day surgery in scotland€¦ · day surgery in scotland, 1997, accounts commission, ... percentage...
TRANSCRIPT

Prepared for the Auditor General for Scotland
Day surgery in Scotland – reviewing progress
April 2004

Auditor General for ScotlandThe Auditor General for Scotland is the Parliament’s watchdog forensuring propriety and value for money in the spending of public funds.
He is responsible for investigating whether public spending bodiesachieve the best possible value for money and adhere to the higheststandards of financial management.
He is independent and not subject to the control of any member of theScottish Executive or the Parliament.
The Auditor General is responsible for securing the audit of the ScottishExecutive and most other public sector bodies except local authoritiesand fire and police boards.
The following bodies fall within the remit of the Auditor General:
• departments of the Scottish Executive eg the Health Department• executive agencies eg the Prison Service, Historic Scotland• NHS boards• further education colleges• Scottish Water• NDPBs and others eg Scottish Enterprise.
AcknowledgmentsAudit Acotland is grateful to David Murphy and Lynne Jarvis of theInformation and Statistics Division of the Common Services Agency andto Phil Clare of the Audit Commission for providing the data for thisreport.
The study team was George Abraham and John Simmons under thegeneral direction of Barbara Hurst, Director of Performance Audit (Healthand Community Care).
Audit Scotland is a statutory body set up in April 2000under the Public Finance and Accountability (Scotland) Act2000. It provides services to the Auditor General forScotland and the Accounts Commission. Together theyensure that the Scottish Executive and public sector bodiesin Scotland are held to account for the proper, efficient andeffective use of public funds.

Contents1
Part 1. IntroductionPage 2
Benefits of day surgeryReviewing day surgery in ScotlandSummary of key findingsPage 3
Part 2. Progress against 1998targetsPage 4
Variation among trustsPage 5
Trends in day surgeryBarriers to day surgeryPage 7
Part 3. Comparison with EnglandPage 9
Part 4 Refining the basket ofproceduresPage 11
Part 5. Increasing day surgeryPage 12
Part 6. Costs of day surgeryPage 13
Part 7. RecommendationsPage 14
Appendix 1Page 15
Appendix 2Page 17
Appendix 3Page 25

Day surgery should be the preferred option where it provides better or more acceptable care for patients, or where the care is of the same standard but the cost is lower.
2
Part 1. Introduction

Benefits of day surgery
1.1 Over a decade ago the RoyalCollege of Surgeons of Englandconcluded that day surgery issuperior to inpatient care for manyconditions and that it can be aneffective way of reducing waitingtimes
1. Day surgery should be the
preferred option where it providesbetter or more acceptable care forpatients, or where the care is of thesame standard but the cost is lower.
1.2 A recent Department of Healthreport
2summarised the benefits of
day surgery as:
• Patients receive treatment that issuited to their needs and whichallows them to recover in theirown home.
• Cancellation of surgery due toemergency pressures in adedicated day surgery unit isunlikely.
• The risk of hospital acquiredinfection is reduced.
• Clinicians can provide high qualitycare for appropriate patients, andrelease inpatient beds for moremajor cases.
• Trusts improve their throughput ofpatients, facilitate bookings, andreduce waiting lists.
Reviewing day surgery in Scotland
1.3 In the early 1990s the AuditCommission developed a basket of20 common surgical procedureswhich were at that time being treatedas either day cases or inpatients. Thebasket accounted for about 40% ofall surgery in the specialtiesrepresented. The Audit Commissionreport highlighted the scope tosignificantly increase the proportionof patients treated as day cases.
A review carried out by the ScottishOffice Audit Unit in 1991 found asimilar picture in Scotland, and thisled to the establishment of Scottishtargets. These were adopted by theScottish Health Service ManagementExecutive in 1994 with the goal ofachieving the targets by 1997.
1.4 The Accounts Commission’s reportBetter by the day? was published in1997 and an up-date report issued in1998
3. Both reports reviewed the
level of day surgery in Scotland forthe selected ‘basket’ of proceduresagainst the 1997 targets. Better bythe day? recommended revisedtargets
4which the then Scottish
Office Health Department adopted.
1.5 The Scottish basket ofprocedures is currently the same asthat adopted by the AuditCommission in 1990 with theexceptions that the Scottish basketdoes not include dilation andcurettage or myringotomy as at thetime of our last review there was abody of opinion that the two areoften used when alternativetreatments would be moreappropriate
5,6. The Scottish basket
splits inguinal hernia betweenprocedures undertaken on adults andthose undertaken on children as achild’s operation is more likely to beappropriate for day surgery. Appendixone provides a short description ofeach of the 19 procedures in theScottish basket.
1.6 The purpose of this data reviewis to compare levels of day surgeryagainst:
• previous performance
• Scottish Executive targets, and
• levels of day surgery in England.
1.7 The Information and StatisticsDivision (ISD) of the CommonServices Agency provided the dataupon which the review is based.
Summary of key findings
1.8 Our main findings are that:
• There is still scope for increasingday surgery. If all trusts achievedthe SEHD 1998 targets set forthe basket of procedures thenumber of day case procedureswould increase by about 10%.
• The percentage of surgeryundertaken as day surgerycontinues to rise but the rate ofincrease has slowed considerably.
• In 2002/03 across Scotland as awhole the Scottish Executive’s1998 targets were achieved foronly seven of the revised basketof 19 procedures.
• The percentage of day surgeryvaries considerably amongsttrusts.
• In general Scotland has lower daysurgery rates than England.
• Some procedures, such ascystoscopies, which werepreviously carried out in inpatientand day case settings can now bedealt with as outpatients due tomedical advances in treatment.During 2002/03 10,000cystoscopies were carried out asinpatients,16,000 as day casesand 3,100 as outpatients. There isa need to monitor these types ofprocedures to ensure that theyare carried out in the mostappropriate setting and that daycase targets are not acting as aperverse incentive.
3Part 1. Introduction
1 Guidelines for Day Case Surgery, (revised edition March 1992), Royal College of Surgeons of England.2 Day Surgery: Operational guide, waiting, booking and choice, August 2002, Department of Health.3 Better by the day? Day surgery in Scotland, 1997, Accounts Commission, Better by the day-update, August 1998, Accounts Commission.4 The targets, a description of the various procedures and the OPCD and ICD codes are given in appendices 1 and 2.5 Diagnostic dilatation and curettage: is it used appropriately?, (1993), Coulter, Klassen, MacKenzie and McPherson.6 Children First: a study of hospital services, (1993), Audit Commission.

