de um sistema integrado para avaliação inicial dos ... thesis... · ana meireles a medisa título...
TRANSCRIPT

| 1Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
desenvolvimento de um sistema integrado para avaliação inicial dos doentes oncológicos admitidos em cuidados paliativos
josé antónio saraiva ferraz gonçalves
porto
2011
Orientador: Professor Doutor Rui NunesCo-orientador: Dr. Nigel Sykes

2 | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Desenvolvimento de um Sistema Integrado para a Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos.
José António Saraiva Ferraz Gonçalves
do autor
978-989-xxxxxxxxxxxxx
2012
Ana Meireles
A Medisa
título
autor
edição
isbn
ano
edição do texto
acabamento

| 3Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Tese de candidatura ao grau de doutorapresentada à Faculdade de Medicina da Universidade do Porto

4 | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 5Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Artigo 48, parágrafo 3º
“A Faculdade não responde pelas doutrinas expedidas na dissertação”
Regulamento da Faculdade de Medicina da Universidade do Porto
Decreto Lei nº 19337, de 29 de Janeiro de 1931

6 | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 7Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Júri da Prova de Doutoramento
Presidente
Vogais
Reitor da Universidade do Porto
Doutor José Eduardo Torres Eckenroth GuimarãesPofessor Catedrático da Faculdade de Medicina da Universidade do Porto
Doutora Maria Amélia Duarte FerreiraPofessora Catedrática da Faculdade de Medicina da Universidade do Porto
Doutor Rui Manuel Lopes NunesPofessor Catedrático da Faculdade de Medicina da Universidade do PortoOrientador da tese
Doutora Guilermina Maria da Silva RegoPofessora Auxiliar da Faculdade de Medicina da Universidade do Porto
Doutora Marília Assunção Rodrigues Ferreira DouradoPofessora Auxiliar da Faculdade de Medicina da Universidade de Coimbra
Doutor António José Feliciano BarbosaPofessor Auxiliar Convidado da Faculdade de Medicina da Universidade de Lisboa

8 | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 9Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
corpo catedrático da faculdade de medicina da universidade do porto
Professores Catedráticos Efectivos
Alberto Manuel Barros da SilvaAltamiro Manuel Rodrigues Costa PereiraAntónio Albino Coelho Marques Abrantes TeixeiraAntónio Carlos Freitas Ribeiro SaraivaDaniel Filipe Lima MouraDeolinda Maria Valente Alves Lima TeixeiraFrancisco Fernando Rocha GonçalvesIsabel Maria Amorim Pereira RamosJoão Francisco Montenegro Andrade Lima BernardesJorge Manuel Mergulhão Castro TavaresJosé Agostinho Marques LopesJosé Carlos Neves da Cunha AreiasJosé Eduardo Torres Eckenroth GuimarãesJosé Henrique Dias Pinto de BarrosJosé Manuel Lopes Teixeira AmaranteJosé Manuel Pereira Dias de Castro LopesManuel Alberto Coimbra Sobrinho SimõesManuel António Caldeira Pais ClementeManuel Jesus Falcão Pestana VasconcelosMaria Amélia Duarte FerreiraMaria Dulce Cordeiro MadeiraMaria Fátima Machado Henriques CarneiroMaria Leonor Martins Soares DavidPatrício Manuel Vieira Araújo Soares SilvaRui Manuel Almeida Mota CardosoRui Manuel Lopes Nunes
10 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Professores Catedráticos Jubilados e Aposentados
Abel José Sampaio da Costa TavaresAbel Vitorino Trigo CabralAlexandre Alberto Guerra Sousa PintoAmândio Gomes Sampaio TavaresAntónio Augusto Lopes VazAntónio Carvalho Almeida CoimbraAntónio Fernandes da FonsecaAntónio Fernandes Oliveira Barbosa Ribeiro BragaAntónio Germano Pina Silva LealAntónio José Pacheco PalhaAntónio Luís Tomé da Rocha RibeiroAntónio Manuel Sampaio de Araújo TeixeiraBelmiro dos Santos PatrícioCândido Alves Hipólito ReisCarlos Rodrigo Magalhães RamalhãoCassiano Pena de Abreu e LimaDaniel Santos Pinto SerrãoEduardo Jorge Cunha Rodrigues PereiraFernando de Carvalho Cerqueira Magro FerreiraFernando Tavarela VelosoFrancisco de Sousa LéHenrique José Ferreira Gonçalves Lecour de MenezesJosé Augusto Fleming TorrinhaJosé Carvalho de OliveiraJosé Fernando Barros Castro CorreiaJosé Luís Medina VieiraJosé Manuel Costa Mesquita GuimarãesLevi Eugénio Ribeiro GuerraLuís Alberto Martins Gomes de AlmeidaManuel Augusto Cardoso de OliveiraManuel Machado Rodrigues GomesManuel Maria Paula BarbosaMaria da Conceição Fernandes Marques MagalhãesMaria Isabel Amorim de AzevedoMário José Cerqueira Gomes BragaSerafim Correia Pinto GuimarãesValdemar Miguel Botelho dos Santos CardosoWalter Friedrich Alfred Osswald

| 11 11Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Para a Ângela, o Daniel e o Ricardo.

12 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 13 13Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
You may say I´m a dreamerBut I´m not the only one…
John Lennon

14 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 15 15Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
agradecimentos
Num trabalho que representa um corte num processo de investigação que começou há vários anos, a par de outros projectos que se vêm a realizar, há muitas pessoas que contribuiram e cujo trabalho merece reconhecimento. Desde logo aos investigadores que participaram em todos os projectos que o compõem. Tenho de agradecer ao meu orientador o Professor Doutor Rui Nunes pelo seu encorajamento, pelas suas sugestões e pela leitura crítica deste trabalho. Agradeço também ao Dr. Nigel Sykes, meu coorientador, as sugestões, sobretudo no que respeita à investigação que consta dos capítulos 4 e 5. Agradeço ainda à Professora Doutora Guilhermina Rego pelo seu apoio e leitura crítica da tese.
Não posso esquecer a minha equipa na Unidade de Cuidados Paliativos da Rede do IPO - Porto sem a qual este trabalho não teria sido possível. Também a colaboração dos doentes e das suas famílias foi indispensável. E por último, mas sem dúvida mais importante, à minha família que tornou possível o atingir deste e doutros objectivos.
16 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 17 17Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
índice
Introdução
· Introdução· A Portuguese Palliative care unit· Objectivos do desenvolvimento do sistema integrado para a avaliação inicial dos doentes oncológicos admitidos em cuidados paliativos
Comunicação
· Comunicação/Informação· Diagnosis disclosure in a portuguese oncological centre· Breaking bad news: experiences and preferences of advanced cancer patients at a portuguese oncology centre· Síntese
Avaliação da Consciência
· Avaliação da consciência· Validation of a conscienciousness levels scale for paliative care· Avaliação da função cognitiva
1
2
3
21
23
29
35
39
41
43
53
61
63
65
67
75

18 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Avaliação dos doentes sem alterações cognitivas
· Avaliação dos doentes sem alterações cognitivas· O método de Delfos· Discussão
Avaliação dos doentes com alterações cognitivas
· Avaliação dos doentes com alterações cognitivos· Estudo 1· Estudo 2· Discussão
Conclusão
· Conclusão
Resumo
· Resumo
Abstract
· Abstract
Anexos
Artigos publicados
Artigos publicados como membro do Research Steering Committee da
Associação Europeia de Cuidados Paliativos
4
5
6
7
8
9
10
11
79
81
83
91
97
99
101
107
109
113
115
119
121
125
127
131
157
273
| 19 19Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
índice de quadros
Distribuição das doenças não oncológicas.
Método de avaliação da confusão.
Lista inicial de sintomas/problemas.
Lista final.
Forma final do instrumento.
Formulário de avaliação.
Regras para aplicação do método de avaliação do sofrimento.
Dados demográficos.
Proporções de concordância.
Dados demográficos.
Quadro 1
Quadro 2
Quadro 3
Quadro 4
Quadro 5
Quadro 6
Quadro 7
Quadro 8
Quadro 9
Quadro 10

20 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 21 21Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
1INTRODUÇÃO

22 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 23 23Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Em Portugal morrem cerca de 100 000 pessoas em cada ano, das quais cerca de 20% de cancro [1]. Uma percentagem ainda maior morre de doenças cardiovasculares, mas também morrem muitos doentes de doenças pulmonares, renais, hepáticas, neurológicas, SIDA, etc. A maioria destas são hoje doenças crónicas, com um período mais ou menos longo em que os tratamentos destinados a alterar o seu desenvolvimento natural não são eficazes. Nesta fase, frequentemente, os doentes continuam a ser tratados da mesma maneira como se a sua situação fosse ainda reversível ou são afastados com a justificação de que “não há nada a fazer”, mesmo que o doente continue a ser seguido ou esteja mesmo internado. Esta situação deve-se ao modelo de medicina que se estabeleceu devido ao seu própriodesenvolvimento. De facto, o grande desenvolvimento que a medicina conheceu no séculoXX, sobretudo na segunda metade, permitiu que finalmente se pudesse modificar eficazmente o desenvolvimento natural de muitas doenças, curar algumas e evitaro aparecimento de doenças infecciosas que no passado constituíram flagelos da humanidade. A varíola foi mesmo erradicada. No entanto, este desenvolvimento levou à situação actual em que o treino dos médicos se focou exclusivamente na cura ou no prolongamento da vida, pelo que quando tal não é possível ficam desarmados e têm dificuldade em responder aos problemas dos doentes.
O reconhecimento da situação atrás descrita deu origem ao chamado movimento dos hospícios - Cicely Saunders fundou o St. Christopher’s Hospice em Londres em 1967. Esta é a data geralmente reconhecida como a que marca o início dos cuidados paliativos.
introdução

24 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
No entanto, Geoffrey Hanks revelou recentemente que já existia um serviço no Royal Marsden, o Continuity Care Service fundado em 1964, com a finalidade de tratar os doentes oncológicos com doença avançada incurável [2]. Considerava-se que, apesar de não haver possibilidade de deter a doença, a medicina possuía recursos que, se usados adequadamente, podiam responder aos problemas destes doentes. Balfour Mount abriu o seu Serviço de Cuidados Paliativos em 1975 no Royal Victoria Hospital de Montreal, empregando pela primeira vez a designação cuidados paliativos, que a partir daí se generalizou [3].
Mais tarde, em 1990, a Organização Mundial de Saúde (OMS) num documento intitulado Cancer Pain Relief and Palliative Care reconheceu a importância dos cuidados paliativos e considerou o tratamento da dor e de outros sintomas como uma das suas prioridades na luta contra o cancro, a par da prevenção primária, do diagnóstico precoce e do tratamento curativo [4]. Nesse importante documento, a OMS afirmava que “durantemuito tempo ainda os cuidados paliativos serão a única solução, ao mesmo tempo humana e realista, para numerosos doentes, e nada é mais importante, para a qualidade de vida desses doentes, que a difusão e a aplicação dos conhecimentos já disponíveis sobre o tratamento da dor e dos outros sintomas”. Os cuidados paliativos são consideradosao mesmo nível dos outros meios de intervenção e não inferiores ou secundários.
Em 2002 a OMS referiu-se aos cuidados paliativos do seguinte modo [5]: “Os cuidados paliativos melhoram a qualidade de vida dos doentes e das suas famílias que encaram uma doença ameaçadora da vida, proporcionando alívio da dor e de outros sintomas, suporte espiritual e psicossocial desde o diagnóstico até ao fim da vida e no luto”.
Os cuidados paliativos:
Proporcionam o alívio da dor e de outros sintomas perturbadores;Afirmam a vida e vêem a morte como um processo normal;Não pretendem apressar ou adiar a morte;Integram os aspectos psicológicos e espirituais nos cuidados aos doentes;Oferecem um sistema de suporte para ajudar os doentes a viver tão activamente quanto possível até à morte;Oferecem um sistema de suporte para ajudar as famílias a lidar com a doença e o luto;
·
·
·
·
·
·

| 25 25Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Usam uma estratégia de equipa para abordar as necessidades dos doentes e das suas famílias, incluindo aconselhamento no luto, se indicado;Melhoram a qualidade de vida e possivelmente também influenciam positivamente o curso das doenças;São aplicáveis cedo no decurso das doenças, em conjunção com outras terapêuticas que pretendem prolongar a vida, tais como a quimioterapia ou a radioterapia, e incluem as investigações necessárias para melhor compreender e tratar complicações clínicas perturbadoras.
·
·
·
Assim a OMS considera que os cuidados paliativos não se devem limitar ao fim da vida, mas considera que deveriam estar disponíveis desde o diagnóstico. A ideia fundamental é a de que os cuidados paliativos ajudem as pessoas a viver o mais activamente possível e não que se concentrem apenas no que rodeia a morte. A ideia é proporcionar uma vida digna e não apenas uma morte digna, aspecto em que outros movimentos se concentram, como os que defendem as formas de morte assistida, as quais, como afirma a OMS não se incluem na prática dos cuidados paliativos.
A realidade é, porém, bem diferente porque o que se verifica na prática é que os doentes são muitas vezes referenciados muito tarde para cuidados paliativos [6]. Há mesmo uma tendência, pelo menos em alguns países, para tratar cada vez mais agressivamente os doentes oncológicos [7]. No entanto, um artigo recente que comparou o tratamento padrão do cancro do pulmão de não-pequenas células com o tratamento padrão mais a intervenção precoce dos cuidados paliativos revelou que os doentes em quem houve intervenção precoce dos cuidados paliativos tiveram uma melhor qualidade de vida, viveram mais tempo e foram submetidos a tratamentos menos agressivos [8].
Os cuidados paliativos começaram por causa dos doentes oncológicos, mas hoje considera-se que devem ser prestados independentemente da doença crónica subjacente. A realidade mostra, no entanto, que os doentes oncológicos continuam a ser os mais referenciados para cuidados paliativos, como acontece no nosso serviço em que mais de 95% dos doentes são oncológicos. Estes dados são semelhantes aos referentes a outros países. Por exemplo, num estudo realizado na Alemanha verificou-se que 96,5% dos 4182 doentes admitidos em unidades de cuidados paliativos eram doentes oncológicos [9]. Os não oncológicos eram 147 (3,5%) e a sua distribuição por doença pode ver-se

26 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
no quadro 1. Isto acontece por uma variedade de razões das quais se destacam a maiorfacilidade em estabelecer o prognóstico nos doentes oncológicos e a conotação negativa que o cancro tem relativamente a outras doenças igualmente, ou mais, letais.
Sistema Nervoso
Doença do neurónio motorAcidente vascular cerebralDemênciaEsclerose múltiplaOutras
Doenças Cardiovasculares
Insuficiência cardíaca crónicaDoença arterial oclusivaEnfarte do miocárdioOutras
Doenças Pulmonares
PneumoniaDoença pulmonar obstrutiva crónicaOutras
Sistema Musculoesquelético
OsteoporoseEspinalOutras
Sistema Urogenital
Insuficiência renalOutras
Sistema HematopoiéticoDoenças HepáticasSistema DigestivoOutras
44 29,9%
20,4%
8,8%
8,2%
6,8%
6,1%
4,1%
4,1%
11,6%
12106410
30
121044
13
544
12
1234
10
82
9
6
6
17
Quadro 1 | Distribuição das doenças não oncológicas [9].
Doença n %
| 27 27Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Em Portugal os cuidados paliativos começaram quase 30 anos mais tarde, em 1994, no Centro do Porto do Instituto Português de Oncologia (IPO - Porto) por iniciativada Liga Portuguesa contra o Cancro. Tivemos a honra de ser o responsável pela direcção desse serviço. Desde então apareceram outros serviços de cuidados paliativos em Portugal mas o seu número é ainda muito insuficiente para as necessidades do país. A recentemente criada Rede Nacional de Cuidados Continuados Integrados prevê o desenvolvimento dos cuidados paliativos em todo o país.
Neste capítulo, descreve-se seguidamente o desenvolvimento da primeira unidade de cuidados paliativos portuguesa através de um artigo intitulado A Portuguese Palliative Care Unit. Na última parte deste capítulo referir-nos-emos aos objectivos desta tese e ao modo como esta se vai desenvolver.

28 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 29 29Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
a portuguese palliative care unit
josé antónio s. ferraz gonçalves
Support Care Cancer (2000); 9:4-7

30 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 31 31Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
10
Support Care Cancer (2000) 9 :4–7DOI 10.1007/s005200000211 SUPPORTIVE CARE INTERNATIONAL
José António S. Ferraz Gonçalves A Portuguese palliative care unit
Published online: 28 October 2000Q Springer-Verlag 2000
J.A.S. Ferraz Gonçalves (Y)Instituto Portugues de Oncologia,Unidade de Cuidados Continuados,R. Dr. António Bernardino de Almeida,4200-072 Porto, PortugalE-mail: ferrazg6ipoporto.min-saude.pt orferrazg6mail.telepac.ptPhone: c351-2-5073940Fax: c351-2-5506833
Abstract The background to thedevelopment of the first Portu-guese palliative care unit isdescribed. The activities of thispioneer unit in Porto, whichinclude patient assistance, teachingand research, are reported, and thepaper closes with some generalthoughts on the possible ways ofproviding a more rapid response tothe suffering of patients with far
advanced chronic diseases in anenvironment where palliative careis not yet well developed.
Keywords Palliative care 7Portugal
Introduction
Palliative care has its source in the recognition of aproblem: the inadequate treatment of patients withadvanced chronic diseases. This treatment can be inad-equate by excess or default, that is, failure to recognizethe situation and consequent continuation with aggres-sive treatments as if the problem were a reversible one,or abandonment of the patient without support. Suchabandonment occurs not only when patients are senthome, but often in the hospital too. In this situation thepatients can be labelled as terminal and not followedup with the same interest as others: their needs may notbe really considered, and the medications and care theydo receive are often quite irrelevant to their condi-tion.
The start of palliative care is usually dated from thefoundation of St. Christopher’s Hospice in 1967 byCecily Saunders. In this way the hospice movement wasinitiated. The term ‘palliative care’ was used officiallyfor the first time in 1975, when Balfour Mount openedthe Palliative Care Service in the Royal VictoriaHospital in Montreal [1]. In 1990, the World HealthOrganization published one of its best-known docu-ments “Treatment of cancer pain and palliative care”[2], in which the importance of palliative care was
recognized. In this document, the WHO stated thatpalliative care was a priority in the fight against cancer,on the same level as prevention, screening and curativetreatment, and the only solution that was both humaneand realistic for many cancer patients. Palliative medi-cine is now a recognized specialty and is a subject inuniversity medical school curricula in the UnitedKingdom and a few other countries.
Since its beginnings, palliative care has spreadquickly through the world, mainly, like everything else,in the more highly developed countries. In Portugal,palliative care is still taking its first steps. It is the veryfirst of these that is described here.
The beginning
The North Section of the Portuguese League AgainstCancer recognized the cancer patients’ situationdescribed above and decided to build a palliative careunit to be called Unidade de Cuidados Continuados,which would work closely with the Porto Section of thePortuguese Institute of Oncology. At a certain point inthe course of the project I was invited to be the medicaldirector of the unit. I was a specialist in internal medi-cine and oncology and I accepted the position on one
10
Support Care Cancer (2000) 9 :4–7DOI 10.1007/s005200000211 SUPPORTIVE CARE INTERNATIONAL
José António S. Ferraz Gonçalves A Portuguese palliative care unit
Published online: 28 October 2000Q Springer-Verlag 2000
J.A.S. Ferraz Gonçalves (Y)Instituto Portugues de Oncologia,Unidade de Cuidados Continuados,R. Dr. António Bernardino de Almeida,4200-072 Porto, PortugalE-mail: ferrazg6ipoporto.min-saude.pt orferrazg6mail.telepac.ptPhone: c351-2-5073940Fax: c351-2-5506833
Abstract The background to thedevelopment of the first Portu-guese palliative care unit isdescribed. The activities of thispioneer unit in Porto, whichinclude patient assistance, teachingand research, are reported, and thepaper closes with some generalthoughts on the possible ways ofproviding a more rapid response tothe suffering of patients with far
advanced chronic diseases in anenvironment where palliative careis not yet well developed.
Keywords Palliative care 7Portugal
Introduction
Palliative care has its source in the recognition of aproblem: the inadequate treatment of patients withadvanced chronic diseases. This treatment can be inad-equate by excess or default, that is, failure to recognizethe situation and consequent continuation with aggres-sive treatments as if the problem were a reversible one,or abandonment of the patient without support. Suchabandonment occurs not only when patients are senthome, but often in the hospital too. In this situation thepatients can be labelled as terminal and not followedup with the same interest as others: their needs may notbe really considered, and the medications and care theydo receive are often quite irrelevant to their condi-tion.
The start of palliative care is usually dated from thefoundation of St. Christopher’s Hospice in 1967 byCecily Saunders. In this way the hospice movement wasinitiated. The term ‘palliative care’ was used officiallyfor the first time in 1975, when Balfour Mount openedthe Palliative Care Service in the Royal VictoriaHospital in Montreal [1]. In 1990, the World HealthOrganization published one of its best-known docu-ments “Treatment of cancer pain and palliative care”[2], in which the importance of palliative care was
recognized. In this document, the WHO stated thatpalliative care was a priority in the fight against cancer,on the same level as prevention, screening and curativetreatment, and the only solution that was both humaneand realistic for many cancer patients. Palliative medi-cine is now a recognized specialty and is a subject inuniversity medical school curricula in the UnitedKingdom and a few other countries.
Since its beginnings, palliative care has spreadquickly through the world, mainly, like everything else,in the more highly developed countries. In Portugal,palliative care is still taking its first steps. It is the veryfirst of these that is described here.
The beginning
The North Section of the Portuguese League AgainstCancer recognized the cancer patients’ situationdescribed above and decided to build a palliative careunit to be called Unidade de Cuidados Continuados,which would work closely with the Porto Section of thePortuguese Institute of Oncology. At a certain point inthe course of the project I was invited to be the medicaldirector of the unit. I was a specialist in internal medi-cine and oncology and I accepted the position on one

32 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
11
5
condition: that I should be allowed to take training inpalliative care, which at that time was only possible inunits outside Portugal.
Over the course of 7 months I visited several Euro-pean units: St. Christopher’s Hospice and St. HelenaHospice in England; Intituto Nazionale dei Tumori inMilan; La Foundation Rive-Neuve and the AubonneHospital in Switzerland; and Gregorio MaranónHospital in Madrid. I believe this was very useful and,in my case, the best approach, because the diversity Isaw showed me different realities, different experi-ences, and different styles of palliative care. Iconcluded that palliative care can be applied in manydifferent conditions, always with the same philosophyand the same principles behind it while the practice isadapted to the local circumstances, and that what isobserved in any palliative care service should be takenas an example of what can be done, rather than a modelto be copied.
The first unit
Because I finished my training period before the unitwas ready, we were allowed to start working with 5beds belonging to the Radiotherapy Service, which hada total of 25 beds. The staff in that service included thenurses who were keen to work in the future palliativeunit, some of whom had had some experience of pallia-tive care in units abroad. Our first patient was admittedon 17 October 1994. This, then, was the day whenpalliative care started in Portugal.
All the personnel, except the chief nurse and myself,were shared between the two services. We starteddoing inpatient care, outpatient care, and consultationin other services within the hospital.
There were various difficulties with this experience:I Problems arising from the physical/architectural set-
up, which did not make it easy for family members tostay with patients, especially at night
I Too few beds for hospital needsI Different treatment of patients in the same serviceI Difficulty in the implementation of specific routines
Other types of problems experienced at this stagewere:I Problems relating to misunderstanding of the
purpose of the new serviceI Referral mainly of patients expected to survive for
only a few daysI Frequent use of the unit as a kind of wastebasket,
that is, not with the idea of sending patients to aplace where they could be more adequately treatedbut to get a bed freeThese early days did also have positive aspects:
I The possibility of offering palliative care at all for thefirst time
Table 2 Evolution of the assistance to patients activity
1995 1996 1997 1998 1999
Inpatient admissions 68 100 221 359 388Outpatient clinic observations 549 1124 1302Internal consultation visits 361 596 910Telephone consultation 449 813Home care visits 212
Table 1 Staff of unit
Doctors 4 – with 1 assigned exclusively to home careNurses 24Nursing auxiliaries 16Social worker 1Psychologist 1Nutritionist 1Chaplain 1Driver 1Porters 7Volunteers 15
I The opportunity of spreading the principles of pallia-tive care more easily, because there was more directcontact with doctors in the other service
I Training the team in more specific work with only afew patients
I Possibility of contact with the reality of palliativecare, thus allowing selection (self-selection, at thattime) of people who really wanted to go on workingin palliative care
I Economy – because the unit was so small it wascheaper to work together with the other service,which made it possible to maintain adequate contin-uous staffing levels of professionals who needed tobe represented at all times, mainly nurses, withouthaving too many professionals relative to the numberof patientsWe can conclude that this experience was useful,
and perhaps it could be viewed as an example for othercentres where only a small unit can be implemented.
The new unit
Finally, the new unit opened on 25 May 1996. We grewstep by step as more people were involved in the team(Table 1). Initially, we maintained the same activities,adding to them as circumstances allowed (Table 2).
Now we have 20 beds, all in single rooms, whichallows a member of any patient’s family or a friend tostay at any time.
The unit has had a day centre since 1997: about 20patients can attend for up to 3 days each week, andthey can enjoy many activities.

| 33 33Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
12
6
Since 1998 we have offered telephone consultationsfor the patients being followed by the unit. Thepatients, their families, or their friends may contact theunit when a problem or a doubt arises, to discuss anadjustment to a medication, or to inform the doctor ofthe effect of a prescription, for example, 24 hours a day.It is usually possible for them to talk with the physicianbetween 09*E00 and 16*E00 o’clock, and with a nurseat other times.
In 1999 we started home care. We intend to makethis service one of the most important elements of theunit, so that patients can stay at home where their fami-lies and their own belongings are, that is to say wheretheir lives are centred. However, the traditionalextended family with three generations under one roofproviding support for all members of the family in diffi-cult times is changing. Families are becoming smallerand smaller; most people work outside the home,mainly in the bigger cities, and there will thereforeprobably be more and more difficulties in keepingpatients at home, as has already happened in otherEuropean countries.
Teaching
As this is a pioneer unit in Portugal and in view of itssize, it was planned that it should be a teaching centre.As professionals working exclusively in palliative care,we have an obligation to contribute to the spread ofknowledge in this field. However, the best thing we cando is to go beyond teaching what can be read in booksand reviews and also, most importantly, share ourexperience. This is why we did not start the multidisci-plinary courses until we had completed 3 years of workas a palliative care team.
Our first multidisciplinary course was in October1997. Since then, we have held four each year. Eachcourse is held for 12 professionals: 6 doctors and 6nurses. This small number allows contact with theeveryday life of the unit and with the patients. Eachcourse involves 35 hours from Monday to Friday in1 week. Up to August 2000, 144 professionals from allover the country, even from the islands of Madeira andthe Azores, had undergone training in 12 courses. Wealways have many more candidates than we can admitto the courses, which shows the interest people have inpalliative care and how much they feel the need oftraining in this special field. To help staff who work inour oncological centre but had not been able to get aplace on any of the multidisciplinary courses we held atheoretical course in 2000, which was attended by 35professionals.
In 2000 we held the first continuing education coursefor doctors and nurses who had already completed themultidisciplinary course. And in the future we intend to
hold update courses to maintain interest in palliativecare and ensure that the knowledge applied is current.
Since the beginning of our activities, members of theunit’s staff have participated in many courses,congresses, and other scientific meetings organized byothers. And, finally, I teach the palliative care portionof the course for the master’s degree in bioethics at theMedical School of Oporto University.
Apart from the courses, many doctors, nurses, socialworkers, psychologists, and priests spend variousperiods of time in the unit.
Research
Again, the position this unit occupies in palliative carein Portugal should make research one of its mostimportant activities, on a level with patient assistanceand teaching. These two activities should support andbe supported continuously by research. However,research takes time to produce results, so that we arenot in a hurry to publish research papers, though weare publishing some review papers in Portuguese.However, we have presented some work at congressesof the European Association for Palliative Care and atother congresses, and we intend to start publishing ourresults soon.
The future
The unit is still evolving: in the future there will bemore than 20 beds, and the home care service will bedeveloped and will reach more patients. Teaching ofpalliative care will remain important, and it is probablethat this unit will continue as the main palliative careteaching centre in Portugal. Faculty members of theOporto Medical Schools have been contacted about theidea of introducing undergraduate palliative careteaching into their curricula, but I have not yet receivedany answers – this would be a very important step.Research will take up the desired place.
The immediate problem is finding people interestedin working exclusively in palliative care. Unlike otherEuropean countries, Portugal does not have an excessof doctors and nurses, so that recruitment of profes-sionals to the unit will not be easy.
Other remarks
Since the opening of the unit, almost 6 years ago, pallia-tive care has not evolved much further in Portugal.There are a few other experiences, but the overallpicture is very poor. The implementation of palliativecare has been difficult in most countries, and in

34 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
13
7
Portugal it will not be any different. Many still seepalliative care not as a resource with its own knowledgeand skills, but as what is offered in places wherenursing and psychological and religious support are themost important aspects whilst the medical input has asecondary, and not especially skilled, role. Somemedical oncologists, for example, claim that theyshould take care of their patients until their death,forgetting that the reality is different in most cases andthat the care patients need when curative treatment isno longer useful must be learned, and is often not whatthey are providing. However, not all patients need tobe treated by palliative care specialists. As in otherspecialties, many patients can be treated by their ownphysicians with some training, but there are difficultsituations that require specialized resources of differenttypes. In addition, research and teaching should becarried out, and usually only specialists have the knowl-edge, the experience, the readiness, and a sufficientlylarge number of patients for this.
Palliative care is now needed in Portugal and mustbe developed. However, I suspect, unfortunately, that it
will be a long time before a serious effort is made to dothis. Nonetheless, something must be done quickly.Palliative care can be provided in many differentcircumstances. Palliative care units are indispensable, inmy view, but home care and inpatient support teamsare examples of other options that would be easier toimplement. In my opinion, it is more important to dosomething useful immediately for patients withadvanced chronic diseases who are suffering unneces-sarily than to wait for conditions that anyone mightimagine to be ideal. When we started, for example,conditions were not ideal, because the unit was not yetready. So, professionals and hospital staff memberswith an interest in this field should start however localconditions allow and then improve their situation at therate that is possible, but without ever forgetting thetraining needed. I also believe that doctors have aspecial responsibility, because if they know and applythe principles and skills of palliative care, even alone,they can have a very important impact on the well-being of their patients with chronic advanced diseases.
References
1. Saunders C (1998) Foreword. In:Doyle D, Hanks GWC, MacDonald N(eds) Oxford Medical Publications,Oxford, pp v–ix
2. World Health Organization (1990)Traitement de la douleur cancéreuse etsoins palliatifs. (Série de rapports tech-niques 804) WHO, Geneva

| 35 35Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
A maioria dos doentes com doenças crónicas avançadas tem múltiplos problemas resultantes da sua doença e por vezes também dos tratamentos anteriormente efectuados. Acresce que os doentes admitidos em cuidados paliativos apresentam-se em situações muito diversas a nível do estado de consciência, da função cognitiva, do estado emocional, da funcionalidade, etc. Os doentes podem estar muito débeis, receosos ou ansiosos. Há também o problema do trabalho que uma equipa muito ocupada tem de fazer e do tempo que tem disponível para cada doente. Por isso, uma avaliação extensa pode ser impossível e pode constituir um fardo para os doentes. Contudo, para ajudar convenientemente os doentes, é necessário identificar e avaliar rigorosamente os seus problemas principais. Mais tarde, outros problemas de mais baixa prioridade poderão ser abordados se for apropriado.
Para resolver os problemas dos doentes é necessário, em primeiro lugar, reconhecê-los.Existem várias escalas para avaliação de múltiplos sintomas e outras desenhadas para avaliar um sintoma isolado como a dor [10] e a fadiga [11], por exemplo. A extensãoe os problemas englobados nessas escalas é variável, embora inevitavelmente tenhampontos comuns, nomeadamente no que se refere aos sintomas físicos mais comuns como dor, dispneia, náuseas, etc. Outro tipo de escalas também com pontos comuns com as anteriores são as que se destinam a avaliar a qualidade de vida, como a EORTC QLQ-C15-PAL [12].
O objectivo desta tese não é acrescentar uma nova escala às já existentes, embora também seja necessário desenvolver métodos de avaliação que estejam de acordo com
objectivos do desenvolvimento do sistema integrado para a avaliação inicial dos doentes oncológicos admitidos em cuidados paliativos
36 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
o objectivo do trabalho. Este consiste no desenvolvimento de um sistema para avaliaçãodos principais problemas dos doentes, nas suas várias dimensões que se adapte às circunstâncias dos doentes.
O sistema deve conter instrumentos que possam avaliar os problemas mais importantes dos doentes com descritores verbais fáceis de compreender por todos os doentes sem alterações da função cognitiva. Por exemplo, o termo dispneia, incompreensível para a maioria das pessoas, deve ser substituído por falta de ar. A extensão é também importante porque pode tornar a avaliação difícil ou cansativa para os doentes mais debilitados ou fastidioso para os que não tenham na altura muitos problemas. A limitação da extensão é um dos objectivos que justifica o desenvolvimento deste sistema.
Há ainda o problema da avaliação dos doentes com alterações cognitivas que impeçama comunicação eficaz. Este aspecto é particularmente difícil, devido à natureza subjectiva dos sintomas/problemas. No entanto, também estes doentes têm de ser avaliados rigorosamente embora de modo diferente. Para isso é necessário desenvolvermétodos de avaliação específicos, adaptados à sua situação. Esta é uma área de intervenção particularmente difícil.
Para avaliar o estado cognitivo há que desenvolver ou utilizar instrumentos já validados que se adeqúem aos objectivos do sistema. Esse estado pode ser óbvio, mas por vezes não é, pelo que as alterações cognitivas podem passar despercebidas ou consideradas erradamente. Nos doentes com um estado de consciência obviamente normal não é necessário rastrear o seu nível de consciência, mas quando não é assim é necessário avaliar esse nível. Também nos doentes que têm alterações cognitivas óbvias, com agitação ou desorientação manifesta, não é necessário fazer qualquer rastreio, mas quando não é assim há que fazê-lo.
A comunicação é um aspecto fundamental nos cuidados de saúde e em cuidados paliativos este aspecto é particularmente valorizado. A comunicação é um processocontínuo, mas sobretudo nas fases de transição como a da admissão em cuidados paliativos, tem uma importância particular porque a informação que os doentes e os familiares receberam anteriormente é com frequência insuficiente ou mesmo errada sobre a finalidade desta nova fase do seu tratamento. É natural também que os doentes e os familiares desejem ser esclarecidos quanto ao que os espera.
| 37 37Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Os cuidados paliativos envolvem os familiares que são afectados pelo sofrimento do seu doente, pelo que também são objecto de avaliação e atenção. No entanto, esse aspecto não será integrado neste sistema que incidirá exclusivamente sobre a avaliação dos doentes.
De acordo com o que anteriormente foi dito, o sistema que nos propomos construir desenvolver-se-á em 5 capítulos, para além deste capítulo introdutório. No segundo capítulo, da comunicação, procuraremos demonstrar a necessidade e o desejo de informação que a maioria dos doentes sentem e a dificuldade com muitas vezes se deparam, através de dois estudos levados a cabo no IPO - Porto nos últimos anos e já publicados. Procura-se mostrar a necessidade de adequar a informação aos desejos dos doentes e não usar princípios rígidos, procurando seguir a vontade e o ritmo destes. Depois, no terceiro capítulo descreve-se o processo de avaliação da consciência tanto ao nível da vigília como do conteúdo. Para avaliar o nível de vigília desenvolveu-se uma escala, entretanto já publicada. Para avaliar a função cognitiva nos doentes com um nível de vigília que permita interacção, introduziu-se um instrumento já em uso na Unidadede Cuidados Paliativos do IPO - Porto, que foi recentemente validado em cuidados paliativos e em português. Depois de definido se o doente tem capacidade para ser avaliado será usado o instrumento descrito no capítulo 4 que foi desenvolvido segundoo método de Delfos, com o envolvimento de peritos internacionais. Para os doentes que não podem ser avaliados directamente por alterações cognitivas foram estudados dois métodos que se descrevem no capítulo 5. Finalmente no capítulo 6 integram-se as diferentes partes do sistema, procurando dar-se uma visão de conjunto e coerência interna a esta ferramenta. Procede-se ainda a uma reflexão sobre a importância que este sistema pode ter na melhoria da qualidade assistencial em cuidados paliativos.

38 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
http://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&indOcorrCod=0001675&selTab=tab2 (acedido em 08/06/2009).
Geoffrey H. Palliative care: careless use of language undermines our identity. Palliat Med 2008; 22:109-110.
Ferraz Gonçalves. Cuidados Paliativos em Oncologia. Arquivos de Medicina 1998; 12 (3):170-173.
WHO expert committee report. Cancer pain relief and palliative care. World Health Organization. Geneva 1990.
http://www.who.int/cancer/palliative/en/.(acedido em 28/05/2009).
Ferraz Gonçalves, Goyanes C. Use of chemotherapy at the end of life in a Portuguese oncology center. Support Care Cancer 2008;16:321–327.
Earle CC, Neville BA, Landrum MB, Ayanian JZ, Block SD, Weeks JC. Trends in the aggressiveness of cancer care near the end of life. J Clin Oncol 2004;22:315–321.
1
2
3
4
5
6
7
referências
Temel JS, Greer JA, Muzikansky A, et al. Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer. N Engl J Med 2010;363:733-742.
Ostgathe C, Alt-Epping B, Golla H, et al. Non-cancer patients in specialized palliative care in Germany: what are the problems? Palliat Med 2010;25:148-152.
Caraceni A, Cherny N, Fainsinger R, Kaasa S, Poulain P, Radbruch L, De Conno F, and the Steering Committeeof the EAPC Research Network. Pain Measurement Tools and Methods in Clinical Research in Palliative Care: Recommendations of an Expert Working Group of the European Association of Palliative Care. J Pain Symptom Manage 2002;23:239–255.
Radbruch L, Strasser F, Elsner F, Ferraz Gonçalves, Løge , Kaasa, Nauck, Stone P, the Research SteeringCommittee of the European Association for Palliative Care (EAPC). Fatigue in palliative care patients - an EAPC approach. Palliat Med 2008; 22: 13–32.
Groenvold M, Petersen MA, Agronson NK, et al. The de-velopment of the EORTC QLQ-C15-PAL. Eur J Cancer2006;42:55-64.
8
9
10
11
12
| 39 39Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
2COMUNICAÇÃO

40 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 41 41Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
A comunicação é um aspecto fundamental nas relações humanas. Na relação dos doentes com os profissionais de saúde a comunicação reveste-se de grande importância e nos cuidados paliativos é-lhe dada tradicionalmente uma particular relevância.
Demonstrou-se que a qualidade da comunicação tem um efeito positivo no bem-estar emocional e físico dos doentes. A boa comunicação associa-se à melhoria da satisfação e ao ajustamento psicológico dos doentes. Para os doentes e suas famílias a comunicação é uma componente vital da qualidade dos cuidados de fim de vida [1]. Contudo, as atitudes relacionadas com a informação prestada aos doentes diferem muito de país para país e tem variado ao longo do tempo. Por exemplo, nos Estados Unidos da América e nos países do Norte da Europa a informação sobre vários aspectos da doença é habitual, enquanto nos países do sul da Europa, nomeadamente em Portugal, a situação parece ser diferente. Invocam-se geralmente questões culturais para explicaressas diferenças e elas existem certamente. Mas há que dizer que a situação não é estática pois tem-se verificado uma evolução no sentido de dar maior informação aos doentes [3]. O maior acesso à informação, a melhoria da literacia e o maior envolvimento em ensaios clínicos farão, certamente, com que os doentes venham a possuir e a exigir maior informação sobre a sua situação.
Na fase de transição para cuidados paliativos há certamente muitas dúvidas e a consequente ansiedade associada. A transição para cuidados paliativos reveste-se de particular dramatismo pelo seu significado. Porque embora os cuidados paliativos possam e devam ser integrados no tratamento dos doentes juntamente com as técnicas curativas, na maioria dos casos ainda significam que a possibilidade de modificar a
comunicação/informação
42 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
evolução da doença está esgotada. Este facto, tem naturalmente um grande impacto psicológico nos doentes que deve ser explorado.
Embora haja a impressão de que em Portugal a informação prestada aos doentes é deficiente, é necessário conhecer o que realmente se passa e quais são as preferências dos doentes quanto a este aspecto. É da investigação por nós realizada nesta área que se dá conta neste capítulo, introduzindo dois artigos já publicados: Diagnosis disclosure in a Portuguese oncological centre - estudo sobre a prática dos oncologistas de um centrooncológico quanto à informação que prestam aos doentes sobre o seu diagnóstico; e Breaking bad news: experiences and preferences of advanced cancer patients at a Portuguese oncology centre - estudo sobre o ponto de vista dos doentes com cancro avançado sobre a informação que receberam. O capítulo termina com uma breve sínteses dos 2 artigos.

| 43 43Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
diagnosis disclosure in a portuguese oncological centre
j. ferraz gonçalves, s. castro
Palliative Medicine (2001); 15:35-41

44 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 45 45Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
21
Diagnosis disclosure in a Portuguese oncologicalcentreJ Ferraz Gonçalves Director and S Castro Psychologist, Unidade de Cuidados Continuados, InstitutoPortuguês de Oncologia, Porto
Abstract: The disclosure of a diagnosis of cancer to patients is a controversial matter.There have been major differences in practice concerning this issue through time andbetween cultures. A questionnaire was sent to the doctors of the Oporto Centre of thePortuguese Institute of Oncology in order to assess their attitudes. We received 45 responses (40%) from the 113 questionnaires sent. Of these, 32 (71%) said thatthey disclose the diagnosis as a general policy or at the patients’ request, and 13 (29%)disclose it rarely or not at all. The most frequent reason indicated by these 13 physicianswas that the disclosure might damage the patients psychologically. Forty-four (98%)doctors inform the family of the diagnosis. Thirty-nine (87%) think that patients aresatisfied with the information provided. This study was carried out in one oncologicalcentre only, so it is inappropriate to conclude that this is what happens throughoutPortugal. As far as we know, this is the first study in Portugal addressing this area ofpractice. This subject is a very important topic of research both in Portugal and in othercountries, as many published recommendations are not research based.
Key words: breaking bad news; communication; diagnosis disclosure; physician–patientrelation
Resumo: A revelação do diagnóstico aos doentes com cancro é um assuntocontroverso. Tem havido grandes diferenças na prática respeitante a esta questão aolongo do tempo e entre as diversas culturas. Enviámos um questionário aos médicosdo Centro do Porto do Instituto Português de Oncologia para avaliar as suas atitudes.Recebemos 45 respostas (40%) dos 113 questionários enviados. Destes, 32 (71%)dizem que revelam o diagnóstico por princípio ou quando os doentes o pedem e 13(29%) revelam-no raramente ou nunca. A razão mais frequentemente indicada por estes13 médicos foi a de que a revelação pode causar dano psicológico aos doentes.Quarenta e quatro (98%) médicos informam a família do diagnóstico. Trinta e nove(87%) pensam que os doentes estão satisfeitos com a informação dada. Este estudofoi feito num único centro oncológico, por isso não podemos dizer que é isto que sepassa, de um modo geral, em Portugal. Tanto quanto sabemos, este é o primeiro estudorealizado em Portugal sobre este aspecto da prática médica. Este é um tópico deinvestigação muito importante tanto em Portugal como noutros países, porque muitasrecomendações práticas publicadas não se baseiam na investigação.
Palavras-chave: dar más notícias; comunicação; revelação do diagnóstico; relaçãomédico–doente
Palliative Medicine 2001; 15: 35–41
© Arnold 2001 0269–2163(01)PM396OA
Address for correspondence: Dr J Ferraz Gonçalves, Unidadede Cuidados Continuados, Instituto Português de Oncologia, R. Dr. António Bernardino de Almeida, 4200-072 Porto,Portugal.
06PM396 9/1/01 3:28 pm Page 35

46 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
22
Introduction
The disclosure of a diagnosis of cancer to patientsis a controversial matter. The dominant attitudeamong physicians has changed over time, and therehave always been voices advocating against it.1 Wewill also find different attitudes when we comparepractice in countries with different cultures. In theUnited States and northern European countries,2–4
for example, the usual practice is to disclose thediagnosis. However, in other countries, includingthose of southern Europe,4–8 the situation is dif-ferent: doctors’ attitudes are more paternalistic, andin many cases they do not disclose the diagnosis.
In Portugal, the current practice seems to be oneof non-disclosure. However, as far as we know, noresearch on this subject has been carried out inPortugal.
Methods
We conducted a survey in the Oporto Centre of thePortuguese Institute of Oncology, which is one ofthe most important Portuguese oncological centres.It has 350 beds and about 4000 new patients areadmitted every year. It has services and equipmentequivalent to those of any major European oncolo-gical centre, including a palliative care unit. Thiscentre is a public hospital that serves the populationfrom the whole of northern Portugal. The patientsbelong to all social classes and education levels.
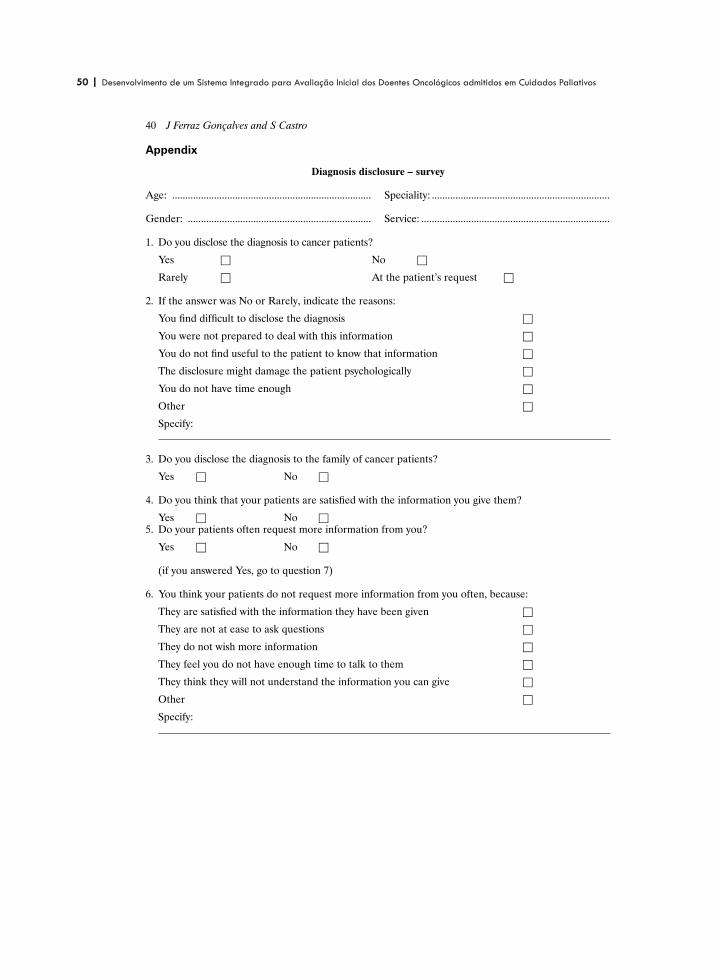
A questionnaire (see the Appendix), specificallydesigned for this study but not subjected to a pilottest, was sent to each doctor at the centre whotreated adult patients. Those with other functions,such as radiologists and pathologists, were exclu-ded. This study was approved by the Ethics Com-
mittee of the Portuguese Institute of Oncology –Oporto Centre.
Results
The questionnaire was sent to 113 doctors, and45 responses (40%) were obtained. In Table 1 weshow the specialities and demographic data of thedoctors who returned the questionnaires. There isa similar percentage in all specialities, with the ex-ception of radiotherapy (Table 1). Nineteen (42%)participants added comments, clarifying their viewsor adding other hypotheses to those included in thequestionnaire. The questions most commented onwere: the one that asked if doctors disclose thediagnosis of cancer to the patients, and if not, whynot; and the questions about the patients’ andfamilies’ participation in therapeutic decisions.
Among our respondents, 14 (31%) doctors statedthat their policy was to disclose the diagnosis, three(7%) do not do it at all, 10 (22%) rarely do it and18 (40%) disclose it only at the patient’s request(Table 2). A much higher number, 44 (98%),inform the family about the patient’s diagnosis; inone case (2%) the answer was omitted. The mostfrequent reason indicated by the 13 doctors (34%),who rarely or never disclose the diagnosis topatients (Table 3), for so acting was the possibilityof damaging the patients psychologically (11, 85%).The comments added to the questions about thedisclosure to patients and the reasons for not dis-closing the cancer diagnosis, again, show a concernwith the eventual psychological damage that the dis-closure might produce. Some examples of thesecomments can be seen in Table 4.
To the question ‘do your patients often requestmore information from you?’ 29 (64%) answered
36 J Ferraz Gonçalves and S Castro
Table 1 Doctors’ speciality and demographic data
Speciality No. of questionnaires No. of questionnaires Total returned Returned per specialitysent returned (%) (%)
Surgery 52 22 49 42Medical oncology 24 12 27 50Radiotherapy 24 5 11 21Other 13 6 13 46Total 113 45 100
Age: mean 46 years (range: 31–65 years); median 45 years.Sex: male 27 (60%); female 17 (38%); not stated 1 (2%).
06PM396 9/1/01 3:28 pm Page 36

| 47 47Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
23
yes and 16 (36%) answered no. These 16 doctorspresume that their patients are satisfied with theinformation they get, or simply do not wish anymore information at all (Table 5). This agrees withthe answers to question 4, to which 39 (87%) saidthat they think their patients are satisfied with theinformation they give them.
Forty-one doctors (91%) think that patientsshould participate in decisions about treatment andfour (9%) think they should not. The reasons forthese opinions are shown in Tables 6 and 7. Only 25(56%) thought that family members should parti-cipate in making treatment decisions. The fewcomments about the patients’ participation in thera-peutic decisions suggest that they should not parti-cipate or even influence them. It was, however,conceded that if offered two equally effective treat-ments the patient can choose the one that is morebearable for him or her. Similar comments weremade about family participation in these decisions.One respondent stated that the decision belongs todoctors, and that family can be involved to encour-age the patient to accept the recommended treat-ment and to endure its toxicity.
Diagnosis disclosure in a Portuguese oncological centre 37
Table 2 Diagnosis disclosure to the patient
No. (%)
Yes 14 (31)No 3 (7)Rarely 10 (22) At patient’s request 18 (40)
Table 3 Reasons invoked for rare or non-disclosure (13doctors)
Reason Yes No
Difficulties in discussing the diagnosis 0 13Not prepared to deal with the situation 0 13Not useful to the patient 3 10Psychologically deleterious 11 2Not having enough time 2 11Others 4 9
Table 4 Examples of comments to questionnaire questions1 and 2
� The decision to disclose the diagnosis should considerthe psychological, intellectual, cultural and socialconditions of the patient
� It is necessary to inform the patients gradually and withsensitivity and gentleness, without coldness
� After the information has been provided, psychologicalsupport is needed
� Most patients are not prepared to receive theinformation of a malignant disease
� The information must be given when it is useful to thepatient
� The information can cause depression� Never use the word cancer� Patients often ask for information to feel hopeful in their
lives (we understand this statement means that thepatient does not really want the truth but a negativeanswer)
Table 5 Reasons to explain why patients often do not re-quest more information from their doctors (16 doctors)
They are satisfied with the information they havebeen given 7
They are not at ease to ask questions 1They do not wish for more information 5They feel you do not have enough time to talk to them 2They think they will not understand the information
you can give 0
Table 6 Reasons why patients should participate in treat-ment decisions (41 doctors)
To preserve patient autonomy 25To make the adherence to treatment easier 35To protect the doctor from legal problems 19To allow the patient to prepare himself for adverse
effects 30To allow the patient to refuse the treatment
eventually 23Other 4
Table 7 Reasons why patients should not participate intreatment decisions (four doctors)
It is difficult for you to discuss treatment withpatients 1
You think it is not useful to patients 2You do not have enough time to discuss treatment
with the patients 4The discussion might damage the patients
psychologically 1Other 1
06PM396 9/1/01 3:28 pm Page 37

48 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
24
Discussion
This study was carried out in an oncological centre,where informing patients about their diagnoses is aneveryday matter.
We only had a 40% response rate, which is ratherlow although similar to that obtained in at least onevery important paper.2 This must be borne in mindwhen considering our findings. The reason why radio-therapists participated less than other specialists isnot clear.
The percentage of doctors (71%) who disclose thediagnosis of cancer as their general policy or whenrequested by patients is smaller than that found inother studies in which questionnaires were add-ressed to doctors,2–4 even some of those carried outin southern European countries.4 But the practiceof informing the family almost always (98%) is thesame as what usually happens in those countries.5
Doctors’ most frequently indicated the reason forrarely or never disclosing the diagnosis was that itmight damage the patients psychologically. It seemsthat those doctors prefer to protect the patientsfrom possible psychological damage rather than torespect their autonomy. A lack of training in dealingwith requests for information was not suggested asa reason for these responses. Doctors whose expe-rience is not to have frequent requests for informa-tion feel that this happens because the patients aresatisfied with the information they get or becausethey just do not want more information at all.Indeed, 87% think that patients are satisfied withthe information provided and this percentage ishigher than those who inform their patients as ageneral policy or when requested. The commentsalso show a concern for the patients’ protection:‘inform with sensitivity and gentleness’; ‘withoutcoldness’; ‘inform those we think have sufficient psy-chological and intellectual resources’; ‘the need forpsychological support’; ‘the information can causedepression’; ‘never use the word cancer’. Again, adecision not to inform seems to be due not to a lackof training or difficulty in dealing with the situationbut to have its roots in a protective attitude to thepatients, in order not to affect them psychologicallyand may be understood as what they really want. Infact, in a study conducted in Spain,6 with a culturesimilar to that of Portugal, of the 68% of 97 patients
admitted to an oncological service and a palliativecare unit who had not been informed of their diag-nosis, 42% did not want to receive more infor-mation. An alternative explanation of our results is,perhaps an element of denial, because breaking badnews is recognized by most experts as being difficultand causing some degree of discomfort, even forexperienced professionals;9 in Portugal this problemis not addressed in any way, except in some limitededucational activity. It is possible that doctors arehiding their own difficulties in dealing with theseaspects of communication behind a paternalisticattitude. Communication with patients can belearned, but denial can delay or prevent the decisionto act accordingly. However, we must be very care-ful with the interpretation of the results obtainedand avoid preconceptions.
It seems to be a contradiction that 91% of thedoctors think that patients should participate intreatment decisions, because this percentage ishigher than those who inform patients, and withoutinformation about their disease it is not possible forpatients to decide rationally about the treatment.On the other hand, doctors think that family mem-bers, who are almost always informed, should parti-cipate in treatment decisions in a much smallerproportion of cases (56%). The comments aboutthe decisions also have a paternalistic characterwhen they state that patients should not decideabout treatment. However, these comments repre-sent a minority because 91% think that patientsshould participate in those decisions. The family isseen as a possible doctor ally, facilitating the ad-herence to treatment and helping the patient toendure the treatment decided on by the doctor.
The available data show that Portuguese doctors,who work in this oncological centre, disclose thediagnosis to patients less frequently than doctorsfrom other countries, including those of thesouthern Europe, such as Greece. This study wascarried out in one centre only so it is inappropriateto generalize, but the result obtained agrees with,or is even higher than, what we expected was hap-pening in Portugal.
This study reflects the way in which doctors seethemselves, not necessarily what happens, and ismore important, in our point of view, if the infor-mation is tailored to the desire of the individual
38 J Ferraz Gonçalves and S Castro
06PM396 9/1/01 3:28 pm Page 38

| 49 49Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
25
patient. So, it is also very important to know whatPortuguese patients think about medical informa-tion issues, not only disclosure of the diagnosis butalso about the prognosis and their participation intherapeutic decisions. The research on these topicsis very important and is not extensive. Most of themedical literature providing practical advice is notresearch based.10
To explain the differences in attitude betweenthe countries in what concerns cancer diagnosisdisclosure, cultural causes have been indicated.However, perhaps these cannot explain, at leastcompletely, those differences, because if we go backto the 1950s and 1960s we find that in the USA mostdoctors used not to disclose a cancer diagnosis totheir patients, but nowadays almost all do so.2 Thereasons for this change are certainly many: thespread of information in the media about cancertreatment advances (real or not) and the treatmentoptions available in some cases, where the choiceonly depends on patients’ wish (for example, con-servative breast surgery); the spread of informationon patients’ rights and the growing demand forquality of medical services; the patients’ enrolmentin research protocols demanding informed consent;and legal matters that involve the medical pro-fession. These matters are progressively arising inPortugal and other countries, and we believe that,as time goes by, the picture concerning cancer diag-nosis disclosure will be similar to that already pre-sent in the USA and northern European countries.
References
1 Reiser SJ. Words as scalpels: transmitting evidencein the clinical dialogue. Ann Intern Med 1980; 92:837–42.
2 Novack DH, Plumer R, Smith RL, Ochitill H,Morrow GR, Bennett JM. Changes in physicians’attitudes toward telling the cancer patient. J AmMed Assoc 1979; 241: 897–900.
3 Loge JH, Kaasa S, Ekeberg Ø, Falkum E, Hytten K.Attitudes toward informing the cancer patient – asurvey of Norwegian physicians. Eur J Cancer 1996;32A: 1344–48.
4 Thomsen OØ, Wulff HR, Martin A, Singer PA.What do gastroenterologists in Europe tell cancerpatients? Lancet 1993; 341: 473–76.
5 Mystakidou K, Liossi C, Viachos L, Papadimitrou J.Disclosure of diagnostic information to cancerpatients in Greece. Palliat Med 1996; 10: 195–200.
6 Cortés CC, Olarte JMN. Questioning diagnosisdisclosure in terminal cancer patients: a prospectivestudy evaluating patients’ responses. Palliat Med1994; 8: 39–44.
7 Estapé J, Palombo H, Hernández E et al. Cancerdiagnosis disclosure in a Spanish hospital. AnnOncol 1992; 3: 451–54.
8 Surbone A. Truth telling to the patient. J Am MedAssoc 1992; 268: 1661–62.
9 Buckman R. Communication in palliative care: apractical guide. In: Doyle D, Hanks GWC,MacDonald N eds. Oxford textbook of palliativemedicine, 2nd edn. Oxford: Oxford University Press,1998: 47–61.
10 Ptacek JT, Eberhardt RL. Breaking bad news. J AmMed Assoc 1996; 276: 496–502.
Diagnosis disclosure in a Portuguese oncological centre 39
06PM396 9/1/01 3:28 pm Page 39
50 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
26
Appendix
Diagnosis disclosure – survey
Age: ............................................................................ Speciality: ....................................................................
Gender: ...................................................................... Service: ........................................................................
1. Do you disclose the diagnosis to cancer patients?
Yes □ No □
Rarely □ At the patient’s request □
2. If the answer was No or Rarely, indicate the reasons:
You find difficult to disclose the diagnosis □
You were not prepared to deal with this information □
You do not find useful to the patient to know that information □
The disclosure might damage the patient psychologically □
You do not have time enough □
Other □
Specify:
3. Do you disclose the diagnosis to the family of cancer patients?
Yes □ No □
4. Do you think that your patients are satisfied with the information you give them?
Yes □ No □5. Do your patients often request more information from you?
Yes □ No □
(if you answered Yes, go to question 7)
6. You think your patients do not request more information from you often, because:
They are satisfied with the information they have been given □
They are not at ease to ask questions □
They do not wish more information □
They feel you do not have enough time to talk to them □
They think they will not understand the information you can give □
Other □
Specify:
40 J Ferraz Gonçalves and S Castro
06PM396 9/1/01 3:28 pm Page 40

| 51 51Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
27
7. Do you think patients should participate in treatment decisions?
Yes □ No □
If your answer is Yes, indicate the alternative(s):
To preserve the patients’ autonomy □
To make easier the adherence to treatment □
To protect the doctor from legal problems □
To allow the patient to prepare himself to adverse effects □
To allow the patient to refuse the treatment eventually □
Other □
Specify:
If you answered No, indicate the alternative(s):
It is difficult for you to discuss treatment with patients □
You think it is not useful to patients □
You do not have enough time to discuss treatment with the patients □
The discussion might damage the patients psychologically □
Other □
Specify:
8. Do you think that the family should participate in the decisions concerning treatment?
Yes □ No □
Diagnosis disclosure in a Portuguese oncological centre 41
06PM396 9/1/01 3:28 pm Page 41

52 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 53 53Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
breaking bad news: experiences and preferences of advanced cancer patients at a portuguese oncology centre
ferraz gonçalves, ágata marques, sónia rocha, pedro leitão, teresa mesquita, susana moutinho
Palliative Medicine (2005); 19:526-531

54 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 55 55Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Breaking bad news: experiences and preferences ofadvanced cancer patients at a Portuguese oncology centreFerraz Goncalves, Agata Marques, Sonia Rocha, Pedro Leitao, Teresa Mesquita and Susana MoutinhoPalliative Care Unit, Portuguese Institute of Oncology, Oporto
The disclosure of information to patients about diagnosis and prognosis and other aspects
of care is still a matter of debate. We have conducted a study in advanced cancer patients
about their experiences and preferences concerning this issue. A questionnaire was
developed and completed during the first appointment in the outpatient clinic of an
oncology centre’s palliative care unit, before the patient had any contact with the staff of the
unit. The study was conducted on a convenience sample of 47 patients. We found that
34 (72%) of those patients thought they had been informed of their diagnosis, most of them
by the hospital doctor. However, not all stated the diagnosis in a manner clearly showing
that they were aware of the nature of their disease. Most patients were with a family
member when the diagnosis was disclosed, which is what the majority had preferred. Of
the 13 uninformed patients, only one preferred to remain uninformed. Most patients (89%)
participated in decisions concerning treatment, although only 68% thought they should
have participated. Some 39 patients (83%) were informed that they were being referred to
the palliative care unit, but surprisingly only eight had received an explanation of the unit’s
function. We concluded that, although most patients had been informed of their disease,
there remains many problems, the most important of which, in our view, is the difference
between the information provided and the patients’ needs.
A revelacao da informacao sobre o diagnostico o prognostico e outros aspectos dos
cuidados e ainda um assunto em debate. Realizamos um estudo em doentes com cancro
avancado sobre as suas experiencias e preferencias no que diz respeito a este tema. Foi
desenvolvido um questionario que foi aplicado na primeira consulta externa de uma unidade
de cuidados paliativos de um centro oncologico, antes de terem contacto com o pessoal da
unidade. O estudo foi realizado numa amostra de conveniencia de 47 doentes.
Constatamos que 34 (72%) desses doentes pensavam que tinham sido informados do
seu diagnostico, a maioria pelo medico do hospital. Contudo, nem todos nomearam o
diagnostico de um modo que mostrasse claramente que tinham nocao da natureza da
sua doenca. A maioria dos doentes estava com um familiar quando o diagnostico foi
revelado e era assim que a maior parte preferia. Dos 13 doentes nao informados so um
preferia manter-se sem informacao. A maior parte dos doentes (89%) participou nas
decisoes terapeuticas, embora so 68% pensasse que devia ter participado. Trinta e nove
doentes (83%) foram informados de que tinham sido referenciados para a unidade de
cuidados paliativos, mas surpreendentemente so oito tinham tido uma explicacao sobre a
funcao da unidade. Concluımos que embora a maioria dos doentes tenha sido informada da
sua doenca ha ainda muitos problemas, sendo o mais importante, do nosso ponto de vista,
a diferenca entre a informacao prestada e as necessidades dos doentes. Palliative
Medicine 2005; 19: 526�/531
Key words: breaking bad news; cancer patients; cultural issues; information disclosure; palliative
care patients
Address for correspondence: Dr Ferraz Goncalves, Unidade deCuidados Continuados, Instituto Portugues de Oncologia, RuaDr Antonio Bernardino de Almeida, 4200-072 Porto, Portugal.E-mail: [email protected]
Palliative Medicine 2005; 19: 526�/531
# 2005 Edward Arnold (Publishers) Ltd 10.1191/0269216305pm1070oa

56 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Introduction
The information delivered to cancer patients is still a
matter of controversy, with wide cultural differences. In
northern European countries,1,2 and the US,3 most
doctors disclose the diagnosis as standard practice, but
in southern and eastern European countries,2,4,5 the
attitude is more paternalistic and patients are often
‘protected’ from such information. However, even in
those countries where the usual practice is now to
disclose the diagnosis, a few decades ago the attitude
was the opposite.3 This shows that the problem of
information can change with time.There are also differences between countries relative to
patients and families’ preferences for the type of infor-
mation they require. A study in a palliative care setting
comparing attitudes in Spain and Canada,6 concluded
that the majority of Canadian patients preferred to be
clearly informed, while the Spanish patients placed less
value on full disclosure. In the same study, family
members in Canada agreed with the detailed information
to patients, while in Spain 89% of family members
indicated that full disclosure was not important to the
patient.
A few years ago, we conducted a survey of doctors at
the Oporto Centre of the Portuguese Institute of
Oncology concerning the disclosure of diagnoses to
patients.7 In that study, 71% of doctors stated that they
always, or at the patient’s request, disclosed a cancer
diagnosis and most doctors who rarely or never disclosed
did not do so because they thought that the information
could be psychologically deleterious. However, uncer-
tainty can be worse than bad news,8 and some patients
assume that a non-threatening diagnosis would be
disclosed to them and the absence of such a disclosure
is taken to indicate that their condition must be serious.9
Non-disclosure isolates patients as it excludes them from
the discussion of problems that probably concern them
most. On the other hand, there is a minority of patients
who prefer to remain uninformed, and that must be
respected as that is the strategy they have evolved to
maintain hope. For those who lose hope of a cure or
longer life due to the disclosure, hope can be kept alive
through other aspects, such as their physician not
abandoning them, their remaining free from significant
suffering, being with their family and close friends and
having time to settle matters important to them.That survey reflected the view of doctors, which can be
very different to patients’ views. Therefore, the obvious
next step was to ask patients for their opinion concerning
the quantity and quality of information they receive from
health professionals and their preferences. Cultural issues
are relevant factors in the attitudes of doctors, patients
and their families in relation to the disclosure of
information. That is why it is important to add data
from different countries, and that is the reason providing
justification for this study.
Methods
A survey was conducted between January 2002 and June
2003 on a convenience sample of patients referred to the
outpatient clinic of our palliative care unit.10 This is a
palliative care unit included in an oncology centre;
therefore all patients had cancer as their primary
diagnosis. All patients were aged 15 or over, as youngerpatients are treated in the paediatric service.
A questionnaire was specifically designed for this study
to acquire the information considered relevant in an
exploratory survey. The aim of the survey was to obtain
patient preference regarding information and to compare
this with what actually occurs. The broad topics of the
questionnaire included: who should be informed first
when a life threatening disease like cancer is diagnosed;who should and who actually did convey the information;
where the information was and where it should have been
conveyed; who was and who should have been with the
patient; participation in the treatment decision-making
process; information provided on palliative care; and a
request to name the diagnosed disease.
Patients were addressed when they arrived for the first
time at the outpatient clinic, before they had any contactwith the health professionals of the unit. Psychology
students undergoing long-term training in the unit
presented the questionnaire to the patients.
Patients that were very frail, bedridden or suffering
cognitive failure, as assessed by the shortened version of
the Confusion Assessment Method,11 were excluded.
A descriptive study of all variables included in the
study was performed. Chi-square and Fisher’s exact testwere used to compare categorical variables with the
status of informed or not informed patients. Age and
follow-up time at the oncology centre, before admission
to the palliative care unit, were compared between
informed and uninformed patients using the Mann�/
Whitney U -test.
The ethics committee of the hospital approved this
study.
Results
The survey included 47 patients, 21 males (45%) and
26 females (55%); their median age was 66 years (range:
21�/86 years); 39 were married (83%), six single (13%)
and two widowed (4%). The median follow-up time at the
oncology centre before admission to the palliative care
unit was 16 months (range: 2�/195).
Breaking bad news 527

| 57 57Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
All patients preferred the questions to be read aloud by
the psychology students instead of filling the question-
naires in themselves. Thirty-four patients (72%) statedthat they had been informed and 13 (28%) that they had
not been informed of their diagnosis.
Disclosure of the diagnosis
Twenty-six (55%) stated that patients should be the first
person to be informed, whereas 21 (45%) preferred afamily member or a friend. Most patients (41�/87%)
thought that the information should be disclosed by a
doctor and no one chose a nurse or a social worker.
Details regarding what actually occurred and the pre-
ferred options for diagnosis disclosure can be seen in
Table 1. Nineteen patients (56%) stated that they were
surprised with the information, while 15 (44%) suspected
the diagnosis. Most patients (68%) received the informa-tion at the outpatient clinic, only two received it in an
inpatient setting, three at home and one in another place;
the three patients who received the information at home
were among those informed by a family member, as
expected.
Most patients preferred to be with a family member
when the diagnosis was disclosed and this was what
actually occurred, but there were differences between thepreferred option and the actual experience (Table 2).
We did not find any correlation between information
and sex, marital status, age or the follow-up time at the
oncology centre before admission to the palliative care
unit.
Information and participation in treatment decision-
making process
Forty-two patients (89%) were always informed about
treatment and two sometimes; therefore only three (6%)
were never informed. Twenty-nine patients (62%) always
participated in decisions regarding treatment and two
participated sometimes; 15 (32%) never participated indecisions regarding treatment (one piece of data missing).
Only 32 (68%) thought they should participate in those
decisions, 23 (49%) thought that close family members
should participate, and 10 (21%) that only doctors should
take the decisions. Seven patients (15%) refused proposed
treatments.
Effectiveness of the information
For 19 patients (56%), the information was disclosedin an acceptable manner, clearly and sensitively, whereas
15 (44%) found the disclosure poorly carried out.
However, none of the latter commented further on why
they deemed it incorrect.
Only one of 13 uninformed patients preferred to
remain so. This group of patients was not informed
because they were not at ease to ask, the information was
refused, they felt they were tricked, the professionals triednot to answer the questions or the information was
unclear. On the other hand, five of the 34 informed
patients preferred that they had not been informed.
Therefore, only six of the 47 patients did not want to
know (Table 3).
The 34 informed patients stated they had one of the
following: ‘cancer’ �/ 15 (44%); ‘a tumour’ �/ 10 (29%); ‘a
bad disease’ �/ one (3%); ‘other’ �/ seven (21%); ‘do notknow’ �/ one (3%). The 13 uninformed patients stated
they had one of the following: ‘cancer’ �/ two (15%);
‘tumour’ �/ 0; ‘other’ �/ four (31%); ‘do not know’ �/ seven
(54%). If we consider all patients stating ‘cancer’,
‘tumour’ and ‘bad disease’ to be informed and all
patients stating ‘they do not know’ or ‘other’ to be
uninformed then the results for informed patients are as
follows: 26 (76%) are really informed and eight (24%)are not informed, and for uninformed patients: two
(15%) are informed and 11 (85%) are not informed; the
Table 1 Who should communicate information about diag-nosis? Actual experience and preferred options of the 34informed patients
Actual experiencen (%)
Preferred optionn (%)
Family doctor 8 (24) 17 (50)Hospital doctor 19 (56) 10 (29)Any doctor �/ 3 (9)Psychologist 0 (0) 1 (3)Nurse 2 (6) 0 (0)Social worker 0 (0) 0 (0)Family member 4 (12) 0 (0)Other 1 (3) 3 (9)
Table 2 Actual experience and preferred option of the 34informed patients on who should be with them when thediagnosis is disclosed
Actual experiencen (%)*
Preferred optionn (%)
Family member 22 (65) 19 (61)Friend 2 (6) 0 (0)Alone 8 (24) 3 (10)Other professionals 8 (24) 1 (3)Other patients 0 (0) 1 (3)Indifferent �/ 7 (23)
*The sum of the actual experience items does not total 34 (or100%) because some patients were with more than oneperson.
Table 3 Information obtained and patients’ preferences
Patients’ preferences
To be informedn (%)
Not to be informedn (%)
Informed patients (n�/34) 29 (85) 5 (15)Uninformed patients (n�/13) 12 (92) 1 (8)Total (n�/47) 41 (87) 6 (13)
528 F Goncalves et al.

58 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
difference between the two groups was significant
(PB/0.001) (Table 3).
Regarding the referral to palliative care, 39 patients(83%) were informed of the referral, but only eight
(17%) had received an explanation regarding the pallia-
tive care unit.
Discussion
The percentage of patients considering themselves to be
informed (72%) is similar to the percentage of doctors
(71%) that always, or at the patients’ request, disclosed
the diagnosis in a former study carried out at our
hospital.7 This number is higher than that observed ina Spanish study about ten years ago, where only 32%
of the patients with advanced cancer had been
informed of the nature of their disease.12 This is
surprising because Spanish culture is deemed to be
similar in many aspects to Portuguese culture. It seems
unlikely that the ten years separating these two studies
can explain the difference. Moreover, 42% of the
uninformed patients did not want to receive moreinformation,12 which again contrasts with our observa-
tion that only one of the 13 uninformed patients (8%)
clearly preferred to remain uninformed. The reasons
why those patients were not informed were related to
the doctors’ attitude and a lack of proactive effort to
find out the patients’ information needs, which can be
inferred from the manner in which the patients
answered this question. On the other hand, five ofthe informed patients preferred that the information
had not been disclosed. Therefore, only a minority of
the patients did not want to be informed.
Usually patients prefer to be informed by a doctor,
and most prefer the family doctor, probably because
they are more familiar with them, as patients do not
like to be informed by unknown doctors.13 However,
most are informed by a hospital doctor, as demon-strated in this and other studies.14�16 Doctors are, in
fact, the preferred person to convey the informa-
tion.17,18 The study of Yun et al .,17 which explores
the reasons for this preference, showed that the most
important factor is the doctor’s understanding of the
disease and capacity to explain the entire situation;
other reasons included trust placed in the doctor, the
doctor’s awareness of the patient’s emotional, psycho-logical, social and physical situation, and the duty of
doctors to provide information.
Most patients were informed about treatments and
only a minority did not participate in decisions
concerning those treatments. But many patients think
that they should not participate in those decisions and
that only doctors should make such decisions, as
observed in other studies;8,11 although in one study,8
this preference was limited to older patients. The
encouragement to participate in treatment decision-
making can be associated with higher levels of anxiety,
which can persist for at least two weeks.19 In the
previous study of doctors at our hospital,7 91%
thought that patients should participate in the deci-
sions regarding treatment, which was a higher percen-
tage than that recorded for doctors who always, or on
request, informed patients (70%); this seems a contra-
dictory fact given that patients need information to
decide rationally; it appears to be the contrary to the
patients’ wishes as observed herein.
Sometimes doctors are not very effective in informing
patients, as shown by the difference recorded between the
information delivered and the patients’ needs, i.e., there
were patients informed that did not want to be informed
and patients not informed that had wanted to be
informed. These observations are very important because
the issue is not the disclosure of information but
matching it to the will of patients. Also, the surprise
that the diagnosis caused in many patients suggests a lack
of appropriate patient preparation concerning the possi-
bility of a diagnosis of cancer during the period of
diagnostic tests.18 Furthermore, many patients thought
they were poorly informed, without commenting further
on why they thought so. This is an important issue
because a poor or insensitive disclosure of information
may have a negative emotional impact. Patients satisfied
with diagnosis communication reported less emotional
distress than patients who would have preferred differ-
ent.18 There are, however, other aspects, besides the way
the information was disclosed, which are considered of
greater importance, such as emotional support and a
shorter period of time between seeking medical assistance
and the confirmation of cancer.13,17,18 Also important for
patient emotional support is the certainty that the
physician will not abandon the patient and will be
available to answer all questions.13
The communication of a poor prognosis is an even
more difficult task that doctors often avoid. That is
probably the explanation why only a few patients were
aware of why they had been referred to the palliative care
unit, even when they knew their diagnosis and partici-
pated in the treatment decisions. This is not exclusive to
our hospital.19,20 For example, Cassileth et al . found that
more patients receiving curative radiotherapy tended to
provide a correct diagnosis than patients receiving
palliative radiotherapy,20 which was also interpreted by
the authors as being due to the difficulties that doctors
have communicating an adverse prognosis. Although
physicians often state that non-disclosure is a means of
protecting patients, in fact there is a reluctance to give
bad news, especially in the transition from curative or life
prolonging therapy to symptomatic treatment.21 An
Breaking bad news 529

| 59 59Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
alternative or complementary explanation for these
observations is denial amongst patients.22
Conclusion
One important limitation of this study is the small
number of patients, which raises questions about the
external validity of the data and whether the findings can
be extrapolated to Portuguese cancer patients as a whole.
This said, we tentatively conclude that most Portuguese
cancer patients want to be informed of their diagnosis
and want to participate in decisions regarding treatment.
However, there are also some patients who do not want
that, mainly in relation to treatment decision-making.
Most patients wish to be with a family member, but not
with other health professionals. Some patients stated they
had been informed but gave ambiguous answers when
asked to name their disease, which does not necessarily
mean that they were wrong but casts doubt on the correct
nature of their information.
Communicating with cancer patients and, in particu-
lar, breaking bad news is a very important aspect of the
patient�/doctor relationship. However, it is often ne-
glected in the training of doctors. Many people, including
health professionals, think that the art of communication
is a natural skill, ignoring the fact that, just as with other
aspects of patient care, it can be learned. There are many
general guidelines published on how to break bad
news,23�28 which provide general basic knowledge on
how to communicate properly, but it is also necessary to
learn via practice, through basic programmes,29,30 with
follow-up and consolidation.31
Perhaps the most important findings of this study, also
verified in all other studies on the problem of information
disclosure, are the large differences observed in patients’
preferences. Even when there is a clear preference on a
particular aspect, there is never unanimity. Therefore, the
data provided by studies of information preferred by
patients in different populations should be seen only as
marking out trends or general indications, because in
the presence of a particular patient we do not know what
he or she wants before we try to find out. Patient
preference should not be assumed based on these general
data. These studies, important as they are, show popula-
tion data, which do not necessarily encompass individual
needs.
The findings of this work can be relevant to anyone
working with cancer patients. It adds data relative to
patients of a southern European environment, which
does not seem to match, at least in those aspects
statistically handled, other cultures deemed to be similar,
such as that of neighbouring Spain.
Acknowledgements
This study was supported in part by the North Section of
the Portuguese League Against the Cancer.
References
1 Loge JH, Kaasa S, Ekeberg Ø/´ , Falkum E, Hytten K.
Attitudes toward informing the cancer patient �/ a surveyof Norwegian physicians. Eur J Cancer 1996; 32A:1344�/48.
2 Thomsen OØ, Wulff HR, Martin A, Singer P. What dogastroenterologists in Europe tell cancer patients? Lancet1993; 341: 473�/76.
3 Novack DH, Plumer R, Smith RL, Ochitill H, MorrowGR, Bennet JM. Changes in physicians’ attitudes towardtelling the cancer patient. JAMA 1979; 241: 897�/900.
4 Estape J, Palombo H, Hernandez E et al . Cancerdiagnosis disclosure in a Spanish hospital. Ann Oncol1992; 3: 451�/54.
5 Mystakidou K, Liossi C, Viachos L, Papadimitriou J.Disclosure of diagnostic information to cancer patientsin Greece. Palliat Med 1996; 10: 195�/200.
6 Fainsinger RL, Nunez-Olarte JM, Demoissac DM. Thecultural differences in perceived value of disclosure andcognition: Spain and Canada. J Palliat Med 2003; 19:43�/48.
7 Ferraz Goncalves J, Castro S. Diagnosis disclosure in aPortuguese oncological centre. Palliat Med 2001; 15: 35�/
41.8 Cassileth BR, ZurpKis RV, Sutton-Smith K, March V.
Information and participation preferences among cancerpatients. Ann Intern Med 1980; 92: 832�/36.
9 McIntosh J. Patients’ awareness and desire for informa-tion about diagnosed but undisclosed malignant disease.Lancet 1976; ii: 300�/303.
10 Ferraz Goncalves JA. A Portuguese palliative care unit.Support Care Cancer 2001; 9: 4�/7.
11 Inouye SK, van Dick CH, Alessi CA, Balkin S, SiegalAP, Horwitz RI. Clarifying confusion: the confusionassessment method. Ann Intern Med 1990; 113: 941�/48.
12 Centeno-Cortes C, Nunez-Olarte JM. Questioning diag-nosis disclosure in terminal cancer patients. Palliat Med1994; 8: 39�/44.
13 Sardell AN, Trierweiler SJ. Disclosing the cancer diag-nosis: procedures that influence patient hopefulness.Cancer 1993; 72: 3355�/65.
14 Chan A, Wooddruff RK. Communicating with patientswith advanced cancer. J Palliat Care 1997; 13: 29�/33.
15 Lind SE, Good MJD, Seidel S, Csordas T, Good BJ.Telling the diagnosis of cancer. J Clin Oncol 1989; 7:583�/89.
16 Barnett MM. Effect of breaking bad news onpatients’ perceptions of doctors. J R Soc Med 2002;95: 343�/47.
17 Yun YH, Lee CG, Kim S, et al . The attitudes of cancerpatients and their families toward the disclosure ofterminal illness. J Clin Oncol 2004; 22: 307�/14.
530 F Goncalves et al.

