20901 MD MONTGOMERY 20902 MD MONTGOMERY 20903 MD MONTGOMERY 20904 MD MONTGOMERY 20905 MD MONTGOMERY 20906 MD MONTGOMERY 20907 MD MONTGOMERY 20908 MD MONTGOMERY 20910 MD MONTGOMERY 20911 MD MONTGOMERY 20912 MD MONTGOMERY 20913 MD MONTGOMERY 20914 MD MONTGOMERY 20915 MD MONTGOMERY 20916 MD MONTGOMERY 20918 MD MONTGOMERY 20997 MD MONTGOMERY 21001 MD HARFORD 21005 MD HARFORD 21009 MD HARFORD 21010 MD HARFORD 21012 MD ANNE ARUNDEL 21013 MD BALTIMORE 21014 MD HARFORD 21015 MD HARFORD 21017 MD HARFORD 21018 MD HARFORD 21020 MD BALTIMORE 21022 MD BALTIMORE 21023 MD BALTIMORE 21027 MD BALTIMORE 21028 MD HARFORD 21029 MD HOWARD 21030 MD BALTIMORE 21031 MD BALTIMORE 21032 MD ANNE ARUNDEL 21034 MD HARFORD 21035 MD ANNE ARUNDEL 21036 MD HOWARD 21037 MD ANNE ARUNDEL 21040 MD HARFORD 21041 MD HOWARD 21042 MD HOWARD 21043 MD HOWARD 21044 MD HOWARD 21045 MD HOWARD 21046 MD HOWARD 21047 MD HARFORD
21048 MD CARROLL 21050 MD HARFORD 21051 MD BALTIMORE 21052 MD BALTIMORE 21053 MD BALTIMORE 21054 MD ANNE ARUNDEL 21055 MD BALTIMORE 21056 MD ANNE ARUNDEL 21057 MD BALTIMORE 21060 MD ANNE ARUNDEL 21061 MD ANNE ARUNDEL 21062 MD ANNE ARUNDEL 21065 MD BALTIMORE 21071 MD BALTIMORE 21074 MD CARROLL 21075 MD HOWARD 21076 MD ANNE ARUNDEL 21077 MD ANNE ARUNDEL 21078 MD HARFORD 21082 MD BALTIMORE 21084 MD HARFORD 21085 MD HARFORD 21087 MD BALTIMORE 21088 MD CARROLL 21090 MD ANNE ARUNDEL 21092 MD BALTIMORE 21093 MD BALTIMORE 21094 MD BALTIMORE 21098 MD ANNE ARUNDEL 21102 MD CARROLL 21104 MD CARROLL 21105 MD BALTIMORE 21106 MD ANNE ARUNDEL 21108 MD ANNE ARUNDEL 21111 MD BALTIMORE 21113 MD ANNE ARUNDEL 21114 MD ANNE ARUNDEL 21117 MD BALTIMORE 21120 MD BALTIMORE 21122 MD ANNE ARUNDEL 21123 MD ANNE ARUNDEL 21128 MD BALTIMORE 21130 MD HARFORD 21131 MD BALTIMORE 21132 MD HARFORD 21133 MD BALTIMORE 21136 MD BALTIMORE 21139 MD BALTIMORE 21140 MD ANNE ARUNDEL 21144 MD ANNE ARUNDEL 21146 MD ANNE ARUNDEL