4
Part 2. Progress against 1998 targets

Part 2. Progress against 1998 targets
Correction bat earsNasal fractureLaparoscopyCystoscopyArthroscopy
GanglionBreast lump
CircumcisionTermination of pregnancy
Anal fissureSquint correction
Varicose veinsSubmucous resection
Carpal tunnelInguinal hernia adultInguinal hernia child
Dupuytren'sOrchidopexy
Cataracts
-20 0 20 40 60 80 100Day case rates
1998/99
Changes in percentage points 1989/99 - 2002-03
1998 Targets
Exhibit 1Change in day surgery rates between 1998/99 and 2002/03
2.4 Appendix 2 shows for each ofthe 19 procedures the performanceof trusts which carried out at least100 operations during 2002/03
7.
2.5 The level of variation isconsiderable, and is greater than canbe explained by location ordifferences in patients’circumstances. As well as thevariation among trusts, there isvariation within trusts. Previous workfor the Waiting List Support Group in1998 showed that there isconsiderable variation amongconsultants in the percentage of daysurgery they carry out.
2.1 Across Scotland as a whole theScottish Executive’s 1998 targetswere achieved for seven of the 19procedures in 2002/03. Although thetarget is still not being met for 12procedures, the percentage of daycases for 15 of the 19 proceduresreviewed has increased since 1998.Four procedures showed a fall inperformance (Exhibit 1).
2.2 The Scottish Executive HealthDepartment has included acomposite annual day surgery ratefor each NHS Board area in thePerformance AssessmentFramework, which is used to supportthe accountability reviews betweenthe Department and each NHS Board.
Variation among trusts
2.3 The Scotland wide positiondisguises the large variation amongtrusts in achieving day case targets.The best performing trusts achieved70% of the 1998 targets in 2002/03.Three trusts achieved less than 25%(Exhibit 2 overleaf). When trusts arecompared against the lower 1997targets six are achieving over 70%but one still only achieves 25%.
5
7 One-hundred operations was chosen as it was felt that less than this number would give unreliable percentages.

Note: These figures include only those procedures where a trust undertook more than 100 operations in 2002/03.
Exhibit 3Trends in day surgery rates
A&
C
Tays
ide
Gra
mpi
an
Nor
th G
lasg
ow
D&
G
Bor
ders
Hig
hlan
d
Lana
rksh
ire
A&
A
Sout
h G
lasg
ow
Wes
t Lot
hian
Forth
Val
ley
York
hill
Loth
ian
Fife
0
10
20
30
40
50
60
70
80
Perc
enta
ge
Trusts
1990/91 1992/93 1994/95 1996/97 1998/99 2000/01 2002/030
10
20
30
40
50
60
70
80
Perc
enta
ge
Year
Breast Lump
Arthroscopy
Varicose Veins
Circumcision
Laparoscopy
6
Exhibit 2Trusts’ performance against the 1998 day case targets
Percentage of 1998 targets met
Percentage of surgery undertaken as day cases

Part 2. Progress against 1998 targets 7
Trends in day surgery
2.6 The general trend is a slowing inthe rate of increase in day surgery(Exhibit 3).
2.7 This may be because trusts havereached the optimum level of daysurgery, or because some trusts arepaying less attention to developingday surgery as an alternative toinpatient care.
2.8 Exhibit 4 overleaf shows thechange in day surgery rates forvaricose veins and arthroscopybetween 1999/2000 and 2002/03. Itdemonstrates that some trusts withlow rates of day surgery have stayedthe same over the time period, whileothers with high rates reduced theirrates. This suggests that trusts havenot reached the optimum level.These two procedures were chosenfor illustrative purposes as they arecarried out in large numbers (4,500and 6,500 day cases per yearrespectively), and are from differentspecialties.
Barriers to day surgery
2.9 One potential barrier to high daysurgery rates in Scotland may be therural nature of some trusts. Extratravel time means some cases mayneed to be treated as inpatientsrather than as day cases. However,there are many examples of ruraltrusts undertaking high percentagesof procedures as day cases whichexceed the 1998 targets (Appendix 2). For example:
• Highland Acute carries out 92%of carpal tunnel procedures asday cases.
• Dumfries and Galloway – 99% ofcataracts as day cases.
• Argyll and Clyde – 58% ofsubmucous resection as daycases.
• Borders – 90% of laparoscopiesas day cases.
2.10 In each case, a rural trust isexceeding the national target, anddoing better than most urban trusts.
2.11 There is variation among ruraltrusts which suggest that geographyis not the only determinant ofperformance. Examples include:
• Laparoscopies, where Bordershas the second highestpercentage rate but Highland andDumfries & Galloway have thelowest.
• Submucous resection, whereArgyll & Clyde has the highestpercentage but Dumfries &Galloway is second lowest.
• Cataracts, where Dumfries &Galloway is the highest and Argyll& Clyde is the second lowest.
2.12 Previous audits found that themain barriers to optimum rates ofday surgery are:
• inappropriate and inadequate useof day surgery units
• poor management andorganisation of day surgery units
• some clinicians preferences forinpatient surgery.
2.13 NHS Boards should monitor thelevels of day surgery by procedureand specialty, to establish where daycase rates are low and takeappropriate action. They should alsomonitor levels of outpatient,endoscopy and day surgery toensure that procedures moreappropriately dealt with in anoutpatient or endoscopy setting arenot inappropriately using day casefacilities.