60 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
18 Butow PN, Kazemi JN, Beeney LJ, Griffin AM, DunnSM, Tattersall MHN. When the diagnosis is cancer:patient communication experiences and preferences.Cancer 1996; 77: 2630�/37.
19 Gattellari M, Voigt KJ, Butow PN, Tattersall MHN.When the treatment goal is not cure: are cancer patientsequipped to make informed decisions? J Clin Oncol2002; 20: 503�/13.
20 Cassileth BR, Volckmar D, Goodman RL. The effectof experience on radiation therapy patients’ desirefor information. Int J Radiat Oncol Biol Phys 1980; 6:493�/96.
21 Fallowfield LJ, Jenkins VA, Beveridge HA. Truth mayhurt but deceit hurts more: communication in palliativecare. Palliat Med 2002; 16: 297�/303.
22 Jones JS. Telling the right patient. Br Med J 1981; 283:291�/92.
23 Faulkner A, Maguire P, Regnard C. Breaking bad news�/ a flow diagram. Palliat Med 1994; 8: 145�/51.
24 Richards MA, Ramirez AJ, Degner LF, Fallowfield LJ,Maher EJ, Neuberger J. Offering choice of treatment topatients with cancer. A review based on a symposiumheld at the 10th Annual Conference of the British
Psychosocial Oncology Group, December 1993. Eur JCancer 1995; 31A: 112�/16.
25 Girgis A, Sanson-Fisher RW. Breaking bad news: con-sensus guidelines for medical practitioners. J Clin Oncol1995; 13: 2449�/56.
26 Fallowfield L. Giving sad and bad news. Lancet 1993;341: 476�/78.
27 Creagan ET. How to break bad news �/ and not de-vastate the patient. Mayo Clin Proc 1994; 69: 1015�/17.
28 Buckman R. How to break bad news. London: PanBooks, 1992.
29 Fallowfield L, Jenkins V, Farewell V, Saul J, Duffy A,Eves R. Efficacy of a cancer research UK communica-tion skills training model for oncologists: a randomisedcontrolled trial. Lancet 2002; 359: 650�/56.
30 Jenkins V, Fallowfield L. Can communication skillstraining alter physicians’ beliefs and behaviour in clinics?J Clin Oncol 2002; 20: 765�/69.
31 Razavi D, Merckaert I, Marchal S, et al . How tooptimize physicians’ communication skills in cancercare: results of a randomized study assessing the useful-ness of post-training consolidation workshops. J ClinOncol 2003; 21: 3141�/49.
Breaking bad news 531

| 61 61Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Tomando estes dois estudos em conjunto pode concluir-se que a informação prestada aos doentes não está muitas vezes de acordo com os seus desejos.
No primeiro estudo, uma razão frequentemente invocada pelos médicos para não dar a informação aos doentes é a possibilidade de lhes causar dano psicológico o que está em contradição com os dados da investigação como referido anteriormente. Não esclarecer os doentes quando esse é o seu desejo pode ter boas intensões e é frequentemente apoiado pelos familiares. Pode, porém, representar uma defesa dos próprios médicos porque a comunicação reveste-se de aspectos muitos difíceis, sobretudo dar más notícias. A investigação, no entanto, sugere que o facto de os doentes não terem uma ideia, pelo menos em termos gerais, da sua situação acarreta muitas consequências. Entre essas consequências estão internamentos desnecessários, aumento da proporção de mortes hospitalares e referenciações tardias para cuidados paliativos ou mesmo a sua ausência [6]. Pode haver também consequências psicológicas, como desconfiança a sentimentos de abandono [6].
No segundo estudo verificou-se que 87% dos doentes desejavam ser informados, enquanto só 72% tinham sido informados. Os que não tinham sido informados referiramque não estavam à vontade para perguntar, a informação foi recusada, foi pouco clara ou porque se sentiram enganados. Verificou-se também que alguns dos doentes que foram informados teriam preferido não o ter sido e vice-versa. Este ponto é muito importante porque o principal não é ser ou não ser informado mas ver satisfeitas as
síntese

62 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
suas necessidades informativas para melhor lidar com a situação. Essas necessidades são variáveis e alguns doentes lidam melhor com a situação sem informação. Há ainda a acrescentar que a informação não pode ser vista como pontual, mas sim como progressivae contínua, podendo os desejos do doente mudar com o tempo.
A constatação de que muitos doentes são referenciados para cuidados paliativos sem que lhes seja dada uma explicação da razão e do significado desse facto reforça a necessidade de que no primeiro encontro se explore essa questão. Verificou-se também que há doentes que não têm informação, mas que por várias razões, que não têm a ver com o seu desejo, não questionam os profissionais. Por isso, os profissionais devem ter uma atitude proactiva.
O facto de não se prestarem as informações que os doentes desejem de forma a poderem tomar decisões informadas é lesivo dos seus interesses e dos seus direitos. Na realidade, sem essa informação não há consentimento informado, condição indispensável para se cumprir o princípio da ética biomédica do respeito pela autonomia. Além da questão ética de não informar, há também violação da legislação, quer do código penal quer do código deontológico dos médicos.
Muito do que hoje é recomendado sobre o processo da comunicação e da informação baseia-se na experiência e no bom senso e não predominantemente na investigação, mas certamente que em primeiro lugar há que saber que informação o doente já tem [5]. O processo de comunicação eficaz requer que não haja alterações cognitivas significativas.O processo de avaliação da consciência é o objecto do capítulo seguinte.
referências
Grunfeld E, Folkes A, Urquhart R. Do available questionnaires measure the communication factors that patients and families consider important at end of life? J Clin Oncol 2008;26:3874-3878.
Ferraz Gonçalves, Castro S. Diagnosis disclosure in a Portuguese oncological centre. Palliative Medicine 2001;15: 35–41.
Novack DH, Plumer R, Smith RL, Ochitill H, Morrow GR, Bennett JM. Changes in physicians’ attitudes toward telling the cancer patient. J Am Med Assoc 1979; 241: 897–900.
1
2
3
4
5
6
Ferraz Gonçalves, Marques A, Rocha S, Leitão P, Mesquita T, Moutinho S. Breaking bad news: experiencesand preferences of advanced cancer patients at a Portuguese oncology centre. Palliative Medicine 2005; 19: 526-/531.
Buckman R. How to break bad news: a guide to health-careprofessionals. Pan Books 1994.
Innes S, Payne S. Advanced cancer patients’ prognosticinformation preferences: a review. Palliat Med 2009;
23:29-39.

| 63 63Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
3AVALIAÇÃO DA CONSCIÊNCIA
64 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 65 65Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
O termo consciência tem sido tomado ao longo do tempo em sentidos diversos. Tem sido objecto de reflexão por diversos filósofos [1] e de estudo científico. Tem sido considerada do ponto de vista moral, a chamada consciência moral.
Mais recentemente, têm sido as neurociências a dominar este campo. Já é muito antigo o conceito de que a consciência depende de uma função cerebral intacta. De facto, já Hipócrates o considerava [2].
A consciência foi definida por William James em 1890 como o estado de conhecimento de si próprio e do ambiente [3]. A consciência tem dois componentes: a vigília e o conteúdo. A vigília é o estar acordado. É aquilo a que normalmente se chama estar consciente. No entanto, esse aspecto apenas não nos diz nada sobre a capacidade cognitiva. Há estados em que os indivíduos estão acordados, mas têm um capacidade cognitiva reduzida ou nula, como acontece nos doentes com delirium, demências ou no estado vegetativo persistente. Nestas situações o estado de vigília pode estar normal ou quase normal mas o conteúdo está mais ou menos afectado. Para se poder avaliar o conteúdo da consciência é necessário, porém, um certo grau de vigília.
Foram desenvolvidos vários métodos de avaliação destas duas dimensões da consciência. Não havia, porém, nenhum instrumento desenvolvido especificamente para a população em cuidados paliativos para avaliar o estado de vigília. Os intrumentos usados foram desenvolvidos para outras situações referidas no artigo inserido neste capítulo, alguns
avaliação da consciência

66 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
dos quais não foram validados. Por isso se validou o presente instrumento que é simples, intuitivo, de fácil apredizagem e que demora apenas alguns segundos a aplicar. Além disso, não carece de qualquer esforço da parte dos doentes. Estas características tornam este instrumento adequado para ser usado em cuidados paliativos e para ser integrado no sistema que nos propusemos desenvolver.
A avaliação da consciência é indispensável no contacto com os doentes, nomeadamente no primeiro encontro. Sem essa avaliação não é possível estar-se seguro da fiabiliadade da avaliação subsequente. Assim, se o estado de vigília não for obviamente normal é necessário determinar o seu nível pelo método validado apresentado a seguir. Se o nível de vigília for suficiente para se fazer a avaliação do conteúdo da consciência e se este não for obviamente anormal deve avaliar-se a função cognitiva.
Neste capítulo apresenta-se a seguir o método de avaliação do estado de vigília, apresentando um artigo já publicado Validation of a Consciousness Level Scale for Palliative Care em que descreve uma escala e o processo da sua validação desenvolvidapor nós especificamente para cuidados paliativos. Segue-se a descrição do método escolhido para avaliação da função cognitiva e a justificação para a sua escolha.

| 67 67Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
validation of a consciousness level scale for palliative care
f. gonçalves, mj bento, m. alvarenga, i. costa and l. costa
Palliative Medicine (2008); 22:724

68 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 69 69Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
40
Validation of a Consciousness Level Scalefor Palliative CareF Gonçalves Palliative Care Unit – Network, Portuguese Institute of Oncology, Porto, MJ BentoEpidemiology Service, Portuguese Institute of Oncology, Porto, M Alvarenga, I Costa and L Costa PalliativeCare Service, Portuguese Institute of Oncology, Porto
The main objective of this study is to validate a Consciousness Scale for palliativecare. The scale was named Consciousness Scale for palliative care (CSPC). The valida-tion had two phases: 1) face validity – the scale was assessed by seven healthcareprofessionals, both doctors and nurses, experienced in palliative care; 2) reliabilityand construct validity – performed by four investigators, two nurses and two doctors.The construct validation was performed by comparing the CSPC with a Visual Ana-logue Scale (VAS) of 100 mm, anchored in the terms ‘awake’ and ‘unarousable’, andthen with the Glasgow Coma Scale (GCS). In this study, all four observers completed44 periods of observation relative to 38 patients resulting in a total of 176 observations.In the phase of face validation, there were no discrepancies in relation to the issue: thescale provides measures for measurement; the scale can be useful to clinical practice;the scale can improve communication among professionals and the scale is easy touse. As a measure of internal consistency, Cronbach’s α was found to be very high(0.99). The inter-rater reliability was also very high with an intraclass correlation coeffi-cient of 0.99 (P < 0.001). The correlation of the CSPC to the VASwas 0.94 (P < 0.001) andthe CSPC to the GCS was −0.82 (P < 0.001). The CSPC can be a very useful tool forassessing consciousness in palliative care patients. It is very ease to use, not time con-suming and can be used withminimal training. Communication between professionalscan be improved in the clinical setting and in the research environment. Palliative Med-icine (2008); 22: 724–729
Key words: consciousness; consciousness level scale; palliative care; sedation
Introduction
A large percentage of palliative care patients undergotemporary or definitive changes in their consciousnesslevel. This can be due to the involvement of the centralnervous system brought on by cancer, metabolic altera-tions, infections, medication or a combination of thesefactors. When it is caused by medication, the level of con-sciousness can be intentionally affected or not. Whenintentional, with the aim of controlling suffering, theaction is called palliative sedation.
Sedation in palliative care is a very important task. Ithas been under discussion for more than a decade. Chateret al.1 defined sedation as ‘the intention to deliberatelyinduce and maintain deep sleep, but not deliberately caus-ing death, in very specific circumstances…’. However, theobjective is to control suffering (physical or psychological
symptoms, existential distress, etc.) and not the level ofsedation. Hence, the deepness of sedation should be,such as to acceptably control, the cause of suffering,which cannot be controlled by any other means.
No validated palliative care scale to measure the levelof consciousness exists. The absence of such a scale is oneof the reasons why data from studies, such as those deal-ing with sedation, are difficult to compare. Therefore,a reliable consciousness level scale could improve commu-nication between professionals, making the comparison ofdata of different studies easier, and it would be useful toclinical practice and research in general. The purpose ofthis study is to develop and validate such a scale for palli-ative care. The scale developed herein is called the Con-sciousness Scale for Palliative Care (CSPC).
Consciousness has two dimensions: wakefulness andawareness.2 There are other scales that measure cognitivefunction, and therefore awareness, for example, the mini-mental state examination,3 and others. The intention ofthat scale is to primarily measure wakefulness and notthe content of consciousness.
Correspondence to: Dr Ferraz Gonçalves, Instituto Portuguêsde Oncologia, UCP-R, Rua Dr. António Bernardino deAlmeida, 4200-072 Porto, Portugal.Email: [email protected] or [email protected]
© 2008 SAGE Publications, Los Angeles, London, New Delhi and Singapore 10.1177/0269216308094104
Palliative Medicine 2008; 22: 724–729
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

70 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
41
Methods
This study was conducted at the Palliative Care Service ofthe Porto Section of the Portuguese Institute of Oncology.The study was approved by the ethics committee of theinstitution. As this study was non-interventional andthere was no added risk to patients, a written informedconsent was waived.
The design of the scaleTo identify other existing level of consciousness scales, aMEDLINE search was done for the period January 1970to September 2003, using the following keywords: comascale, coma assessment, sedation scale and sedation assess-ment. Reference lists of the resulting articles were reviewed.
Although there are many scales used in different envir-onments, only a small number were assessed for reliabilityand validity, which was also observed by others.4,5 Mostof them were designed for use in intensive care units (ICU)or on neurological patients. None have been designed foror studied in a palliative care setting.
None of the identified scales are suited to use in a palli-ative care setting for a large number of reasons, the mostrelevant being:
� Most of the scales used in ICU include the assessmentof items such as anxiety or agitation.6–11
� Other scales used in ICU have items related to compli-ance with mechanical ventilation.6,11–13
� Some scales were designed for neurological conditions;therefore, they contain items that are irrelevant to ourpurpose.14–17
� Some scales were designed to focus on particular con-ditions and therefore contain items that are only ofrelevance to such conditions.18–22
� Some were designed for children.23,24� Many do not have the levels of the scale clearly
defined, or these are not mutually exclusive.25,26
Although the existing scales were considered inadequatefor use in palliative care, they included the elements thatshould be used in a new scale. There are, therefore, ele-ments common to all these scales. In fact, following thestudy of those scales, the CSPC was constructed based onthe responses to the stimuli ranked in a logical manner. Thechosen responses are mutually exclusive. The stimuli,which are common to many scales, are simple and alsoperformed in a logical progression: first observation then,if required, vocal stimulus and finally painful stimulus.
This study included bedridden patients over 18 years ofage, on a convenience basis. A patient may be includedmore than once if observations are carried out at least48 h apart. The data collected included age, gender, diag-
nosis, metastases, sedative medication and if the patientwas intentionally sedated or not.
The study had two phases. In phase 1, face/contentvalidity was carried out. Seven healthcare professionalsexperienced in palliative care, three doctors and fournurses, not involved in the design of the scale, appliedthe scale to about 20 patients each in order to familiarisethemselves with it. They then answered the followingquestions using a five-point scale ranging from ‘stronglyagree’ to ‘strongly disagree’:
� Does the scale measure what it is intended to measure?� Can the scale be useful to clinical practice?� Can the scale improve communication among health-
care professionals with regard to consciousness level?� Is the scale easy to use?
The investigators were asked to give suggestions thatmight improve the scale, if they thought the scale couldbe improved.
In phase 2, reliability and construct validation wereperformed. Because there is not any golden standard toevaluate consciousness level against which the CSPC canbe compared, a criterion validation could not be per-formed. Therefore, we had to perform a construct valida-tion of the scale, comparing it with other tools we thinkcan measure consciousness level, as is usually the case inthese types of study. A visual analogue scale (VAS) andthe Glasgow Coma Scale (GCS) were used, as was thecase in similar studies undertaken in different settings,such as in an ICU environment.4,6,7,13 The VAS wasassessed by drawing a perpendicular mark on a 100 mmhorizontal line based on the terms ‘awake’ and ‘unarousa-ble’, and then the distance between the left end of the lineand the mark was measured in millimetres.
The data were collected by four investigators involvedin the study: two doctors and two nurses. All four investi-gators underwent a training period with the VAS for eval-uating consciousness level, to familiarise with the scale.Each patient was simultaneously observed by three inves-tigators, one doctor and two nurses. One investigatorinteracted with the patient, as per the instructions setforth in the appendix, and rated the patient, whereas theother two observed and rated the patient independently:two scored using the CSPC and one using the VAS. In all,15 min later, the other doctor performed the GCS, record-ing the score of each item (motor and verbal responses,and eye opening). A rotation system was used so thateach healthcare professional performed all the roles a sim-ilar number of times, except with regards to the GCS,which was always performed by the doctors and alwaysby the doctor who did not participate in the first part ofevaluation.
Consciousness Level Scale for Palliative Care 725
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

| 71 71Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
42
Statistical analysis
� Cronbach’s α was performed to measure internalconsistency.27
� The intraclass correlation coefficient was used to mea-sure the degree of concurrence between raters.28
� The association between the CSPC, VAS and GCSwas evaluated using Spearmen’s ρ.29
� The non-parametric Wilcoxon rank sum test was usedto compare CSPC values with previously identifiedsubgroups (gender, age, use of sedatives).30
Results
In this study, all four observers made 44 periods of obser-vation relative to 38 patients, resulting in 176 observa-tions. None of the patients was subject to more than twoperiods of observation. The demographic data of thosepatients are detailed in Table 1.
Forty-two patients (96%) were medicated with one ormore drugs with sedative effects: 91% opioids, 57% neuro-leptics, 43% benzodiazepines and 30% others. Six patientswere intentionally sedated: 1 was at level 4, 3 at level 5 and2 at level 6 of the scale. There was, in those patients, 100%coincidence between the two raters of the scale.
Face validityThe results for face validity were as follows:
� The scale measures what it is intended to measure.Mean = 1.7 (range: 1 to 2).
� The scale can be useful to clinical practice. Mean = 1.6(range: 1 to 3).
� The scale can improve communication among health-care professionals: Mean = 2.0 (range: 1 to 3).
� The scale is easy to use. Mean = 1.6 (1 to 2).
Therefore, the range of responses went from stronglyagree to the middle of the scale, without anydisagreements.
Internal consistencyAs a measure of internal consistency, the Cronbach’s αwas very high (0.99).
Inter-rater reliabilityThe scores recorded by the raters are displayed in Table 2.The same score on the scale was selected in 39 cases (89%).In the five cases where a different score was selected, thedifference was always not more than one level of the scale.The degree of agreement between raters with regard tothe scale was, therefore, very high, with an intraclass cor-relation coefficient of 0.99 (P < 0.001).
There were no significant within-subject differences insubgroups (age, gender) when analyzed by the Wilcoxonrank sum text. The median age of the patients (68 years)was used to divide this item into two groups. In womenand those aged over 68 years, the scores coincided. Theanalysis of the group that used sedatives was not per-formed because 96% of the patients were using them.
Construct validityThe correlation of the CSPC to the VAS and GCS wasvery high (Table 3). The correlation coefficient of theCSPC to the VAS was 0.94 (P < 0.001) for the firstobserver and 0.95 (P < 0.001) for the second. The correla-tion coefficient of the scale to the GCS was −0.82(P < 0.001) for the first observer and −0.85 (P < 0.001)for the second. Note that the coefficient of the CSPC to
Table 1 Demographic data
No. (%)
GenderMale 19 (50)Female 19 (50)
PrimaryGynaecologic 8 (21)Colorectal 6 (16)Head and neck 5 (13)Gastric 3 (8)Astrocytoma 3 (8)Lung 2 (5)Melanoma 2 (5)Other 9 (24)
Age: median of 68 years (range: 38–82).
Table 2 Distribution of consciousness scale for palliativecare scores between raters
Scores 2nd rater
1 2 3 4 5 6
1st rater 1 9 2 0 0 0 02 2 9 0 0 0 03 0 0 5 1 0 04 0 0 0 3 0 05 0 0 0 0 6 06 0 0 0 0 0 7
Table 3 Correlation between scales
Scales ρ P
CSPC1–CSPC2 0.98 <0.001CSPC1–VAS 0.96 <0.001CSPC2–VAS 0.96 <0.001CSPC1–GCS 0.88 <0.001CSPC2–GCS 0.88 <0.001
CSPC1 and CSPC2 are the 1st and 2nd ratings of the scale.CSPC, Consciousness Scale for Palliative Care; VAS,Visual Analogue Scale; GCS, Glasgow Coma Scale.
726 F Gonçalves et al.
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

72 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
43
the GCS was negative due to the scales’ scoring beinginverted in relation to each other; in other words, thebest score of the CSPC is the lowest, whereas the bestscore of the GCS is the highest.
Discussion
An ideal assessment tool should be inexpensive, easy tolearn and easy to use by doctors and nurses at bedsides.This last aspect is particularly important in palliative carebecause it is practised in many settings and by healthcareprofessionals from heterogeneous backgrounds. Yet, theassessment tool should undergo rigorous testing to showvalidity and reliability. Probably, the most used scale isthe Ramsay Scale. This scale was developed in an ICU tocontrol the level of sedation with alphaxalone-alphadoloneand published in the British Medical Journal in 1974.25 Thescale was really a secondary aspect of the article; however,since then, it has been widely used in many settings withoutundergoing any process of validation. This was carried outrecently.31 Although that scale has been extensively used,it has been criticised for many reasons,32 the criticismsmos-t relevant to palliative care being: ‘the six levels of the Ram-say scale are not mutually exclusive’; ‘patients may be rest-less or agitated (level 1), whereas at the same time beingresponsive only to light physical or loud auditory stimulus(level 4 and 5)’ and ‘the sedation levels are not clearlydefined or fully inclusive’.
The goal of this study was the development and valida-tion of a scale with the above-described characteristics, inan attempt to avoid the drawbacks of the Ramsay scaleand other scales.
The structure of the scale is very ease to use and thelevels are clearly defined, with a phase of observationand, if required, consecutive phases of verbal interactionand of physical stimulation. The scale can be administeredin a few seconds, using common and unambiguous stimuliin a logical sequence. The stimuli are also standardized,which does not happen with most scales.
The inter-rater reliability of the scale was very goodfor all patients, with coincident scores in almost 90% ofthe cases, and in the few cases without coincidence, thedifference was never greater than one level. In womenand in patients aged over 68 years, there was completeagreement in the scores, as well as among the six patientswho were intentionally sedated.
As no gold standard exists for sedation, against which theCSPC could be compared to validate it, the validation of theCSPC was performed by correlating it to a VAS based onthe terms ‘awake’ and ‘unarousable’ and theGCS,which is ascale that was designed to assess the prognosis of coma afterhead injury33 but which is widely used in many settings toassess the consciousness level. The correlation of the CSPCto the VAS and the GCS was very high.
There are potential limitations to the use of the CSPC.Asit relies on the patients’ auditory and visual acuity, it is notsuitable for use on patients with major impairment of thesesenses.The intensityof the stimuli canvarywith theobserver;in other words, louder voices or more firm pinching of thetrapezius might eventually result in different scores. Patientscan have a ‘not normal’ score simply because they were nor-mally sleeping, but this is common to all scales.
Nevertheless, the CSPC can be a very useful tool forassessing consciousness in palliative care patients. It isvery ease to use, not time consuming and can be per-formed with minimal training. Communication betweenhealthcare professionals can be improved in the clinicalsetting and in a research environment by the lack of ambi-guity of the levels and of the method of interaction withthe patient. However, the scale should be evaluated inother locations in a palliative care setting to confirm theresults achieved by this study.
References
1 Chater, S, Viola, R, Paterson, J, Jarvis, V. Sedation forintractable distress in the dying – a survey of experts. Pal-liat Med 1998; 12: 255–269.
2 Laureys, S. The neural correlate of (un)awareness: les-sons from the vegetative state. Trends Cogn Sci 2005;19: 556–559.
3 Folstein, MF, Folstein, SE, McHugh, PR. Mini-mentalstate: a practical method for grading the cognitive state ofpatients for the clinician. JPsychiatr Res 1975; 12: 188–189.
4 Ely, EW, Truman, B, Shintani, A, Thomason, JW,Wheeler, AP, Gordon, S, et al. Monitoring sedation sta-tus over time in ICU patients: reliability and validity ofthe Richmond Agitation-Sedation Scale (RASS). JAMA2003; 289: 2983–2991.
5 Jacobi, J, Fraser,G, Coursin, DB, Riker, RR, Fontaine, D,Wittbrodt, ET, et al. Clinical practice guidelines for the sus-tained use of sedatives and analgesics in the critically illadults. Crit Care Med 2002; 30: 119–141.
6 Sessler, CN, Gosnell, MS, Grap, MJ, Brophy, GM,O’Neal, PV, Keane, KA, et al. The RichmondAgitation-Sedation Scale: validity and reliability inadult intensive care unit patients. Am J Respir Crit CareMed 2002; 166: 1338–1344.
7 Devlin, JW, Boleski, G, Mlynarek, M, Nerenz, DR,Peterson, E, Jankowski, M, et al. Motor Activity Assess-ment Scale: a valid and reliable sedation scale for use withmechanically ventilated patients in an adult surgicalintensive care. Crit Care Med 1999; 27: 1271–1275.
8 Riker, RR, Picard, JT, Fraser, GL. Prospective evalua-tion of the Sedation-Agitation Scale for adult critically illpatients. Crit Care Med 1999; 27: 1325–1329.
9 Detriche, O, Berré, J, Massaut, J, Vincent, JL. The Brus-sels Sedation Scale: use of a simple clinical sedation scale
Consciousness Level Scale for Palliative Care 727
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

| 73 73Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
44
can avoid excessive sedation in patients undergoingmechanical ventilation in the intensive care unit. Br JAnaesth 1999; 83: 698–701.
10 Chaudhri, S, Kenny, GNC. Sedation after cardiac bypasssurgery: comparison of propofol and midazolam in thepresence of a computerized closed loop arterial pressurecontroller. Br J Anaesth 1992; 68: 98–99.
11 Riker, RR, Fraser, GL, Cox, PM. Continuous infusionof haloperidol controls agitation in critically ill patients.Crit Care Med 1994; 22: 433–440.
12 Mallick, A, Smith, SN, Bodenham, AR. Local anaesthe-sia to the airway reduces sedation requirements inpatients undergoing artificial ventilation. Br J Anaesth1996; 77: 731–734.
13 Riker, RR, Fraser, GL, Simmons, LE, Wilkins, ML.Validating the Sedation-Agitation Scale with the bispec-tral index and Visual Analog Scale in adult ICU aftercardiac surgery. Intensive Care Med 2001; 27: 853–858.
14 Wijdicks, EFM, Kokmen, E, O’Brien, PC. Measurementof impaired consciousness in the neurological intensivecare unit: a new test. J Neurol Neurosurg Psychiatry1998; 64: 117–119.
15 Stanczak, DE, White, JG, Gouview, WD, Moehle, KA,Daniel, M, Novack, T, et al. Assessment of level of con-sciousness following severe neurological insult: a compar-ison of the psychometric qualities of the Glasgow ComaScale and the Comprehensive Level of ConsciousnessScale. J Neurosurg 1984; 60: 955–960.
16 Sugiura, K, Muraoka, K, Chishiki, T, Baba, M. TheEdinburg-2 Coma Scale : a CSPC for assessing impairedconsciousness. Neurosurgery 1983; 12: 411–415.
17 Benzer, A, Mitterschiffthaler, G, Marosi, M, Luef, G,Pühringer, F, De La Renotiere, K, et al. Prediction ofnon-survival after trauma: Innsbruck Coma Scale. Lan-cet 1991; 338: 977–978.
18 Miller, DR,Martineau, RJ, Hull, KA, Vallé, F, LeBel, M.Optimizing sedation following major vascular surgery: adouble-blind study of midazolam administered by contin-uous infusion. Can J Anaesth 1994; 41: 782–793.
19 Sanchez-Izquierdo-Riera, JA, Caballero-Cubedo, RE,Perez-Vela, JL, Ambros-Checa, A, Cantalapiedra-Santiago, JA, Alted-Lopez, E. Propofol versus midazo-lam: safety and efficacy for sedating the severe traumapatient. Anesth Analg 1998; 86: 1219–1224.
20 Eddleston, JM, Pollard, BJ, Blades, JF, Doram, B.The use of propofol for sedation of critically ill patients
undergoing haemodiafiltration. Intensive Care Med 1995;21: 342–347.
21 Checketts, MR, Gilhooly, CJ, Kenny, GNC. Patient-maintained analgesia with target-controlled alfentanilinfusion after cardiac surgery: a comparison with mor-phine PCA. Br J Anaesth 1998; 80: 748–751.
22 Irwin, MG, Thompson, N, Kenny, GNC. Patient-maintained propofol sedation. Anaesthesia 1997; 52:525–530.
23 Malviya, S, Voepel-Lewis, T, Huntington, J, Siewert, M,Green, W. Effects of anesthetic technique on side effectsassociated with fentanyl oralet premedication. J ClinAnesth 1997; 9: 374–378.
24 Ambuel, B, Hamlett, KW, Marx, CM, Blumer, JL.Assessing distress in pediatric intensive care environ-ments: the COMFORT scale. J Pediatric Psychol 1992;17: 95–109.
25 Ramsay,MAE, Savege, TM, Simpson, BRJ, Goodwin, R.Controlled sedation with alphaxalone-alphadolone. BMJ1974; 2: 656–659.
26 De Jonghe, B, Cook, D, Appere-De-Vecchi, C, Guyatt, G,Meade, M, Outin, H. Using and understanding sedationscoring systems: a systematic review. Intensive Care Med2002; 26: 275–285.
27 Bland, JM, Altman, DG. Cronbach’s alpha. BMJ 1997;314: 572.
28 Análisis de la concordancia. In: Pallás, JMA, Villa, JJ,(Eds), Métodos de investigación: clínica e epidemiológica,segunda edición. Madrid: Ediciones Harcourt S.A., 2000;p. 321–325.
29 Relation between two continuous variables. In: Altman,DG, (Ed), Practical statistics for medical research. 1st ed.London: Chapman and Hall, 1991; p. 277–324.
30 Comparing groups – continuous data. In: Altman, DG,(Ed), Practical statistics for medical research, 1st ed. Lon-don: Chapman and Hall, 1991; p. 179–228.
31 Yate, PM, Thomas, D, Short, SM, Sebel, PS, Morton, J.Comparison of infusions of alfentanil or pethidine forsedation of ventilated patients of the ITU. Br J Anaesth1986; 58: 1091–1099.
32 Hansen-Flaschen, J, Cowen, J, Polomano, RC. Beyondthe Ramsay Scale: need for a validated measure of sedat-ing drug efficacy in the intensive care unit. Crit Care Med1994; 22: 732–733.
33 Teasdale, G, Jennett, B. Assessment of coma andimpaired consciousness. Lancet 1974; 13: 81–84.
728 F Gonçalves et al.
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from
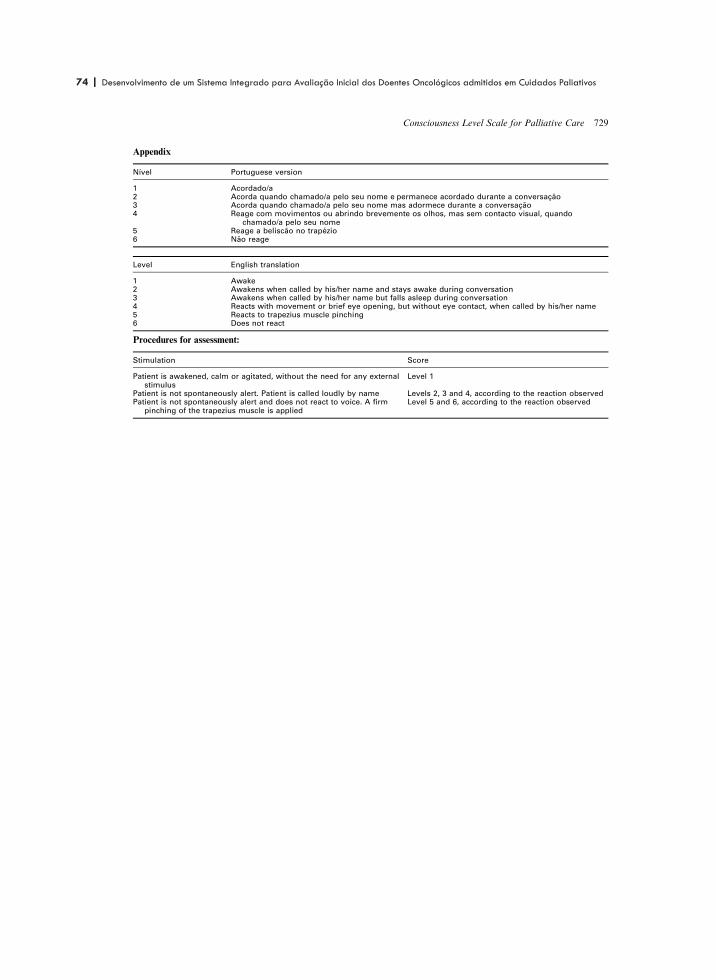
74 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
45
Appendix
Nível Portuguese version
1 Acordado/a2 Acorda quando chamado/a pelo seu nome e permanece acordado durante a conversação3 Acorda quando chamado/a pelo seu nome mas adormece durante a conversação4 Reage com movimentos ou abrindo brevemente os olhos, mas sem contacto visual, quando
chamado/a pelo seu nome5 Reage a beliscão no trapézio6 Não reage
Level English translation
1 Awake2 Awakens when called by his/her name and stays awake during conversation3 Awakens when called by his/her name but falls asleep during conversation4 Reacts with movement or brief eye opening, but without eye contact, when called by his/her name5 Reacts to trapezius muscle pinching6 Does not react
Procedures for assessment:
Stimulation Score
Patient is awakened, calm or agitated, without the need for any externalstimulus
Level 1
Patient is not spontaneously alert. Patient is called loudly by name Levels 2, 3 and 4, according to the reaction observedPatient is not spontaneously alert and does not react to voice. A firm
pinching of the trapezius muscle is appliedLevel 5 and 6, according to the reaction observed
Consciousness Level Scale for Palliative Care 729
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from
| 75 75Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
A insuficiência cognitiva é muito frequente nos doentes com doenças avançadas. Há vários distúrbios associados à insuficiência cognitiva, sendo o delirium o mais frequente na fase final da vida. Para se poder avaliar o estado cognitivo, o conteúdo da consciência,é necessário que haja uma certa capacidade de estar vígil. O delirium ocorre em 28% a 83% dos doentes quando próximos do fim da vida [4]. O delirium pode ser óbvio, sobretudo a sua variante hiperactiva em que há agitação psicomotora, mas numa percentagem que pode atingir os 50% pode não ser detectado. Isto deve- se a diversos motivos dos quais se destacam: a flutuação do comportamento dos doentes ao longo do dia, com este a aproximar-se do normal, em geral mais frequentemente de manhã, agravando-se à medida que o dia avança, tornando-se pior ao fim da tarde e à noite; e a variante hipoactiva em que a agitação geralmente associada ao delirium não está presente ou ocorre episodicamente.
O problema de não se detectar uma percentagem significativa dos casos de deliriumnão se limita aos cuidados paliativos, verificando-se frequentemente nos doentes internados em geral, sobretudo nos idosos, no pós-operatório e nos cuidados intensivos. Por isso, foram desenvolvidos inúmeros instrumentos com o fim de melhorar o rastreio e/ou o diagnóstico do delirium [5].
O interesse de se fazer o rastreio do delirium reside no facto de ser reversível em muitos casos e em poder ser indicativo, por vezes o único sinal em doentes debilitados, de uma ocorrência que complique o estado dos doentes, como uma infecção ou hipercalcemia, por exemplo.
avaliação da função cognitiva

76 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
O método de rastreio mais conhecido e usado é sem dúvida o Mini Exame do Estado Mental (Mini-Mental-Status Examination) [6]. Este instrumento tem uma validade excelente para detectar alterações cognitivas e para avaliar a sua gravidade, podendo assim servir para avaliar a sua evolução, mas não permite o diagnóstico de delirium. O problema principal quanto a nós é o de exigir uma participação importante dos doentes, nomeadamente a realização de um desenho. Num estudo recente, Fayers et al. concluíram que é possível reduzir o número de perguntas mantendo uma boa acurácia para o rastreio de alterações cognitivas [7].
Outro instrumento muito usado pela sua simplicidade, sobretudo na sua versão curtatambém designada algoritmo, é o Método de Avaliação da Confusão (MAC) [8]. É composto apenas por quatro itens e não exige qualquer esforço do doente, já que é pela observação do comportamento e das respostas do doente durante a consultaque o profissional de saúde diagnosticará ou não delirium. Este método permite o diagnóstico de delirium ao contrário do Mini-Exame do Estado Mental (MEEM), mas por outro lado não é quantitativo, pelo que não permite medir a gravidade nem a evolução da situação. Este método foi recentemente validado em cuidados paliativos [9]. No entanto, o MAC foi desenhado para ser aplicado baseado em observações realizadas durante uma avaliação cognitiva formal com instrumentos como o MEEM [8,10]. O MAC quando aplicado por enfermeiros sem uma avaliação cognitiva formal revelou uma sensibilidade baixa, embora mantendo uma especificidade alta [11].
O MAC foi recentemente validado em português, embora no Brasil [12]. A versão validada foi a versão completa e não o algoritmo, mas este é apenas uma forma resumida da versão completa. Por outro lado, tem sido usado por nós desde há cerca de 15 anos.
Por todas estas razões, ser um método simples, validado em português e praticado por nós desde há muito tempo será o método adoptado neste sistema (quadro 2), reconhecendo que não está isento de problemas.
A avaliação destes 2 aspectos da consciência apresentados neste capítulo é que permitirão decidir a forma de avaliação a efectuar, cujas variantes se apresentam nos 2 capítulos seguintes.
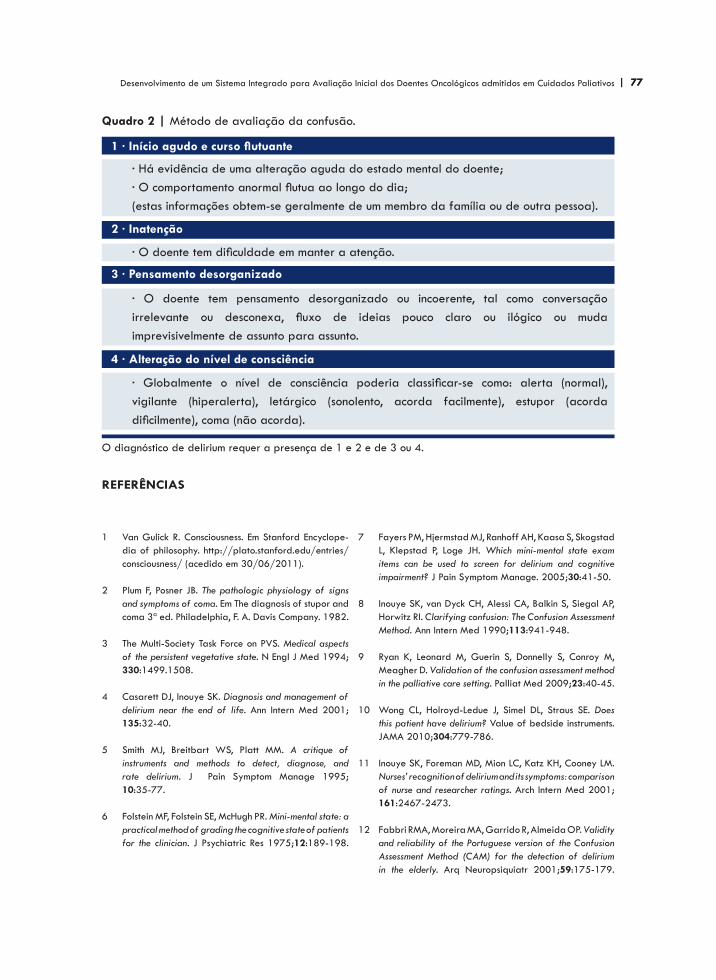
| 77 77Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
· Há evidência de uma alteração aguda do estado mental do doente;· O comportamento anormal flutua ao longo do dia;(estas informações obtem-se geralmente de um membro da família ou de outra pessoa).
Quadro 2 | Método de avaliação da confusão.
· O doente tem pensamento desorganizado ou incoerente, tal como conversação irrelevante ou desconexa, fluxo de ideias pouco claro ou ilógico ou muda imprevisivelmente de assunto para assunto.
· Globalmente o nível de consciência poderia classificar-se como: alerta (normal), vigilante (hiperalerta), letárgico (sonolento, acorda facilmente), estupor (acorda dificilmente), coma (não acorda).
Van Gulick R. Consciousness. Em Stanford Encyclope-dia of philosophy. http://plato.stanford.edu/entries/consciousness/ (acedido em 30/06/2011).
Plum F, Posner JB. The pathologic physiology of signs and symptoms of coma. Em The diagnosis of stupor and coma 3ª ed. Philadelphia, F. A. Davis Company. 1982.
The Multi-Society Task Force on PVS. Medical aspectsof the persistent vegetative state. N Engl J Med 1994;330:1499.1508.
Casarett DJ, Inouye SK. Diagnosis and management ofdelirium near the end of life. Ann Intern Med 2001;135:32-40.
Smith MJ, Breitbart WS, Platt MM. A critique ofinstruments and methods to detect, diagnose, and rate delirium. J Pain Symptom Manage 1995;10:35-77.
Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method of grading the cognitive state of patients for the clinician. J Psychiatric Res 1975;12:189-198.
1
2
3
4
5
6
Fayers PM, Hjermstad MJ, Ranhoff AH, Kaasa S, SkogstadL, Klepstad P, Loge JH. Which mini-mental state exam items can be used to screen for delirium and cognitive impairment? J Pain Symptom Manage. 2005;30:41-50.
Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP,Horwitz RI. Clarifying confusion: The Confusion AssessmentMethod. Ann Intern Med 1990;113:941-948.
Ryan K, Leonard M, Guerin S, Donnelly S, Conroy M, Meagher D. Validation of the confusion assessment methodin the palliative care setting. Palliat Med 2009;23:40-45.
Wong CL, Holroyd-Ledue J, Simel DL, Straus SE. Does this patient have delirium? Value of bedside instruments. JAMA 2010;304:779-786.
Inouye SK, Foreman MD, Mion LC, Katz KH, Cooney LM. Nurses’ recognition of delirium and its symptoms: comparisonof nurse and researcher ratings. Arch Intern Med 2001;161:2467-2473.
Fabbri RMA, Moreira MA, Garrido R, Almeida OP. Validityand reliability of the Portuguese version of the Confusion Assessment Method (CAM) for the detection of delirium in the elderly. Arq Neuropsiquiatr 2001;59:175-179.
7
8
9
10
11
12
· O doente tem dificuldade em manter a atenção.
referências
1 · Início agudo e curso flutuante
2 · Inatenção
3 · Pensamento desorganizado
4 · Alteração do nível de consciência
O diagnóstico de delirium requer a presença de 1 e 2 e de 3 ou 4.
78 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 79 79Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
4AVALIAÇÃO DOS DOENTES SEM ALTERAÇÕES COGNITIVAS

80 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 81 81Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Os doentes em cuidados paliativos têm uma grande variedade de sintomas/problemas. Verificou-se que há uma diferença significativa entre o número de sintomas referidoespontaneamente e o número detectado quando os doentes são sistematicamente interrogados, sendo maior este último [1]. A diferença não foi igual para todos os tiposde sintomas. Assim, sintomas como dor, alterações intestinais, náuseas e vómitos e problemas de mobilidade foram mais frequentemente referidos espontaneamente, enquanto sintomas como fadiga, perda de apetite, perda de peso e edemas foram mais frequentemente detectados quando interrogados. Pode haver várias razões para isso, sendo uma forte hipótese o facto de os doentes atribuírem mais importância a uns sintomas do que a outros, quer porque uns têm uma maior influência no seu bem-estardo que outros quer porque não atribuem importância a outros por os considerarem inevitáveis na sua situação ou porque os atribuem a outros factores, como a idade, por exemplo. Desta observação se pode concluir que, por um lado, é importante fazer uma avaliação sistemática de sintomas e outros problemas e, por outro lado, não é necessário fazer uma avaliação abrangente na fase inicial porque os doentes não atribuem a mesma importância a todos os sintomas/problemas. Acresce a circunstância de na avaliação inicial poder não haver possibilidade ou conveniência de se fazer essa avaliação abrangente pelas razões já aduzidas na introdução.
Na literatura de cuidados paliativos encontram-se, como já foi referido, muitosinstrumentos de avaliação que, embora naturalmente incluam problemas comuns, como a dor, incluem uma variedade grande de sintomas/problemas e são assim muito diferentes em termos de conteúdo e extensão. Para exemplificar essa variedade mostram-se no anexo 1 os sintomas/problemas físicos incluídos em 10 instrumentos. Em face desta diversidade considerou-se que havia espaço para evoluir.
avaliação dos doentes sem alterações cognitivas

82 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Para cumprir a finalidade deste sistema, expressa na introdução, há que reduzir o número de sintomas/problemas a avaliar ao essencial para a primeira avaliação, independentemente de avaliações subsequentes. O método escolhido para a selecção dos sintomas/problemas foi o método de Delfos.
| 83 83Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
O método de Delfos foi desenvolvido nos anos 50 do século XX pela Companhia Rand de Santa Monica, California, com fins militares [2]. O nome deriva do Oráculo de Delfos da Grécia antiga onde as sacerdotisas de Apolo, as Pitonisas, faziam profecias. As profecias do oráculo são “predições não refutáveis, porque não têm a propriedade de serem verdadeiras ou falsas”[2].
O método de Delfos é uma forma de estudo de assuntos controversos. É uma forma de obter consensos através da opinião de peritos que individual e anonimamente respondem às questões colocadas em duas ou mais voltas [3]. Ao fim de cada volta os peritos envolvidos recebem um sumário das respostas de todos os outros e têm a oportunidade de reconsiderar as suas respostas e eventualmente de as modificar na volta seguinte. As vantagens do método de Delfos na obtenção de consensos residem:
·
·
·
o método de delfos
No facto de os peritos poderem exprimir as suas opiniões sem contrangimentos, isto é, anonimamente e sem discussão directa com outros peritos, não conduzindo a um eventual predomínio das opiniões de quem tem uma personalidade dominante ou de quem se expresse com mais facilidade; Em poder-se fazer por correio electrónico, não havendo, portanto, limitações geográficas; Por ser mais barato já que não é necessário fazer reuniões num determinado local, com os custos inerentes, por se fazer por correio electrónico.
84 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
O método de Delfos é uma técnica de investigação flexível que tem sido aplicado de formas variadas de acordo com os objectivos do projecto de investigação [4]. Por todas estas razões, o uso do método de Delfos tem vindo a expandir-se na medicina em geral e em particular em cuidados paliativos [5,6].
A primeira fase
O primeiro passo foi uma revisão extensa da literatura de cuidados paliativos relevantepara a finalidade do estudo. Foi construída uma lista dos problemas/sintomas a partir de instrumentos conhecidos e validados como: Rotterdam Symptom Checklist [7], The Memorial Symptom Assessment Scale Short Form [8], Problems and Needs in Palliative Care Questionnaire - short form [9], Edmonton Symptom Assessment Scale (ESAS) [10], The European Organization for Research and Treatment of Cancer QLQ-30 [11], the Needs Near the End-of-Life Care Screening Tool [12], o M. D. Anderson Symptom Inventory [13], o Cancer Rehabilitation Evaluation System - Short Form (CARES-SF) [14] entre outros [15-17]. Foram consideradas escalas desenvolvidas para a avaliação da qualidade de vida, como a EORTC QLQ-C15-PAL [18] e a Hospice Quality of Life Index [19] desenvolvidas especificamente para cuidados paliativos. Foram também considerados estudos sobre a prevalência de sintomas/problemas no cancro avançado a vários níveis [20-23]. Foram ainda analisados instrumentos específicos de algumas dimensões. Por exemplo, relativamente à espiritualidade foi analisada a Spiritual Transformation Scale [24]. Foram estudados outros instrumentos, mas verificou-se que não acrescentavam nova informação, visto que os mesmos itens se repetiam, embora com composições diversas.
Foi feita uma lista abrangente com base nos problemas contidos nesses instrumentos, excluindo alguns que eram evidentemente menos relevantes de modo a manter a lista num tamanho manejável e, nos casos em que havia termos equivalentes escolheram-se os que aparentemente seriam de mais fácil compreensão.
A lista continha uma pergunta aberta geral “o que é que o incomoda mais?” Esta perguntaera já utilizada há vários anos na avaliação inicial na nossa unidade de cuidados paliativos como forma de hierarquizar as prioridades do ponto de vista do doente, mas é suportada também pelo estudo de Shah et al. [25]. De forma semelhante o estudo de Hoekstra et al. também mostra que determinar qual o sintoma mais perturbador tem um valor adicional relativamente à determinação apenas da presença e intensidade dos sintomas [26].
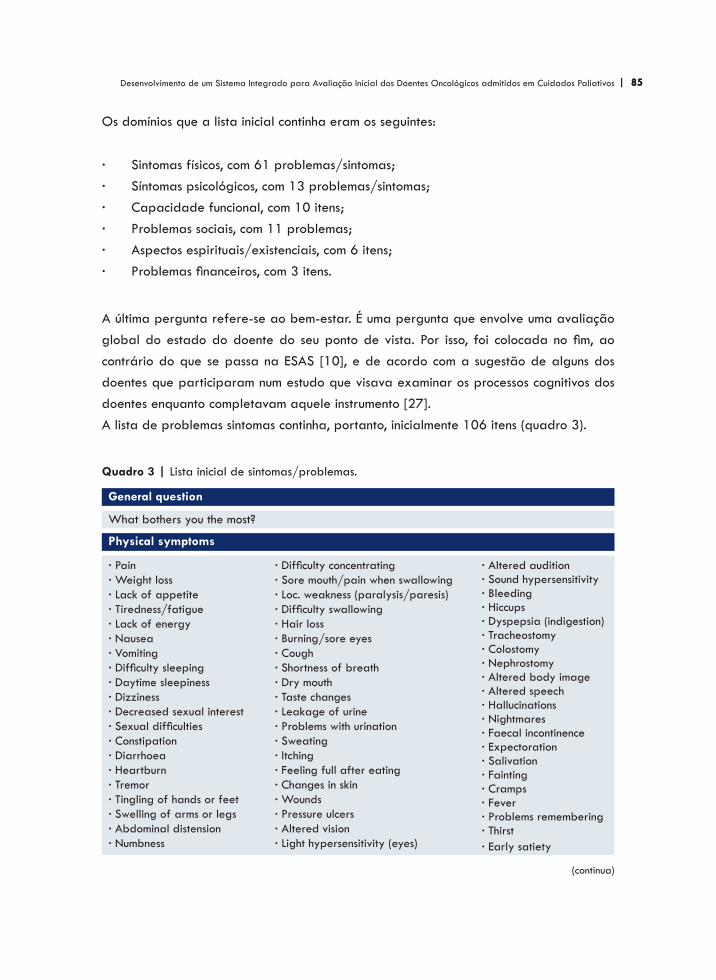
| 85 85Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Os domínios que a lista inicial continha eram os seguintes:
Sintomas físicos, com 61 problemas/sintomas;Síntomas psicológicos, com 13 problemas/sintomas;Capacidade funcional, com 10 itens;Problemas sociais, com 11 problemas;Aspectos espirituais/existenciais, com 6 itens;Problemas financeiros, com 3 itens.
A última pergunta refere-se ao bem-estar. É uma pergunta que envolve uma avaliação global do estado do doente do seu ponto de vista. Por isso, foi colocada no fim, ao contrário do que se passa na ESAS [10], e de acordo com a sugestão de alguns dos doentes que participaram num estudo que visava examinar os processos cognitivos dos doentes enquanto completavam aquele instrumento [27]. A lista de problemas sintomas continha, portanto, inicialmente 106 itens (quadro 3).
·
·
·
·
·
·
What bothers you the most?
Quadro 3 | Lista inicial de sintomas/problemas.
· Pain· Weight loss· Lack of appetite· Tiredness/fatigue· Lack of energy· Nausea· Vomiting· Difficulty sleeping· Daytime sleepiness· Dizziness· Decreased sexual interest · Sexual difficulties· Constipation· Diarrhoea· Heartburn· Tremor· Tingling of hands or feet· Swelling of arms or legs· Abdominal distension· Numbness
· Difficulty concentrating· Sore mouth/pain when swallowing· Loc. weakness (paralysis/paresis)· Difficulty swallowing· Hair loss· Burning/sore eyes· Cough· Shortness of breath· Dry mouth· Taste changes· Leakage of urine· Problems with urination· Sweating· Itching · Feeling full after eating· Changes in skin· Wounds· Pressure ulcers· Altered vision· Light hypersensitivity (eyes)
General question
· Altered audition· Sound hypersensitivity· Bleeding· Hiccups· Dyspepsia (indigestion)· Tracheostomy· Colostomy· Nephrostomy· Altered body image· Altered speech· Hallucinations· Nightmares· Faecal incontinence· Expectoration· Salivation· Fainting· Cramps· Fever· Problems remembering· Thirst· Early satiety
Physical symptoms
(continua)

86 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
· Care for yourself (dress, wash, etc)· Walk at home· Light housework· Climb stairs· Heavy housework· Walk out of doors· Shopping· Go to work· Hobbies· Not being able to do the things you used to do
Physicological symptoms/problems
· Irritability· Worrying· Depression · Nervousness· Despairing about the future· Tension· Anxiety · Sadness· Fear of future· Fear of suffering· Loss of autonomy· Distress· Worrying about work
Activity level
· Problems in the relationship with companion· Difficulties in talking about the disease with the companion· Difficulties of communication with the companion· Difficult interaction with the companion· Neglected by the companion· Support from family/friends· Difficulties in talking about the disease· Difficulties in finding someone to talk· Difficulties in the contact with family and friends· Loneliness· Housing problems
· Extra expenses because of the disease· Loss of income because of the disease· Financial difficulties
· Belief/faith (Do you have religious belief/faith?)· Importance of the belief/faith· Importance of addressing this issues· Difficulties in accepting the disease· Feelings of guilt· Feelings of shame
· Well-being
Social issues
Spiritual issues
Finantial problems
Overall quality of life
A aplicação do método de Delfos
Esta longa lista inicial, incomportável para uma avaliação útil e eficaz foi então submetida a um processo de selecção utilizando a técnica de Delfos.
Os critérios de selecção dos peritos a convidar para participar no processo foi seremmédicos envolvidos em cuidados paliativos e serem bem conhecidos internacionalmentepor terem publicado vários estudos no âmbito dos cuidados paliativos. Segundo estes critérios foram abordados 20 médicos por correio electrónico convidando-os a participar. O texto enviado foi o seguinte:

| 87 87Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Dear Colleague,
There are many tools to assess the problems and symptoms of patients in palliative care. As you know, they are very different and to illustrate this point I am sending attached a table which includes only the physical symptoms of a few of those tools. Therefore, we feel that there is room to improvement.In my unit we have a particular research question which is: what should be assessed in the first contact with a palliative care patient? Why this question? Patients contact palliative care in very different conditions at the consciousness, cognitive, emotional, performance status and symptom burden levels. The patient can be insecure or anxious, particularly in this situation of change from a curative paradigm to a palliative one. Therefore, a comprehensive assessment can be a burden to the patient. There is also the problem of all the work that must be done in a busy unit. However, the main problems should not be missed. For now, our focus is cancer patients without cognitive failure. The objective is to develop a screening tool that must be short, not time consuming, but able to detect the main problems of those patients in the first encounter, despite the assessment of other problems/symptoms in a later moment.With this aim we have made an extensive review of the literature. From this review a long list of problems/symptoms resulted. To shorten it to the essential ones we believe that a good way would be a consensus and among the different methods to reach a consensus the Delphi method would be the most reasonable. Probably two rounds will be needed to reach the consensus.As you are a recognized expert in the field of palliative care I am kindly asking for your help in our project. I hope you accept. In that case, I will send you the list of the problems/symptoms.
Warmest regards.
Desses 20 médicos, 13 aceitaram participar. As suas nacionalidades são as seguintes: alemã: 1; canadiana: 1; espanhola: 3; francesa: 1; inglesa: 1; italiana: 2; norueguesa: 2;sueca: 1; suíça:1. A lista de sintomas/problemas foi enviada pedindo a cada médico que pontuasse numa escala de 0 a 10 cada sintoma/problema quanto à sua relevância para a avaliação dos doentes em cuidados paliativos (anexo 2).

88 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Considerou-se que foi atingido o consenso nos casos em que a média das pontuações foi ≥ 8 ou <5, sendo que os primeiros foram incluídos e os segundos excluídos. Nos casos que se situaram entre os dois valores considerou-se que não havia consenso, tendo a lista dos sintomas/problemas sem consenso sido enviada para uma segunda ronda. Nesta ronda foi enviada também a informação sobre a média das pontuações do próprio médico e as respostas dos outros membros do painel. Um exemplo desse processo pode ver-se no anexo 3. Com as respostas da segunda ronda não foi incluído nenhum sintoma/problema, mas foram excluídos muitos, usando os mesmos critérios da primeira ronda. Para não perpetuar o processo, na terceira ronda foi pedido que a resposta fosse de sim ou não, com a concordância de todos os peritos. Os sintomas/problemas cujo número de sins foi maioritário, isto é ≥ 7 foram incluídos e os outros excluídos. Foi feita uma lista final com os sintomas/problemas incluídos nas três rondas (quadro 4).
Quadro 4 | Lista final.
General question
What brothers you the most?
Physical symptoms
· Pain· Lack of appetite· Vomiting· Tiredness/fatigue· Nausea· Constipation· Shortness of breath
Psychological symptoms/problems
· Depression · Anxiety · Difficulty sleeping
Activity level
Care for yourself (dress, wash, etc)
Social issues
Support from family/friends
Overall quality of life
Well-being

| 89 89Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
A lista foi construída em inglês para permitir a intervenção dos médicos estrangeiros. Foi depois submetida a uma tradução para português por uma pessoa cuja língua mãe é o português e de novo retrovertida para inglês por uma pessoa cuja língua mãe é o inglês, sendo que ambos têm conhecimentos extensos da outra língua. A tradução e a retroversão não produziram resultados controversos que necessitassem de outras intervenções.
Aos itens deste instrumento é possível adicionar um ou mais sintomas/problemas que os doentes considerem importantes no seu caso particular. A aplicação prática dos itens seleccionados será feita numa escala tipo Likert de cinco pontos. Decidiu-se avaliar os sintomas do ponto de vista da influência que têm no bem-estar e não na sua intensidade, porque na realidade é isso que mais interessa (quadro 5). Os termos usados na escala foram submetidos à apreciação de médicos e enfermeiros do serviço, que sugeriram algumas alterações. Foram aceites as que pareceram melhorar a escala.
Quadro 5 | Forma final do instrumento.
Avaliação inicial de sintomas/problemas
Durante a última semana quais foram os sintomas ou problemas que o incomodaram?
O que o incomoda mais? Nada Um pouco Bastante Muito Muitíssimo
DorFalta de apetiteVómitosCansaço/FadigaNáuseas/EnjoosObstipação/Prisão de ventreFalta de arDepressão/TristezaAnsiedade/NervosismoDificuldade em dormirOutro:
NadaNadaNadaNadaNadaNadaNadaNadaNadaNadaNada
Um poucoUm poucoUm poucoUm poucoUm poucoUm poucoUm poucoUm poucoUm poucoUm poucoUm pouco
BastanteBastanteBastanteBastanteBastanteBastanteBastanteBastanteBastanteBastanteBastante
MuitoMuitoMuitoMuitoMuitoMuitoMuitoMuitoMuitoMuitoMuito
MuitíssimoMuitíssimoMuitíssimoMuitíssimoMuitíssimoMuitíssimoMuitíssimoMuitíssimoMuitíssimoMuitíssimoMuitíssimo
Cuidar de sí (vestir-se, lavar-se, etc)
Independente Com dificuldade Só com ajuda Muito pouco Incapaz
Apoio da família/amigos
Total Bastante Quando peço Pouco Nenhum
Bem-estar
Excelente Bom Razoável Mau Muito mau
90 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Há ainda a decidir se esta parte do sistema será feita por autoavaliação ou com assistência de profissionais como sugerido por doentes incluídos num estudo do ESAS [27]. É também da experiência de outros estudos realizados por nós em Portugal que os doentes preferem que sejam os profissionais a fazer as perguntas e a preencher os formulários [28].

| 91 91Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Neste estudo foram incluídos 13 médicos peritos em cuidados paliativos. O número apropriado de peritos a envolver num estudo de Delfos não obtem consenso na literatura [29]. De facto, há grandes diferenças entre os estudos. Um número de 10 a 15 peritos pode ser adequado se tiverem uma experiência homogénea no assunto em causa [29]. No caso presente é isso mesmo que se passa, pelo que o número de peritos pode considerar-se suficiente.
Este processo produziu um instrumento de avaliação inicial dos doentes admitidos em cuidados palitivos sem alterações cognitivas que inclui os sintomas/problemas incluidos na maioria dos instrumentos semelhantes, excluindo muitos outros cuja relevância não foi considerada suficiente para a finaliadade em vista. No entanto, a possibilidade de incluir outros itens que pertubem um ou outro doente resolve a questão da grande diversidade de problemas que podem afectar os doentes.
Um instrumento semelhante é a ESAS [10] que tem 10 itens. A ESAS é provavelmente o instrumento mais usado em cuidados paliativos. Embora haja semelhanças entre os dois instrumentos eles não são idênticos. A ESAS não inclui sintomas como vómitos, fadiga, obstipação e dificuldade em dormir. Por outro lado, o presente instrumento não inclui os itens sonolência e “distress”. A ESAS também não inclui a dimensão social e trata de modo diferente a actividade. É de notar que estes dois instrumentos têm finalidades diferentes. A ESAS é um instrumento que foi desenvolvido para ser aplicado diariamente (na realidade em Edmonton onde foi desenvolvida é aplicada duas vezes por dia), para a avaliação dos sintomas físicos e psicológicos, embora já tenha sido usado com outras finalidades, por exemplo, como um instrumento de auditoria [30]. O presente instrumento,
discussão
92 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
porém, foi construído para a avaliação inicial dos doentes admitidos em cuidados paliativos, o que pode explicar algumas das diferenças.
Os sintomas físicos e psicológicos seleccionados são naturalmente dos mais frequentes como mostram vários estudos de prevalência de sintomas no cancro avançado [20-23]. Duas dimensões foram completamente excluídas: a espiritual e a financeira. Não é claro porque o foram, mas é certo que não foram consideradas suficientemente relevantes para avaliação no primeiro encontro. Não que fossem consideradas dimensões menores na avaliação dos doentes. Talvez se tenha considerado que no primeiro encontro não há intimidade suficiente para se abordarem essas questões, sobretudo no que diz respeito às questões espirituais, podendo ser abordadas mais tarde.
O caso particular dos problemas psicológicos
A National Comprehensive Cancer Network define “distress” como uma experiência emocional desagradável que se estende ao longo de uma continuidade que vai de sentimentos normais comuns de vulnerabilidade, tristeza e receios, a problemas que se podem tornar incapacitantes, como depressão, ansiedade, pânico, isolamento social e crises existenciais e espirituais [31]. Ora são estes que interessa detectar e, de facto, o foco de atenção tem sido nos diagnósticos psiquiátricos convencionais como a depressão.
A prevalência da depressão nos doentes com cancro avançado, segundo a literatura, varia entre 3,7% e 58% [32]. Esta disparidade de números reflecte bem o problemada detecção da depressão nestes doentes. De facto, os critérios de diagnóstico de depressão incluem sintomas físicos, como alterações do apetite, astenia e alterações do sono são comuns nestes doentes devido à própria doença. Por outro lado, a tristeza é um sintoma comum nos doentes com cancro avançado, sendo uma manifestação normal dada a situação difícil com que os doentes se confrontam. No entanto, a tristeza por si só não significa depressão, embora comummente se associem os termos. Sabe-se também que mais de 50% dos problemas psicológicos não são detectados por rotina em contextos médicos [33].
A importância da detecção da depressão reside na possibilidade de a tratar e no impacto negativo que tem na qualidade de vida dos doentes e das suas famílias quando presente.
| 93 93Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Existem vários questionários de extensão variável para o rastreio da depressão, mas poucos foram validados em cuidados paliativos. Numa revisão feita por um grupo de trabalho de peritos para a Associação Europeia de Cuidados Paliativos concluiu-seque a evidência actual não permite recomendar nenhum método de rastreio da depressão para cuidados paliativos [32]. A validação destes questionários deverá ser feita por comparação com um gold standard. No caso da depressão o método que mais se aproxima de um gold standard é a entrevista psiquiátrica [32]. No entanto, este é um recurso moroso, que poucos dominam e, portanto, pouco adequado como método de rastreio. De acordo com o objectivo do instrumento aqui desenvolvido, o método de rastreio deve basear-se num número de perguntas o mais pequeno possível. O resultado obtido resultou numa só pergunta, como no estudo de Chochinov et al [34]. Neste estudo,a pergunta: “Está deprimido(a)?” atingiu uma sensibilidade e especificidade de 100%. No entanto, estes resultados não foram replicados noutros estudos, o que pode ter sido influenciado por razões culturais [35]. A definição de depressão no estudo de Chochinov et al. incluía a depressão minor. Portanto, o que se determinou foi a capacidade de detectar humor deprimido e não apenas casos de depressão major [36]. Payne et al. estudaram a sensibilidade e a especificidade de duas perguntas: “Está deprimido(a)?” e “Perdeu interesse em coisas ou actividades de que normalmente gostava?” [37]. Neste estudo a combinação das duas perguntas mostrou uma sensibilidade de 90,7% e uma especificidade de 72,6%. Por se tratar de um método de rastreio, a sensibilidade deve ser privilegiada em relação à especificidade pelo que aquela especificidade pode ser aceitável.
A inclusão de um item que aborde a questão do humor deprimido é importante. A pergunta é usada como rastreio e não para diagnóstico. O humor deprimido é um elemento essencial no diagnóstico de depressão segundo, por exemplo, o Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) [38]. Não há depressão sem humor deprimido, portanto, a pergunta sobre o humor é fundamental num instrumento de rastreio da depressão.

94 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
referências
White C, McMullan D, Doyle J. Now that you mentionit, doctor: symptom reporting and the need for systematic questioning in a specialist palliative care unit. J Palliat Med 2009;12: 447-450.
Delphi method. http://www.u ido.org/fileadmin/import/16959_DelphiMethod.pdf (acedido em 02/06/11).
Fink A, Kosecoff J, Chassin M, Brook RH. Consensusmethods: characteristics and guidelines for use. Am J Public Health 1984;74:979-983.
Skulmoski GJ, Hartman FT, Krahn J. The Delphi methodfor graduate research. J Inform Technol Ed 2007;6:1-21.
Pigni A, Brunelli C, Gibbins J, Hanks G, DeConno F, Kaasa S, Klepstad P, Radbruch L, Caraceni A. Contentdevelopment for European guidelines on the use of opioids for cancer pain: a systematic review and expert consensus study. Minerva Anestisiol 2010;76:833-843.
Biondo PD, Nekolaichuk CL, Stiles C, Fainsinger R, HagenNA. Applying the Delphi process to palliative care tool development: lessons learned. Support Care Cancer 2008;16:935-942.
de Haes JCJM, Olschewski, Fayers P, Visser MRM, Cull A, Hopwood Sanderman R. The Rotterdam SymptomChecklist (RSCL): a manual. Northern Centre for Healthcare Research. University of Groningen, The Netherlands; 1966.
Chang VT, Hwang SS, Feuerman M, Kasimis BS, ThalerHT. The Memorial Symptom Assessment Scale Short Form (MSAS-SF) Cancer 2000;89:1162-1171.
Osse BHP, Vernooij-Dassen MJFJ, Schadé E, Grol RPTM. A practical instrument to explore patients’ needs inpalliative care: the Problems and Needs in PalliativeCare questionnaire - short version. Palliat Med 2007;21:391-399.
Chang VT, Hwang SS, Feuerman M. Validation of the Edmonton Symptom Assessment Scale. Cancer 2000;88:2164-2171.
Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993;85:365-376.
1
2
3
4
5
6
7
8
9
10
11
Emanuel LL, Alpert HR, Emanuel EE. Concise screeningquestions for clinical assessment of terminal care: the Needs Near the End-of-Life Care Screening Tool. J Palliat Med 2001;4:465-474.
Cleeland CS, Mendonza TR, Wang XS, Chou C, Harle MT, Morrisey M, Engstrom MC. Assessing symptom distress in cancer patients. Cancer 2000;89:1634-1646.
Schag CAC, Ganz PA, Heinrich RL. Cancer Rehabilitation Evaluation System - Short Form (CARES-SF): a cancer specificrehabilitation and quality of life instrument. Cancer 1991;68:1406-1413.
Barresi MJ, Shadbolt Byrne D, Stuart-Harris R. The development of the Canberra symptom scorecard: a tool to monitor the physical symptoms of patients with advanced tumours. BMC Cancer 2003;3:32.
Hoekstra J, Bindels PJE, van Duijn NP, Shadé E. The symptommonitor. A diary for monitoring physical symptoms for cancer patients in palliative care: feasibility, reliability and compliance. J Pain Symptom Manage 2004:27:24-35.
Berry DL, TRigg LJ, Lober WB, Karras TB, Galligan ML, Austin-Seymour M, Martin S. Computerized symptom and quality-of-life assessment for patients with cancer part 1: development and pilot testing. Oncol Nurs Forum 2004;31:E75-E83.
Groenvold M, Petersen MA, Agronson NK, et al. The development of the EORTC QLQ-C15-PAL. Eur J Cancer 2006;42:55-64.
McMillan SC, Mahon M. Measuring quality of life in hospicepatients using a newly developed Hospice Quality of Life Index. Qual Life Res 1994;3:437-447.
Teunissen SCCM, Wesker W, Kruitwagen C, de Haes HCJM,Voest EE, Graeff A. Symptom prevalence in patients with incurable cancer: a systematic review. J Pain Symptom Manage 2007;34:94-104.
Strömgren AS, Groenvold M, Pedersen L, Olsen AK, Sjogren P. Symptomatology of cancer patients in palliative care: content validation of self-assessment questionnaires against medical records. Eur J Cancer 2002;38:788-794.
12
13
14
15
16
17
18
19
20
21

| 95 95Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Jiménez-Gordo AM, Feliu J, Martínez B, et al. Descriptiveanalysis of clinical factors affecting terminally ill cancer patients. Support Care Cancer 2009;17:261-269.
Lidstone V, Butters E, Seed PT, Sinnot C, Beynon T, Richards M. Symptoms and concerns amongst cancer outpatients: identifying the need for specialist palliative care. Palliat Med 2003;17:588-595.
Cole BS, Hopkins CM, Tisak J, Steel JL, Carr BI. Assessingspiritual growth and spiritual decline following a diagnosis of cancer: reliability and validity of the spiritual transformation scale. Psycho-Oncology 2008;17:112-121.
Shah M, Quill T, Norton S, Sada Y, Buckley M, Fridd C. What bothers you most? Initial responses from patients receiving palliative care consultation.Am J Hosp Palliat Care 2008;25:88-92.
Hoekstra J, Vernooij MJFJ, de Vos R, Bindels PJE. Theadded value of assessing the most troublesome symptomamong patients with cancer in the palliative phase. PatientEduc Counsel 2007;65:223-229.
Watanabe S, Nekolaichuk C, Beaumont C, Mawani A. The Edmonton symptom assessment system - what do patients think? Support Care Cancer 2009;17:675-683.
Ferraz Gonçalves, Marques A, Rocha S, Leitão P, Mesquita T, Moutinho S. Breaking bad news: experiencesand preferences of advanced cancer patients at a Portuguese oncology centre. Palliative Medicine 2005; 19: 526-/531.
Hsu CC, Sandford BA. The Delphi technique: making sense of consensus. Practical Assessment, Research and Evaluation 2007;12:10.
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
Dudgeon DJ, Harlos M, Clinch JJ. The Edmonton Assessmente Scale (ESAS) as an audit tool. J Palliat Care 1999;15:14-19.
National Comprehensive Cancer Network. Clinical practice guidelines in oncology v.1. 2009. http://www.nccn.org/professionals/physician_gls/PDF/distress.pdf. (acedido em 18/05/2009).
Stiefel F, Trill Md, Berney A, Olarte JMN, Razavi D.Depression in palliative care: a pragmatic report from the Expert Working Group of the European Association for Palliative Care. Support Care Cancer 2001;9:477-488.
Thekkumpurath P, Venkateswaran C, Kumar M, Bennet MI.Screening for psychological distress in palliative care: a systematic review. J Pain Symptom manage 2008;36:520.528.
Chochinov HM, Wilson KG, Enns M, Lander S. Are youdepressed? Screening for depression in the terminally ill. Am J Psychiatry. 1997;154:674-676.
Lloyd-Williams M, Spiller J, Ward J. Which depression screening tools should be used in palliative care? Palliat Med 2003;17:40-43.
Rayner L, Loge JH, Wasteson E, Higginson I. The detectionof depression in palliative care. Curr Opin Support PalliatCare 2009;3:55-60.
Payne A, Barry S, Creedon B, Stone C, Sweeney C,O’Brien T, O’Sullivan K. Sensitivity and specificity of a two-question screening tool for depression in a specia-list palliative care unit. Palliat Med 2007;21:193-198.
http://emedicine.medscape.com/article/286759 overview (acedido em 13/05/2010).

96 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 97 97Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
5AVALIAÇÃO DOS DOENTES COM ALTERAÇÕES COGNITIVAS

98 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 99 99Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Há pessoas com alterações cognitivas que ainda assim são capazes de comunicar os seus problemas de modo suficientemente claro. No entanto, muitas dessas pessoas não são capazes de o fazer [1].
A natureza subjectiva dos sintomas torna o relato do doente a melhor forma de avaliar os seus sintomas/problemas. Quando as alterações cognitivas não o permitem fazer é necessário utilizar outros meios. Uma alternativa é a avaliação por um familiar ou outra pessoa próxima. No entanto, parece que esta forma de avaliação só é útil se houver um contacto regular como o/a doente [2]. Outro problema que este método acarreta é a necessidade da presença dessas pessoas na altura da avaliação, o que torna o método problemático.
A alternativa mais usada é a avaliação comportamental. Seguindo esta linha, foram desenvolvidos vários instrumentos para avaliar doentes com alterações cognitivas. A maioria concentra-se no problema da avaliação da dor [3-9]. Há também instrumentos desenvolvidos para a avaliação de outros sintomas [10], para avaliar a qualidade de vida [11-14] e para a detecção do sofrimento em geral [15,16]. Muitos dos estudos realizados para avaliação dos sintomas/problemas dos doentes com alterações cognitivas centraram-se nos doentes com demências [2,6-17], em doentes com alterações cognitivas de outra causa [5] e nos doentes em cuidados intensivos [18].
Esses instrumentos avaliam os sintomas/problemas pelas expressões faciais, actividade,humor, interacção social, comportamento vocal, etc. Como foi referido a maioria foi desenvolvida para avaliação da dor. No entanto, há muitos outros sintomas para além
avaliação dos doentes com alterações cognitivas
100 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
da dor. Uma dificuldade inerente à avaliação destes sintomas em doentes que não podem dizer o que sentem é a de saber se as manifestações de sofrimento inferidas por esses instrumentos se devem a dor ou a qualquer outro tipo de causa física ou afectiva ou mesmo às próprias alterações cognitivas.
Depois de se ter considerado o exposto no parágrafo anterior, o primeiro passo deverá ser determinar se o doente tem ou não manifestações de desconforto ou sofrimento. Se as tiver, as possibilidades de inferir a causa serão através da história anterior às alterações cognitivas colhida através dos familiares ou da informação clínica que eventualmente acompanhe o doente e do exame físico. Haverá, certamente, situações em que não será possível chegar a uma conclusão sobre a causa do sofrimento manifestado pelo doente.
Os instrumentos até agora desenvolvidos revelaram fragilidades de vária ordem, incluindo as suas propriedades psicométricas e utilidade clínica [3,19]. Por esse motivo tentou-se desenvolver um outro método de avaliação. De acordo com a finalidade geraldeste sistema pretendeu-se detectar sinais de sofrimento que necessitassem de uma exploração posterior ou se esses sinais estavam ausentes e nenhuma intervenção diferente das que estavam em curso necessitaria de ser executada.

| 101 101Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Métodos
O primeiro passo foi fazer uma revisão extensa da literatura para verificar se existiria alguminstrumento que pudesse estar validado e pudesse ser usado na avaliação dos doentes, tendo-se detectado os problemas já referidos. No entanto, esses instrumentos foramusados para seleccionar os elementos que vieram a constituir o presente instrumento.
Os elementos escolhidos para a construção do instrumento foram a expressão facial, a vocalização e as reacções físicas (quadro 6). Estes elementos pareceram os mais adequados, eliminando-se aspectos sociais que se mostraram pouco consistentes em alguns estudos. Os elementos iniciais foram sujeitos a um teste com os 8 investigadores envolvidos, médicos e enfermeiros. Nessa avaliação inicial foram reconhecidos alguns problemas, nomeadamente de compreensão dos itens que compunham o instrumento. Foi corrigido o que segundo a avaliação inicial havia a corrigir e foram escritas instruções para a sua aplicação (quadro 7).
estudo 1
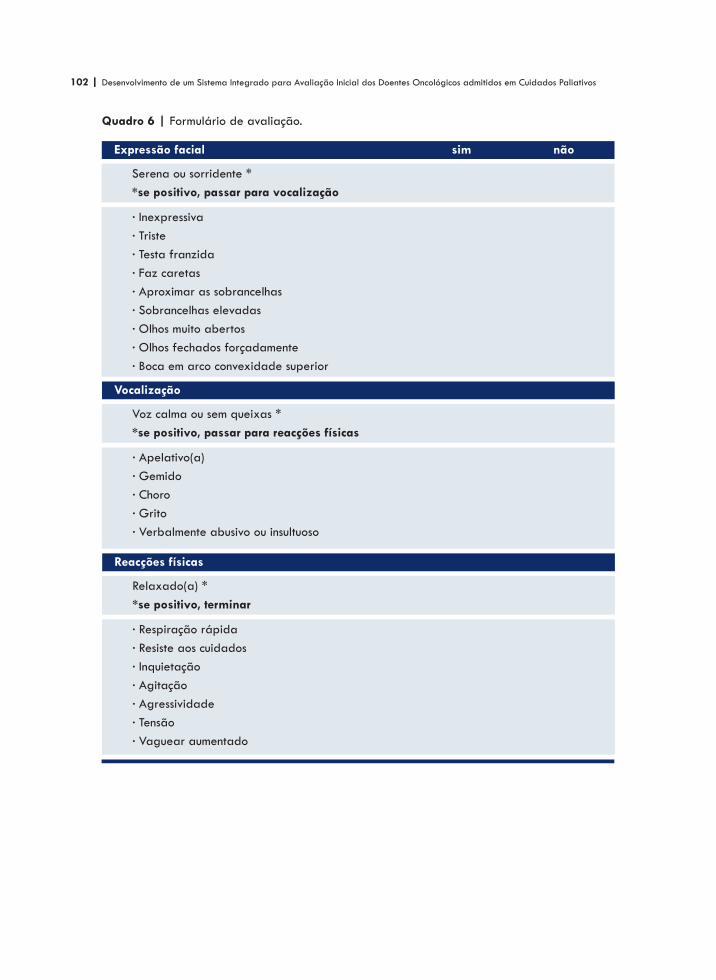
102 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Quadro 6 | Formulário de avaliação.
Expressão facial
Serena ou sorridente **se positivo, passar para vocalização
· Inexpressiva· Triste· Testa franzida· Faz caretas· Aproximar as sobrancelhas· Sobrancelhas elevadas· Olhos muito abertos· Olhos fechados forçadamente· Boca em arco convexidade superior
Vocalização
Voz calma ou sem queixas **se positivo, passar para reacções físicas
· Apelativo(a)· Gemido· Choro· Grito· Verbalmente abusivo ou insultuoso
Reacções físicas
Relaxado(a) **se positivo, terminar
· Respiração rápida· Resiste aos cuidados· Inquietação· Agitação· Agressividade· Tensão· Vaguear aumentado
sim não
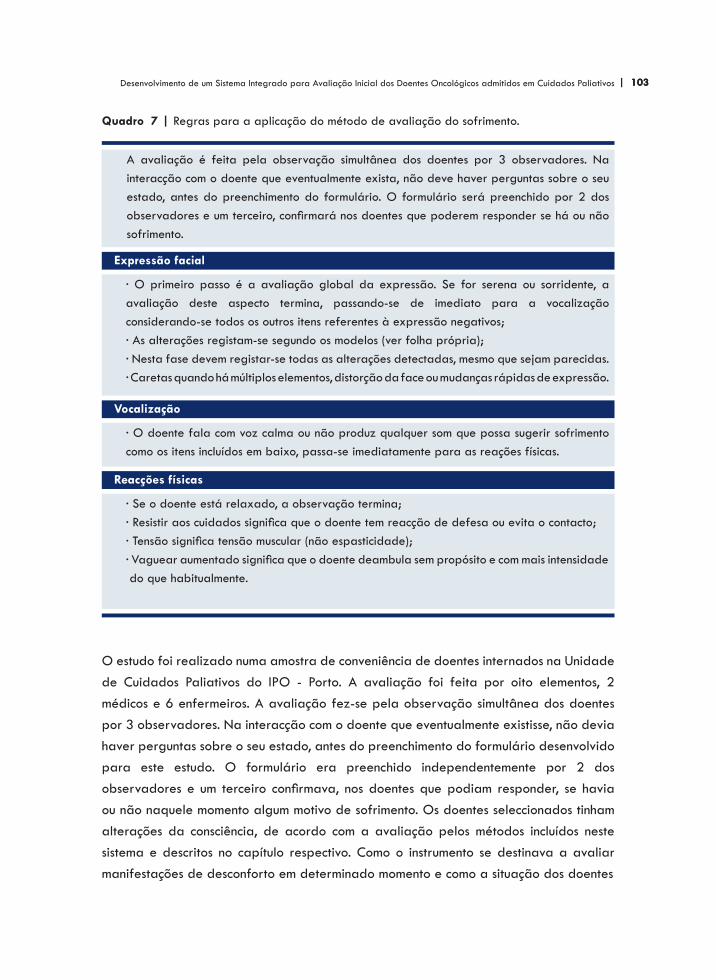
| 103 103Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Quadro 7 | Regras para a aplicação do método de avaliação do sofrimento.
O estudo foi realizado numa amostra de conveniência de doentes internados na Unidadede Cuidados Paliativos do IPO - Porto. A avaliação foi feita por oito elementos, 2 médicos e 6 enfermeiros. A avaliação fez-se pela observação simultânea dos doentes por 3 observadores. Na interacção com o doente que eventualmente existisse, não deviahaver perguntas sobre o seu estado, antes do preenchimento do formulário desenvolvidopara este estudo. O formulário era preenchido independentemente por 2 dos observadores e um terceiro confirmava, nos doentes que podiam responder, se havia ou não naquele momento algum motivo de sofrimento. Os doentes seleccionados tinham alterações da consciência, de acordo com a avaliação pelos métodos incluídos neste sistema e descritos no capítulo respectivo. Como o instrumento se destinava a avaliar manifestações de desconforto em determinado momento e como a situação dos doentes
Expressão facial
A avaliação é feita pela observação simultânea dos doentes por 3 observadores. Na interacção com o doente que eventualmente exista, não deve haver perguntas sobre o seu estado, antes do preenchimento do formulário. O formulário será preenchido por 2 dos observadores e um terceiro, confirmará nos doentes que poderem responder se há ou não sofrimento.
· O primeiro passo é a avaliação global da expressão. Se for serena ou sorridente, a avaliação deste aspecto termina, passando-se de imediato para a vocalização considerando-se todos os outros itens referentes à expressão negativos;· As alterações registam-se segundo os modelos (ver folha própria);· Nesta fase devem registar-se todas as alterações detectadas, mesmo que sejam parecidas.· Caretas quando há múltiplos elementos, distorção da face ou mudanças rápidas de expressão.
Vocalização
· O doente fala com voz calma ou não produz qualquer som que possa sugerir sofrimento como os itens incluídos em baixo, passa-se imediatamente para as reações físicas.
Reacções físicas
· Se o doente está relaxado, a observação termina;· Resistir aos cuidados significa que o doente tem reacção de defesa ou evita o contacto;· Tensão significa tensão muscular (não espasticidade);· Vaguear aumentado significa que o doente deambula sem propósito e com mais intensidade do que habitualmente.

104 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
é dinâmica alterando-se por vezes rapidamente com períodos de tranquilidade e outros de algum desconforto, alguns doentes foram avaliados várias vezes desde que em dias diferentes.
Dado não existir nenhum método que se possa considerar um gold standard, a única possibilidade de confirmar o resultado da avaliação é o relato dos doentes. Deste modo, alguns dos doentes com alterações cognitivas que tinham a possibilidade de responder, pelo menos em termos de sim ou não, eram questionados sobre se havia algum factor de sofrimentos na altura da avaliação.
Os métodos estatísticos utilizados para avaliar a concordância entre os avaliadores foram o coeficiente kappa de Cohen [20] e as proporções de concordância positiva e negativa [21]. Foi ainda determinada a sensibilidade, a especificidade e os valores preditivos positivo e negativo.
O estudo foi aprovado pela Comissão de Ética e pelo Conselho de Administração do IPO - Porto. Sempre que possível era pedida autorização aos familiares, por escrito, após esclarecimento da finalidade do estudo. Porém, dado que não era possível em muitos casos fazê-lo e como o estudo não envolvia nenhuma manobra invasiva nem qualquer esforço e, por outro lado, podia ter vantagem directa e imediata para os doentes, muitos doentes foram envolvidos sem a autorização da família à luz da doutrina do consentimento presumido.
Resultados
O estudo decorreu entre 07/04/2011 e 13/05/2011, tendo sido feitas 75 observações, numa base de conveniência, em 24 doentes, cujos dados demográficos se encontram no quadro 8. O número de observações variou entre 1 e 9, mediana 1. Das 75 observações, em 53 (71%) foi possível obter uma resposta: positiva em 19 (36%) e negativa em 34 (64). Das 19 respostas positivas, a dor foi a razão em 13 (68%), mal-estar em 4 (21%), dispneia em 1 (11%) e em 3 (16%) não foi possível obter resposta sobre a razão do desconforto.

| 105 105Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Quadro 8 | Dados demográficos.
Tumor primário
GinecológicoBexigaPulmãoCabeça/pescoçoSNCPróstataMamaVias biliaresOutro
n %
Total
433222224
(17)(13)(13)(8)(8)(8)(8)(8)(8)
24 (100)
Género: MasculinoFemininoIdade: mediana
816
76 anos
(33%)(67%)
(15-90)
O coeficiente kappa revelou uma concordância entre os avaliadores boa, (0,61 a 0,80) segundo Altman [22], apenas no item Apelativo(a) da secção Vocalização. Todos os outros foram inferiores (quadro 9). Nos itens com um coeficiente kappa pelo menos moderado (> 0,40) [22], foram calculadas as proporções de concordância positivas e negativas. Verificou-se que a proporção de concordância positiva foi relativamente baixa, quer dizer, a concordância dos avaliadores sobre a positividade de um item foi baixa, enquanto que a proporção de concordância negativa foi alta e em alguns casos muito alta, atingindo mais de 0,90, muito perto da concordância total que é 1. Quanto ao kappa global, isto é, a comparação da concordância entre todos os itens negativos e a comparação de concordância de haver pelo menos um item positivo foi de -0,09. A sensibilidade do instrumento foi de 21% (IC 95%: 0,10-0,32) e a especificidade de 97% (IC 95%: 0,92-1,00), com um valor preditivo positivo de 80% (IC 95%: 0,68-0,91) e um valor preditivo negativo de 69% (IC 95%: 0,56-0,81).