53
21150 MD HOWARD 21152 MD BALTIMORE 21153 MD BALTIMORE 21154 MD HARFORD 21155 MD BALTIMORE 21156 MD BALTIMORE 21157 MD CARROLL 21158 MD CARROLL 21160 MD HARFORD 21161 MD HARFORD 21162 MD BALTIMORE 21163 MD HOWARD 21201 MD BALTIMORE CITY 21202 MD BALTIMORE CITY 21203 MD BALTIMORE CITY 21204 MD BALTIMORE 21205 MD BALTIMORE CITY 21206 MD BALTIMORE CITY 21207 MD BALTIMORE 21208 MD BALTIMORE 21209 MD BALTIMORE CITY 21210 MD BALTIMORE CITY 21211 MD BALTIMORE CITY 21212 MD BALTIMORE CITY 21213 MD BALTIMORE CITY 21214 MD BALTIMORE CITY 21215 MD BALTIMORE CITY 21216 MD BALTIMORE CITY 21217 MD BALTIMORE CITY 21218 MD BALTIMORE CITY 21219 MD BALTIMORE 21220 MD BALTIMORE 21221 MD BALTIMORE 21222 MD BALTIMORE 21223 MD BALTIMORE CITY 21224 MD BALTIMORE CITY 21225 MD BALTIMORE CITY 21226 MD ANNE ARUNDEL 21227 MD BALTIMORE 21228 MD BALTIMORE 21229 MD BALTIMORE CITY 21230 MD BALTIMORE CITY 21231 MD BALTIMORE CITY 21233 MD BALTIMORE CITY 21234 MD BALTIMORE 21235 MD BALTIMORE CITY 21236 MD BALTIMORE 21237 MD BALTIMORE 21239 MD BALTIMORE CITY 21240 MD ANNE ARUNDEL 21241 MD BALTIMORE CITY
21244 MD BALTIMORE 21250 MD BALTIMORE 21251 MD BALTIMORE 21252 MD BALTIMORE 21263 MD BALTIMORE CITY 21264 MD BALTIMORE CITY 21265 MD BALTIMORE CITY 21268 MD BALTIMORE CITY 21270 MD BALTIMORE CITY 21273 MD BALTIMORE CITY 21274 MD BALTIMORE CITY 21275 MD BALTIMORE CITY 21278 MD BALTIMORE CITY 21279 MD BALTIMORE CITY 21280 MD BALTIMORE CITY 21281 MD BALTIMORE CITY 21282 MD BALTIMORE 21283 MD BALTIMORE CITY 21284 MD BALTIMORE 21285 MD BALTIMORE 21286 MD BALTIMORE 21287 MD BALTIMORE CITY 21288 MD BALTIMORE CITY 21289 MD BALTIMORE CITY 21290 MD BALTIMORE CITY 21297 MD BALTIMORE CITY 21298 MD BALTIMORE CITY 21401 MD ANNE ARUNDEL 21402 MD ANNE ARUNDEL 21403 MD ANNE ARUNDEL 21404 MD ANNE ARUNDEL 21405 MD ANNE ARUNDEL 21411 MD ANNE ARUNDEL 21412 MD ANNE ARUNDEL 21501 MD ALLEGANY 21502 MD ALLEGANY 21503 MD ALLEGANY 21504 MD ALLEGANY 21505 MD ALLEGANY 21520 MD GARRETT 21521 MD ALLEGANY 21522 MD GARRETT 21523 MD GARRETT 21524 MD ALLEGANY 21528 MD ALLEGANY 21529 MD ALLEGANY 21530 MD ALLEGANY 21531 MD GARRETT 21532 MD ALLEGANY 21536 MD GARRETT 21538 MD GARRETT

54
21539 MD ALLEGANY 21540 MD ALLEGANY 21541 MD GARRETT 21542 MD ALLEGANY 21543 MD ALLEGANY 21545 MD ALLEGANY 21550 MD GARRETT 21555 MD ALLEGANY 21556 MD ALLEGANY 21557 MD ALLEGANY 21560 MD ALLEGANY 21561 MD GARRETT 21562 MD ALLEGANY 21601 MD TALBOT 21606 MD TALBOT 21607 MD QUEEN ANNES 21609 MD CAROLINE 21610 MD KENT 21612 MD TALBOT 21613 MD DORCHESTER 21617 MD QUEEN ANNES 21619 MD QUEEN ANNES 21620 MD KENT 21622 MD DORCHESTER 21623 MD QUEEN ANNES 21624 MD TALBOT 21625 MD TALBOT 21626 MD DORCHESTER 21627 MD DORCHESTER 21628 MD QUEEN ANNES 21629 MD CAROLINE 21631 MD DORCHESTER 21632 MD CAROLINE 21634 MD DORCHESTER 21635 MD KENT 21636 MD CAROLINE 21638 MD QUEEN ANNES 21639 MD CAROLINE 21640 MD CAROLINE 21641 MD CAROLINE 21643 MD DORCHESTER 21644 MD QUEEN ANNES 21645 MD KENT 21647 MD TALBOT 21648 MD DORCHESTER 21649 MD CAROLINE 21650 MD KENT 21651 MD KENT 21652 MD TALBOT 21653 MD TALBOT 21654 MD TALBOT
21655 MD CAROLINE 21656 MD QUEEN ANNES 21657 MD QUEEN ANNES 21658 MD QUEEN ANNES 21659 MD DORCHESTER 21660 MD CAROLINE 21661 MD KENT 21662 MD TALBOT 21663 MD TALBOT 21664 MD DORCHESTER 21665 MD TALBOT 21666 MD QUEEN ANNES 21667 MD KENT 21668 MD QUEEN ANNES 21669 MD DORCHESTER 21670 MD CAROLINE 21671 MD TALBOT 21672 MD DORCHESTER 21673 MD TALBOT 21675 MD DORCHESTER 21676 MD TALBOT 21677 MD DORCHESTER 21678 MD KENT 21679 MD TALBOT 21681 MD CAROLINE 21682 MD CAROLINE 21683 MD CAROLINE 21684 MD CAROLINE 21685 MD CAROLINE 21686 MD CAROLINE 21687 MD CAROLINE 21688 MD CAROLINE 21690 MD QUEEN ANNES 21701 MD FREDERICK 21702 MD FREDERICK 21703 MD FREDERICK 21704 MD FREDERICK 21705 MD FREDERICK 21709 MD FREDERICK 21710 MD FREDERICK 21711 MD WASHINGTON 21713 MD WASHINGTON 21714 MD FREDERICK 21715 MD WASHINGTON 21716 MD FREDERICK 21717 MD FREDERICK 21718 MD FREDERICK 21719 MD WASHINGTON 21720 MD WASHINGTON 21721 MD WASHINGTON 21722 MD WASHINGTON