8
Gra
mpi
an U
niv
Nor
th G
lasg
ow U
niv
Dum
fries
& G
allo
way
Acu
te
Arg
yll &
Cly
de A
cute
Lana
rksh
ire A
cute
Ayr
shire
& A
rran
Acu
te
Loth
ian
Uni
v
Sout
h G
lasg
ow U
niv
Forth
Val
ley
Acu
te
Tays
ide
Uni
v
Hig
hlan
d A
cute
Bor
ders
Acu
te
Wes
t Lot
hian
Hea
lthca
re
Fife
Acu
te
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge
Trusts
1999/2000
2002/03
Bor
ders
Acu
te
Wes
t Lot
hian
Hea
lthca
re
Arg
yll &
Cly
de A
cute
Tays
ide
Uni
v
Sout
h G
lasg
ow U
niv
Forth
Val
ley
Acu
te
Lana
rksh
ire A
cute
Dum
fries
& G
allo
way
Acu
te
Hig
hlan
d A
cute
Nor
th G
lasg
ow U
niv
Ayr
shire
& A
rran
Acu
te
Loth
ian
Uni
v
Gra
mpi
an U
niv
Fife
Acu
te
0
10
20
30
40
50
60
70
80
Perc
enta
ge
Trusts
1999/2000
2002/03
Exhibit 4Trends in day surgery rates for varicose veins and arthroscopy
Varicose Veins
Arthroscopy

9
3.2 Exhibit 5 overleaf shows thelevels of day surgery for Scotland andEngland for the revised ‘basket’ ofprocedures. The English figuresshown are the median for 2001/02.The Scottish figures are for 2002/03and show both the means andmedians. Because of the smallnumber of trusts in Scotland themedian is sensitive so we haveincluded the mean to give anotherway of measuring Scottishperformance. This comparisonhighlights again the opportunity toincrease day surgery.
3.3 These English indicators includemyringotomy and D&C/hysteroscopy.Neither myringotomy or D&C wereincluded in our original report or thefirst part of this report. The decisionnot to include D&C and myringotomywas taken in 1997 as there was abody of opinion that the two wereoften used when alternativetreatments would be moreappropriate.
3.1 We compared the performanceof Scottish hospitals with Englishhospitals for 25 procedures whichmake up the current basket of daysurgery procedures used by theAudit Commission. Overall Scotlandhas lower day surgery rates thanEngland:
• The percentage of day cases wassimilar for 12 procedures.
• English hospitals carry out ahigher percentage of day casesfor a further 11 procedures.
• Scottish hospitals carry out ahigher percentage of day cases intwo procedures.
Part 3. Comparison with EnglandPart 3. Comparison with England

Note: Dilatation and curettage and myringotomy are included although these are not included in the Scottish basket.
Sub-mucous resection
Haemorrhoidectomy
Excision of breast lump
Operation for bat ears
Anal fissure dilation/excision
D&C / hysteroscopy
Removal of metalware
Extraction of cataract w/wo implant
Correction of squint
Inguinal hernia
Laparoscopy
Orchidopexy
Varicose vein stripping/ligation
Reduction nasal fracture
Myringotomy w/wo grommets
Arthroscopy
Circumcision
Excision dupuytren's contracture
Excision of ganglion
Termination of pregnancy
TUR bladder tumour
Tonsillectomy
Laparoscopic cholecystectomy
Carpal tunnel decompression
Bunion operations
Scottish mean
Scottish median
English median
0 20 40 60 80 100
Percentage day cases
10
Exhibit 5Scottish and English day surgery rates

11
be carried out on an outpatient basisand so is no longer a reliable measureof progress with day surgery.
4.3 We asked ISD to check six of theprocedures to see if they are nowroutinely done as outpatients. Dataon outpatient procedures are not asrobust as for day and inpatientsurgery and therefore the results arenot as comprehensive. But, in linewith England, the only procedure toshow any significant number ofoutpatient cases was cystoscopy. In2002/03 there were about 26,000day and inpatient cases and about3,100 outpatient cases. For the otherprocedures checked the number ofoutpatient operations recorded wasin single figures.
4.4 One trust undertakes a largenumber of cataract operations asoutpatient procedures while stillundertaking large numbers as bothday cases and inpatients. This, alongwith the changes taking place in theprovision of cystoscopy procedures,demonstrates the need to collectinformation on outpatient, day caseand inpatient treatment on a consistentbasis. We recommend that:
• SEHD adopts the revised basketof procedures in use in Englandwith the exception of inguinalhernia which we wouldrecommend remains splitbetween children and adults. Thiswould allow:
– the comparison of overallperformance of Scotland withEngland
– comparisons with a largernumber of trusts. This wouldbe useful for all proceduresbut would have a particularvalue for children’s hospitalswhere the comparisonsavailable on a Scotland widebasis are limited.
• Information on outpatient, daycase and inpatient treatment iscollected on a consistent basis toallow monitoring of how boardsare progressing the shift frominpatient to day case and frominpatient and day case to outpatient care.
4.1 A basket of procedures is used toprovide a consistent measure ofperformance. The original basketused in Scotland and Englandincluded procedures which:
• are commonly performed, so thatthey account for a large volume ofsurgery
• are suitable for treatment as daycases
• would not generally be performedin an outpatient setting, thusfocusing attention on the potentialto treat more inpatients as daycases.
4.2 However, advances in medicaltreatment mean that the basketneeds revising periodically to ensurethat the procedures are stillappropriate for day surgery ratherthan outpatient treatment. In 2000the Audit Commission, in liaison withthe British Association of DaySurgery, revised its basket ofprocedures. The Audit Commissionretained all the procedures used inthe Scottish ‘basket’ exceptcystoscopy. This procedure can now
Part 4. Refining the basket of procedures
Part 4. Refining the basket of procedures