106 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Quadro 9 | Proporções de concordância.
Expressão facial
Serena ou sorridenteInexpressivaTristeTesta franzidaFaz caretasAproximar as sobrancelhasSobrancelhas elevadasOlhos muito abertosOlhos fechados forçadamenteBoca em arco convexidade superior
Proporção de concordância
K = 0,51; cp = 0,73; cn = 0,79K = 0,02K = 0,41; cp = 0,40; cn = 0,96K = 0,48; cp = 0,53; cn =0,95K = 0,32K = 0,59; cp= 0,69; cn =0,90K = 0,22*K = 0,49; cp = 0,50; cn = 0,99K = 0,42; cp = 0,53; cn = 0,88
K = coeficiente kappa; cp = concordância positiva; cn = concordância negativa* Nestes itens não houve qualquer caso
Vocalização
Reacções físicas
Voz calma ou sem queixasApelativo(a)GemidoChoroGritoVerbalmente abusivo ou insultuoso
K = 0,48; cp = 0,53; cn = 0,95K = 0,65; cp = 0,67; cn = 0,99K = 0,47; cp = 0,50; cn = 0,97***
Relaxado(a)Respiração rápidaResiste aos cuidadosInquietaçãoAgitaçãoAgressividadeTensãoVaguear aumentado
K = 0,50; cp = 0,57; cn = 0,93K = 0,31*K = 0,28K = 0,00*K = 0,28 *

| 107 107Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
estudo 2
Dado a avaliação do instrumento anterior não ter sido satisfatória procurou-se mudar de estratégia realizando outro estudo. Neste estudo procurou-se fazer uma avaliação pelo aspecto global do doente assinalando se apresentava ou não sinais de desconforto.Portanto, há apenas que responder a uma pergunta: o/a doente apresenta sinais de desconforto? Esta avaliação global era já utilizada na Unidade de Cuidados Paliativos do IPO - Porto nos casos de alterações da consciência ou grande dificuldade de comunicação. Com este estudo procurava-se evitar focar a atenção em detalhes que, em geral, não se mostraram consistentes no estudo anterior e fazer a avaliação global, evitando olhar para as árvores focando a atenção na floresta.
Métodos
A estrutura do estudo foi semelhante à do anterior, com 2 investigadores a avaliarem simultaneamente o/a doente, registando de forma independente a sua avaliação. Um terceiro investigador perguntava aos doentes que retinham capacidade de comunicação se na altura se sentiam desconfortáveis. Os investigadores são elementos da Unidade de Cuidados Paliativos do IPO - Porto, 2 médicos e 5 enfermeiros que não tinham participadono estudo 1. Os métodos estatísticos utilizados foram os mesmos do estudo 1.
Resultados
O estudo decorreu entre 12/05/2011 e 30/06/2011. Foram avaliados 32 doentes de 1 a 8 vezes, mediana 2 avaliações, numa base de conveniência, totalizando 64 avaliações. Os dados demográficos podem ver-se no quadro 10. Das 64 observações,
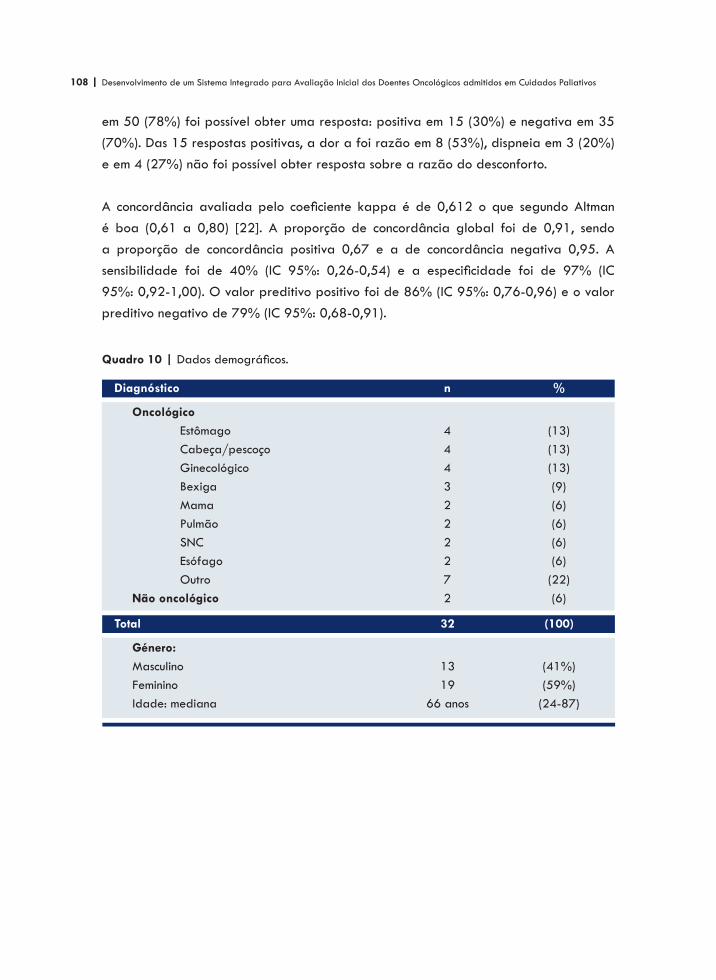
108 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
em 50 (78%) foi possível obter uma resposta: positiva em 15 (30%) e negativa em 35 (70%). Das 15 respostas positivas, a dor a foi razão em 8 (53%), dispneia em 3 (20%) e em 4 (27%) não foi possível obter resposta sobre a razão do desconforto.
A concordância avaliada pelo coeficiente kappa é de 0,612 o que segundo Altman é boa (0,61 a 0,80) [22]. A proporção de concordância global foi de 0,91, sendo a proporção de concordância positiva 0,67 e a de concordância negativa 0,95. A sensibilidade foi de 40% (IC 95%: 0,26-0,54) e a especificidade foi de 97% (IC 95%: 0,92-1,00). O valor preditivo positivo foi de 86% (IC 95%: 0,76-0,96) e o valor preditivo negativo de 79% (IC 95%: 0,68-0,91).
Quadro 10 | Dados demográficos.
Diagnóstico
Oncológico Estômago Cabeça/pescoço Ginecológico Bexiga Mama Pulmão SNC Esófago OutroNão oncológico
n %
Total
4443222272
(13)(13)(13)(9)(6)(6)(6)(6)(22)(6)
32 (100)
Género: MasculinoFemininoIdade: mediana
1319
66 anos
(41%)(59%)
(24-87)
| 109 109Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
discussão
Procurava-se construir um método para avaliação de manifestações de sofrimento em doente sem capacidade de o comunicarem por si próprios. É um assunto que tem sido estudado sobretudo nos doentes com demências para os quais foram desenvolvidos vários instrumentos focados essencialmente na avaliação da dor. Não há nenhum método desenvolvido especificamente para cuidados pliativos. Os Intrumentos até agora desenvolvidos revelaram vários problemas, incluindo a suas propriedade psicométricas e utilidade clínica [3,19]. Numa revisão sistemática das escalas de avaliação da dor em idosos com demência grave concluiu-se que actualmente nenhuma dessas escalas de avaliação pode de modo convincente ser indicado como o mais apropriado para avaliar a dor nos idosos com demência [3].
No referido estudo destacava-se, no entanto, a escala DOLOPLUS-2 [3]. Esta escala foi validada em várias línguas, nomeadamente em português, validação essa para a qual contribuímos [23]. A escala DOLOPLUS [4] foi desenvolvida a partir da escala Douleur Enfant Gustave Roussy para crianças [3]. Esta escala foi tida em conta na construção do instrumento utilizado no Estudo 1, porém excluímos o domínio psicossocial porque se revelou pouco útil e de validade duvidosa [24].
A escala DOLOPLUS tem também uma finalidade diferente do nosso instrumento. Enquanto que pretendíamos avaliar o desconforto num dado momento, porque os sintomas e a sua intensidade variam, por isso é que se prescreve sempre medicação de resgate para administrar se houver um aumento pontual da intensidade dos sintomas. A finalidade de ser incluída no sistema de avaliação inicial dos doentes implica também que a avaliação possa ser feita pelo profissional que estiver presente,
110 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
independentemente de conhecer o doente ou não. Este instrumento deveria também ser utilizado noutros contextos. Pelo contrário a escala DOLOPLUS foi construída para uma avaliação colectiva, pela equipa cuidadora, não num dado momento, e que visa essencialmente monitorizar a evolução individual da dor e do seu controlo ao longo do tempo.
Os resultados dos estudos que realizamos demonstram a dificuldade de avaliar os sintomas/problemas nos doentes com alterações cognitivas. No Estudo 1 verificou-se que a concordância entre os avaliadores pelo coeficiente kappa era inferior a moderada na maioria dos itens segundo Altman [22], apenas com um item com uma concordância boa. No entanto, a concordância negativa foi em muitos casos superior a 90% o que significa que quando esses itens eram classificados como negativos, os avaliadores tendiam a concordar mais vezes do que quando eram cassificados como positivos. A concordância global foi aproximadamente como se a resposta tivesse sido aleatória. Isto significa que o instrumento na sua presente forma não é útil.
Na tentativa de resolver o problema em causa estudou-se o método em uso no serviço que foi adoptado há muito tempo, embora sem qualquer estudo prévio. Não foi estudado antes porque na realidade é muito diferente dos instrumentos referidos na literatura que têm a mesma finalidade. A concordância entre os avaliadores segundo o coeficiente kappa foi boa, embora marginalmente. A proporção de concordância negativa foi mesmo muito alta, quase perfeita. A especificidade foi também muito alta, reflectindo-se também no alto valor predictivo positivo, significando que quando o teste é positivo, isto é, quando há sinais de desconforto a probabilidade de haver efectivamente desconforto é muito alta. O grande problema é o da sensibilidade do método que é de apenas 40%, o que significa que só uma minoria de casos de desconforto é detectada, o que afecta gravemente o método como método de rastreio.
O que poderá ter conduzido a estes resultados? O reduzido número de doentes envolvidos no Estudo 1 pode ter afectado os resultados, mas a nossa escolha de preferir o número de observações, visto que em momentos diferentes a intensidade dos sintomasvaria, tornou o tamanho da amostra razoável. O estudo foi interrompido neste ponto quando a análise preliminar então realizada tornou claro que o método de avaliação não se revelava útil. O Estudo 2 teve também um número de avaliações razoável

| 111 111Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
atendendo ao reduzido número de variáveis em estudo. Outra possibilidade poderá ser a influência que as alterações cognitivas possam ter tido na precisão das respostas dealguns doentes. Finalmente, os itens que constituiram os dois instrumentos pode não ter sido os mais adequados.
Os resultados do Estudo 2 podem ter ainda assim alguma utilidade visto que a sua especificidade é muito alta. O seu alto valor preditivo positivo assegura que os casos detectados correspondem de facto a desconforto que requer intervenção. O problema principal é o da baixa sensibilidade que diminui o método como instrumento de rastreio. A sensibilidade é referida poucas vezes na validação dos instrumentos de avaliação dos doentes com dificuldades de comunicação, mas já tem sido referida como próxima da verificada neste estudo. No anexo 4 pode ver-se o comentário do coorientador desta tese.
Em conclusão, a questão da avaliação do sofrimento em geral ou de sintomas específicos tem-se revelado difícil, não existindo actualmente nenhum método consensual. Os estudosaqui apresentados obtiveram resultados que estão longe dos ideais, pelo que este aspecto necessita de continuara ser investigado no futuro.
referências
Volicer L, Hurley AC, Blasi ZV. Scales for evaluation of end-of-life care in dementia. Alzheimer. Dis Assoc Disord 2001;15:194-200.
Cohen-Mansfield J. Relatives’ assessment of pain in cognitively impaired nursing homes residents. J Pain Symptom Manage 2002;24:562-571.
Zwakhalen SM, Hamers JP, Abu-Saad HH, Berger MP. Pain in elderly people with severe dementia: a systematic review of behavioral pain assessment tools. BMC Geriatr.2006 Jan 27;6:3.
Wary B, collectif Doloplus: Doloplus-2, une échelle pourévaluer la douleur. Soins Gérontologie 1999;19:25-27.
Lotan M, Ljunggren EA, Johnsen TB, Defrin R, Pick CG, Strand LI. A modified version of the Non-communicating Children Pain Checklist-Revised, adapted to adults with intellectual and developmental disabilities: sensitivity to pain and internal consistency. J Pain 2009;10:398-407.
1
2
3
4
5
Fuchs-Lacelle S, Hadjistavropoulos T. Development and preliminary validation of the pain assessment checklist for seniors with limited ability to communicate (PACSLAC). Pain Manag Nurs 2004;5:37-49.
Manfredi PL, Breuer B, Meier DE, Libow L. Pain assessmentin elderly patients with severe dementia. J Pain Symptom Manage 2003;25:48-52.
Morrelo R, Jean A, Alix M, Sellin-Peres D, Fermanian J.A scale to measure pain in non-verbally communicating olderpatients: the EPCA-2 study of its psychometrics properties. Pain 2007;133:87-98.
Horgas A, Miller L. Pain assessment in people with dementia.AJN 2008;108:62-70.
Campbell ML, Templim T, Walch J. A respiratory distress observation scale for patients unable to self-report dyspnea.J Palliat Med 2010;13:285-290.
6
7
8
9
10

112 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Logsdon RG, Gibbons LE, McCurry SM, Teri L. Quality of life in Alzheimer disease: patient and caregiver reports.J Mental Health Aging 1999;5:21-31.
Kasper JD, Black BS, Shore AD, Rabins PV. Evaluationof the validity and reliability of the Alzheimer Disease-related Quality of Life Assessment Instrument. Alzheimer Dis Assoc Disord 2009;0:1-10.
Martin-Cook K, Hynan LS, Rice-Koch K, Svetlik DA, WeinerMF. Responsiveness of the Quality of Life in Late-stageDementia Scale to psychotropic drug treatment in late-stagedementia. Dement Geriatr Cogn Disord 2005;19:82-85.
Ettema TP, Dröes RM, de Lange J, Mellenberg GJ, RibbeMW. A review of quality of life instruments used in dementia. Qual Life Res 2005;14:675-686.
Aminoff BZ, Purits E, Noy S, Adunsky A. Measuring thesuffering of end-stage dementia: reliability and validity of the Mini-Suffering State Examination. Arch Gerontol Geriatr 2004;38:123-130.
Kovach CR, Noonan PE, Griffie J, Muchka S, Weissman DE. The Assessment of Discomfort in Dementia Protocol. Pain Manage Nurs 2002;3:16-27.
Volicer L, Hurley AC, Blasi ZV. Scales for evaluation of end-of-life care in dementia. Alzheimer Dis Assoc Disord 2001;15:194-200.
Gélinas C, Harel F, Fillion L, Puntillo KA, Johnston C. Sensitivity and specificity of the Critical-care Pain Observation Tool for the detection of pain in intubated adults after cardiac surgery. J pain Symptom Manage 2009;37:58-67.
Hølen JC, Saltvedt, Fayers PM, Hjermstad MJ, Loge JH, Kaasa S. Doloplus-2, a valid tool for behavioural pain assessment? BMC Geriatrics 2007;7:29.
Cohen J. A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 1960, 20, 37-46.
http://www.john-uebersax.com/stat/raw.htm (acedido em 01/07/2011).
Altman DG (1991) Practical statistics for medical research.London: Chapman and Hall.
Pickering G, Gibson SJ, Serbouti S, Odetti P, FerrazGonçalves J, Gambassi G, Guarda H, Hamers JP, Lussier D, Monacelli F, Pérez-Castejón Garrote JM, Zwakhalen SM, Barneto D; Collectif Doloplus, Wary B. Reliability study in five languages of the translationof the pain behavioural scale Doloplus. Eur J Pain 2010;14:545.e1-10.
Hølen JC, Saltvedt I, Fayers PM, Bjørnnes M, Stenseth G, Hval B, Filbet M, Loge JH, Kaasa S. The Norwegian Doloplus-2, a tool for behavioural pain assessment: translation and pilot-validation in nursing home patients with cognitive impairment. Palliat Med. 2005l;19:411-417.
18
19
20
21
22
23
24
11
12
13
14
15
16
17
| 113 113Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
6CONCLUSÃO

114 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 115 115Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
conclusão
Os cuidados paliativos constituem hoje o padrão de intervenção para os doentes com doenças avançadas e progressivas quando os tratamentos que visam alterar a sua progressão não são eficazes, mas também em fases mais precoces em conjunto com esses tratamento. Desde Cicely Saunders que se tem procurado credibilizar os cuidados paliativos como disciplina científica. No entanto, muitas pessoas chegaram aos cuidadospaliativos imbuídas sobretudo de sentimentos humanitários, desconhecendo a necessidade de evolução científica desta área. Esta atitude vai-se progressivamente reduzindo, havendo um crescente esforço de incluir práticas baseadas na evidência.
Este trabalho procura ir no sentido de desenvolver práticas baseadas na investigação. A razão de ser do desenvolvimento deste sistema integrado de avaliação inicial dos doentes oncológicos admitidos em cuidados paliativos é, como foi referido na introdução, a avaliação rigorosa e eficiente dos doentes no primeiro encontro com os cuidados paliativos, seja qual for o seu estado. As vantagens de uma avaliação sistemática e padronizada são as de permitir a avaliação em menos tempo, sem perder rigor nem a abrangência necessária para detectar os problemas principais, condições indespensáveis para uma intervenção rigorosa.
Mas este sistema de avaliação deve ser visto como um ponto de partida, um sistema de rastreio. Não basta saber se um doente sem alterações cognitivas que impeçam a avaliação directa tem dor ou não. Se tiver é necessário iniciar o processo específico de avaliação da dor, das suas caractarísticas como a sua intensidade, os factores que a agravam e os que a aliviam, os eventuais tratamentos que fez anteriormente para a controlar e a sua eficácia e efeitos indesejados, outros problemas de saúde que possam

116 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
contraindicar certos fármacos, pedir exames que eventualmente sejam necessários para esclarecer um ou outro aspecto, etc. Só depois se poderá tratar a dor eficazmente. Isto aplica-se a qualquer outro sintoma físico ou psicológico, a alterações da consciência, seja da capacidade de acordar seja do conteúdo da consciência.
Nos doentes com alterações que não permitam uma avaliação directa, a detecção de sinais de sofrimento põe o problema imediato de determinar a sua causa. Resolver este problema pode ser difícil. Nesta situação a história do doente colhida das informações de quem o referencia e/ou de quem o acompanha pode ser determinante, assim como o exame físico ou a atitude do doente. Se o doente imoblizar uma zona do corpo ou gemer quando um determinado segmento é mobilizado isso indica que a causa é muito provavelmente dor. Se o doente está polipneico com baixa saturação de oxigénio e alterações auscultatórias o problema é certamente dispneia. Por vezes os sinais de desconforto ou sofrimentos podem dever-se às alterações cognitivas.
O funcionamento global do sistema será do modo que a seguir se apresenta:
Se o doente estiver em sofrimento evidente (ex. dor não controlada) que não permita prosseguir a avaliação: a. Controlar a sua causa: i. Pode não ser possível prosseguir nesta altura a avaliação porque o problema é de difícil resolução ou porque o efeito dos meios utilizados o impede (ex. sonolência provocada por um opióide).
1 ·
Se o problema for controlado ou não havia sofrimento que impedisse a avaliação: a. Determinar o estado de consciência (vigília), se não obviamente normal: i. Se o doente se apresenta acordado o seu estado de vigília é obviamente normal, mas se não se apresenta assim o seu estado deve ser avaliado pelo método indicado no capítulo 3.
b. Determinar o estado cognitivo, se não obviamente anormal: i. Se o doente se apresenta agitado é evidente que o seu conteúdo da consciência é anormal, mas se não for assim é necessária a avaliação pelo método indicado no capítulo 3; ii. Esta avaliação faz-se no decorrer da avaliação global observando se ocorrem alterações incluídas no método de avaliação da confusão.
2 ·
| 117 117Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
c. Determinação das necessidades de informação: i. É um aspecto importantíssimo que pode ocorrer noutro momento; ii. Nos doentes com alterações cognitivas pode não ser possível dependendo da sua gravidade; iii. A comunicação ocorre, porém, durante toda a consulta.
d. Avaliação dos problemas principais, se cognição normal: i. Pelo método indicado no capítulo 4; e. Avaliação dos problemas principais, se cognição anormal que não permita a avaliação directa; i. Pelo método indicado no capítulo 5.
Tendo sido desenvolvido com o objectivo da avaliação inicial dos doentes admitidos em cuidados paliativos, a maioria dos elementos pode ser usado como método de rastreio na avaliação por rotina dos doentes. Assim, a Escala do Nível de Consciência para Cuidados Paliativos pode ser aplicada em qualquer altura. Também o Método de Avaliação da Confusão pode ser aplicado regularmente. A avaliação dos doentes com alterações cognitivas pode ser usada sempre que ocorram alterações que impeçam a avaliação pelo relato do doente. Esta escala apesar da sua baixa sensibilidade tem uma especificidade muito alta e um valor preditivo positivo alto, pelo que pode ser útil, embora a investigação nesta área tenha de continuar.
A investigação é um processo contínuo. Mesmo instrumentos validados devem continuar a ser estudados sobre outros aspectos. Alguns dos instrumentos mais usados têm vindo a ser estudados há 15 ou mais anos. Este sistema, fruto do resultado de largos anos de trabalho de equipa e de investigação sistemática, parece ser útil para a finalidade com que foi construído podendo inclusivamente ser utilizado noutros contextos clínicos devendo, porém, ser alvo de um processo de aperfeiçoamento contínuo. Esta tese insere-se num processo de procura de soluções para questões que se colocam na prática diária. Foi esse processo que me levou a explorar os problemas éticos do fim de vida que se concretizou na minha tese de mestrado concluída há cerca de 4 anos.

118 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 119 119Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
7RESUMO

120 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 121 121Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
resumo
Geralmente reconhece-se a fundação do St. Christopher’s Hospice em Londres em 1967 por Cicely Saunders como o início dos cuidados paliativos modernos. Desde então, tem vindo a expandir-se por todo o mundo. Em Portugal os cuidados paliativos tiveram início em 1994 com a abertura da Unidade de Cuidados Continuados no IPO - Porto. Hoje, são considerados os cuidados padrão para os doentes com doenças crónicas avançadas e progressivas, podendo ser usados em conjunto com os tratamentos “curativos”.
Os cuidados paliativos começaram por causa dos problemas dos doentes com cancro avançado, mas hoje considera-se que devem ser prestados independentemente da doença crónica subjacente. A realidade mostra, no entanto, que os doentes oncológicos continuam a ser os mais referenciados para cuidados paliativos.
A maioria dos doentes com doenças crónicas avançadas tem múltiplos problemas resultantes da sua doença e por vezes também dos tratamentos anteriormente efectuados. Além disso, os doentes admitidos em cuidados paliativos apresentam-se em situações muito diversas a nível do estado de consciência, da função cognitiva, do estado emocional, da funcionalidade, dos sintomas etc. Os doentes podem estar muito débeis, receosos ou ansiosos. Há também o problema do trabalho que uma equipa muito ocupada tem que fazer e do tempo que tem disponível para cada doente. Por isso, uma avaliação extensa pode ser impossível e pode constituir um fardo para os doentes. Contudo, para os ajudar, é necessário identificar e avaliar rigorosamente os seus problemas principais. Mais tarde, outros problemas de mais baixa prioridade poderão ser abordados se for apropriado.

122 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Para responder às questões anteriormente colocadas procurou desenvolver-se um sistema integrado para a avaliação inicial dos principais problemas dos doentes oncológicos admitidos em cuidados paliativos que se adapte às diversas circunstâncias em que se podem apresentar. Este sistema deve ser considerado como um sistema de rastreio, pelo que os problemas detectados necessitam de ser explorados sobre as suas características e causas para poderem ser resolvidos.
Os elementos que constituem o sistema são apresentados em quatro capítulos:
No capítulo Comunicação procura-se demonstrar a necessidade e o desejo de informação que a maioria dos doentes sentem e a dificuldade com que muitas vezes se deparam, através de dois estudos levados a cabo no IPO - Porto nos últimos anos e já publicados. Procura-se mostrar a necessidade de adequar a informação aos desejos dos doentes e não usar princípios rígidos, procurando seguir a vontade e o ritmo destes;No terceiro capítulo descreve-se o método de avaliação da consciência tanto ao nível da vigília como do conteúdo. Para avaliar o nível de vigília desenvolveu-se uma escala, entretanto já publicada. Para avaliar a função cognitiva nos doentes com um nível de vigília que permita interacção, introduziu-se o Método de Avaliação da Confusão porque já estava em uso na Unidade de Cuidados Paliativos do IPO - Porto e porque foi recentemente validado em cuidados paliativos e em português;No quarto capítulo apresenta-se um instrumento desenvolvido segundo o método de Delfos, com o envolvimento de peritos internacionais, para a avaliação dos doentes sem alterações cognitivas. O instrumento inclui 10 sintomas, uma questão sobre a capacidade de os doentes de se autocuidarem, uma questão social e uma questão geral sobre a avaliação que os doentes fazem do seu bem-estar;Para os doentes que não podem ser avaliados directamente por alterações cognitivas foram estudados dois métodos que se descrevem no capítulo 5. O método que melhores resultados produziu foi a avaliação geral de sinais de desconforto. Mesmo assim, a sensibilidade do método foi relativamente baixa (40%), embora a especificidade tenha sido muito alta (97%) assim como o valor preditivo positivo (86%).
a.
b.
c.
d.

| 123 123Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
O funcionamento global do sistema será do modo que a seguir se apresenta:
Se o doente estiver em sofrimento evidente (ex. dor não controlada) que não permita prosseguir a avaliação: a. Controlar a sua causa i. Pode não ser possível prosseguir nesta altura a avaliação porque o problema é de difícil resolução ou porque o efeito dos meios utilizados o impede (ex. sonolência provocada por um opióide).
Se o problema for controlado ou se não havia sofrimento que impedisse a avaliação: a. Avaliação do estado de consciência (vigília) com o método incluído no capítulo 3: b. Avaliação do estado cognitivo, se o estado de vigília o permitir, usando o MAC: i. A avaliação faz-se no decorrer da avaliação global observando se ocorrem alterações incluídas no MAC. c. Avaliação das necessidades de informação, se for adequado: i. É um aspecto importantíssimo que pode ocorrer neste ou noutro momento; d. Avaliação dos problemas principais, se a cognição o permitir, usando o método indicado no capítulo 4. e. Avaliação dos problemas principais, se a cognição for anormal não permitindo a avaliação directa, usando o método indicado no capítulo 5.
1 ·
2 ·
Embora este método tenha sido desenvolvido para a avaliação inicial dos doentes oncológicos admitidos em cuidados paliativos, a maioria dos elementos deste instrumento também pode ser usada na rotina diária. Este sistema, fruto do resultado de largos anos de trabalho de equipa e de investigação sistemática, parece ser útil para a finalidade com que foi construído e pode provavelmente ser utilizado noutros contextos clínicos. Porém, deve ser melhorado continuamente.

124 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 125 125Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
8ABSTRACT

126 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 127 127Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
abstract
Usually the foundation of the St. Christopher’s Hospice in London in 1967 by Cicely Saunders is recognized as the beginning of modern palliative care. Since then, palliative care has spread all over the world. In Portugal palliative care began in 1994 with the opening of the Continuing Care Unit at the Portuguese Institute of Oncology (IPO) - Porto. Nowadays, palliative care is the standard of treatment for patients with advanced and progressive chronic diseases and can also be used alongside “curative” treatments.
Palliative care began because of the problems of patients with advanced cancer; but today there is a consensus about its potential usefulness independently of the type of underlying chronic disease. However, it remains the case that oncological patients continue to make up the greatest number of people referred to palliative care.
Most patients with chronic diseases have multiple problems due to their disease and sometimes also to the treatment they underwent previously. Furthermore, patients admitted to palliative care arrive with very different conditions in aspects such as consciousness, cognitive function, emotional state, performance, symptoms, etc. Patients may be very frail, frightened or anxious. There is also the problem of the work that a busy team has and the time available to each patient. Therefore, an extensive evaluation might be impossible and can be also a burden for the patient. However, to help the patients the main problems should be identified rigorously. Other problems can be addressed later if appropriate.

128 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
To respond to the variety of situations explained above an integrated system for the initial evaluation of the main problems of oncological patients was developed which can adapt to those diverse circumstances. The system should be seen as a screening method, as the problems detected need to be assessed further in their characteristics and causes if they are to be solved.
The elements of the system are presented in four of the chapters of this thesis:
In the chapter Communication we try to demonstrate the need and the wish for information that most patients feel and the difficulties they often have to obtain it with two studies concluded some years ago in the IPO - Porto which have already been published. We try to show the need to match the information disclosed to patients’ wishes without following rigid principles, but following the patients’ will and rhythm;In the third chapter the method to assess consciousness is described at the wakefulness and the content levels. To assess wakefulness a scale was developed, which has been published. To assess the cognitive function in those patients with a wakefulness level allowing interaction, the Confusion Assessment Method was included because it was already in use in the Palliative Care Unit of the IPO - Porto and because it was recently validated in palliative care and in Portuguese;In the fourth chapter a tool developed with the Delphi method, involving international experts, for the assessment of patients without cognitive failure is presented. The tool includes 10 symptoms, a question about the patients’ capacityfor self care, a question about social issues and a general question about the evaluation that patients do about their own well-being;For those patients who cannot be assessed directly because of cognitive failure two methods were studied that are described in chapter 5. The method with the better results was the general evaluation of signs of discomfort. Even so, its sensitivity was relatively low (40%); although its specificity was very high (97%) as was the positive predictive value (86%).
a.
b.
c.
d.
| 129 129Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
The general mode of functioning of the system is the following:
If the patient were obviously suffering (eg. uncontrolled pain) making it inappropriate to pursue the assessment: a. Control its cause: i. The assessment may not be pursued at that time because the problem is difficult to solve or the side effects of the treatment do not allow it (eg. somnolence caused by an opioid).
If the problem can be controlled without problems at that moment or if there was no suffering which precluded the assessment: a. Assess the wakefulness using the method included in chapter 3; b. Assess cognition, if the wakefulness state allows it, using the CAM: i. The assessment should be done while the patient is globally evaluated, looking for the problems included in the CAM. c. Assessment of information needs if cognition is adequate: i. This is a very important issue, but the delivery of information can occur at this or at another moment; d. Assessment of the main problems if cognition allows it using the method indicated in chapter 4. e. Assessment of the main problems, if cognition is abnormal not allowing the direct assessment, using the method indicated in chapter 5.
1 ·
2 ·
Although this method of screening has been developed for the initial assessment the problems of oncological patients admitted in palliative care, most elements of the tool can also be used in the everyday work routine. This system results from many years of team work and systematic clinical research. It seems to meet its aim and probably can be used in other clinical settings. However, it should be continuously improved.

130 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 131 131Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
9ANEXOS

132 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 133 133Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
1
ferramentas de avaliação - domínio dos sintomas físicos

134 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 135 135Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados PaliativosA
NE
XO
1
Fer
ram
enta
s de
ava
liaçã
o –
Dom
ínio
dos
sin
tom
as fí
sico
s R
SC
L[1
] M
SA
S-S
F[2
] P
NP
C[3
] E
SA
S[4
] S
DS
[5]
EO
RT
C Q
LQ
-30
[6]
NA
CP
RD
[7]
M
DA
SI [
8]
BH
I [9]
E
OR
TC
QL
Q-C
15-
PA
L [
10]
Lack
app
etite
La
ck a
ppet
ite
La
ck a
ppet
ite
Lack
app
etite
La
ck a
ppet
ite
Lack
app
etite
La
ck a
ppet
ite
Lack
app
etite
La
ck a
ppet
ite
Tire
dnes
s
(±)F
atig
ue
(±
)Fat
igue
(±
)Fat
igue
T
iredn
ess
(±)F
atig
ue
Tire
dnes
s T
iredn
ess
Sor
e m
uscl
es
La
ck e
nerg
y La
ck o
f ene
rgy
La
ck o
f ene
rgy
La
ck o
f ene
rgy
Low
bac
k pa
in
N
ause
a N
ause
a
Nau
sea
Nau
sea
Nau
sea
Nau
sea
Nau
sea
Nau
sea
Nau
sea
Difi
cult
Sle
epin
g D
ificu
lt S
leep
ing
Difi
cult
Sle
epin
g
Difi
cult
Sle
epin
g
Difi
cult
Sle
epin
g D
ificu
lt S
leep
ing
D
ificu
lt S
leep
ing
Hea
dach
es
H
eada
ches
Vom
iting
V
omiti
ng
V
omiti
ng
Vom
iting
V
omiti
ng
Diz
zine
ss
Diz
zine
ss
Diz
zine
ss
D
ec. s
exua
l int
eres
t D
ec. s
exua
l int
eres
t D
ec. s
exua
l int
eres
t
Abd
omin
al a
ches
Con
stip
atio
n C
onst
ipat
ion
Con
stip
atio
n C
onst
ipat
ion
Con
stip
atio
n
Dia
rrho
ea
Dia
rrho
ea
Dia
rrho
ea
Dia
rrho
ea
Dia
rrho
ea
A
cid
indi
gest
ion
S
hive
ring
T
ingl
ing
hand
s/fe
et
Tin
glin
g ha
nds/
feet
T
ingl
ing
hand
s/fe
et
Tin
glin
g ha
nds/
feet
Diff
ic. c
once
ntra
ting
Diff
ic. c
once
ntra
ting
Diff
ic. c
once
ntra
ting
Diff
ic. c
once
ntra
ting
Sor
e m
outh
S
ore
mou
th
Sor
e m
outh
Lo
ss o
f air
Loss
of a
ir
B
urni
ng e
yes
S
hort
ness
of b
reat
h S
hort
ness
of b
reat
h S
hort
ness
of b
reat
h S
hort
ness
of b
reat
h
Sho
rtne
ss o
f bre
ath
Sho
rtne
ss o
f bre
ath
Sho
rtne
ss o
f bre
ath
Sho
rtne
ss o
f bre
ath
Sho
rtne
ss o
f bre
ath
Dry
mou
th
Dry
mou
th
D
ry m
outh
P
ain
Pai
n P
ain
Pai
n P
ain
Pai
n P
ain
Pai
n P
ain
C
ough
C
ough
S
kin
chan
ges
F
eelin
g dr
owsy
Fee
ling
drow
sy
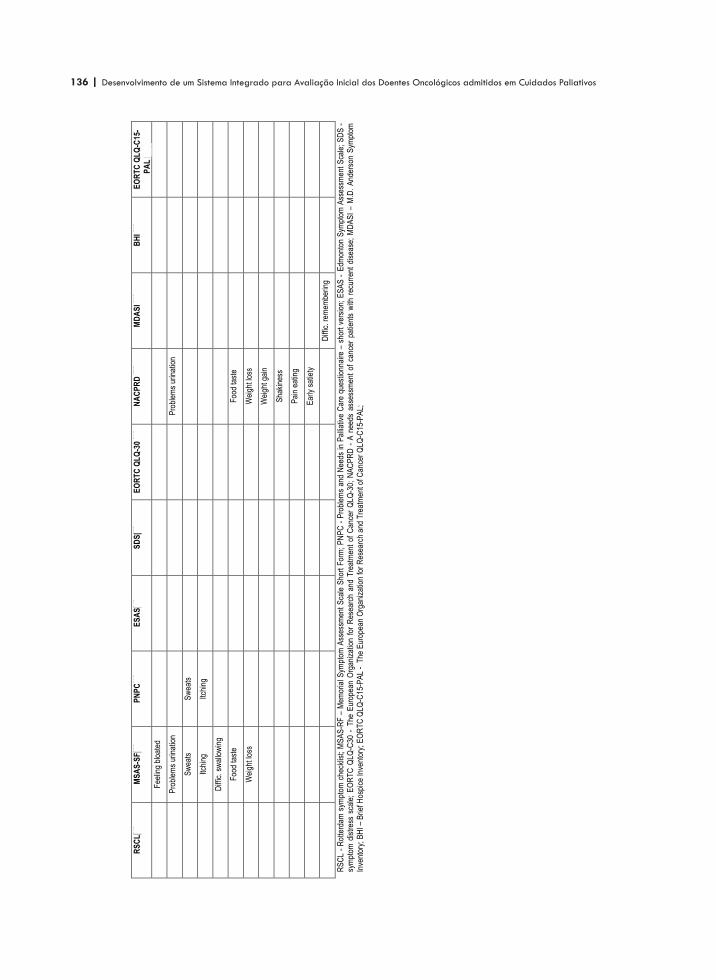
136 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
RS
CL
[1]
MS
AS
-SF
[2]
PN
PC
[3]
ES
AS
[4]
SD
S[5
] E
OR
TC
QL
Q-3
0 [6
] N
AC
PR
D [
7]
MD
AS
I [8]
B
HI [
9]
EO
RT
C Q
LQ
-C15
-
PA
L [
10]
F
eelin
g bl
oate
d
Pro
blem
s ur
inat
ion
Pro
blem
s ur
inat
ion
Sw
eats
S
wea
ts
Itchi
ng
Itchi
ng
Diff
ic. s
wal
low
ing
F
ood
tast
e
F
ood
tast
e
W
eigh
t los
s
W
eigh
t los
s
Wei
ght g
ain
S
haki
ness
Pai
n ea
ting
E
arly
sat
iety
D
iffic
. rem
embe
ring
RS
CL
- R
otte
rdam
sym
ptom
che
cklis
t; M
SA
S-R
F –
Mem
oria
l Sym
ptom
Ass
essm
ent
Sca
le S
hort
For
m;
PN
PC
- P
robl
ems
and
Nee
ds in
Pal
liativ
e C
are
ques
tionn
aire
– s
hort
ver
sion
; E
SA
S - E
dmon
ton
Sym
ptom
Ass
essm
ent
Sca
le;
SD
S -
sy
mpt
om d
istr
ess
scal
e; E
OR
TC
QLQ
-C30
- T
he E
urop
ean
Org
aniz
atio
n fo
r R
esea
rch
and
Tre
atm
ent
of C
ance
r Q
LQ-3
0; N
AC
PR
D -
A n
eeds
ass
essm
ent
of c
ance
r pa
tient
s w
ith r
ecur
rent
dis
ease
; M
DA
SI
– M
.D.
And
erso
n S
ympt
om
Inve
ntor
y; B
HI –
Brie
f Hos
pice
Inve
ntor
y; E
OR
TC
QLQ
-C15
-PA
L -
The
Eur
opea
n O
rgan
izat
ion
for
Res
earc
h an
d T
reat
men
t of C
ance
r Q
LQ-C
15-P
AL;

| 137 137Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
2
list of symptoms/problems

138 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
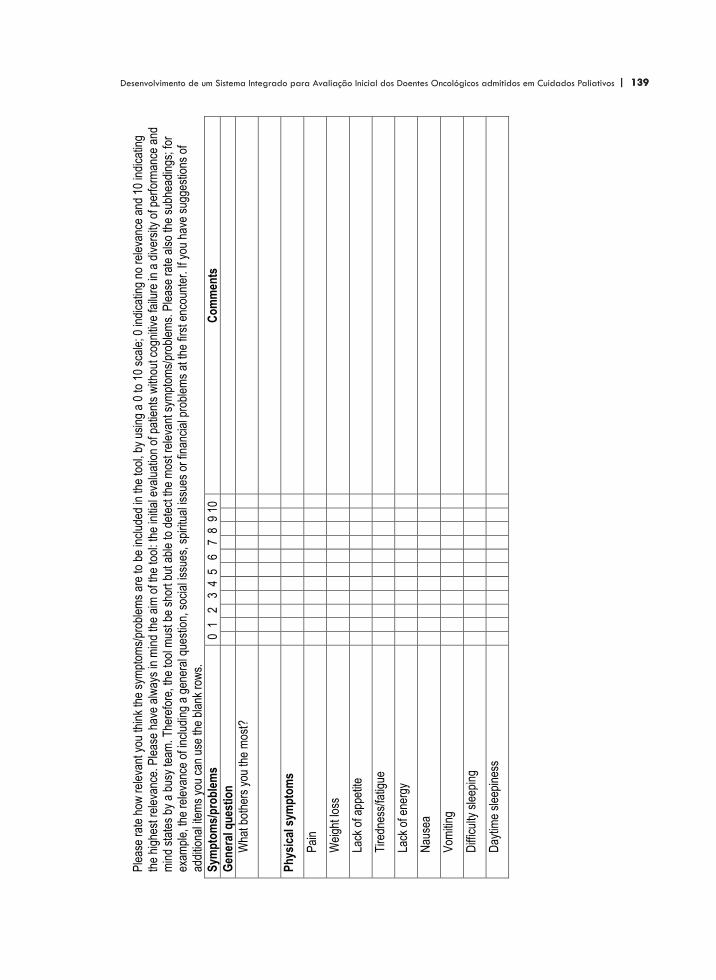
| 139 139Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
1
An
exo
2
Lis
t o
f sy
mp
tom
s/p
rob
lem
s
Ple
ase
rate
how
rel
evan
t you
thin
k th
e sy
mpt
oms/
prob
lem
s ar
e to
be
incl
uded
in th
e to
ol, b
y us
ing
a 0
to 1
0 sc
ale;
0 in
dica
ting
no r
elev
ance
and
10
indi
catin
g th
e hi
ghes
t rel
evan
ce. P
leas
e ha
ve a
lway
s in
min
d th
e ai
m o
f the
tool
: the
initi
al e
valu
atio
n of
pat
ient
s w
ithou
t cog
nitiv
e fa
ilure
in a
div
ersi
ty o
f per
form
ance
and
m
ind
stat
es b
y a
busy
team
. The
refo
re, t
he to
ol m
ust b
e sh
ort b
ut a
ble
to d
etec
t the
mos
t rel
evan
t sym
ptom
s/pr
oble
ms.
Ple
ase
rate
als
o th
e su
bhea
ding
s; fo
r ex
ampl
e, th
e re
leva
nce
of in
clud
ing
a ge
nera
l que
stio
n, s
ocia
l iss
ues,
spi
ritua
l iss
ues
or fi
nanc
ial p
robl
ems
at th
e fir
st e
ncou
nter
. If y
ou h
ave
sugg
estio
ns o
f ad
ditio
nal i
tem
s yo
u ca
n us
e th
e bl
ank
row
s.
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Gen
eral
qu
esti
on
Wha
t bot
hers
you
the
mos
t?
Ph
ysic
al s
ymp
tom
s
Pai
n
Wei
ght l
oss
Lack
of a
ppet
ite
Tire
dnes
s/fa
tigue
Lack
of e
nerg
y
Nau
sea
Vom
iting
Diff
icul
ty s
leep
ing
Day
time
slee
pine
ss

140 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
2
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Diz
zine
ss
Dec
reas
ed s
exua
l int
eres
t
Sex
ual d
iffic
ultie
s
Con
stip
atio
n
Dia
rrho
ea
Hea
rtbu
rn
Tre
mor
Tin
glin
g of
han
ds o
r fe
et
Sw
ellin
g of
arm
s or
legs
Abd
omin
al d
iste
nsio
n
Num
bnes
s
Diff
icul
ty c
once
ntra
ting
Sor
e m
outh
/pai
n w
hen
swal
low
ing
Diff
icul
ty s
wal
low
ing
Hai
r lo
ss
Bur
ning
/sor
e ey
es
Cou
gh
Sho
rtne
ss o
f bre
ath
Dry
mou
th

| 141 141Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
3
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Tas
te c
hang
es
Leak
age
of u
rine
Pro
blem
s w
ith u
rinat
ion
Sw
eatin
g
Itchi
ng
Fee
ling
full
afte
r ea
ting
Cha
nges
in s
kin
Wou
nds
Pre
ssur
e ul
cers
Alte
red
visi
on
Ligh
t hyp
erse
nsiti
vity
(ey
es)
Alte
red
audi
tion
Sou
nd h
yper
sens
itivi
ty
Ble
edin
g
Hic
cups
Loca
lized
wea
knes
s (p
aral
ysis
/par
esis
)
Dys
peps
ia (
indi
gest
ion)
Tra
cheo
tom
y
Col
osto
my
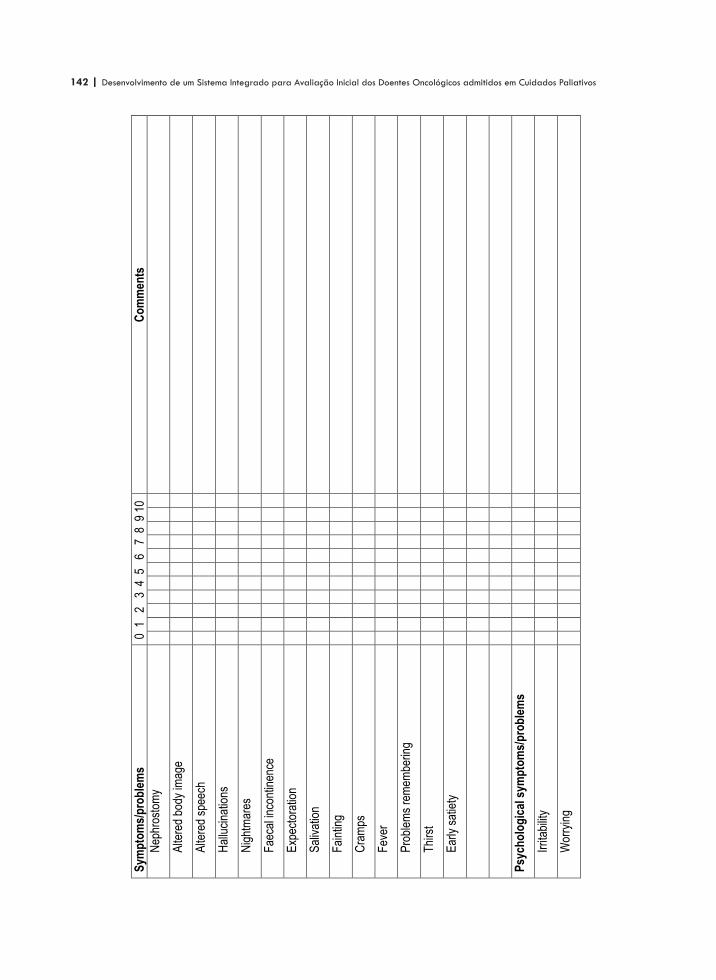
142 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
4
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Nep
hros
tom
y
Alte
red
body
imag
e
Alte
red
spee
ch
Hal
luci
natio
ns
Nig
htm
ares
Fae
cal i
ncon
tinen
ce
Exp
ecto
ratio
n
Sal
ivat
ion
Fai
ntin
g
Cra
mps
Fev
er
Pro
blem
s re
mem
berin
g
Thi
rst
Ear
ly s
atie
ty
Psy
cho
log
ical
sym
pto
ms/
pro
ble
ms
Irrit
abili
ty
Wor
ryin
g
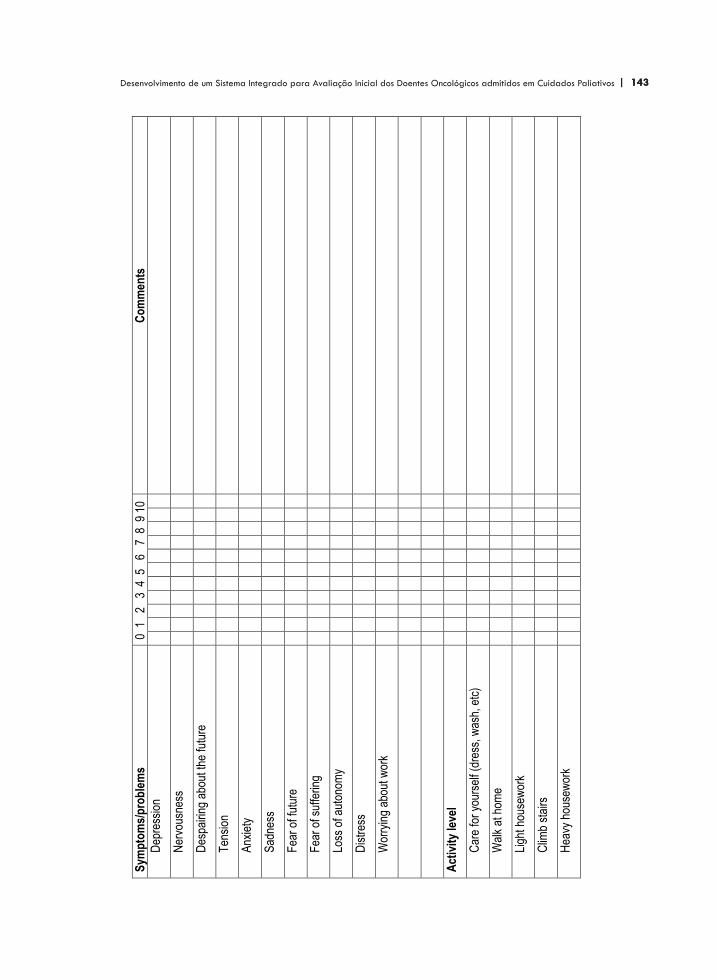
| 143 143Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
5
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Dep
ress
ion
Ner
vous
ness
Des
pairi
ng a
bout
the
futu
re
Ten
sion
Anx
iety
Sad
ness
Fea
r of
futu
re
Fea
r of
suf
ferin
g
Loss
of a
uton
omy
Dis
tres
s
Wor
ryin
g ab
out w
ork
Act
ivit
y le
vel
Car
e fo
r yo
urse
lf (d
ress
, was
h, e
tc)
Wal
k at
hom
e
Ligh
t hou
sew
ork
Clim
b st
airs
Hea
vy h
ouse
wor
k
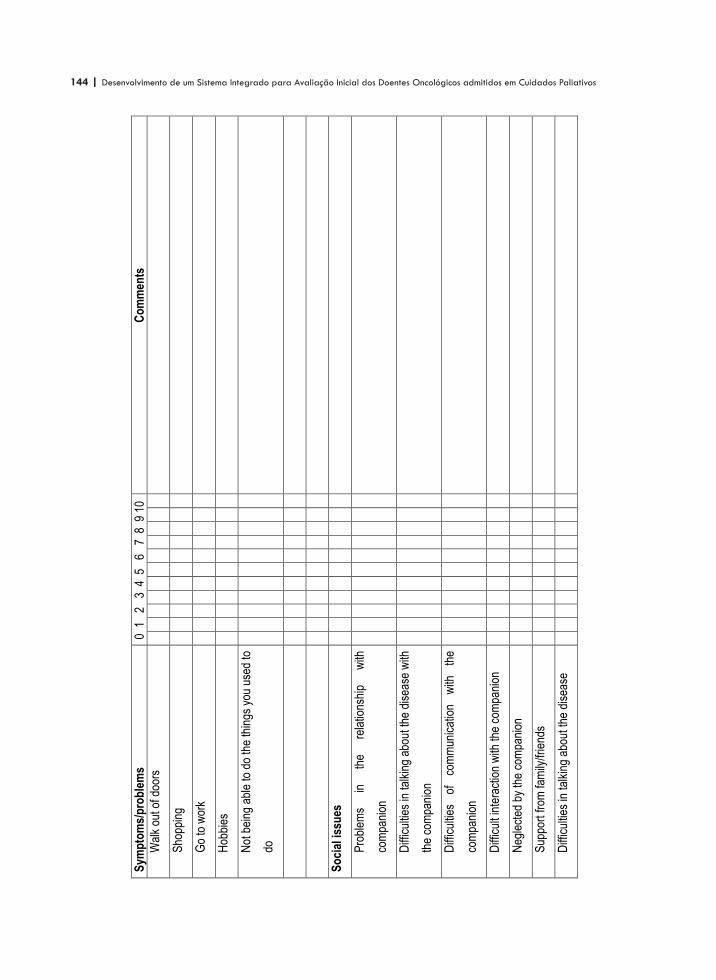
144 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
6
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Wal
k ou
t of d
oors
Sho
ppin
g
Go
to w
ork
Hob
bies
Not
bei
ng a
ble
to d
o th
e th
ings
you
use
d to
do
So
cial
issu
es
Pro
blem
s in
th
e re
latio
nshi
p w
ith
com
pani
on
Diff
icul
ties
in ta
lkin
g ab
out t
he d
isea
se w
ith
the
com
pani
on
Diff
icul
ties
of
com
mun
icat
ion
with
th
e
com
pani
on
Diff
icul
t int
erac
tion
with
the
com
pani
on
Neg
lect
ed b
y th
e co
mpa
nion
Sup
port
from
fam
ily/fr
iend
s
Diff
icul
ties
in ta
lkin
g ab
out t
he d
isea
se
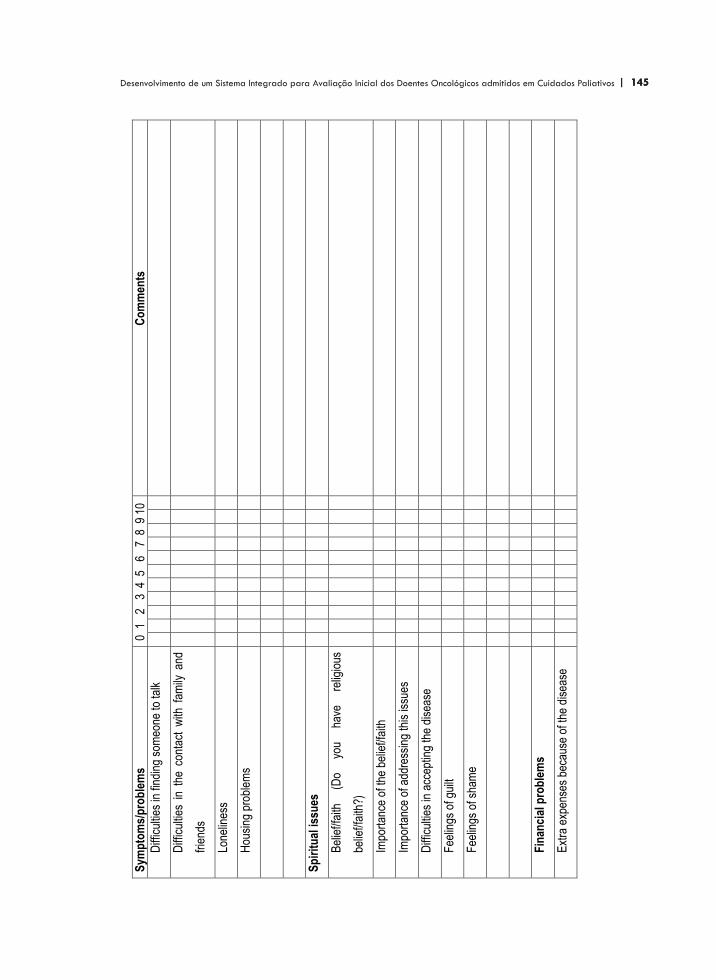
| 145 145Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
7
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Diff
icul
ties
in fi
ndin
g so
meo
ne to
talk
Diff
icul
ties
in t
he c
onta
ct w
ith f
amily
and
frie
nds
Lone
lines
s
Hou
sing
pro
blem
s
Sp
irit
ual
issu
es
Bel
ief/f
aith
(D
o yo
u ha
ve
relig
ious
belie
f/fai
th?)
Impo
rtan
ce o
f the
bel
ief/f
aith
Impo
rtan
ce o
f add
ress
ing
this
issu
es
Diff
icul
ties
in a
ccep
ting
the
dise
ase
Fee
lings
of g
uilt
Fee
lings
of s
ham
e
Fin
anci
al p
rob
lem
s
Ext
ra e
xpen
ses
beca
use
of th
e di
seas
e
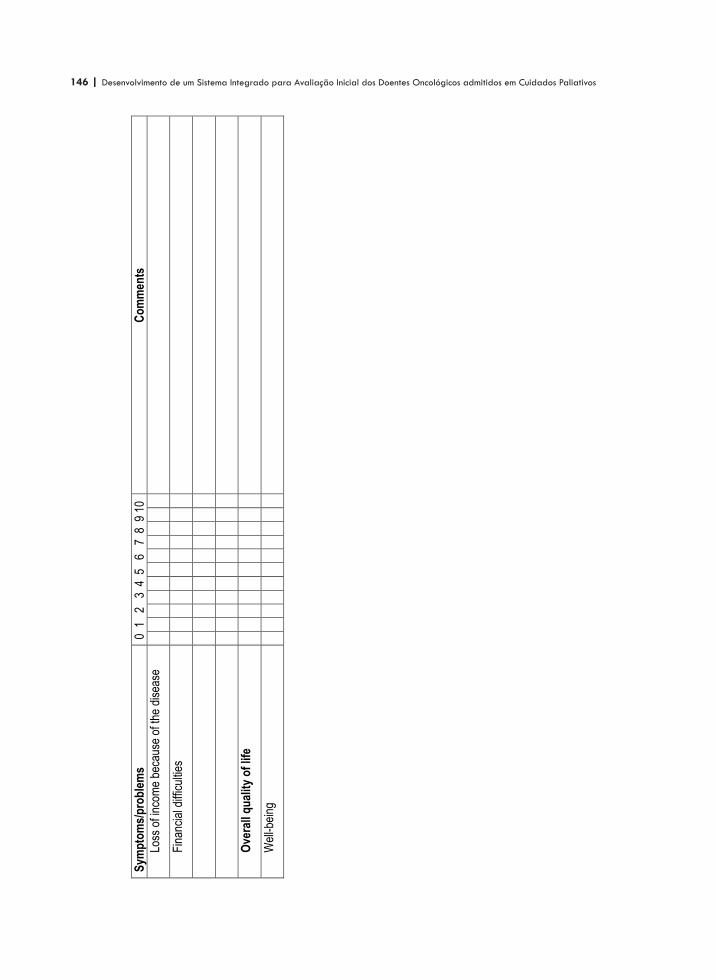
146 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
8
Sym
pto
ms/
pro
ble
ms
0 1
2
3 4
5
6 7
8 9
10
Co
mm
ents
Loss
of i
ncom
e be
caus
e of
the
dise
ase
Fin
anci
al d
iffic
ultie
s
Ove
rall
qu
alit
y o
f lif
e
Wel
l-bei
ng
| 147 147Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
3
delphi - round 2

148 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 149 149Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados PaliativosA
nex
o 3
Del
phi -
rou
nd 2
Exp
ert
's n
am
e
Sym
pto
ms/
pro
ble
ms
0
1
2
3
4
5
6
7
8
9
10
C
om
men
ts
Ph
ysic
al s
ymp
tom
s
Wei
ght l
oss
You
r pr
evio
us s
core
= 7
; m
ean
= 6
,8
1
1
2
3
2
3
Lack
of e
nerg
y
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,7
2
1
1
1
2
4
1
Vom
iting
You
r pr
evio
us s
core
= 9
; m
ean
= 7
,7
1
1
1
2
1
2
4
Diff
icul
ty s
leep
ing
You
r pr
evio
us s
core
= 8
; m
ean
= 7
,8
3
1
1
2
1
4
Day
time
slee
pine
ss
You
r pr
evio
us s
core
= 8
; m
ean
= 6
,0
1
1
1
3
3
1
2
Diff
icul
ty c
once
ntra
ting
You
r pr
evio
us s
core
= 9
; m
ean
= 5
,1
1
2
1
3
1
1
1
2
Sor
e m
outh
/pai
n w
hen
swal
low
ing
You
r pr
evio
us s
core
= 9
; m
ean
= 5
,1
3
1
1
2
1
1
1
1
Diff
icul
ty s
wal
low
ing
You
r pr
evio
us s
core
= 9
; m
ean
= 5
,6
1
1
1
3
2
2
1
1
Cou
gh
You
r pr
evio
us s
core
= 9
; m
ean
= 5
,5
2
1
3
2
2
1
Dry
mou
th
You
r pr
evio
us s
core
= 9
; m
ean
= 6
,5
1
1
3
1
1
1
2
1
Pro
blem
s w
ith u
rinat
ion
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,4
3
1
1
1
5
1
1
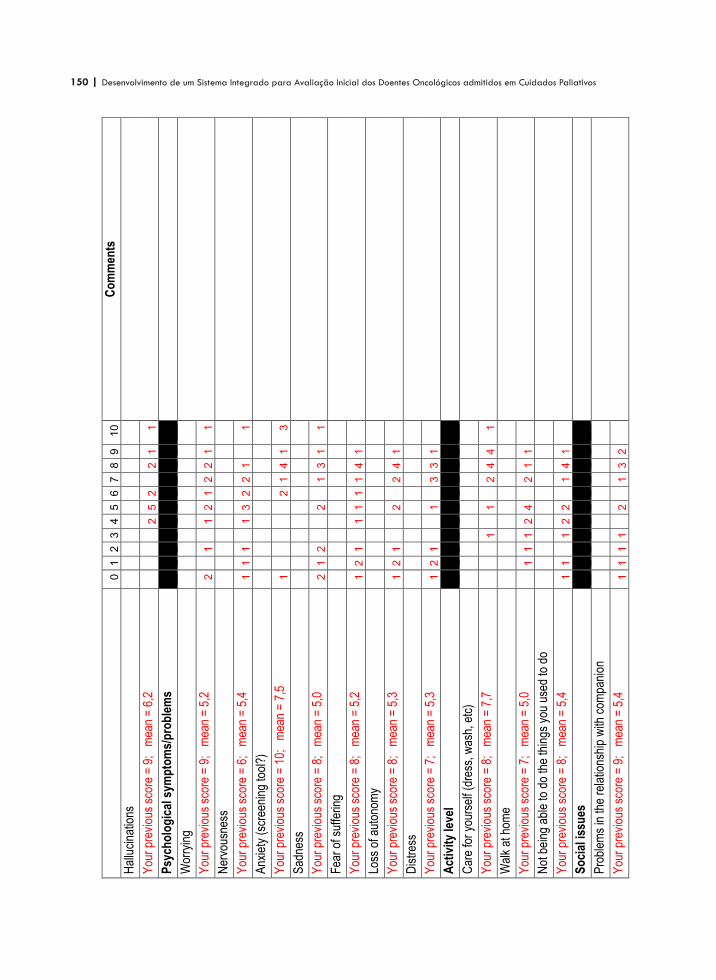
150 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
0
1
2
3
4
5
6
7
8
9
1
0
Co
mm
ents
Hal
luci
natio
ns
You
r pr
evio
us s
core
= 9
; m
ean
= 6
,2
2
5
2
2
1
1
Psy
cho
log
ical
sym
pto
ms/
pro
ble
ms
Wor
ryin
g
You
r pr
evio
us s
core
= 9
; m
ean
= 5
,2
2
1
1
2
1
2
2
1
1
Ner
vous
ness
You
r pr
evio
us s
core
= 6
; m
ean
= 5
,4
1
1
1
1
3
2
2
1
1
Anx
iety
(sc
reen
ing
tool
?)
You
r pr
evio
us s
core
= 1
0;
mea
n =
7,5
1
2
1
4
1
3
Sad
ness
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,0
2
1
2
2
1
3
1
1
Fea
r of
suf
ferin
g
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,2
1
2
1
1
1
1
1
4
1
Loss
of a
uton
omy
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,3
1
2
1
2
2
4
1
Dis
tres
s
You
r pr
evio
us s
core
= 7
; m
ean
= 5
,3
1
2
1
1
3
3
1
Act
ivit
y le
vel
Car
e fo
r yo
urse
lf (d
ress
, was
h, e
tc)
You
r pr
evio
us s
core
= 8
; m
ean
= 7
,7
1
1
2
4
4
1
Wal
k at
hom
e
You
r pr
evio
us s
core
= 7
; m
ean
= 5
,0
1
1
1
2
4
2
1
1
Not
bei
ng a
ble
to d
o th
e th
ings
you
use
d to
do
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,4
1
1
1
2
2
1
4
1
So
cial
issu
es
Pro
blem
s in
the
rela
tions
hip
with
com
pani
on
You
r pr
evio
us s
core
= 9
; m
ean
= 5
,4
1
1
1
1
2
1
3
2
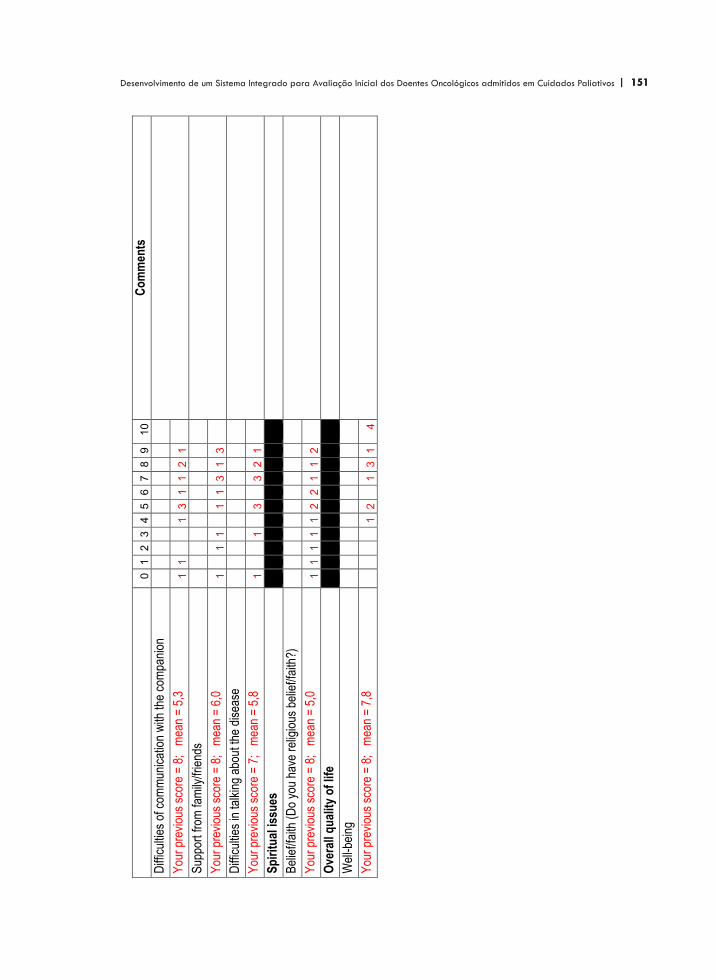
| 151 151Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
0
1
2
3
4
5
6
7
8
9
1
0
Co
mm
ents
Diff
icul
ties
of c
omm
unic
atio
n w
ith th
e co
mpa
nion
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,3
1
1
1
3
1
1
2
1
Sup
port
from
fam
ily/fr
iend
s
You
r pr
evio
us s
core
= 8
; m
ean
= 6
,0
1
1
1
1
1
3
1
3
Diff
icul
ties
in ta
lkin
g ab
out t
he d
isea
se
You
r pr
evio
us s
core
= 7
; m
ean
= 5
,8
1
1
3
3
2
1
Sp
irit
ual
issu
es
Bel
ief/f
aith
(D
o yo
u ha
ve r
elig
ious
bel
ief/f
aith
?)
You
r pr
evio
us s
core
= 8
; m
ean
= 5
,0
1
1
1
1
1
2
2
1
1
2
Ove
rall
qu
alit
y o
f lif
e
Wel
l-bei
ng
You
r pr
evio
us s
core
= 8
; m
ean
= 7
,8
1
2
1
3
1
4

152 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 153 153Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
4
parecer do co-orientador, dr. nigel sykes

154 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
| 155 155Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Anexo 4
Dear Jose Antonio, This is very interesting and I think shows what a difficult area this is to tackle. Negative results are still important and it is rather fascinating that observers are so disagreed on what constitute signs of discomfort. I wonder if there is any way of exploring why there was so little agreement? Perhaps at this distance from the original assessments there isn't, as I guess you would have to do two (or more) assessments straight after each other and then get the raters together in front of the patient to explain their thought processes to each other. Again, it is interesting that while it is fairly easy to be sure when a patient is distressed it is much harder to say when they are not. Given the range of types of distress and the range of degrees of stoicism this might, perhaps, be expected. It seems to me that what you propose by way of including this measure, set appropriately against the background of the existing literature on the assessment of non-communicating patients, is reasonable. But your negative results, with accompanying discussion of why they might have arisen, are also an important part of the results. Best wishes, Nigel Dr Nigel Sykes
Medical Director Consultant in Palliative Medicine
St Christopher's Hospice
Lawrie Park Road
London SE26 6DZ
Tel: 020 8768 4551 Fax: 020 8659 8680

156 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 157 157Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
10ARTIGOS PUBLICADOS

158 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 159 159Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
10
Support Care Cancer (2000) 9 :4–7DOI 10.1007/s005200000211 SUPPORTIVE CARE INTERNATIONAL
José António S. Ferraz Gonçalves A Portuguese palliative care unit
Published online: 28 October 2000Q Springer-Verlag 2000
J.A.S. Ferraz Gonçalves (Y)Instituto Portugues de Oncologia,Unidade de Cuidados Continuados,R. Dr. António Bernardino de Almeida,4200-072 Porto, PortugalE-mail: ferrazg6ipoporto.min-saude.pt orferrazg6mail.telepac.ptPhone: c351-2-5073940Fax: c351-2-5506833
Abstract The background to thedevelopment of the first Portu-guese palliative care unit isdescribed. The activities of thispioneer unit in Porto, whichinclude patient assistance, teachingand research, are reported, and thepaper closes with some generalthoughts on the possible ways ofproviding a more rapid response tothe suffering of patients with far
advanced chronic diseases in anenvironment where palliative careis not yet well developed.
Keywords Palliative care 7Portugal
Introduction
Palliative care has its source in the recognition of aproblem: the inadequate treatment of patients withadvanced chronic diseases. This treatment can be inad-equate by excess or default, that is, failure to recognizethe situation and consequent continuation with aggres-sive treatments as if the problem were a reversible one,or abandonment of the patient without support. Suchabandonment occurs not only when patients are senthome, but often in the hospital too. In this situation thepatients can be labelled as terminal and not followedup with the same interest as others: their needs may notbe really considered, and the medications and care theydo receive are often quite irrelevant to their condi-tion.
The start of palliative care is usually dated from thefoundation of St. Christopher’s Hospice in 1967 byCecily Saunders. In this way the hospice movement wasinitiated. The term ‘palliative care’ was used officiallyfor the first time in 1975, when Balfour Mount openedthe Palliative Care Service in the Royal VictoriaHospital in Montreal [1]. In 1990, the World HealthOrganization published one of its best-known docu-ments “Treatment of cancer pain and palliative care”[2], in which the importance of palliative care was
recognized. In this document, the WHO stated thatpalliative care was a priority in the fight against cancer,on the same level as prevention, screening and curativetreatment, and the only solution that was both humaneand realistic for many cancer patients. Palliative medi-cine is now a recognized specialty and is a subject inuniversity medical school curricula in the UnitedKingdom and a few other countries.
Since its beginnings, palliative care has spreadquickly through the world, mainly, like everything else,in the more highly developed countries. In Portugal,palliative care is still taking its first steps. It is the veryfirst of these that is described here.
The beginning
The North Section of the Portuguese League AgainstCancer recognized the cancer patients’ situationdescribed above and decided to build a palliative careunit to be called Unidade de Cuidados Continuados,which would work closely with the Porto Section of thePortuguese Institute of Oncology. At a certain point inthe course of the project I was invited to be the medicaldirector of the unit. I was a specialist in internal medi-cine and oncology and I accepted the position on one
10
Support Care Cancer (2000) 9 :4–7DOI 10.1007/s005200000211 SUPPORTIVE CARE INTERNATIONAL
José António S. Ferraz Gonçalves A Portuguese palliative care unit
Published online: 28 October 2000Q Springer-Verlag 2000
J.A.S. Ferraz Gonçalves (Y)Instituto Portugues de Oncologia,Unidade de Cuidados Continuados,R. Dr. António Bernardino de Almeida,4200-072 Porto, PortugalE-mail: ferrazg6ipoporto.min-saude.pt orferrazg6mail.telepac.ptPhone: c351-2-5073940Fax: c351-2-5506833
Abstract The background to thedevelopment of the first Portu-guese palliative care unit isdescribed. The activities of thispioneer unit in Porto, whichinclude patient assistance, teachingand research, are reported, and thepaper closes with some generalthoughts on the possible ways ofproviding a more rapid response tothe suffering of patients with far
advanced chronic diseases in anenvironment where palliative careis not yet well developed.
Keywords Palliative care 7Portugal
Introduction
Palliative care has its source in the recognition of aproblem: the inadequate treatment of patients withadvanced chronic diseases. This treatment can be inad-equate by excess or default, that is, failure to recognizethe situation and consequent continuation with aggres-sive treatments as if the problem were a reversible one,or abandonment of the patient without support. Suchabandonment occurs not only when patients are senthome, but often in the hospital too. In this situation thepatients can be labelled as terminal and not followedup with the same interest as others: their needs may notbe really considered, and the medications and care theydo receive are often quite irrelevant to their condi-tion.
The start of palliative care is usually dated from thefoundation of St. Christopher’s Hospice in 1967 byCecily Saunders. In this way the hospice movement wasinitiated. The term ‘palliative care’ was used officiallyfor the first time in 1975, when Balfour Mount openedthe Palliative Care Service in the Royal VictoriaHospital in Montreal [1]. In 1990, the World HealthOrganization published one of its best-known docu-ments “Treatment of cancer pain and palliative care”[2], in which the importance of palliative care was
recognized. In this document, the WHO stated thatpalliative care was a priority in the fight against cancer,on the same level as prevention, screening and curativetreatment, and the only solution that was both humaneand realistic for many cancer patients. Palliative medi-cine is now a recognized specialty and is a subject inuniversity medical school curricula in the UnitedKingdom and a few other countries.
Since its beginnings, palliative care has spreadquickly through the world, mainly, like everything else,in the more highly developed countries. In Portugal,palliative care is still taking its first steps. It is the veryfirst of these that is described here.
The beginning
The North Section of the Portuguese League AgainstCancer recognized the cancer patients’ situationdescribed above and decided to build a palliative careunit to be called Unidade de Cuidados Continuados,which would work closely with the Porto Section of thePortuguese Institute of Oncology. At a certain point inthe course of the project I was invited to be the medicaldirector of the unit. I was a specialist in internal medi-cine and oncology and I accepted the position on one

160 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
11
5
condition: that I should be allowed to take training inpalliative care, which at that time was only possible inunits outside Portugal.
Over the course of 7 months I visited several Euro-pean units: St. Christopher’s Hospice and St. HelenaHospice in England; Intituto Nazionale dei Tumori inMilan; La Foundation Rive-Neuve and the AubonneHospital in Switzerland; and Gregorio MaranónHospital in Madrid. I believe this was very useful and,in my case, the best approach, because the diversity Isaw showed me different realities, different experi-ences, and different styles of palliative care. Iconcluded that palliative care can be applied in manydifferent conditions, always with the same philosophyand the same principles behind it while the practice isadapted to the local circumstances, and that what isobserved in any palliative care service should be takenas an example of what can be done, rather than a modelto be copied.
The first unit
Because I finished my training period before the unitwas ready, we were allowed to start working with 5beds belonging to the Radiotherapy Service, which hada total of 25 beds. The staff in that service included thenurses who were keen to work in the future palliativeunit, some of whom had had some experience of pallia-tive care in units abroad. Our first patient was admittedon 17 October 1994. This, then, was the day whenpalliative care started in Portugal.
All the personnel, except the chief nurse and myself,were shared between the two services. We starteddoing inpatient care, outpatient care, and consultationin other services within the hospital.
There were various difficulties with this experience:I Problems arising from the physical/architectural set-
up, which did not make it easy for family members tostay with patients, especially at night
I Too few beds for hospital needsI Different treatment of patients in the same serviceI Difficulty in the implementation of specific routines
Other types of problems experienced at this stagewere:I Problems relating to misunderstanding of the
purpose of the new serviceI Referral mainly of patients expected to survive for
only a few daysI Frequent use of the unit as a kind of wastebasket,
that is, not with the idea of sending patients to aplace where they could be more adequately treatedbut to get a bed freeThese early days did also have positive aspects:
I The possibility of offering palliative care at all for thefirst time
Table 2 Evolution of the assistance to patients activity
1995 1996 1997 1998 1999
Inpatient admissions 68 100 221 359 388Outpatient clinic observations 549 1124 1302Internal consultation visits 361 596 910Telephone consultation 449 813Home care visits 212
Table 1 Staff of unit
Doctors 4 – with 1 assigned exclusively to home careNurses 24Nursing auxiliaries 16Social worker 1Psychologist 1Nutritionist 1Chaplain 1Driver 1Porters 7Volunteers 15
I The opportunity of spreading the principles of pallia-tive care more easily, because there was more directcontact with doctors in the other service
I Training the team in more specific work with only afew patients
I Possibility of contact with the reality of palliativecare, thus allowing selection (self-selection, at thattime) of people who really wanted to go on workingin palliative care
I Economy – because the unit was so small it wascheaper to work together with the other service,which made it possible to maintain adequate contin-uous staffing levels of professionals who needed tobe represented at all times, mainly nurses, withouthaving too many professionals relative to the numberof patientsWe can conclude that this experience was useful,
and perhaps it could be viewed as an example for othercentres where only a small unit can be implemented.
The new unit
Finally, the new unit opened on 25 May 1996. We grewstep by step as more people were involved in the team(Table 1). Initially, we maintained the same activities,adding to them as circumstances allowed (Table 2).
Now we have 20 beds, all in single rooms, whichallows a member of any patient’s family or a friend tostay at any time.
The unit has had a day centre since 1997: about 20patients can attend for up to 3 days each week, andthey can enjoy many activities.

| 161 161Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
12
6
Since 1998 we have offered telephone consultationsfor the patients being followed by the unit. Thepatients, their families, or their friends may contact theunit when a problem or a doubt arises, to discuss anadjustment to a medication, or to inform the doctor ofthe effect of a prescription, for example, 24 hours a day.It is usually possible for them to talk with the physicianbetween 09*E00 and 16*E00 o’clock, and with a nurseat other times.
In 1999 we started home care. We intend to makethis service one of the most important elements of theunit, so that patients can stay at home where their fami-lies and their own belongings are, that is to say wheretheir lives are centred. However, the traditionalextended family with three generations under one roofproviding support for all members of the family in diffi-cult times is changing. Families are becoming smallerand smaller; most people work outside the home,mainly in the bigger cities, and there will thereforeprobably be more and more difficulties in keepingpatients at home, as has already happened in otherEuropean countries.
Teaching
As this is a pioneer unit in Portugal and in view of itssize, it was planned that it should be a teaching centre.As professionals working exclusively in palliative care,we have an obligation to contribute to the spread ofknowledge in this field. However, the best thing we cando is to go beyond teaching what can be read in booksand reviews and also, most importantly, share ourexperience. This is why we did not start the multidisci-plinary courses until we had completed 3 years of workas a palliative care team.
Our first multidisciplinary course was in October1997. Since then, we have held four each year. Eachcourse is held for 12 professionals: 6 doctors and 6nurses. This small number allows contact with theeveryday life of the unit and with the patients. Eachcourse involves 35 hours from Monday to Friday in1 week. Up to August 2000, 144 professionals from allover the country, even from the islands of Madeira andthe Azores, had undergone training in 12 courses. Wealways have many more candidates than we can admitto the courses, which shows the interest people have inpalliative care and how much they feel the need oftraining in this special field. To help staff who work inour oncological centre but had not been able to get aplace on any of the multidisciplinary courses we held atheoretical course in 2000, which was attended by 35professionals.
In 2000 we held the first continuing education coursefor doctors and nurses who had already completed themultidisciplinary course. And in the future we intend to
hold update courses to maintain interest in palliativecare and ensure that the knowledge applied is current.
Since the beginning of our activities, members of theunit’s staff have participated in many courses,congresses, and other scientific meetings organized byothers. And, finally, I teach the palliative care portionof the course for the master’s degree in bioethics at theMedical School of Oporto University.
Apart from the courses, many doctors, nurses, socialworkers, psychologists, and priests spend variousperiods of time in the unit.
Research
Again, the position this unit occupies in palliative carein Portugal should make research one of its mostimportant activities, on a level with patient assistanceand teaching. These two activities should support andbe supported continuously by research. However,research takes time to produce results, so that we arenot in a hurry to publish research papers, though weare publishing some review papers in Portuguese.However, we have presented some work at congressesof the European Association for Palliative Care and atother congresses, and we intend to start publishing ourresults soon.
The future
The unit is still evolving: in the future there will bemore than 20 beds, and the home care service will bedeveloped and will reach more patients. Teaching ofpalliative care will remain important, and it is probablethat this unit will continue as the main palliative careteaching centre in Portugal. Faculty members of theOporto Medical Schools have been contacted about theidea of introducing undergraduate palliative careteaching into their curricula, but I have not yet receivedany answers – this would be a very important step.Research will take up the desired place.
The immediate problem is finding people interestedin working exclusively in palliative care. Unlike otherEuropean countries, Portugal does not have an excessof doctors and nurses, so that recruitment of profes-sionals to the unit will not be easy.
Other remarks
Since the opening of the unit, almost 6 years ago, pallia-tive care has not evolved much further in Portugal.There are a few other experiences, but the overallpicture is very poor. The implementation of palliativecare has been difficult in most countries, and in

162 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
13
7
Portugal it will not be any different. Many still seepalliative care not as a resource with its own knowledgeand skills, but as what is offered in places wherenursing and psychological and religious support are themost important aspects whilst the medical input has asecondary, and not especially skilled, role. Somemedical oncologists, for example, claim that theyshould take care of their patients until their death,forgetting that the reality is different in most cases andthat the care patients need when curative treatment isno longer useful must be learned, and is often not whatthey are providing. However, not all patients need tobe treated by palliative care specialists. As in otherspecialties, many patients can be treated by their ownphysicians with some training, but there are difficultsituations that require specialized resources of differenttypes. In addition, research and teaching should becarried out, and usually only specialists have the knowl-edge, the experience, the readiness, and a sufficientlylarge number of patients for this.
Palliative care is now needed in Portugal and mustbe developed. However, I suspect, unfortunately, that it
will be a long time before a serious effort is made to dothis. Nonetheless, something must be done quickly.Palliative care can be provided in many differentcircumstances. Palliative care units are indispensable, inmy view, but home care and inpatient support teamsare examples of other options that would be easier toimplement. In my opinion, it is more important to dosomething useful immediately for patients withadvanced chronic diseases who are suffering unneces-sarily than to wait for conditions that anyone mightimagine to be ideal. When we started, for example,conditions were not ideal, because the unit was not yetready. So, professionals and hospital staff memberswith an interest in this field should start however localconditions allow and then improve their situation at therate that is possible, but without ever forgetting thetraining needed. I also believe that doctors have aspecial responsibility, because if they know and applythe principles and skills of palliative care, even alone,they can have a very important impact on the well-being of their patients with chronic advanced diseases.
References
1. Saunders C (1998) Foreword. In:Doyle D, Hanks GWC, MacDonald N(eds) Oxford Medical Publications,Oxford, pp v–ix
2. World Health Organization (1990)Traitement de la douleur cancéreuse etsoins palliatifs. (Série de rapports tech-niques 804) WHO, Geneva

| 163 163Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
21
Diagnosis disclosure in a Portuguese oncologicalcentreJ Ferraz Gonçalves Director and S Castro Psychologist, Unidade de Cuidados Continuados, InstitutoPortuguês de Oncologia, Porto
Abstract: The disclosure of a diagnosis of cancer to patients is a controversial matter.There have been major differences in practice concerning this issue through time andbetween cultures. A questionnaire was sent to the doctors of the Oporto Centre of thePortuguese Institute of Oncology in order to assess their attitudes. We received 45 responses (40%) from the 113 questionnaires sent. Of these, 32 (71%) said thatthey disclose the diagnosis as a general policy or at the patients’ request, and 13 (29%)disclose it rarely or not at all. The most frequent reason indicated by these 13 physicianswas that the disclosure might damage the patients psychologically. Forty-four (98%)doctors inform the family of the diagnosis. Thirty-nine (87%) think that patients aresatisfied with the information provided. This study was carried out in one oncologicalcentre only, so it is inappropriate to conclude that this is what happens throughoutPortugal. As far as we know, this is the first study in Portugal addressing this area ofpractice. This subject is a very important topic of research both in Portugal and in othercountries, as many published recommendations are not research based.
Key words: breaking bad news; communication; diagnosis disclosure; physician–patientrelation
Resumo: A revelação do diagnóstico aos doentes com cancro é um assuntocontroverso. Tem havido grandes diferenças na prática respeitante a esta questão aolongo do tempo e entre as diversas culturas. Enviámos um questionário aos médicosdo Centro do Porto do Instituto Português de Oncologia para avaliar as suas atitudes.Recebemos 45 respostas (40%) dos 113 questionários enviados. Destes, 32 (71%)dizem que revelam o diagnóstico por princípio ou quando os doentes o pedem e 13(29%) revelam-no raramente ou nunca. A razão mais frequentemente indicada por estes13 médicos foi a de que a revelação pode causar dano psicológico aos doentes.Quarenta e quatro (98%) médicos informam a família do diagnóstico. Trinta e nove(87%) pensam que os doentes estão satisfeitos com a informação dada. Este estudofoi feito num único centro oncológico, por isso não podemos dizer que é isto que sepassa, de um modo geral, em Portugal. Tanto quanto sabemos, este é o primeiro estudorealizado em Portugal sobre este aspecto da prática médica. Este é um tópico deinvestigação muito importante tanto em Portugal como noutros países, porque muitasrecomendações práticas publicadas não se baseiam na investigação.
Palavras-chave: dar más notícias; comunicação; revelação do diagnóstico; relaçãomédico–doente
Palliative Medicine 2001; 15: 35–41
© Arnold 2001 0269–2163(01)PM396OA
Address for correspondence: Dr J Ferraz Gonçalves, Unidadede Cuidados Continuados, Instituto Português de Oncologia, R. Dr. António Bernardino de Almeida, 4200-072 Porto,Portugal.
06PM396 9/1/01 3:28 pm Page 35

164 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
22
Introduction
The disclosure of a diagnosis of cancer to patientsis a controversial matter. The dominant attitudeamong physicians has changed over time, and therehave always been voices advocating against it.1 Wewill also find different attitudes when we comparepractice in countries with different cultures. In theUnited States and northern European countries,2–4
for example, the usual practice is to disclose thediagnosis. However, in other countries, includingthose of southern Europe,4–8 the situation is dif-ferent: doctors’ attitudes are more paternalistic, andin many cases they do not disclose the diagnosis.
In Portugal, the current practice seems to be oneof non-disclosure. However, as far as we know, noresearch on this subject has been carried out inPortugal.
Methods
We conducted a survey in the Oporto Centre of thePortuguese Institute of Oncology, which is one ofthe most important Portuguese oncological centres.It has 350 beds and about 4000 new patients areadmitted every year. It has services and equipmentequivalent to those of any major European oncolo-gical centre, including a palliative care unit. Thiscentre is a public hospital that serves the populationfrom the whole of northern Portugal. The patientsbelong to all social classes and education levels.
A questionnaire (see the Appendix), specificallydesigned for this study but not subjected to a pilottest, was sent to each doctor at the centre whotreated adult patients. Those with other functions,such as radiologists and pathologists, were exclu-ded. This study was approved by the Ethics Com-
mittee of the Portuguese Institute of Oncology –Oporto Centre.
Results
The questionnaire was sent to 113 doctors, and45 responses (40%) were obtained. In Table 1 weshow the specialities and demographic data of thedoctors who returned the questionnaires. There isa similar percentage in all specialities, with the ex-ception of radiotherapy (Table 1). Nineteen (42%)participants added comments, clarifying their viewsor adding other hypotheses to those included in thequestionnaire. The questions most commented onwere: the one that asked if doctors disclose thediagnosis of cancer to the patients, and if not, whynot; and the questions about the patients’ andfamilies’ participation in therapeutic decisions.
Among our respondents, 14 (31%) doctors statedthat their policy was to disclose the diagnosis, three(7%) do not do it at all, 10 (22%) rarely do it and18 (40%) disclose it only at the patient’s request(Table 2). A much higher number, 44 (98%),inform the family about the patient’s diagnosis; inone case (2%) the answer was omitted. The mostfrequent reason indicated by the 13 doctors (34%),who rarely or never disclose the diagnosis topatients (Table 3), for so acting was the possibilityof damaging the patients psychologically (11, 85%).The comments added to the questions about thedisclosure to patients and the reasons for not dis-closing the cancer diagnosis, again, show a concernwith the eventual psychological damage that the dis-closure might produce. Some examples of thesecomments can be seen in Table 4.
To the question ‘do your patients often requestmore information from you?’ 29 (64%) answered
36 J Ferraz Gonçalves and S Castro
Table 1 Doctors’ speciality and demographic data
Speciality No. of questionnaires No. of questionnaires Total returned Returned per specialitysent returned (%) (%)
Surgery 52 22 49 42Medical oncology 24 12 27 50Radiotherapy 24 5 11 21Other 13 6 13 46Total 113 45 100
Age: mean 46 years (range: 31–65 years); median 45 years.Sex: male 27 (60%); female 17 (38%); not stated 1 (2%).
06PM396 9/1/01 3:28 pm Page 36

| 165 165Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
23
yes and 16 (36%) answered no. These 16 doctorspresume that their patients are satisfied with theinformation they get, or simply do not wish anymore information at all (Table 5). This agrees withthe answers to question 4, to which 39 (87%) saidthat they think their patients are satisfied with theinformation they give them.
Forty-one doctors (91%) think that patientsshould participate in decisions about treatment andfour (9%) think they should not. The reasons forthese opinions are shown in Tables 6 and 7. Only 25(56%) thought that family members should parti-cipate in making treatment decisions. The fewcomments about the patients’ participation in thera-peutic decisions suggest that they should not parti-cipate or even influence them. It was, however,conceded that if offered two equally effective treat-ments the patient can choose the one that is morebearable for him or her. Similar comments weremade about family participation in these decisions.One respondent stated that the decision belongs todoctors, and that family can be involved to encour-age the patient to accept the recommended treat-ment and to endure its toxicity.
Diagnosis disclosure in a Portuguese oncological centre 37
Table 2 Diagnosis disclosure to the patient
No. (%)
Yes 14 (31)No 3 (7)Rarely 10 (22) At patient’s request 18 (40)
Table 3 Reasons invoked for rare or non-disclosure (13doctors)
Reason Yes No
Difficulties in discussing the diagnosis 0 13Not prepared to deal with the situation 0 13Not useful to the patient 3 10Psychologically deleterious 11 2Not having enough time 2 11Others 4 9
Table 4 Examples of comments to questionnaire questions1 and 2
� The decision to disclose the diagnosis should considerthe psychological, intellectual, cultural and socialconditions of the patient
� It is necessary to inform the patients gradually and withsensitivity and gentleness, without coldness
� After the information has been provided, psychologicalsupport is needed
� Most patients are not prepared to receive theinformation of a malignant disease
� The information must be given when it is useful to thepatient
� The information can cause depression� Never use the word cancer� Patients often ask for information to feel hopeful in their
lives (we understand this statement means that thepatient does not really want the truth but a negativeanswer)
Table 5 Reasons to explain why patients often do not re-quest more information from their doctors (16 doctors)
They are satisfied with the information they havebeen given 7
They are not at ease to ask questions 1They do not wish for more information 5They feel you do not have enough time to talk to them 2They think they will not understand the information
you can give 0
Table 6 Reasons why patients should participate in treat-ment decisions (41 doctors)
To preserve patient autonomy 25To make the adherence to treatment easier 35To protect the doctor from legal problems 19To allow the patient to prepare himself for adverse
effects 30To allow the patient to refuse the treatment
eventually 23Other 4
Table 7 Reasons why patients should not participate intreatment decisions (four doctors)
It is difficult for you to discuss treatment withpatients 1
You think it is not useful to patients 2You do not have enough time to discuss treatment
with the patients 4The discussion might damage the patients
psychologically 1Other 1
06PM396 9/1/01 3:28 pm Page 37

166 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
24
Discussion
This study was carried out in an oncological centre,where informing patients about their diagnoses is aneveryday matter.
We only had a 40% response rate, which is ratherlow although similar to that obtained in at least onevery important paper.2 This must be borne in mindwhen considering our findings. The reason why radio-therapists participated less than other specialists isnot clear.
The percentage of doctors (71%) who disclose thediagnosis of cancer as their general policy or whenrequested by patients is smaller than that found inother studies in which questionnaires were add-ressed to doctors,2–4 even some of those carried outin southern European countries.4 But the practiceof informing the family almost always (98%) is thesame as what usually happens in those countries.5
Doctors’ most frequently indicated the reason forrarely or never disclosing the diagnosis was that itmight damage the patients psychologically. It seemsthat those doctors prefer to protect the patientsfrom possible psychological damage rather than torespect their autonomy. A lack of training in dealingwith requests for information was not suggested asa reason for these responses. Doctors whose expe-rience is not to have frequent requests for informa-tion feel that this happens because the patients aresatisfied with the information they get or becausethey just do not want more information at all.Indeed, 87% think that patients are satisfied withthe information provided and this percentage ishigher than those who inform their patients as ageneral policy or when requested. The commentsalso show a concern for the patients’ protection:‘inform with sensitivity and gentleness’; ‘withoutcoldness’; ‘inform those we think have sufficient psy-chological and intellectual resources’; ‘the need forpsychological support’; ‘the information can causedepression’; ‘never use the word cancer’. Again, adecision not to inform seems to be due not to a lackof training or difficulty in dealing with the situationbut to have its roots in a protective attitude to thepatients, in order not to affect them psychologicallyand may be understood as what they really want. Infact, in a study conducted in Spain,6 with a culturesimilar to that of Portugal, of the 68% of 97 patients
admitted to an oncological service and a palliativecare unit who had not been informed of their diag-nosis, 42% did not want to receive more infor-mation. An alternative explanation of our results is,perhaps an element of denial, because breaking badnews is recognized by most experts as being difficultand causing some degree of discomfort, even forexperienced professionals;9 in Portugal this problemis not addressed in any way, except in some limitededucational activity. It is possible that doctors arehiding their own difficulties in dealing with theseaspects of communication behind a paternalisticattitude. Communication with patients can belearned, but denial can delay or prevent the decisionto act accordingly. However, we must be very care-ful with the interpretation of the results obtainedand avoid preconceptions.
It seems to be a contradiction that 91% of thedoctors think that patients should participate intreatment decisions, because this percentage ishigher than those who inform patients, and withoutinformation about their disease it is not possible forpatients to decide rationally about the treatment.On the other hand, doctors think that family mem-bers, who are almost always informed, should parti-cipate in treatment decisions in a much smallerproportion of cases (56%). The comments aboutthe decisions also have a paternalistic characterwhen they state that patients should not decideabout treatment. However, these comments repre-sent a minority because 91% think that patientsshould participate in those decisions. The family isseen as a possible doctor ally, facilitating the ad-herence to treatment and helping the patient toendure the treatment decided on by the doctor.
The available data show that Portuguese doctors,who work in this oncological centre, disclose thediagnosis to patients less frequently than doctorsfrom other countries, including those of thesouthern Europe, such as Greece. This study wascarried out in one centre only so it is inappropriateto generalize, but the result obtained agrees with,or is even higher than, what we expected was hap-pening in Portugal.
This study reflects the way in which doctors seethemselves, not necessarily what happens, and ismore important, in our point of view, if the infor-mation is tailored to the desire of the individual
38 J Ferraz Gonçalves and S Castro
06PM396 9/1/01 3:28 pm Page 38

| 167 167Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
25
patient. So, it is also very important to know whatPortuguese patients think about medical informa-tion issues, not only disclosure of the diagnosis butalso about the prognosis and their participation intherapeutic decisions. The research on these topicsis very important and is not extensive. Most of themedical literature providing practical advice is notresearch based.10
To explain the differences in attitude betweenthe countries in what concerns cancer diagnosisdisclosure, cultural causes have been indicated.However, perhaps these cannot explain, at leastcompletely, those differences, because if we go backto the 1950s and 1960s we find that in the USA mostdoctors used not to disclose a cancer diagnosis totheir patients, but nowadays almost all do so.2 Thereasons for this change are certainly many: thespread of information in the media about cancertreatment advances (real or not) and the treatmentoptions available in some cases, where the choiceonly depends on patients’ wish (for example, con-servative breast surgery); the spread of informationon patients’ rights and the growing demand forquality of medical services; the patients’ enrolmentin research protocols demanding informed consent;and legal matters that involve the medical pro-fession. These matters are progressively arising inPortugal and other countries, and we believe that,as time goes by, the picture concerning cancer diag-nosis disclosure will be similar to that already pre-sent in the USA and northern European countries.
References
1 Reiser SJ. Words as scalpels: transmitting evidencein the clinical dialogue. Ann Intern Med 1980; 92:837–42.
2 Novack DH, Plumer R, Smith RL, Ochitill H,Morrow GR, Bennett JM. Changes in physicians’attitudes toward telling the cancer patient. J AmMed Assoc 1979; 241: 897–900.
3 Loge JH, Kaasa S, Ekeberg Ø, Falkum E, Hytten K.Attitudes toward informing the cancer patient – asurvey of Norwegian physicians. Eur J Cancer 1996;32A: 1344–48.
4 Thomsen OØ, Wulff HR, Martin A, Singer PA.What do gastroenterologists in Europe tell cancerpatients? Lancet 1993; 341: 473–76.
5 Mystakidou K, Liossi C, Viachos L, Papadimitrou J.Disclosure of diagnostic information to cancerpatients in Greece. Palliat Med 1996; 10: 195–200.
6 Cortés CC, Olarte JMN. Questioning diagnosisdisclosure in terminal cancer patients: a prospectivestudy evaluating patients’ responses. Palliat Med1994; 8: 39–44.
7 Estapé J, Palombo H, Hernández E et al. Cancerdiagnosis disclosure in a Spanish hospital. AnnOncol 1992; 3: 451–54.
8 Surbone A. Truth telling to the patient. J Am MedAssoc 1992; 268: 1661–62.
9 Buckman R. Communication in palliative care: apractical guide. In: Doyle D, Hanks GWC,MacDonald N eds. Oxford textbook of palliativemedicine, 2nd edn. Oxford: Oxford University Press,1998: 47–61.
10 Ptacek JT, Eberhardt RL. Breaking bad news. J AmMed Assoc 1996; 276: 496–502.
Diagnosis disclosure in a Portuguese oncological centre 39
06PM396 9/1/01 3:28 pm Page 39

168 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
26
Appendix
Diagnosis disclosure – survey
Age: ............................................................................ Speciality: ....................................................................
Gender: ...................................................................... Service: ........................................................................
1. Do you disclose the diagnosis to cancer patients?
Yes □ No □
Rarely □ At the patient’s request □
2. If the answer was No or Rarely, indicate the reasons:
You find difficult to disclose the diagnosis □
You were not prepared to deal with this information □
You do not find useful to the patient to know that information □
The disclosure might damage the patient psychologically □
You do not have time enough □
Other □
Specify:
3. Do you disclose the diagnosis to the family of cancer patients?
Yes □ No □
4. Do you think that your patients are satisfied with the information you give them?
Yes □ No □5. Do your patients often request more information from you?
Yes □ No □
(if you answered Yes, go to question 7)
6. You think your patients do not request more information from you often, because:
They are satisfied with the information they have been given □
They are not at ease to ask questions □
They do not wish more information □
They feel you do not have enough time to talk to them □
They think they will not understand the information you can give □
Other □
Specify:
40 J Ferraz Gonçalves and S Castro
06PM396 9/1/01 3:28 pm Page 40
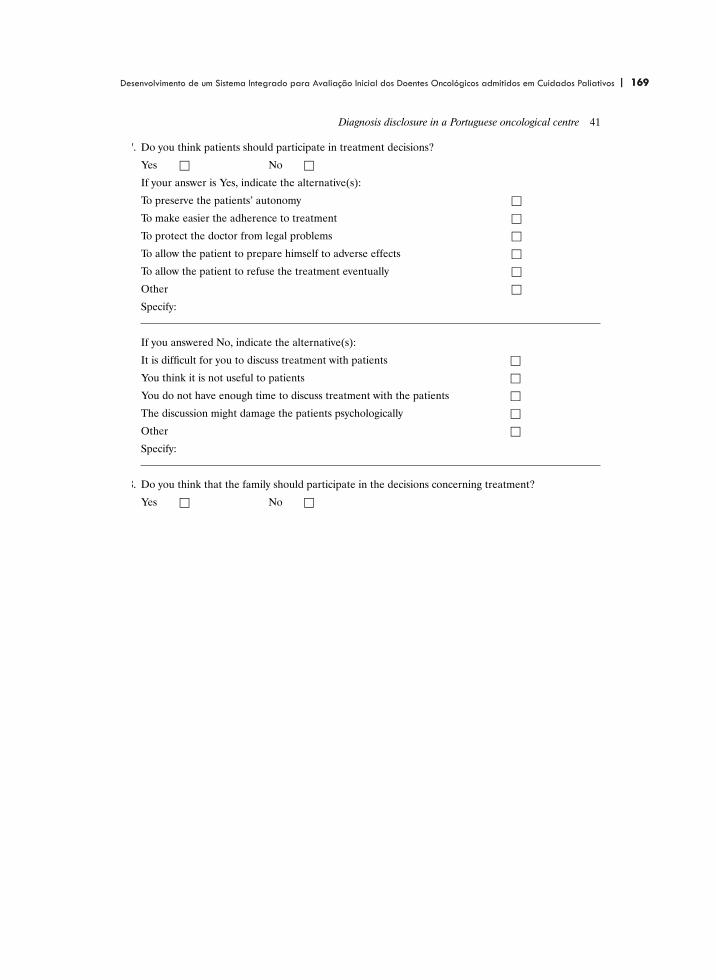
| 169 169Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
27
7. Do you think patients should participate in treatment decisions?
Yes □ No □
If your answer is Yes, indicate the alternative(s):
To preserve the patients’ autonomy □
To make easier the adherence to treatment □
To protect the doctor from legal problems □
To allow the patient to prepare himself to adverse effects □
To allow the patient to refuse the treatment eventually □
Other □
Specify:
If you answered No, indicate the alternative(s):
It is difficult for you to discuss treatment with patients □
You think it is not useful to patients □
You do not have enough time to discuss treatment with the patients □
The discussion might damage the patients psychologically □
Other □
Specify:
8. Do you think that the family should participate in the decisions concerning treatment?
Yes □ No □
Diagnosis disclosure in a Portuguese oncological centre 41
06PM396 9/1/01 3:28 pm Page 41

170 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 171 171Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
113
JOURNAL�OF�PALLIATIVE�MEDICINEVolume�6,�Number�6,�2003©�Mary�Ann�Liebert,�Inc.
The�Last�Forty-Eight�Hours�of�Life�in�a�PortuguesePalliative�Care�Unit:�Does�it�Differ�from�Elsewhere?
J.�FERRAZ�GONÇALVES,�M.D.,1 MARGARIDA�ALVARENGA,�R.N.,1
and�ALEXANDRA�SILVA,�R.N.2
ABSTRACT
The�last�few�days�of� life�have�received�significant�attention�in�the�literature.�Reports�haveshown�similarities�and�differences�between�programs.�As�a�palliative�care�service�in�a�cul-tural�context�that�has�not�been�reported�on,�we�thought�that�an�audit�of�our�own�experiencein�the�care�of�patients�in�the�last�48�hours�of�life�and�a�comparison�with�other�programs�wouldbe�important.�A�prospective�audit�was�designed�to�record�data�for�four�general�domains:�gen-eral� demographic� information,� symptom� prevalence,�patient� performance� status,� and� per-ceived�level�of�comfort.�The�inclusion�criteria�of�patients�were:�older�than�15�years�of�age�(anadmission�criterion�for�patients�of�the�unit),�diagnosis�of�cancer,�no�active�cancer-direct�treat-ments,�and�patients�who�were�on�the�unit�for�longer�than�48�hours.�The�audit�was�completedwhen�the�300th�eligible�patient�died�in�the�unit.�Twenty-nine�of�300�patients�(9.6%)�requiredsedation�and�the�most�common�cause�was�delirium.�Morphine�was�the�most�widely�prescribedmedication�(85%�of�patients).�The�subcutaneous�route�was�utilized�extensively.�Only�12%�ofthe�patients�received�parenteral�fluids,�usually�via�hypodermoclisis.�Death�was�consideredby�staff�to�have�been�peaceful�in�86%�of�cases.�Our�practice�appears�to�mirror� that�of�otherpalliative�care�groups.
895
INTRODUCTION
WITHIN THE CONTINUUM OF CARE that�palliativecare�provides,�the�last�few�days�of�life�have
received�significant�attention�in�the�literature.1–5
Issues� such�as� frequency� of�various� symptoms,symptom� management,� and� palliative� sedationare�among�the�subjects�that�have�been�reportedon.�These�reports,�from�various�centers�and�caresettings,� have� indicated� similarities� and� differ-ences�between�programs�and�have�prompted�dis-cussion�and�reflection.
Being�a�relatively�new�palliative�care�service6 in
a�cultural�context�that�has�not�previously�been�re-ported�on,�we� felt� that� it�would�be� important� todocument�our�own�experiences� in� caring� for�pa-tients�in�the�last�48�hours�of�life�and�compare�thesewith�experiences�of�other�programs�for�the�purposeof�clinical�audit�and�improvement�of�care.�The�au-dit�focused�on�the�frequency�of�use�of�palliative�se-dation,� the� indications� for�palliative� sedation,� thepresence�of�various�symptoms�and�problems,�andwhether�or�not�the�interdisciplinary� team�felt�thatthe� patients� appeared� comfortable� or�not,� recog-nizing� the� limitations� of� viewing� this� parameterfrom�a�health�care�professional’s�perspective.
1Unidade�de�Cuidados�Continuados,�Instituto�Português�de�Oncologia,�Porto,�Portugal.2Serviço�de�Medicina�A,�Hospital�de�S.�Pedro-Vila�Real,�Vila�Real,�Portugal.