55
21723 MD HOWARD 21727 MD FREDERICK 21733 MD WASHINGTON 21734 MD WASHINGTON 21737 MD HOWARD 21738 MD HOWARD 21740 MD WASHINGTON 21741 MD WASHINGTON 21742 MD WASHINGTON 21746 MD WASHINGTON 21747 MD WASHINGTON 21748 MD WASHINGTON 21749 MD WASHINGTON 21750 MD WASHINGTON 21754 MD FREDERICK 21755 MD FREDERICK 21756 MD WASHINGTON 21757 MD CARROLL 21758 MD FREDERICK 21759 MD FREDERICK 21762 MD FREDERICK 21765 MD HOWARD 21766 MD ALLEGANY 21767 MD WASHINGTON 21769 MD FREDERICK 21770 MD FREDERICK 21771 MD FREDERICK 21773 MD FREDERICK 21774 MD FREDERICK 21775 MD FREDERICK 21776 MD CARROLL 21777 MD FREDERICK 21778 MD FREDERICK 21779 MD WASHINGTON 21780 MD FREDERICK 21781 MD WASHINGTON 21782 MD WASHINGTON 21783 MD WASHINGTON 21784 MD CARROLL 21787 MD CARROLL 21788 MD FREDERICK 21790 MD FREDERICK 21791 MD CARROLL 21792 MD FREDERICK 21793 MD FREDERICK 21794 MD HOWARD 21795 MD WASHINGTON 21797 MD HOWARD 21798 MD FREDERICK 21801 MD WICOMICO 21802 MD WICOMICO
21803 MD WICOMICO 21804 MD WICOMICO 21810 MD WICOMICO 21811 MD WORCESTER 21813 MD WORCESTER 21814 MD WICOMICO 21817 MD SOMERSET 21821 MD SOMERSET 21822 MD WORCESTER 21824 MD SOMERSET 21826 MD WICOMICO 21829 MD WORCESTER 21830 MD WICOMICO 21835 MD DORCHESTER 21836 MD SOMERSET 21837 MD WICOMICO 21838 MD SOMERSET 21840 MD WICOMICO 21841 MD WORCESTER 21842 MD WORCESTER 21843 MD WORCESTER 21849 MD WICOMICO 21850 MD WICOMICO 21851 MD WORCESTER 21852 MD WICOMICO 21853 MD SOMERSET 21856 MD WICOMICO 21857 MD SOMERSET 21861 MD WICOMICO 21862 MD WORCESTER 21863 MD WORCESTER 21864 MD WORCESTER 21865 MD WICOMICO 21866 MD SOMERSET 21867 MD SOMERSET 21869 MD DORCHESTER 21870 MD SOMERSET 21871 MD SOMERSET 21872 MD WORCESTER 21874 MD WICOMICO 21875 MD WICOMICO 21890 MD SOMERSET 21901 MD CECIL 21902 MD CECIL 21903 MD CECIL 21904 MD CECIL 21911 MD CECIL 21912 MD CECIL 21913 MD CECIL 21914 MD CECIL 21915 MD CECIL

56
21916 MD CECIL 21917 MD CECIL 21918 MD CECIL 21919 MD CECIL 21920 MD CECIL 21921 MD CECIL 21922 MD CECIL 21930 MD CECIL Updated 1-31-03

57
Appendix G
2002 MCDB Payers & Payer ID Numbers
ORGANIZATION Payer ID # ORGANIZATION Payer ID
#
Aetna U.S. Healthcare P030 Group Hospitalization & Medical Services, Inc.
P340-P130
Aetna Life & Health Insurance Co. P020-P030 Kaiser Foundation Health Plan of Mid-Atlantic
P480
Allianz Life Ins. Co. of North America P040 MAMSI Life and Health Ins. Co. P500
American Republic Insurance Co. P070 Maryland Fidelity Insurance Co. P510
CareFirst DC P130 MD-Individual Practice Association, Inc. P520-P500
CareFirst MD P131 Mega Life & Health Insurance Co. P530-P650
CIGNA Healthcare Mid-Atlantic, Inc. P160 New York Life Insurance Co. P600-P030
Connecticut General Life Ins. Co. P180-P160 Optimum Choice, Inc. P620-P500
Corporate Health Insurance Co. P220-P030 PFL Life Insurance Company P650
Coventry Healthcare of Delaware, Inc. P680 PHN-HMO, Inc. P660
Delmarva Health Plan P230-P131 State Farm Mutual Automobile Ins. Co. P760
Educators Mutual Life Insurance Co. P240 Trustmark Insurance Co. P830
Fortis Insurance Co. P280 Unicare Life & Health Insurance Co. P471
Free State Health Plan, Inc. P290-P131 Union Labor Life Insurance Co. P850
Golden Rule Insurance Co. P320 United Healthcare Insurance Co. P820
Graphic Arts Benefit Corporation P325 United Healthcare of the Mid-Atlantic, Inc.
P870
Great-West Life & Annuity Ins. Co. P330 United Wisconsin Life Insurance Co. P890