5.4 As surgery continues to developand new procedures becomeappropriate for day surgery oroutpatient treatment, there will bemore opportunities to move awayfrom inpatient care. Targets for daysurgery are an important way ofencouraging new methods oftreatment, but they need to be usedflexibly to avoid constraining furtherchange in future.
5.1 Comparisons against Scottishtargets and English performancedemonstrate that there is stillpotential to increase day surgeryrates. This is supported by thevariation among trusts, with someachieving the 1998 targets but manyfalling considerably short.
5.2 To give some indication of thepotential for increase, we calculatethat if all trusts achieved the 1998targets, then day case rates for thebasket of procedures would increaseby about 10% which equates to anextra 5,700 cases (Appendix 3 showsthe number of inpatient and daycases for each procedure).
5.3 More than a quarter of Englishtrusts are performing above the 1998targets for fourteen out of sixteenScottish procedures for which wehave English comparators. This,together with the number of Scottishtrusts already achieving the targets,confirms that the targets areachievable.
12
Part 5. Increasing day surgery

Part 6. Costs of day surgery 13
Part 6. Costs of day surgery
6.1 The importance of day surgery isthat, for appropriate procedures, itcan provide better care and be morecost effective than inpatienttreatment. A number of studies sincethe 1970s have shown that,managed efficiently, day surgery ischeaper than inpatient surgery.
Variations in cost
6.2 The Scottish Health ServicesCosts Book gives the average cost ofa day case as £450. The average costranges from £245 at the VictoriaInfirmary, Glasgow to £758 inBorders General Hospital. Atspecialty level, for general surgerythe range is from £141 at VictoriaInfirmary, Glasgow to £1,569 atBorders General Hospital. Howeverthese aggregated figures are oflimited use. The cost of differentprocedures varies, so comparing theaverage cost per case of all daysurgery can be misleading as it doesnot take account of case mixvariations.
6.3 Variation in cost can also be dueto other factors:
• day cases in one trust mayinclude procedures which arecommonly being carried out in outpatient settings in other trusts
• even for similar day caseprocedures the financialinformation may not be compiledon a like-for-like basis.
6.4 Using an agreed basket ofprocedures helps address theproblem of inconsistency, but it doesnot resolve the difficulty of differentcosting methods.
Comparative costs – inpatients and
day surgery
6.5 For day surgery to be costeffective the alternative must beinpatient surgery rather thanoutpatient treatment. All 19procedures in the Scottish basket,with the exception of cystoscopy, arestill appropriately treated as eitherday cases or inpatients.
6.6 We asked ISD to produceinpatient and day case costs for twoof our basket of procedures –excision of breast lump andlaparoscopy. Inpatient cases werebetween 2 and 2.5 times moreexpensive – £1,266 compared to£511 for excision of a breast lump,and £1,350 compared to £606 forlaparoscopy. This level of saving maynot be achievable in practice, aspatients who are likely to experiencecomplications are more likely to betreated as inpatients which in itselfmay increase costs.
6.7 Real savings can be made if daysurgery directly substitutes forinpatient surgery, and inpatient bedsare reduced as a result. However, inmany cases beds released by daysurgery are used for other patients.In this situation total costs will rise,but as more patients have beentreated in a less expensive way thecost per case will fall. Both scenariosare cost effective, but only oneachieves a real cost reduction.
Cost effectiveness of changes in
the treatment of cataract removal
6.8 Between 1990/91 and 1996/97the total number of cataractremovals increased from 10,000to 16,000. The increase was allday cases; the number of inpatientcases remained the same at10,000. There was no substitutionof day cases for inpatient casesover this period; instead all theincrease in demand was cateredfor by increased day case activity.
6.9 Between 1996/97 and 2002/03the total number of cataractremovals increased from 16,000to 20,000. Over this period, thenumber of inpatient casesdropped from 10,000 to 3,500.The increase in day cases from6,000 to 16,500 not only coveredall the increases in cases as in theearlier period, but also directlysubstituted for inpatient cases,allowing inpatient numbers to dropby over 6,500.
6.10 In summary change in costs arenot simple to predict. It depends onabsolute levels of care as well aslocal circumstances. But day surgeryis more cost-effective than inpatientcare, and allows more patients to betreated for a given level of resources.