172 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
114
METHODS
A�prospective�audit�was�designed�to�record�var-ious�facets�of�care�during�the�last�48�hours�of�lifeprior�to�the�death�of�patients�admitted�to�the�pal-liative�care�unit�of�the�Portuguese�Institute�of�On-cology�of�Porto,�Portugal.�Data�were�collected�onfour�general�domains:�general�demographic�infor-mation,�symptom�prevalence,�patient�performancestatus,� and�perceived� level� of�comfort�(the� latterperceived� by� the� attending� physician� and/ornurse�present�at�the�time�of�death).�A�data�record-ing�sheet�was�utilized�to�document�the�data.
The� inclusion� criteria� of� patients� were:� olderthan�15�years�of�age� (an�admission�criterion� forpatients�of�the�unit),�diagnosis�of�cancer,�no�ac-tive� cancer-direct� treatments,� and� patients� whowere�on�the�unit�for�longer�than�48�hours.�Patientswho�were�on�the�unit� for� less� than�48�were� ex-cluded�from�this�audit.
All�consecutive�admissions�to�the�unit�were�re-viewed� and� the� audit� was� completed� once� 300consecutive�patients�who�met�the�inclusion�crite-ria�had�been� admitted.�The�audit�was�begun� inJanuary�1995� and�completed� in�July�1998,� whenthe�300th�eligible�patient�died�in�the�unit.
For�the�purposes�of�this�audit,�the�presence�orabsence� of� a� symptom� or� problem� was� docu-mented.�Many�patients� in� their� last� 48�hours�oflife� are� unable� to� report� the� intensity� of� theirsymptoms�for�reasons�of�frailty�or�confusion.�Aspart�of�the�normal�practice�of�the�unit,�the�pres-ence�or�absence�of�various�symptoms�and�prob-lems�are�recorded�on�a�daily�basis�using�a�stan-dardized�checklist.�In�addition�to�more�commonsymptoms� such� as� pain,� dyspnea,� and� nausea,other�problems� such� coughing,� fever,� sweating,myoclonus,�hemorrhaging,�upper�airway�rattlingfrom� secretions,� urinary� retention,� catheteriza-tion,� and� ostomy� tubes� are� routinely� docu-mented.�These� data� were� analyzed� for�the� pur-pose�of�this� audit.� The� symptoms�are� routinelymeasured�in�the�unit�using�a�0�to�4�scale,�where0�indicates�the�absence�of�symptoms�and�4�indi-cates�an�unbearably�high�intensity�of�that�symp-tom.�The�range�of�symptoms�is� similar� to�thoseused� in� the� Memorial� Symptom� AssessmentScale.7 A�verbal�scale�(none,�light,�moderate,�se-vere,� unbearable)� is� utilized� when� patients� areunable�to�use�the�numeric�scale.�When�this�hap-pens,�the�data�are�transformed�to�a�numeric�scaleso� as� to� facilitate� data� entry� and� analyses.� Forthose�patients�who�are�unable�to�report�their�own
symptom� distress� and� intensity,� a� nurse� or� aphysician�does�a�proxy�assessment.�However,�itis� recognized� that� proxy� assessments� by� bothhealth�care�providers�and�families� are�often�un-reliable.8 It� is�also�customary�on�the�unit� to�ex-clude� certain� symptoms� such� as� fatigue� andanorexia�from�the�list�of�symptoms�when�patientswere�frail�and�obviously�in�their�last�days�of�life,to�minimize�patient�burden,�and�because�their�as-sessment� is�unlikely� to�modify�management.� Inaddition�to�the�scales,�the�presence�or�absence�ofcertain� problems� such� as� hemorrhaging,� fever,urinary� incontinence� and� retention,� and� my-oclonus�is�recorded�using�a�checklist.
The�short�version�of�the�Confusion�AssessmentMethod� (CAM)9 is� used� to� screen� for�delirium.The�CAM�is�applied�once�a�week�and�wheneverthere�is�any�mental�alteration�detected�by�a�mem-ber�of�the�staff�or�family.
For�the�purposes�of�this�audit,�communicationwas�broadly�defined�as�the�ability�to�understandat�least�simple�questions�(example:�Do�you�havepain?)�and�make�oneself�understood,�even�if�in-termittently.
The�definition�by�Chater�et�al.10 of�palliative�se-dation� was� used:� “The� intention� of�deliberatelyinducing�and�maintaining�deep�sleep,�but�not�de-liberately� causing�death�. . .�for�the�relief�of�oneor�more�intractable�symptoms�when�all�other�pos-sible�interventions�have�failed�and�the�patient�isperceived� to�be�close�to�death� . . .�”�At�the�startof� this� audit,� this� definition� had� not�been� pub-lished�and�a�broader�definition�was�being�used.When�this�definition�was�published,�we�felt�thatit�constituted�a�more�reliable�definition�and�there-fore� conducted� a� retrospective� review� of� thecharts,� applying� the� definition� suggested� byChater�and�colleagues.�The�policy�on�the�unit�isto�include�patients,� if�they�are�competent,�in�thedecision-making� process� when� palliative� seda-tion�is�considered.�If� incompetent,� family� mem-bers�or�guardians�are�approached.�Exceptions�tothis�are�when�patients�are�incompetent�and�fam-ily�members�absent�when�unexpected�crises�thatrequire�prompt�sedation�occur.
The� physicians� of� the� unit� also� indicatedwhether�or�not�the�patient’s�death�was�expectedand�if�they�felt�the�patient�was�“comfortable�andpeaceful”�in�the�last�48�hours.�For�the�purpose�ofthis� study,�peacefulness� was� defined� as� a� goodlevel�of�comfort�from�the�perspective�of�the�physi-cian� and/or�nurse�present� at� the� time�of�death.The�medications�administered�were�also�audited.
GONÇALVES�ET�AL.896

| 173 173Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
115
The� attending� physician,� with� the� nurseand/or�the�physician�present�at�the�time�of�death,was� required� to� review� the� patient� chart� andrecord�the�data�within� 48�hours�of�the�patient’sdeath�on�the�data�form.
The�palliative� care�unit� is�a� freestanding�unitwithin�an�oncology�center�complex�in�Porto,�Por-tugal.�It�started�with�5�beds�and�now�has�20�beds6
and� shares� resources� with� the� oncology� center.The�unit�receives�its�referrals�from�the�cancer�cen-ter.� Physicians,� nurses,� a� psychologist,� a� socialworker,�and�a�nutritionist�make�up�the�unit’s�in-terdisciplinary�team.
The�investigators�did�not�seek�approval� fromthe�institution’s�ethics�research�board�on�the�ba-sis�that�the�data�collected�were�derived�from�nor-mal� daily� screening� and� evaluation� practices.Moreover,�the�study�did�not�evaluate�any�directintervention�on�patients.�However,�the�investiga-tors�acknowledge� that� current� standards�wouldlikely�require�approval�from�an�ethics�board.
RESULTS
From�January�1995� to�the�closure�of�the�auditin�July�1998�a�total�of�597�patients�were�admittedto�the�unit.�Of�these,�354�died�(59%)�and�243�(41%)were�discharged�back�home�or�to�other�hospitals.Fifty-four� patients� died� within� 48� hours� of� ad-mission� to� the� unit� and� were� therefore� not� in-cluded� in� the� analysis.� Three� hundred� patientsmet� the� inclusion� and� exclusion� criteria.� Thesenumbers� represent� patients� not� admissions,� al-though�some�patients�had�more�than�one�admis-sion.
The�demographic�profiles�of�the�300�eligible�pa-tients�are�listed�in�Table�1.�Table�2�lists�the�preva-lence�of�symptoms�and�problems�experienced�bythe�300�eligible�patients�in�the�last�48�hour�of�theirlives.
Twenty-nine� of� 300� patients� (9.6%)� requiredpalliative� sedation.�The�indications�for�these�arelisted�in�Table�3.�Delirium�was�the�most�commonindication�for�palliative�sedation.�Palliative�seda-tion�was�initiated�in�one�patient�after�the�patientrequested�to�be� sedated.�This�patient� had�bron-cheoloalveolar� carcinoma�of�the� lung�with� dys-pnea�and�anxiety�that�worsened�and�became�un-treatable� a� few� hours� before� death.� Palliativesedation�was�implemented� in�two�patients�for�acombination�of�intractable�symptoms:�the�first�forpain� and� dyspnea� and� the� second� for� agitationand� dyspnea.� Midazolam� was� the� most� fre-quently� used� drug� to� achieve� palliative� seda-tion—26�patients�requiring�sedation�received�thismedication.�The�time�from�starting�the�palliativesedation� and� death� was� 20.5� hours� (mean)� and9.0�hours�(median),�with�a�range�of�5�minutes�to72.5�hours.
One�hundred�forty-six�of�the�300�patients�(49%)patients�entered�the�last�48�hours�of�their�life�witha�normal� consciousness�level.� Of�these�patients,only� 26� (9%)� maintained� a� full� level� of� con-sciousness� up� until� the� time� of� the� death.� Onehundred� sixty-nine� (56%)� were� communicative.This�decreased� to�42� (14%)�patients� on�the�dateof�death.�Thirty-one�(10%)�were�walking�with�theassistance�of�others�2�days�before�dying�and�only10�patients�(3%)�were�walking�without�assistance.Nine� (3%)�were�mobile�up�to�the�time�of�death.
PORTUGUESE�PALLIATIVE�CARE�UNIT 897
TABLE 1. DEMOGRAPHICS AND PRIMARY TUMORS
Tumor No. (%)
Head�and�neck 44 15Stomach 42 14Breast 39 13Colorectal 29 10Lung 25 8Cervix 21 7Gastrointestinal�others 14 5Genito-urinary�male 12 4Ovary 9 3Multiple 9 3Other 56 19
Gender:�male,�148�(49%);�female,�152�(51%).Age:�median,�61�years;�range,�17–95.Length�of�stay:�median,�14�days;�range,�2–121.
TABLE 2. SYMPTOM PREVALENCE IN
THE 300�ELIGIBLE PATIENTS
Symptom No. (%)
Delirium 146 49Incident�pain 141 47Death�rattle 139 46Fever 118 39Dyspnea 105 36Sweating 93 31Nausea/vomiting 51 17Cough 48 16Hemorrhage 45 15Background�pain 26 9Myoclonus 18 6Seizures 6 2Incontinence�urinary 66 22Retention� urinary 24 8

174 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
116
Table�4�lists�the�medications�used�in�the�last�48hours.�Morphine�was�the�most�widely�prescribedmedication�and�255�patients� (85%)�were�on�thisopioid�in�the�last�48�hours�of�life.�Dexamethasone,haloperidol,�and�midazolam�were�used�relativelyfrequently� in�contrast�to�drugs�such�as�antibiot-ics,� nonsteroidal� anti-inflammatory� drugs,� anddiuretics,� which� were� used� less� frequently.� Thesubcutaneous� route� of� administration� was� uti-lized� extensively.� Only� a� small� number� of� pa-tients�(12%)�were�receiving�parenteral�fluid�in�thelast�48�hours�and�when�administered�was�usuallyvia� subcutaneous� hypodermoclysis.� In� mostcases,�a�combination�of�different�routes�was�usedin�patients.
The�attending�physicians�recorded�that�16�(5%)deaths�were�unexpected.�The�physicians�and/ornurses�felt�that�the�last�48�hours�were�peaceful�in258�patients�(86%).�Of�the�42�patients�(14%)�thatthey�thought�were�uncomfortable,�8�required�se-dation—4�patients� for�hemorrhaging,� 3�patients
for�delirium,� and�1�patient� for�a�combination�ofdyspnea�and�pain.
DISCUSSION
Delirium�was�the�most�frequent�symptom,�af-fecting�almost�half�of�the�patients.�This�and�thefrequency�of�other�symptoms�such�as�pain� anddyspnea�are�consistent�with�previous�reports.11–13
The�relatively�high�frequency�of�“incident�pain”reported� here� can� be� somewhat� misleading� be-cause� in�cognitively� impaired�patients� the�pain-related� behavior� can� be� difficult� to� distinguishfrom�delirium-related�behavior.�Therefore,�somecases�ascribed�by� the� staff�as�pain� with�passiveturning�of�patients�in�bed�were�likely�manifesta-tions�of�delirium.�Respiratory�tract�“rattling”�oc-curred� frequently� and� was� in� most� cases� man-aged�by�reassuring�families.�When�severe,�it�wastreated�pharmacologically� with�hyoscine�hydro-bromide� (scopolamine),� although� the� impact� ofthis� on� patient� comfort� is� uncertain.� Fever� andsweating� are� rarely� mentioned� in�other�studies,but�in�this�audit�they�occurred�in�a�high�percent-age.� Future� studies� should�assess� the� impact� ofthese�problems�on�patient�comfort�and�quality�oflife.
A�relatively�small�number�of�patients�(10%)�re-quired�palliative� sedation.�This�number�is�lowerthan�the�rates�reported�in�other�acute�and�tertiaryunits.1,2,5,14,15 However,� this� may� be� difficult� to
GONÇALVES�ET�AL.898
TABLE 3. REASONS FOR SEDATION
No. (%)
Delirium 15 51.7Hemorrhage 6 20.7Dyspnea 5 17.2Patient�wish 1 3.4Pain/dyspnea 1 3.4Agitation/dyspnea 1 3.4Total 29 100
TABLE 4. FREQUENCY OF USE OF DIFFERENT MEDICATIONS IN THE LAST 48�HOURS
Total Oral SC IV Other
Drug No. % No. % No. % No. % No. %
Morphine 255 85 42 14 212 71 2 1 21 7Dexamethasone 111 37 44 15 56 19 5 2 11 4Midazolam 100 33 0 0 94 31 1 1 10 3Haloperidol 100 33 21 7 74 25 0 0 10 3Laxatives 79 26 73 24 0 0 0 0 10 3Scopolamine�butylbromide 70 23 0 0 68 23 2 1 0 0Scopolamine�hydrobromide 68 23 0 0 68 23 0 0 0 0Lorazepam 68 23 37 12 0 0 0 0 31 10Metoclopramide 66 22 16 5 51 17 2 1 2 1Paracetamol 53 18 23 8 0 0 0 0 30 10Salbutamol 36 12 0 0 0 0 0 0 36 12Parenteral�fluids 35 12 0 0 25 8 14 5 0 0Antibiotics 26 9 12 4 0 0 14 5 4 1NSAIDs 24 8 13 4 9 3 0 0 2 1Diuretic 18 6 20 7 0 0 0 0 2 1
No.�means�the�number�of�patients�who�use�the�drug;�total�or�by�the�indicated�route.SC,�subcutaneous;�IV,�intravenous;�NSAIDS,�nonsteroidal�anti-inflammatory�drugs.

| 175 175Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
117
compare� because� of� inconsistencies� in� definingpalliative� sedation.
Midazolam�was�the�most�frequently�used�drugfor�sedation.�However,�there�were�differences�inthe�method�depending�on�the�symptom.�In�agi-tated�delirium,�haloperidol�was�often�used�first-line.� In�dyspnea,�midazolam�was�used�first-lineif�sedation�was�required.� In�hemorrhage�a�stan-dardized�protocol�was�used�with�morphine�10�mgand� midazolam� 10� mg� intramuscularly� as� rec-ommended� in� the� Oxford� Textbook� of� PalliativeMedicine16;�more�recently�we�changed�the�proto-col� to� midazolam� 15� mg� intramuscularly.� Thisroute�is�used�because�significant�vasoconstrictionlimits�the�subcutaneous�route.�Otherwise,�the�in-tramuscular� route� is� rarely� used� to� administerdrugs.
The�most�frequent�indications�for�palliative�se-dation�in�our�audit�were�delirium�and�dyspnea.Intractable� pain� was� an� uncommon� reason� for�initiating� palliative� sedation.�These� findings�areconsistent�with�the�results�of�studies�in�other�cen-ters.5,14,15 The�relatively�high�frequency�of�pallia-tive�sedation�for�hemorrhaging�probably�reflectsthe�large�numbers�of�patients�admitted�with�headand�neck� tumors,�many�of� them�with� large,� ul-cerating�lesions.
Unlike�North�America,�advanced�directives,�in-cluding� do-not-resuscitate� orders,� are� generallynot�discussed�with�patients.� Furthermore,� thereis�no�legislation�that�mandates�these�discussions.This�may�reflect�the�same�paternalistic�approach,fears,�and�discomforts�of�health�care�profession-als� to�discuss� this� issues� with� terminally� ill� ob-served�in�North�America�a�few�decades�ago.
Our�decision�to�assess�the�perception�of�deathfrom�a�health�care�professional’s�perspective�wasbased�on�the�impact�that�dying�has�on�staff.�Whilemuch�time� is� justifiably�dedicated� to�evaluatingthe�last�stages�of�dying�(last�48�hours)�from�a�pa-tient’s� and� family’s� perspective,� reviewing� theperception�of�staff�merits� attention.�The�staff� inour�audit� considered�death�nonpeaceful� in�14%of�patients.�The�impact�of�this�on�staff�needs�tobe�explored,�along�with�ways�to�better� improvecare� in�the� last�days�of�life,� to�prepare� for�diffi-cult� cases� and� become� aware� of� personal� re-sponses�and� team� responses� to�difficult� deaths.Interestingly,�eight�of�the�patients�whom�staff�feltexperienced� a� nonpeaceful� death� were� sedated.This�perception�need�to�be� further�explored�be-cause� it� may� reflect� the� staff’s� own�discomfort,rather� than�that�of�the�patient’s.�Although�there
are� limitations� to� defining� and� standardizing“peacefulness”� as� perceived� by� the� health� careprofessionals,�this�problem�has�an�important�im-pact�on�the�staff.�Opportunities�for�debriefing�arerequired.
Morphine�was�the�most�used�drug�more�oftenby� the� subcutaneous� route.� It� was� used� in� thetreatment� of� pain� and� dyspnea.� The� subcuta-neous�route�was�the�most�used�in�this�phase�be-cause�it�is�the�most�convenient�alternative�to�theoral�route.�However�most�patients�had�more�thanone�route�used.�The�intravenous�route�was�alsoused�in�a�few�cases.�We�use�the�intravenous�routemainly�when�patients�already�have�peripheral�orcentral�access�at�the�time�of�admission.�Parenteralhydration�is�administered�infrequently.�When�in-dicated,� we� generally� administer� via� hypoder-moclysis.
Apart� from� standardizing� the� definition� ofpeacefulness,�this�study�has�several�other�limita-tions.�The� retrospective� assessment� of� sedation,introduced� towards� the� end� of� the� study,� mayhave�provided� less�accurate� information� than� ifit�were�done�prospectively.� In�future�studies�se-dation�should�be�graduated�in�several�levels,�andnot�just�seen�on�a�“yes”�or�“no”�basis,�because�thegoal�is�symptom�control�and�the�deepness�of�se-dation� to� reach� it� is� not� necessarily� always� thesame.� Assessing� the� symptom� intensity� is� chal-lenging.�Self-reporting�of�symptoms,�while�a�goldstandard,�is�often�not�possible�in�the�last�48�hours.Proxy-graded� observations,� made� by� profes-sional�or�by�a�family�member�have�been�shownto�be�largely�unreliable.8
The� results� of� this� audit� will� be� discussedamong�the�staff�in�order�to�identify�areas�for�im-provement�of�care.�What�can�be�done�about�pa-tients� whose� deaths� are� not� peaceful?� Couldsomething� else� be� done�at� least� in� some� cases?Should�some�of�those�patients�have�been�sedated?Are�our�feelings�interfering�with�our�practice?
CONCLUSIONS
We�recognize� the�need� for� regularly� ongoingclinical� audit� for� improvement�of�care.� It� is� im-portant�that�those�involved�in�palliative�care�au-dit�their�practice� in�order�to�compare�them�withthe�results�of�others�and�so�evaluate� the�qualityof�their�work�and�eventually� change� their�prac-tice.�While�in�many�ways�our�patterns�of�practiceappear�to�be�similar�to�other�groups,�several�areas
PORTUGUESE�PALLIATIVE�CARE�UNIT 899

176 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
118
for�improvement�and�reflection�have�been�iden-tified.
ACKNOWLEDGMENT
The� authors� are� grateful� to� Dr.� José� Pereira,from�the�Division�of�Palliative�Medicine,�Univer-sity�of�Calgary,�Calgary,�Canada,�for�his�invalu-able� help� and� advise� in� the� preparation� of� themanuscript.
REFERENCES
1. Ventafrida�V,�Ripamonti�C,�De�Conno�F,�TamburiniM,� Cassileth� BR:� Symptom� prevalence� and� controlduring�cancer�patients’�last�days�of�life.�J�Palliat�Care1990;6:7–11.
2. Peruselli� C,� Di� Giulio� P,� Toscani� F,� Gallucci� M,Brunelli�C,�Costantini�M,�Tamburini�M,�Paci�E,�Mic-cinesi�G,�Addington-Hall�JM,�Higginson�IJ:�Home�pal-liative�care�for�terminal�cancer�patients:�a�survey�onthe�final�week�of�life.�Palliat�Med�1999;13:233–241.
3. Turner� K,� Chye� R,� Aggarwal� G,�Philip� J,� Skeels� A,Luckiss�N:�Dignity� in�dying:�A�preliminary�study�ofpatients� in� the� last� three� days� of� life.� J�Palliat�Care1996;12:7–13.
4. Lichter� I,�Hunt�E:�The� last�48�hours�of� life.� J�PalliatCare�1990;6:7–15.
5. Fainsinger� R,� Miller� MJ,� Bruera� E,� Maceachern� T:Symptom�control�during�the�last�week�of�life�on�a�pal-liative�care�unit.�J�Palliat�Care�1991;7:5–11.
6. Ferraz� Gonçalves� JA:� A� Portuguese� palliative� careunit.�Support�Care�Cancer�2001;9:4–7.
7. Portenoy� RK,�Thaler�HT,�Kornblith� AB,�Lepore� JM,Friedlander-Klar�H,�Kiyasu�E,�Sobel�K,�Coyle�N,�Ke-meny�N,�Norton�L,�et�al:�The�Memorial�symptom�as-sessment� scale:� an� instrument� for� the� evaluation� ofsymptom�prevalence,�characteristics�and�distress.�EurJ�Cancer�1994;30A:1326–1336.
8. Nekolaichuk�CL,�Bruera�E,�Spachynski�K,�MacEach-ern� T,�Hanson� J,�Maguire�TO:�A� comparison�of�pa-tient� and� proxy� symptom� assessments� in� advancedcancer�patients.�Palliat�Med�1999;13:311–323.
9. Inouye�SK,�van�Dyck�CH,�Alessi�CA,�Balkin�S,�SiegalAP,�Horwitz�RI:�Clarifying�confusion:�The�confusionassessment� method:�A�new�method� for�detection�ofdelirium.�Ann�Intern�Med�1990:113:941–948.
10. Chater�S,�Viola�R,�Paterson� J,�Jarvis�V:�Sedation�forintractable�distress�in�the�dying—A�survey�of�experts.Palliat�Med�1998;12:255–269.
11. Fainsinger�RL,�Tapper�M,�Bruera�E:�A�perspective�onthe�management�of�delirium�in�terminally�ill�patientson�a�palliative�care�unit.�J�Palliat�Care�1993;9:4–8.
12. Higginson� I,�McCarthy�M:�Measuring� symptoms� interminal�cancer:�Are�pain�and�dyspnoea�controlled?�JR�Soc�Med�1989;82:264–267.
13. Reuben�DB,�Mor�V:�Dyspnea�in� terminally� ill�cancerpatients.�Chest�1986;89:234–236.
14. Fainsinger� RL,�Landman�W,�Hoskings� M,�Bruera�E:Sedation� for� uncontrolled� symptoms� in� a� southafrican� hospice.� J� Pain� Symptom� Manage� 1998;16:145–152.
15. Fainsinger� RL,� Waller� A,� Bercovici� M,� Bengtson� K,Landman� W,� Hosking� M,� Nunez-Olarte� JM,� deMoissac�D:�A�multicentre� international� study� of�se-dation�for�uncontrolled�symptoms�in�terminally�ill�pa-tients.�Palliat�Med�2000;14:257–265.
16. Twycross�RG,�Lichter�I:�The�terminal�phase.�In:�DoyleD,�Hanks�GWC,�MacDonald�N�(eds):�Oxford�Textbookof�Palliative�Medicine. Oxford:�Oxford�University�Press,1993,�pp.�651–661.
Address�reprint�requests�to:Dr.�J.�Ferraz�Gonçalves
Unidade�de�Cuidados�ContinuadosInstituto�Português�de�Oncologia
R.�Dr.�António�Bernardino�de�Almeida4200-072� Porto
Portugal
E-mail: [email protected]
GONÇALVES�ET�AL.900

| 177 177Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
119
JOURNAL OF PALLIATIVE MEDICINEVolume 8, Number 3, 2005© Mary Ann Liebert, Inc.
Temporal Distribution of Deaths in Cancer PatientsDuring the Day in Different Settings
JOSÉ FERRAZ GONÇALVES,1 EUGÉNIA FONSECA,1 MARGARIDA ALVARENGA,1and MARIA ROSA MORAIS2
ABSTRACT
Background: All living organisms perform their functions normally according to circadianrhythms. Certain diseases, such as ischemic heart disease and asthma, produce symptoms thatare distributed during the day in a nonrandom fashion. Chronomodulated therapy with someregimens of chemotherapy and other drugs produce better results than traditional schedules.Even death is not evenly distributed during the day. Significant differences in the time ofdeath through the day could influence the work planning and care activities.
Objective: To determine whether timing of death from a population of cancer patients ad-mitted at our Oncology Institute varied during the day and according to different settings: athome (H), at the palliative care unit (PCU), and at other services (OS) of the hospital. Com-paring the timing of deaths from different settings can give some clues about the possible ex-istence of a circadian rhythm and the influence of external circumstances in the time of deathof cancer patients.
Design: We conducted a retrospective study of the records of time of death at the differentsettings.
Results: The study involved 772 patients from the PCU and 997 from OS who died betweenMay 25, 1996, and May 24, 2000, and 347 patients who died at H between April 1, 1999, andDecember 31, 2001. A statistically significant difference was found in the distribution of timeof death in patients at the PCU (p � .001), but not at OS or at H. There were two peaks be-tween 08:00 and 10:00 and between 00:00 and 02:00, and one trough between 04:00 and 08:00.This suggests that a temporal variation occurs in the time of death of cancer patients dyingin the PCU, but not in other settings.
Conclusions: The clinical relevance of the results obtained in this study would depend onthe amplitude of the eventual variation detected in the number of deaths during the day.Therefore, although there was a statistically significant variation at the time of death duringthe day, its amplitude is not high enough to make it clinically significant. The differencesobserved among the various settings suggest that, even if circadian rhythms exist at the timeof death in cancer patients, external factors can overcome these rhythms.
528
INTRODUCTION
ROTATION OF EARTH ABOUT ITS AXIS and its rev-olution about the sun produce rhythmic
events. These events influence the functioning ofall living organisms. The rotation about its axis
creates the succession of days and nights. The bi-ologic events connected with this succession re-peated with a period of about 24 hours are re-ferred to as circadian (circa, about; dies, day).These events result from the biological adapta-tion to the natural 24-hour cycle of light and dark-
1Palliative Care Unit and 2Statistics Service, Portguese Institute of Oncology–Porto Center.

178 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
120
TEMPORAL DISTRIBUTION OF DEATHS IN CANCER PATIENTS 529
ness. A biologic clock controls circadian rhythms,which is located in mammals in the suprachias-matic nuclei of the hypothalamus.1 At the sub-cellular level, circadian rhythms are generated bytranscriptional positive and negative feedbackloops involving multiple clock genes.1,2 The in-ternal clock has a free-running period of about 25hours that does not exactly match the 24-hourday.2 Therefore, the internal clock must be resetevery day to stay synchronized with the solartime. The main synchronizer in most species islight, but in humans, who use artificial light, thesynchronization is made by the sleep–wake cycleand, perhaps, social interactions.3
Traditionally, the internal milieu of the organismis seen as constant (the homeostatic theory).4 How-ever, the functional integrity of an organism de-pends mainly on the maintenance of synchronizedtemporal relationships between oscillating vari-ables.3 In human beings, body temperature, sleep,hormonal levels, cognitive and motor efficiency,urinary volume, and the like, vary, following a dailyrhythm. Circadian rhythms also influence the ac-tivity and metabolism of some medications, such aschemotherapy, which when chronomodulated canresult in less side effects, better objective response,and longer patient survival5,6; other examples aretheophylline, nonsteroidal antiinflammatory drugs,and corticosteroids.4 There are also variations in thesurvival of elderly patients associated with the timeof day they undergo hemodialysis,7 the frequencyof asthma attacks,8 myocardial infarction,9 anddeath itself.
Many studies indicate that the distribution ofsudden deaths of cardiac cause is not uniformduring the day.9–14 Only two reports exist15,16 inthe literature concerning the timing of death incancer patients, and both were conducted in pal-liative care units. Our study differs from these be-cause, besides including patients who died at ourpalliative care unit, patients who died at homeand at other services in the hospital were also in-cluded to see if the same pattern occurred in thosesettings and whether clues on the existence of acircadian rhythm at the time of death or externalcircumstances were more important.
The potential relevance of this study to clinicalpractice depends on the existence of a variationin the number of deaths during the day and onthe amplitude of this variation. If the differencesare high enough, the reflection about the possi-ble causes can lead to changes in work planningand care activities.
METHODS
The Porto Center of the Portuguese Institute ofOncology has 400 beds and admits about 4000new patients every year. The hospital has servicesequivalent to any advanced oncology center inEurope, as well as a palliative care unit (PCU).This center is a public hospital that serves thepopulation from the northern part of the country.Patients belong to all social classes and educa-tional levels. In the PCU, beyond the inpatientservice with 20 single rooms, patients are fol-lowed in an ambulatory regimen, home care regimen, and at the day center.17 All patients ad-mitted to the PCU had cancer, were not under-going any antineoplastic treatment, and wereolder than 15 years, since younger patients aretreated in the pediatrics service.
One hospital policy is to officially record pa-tients’ time of death, independently of which ser-vice this occurs. We retrospectively reviewedthese documents from patients who:
1. Died at the PCU from May 25, 1996 (the opening date of the PCU), until May 24, 2000.
2. Died during the same period of time at otherservices (OS), including Medical Oncology,Surgery, and Radiotherapy, with the exclusionof special services as the Bone Marrow Trans-plantation Unit, Intensive Care Unit, and Pediatrics.
3. Were followed by the PCU and died at home(H). The decision to include these patients wastaken later, and therefore the time of deathrecordings in this group began on April 1,1999. Also, due to the small number of patientsin this group, recordings were prolonged un-til December 31, 2001.
The homogeneity of the distribution of deathsduring the day was analyzed in periods of 1 hourusing the Pearson chi-square test for nonparamet-ric variables; that is, the actual hourly distributionof the number of deaths was compared with thenumber of deaths that would occur if the numberof deaths were evenly distributed during the day.Significance was accepted at the 95% confidencelevel.
RESULTS
Seven hundred and seventy two deaths oc-curred at the PCU and 997 deaths occurred at OS.

| 179 179Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
121
FERRAZ GONÇALVES ET AL.530
Of the 347 deaths that occurred at H, time of deathwas obtained from 251 (72%).
Figure 1 shows the frequency of death by timeat the PCU. The difference between the numberof deaths observed and the number of deaths ex-pected, if the distribution throughout the hoursof the day was uniform, was statistically signifi-cant: �2 � 54.438 (p � .001). The period with thegreatest number of deaths occurred between thetime interval of 08:00 and 16:00, followed by 00:00and 08:00. The lowest number of deaths occurredbetween 16:00 and 24:00 (Table 1), the most sta-ble 8-hour period, with very small hourly varia-tions. We can observe a trough between 04:00 and08:00 and peaks between 00:00 and 02:00 and08:00 and 10:00.
Figure 2 shows the distribution of deaths at OS.No significant variation in the distribution ofdeaths was observed: �2 � 30.024 (p � 0.1). Al-though no significant differences were observedat OS, the period with the highest number ofdeaths was observed between 08:00 and 16:00,followed by 16:00 and 24:00 and between 00:00and 08:00.
The distribution of deaths during the day at His shown in Fig. 3. No significant variation wasobserved in this setting: �2 � 24.815 (p � 0.2).
DISCUSSION
The results of our study show a statistically sig-nificant temporal variation in the number ofdeaths during the day at the PCU, but not in the
number of deaths at the OS of the institute or withpatients dying at H.
The data obtained from studies of cancer pa-tients dying at palliative care units show:
• In the study of Davies, a trough was observedbetween 02:00 and 05:00, without any peak.16
• The study of Neumann et al. shows a peak be-tween 08:00 and 10:00 and between 18:00 and20:0015 and, although not mentioned in thetext, a trough could be observed in one graphicpresented, between 00:00 and 04:00.
• Our study shows a prolonged trough between04:00 and 08:00, preceded by a peak between00:00 and 02:00, and followed by another peakbetween 08:00 and 10:00.
These three studies show in common a consis-tent trough in the number of deaths existing dur-ing the night, although the exact time variessomewhat among the studies, in patients dyingin palliative care units. Also, in two of these threestudies, a peak was observed between 08:00 and10:00.
The analysis of our data in the present studyraises some questions. One is whether the differ-
TABLE 1. FREQUENCY OF DEATHS IN DIFFERENT SETTINGS
PCU OS HHours (%) (%) (%)
0–7 31.9 32.7 35.18–15 39.2 33.9 32.216–23 28.9 33.4 32.7
FIG. 1. Frequency of deaths by time of day at the PCU.

180 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
122
TEMPORAL DISTRIBUTION OF DEATHS IN CANCER PATIENTS 531
ences observed in the distribution of time of deathare real. Recordings obtained from the H settingmay be inaccurate since patients’ death is notrecorded by a professional, whereas in the hos-pital setting (PCU and OS) this is unlikely. Theofficially recorded time of death does not excludesome small deviations relative to the real time.However, some inaccuracy of the records cannotbe completely excluded.
Accepting the differences as real, a possible ex-planation for the pattern observed in the PCUmay be the influence of factors related to routinepractices in the unit, such as medication sched-ules, and different levels of activity and care dur-ing the 24 hours and not to a natural occurrenceresulting from circadian rhythms. This can also
explain the differences in the exact time of thevariations observed among the studies of time ofdeath of cancer patients.
Can we establish an analogy or even a rela-tionship between cardiovascular events and thepattern of deaths of cancer patients in this study?That is, is there a circadian rhythm at the time ofdeath that is modified by certain circumstancesas it occurs in events and deaths due to cardio-vascular causes? If there is an association, it couldexplain the differences observed among settings.For example:
• Can the peak seen at the PCU between 08:00 and10:00 be related to the wake-up period and thepeak of activity in the service? Events of cardio-
FIG. 2. Frequency of deaths by time of day at OS.
FIG. 3. Frequency of deaths by time of day at H.

| 181 181Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
123
vascular cause, among them sudden death, pre-dominate between 07:00 and 11:00, with a sec-ondary peak in the late afternoon and earlyevening, and a trough between 24:00 and 06:00.18
Willich et al. showed that the highest risk of car-diovascular events occurred in the first 3 hoursafter wake-up10; therefore, it seems that the riskof sudden death is more related with wake-upthan with the time of day. One possible expla-nation given for the wake-up morning peak wasthe assumption of the upright posture associat-ing with the rising of catecholamines, which in-creases vascular reactivity, heart rate, bloodpressure, ventricular ectopy, platelet adhesive-ness and aggregability, and other interrelatedprocesses. However, the peak at the end of theday is more difficult to explain.18 At the PCU,the explanation cannot be for most patients theassumption of the upright posture, but this pe-riod of the morning is certainly the peak of ac-tivity related with nursing care, such as bathsand dressing changes. These can induce stressaffecting the cardiovascular system, which canprecipitate death, such as occurs in cardiac pa-tients. At the PCU the peak at the early night isalso difficult to explain, as is the peak observedat evening in cardiovascular deaths.
• Can the absence of significant variation in OSresult from factors interfering with sleep andso affecting patients’ biologic clocks? Cardiacdeaths in hospitalized patients seem to be ran-domly distributed in the 24 hours, contrary topatients not hospitalized. This has been ex-plained by the fact that these patients are sub-mitted to a variety of stimuli during the nightand are in bed during a large part of the day,which can affect their biologic clock.18 At thePCU, where all patients are in single rooms anda good night’s sleep is a goal of care, a lowerlevel of stimulation occurs than for OS, and sothe biologic clock is probably less affected.Therefore, there is an analogy between cancerpatients and cardiac patients in this situationwhen there is an activity in services, which in-terferes with circadian rhythms.
• Can the absence of significant variation at H bedue to probably less rigid schedules and rou-tines that could attenuate the circadianrhythm? Another factor could be a less rigor-ous recording of the time of death.
Another question, perhaps the most important,is the meaning of the variation at the time of death
at the PCU. The statistical significance observeddoes not necessarily imply it is clinically signifi-cant. The clinical significance depends, in firstplace, on the magnitude of the difference. How-ever, the difference seen in this study does not in-dicate any significant clinical meaning, perhapswith the exception of the morning peak. The in-crease in the number of deaths in the morning,observed in our study and in the study of Neu-mann et al.,15 but not observed in other settingsin our study, should be further explored in otherstudies to find out if there are any external fac-tors that can influence it.
In conclusion, studies reporting time of deathproduce many questions regarding death and itsnearest causes. The differences related to the timeof day at our PCU and among the settings allowan analogy with cardiac patient deaths and spec-ulation on possible reasons to explain them. Thedifferences seen among the various settings sug-gest that, even if circadian rhythms exist at thetime of death in cancer patients, external factorscan overcome them. This is the first study ex-ploring the differences at the time of death of can-cer patients among different settings, so these dif-ferences may be confirmed in other studies.
REFERENCES
1. Sassone-Corsi P. Molecular clocks: mastering time bygene regulation. Nature 1998;392:871–874.
2. Rajaratnam SMW, Arent J. Health in a 24-h society.Lancet 2001;358:999–1005.
3. McFadden ER. Circadian rhythms. Am J Med 1988;85(suppl 1B):2–5.
4. Smolensky MH, D’Alonzo GE. Biologic rhythms andmedicine. Am J Med 1988;85(suppl 1B):34–46.
5. Bjarnason GA. Chronobiology: implications for can-cer chemotherapy. Acta Oncolog 1995;34:615–624.
6. Lévi F, Zidani R, Brienza S, Dogliotti L, Perpoint B,Rotarski M, Letoumeau Y, Llory JF, Chollet P, Le RoiA, Focan C. A multicenter evaluation of intensified,ambulatory, chronomodulated chemotherapy withoxaliplatin, 5-fluorouracil, and leucovorin as initialtreatment of patients with metastatic colorectal car-cinoma. Cancer 1999;85:2532–2540.
7. Bliwise DL, Kutner NG, Zhang R, Parker KP. Survivalby time of day of hemodialysis in an elderly cohort.JAMA 2001;286:2690–2694.
8. Pincus DJ, Beam WR, Martin RJ. Chronobiology andchronotherapy of asthma. Clin Chest Med 1995;16:699–713.
9. Cohen MC, Rohtla KM, Lavery CE, Muller JE, Mit-tleman MA. Meta-analysis of the morning excess ofacute myocardial infarction and sudden cardiacdeath. Am J Cardiol 1997;79:1512–1516.
FERRAZ GONÇALVES ET AL.532

182 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
124
TEMPORAL DISTRIBUTION OF DEATHS IN CANCER PATIENTS 533
10. Willich SN, Goldberg RJ, Maclure M, Perriello L,Muller JE. Increased onset of sudden cardiac death inthe first three hours after awakening. Am J Cardiol1992;70:65–68.
11. Behrens S, Fisher SG, Fletcher RD, Franz MR, SinghSN. Effects of amiodarone on the circadian pattern ofsudden cardiac death. Am J Cardiol 1997;80:45–48.
12. Thakur RK, Hoffmann RG, Olson DW, Joshi R,Tresch DD, Aufderheide TP, Ip JH. Circadian vari-ation in sudden cardiac death: effects of age, sex,and initial cardiac rhythm. Ann Emerg Med1996;27:29–34.
13. Hayashi S, Toyoshima H, Miyanishi K, Tanabe N, Fu-nazaki T, Obata A, Kamimura K. Circadian variationsof sudden death. Nippon Koshu Eisei Zasshi 1992;39:83–89.
14. Hayashi S, Toyoshima H, Tanabe N, Miyanishi K.Daily peaks in the incidence of sudden cardiac deathand fatal stroke in Niigata Prefecture. Jpn Circ J1996;60:193–200.
15. Neumann CM, Hanson J, Kuehn N, Bruera E. Tem-poral distribution of deaths in cancer patients admit-
ted to a palliative care unit. J Palliat Care 1999;15:10–13.
16. Davies AN. Circadian variation in time of death inpatients with cancer. Palliat Med 1998;12:483.
17. Ferraz Gonçalves JA. A Portuguese palliative careunit. Support Care Cancer 2001;9:4–7.
18. Peters RW. Circadian patterns and triggers of suddencardiac death. Cardiol Clin 1996;14:185–194.
Address reprint requests to:Dr. Ferraz Gonçalves
Unidade de Cuidados ContinuadosInstituto Português de Oncologia
Rua Dr António Bernardino de Almeida4200-072 Porto
Portugal
E-mail: [email protected] [email protected]

| 183 183Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
125
Support Care Cancer (2005) 13: 752–756DOI 10.1007/s00520-005-0800-0 SHORT COMMUNICATION
José Ferraz GonçalvesIsabel CostaCarolina Monteiro
Received: 30 August 2004Accepted: 23 February 2005Published online: 31 March 2005# Springer-Verlag 2005
Development of a prognostic index in cancerpatients with low performance status
Abstract Background: Prognosis isa very important medical function. Inadvanced cancer it is also important tohelp planning the care to deliver toindividual patients with more accura-cy, in the process of decision aboutthe opportunity for some interven-tions and in the selection of patientsfor clinical trials. Although the per-formance status indexes are by them-selves prognostic factors, amongpatients in all stages there are widevariations in survival. In what con-cerns bedridden patients, survivalvaries between hours and months.Therefore it would be useful todevelop a method which could allowa more precise estimation of thelength of survival in these patients.Patients and methods: We havestudied prospectively 110 bedriddenpatients exploring six variables: con-sciousness level, recognition offamiliar people, continence andcapacity to communicate, to eat andto swallow. Each factor was scoredon a scale of 0 to 2. Our aim was to
construct a classification system withthe sum of the scores of the variablessignificantly correlated with survival.The cut-off-points were calculatedusing the percentiles ≤25, 50 and ≥75according to the method of Altmanet al. (J Natl Cancer Inst 86:829–835.1994). Results: Four of the variableswere significantly associated withsurvival, and an index with threestages was constructed with the sumof these four variables: I–0 to 3; II–4to 6; III–7 to 8. The differences insurvival among the stages are statis-tically significant and the probabilityof survival at the 7th, 30th, 60th,and 90th days is also different.Conclusion: The differences insurvival observed among the stagescan be clinically relevant to theestablishment of a prognostic toindividual patients.
Keywords Advanced cancer .Prognosis . Bedridden patients .Palliative care
When the goal of the treatment of patients with cancer is nolonger to cure or prolong survival, the strategy must bechanged and the interventions to be implemented must bedirected to the well-being of the patients and their families.This is the aim of palliative care.
In palliative care, one of the concerns expressed by thepatients and/or their families is life expectancy. Accurateprediction of patients’ survival is important to facilitatebetter planning of care of individual patients and to helpin the process of decision making about opportunities for
J. F. Gonçalves (*) . I. Costa .C. MonteiroUnidade de Cuidados Continuados,Instituto Português de Oncologia,Rua Dr António Bernardino de Almeida,4200-072 Porto, Portugale-mail: [email protected].: +351-22-5073940Fax: +351-22-5506833

184 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
126
some interventions and in the selection of patients forclinical trials. Therefore, the study of factors and the con-struction of prognostic scores that can help in estimatingthe life span of patients with end-stage cancer is an im-portant objective for research.
Several studies have addressed the problem of prognosisin advanced cancer. The studies completed so far includedthe evaluation of performance status index [1–5], the clin-ical estimation of survival [2, 6–9], evaluation of symptoms[10–19], and study of biochemical and hematological var-iables [15, 18, 20–22]. Some of these studies used a com-bination of these different types of factors.
The performance status index proved to be an importantprognostic factor [1–5, 10, 23]. However, there are widevariations in survival in all stages of a disease. In the caseof bedridden patients, those with the lowest performancestatus, therefore having the worst prognosis, duration ofsurvival varies between hours and months. We tried to de-velop a prognostic index to predict more accurately the lengthof survival of these patients based on observed variablesthat do not need the active participation of patients or re-quire invasive procedures (e.g., venous punctures) and aretherefore applicable to all patients, independently of theircondition.
Patients and methods
This study was carried out in a palliative care unit in anoncological center described elsewhere [24]. The perfor-mance status index used at the unit is the Eastern Coop-erative Oncology Group (ECOG) scale. We studied 110bedridden patients due to advanced cancer, classified asECOG stage 4, and some that could be classified as ECOG3who were successively admitted to the palliative care unitbetween March 2000 and April 2001. Because the per-formance status is a continuous variable that is classified instages that creates a twilight zone between themwherein theclassification of patients may not be easy, we decided tostudy bedridden patients without other considerations.
Six variables were explored prospectively: conscious-ness level, capacity to communicate, recognition of familiarpeople, capacity to eat, capacity to swallow, and continence.These factors were chosen for three main reasons: theymake clinical sense, that is, they are associated with thefunctional status and so possibly with survival; some ofthem proved to be relevant to prognosis in other studies; andthe data result from observation and, therefore, do not needany participation from the patients or any invasive inter-vention. Each factor was scored on a scale of 0 to 2, asindicated in Table 1. Our aim was to construct a classifi-cation system with the sum of the scores of the variablessignificantly correlated with survival. The index was con-structed with three stages whose cutoff points were deter-mined using the percentiles ≤25, 50, and ≥75 according tothe method of Altman et al. [25]. The cutoff points of 7, 30,
60, and 90 days to evaluate the probability of survival werechosen on the basis of clinical utility in order to classifypatient survival into short term, intermediate term, andlonger term. Survival was defined as the number of daysbetween the evaluation and death. The three physicians ofthe palliative care unit rated patients only once, at the firstcontact with them or when they became bedridden.
The analysis of data used methods of descriptive sta-tistics. Adjustment of data to simple linear regressions wasdone by the least squares method with survival time as adependent variable. The Student t test was used to assess thesignificance of the coefficients of regression and correla-tion. The Kaplan–Meier method was applied to determinethe survival curves, and the log-rank or Breslow test tocompare studies concerning the length of survival.
Results
The median age was 65 years (range, 26–90). Forty-one(37%) patients were men and 69 (63%) were women. Theprimary tumors are shown in Table 2. The median survivaltime was 11 days (range, 1–201).
From the six variables, consciousness level, communi-cation, and the capacity to eat and to swallow were sig-nificantly associated with survival (Table 3). Using thepercentiles ≤25, 50 and ≥75 to determine the cutoff points,the scores of the three stages were as follows: I, 0 to 3; II, 4
Table 1 Variables anddefinition of the scores
Consciousness levelNormal 2Sleepiness, wakens easily 1Wakens with difficulty ornot at all
0
CommunicationNormal 2Difficult 1Not at all 0Recognize familiar peopleAlways 2Irregularly 1Never 0Feeding capacityIndependent 2With help 1Not at all 0Swallowing capacityNormal 2Difficult 1Not at all 0Continence, feces and urineAlways 2Occasional leaks 1Not at all 0
753

| 185 185Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
127
to 6; III, 7 to 8. The number of patients in each stage was I,28; II, 52; III, 30. The median survival times for stages I, II,and III were 4, 10, and 29 days, respectively. The com-parative study of the differences in survival among the threestages is significant, with patients in stage I showing theworst survival (Table 4). The probabilities of survival for
each stage at 7, 30, 60, and 90 days are shown in Table 5.Survival beyond 60 days was infrequent (Fig. 1).
Discussion
All the studies trying to find out prognostic factors resultfrom the fact that clinical estimation alone is not reliable.Studies of the clinical length of survival produced heterog-eneous results [2, 6–9]. However, a review of the literatureshows that clinical estimation is an independent prognosticfactor [10], and a more recent systematic review revealedthat clinical estimation is highly correlated with survival,although clinicians consistently overestimate survival [26].However, those clinical estimations should be considered asonly one among other prognostic factors and not as an iso-lated one [9, 10].
Performance status indexes such as Karnofsky or ECOGare prognostic factors that have been used for many years incancer patients with success. In advanced cancer, the per-formance status has also proved to be one of the most im-portant prognostic factors [1, 3, 4, 13]. However, as statedbefore, patients at each level show wide variations in sur-vival. In palliative care, many patients are bedridden and asystem to provide a more accurate prediction of their lifespan would be useful. Because many of these patients arevery frail and have cognitive failure it can be ethicallyproblematic to perform invasive procedures such as venouspunctures to make blood tests and impracticable to evaluatesymptoms. Therefore, in order to include all patients, in-dependently of their condition, we tried to develop a prog-nostic index only with factors observed without the need ofthe patients’ participation.
From the initial variables, we chose the four significantlyassociated to survival. The non-significant variables, con-tinence and capacity to recognize familiar people, had someproblems of classification that could have contributed to
Table 2 Primary tumors and demographic data
Tumor Number (%)
Breast 16 (15)Stomach 16 (15)Colorectal 9 (8)Prostate 8 (7)Cervix 8 (7)Gynecologic others 8 (7)Pancreas 7 (6)Lung 6 (5)Bladder 6 (5)Head and neck 5 (5)Melanoma 4 (4)Others 17 (15)Total 110 (100)
Men, n=41(37%); women, n=69 (63%). Age: median, 65; range,26–90
Table 3 Variables studied and their correlation with survival
Variables t r2 r p
Consciousness level 3.40 0.097 0.311 <0.0001Feeding capacity 2.54 0.057 0.239 <0.001Swallow capacity 2.56 0.058 0.241 <0.001Communication 2.20 0.043 0.207 <0.05Recognizing people 1.74 0.043 0.207 nsContinence 1.44 0.019 0.138 ns
ns non-significant
Table 4 Comparison of survi-val between stages
χ2 p
I vs II 9.17 0.003I vs III 20.05 <0.0001II vs III 3.52 0.02
Table 5 Probability of survivalby stage
Days I (%) II (%) III (%)
7 29 65 8730 11 31 4760 4 15 1390 – 4 13
Days
210
195
180
165
150
135
120
105
90
75
60
45
30
15
0
Cum
Sur
viva
l
1,1
1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
I
II
III
I – Stage III – Stage II III – Stage III
Fig. 1 Overall survival and stage
754

186 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
128
their non-significance: continence was impossible to clas-sify in patients with indwelling urinary catheters, and thesigns of recognition of familiar people were difficult to in-terpret in the most frail patients who often had a very limitedcapacity to communicate. The stages constructed showeddifferences in the probability of the length of survival amongthem high enough to help the health professionals to plan thedecisions concerning care and satisfying the patients andtheir families’ information needs.
Other studies also concluded that feeding and swallow-ing problems are factors significantly associated with sur-vival [10, 11, 13, 15–18], although there are significantmethodological differences relative to our study. In general,these symptoms were reported by patients [11, 13, 15–18]instead of being reported by the observer as in our study,excluding the patients unable to do that. Other studies dif-fered in other ways. For example, the study of Reuben etal. [13], with 1,592 patients, differed from our study be-cause it did not include only bedridden patients, the feed-ing problems were not clearly defined, and there was alarge percentage (29%) of patients unable to answer whowere substituted in the evaluation by the primary careperson, which proved to be largely unreliable [14].
Cognitive failure was an important prognostic factor insome studies [10, 12, 19]. In our study, cognitive failure wasalso a relevant factor, as evaluated by the consciousnesslevel and the capacity to communicate. The capacity torecognize familiar people, which could be also an indicatorof the cognitive status, was not significantly associated withsurvival probably because of the problems referred to above.
Prognostication is an important topic in medicine in gen-eral and in palliative care in particular, where time is usuallyshort. The present study intends to be one step further in theconstruction of a more reliable way to preview survival ofpatients with advanced cancer, particularly those who, bythe criterion of the performance status, already have a badprognosis. The prognostic index based on observation is anew approach to this problem. Our aim when we plannedthis study was to construct a quantifiable prognostic indexthat would allow health professionals to predict more re-liably survival of bedridden patients in periods useful forclinical practice. We believe that this index can be a usefultool.
Acknowledgements The authors would like to thank Dr. MariaJosé Bento for her invaluable help in the statistic analysis.
References
1. Evans C, McCarthy M (1985) Prog-nostic uncertainty in terminal care: canthe Karnofsky index help? Lancet1:1204–1206
2. Maltoni M, Nanni O, Derni S et al(1994) Clinical prediction of survival ismore accurate than the Karnofskyperformance status in estimating lifespan of terminally ill cancer patients.Eur J Cancer 30A:764–766
3. Mor V, Laliberte L, Morris JN,Wiemann M (1984) The Karnofskyperformance status: an examination ofits reliability and validity in a researchsetting. Cancer 53:2002–2007
4. Yates JW, Chalmer B, McKegney P(1980) Evaluation of patients withadvanced cancer using the Karnofskyperformance status. Cancer45:2220–2224
5. Maltoni M, Pirovano M, Nanni O,Labianca R, Amadori D (1994) Prog-nostic factors in terminal cancer pa-tients. Eur J Palliat Care 1:122–125
6. Forster LE, Lynn J (1988) Predictinglife span for applicants to inpatienthospice. Arch Intern Med148:2540–2543
7. Oxenham D, Cornbleet MA (1998)Accuracy of prediction of survival bydifferent professional groups in a hos-pice. Palliat Med 12:117–118
8. Hardy J, Turner R, Edmonds P,A’Hern R (1997) Prediction of survivalin patients referred to a palliative careunit. Palliat Med 11:73
9. Parkes CM (1972) Accuracy of pre-dictions of survival in later stages ofcancer. BMJ 2:29–31
10. Viganò A, Dorgan M, Buckingham J,Bruera E, Suarez-Almanzor ME (2000)Survival prediction in terminal cancerpatients: a systematic review of themedical literature. Palliat Med14:363–374
11. Llobera J, Esteva M, Rifà J et al (2000)Terminal cancer: duration and predic-tion of survival time. Eur J Cancer36:2036–2043
12. Bruera E, Miller MJ, Kuehn N,MacEachern T, Hanson J (1992) Esti-mates of survival of patients admittedto a palliative care unit: a prospectivestudy. J Pain Symptom Manage7:82–86
13. Reuben DB, Mor V, Hiris J (1988)Clinical symptoms and length of sur-vival in patients with terminal care.Arch Intern Med 148:1586–1591
14. Nekolaichuk CL, Bruera E, SpachynskiK, MacEachern T, Hanson J, MaguireTO (1999) A comparison of patient andproxy symptom assessments in ad-vanced cancer patients. Palliat Med13:311–323
15. Glare P, Virik K (2001) Independetprospective validation of the PaP Scorein terminally ill patients referred to ahospital-based palliative medicine con-sultation service. J Pain SymptomManage 22:891–898
16. Walsh D, Rybicki L, Nelson KA,Donnelly S (2002) Symptoms andprognosis in advanced cancer. SupportCare Cancer 10:385–388
17. Maltoni M, Pirovano M, Scarpi E et al(1995) Prediction of survival of patientsterminally ill with cancer. Cancer75:2613–2622
18. Maltoni M, Nanni O, Pirovano M et al(1999) Successful validation of thepalliative prognostic score in terminallyill cancer patients. J Pain SymptomManage 17:240–247
19. Caraceni A, Nanni O, Maltoni M et al(2000) Impact of delirium on the shortterm prognosis of advanced cancerpatients. Cancer 89:1145–1149
20. Fainsinger RL, Tapper M, Bruera E(1993) A perspective on the manage-ment of delirium in terminally illpatients on a palliative care unit.J Palliat Care 9:4–8
21. Romagnoli A, Rapin CH (1991) Valeurpronostique de certains paramètresbiologiques chez des sujects âgéshospitalisés. Age Nutri 2:130–136
755

| 187 187Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
129
22. Fülöp T, Herrmann F, Rapin CH (1991)Prognostic role of serum prealbuminlevels in elderly patients at admission toa geriatric hospital. Arch GerontolGeriatr 12:31–39
23. den Daas N (1995) Estimating length ofsurvival in end-stage cancer: a reviewof the literature. J Pain SymptomManage 10:548–555
24. Ferraz Gonçalves JA (2001) A Portu-guese palliative care unit. Support CareCancer 9:4–7
25. Altman DG, Lousen B, Sauerbrei W,Schumacher M (1994) Dangers ofusing “optimal” cut-off-points in theevaluation of prognostic factors. J NatlCancer Inst 86:829–835
26. Glare P, Virik K, Jones M et al (2003)A systematic review of physicians’survival prediction in terminally illcancer patients. BMJ 327:195–200
756

188 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 189 189Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Breaking bad news: experiences and preferences ofadvanced cancer patients at a Portuguese oncology centreFerraz Goncalves, Agata Marques, Sonia Rocha, Pedro Leitao, Teresa Mesquita and Susana MoutinhoPalliative Care Unit, Portuguese Institute of Oncology, Oporto
The disclosure of information to patients about diagnosis and prognosis and other aspects
of care is still a matter of debate. We have conducted a study in advanced cancer patients
about their experiences and preferences concerning this issue. A questionnaire was
developed and completed during the first appointment in the outpatient clinic of an
oncology centre’s palliative care unit, before the patient had any contact with the staff of the
unit. The study was conducted on a convenience sample of 47 patients. We found that
34 (72%) of those patients thought they had been informed of their diagnosis, most of them
by the hospital doctor. However, not all stated the diagnosis in a manner clearly showing
that they were aware of the nature of their disease. Most patients were with a family
member when the diagnosis was disclosed, which is what the majority had preferred. Of
the 13 uninformed patients, only one preferred to remain uninformed. Most patients (89%)
participated in decisions concerning treatment, although only 68% thought they should
have participated. Some 39 patients (83%) were informed that they were being referred to
the palliative care unit, but surprisingly only eight had received an explanation of the unit’s
function. We concluded that, although most patients had been informed of their disease,
there remains many problems, the most important of which, in our view, is the difference
between the information provided and the patients’ needs.
A revelacao da informacao sobre o diagnostico o prognostico e outros aspectos dos
cuidados e ainda um assunto em debate. Realizamos um estudo em doentes com cancro
avancado sobre as suas experiencias e preferencias no que diz respeito a este tema. Foi
desenvolvido um questionario que foi aplicado na primeira consulta externa de uma unidade
de cuidados paliativos de um centro oncologico, antes de terem contacto com o pessoal da
unidade. O estudo foi realizado numa amostra de conveniencia de 47 doentes.
Constatamos que 34 (72%) desses doentes pensavam que tinham sido informados do
seu diagnostico, a maioria pelo medico do hospital. Contudo, nem todos nomearam o
diagnostico de um modo que mostrasse claramente que tinham nocao da natureza da
sua doenca. A maioria dos doentes estava com um familiar quando o diagnostico foi
revelado e era assim que a maior parte preferia. Dos 13 doentes nao informados so um
preferia manter-se sem informacao. A maior parte dos doentes (89%) participou nas
decisoes terapeuticas, embora so 68% pensasse que devia ter participado. Trinta e nove
doentes (83%) foram informados de que tinham sido referenciados para a unidade de
cuidados paliativos, mas surpreendentemente so oito tinham tido uma explicacao sobre a
funcao da unidade. Concluımos que embora a maioria dos doentes tenha sido informada da
sua doenca ha ainda muitos problemas, sendo o mais importante, do nosso ponto de vista,
a diferenca entre a informacao prestada e as necessidades dos doentes. Palliative
Medicine 2005; 19: 526�/531
Key words: breaking bad news; cancer patients; cultural issues; information disclosure; palliative
care patients
Address for correspondence: Dr Ferraz Goncalves, Unidade deCuidados Continuados, Instituto Portugues de Oncologia, RuaDr Antonio Bernardino de Almeida, 4200-072 Porto, Portugal.E-mail: [email protected]
Palliative Medicine 2005; 19: 526�/531
# 2005 Edward Arnold (Publishers) Ltd 10.1191/0269216305pm1070oa

190 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
Introduction
The information delivered to cancer patients is still a
matter of controversy, with wide cultural differences. In
northern European countries,1,2 and the US,3 most
doctors disclose the diagnosis as standard practice, but
in southern and eastern European countries,2,4,5 the
attitude is more paternalistic and patients are often
‘protected’ from such information. However, even in
those countries where the usual practice is now to
disclose the diagnosis, a few decades ago the attitude
was the opposite.3 This shows that the problem of
information can change with time.There are also differences between countries relative to
patients and families’ preferences for the type of infor-
mation they require. A study in a palliative care setting
comparing attitudes in Spain and Canada,6 concluded
that the majority of Canadian patients preferred to be
clearly informed, while the Spanish patients placed less
value on full disclosure. In the same study, family
members in Canada agreed with the detailed information
to patients, while in Spain 89% of family members
indicated that full disclosure was not important to the
patient.
A few years ago, we conducted a survey of doctors at
the Oporto Centre of the Portuguese Institute of
Oncology concerning the disclosure of diagnoses to
patients.7 In that study, 71% of doctors stated that they
always, or at the patient’s request, disclosed a cancer
diagnosis and most doctors who rarely or never disclosed
did not do so because they thought that the information
could be psychologically deleterious. However, uncer-
tainty can be worse than bad news,8 and some patients
assume that a non-threatening diagnosis would be
disclosed to them and the absence of such a disclosure
is taken to indicate that their condition must be serious.9
Non-disclosure isolates patients as it excludes them from
the discussion of problems that probably concern them
most. On the other hand, there is a minority of patients
who prefer to remain uninformed, and that must be
respected as that is the strategy they have evolved to
maintain hope. For those who lose hope of a cure or
longer life due to the disclosure, hope can be kept alive
through other aspects, such as their physician not
abandoning them, their remaining free from significant
suffering, being with their family and close friends and
having time to settle matters important to them.That survey reflected the view of doctors, which can be
very different to patients’ views. Therefore, the obvious
next step was to ask patients for their opinion concerning
the quantity and quality of information they receive from
health professionals and their preferences. Cultural issues
are relevant factors in the attitudes of doctors, patients
and their families in relation to the disclosure of
information. That is why it is important to add data
from different countries, and that is the reason providing
justification for this study.
Methods
A survey was conducted between January 2002 and June
2003 on a convenience sample of patients referred to the
outpatient clinic of our palliative care unit.10 This is a
palliative care unit included in an oncology centre;
therefore all patients had cancer as their primary
diagnosis. All patients were aged 15 or over, as youngerpatients are treated in the paediatric service.
A questionnaire was specifically designed for this study
to acquire the information considered relevant in an
exploratory survey. The aim of the survey was to obtain
patient preference regarding information and to compare
this with what actually occurs. The broad topics of the
questionnaire included: who should be informed first
when a life threatening disease like cancer is diagnosed;who should and who actually did convey the information;
where the information was and where it should have been
conveyed; who was and who should have been with the
patient; participation in the treatment decision-making
process; information provided on palliative care; and a
request to name the diagnosed disease.
Patients were addressed when they arrived for the first
time at the outpatient clinic, before they had any contactwith the health professionals of the unit. Psychology
students undergoing long-term training in the unit
presented the questionnaire to the patients.
Patients that were very frail, bedridden or suffering
cognitive failure, as assessed by the shortened version of
the Confusion Assessment Method,11 were excluded.
A descriptive study of all variables included in the
study was performed. Chi-square and Fisher’s exact testwere used to compare categorical variables with the
status of informed or not informed patients. Age and
follow-up time at the oncology centre, before admission
to the palliative care unit, were compared between
informed and uninformed patients using the Mann�/
Whitney U -test.
The ethics committee of the hospital approved this
study.
Results
The survey included 47 patients, 21 males (45%) and
26 females (55%); their median age was 66 years (range:
21�/86 years); 39 were married (83%), six single (13%)
and two widowed (4%). The median follow-up time at the
oncology centre before admission to the palliative care
unit was 16 months (range: 2�/195).
Breaking bad news 527

| 191 191Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
All patients preferred the questions to be read aloud by
the psychology students instead of filling the question-
naires in themselves. Thirty-four patients (72%) statedthat they had been informed and 13 (28%) that they had
not been informed of their diagnosis.
Disclosure of the diagnosis
Twenty-six (55%) stated that patients should be the first
person to be informed, whereas 21 (45%) preferred afamily member or a friend. Most patients (41�/87%)
thought that the information should be disclosed by a
doctor and no one chose a nurse or a social worker.
Details regarding what actually occurred and the pre-
ferred options for diagnosis disclosure can be seen in
Table 1. Nineteen patients (56%) stated that they were
surprised with the information, while 15 (44%) suspected
the diagnosis. Most patients (68%) received the informa-tion at the outpatient clinic, only two received it in an
inpatient setting, three at home and one in another place;
the three patients who received the information at home
were among those informed by a family member, as
expected.
Most patients preferred to be with a family member
when the diagnosis was disclosed and this was what
actually occurred, but there were differences between thepreferred option and the actual experience (Table 2).
We did not find any correlation between information
and sex, marital status, age or the follow-up time at the
oncology centre before admission to the palliative care
unit.
Information and participation in treatment decision-
making process
Forty-two patients (89%) were always informed about
treatment and two sometimes; therefore only three (6%)
were never informed. Twenty-nine patients (62%) always
participated in decisions regarding treatment and two
participated sometimes; 15 (32%) never participated indecisions regarding treatment (one piece of data missing).
Only 32 (68%) thought they should participate in those
decisions, 23 (49%) thought that close family members
should participate, and 10 (21%) that only doctors should
take the decisions. Seven patients (15%) refused proposed
treatments.
Effectiveness of the information
For 19 patients (56%), the information was disclosedin an acceptable manner, clearly and sensitively, whereas
15 (44%) found the disclosure poorly carried out.
However, none of the latter commented further on why
they deemed it incorrect.
Only one of 13 uninformed patients preferred to
remain so. This group of patients was not informed
because they were not at ease to ask, the information was
refused, they felt they were tricked, the professionals triednot to answer the questions or the information was
unclear. On the other hand, five of the 34 informed
patients preferred that they had not been informed.
Therefore, only six of the 47 patients did not want to
know (Table 3).
The 34 informed patients stated they had one of the
following: ‘cancer’ �/ 15 (44%); ‘a tumour’ �/ 10 (29%); ‘a
bad disease’ �/ one (3%); ‘other’ �/ seven (21%); ‘do notknow’ �/ one (3%). The 13 uninformed patients stated
they had one of the following: ‘cancer’ �/ two (15%);
‘tumour’ �/ 0; ‘other’ �/ four (31%); ‘do not know’ �/ seven
(54%). If we consider all patients stating ‘cancer’,
‘tumour’ and ‘bad disease’ to be informed and all
patients stating ‘they do not know’ or ‘other’ to be
uninformed then the results for informed patients are as
follows: 26 (76%) are really informed and eight (24%)are not informed, and for uninformed patients: two
(15%) are informed and 11 (85%) are not informed; the
Table 1 Who should communicate information about diag-nosis? Actual experience and preferred options of the 34informed patients
Actual experiencen (%)
Preferred optionn (%)
Family doctor 8 (24) 17 (50)Hospital doctor 19 (56) 10 (29)Any doctor �/ 3 (9)Psychologist 0 (0) 1 (3)Nurse 2 (6) 0 (0)Social worker 0 (0) 0 (0)Family member 4 (12) 0 (0)Other 1 (3) 3 (9)
Table 2 Actual experience and preferred option of the 34informed patients on who should be with them when thediagnosis is disclosed
Actual experiencen (%)*
Preferred optionn (%)
Family member 22 (65) 19 (61)Friend 2 (6) 0 (0)Alone 8 (24) 3 (10)Other professionals 8 (24) 1 (3)Other patients 0 (0) 1 (3)Indifferent �/ 7 (23)
*The sum of the actual experience items does not total 34 (or100%) because some patients were with more than oneperson.
Table 3 Information obtained and patients’ preferences
Patients’ preferences
To be informedn (%)
Not to be informedn (%)
Informed patients (n�/34) 29 (85) 5 (15)Uninformed patients (n�/13) 12 (92) 1 (8)Total (n�/47) 41 (87) 6 (13)
528 F Goncalves et al.

192 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
difference between the two groups was significant
(PB/0.001) (Table 3).
Regarding the referral to palliative care, 39 patients(83%) were informed of the referral, but only eight
(17%) had received an explanation regarding the pallia-
tive care unit.
Discussion
The percentage of patients considering themselves to be
informed (72%) is similar to the percentage of doctors
(71%) that always, or at the patients’ request, disclosed
the diagnosis in a former study carried out at our
hospital.7 This number is higher than that observed ina Spanish study about ten years ago, where only 32%
of the patients with advanced cancer had been
informed of the nature of their disease.12 This is
surprising because Spanish culture is deemed to be
similar in many aspects to Portuguese culture. It seems
unlikely that the ten years separating these two studies
can explain the difference. Moreover, 42% of the
uninformed patients did not want to receive moreinformation,12 which again contrasts with our observa-
tion that only one of the 13 uninformed patients (8%)
clearly preferred to remain uninformed. The reasons
why those patients were not informed were related to
the doctors’ attitude and a lack of proactive effort to
find out the patients’ information needs, which can be
inferred from the manner in which the patients
answered this question. On the other hand, five ofthe informed patients preferred that the information
had not been disclosed. Therefore, only a minority of
the patients did not want to be informed.
Usually patients prefer to be informed by a doctor,
and most prefer the family doctor, probably because
they are more familiar with them, as patients do not
like to be informed by unknown doctors.13 However,
most are informed by a hospital doctor, as demon-strated in this and other studies.14�16 Doctors are, in
fact, the preferred person to convey the informa-
tion.17,18 The study of Yun et al .,17 which explores
the reasons for this preference, showed that the most
important factor is the doctor’s understanding of the
disease and capacity to explain the entire situation;
other reasons included trust placed in the doctor, the
doctor’s awareness of the patient’s emotional, psycho-logical, social and physical situation, and the duty of
doctors to provide information.
Most patients were informed about treatments and
only a minority did not participate in decisions
concerning those treatments. But many patients think
that they should not participate in those decisions and
that only doctors should make such decisions, as
observed in other studies;8,11 although in one study,8
this preference was limited to older patients. The
encouragement to participate in treatment decision-
making can be associated with higher levels of anxiety,
which can persist for at least two weeks.19 In the
previous study of doctors at our hospital,7 91%
thought that patients should participate in the deci-
sions regarding treatment, which was a higher percen-
tage than that recorded for doctors who always, or on
request, informed patients (70%); this seems a contra-
dictory fact given that patients need information to
decide rationally; it appears to be the contrary to the
patients’ wishes as observed herein.
Sometimes doctors are not very effective in informing
patients, as shown by the difference recorded between the
information delivered and the patients’ needs, i.e., there
were patients informed that did not want to be informed
and patients not informed that had wanted to be
informed. These observations are very important because
the issue is not the disclosure of information but
matching it to the will of patients. Also, the surprise
that the diagnosis caused in many patients suggests a lack
of appropriate patient preparation concerning the possi-
bility of a diagnosis of cancer during the period of
diagnostic tests.18 Furthermore, many patients thought
they were poorly informed, without commenting further
on why they thought so. This is an important issue
because a poor or insensitive disclosure of information
may have a negative emotional impact. Patients satisfied
with diagnosis communication reported less emotional
distress than patients who would have preferred differ-
ent.18 There are, however, other aspects, besides the way
the information was disclosed, which are considered of
greater importance, such as emotional support and a
shorter period of time between seeking medical assistance
and the confirmation of cancer.13,17,18 Also important for
patient emotional support is the certainty that the
physician will not abandon the patient and will be
available to answer all questions.13
The communication of a poor prognosis is an even
more difficult task that doctors often avoid. That is
probably the explanation why only a few patients were
aware of why they had been referred to the palliative care
unit, even when they knew their diagnosis and partici-
pated in the treatment decisions. This is not exclusive to
our hospital.19,20 For example, Cassileth et al . found that
more patients receiving curative radiotherapy tended to
provide a correct diagnosis than patients receiving
palliative radiotherapy,20 which was also interpreted by
the authors as being due to the difficulties that doctors
have communicating an adverse prognosis. Although
physicians often state that non-disclosure is a means of
protecting patients, in fact there is a reluctance to give
bad news, especially in the transition from curative or life
prolonging therapy to symptomatic treatment.21 An
Breaking bad news 529

| 193 193Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
alternative or complementary explanation for these
observations is denial amongst patients.22
Conclusion
One important limitation of this study is the small
number of patients, which raises questions about the
external validity of the data and whether the findings can
be extrapolated to Portuguese cancer patients as a whole.
This said, we tentatively conclude that most Portuguese
cancer patients want to be informed of their diagnosis
and want to participate in decisions regarding treatment.
However, there are also some patients who do not want
that, mainly in relation to treatment decision-making.
Most patients wish to be with a family member, but not
with other health professionals. Some patients stated they
had been informed but gave ambiguous answers when
asked to name their disease, which does not necessarily
mean that they were wrong but casts doubt on the correct
nature of their information.
Communicating with cancer patients and, in particu-
lar, breaking bad news is a very important aspect of the
patient�/doctor relationship. However, it is often ne-
glected in the training of doctors. Many people, including
health professionals, think that the art of communication
is a natural skill, ignoring the fact that, just as with other
aspects of patient care, it can be learned. There are many
general guidelines published on how to break bad
news,23�28 which provide general basic knowledge on
how to communicate properly, but it is also necessary to
learn via practice, through basic programmes,29,30 with
follow-up and consolidation.31
Perhaps the most important findings of this study, also
verified in all other studies on the problem of information
disclosure, are the large differences observed in patients’
preferences. Even when there is a clear preference on a
particular aspect, there is never unanimity. Therefore, the
data provided by studies of information preferred by
patients in different populations should be seen only as
marking out trends or general indications, because in
the presence of a particular patient we do not know what
he or she wants before we try to find out. Patient
preference should not be assumed based on these general
data. These studies, important as they are, show popula-
tion data, which do not necessarily encompass individual
needs.
The findings of this work can be relevant to anyone
working with cancer patients. It adds data relative to
patients of a southern European environment, which
does not seem to match, at least in those aspects
statistically handled, other cultures deemed to be similar,
such as that of neighbouring Spain.
Acknowledgements
This study was supported in part by the North Section of
the Portuguese League Against the Cancer.
References
1 Loge JH, Kaasa S, Ekeberg Ø/´ , Falkum E, Hytten K.
Attitudes toward informing the cancer patient �/ a surveyof Norwegian physicians. Eur J Cancer 1996; 32A:1344�/48.
2 Thomsen OØ, Wulff HR, Martin A, Singer P. What dogastroenterologists in Europe tell cancer patients? Lancet1993; 341: 473�/76.
3 Novack DH, Plumer R, Smith RL, Ochitill H, MorrowGR, Bennet JM. Changes in physicians’ attitudes towardtelling the cancer patient. JAMA 1979; 241: 897�/900.
4 Estape J, Palombo H, Hernandez E et al . Cancerdiagnosis disclosure in a Spanish hospital. Ann Oncol1992; 3: 451�/54.
5 Mystakidou K, Liossi C, Viachos L, Papadimitriou J.Disclosure of diagnostic information to cancer patientsin Greece. Palliat Med 1996; 10: 195�/200.
6 Fainsinger RL, Nunez-Olarte JM, Demoissac DM. Thecultural differences in perceived value of disclosure andcognition: Spain and Canada. J Palliat Med 2003; 19:43�/48.
7 Ferraz Goncalves J, Castro S. Diagnosis disclosure in aPortuguese oncological centre. Palliat Med 2001; 15: 35�/
41.8 Cassileth BR, ZurpKis RV, Sutton-Smith K, March V.
Information and participation preferences among cancerpatients. Ann Intern Med 1980; 92: 832�/36.
9 McIntosh J. Patients’ awareness and desire for informa-tion about diagnosed but undisclosed malignant disease.Lancet 1976; ii: 300�/303.
10 Ferraz Goncalves JA. A Portuguese palliative care unit.Support Care Cancer 2001; 9: 4�/7.
11 Inouye SK, van Dick CH, Alessi CA, Balkin S, SiegalAP, Horwitz RI. Clarifying confusion: the confusionassessment method. Ann Intern Med 1990; 113: 941�/48.
12 Centeno-Cortes C, Nunez-Olarte JM. Questioning diag-nosis disclosure in terminal cancer patients. Palliat Med1994; 8: 39�/44.
13 Sardell AN, Trierweiler SJ. Disclosing the cancer diag-nosis: procedures that influence patient hopefulness.Cancer 1993; 72: 3355�/65.
14 Chan A, Wooddruff RK. Communicating with patientswith advanced cancer. J Palliat Care 1997; 13: 29�/33.
15 Lind SE, Good MJD, Seidel S, Csordas T, Good BJ.Telling the diagnosis of cancer. J Clin Oncol 1989; 7:583�/89.
16 Barnett MM. Effect of breaking bad news onpatients’ perceptions of doctors. J R Soc Med 2002;95: 343�/47.
17 Yun YH, Lee CG, Kim S, et al . The attitudes of cancerpatients and their families toward the disclosure ofterminal illness. J Clin Oncol 2004; 22: 307�/14.
530 F Goncalves et al.