7.3 SEHD should consider thebenefits of adopting the same basketof procedures as used in Englandwith the exception of retaining bothadult and children’s inguinal hernia.This would allow comparison withEngland and would also mean theadoption of a basket which hadalready been developed inconsultation with the BritishAssociation for Day Surgery.
7.4 SEHD in conjunction with ISDshould ensure information onoutpatient, day case and inpatienttreatment is collected on a consistentbasis to allow monitoring of howboards are progressing the shift frominpatient to day case and frominpatient and day case to outpatientcare.
7.1 NHS Boards should monitor thelevels of day surgery by procedureand specialty, to establish where daycase rates are low and takeappropriate action. They should alsomonitor levels of outpatient,endoscopy and day surgery toensure that procedures moreappropriately dealt with in an outpatient or endoscopy setting arenot inappropriately using day casefacilities
7.2 The Scottish Executive HealthDepartment (SEHD) should monitorthe performance of NHS Boards.
14
Part 7. Recommendations

Appendix 1 15
Appendix 1: The ‘basket’ of procedures1. Inguinal hernia operations: repair
of a rupture in the groin.
This operation is to remove anoutpouching of the abdominal sack.In children it is usually sufficient to tieoff the sack (Herniotomy) but inadults it is also necessary to repairthe weakness in the muscles byusing a darn of strong thread or wire(Herniorraphy). Although these aretechnically correct terms, bothoperations are commonly referred toas ‘hernia repair’.
Specialties usually performing thisprocedure are general surgery andpaediatric surgery.OPCS 4 & ICD 9 codes: T19 throughto T21
2. Excision of breast lump
The operation may consist ofremoving the whole lump or onlypart of it. Sometimes, if it is thoughtlikely to be cancer, the biopsy can beexamined immediately using amicroscopy technique called ‘frozensection’. In this case, the intentionmay be to proceed straight away to amastectomy (breast removal) if theresult confirms cancer, and suchcases will not be day cases.
The specialty usually performing thisprocedure is general surgery.OPCS 4 & ICD 9 codes: B32, B28.3
3. Anal fissure dilatation or excision
Treatment for a tear of the bowellining just inside the anus. Analdilatation is also used in the absenceof a fissure as a treatment forhaemorrhoids.
The specialty usually performing thisprocedure is general surgery.OPCS 4 & ICD 9 codes: H54, H56.2,H56.4
4. Varicose vein stripping or ligation
The removal or tying off of tortuousveins in the leg.
The specialty usually performing thisprocedure is general surgery.OPCS 4 & ICD 9 codes: L85, L87
5. Cystoscopy, diagnostic and
operative
Inspection of the inside of thebladder to establish a diagnosisand/or carry out simple procedures.
The specialty usually performing thisprocedure is urological surgery.OPCS 4 & ICD 9 codes: M28, M29,M30, M42, M43, M44, M45, M76,M77, M32.1, M32.2 M32.3
6. Circumcision
The cutting off of the foreskin orprepuce.
Specialties usually performing thisprocedure are general surgery,urological surgery and paediatricsurgery.OPCS 4 & ICD 9 codes: N30.3
7. Excision of Dupuytren’s
contracture
Removal of contracted fibrous tissue(fascia) under the skin of the palm.
The specialty usually performing thisprocedure is orthopaedic surgery.OPCS 4 & ICD 9 codes: If principaldiagnosis = 728.6 and op codes T52,T54
8. Carpal tunnel decompression
A nerve, called the median nerve,runs down the arm to supply someof the muscles and skin sensation inthe hand. Sometimes it becomescompressed where it passes throughthe wrist, under a band of fibroustissue. The treatment is to make anincision at the wrist and release thenerve.
The specialty usually performing thisprocedure is orthopaedic surgery.OPCS 4 & ICD 9 codes: A65
9. Arthroscopy – any joint diagnostic
and operative
Inspection of the inside of a joint-most commonly the knee.
The specialty usually performing thisprocedure is orthopaedic surgery.OPCS 4 & ICD 9 codes: W82through to W88
10. Excision of ganglion
Removal of the outpouching of thelining of a small joint.
The specialty usually performing thisprocedure is orthopaedic surgery.OPCS 4 & ICD 9 codes: T59, T60
11. Orchidopexy
An operation to correct undescendedtestes, usually in children aged 2 - 8years. It is very rare in adults.
Specialties usually performing thisprocedure are general surgery,urological surgery and paediatricsurgery.OPCS 4 & ICD 9 codes: N08, N09
12. Cataract extraction, with or
without implant
Removal of an opacified lens fromthe eye sometimes including theinsertion of an artificial lens.
The specialty usually performing thisprocedure is ophthalmology.OPCS 4 & ICD 9 codes: If principaldiagnosis = 366 and op. Codes C71through to C77.
13. Correction of squint
A squint is caused by disturbance tothe balance of pull of the six muscleswhich move the eyeball in its socket.Correction involves re-positioning ofthe muscles on the eyeball to reducethe effect of some by recession andincrease the effect of others byresection or shortening.

16
The specialty usually performing thisprocedure is ophthalmology.OPCS 4 & ICD 9 codes: If principaldiagnosis = 378 and op. Codes C31through to C35.
14. Myringotomy, with or without
insertion of grommets
A hole is made in the ear drum(myringotomy), then a small tube orgrommet may be inserted into theear drum to keep the hole open.
Specialties usually performing thisprocedure are ear, nose and throatsurgery (ENT) and paediatric surgery.OPCS 4 & ICD 9 codes: D15, D20.2,D20.3
15. Sub mucous resection
An incision is made in the mucousmembrane covering the septum, andmisplaced cartilage and bone arethen cut away.
The specialty usually performing thisprocedure is ENT surgery.OPCS 4 & ICD 9 codes: E04, E03.1,E03.6
16. Reduction of nasal fracture
The realignment of displaced bonesfollowing a broken nose.
The specialty usually performing thisprocedure is ENT surgery.OPCS 4 & ICD 9 codes: V09.2
17. Operation for ‘bat’ ears
The removal of skin and soft tissuefrom behind the ears to allow the earto sit back flatter against the head.
The specialty usually performing thisprocedure is plastic surgery.OPCS 4 & ICD 9 codes: D03.3
18. Dilatation & Curettage
The opening up of the neck of thewomb to allow for its lining to bescraped out.
The specialty usually performing thisprocedure is gynaecology.OPCS 4 & ICD 9 codes: Q10.3
19. Laparoscopy, with or without
sterilisation
The inspection of the abdominalcavity sometimes including blockingthe ‘tubes’ from the ovaries to thewomb.
The specialty usually performing thisprocedure is gynaecology.OPCS 4 & ICD 9 codes: Q35, Q36,Q38, Q39, Q41, Q49, Q50, Q37.1,T43.9
20. Termination of pregnancy
Removal of an intra-uterinepregnancy through the neck of thewomb.
The specialty usually performing thisprocedure is gynaecology.OPCS 4 & ICD 9 codes: If principaldiagnosis = 635 and Q10, Q11, Q14in 1st or 2nd position.
Appendix 2
Nor
th G
lasg
ow U
niv
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
niv
Dum
fries
& G
allo
way
Acu
te
Fife
Acu
te
Arg
yll &
Cly
de A
cute
Sout
h G
lasg
ow U
niv
Loth
ian
Uni
v
Tays
ide
Uni
v
Wes
t Lot
hian
Hea
lthca
re
Hig
hlan
d A
cute
Lana
rksh
ire A
cute
Forth
Val
ley
Acu
te
0
10
20
30
40
50
60
70
80
Perc
enta
ge d
ay c
ases
Trusts
1998 target1997 target
17
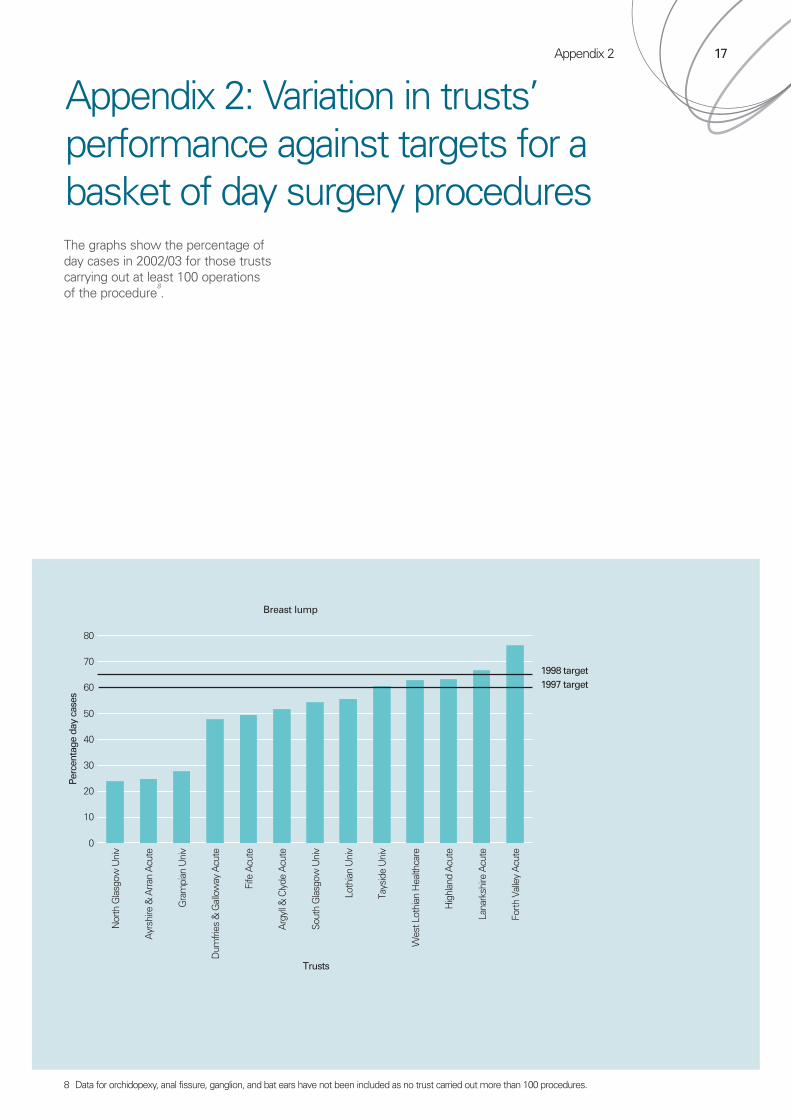
The graphs show the percentage ofday cases in 2002/03 for those trustscarrying out at least 100 operationsof the procedure
8.
Appendix 2: Variation in trusts’performance against targets for a basket of day surgery procedures
8 Data for orchidopexy, anal fissure, ganglion, and bat ears have not been included as no trust carried out more than 100 procedures.
Breast lump