194 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
18 Butow PN, Kazemi JN, Beeney LJ, Griffin AM, DunnSM, Tattersall MHN. When the diagnosis is cancer:patient communication experiences and preferences.Cancer 1996; 77: 2630�/37.
19 Gattellari M, Voigt KJ, Butow PN, Tattersall MHN.When the treatment goal is not cure: are cancer patientsequipped to make informed decisions? J Clin Oncol2002; 20: 503�/13.
20 Cassileth BR, Volckmar D, Goodman RL. The effectof experience on radiation therapy patients’ desirefor information. Int J Radiat Oncol Biol Phys 1980; 6:493�/96.
21 Fallowfield LJ, Jenkins VA, Beveridge HA. Truth mayhurt but deceit hurts more: communication in palliativecare. Palliat Med 2002; 16: 297�/303.
22 Jones JS. Telling the right patient. Br Med J 1981; 283:291�/92.
23 Faulkner A, Maguire P, Regnard C. Breaking bad news�/ a flow diagram. Palliat Med 1994; 8: 145�/51.
24 Richards MA, Ramirez AJ, Degner LF, Fallowfield LJ,Maher EJ, Neuberger J. Offering choice of treatment topatients with cancer. A review based on a symposiumheld at the 10th Annual Conference of the British
Psychosocial Oncology Group, December 1993. Eur JCancer 1995; 31A: 112�/16.
25 Girgis A, Sanson-Fisher RW. Breaking bad news: con-sensus guidelines for medical practitioners. J Clin Oncol1995; 13: 2449�/56.
26 Fallowfield L. Giving sad and bad news. Lancet 1993;341: 476�/78.
27 Creagan ET. How to break bad news �/ and not de-vastate the patient. Mayo Clin Proc 1994; 69: 1015�/17.
28 Buckman R. How to break bad news. London: PanBooks, 1992.
29 Fallowfield L, Jenkins V, Farewell V, Saul J, Duffy A,Eves R. Efficacy of a cancer research UK communica-tion skills training model for oncologists: a randomisedcontrolled trial. Lancet 2002; 359: 650�/56.
30 Jenkins V, Fallowfield L. Can communication skillstraining alter physicians’ beliefs and behaviour in clinics?J Clin Oncol 2002; 20: 765�/69.
31 Razavi D, Merckaert I, Marchal S, et al . How tooptimize physicians’ communication skills in cancercare: results of a randomized study assessing the useful-ness of post-training consolidation workshops. J ClinOncol 2003; 21: 3141�/49.
Breaking bad news 531

| 195 195Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
136

196 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
137

| 197 197Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
138
Support Care Cancer (2006) 14: 1147–1151DOI 10.1007/s00520-006-0045-6 SHORT COMMUNICATION
Ferraz GonçalvesMónica MozesIsabel SaraivaCristina Ramos
Received: 29 September 2005Accepted: 16 February 2006Published online: 20 April 2006# Springer-Verlag 2006
Gastrostomies in palliative care
Abstract Objective: In palliativecare, gastrostomies are used to pro-vide nutritional support or to decom-press the bowel. To evaluate whathappened to the patients monitored atour palliative care unit (PCU) whounderwent gastrostomy between Oc-tober 1994 and January 2005, aretrospective audit was made.Method: The charts of 154 patientswere reviewed. Results: The mostfrequent reason why a patient under-went a gastrostomy was dysphagiadue to head and neck and/or esopha-geal cancer. Only one patient under-went a drainage gastrostomy becauseof intestinal obstruction. Interven-tional radiology performed 96% ofthe gastrostomies. Early complica-tions occurred in 53 patients (34%)who underwent the gastrostomy forfeeding and the most common waslocal pain, usually mild. However,
there was one death due to peritonitis,probably related with the procedure.Late complications also occurred in53 patients and major complicationsoccurred in 22 patients, the mostcommon was extrusion. The mediansurvival after the performance of thegastrostomy was 61 days (range 1 to551 days). Nineteen patients (12%)survived 1 week or less, 28 (18%)between 8 and 30 days, 51 (33%)from 31 to 90 days, 53 (35%) 91 daysor more, and one unknown. Thepatient who underwent a gastrostomyfor bowel obstruction survived foronly 7 days. One hundred and twenty-five patients (81%) died at the PCU,26 (17%) at home, and four (3%) atother places.
Keywords Gastrostomies . Palliativecare . Nutrition . Dysphagia . Bowelobstruction
Introduction
Gastrostomies are used to provide nutritional support inpatients who are unable to ingest food and drinks normallyfor neurological or mechanical reasons. More rarely, theyare performed to decompress the bowel in patients withintestinal obstruction.
The procedure involves the placement of a tube into thestomach through the abdominal wall. Egeberg, a Norwe-gian surgeon, conceived the surgical technique in 1837 andCharles Sedillot of Stasbourg performed the first recordedoperation of this type in 1849 [1]. Since then, all the
gastrostomies recorded ended in the patient’s death, usuallyfrom peritonitis, as it was only in 1876 when Verneuilperformed the first successful surgical gastrostomy in Paris[1]. It was not before 1979 that a new technique waspresented when the Americans Gauderer and Ponskyperformed the first percutaneous endoscopic gastrostomy(PEG) [2]. Two years later in 1981, the Canadian Preshawintroduced the percutaneous radiological gastrostomy(PRG) [3].
In palliative care, it is quite common to treat patientswith dysphagia or intestinal obstruction. To assess whathappened to the patients monitored at our palliative care
F. Gonçalves (*) . M. Mozes .I. Saraiva . C. RamosUnidade de Cuidados Continuados,Instituto Português de Oncologia,Rua Dr. António Bernardinode Almeida,Porto 4200-072, Portugale-mail: [email protected].: +351-225073940Fax: +351-225506833

198 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
139
unit (PCU) who underwent a gastrostomy, a retrospectiveaudit was made.
Materials and methods
A retrospective review was done on the charts of allpatients admitted in the PCU of the Porto section of thePortuguese Institute of Oncology since its foundation untilJanuary 2005, who had a gastrostomy and died. The unitwas founded in 1994 and is described elsewhere [4].
All patients admitted to the PCU who are candidates toundergo a procedure, such as a gastrostomy, are informedof the method, advantages, and risks involved. They sign astandard informed consent document according to thepolicy of our hospital.
The search was made through the computerized databaseof the hospital. The patients’ charts were reviewed by threedoctors for demographic data, diagnosis, performancestatus using the Eastern Cooperative Oncology Group(ECOG) index, reason to undergo the gastrostomy,presence of tracheostomy, metastasis, method, complica-tions, and place of death.
To analyze the complications of the gastrostomies, wedivided them according to early and late when itsoccurrence was in the first 5 days after the procedure orafter 5 days. The rational to this classification was thedistinction between complications related with the perfor-mance of the procedure and those related with the use of thetube. The severity of the complications was classified asminor or major according to the following criteria: minorwhen they are light, transitory, and controllable by simplemeasures and major when there were severe symptoms, thecomplication was actually or potentially dangerous, orneeded the cooperation of professionals from outside theunit to be solved, such as tube extrusion.
The analysis of data used methods of descriptivestatistic. The method of Kaplan Meier was applied todetermine the survival curves and the Breslow test to do thecomparative studies concerning the length of survival afterthe gastrostomy among the ECOG scores.
Results
From a total of 167 patients admitted to the PCU who hadundergone a gastrostomy since its foundation in October1994 until the end of January 2005, only the charts of 154(92%) could be reviewed because the other 13 could not befound. From those 154, 69 (45%) underwent the gastros-tomy before the admission to the PCU and 86 (56%) afterit. Only one patient underwent a gastrostomy for drainagedue to intestinal obstruction. In all the others, thegastrostomy was performed for nutrition. Due to thishuge disparity, the analysis of the data includes only the153 patients who underwent a gastrostomy for nutrition.
Data of the patient with bowel obstruction will be presentedseparately and only when indicated.
The demographic data are shown in Table 1. The mostfrequent reason why a patient underwent a gastrostomywas dysphagia caused by head and neck cancer and/oresophagus cancer (Table 2).
Table 1 Demographic data of the 153 patients who underwent thegastrostomy for feeding
GenderMale 123 (80%)Female 30 (20%)Age (year)Median 56Minimum 26Maximum 85ECOGa
1 1 (1%)2 18 (21%)3 34 (40%)4 20 (24%)Unknown 12 (14%)DiagnosisHead & neck 124 (81.0%)Esophagus 20 (13.1%)Head & neck + esophagus 6 (3.9%)Colon 1 (0.7%)Breast 1 (0.7%)Primary unknown 1 (0.7%)MetastasisLocally advanced 145 (95%)Lymph nodes 77 (50%)aTotal of 85 patients who underwent gastrostomy after the admissioninto the PCU
Table 2 Motives, goals, and methods for gastrostomies in all the154 patients
Number of patients (%)
MotiveDysphagia 142 (92)Fistula orocutaneous 8 (5)Fistula tracheoesophageal 1 (1)Bowel obstruction 1 (1)Unknown 2 (1)GoalFeeding 153 (99)Drainage 1 (1)MethodRadiological 148 (96)Surgery 3 (2)Endoscopy 1 (1)Unknown 2 (1)
1148

| 199 199Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
140
Most tumors were local recurrences or were locallyadvanced at the time of the diagnosis; the most frequentmetastases were in the regional lymph nodes. Reflectingthe localization of the underlying disease, 79 (52%)patients also had a tracheostomy.
Interventional radiology performed almost all thegastrostomies (Table 2), as this was the commonly usedmethod at our hospital. Early complications occurred in 53(34%) patients. The most common early complication waslocal pain, which was minor in general (Table 3). Majorearly complications occurred in five patients with one deathat the forth day after the gastrostomy due to peritonitisprobably related with the performance of the gastrostomy.Late complications also occurred in 53 patients. Majorcomplications were more frequent in these ones, occurringin 22, and the most common was extrusion, but there was acase of pneumoperitoneum and septic shock, whichrequired a laparotomy and treatment with antibiotics(Table 3). However, the patient recovered dying only2 months later.
The overall median survival after the procedure forfeeding was 61 days (range 1 to 551 days). Nineteenpatients (12%) survived 1 week or less after performing thegastrostomy, 28 (18%) between 8 and 30 days, 51 (33%) 31to 90 days, 53 (35%) 91 days or more, and two unknown.In other words, 31% survived for 1 month or less and 69%survived for more than 1 month. Analyzing the survival ofonly the 73 patients who only underwent the gastrostomy
for nutrition after the admission to the PUC and whoseECOG performance status index was known, we canobserve that 14 patients (19%) died in the first week(Table 4). From those patients, 20 were classified as ECOG4, although nine of them survived for more than 1 monthand two for more than 3 months. On the other hand, theonly patient in this series with a performance status ECOG1 survived for only 1 day due to a cause probably unrelatedwith the gastrostomy and two patients classified as ECOG2 died in the first week after the gastrostomy (Table 4). Infact, the only statistically significant difference wasobserved between the survival after the gastrostomy ofECOG 2 and ECOG 4 patients (p<0.05).
The patient who underwent a gastrostomy for bowelobstruction was a 52-year-old man with colon cancer withperitoneal carcinomatosis and an ECOG 3 when thegastrostomy was performed. He survived for only 7 days.The only complication observed was mild local pain.
One hundred and twenty-five patients (81%) died at thePCU, 26 (17%) at home, and four (3%) at other places.
Discussion
In palliative care, feeding can have different objectives.Eating can be one of the most pleasant activities in life; oneof its goals is to maintain nutritional status and functionalperformance; another goal is to satisfy hunger and thirst.Nutrition prevents cachexia and related symptoms,although not always; feeding has a comfort objective,which in some cases, mainly in the last phase of life, is theonly one. Food and meals also have important social andemotional aspects, which in many cases influence thefeelings and decisions of patients and their families andthey tend to pressure the professionals to do something tokeep feeding them in situations when it is biologicallyfutile, even after detailed explanations.
The goals of enteral nutrition, in this case via gastros-tomy, is more modest, however important. The biologicgoals are to restore or maintain the nutritional status and toimprove or prevent the symptoms related to malnutritionsuch as weakness, nausea, depression, irritability, and loss
Table 3 Complications observed in the 153 patients who underwentthe gastrostomy for nutrition
Early LateNumber of patients(%)
Number of patients(%)
MinorAbdominal pain, mild 39 (25) 17 (11)Fullness after feeding 4 (3) 5 (3)Nausea/vomiting 3 (2) 1 (1)Infection, local 2 (1) 5 (3)Tube blockage 4 (3) 4 (3)Stomal leak 2 (1) 2 (1)Total 55 35MajorPeritonitis 1 (1)Pneumoperitoneum +septic shock
1 (1)
Tube extrusion 1 (1) 16 (10)Infection, local severe 3 (2)Abdominal pain,replacement needed
1 (1)
Abdominal pain,severe
2 (1) 2 (1)
Total 5 22
Some patients had more than one complication
Table 4 Survival after gastrostomy performance for nutrition of the73 patients whose ECOG score was known
Survival after the gastrostomy (days)
1–7 8–30 31–90 >90
ECOG1 12 2 1 7 83 7 10 10 74 4 7 7 2Total 14 18 24 17
All patients underwent the gastrostomy after admission to the PCU
1149

200 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
141
of concentration. There are also emotional effects becausethe patient is being fed. At our unit, when the situation isstable, usually 30 kcal/kg of body weight per day are given,as calculated by the nutritionist, besides hydration. Withthe evolution of the disease and the deterioration of thepatient’s condition, the situation is frequently reviewed andin the last days, if it is foreseeable, only hydration is given.When gastrostomies are in place, they can also be veryuseful for medication, besides nutrition and hydration.
Dysphagia is common in head and neck and esophaguscancers. This is a situation very different from theincapacity of swallowing due to frailty when patients areclose to death. Frequently, head and neck and esophagealcancers cause dysphagia not necessarily because they arefar advanced but due to its strategic position. However,starvation caused by dysphagia can deteriorate patients’quality of life quickly. Therefore, bypassing the obstructioncan be justified. Besides dysphagia, there are otherjustifications for bypassing the mouth or the esophaguslike fistulas orocutaneous, which can cause leaks of liquidsand food from the mouth, or fistulas tracheoesophageal,which allow the passage to the trachea causing cough,infections, and dyspnea.
There are various methods to feed patients, eitherparenteral or enteral. Parenteral nutrition should bereserved for patients who cannot tolerate enteral feedingand have a reasonable prognosis [5]. Enteral feeding is amore physiologic approach, besides a much less expensiveone, and should be used when the digestive tract isfunctional. The gastrointestinal delivery of nutrients isthought to improve the status of the gut immune systemand maintain the normal gut architecture and microflora[6].
The nasogastric tube (NG) is an easy and inexpensivemethod. However, it should be reserved for short-termfeeding because it can cause a number of complicationssuch as: migration of the tube (mainly into the esophagus),pulmonary aspiration of infused solutions, lesions of thegastrointestinal tract mucosa by the tip of the tube, ear andnose infections, esophageal strictures, vocal cord andpharyngeal paralysis, and others [6]. Besides these possiblecomplications, there is the problem of the self-image.
Studies comparing NG with PRG in advanced head andneck cancer [7] and with PEG in neurological patients [8]showed that gastrostomy is a safe and effective method ofproviding long-term parenteral nutrition and offers im-portant advantages over NG. Considering all those reasons,gastrostomy is probably the method of choice for long-termenteral feeding. There are other methods that can beused such as jejunostomy, cervical pharyngostomy, andesophagostomy.
There are, however, a number of complications related tothe procedure, most of them minor. The criteria used inother studies to classify the severity of the complicationswere usually not stated and sometimes the classification
was contentious such as when aspiration pneumonia wasconsidered a minor problem [8].
Some complications are early, the most frequent is locallight pain related with the procedure, which disappears in afew days. Others are late, the most common is tubeextrusion, which usually does not result in a bad outcome,although it is inconvenient because it upsets the patientsand the family and requires travelling to the place where thesituation can be solved, such as when the patient is at home,and sometimes a new gastrostomy must be done. There israrely a fatal outcome, as described by others [9] due toperitonitis or respiratory problems. In one study of 50patients with head and neck cancer, there were tworespiratory arrests during the PEG performance thatrecovered uneventfully [10].
Although we have some patients with NGs andjejunostomies, by far the most used method for enteralfeeding is percutaneous gastrostomy performed by inter-ventional radiology. However, the Service of Gastroenter-ology of our hospital has started to perform PEG recently,so probably in the future they will be more used than PRGbecause they allow the use of tubes with wider calibre.PRG, however, will remain a useful alternative to PEGwhen they cannot be performed due to an obstruction of theupper digestive tract preventing the introduction of theendoscope.
Other useful use of enteric tubes is to decompress the gutwhen there is intestinal obstruction in selected cases whensurgery is not indicated and pharmacological measures failto acceptably palliate the symptoms. Malone et al. [11] in1986 were the first to report the use of gastrostomies todecompress the bowel under radiological guidance. Thisallows patients to ingest at least liquids at ease withoutvomiting by opening the tube from time to time or whenthey feel nausea. In our study, only one patient underwent agastrostomy to drain the bowel content, but in the study ofHull et al. [9], 67% of the gastrostomies were performed inpatients with bowel obstruction. There are also studiesdescribing only gastrostomies for drainage [11, 13–15]showing satisfactory safety and significant improvement inthe patients’ quality of life.
Nineteen patients (12%) lived for 1 week or less. Thatcould be due to the inadequate selection of some of themand/or to the well-known uncertainly in prognostication.Anyway, we should be attentive to this fact and discuss it inthe team to try to make a better selection of the patients forgastrostomies. The ECOG performance status indexdemonstrates in this study that it is not accurate enoughto select patients to gastrostomies because there is, in eachlevel of the ECOG, a wide range of survival times.
This study has the weaknesses typical to retrospectivestudies. There is a number of missing data and somedifficulty to interpret the records, which usually are notsuited to be studied later. It would be important to assessthe level of patients’ satisfaction with the procedure and
1150

| 201 201Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
142
nutritional status before the operation and regularly duringthe follow-up and to assess its impact in symptoms such asfatigue and the quality of life.
Conclusion
Gastrostomies are a useful method to palliate dysphagiaand some cases of bowel obstruction. However, there are a
number of complications, usually minor, but some of thempotentially severe and even rarely fatal. Palliative carepatients are probably particularly vulnerable to complica-tions because of their weakness and denutrition associatedwith advanced disease. Therefore, the patients should becarefully selected to undergo gastrostomies. Patients with avery short survival do not benefit from the procedure andso it should not be considered. It would be interesting toknow the results of the practice of other PCUs.
References
1. Walker LG (1984) L. L. Straton MD,and the first successful gastrostomy inAmerica. Surg Gynecol Obstet158:387–388
2. Wollman B, D’Agostino HB, Walus-Wigle JR, Easter DW, Beale A (1995)Radiologic, endoscopic, and surgicalgastrostomy: an institutional evaluationand meta-analysis of the literature.Radiology 197:699–704
3. Preshaw RM (1981) A percutaneousmethod for inserting a feeding gastros-tomy tube. Surg Gynecol Obstet152:659–660
4. Ferraz Gonçalves JAS (2001) A Por-tuguese palliative care unit. SupportCare Cancer 9:4–7
5. Mercadante S (1998) Parenteral versusenteral nutrition in cancer patients:indications and practice. Support CareCancer 6:85–93
6. Waitzberg DL, Plopper C, Terra RM(2000) Access route for nutritionaltherapy. World J Surg 24:1468–1476
7. Magné N, Marcy PY, Foa C, FaleweeMN, Schneider M, Demard F,Bensadoun RJ (2001) Comparisonbetween nasogastric tube feeding andpercutaneous fluoroscopic gastrostomyin advanced head and neck cancerpatients. Eur Arch Otorhinolaryngol258:89–92
8. Park RHR, Allison MC, Lang J et al(1992) Randomised comparison ofpercutaneous endoscopic gastrostomyand nasogastric tube feeding in patientswith persisting neurological dysphagia.BMJ 304:1406–1409
9. Hull MA, Rawlings J, Murray FE et al(1993) Audit of outcome of long-termenteral nutrition by percutaneous endo-scopic gastrostomy. Lancet 341:869–872
10. Hunter JG, Lauretano L, Shellito PC(1989) Percutaneous endoscopic gas-trostomy in head and neck cancerpatients. Ann Surg 210:42–46
11. Malone JM, Koonce T, Larson DM,Freedman RS, Carrasco CHO, Saul PB(1986) Palliation of small bowel ob-struction by percutaneous gastrostomyin patients with progressive ovariancarcinoma. Obstet Gynecol 68:431–433
12. O’Keeffe F, Carrasco CH, CharnsangajevC, Richli WR, Wallace S, FreedmanRS (1989) Percutaneous drainage andfeeding gastrostomies in 100 patients.Radiology 172:341–343
13. Scheidbach H, Horbach T, Groitl H,Hohenberger W (1999) Percutaneousendoscopic gastrostomy/jejunostomy(PEG/PEJ) for decompression in theupper gastrointestinal tract. Surg En-dosc 13:1103–1005
14. Pothuri B, Montemarano M, Gerardi Met al (2005) Percutaneous endoscopicgastrostomy tube placement in patientswith malignant bowel obstruction dueto ovarian carcinoma. Gynecol Oncol96:330–334
15. Brooksbank MA, Game PA, AshbyMA (2002) Palliative venting gastros-tomy in malignant intestinal obstruc-tion. Palliat Med 16:520–526
1151

202 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 203 203Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
143

204 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
144

| 205 205Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
145

206 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 207 207Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
146
Sedation and Expertise inPalliative Care
TO THE EDITOR: Sedation intending to control pain related witha procedure is not an ethical problem, is used in many fields ofmedicine, and is widely accepted. Therefore, I will not address thisparticular context and I will only focus on sedation used to control thesuffering that doctors cannot treat by any other means.
Among palliative care professionals there is a consensus thatsedation is, in certain conditions, an acceptable method to controlsymptoms that cannot be controlled without affecting the conscious-ness level. However, this consensus does not exist among all healthprofessionals, as this practice was thought by some of them to berelated with euthanasia,1 and sometimes is called slow euthanasia.2
Palliative care literature has produced important definitions andguidelines regarding this kind of sedation, trying to create an ethicalframework and a common language, in order to reach comparabilityamong data from diverse settings. I believe there is now a consensusthat the level of sedation to be reached should be the one that relievesthe symptom and not necessarily a deep sedation, as the definition ofChater et al implies.3 That is, the goal is symptom control, not a certainlevel of consciousness. Mild sedation (conscious sedation) if enoughto make a patient comfortable is not an ethical problem, but deepsedation can make physicians and ethicists disagree about its legiti-macy, namely if nutrition and hydration should be maintained andthe implication of withholding or withdrawing them on survival.1,4
I also believe that there is a consensus among palliative carephysicians that the decision to initiate sedation is legitimate only if thesymptom is refractory. And a refractory symptom, according toCherny and Portenoy,5 can be defined as one that “cannot be ade-quately controlled despite aggressive efforts to identify a tolerabletherapy that does not compromise consciousness” and the physicianshould perceive that other intervention either invasive or noninvasiveare: “(A) incapable of providing adequate relief, (B) associated withexcessive and intolerable acute or chronic morbidity, or (C) unlikelyto provide relief within a tolerable time frame.”5 A different situationwould be a symptom that is difficult to control, but that is potentiallycontrollable within a tolerable time frame, and in this case, sedatingthe patient is not indicated.
Another consensus, implied by the definition of refractory symp-tom, is the expertise and experience required in palliative care andsymptom control in order to ensure that sedation is used as a lastresource, when nothing else effectively works.
Expertise and experience are, however, a relative concept andheterogeneous in a worldwide context and even within the countries.Although, trying to distinguish difficult from refractory symptoms isan important theoretic effort, the distinction will never be settled in away that can be universally applied. There are countries where thereare only a few palliative care teams, if there are any. The stage ofdevelopment of the teams can be very different. Probably, in mostcountries, the majority of the patients with very advanced chronic
diseases are treated by doctors and teams without any expertise insymptom control. What can we recommend in this situation? Shouldwe say that, as they are not experts in palliative care, perhaps theproblem could be controlled by someone else? However, someone elsewho might know what to do is probably not available. And, certainly,the most important concern is to relieve patients’ suffering. To letthem suffer is not an option. As Robert Twycross wrote about eutha-nasia “a doctor who leaves a patient to suffer intolerably is morallymore reprehensible than the doctor who performs euthanasia.”6 Morereprehensible would be to leave a patient suffer without trying a methodwhich is, in general, believed as morally much less problematic.
My point is that the rules that palliative care physicians establishfor themselves in order to control the quality of their work and achievethe excellence of care which patients deserve are not universally appli-cable. Without expertise in palliative care, the priority should continueto be the control of suffering, certainly involving discussion in theteam and all the knowledge available of colleagues, pain specialists,psychiatrists, and all others who can help, without forgetting that timecan be an important variable. But, if after that, the problem is notsatisfactorily solved and many doubts remain, I believe that if thepatient agrees (if the patient is incompetent, the team should actaccording to the patient’s best interests—this is another discussion),the sedation needed to control the problem should start. However, inthose contexts of much uncertainty, sedation should proceed carefully(well, in all contexts it should) and if deep sedation is required, itshould be intermittent with scheduled periods of relief and revalua-tion. At least hydration should be maintained in order to keep thereversibility of the process, unless the patient was not eating or drink-ing anymore or is obviously dying in a few hours.
Usually, sedation is morally justified by the principle of doubleeffect,7 which distinguishes the intended from the foreseen conse-quences of an act. However, these intensions may be ambiguous andsometimes even the actor is not sure about their real intensions. It is,perhaps, more realistic to consider that the primary obligation of adoctor to a suffering patient, with an untreatable very advancedchronic disease, is to relieve him or her, and sometimes there is not asolution for it that does not compromise consciousness. The will of thepatient, if can be expressed, is essential in the process of decision.
I believe that this topic deserves a broad discussion. Therefore, Ihope to hear comments on this letter.
José Antonio Ferraz GoncalvesInstituto Portugues de Oncologia, Porto, Portugal
REFERENCES1. Orentlicher D: The Supreme court and physician-assisted suicide: Rejecting
assisted suicide but embracing euthanasia. N Engl J Med 337:1236-1239, 19972. Billings JA, Block SD: Slow euthanasia. J Palliat Care 12:21-30, 19963. Chater S, Viola R, Paterson J, et al: Sedation for intractable distress in the
dying: A survey of experts. Palliat Med 12:255-269, 19984. Craig GM: On withholding artificial hydration and nutrition from terminally ill
sedated patients: The debate continues. J Med Ethics 22:147-153, 19965. Cherny NI, Portenoy RK: Sedation in the management of refractory symp-
toms: Guidelines for evaluation and treatment. J Palliat Care 10:31-38, 19946. Twycross RG: Euthanasia: Going Dutch? J R Soc Med 89:61-63, 1996
JOURNAL OF CLINICAL ONCOLOGY C O R R E S P O N D E N C E
VOLUME 24 � NUMBER 25 � SEPTEMBER 1 2006
e44 Journal of Clinical Oncology, Vol 24, No 25 (September 1), 2006: pp e44-e45
Copyright © 2006 by the American Society of Clinical Oncology. All rights reserved. Downloaded from jco.ascopubs.org on June 5, 2009 . For personal use only. No other uses without permission.

208 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
147
7. Rousseau P: The ethical validity and clinical experience of palliative seda-tion. Mayo Clin Proc 75:1064-1069, 2000
DOI: 10.1200/JCO.2006.07.6810■ ■ ■
Author’s Disclosures of Potential Conflicts of InterestThe author indicated no potential conflicts of interest.
Correspondence
www.jco.org e45
Copyright © 2006 by the American Society of Clinical Oncology. All rights reserved. Downloaded from jco.ascopubs.org on June 5, 2009 . For personal use only. No other uses without permission.
| 209 209Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
149
Palliative Medicine 2008; 22: 13–32
© 2008 SAGE Publications, Los Angeles, London, New Delhi and Singapore 10.1177/0269216307085183
Introduction
Fatigue is a frequent, almost ubiquitous symptom in cancerpatients as well as in noncancer patients with progressive
life-threatening diseases such as multiple sclerosis, amy-otrophic lateral sclerosis or chronic heart or lung disease.Fatigue has a major impact on the quality of life in thesepatients.
The prevalence and impact of fatigue often have not beenrecognized by physicians.1 In a US survey, more than half ofthe patients reported that they had never talked about fatiguewith their physician and the two most frequent reasons forthis were the doctors’ failure to offer interventions and thepatients’ lack of awareness of effective treatments.2
Fatigue in palliative care patients – an EAPC approachLukas Radbruch* Department of Palliative Medicine, RWTH Aachen University, Aachen, Florian Strasser* Department of Internal Medicine, Cantonal Hospital, St. Gallen, Frank Elsner Departmentof Palliative Medicine, RWTH Aachen University, Aachen, Jose Ferraz Gonçalves Department of PalliativeCare, Portuguese Institute of Oncology, Porto, Jon Løge Department of Behavioral Sciences in Medicine,University of Oslo, Oslo, Stein Kaasa Palliative Medicine Unit, Department of Oncology, St Olavs Hospital,Trondheim, Friedemann Nauck Department of Palliative Medicine, University of Göttingen, Göttingen, Patrick Stone Department of Mental Health, St George’s Hospital Medical School, London and the ResearchSteering Committee of the European Association for Palliative Care (EAPC)
Fatigue is one of the most frequent symptoms in palliative care patients, reported in .80%of cancer patients and in up to 99% of patients following radio- or chemotherapy. Fatiguealso plays a major role in palliative care for noncancer patients, with large percentages ofpatients with HIV, multiple sclerosis, chronic obstructive pulmonary disease or heart failurereporting fatigue.This paper presents the position of an expert working group of theEuropean Association for Palliative Care (EAPC), evaluating the available evidence on diag-nosis and treatment of fatigue in palliative care patients and providing the basis for futurediscussions. As the expert group feels that culture and language influence the approach tofatigue in different European countries, a focus was on cultural issues in the assessmentand treatment of fatigue in palliative care.As a working definition, fatigue was defined as a subjective feeling of tiredness, weaknessor lack of energy. Qualitative differences between fatigue in cancer patients and in healthycontrols have been proposed, but these differences seem to be only an expression of theoverwhelming intensity of cancer-related fatigue.The pathophysiology of fatigue in palliative care patients is not fully understood. For a sys-tematic approach, primary fatigue, most probably related to high load of proinflammatorycytokines and secondary fatigue from concurrent syndromes and comorbidities may be differentiated. Fatigue is generally recognized as a multidimensional construct, with a physical and cognitive dimension acknowledged by all authors. As fatigue is an inherentword only in the English and French language, but not in other European languages,screening for fatigue should include questions on weakness as a paraphrase for the physical dimension and on tiredness as a paraphrase for the cognitive dimension.Treatment of fatigue should include causal interventions for secondary fatigue and symptomatic treatment with pharmacological and nonpharmacological interventions.Strong evidence has been accumulated that aerobic exercise will reduce fatigue levels incancer survivors and patients receiving cancer treatment.In the final stage of life, fatigue may provide protection and shielding from suffering for thepatient and thus treatment may be detrimental. Identification of the time point, wheretreatment of fatigue is no longer indicated is important to alleviate distress at the end of life. Palliative Medicine 2008; 22: 13–22.
Key words: fatigue; palliative care; cancer-related fatigue; recommendations
Address for correspondence: Professor Dr Lukas Radbruch,Department of Palliative Medicine, RWTH Aachen University,52074 Aachen, Germany. E-mail: [email protected]*Both authors contributed equally to the paper.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

210 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
150
14 L Radbruch et al.
However, fatigue has received more attention in recentyears, as quality of life has increasingly been used as an end-point in oncological trials. In addition, research on anaemiaand cachexia has provided some insight into the pathophys-iology of fatigue. The role of proinflammatory cytokines incachexia and fatigue is under investigation (reviewed in3–5).Cancer trials using erythropoietin found less fatigue withincreased haemoglobin levels (reviewed in6,7). The NationalInstitute of Health has included fatigue together with painand depression in their call for increased awareness insymptom management in cancer,8 and the 6th FrameworkProgramme on Research, Technological Development andDemonstration of the European Union has taken this up inthe call for research proposals.
Fatigue also is coming into focus in palliative careresearch. Pharmacological treatment of opioid-inducedsedation with methylphenidate or other drugs has suggestedthat fatigue may be relieved in palliative care patients.9,10
In the light of the increased awareness of fatigue, thequestion can be raised whether fatigue has reached the pointthat cancer pain management passed 20 years ago: aware-ness of the problem leading to clear and easy treatmentguidelines, providing adequate symptom relief for mostpatients. On the other hand, it has been argued that fatigue isfundamentally different from other symptoms, as it may bean inevitable part of the end of life itself.
A consensus position on fatigue is an important first steptowards developing recommendations for clinical practiceand a research agenda. Recognizing the need for a struc-turedapproach, the Research Network of the European Associationfor Palliative Care (EAPC) has initiated an expert workinggroup on fatigue in palliative care, to provide consensualpositions and define areas where consensus is not available.
Methodology
An expert working group of the EAPC met in November2003 to evaluate the available evidence on diagnosis andtreatment of fatigue in palliative care patients. The expertgroup did not follow a formal consensus process. The expertgroup also decided against an attempt to produce evidence-based guidelines.
The authors felt that there is not enough consensus onmany fatigue topics. Even the definition of fatigue is notused unanimously in trials and publications, preventing com-parison of outcomes. Most available evidence on treatmentoptions has been gathered in cancer patients undergoingchemotherapy and it is not clear how much of this data istransferable to palliative care patients. A purely evidence-based approach would also not be able to integrate resultsfrom qualitative research, which can provide valuableinsights into symptom burden and the need for treatment inpatients with fatigue.
The authors decided to present a comprehensive review onfatigue in palliative care patients. This paper represents theposition of the working group. It establishes the importanceof adequate recognition, assessment and treatment of fatiguein palliative care.
The focus of this paper is on patients with far advanced can-cer or at the end stages of other progressive diseases receivingpalliative care. The expert group feel that since culture andlanguage influence the approach to fatigue in differentEuropean countries, it is important to acknowledge culturalissues wherever appropriate. The expert group formulatedstatements that reflect consensus in the expert group whereverpossible, supported by evidence where available and the needfor discussion and further research in other areas.
Draft statements were based on the workshop discussionsand refined in an ongoing email discussion among theauthors. For each statement, the literature was searchedusing Medline (Pubmed) and palliative care textbooks byone of the authors (LR) with appropriate search strategiesfor evidence supporting or refuting the statement. Thestatements were further refined wherever the evidencenecessitated adaptation or change.
Other reviews and expert papers on fatigue in cancerpatients have been published recently11–17 and these reviewswill be referred to if possible. Evidence-based guidelineshave been presented by the National Comprehensive CancerNetwork (NCCN)18 for cancer patients, collating predomi-nantly nonpharmacological treatment options for fatigue.
Epidemiology and impact of fatigueFatigue is one of the most frequent symptoms in palliativecare patients, impairing quality of life considerably. Fatigueis reported by not only a majority of patients with advancedcancer, but also many cancer survivors, patients withcardiac failure or with HIV/AIDS.
Fatigue in cancer and noncancer palliative care patientsis under-recognized, under-assessed and under-treated.
Fatigue is one of the most frequent symptoms of cancer andcancer treatment. Fatigue (84%), weakness (66%) and lack ofenergy (61%) were three of the five most frequent symptomsin a study of 1000 patients in an American palliative care program.19 Fatigue has been reported in up to 99% of patientsfollowing radiotherapy or chemotherapy (review in11,20).Seventeen to 56% of long-term survivors report fatigue as oneof the major symptoms impairing quality of life even monthsafter treatment has ended (review in11). In interviews with par-ents of children who had died from cancer, fatigue was themost common symptom affecting 57% of patients.21
Physical fatigue prevents participation in preferred activi-ties and impedes activities of everyday living. Cognitivefatigue complicates activities such as reading or driving a carand thus prevents leisure activities. Fatigue often is associ-ated with affective disturbances and patients feel listless,depressed, irked or paralyzed. In many cancer patients
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 211 211Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
151
Fatigue in palliative care patients 15
fatigue impedes quality of life significantly. Patients under-going chemotherapy rated fatigue as the symptom with thehighest impact on daily living, with 91% of fatigued patientsstating that fatigue prevented them from leading a ‘normal’life.22 Patients felt that fatigue affected their daily life morethan pain after chemo- or radiotherapy, whereas physiciansbelieved that pain adversely affected their patients more thanfatigue.1
Fatigue also plays a major role in palliative care for non-cancer patients. More than half of the patients with multiplesclerosis describe fatigue as one of their most troublingsymptoms (reviews at23–25). Fatigue has also been reportedfor the majority of patients with chronic obstructive pul-monary disease26 and heart failure.27 Approximately half ofthe HIV-patients suffer from fatigue.28,29 As with cancer-related fatigue, the aetiology often is multifactorial.30
Despite being a common symptom, fatigue has notreceived much attention from palliative care specialistscompared with other symptoms such as pain or dyspnoea.Both nonspecialized and specialized physicians frequentlyconsider fatigue as a natural trait of advanced, incurableillness that has to be endured. Treatment options for fatigueare often perceived as scarce and reduction of patient activi-ties is often the only advice given. The consensus group feltthat inadequate assessment skills and insufficient knowledgeabout multidimensional treatment options can lead to non-recognition, under-assessment and under-treatment offatigue in the vast majority of patients.
Definition of fatigueAs a working definition fatigue is defined as a subjectivefeeling of tiredness, weakness or lack of energy.Qualitative differences between fatigue in cancer patientsand in healthy controls have been proposed. However, thesedifferences seem to be only an expression of the overwhelm-ing intensity of cancer-related fatigue.
In the nonmedical setting, fatigue can have various mean-ings. In humans and animals, it can be used as a noun for the‘temporary loss of strength and energy resulting from hardphysical or mental work’. In materials (especially metals), itcan mean ‘the state of being weakened by long stress’. It canalso be used as a verb to mean ‘to exhaust or tire through over-use or great strain or stress’ (http://www.hyperdictionary.com,access date 19 September 2006).
In the medical context of cancer, different definitions havebeen proposed for fatigue. National Comprehensive CancerNetwork defines cancer-related fatigue as a ‘distressing,persistent, subjective sense of tiredness or exhaustion relatedto cancer or cancer treatment that is not proportional torecent activity and interferes with usual functioning’(www.nccn.org/physician_gls/PDF/fatigue.pdf, access date19 September 2006). A similar definition has been used forfatigue in multiple sclerosis: ‘a subjective lack of physicaland/or mental energy that is perceived by the individual orcaregiver to interfere with usual and desired activities’.23
The Oncology Nursing Society defines cancer-relatedfatigue ‘as a feeling of debilitating tiredness or total lack ofenergy that can last for days, weeks or months; commonlycaused by anaemia, fatigue is the side effect of chemother-apy that affects patients the most – more than nausea, pain ordepression; symptoms include feeling weak or worn out,having difficulties climbing stairs, walking short distancesand performing simple daily tasks; proper nutrition, lightexercise, short naps and medications may help alleviate thefatigue’ (http://www.cancersymptoms.org/glossary.shtml,access date 19 September 2006).
Glaus has stressed the qualitative difference of cancer-related fatigue to fatigue in everyday life: ‘Fatigue in cancerpatients is a subjective feeling of unusual tiredness, affectingthe body (physical), the emotions (affective) and the mentalfunction (mental), persisting for several weeks and relievedonly partially or not at all with rest or sleep. Fatigue inhealthy people is a subjective feeling with circadian rhythm,which may be pleasant and normally is relieved by rest’.31
Fatigue has also been defined as a clinical syndrome. TheFatigue coalition has suggested the use of the InternationalClassification of Diseases-10 (ICD-10) criteria for the defi-nition of cancer-related fatigue requiring ‘significant fatigue,diminished energy or increased need to rest, disproportion-ate to any recent change in activity level’ to be present everyday or nearly every day for two consecutive weeks out of thelast month (Table 1). Five out of ten additional symptoms
Table 1 Definition of fatigue in the international classifica-tion of diseases (ICD-10)32
A1 and at least five out of A2–A11 have been present formost days in at least two consecutive weeks in the pastmonth
AA1 Significant fatigue, diminished energy or increased
need to rest, disproportionate to any recent change in activity level
A2 Generalized weakness, limb heavinessA3 Diminished concentration or attentionA4 Decreased motivation or interest to engage in usual
activitiesA5 Insomnia or hypersomniaA6 Experience of sleep as unrefreshing or nonrestorativeA7 Perceived need to struggle to overcome inactivityA8 Marked emotional reactivity (such as sadness,
frustration, irritability) to feeling fatiguedA9 Difficulty completing daily tasks attributed to feeling
fatiguedA10 Perceived problem with short-term memoryA11 Postexertional malaise lasting several hours
B The symptoms cause clinically significant distress or impairment in social, occupational or other important areas of functioning
C Evidence from history, physical examination or laboratoryfindings, that symptoms are a consequence of canceror cancer treatment
D Symptoms are not primarily a consequence of comorbidpsychicatric disorders such as major depression, somatization disorder, somatoform disorder or delirium
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

212 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
152
16 L Radbruch et al.
such as generalized weakness, diminished concentration,insomnia or hypersomnia and unrestorative sleep arerequired for the diagnosis.32 The authors emphasize thatfatigue must cause significant distress or impairment, is to beassociated with cancer or cancer treatment and must not bedue to a comorbid psychiatric disorder. This definition issimilar to that used for Chronic Fatigue Syndrome (CFS),which has been described as a specific illness in its own rightand is probably caused by central nervous dysfunction(review in33). The threshold of six symptoms (fatigue and fiveothers) and the time span of at least two weeks have beenchosen arbitrarily, with the intention of capturing variouscauses of fatigue, but so as not to render the diagnosis triv-ial.34 The authors found that although 37% of cancer patientsreported fatigue for at least two weeks in the previous month,only 17% fulfilled their strict criteria for cancer-relatedfatigue syndrome. However, since 79% of the patientsreported ‘debilitating fatigue,’32 it may be that this ratherstrict definition of the fatigue syndrome excludes manypatients who should have been assessed and treated forfatigue. The International Classification of Diseases-10 crite-ria have been defined to recognize the fatigue syndrome in allstages of cancer from active treatment to advanced stages aswell as to survivorship, but may be of limited value for diag-nosis of fatigue in the palliative care setting, where the preva-lence of concomitant psychological disorders is high.35,36
Some authors state that cancer-related fatigue is qualita-tively different from the fatigue that everyone feels afterexercise,32,37–39 and cancer patients report that they are lesslikely to recover from fatigue during sleep. A self-reportdescribed cancer-related fatigue as totally unlike even themost profound fatigue of an otherwise well person.40
However, the consensus group emphasized that cancer-related fatigue does not seem to be qualitatively differentfrom fatigue in healthy humans, but simply represents oneend of a continuum of intensity. Less severe fatigue in can-cer patients may also be relieved by rest.
Fatigue is not uncommon in the general population. Aprevalence of fatigue up to 28% has been found in unse-lected patient groups treated by general practitioners.41,42
Pawlikowska et al. looked at the prevalence of fatigue in ageneral population and found that fatigue is continuouslydistributed in the community. Substantial fatigue lasting sixmonths or longer was reported by 18% of the respondents.43
Stone et al. defined severe fatigue as an intensity score inexcess of the 95th percentile of a healthy control group andfound the prevalence of severe fatigue to vary between 15%in recently diagnosed breast cancer patients and 78% inpatients receiving inpatient palliative care.44 Mendoza et al.found that healthy controls consistently rated fatigue levelsas lower than cancer patients using a variety of differentfatigue instruments.45
The second edition of the Oxford Textbook of PalliativeMedicine uses the concept of asthenia and finds that fatigueis only one of the dimensions of asthenia: ‘Astenos (Greek)
means absence or loss of strength. Asthenia includes threedifferent major symptoms: (1). fatigue or lassitude defined aseasy tiring and decreased capacity to maintain performance;(2). generalized weakness defined as the anticipatory sensa-tion of difficulty in initiating a certain activity and (3).mental fatigue defined as the presence of impaired mentalconcentration, loss of memory and emotional lability’.46
Finally, fatigue has been described not as a clinical symp-tom, but as a behavioural concept, where the symptom is partof a continuum ranging from tiredness to fatigue and then toexhaustion.47 These stages are related to defined behaviouralpatterns. Nonadaptation will lead to progression towardsexhaustion, at least in patients with normal haemoglobinlevels.
These differences in the concepts of fatigue present anobstacle to producing a common definition of fatigue inEurope. Nevertheless, agreement on a working definition isclearly necessary. The working definition of fatigue shouldbe simple and should take into account that fatigue in pallia-tive care is a symptom that may be caused by the underlyingdisease, its treatment or by other comorbidities. For thispaper, the following working definition is used: Fatigue is asubjective feeling of tiredness, weakness or lack of energy.
This definition corresponds closely to the fatigue subscaleof the quality of life questionnaire of the EuropeanOrganisation for Research and Treatment of Cancer(EORTC QLQ-C30 version 3) that is calculated from thethree questions ‘have you felt weak?’, ‘were you tired?’ and‘did you need to rest?’.48,49 This pragmatic approach facili-tates comparable working definitions in different Europeanlanguages, as the EORTC QLQ-C30 has been translated andvalidated in more than 50 languages.
The working definition does not include any qualitativedifference between cancer-related fatigue and fatigue in othersettings, as the inability to relieve fatigue with rest as well asinterference with function seem to be indicators of the inten-sity of fatigue rather than criteria for the quality of fatigue.
Cancer-related fatigue usually is considered a negativeemotion. However, in a German study, two out of 117 patientswith chronic pain commented that they found it pleasant.50
The working definition relies on the subjective assessmentof the patient only. Currently no objective measurement offatigue is feasible, though objective activity assessment forweakness as a subdimension of fatigue has been proposed.However, as palliative care focuses on the subjective condi-tion of the patient, the subjective assessment should be theindicator for treatment.
There seems to be considerable overlap between fatigueand depression.51 Weakness and tiredness are among thepredominant symptoms of depression and feeling depressedoften is part of the affective dimension of fatigue. However,there are some symptoms that are reported only with depres-sion (such as sustained feelings of worthlessness, recurrentthoughts of death) and some symptoms are specific forfatigue (such as postexertional malaise).51
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from
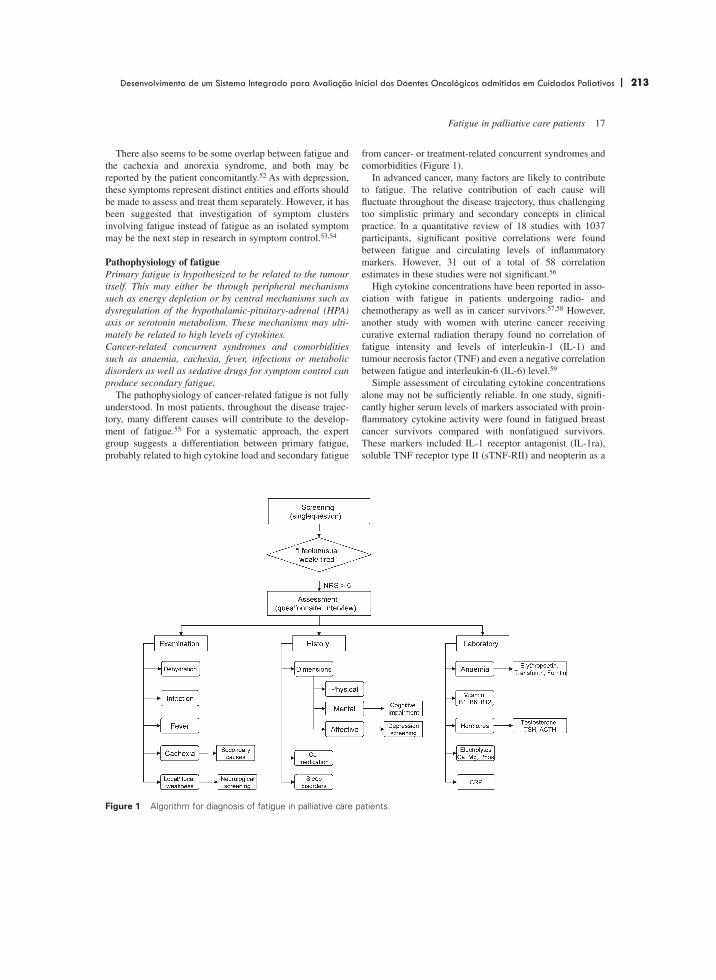
| 213 213Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
153
Fatigue in palliative care patients 17
There also seems to be some overlap between fatigue andthe cachexia and anorexia syndrome, and both may bereported by the patient concomitantly.52 As with depression,these symptoms represent distinct entities and efforts shouldbe made to assess and treat them separately. However, it hasbeen suggested that investigation of symptom clustersinvolving fatigue instead of fatigue as an isolated symptommay be the next step in research in symptom control.53,54
Pathophysiology of fatiguePrimary fatigue is hypothesized to be related to the tumouritself. This may either be through peripheral mechanismssuch as energy depletion or by central mechanisms such asdysregulation of the hypothalamic-pituitary-adrenal (HPA)axis or serotonin metabolism. These mechanisms may ulti-mately be related to high levels of cytokines.Cancer-related concurrent syndromes and comorbiditiessuch as anaemia, cachexia, fever, infections or metabolicdisorders as well as sedative drugs for symptom control canproduce secondary fatigue.
The pathophysiology of cancer-related fatigue is not fullyunderstood. In most patients, throughout the disease trajec-tory, many different causes will contribute to the develop-ment of fatigue.55 For a systematic approach, the expertgroup suggests a differentiation between primary fatigue,probably related to high cytokine load and secondary fatigue
from cancer- or treatment-related concurrent syndromes andcomorbidities (Figure 1).
In advanced cancer, many factors are likely to contributeto fatigue. The relative contribution of each cause willfluctuate throughout the disease trajectory, thus challengingtoo simplistic primary and secondary concepts in clinicalpractice. In a quantitative review of 18 studies with 1037participants, significant positive correlations were foundbetween fatigue and circulating levels of inflammatorymarkers. However, 31 out of a total of 58 correlationestimates in these studies were not significant.56
High cytokine concentrations have been reported in asso-ciation with fatigue in patients undergoing radio- andchemotherapy as well as in cancer survivors.57,58 However,another study with women with uterine cancer receivingcurative external radiation therapy found no correlation offatigue intensity and levels of interleukin-1 (IL-1) andtumour necrosis factor (TNF) and even a negative correlationbetween fatigue and interleukin-6 (IL-6) level.59
Simple assessment of circulating cytokine concentrationsalone may not be sufficiently reliable. In one study, signifi-cantly higher serum levels of markers associated with proin-flammatory cytokine activity were found in fatigued breastcancer survivors compared with nonfatigued survivors.These markers included IL-1 receptor antagonist (IL-1ra),soluble TNF receptor type II (sTNF-RII) and neopterin as a
Figure 1 Algorithm for diagnosis of fatigue in palliative care patients.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

214 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
154
18 L Radbruch et al.
measure of macrophage activity.60 Significant correlationsbetween fatigue and IL-1ra and between fatigue andneopterin have been confirmed in a review.56 However, insurvivors from lymphoma with high levels of fatigue 4–10years after bone marrow transplantation, no correlation offatigue intensity with cytokine levels or levels of cytokinemarkers was found.61 Increased levels of vascular endothelialgrowth factor and soluble intercellular adhesion molecule-1(sICAM-1) were related to increased fatigue followinganthracycline-based chemotherapy in patients with advancedbreast cancer.62
The pathophysiology of cytokine-related primary fatigueincludes both peripheral and central components. Peripheralmechanisms may be related to energy imbalance, such asaltered muscular metabolism and central mechanisms mayinvolve changes in the neural function of the HPA axis andneuronal systems underlying arousal and fatigue.38
Peripheral energy depletion following reduced intake offood has been postulated as a cause of fatigue.63 Adenosinetriphospate has been used with good effect on fatigue andcachexia in an open-label, randomized controlled trial,64
leaving the discussion open whether energy delivery or stim-ulation of P2 purinergic-receptors caused the effects. It is notclear whether energy depletion in fatigued patients is mainlya manifestation of concomittant cachexia.
Another hypothesis on primary fatigue relies on evidencefrom animal studies suggesting a reflex circuit with thereduction of somatic muscle tone from vagal afferent stimu-lation. Intraperitoneal injection of IL-1� induced sicknessbehaviour with decreased activity and increased sleep in ratsand abdominal vagotomy abolished or attenuated thisresponse.63 However, evidence in support of this vago-somaticinhibitory reflex is scant.
Comparing patients with cancer-related fatigue withhealthy volunteers, Davis et al. found a reduction of centraldrive in the cancer group, whereas resting twitch force in thebiceps muscle was similar and postfatigue twitch force waseven greater in the cancer group, indicating less physiologi-cal fatigue in the cancer patients.65 These results point to apredominantly central change as the cause of cancer-relatedfatigue.
Dysregulation of the HPA axis has been suggested as a pos-sible central mechanism of primary fatigue. The diurnal corti-sol rhythm was subtly, but significantly changed in fatiguedbreast cancer survivors with a less rapid decline in cortisol levels in the evening hours.66 Compared with nonfatigued survivors, the cortisol response to stress was blunted in thispatient group.67 Fatigue also may be linked to serotonin metab-olism in the brain. The 5-hydroxytryptamine (5-HT) trans-porter, the main mechanism for removal of 5-HT from thesynaptic space, is up-regulated by increased levels of TNF.63
Concurrent syndromes and comorbidities may furtherdrain the reduced resources of energy and increase the feel-ing of fatigue and lack of energy. Proinflammatory cytokinessuch as IL-1, IL-6, TNF or interferon play a major role in thepathophysiology of cachexia, anaemia, fever and infection,all of which can cause or aggravate fatigue (Table 2).68
Cachexia does not only result from reduced nutritionalintake, but has been predominantly linked to a profoundchange in metabolism, with increased proteolysis in skeletalmuscle and increased synthesis of acute phase proteins in theliver.69,70 The involvement of cytokines in cancer-relatedanorexia and cachexia have been extensively researched(reviews in4,69).
Anaemia clearly is a cause of fatigue in cancer patientsand anaemic patients are more fatigued than nonanaemic
Table 2 Laboratory parameters for differential diagnosis of fatigue
Comorbidities Parameter
Anaemia Haemoglobin, transferrin, ferritin, iron, erythropoetin
Electrolytes Calcium (and albumin), magnesium, phosphate
Organ dysfunction Creatinine, bilirubinHypothyroidism TSH, free T3 and T4Infection WBC (white blood cell count),
C-reactive proteinHormones ACTH, cortisol, Cortisol requires a 24-h
free testosterone, melatonin profileVitamin deficiency Vitamin B1, vitamin B6,
vitamin B12Cytokine load Interleukin 1, interleukin 6, Markers for increased
TNF-� (tumour necrosis factor) cytokine load might be better suited than cytokines themselves: IL-1 receptor antagonist (IL-1ra), soluble tumour necrosis factor receptor type II (sTNF-RII) and neopterin (macrophage activity marker)
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 215 215Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
155
Fatigue in palliative care patients 19
patients.71 High cytokine levels diminish erythropoetinsecretion and blunt the erythropoetin response to cancer-related anaemia. Treatment of anaemia with erythropoetincan result in alleviation of fatigue (reviewed in6). However,as the association between haemoglobin level and fatigueintensity is only weak, it has been hypothesized thatimpaired functionality of the haemoglobin instead of justlower levels may be responsible for fatigue.72 However,investigating oxyhaemoglobin dissociation as an indicator ofthe function of the haemoglobin, no differences were foundbetween cancer patients and healthy controls.
Other metabolic disorders such as hypothyroidism,hypogonadism,73 dehydration or electrolyte disturbancessuch as hypercalcaemia, hepatic, cardiac or renal failure,sleep disorders, anxiety or emotional stress may contributeto cancer-related fatigue,74 and treatment of these causesmay alleviate fatigue considerably. New anti-neoplastic ther-apies may be associated with novel causes for secondaryfatigue. Hypomagnesaemia following anti-neoplastic treatment with cetuximab, a monoclonal antibody to theepithelial growth factor receptor has been reported recentlyas a cause of secondary fatigue.75,76 Depression has beenlinked with fatigue and fatigue is one of the main symptomsof major depression.77 Fatigue can also be aggravated byother cancer- or treatment-related symptoms. In a group ofbreast cancer survivors, fatigue was significantly correlatedwith dyspnoea, insufficient sleep and depression, with these three variables accounting for a total of 46% of vari-ance in fatigue.78
Many drugs with sedative properties regularly used inpalliative care such as opioid analgesics, benzodiazepines,anti-depressants or anti-convulsants can add to the fatigueload.
As with cancer, fatigue and sleep disturbances havemultiple causes in most patients with HIV infection andAIDS.30 Increased levels of IL-1 and TNF from HIV infec-tion may lead to sleep disturbances and fatigue (reviewedin79). Anti-viral treatment with cytokines may boost fatiguedramatically.80–83 Anaemia,84 dysregulation of growthhormone85 or hypothyroidism86 have also been implicated inthe pathophysiology of fatigue with HIV.
Whereas some work has been done on the pathophysiol-ogy of cardiac cachexia,87 only little research is available onthe pathophysiology of fatigue in patients with cardiac fail-ure. Cachexia-related loss of skeletal muscle may contributeto fatigue in these patients. Reduced muscle strength andendurance has been linked to changes in histology andmetabolism in patients with chronic heart failure.88 Thesechanges seem to be related to imbalances of anabolic andcatabolic factors. The cause of this shift is not clear, but maybe due to continuous haemodynamic stress from decreasedperipheral perfusion. Fatigue may be aggravated by theergoreflex from metabolic stimulation of ergoreceptors in themuscle, causing increased ventilation and sympatheticactivation after exercise.
Fatigue in chronic progressive disease has also beendescribed as part of the cytokine-induced sickness behaviourtogether with other symptoms such as loss of appetite,sleepiness, fever and aching joints.89 This seems to be aphysiological adaptive response reorganizing priorities tofacilitate recovery from an infection. Chronic sicknessbehaviour from inappropriate prolonged activation of theimmune system may offer an explanation for chronic fatiguein a wide range of chronic diseases, ranging fromAlzheimer’s disease to stroke.
Assessment of fatigueA physical and cognitive dimension seem to be acknowl-edged by all authors.Weakness seems to be useful as a paraphrase for the physi-cal dimension and tiredness for the cognitive dimension.Screening for fatigue should include questions on weaknessand tiredness such as ‘Do you feel unusually tired or weak?’or ‘How weak are you?’ / ‘How tired are you?’
Multidimensional specific questionnaires should be usedfor research projects on fatigue.
Assessment of fatigue should depend on subjective self-evaluation by the patient, substituted by estimations of carersor medical staff only where self-assessment is not possible.As with the definition of fatigue, various approaches toassessment have been proposed. Fatigue may be regarded asa single symptom, as a symptom cluster or as a clinicalsyndrome. For the single-symptom approach, single itemscales (‘do you get tired for no reason?’) have beenproposed. For the symptom cluster approach, checklists andquestionnaires with multiple dimensions have been validated(review in,90 Table 3). Using the clinical syndrome approachthe physician has to assess fatigue with a checklist followingthe definition of the ICD-10.
Many instruments have been constructed for the symptomcluster approach. Some of these instruments are rather longsuch as the Functional Assessment of Cancer Therapy –Fatigue (FACT-F)91 with 47 items (although the 13-itemfatigue subscale can be used as a stand-alone questionnaire).The Piper fatigue inventory has recently been shortened to22 items.92 The Multidimensional fatigue inventory wasconstructed with 20 items.93 Some instruments such as thefatigue subscale of the FACT do not cover the differentdimensions of fatigue. The brief fatigue inventory (BFI) wasconstructed in a similar fashion to the brief pain inventory. It assesses severity and impairment from fatigue using only9 questions. However, the BFI taps only a single dimensiondescribed as ‘severity’ of fatigue.45 The EORTC QLQ-C30includes a subscale on fatigue with three items.48 TheEORTC and FACT quality of life questionnaires and the BFIare available in many languages.
Although there is no generally accepted definition offatigue, it is widely recognized as a multidimensionalconstruct. Glaus described physical, cognitive and affectivedimensions of cancer-related fatigue.94,95 Other authors have
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

216 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
156
20 L Radbruch et al.
described interference with function, vigour, mood, reducedactivity, reduced motivation or distress from fatigue asadditional dimensions of cancer-related fatigue, usually inconnection with the development of assessment instruments(Table 3).
A physical and a cognitive dimension seem to beacknowledged by all authors. Weakness seems to be usefulas a paraphrase for the physical dimension and tiredness forthe cognitive dimension.
However, semantic problems impede the discussion aboutdefinitions and assessment tools. Fatigue is inherent only inthe English and French languages, but not in other Europeantongues (Table 4).
In all European countries, fatigue has been used fre-quently in oncology research and assessment of fatigue hasbeen introduced in many oncology trials. However, it is notclear how much explanation about fatigue patients receiveand whether the concept of fatigue is understood by patientswith native languages other than English or French. Even ifthe oncology or palliative care specialist has adequate under-standing of fatigue, he may not be able to transfer thisknowledge and understanding to a patient who is not famil-iar with the concept. Patients not included in oncologicalresearch will only rarely learn of fatigue.
Translation of fatigue into other languages where the termis not commonly used is not without pitfalls. Glaus et al.stated that for German-speaking patients, fatigue would betranslated with ‘Ermüdung’ or ‘Ermüdbarkeit’, whereas‘Müdigkeit’ would rather be equivalent with tiredness.39
Other European languages may have similar problems withtranslation.
Even with adequate care in translation, equivalent wordsin other languages may not always cover the different dimen-sions of fatigue. Care has to be taken that the translatedquestionnaire covers the same dimensions as the originalversions. Patients in a German validation study clearlyrelated fatigue more with cognitive and affective areas thanwith physical exhaustion and cut-off points for worst fatiguediffered in the German and English versions of the BFI.50 Itshould be assumed that translation of fatigue into otherlanguages will find similar differences and problems.
The expert group recommends a differentiated assessmentof fatigue depending on the setting. Screening for fatigue innonspecialized settings such as oncology departments orgeneral practice should be done with single-item questionssuch as ‘Do you feel unusually tired or weak?’.
Screening in specialized services such as palliative careunits should include questions on weakness and tiredness asthe two main dimensions of fatigue at initial assessment andon regular follow-up. Documentation systems such as themodified Edmonton symptom assessment score96 or theminimal documentation system97 that include weakness andtiredness are recommended for routine use in specializedservices. Patients with high scores (severe weakness/tiredness, NRS � 5) should receive special attention, to
detect reversible causes of fatigue or to identify distressassociated with perceived fatigue. If fatigue is a priority syn-drome for care, they may be asked to complete a standardizedmultidimensional questionnaire or (preferably) be interviewedto assess the areas and scope of impairment.
Research projects on fatigue should follow a moredetailed approach. Specific questionnaires such as the BFI orthe anaemia and fatigue subscale of the FACT should becompleted at study entry, before and after interventions andat study completion.
Cognitive impairment may prevent self-assessment withstandardized questionnaires. Patients with mild cognitiveimpairment will be able to self-assess fatigue on simplecategorical scales, but patients with moderate or severeimpairment may not be able to do so. The expert grouprecommends assessment of fatigue by carers or staff in thesepatients, taking into account that carers tend to overestimateand staff tend to underestimate fatigue severity.
Children also may not be able to self-assess fatigue withstandardized scales or questionnaires. As with pain assess-ment, school children and adolescents usually will be able touse the same fatigue assessment instruments as adults, butsmaller children will lack the ability for abstract thinkingrequired for the assessment scales. No instruments have beendeveloped for assessment of fatigue in children yet. Theexpert group recommends assessment by parents or by staffin these children, using behavioural observations such aschanges of the sleep-wake times, frequent dozing, continu-ous lack of interest or concentration difficulties.
The cognitive dimension of fatigue may be tested withpsychomotor tests such as finger tapping or more complexmethods such as the battery used for assessment of drivingability.98 However, these tests will only have limited value ina palliative care setting, as cognitive or physical impairmentwill prevent participation of the vast majority of patients insuch tests.
Trying to assess the physical dimension of fatigue withobjective measures, for example with an ergometer, has beenwithout much success in patients with advanced cancer.However, newer electronic physical activity meters arecurrently being evaluated in clinical trials. Using devices thatrecord postural changes and other aspects of physicalactivity, information about the activity level of patients in apalliative care setting may be obtained. This may signify thebeginning of a change from subjective self-assessment of thepatient to more complex assessment using subjective assess-ment of impairment together with objective information onphysical and cognitive activity.
Treatment of fatigueSecondary causes for fatigue should be treated causally ifpossible. Causal treatment of primary fatigue with anti-cytokine or anti-inflammatory pharmacological approachesis under investigation although is currently lacking bothpromising results and a favourable risk-benefit relationship.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 217 217Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
157
Fatigue in palliative care patients 21
Tab
le 3
Ass
essm
ent
inst
rum
ents
for
fat
igue
in p
allia
tive
care
Inst
rum
ent
Item
sE
xam
ple
Sca
les
EO
RTC
QLQ
C30
V2.
0176
Thirt
y ite
ms,
Did
you
nee
d to
res
t?Fo
ur-s
tep
VR
S:
Tran
slat
ed a
nd v
alid
ated
am
ong
them
thr
ee q
uest
ions
H
ave
you
felt
wea
k?no
t at
all,
a li
ttle
,in
man
y la
ngua
ges
on f
atig
ueW
ere
you
tired
?qu
ite a
bit,
ver
y m
uch
FAC
T –
An
and
F91
Thirt
een
item
s (F
AC
T-F)
,I f
eel f
atig
ued
Five
-ste
p N
RS
:Tr
ansl
ated
and
val
idat
ed
Sev
en it
ems
(FA
CT-
An)
,I f
eel w
eak
all o
ver
0, n
ot a
t al
l; 4,
ver
y m
uch
in m
any
lang
uage
sus
ed t
oget
her
with
the
27
I am
fru
stra
ted
with
bei
ng t
oo
item
s of
the
FA
CT-
Gtir
ed t
o do
the
thi
ngs
I wan
t to
do
Pip
er f
atig
ue s
cale
92Tw
enty
-sev
en it
ems,
To w
hat
degr
ee is
the
fat
igue
A
djec
tive
wor
ding
sca
les
(22
item
s),
Onl
y in
Eng
lish
lang
uage
beha
viou
ral/s
ever
ity (s
ix it
ems)
,th
at y
ou a
re f
eelin
g no
w c
ausi
ng
open
que
stio
ns (fi
ve it
ems)
affe
ctiv
e m
eani
ng (fi
ve it
ems)
,yo
u di
stre
ss?
To w
hat
degr
ee
sens
ory
(five
item
s),
are
you
now
fee
ling
livel
y/lis
tless
?co
gniti
ve/m
ood
(six
item
s),
five
addi
tiona
l ite
ms
BFI
45Te
n ite
ms,
Hav
e yo
u fe
lt un
usua
lly t
ired
orE
leve
n-st
ep N
RS
:E
nglis
h, G
erm
an a
nd
inte
nsity
(thr
ee it
ems)
,fa
tigue
d in
the
last
wee
k? (y
es, n
o0,
no
fatig
ue, 1
0, a
s ba
d Ja
pane
se la
ngua
ges,
impa
irmen
t (s
ix it
ems)
Ple
ase
rate
you
r fa
tigue
as y
ou c
an im
agin
eot
her
tran
slat
ions
in t
he
(wea
rines
s, t
iredn
ess)
by
circ
ling
proc
ess
of v
alid
atio
nth
e on
e nu
mbe
r th
at b
est
desc
ribes
you
r fa
tigue
rig
ht n
ow.
Fatig
ue s
ympt
om in
vent
ory1
77,1
78Th
irtee
n ite
ms,
Rat
e th
e le
vel o
f fa
tigue
on
the
day
Ele
ven-
step
NR
S:
Eng
lish
and
Ital
ian
vers
ions
inte
nsity
(fou
r ite
ms)
, dur
atio
n yo
u fe
lt m
ost
fatig
ued
durin
g th
e 0,
not
at
all f
atig
ued;
10,
as
(tw
o ite
ms)
: int
erfe
renc
e w
ith
past
wee
k fa
tigue
d as
I co
uld
befu
nctio
nal s
tatu
s (s
even
item
s)R
ate
how
muc
h, in
the
pas
t w
eek,
fatig
ue in
terf
ered
with
you
rge
nera
l lev
el o
f ac
tivity
Mul
tidim
ensi
onal
fat
igue
E
ight
y-th
ree
item
s, s
hort
for
m
I fee
l slu
ggis
hFi
ve-s
tep
VR
S:
Eng
lish,
Est
onia
n, F
inni
sh,
sym
ptom
inve
ntor
y179
with
30
item
s (c
urre
ntly
tes
ted)
,M
y ar
ms
feel
wea
kno
t at
all,
a li
ttle
, mod
erat
ely,
Fren
ch f
or C
anad
a, H
ebre
w a
nd
gene
ral d
imen
sion
(six
item
s),
I fee
l ten
sequ
ite a
bit,
ext
rem
ely
Lith
uani
an la
ngua
ge v
ersi
ons
phys
ical
dim
ensi
on (s
ix it
ems)
,em
otio
nal d
imen
sion
(six
item
s)m
enta
l dim
ensi
on (s
ix it
ems)
vigo
ur (s
ix it
ems)
Mul
tidim
ensi
onal
Tw
enty
item
s,I f
eel fi
t P
hysi
cally
, S
even
-ste
p Li
cker
t S
cale
:E
nglis
h, D
utch
, Fre
nch,
Ger
man
, fa
tigue
inve
ntor
y93
gene
ral f
atig
ue,
I fee
l onl
y ab
le t
o do
a li
ttle
1, y
es t
hat
is t
rue;
7, n
o,D
anis
h an
d S
wed
ish
phys
ical
fat
igue
,I f
eel v
ery
activ
eth
at is
not
tru
ela
ngua
ge v
ersi
ons
redu
ced
activ
ity,
redu
ced
mot
ivat
ion,
men
tal f
atig
ueFa
tigue
ass
essm
ent
Twen
ty-t
hree
item
s,D
id y
ou e
xper
ienc
e w
eakn
ess,
Fo
ur-s
tep
VR
S: n
ot a
t al
l, a
little
,E
nglis
h an
d G
erm
an la
ngua
ge
ques
tionn
aire
95in
tens
ity (t
hree
item
s),
loss
of
stre
ngth
? qu
ite a
bit,
ver
y m
uch
VAS
for
vers
ions
phys
ical
dim
ensi
on (1
1 ite
ms)
,D
id y
ou e
xper
ienc
e in
tens
ity: I
did
not
fee
l unu
sual
lyaf
fect
ive
dim
ensi
on (fi
ve it
ems)
diffi
culti
es in
con
cent
ratin
g?tir
ed a
t al
l – I
felt
extr
emel
y co
gniti
ve d
imen
sion
(thr
ee it
ems)
Did
you
fee
l sad
?tir
ed, e
xhau
sted
slee
ping
pro
blem
s (s
ingl
e ite
m)
‘I ge
t tir
ed f
or n
o re
ason
’180
Sin
gle
item
I get
tire
d fo
r no
rea
son
Four
-ste
p V
RS
(non
e or
a li
ttle
of
the
Eng
lish
lang
uage
onl
ytim
e to
mos
t or
all
of t
he t
ime)
Rho
ten
fatig
ue s
cale
181
Sin
gle
item
Ten-
poin
t N
RS
((0,
not
tire
d, p
eppy
; 10
, tot
al e
xhau
stio
n)
VR
S�
Verb
al r
atin
g sc
ale
NR
S�
Num
eric
al r
atin
g sc
ale
VAS
�Vi
sual
ana
logu
e sc
ale
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from
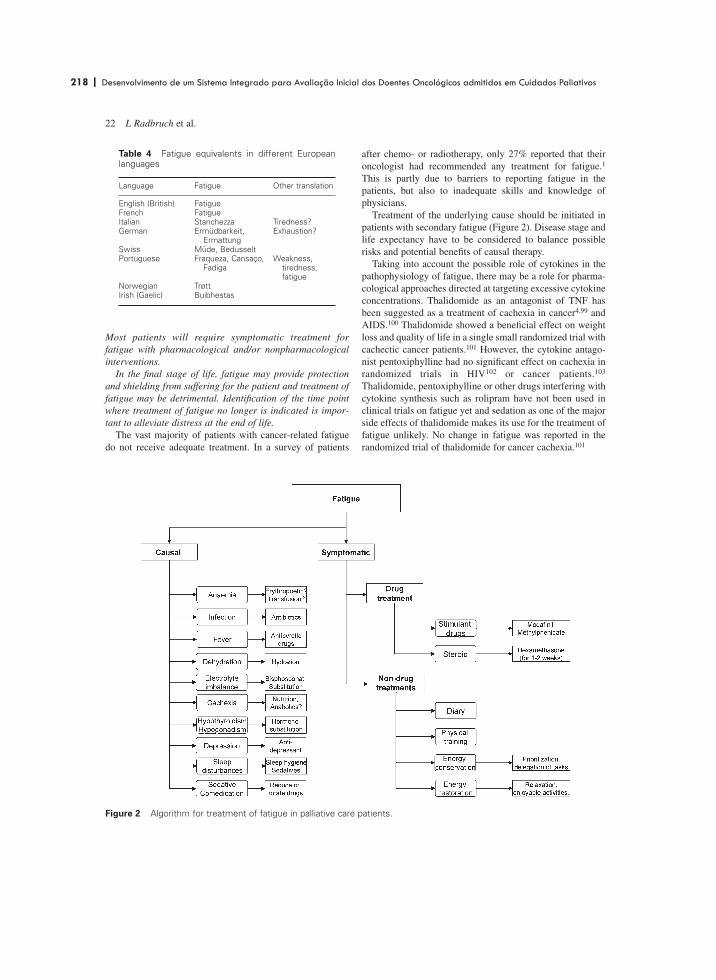
218 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
158
22 L Radbruch et al.
Most patients will require symptomatic treatment for fatigue with pharmacological and/or nonpharmacologicalinterventions.
In the final stage of life, fatigue may provide protectionand shielding from suffering for the patient and treatment offatigue may be detrimental. Identification of the time pointwhere treatment of fatigue no longer is indicated is impor-tant to alleviate distress at the end of life.
The vast majority of patients with cancer-related fatiguedo not receive adequate treatment. In a survey of patients
after chemo- or radiotherapy, only 27% reported that theironcologist had recommended any treatment for fatigue.1
This is partly due to barriers to reporting fatigue in thepatients, but also to inadequate skills and knowledge ofphysicians.
Treatment of the underlying cause should be initiated inpatients with secondary fatigue (Figure 2). Disease stage andlife expectancy have to be considered to balance possiblerisks and potential benefits of causal therapy.
Taking into account the possible role of cytokines in thepathophysiology of fatigue, there may be a role for pharma-cological approaches directed at targeting excessive cytokineconcentrations. Thalidomide as an antagonist of TNF hasbeen suggested as a treatment of cachexia in cancer4,99 andAIDS.100 Thalidomide showed a beneficial effect on weightloss and quality of life in a single small randomized trial withcachectic cancer patients.101 However, the cytokine antago-nist pentoxiphylline had no significant effect on cachexia inrandomized trials in HIV102 or cancer patients.103
Thalidomide, pentoxiphylline or other drugs interfering withcytokine synthesis such as rolipram have not been used inclinical trials on fatigue yet and sedation as one of the majorside effects of thalidomide makes its use for the treatment offatigue unlikely. No change in fatigue was reported in therandomized trial of thalidomide for cancer cachexia.101
Table 4 Fatigue equivalents in different Europeanlanguages
Language Fatigue Other translation
English (British) FatigueFrench FatigueItalian Stanchezza Tiredness?German Ermüdbarkeit, Exhaustion?
ErmattungSwiss Müde, BedusseltPortuguese Fraqueza, Cansaço, Weakness,
Fadiga tiredness, fatigue
Norwegian TrøttIrish (Gaelic) Buibhestas
Figure 2 Algorithm for treatment of fatigue in palliative care patients.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 219 219Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
159
Fatigue in palliative care patients 23
For most patients, causal treatment of primary or second-ary fatigue will not be effective enough or will take too long.For these patients, symptomatic treatment should beconsidered. Symptomatic treatment should comprisepharmacological and nonpharmacological interventions.
The expert group discussed the need for treatment withrespect to the stage of the patients’ illness. It should be keptin mind that in the terminal stage of life fatigue might beconsidered a ‘normal’ response, protecting and shielding thepatient from suffering and facilitating the transfer from lifeto death. In the final hours and days of life, effective treat-ment of fatigue could produce a cruel relapse into the fulldramatic experience of the disease when sedation, weaknessand emotional deprivation are reduced. Identifying the timepoint where vigorous treatment of fatigue is no longerindicated is important to alleviate distress at the end of life.
Treatment of secondary fatigueTreatment of anaemia with erythropoetic agents effectivelyincreases haemoglobin levels, thereby alleviating fatigue, butusually life expectancy is too short in palliative care patientsto pursue this option.The efficacy of treatments for cachexia, depression, fluid orelectrolyte imbalances, fever or infection on fatigue have notbeen investigated, but should be considered in patients withfatigue related to these underlying causes.
Some causes of secondary fatigue such as anaemia,depression, infection, dehydration, malnutrition, hypercal-caemia, hypomagnesiaemia or treatment with opioids orother sedative drugs can be treated and effective causaltreatment should alleviate fatigue.
The treatment of anaemia with erythropoetic agents suchas erythropoetin or darbepoetin alfa has been a recent focusof interest in oncology. Fatigue has been named as thepredominant symptom of anaemia and treatment with ery-thropoetic agents has been specifically directed to alleviatecancer- and treatment-related fatigue.104 Randomized trialswith darbepoetin71 and erythropoetin7,105 have consistentlyshown reduced levels of fatigue with increasing haemoglo-bin concentrations. Other reviews have confirmed theefficacy of erythropoetic agents.6,106 Treatment of anaemia isrecommended for cancer patients with haemoglobin levelsbelow 12 g/dL.107 However, treatment with erythropoetinwill take up to 12 weeks to take effect and many patients inpalliative care will not have a life expectancy to match this.Considering also the high costs of erythropoetin treatmentand potential complications such as thrombosis or pure redcell aplasia, it is not surprising that palliative care physiciansseem to make little use of erythropoetic agents.
There was consensus in the expert group that bloodtransfusions may also increase haemoglobin levels effec-tively, and may be indicated for palliative care patients withfatigue related to anaemia. The effects of blood transfusionsare short-term and transfusions often have to be repeated,sometimes several times per week. Potential transfusion
complications, financial and resource burden, all conspire tomake routine transfusion unsuitable as a first-line treatmentapproach. However, in selected patients repeated bloodtransfusions may have a role in management.
As with blood transfusions, no clinical trials are availablefor treatment of other secondary causes of fatigue, eventhough published guidelines stress the importance of causaltherapy wherever possible.74,108
The use of antibiotics has sometimes been consideredcontroversial in palliative care. In such patients, infectiondoes not always lead to antibiotic therapy. Some palliativecare programs will not support the use of antibiotics in theirpatients, whereas others use them with the aim of symptomcontrol. The expert group stated that treatment of fever orinfections with antipyretic or antibiotic drugs may beindicated to treat fatigue-related impairment.
The cachexia-anorexia syndrome (CAS) has been investi-gated intensively in recent years. However, effectivetreatment strategies are still scarce. Increasing the caloricintake alone does not seem to improve CAS. Nutritionalsupplementation with anti-inflammatory polyunsaturatedfatty acid or eicosapentanoic acid seems to be beneficial inpreclinical and phase II trials (review in109). However, threerecent randomized trials failed to prove a beneficial effect inpatients with CAS.110–112 Megestrol acetate was shown toimprove appetite compared with placebo in several random-ized trials113–115 and compared with dronabinol in onetrial.116 In some of these studies there was also an improve-ment in quality of life. However, three randomized trialsfailed to find any benefit for fatigue.115,117,118
Cyproheptadine, hydrazine sulfate and cannabinoids haveall been suggested as treatments for anorexia but clinicaltrials have found no benefit for appetite or energy levels(review in119,120). Corticosteroids have been shown toincrease appetite and daily activity in a randomized trial inadvanced cancer patients but with no effect on subjectivefatigue.121 After prolonged treatment with corticosteroids,insulin resistance (aggravating cachexia), proximal myopathy(causing muscle weakness) and increased risk for infections(and cytokine activity) may aggravate fatigue.
Recent data from animal trials have suggested the beta2-agonists clenbuterol and formoterol as potential therapeutictools for the CAS, probably via an inhibitory effect on theATP-ubiquitin-dependent proteolytic system of skeletalmuscles.122 Prostaglandin inhibitors such as celecoxib alsoseem to reverse wasting in the animal model123 and clinicaltrials are ongoing. However, the benefit of these drugs onfatigue has not been investigated yet.
As discussed above, there is considerable overlap betweendepression and fatigue in patients with advanced cancer andtreatment with anti-depressants may alleviate fatigue in cancerpatients with major depression. However, in a randomizedcontrolled trial, paroxetine did not lead to a reduction offatigue in patients with breast cancer receiving chemotherapy,even though depression was reduced significantly compared
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

220 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
160
24 L Radbruch et al.
to placebo.124 Sedation may be a side effect of anti-depressanttherapy, counteracting any potential effects on fatigue.
Other causes of fatigue such as hypothyroidism, dehydra-tion, electrolyte imbalances (eg, hypercalcaemia or hypo-magnesemia) or other metabolic disorders should also betreated even though little evidence from randomized trials isavailable on the efficacy of these treatments. In a randomizedtrial, comparing 1000 versus 100 ml saline subcutaneously,there was no significant difference in improvement of fatiguebetween the groups.125
Symptomatic nonpharmacological treatmentAerobic exercise effectively alleviates fatigue in patientsreceiving cancer treatment.Other nonpharmacological interventions have been investi-gated less thoroughly. Strategies on energy conservation andrestoration may be useful and counselling for thesestrategies should be offered.
Nonpharmacological treatment options include provisionof information, keeping a diary, energy expenditure planningand physical exercise. Most patients will try to counteractexhaustion and fatigue with prolonged periods of rest.126
This may even be augmented by healthcare professionals. Ina British survey, the most common advice on fatigue was totake more rest and relaxation.127 However, rest often will notrestore energy and persistent reduction of physical activitymay even promote fatigue. Counselling on coping strategiesshould be an effective intervention in these patients.
The effect of physical exercise for cancer patients hasbeen investigated in many clinical trials. Several reviews andmeta-analyses have accumulated strong evidence that aero-bic exercise will reduce fatigue levels in cancer survivors andpatients receiving cancer treatment.128,129 Recent studiessupport the use of resistance training or ‘anabolic’ exer-cise.130 However, most trials have been done in patients withbreast cancer and good performance status. Only little infor-mation is available on patients with far advanced disease andimpaired performance status. A 50-min group exercise pro-gram twice a week for six weeks reduced fatigue in cancerpatients with short life expectancy.131 The expert groupstates that these patients are likely to benefit from exercisetraining, but that training has to be adapted to reducedperformance status, for example sessions with sitting up atthe bedside several times per day might be consideredadequate training for a bedridden patient.
Other nonpharmacological interventions have beeninvestigated less thoroughly. A sleep intervention has beeninvestigated in patients with breast cancer. Using an individ-ualized sleep promotion plan with four components: sleephygiene, relaxation therapy, stimulus control and sleeprestriction techniques patients were able to maintain normalsleep and manage fatigue during chemotherapy.132
Other recommendations from guidelines on fatigue havebeen the keeping of a diary on daily activities and fatigueand counselling for energy conservation principles. Energy
conservation should include planning of daily activities withprioritizing of activities. Patients should learn to do the mostimportant things when their individual energy levels arehighest and delegate less important tasks to others.11,37,74
This should be supported by energy restoration strategiessuch as ensuring adequate rest and nutrition, reducing stressthrough meditation or relaxation and participating inenjoyable activities.
Other nonpharmacological interventions have been usedfor the treatment of fatigue in patients receiving cancer treat-ment. Clinical trials on the use of aromatherapy and mas-sage,133 psychotherapy,134 relaxation therapy135 or participationin support groups136,137 have been published. Even whenthese trials did show some effect on fatigue, it is not clearwhether this can be extended to the palliative care setting.
Complex multidimensional intervention programmes maybe beneficial compared to more restricted approaches. Anintervention designed to minimize or prevent attentionalfatigue through regular participation in activities that engagefascination was shown to be effective in two small controlledtrials after breast cancer surgery.138,139 In patients undergoingautologous blood stem cell transplantation, a comprehensivecoping strategy programme with counselling, education,written material, an audio tape providing information andinstruction in guided imagery and relaxation proved effectivecompared to the control group.140 In a randomized study anintervention consisting of an information pack, a fatiguediary and monthly coaching from support nurses who visitedpatients at home was found to be more effective than theusual support.141 In another recent paper patients participat-ing in a programme with physical exercise, relaxation andbody awareness training and massage reported significantrelief of fatigue.142 However, training comprised 9 h perweek for six weeks and the feasibility of such programmesin advanced cancer must be questioned. Only a minority ofpalliative care patients will be able and willing to spend somuch time on a training programme. No studies have beenpublished on the efficacy of training programmes for patientswith advanced cancer and impairment of physical andcognitive function.
Symptomatic pharmacological treatmentTreatment with methylphenidate (investigated predominantlyin opioid-induced sedation and cancer-related fatigue) andmodafinil (in advanced neurological diseases and AIDS)may reduce fatigue.The efficacy of other stimulant drugs such as pemoline ordonepezil as well as the efficacy of corticosteroids on fatiguehave been less well investigated.
Research on symptomatic treatment of fatigue in pallia-tive care patients has concentrated on stimulant drugs suchas methylphenidate, modafinil, pemoline and donazepil.Although there is evidence from randomized trials on someof these drugs, the routine use of these drugs in palliativecare patients was considered controversial in the expert
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 221 221Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
161
Fatigue in palliative care patients 25
group. Reluctance to recommend the routine use of stimulantdrugs in fatigued patients partly came from the evaluation ofavailable evidence as being too poor, and partly fromdifferences about the concept of fatigue that might not besusceptible to pharmacological treatment.
Methylphenidate is an amphetamine derivate. It acts byenhancing monoaminergic transmitters in the synaptic gap,either by blocking uptake of dopamine or by facilitatingcatecholamine release.143 Methylphenidate has been shownto improve cognitive function in patients receiving continu-ous opioid infusions.144 Methylphenidate has a rather lowbioavailability (11–52%) and a short half-life of ~2 h. Aftermetabolization in the liver the inactive metabolites areexcreted renally.
Methylphenidate has been approved for the treatment ofdepression and of attention-deficit disorder, but is notavailable in all European countries. Its usefulness for thetreatment of depression in palliative care has beendescribed,145,146 as a fast onset of anti-depressant activity isrequired for patients with restricted life expectancy.
Methylphenidate has been reported to be effective in sev-eral trials for the treatment of opioid-induced sedation147–149
and for fatigue in advanced cancer patients.9,150,151
Methylphenidate and exercise both reduced fatigue,increased functional ability and stabilized cognitive functionin melanoma patients undergoing interferon treatment,whereas cognitive function deteriorated in the exercise-onlygroup.152 However, a recent placebo-controlled trial chal-lenged these positive results, as methylphenidate andplacebo both improved fatigue with no significant advantageof methylphenidate.153 Similarly, donepezil was not superiorto placebo in a recent randomized trial.154 With regard to thehigh placebo response rate, it may be important to identifycancer patients who will benefit from methylphenidate orother drugs more than from other treatment options.
Less information is available on fatigue in noncancerdiseases. Methylphenidate and pemoline were effective in thetreatment of fatigue in patients with AIDS, with 41%responding to methylphenidate and 36% responding to pemo-line compared with a 15% response rate with placebo.155 In areport on a patient with myotonic dystrophy, methylphenidateimproved daytime sleepiness and cognitive impairment.156
No difference was reported comparing methylphenidate andplacebo in elderly patients with fatigue.157
Treatment with methylphenidate usually is initiated with5–10 mg in the morning. With monitoring of response andside effects, the dose may be titrated up to 40–60 mg per daydistributed into morning and midday doses. In a recent reportpatient-controlled oral titration with 5 mg methylphenidateevery 2 h as needed showed fast relief of fatigue and otherparameters in advanced cancer patients,10 however, this wasnot reproduced in a subsequent placebo-controlled trial.153
Side effects may be dose limiting and include nervousness,jitteriness, agitation and sometimes cardiac side effects suchas arrhythmia and tachycardia.
Modafinil acts via the inhibition of GABA, therebypromoting the release of excitatory neurotransmitters such asdopamine, norepinephrine and serotonin in the sleep-wakeregulation centres of the central nervous system.158,159
Modafinil is a racemat with a half-life of ~15 h after multipledosing. After metabolization in the liver, the inactivemetabolites are excreted renally. Modafinil was approved bythe FDA in 1998 for the treatment of daytime sleepiness in patients with narcolepsy. In Europe modafinil is releasedfor the same indication.
Modafinil has been used in trials for treatment of fatiguein advanced neurological diseases such as multiplesclerosis,160–162 amyotrophic lateral sclerosis,163 myotonicdystrophy164 Parkinson’s diseases165 and in patients withAIDS/HIV.166 Modafinil also reduced opioid-inducedsedation in a retrospective survey.167 No direct comparisonof modafinil and methylphenidate is available. Only fourstudies were randomized and blinded.161,162,164,165 One ofthese studies did not show any difference against placebo inthe relief of fatigue in multiple sclerosis162 and another onefailed to improve daytime somnolence in Parkinson’sdisease.165 However, some evidence seems to point towardsmodafinil as a treatment option for fatigue in palliative care.Studies with modafinil against cancer-related fatigue arecurrently under way.
A starting dose of 200 mg per day is recommended formodafinil. In some patients titration to effect will be requiredwith dosages up to 400 mg. In older patients or patients withimpaired liver function a lower starting dose of 100 mgshould be used. Major side effects can be agitation,nervousness, sleep disturbances, nausea or diarrhoea.
Pemoline acts via the same mechanism as methylphenidate,increasing the amount of monoaminergic transmitters in thesynaptic gap. Pemoline was as effective as methylphenidate in the treatment of fatigue in patients with AIDS and was superior to placebo.155 However, potential liver toxicity haslimited the use of pemoline.
Donepezil is a centrally acting acetylcholinesteraseinhibitor, approved for symptomatic treatment of Alzheimer’sdisease. Opioid-induced sedation may be related to func-tional deficits of acetylcholine and preliminary studies withdonepezil have suggested at least short-term benefit inpatients treated with opioids.168 Donezepil also was effectivefor treatment of opioid-induced sedation in an uncontrolledtrial.169 A prolonged elimination half-life of 70 h or more and a high plasma protein binding of 96% may make its useproblematic in palliative care patients.
Amantadine, a central acting drug with effects oncholinergic, dopaminergic, adrenergic and glutamatergicneurotransmission has been used for treatment of fatigue inmultiple sclerosis in several older, small, placebo-controlledstudies, showing modest but significant benefits of this drug(reviewed in170).
Anecdotal observation and very limited data fromcontrolled trials support the use of low-dose corticosteroids
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

222 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
162
26 L Radbruch et al.
in fatigued patients with advanced disease and multiplesymptoms.74 In a randomized trial in patients with advancedcancer, methylprednisolone 32 mg resulted not only inincreased appetite, but also in improved daily activity in 21 of 31 patients.121 Low-dose prednisone in daily doses up to 10 mg led to improvement in several quality-of-lifedimensions in patients with bone metastases from prostatecancer.171 Other randomized trials found no significantbenefit on strength172 and no or only transient improvementof weakness.173,174 Fatigue was not a primary outcomeparameter in these studies and the evidence on the impact ofsteroids on fatigue is still pending. However, the expertgroup agreed that the experience in clinical practice is thatsteroids such as methylprednisolone or dexamethasone areeffective in relieving fatigue for a short period of time, usu-ally one or two weeks and that they may be used to alleviatefatigue for well-defined goals, for example allowing thepatient to spend a holiday or Christmas time with his family.
Research agenda on fatigueResearch into the underlying pathophysiology of the fatiguesyndrome and suitable animal models is paramount as pre-requisites for translational clinical research. Basic researchshould aim for the identification of central and peripheralmechanisms of fatigue in cancer and other diseases.Basic and clinical research should extend from cancer-related fatigue to fatigue in other patients in the palliativecare setting, for example patients with amyotrophic lateralsclerosis or geriatric patients.
A major drawback of the research on fatigue in palliativecare is the lack of suitable animal models for fatigue.38
A model of motivated motor activity has been developed,where mice are trained to run on a wheel voluntarily forextended periods of time. Once trained, the effect of inter-ventions can be monitored.175 However, compared with thewealth of different animal models in pain research, wherestudies can be tailored to the pathophysiology of the painsyndrome, a lack of similar models has hampered researchon fatigue considerably.
Basic research is required to clarify the role of cytokinesand of neurotransmitters in the sleep-wake cycle, and toidentify central and peripheral mechanisms of fatigue incancer and other diseases. Research is also needed on thesimilarities and discrepancies between fatigue in palliativecare and CFS, major depression or cachexia.
Considering that excessive cytokine production is a possi-ble cause of fatigue in cancer patients, it stands to reason thatdrugs interfering with cytokine synthesis (eg, pentoxi-phylline, rolipram and thalidomide) or TNF-antibodies (eg,etanercep and infliximab) or antibodies against othercytokines (eg, anti-IL-6) may become effective treatmentoptions (reviewed for use in cancer-related anorexia andcachexia in4). The efficacy of these agents for cancer-relatedfatigue is currently being investigated in clinical trials, butpreliminary results challenge the potential of these drugs as
general remedies for fatigue. Future research with thesedrugs may focus on the efficacy in selected patient groups inpalliative care.
Most research on cancer-related fatigue has been donein cancer survivors or patients undergoing chemo- orradiotherapy. Little evidence is available on the efficacy ofinterventions in the palliative care setting. Interventions suchas physical or cognitive training programmes may not besuitable for palliative care patients. For treatment of fatiguein palliative care patients’ available interventions should beadapted and specific interventions developed taking intoaccount the limited resources of these patients. There is aneed for clinical trials on the efficacy of these interventionsin patients with advanced cancer.
Whereas a wealth of information has been published on thetreatment of cancer-related fatigue, only limited research hasbeen undertaken on fatigue in advanced cancer patients or innoncancer palliative care patients. As with the pathophysiol-ogy of fatigue, specific efforts should be directed towards theinvestigation of interventions for treatment of fatigue in thesegroups. This will be even more important considering theincreasing percentage of noncancer patients requiring andreceiving palliative care in many countries. There will bespecific research questions in this area, for example, to whatextent diminished energy levels and decreasing physical andcognitive resources might be deemed normal with old ageand whether a threshold can be identified where fatigue in theelderly requires assessment and treatment.
Conclusions
This paper of the expert working group of the EAPC hasdiscussed the definition of fatigue and collated the availableevidence on assessment and treatment.
Most management strategies have been developed for thetreatment of fatigue in survivors or for the treatment offatigue arising as a side effect of cancer treatment. Transferof these approaches into clinical palliative care practice isparamount. It is likely that some adaptation to thesetreatment options might provide relief of fatigue in palliativecare patients.
Research on fatigue should focus on the evaluation of theefficacy of available treatment options in the palliative caresetting. In addition basic research is needed on the patho-physiology of fatigue, with the aim of identifying new causaland symptomatic approaches to the treatment of fatigue inpalliative care.
However, one of the major strengths of palliative care isthe consideration of the individual preferences and needs ofthe patient. This has to be applied to the assessment andtreatment of fatigue as to any other symptom in palliativecare. The severity and impact of fatigue may change in thecourse of the disease trajectory. Following guidelines blindly
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 223 223Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
163
Fatigue in palliative care patients 27
without consideration may not only be without benefit, butmay adversely affect patients. For most patients discontinu-ation of fatigue treatment in the final stage of life should bediscussed. In the terminal stages fatigue may be consideredan acceptable final common path, shielding and protectingthe patient from what otherwise might be overwhelmingemotional and physical distress.
Balancing the impact of fatigue and the advantages anddisadvantages of fatigue treatment in the individual situationis an important skill for palliative care specialists and shouldreceive adequate attention in training and clinical practice.Treating fatigue vigorously in those patients who benefit andwithdrawing or withholding assessment and treatmentprocedures from those patients who do not benefit willprovide optimal care for the large number of palliative carepatients with fatigue.
AcknowledgementsThe Research Steering Committee of the EuropeanAssociation consists of Franco De Conno (Chair), AugustoCaraceni, Nathan Cherny, Carl Johan Fürst, Jose Ferraz-Gonçalves, Geoffrey Hanks, Stein Kaasa, SebastianoMercadante, Juan Manuel Nunez Olarte, Lukas Radbruch,Carla Ripamonti, Friedrich Stiefel and Florian Strasser. Theauthors would like to thank Jose Pereira for his engagementand support of the expert’s work.
The meeting of the expert group was supported by anunrestricted educational grant from the Grünenthal company.
References
1 Vogelzang NJ, Breitbart W, Cella D et al. Patient, caregiver,and oncologist perceptions of cancer-related fatigue: resultsof a tripart assessment survey. The fatigue coalition. SeminHematol 1997; 34: 4–12.
2 Passik SD, Kirsh KL, Donaghy K et al. Patient-relatedbarriers to fatigue communication. Initial validation of thefatigue management barriers questionnaire. J Pain SymptomManage 2002; 24: 481–93.
3 Wood LJ, Nail LM, Gilster A, Winters KA, Elsea CR.Cancer chemotherapy-related symptoms: evidence tosuggest a role for proinflammatory cytokines. Oncol NursForum 2006; 33: 535–42.
4 Argiles JM, Busquets S, Lopez-Soriano FJ. The pivotal roleof cytokines in muscle wasting during cancer. Int J BiochemCell Biol 2005; 37: 2036–46.
5 Muscaritoli M, Bossola M, Aversa Z, Bellantone R, RossiFanelli F. Prevention and treatment of cancer cachexia: newinsights into an old problem. Eur J Cancer 2006; 42:31–41.
6 Cella D, Dobrez D, Glaspy J. Control of cancer-relatedanemia with erythropoietic agents: a review of evidence forimproved quality of life and clinical outcomes. Ann Oncol2003; 14: 511–9.
7 Crawford J. Recombinant human erythropoietin in cancer-related anemia. Review of clinical evidence. Oncology(Huntingt) 2002; 16: 41–53.
8 Patrick DL, Ferketich SL, Frame PS et al. National insti-tutes of health state-of-the-science conference statement:symptom management in cancer: pain, depression, andfatigue, 15–17 July 2002. J Natl Cancer Inst Monogr 2004;32: 9–16.
9 Hanna A, Sledge G, Mayer ML et al. A phase II study ofmethylphenidate for the treatment of fatigue. Support CareCancer 2006; 14: 210–5.
10 Bruera E, Driver L, Barnes EA et al. Patient-controlledmethylphenidate for the management of fatigue in patientswith advanced cancer: a preliminary report. J Clin Oncol2003; 21: 4439–43.
11 Lawrence DP, Kupelnick B, Miller K, Devine D, Lau J.Evidence report on the occurrence, assessment, and treat-ment of fatigue in cancer patients. J Natl Cancer InstMonogr 2004; 32: 40–50.
12 Stasi R, Abriani L, Beccaglia P, Terzoli E, Amadori S.Cancer-related fatigue: evolving concepts in evaluation andtreatment. Cancer 2003; 98: 1786–801.
13 Escalante CP. Treatment of cancer-related fatigue: anupdate. Support Care Cancer 2003; 11: 79–83.
14 Lesage P, Portenoy RK. Management of fatigue in thecancer patient. Oncology (Williston Park) 2002; 16: 373–8,381, discussion 381–2, 385–6, 388–9.
15 Barnes EA, Bruera E. Fatigue in patients with advancedcancer: a review. Int J Gynecol Cancer 2002; 12: 424–8.
16 Stone P. The measurement, causes and effective manage-ment of cancer-related fatigue. Int J Palliat Nurs 2002; 8:120–8.
17 Tavio M, Milan I, Tirelli U. Cancer-related fatigue (review).Int J Oncol 2002; 21: 1093–9.
18 National Comprehensive Cancer Network. Cancer relatedfatigue. Retrieved 28 November 2006, from http://www.nccn.org/professionals/physician_gls/PDF/fatigue.pdf
19 Walsh D, Donnelly S, Rybicki L. The symptoms ofadvanced cancer: relationship to age, gender, and perform-ance status in 1,000 patients. Support Care Cancer 2000; 8:175–9.
20 Servaes P, Verhagen C, Bleijenberg G. Fatigue in cancerpatients during and after treatment: prevalence, correlatesand interventions. Eur J Cancer 2002; 38: 27–43.
21 Wolfe J, Grier HE, Klar N et al. Symptoms and suffering atthe end of life in children with cancer. N Engl J Med 2000;342: 326–33.
22 Curt GA, Breitbart W, Cella D et al. Impact of cancer-related fatigue on the lives of patients: new findings fromthe fatigue coalition. Oncologist 2000; 5: 353–60.
23 National Multiple Sclerosis Society. Management of MS-related fatigue. Retrieved 17 November 2005, fromhttp://www.nationalmssociety.org/PRC.asp
24 Bakshi R. Fatigue associated with multiple sclerosis:diagnosis, impact and management. Mult Scler 2003; 9:219–27.
25 Krupp LB. Fatigue in multiple sclerosis: definition, patho-physiology and treatment. CNS Drugs 2003; 17: 225–34.
26 Elkington H, White P, Addington-Hall J, Higgs R, Edmonds P.The healthcare needs of chronic obstructive pulmonary
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

224 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
164
28 L Radbruch et al.
disease patients in the last year of life. Palliat Med 2005; 19:485–91.
27 Goodlin SJ. Palliative care for end-stage heart failure. CurrHeart Fail Rep 2005; 2: 155–60.
28 Breitbart W, McDonald MV, Rosenfeld B, Monkman ND,Passik S. Fatigue in ambulatory AIDS patients. J PainSymptom Manage 1998; 15: 159–67.
29 Norval DA. Symptoms and sites of pain experienced byAIDS patients. S Afr Med J 2004; 94: 450–4.
30 Adinolfi A. Assessment and treatment of HIV-related fatigue. J Assoc Nurses AIDS Care 2001; 12(Supp): 29–34, (quiz 35–8).
31 Glaus A, Crow R, Hammond S. Fatigue in healthy and can-cer patients. 1. A qualitative study on conceptual analysis.Pflege 1999; 12: 11–9.
32 Cella D, Davis K, Breitbart W, Curt G. Cancer-relatedfatigue: prevalence of proposed diagnostic criteria in aUnited States sample of cancer survivors. J Clin Oncol2001; 19: 3385–91.
33 Clauw DJ, Chrousos GP. Chronic pain and fatigue syn-dromes: overlapping clinical and neuroendocrine features andpotential pathogenic mechanisms. Neuroimmunomodulation1997; 4: 134–53.
34 Cella D, Peterman A, Passik S, Jacobsen P, Breitbart W.Progress toward guidelines for the management of fatigue.Oncology (Huntingt) 1998; 12: 369–77.
35 Fernandes R, Stone P, Andrews P, Morgan R, Sharma S.Comparison between fatigue, sleep disturbance, and circa-dian rhythm in cancer inpatients and healthy volunteers:evaluation of diagnostic criteria for cancer-related fatigue. J Pain Symptom Manage 2006; 32: 245–54.
36 Murphy H, Alexander S, Stone P. Investigation of diagnosticcriteria for cancer-related fatigue syndrome in patients withadvanced cancer: a feasibility study. Palliat Med 2006; 20:413–8.
37 Mock V, Atkinson A, Barsevick A et al. NCCN practiceguidelines for cancer-related fatigue. Oncology (Huntingt)2000; 14: 151–61.
38 Gutstein HB. The biologic basis of fatigue. Cancer 2001;92: 1678–83.
39 Glaus A, Crow R, Hammond S. A qualitative study to explorethe concept of fatigue/tiredness in cancer patients and inhealthy individuals. Support Care Cancer 1996; 4: 82–96.
40 Poulson MJ. Not just tired. J Clin Oncol 2001; 19: 4180–1.41 Kroenke K, Wood DR, Mangelsdorff AD, Meier NJ,
Powell JB. Chronic fatigue in primary care: prevalencepatient characteristics and outcome. J Am Med Assoc 1988;260: 929–34.
42 David A, Pelosi A, McDonald E et al. Tired, weak, or inneed of rest: fatigue among general practice attenders. BMJ1990; 301: 1199–202.
43 Pawlikowska T, Chalder T, Hirsch SR, Wallace P, Wright DJ,Wessely SC. Population based study of fatigue andpsychological distress. BMJ 1994; 308: 763–6.
44 Stone P, Richards M, A’Hern R, Hardy J. A study to investi-gate the prevalence, severity and correlates of fatigue amongpatients with cancer in comparison with a control group ofvolunteers without cancer. Ann Oncol 2000; 11: 561–7.
45 Mendoza TR, Wang XS, Cleeland CS et al. The rapidassessment of fatigue severity in cancer patients: use of theBrief Fatigue Inventory. Cancer 1999; 85: 1186–96.
46 Neuenschwander H, Bruera E. Astenia. In: Doyle D, Hanks G,MacDonald RN eds. Oxford textbook of palliative medicine,second edition. Oxford: Oxford University Press; 1998:573–81.
47 Olson K. A new way of thinking about fatigue: a reconcep-tualization. Oncol Nurs Forum 2007; 34: 93–99.
48 Aaronson NK, Ahmedzai S, Bergman B et al. The Europeanorganization for research and treatment of cancer QLQ-C30: a quality-of-life instrument for use in internationalclinical trials in oncology. J Natl Cancer Inst 1993; 85:365–76.
49 Osoba D, Aaronson N, Zee B, Sprangers M, te Velde A.Modification of the EORTC QLQ-C30 (version 2.0) basedon content validity and reliability testing in large samples ofpatients with cancer. The study group on quality of life ofthe eortc and the symptom control and quality of life com-mittees of the NCI of Canada clinical trials group. Qual LifeRes 1997; 6: 103–8.
50 Radbruch L, Sabatowski R, Elsner F, Everts J, Mendoza T,Cleeland C. Validation of the German version of the brieffatigue inventory. J Pain Symptom Manage 2003; 25: 449–58.
51 Jacobsen PB, Donovan KA, Weitzner MA. Distinguishingfatigue and depression in patients with cancer. Semin ClinNeuropsychiatry 2003; 8: 229–40.
52 Stewart GD, Skipworth RJ, Fearon KC. Cancer cachexiaand fatigue. Clin Med 2006; 6: 140–3.
53 Miaskowski C, Dodd M, Lee K. Symptom clusters: the newfrontier in symptom management research. J Natl CancerInst Monogr 2004; 32: 17–21.
54 Dodd MJ, Miaskowski C, Lee KA. Occurrence of symptomclusters. J Natl Cancer Inst Monogr 2004; 32: 76–8.
55 Yennurajalingam S, Bruera E. Palliative management offatigue at the close of life: ‘it feels like my body is just wornout’. JAMA 2007; 297: 295–304.
56 Schubert C, Hong S, Natarajan L, Mills PJ, Dimsdale JE.The association between fatigue and inflammatory markerlevels in cancer patients: A quantitative review. Brain BehavImmun 2007; 21: 413–27.
57 Meyers CA, Albitar M, Estey E. Cognitive impairment,fatigue, and cytokine levels in patients with acute myeloge-nous leukemia or myelodysplastic syndrome. Cancer 2005;104: 788–93.
58 Greenberg DB, Gray JL, Mannix CM, Eisenthal S, Carey M.Treatment-related fatigue and serum interleukin-1 levels inpatients during external beam irradiation for prostate cancer.J Pain Symptom Manage 1993; 8: 196–200.
59 Ahlberg K, Ekman T, Gaston-Johansson F. Levels of fatiguecompared to levels of cytokines and hemoglobin duringpelvic radiotherapy: a pilot study. Biol Res Nurs 2004; 5:203–10.
60 Bower JE, Ganz PA, Aziz N, Fahey JL. Fatigue and proin-flammatory cytokine activity in breast cancer survivors.Psychosom Med 2002; 64: 604–11.
61 Knobel H, Loge JH, Nordoy T et al. High level of fatigue inlymphoma patients treated with high dose therapy. J PainSymptom Manage 2000; 19: 446–56.
62 Mills PJ, Parker B, Dimsdale JE, Sadler GR, Ancoli-IsraelS. The relationship between fatigue and quality of life andinflammation during anthracycline-based chemotherapy inbreast cancer. Biol Psychol 2005; 69: 85–96.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 225 225Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
165
Fatigue in palliative care patients 29
63 Morrow GR, Andrews PL, Hickok JT, Roscoe JA, MattesonS. Fatigue associated with cancer and its treatment. SupportCare Cancer 2002; 10: 389–98.
64 Agteresch HJ, Dagnelie PC, van der Gaast A, Stijnen T,Wilson JH. Randomized clinical trial of adenosine 5’-triphosphate in patients with advanced non-small-celllung cancer. J Natl Cancer Inst 2000; 92: 321–8.
65 Davis MP, Ranganathan VK, Walsh D et al. Cancer relatedfatigue: central or peripheral. MASCC, Geneva, 2004.
66 Bower JE, Ganz PA, Dickerson SS, Petersen L, Aziz N,Fahey JL. Diurnal cortisol rhythm and fatigue in breast can-cer survivors. Psychoneuroendocrinology 2005; 30: 92–100.
67 Bower JE, Ganz PA, Aziz N. Altered cortisol response topsychologic stress in breast cancer survivors with persistentfatigue. Psychosom Med 2005; 67: 277–80.
68 Kurzrock R. The role of cytokines in cancer-related fatigue.Cancer 2001; 92: 1684–8.
69 Tisdale MJ. Loss of skeletal muscle in cancer: biochemicalmechanisms. Front Biosci 2001; 6: D164–74.
70 Strasser F. Pathophysiology of the anorexia/cachexiasyndrome. In Doyle D, Hanks G, Cherny NI, Calman K eds.Oxford textbook of palliative medicine. Oxford: OxfordUniversity Press, 2004: 520–33.
71 Cella D, Kallich J, McDermott A, Xu X. The longitudinalrelationship of hemoglobin, fatigue and quality of life inanemic cancer patients: results from five randomizedclinical trials. Ann Oncol 2004; 15: 979–86.
72 Stone PC, Abdul-Wahab A, Gibson JS, Wright RJ, AndrewsPL. Fatigue in cancer patients is not related to changes inoxyhaemoglobin dissociation. Support Care Cancer 2005;13: 854–8.
73 Strasser F, Palmer JL, Schover LR et al. The impact ofhypogonadism and autonomic dysfunction on fatigue,emotional function, and sexual desire in male patients withadvanced cancer: a pilot study. Cancer 2006; 107: 2949–57.
74 Portenoy RK, Itri LM. Cancer-related fatigue: guidelines forevaluation and management. Oncologist 1999; 4: 1–10.
75 Schrag D, Chung KY, Flombaum C, Saltz L. Cetuximabtherapy and symptomatic hypomagnesemia. J Natl CancerInst 2005; 97: 1221–4.
76 Fakih MG, Wilding G, Lombardo J. Cetuximab-inducedhypomagnesemia in patients with colorectal cancer. ClinColorectal Cancer 2006; 6: 152–6.
77 Visser MR, Smets EM. Fatigue, depression and quality oflife in cancer patients: how are they related? Support CareCancer 1998; 6: 101–8.
78 Okuyama T, Akechi T, Kugaya A et al. Factors correlatedwith fatigue in disease-free breast cancer patients: applica-tion of the Cancer Fatigue Scale. Support Care Cancer2000; 8: 215–22.
79 Darko DF, Mitler MM, Henriksen SJ. Lentiviral infection,immune response peptides and sleep. Adv Neuroimmunol1995; 5: 57–77.
80 Riddell LA, Pinching AJ, Hill S et al. A phase III study ofrecombinant human interferon gamma to prevent oppor-tunistic infections in advanced HIV disease. AIDS Res HumRetroviruses 2001; 17: 789–97.
81 Goldstein D, Hertzog P, Tomkinson E et al. Administrationof imiquimod, an interferon inducer, in asymptomatic humanimmunodeficiency virus-infected persons to determine
safety and biologic response modification. J Infect Dis1998; 178: 858–61.
82 Grady C, Anderson R, Chase GA. Fatigue in HIV-infectedmen receiving investigational interleukin-2. Nurs Res 1998;47: 227–34.
83 Kovacs JA, Vogel S, Albert JM et al. Controlled trial ofinterleukin-2 infusions in patients infected with the humanimmunodeficiency virus. N Engl J Med 1996; 335: 1350–6.
84 Moyle G. Anaemia in persons with HIV infection: prog-nostic marker and contributor to morbidity. AIDS Rev2002; 4: 13–20.
85 Darko DF, Mitler MM, Miller JC. Growth hormone,fatigue, poor sleep, and disability in HIV infection.Neuroendocrinology 1998; 67: 317–24.
86 Derry DM. Thyroid therapy in HIV-infected patients. MedHypotheses 1995; 45: 121–4.
87 Anker SD, Steinborn W, Strassburg S. Cardiac cachexia.Ann Med 2004; 36: 518–29.
88 Clark AL. Origin of symptoms in chronic heart failure.Heart 2006; 92: 12–6.
89 Dantzer R, Kelley KW. Twenty years of research oncytokine-induced sickness behavior. Brain Behav Immun2007; 21: 153–60.
90 Dittner AJ, Wessely SC, Brown RG. The assessment offatigue: a practical guide for clinicians and researchers. J Psychosom Res 2004; 56: 157–70.
91 Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E.Measuring fatigue and other anemia-related symptomswith the Functional Assessment of Cancer Therapy(FACT) measurement system. J Pain Symptom Manage1997; 13: 63–74.
92 Piper BF, Dibble SL, Dodd MJ, Weiss MC, Slaughter RE,Paul SM. The revised Piper Fatigue Scale: psychometricevaluation in women with breast cancer. Oncol NursForum 1998; 25: 677–84.
93 Smets EM, Garssen B, Bonke B, De Haes JC. The multi-dimensional fatigue inventory (MFI) psychometric quali-ties of an instrument to assess fatigue. J Psychosom Res1995; 39: 315–25.
94 Glaus A, Crow R, Hammond S. Fatigue in the healthy andin cancer patients. II. A qualitative study for conceptualanalysis. Pflege 1999; 12: 75–81.
95 Glaus A. Fatigue in patients with cancer. Analysis andassessment. Recent Results Cancer Res 1998; 145: I–XI,1–172.
96 Philip J, Smith WB, Craft P, Lickiss N. Concurrent valid-ity of the modified edmonton symptom assessment systemwith the rotterdam symptom checklist and the brief paininventory. Support Care Cancer 1998; 6: 539–41.
97 Radbruch L, Sabatowski R, Loick G, Jonen-Thielemann I,Elsner F, Hörmann E. MIDOS – Validierung eines mini-malen Dokumentationssystems für die Palliativmedizin.Schmerz 2000; 14: 231–39.
98 Sabatowski R, Schwalen S, Rettig K, Herberg KW, KasperSM, Radbruch L. Driving ability under long-term treat-ment with transdermal fentanyl. J Pain Symptom Manage2003; 25: 38–47.
99 Fanelli M, Sarmiento R, Gattuso D et al. Thalidomide: anew anticancer drug? Expert Opin Investig Drugs 2003;12: 1211–25.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

226 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
166
30 L Radbruch et al.
100 Smith D. Thalidomide and HIV: several possible uses.AIDS Treat News 1995: 1–4.
101 Gordon JN, Trebble TM, Ellis RD, Duncan HD, Johns T,Goggin PM. Thalidomide in the treatment of cancercachexia: a randomised placebo controlled trial. Gut 2005;54: 540–5.
102 Goldberg RM, Loprinzi CL, Mailliard JA et al.Pentoxifylline for treatment of cancer anorexia andcachexia? A randomized, double-blind, placebo-controlledtrial. J Clin Oncol 1995; 13: 2856–9.
103 Kruse A, Rieneck K, Kappel M et al. Pentoxifylline ther-apy in HIV seropositive subjects with elevated TNF.Immunopharmacology 1995; 31: 85–91.
104 Cella D. The effects of anemia and anemia treatment onthe quality of life of people with cancer. Oncology(Huntingt) 2002; 16: 125–32.
105 Itri LM. Managing cancer-related anaemia with epoetinalfa. Nephrol Dial Transplant 2002; 17(Supp 1): 73–7.
106 Jones M, Schenkel B, Just J, Fallowfield L. Epoetin alfaimproves quality of life in patients with cancer: results ofmetaanalysis. Cancer 2004; 101: 1720–32.
107 Rodgers GM III, Cella D, Chanan-Khan A et al. Cancer-and treatment-related anemia. J Natl Compr Canc Netw2005; 3: 772–89.
108 National Comprehensive Cancer Network. Cancer relatedfatigue. Retrieved 15 May 2005, from http://www.nccn.org/professionals/physician_gls/PDF/fatigue.pdf
109 Argiles JM. Cancer-associated malnutrition. Eur J OncolNurs 2005; 9(Supp 2): S39–50.
110 Jatoi A, Rowland K, Loprinzi CL et al. An eicosapen-taenoic acid supplement versus megestrol acetate versusboth for patients with cancer-associated wasting: a NorthCentral Cancer Treatment Group and National CancerInstitute of Canada collaborative effort. J Clin Oncol 2004;22: 2469–76.
111 Fearon KC, Barber MD, Moses AG et al. Double-blind,placebo-controlled, randomized study of eicosapentaenoicacid diester in patients with cancer cachexia. J Clin Oncol2006; 24: 3401–7.
112 Fearon KC, Von Meyenfeldt MF, Moses AG et al. Effect ofa protein and energy dense N-3 fatty acid enriched oralsupplement on loss of weight and lean tissue in cancercachexia: a randomised double blind trial. Gut 2003; 52:1479–86.
113 Bruera E, Ernst S, Hagen N et al. Effectiveness of mege-strol acetate in patients with advanced cancer: a random-ized, double-blind, crossover study. Cancer Prev Control1998; 2: 74–8.
114 Bruera E, Macmillan K, Kuehn N, Hanson J, MacDonaldRN. A controlled trial of megestrol acetate on appetite,caloric intake, nutritional status, and other symptoms inpatients with advanced cancer. Cancer 1990; 66: 1279–82.
115 De Conno F, Martini C, Zecca E et al. Megestrol acetatefor anorexia in patients with far-advanced cancer: a dou-ble-blind controlled clinical trial. Eur J Cancer 1998; 34:1705–9.
116 Jatoi A, Windschitl HE, Loprinzi CL et al. Dronabinolversus megestrol acetate versus combination therapy forcancer-associated anorexia: a North Central CancerTreatment Group study. J Clin Oncol 2002; 20: 567–73.
117 Simons JP, Aaronson NK, Vansteenkiste JF et al. Effects ofmedroxyprogesterone acetate on appetite, weight, andquality of life in advanced-stage non-hormone-sensitivecancer: a placebo-controlled multicenter study. J ClinOncol 1996; 14: 1077–84.
118 Westman G, Bergman B, Albertsson M et al. Megestrolacetate in advanced, progressive, hormone-insensitivecancer. Effects on the quality of life: a placebo-controlled,randomised, multicentre trial. Eur J Cancer 1999; 35:586–95.
119 Bruera E. Clinical management of anorexia and cachexiain patients with advanced cancer. Oncology 1992; 49(Supp2): 35–42.
120 Davis MP, Dreicer R, Walsh D, Lagman R, LeGrand SB.Appetite and cancer-associated anorexia: a review. J ClinOncol 2004; 22: 1510–7.
121 Bruera E, Roca E, Cedaro L, Carraro S, Chacon R. Actionof oral methylprednisolone in terminal cancer patients: aprospective randomized double-blind study. Cancer TreatRep 1985; 69: 751–4.
122 Busquets S, Figueras MT, Fuster G et al. Anticachecticeffects of formoterol: a drug for potential treatment ofmuscle wasting. Cancer Res 2004; 64: 6725–31.
123 Davis TW, Zweifel BS, O’Neal JM et al. Inhibition ofcyclooxygenase-2 by celecoxib reverses tumor-inducedwasting. J Pharmacol Exp Ther 2004; 308: 929–34.
124 Roscoe JA, Morrow GR, Hickok JT et al. Effect of parox-etine hydrochloride (Paxil) on fatigue and depression inbreast cancer patients receiving chemotherapy. BreastCancer Res Treat 2005; 89: 243–9.
125 Bruera E, Sala R, Rico MA et al. Effects of parenteralhydration in terminally ill cancer patients: a preliminarystudy. J Clin Oncol 2005; 23: 2366–71.
126 Richardson A, Ream EK. Self-care behaviours initiated bychemotherapy patients in response to fatigue. Int J NursStud 1997; 34: 35–43.
127 Stone P, Ream E, Richardson A et al. Cancer-related fatigue – a difference of opinion? Results of a multicentresurvey of healthcare professionals, patients and caregivers.Eur J Cancer Care (Engl) 2003; 12: 20–7.
128 Schmitz KH, Holtzman J, Courneya KS, Masse LC, DuvalS, Kane R. Controlled physical activity trials in cancersurvivors: a systematic review and meta-analysis. CancerEpidemiol Biomarkers Prev 2005; 14: 1588–95.
129 Mock V. Evidence-based treatment for cancer-relatedfatigue. J Natl Cancer Inst Monogr 2004: 32: 112–8.
130 Galvao DA, Newton RU. Review of exercise interventionstudies in cancer patients. J Clin Oncol 2005; 23: 899–909.
131 Oldervoll LM, Loge JH, Paltiel H et al. The effect of aphysical exercise program in palliative care: A phase IIstudy. J Pain Symptom Manage 2006; 31: 421–30.
132 Berger AM, VonEssen S, Khun BR et al. Feasibilty of asleep intervention during adjuvant breast cancerchemotherapy. Oncol Nurs Forum 2002; 29: 1431–41.
133 Fellowes D, Barnes K, Wilkinson S. Aromatherapy andmassage for symptom relief in patients with cancer.Cochrane Database Syst Rev 2004; 2: CD002287.
134 Forester B, Kornfeld DS, Fleiss JL. Psychotherapy duringradiotherapy: effects on emotional and physical distress.Am J Psychiatry 1985; 142: 22–7.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 227 227Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
167
Fatigue in palliative care patients 31
135 Decker TW, Cline-Elsen J, Gallagher M. Relaxation ther-apy as an adjunct in radiation oncology. J Clin Psychol1992; 48: 388–93.
136 Spiegel D, Bloom JR, Yalom ID. Group support formetastatic cancer paitents: a randomized prospectiveoutcome study. Arch Gen Psychiatry 1981; 38: 527–33.
137 Spiegel D, Bloom JR. Group therapy and hypnosis reducemetastatic breast carcinoma pain. Psychosom Med 1983;45: 333–9.
138 Cimprich B. Development of an intervention to restoreattention in cancer patients. Cancer Nurs 1993; 16: 83–92.
139 Cimprich B, Ronis DL. An environmental intervention torestore attention in women with newly diagnosed breastcancer. Cancer Nurs 2003; 26: 284–92 (quiz 293–4).
140 Gaston-Johansson F, Fall-Dickson JM, Nanda J et al. Theeffectiveness of the comprehensive coping strategy pro-gram on clinical outcomes in breast cancer autologous bonemarrow transplantation. Cancer Nurs 2000; 23: 277–85.
141 Ream E, Richardson A, Alexander-Dann C. Supportiveintervention for fatigue in patients undergoing chemother-apy: a randomized controlled trial. J Pain SymptomManage 2006; 31: 148–61.
142 Adamsen L, Quist M, Midtgaard J et al. The effect of a mul-tidimensional exercise intervention on physical capacity,well-being and quality of life in cancer patients undergoingchemotherapy. Support Care Cancer 2006; 14: 116–27.
143 Homsi J, Walsh D, Nelson KA. Psychostimulants insupportive care. Support Care Cancer 2000; 8: 385–97.
144 Bruera E, Miller MJ, Macmillan K, Kuehn N.Neuropsychological effects of methylphenidate in patientsreceiving a continuous infusion of narcotics for cancerpain. Pain 1992; 48: 163–6.
145 Homsi J, Walsh D, Nelson KA, LeGrand S, Davis M.Methylphenidate for depression in hospice practice: a caseseries. Am J Hosp Palliat Care 2000; 17: 393–8.
146 Homsi J, Nelson KA, Sarhill N et al. A phase II study ofmethylphenidate for depression in advanced cancer. Am J Hosp Palliat Care 2001; 18: 403–7.
147 Bruera E, Chadwick S, Brenneis C, Hanson J, MacDonaldRN. Methylphenidate associated with narcotics for the treat-ment of cancer pain. Cancer Treat Rep 1987; 71: 67–70.
148 Bruera E, Fainsinger R, MacEachern T, Hanson J. The useof methylphenidate in patients with incident cancer painreceiving regular opiates. A preliminary report. Pain 1992;50: 75–7.
149 Wilwerding MB, Loprinzi CL, Mailliard JA et al. Arandomized, crossover evaluation of methylphenidate incancer patients receiving strong narcotics. Support CareCancer 1995; 3: 135–8.
150 Sugawara Y, Akechi T, Shima Y et al. Efficacy ofmethylphenidate for fatigue in advanced cancer patients: apreliminary study. Palliat Med 2002; 16: 261–3.
151 Sarhill N, Walsh D, Nelson KA, Homsi J, LeGrand S,Davis MP. Methylphenidate for fatigue in advanced can-cer: a prospective open-label pilot study. Am J Hosp PalliatCare 2001; 18: 187–92.
152 Schwartz AL, Thompson JA, Masood N. Interferon-induced fatigue in patients with melanoma: a pilot study ofexercise and methylphenidate. Oncol Nurs Forum 2002;29: E85–90.
153 Bruera E, Valero V, Driver L et al. Patient-controlledmethylphenidate for cancer fatigue: a double-blind,randomized, placebo-controlled trial. J Clin Oncol 2006;24: 2073–8.
154 Bruera E, El Osta B, Valero V et al. Donepezil for cancerfatigue: a double-blind, randomized, placebo-controlledtrial. J Clin Oncol 2007; 25: 3475–81.
155 Breitbart W, Rosenfeld B, Kaim M, Funesti-Esch J. Arandomized, double-blind, placebo-controlled trial of psy-chostimulants for the treatment of fatigue in ambulatorypatients with human immunodeficiency virus disease. ArchIntern Med 2001; 161: 411–20.
156 Miyamoto T, Miyamoto M, Suga T, Aizawa C, TakekawaH, Hirata K. Methylphenidate hydrochloride for excessivedaytime sleepiness in a patient with myotonic dystrophy.Psychiatry Clin Neurosci 2002; 56: 271–2.
157 Larsson M, Ervik M, Lundborg P, Sundh V, Svanborg A.Comparison between methylphenidate and placebo asadjuvant in care and rehabilitation of geriatric patients.Compr Gerontol [A] 1988; 2: 53–9.
158 Ferraro L, Antonelli T, O’Connor WT, Tanganelli S,Rambert FA, Fuxe K. Modafinil: an antinarcoleptic drugwith a different neurochemical profile to d-amphetamineand dopamine uptake blockers. Biol Psychiatry 1997; 42:1181–3.
159 Ferraro L, Antonelli T, Tanganelli S et al. The vigilancepromoting drug modafinil increases extracellular gluta-mate levels in the medial preoptic area and the posteriorhypothalamus of the conscious rat: prevention by localGABAA receptor blockade. Neuropsychopharmacology1999; 20: 346–56.
160 Zifko UA, Rupp M, Schwarz S, Zipko HT, Maida EM.Modafinil in treatment of fatigue in multiple sclerosis.Results of an open-label study. J Neurol 2002; 249: 983–7.
161 Rammohan KW, Rosenberg JH, Lynn DJ, BlumenfeldAM, Pollak CP, Nagaraja HN. Efficacy and safety ofmodafinil (provigil) for the treatment of fatigue in multiplesclerosis: a two centre phase 2 study. J Neurol NeurosurgPsychiatry 2002; 72: 179–83.
162 Stankoff B, Waubant E, Confavreux C et al. Modafinil forfatigue in MS: a randomized placebo-controlled double-blind study. Neurology 2005; 64: 1139–43.
163 Carter GT, Weiss MD, Lou JS et al. Modafinil to treatfatigue in amyotrophic lateral sclerosis: an open label pilotstudy. Am J Hosp Palliat Care 2005; 22: 55–9.
164 MacDonald JR, Hill JD, Tarnopolsky MA. Modafinil reducesexcessive somnolence and enhances mood in patients withmyotonic dystrophy. Neurology 2002; 59: 1876–80.
165 Ondo WG, Fayle R, Atassi F, Jankovic J. Modafinil fordaytime somnolence in Parkinson’s disease: double blind,placebo controlled parallel trial. J Neurol NeurosurgPsychiatry 2005; 76: 1636–9.
166 Rabkin JG, McElhiney MC, Rabkin R, Ferrando SJ.Modafinil treatment for fatigue in HIV� patients: a pilotstudy. J Clin Psychiatry 2004; 65: 1688–95.
167 Webster L, Andrews M, Stoddard G. Modafinil treatmentof opioid-induced sedation. Pain Med 2003; 4: 135–40.
168 Slatkin NE, Rhiner M. Treatment of opiate-related seda-tion: utility of the cholinesterase inhibitors. J SupportOncol 2003; 1: 53–63.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

228 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
168
169 Bruera E, Strasser F, Shen L, et al. The effect of donepezilon sedation and other symptoms in patients receivingopioids for cancer pain: a pilot study. J Pain SymptomManage 2003; 26: 1049–54.
170 Schwid SR, Murray TJ. Treating fatigue in patients withMS: one step forward, one step back. Neurology 2005; 64:1111–2.
171 Tannock I, Gospodarowicz M, Meakin W, Panzarella T,Stewart L, Rider W. Treatment of metastatic prostatic can-cer with low-dose prednisone: evaluation of pain and qual-ity of life as pragmatic indices of response. J Clin Oncol1989; 7: 590–7.
172 Moertel CG, Schutt AJ, Reitemeier RJ, Hahn RG.Corticosteroid therapy of preterminal gastrointestinalcancer. Cancer 1974; 33: 1607–9.
173 Popiela T, Lucchi R, Giongo F. Methylprednisolone aspalliative therapy for female terminal cancer patients. TheMethylprednisolone Female Preterminal Cancer StudyGroup. Eur J Cancer Clin Oncol 1989; 25: 1823–9.
174 Della Cuna GR, Pellegrini A, Piazzi M. Effect of methylprednisolone sodium succinate on quality of life inpreterminal cancer patients: a placebo-controlled, multi-center study. The Methylprednisolone Preterminal CancerStudy Group. Eur J Cancer Clin Oncol 1989; 25:1817–21.
175 Ottenweller JE, Natelson BH, Gause WC et al. Mouserunning activity is lowered by brucella abortus treatment:a potential model to study chronic fatigue. Physiol Behav1998; 63: 795–801.
176 Bjordal K, de Graeff A, Fayers PM et al. A 12 country fieldstudy of the EORTC QLQ-C30 (version 3.0) and the headand neck cancer specific module (EORTC QLQ-H&N35)in head and neck patients. EORTC Quality of Life Group.Eur J Cancer 2000; 36: 1796–807.
177 Hann DM, Jacobsen PB, Azzarello LM et al. Measurementof fatigue in cancer patients: development and validationof the fatigue symptom inventory. Qual Life Res 1998; 7:301–10.
178 Hann DM, Denniston MM, Baker F. Measurement offatigue in cancer patients: further validation of the FatigueSymptom Inventory. Qual Life Res 2000; 9: 847–54.
179 Stein KD, Martin SC, Hann DM, Jacobsen PB. A multidi-mensional measure of fatigue for use with cancer patients.Cancer Pract 1998; 6: 143–52.
180 Kirsh KL, Passik S, Holtsclaw E, Donaghy K, Theobald D.I get tired for no reason: a single item screening for cancer-related fatigue. J Pain Symptom Manage 2001; 22: 931–7.
181 Rhoten D. Fatigue and the postsurgical patient. In Norris Ced. Concept clarification in nursing. Rockville: AspenSystems, 1982: 277–300
32 L Radbruch et al.
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at IST Nazionale Tumori on January 24, 2008 http://pmj.sagepub.comDownloaded from

| 229 229Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
170
Letter to the Editor
The importance of a word:how to translate ‘breakthrough’
Portenoy and Hagen defined breakthrough pain as a‘transitory increase in pain to greater than moderateintensity, which occurred on a baseline pain of moderateintensity or less’.1 Although the term ‘breakthrough pain’includes a heterogeneous group of pains, it is widely usedand usually its meaning is well understood by palliativecare and pain specialists. However, there has been somedifficulty in finding a translation of breakthrough pain inother languages, such as the Latin languages.2 The term‘episodic pain’ was suggested to overcome that difficulty,2
but apparently it was not successful. Therefore, in thoselanguages there are other words or expressions being used.For example, some years ago, ‘dor incidental’ (incidentpain) was perhaps the term most commonly used to referto breakthrough pain in Portugal. But ‘incident pain’ isnot a good term for translating breakthrough pain,because this term refers to a subtype of breakthroughpain caused by an incident, such as a movement.1 In Ital-ian, there isn’t a single word in use that is equivalent tobreakthrough pain. One option in Italian is ‘dolore episo-dico intenso’ (Sebastiano Mercadante, personal e-mail),meaning ‘severe episodic pain’. In French, there is thesame problem and ‘accès douloureux paroxystique’ isoften used (Marilène Filbert, personal e-mail), meaning‘paroxysmal painful bout’. The same problem certainlyexists in other languages, both Latin and non-Latin ones.
Since the end of the nineties, I have been using the word‘irruptiva’ in Portuguese as a translation for breakthrough(‘dor irruptiva’ meaning breakthrough pain). In fact, thatword means to penetrate or appear suddenly,3 a meaningclose to breakthrough. Some time later in a meeting of theResearch Steering Committee of the European Associa-tion for Palliative Care, I mentioned this to the Spanishdoctor Juan Manuel Nuñez-Olarte, who also found thetranslation adequate and one that could be used in Span-ish, and so he enthusiastically adopted it. Rapidly theterm ‘dolor irruptivo’ spread among Spanish palliativecare physicians. Nowadays, the terms ‘dor irruptiva’ and‘dolor irruptivo’ are used in Portugal and Spain, respec-tively, by all doctors working in palliative care and paintherapy, probably without any knowledge of its source.
Other Latin and non-Latin languages contain wordssimilar to the Portuguese word ‘irruptiva’. However,those words may not be currently in use and are noteven included in all dictionaries, but they exist. For exam-ple, the Italian word ‘irruttivo’ and the French word‘irruptif’ have the same meaning as the Portuguese word‘irruptivo’. However, when I tried to look them up insome Internet dictionaries, I was unsuccessful. Probably,the same is true with other languages.
Although there may be some controversy regarding thedefinition of breakthrough pain and recognizing that theterm is an umbrella that covers a heterogeneous reality, itis well established through use, and all palliative and paindoctors use and understand it. It is somewhat similar tothe famous phrase, ‘though I cannot define an elephant, Ican recognize one when I see it’. Therefore, a single wordequivalent to breakthrough accepted in each languagecould be useful.
AcknowledgementThe author would like to thank the Portuguese LeagueAgainst Cancer for funding the translation of this letter.
José António Ferraz GonçalvesUnidade de Cuidados Paliativos – RedeInstituto Português de Oncologia,Rua Dr. António Bernardino de Almeida, 4200-072 Porto,PortugalEmail: [email protected] or [email protected]
References
1 Portenoy, RK, Hagen, NA. Breakthrough pain: defini-tion, prevalence and characteristics. Pain 1990; 41: 273–281.
2 Mercadante, S, Radbruch, L, Caraceni, A, et al. Episodic(breakthrough) pain: consensus conference of an expertworking group of the European Association for PalliativeCare. Cancer 2002; 94: 832–839.
3 Grande Dicionário da Língua Portuguesa. Lisboa: Publi-cações Alfa, S.A., 1991.
© 2008 SAGE Publications, Los Angeles, London, New Delhi and Singapore 10.1177/0269216307087141
Palliative Medicine 2008; 22: 195
© 2008 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. by José António Ferraz Gonçalves on March 27, 2008 http://pmj.sagepub.comDownloaded from

230 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 231 231Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
171
SUPPORTIVE CARE INTERNATIONAL
Use of chemotherapy at the end of life in a Portugueseoncology center
José Ferraz Gonçalves & Carmen Goyanes
Received: 19 February 2007 /Accepted: 11 July 2007 /Published online: 22 August 2007# Springer-Verlag 2007
AbstractGoals of work Chemotherapy plays a major role in thetreatment of cancer. However, it is sometimes thought of asbeing taken too far, being used in many cases close todeath. The purpose of this study is to determine theproximity of chemotherapy use to the patient’s death inour hospital.Materials and methods This study comprised the analysisof the charts of 1,064 patients aged over 16 years with solidtumors who died in 2002 and were treated at the PortoSection of the Portuguese Institute of Oncology.Main results Four hundred ten of the 1,064 patients (39%)underwent chemotherapy. Fifty-two percent of those thatunderwent chemotherapy did so in the last 6 months of theirlives, 31% in the last 3 months, 13% in the last month, and3% in the last week. In the context of the total cohort of1,064, the percentages of those that underwent chemother-apy was 20, 12, 5, and 1%, respectively. By multivariateanalysis, age <65 years, breast and lung cancers, andmetastases were positively associated with chemotherapy;kidney cancer and comorbidity were associated with alower probability of undergoing chemotherapy. Threehundred sixty-one patients (34%) were admitted to thepalliative care unit of the hospital.Conclusion It was concluded that in this hospital, chemo-therapy is not used as close to death as often as mostprofessionals feel and the literature reports. There arevarious possible explanations for this discrepancy; one ofthem may be the influence of health care systems. It would
be useful to see what is happening in other countries withdifferent health care systems.
Keywords Chemotherapy . Advanced cancer . End of life .
Symptom Control . Palliative care
Introduction
The evolution of chemotherapy as a method for cancertreatment, from the second half of the twentieth centuryonwards, provided an important improvement to thesurvival prospects of many patients. Its impact on the cureof not only mainly hematological cancer but also on somesolid tumors is very positive. As an adjuvant treatment ofsome cancers, such as breast and colorectal cancer, it alsohas an important positive influence on the survival of manypatients. Even when cure is an unattainable aim, it ispossible to usefully prolong the life of many patients withsome types of cancers that are responsive to chemotherapy.
However, there are a number of cancers for which theprobability of improvement is very small, such as pancreasor liver cancers and melanoma. The probability of aresponse drastically diminishes, even with usually chemo-responsive cancers, if patients have already been treatedwith chemotherapy, sometimes with a number of differentregimens.
Another problem is the toxicity of chemotherapy, whichcan be very important and even endanger the life of somepatients. Therefore, chemotherapy should be used judi-ciously when the probabilities of a successful outcome arereasonable because the cancer is responsive and the patientis fit enough. However, many patients see chemotherapy astheir only hope and insist on undergoing it despite theobjective data.
Support Care Cancer (2008) 16:321–327DOI 10.1007/s00520-007-0316-x
J. F. Gonçalves (*) :C. GoyanesDepartment of Medical Oncology,Portuguese Institute of Oncology,Rua Dr. António Bernardino de Almeida,Porto 4200-072, Portugale-mail: [email protected]
J. Ferraz Gonçalves (*) & C. Goyanes

232 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
172
Appropriately withdrawing or withholding chemothera-py in patients with advanced cancer does not meanabandoning them. Usually, those patients are in greaterneed of help than beforehand due to their multipleproblems, which are not only physical but also psycholog-ical, social, and existential. For them, palliative care may bethe best option.
There is the idea that chemotherapy is often prolongedmore than is desirable or beneficial to patients and that theyare not referred to palliative care as often and as soon asthey should be. However, there is only a small amount ofdata on this issue in medical literature and, as far as weknow, none concerning Portugal. As this is a very importantissue, a revision of the charts of all non-pediatric patientswith a solid tumor who had died during 2002 was done,with the primary aim being to ascertain the time intervalbetween the last chemotherapy procedure and death.
Materials and methods
The Porto section of the Portuguese Institute of Oncology isthe largest Portuguese oncological center. It is a publichospital that serves all of northern Portugal, with acatchment population of about 3 million people. About4,000 new patients are admitted every year. There are alsogeneral hospitals that treat cancer patients in that region.Often cancer patients that have been treated in otherhospital choose to be treated or are referred to this centerto undergo active antineoplastic treatments. However, theopposite is quite uncommon; patients treated at our hospitalare sometimes referred to other hospitals to be closer totheir families when they are near to the end of life but not toundergo aggressive treatments such as chemotherapy,radiotherapy, or surgery. This center includes a 20-bedpalliative care unit (PCU). As is usual in PCUs chemother-apy is not used as a method of palliation.
Using the hospital’s computer records, a list of patientsdiagnosed with a solid tumor that died in 2002 was made.Patients younger than 16 years who were treated by thepediatrics service were not included. The data collectedincluded demographic data, primary tumor, the extension ofthe disease, comorbidity, treatments, whether chemotherapywas given, when the last course of chemotherapy wasinitiated and its last cycle, what was the line of the lastchemotherapy and its aim (palliative vs curative), whetherchemotherapy was postponed due to toxicity, the cause andplace of death, and the reference to the PCU. Cancers witha frequency ≤2% were classified as others.
The method used to record the date of patients’ death atour hospital is as follow: when the patients die at thehospital, deaths are immediately recorded; when patientsdie in other locations, given that there are always appoint-
ments scheduled, their non-attendance is always investigat-ed via contact by telephone or mail to find out whathappened and if the cause of non-attendance was death,then the date is input in the hospital records but not thecause or place of death. In such cases, the place of deathwas classified as unknown for this study. As regards thecause of death, if the patient died outside of the hospital andthe chart showed a deterioration of the patient’s condition,then the cause of death was classified as progressivedisease; if, however, it is not possible to ascertain the causeof death or doubts remain, then the cause of death wasclassified as unknown.
Descriptive statistics methods were used for the statisti-cal analysis of the data. The comparisons between the studygroups were performed using the Mann–Whitney test forcontinuous variables and the chi-square test for categoricalvariables. Logistic regression was used for multivariateanalysis. P<0.05 was considered significant.
Results
Of the 1,356 patients who were recorded as aged over16 years and having died in 2002 with a solid tumor, 184did not actually die in 2002, 39 had no cancer, 35 diedbefore diagnosis, and the charts of 34 patients could not befound. Therefore, this study includes the remaining 1,064patients. The median age was 69 years with a range from 23to 99. Other demographic data are shown in Table 1.Antineoplastic treatment was given to 911 patients (86%):690 (65%) underwent surgery and 488 (46%) underwentradiotherapy.
The use of chemotherapy
Four hundred ten patients (39%) underwent chemotherapy.The median between the beginning of the last chemother-apy regimen and death was 268 days (range, 2 to8,965 days), and the median interval between the last cycleof chemotherapy and death was 168 days (range, 1 to8,715 days); details of this interval are shown in Table 2.Chemotherapy was considered palliative in 366 patients(89%) and curative in 44 (11%). The chemotherapy wasfirst-line for 272 patients (66%), second-line for 94 (23%),third-line for 32 (8%), and higher than third-line for 12(3%). In 187 patients (46%), chemotherapy was delayed, atleast once, due to toxicity. Chemotherapy was used from 1to 4,860 days, median 120.5 days: 36 patients (9%)underwent only one cycle of chemotherapy; 29 (7%) fromone cycle to 30 days; 101 (25%) 2 to 3 months; 97 (24%) 3to 6 months; and 147 (36%) more than 6 months.
By univariate analysis, the probability of undergoingchemotherapy was influenced by: age, with patients younger
322 Support Care Cancer (2008) 16:321–327

| 233 233Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
173
than 65 years undergoing chemotherapy more often thanthose older than 65 years; gender, with women being morelikely to undergo chemotherapy than men; profession, withthe more affluent undergoing chemotherapy more often;cancer type; metastases; and comorbidity, with patients withcomorbidity excluded more often from the chemotherapyprotocols (Table 3). As regards cancer type, patients withgastric, head and neck, and kidney and prostate cancerswere less likely to undergo chemotherapy, whereasbreast and lung cancers were more likely to undergochemotherapy. Patients with metastatic cancer had a higherprobability of undergoing chemotherapy than those withlocally advanced cancer. The probability of undergoingchemotherapy was not influenced by the distance of thepatient’s residence from the hospital and the place of
residence; in other words, chemotherapywas used irrespectiveof whether the place of residence was an important city, asmall town, or a rural area.
The mean age of those who underwent chemotherapywas 60.5 years against 70.4 years for those who did not (p<0.001). To compare our data with other studies, thepopulation was divided into two groups: patients under65 years and patients aged 65 years or more. Details of theinterval between the last chemotherapy and death areshown in Table 4. As can be seen, there was a number ofpatients who underwent chemotherapy very close to deathin both groups. However, there is a significant difference(p=0.035) between the two age layers.
In the multivariate analysis, only age <65, breast and lungcancers, and metastases were positively associated withchemotherapy. Kidney cancer and comorbidity were associatedwith a lower probability of undergoing chemotherapy (Table 5).
Cause and place of death
Three hundred sixty-one patients (34%) were admitted tothe PCU where they were monitored from 1 to 1,338 days,median of 34 days.
The overall most frequent cause of death was progres-sive disease, which occurred in 453 (69.3%) of the patientsthat did not undergo chemotherapy, and in those whounderwent chemotherapy, it was the cause of death in 366(89%) (Table 6).
In 520 patients (49%), the place of death was unknown.Presumably, most of these patients died at home. The places ofdeath that we do know were 234 (22%) in the PCU, 236 (22%)in other services of the hospital, 49 (5%) at home, 17 (2%) atother hospitals, and 8 (1%) at other places. Fifty-three percent ofthe patients who underwent chemotherapy died in our hospital,while only 38% of those who did not die here (p<0.001).
Discussion
The main goal of this study was to examine how closechemotherapy use is to the patients’ death. The overall
Table 2 Interval between the last chemotherapy and death
Numberof days
Number of patientson chemotherapy
Percent patients onchemotherapy
Percent allpatients(n=1,064)
1 to 7 11 3 18 to 30 41 10 431 to 90 75 18 791 to 180 85 21 8>180 198 48 19Total 410 100 39
Table 1 Demographic data
(n=1,064)
GenderMale 583(55)Female 481(45)
ResidenceBig city 350(33)Small town 297(28)Rural area 417(39)
Distance from the hospital<30 km 397(37)30 to 100 km 314(30)100 to 200 km 224(21)>200 km 129(12)
Professiona
1 49(5)2 108(10)3 63(6)4 309(29)5 510(48)Unknown 25(2)
CancerHead and neck 170(16)Breast 161(15)Colorectal 111(10)Stomach 86(8)Lung 80(8)Prostate 76(7)Esophagus 44(4)Cervix 39(4)Bladder 36(3)Endometrium 33(3)Melanoma 33(3)Primary unknown 27(3)Kidney 22(2)Other 146(14)
a The professional levels were defined according to the Graffar index[18]. Level 1 is the highest and includes enterprise director, profes-sionals with a university degree, etc. Level 5 includes undifferentiatedworkers.
Support Care Cancer (2008) 16:321–327 323

234 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
174
percentage of patients undergoing chemotherapy (39%) atthis center is very similar to the percentage of the Aragon-Ching et al. [1] study (38%), but our percentage is higher inthe last 6 months of life, 52 vs 43%. However, in the lastmonth, only 5% of our patients underwent chemotherapy,
contrasting with the 26% in the Aragon-Ching et al. study.In a study by Emmanuel et al. [2] with patients aged over65 years, in 1996, 33% of the patients underwentchemotherapy in the last 6 months of life, 23% in the last3 months, and 9% in last month in cancer decedents in
Table 3 Differences between patients who did and did not undergo chemotherapy by univariate analysis
Chemotherapy P value
Yes (n=410) N (%) No (n=654) N (%)
GenderMale 203(35) 38(65) 0.006Female 207(43) 274(57)
Age<65 243(56) 188(44)≥65 167(26) 466(74) <0.001
ResidenceBig city 143(41) 207(59)Small town 125(42) 172(58) 0.052Rural place 142(34) 275(66)
Distance from the hospital<30 km 154(39) 243(61)30 to 100 km 124(40) 190(60) 0.506100 to 200 km 90(40) 134(60)>200 km 42(33) 87(67)
Professiona
1 29(59) 20(41) 0.0082 48(44) 60(56)3 26(41) 37(59)4 122(40) 187(60)5 179(35) 331(65)Unknown 6(24) 19(76)
CancerStomach 24(28) 62(72) 0.035Breast 98(61) 63(39) <0.001Head and neck 43(25) 172(75) <0.001Esophagus 15(34) 29(66) 0.536Lung 50(63) 30(37) <0.001Colorectal 50(45) 61(55) 0.136Bladder 18(50) 18(50) 0.150Primary unknown 11(41) 16(59) 0.811Kidney 4(18) 18(82) 0.047Endometrium 12(36) 21(64) 0.795Prostate 15(20) 61(80) <0.001Cervix 10(26) 29(74) 0.092Melanoma 16(48) 17(52) 0.233Other 44(30) 102(70) 0.025
MetastasesLocally advanced 247(40) 366(60) 0.169Brain 37(67) 18(33) <0.001Lung 111(59) 77(41) <0.001Liver 105(54) 88(46) <0.001Bone 116(59) 82(41) <0.001Peritoneum 48(49) 51(51) 0.033Comorbidity 181(31) 401(69) <0.001
a The professional levels were defined according to the Graffar index [18]. Level 1 is the highest and includes enterprise director, professionalswith a university degree, etc. Level 5 includes undifferentiated workers.
324 Support Care Cancer (2008) 16:321–327

| 235 235Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
175
Massachusetts, and in California, the percentages were 26,20, and 9%, respectively. These percentages are muchhigher than ours: 12, 7, and 4%, respectively, for patientsaged 65 years and over. Another study including onlypatients aged 65 years and older who underwent chemo-therapy showed that, in 1996, 18.5% of the patients werestill receiving chemotherapy 2 weeks before death [3]. Thistoo differs from the 14% of patients aged 65 years and olderwho underwent chemotherapy in the last month of life atour hospital. The reasons for the differences existingbetween the percentage of patients that undergo chemo-therapy in the USA and Portugal are not clear. Probably, thedifferences in the results of the studies are due to acombination of reasons. Differences in the types of cancers,namely, the inclusion of hematological neoplasms in onestudy [2], which tend to be treated with chemotherapy moreoften and until a later stage, or possible differences incomorbidity could contribute to the differences observed.Perhaps, different diagnosis and prognosis disclosurepractices result in different attitudes regarding possibletreatments. Differences in the health systems, with a publicand universal system in Portugal and a predominantly
private practice in the USA can result in substantialdifferences in the decisions to initiate and/or maintainchemotherapy. In the Portuguese public system, doctors donot have any incentive to provide treatments consideredunnecessary. On the other hand, in USA, health careproviders are likely to be reimbursed for ordering chemo-therapy [4], which can be an incentive to initiate ormaintain chemotherapy, perhaps facilitating patients’requests. Maybe a public system largely generates morestreamlined expenses. Could this explain, at least in part,the huge differences in health care expenses? It would beimportant to see data from other countries with differenthealth systems.
In the study of Emmanuel et al. [2], cancers that tend tobe unresponsive were as likely as responsive tumors toreceive chemotherapy, although the former were morelikely to have only a short course of therapy. At ourhospital, that also happened to some point. However, therewere significant differences with most patients with breastand lung cancers, which are responsive cancers although indifferent manners, undergoing chemotherapy more often,whereas only a few patients with kidney cancer, whichrespond poorly, underwent chemotherapy.
Comorbidity is also a factor that negatively influencesthe decision to perform chemotherapy, which was expectedand observed by others [3]. Women underwent chemother-
Table 4 Interval between the last chemotherapy and death according with age
Number of days Number and percent of patients on chemotherapy, n (%) Percent of the total of each age layer %
<65 years ≥65 years <65 yearsa ≥65 years*
1 to 7 6(3) 5(3) 1.4 0.88 to 30 22(9) 19(11) 5.1 3.031 to 90 56(23) 19(11) 13.0 3.091 to 180 52(21) 33(20) 12.0 5.2>180 107(44) 91(55) 24.8 14.4Total 243(100) 167(100)
a Total number of patients under 65=431; total number 65 years or more=633
Table 5 Factors associated with chemotherapy by multivariateanalysis
OR 95% CI P value
CancerBreast 2.80 1.87–4.20 <0.001Lung 2.94 1.75–4.95 <0.001Kidney 0.30 0.09–0.98 0.046MetastasesBrain 1.95 1.95–3.69 0.041Lung 1.82 1.26–2.62 0.001Peritoneum 1.80 1.14–2.85 0.012Liver 1.91 1.33–2.74 <0.001Bone 1.78 1.23–2.57 0.002Comorbidity 0.67 .051–0.89 0.006Age <65 2.96 2.23–3.94 <0.001
Table 6 Causes of death
Overall groupn (%)
Chemotherapy groupn (%)
Progressive disease 819(77.0) 366(89.0)Drug toxicity 13(1.2) 10(2.4)Postoperative complication 12(1.1) 2(0.5)Digestive hemorrhage 9(0.8) 3(0.7)Sepsis 8(0.8) 1(0.2)Other 439(3.7) 5(1.2)Unknown 164(15.4) 23(5.6)Total 1064(100) 410(100)
Support Care Cancer (2008) 16:321–327 325

236 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
176
apy more often than men, as in the Aragon-Ching et al. study[1], although in our study, the difference was not significantin the multivariate analysis. Profession was also significantin the univariate analysis but not in multivariate analysis.Therefore, there seems to be a fair distribution of resources,as socioeconomics variables were irrelevant in the decisionto use chemotherapy, and gender, profession, distance, andplace of residence were not significant in the option ofchemotherapy, different to the findings of others [5].However, as in other studies [5–7], age was an independentfactor that significantly influenced the decision to initiatechemotherapy. This is perhaps based on a common sensejudgment, although it is not an evidence-based decision.
The toxicity of chemotherapy is well demonstrated in thisstudy through the 46% patients whose treatment waspostponed at least once due to toxicity. Chemotherapy caneven be a cause of death, as occurred in our study wherealmost all deaths due to drug toxicity were due tochemotherapy. Chemotherapy is in fact an aggressiveweapon that can cause major toxicity. Therefore, it shouldbe used cautiously only and when there is a reasonableprobability of success and reasonable patient fitness.However, that which a physician perceives as aggressivetreatment may be perceived to be routine care by patients [4].
Patients often have unrealistic expectations from chemo-therapy. Many think that chemotherapy can make them livelonger and that the probability of cure is moderately high orhigh, even when this is not the case [8]. Patients and theirfamilies can call on it as a last, desperate remedy, as a lastresource to prolong life even in the face of a very lowprobability of benefit and with the possibility of majortoxicity [9, 10]. Doctors confronted with this situation canagree to do one or two cycles of chemotherapy. On theother hand, many doctors have difficulties in communicat-ing bad news [9], mainly telling patients that antineoplastictreatment is no more beneficial and that it is better tochange to symptomatic treatment; this can be seen assomething that can affect hope [10].
Pharmaceutical companies run campaigns that influence allparticipants in the decision-making process: doctors, patients,and families [11]. Patients and families may hear about theefficacy of a treatment for their disease and request a trial,even if it is not adequate for their specific case [11].
In other cases, the explanations for the use of chemotherapyat the end of life can be related with the well-known difficulty inaccurately calculating patients’ survival. Doctors tend to beover-optimistic and overestimate the survival of patients [12].There is also some uncertainty regarding the responsiveness tochemotherapy in particular cases. In view of this uncertainty, itis usual to try one or two cycles of chemotherapy to assess itseffect and thus the usefulness of continuing with it.
The prolongation of life is not chemotherapy’s only goal,as it can also be used to palliate symptoms and so improvethe quality of life [13]. In fact, a number of studies haveshown that chemotherapy can improve the quality of life ofpatients with lung [13, 14], colorectal [15], ovary [8], andpancreas [16] cancers, despite low objective responses. Thisis the rationale for the use of chemotherapy in some cases.Although the quality of life, as stated by patients, seems tobe related with the gap between expectations and whatactually occurs [17], patients can show a significantimprovement in quality of life despite unrealistically highexpectations relative to the results of chemotherapy [8]. Toexplain this, Doyle et al. [8] hypothesized that unrealisticexpectations can be related to the patients’ way of copingwith stress, to not acknowledge the prospect of dying fromthe disease, and to poor doctor–patient communication. Theusefulness of chemotherapy in the palliation of symptomsdespite expected low objective responses raises the issuethat the cooperation between oncologists and palliative carespecialists can result in many cases in better outcomes fortheir patients than if they work apart.
The results of our hospital seem to compare favorablywith the results of others, concerning the appropriateness ofthe use of chemotherapy at the end of life, as it seems to beused less often in patients near death. The use ofchemotherapy seems appropriately related to the probabilityof response as per cancer type and negatively related in thepresence of comorbidity. However, in this study, it is notpossible to find out if patients who would benefit fromchemotherapy did not undergo it.
This study has a number of weaknesses. As described in the“Materials and methods” section, at this hospital, there is acancer register system and whenever a patient misses anappointment, he or she is contacted by telephone or mail tofind out what happened. This is not a perfect system andprobably there are a number of cases missed, but this is theonly possible way of detecting deaths. However, the numberobtained is high enough to allow conclusions to be drawn inregard to this center. The high number of unknown placesand causes of death are due to that system. In particular, thedifference between the cause of death being classified asprogressive disease in patients who underwent chemotherapyand those who did not is due probably to the fact that thosepatients that underwent chemotherapy were more closelymonitored by the hospital and more often died in thehospital. Our data might not be generalizable to the wholecountry because the study was performed in an oncologicalcenter; therefore, it is not a population-based study, andbecause the center has a PCU, in a country where palliativecare is not widely available, and the impact that this fact hason the decision to initiate chemotherapy is unknown.
326 Support Care Cancer (2008) 16:321–327

| 237 237Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
177
Conclusion
The use of chemotherapy near the end of life seems to be lessfrequent at this hospital when compared with other reports.There are a number of possible explanations to this, includinghealth systems differences, that is why, studies in othercountries would be useful to clarify this important point. It isnot possible, on the other hand, to see in this study ifchemotherapy was in some cases inappropriately withheld orwithdrew nor was it possible to gauge the possible influenceof the availability of a PCU on the decision process. There isalways a balance that must be made between the benefits andburdens, but the variables are often largely uncertain.
Acknowledgements This work was supported in part by the NorthPortugal Section of the Portuguese League against Cancer.
References
1. Aragon-Ching JB, Cohn JB, Cohn A (2003) Chemotherapy at theend of life. Proc Am Soc Clin Oncol 22(abst 3119)
2. Emanuel EJ, Young-Xu Y, Levinsky NG, Gazelle G, Saynina O,Ash AS (2003) Chemotherapy use among Medicaire beneficiariesat the end of life. Ann Intern Med 138:639–643
3. Earle CC, Neville BA, Landrum MB, Ayanian JZ, Block SD,Weeks JC (2004) Trends in the aggressiveness of cancer care nearthe end of life. J Clin Oncol 22:315–321
4. Matsuyama R, Reddy S, Smith TJ (2006) Why do patients choosechemotherapy near the end of life? A review of the perspective ofthose facing death from cancer. J Clin Oncol 24:3490–3496
5. Earle CC, Venditti LN, Neumann PJ, Gelber RD, Weinstein MC,Potosky AL, Weeks JC (2000) Who gets chemotherapy formetastatic lung cancer. Chest 117:1239–1246
6. Harlan LC, Clegg LX, Trimble EL (2003) Trends in surgery andchemotherapy for women diagnosed with ovarian cancer in theUnited States. J Clin Oncol 21:3488–3494
7. Hurria A, Naeim A, Elkin E, Limaye S, Grover A, Hudis C,Pearce C, Robson M (2007) Adjuvant treatment recommendationsin older women with breast cancer: a survey of oncologists. CritRev Oncol Hematol 61:255–260
8. Doyle C, Crump M, Pintilie M, Oza AM (2001) Does palliativechemotherapy palliate? Evaluation of expectations, outcomes, andcosts in women receiving chemotherapy for advanced ovariancancer. J Clin Oncol 19:1266–1274
9. Slevin ML, Stubbs I, Plant HJ et al (1990) Attitudes tochemotherapy: comparative views of patients with cancer withthose of doctors, nurses, and general public. BMJ 300:1458–1460
10. Yellen SB, Cella DF (1995) Someone to live for: social well-being, parenthood status and decision-making in oncology. J ClinOncol 13:1255–1264
11. Jirillo A, Boscaro M, Passeto LM, Monfardini S (2005)Chemotherapy at the end of life: an open question. Tumori91:104–105
12. Glare P, Virik K, Jones M et al (2003) A systematic review ofphysicians’ predictions in terminally ill cancer patients. BMJ327:195–200
13. Ellis PA, Smith IE, Hardy JR, Nicolson MC, Talbot DC, AshleySE, Priest K (1995) Symptom relief with MVPP (mitomycin C,vinblastine and cisplatina) chemotherapy in advanced non-small-cell lung cancer. BJC 71:366–370
14. Cullen MH, Billingham LJ, Woodroffe CM et al (1999)Mitomycin, ifosfamide, and cisplatin in unresectable non-small-cell lung cancer: effects on survival and quality of life. J ClinOncol 17:3188–3194
15. Cunningham D, Pyrhönen S, James RD et al (1998) Randomisedtrial of irinotecan plus supportive care versus supportive carealone after fluorouracil failure for patients with metastaticcolorectal cancer. Lancet 352:1413–1418
16. Burris HA, Moore MJ, Andersen MJ et al (1997) Improvements insurvival and clinical benefit with gemcitabine as first-line therapyfor patients with advanced pancreas cancer: a randomized trial. JClin Oncol 15:2403–2413
17. Wan GJ, Counte MA, Cella DF (1997) The influence of personalexpectations on cancer patients’ report of health-related quality oflife. Psycho-Oncol 6:1–11
18. Graffar M (1956) Une méthode de Classification Social d’échan-tillon de la population. Courier 6:455–459
Support Care Cancer (2008) 16:321–327 327

238 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 239 239Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
40
Validation of a Consciousness Level Scalefor Palliative CareF Gonçalves Palliative Care Unit – Network, Portuguese Institute of Oncology, Porto, MJ BentoEpidemiology Service, Portuguese Institute of Oncology, Porto, M Alvarenga, I Costa and L Costa PalliativeCare Service, Portuguese Institute of Oncology, Porto
The main objective of this study is to validate a Consciousness Scale for palliativecare. The scale was named Consciousness Scale for palliative care (CSPC). The valida-tion had two phases: 1) face validity – the scale was assessed by seven healthcareprofessionals, both doctors and nurses, experienced in palliative care; 2) reliabilityand construct validity – performed by four investigators, two nurses and two doctors.The construct validation was performed by comparing the CSPC with a Visual Ana-logue Scale (VAS) of 100 mm, anchored in the terms ‘awake’ and ‘unarousable’, andthen with the Glasgow Coma Scale (GCS). In this study, all four observers completed44 periods of observation relative to 38 patients resulting in a total of 176 observations.In the phase of face validation, there were no discrepancies in relation to the issue: thescale provides measures for measurement; the scale can be useful to clinical practice;the scale can improve communication among professionals and the scale is easy touse. As a measure of internal consistency, Cronbach’s α was found to be very high(0.99). The inter-rater reliability was also very high with an intraclass correlation coeffi-cient of 0.99 (P < 0.001). The correlation of the CSPC to the VASwas 0.94 (P < 0.001) andthe CSPC to the GCS was −0.82 (P < 0.001). The CSPC can be a very useful tool forassessing consciousness in palliative care patients. It is very ease to use, not time con-suming and can be used withminimal training. Communication between professionalscan be improved in the clinical setting and in the research environment. Palliative Med-icine (2008); 22: 724–729
Key words: consciousness; consciousness level scale; palliative care; sedation
Introduction
A large percentage of palliative care patients undergotemporary or definitive changes in their consciousnesslevel. This can be due to the involvement of the centralnervous system brought on by cancer, metabolic altera-tions, infections, medication or a combination of thesefactors. When it is caused by medication, the level of con-sciousness can be intentionally affected or not. Whenintentional, with the aim of controlling suffering, theaction is called palliative sedation.
Sedation in palliative care is a very important task. Ithas been under discussion for more than a decade. Chateret al.1 defined sedation as ‘the intention to deliberatelyinduce and maintain deep sleep, but not deliberately caus-ing death, in very specific circumstances…’. However, theobjective is to control suffering (physical or psychological
symptoms, existential distress, etc.) and not the level ofsedation. Hence, the deepness of sedation should be,such as to acceptably control, the cause of suffering,which cannot be controlled by any other means.
No validated palliative care scale to measure the levelof consciousness exists. The absence of such a scale is oneof the reasons why data from studies, such as those deal-ing with sedation, are difficult to compare. Therefore,a reliable consciousness level scale could improve commu-nication between professionals, making the comparison ofdata of different studies easier, and it would be useful toclinical practice and research in general. The purpose ofthis study is to develop and validate such a scale for palli-ative care. The scale developed herein is called the Con-sciousness Scale for Palliative Care (CSPC).
Consciousness has two dimensions: wakefulness andawareness.2 There are other scales that measure cognitivefunction, and therefore awareness, for example, the mini-mental state examination,3 and others. The intention ofthat scale is to primarily measure wakefulness and notthe content of consciousness.
Correspondence to: Dr Ferraz Gonçalves, Instituto Portuguêsde Oncologia, UCP-R, Rua Dr. António Bernardino deAlmeida, 4200-072 Porto, Portugal.Email: [email protected] or [email protected]
© 2008 SAGE Publications, Los Angeles, London, New Delhi and Singapore 10.1177/0269216308094104
Palliative Medicine 2008; 22: 724–729
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

240 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
41
Methods
This study was conducted at the Palliative Care Service ofthe Porto Section of the Portuguese Institute of Oncology.The study was approved by the ethics committee of theinstitution. As this study was non-interventional andthere was no added risk to patients, a written informedconsent was waived.
The design of the scaleTo identify other existing level of consciousness scales, aMEDLINE search was done for the period January 1970to September 2003, using the following keywords: comascale, coma assessment, sedation scale and sedation assess-ment. Reference lists of the resulting articles were reviewed.
Although there are many scales used in different envir-onments, only a small number were assessed for reliabilityand validity, which was also observed by others.4,5 Mostof them were designed for use in intensive care units (ICU)or on neurological patients. None have been designed foror studied in a palliative care setting.
None of the identified scales are suited to use in a palli-ative care setting for a large number of reasons, the mostrelevant being:
� Most of the scales used in ICU include the assessmentof items such as anxiety or agitation.6–11
� Other scales used in ICU have items related to compli-ance with mechanical ventilation.6,11–13
� Some scales were designed for neurological conditions;therefore, they contain items that are irrelevant to ourpurpose.14–17
� Some scales were designed to focus on particular con-ditions and therefore contain items that are only ofrelevance to such conditions.18–22
� Some were designed for children.23,24� Many do not have the levels of the scale clearly
defined, or these are not mutually exclusive.25,26
Although the existing scales were considered inadequatefor use in palliative care, they included the elements thatshould be used in a new scale. There are, therefore, ele-ments common to all these scales. In fact, following thestudy of those scales, the CSPC was constructed based onthe responses to the stimuli ranked in a logical manner. Thechosen responses are mutually exclusive. The stimuli,which are common to many scales, are simple and alsoperformed in a logical progression: first observation then,if required, vocal stimulus and finally painful stimulus.
This study included bedridden patients over 18 years ofage, on a convenience basis. A patient may be includedmore than once if observations are carried out at least48 h apart. The data collected included age, gender, diag-
nosis, metastases, sedative medication and if the patientwas intentionally sedated or not.
The study had two phases. In phase 1, face/contentvalidity was carried out. Seven healthcare professionalsexperienced in palliative care, three doctors and fournurses, not involved in the design of the scale, appliedthe scale to about 20 patients each in order to familiarisethemselves with it. They then answered the followingquestions using a five-point scale ranging from ‘stronglyagree’ to ‘strongly disagree’:
� Does the scale measure what it is intended to measure?� Can the scale be useful to clinical practice?� Can the scale improve communication among health-
care professionals with regard to consciousness level?� Is the scale easy to use?
The investigators were asked to give suggestions thatmight improve the scale, if they thought the scale couldbe improved.
In phase 2, reliability and construct validation wereperformed. Because there is not any golden standard toevaluate consciousness level against which the CSPC canbe compared, a criterion validation could not be per-formed. Therefore, we had to perform a construct valida-tion of the scale, comparing it with other tools we thinkcan measure consciousness level, as is usually the case inthese types of study. A visual analogue scale (VAS) andthe Glasgow Coma Scale (GCS) were used, as was thecase in similar studies undertaken in different settings,such as in an ICU environment.4,6,7,13 The VAS wasassessed by drawing a perpendicular mark on a 100 mmhorizontal line based on the terms ‘awake’ and ‘unarousa-ble’, and then the distance between the left end of the lineand the mark was measured in millimetres.
The data were collected by four investigators involvedin the study: two doctors and two nurses. All four investi-gators underwent a training period with the VAS for eval-uating consciousness level, to familiarise with the scale.Each patient was simultaneously observed by three inves-tigators, one doctor and two nurses. One investigatorinteracted with the patient, as per the instructions setforth in the appendix, and rated the patient, whereas theother two observed and rated the patient independently:two scored using the CSPC and one using the VAS. In all,15 min later, the other doctor performed the GCS, record-ing the score of each item (motor and verbal responses,and eye opening). A rotation system was used so thateach healthcare professional performed all the roles a sim-ilar number of times, except with regards to the GCS,which was always performed by the doctors and alwaysby the doctor who did not participate in the first part ofevaluation.
Consciousness Level Scale for Palliative Care 725
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

| 241 241Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
42
Statistical analysis
� Cronbach’s α was performed to measure internalconsistency.27
� The intraclass correlation coefficient was used to mea-sure the degree of concurrence between raters.28
� The association between the CSPC, VAS and GCSwas evaluated using Spearmen’s ρ.29
� The non-parametric Wilcoxon rank sum test was usedto compare CSPC values with previously identifiedsubgroups (gender, age, use of sedatives).30
Results
In this study, all four observers made 44 periods of obser-vation relative to 38 patients, resulting in 176 observa-tions. None of the patients was subject to more than twoperiods of observation. The demographic data of thosepatients are detailed in Table 1.
Forty-two patients (96%) were medicated with one ormore drugs with sedative effects: 91% opioids, 57% neuro-leptics, 43% benzodiazepines and 30% others. Six patientswere intentionally sedated: 1 was at level 4, 3 at level 5 and2 at level 6 of the scale. There was, in those patients, 100%coincidence between the two raters of the scale.
Face validityThe results for face validity were as follows:
� The scale measures what it is intended to measure.Mean = 1.7 (range: 1 to 2).
� The scale can be useful to clinical practice. Mean = 1.6(range: 1 to 3).
� The scale can improve communication among health-care professionals: Mean = 2.0 (range: 1 to 3).
� The scale is easy to use. Mean = 1.6 (1 to 2).
Therefore, the range of responses went from stronglyagree to the middle of the scale, without anydisagreements.
Internal consistencyAs a measure of internal consistency, the Cronbach’s αwas very high (0.99).
Inter-rater reliabilityThe scores recorded by the raters are displayed in Table 2.The same score on the scale was selected in 39 cases (89%).In the five cases where a different score was selected, thedifference was always not more than one level of the scale.The degree of agreement between raters with regard tothe scale was, therefore, very high, with an intraclass cor-relation coefficient of 0.99 (P < 0.001).
There were no significant within-subject differences insubgroups (age, gender) when analyzed by the Wilcoxonrank sum text. The median age of the patients (68 years)was used to divide this item into two groups. In womenand those aged over 68 years, the scores coincided. Theanalysis of the group that used sedatives was not per-formed because 96% of the patients were using them.
Construct validityThe correlation of the CSPC to the VAS and GCS wasvery high (Table 3). The correlation coefficient of theCSPC to the VAS was 0.94 (P < 0.001) for the firstobserver and 0.95 (P < 0.001) for the second. The correla-tion coefficient of the scale to the GCS was −0.82(P < 0.001) for the first observer and −0.85 (P < 0.001)for the second. Note that the coefficient of the CSPC to
Table 1 Demographic data
No. (%)
GenderMale 19 (50)Female 19 (50)
PrimaryGynaecologic 8 (21)Colorectal 6 (16)Head and neck 5 (13)Gastric 3 (8)Astrocytoma 3 (8)Lung 2 (5)Melanoma 2 (5)Other 9 (24)
Age: median of 68 years (range: 38–82).
Table 2 Distribution of consciousness scale for palliativecare scores between raters
Scores 2nd rater
1 2 3 4 5 6
1st rater 1 9 2 0 0 0 02 2 9 0 0 0 03 0 0 5 1 0 04 0 0 0 3 0 05 0 0 0 0 6 06 0 0 0 0 0 7
Table 3 Correlation between scales
Scales ρ P
CSPC1–CSPC2 0.98 <0.001CSPC1–VAS 0.96 <0.001CSPC2–VAS 0.96 <0.001CSPC1–GCS 0.88 <0.001CSPC2–GCS 0.88 <0.001
CSPC1 and CSPC2 are the 1st and 2nd ratings of the scale.CSPC, Consciousness Scale for Palliative Care; VAS,Visual Analogue Scale; GCS, Glasgow Coma Scale.
726 F Gonçalves et al.
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