Arg
yll &
Cly
de A
cute
Nor
th G
lasg
ow U
niv
Tays
ide
Uni
v
Wes
t Lot
hian
Hea
lthca
re
Ayr
shire
& A
rran
Acu
te
Loth
ian
Uni
v
Forth
Val
ley
Acu
te
Dum
fries
& G
allo
way
Acu
te
Sout
h G
lasg
ow U
niv
Hig
hlan
d A
cute
Lana
rksh
ire A
cute
Gra
mpi
an U
niv
Fife
Acu
te
0
10
20
30
40
50
60
70
80
90
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
Dum
fries
& G
allo
way
Tays
ide
Uni
v
Gra
mpi
an U
niv
Hig
hlan
d A
cute
Ayr
shire
& A
rran
Acu
te
Bor
ders
Acu
te
Fife
Acu
te
Wes
tern
Isle
s
Nor
th G
lasg
ow U
niv
Sout
h G
lasg
ow U
niv
Lana
rksh
ire A
cute
Arg
yll &
Cly
de A
cute
Loth
ian
Uni
v
Forth
Val
ley
Acu
te
Wes
t Lot
hian
Hea
lthca
re
0
10
20
30
40
50
60
70
80
90
Perc
enta
ge d
ay c
ases
Trusts
1997 and 1998 target
18
Cystoscopy
Varicose veins

Appendix 2
Gra
mpi
an U
nive
rsity
Tays
ide
Uni
vers
ity
Ayr
shire
& A
rran
Nor
th G
lasg
ow U
nive
rsity
Wes
t Lot
hian
Hea
lthca
re
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
19
Nor
th G
lasg
ow U
niv
Arg
yll &
Cly
de A
cute
Lana
rksh
ire A
cute
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
niv
Forth
Val
ley
Acu
te
Fife
Acu
te
Loth
ian
Uni
v
York
hill
Tays
ide
Uni
v
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
Dupuytren’s
Circumcision

Arg
yll &
Cly
de A
cute
Tays
ide
Uni
v
Lana
rksh
ire A
cute
Forth
Val
ley
Acu
te
Wes
t Lot
hian
Hea
lthca
re
Loth
ian
Uni
v
Nor
th G
lasg
ow U
niv
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
niv
Sout
h G
lasg
ow U
niv
Hig
hlan
d A
cute
Fife
Acu
te
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target1997 target
Nor
th G
lasg
ow U
niv
Dum
fries
& G
allo
way
Acu
te
Gra
mpi
an U
niv
Arg
yll &
Cly
de A
cute
Lana
rksh
ire A
cute
Ayr
shire
& A
rran
Acu
te
Bor
ders
Acu
te
Sout
h G
lasg
ow U
niv
Forth
Val
ley
Acu
te
Hig
hlan
d A
cute
Loth
ian
Uni
v
Tays
ide
Uni
v
Fife
Acu
te
Wes
t Lot
hian
Hea
lthca
re
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
20
Arthroscopy
Carpal tunnel

Appendix 2
Grampian University North Glasgow Tayside University Lothian University Yorkhill0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
21
Gra
mpi
an U
niv
Arg
yll &
Cly
de A
cute
Wes
tern
Isle
s
Tays
ide
Uni
v
Hig
hlan
d A
cute
Sout
h G
lasg
ow U
niv
Forth
Val
ley
Acu
te
Loth
ian
Uni
v
Fife
Acu
te
Nor
th G
lasg
ow U
niv
Bor
ders
Acu
te
Ayr
shire
& A
rran
Acu
te
Lana
rksh
ire A
cute
Wes
t Lot
hian
Hea
lthca
re
Dum
fries
& G
allo
way
Acu
te
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 and 1997 target
Squint correction
Cataracts

Wes
t Lot
hian
Dum
fries
& G
allo
way
Acu
te
Tays
ide
Uni
v
Fife
Acu
te
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
niv
Nor
th G
lasg
ow U
niv
Sout
h G
lasg
ow U
niv
Loth
ian
Uni
v
Lana
rksh
ire A
cute
Arg
yll &
Cly
de A
cute
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
Nor
th G
lasg
ow
Sout
h G
lasg
ow U
nive
sity
Lana
rksh
ire A
cute
Tays
ide
Uni
vers
ity
Loth
ian
Uni
vers
ity
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1997 and 1998 target
22
Nasal fracture
Submucous resection

Appendix 2
Hig
hlan
d A
cute
Dum
fries
& G
allo
way
Acu
te
Forth
Val
ley
Acu
te
Arg
yll &
Cly
de A
cute
Nor
th G
lasg
ow U
niv
Sout
h G
lasg
ow U
niv
Wes
t Lot
hian
Hea
lthca
re
Gra
mpi
an U
niv
Bor
ders
Acu
te
Lana
rksh
ire A
cute
Tays
ide
Uni
v
Loth
ian
Uni
v
Ayr
shire
& A
rran
Acu
te
Fife
Acu
te
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
23
Hig
hlan
d A
cute
Dum
fries
& G
allo
way
Acu
te
Gra
mpi
an U
niv
Arg
yll &
Cly
de A
cute
Sout
h G
lasg
ow U
niv
Nor
th G
lasg
ow U
niv
Tays
ide
Uni
v
Forth
Val
ley
Acu
te
Lana
rksh
ire A
cute
Ayr
shire
& A
rran
Acu
te
Fife
Acu
te
Loth
ian
Uni
v
Bor
ders
Acu
te
Wes
t Lot
hian
Hea
lthca
re
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge d
ay c
ases
Trusts
1998 target1997 target
Termination of pregnancy
Laparoscopy