242 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
43
the GCS was negative due to the scales’ scoring beinginverted in relation to each other; in other words, thebest score of the CSPC is the lowest, whereas the bestscore of the GCS is the highest.
Discussion
An ideal assessment tool should be inexpensive, easy tolearn and easy to use by doctors and nurses at bedsides.This last aspect is particularly important in palliative carebecause it is practised in many settings and by healthcareprofessionals from heterogeneous backgrounds. Yet, theassessment tool should undergo rigorous testing to showvalidity and reliability. Probably, the most used scale isthe Ramsay Scale. This scale was developed in an ICU tocontrol the level of sedation with alphaxalone-alphadoloneand published in the British Medical Journal in 1974.25 Thescale was really a secondary aspect of the article; however,since then, it has been widely used in many settings withoutundergoing any process of validation. This was carried outrecently.31 Although that scale has been extensively used,it has been criticised for many reasons,32 the criticismsmos-t relevant to palliative care being: ‘the six levels of the Ram-say scale are not mutually exclusive’; ‘patients may be rest-less or agitated (level 1), whereas at the same time beingresponsive only to light physical or loud auditory stimulus(level 4 and 5)’ and ‘the sedation levels are not clearlydefined or fully inclusive’.
The goal of this study was the development and valida-tion of a scale with the above-described characteristics, inan attempt to avoid the drawbacks of the Ramsay scaleand other scales.
The structure of the scale is very ease to use and thelevels are clearly defined, with a phase of observationand, if required, consecutive phases of verbal interactionand of physical stimulation. The scale can be administeredin a few seconds, using common and unambiguous stimuliin a logical sequence. The stimuli are also standardized,which does not happen with most scales.
The inter-rater reliability of the scale was very goodfor all patients, with coincident scores in almost 90% ofthe cases, and in the few cases without coincidence, thedifference was never greater than one level. In womenand in patients aged over 68 years, there was completeagreement in the scores, as well as among the six patientswho were intentionally sedated.
As no gold standard exists for sedation, against which theCSPC could be compared to validate it, the validation of theCSPC was performed by correlating it to a VAS based onthe terms ‘awake’ and ‘unarousable’ and theGCS,which is ascale that was designed to assess the prognosis of coma afterhead injury33 but which is widely used in many settings toassess the consciousness level. The correlation of the CSPCto the VAS and the GCS was very high.
There are potential limitations to the use of the CSPC.Asit relies on the patients’ auditory and visual acuity, it is notsuitable for use on patients with major impairment of thesesenses.The intensityof the stimuli canvarywith theobserver;in other words, louder voices or more firm pinching of thetrapezius might eventually result in different scores. Patientscan have a ‘not normal’ score simply because they were nor-mally sleeping, but this is common to all scales.
Nevertheless, the CSPC can be a very useful tool forassessing consciousness in palliative care patients. It isvery ease to use, not time consuming and can be per-formed with minimal training. Communication betweenhealthcare professionals can be improved in the clinicalsetting and in a research environment by the lack of ambi-guity of the levels and of the method of interaction withthe patient. However, the scale should be evaluated inother locations in a palliative care setting to confirm theresults achieved by this study.
References
1 Chater, S, Viola, R, Paterson, J, Jarvis, V. Sedation forintractable distress in the dying – a survey of experts. Pal-liat Med 1998; 12: 255–269.
2 Laureys, S. The neural correlate of (un)awareness: les-sons from the vegetative state. Trends Cogn Sci 2005;19: 556–559.
3 Folstein, MF, Folstein, SE, McHugh, PR. Mini-mentalstate: a practical method for grading the cognitive state ofpatients for the clinician. JPsychiatr Res 1975; 12: 188–189.
4 Ely, EW, Truman, B, Shintani, A, Thomason, JW,Wheeler, AP, Gordon, S, et al. Monitoring sedation sta-tus over time in ICU patients: reliability and validity ofthe Richmond Agitation-Sedation Scale (RASS). JAMA2003; 289: 2983–2991.
5 Jacobi, J, Fraser,G, Coursin, DB, Riker, RR, Fontaine, D,Wittbrodt, ET, et al. Clinical practice guidelines for the sus-tained use of sedatives and analgesics in the critically illadults. Crit Care Med 2002; 30: 119–141.
6 Sessler, CN, Gosnell, MS, Grap, MJ, Brophy, GM,O’Neal, PV, Keane, KA, et al. The RichmondAgitation-Sedation Scale: validity and reliability inadult intensive care unit patients. Am J Respir Crit CareMed 2002; 166: 1338–1344.
7 Devlin, JW, Boleski, G, Mlynarek, M, Nerenz, DR,Peterson, E, Jankowski, M, et al. Motor Activity Assess-ment Scale: a valid and reliable sedation scale for use withmechanically ventilated patients in an adult surgicalintensive care. Crit Care Med 1999; 27: 1271–1275.
8 Riker, RR, Picard, JT, Fraser, GL. Prospective evalua-tion of the Sedation-Agitation Scale for adult critically illpatients. Crit Care Med 1999; 27: 1325–1329.
9 Detriche, O, Berré, J, Massaut, J, Vincent, JL. The Brus-sels Sedation Scale: use of a simple clinical sedation scale
Consciousness Level Scale for Palliative Care 727
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

| 243 243Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
44
can avoid excessive sedation in patients undergoingmechanical ventilation in the intensive care unit. Br JAnaesth 1999; 83: 698–701.
10 Chaudhri, S, Kenny, GNC. Sedation after cardiac bypasssurgery: comparison of propofol and midazolam in thepresence of a computerized closed loop arterial pressurecontroller. Br J Anaesth 1992; 68: 98–99.
11 Riker, RR, Fraser, GL, Cox, PM. Continuous infusionof haloperidol controls agitation in critically ill patients.Crit Care Med 1994; 22: 433–440.
12 Mallick, A, Smith, SN, Bodenham, AR. Local anaesthe-sia to the airway reduces sedation requirements inpatients undergoing artificial ventilation. Br J Anaesth1996; 77: 731–734.
13 Riker, RR, Fraser, GL, Simmons, LE, Wilkins, ML.Validating the Sedation-Agitation Scale with the bispec-tral index and Visual Analog Scale in adult ICU aftercardiac surgery. Intensive Care Med 2001; 27: 853–858.
14 Wijdicks, EFM, Kokmen, E, O’Brien, PC. Measurementof impaired consciousness in the neurological intensivecare unit: a new test. J Neurol Neurosurg Psychiatry1998; 64: 117–119.
15 Stanczak, DE, White, JG, Gouview, WD, Moehle, KA,Daniel, M, Novack, T, et al. Assessment of level of con-sciousness following severe neurological insult: a compar-ison of the psychometric qualities of the Glasgow ComaScale and the Comprehensive Level of ConsciousnessScale. J Neurosurg 1984; 60: 955–960.
16 Sugiura, K, Muraoka, K, Chishiki, T, Baba, M. TheEdinburg-2 Coma Scale : a CSPC for assessing impairedconsciousness. Neurosurgery 1983; 12: 411–415.
17 Benzer, A, Mitterschiffthaler, G, Marosi, M, Luef, G,Pühringer, F, De La Renotiere, K, et al. Prediction ofnon-survival after trauma: Innsbruck Coma Scale. Lan-cet 1991; 338: 977–978.
18 Miller, DR,Martineau, RJ, Hull, KA, Vallé, F, LeBel, M.Optimizing sedation following major vascular surgery: adouble-blind study of midazolam administered by contin-uous infusion. Can J Anaesth 1994; 41: 782–793.
19 Sanchez-Izquierdo-Riera, JA, Caballero-Cubedo, RE,Perez-Vela, JL, Ambros-Checa, A, Cantalapiedra-Santiago, JA, Alted-Lopez, E. Propofol versus midazo-lam: safety and efficacy for sedating the severe traumapatient. Anesth Analg 1998; 86: 1219–1224.
20 Eddleston, JM, Pollard, BJ, Blades, JF, Doram, B.The use of propofol for sedation of critically ill patients
undergoing haemodiafiltration. Intensive Care Med 1995;21: 342–347.
21 Checketts, MR, Gilhooly, CJ, Kenny, GNC. Patient-maintained analgesia with target-controlled alfentanilinfusion after cardiac surgery: a comparison with mor-phine PCA. Br J Anaesth 1998; 80: 748–751.
22 Irwin, MG, Thompson, N, Kenny, GNC. Patient-maintained propofol sedation. Anaesthesia 1997; 52:525–530.
23 Malviya, S, Voepel-Lewis, T, Huntington, J, Siewert, M,Green, W. Effects of anesthetic technique on side effectsassociated with fentanyl oralet premedication. J ClinAnesth 1997; 9: 374–378.
24 Ambuel, B, Hamlett, KW, Marx, CM, Blumer, JL.Assessing distress in pediatric intensive care environ-ments: the COMFORT scale. J Pediatric Psychol 1992;17: 95–109.
25 Ramsay,MAE, Savege, TM, Simpson, BRJ, Goodwin, R.Controlled sedation with alphaxalone-alphadolone. BMJ1974; 2: 656–659.
26 De Jonghe, B, Cook, D, Appere-De-Vecchi, C, Guyatt, G,Meade, M, Outin, H. Using and understanding sedationscoring systems: a systematic review. Intensive Care Med2002; 26: 275–285.
27 Bland, JM, Altman, DG. Cronbach’s alpha. BMJ 1997;314: 572.
28 Análisis de la concordancia. In: Pallás, JMA, Villa, JJ,(Eds), Métodos de investigación: clínica e epidemiológica,segunda edición. Madrid: Ediciones Harcourt S.A., 2000;p. 321–325.
29 Relation between two continuous variables. In: Altman,DG, (Ed), Practical statistics for medical research. 1st ed.London: Chapman and Hall, 1991; p. 277–324.
30 Comparing groups – continuous data. In: Altman, DG,(Ed), Practical statistics for medical research, 1st ed. Lon-don: Chapman and Hall, 1991; p. 179–228.
31 Yate, PM, Thomas, D, Short, SM, Sebel, PS, Morton, J.Comparison of infusions of alfentanil or pethidine forsedation of ventilated patients of the ITU. Br J Anaesth1986; 58: 1091–1099.
32 Hansen-Flaschen, J, Cowen, J, Polomano, RC. Beyondthe Ramsay Scale: need for a validated measure of sedat-ing drug efficacy in the intensive care unit. Crit Care Med1994; 22: 732–733.
33 Teasdale, G, Jennett, B. Assessment of coma andimpaired consciousness. Lancet 1974; 13: 81–84.
728 F Gonçalves et al.
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

244 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
45
Appendix
Nível Portuguese version
1 Acordado/a2 Acorda quando chamado/a pelo seu nome e permanece acordado durante a conversação3 Acorda quando chamado/a pelo seu nome mas adormece durante a conversação4 Reage com movimentos ou abrindo brevemente os olhos, mas sem contacto visual, quando
chamado/a pelo seu nome5 Reage a beliscão no trapézio6 Não reage
Level English translation
1 Awake2 Awakens when called by his/her name and stays awake during conversation3 Awakens when called by his/her name but falls asleep during conversation4 Reacts with movement or brief eye opening, but without eye contact, when called by his/her name5 Reacts to trapezius muscle pinching6 Does not react
Procedures for assessment:
Stimulation Score
Patient is awakened, calm or agitated, without the need for any externalstimulus
Level 1
Patient is not spontaneously alert. Patient is called loudly by name Levels 2, 3 and 4, according to the reaction observedPatient is not spontaneously alert and does not react to voice. A firm
pinching of the trapezius muscle is appliedLevel 5 and 6, according to the reaction observed
Consciousness Level Scale for Palliative Care 729
by José António Ferraz Gonçalves on October 7, 2008 http://pmj.sagepub.comDownloaded from

| 245 245Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
185
ORIGINAL ARTICLE
Attitudes toward assisted death amongstPortuguese oncologists
Ferraz Gonçalves
Received: 10 January 2009 /Accepted: 13 May 2009 /Published online: 1 June 2009# Springer-Verlag 2009
AbstractBackground The attitudes and practise of doctorsconcerning euthanasia and assisted suicide have been thesubject of studies performed in many countries. However,these issues have not been studied properly in Portugal.Materials and method This study is a survey of 450Portuguese oncologists by postal means and personal contact.Results The response rate was 33% (143). Only 13% wouldpractise euthanasia with the present law in force forbiddingsuch practise, and 24% would do so if it were legalised; 39%favoured its legalisation and 36% would like to have theoption of euthanasia if they had a terminal disease. Aboutassisted suicide, 15% would do it with the current law in forceforbidding such action and 25% would do so if it were madelegal; 32% favoured its legalisation and 24% would like tohave that option if they had a terminal disease. There was onecase of euthanasia and no cases of assisted suicide. The mostimportant factor related with the acceptance of euthanasia andassisted suicide was religion, with non-practising Catholicsaccepting such practises more often than practising Catholics.The Portuguese oncologists have a very positive view on thepotential role of palliative care in preventing many requestsfor euthanasia and assisted suicide.Conclusion Portuguese oncologists are mainly against thepractise of euthanasia and assisted suicide and the numberof requests is also relatively low; consequently, the numberof episodes of assisted death is also apparently very low.
Keywords Assisted death . Euthanasia . Assisted suicide .
End-of-life decisions . Palliative care
Attitudes toward assisted death amongst Portugueseoncologists
At the end of life, there are often many problems andcomplex situations which require decisions involvingethical issues. Some of the problems that physicians facewhen their patients are near the end of life include what todo when a patient requests euthanasia or physician-assistedsuicide, withholding or withdrawing treatment includingnutrition and hydration, how to respond to requests byfamilies relative to incompetent patients, and the use ofdrug therapy to control suffering with the potential tohasten death. Studies have been performed in variouscountries on the opinion and the practises of doctorsconcerning end-of-life situations [1–11], and the discussionof those issues, in which euthanasia and physician-assistedsuicide, primarily, has been very strong. In Portugal,however, the discussion has not undergone significantpublic debate, except at periods of time coinciding withthe modification of legislation or with news of debateoccurring in other places. Probably, this issue may be thetopic of greater discussion in the future.
Euthanasia and or physician-assisted suicide have beinglegalised in some countries or states, such as Australia (notcurrently in force), Holland, Belgium, Switzerland, andOregon (USA). In Portugal, the Penal Code does notspecifically mention the words euthanasia or assistedsuicide but it states:
Article 131 (homicide)Anyone who kills another person shall be liable to
imprisonment for a term of 8 to 16 years.Article 133 (homicide in special circumstances)Anyone who is moved to kill another person under the
influence of an understandable violent emotion, compas-
Support Care Cancer (2010) 18:359–366DOI 10.1007/s00520-009-0661-z
F. Gonçalves (*)Instituto Português de Oncologia, UCP-R,Rua Dr. António Bernardino de Almeida,4200-072 Porto, Portugale-mail: [email protected]

246 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
186
sion or despair, or for any other reason of significant socialor moral scope that appreciably diminishes the culprit’sculpability, shall be liable to imprisonment for a term of 1to 5 years.
Article 134 (homicide at the victim’s request)Anyone who kills a person in response to that person’s
serious, vehement and expressed request, shall be liable toimprisonment for a term of up to 3 years.
Article 135 (incitement or assistance in committingsuicide)
Anyone who incites another person to commit suicide,or aids that person to that end, shall be liable toimprisonment for a term of up to 3 years, whether thesuicide is attempted or successful.
Therefore, under the Portuguese law, euthanasia andassisted suicide are not permitted. However, the legislatordistinguishes between a homicide with other motivationsand the homicide motivated by compassion or at thevictim’s request, determining a lower punishment in thesecases.
The opinions and the testimonies of Portuguese physi-cians are not known, but they are essential to that debate.This lack of knowledge regarding what doctors think canlead to speculation. For example, sometimes people say thatthe practise of euthanasia in Portugal is not rare, but that isnot my idea based on my practise and on the contact I havewith my colleagues. Faced by this uncertainty, I believe thatis worthwhile to try to find out what is really happening.That is the reason why this exploratory study wasperformed.
Materials and methods
After the study of questionnaires used in other countries,namely, those kindly sent to me at my request by HelgaKuhse [5], Frederich Stiefel [12], David Doukas [13], andDiane Meier [14], a new questionnaire was developed. Asall the questionnaires consulted were different from eachother, some choices had to be made with the selection ofquestions, which had to be clear and informative and nottoo many. After the design of the questionnaire, it wassubmitted to face validation by 15 doctors, mainlyoncologists. They were asked to complete the questionnaireand comment on the relevance and coherence of thequestions and also suggest any necessary alterations. Minoralterations were made when considered pertinent, based onthose suggestions.
The questionnaires included questions concerningdemographic data, euthanasia, assisted suicide andpalliative care. Questions on other end-of-life issueswere included in the questionnaire, but they will be
presented in another paper. The questions referring toeuthanasia and assisted suicide were identical and canbe seen in Table 1. The definitions of euthanasia andassisted suicide proposed in this study are shown inTable 2. As there is no consensus on those definitions, thedefinition was constructed from what was viewed as beingthe main elements of various definitions, which wouldensure the concept was clearly defined. For example, thedefinition of euthanasia includes the intentional killing ofthe patient by a doctor as is the case with manydefinitions, such as those used by Bittel et al. [12] andMaterstvedt et al. [15]; the aspect of the “explicit,repeated, informed and well-considered request” is iden-tical to the Materstvedt et al. definition [15]; advanceddisease is a common element; and without pain is includedin the definitions of, for example, Bittel et al. [12] andGielen et al. [16].
The questionnaires were sent by mail to all doctorsbelonging to the Portuguese Society of Oncology (PSO),included on a list provided by the board of that society.Four hundred eight doctors were surveyed in total. Aletter explaining the reasons and the importance of thestudy and assuring the anonymity of replies was enclosedwith the questionnaire; a prepaid envelop without anycode or other means of identifying the person that sent itback was also included. Three weeks later, a new letterwas sent to all doctors asking those who had still notreplied to please do so. During this process, it wasconcluded that many doctors working in oncology didnot belong to the PSO. The total number of such doctorsis obviously unknown. Forty-two of these doctorsworking at different hospitals and whose position onthese issues were not publicly known, were personallyinvited to fill in the questionnaire. They were providedwith a questionnaire, letter and prepaid envelop identicalin every way to those that had previously been sent bymail. Three weeks later, they were contacted again andasked to complete and return the questionnaire if theyhad not already done so.
This study was approved by the Bioethics Service of theFaculty of Medicine of Porto University.
An initial analysis was performed for statisticalpurposes, to identify coding errors, inconsistencies andthe presence of missing categories or small numbers, andcorrections were made where needed. An exploratoryanalysis of the data was performed so as to describe thesample. The variables were analysed by graphicalmethods, proportions and means. To evaluate the exis-tence or not of associations between categorical variablesthe chi-square test was used. The level of significancewas deemed to be 0.05. SPSS (Statistical Package forSocial Sciences) version 14.0 statistical software wasused to analyse the data.
360 Support Care Cancer (2010) 18:359–366

| 247 247Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
187
Results
From the total of 450 questionnaires sent, 12 werereturned because the doctor had moved house or haddied. One hundred forty-three (33%) of the remaining438 questionnaires were sent back completed. Table 3shows the demographic data of the doctors who sent backthe questionnaire. The questionnaires had been completedin a careful and consistent manner. Not much data was
missing, though religion was the data variable mostomitted. However, 132 (92%) reported their religion. Ofthose, 126 (96%) were Catholic and 121 of them declarethemselves as practising or non-practising Catholics.Therefore, in the analysis concerning religion, only thisgroup of 121 was considered because the other groupswere too small.
The age and gender of 80% of the non-respondentdoctors were known. The gender comparison of those who
Table 1 Questions on euthanasia and assisted suicide
Considering the definition of euthanasia (or assisted suicide) presented, please answer thefollowing questions:
1. Portuguese legislation does not allow the practice of euthanasia (or assisted suicide). Evenso, are there any circumstances in which you would practise it?Yes No I do not have a definite opinion
2. If legislation allowed the practice of euthanasia (or assisted suicide), would you practise it? Yes No I do not have a definite opinion
3. Have you ever been requested to perform euthanasia (or assisted suicide)?Yes NoAbout how many?
4. Have you received a request for euthanasia (or assisted suicide) in the last year?Yes NoHow many?
5. Have you ever practised euthanasia (or assisted suicide) in the sense of the above-stateddefinition? Yes No How many times?
6. Do you think that euthanasia (or assisted suicide) should be permitted by Portuguese law? Yes No I do not have a definite opinion
7. If you had an incurable and progressive disease, which inexorably led to death, would youlike to have the available option of euthanasia (or assisted suicide)? Yes No I do not have a definite opinion
The questionnaire included one set of seven questions on euthanasia and another identical seton assisted suicide. The definition of euthanasia or assisted suicide was presented above eachset.
Table 2 Definitions of euthanasia and assisted suicide
Euthanasia: the deliberate termination without pain of the life of a person who has an incurable, advanced and progressive disease that willinexorably lead to death, at his or her explicit, repeated, informed and well-considered request, through the administration of one or more drugs inlethal doses.
Assisted suicide: assistance in the suicide of a person with an incurable, advanced and progressive disease that will inexorably lead to death, at hisor her explicit, repeated, informed and well-considered request, prescribing the drugs and giving him or her the necessary instructions on their use.
Support Care Cancer (2010) 18:359–366 361
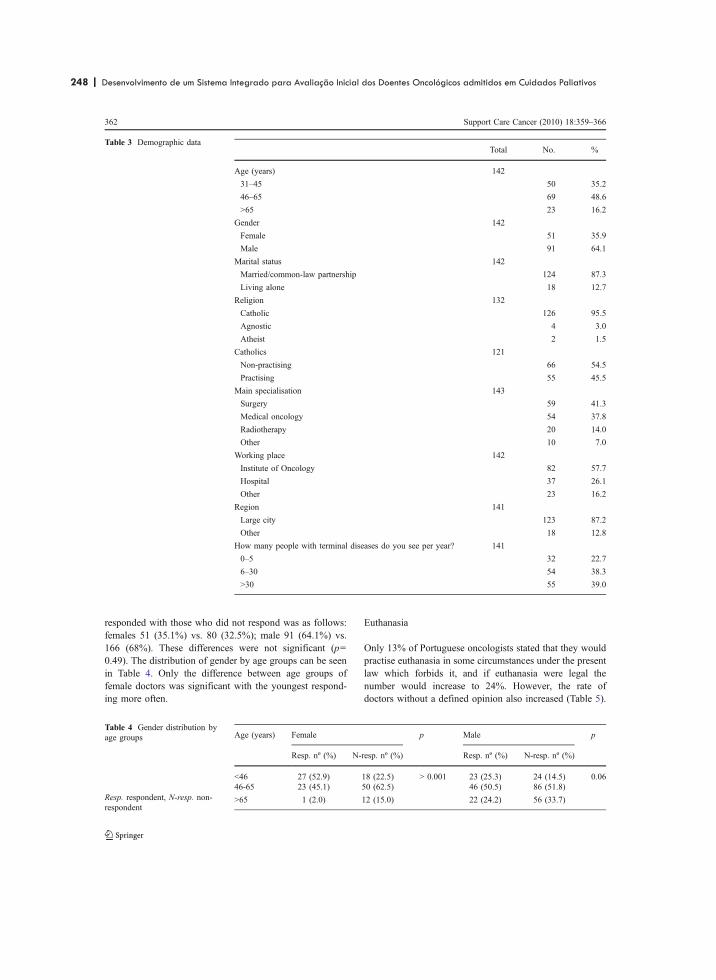
248 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
188
responded with those who did not respond was as follows:females 51 (35.1%) vs. 80 (32.5%); male 91 (64.1%) vs.166 (68%). These differences were not significant (p=0.49). The distribution of gender by age groups can be seenin Table 4. Only the difference between age groups offemale doctors was significant with the youngest respond-ing more often.
Euthanasia
Only 13% of Portuguese oncologists stated that they wouldpractise euthanasia in some circumstances under the presentlaw which forbids it, and if euthanasia were legal thenumber would increase to 24%. However, the rate ofdoctors without a defined opinion also increased (Table 5).
Total No. %
Age (years) 142
31–45 50 35.2
46–65 69 48.6
>65 23 16.2
Gender 142
Female 51 35.9
Male 91 64.1
Marital status 142
Married/common-law partnership 124 87.3
Living alone 18 12.7
Religion 132
Catholic 126 95.5
Agnostic 4 3.0
Atheist 2 1.5
Catholics 121
Non-practising 66 54.5
Practising 55 45.5
Main specialisation 143
Surgery 59 41.3
Medical oncology 54 37.8
Radiotherapy 20 14.0
Other 10 7.0
Working place 142
Institute of Oncology 82 57.7
Hospital 37 26.1
Other 23 16.2
Region 141
Large city 123 87.2
Other 18 12.8
How many people with terminal diseases do you see per year? 141
0–5 32 22.7
6–30 54 38.3
>30 55 39.0
Table 3 Demographic data
Age (years) Female p Male p
Resp. nº (%) N-resp. nº (%) Resp. nº (%) N-resp. nº (%)
<46 27 (52.9) 18 (22.5) > 0.001 23 (25.3) 24 (14.5) 0.0646-65 23 (45.1) 50 (62.5) 46 (50.5) 86 (51.8)
>65 1 (2.0) 12 (15.0) 22 (24.2) 56 (33.7)
Table 4 Gender distribution byage groups
Resp. respondent, N-resp. non-respondent
362 Support Care Cancer (2010) 18:359–366

| 249 249Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
189
Twenty-nine doctors (21%) received a varying number ofrequests to commit euthanasia (Table 6), six (4%) in theprevious year. Only one doctor (0.7%) did actually commiteuthanasia; that doctor had received three requests, thoughnone in the previous year.
Higher rates were observed in the following, relative toother questions: 39% of doctors think that euthanasiashould be legalised and 36% would like to have the optionof euthanasia if they had an incurable and progressivedisease which would inexorably lead to death (Table 5).The rate of doctors without a defined opinion concerningthese issues was also higher.
No correlation between euthanasia and age, gender, maritalstatus, specialisation, work place and region of practise wasfound. The factor most consistently related to the acceptabilityof euthanasia was religion, with statistically significantdifferences between practising and non-practising Catholicsin regard to all questions included in Table 5; with the latteragreeing to it more often, although the number of those whodo not agree to it is higher in both groups.
Another statistically significant factor concerning wheth-er doctors would practise euthanasia if permitted by lawwas the number of patients with incurable and progressivediseases observed per year, wherein those seeing more than
30 such patients replied affirmatively less often, but alsoreplying that they had no defined opinion more often (p=0.035). There was also a tendency for those aged over65 years to reply negatively to the questions on euthanasia,although the correlation was not statistically significant.This group was the one with the least replies of non-definedopinion.
Assisted suicide
Regarding the questions on the practise of assisted suicideunder current Portuguese legislation and if it were legalised,the answers are similar to those given for euthanasia.However, there are a lower number of doctors who thinkthat assisted suicide should be legalised and also a lowernumber that would like to have that option at the end oflife. In this last question, there is also a higher number ofdoctors without an opinion, than that in regard to euthanasia(Table 7).
Only five doctors (3.5%) have been requested to practiseassisted suicide: two have received one request, onereceived four and another six. One of those requests wasin the previous year. No doctor practised assisted suicide.
The most significant statistical difference concerning theacceptability of assisted suicide was again provided by thedoctor being a practising Catholic or not—with non-practising Catholics approving of assisted suicide moreoften, though they did not have an opinion on the issue ingreater numbers. Another statistically significant associa-tion was between age and the legalisation of assistedsuicide, with those aged over 65 years being more oftenagainst it (p=0.027), and none did not have an opinion.There was also an association in the same direction betweenage and the possibility of having the option of assistedsuicide if the doctor had a terminal disease (p=0.029); buthere, some doctors did not have an opinion. It was alsoobserved that doctors older than 65 years tend to be more
Table 6 Number of requests for euthanasia received in the last year
Number of requests Number of doctors %
0 110 79.1
1 4 2.9
2 9 6.5
3 6 4.3
4–6 5 3.6
> 6 5 3.6
139 100
Table 5 Euthanasia
Question Total Yes (%) No (%) I do not have adefinite opinionno. (%)
Practising vs. non-practisingCatholic p
Portuguese legislation does not allow the practise of euthanasia.Even so, are there any circumstances in which you would practiseit?
143 19 (13.3) 112 (78.3) 12 (8.4) 0.005
If legislation allowed the practise of euthanasia, would youpractise it?
143 34 (23.8) 91 (63.6) 18 (12.6) 0.004
Do you think that euthanasia should be permitted by Portugueselaw?
142 55 (38.7) 60 (42.3) 27 (19.0) <0.001
If you had an incurable and progressive disease, which inexorablyled to death, would you like to have the available option ofeuthanasia?
143 51 (35.7) 59 (41.3) 33 (23.1) <0.001
Support Care Cancer (2010) 18:359–366 363

250 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
190
often against the other questions about assisted suicide,although the correlations were not significant. This agegroup was the one that provided the least no-opinionanswers. No correlations between assisted suicide andgender, marital status, specialisation, work place, regionof practise and the number of cases seen per year werefound.
Palliative care
Most doctors believe that palliative care could preventeuthanasia and assisted suicide requests: 12 doctors (8.4%)believed that such care could prevent all requests; 102(71.3%) most requests; 19 (13.3%) some requests; four(2.8%) not at all; six (4.2%) had no opinion.
Discussion
In this study, most Portuguese oncologists reject euthanasiaand assisted suicide. The rate of requests and the rate ofdoctors accepting requests are lower than that observed inmost studies performed in other countries, on differentcontinents, although the results of those are heterogeneous[1–3, 5, 7, 10, 11, 17–21]. The differences can reflect thecultural factors of doctors, patients and their families,including religious beliefs. The low level of debate onthese issues in Portugal possibly reflects the low level ofconsideration that such issues presently have in thiscountry. The fact that the doctors were oncologists mayhave influenced the results, since, although they are moreexposed to terminal patients and suffering, they tend tooppose the practises of assisted death [22].The possibilityof a bias induced by the low rate of replies cannot beexcluded.
The requests for euthanasia and assisted suicide werefocused on a few doctors, some of them with an exceptionalnumber of requests compared with the majority that did not
receive any requests at all. This might be related to theattitude of those doctors toward their patients; maybe theyhave a closer and more intimate relationship with theirpatients than others, allowing a deeper expression ofpatients’ feeling.
The rate of Portuguese oncologists who support thelegalisation of assisted death, 39% for euthanasia and 32%for assisted suicide, is roughly in the middle of the ratesobserved in a recent review of the attitudes observed inEuropean countries [16]. In Portugal, the rate of oncologistswho support assisted suicide is lower than that supportingeuthanasia, as found in the study of Pasterfield et al. [23], butit is the reverse of the results of most studies [16]. It wasobserved that doctors who favour the legalisation ofeuthanasia and assisted suicide were greater in number thanthose who would practise it if it were legalised. These datafollow the same trend as that observed in the study of Cohenet al. [22], carried out in Washington where 54% thought thateuthanasia should be legalised in some situations, but only33% would want to practise it, while in relation to assistedsuicide, the rates were 53% and 40%, respectively. Thosedata can be interpreted by some doctors as recognition of thepatients’ right to assisted death; however, the doctormaintains the right to refuse to provide such assistance.Those positions are, however, a minority in Portugal.
More doctors wish to have the option of euthanasiaavailable if they had a terminal disease than those whowould practise it on patients, but the same does not occurwith assisted suicide. In the study of Howard et al. [18] asimilar difference, although lower, was observed.
The most consistent relationship between the pro andcon opinions in various questions concerning euthanasiaand assisted suicide and demographic factors was thatconcerning religion. In fact, there were very significantdifferences between practising and non-practising Catho-lics. This may result from the fact that in Portugal mostpeople have been christened and have had a Catholiceducation, and so they see themselves as Catholic, that is,
Table 7 Assisted suicide
Questions Total Yes (%) No (%) I do not have adefinite opinion(%)
Practising vs.non-practisingCatholic p
Portuguese legislation does not permit the practise of assistedsuicide. Even so, are there any circumstances in which you wouldpractise it?
142 21 (14.8) 105 (73.9) 16 (11.3) 0.001
If legislation allowed the practise of assisted suicide, would youpractise it?
143 36 (25.4) 89 (62.7) 17 (12.0) 0.005
Do you think that assisted suicide should be permitted byPortuguese law?
142 45 (31.9) 73 (51.8) 23 (16.3) 0.001
If you had an incurable and progressive disease, which inexorablyled to death, would you like to have the available option of assistedsuicide?
143 34 (23.8) 72 (50.3) 37 (25.9) 0.005
364 Support Care Cancer (2010) 18:359–366

| 251 251Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
191
they are inserted into Catholic culture and tradition, butthey do not show firmness in their convictions, so theyconsider themselves as “non-practising Catholics”. Theresult of this is that, probably, people adopt positions thatare against those usually accepted by convinced Catholics,namely the moral doctrine of the Catholic Church. Theinfluence of religion on these issues seems to be veryimportant and was also observed in other studies. InOregon, the variables significantly associated with thewillingness to participate in assisted suicide included theJewish affiliation, no religious affiliation and other non-Christian affiliations; whereas the unwillingness to partic-ipate in assisted suicide was a Catholic affiliation or otherChristian affiliation [1]. In a study in Washington, religiousbeliefs were also a reason for being against euthanasia andassisted suicide [22]. In another study, the Catholics and the“very religious” were less likely to desire that euthanasia orassisted suicide be performed on themselves [18]. However,in a study conducted by the German Association forPalliative Medicine religious convictions did not play asignificant role in the decision-making process [19]. In thisstudy, however, the rate of positive responses, 9.6%, wasvery low reflecting the common position of palliative carephysicians who are usually against assisted death [16].
It was also observed that the over 65 years age groupopposed euthanasia and assisted suicide more often thanother age groups. The finding that older doctors morefrequently oppose assisted death than younger ones iscommon in studies on these issues [20, 21]. Perhaps thisassociation is due to their education, which was at a timewhen the ethical principle that dominated all others wasundoubtedly beneficence, and when the doctors’ attitude topatients was mainly paternalistic. The primacy of therespect for autonomy is more recent, with the possibleextension of the concept to include the right to choose theway of dying.
In general, the answers that reveal more indecision werethose concerning the option for euthanasia or assistedsuicide by the doctors themselves if they had a terminaldisease. This suggests that it is more difficult to decide intheir own cause than when the decision concerns others.
It seems that the problems concerning euthanasia aremore relevant among both doctors and patients, taking intoconsideration the number of requests indicated by doctors,than those related to assisted suicide. Maybe this is becauseeuthanasia has more visibility. In fact, in Portugal, the fewdiscussions on assisted death are usually limited toeuthanasia.
The Portuguese oncologists looked very positively onthe value of palliative care in responding to the problems ofpatients with advanced chronic diseases and its potential inpreventing many requests for assisted death. This is a veryimportant and encouraging aspect for the development of
palliative care in a country where only a few teams areworking in this field.
An important potential limitation of this study is the lowpercentage of questionnaires received. It was lower thanthat of studies with similar questions carried out in othercountries [1, 2, 5, 17, 18]. However, it is higher than thatusually observed in studies carried out in Portugal usingquestionnaires sent by mail to doctors [24]. The meaning ofthis is unknown, but it does indicate general disinterest bythe Portuguese public and Portuguese doctors in surveys. Infact, there are other examples of studies with even lowerreply percentages [24]. The sensitivity of the topic couldmake some fear for being identified and their opinions andpractises being made public, even if anonymity wasguaranteed in the cover letter sent together with thequestionnaire. Or does it mean that there is no reflectionon these issues? It is probably a combination of factors.Some of those factors identified above were associated to alower percentage of replies, although the results are notcompletely consistent—these factors being related to thedoctors’ population, the inquiry being anonymous or thesensitivity of the theme [25, 26]. However, so long as thenumber of replies is sufficiently high to perform statisticalanalysis, the only problem that exists is if those who did notreply were significantly different to those who did.Therefore, although a low rate of replies increases theprobability of bias, there is not necessarily an associationbetween the reply rate and bias [26]. In this study, only thedistribution of females by age groups was significantlydifferent in regards to those who responded and those whodid not. Even so, the results can be deemed non-representative of the opinion of the population studied.However, this is the best approach made until nowregarding the opinion of Portuguese oncologists on eutha-nasia and assisted suicide and we believe that these resultsdeserve consideration.
Conclusion
Most Portuguese oncologists are against assisted death. Inparallel, there seems to be a reduced number of requests forassisted death, based on the physicians’ answers. Positiveresponses to requests for assisted death seem to be quiterare. Portuguese oncologists value the potentially positiverole of palliative care in the treatment of patients withincurable and advanced chronic diseases thereby preventingat least many cases of requests for assisted death. Religiongreatly influences the attitudes of Portuguese oncologists asregards their opinions on assisted death.
Acknowledgements I would like to thank Prof. Rui Nunes, as advisorof the Master’s Degree in Bioethics from where this work was extracted;
Support Care Cancer (2010) 18:359–366 365

252 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
192
Prof. Henrique de Barros and Dr. Joselina Barbosa and Dr. Milton Severofrom the Epidemiology Service of the Faculty of Medicine of PortoUniversity for their help in data extraction and statistical analysis; HelgaKuhse, Frederich Stiefel, David Doukas and Diane Meier for makingavailable the questionnaires used in their studies; and The PortugueseLeague against Cancer for funding the study.
References
1. Lee MA, Nelson HD, Tilden VP, Ganzini L, Schmidt TA, Tolle SW(1996) Legalizing assisted suicide—views of physicians in Oregon.N Engl J Med 334:310–315. doi:10.1056/NEJM199602013340507
2. Back AL, Wallace JI, Starks HE, Pearlman RA (1996) Physician-assisted suicide and euthanasia in Washington state: patientrequests and physician responses. JAMA 275:919–925.doi:10.1001/jama.275.12.919
3. Emanuel EJ, Fairclough D, Clarridge BC et al (2000) Attitudesand practices of U.S. oncologists regarding euthanasia andphysician-assisted suicide. Ann Intern Med 133:527–532
4. van der Maas PJ, Van Delden JJM, Pijnenborg L, Looman CWN(1991) Euthanasia and other medical decisions concerning the endof life. Lancet 338:669–674. doi:10.1016/0140-6736(91) 91241-L
5. Kuhse H, Singer P, Baume P, Clark M, Rickard M (1997) End-of-life decisions in Australian medical practice. MJA 166:191–196
6. Deliens L, Mortier F, Bilsen J, Cosyns M, Stichele RV,Vanoverloop J, Ingels K (2000) End-of-life decisions in medicalpractice in Flanders, Belgium: a nationwide survey. Lancet356:1806–1811. doi:10.1016/S0140-6736(00) 03233-5
7. Mitchell K, Owens G (2003) National survey of medical decisionsat end of life made by New Zealand general practitioners. BMJ327:202–203. doi:10.1136/bmj.327.7408.202
8. CombyMC, Filbert M (2005) The demand for euthanasia in palliativecare units: a prospective study in seven units of the “Rhône-Alpes”region. Palliat Med 19:587–593. doi:10.1191/0269216305pm1081oa
9. Førde R, Aasland OG, Falkum E (1997) The ethics of euthanasia—attitudes and practice among Norwegian physicians. Soc SciMed 45:887–892. doi:10.1016/S0277-9536(96) 00430-3
10. van der Heide A, Deliens L, Faisst K, Nilstun T, Norup M, Paci E,van der Wal G, van der Maas PJ (2003) End-of-life decision-making in six European countries: descriptive study. Lancet362:345–350. doi:10.1016/S0140-6736(03) 14019-6
11. Seale C (2006) National survey of end-of-life decisions made byUK medical practitioners. Palliat Med 20:3–10. doi:10.1191/0269216306pm1094oa
12. Bittel N, Neuenschwander H, Stiefel F (2002) "Euthanasia": asurvey by the Swiss Association for Palliative Care. Support CareCancer 10:265–271. doi:10.1007/s00520-001-0325-0
13. Doukas DJ, Waterhouse D, Gorenflo DW, Seid J (1995) Attitudesand behaviours on physician-assisted death: a study of Michiganoncologists. J Clin Oncol 13:1055–1061
14. Meier DE, Emmons CA, Wallenstein S, Quill T, Morrison RS,Cassel CK (1998) A national survey of physician-assisted suicideand euthanasia in the United States. N Engl J Med 338:1193–1201. doi:10.1056/NEJM199804233381706
15. Masterstvedt LJ, Kaasa S (2002) Euthanasia and physician-assisted suicide in Scandinavia—with a conceptual suggestionregarding international research in relation to the phenomena.Palliat Med 16:17–32. doi:10.1191/0269216302pm470oa
16. Gielen J, van der Branden S, Broeckaert B (2008) Attitudesof European physicians toward euthanasia and physician-assisted suicide: a review of the recent literature. J PalliatCare 24:173–184
17. van der Maas PJ, van der Wal G, Haverkate I et al (1996)Euthanasia, physician-assisted suicide, and other medical practicesinvolving the end of life in the Netherlands, 1990–1995. N Engl JMed 335:1699–1705. doi:10.1056/NEJM199611283352227
18. Howard OM, Fairclough DL, Daniels R, Emanuel EJ (1997)Physician desire for euthanasia and assisted suicide: wouldphysicians practise what they preach? J Clin Oncol 15:428–432
19. Müller-Busch HC, Oduncu FS, Woskanjan S, Klaschik E (2004)Attitudes on euthanasia, physician-assisted suicide and terminalsedation—a survey of the members of the German Association forPalliative Medicine. Med Health Care Philos 7:333–339.doi:10.1007/s11019-004-9349-9
20. Miccinesi G, Fisher S, Paci E et al (2005) Physicians’ attitudestowards end-of-life decisions. A comparison between sevencountries. Soc Sci Med 60:1961–1974. doi:10.1016/j.socs-cimed.2004.08.061
21. Ryynänen O-P, Myllykangas M, Viren M, Heino H (2002)Attitudes towards euthanasia among physicians, nurses and thegeneral public in Finland. Public Health 116:322–331.doi:10.1016/S0033-3506(02) 00556-5
22. Cohen JS, Fihn SD, Boyko EJ, Jonsen AR, Wood RW (1994)Attitudes toward assisted suicide and euthanasia among physi-cians in Washington state. N Engl J Med 331:89–94
23. Pasterfield D, Wilkinson C, Finlay IG, Neal RD, Hulbert NJG(2006) P’s views on changing the law on physician-assistedsuicide and euthanasia, and willingness to prescribe or inject lethaldrugs: a survey from Wales. Br J Gen Pract 56:450–452
24. INFARMED Informação científica sobre medicamentos: relatório.[Scientific information on medicaments: report] http://www.i n f a r m e d . p t / p o r t a l / p a g e / p o r t a l / I N FA R M E D /MONITORIZACAO_DO_MERCADO/OBSERVATORIO/INTRODUCAO_DE_FICHEIROS/ICM_rel_preliminar.pdf(accessed in April 2007).
25. Edwards P, Roberts I, Clarke M, DiGuiseppi C, Pratap S, WentzR, Kwan I (2002) Increasing response rates to postal question-naires: systematic review. BMJ 324:1183–1185. doi:10.1136/bmj.324.7347.1183
26. Asch DA, Jedrziewski K, Christakis NA (1997) Response rates tomail surveys published in medical journals. J Clin Epidemiol50:1129–1136. doi:10.1016/S0895-4356(97) 00126-1
366 Support Care Cancer (2010) 18:359–366

| 253 253Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
193
ORIGINAL ARTICLE
Attitudes toward end-of-life situations other than euthanasiaand assisted suicide among Portuguese oncologists
José António Ferraz Gonçalves
Received: 10 January 2009 /Accepted: 10 September 2009 /Published online: 6 October 2009# Springer-Verlag 2009
AbstractBackground The aim of this study was to determine theattitude of Portuguese oncologists toward end-of-lifesituations other than euthanasia and assisted suicide.Methods This study used a survey of 450 Portugueseoncologists by postal means and personal contact.Main results The response rate was 33% (143). Only 7.7%doctors would give lethal doses of drugs to someone withan incurable, advanced, and progressive disease that isunable to make decisions, at the request of a family memberor other close person. However, 30 doctors (21.3%) wouldprefer, in the event they were in such a situation, that thedrugs be given them at their request. None of the 12.4%who have received such requests admitted to committingany of those acts. Almost 70% of the doctors wouldwithdraw life support measures at the patient's request if thesame had an incurable, advanced, and progressive disease,and a further 14% would do it in certain circumstances, butonly 41% would withdraw measures such as nutrition andhydration. Fewer doctors would withdraw such measuresincluding nutrition and hydration at a family member'srequest or on their own initiative. Religion has a majorinfluence on the doctors' opinion. Most doctors (96.5%)agreed with the administration of drugs for symptomcontrol even foreseeing that they could shorten life.Conclusion Most Portuguese oncologists respect patients'autonomy, favoring the withdrawal of life support treatmentat the patients' request when appropriate and much less doso on the request of others or by their own initiative. They
appropriately do not confuse those practices with symptomrelief even when hastened death can be envisaged.
Keywords End-of-life decisions . Life-terminating actswithout explicit request of patient . Treatment withdrawal .
Symptom control
The most discussed end-of-life issues are probably euthana-sia and assisted suicide. However, doctors, patients, andfamilies face many other situations requiring difficultdecisions. Examples of those are decisions about withhold-ing and withdrawing life-supporting treatments at thepatient's request or, if the patient is not competent, how torespond to eventual requests by family members and whetheror not a doctor or a healthcare team can decide unilaterally.Should nutrition and hydration be considered as treatment oras basic care, that is, may they be withheld or withdrawn incertain circumstances, or never? There are also issuesconcerning the provision of lethal doses of drugs to terminatethe life of patients without their explicit request, also referredto as involuntary or nonvoluntary euthanasia depending onwhether the patient is competent or not, although thisdesignation is not appropriated because euthanasia impliesa patient's request. Other issues are the administration ofdrugs to relieve suffering, even when this carries thepossibility of shortening life, and palliative sedation. Allthose situations sometimes generate difficult decisions, andhealth professionals should have clear perception in relationto those issues. The withholding or withdrawing of life-prolonging treatments or symptom control in a terminalpatient even if death can be foreseen are, in the appropriatecircumstances, legitimate acts that must be accomplished.
Those acts are of a completely different nature toeuthanasia or assisted suicide because they are intended to
J. A. F. Gonçalves (*)Instituto Português de Oncologia, UCP-R,Rua Dr. António Bernardino de Almeida,4200-072 Porto, Portugale-mail: [email protected]
Support Care Cancer (2010) 18:1271–1277DOI 10.1007/s00520-009-0743-y

254 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
194
relieve suffering or avoid prolonging the process of dyingrather than directly causing the patient's death. Manydoctors use the argument of the principle of double effectto justify such actions and separate them from euthanasia.This implies, as far as medicine is concerned, that a doctorcan make a correct action even if he/she foresees that a badconsequence can also occur without being his/her intention,if there is no other alternative. However, the issue ofintentions is problematic because they cannot be objectivelyevaluated. Therefore, in my view, there is no need to invokethe principle of double effect to justify acts like withholdingor withdrawing treatments or symptom control in a terminalpatient even if death can be foreseen. The problem shouldbe defined in terms of the adequacy of the means used, afterthe evaluation of the benefits to and burdens on the patientand the patient's will.
Those issues have been studied in several countries [1–5]. For example, in Holland, in a famous study sponsoredby the Dutch government [2] on acts that terminate life, itwas observed that the administration of drugs in lethaldoses without explicit request from the patients occurred in0.8% of all deaths. In a deeper analysis made laterregarding the circumstances surrounding those cases, 27%of the doctors answered that they had carried out one ofthose acts at least once and 32% had never done it butcould imagine a situation where they might. According tothose doctors, in almost all cases, the patient was sufferingunbearably with no possibility of improvement, as thepossibilities of palliation had been exhausted. The authorsof that study hold the view that such acts can be a responseto the injustice of a patient's situation, when he/she isunable to make an explicit request, thereby having to sufferto the end when their doctors, who may have beenresponsible for treatment for a long time, and their familiesagree on the termination of their life, in a country whereeuthanasia is usually not punished; they add that thelifetime shortened by such a practice is usually lower thanthat related to euthanasia. On the other hand, such acts canbe seen as homicide and they illustrate the slippery slopethat would emerge if euthanasia were accepted. As anotherexample, in an Australian study, 6.4% of the doctors statedthat they had terminated the life of patients without theirexplicit request [1]. In this study, not all patients wereincompetent, and some doctors declared that “discussionwould have done more harm than good.” This is a strangeway of thinking because it means that discussing theproblem with the patients is more harmful than killingthem.
The law and the practices regarding end-of-life issues arechanging, namely, in Europe and the United States, withgreater openness towards assisted death. In Portugal, end-of-life problems have not deserved much attention instudies. However, it is important to know what doctors
think and feel about them and consequently what they do,as was the case in other countries. Doctors of somespecialties, such as oncologists, are faced with thoseproblems in their everyday practice, so they are particularlywell suited to explore such questions.
The data presented in this paper are part of anexploratory study that also included questions on euthana-sia and assisted suicide, the results of which were presentedin a separate paper [6].
Methods
The questionnaire was developed for this study partiallybased on other published papers kindly sent to me at myrequest by the authors [1, 7–9]. After the design of thequestionnaire, it was submitted to face validation by 15doctors, mainly oncologists. They were asked to completethe questionnaire and comment on the relevance andcoherence of the questions and also suggest any necessaryalterations. Minor alterations were made when consideredpertinent, according to those suggestions.
The questionnaires were sent by mail to the 408 doctorsbelonging to the Portuguese Society of Oncology (PSO)included on a list provided by the board of that society andto 42 oncologists not belonging to the PSO and whosepositions on these issues were not publicly known. Themembers of the PSO received the questionnaire with a letterexplaining the reasons and the importance of the study andassuring the anonymity of replies by mail; a prepaidenvelop without any code or other means of identifyingthe person replying was also included. Three weeks later, anew letter was sent to all doctors asking those who had stillnot replied to please do so. The other oncologists werepersonally invited to fill in the questionnaire. They wereprovided with a questionnaire, letter, and prepaid envelopidentical in every way to those that had previously beensent by mail. Three weeks later, they were contacted againand asked to complete the questionnaire if they had notalready done so.
The questionnaires contained questions concerning de-mographic data, administration of drugs to incompetentpatients, withdrawal of life support treatments includingfeeding and nutrition, and symptom control with the risk ofhastened death. Questions on euthanasia and assistedsuicide issues were included in the questionnaire, but theywere presented in another paper.
This study was approved by the Bioethics Service of theFaculty of Medicine of Porto University.
An initial analysis was performed for statistical proposesin order to identify coding errors, inconsistencies, and thepresence of missing categories or small numbers, andcorrections where made where needed. An exploratory
1272 Support Care Cancer (2010) 18:1271–1277

| 255 255Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
195
analysis of the data was performed so as to describe thesample. The variables were analyzed by graphical methods,proportions, and means. To evaluate the existence or not ofassociations between categorical variables, the chi-squaretest was used. The level of significance was deemed to be0.05. The Statistical Package for Social Sciences (SPSS)version 14.0 statistical software was used to analyze thedata.
Results
From the total of 450 questionnaires sent out, 12 werereturned because the doctors concerned had either movedhouse or died. Of the remaining 438 questionnaires, 143(33%) were sent back filled in. Table 1 shows thedemographic data of the doctors who returned the ques-tionnaire. These have been filled in a careful and consistentmanner. There was not much missing data, but religion wasthe variable most frequently omitted. Even so, 132 (92%)reported their religion. Of those, 126 (96%) were Catholicand 121 of them declared themselves to be practicing ornonpracticing Catholics. Therefore, in the analysisconcerning religion, only this group of 121 were consideredbecause the others groups were too small.
The age and gender of 80% of the doctors that did notreply were known. The comparison by gender of those whoreplied with those who did not was as follow: females 51(35.1%) vs. 80 (32.5%); males 91 (64.1%) vs. 166 (68%).These differences were not significant (p=0.49). Thedistribution of gender by age groups can be seen in Table 2.Only the difference among the age groups of femaledoctors was significant with the youngest responding moreoften.
Incompetent patients
All the opinions about giving lethal doses of drugs toincompetent patients were favored only by a small minorityof doctors. Only 11 doctors (7.7%) would give lethal dosesof one or more drugs to someone with an incurable,advanced, and progressive disease unable to make deci-sions, at the request of a family member or other closeperson. However, 30 doctors (21.3%) would prefer, in theevent that they were in such a situation, that the drugs weregiven to them at the request of a family member or otherclose person (Table 3); but there were also more doctorswithout an opinion in relation to this hypothetical situation.Twelve doctors (8.4%) have received that type of requestand four of them had received between one and threerequests in the previous year. No doctor committed any ofthose acts. However, 24 doctors (17.3%) favored that thoseacts should be permitted by legislation.
In the similar question on drugs' administration, thoughby the doctors' initiative, there were more affirmativeanswers to the hypothesis of the doctor personally beingin that situation than to the doctor having to do such to apatient. Once again, there were more doctors without anopinion in the event that the doctor is personally in thatsituation, although the difference is not statistically signif-icant (Table 3). However, the number of positive answerswas lower than in the scenario of drugs given on request.Also, no doctor has committed any one of those acts.Nineteen (13.5%) were of the opinion that those acts shouldbe permitted by legislation.
In those questions, statistically significant differencesbetween doctors in different work places were observed,
Table 1 Demographic data
Total Number Percentage
Age (years) 142
31–45 50 35.2
46–65 69 48.6
>65 23 16.2
Gender 142
Female 51 35.9
Male 91 64.1
Marital status 142
Married/common-law partnership 124 87.3
Living alone 18 12.7
Religion 132
Catholic 126 95.5
Agnostic 4 3.0
Atheist 2 1.5
Catholics 121
Nonpracticing 66 54.5
Practicing 55 45.5
Main specialty 143
Surgery 59 41.3
Medical oncology 54 37.8
Radiotherapy 20 14.0
Other 10 7.0
Working place 142
Institute of Oncology 82 57.7
Hospital 37 26.1
Other 23 16.2
Region 141
Large city 123 87.2
Other 18 12.8
How many people with terminaldiseases do you see per year?
141
0–5 32 22.7
6–30 54 38.3
>30 55 39.0
Support Care Cancer (2010) 18:1271–1277 1273
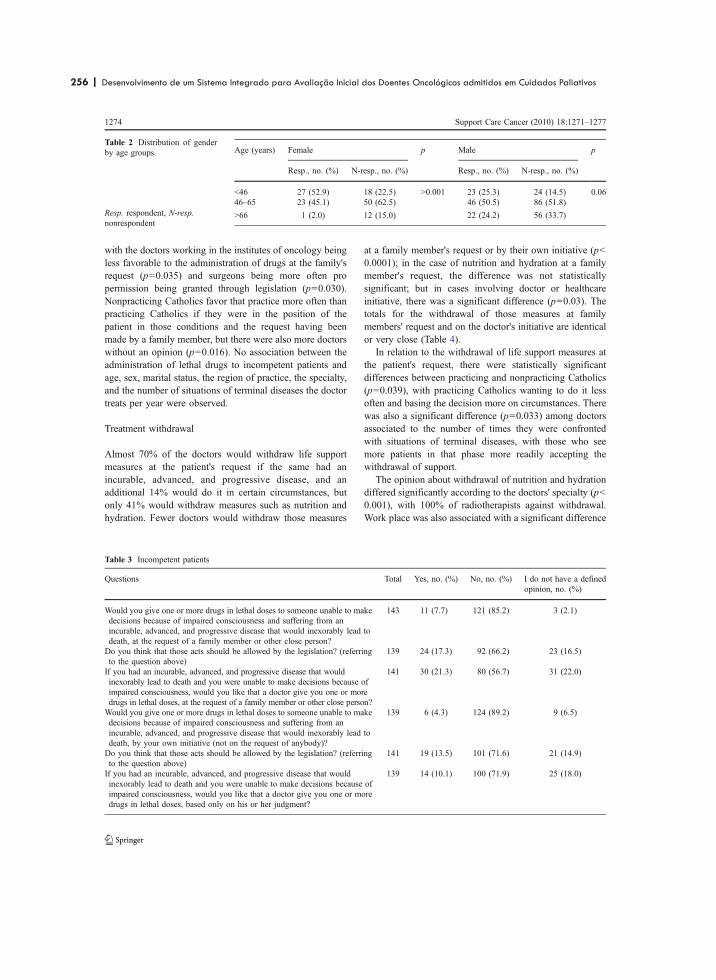
256 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
196
with the doctors working in the institutes of oncology beingless favorable to the administration of drugs at the family'srequest (p=0.035) and surgeons being more often propermission being granted through legislation (p=0.030).Nonpracticing Catholics favor that practice more often thanpracticing Catholics if they were in the position of thepatient in those conditions and the request having beenmade by a family member, but there were also more doctorswithout an opinion (p=0.016). No association between theadministration of lethal drugs to incompetent patients andage, sex, marital status, the region of practice, the specialty,and the number of situations of terminal diseases the doctortreats per year were observed.
Treatment withdrawal
Almost 70% of the doctors would withdraw life supportmeasures at the patient's request if the same had anincurable, advanced, and progressive disease, and anadditional 14% would do it in certain circumstances, butonly 41% would withdraw measures such as nutrition andhydration. Fewer doctors would withdraw those measures
at a family member's request or by their own initiative (p<0.0001); in the case of nutrition and hydration at a familymember's request, the difference was not statisticallysignificant; but in cases involving doctor or healthcareinitiative, there was a significant difference (p=0.03). Thetotals for the withdrawal of those measures at familymembers' request and on the doctor's initiative are identicalor very close (Table 4).
In relation to the withdrawal of life support measures atthe patient's request, there were statistically significantdifferences between practicing and nonpracticing Catholics(p=0.039), with practicing Catholics wanting to do it lessoften and basing the decision more on circumstances. Therewas also a significant difference (p=0.033) among doctorsassociated to the number of times they were confrontedwith situations of terminal diseases, with those who seemore patients in that phase more readily accepting thewithdrawal of support.
The opinion about withdrawal of nutrition and hydrationdiffered significantly according to the doctors' specialty (p<0.001), with 100% of radiotherapists against withdrawal.Work place was also associated with a significant difference
Age (years) Female p Male p
Resp., no. (%) N-resp., no. (%) Resp., no. (%) N-resp., no. (%)
<46 27 (52.9) 18 (22.5) >0.001 23 (25.3) 24 (14.5) 0.0646–65 23 (45.1) 50 (62.5) 46 (50.5) 86 (51.8)
>66 1 (2.0) 12 (15.0) 22 (24.2) 56 (33.7)
Table 2 Distribution of genderby age groups
Resp. respondent, N-resp.nonrespondent
Table 3 Incompetent patients
Questions Total Yes, no. (%) No, no. (%) I do not have a definedopinion, no. (%)
Would you give one or more drugs in lethal doses to someone unable to makedecisions because of impaired consciousness and suffering from anincurable, advanced, and progressive disease that would inexorably lead todeath, at the request of a family member or other close person?
143 11 (7.7) 121 (85.2) 3 (2.1)
Do you think that those acts should be allowed by the legislation? (referringto the question above)
139 24 (17.3) 92 (66.2) 23 (16.5)
If you had an incurable, advanced, and progressive disease that wouldinexorably lead to death and you were unable to make decisions because ofimpaired consciousness, would you like that a doctor give you one or moredrugs in lethal doses, at the request of a family member or other close person?
141 30 (21.3) 80 (56.7) 31 (22.0)
Would you give one or more drugs in lethal doses to someone unable to makedecisions because of impaired consciousness and suffering from anincurable, advanced, and progressive disease that would inexorably lead todeath, by your own initiative (not on the request of anybody)?
139 6 (4.3) 124 (89.2) 9 (6.5)
Do you think that those acts should be allowed by the legislation? (referringto the question above)
141 19 (13.5) 101 (71.6) 21 (14.9)
If you had an incurable, advanced, and progressive disease that wouldinexorably lead to death and you were unable to make decisions because ofimpaired consciousness, would you like that a doctor give you one or moredrugs in lethal doses, based only on his or her judgment?
139 14 (10.1) 100 (71.9) 25 (18.0)
1274 Support Care Cancer (2010) 18:1271–1277

| 257 257Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
197
(p=0.027), with doctors of the institutes of oncology beingmore often against withdrawal of nutrition and hydrationthan doctors from other hospitals, but this may be due to theinfluence of the radiotherapists because they are concen-trated in those institutes; doctors from other work placeswere the least in favor. There was no relationship betweenwithdrawal of life support, namely, nutrition and hydration,and age, gender, marital status, and the region of practice.
The withdrawal of life support at the request of familiesor another close person is associated with a significantdifference in relation to specialties (p=0.040), with 75% ofradiotherapists against the withdrawal under those circum-stances. That difference increases in regard to nutrition andhydration withdrawal, with 100% of radiotherapists an-swering no (p=0.003). In relation to withdrawal by thedoctor or on the health team's initiative, there are nosignificant differences, except in what concerns nutritionand hydration, with practicing Catholics being more oftenagainst (p=0.009) and, again, 100% of radiotherapists alsoagainst it (p=0.013).
Symptom control
As regards the question of the administration of drugs forsymptom control even foreseeing that they could shortenlife, 138 (96.5%) agreed with it, four admitted it in certaincircumstances, one had no opinion, but none answerednegatively. And on the hypothesis of the doctor being inthat suffering situation, 100% would like for someone toadminister a drug that would relieve their suffering even ifit could shorten their lives.
Discussion
It seems that there is a broad consensus among Portugueseoncologists as regards the questions on incompetentpatients included in this study. Only a few doctors wouldgive drugs in lethal doses to an incompetent patient at thefamily' request; and even less would give them on theirown initiative. Although some of them had received thoserequests, not one doctor did so. A few more, but even soonly a few, favored the legalization of these kinds of acts.
The questions concerning what doctors would want ifthey were in the patients' position are those that mostfrequently had “no opinion” answers. As it happens, on theother hand, many more doctors would like drugs to beadministered to them at their family's request than thosewho would do it to their patients, suggesting that somedoctors would want, in regard to themselves, that otherstake a decision, the responsibility for which they are notprepared to take. A much lower number would like thedecision to be taken unilaterally by a doctor, suggesting thatthey fear the possibility of abuse.
A small minority agree with the legalization of thoseacts, which are now legal in Holland [10]. This is anevolution of the Dutch law once again interpreted by manyas proof of the slippery slope that is created through thevery significant danger of the legalization of assisted death.
The vast majority of oncologists agree with the with-drawal of life support treatment at the patient's request,under the circumstances defined in the questionnaire,although they agreed less often when the questions wereabout withdrawing feeding and hydration. Probably, most
Table 4 Treatment withdrawal
Question Total Yes, no. (%) No, no. (%) In certain circumstances,no. (%)
Do you think that in relation to someone with an incurable, advanced, andprogressive disease that would inexorably lead to death, it is legitimate towithdraw support of life measures at his or her explicit, repeated,informed, and well-pondered request?
142 95 (66.9) 27 (19.0) 20 (14.1)
Would you withdraw measures such as feeding and hydration? (referringto the question above)
142 58 (40.8) 84 (59.2)
Do you think that in relation to someone with an incurable, advanced, andprogressive disease that would inexorably lead to death, who is unable tomake decisions because of impaired consciousness, it is legitimate towithdraw support of life measures at the request of a family member orother close person?
142 52 (36.6) 66 (46.5) 24 (16.9)
Would you withdraw measures such as feeding and hydration? (referringto the question above)
141 44 (31.2) 97 (68.8)
Do you think that in relation to someone with an incurable, advanced, andprogressive disease that would inexorably lead to death, who is unable tomake decisions because of impaired consciousness, it is legitimate towithdraw support of life measures by the unilateral decision of the doctoror the healthcare team?
143 52 (36.6) 66 (46.2) 25 (17.5)
Would you withdraw measures such as feeding and hydration? (referringto the question above)
136 39 (28.7) 97 (71.3)
Support Care Cancer (2010) 18:1271–1277 1275

258 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
198
of those see feeding and hydration as basic care and not astreatments. However, in regard to the withdrawal of thosetreatments at the families' request or by the doctor's owninitiative, the number of positive answers was identical butmuch lower than when it was at the patient's request.Therefore, it seems that doctors effectively respect patients'autonomy and that many think that others, namely, them-selves, do not have the legitimacy to make those decisions.Here again, the fear of abuse may have played a role.
In an Australian study [1], 36% of doctors said that theyhad already taken a decision to withhold or withdrawtreatments, 81% with the explicit intention of hasteningdeath. This is a dubious statement because when lifesupport treatments are withheld or withdrawn it is predict-able that death occurs sooner, but it is appropriate in certaincircumstances. Therefore, the problem of intention is anequivocal one. Once again, the problem should be put onthe adequacy of the means used, after the evaluation of thebenefits and burdens to the patient and the patient's will.
Religion was the factor that most consistently influences theanswers on incompetent patients and the withdrawal of treat-ments, with practicing Catholics opposing more those acts thannonpracticing Catholics. In a country where most physicianshave been christened and have had a Catholic education, and sothey say they are Catholics, many, in particular the nonpractic-ing Catholics, probably do not have firm convictions. Physi-cians' religiosity is a factor that has been consistently observedin various studies as related with their opinions and attitudesregarding end-of-life issues [11–14].
The difference between areas of specialty was curious,particularly in relation to radiotherapy, and the 100% thatwere against the withdrawal of feeding and hydration. Thereasons for this difference are not clear, but we canspeculate that doctors of that specialty probably accompanypatients near the end of life less often, so they do not facethese problems in this phase. This hypothesis seems to besupported by the observation that doctors who morefrequently face such situations more often favor thewithdrawal of life support treatment.
Almost all oncologists would give a drug for symptomrelief even if they foresaw that life could be shortened. Intheir own case, all would like for the drugs to be given tothem. Therefore, there were no doubts on this issue and noconfusion with other acts as regards giving drugs with theexplicit or implicit aim of killing the patient. In otherstudies [1, 3], some doctors who gave drugs for symptomrelief had the partial intention of hastening death. However,in one of those studies [3], the relatively low doses ofopioids and the high number of patients who were onopioids before made the authors raise doubts whether thedoctors were correct in attributing death-hastening effects totheir practices. The authors comment further that unfound-ed concerns may have resulted in less than optimal
symptom management in the care of those dying patients[3]. This is a very important topic because at the end of lifethe primary role of physicians is to control patients'suffering. Therefore, the right drugs in the right dosesshould be given in order to control that suffering, even ifthe doctor fears that there is a risk of death. Once again, it isthe balance of benefits and burdens and the patient's willthat should govern our acts.
Taking all the results together, the logical conclusion isthat Portuguese oncologists have clear concepts about end-of-life issues. Almost all are against the administration ofdrugs in lethal doses to incompetent patients. On the otherhand, they are prepared to withdrawal life support measuresat the request of a patient with an incurable, advanced, andprogressive disease. They are also prepared to administerdrugs for symptom control even when foreseeing that theycould shorten life. Therefore, it seems that there is noconfusion at all with the concepts. In relation to thewithdrawal of artificial nutrition and hydration, there is alarger division among doctors, but this is also a morecontroversial issue.
About 60% of doctors accompany less than 30 terminalpatients per year. The doctors included in this study aremedical oncologists, surgeons, and radiotherapists and,although they accompany many patients, surgeons andradiotherapists usually only assist a few in the terminalphase. In this phase, medical oncologists are the doctorswho treat most patients. Even so, the contact of doctorsworking in oncology with the reality of patients with faradvanced disease is a frequent event.
A potential limitation of this study is the low percentageof questionnaires received. It was lower than that of studiesin other countries [1, 3, 15–17], but the percentage is notlow compared to the universe of other studies performed inPortugal [18]. However, so long as the number is highenough to perform statistical analysis, the only problemthat exists is if those who did not reply are significantlydifferent from those who did. Therefore, although a lowrate of replies increases the probability of bias, there is notnecessarily an association between the reply rate and bias[19]. In this study, only the distribution of females by agegroups was significantly different between those whoreplied and those who did not. Therefore, we believe that,even with a low rate of replies, these results deserveconsideration and these are the only data collected untilnow regarding the opinion of Portuguese oncologists aboutend-of-life issues.
Conclusion
Most Portuguese oncologists favor the withdrawal of lifesupport treatments at the patients' request but much less do
1276 Support Care Cancer (2010) 18:1271–1277

| 259 259Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
199
so on the request of others or by their own initiative.However, many of those do not favor the withdrawal offeeding and hydration, probably because they see them asbasic care. The majority is against the administration ofdrugs in lethal doses to incompetent patients and they donot confuse those practices with symptom relief, even whenhastened death can be possible. Religion is the factor thatmost influences the attitudes of Portuguese oncologists inrelation to end-of-life decisions.
Acknowledgements I would like to thank Prof. Rui Nunes, as advisorof the Master's Degree in Bioethics from where this work was extracted;Prof. Henrique de Barros, Dr. Joselina Barbosa, and Dr. Milton Severofrom the Epidemiology Service of the Faculty of Medicine of PortoUniversity for their help in data extraction and statistical analysis; HelgaKuhse, Frederich Stiefel, David Doukas, and Diane Meier for makingavailable the questionnaires used in their studies; and the PortugueseLeague against Cancer for funding the study.
References
1. Kuhse H, Singer P, Baume P, Clark M, Rickard M (1997) End-of-life decisions in Australian medical practice. Med J Aust166:191–196
2. Pijnenborg L, van der Maas PJ, van Delden JJ, Looman CWN(1993) Life-terminating acts without explicit request of patients.Lancet 341:1196–1199
3. Bilsen J, Norup M, Delians L et al (2006) Drugs to alleviatesymptoms with life shortening as a possible side effect: end-of-lifecare in six European countries. J Pain Symptom Manage 31:111–121
4. van der Heide A, Deliens L, Faisst K, Nilstun T, Norup M, Paci E,van der Wal G, van der Maas PJ, on behalf of the EURELDconsortium (2003) End-of-life decision-making in six Europeancountries: descriptive study. Lancet 362:345–350
5. Buiting HM, van Delden JM, Rietjens AC, Onwuteaka-PhilipsenBD, Bielsen J, Fischer S, Löfmark R, Miccinesi G, Norup M, vander Heide A, on behalf of the EURELD-Consortium (2007) J PainSymptom Manage 34:305313
6. Gonçalves F (2009) Attitudes toward assisted death amongstPortuguese oncologists. Support Care Cancer (in press)
7. Bittel N, Neuenschwander H, Stiefel F (2002) “Euthanasia”: asurvey by the Swiss Association for Palliative Care. Support CareCancer 10:265–271
8. Doukas DJ, Waterhouse D, Gorenflo DW, Seid J (1995) Attitudesand behaviours on physician-assisted death: a study of Michiganoncologists. J Clin Oncol 13:1055–1061
9. Meier DE, Emmons CA, Wallenstein S, Quill T, Morrison RS,Cassel CK (1998) A national survey of physician-assisted suicideand euthanasia in the United States. N Engl J Med 338:1193–1201
10. Englert Y (2004) Belgium—evolution of the debate. Em:Euthanasia. Volume II. National and European perspectives.Council of Europe Publishing, Strasbourg, pp 13–24
11. Lee MA, Nelson HD, Tilden VP, Ganzini L, Schmidt TA, TolleSW (1996) Legalizing assisted suicide—views of physicians inOregon. N Engl J Med 334:310–315
12. Cohen JS, Fihn SD, Boyko EJ, Jonsen AR, Wood RW (1994)Attitudes toward assisted suicide and euthanasia among physi-cians in Washington state. N Engl J Med 331:89–94
13. Howard OM, Fairclough DL, Daniels R, Emanuel EJ (1997)Physician desire for euthanasia and assisted suicide: wouldphysicians practice what they preach? J Clin Oncol 15:428–432
14. Wenger NS, Carmel S (2004) Physicians' religiosity and end-of-life care attitudes and behaviours. Mt Sinai J Med 71:335–343
15. Back AL, Wallace JI, Starks HE, Pearlman RA (1996) Physician-assisted suicide and euthanasia in Washington state: patientrequests and physician responses. JAMA 275:919–925
16. Ganzini L, Nelson HD, Schmidt TA, Kreamer DF, Delorit MA,Lee MA (2000) Physicians' experience with the Oregon deathwith dignity act. N Engl J Med 324(20):557–563
17. Edwards P, Roberts I, Clarke M, DiGuiseppi C, Pratap S, WentzR, Kwan I (2002) Increasing response rates to postal question-naires: systematic review. BMJ 324:1183–1185
18. INFARMED. Informação científica sobre medicamentos: relatório[Scientific information on drugs: report]. Available at http://www.infarmed.pt/portal/page/portal/INFARMED/MONITORIZACAO_DO_MERCADO/OBSERVATORIO/INTRODUCAO_DE_FICHEIROS/ICM_rel_preliminar.pdf. Accessed April 2007
19. Asch DA, Jedrziewski K, Christakis NA (1997) Response rates tomail surveys published in medical journals. J Clin Epidemiol50:1129–1136
Support Care Cancer (2010) 18:1271–1277 1277

260 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 261 261Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
200
Reliability study in five languages of the translation of the pain behavioural scaleDoloplus�
G. Pickering a,b,c,*, S.J. Gibson d, S. Serbouti e, P. Odetti f, J. Ferraz Gonçalves g, G. Gambassi h, H. Guarda i,J.P. Hamers j, D. Lussier k, F. Monacelli f, J.M. Pérez-Castejón Garrote l, S.M. Zwakhalen j, D. Barnetom,Collectif Doloplus� e, B. Wary e
aCHU Clermont-Ferrand, Centre de Pharmacologie Clinique, F-63003 Clermont-Ferrand, Franceb Inserm, CIC 501, UMR 766, F-63003 Clermont-Ferrand, FrancecUniv. Clermont1, F-63001 Clermont-Ferrand, FrancedNational Ageing Research Institute, Parkville, Australiae Palliative Care Unit, Regional Hospital, Metz-Thionville, FrancefUnit of Geriatrics, Department of Internal Medicine and Medical Specialties, University of Study, Genoa, ItalygPalliative Care Unit, Portuguese Cancer Institute, Porto, PortugalhCentro Medicina Invecchiamento, Università Cattolica Sacro Cuore, Rome, ItalyiCentro de Saúde da Lapa, Lisboa, PortugaljDepartment of Health Care and Nursing Science, Maastricht University, The NetherlandskDivision of Geriatric Medicine and Center for research on pain, Mc Gill University, Montreal, CanadalCSS Clinica Barceloneta, C/Pescadores, Barcelona, Spainm Santa Creu de Vic Hospital, Barcelona, Spain
a r t i c l e i n f o
Article history:Received 2 June 2008Received in revised form 10 August 2009Accepted 10 August 2009Available online 10 September 2009
Keywords:Pain assessmentCognitive impairmentElderly
a b s t r a c t
Non-verbal pain assessment scales are useful tools for pain evaluation in persons with communicationdisorders and moderate–severe dementia. The Doloplus� was one of the first scales to be developedand validated as a pain assessment tool in older adults with dementia. This study aims at evaluatingthe translation of the Doloplus� scale in five languages, as regards test–retest and inter-rater reliability.Results show that both tests are good or excellent for the English, Italian, Portuguese and Spanish ver-sions and moderate for the Dutch version. These results bring a unique opportunity to include the trans-lated Doloplus� scale in daily assessment of elderly persons with communication disorders, and futurestudies should focus on enriching the validation of the scale in each language.� 2009 European Federation of International Association for the Study of Pain Chapters. Published by
Elsevier Ltd. All rights reserved.
1. Introduction
Persistent pain is recognised as a very common problem in long-term aged care facilities, affecting up to 80% of residents (Roy, 1986;Parmelee et al., 1993; Gibson and Helme, 2000). Undetected or un-der-treated pain can have serious adverse effects on frail olderadults including poorer cognitive performance, reduced quality oflife, increased depression and functional disability (Gibson, 2007;Leong et al., 2007; Scherder et al., 2008). In the adult population,the group at most risk of undetected pain and poor pain manage-
ment are frail older persons with communication problems, andparticularly those with dementia (Pickering et al., 2000; Marzinski,1991). There is mounting evidence to show that older adults withdementia receive less analgesic medication than cognitively intactadults, despite the presence of similar levels of disease or injury(Scherder and Bouma, 1997; Horgas and Tsai, 1998; Pickeringet al., 2006; Gibson, 2007). The identification and treatment of paindepends on appropriate pain assessment and this is often a very dif-ficult task in those with dementia. Self-report is generally recogni-sed as the de facto gold standard for pain assessment, but verbalcommunication skills are often lost or compromised in those withmoderate–severe dementia. Non-verbal pain assessment methodsprovide an alternative strategy, and may be the preferred assess-ment choice in cases of moderate–severe dementia (Hadjistavropo-ulos et al., 2007). Recent reviews of the literature catalogue morethan 20 observer-rated behavioural pain assessment tools that have
1090-3801/$36.00 � 2009 European Federation of International Association for the Study of Pain Chapters. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.ejpain.2009.08.004
* Corresponding author. Address: Clinical Pharmacology Centre, Batiment 3C,CHU, Hopital G Montpied, 63001 Clermont-Ferrand cedex, France. Tel.: +33 0 4 7317 84 16; fax: +33 0 4 73 17 84 12.
E-mail address: [email protected] (G. Pickering).
European Journal of Pain 14 (2010) 545.e1–545.e10
Contents lists available at ScienceDirect
European Journal of Pain
journal homepage: www.EuropeanJournalPain.com