Yorkhill Lothian University0
10
20
30
40
50
60
70
80
90
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
Bor
ders
Acu
te
Arg
yll &
Cly
de A
cute
Wes
t Lot
hian
Hea
lthca
re
Nor
th G
lasg
ow U
niv
Hig
hlan
d A
cute
Dum
fries
& G
allo
way
Acu
te
Forth
Val
ley
Acu
te
Tays
ide
Uni
v
Ayr
shire
& A
rran
Acu
te
Sout
h G
lasg
ow U
niv
Lana
rksh
ire A
cute
Gra
mpi
an U
niv
Loth
ian
Uni
v
Fife
Acu
te
0
10
20
30
40
50
60
70
Perc
enta
ge d
ay c
ases
Trusts
1998 target
1997 target
24
Inguinal hernia – adult
Inguinal hernia – children
Appendix 3 25
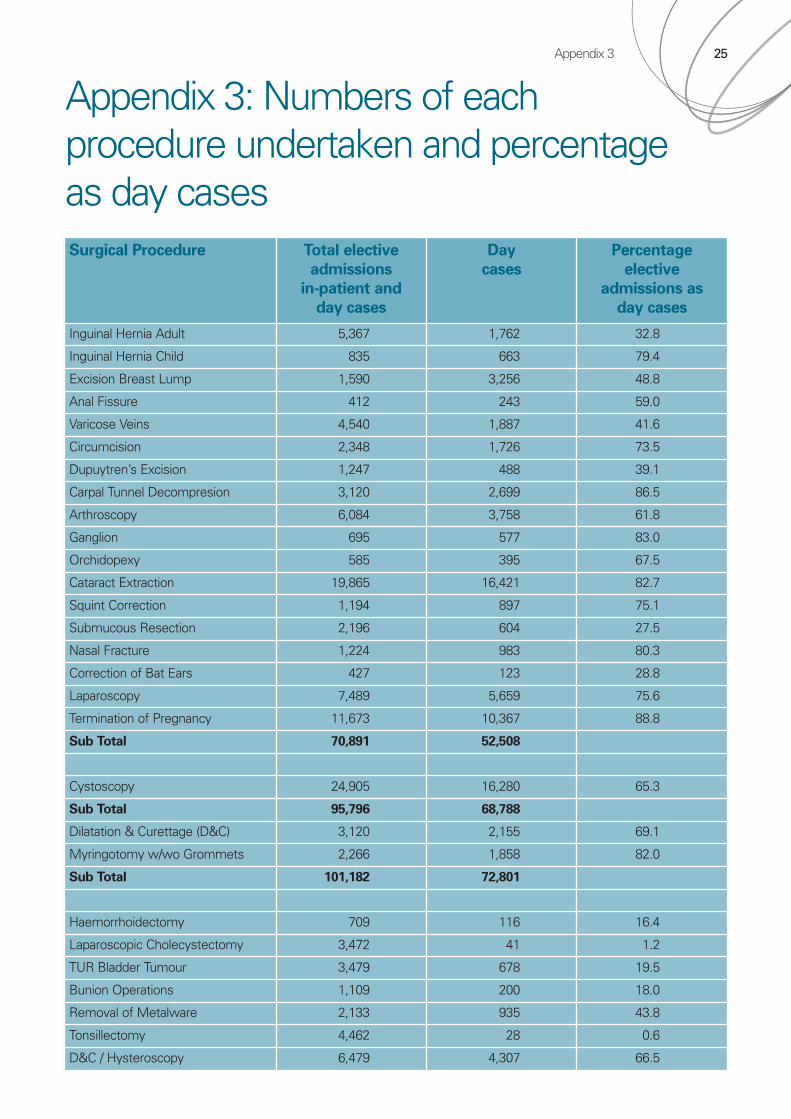
Appendix 3: Numbers of each procedure undertaken and percentage as day casesSurgical Procedure Total elective
admissions
in-patient and
day cases
Day
cases
Percentage
elective
admissions as
day cases
Inguinal Hernia Adult 5,367 1,762 32.8
Inguinal Hernia Child 835 663 79.4
Excision Breast Lump 1,590 3,256 48.8
Anal Fissure 412 243 59.0
Varicose Veins 4,540 1,887 41.6
Circumcision 2,348 1,726 73.5
Dupuytren’s Excision 1,247 488 39.1
Carpal Tunnel Decompresion 3,120 2,699 86.5
Arthroscopy 6,084 3,758 61.8
Ganglion 695 577 83.0
Orchidopexy 585 395 67.5
Cataract Extraction 19,865 16,421 82.7
Squint Correction 1,194 897 75.1
Submucous Resection 2,196 604 27.5
Nasal Fracture 1,224 983 80.3
Correction of Bat Ears 427 123 28.8
Laparoscopy 7,489 5,659 75.6
Termination of Pregnancy 11,673 10,367 88.8
Sub Total 70,891 52,508
Cystoscopy 24,905 16,280 65.3
Sub Total 95,796 68,788
Dilatation & Curettage (D&C) 3,120 2,155 69.1
Myringotomy w/wo Grommets 2,266 1,858 82.0
Sub Total 101,182 72,801
Haemorrhoidectomy 709 116 16.4
Laparoscopic Cholecystectomy 3,472 41 1.2
TUR Bladder Tumour 3,479 678 19.5
Bunion Operations 1,109 200 18.0
Removal of Metalware 2,133 935 43.8
Tonsillectomy 4,462 28 0.6
D&C / Hysteroscopy 6,479 4,307 66.5

Day surgery in Scotland – reviewing progress
Audit Scotland110 George StreetEdinburgh EH2 4LH
Telephone0131 477 1234Fax0131 477 4567
www.audit-scotland.gov.uk ISBN 1 904651 38 0 AGS/2004/3