262 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
201
been developed for specific use in older persons with dementia. Afewof themost researched alternatemeasures are: Abbey Pain Scale(Abbey et al., 2004), Checklist of Non-verbal Pain Indicators (Feldt,2000), Discomfort in Dementia of the Alzheimer’s type (Hurleyet al., 1992), Non-Communicative Patient’s Pain Assessment Instru-ment (Snow et al., 2004), Pain Assessment Checklist for Seniors withLimited Ability to Communicate (Fuchs-Lacelle andHadjistavropou-los, 2004), Pain Assessment in the Dementing Elderly (Villanuevaet al., 2003), Pain Assessment In Advanced Dementia (Wardenet al., 2003) and the Doloplus� (Wary et al., 2001). The French ver-sion of the Doloplus� behaviour rating scale was one of the firstscales to be developed in older adults with dementia (Wary andCollectif, 1999) and has been validated in a group of 510 residents(Lefevre-Chapiro and Collectif, 2001; Wary et al., 2001). Validationof the French version of theDoloplus� scale included test–retest reli-ability (Spearman’s correlation coefficient is >0.75 on all items of theDoloplus� scale (r = 0.75–0.94), inter-rater reliability (r = 0.90),internal consistency (Chronbach’s alpha = 0.82) and concurrentvalidity (r = 0.65), when compared with self-rated pain using a vi-sual analog scale among patientswho can complete self-reportmea-sures (Lefevre-Chapiro and Collectif, 2001; Wary et al., 2001).Considering the need for reliable and valid tools for older personswith moderate–severe cognitive impairment, the aim of the currentstudy was to examine the intra (test–retest) and inter-rater reliabil-ity of the translation of the Doloplus� scale into English, Dutch,Italian, Portuguese and Spanish, in a large multicultural sample ofolder persons with moderate–severe cognitive impairment. SeeTables S1–S5, see the online version at doi:10.1016/j.ejpain.2009.08.004.
2. Method
This is a multicentre study of the translated version of the Dolo-plus� scale in five languages.
2.1. Measures
Doloplus� was used to assess pain: the Doloplus� scale consistsof ten items, each scored on 0–3 point scales, five somatic, twopsychomotor and three psychosocial items. It takes only about2–3 min to complete by French teams and has sufficient items toavoid missing idiosyncratic pain expressions that may be specificto pain with cognitive disorders.
Prior to the study Doloplus� was translated. The main diffi-culty in the translation of scales is indeed to maintain the con-tent equivalence of the original instrument in the translatedversion and there is no gold standard of translation techniquesin international research. The French version of the scale hasbeen translated from French to another language (forward trans-lation) and the reverse (backward translation) (Cull et al., 1998;MOT, 1997). Two independent bilingual health professionals(their mother tongue is the second language) translated indepen-dently the questionnaire into their native tongue. A reconcilia-tion meeting was conducted to obtain a consensus version.Then two native French speakers who were blinded to the origi-nal version retranslated the new scale into French. The last stepof the translation procedure was the pre-testing of the translatedinstrument using a small sample of elderly persons with commu-nication disorders with a final debriefing summary including allparticipants.
Besides pain scores, demographic information (e.g. age, gen-der) was gathered from all the participants and recorded on acase report form. Cognitive status of all residents was evaluatedusing the Mini Mental State Examination (MMSE) (Folsteinet al., 1975). This test ranges from 0 to 30 points and is widely
used to screen for cognitive impairment. Efforts were made tohave the MMSE assessment undertaken as close to the painassessment as possible and while most evaluations were takenin the preceding week, in a few isolated cases the evaluationwas up to 3 months old. At the end of the study, the qualitativeopinion of the participating physicians concerning the acceptabil-ity of the Doloplus� scale was sought with special regard to itsease of use.
2.2. Ethics committee
The protocol was approved by the French Ethics Committee.When required, it was also approved by the local Ethics Commit-tee and informed consent of the patient or surrogate consent wasobtained. Informed consent was obtained by a doctor not in-volved in the pain evaluation. This protocol did not change thenormal care of the patients and might even have improved it,as the protocol created a dynamic awareness among the staff topain assessment in the institution where pain was systematicallyevaluated.
2.3. Investigators
Nine teams (one for Dutch and two for each of the other lan-guages) have been selected on the basis of their experience andcompetence in geriatrics and in pain evaluation of elderly patientswith communication disorders. Each team tested the scale in theirnative language with at least 40 elderly persons.
2.4. Patients
Males and females aged 65 or above, with communication dis-orders, with or without suspected pain, were included. Any changein behaviour (posture and movement, facial expression, prostra-tion, loss of appetite, vocal complaint, psychological and behav-ioural disturbances) was also an inclusion criteria.
Pain is always a potential cause of behaviour changes and eventhough pain might not be the most likely cause of behaviouralchange, it must always be considered as a potential cause in pa-tients with dementia. The enrolment of patients without suspectedpain was aimed at overcoming the misdiagnoses of pain in patientsaffected by dementia.
Excluded from the protocol were: patients who had acute painneeding immediate pharmacological pain management (patientwith any major behavioural changes, obvious sign of distressand agitation, or complaining overtly) or who had recent analge-sic treatment (within the previous 4 h), or who refused to partic-ipate. Finally, we excluded patients when they were agitated andcould not be observed quietly for a few minutes by the physi-cians of the unit in order to have an adequate scoring of theDoloplus� scale. The level of agitation was assessed clinically(interference with and opposition to daily care) and/or by admin-istration of the neuropsychiatric inventory scale (NPI with cut off>40/120).
Withdrawn from the protocol were: any patient who had achange of treatment between the retest evaluations or a changeof treatment between the evaluations of both practitioners, any pa-tient who refused to participate after having given informed con-sent. The decision to initiate analgesics or to administer a rescuedose was essentially based on a clinical evaluation indicative ofobvious pain and based on a Doloplus� score >15.
2.5. Procedure
Prior to the start of the study, the teams met in order to discussthe inclusion/exclusion criteria and the methodology. They were
545.e2 G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10

| 263 263Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
202
provided with the Doloplus� video, instructions for the use of theDoloplus� scale, the agreement of the French ethics committee,and the recommendation that only two physicians should be in-volved per team. An important recommendation was that the phy-sicians should get fully accustomed to, and confident in, the use ofthe scale before starting the study. Considering the polymorphismof elderly patients, the training consisted of a number of evalua-tions with the help of the paper and video backups. B. Wary andthe collective Doloplus� team who have 10 years experience inusing the Doloplus� scale recommended that before starting thestudy, the teams should allow themselves a few days to becomefamiliar with the scale, to include it in the clinical routine of theward, to assess 8–10 elderly patients with communication disor-ders and to discuss collectively between all raters the Doloplus�
scores obtained. On the day of the study, pain assessment wasimplemented during the provision of the usual care in order tointegrate it as much as possible to the customary routine of theunit. Selection of the patients took place on the days where bothphysicians were available and was done after the round by theteam of the ward.
At least 40 patients per team were required and were assessedtwice by a trained physician (rater 1) at initial contact (t0) andagain 4 h later (t4) without any treatment in between, and thesame patient was assessed once by a second physician at t0 (rater2). Observations were timed to avoid potentially painful experi-ences, such as movement or invasive nursing care.
During the study, each physician assessed the patients byobserving them for a few minutes prior to scoring the Doloplus�
scale. The raters were blind to each other’s ratings and undertookthe observation and completion of the Doloplus� scale in a sequen-tial fashion. There was no discussion between the raters about thescores they obtained and no access to each others scores nor totheir own previous score in the case of retest assessments (for rater1). The assessment is easier and quicker if the investigator is famil-iar with the patient, especially concerning facial expressions andbody movement; all physicians were familiar with the patient inour study and provided daily medical care. The test took an averageof 5 min per patient to be performed. The study protocol did notdisrupt nor change the normal care of the patients.
3. Data analysis
In each language, data collected with the scale administered bythe same physician, on two occasions at 4 h intervals (t0 and t4)were used to explore the test–retest reliability. A 4-h intervalwas chosen because it is the usual interval of time for pain assess-ment in clinical practice. In our study, the Doloplus� scale scores att0 were compared with their t4 scores using Student t-test.
In each language, the data collected independently by twotrained physicians (raters 1 and 2) were compared using Studentt -test. Kappa statistics (Landis and Koch, 1977) were calculatedfor each item of the Doloplus� scale. Kappa coefficient is a statisti-cal measure of inter-rater reliability. It is generally thought to be amore robust measure than simple percent agreement calculation.A Kappa value higher than 0.81 typically indicates excellentinter-rater reliability, between 0.61 and 0.80 the test is good andbetween 0.41 and 0.60 it is moderate. Test–retest and inter-raterreliabilities were evaluated with the Pearson and the Intra-classcorrelation coefficients: coefficients above 0.75 are considered asgood to excellent.
Differences between the settings concerning missing data andwithdrawals have been compared with Chi square.
We chose a per protocol analysis rather than an intention-to-treat (ITT) analysis of the data in order to obtain a reliablevalidation of the translation with only complete case report forms.
4. Results
4.1. Completion of the scales
The nine teams recruited at least 40 patients each. In each of theeight teams, two physicians took all the training assessments withabout eight patients. In the Dutch team, four physicians used thescale with about two patients as a pilot training exercise. In allteams, the same physicians undertook all the evaluations of thestudy thereafter. The assessment scales were completed in 406 pa-tients, but due to missing data or patients being excluded becauseof an implemented treatment in the course of the study, statisticswere undertaken on the complete data of 342 patients.
Data from the 64 patients that were excluded from the studycomprised: 10 patients were excluded because of severe agitationassessed clinically and through Neuro Psychiatric Inventory, 16 pa-tients needed a treatment for acute pain and were withdrawn fromthe evaluation and data were not fully completed or missing in 38subjects (9% of our population). Several files per team were notanalysed, mainly because one out of the 40 items had not beenfilled in properly or there was a missing date of birth or MMSEscore. Looking for the report of missing data in the literature onscales validation the rate of missing data is not always indicated.In CNPI scale validation, Feldt, 2000; report 8% missing data, a ratequite comparable to ours. There were no significant differences be-tween the settings concerning missing data and withdrawals (pvalue = 0.996).
No patient refused to consent to participate.
4.2. Demographical data
Seventy percentage women and 30% men (16% single, 25% mar-ried, 3% divorced and 56% widowed), aged 82 ± 2 years old were in-cluded by nine teams in five languages across six countries;Australia, Canada, Italy, Portugal, Spain and The Netherlands.Demographical data are presented in Table 1 for each of the fivelanguages and detail the institution where the patient lives, his/her handicap (incapacity), age, gender and marital status. MMSE(±SD) ranged from 0 to 12 for all patients: 2(4) for Dutch, 12(10)for English, 12(5) for Italian, 4(7) for Portuguese and 8(9) for Span-ish settings.
Table 1Demographical data.
Language Dutch English Italian Portuguese Spanish
Number of residents 40 90 88 57 67
Institution (%)Nursing home 100 52 84 65 0Long-term care setting 0 44 0 0 78Rehabilitation 0 0 13 0 21Home dwelling 0 0 0 2 0Acute care 0 3 0 0 0Other 0 1 3 33 1
Incapacity (%)Dementia 100 81 45 44 57Aphasia 0 2 37 2 18Behavioural disorders 0 1 18 26 13Other 0 16 0 28 12
Age in years (SD) 80 (6.9) 84 (7.8) 81 (7.7) 84 (8.4) 82 (10)
Male n (%) 7 (17.5) 30 (33) 27 (45) 9 (16) 26 (39)
Marital status (%)Single 3 8 19 32 19Married 25 36 22 24 28Divorced 5 2 5 0 3Widowed 67 54 54 44 50
G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10 545.e3
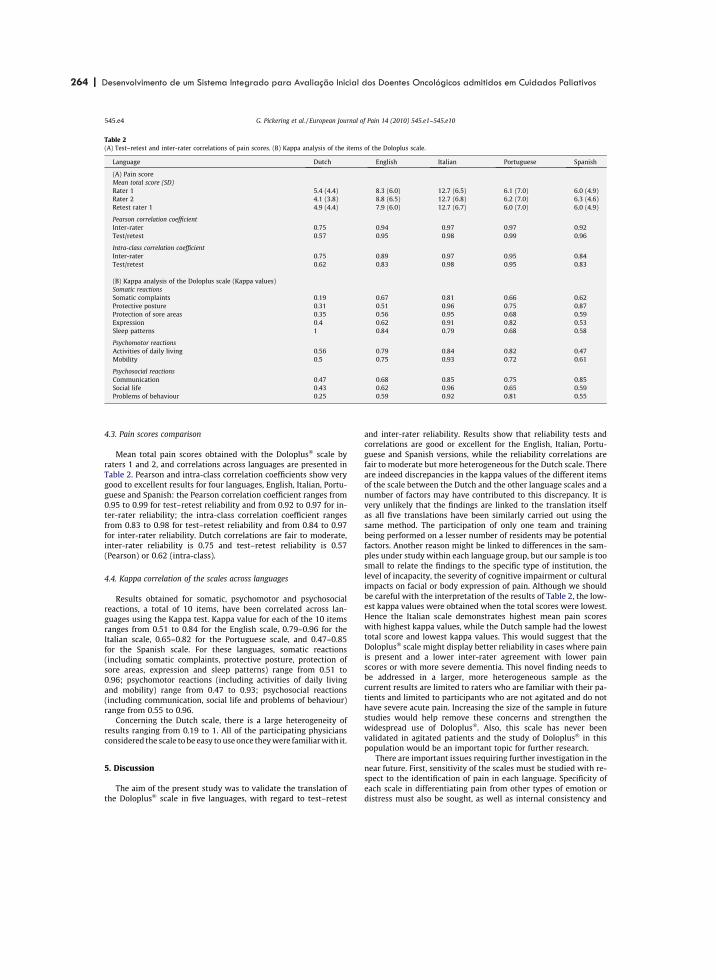
264 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
203
4.3. Pain scores comparison
Mean total pain scores obtained with the Doloplus� scale byraters 1 and 2, and correlations across languages are presented inTable 2. Pearson and intra-class correlation coefficients show verygood to excellent results for four languages, English, Italian, Portu-guese and Spanish: the Pearson correlation coefficient ranges from0.95 to 0.99 for test–retest reliability and from 0.92 to 0.97 for in-ter-rater reliability; the intra-class correlation coefficient rangesfrom 0.83 to 0.98 for test–retest reliability and from 0.84 to 0.97for inter-rater reliability. Dutch correlations are fair to moderate,inter-rater reliability is 0.75 and test–retest reliability is 0.57(Pearson) or 0.62 (intra-class).
4.4. Kappa correlation of the scales across languages
Results obtained for somatic, psychomotor and psychosocialreactions, a total of 10 items, have been correlated across lan-guages using the Kappa test. Kappa value for each of the 10 itemsranges from 0.51 to 0.84 for the English scale, 0.79–0.96 for theItalian scale, 0.65–0.82 for the Portuguese scale, and 0.47–0.85for the Spanish scale. For these languages, somatic reactions(including somatic complaints, protective posture, protection ofsore areas, expression and sleep patterns) range from 0.51 to0.96; psychomotor reactions (including activities of daily livingand mobility) range from 0.47 to 0.93; psychosocial reactions(including communication, social life and problems of behaviour)range from 0.55 to 0.96.
Concerning the Dutch scale, there is a large heterogeneity ofresults ranging from 0.19 to 1. All of the participating physiciansconsidered the scale to be easy touseonce theywere familiarwith it.
5. Discussion
The aim of the present study was to validate the translation ofthe Doloplus� scale in five languages, with regard to test–retest
and inter-rater reliability. Results show that reliability tests andcorrelations are good or excellent for the English, Italian, Portu-guese and Spanish versions, while the reliability correlations arefair to moderate but more heterogeneous for the Dutch scale. Thereare indeed discrepancies in the kappa values of the different itemsof the scale between the Dutch and the other language scales and anumber of factors may have contributed to this discrepancy. It isvery unlikely that the findings are linked to the translation itselfas all five translations have been similarly carried out using thesame method. The participation of only one team and trainingbeing performed on a lesser number of residents may be potentialfactors. Another reason might be linked to differences in the sam-ples under study within each language group, but our sample is toosmall to relate the findings to the specific type of institution, thelevel of incapacity, the severity of cognitive impairment or culturalimpacts on facial or body expression of pain. Although we shouldbe careful with the interpretation of the results of Table 2, the low-est kappa values were obtained when the total scores were lowest.Hence the Italian scale demonstrates highest mean pain scoreswith highest kappa values, while the Dutch sample had the lowesttotal score and lowest kappa values. This would suggest that theDoloplus� scale might display better reliability in cases where painis present and a lower inter-rater agreement with lower painscores or with more severe dementia. This novel finding needs tobe addressed in a larger, more heterogeneous sample as thecurrent results are limited to raters who are familiar with their pa-tients and limited to participants who are not agitated and do nothave severe acute pain. Increasing the size of the sample in futurestudies would help remove these concerns and strengthen thewidespread use of Doloplus�. Also, this scale has never beenvalidated in agitated patients and the study of Doloplus� in thispopulation would be an important topic for further research.
There are important issues requiring further investigation in thenear future. First, sensitivity of the scales must be studied with re-spect to the identification of pain in each language. Specificity ofeach scale in differentiating pain from other types of emotion ordistress must also be sought, as well as internal consistency and
Table 2(A) Test–retest and inter-rater correlations of pain scores. (B) Kappa analysis of the items of the Doloplus scale.
Language Dutch English Italian Portuguese Spanish
(A) Pain scoreMean total score (SD)Rater 1 5.4 (4.4) 8.3 (6.0) 12.7 (6.5) 6.1 (7.0) 6.0 (4.9)Rater 2 4.1 (3.8) 8.8 (6.5) 12.7 (6.8) 6.2 (7.0) 6.3 (4.6)Retest rater 1 4.9 (4.4) 7.9 (6.0) 12.7 (6.7) 6.0 (7.0) 6.0 (4.9)
Pearson correlation coefficientInter-rater 0.75 0.94 0.97 0.97 0.92Test/retest 0.57 0.95 0.98 0.99 0.96
Intra-class correlation coefficientInter-rater 0.75 0.89 0.97 0.95 0.84Test/retest 0.62 0.83 0.98 0.95 0.83
(B) Kappa analysis of the Doloplus scale (Kappa values)Somatic reactionsSomatic complaints 0.19 0.67 0.81 0.66 0.62Protective posture 0.31 0.51 0.96 0.75 0.87Protection of sore areas 0.35 0.56 0.95 0.68 0.59Expression 0.4 0.62 0.91 0.82 0.53Sleep patterns 1 0.84 0.79 0.68 0.58
Psychomotor reactionsActivities of daily living 0.56 0.79 0.84 0.82 0.47Mobility 0.5 0.75 0.93 0.72 0.61
Psychosocial reactionsCommunication 0.47 0.68 0.85 0.75 0.85Social life 0.43 0.62 0.96 0.65 0.59Problems of behaviour 0.25 0.59 0.92 0.81 0.55
545.e4 G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10

| 265 265Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
204
congruency. Socio-cultural factors should be considered and thisapplies especially to Latin American Spanish and Portuguese pop-ulations, although potential linguistic adaptations of the Doloplus�
scale appear to be minor. Several projects in Anglo-Saxon andAmerican English or South American Spanish and Portuguese lan-guages are in preparation for these adaptations of the scale andother reliability studies are being completed, including, German,Chinese, Japanese, Arabic and Czech.
Although the participating physicians considered the scale to beeasy to use once familiar with the tool, their opinion should besought with a standardized evaluation in future studies. The opin-ion of nurses, physical therapists, psychologists and more generallyof health care professionals taking care of elderly patients withdementia and communication disorders will also be important tocollect. Indeed Doloplus� has been rated by Dutch nurses as beingthe least useful of the scales when examined in a comparativestudy (Zwakhalen et al., 2006), while in France, the Doloplus� scaleis now included in the Ministry of Health official guidelines forpain evaluation of persons with communication disorders anddementia (called Mobiqual�). Indeed, it is present in the packagefor pain evaluation in the elderly that is distributed to health careprofessionals of all nursing homes to raise awareness of the needfor systematic pain evaluation especially when communicationdisorders are present.
The reliability testing of the English, Italian, Portuguese andSpanish translations of the Doloplus� scale allows a unique oppor-tunity to include this scale in the daily pain assessment and instudies concerning elderly persons with communication disorders.Compared to other scales, the strong psychometric properties ofthe Doloplus� have already been acknowledged and it has beenrecommended as the preferred choice among the scales that arecurrently available. Herr et al. (2006) describe the Doloplus� as‘‘comprehensive, covering five of the six behaviour categoriesproposed by the American Geriatrics Society”. The scale was alsoconsidered to be clear, requiring a short time to be administeredbut was lacking validation in languages other than French. In a re-cent study (Zwakhalen et al., 2006), similar issues were recognized,namely, satisfactory stability on retest, good correlation withvisual analog scale test, good levels of internal consistency. A com-monly recognized pitfall has always been the lack of adequateinformation on parameters of validity like inter-rater andtest–retest reliability, in languages other than French. Finally, theDoloplus� scale is cited, but not thoroughly examined, by the(Stolee et al., 2007) review because reliability and validity dataare missing.
Our study provides evidence that the Doloplus� scale is a reli-able and easy to use instrument but the validity of the scale mustbe assessed in larger samples in order to undertake a full constructvalidation in each language. Furthermore, the follow-up of a largersample would add greater confidence in the psychometric proper-ties of the behavioural pain assessment scales in each language. Fu-ture studies should also focus on improving the scale in eachlanguage, in order to optimize pain evaluation in the populationof elderly personswith communication disorders, since these scalesare intended for use in this highly dependent and vulnerable group.
Acknowledgements
The Doloplus� team thanks all the persons who participated inthis study, patients and staff of the nursing homes. We wish tothank Grünenthal-France Laboratories who have generously
helped and supported all the steps of this study. There are no con-flicts of interest.
References
Abbey J, Piller N, Bellis de A, Esterman A, Parker D, Giles L, et al. The Abbey painscale: a 1-min numerical indicator for people with end stage dementia. Int JPalliat Nurs 2004;10:6–14.
Cull A, Sprangers M, Bjordal K, Aaronson N. On behalf of the EORTC quality of lifestudy group. EORTC quality of life study group translation procedure. Brussels:EORTC; 1998.
Feldt KS. The checklist of nonverbal pain indicators. Pain Manag Nurs2000;1:13–21.
Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method forgrading the cognitive state of patients for the clinician. J Psychiatric Res1975;12:189–98.
Fuchs-Lacelle S, Hadjistavropoulos HD. Development and preliminary validation ofthe pain assessment checklist for seniors with limited ability to communicate(PACSLAC). Pain Manag Nurs 2004;1:37–49.
Gibson SJ, Helme RD. Cognitive factors and the experience of pain and suffering inolder persons. Pain 2000;85(3):375–83.
Gibson SJ. IASP global year against pain in older persons: highlighting the currentstatus and future perspectives in geriatric pain. Expert Rev Neurother2007;7(6):627–35.
Hadjistavropoulos T, Herr K, Turk DC, Fine PG, Dworkin RH, Helme R, et al. Aninterdisciplinary expert consensus statement on assessment of pain in olderpersons. Clin J Pain 2007;23(Suppl. 1):S1–43.
Herr K, Bjoro K, Decker S. Tools for assessment of pain in nonverbal older adultswith dementia: a state-of-the-science review. J Pain Symptom Manage2006;31(2):170–92.
Horgas AL, Tsai PF. Analgesic drug prescription and use in cognitively impairednursing home residents. Nurs Res 1998;47(4):235–42.
Hurley AC, Volicer BJ, Hanrahan PA, Houde S, Volicer L. Assessment of discomfort inadvanced Alzheimer patients. RINAH 1992;15:369–77.
Landis JR, Koch GG. A one-way components of variance model for categorical data.Biometrics 1977;33:671–9.
Lefevre-Chapiro S, Collectif Doloplus. The Doloplus scale – evaluating pain in theelderly. Eur J Pall Care 2001;8(5):191–3.
Leong IY, Farrell MJ, Helme RD, Gibson SJ. The relationship between medicalcomorbidity and self-rated pain, mood disturbance, and function in olderpeople with chronic pain. J Gerontol A Biol Sci Med Sci 2007;62(5):550–5.
Marzinski LR. The tragedy of dementia: clinically assessing pain in the confusednonverbal elderly. J Gerontol Nurs 1991;17(6):25–8.
Medical Outcomes Trust. Trust introduces new translation criteria. Trust Bull1997;5:1–4.
Parmelee PA, Smith B, Katz IR. Pain complaints and cognitive status among elderlyinstitution residents. J Am Geriatr Soc 1993;41(5):517–22.
Pickering G, Eschalier A, Dubray C. Pain and Alzheimer’s disease. Gerontology2000;46(5):235–41.
Pickering G, Jourdan D, Dubray C. Acute versus chronic pain treatment inAlzheimer’s disease. Eur J Pain 2006;10(4):379–84.
Roy R. A psychosocial perspective on chronic pain and depression in the elderly. SocWork Health Care 1986;12(2):27–36.
Scherder EJ, Bouma A. Is decreased use of analgesics in Alzheimer disease due to achange in the affective component of pain. Alzheimer Dis Assoc Disord1997;11(3):171–4.
Scherder EJ, Eggermont L, Plooij B, Oudshoorn J, Vuijk PJ, Pickering G, et al.Relationship between chronic pain and cognition in cognitively intact olderpersons and in patients with Alzheimer’s disease. The Need to Control for Mood.Gerontology. 2008;54(1):50–58.
Snow AL, Weber JB, O’Malley KL, Cody M, Beck C, Bruera E, et al. NOPPAIN: a nursingassistant administered pain assessment instrument for use in dementia.Dement Geriatr Cogn Disord 2004;17:240–6.
Stolee P, Hillier LM, Esbaugh J, Bol N, Mckellar L, Gauthier N, et al. Pain assessmentin a geriatric psychiatry program. Pain Res Manag 2007;12(4):273–80.
Villanueva MR, Smith TL, Erickson JS, Lee AC, Singer CM. Pain assessment for thedementing elderly (PADE): reliability and validity of a new measure. J Am MedDir Assoc 2003;4:1–8.
Warden V, Hurley AC, Volicer L. Development and psychometric evaluation of thepain assessment in advanced dementia (PAINAD) scale. J Am Med Dir Assoc2003;4:9–15.
Wary B, Collectif Doloplus. Doloplus, une échelle pour évaluer la douleur. SoinsGérontologie 1999;19:25–7.
Wary B, Serbouti S, Collectif Doloplus. Doloplus 2. Validation d’une échelled’évaluation comportementale de la douleur chez la personne âgée. Douleurs2001:2.
Zwakhalen SM, Hamers JP, Berger MP. The psychometric quality and clinicalusefulness of three pain assessment tools for elderly people with dementia. Pain2006;126(1–3):210–20.
G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10 545.e5

266 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
205
Table S1English version of the Doloplus2� scale.
545.e6 G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10
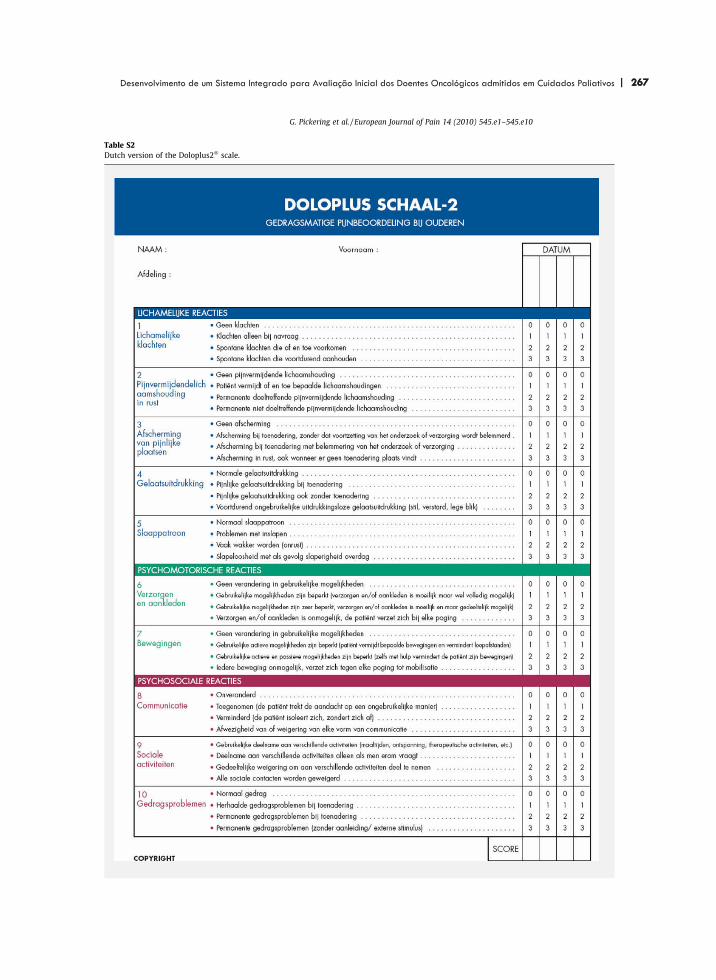
| 267 267Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
206
Table S2Dutch version of the Doloplus2� scale.
G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10 545.e7
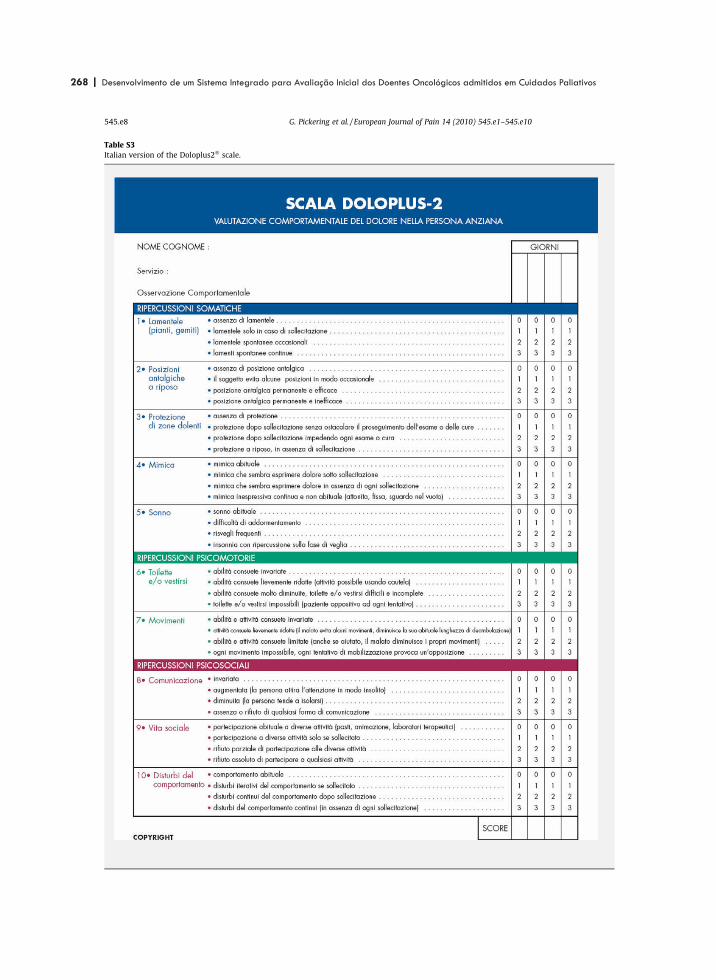
268 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
207
Table S3Italian version of the Doloplus2� scale.
545.e8 G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10

| 269 269Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
208
Table S4Portuguese version of the Doloplus2� scale.
G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10 545.e9

270 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
209
Table S5Spanish version of the Doloplus2� scale.
545.e10 G. Pickering et al. / European Journal of Pain 14 (2010) 545.e1–545.e10

| 271 271Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
211
Thalidomide for the Control of SevereParaneoplastic Pruritus Associated WithHodgkin’s Disease
Ferraz Goncalves, MD1
AbstractA 22-year-old woman with nodular sclerosis type II Hodgkin lymphoma diagnosed in June 2001. She initially underwentchemotherapy with 6 cycles of ABVD (adriamycin, bleomycin, vincristine, dacarbazine) regimen, leading to clinical remission.As it relapsed, she was again treated with 2 different chemotherapy regimens. In November 2003, she underwent bone marrowautotransplantation, but it relapsed after 2 months. After that, she was treated with chemotherapy in monotherapy untilNovember 2005. In December 2005, she was referred to palliative care. Her main symptom was very severe pruritus that inter-fered with all aspects of her life, making her scratch continuously and interfering in all aspects of her life. She was treated withloratadine, hydroxyzine, prednisolone, paroxetine, mirtazapine, cimetidine, and ondansetron, individually and in various combina-tions. She also underwent ultraviolet phototherapy. All trials failed and her pruritus remained at level 8 of 10 most of the time. InApril 2006, she started on thalidomide, 200 mg at night. The pruritus significantly improved to a level of 3 of 10 but did notdisappear completely. She was at last able to sleep properly at night. She remained with a low level of pruritus until her deathin July 2008, at the same dose of thalidomide.
KeywordsHodgkin’s disease, palliative care, itch, thalidomide
Clinical Case
A 22-year-old woman with nodular sclerosis type II Hodgkin
lymphoma diagnosed in June 2001. She initially underwent
chemotherapy with 6 cycles of ABVD (adriamycin, bleomycin,
vincristine, dacarbazine) regimen, leading to clinical remis-
sion. However, it soon relapsed and she was again treated with
chemotherapy: the ESHAP (etoposide, solumedrol, high-dose
ara-C, cisplatin) and MOPP (mechlorethamine, oncovin, pro-
carbazine, and prednisone) regimens. In November 2003, she
underwent bone marrow autotransplantation, but it relapsed
after 2 months. After that, she was treated with chemotherapy
in monotherapy until November 2005.
In December 2005, she was referred to palliative care. She
was a young woman with a good performance status (ECOG
2). Her principal symptom was very severe pruritus that
interfered with all aspects of her life, making her scratch
continuously. She was unable to sleep properly due to pruritus.
She would take more than 1 cold shower during the night to
obtain transient relief from the pruritus. Her body was covered
with lesions, many of them ulcerated. She was not jaundiced
and blood tests of liver function were normal. A biopsy of a
skin ulcer was compatible with scratching lesions.
She was treated with loratadine, hydroxyzine, prednisolone,
paroxetine, mirtazapine, cimetidine, and ondansetron,
individually and in various combinations. She also underwent
ultraviolet phototherapy. All trials failed and her pruritus
remained at level 8 of 10 most of the time. She was also being
treated with morphine, sodium picosulphate, zolpidem, and
diazepam.
In April 2006, she started on thalidomide, 200 mg at night.
The pruritus significantly improved to a level of 3 of 10 but did
not disappear completely. She was at last able to sleep properly
at night. She remained with a low level of pruritus until her
death in July 2008, at the same dose of thalidomide.
Discussion
Cutaneous manifestations of Hodgkin’s disease are common;
most are nonspecific and can be present in over 50% of
patients. The most well-recognized paraneoplastic finding is
severe pruritus.1 Sometimes it is the presenting symptom of
Hodgkin’s disease, but it is usually a sign of far advanced
disease. Sometimes it persists after disease remission.2 In a
1 Instituto Portugues de Oncologia, Porto, Portugal
Corresponding Author:
Ferraz Goncalves, Instituto Portugues de Oncologia, UCP-R, Rua Dr. Antonio
Bernardino de Almeida, 4200-072 Porto, Portugal.
Email: [email protected]; [email protected]
American Journal of Hospice& Palliative Medicine®
27(7) 486-487ª The Author(s) 2010Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/1049909110362523http://ajhpm.sagepub.com
486
by José António Ferraz Gonçalves on November 17, 2010ajh.sagepub.comDownloaded from

272 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
212
few cases the pruritus of Hodgkin’s disease is due to liver
involvement and colestasis, but this patient was not jaundiced
and the blood tests on liver function were normal.
Recommended treatment of pruritus related with Hodgkin’s
disease includes palliative chemotherapy, corticosteroids,
cimetidine, and mirtazapine.2 This patient underwent all these
treatments and others without any benefit.
Thalidomide, a drug synthesized in 1954, was used
extensively as a sedative, tranquilizer, and antiemetic. Thalido-
mide was the cause of multiple congenital abnormalities
mainly concerning the limbs when used during gestation,
sometimes after only a single dose.3 Because of these effects,
it was withdrawn from markets at the beginning of the 1960s.
Later on, the drug proved to be effective in the treatment of
erythema nodosum leprosum. Nowadays, it is used for the
treatment of many diseases and symptoms, namely in advanced
cancer, such as anorexia. There are very rigid rules in women
with reproductive potential to prevent its use during pregnancy.
The antipruritic activity of thalidomide can be secondary
to the inhibition of tumor necrosis factor alpha.4 Another
possibility is that its antipruritic effect results from its central
depressive action.5 This nonspecific action seems more likely
as thalidomide has proven to be effective in the relief of
pruritus originating from very different causes. Besides terato-
genicity, the major adverse effect of thalidomide is peripheral
neuropathy. Other frequent adverse effects include rash,
dizziness, constipation, tremor, mood changes, headache, and
thromboembolism.3 This patient had none of those adverse
effects. Thalidomide enhances the activity of alcohol, barbitu-
rates, and chlorpromazine, and raises the serum levels of para-
cetamol, increasing its toxicity.6 Drugs that cause sedation or
neuropathy should be used carefully, as well as drugs that
decrease the efficacy of oral contraceptives.6
Recently, Rubinstein and Duvic found that the pruritus of
Hodgkin’s disease is commonly associated to Staphylococcus
aureus colonization and that antibiotic therapy can signifi-
cantly reduce the pruritus.1 We do not know whether this
patient could have benefited from antibiotic therapy because
this information was not available at the time and S aureus was
not detected. Korfitis and Trafalis describe 4 patients, 3 with
lymphoma and 1 with multiple myeloma, with intense
generalized pruritus who improved with carbamazepine.7 Car-
bamazepine has previously been reported to alleviate pruritus
associated to multiple sclerosis but not as far as I know in any
other cases.4 Could carbamazepine have been a solution for this
young woman?
Although, thalidomide has been described in several situa-
tions as an effective drug for pruritus, this is the first time that
its effect was described in Hodgkin’s disease, as far as I know.
Conclusion
Pruritus may be a very distressing symptom. It is relatively
frequent in Hodgkin disease and sometimes its control is very
difficult as it was in this young woman. In such cases, thalido-
mide should be considered a potentially useful alternative.
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the
authorship and/or publication of this article.
Funding
This work was supported in part by the North Portugal Section of the
Portuguese League against Cancer.
References
1. Rubinstein M, Duvic M. Cutaneous manifestations of Hodgkin’s
disease. Int J Dermatol. 2006;45(3):251-256.
2. Twycross R, Greaves MW, Handwerker H, et al. Itch: scratching
more than the surface. QJM. 2003;96(1):7-26.
3. Franks ME, Macpherson GR, Figg WD. Thalidomide. Lancet.
2004;363(9423):1802-1811.
4. Summey BT, Yosipovitch G. Pharmacologic advances in the
systemic treatment of itch. Dermatol Ther. 2005;18(4):328-332.
5. Daly BM, Shuster S. Antipruritic action of thalidomide. Acta Derm
Venereol. 2000;80(1):24-25.
6. Wu JJ, Huang DB, Pang KR, Hsu S, Tyring SK. Thalidomide:
dermatological indications, mechanisms of action and side effects.
Br J Dermatol. 2005;153(2):254-273.
7. Korfitis C, Trafalis TD. Carbamazepine can be effective in
alleviating tormenting pruritus in patients with haematological
malignancy. J Pain Symptom Manage. 2008;35(6):571-572.
Goncalves 487
487
by José António Ferraz Gonçalves on November 17, 2010ajh.sagepub.comDownloaded from
| 273 273Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
11ARTIGOS PUBLICADOS
COMO MEMBRO DO RESEARCH STEERING COMMITTEE
DA ASSOCIAÇÃO EUROPEIA DE CUIDADOS PALIATIVOS

274 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 275 275Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
214
SPECIAL ARTICLE
Strateg ies to Manage the Adverse Ef fects of OralMorphine : An Evidence-Based Report
By Nathan Cherny, Carla Ripamonti, Jose Pereira, Carol Davis, Marie Fallon, Henry McQuay, Sebastiano Mercadante,Gavril Pasternak, and Vittorio Ventafridda for the Expert Working Group of the European Association of
Palliative Care Network
Abstract: Successful pain management with opioidsrequires that adequate analgesia be achieved withoutexcessive adverse effects. By these criteria, a substan-tial minority of patients treated with oral morphine(10% to 30%) do not have a successful outcome becauseof (1) excessive adverse effects, (2) inadequate analge-sia, or (3) a combination of both excessive adverseeffects along with inadequate analgesia. The manage-ment of excessive adverse effects remains a majorclinical challenge. Multiple approaches have been de-scribed to address this problem. The clinical challengeof selecting the best option is enhanced by the lack ofdefinitive, evidence-based comparative data. Indeed,this aspect of opioid therapeutics has become a focus ofsubstantial controversy. This study presents evidence-
based recommendations for clinical-practice formu-lated by an Expert Working Group of the EuropeanAssociation of Palliative Care (EAPC) Research Net-work. These recommendations highlight the need forcareful evaluation to distinguish between morphineadverse effects from comorbidity, dehydration, or druginteractions, and initial consideration of dose reduction(possibly by the addition of a co analgesic). If sideeffects persist, the clinician should consider options ofsymptomatic management of the adverse effect, opioidrotation, or switching route of systemic administration.The approaches are described and guidelines are pro-vided to aid in selecting between therapeutic options.
J Clin Oncol 19:2542-2554. © 2001 by AmericanSociety of Clinical Oncology.
ACCORDING TO THE World Health Organizationguidelines for patients with pain of moderate severity
or greater, opioid analgesics are the mainstay of cancer painmanagement.1 For patients with moderate to severe pain,oral morphine is conventionally the opioid of choice.1 Thisrecommendation was derived by virtue of availability,familiarity to clinicians, established effectiveness, simplic-ity of administration, and relative inexpensive cost. It is notbased on proven therapeutic superiority over other options.Guidelines for the use of oral morphine have been presented
by a previous expert working group,2 and an update is inpreparation.Successful pain management with opioids requires that
adequate analgesia be achieved without excessive adverseeffects. By these criteria, a substantial minority of patientstreated with oral morphine (10% to 30%) do not have asuccessful outcome because of (1) excessive adverse ef-fects, (2) inadequate analgesia, or (3) a combination of bothexcessive adverse effects along with inadequate analgesia.2
The management of excessive adverse effects remains amajor clinical challenge. Multiple approaches have beendescribed to address this problem. The clinical challenge ofselecting the best option is enhanced by the lack of studiescomparing various therapeutic approaches to manage theseproblems. Indeed, this aspect of opioid therapeutics hasbecome a focus of substantial controversy.Given this situation, the Steering Committee of the
European Association of Palliative Care (EAPC) ResearchNetwork felt that clinicians would benefit from evidence-based clinical-practice recommendations by an ExpertWorking Group. A panel of experts including Carla Ripam-onti (cochair), Nathan Cherny (cochair), Jose Pereira, HenryMcQuay, Gavril Pasternak, Sebastiano Mercandante, Vit-torio Ventafridda, Carol Davis, and Marie Fallon wereinvited to participate. They met in Oporto, Portugal, inFebruary 1998, where they reviewed all the available data,discussed the evidence, and discussed what practical rec-ommendations could be derived from it. On the basis of the
From the Cancer Pain and Palliative Medicine Service, Departmentof Oncology, Shaare Zedek Medical Center, Jerusalem, Israel; Reha-bilitation and Palliative Care Division, National Cancer Institute, andFondazione Floriani, Milan; Palliative Care Department, NationalCancer Institute, Palermo, Italy; Countess Mountbatten House,Southampton; Department of Palliative Care, Western General Hos-pital, Edinburgh; Pain Research Department, Nuffield Department ofAnaesthetics, University of Oxford, The Churchill Oxford RadcliffeHospital, Oxford, United Kingdom; Department of Neurology, Memo-rial Sloan-Kettering Cancer Center, New York, NY; and Division ofPalliative Medicine, University of Alberta, Edmonton, Canada.Submitted October 18, 2000; accepted January 30, 2001.Address reprint requests to Nathan Cherny, MBBS, FRACP,
Director Cancer Pain and Palliative Medicine, Department ofOncology, Shaare Zedek Medical Center, Jerusalem, Israel; email:[email protected].© 2001 by American Society of Clinical Oncology.0732-183X/01/1909-2542
2542 Journal of Clinical Oncology, Vol 19, No 9 (May 1), 2001: pp 2542-2554

276 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
215
content and conclusions of that meeting, Drs Cherny andRipamonti drafted these recommendations that have sincebeen approved by all participating experts.
OPIOID-INDUCED ADVERSE EFFECTS
Successful opioid therapy requires that the benefits ofanalgesia clearly outweigh treatment-related adverse ef-fects. This implies that a detailed understanding of adverseopioid effects and the strategies used to prevent and managethem are essential skills for all involved in cancer painmanagement. The adverse effects that are frequently ob-served in patients receiving oral morphine and other opioidsare summarized in Table 1.
FACTORS PREDICTIVE OF OPIOID ADVERSE EFFECTS
Drug Related
Overall, there is very little reproducible evidence sug-gesting that any one opioid agonist has a substantially betteradverse effect profile than any other does.Pethidine (meperidine) is not recommended in the man-
agement of chronic cancer pain because of concerns regard-ing its side effect profile. Accumulation of norpethidineafter repetitive dosing of pethidine can result in CNStoxicity characterized by subtle adverse mood effects, trem-ulousness, multifocal myoclonus and, occasionally, sei-zures.3,4 Although accumulation of norpethidine is mostlikely to affect the elderly and patients with overt renaldisease, toxicity is sometimes observed in younger patientswith normal renal function.5,6 The most serious toxicityassociated with pethidine is norpethidine-induced seizures.Naloxone does not reverse this effect, and indeed, couldtheoretically precipitate seizures in patients receiving pethi-
dine by blocking the depressant action of pethidine andallowing the convulsant activity of norpethidine to becomemanifest.7,8 If naloxone must be administered to a patientreceiving pethidine, it should be diluted and slowly titratedwhile appropriate seizure precautions are taken.
Route Related
There is very limited evidence to suggest differences inadverse effects associated with specific routes of systemicadministration. Compared with oral morphine administra-tion, small studies have demonstrated less nausea andvomiting with rectal9 and subcutaneous administration.10
Three studies comparing transdermal fentanyl to oral mor-phine demonstrated less constipation among the patientsreceiving transdermal fentanyl. It is not clear as to whetherthis is a route- or drug-related effect.11-13
Patient Related
For reasons that are not well explained, there is strikinginterindividual variability in the sensitivity to adverse ef-fects from morphine and other opioid drugs. Genetic vari-ability clearly affects the sensitivity to opioid analgesia,particularly related to codeine,14,15 dihydrocodeine16 and,possibly, oxycodone,17 and it is reasonable to assume thatthe genetic background plays a similarly important role inthe predisposition to adverse effects.Some of this variability is related to comorbidity. Aging
is associated with altered pharmacokinetics particularlycharacterized by diminished clearance and volume of dis-tribution. This has been well evaluated for morphine18 andfentanyl.19,20 In studies of morphine use among elderlypatients with chronic cancer pain, the older patients requiredlower doses than their younger counterparts, but they didnot exhibit an enhanced risk for opioid-induced adverseeffects.21,22 Studies among patients with postoperative painsimilarly found that age was a major predictor of lowermorphine dose requirement.23 In patients with impairedrenal function there is delayed clearance of an activemetabolite of morphine, morphine-6-glucuronide.24 Anec-dotally, high concentrations of morphine-6-glucuronidehave been associated with toxicity25-27; however, in aprospective study of patients with opioid-induced deliriumor myoclonus, no relationship to renal function was ob-served.28 Patients with liver disease may have decreasedclearance of meperidine, pentazocine, and propoxyphenethat may result in increased bioavailability and prolongedhalf-lives, which may result in plasma concentrations higherthan normal.29,30 Regarding morphine, mild or moderatehepatic impairment has only minor impact on morphineclearance31,32; however, advanced disease may be associ-ated with reduced elimination.33
Table 1. Common Opioid-Induced Adverse Effects
Gastrointestinal NauseaVomitingConstipation
Autonomic XerostomiaUrinary retentionPostural hypotension
CNS DrowsinessCognitive impairmentHallucinationsDeliriumRespiratorydepressionMyoclonusSeizure disorderHyperalgesia
Cutaneous ItchSweating
2543ADVERSE EFFECTS OF ORAL MORPHINE

| 277 277Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
216
Drug Interactions
Patients who require opioid analgesia for chronic painrelated to cancer or other chronic disorders commonlysuffer from conditions requiring other medications that mayincrease the likelihood of adverse effects by several distinctmechanisms. Commonly, the adverse effects of the othermedication may be synergistic or cumulative to thoseassociated with opioid medications (Table 2). Drugs thatmay alter opioid absorption, metabolism, or clearance ofopioid analgesics have recently been reviewed.34
Dose Related
Among adverse effects, there is substantial variability intheir dose response. A dose-response relationship is mostcommonly evident regarding the CNS adverse effects ofsedation, cognitive impairment, hallucinations, myoclonus,and respiratory depression. Even among these, however,there is very substantial interindividual variability to manyof these effects. Additionally, as tolerance develops to someeffects, the spectrum of adverse effects varies with pro-longed use. Commonly, patients who have had prolongedopioid exposure have a lesser tendency to develop sedationor respiratory depression, and the predominant CNS effectsbecome the neuroexcitatory ones of delirium and myoclo-
nus. Gastrointestinal adverse effects generally have aweaker dose-response relationship. Some, like nausea andvomiting, are common with the initiation with therapy butare subsequently unpredictable with resolution among somepatients and persistence among others. Constipation isvirtually universal, and it demonstrates a very weak doserelationship and no tolerance over time.
Opioid Initiation and Dose Escalation
After the initiation of an opioid or after dose escalationsome adverse effects appear transiently and spontaneouslyabate. This phenomenon has been well demonstrated in aprospective study on the effect of morphine dose escalationon cognitive performance.35 This study demonstrated thatcognitive impairment associated with the initiation of opioidtherapy or dose escalation commonly improved after 7 days.This phenomenon, although often described, has not beenformally studied regarding other adverse effects such asnausea, vomiting, and delirium.
DIFFERENTIAL DIAGNOSIS
Adverse changes in patient well-being among patientsreceiving opioids are not always caused by the opioid.Adverse effects must be differentiated from other causes of
Table 2. Comorbidity That May Mimic Opioid-Induced Adverse Effects
Cause Adverse Effects
CNSCerebral metastases Drowsiness, cognitive impairment, nausea, vomitingLeptomeningeal metastases Drowsiness, cognitive impairment, nausea, vomitingCerebrovascular event Drowsiness, cognitive impairmentExtradural hemorrhage Drowsiness, cognitive impairment
MetabolicDehydration Drowsiness, cognitive impairmentHypercalcemia Drowsiness, cognitive impairment, nausea, vomitingHyponatremia Drowsiness, cognitive impairmentRenal failure Drowsiness, cognitive impairment, nausea, vomiting, myoclonusLiver failure Drowsiness, cognitive impairment, nausea, vomiting, myoclonusHypoxemia Drowsiness, cognitive impairment
Sepsis/infection Drowsiness, cognitive impairment, nausea, vomitingMechanical
Bowel obstruction Nausea, vomitingIatrogenic
Tricyclics Drowsiness, cognitive impairment, constipationBenzodiazepines Drowsiness, cognitive impairmentAntibiotics Nausea and vomitingVinca alkaloids ConstipationFlutamide ConstipationCorticosteroids Agitated deliriumNonsteroidal anti-inflammatory drugs
Nausea, drowsiness
Chemotherapy Nausea, vomiting, drowsiness, cognitive impairmentRadiotherapy Nausea, vomiting, drowsiness
2544 CHERNY ET AL

278 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
217
comorbidity that may develop in the treated patient andfrom drug interactions. Common causes of comorbidity thatmay mimic opioid-induced adverse effects are presented inTable 2.Indeed, the appearance of a new adverse change in patient
well-being that occurs in the setting of stable opioid dosingis rarely caused by the opioid alone, and an alternateexplanation should be vigorously sought. Since polyphar-macy is common among patients with advanced cancer, it isessential to scrutinize medication records and patient reportsof drug administration to evaluate for possible drug inter-actions or some other drug-related explanation for thereported symptoms.
OVERVIEW OF ALTERNATIVE APPROACHES TOTREATING OPIOID ADVERSE EFFECTS
In general, four different approaches to the managementof opioid adverse effects have been described:1. Dose reduction of systemic opioid2. Symptomatic management of the adverse effect3. Opioid rotation (or switching)4. Switching route of systemic administration
Dose Reduction of Systemic Opioid
Reducing the dose of administered opioid usually resultsin a reduction in dose-related adverse effects. When patientshave well controlled pain, gradual reduction in the opioiddose will often result in the resolution of dose-relatedadverse effects while preserving adequate pain relief.36
When opioid doses cannot be reduced without the loss ofpain control, reduction in dose must be accompanied by theaddition of an accompanying synergistic approach. Fourapproaches are commonly applied:1. The addition of a nonopioid coanalgesic. The anal-
gesia achieved from nonopioid coanalgesics from the non-steroidal anti-inflammatory class of agents is additive andoften synergistic with that achieved by opioids. This issupported from a number of prospective studies37-40 andfrom one retrospective drug utilization survey.41 Nonopioidcoanalgesics, particularly the nonsteroidal anti-inflamma-tory agents, have the potential to cause side effects that maybe additive to the opioid-induced adverse effects that arealready problematic. In evaluating the utility of one of theseagents in a particular patient setting, one must consider thelikelihood of benefit, the risk of adverse effects, the ease ofadministration, and patient convenience.2. The addition of an adjuvant analgesic that is appro-
priate to the pain syndrome and mechanism. Adjuvantanalgesics, drugs that have a primary indication other thanpain but which are analgesic in some conditions, may becombined with primary analgesics to improve the outcome
for patients who cannot otherwise attain an acceptablebalance between relief and side effects.42 There is greatinterindividual variability in the response to all adjuvantanalgesics and, for most, the likelihood of benefit is limited.Furthermore, many of the adjuvant analgesics have thepotential to cause side effects that may be additive to theopioid-induced adverse effects that are already problematic.In evaluating the utility of an adjuvant agent in a particularpatient setting, one must consider the likelihood of benefit,the risk of adverse effects, the ease of administration, andpatient convenience.3. The application of a therapy targeting the cause of the
pain. Specific antitumor therapies, such as radiotherapy,chemotherapy, or surgery targeting the cause of cancer-related pain can provide substantial relief and thus lower theneed for opioid analgesia. The analgesic effectiveness ofradiotherapy is documented by abundant data and a favor-able clinical experience in the treatment of painful bonemetastases,43-45 epidural neoplasm,44 and headache attrib-utable to cerebral metastases.46-48 In other settings, how-ever, there is a lack of data, and the use of radiotherapy islargely anecdotal. Despite a paucity of data concerning thespecific analgesic benefits of chemotherapy,49,50 there is astrong clinical impression that tumor shrinkage is generallyassociated with relief of pain. Although there are somereports of analgesic effect even in the absence of significanttumor shrinkage,51-53 the likelihood of a favorable effect onpain is generally related to the likelihood of tumor response.Surgery may have a role in the relief of symptoms caused byspecific problems, such as obstruction of a hollow vis-cus,54-57 unstable bony structures,58-60 and compression ofneural tissues.61-63 Bone pain may similarly be relieved bysystemically administered local treatments, includingbisphosphonates64,65 or radiopharmaceuticals such asstrontium-89.66
4. The application of a regional anesthetic or neuroab-lative intervention. The results of the World Health Orga-nization “analgesic ladder” validation studies suggest that10% to 30% of patients with cancer pain do not achieve asatisfactory balance between relief and side effects usingsystemic pharmacotherapy alone.67-72 Anesthetic and neu-rosurgical techniques may reduce or eliminate the require-ment for systemically administered opioids to achieveadequate analgesia. In general, regional analgesic tech-niques such as intraspinal opioid and local anestheticadministration or intrapleural local anesthetic administra-tion are usually considered first because they can achievethis end without compromising neurologic integrity. Neu-rodestructive procedures, however, are valuable in a smallsubset of patients; and some of these procedures, such asceliac plexus blockade in patients with pancreatic cancer,
2545ADVERSE EFFECTS OF ORAL MORPHINE

| 279 279Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
218
may have a favorable enough risk:benefit ratio that earlytreatment is warranted. The application of these approacheswill be the subject for future Expert Working Group reports.In general, consideration of invasive approaches requires aword of caution. Interpretation of data regarding the use ofalternative analgesic approaches and extrapolation to thepresenting clinical problem requires care. The literature ischaracterized by the lack of uniformity in patient selection,inadequate reporting of previous analgesic therapies, incon-sistencies in outcome evaluation, and paucity of long-termfollow-up. Furthermore, reported outcomes in the literaturemay not predict the outcomes of a procedure performed ona medically ill patient by a physician who has more limitedexperience with the techniques involved.
Symptomatic Management of the Adverse Effect
Symptomatic drugs used to prevent or control opioidadverse effects are commonly employed. Most of theseapproaches are based on cumulative anecdotal experience.With few exceptions, the literature describing these ap-proaches is anecdotal or “expert opinion.” Very few studieshave prospectively evaluated efficacy, and no studies haveevaluated the toxicity of these approaches over the longterm. In general, this approach involves the addition of anew medication. Implicitly, polypharmacy adds to medica-tion burden and invokes associated risks of adverse effects,drug interaction, and diminished compliance.73
Opioid Rotation (Also Called Opioid Switching orSubstitution)
Over the past 10 years, numerous clinicians and cancerpain services have reported successful reduction in opioidside effects by switching from the currently administeredopioid to an alternative opioid.74-88 This approach has beentermed opioid rotation,78,89 and it is also commonly referredto as opioid switching or opioid substitution. Using thisapproach, the reporting clinicians have described improve-ments in cognitive impairment, sedation, hallucinations,nausea, vomiting, and myoclonus.The biologic basis for the observed intraindividual vari-
ability in sensitivity to opioid analgesia and adverse effectsis multifactorial. Preclinical studies show that opioids canact on different receptors or subtype receptors,78,90-99 andindividual receptor profiles may influence the analgesia aswell as the side effects. The genetic makeup of the individ-ual plays and important role in analgesia for some opi-oids,14-16,100-103 and similar phenomena may contribute tovariability in adverse-effect sensitivity.This approach requires familiarity with a range of opioid
agonists and with the use of the opioid dose conversiontables when switching between opioids. It is important to
appreciate, however, that doses calculated using such tablesmay not be accurate among patients tolerant to opioids. Thisinaccuracy is explained to some extent by the large SDsobserved in many of the initial relative potency studies thatformed the scientific basis for the development of thesetables.104 Furthermore, the phenomenon of incompletecross-tolerance can lead to unanticipated potency in a newagent, even when from the same general class of opioidanalgesic. The use of the opioid dose conversion tables iscritical to this strategy. Guidelines for switching and rotat-ing opioids are presented in Appendix A, and a doseconversion table appears in Appendix B.While opioid rotation has the practical advantage of
minimizing polypharmacy, outcomes are variable andsomewhat unpredictable. While many patients will have animproved balance between analgesia and side effects, insome cases, patients may have an unimproved or worseoutcome with the new agent that may necessitate a furthertrial of rotation or a change in therapeutic strategy. Indeed,in one prospective survey, 20% of patients needed toundergo two or more switches until a satisfactory outcomewas achieved.77
Switching Route of Systemic AdministrationLimited data indicates that some adverse effects among
patients receiving oral morphine can be relieved by switch-ing the route of admission to the subcutaneous route. In onesmall study, this phenomenon was reported for nausea andvomiting10; in another study, there was less constipation,drowsiness, and nausea.105
INITIAL MANAGEMENT OF THE PATIENT RECEIVINGORAL MORPHINE WHO PRESENTS WITH ADVERSE
EFFECTS
Among the experts, there was consensus regarding theinitial steps in the management of adverse effects.
Distinguish Between Morphine Adverse Effects FromComorbidity or Drug InteractionsThis step requires careful evaluation of the patient for
factors outlined in Table 2. If present, these factors shouldbe redressed. Metabolic disorders, dehydration, or sepsisshould be treated, nonessential drugs that may be producingan adverse interaction should be discontinued. This situa-tion requires a high level of clinical vigilance with closefollow-up. Often, symptomatic measures to provide relief ofthe distressing symptoms will be required until improve-ment in patient well-being is observed.
Consider Dose ReductionIf the patient has good pain control, consider reducing the
morphine dose. If the adverse effect is mild to moderate,
2546 CHERNY ET AL

280 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
219
this may be achieved by reducing the morphine dose by25% to 50%. This recommendation is based on the knowndose-response relationship for some opioid adverse effectssuch as drowsiness, delirium and myoclonus as derivedfrom pharmacokinetic/pharmacodynamic studies106-108 andclinical observations.87,109-113 In the setting of severe ad-verse effects, particularly neurotoxicity, often a completecessation of morphine will be needed to allow circulatingmorphine levels to fall sufficiently for the adverse effects toresolve. Once resolution has occurred, consideration can begiven to recommencing morphine at a lower dose orswitching to an alternative opioid in accordance with thedata presented below.
SPECIFIC ADVERSE EFFECTS: BEYOND THE INITIALSTEPS
Beyond these initial steps, the Expert Working Groupconcluded that a range of reasonable options commonlycoexisted. In the sections below, the Expert Working Groupsummarizes the existing data regarding symptomatic man-agement, opioid rotation, and switching the route of sys-temic opioid administration in the management of specificadverse effects and presents a rational approach to prudentdecision making.
Nausea and Vomiting
Scope of the problem. Data from prospective studiesindicates that chronic nausea is observed in 15% to 30% ofpatient receiving oral morphine for chronic cancerpain.9,11,13,114-121
Symptomatic management. These are no studies to in-dicate the superiority of one antiemetic over another in themanagement of opioid-induced nausea. Commonly, recom-mendations have been made on the basis of the inferredmechanism of opioid-induced nausea. These recommenda-tions are unsupported by any prospective study or evensystematic evaluation of retrospective data. Among theagents that have been suggested are metoclopramide, halo-peridol, prochlorperazine, dimenhydrinate, phenothiazine,transdermal scopolamine, cisapride, ondansetron (and other5-HT3 antagonists), and dexamethasone (and othercorticosteroids).Opioid rotation. In five reports, the prevalence and
severity of nausea and vomiting were substantially reducedby switching to an alternative opioid.77,78,83,84,86
Switching route. In two small studies, the switch fromoral to subcutaneous morphine produced significantly lessnausea10,105 and vomiting.10 There is conflicting data re-garding the effect of switching to the rectal route.9,122,123 Ifpresent, this effect is small.
Constipation
Scope of the problem. Data from prospective studiesindicates that chronic constipation is observed in 40% to70% of patient receiving oral morphine for chronic cancerpain.9,11,13,114-121 Opioid-induced constipation can be exac-erbated by metabolic alterations (diabetes, hypercalcemia,hypokalemia, uremia, hypothyroidism), dehydration, ad-vanced age, reduced physical activity/immobility, low-fluidand/or low-fiber diet intake, difficulty reaching the bath-room, mechanical obstruction, neurologic disorders, auto-nomic failure, drugs with anticholinergic action such asondansetron, diuretics, anticonvulsants, iron, vinca alka-loids, and some antihypertensive drugs.124,125
Symptomatic management. These are no studies to in-dicate the superiority of one laxative over another in themanagement of opioid-induced constipation. Commonly,recommendations have been made on the basis of personalexperience and clinical observations. These recommenda-tions are generally unsupported by any prospective study oreven systematic evaluation of retrospective data. Among theagents that have been suggested are docusate, senna, bisaco-dyl, phenophthalein, and lactulose. Prospective data hasdemonstrated efficacy of senna126 and oral naloxone.127-129
Opioid rotation. In one small series, opioid rotation ofmorphine to methadone resulted in a reduction inconstipation.130
Switching route. Reduction in constipation was notreported in any of the studies on changes in morphine routeof administration.Switching drug and route. Three recent crossover stud-
ies have demonstrated a reduced tendency to constipationamong patients treated with transdermal fentanyl comparedwith oral morphine.11-13
Sedation
Scope of the problem. Data from prospective studiesindicates that sedation or drowsiness is observed in 20% to60% of patients receiving oral morphine for chronic cancerpain.9,11,13,114-121
Symptomatic management. The data indicating themerit of amphetamine psychostimulants is limited. In asingle-dose study, dextroamphetamine antagonized opioid-induced sedation and cognitive impairment in postsurgicalpatients.131 Several small controlled clinical trials of meth-ylphenidate demonstrated efficacy in reducing drowsinessand confusion.132-137 Positive outcomes were also observedin a small open label study of these agents in adolescentswith chronic cancer pain.138 All authors note that theseagents can produce adverse effects such as hallucinations,delirium or psychosis, decreased appetite, tremor, and
2547ADVERSE EFFECTS OF ORAL MORPHINE

| 281 281Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
220
tachycardia. These drugs are contraindicated in patientswith a history of psychiatric disorders and are relativelycontraindicated in patients with a history of substance abuseor with paroxysmal tachyarrhythmias.Switching route. In one small study, the switch from
oral to subcutaneous morphine produced significantly lessdrowsiness.105
Opioid rotation. In five reports, the prevalence andseverity of drowsiness and/or sedation were substantiallyreduced by opioid rotation.76,78,80,84,86
Cognitive Failure
Scope of the problem. Mild cognitive impairment iscommon after the initiation of opioid therapy or doseescalation.35,139 There is no data on the prevalence of severeopioid-induced cognitive failure or delirium.Symptomatic therapy. Neuroleptics, specifically halo-
peridol, are most commonly recommended in the symptom-atic management of patients with delirium. When associatedwith severe agitation, a benzodiazepine is often coadminis-tered.140 These recommendations largely derive from theextensive experience and studies in the management ofacute delirium in the medically ill.140-145 Anecdotal experi-ence among cancer patients supports this approach.146,147
Opioid rotation. Delirium or agitated confusion wasreported to improve after opioid rotation in five retrospec-tive series.77,78,80,85,86 In the only prospective study of itstype, Maddocks et al83 switched patients who developeddelirium while taking oral or subcutaneous morphine to acontinuous subcutaneous infusion of oxycodone, with res-olution of the delirium in eight of 13 patients.Switching route. Reduction in delirium was not re-
ported in any of the studies on changes in morphine route ofadministration.
Myoclonus
Scope of the problem. Myoclonus may occur in patientson chronic opioid therapy, and it seems to be dose related ina unpredictable manner. In a small study of patients receiv-ing more than 500 mg morphine per day, 12 of 19 hadsignificant myoclonus.148 A study of patients with mor-phine-related adverse effects indicated that the prevalenceof myoclonus was threefold higher among patients receiv-ing oral morphine than among those receiving parenteralmorphine, suggesting a role of metabolite production by theliver.28
Symptomatic management. There are no prospectivestudies on the treatment of opioid-induced myoclonus.Consequently, current recommendations for the treatmentof myoclonus are empiric and anecdotal. Agents that havebeen recommended include baclofen,149-151 diazepam152,153
and clonazepam,154-156 midazolam,157,158 valproic ac-id,155,156 and dantrolene sodium.159
Opiod rotation. Improvement in myoclonus after opi-oid rotation, commonly with total resolution of the symp-tom, is reported in five retrospective series.77,78,84,86,87
Switching route. Reduction in myoclonus was not re-ported in any of the studies on changes in morphine route ofadministration.
Pruritus
Scope of the problem. Data from prospective studiesindicate that chronic itch is observed in 2% to 10% ofpatient receiving oral morphine for chronic cancerpain.9,11,13,114-121
Symptomatic management. There are no prospectivestudies on the treatment of opioid-induced pruritus. Conse-quently, current recommendations for the treatment ofpruritus are empiric and anecdotal. Antihistamines arecommonly recommended. Anecdotal positive experiencehas been reported with paroxetine.160
Opioid rotation. There are conflicting data suggestingthat fentanyl and oxymorphone are less likely to producehistamine release.161,162 A case where persistent morphine-induced itch resolved after switching opioid has beenreported.163
Switching route. Reduction in pruritus was not reportedin any of the studies on changes in morphine route ofadministration.
SELECTING BETWEEN THERAPEUTIC OPTIONS IN THEMANAGEMENT OF OPIOID ADVERSE EFFECTS
The members of the Expert Working Group concludedthat there were inadequate data to formulate specific rec-ommendations regarding the management of morphine sideeffects, and they recognized that even among expert clini-cians there is considerable variability in individual prac-tices. Despite this, they agreed on six factors to be taken intoconsideration when considering therapeutic options in themanagement of morphine adverse effects:1. Convenience: Compliance with analgesic therapy is
enhanced when the treatment program is simple.73 Ingeneral, polypharmacy should be minimized when-ever possible.
2. Availability: Drug availability is highly variable be-tween countries and the range of available therapeuticoptions strongly influences clinical decision making.
3. Cost: Some opioid formulations, nonsteroidal anti-inflammatory drugs, adjuvant analgesics, and symp-tomatic remedies are expensive. This must be consid-ered when budgetary constraints exist, and wheninsurance coverage is limited.
2548 CHERNY ET AL

282 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
221
4. Familiarity: Clinician bias favors the selecting ofoptions with which the clinician has greatest familiar-ity and experience. Since the most familiar option maynot be the best option, clinicians should be sensitive tothis bias and should familiarize themselves with arange of therapeutic options, including facility with allof the opioid drugs available in their country. Ofcritical issue is the need to be familiar with the use ofthe dose conversion tables in the calculation of doseswhen switching between different opioids and be-tween routes of opioid administration.
5. Availability of appropriate experience and expertise:If invasive procedures are considered, it is importantto consider the availability of local expertise. Theoutcome of invasive techniques is very operator-dependent, and outcomes reported in the literaturemay not predict the outcomes of a procedure per-formed by a physician who has more limited experi-ence with the techniques involved.
6. Patient preference: In some situations, patients mayhave strong preference for an option of adding anothermedication or switching to an alternative mono-therapy. Therapeutic options should be presented tothe patient, and patient preferences should weigh intofinal decision making.
DIRECTIONS FOR FUTURE RESEARCH
The Expert Working Group identified the need for pro-spective research using validated outcome measures of painand adverse effects to evaluate:1. The efficacy of opioid-sparing approaches with the
use of nonopioid and adjuvant analgesics and invasiveapproaches, including regional drug delivery and neu-roablative techniques
2. The efficacy of dose reduction in the management ofadverse effects
3. The efficacy of specific strategies in the symptomaticmanagement of adverse effects
4. The efficacy of opioid rotation in management ofadverse effects
5. The efficacy of switching routes of administration inmanagement of adverse effects
6. Comparative studies randomizing patients betweenvarious approaches
In summary, the following conclusions can be drawnfrom this study:1. There is no sound evidence from well-designed clin-
ical trials of the superiority of one opioid over anotherregarding the side effect profile and/or analgesicprofile.
2. There are now numerous reports describing improve-ment or resolution in adverse effects from morphineafter switching to an alternative opioid. Data derivedfrom observational studies and reports of opioid rota-tion indicate substantial intraindividual variability inanalgesic effect and propensity to adverse effects.
3. When opioid rotation is applied in the setting ofunacceptable adverse effects, the selection of an alter-native opioid is largely empiric. A pure opioid agonistsuch as oxycodone, methadone, hydromorphone, andfentanyl is recommended. The outcome is not predict-able and several different agents may need to be triedsequentially.
4. Despite the presence of multiple recommendations forthe symptomatic management of opioid-induced ad-verse effects, the level of evidence supporting specificefficacy is very low.
5. Clinical research is needed to more formally evaluatethe relative merits of these approaches.
ACKNOWLEDGMENT
We wish to acknowledge the Steering Committee of the ResearchNetwork of the EAPC who have participated in review and preparationof this manuscript: Franco De Conno (Chair), Augusto Caraceni,Nathan Cherny, Carl Johan Furst, Jose Antonio Ferraz Goncalves,Geoffrey Hanks, Stein Kaasa, Sebastiano Mercadante, Juan ManuelNunez Olarte, Philippe Poulain, Lukas Radbruch, Carla Ripamonti,Friedrich Stiefel, Peter Thomas. Additionally, we acknowledge theAIRC (Italian Association for Research in Cancer), the PortugueseAssociation of Palliative Care, and the Portuguese League againstCancer Association for Pain Control for supporting the Expert WorkingGroup.
2549ADVERSE EFFECTS OF ORAL MORPHINE

| 283 283Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
222
APPENDIX A
Guidelines for Switching and Rotating Opioids1. Use dose conversion tables. When switching from one opioid to another in naıve patients, dose conversion tables are used to calculate the
dose of the new opioid. Ensure that the table being used relates to the management of chronic pain. Tables used in acute pain managementgenerally depict single-dosing, which cannot be applied in the chronic pain setting. In tolerant patients, the possibility of incompletecross-tolerance makes the use of a simple conversion on the basis of dose conversion tables potentially hazardous.
2. Dose conversion tables are guidelines only. It must be noted that the values depicted in dose conversion tables are guidelines only. There existslarge interindividual variability in response to various opioids, and this variability cannot be captured in these tables. Recent studies indicatea wide range of dose ratios relative to morphine. However, with the exception of methadone, current literature does not clarify the exact ranges.A suggestion, which is not supported by strong evidence, would be to decrease the dose of the new opioid by an additional 30% to 50%. Thiswould accommodate the variability in most cases and address the phenomenon of a lack of complete cross-tolerance when switching from oneopioid to another.
3. Dosing with the new opioid. The initial goal when switching opioids is to convert the patient to the new drug safely. As noted above,incomplete cross-tolerance may result in a patient who is far more sensitive to the new agent than expected. Thus, it is suggested that cliniciansbe conservative in their calculations when switching between opioids. It is advisable to start at doses of the new opioid lower than thosepredicted by the dose conversion tables, monitor patients closely during the switch-over period and titrate to clinical effect. If pain is not wellcontrolled, the dose can be increased, whereas if the patient experiences adverse effects such as excessive somnolence, the dose may need tobe titrated down. It is always better to start at a lower dose and then titrate upward than to start with a dose that is too high. Close monitoringof patients during the switch is crucial.
APPENDIX BDose Conversion Table of Opioids in the Setting of Cancer Pain Management
Opioid Relative Equianalgesic Doses
Morphine122,123,164-166 10 mg PO: 7-10 mg PR10 mg PO: 3-5 mg SC or IV
Hydromorphone74,75,167,168 Morphine 10 mg PO: hydromorphone 2 mg POHydromorphone 2 mg PO: hydromorphone 1 mg SC or IV
Oxycodone120,166,169,170 Morphine 10 mg PO: oxycodone 7.5 mg POOxycodone 10 mg PO: oxycodone 5 mg SC or IV
Methadone82 N.B.—the ratio depends on the dose of previous opioid.3 If morphine 30 mg to 90 mg PO use ratio of 4:1(ie, morphine 30 mg is approximately equivalent to 7 mg of methadone3 If morphine 90 to 300 mg PO use ratio of 8:1(ie, morphine 300 mg PO is approximately equivalent to 35 mg methadone PO)3 If morphine � 300 mg PO use ratio of 12:1(ie, morphine 400 mg PO is approximately equivalent to 35 mg methadone PO)If previous morphine dose is much higher than 300 mg, the dose ratio will be higher than 12:1
Fentanyl171,172 Readers are referred to tables distributed by the manufactures for dose ratios related totransdermal fentanyl. Wide ranges are noted in these tables.A dose ratio of morphine SC: fentanyl SC of 100:1 is suggested for parenteral fentanyl.
NOTE. Doses are depicted to indicate relative potency, ie, morphine 10 mg PO is approximately equivalent in potency to hydromorphone 2 mg PO. This wouldgive an equianalgesic dose ratio of morphine to hydromorphone of 5:1.
Abbreviations: PO, oral route; SC, subcutaneous route; IV, intravenous route; PR, rectal route.
REFERENCES
1. World Health Organization: Cancer Pain Relief (ed 2). Geneva,Switzerland, World Health Organization, 19962. European Association for Palliative Care: Morphine in cancer
pain: Modes of administration—Expert Working Group of the Euro-pean Association for Palliative Care. BMJ 312:823-826, 1996
3. Szeto HH, Inturrisi CE, Houde R, et al: Accumulation ofnormeperidine, an active metabolite of meperidine, in patients withrenal failure of cancer. Ann Intern Med 86:738-741, 19774. Eisendrath SJ, Goldman B, Douglas J, et al: Meperidine-induced
delirium. Am J Psychiatry 144:1062-1065, 1987
2550 CHERNY ET AL
284 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
223
5. Marinella MA: Meperidine-induced generalized seizures withnormal renal function. South Med J 90:556-558, 19976. Kaiko RF, Foley KM, Grabinski PY, et al: Central nervous
system excitatory effects of meperidine in cancer patients. Ann Neurol13:180-185, 19837. Czuczwar SJ, Frey HH: Effect of morphine and morphine-like
analgesics on susceptibility to seizures in mice. Neuropharmacology25:465-469, 19868. Umans JG, Inturrisi CE: Antinociceptive activity and toxicity of
meperidine and normeperidine in mice. J Pharmacol Exp Ther 223:203-206, 19829. Babul N, Provencher L, Laberge F, et al: Comparative efficacy
and safety of controlled-release morphine suppositories and tablets incancer pain. J Clin Pharmacol 38:74-81, 199810. McDonald P, Graham P, Clayton M, et al: Regular subcutaneous
bolus morphine via an indwelling cannula for pain from advancedcancer. Palliat Med 5:323-329, 199111. Ahmedzai S, Brooks D: Transdermal fentanyl versus sustained-
release oral morphine in cancer pain: Preference, efficacy, and qualityof life—The TTS-Fentanyl Comparative Trial Group. J Pain SymptomManage 13:254-261, 199712. Donner B, Zenz M, Tryba M, et al: Direct conversion from oral
morphine to transdermal fentanyl: A multicenter study in patients withcancer pain. Pain 64:527-534, 199613. Payne R, Mathias SD, Pasta DJ, et al: Quality of life and cancer
pain: Satisfaction and side effects with transdermal fentanyl versus oralmorphine. J Clin Oncol 16:1588-1593, 199814. Poulsen L, Brosen K, Arendt-Nielsen L, et al: Codeine and
morphine in extensive and poor metabolizers of sparteine: Pharmaco-kinetics, analgesic effect and side effects. Eur J Clin Pharmacol51:289-295, 199615. Sindrup SH, Brosen K: The pharmacogenetics of codeine
hypoalgesia. Pharmacogenetics 5:335-346, 199516. Fromm MF, Hofmann U, Griese EU, et al: Dihydrocodeine: A
new opioid substrate for the polymorphic CYP2D6 in humans. ClinPharmacol Ther 58:374-382, 199517. Lurcott G: The effects of the genetic absence and inhibition of
CYP2D6 on the metabolism of codeine and its derivatives, hydroc-odone and oxycodone. Anesth Prog 45:154-156, 199818. Baillie SP, Bateman DN, Coates PE, et al: Age and the
pharmacokinetics of morphine. Age Ageing 18:258-262, 198919. Holdsworth MT, Forman WB, Killilea TA, et al: Transdermal
fentanyl disposition in elderly subjects. Gerontology 40:32-37, 199420. Bentley JB, Borel JD, Nenad RE Jr, et al: Age and fentanyl
pharmacokinetics. Anesth Analg 61:968-971, 198221. Rapin CH: The treatment of pain in the elderly patient: The use
of oral morphine in the treatment of pain. J Palliat Care 5:54-55, 198922. Vigano A, Bruera E, Suarez-Almazor ME: Age, pain intensity,
and opioid dose in patients with advanced cancer. Cancer 83:1244-1250, 199823. Macintyre PE, Jarvis DA: Age is the best predictor of postop-
erative morphine requirements. Pain 64:357-364, 199624. Osborne R, Joel S, Grebenik K, et al: The pharmacokinetics of
morphine and morphine glucuronides in kidney failure. Clin PharmacolTher 54:158-167, 199325. Hagen NA, Foley KM, Cerbone DJ, et al: Chronic nausea and
morphine-6-glucuronide. J Pain Symptom Manage 6:125-128, 199126. Osborne RJ, Joel SP, Slevin ML: Morphine intoxication in renal
failure: The role of morphine-6-glucuronide. BMJ 292:1548-1549,1986
27. Sjogren P, Dragsted L, Christensen CB: Myoclonic spasmsduring treatment with high doses of intravenous morphine in renalfailure. Acta Anaesthesiol Scand 37:780-782, 199328. Tiseo PJ, Thaler HT, Lapin J, et al: Morphine-6-glucuronide
concentrations and opioid-related side effects: A survey in cancerpatients. Pain 61:47-54, 199529. Neal EA, Meffin PJ, Gregory PB, et al: Enhanced bioavailability
and decreased clearance of analgesics in patients with cirrhosis.Gastroenterology 77:96-102, 197930. Pond SM, Tong T, Benowitz NL, et al: Enhanced bioavailability
of pethidine and pentazocine in patients with cirrhosis of the liver. AustN Z J Med 10:515-519, 198031. Crotty B, Watson KJ, Desmond PV, et al: Hepatic extraction of
morphine is impaired in cirrhosis. Eur J Clin Pharmacol 36:501-506,198932. Patwardhan RV, Johnson RF, Hoyumpa A, Jr., et al: Normal
metabolism of morphine in cirrhosis. Gastroenterology 81:1006-1011,198133. Hasselstrom J, Eriksson S, Persson A, et al: The metabolism and
bioavailability of morphine in patients with severe liver cirrhosis. Br JClin Pharmacol 29:289-297, 199034. Bernard SA, Bruera E: Drug Interactions in Palliative Care.
J Clin Oncol 18:1780-1799, 200035. Bruera E, Macmillan K, Hanson J, et al: The cognitive effects of
the administration of narcotic analgesics in patients with cancer pain.Pain 39:13-16, 198936. Fallon MT, B ON: Substitution of another opioid for morphine:
Opioid toxicity should be managed initially by decreasing the opioiddose. BMJ 317:81, 1998 (letter)37. Joishy SK, Walsh D: The opioid-sparing effects of intravenous
ketorolac as an adjuvant analgesic in cancer pain: Application in bonemetastases and the opioid bowel syndrome. J Pain Symptom Manage16:334-339, 199838. Minotti V, De Angelis V, Righetti E, et al: Double-blind
evaluation of short-term analgesic efficacy of orally administereddiclofenac, diclofenac plus codeine, and diclofenac plus imipramine inchronic cancer pain. Pain 74:133-137, 199839. Bjorkman R, Ullman A, Hedner J: Morphine-sparing effect of
diclofenac in cancer pain. Eur J Clin Pharmacol 44:1-5, 199340. Sevarino FB, Sinatra RS, Paige D, et al: The efficacy of
intramuscular ketorolac in combination with intravenous PCA mor-phine for postoperative pain relief. J Clin Anesth 4:285-288, 199241. Zech DF, Grond S, Lynch J, et al: Validation of World Health
Organization Guidelines for cancer pain relief: A 10-year prospectivestudy. Pain 63:65-76, 199542. Portenoy RK: Adjuvant analgesic agents. Hematol Oncol Clin
North Am 10:103-119, 199643. Hoskin PJ: Radiotherapy for bone pain. Pain 63:137-139, 199544. Bates T: A review of local radiotherapy in the treatment of bone
metastases and cord compression. Int J Radiat Oncol Biol Phys23:217-221, 199245. Janjan NA: Radiation for bone metastases: conventional tech-
niques and the role of systemic radiopharmaceuticals. Cancer 80:1628-1645, 199746. Vermeulen SS: Whole brain radiotherapy in the treatment of
metastatic brain tumors. Semin Surg Oncol 14:64-69, 199847. Sneed PK, Larson DA, Wara WM: Radiotherapy for cerebral
metastases. Neurosurg Clin N Am 7:505-515, 199648. Coia LR: The role of radiation therapy in the treatment of brain
metastases. Int J Radiat Oncol Biol Phys 23:229-238, 1992
2551ADVERSE EFFECTS OF ORAL MORPHINE
| 285 285Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
224
49. Rubens RD, Towlson KE, Ramirez AJ, et al: Appropriatechemotherapy for palliating advanced cancer. BMJ 304:35-40, 199250. Queisser W: Chemotherapy for the treatment of cancer pain.
Recent Results Cancer Res 89:171-177, 198451. Patt YZ, Peters RE, Chuang VP, et al: Palliation of pelvic
recurrence of colorectal cancer with intraarterial 5-fluorouracil andmitomycin. Cancer 56:2175-2180, 198552. Rothenberg ML: New developments in chemotherapy for pa-
tients with advanced pancreatic cancer. Oncology (Huntingt) 10:18-22,199653. Thatcher N, Anderson H, Betticher DC, et al: Symptomatic
benefit from gemcitabine and other chemotherapy in advanced non-small cell lung cancer: Changes in performance status and tumour-related symptoms. Anticancer Drugs 6:39-48, 1995 (suppl 6)54. Barbalias GA, Siablis D, Liatsikos EN, et al: Metal stents: A
new treatment of malignant ureteral obstruction. J Urol 158:54-58,199755. Mainar A, Tejero E, Maynar M, et al: Colorectal obstruction:
Treatment with metallic stents. Radiology 198:761-764, 199656. Parker MC, Baines MJ: Intestinal obstruction in patients with
advanced malignant disease. Br J Surg 83:1-2, 199657. Jong P, Sturgeon J, Jamieson CG: Benefit of palliative surgery
for bowel obstruction in advanced ovarian cancer. Can J Surg 38:454-457, 199558. Tarn TS, Lee TS: Surgical treatment of metastatic tumors of the
long bones. Chung Hua I Hsueh Tsa Chih 54:170-175, 199459. Algan SM, Horowitz SM: Surgical treatment of pathologic hip
lesions in patients with metastatic disease. Clin Orthop 332:223-231,199660. Braun A, Rohe K: Orthopedic surgery for management of tumor
pain. Recent Results Cancer Res 89:157-170, 198461. Harris JK, Sutcliffe JC, Robinson NE: The role of emergency
surgery in malignant spinal extradural compression: Assessment offunctional outcome. Br J Neurosurg 10:27-33, 199662. Gokaslan ZL: Spine surgery for cancer. Curr Opin Oncol
8:178-181, 199663. Sucher E, Margulies JY, Floman Y, et al: Prognostic factors in
anterior decompression for metastatic cord compression: An analysis ofresults. Eur Spine J 3:70-75, 199464. Hillner BE, Ingle JN, Berenson JR, et al: American Society of
Clinical Oncology guideline on the role of bisphosphonates in breastcancer: American Society of Clinical Oncology BisphosphonatesExpert Panel. J Clin Oncol 18:1378-1391, 200065. Fulfaro F, Casuccio A, Ticozzi C, et al: The role of bisphos-
phonates in the treatment of painful metastatic bone disease: A reviewof phase III trials. Pain 78:157-169, 199866. Ben-Josef E, Porter AT: Radioisotopes in the treatment of bone
metastases. Ann Med 29:31-35, 199767. Takeda F: Japanese field-testing of WHO guidelines. PRN
Forum 4:4-5, 198568. Ventafridda V, Tamburini M, Caraceni A, et al: A validation
study of the WHO method for cancer pain relief. Cancer 59:850-856,198769. Walker VA, Hoskin PJ, Hanks GW, et al: Evaluation of WHO
analgesic guidelines for cancer pain in a hospital-based palliative careunit. J Pain Symptom Manage 3:145-149, 198870. Schug SA, Zech D, Dorr U: Cancer pain management according
to WHO analgesic guidelines. J Pain Symptom Manage 5:27-32, 199071. Goisis A, Gorini M, Ratti R, et al: Application of a WHO
protocol on medical therapy for oncologic pain in an internal medicinehospital. Tumori 75:470-472, 1989
72. Grond S, Zech D, Schug SA, et al: Validation of World HealthOrganization guidelines for cancer pain relief during the last days andhours of life. J Pain Symptom Manage 6:411-422, 199173. Fincke BG, Miller DR, Spiro A III: The interaction of patient
perception of overmedication with drug compliance and side effects.J Gen Intern Med 13:182-185, 199874. Lawlor P, Turner K, Hanson J, et al: Dose ratio between
morphine and hydromorphone in patients with cancer pain: A retro-spective study. Pain 72:79-85, 199775. Bruera E, Pereira J, Watanabe S, et al: Opioid rotation in
patients with cancer pain: A retrospective comparison of dose ratiosbetween methadone, hydromorphone, and morphine. Cancer 78:852-857, 199676. Bruera E, Franco JJ, Maltoni M, et al: Changing pattern of
agitated impaired mental status in patients with advanced cancer:Association with cognitive monitoring, hydration, and opioid rotation.J Pain Symptom Manage 10:287-291, 199577. Cherny NJ, Chang V, Frager G, et al: Opioid pharmacotherapy
in the management of cancer pain: A survey of strategies used by painphysicians for the selection of analgesic drugs and routes of adminis-tration. Cancer 76:1283-1293, 199578. de Stoutz ND, Bruera E, Suarez-Almazor M: Opioid rotation for
toxicity reduction in terminal cancer patients. J Pain Symptom Manage10:378-384, 199579. Thomas Z, Bruera E: Use of methadone in a highly tolerant
patient receiving parenteral hydromorphone. J Pain Symptom Manage10:315-317, 199580. Galer BS, Coyle N, Pasternak GW, et al: Individual variability
in the response to different opioids: Report of five cases. Pain 49:87-91,199281. Fitzgibbon DR, Ready LB: Intravenous high-dose methadone
administered by patient controlled analgesia and continuous infusionfor the treatment of cancer pain refractory to high-dose morphine. Pain73:259-261, 199782. Ripamonti C, Groff L, Brunelli C, et al: Switching from
morphine to oral methadone in treating cancer pain: What is theequianalgesic dose ratio? J Clin Oncol 16:3216-3221, 199883. Maddocks I, Somogyi A, Abbott F, et al: Attenuation of
morphine-induced delirium in palliative care by substitution withinfusion of oxycodone. J Pain Symptom Manage 12:182-189, 199684. Vigano A, Fan D, Bruera E: Individualized use of methadone
and opioid rotation in the comprehensive management of cancer painassociated with poor prognostic indicators. Pain 67:115-119, 199685. Paix A, Coleman A, Lees J, et al: Subcutaneous fentanyl and
sufentanil infusion substitution for morphine intolerance in cancer painmanagement. Pain 63:263-269, 199586. Ashby MA, Martin P, Jackson KA: Opioid substitution to reduce
adverse effects in cancer pain management. Med J Aust 170:68-71,199987. Hagen N, Swanson R: Strychnine-like multifocal myoclonus
and seizures in extremely high-dose opioid administration: Treatmentstrategies. J Pain Symptom Manage 14:51-58, 199788. Makin MK, Ellershaw JE: Substitution of another opioid for
morphine: Methadone can be used to manage neuropathic pain relatedto cancer. BMJ 317:81, 1998 (letter)89. Mercadante S: Opioid rotation for cancer pain: Rationale and
clinical aspects. Cancer 86:1856-1866, 199990. Rossi GC, Leventhal L, Pan YX, et al: Antisense mapping of
MOR-1 in rats: Distinguishing between morphine and morphine-6beta-glucuronide antinociception. J Pharmacol Exp Ther 281:109-114,1997
2552 CHERNY ET AL
286 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
225
91. Leventhal L, Stevens LB, Rossi GC, et al: Antisense mapping ofthe MOR-1 opioid receptor clone: Modulation of hyperphagia inducedby DAMGO. J Pharmacol Exp Ther 282:1402-1407, 199792. Brown GP, Yang K, King MA, et al: 3-Methoxynaltrexone, a
selective heroin/morphine-6 beta-glucuronide antagonist. FEBS Lett412:35-38, 199793. Blake AD, Bot G, Li S, et al: Differential agonist regulation of
the human kappa-opioid receptor. J Neurochem 68:1846-1852, 199794. Rossi GC, Brown GP, Leventhal L, et al: Novel receptor
mechanisms for heroin and morphine-6 beta-glucuronide analgesia.Neurosci Lett 216:1-4, 199695. Rossi GC, Pan YX, Brown GP, et al: Antisense mapping the
MOR-1 opioid receptor: Evidence for alternative splicing and a novelmorphine-6 beta-glucuronide receptor. FEBS Lett 369:192-196, 199596. Pasternak GW, Standifer KM: Mapping of opioid receptors
using antisense oligodeoxynucleotides: Correlating their molecularbiology and pharmacology. Trends Pharmacol Sci 16:344-350, 199597. Zadina JE, Kastin AJ, Harrison LM, et al: Opiate receptor
changes after chronic exposure to agonists and antagonists. Ann N YAcad Sci 757:353-361, 199598. Pasternak GW: Pharmacological mechanisms of opioid analge-
sics. Clin Neuropharmacol 16:1-18, 199399. Moulin DE, Ling GS, Pasternak GW: Unidirectional analgesic
cross-tolerance between morphine and levorphanol in the rat. Pain33:233-239, 1988100. Brosen K, Sindrup SH, Skjelbo E, et al: Role of genetic
polymorphism in psychopharmacology: An update. PsychopharmacolSer 10:199-211, 1993101. Heiskanen T, Olkkola KT, Kalso E: Effects of blocking
CYP2D6 on the pharmacokinetics and pharmacodynamics of oxyc-odone. Clin Pharmacol Ther 64:603-611, 1998102. Kirkwood LC, Nation RL, Somogyi AA: Characterization of
the human cytochrome P450 enzymes involved in the metabolism ofdihydrocodeine. Br J Clin Pharmacol 44:549-555, 1997103. Sindrup SH, Poulsen L, Brosen K, et al: Are poor metabolisers
of sparteine/debrisoquine less pain tolerant than extensive metabolis-ers? Pain 53:335-339, 1993104. Foley KM, Houde RW: Methadone in cancer pain management:
Individualize dose and titrate to effect. J Clin Oncol 16:3213-15, 1998(editorial)105. Drexel H, Dzien A, Spiegel RW, et al: Treatment of severe
cancer pain by low-dose continuous subcutaneous morphine. Pain36:169-176, 1989106. Houde RW, Wallenstein SL, Beaver WT: Evaluation of
analgesics in patients with cancer pain, in Lasagna L (ed): InternationalEncyclopedia of Pharmacology and Therapeutics. New York, NY,Pergamon Press, 1966, pp 59-67107. Galway JE, Morrison JD, Dundee JW: Dosage-side-effect
relationships of morphine and meperidine. Anesth Analg 52:536-541,1973108. Inturrisi CE, Colburn WA, Kaiko RF, et al: Pharmacokinetics
and pharmacodynamics of methadone in patients with chronic pain.Clin Pharmacol Ther 41:392-401, 1987109. Ferris DJ: Controlling myoclonus after high-dosage morphine
infusions. Am J Health Syst Pharm 56:1009-1010, 1999110. Christie JM, Simmonds M, Patt R, et al: Dose-titration,
multicenter study of oral transmucosal fentanyl citrate for the treatmentof breakthrough pain in cancer patients using transdermal fentanyl forpersistent pain. J Clin Oncol 16:3238-3245, 1998111. Hanks GW, Forbes K: Opioid responsiveness. Acta Anaesthe-
siol Scand 41:154-158, 1997
112. Hanks GW, WM ON, Simpson P, et al: The cognitive andpsychomotor effects of opioid analgesics: II. A randomized controlledtrial of single doses of morphine, lorazepam and placebo in healthysubjects. Eur J Clin Pharmacol 48:455-460, 1995113. Schug SA, Zech D, Grond S, et al: A long-term survey of
morphine in cancer pain patients. J Pain Symptom Manage 7:259-266,1992114. Mercadante S, Salvaggio L, Dardanoni G, et al: Dextropropoxy-
phene versus morphine in opioid-naive cancer patients with pain. J PainSymptom Manage 15:76-81, 1998115. Broomhead A, Kerr R, Tester W, et al: Comparison of a
once-a-day sustained-release morphine formulation with standard oralmorphine treatment for cancer pain. J Pain SymptomManage 14:63-73,1997116. Wong JO, Chiu GL, Tsao CJ, et al: Comparison of oral
controlled-release morphine with transdermal fentanyl in terminalcancer pain. Acta Anaesthesiol Sin 35:25-32, 1997117. Levy MH, Fitzmartin R, Reder R: Comparison of immediate vs
controlled release morphine (MS Contin) in the long-term managementof cancer-related pain. Proc Am Soc Clin Oncol 12:455, 1993 (abstr1582)118. Boureau F, Saudubray F, d’Arnoux C, et al: A comparative
study of controlled-release morphine (CRM) suspension and CRMtablets in chronic cancer pain. J Pain Symptom Manage 7:393-399,1992119. Walsh TD, MacDonald N, Bruera E, et al: A controlled study of
sustained-release morphine sulfate tablets in chronic pain from ad-vanced cancer. Am J Clin Oncol 15:268-272, 1992120. Kalso E, Vainio A: Morphine and oxycodone hydrochloride in
the management of cancer pain. Clin Pharmacol Ther 47:639-646, 1990121. Homesley HD: Morphine: immediate release vs. controlled
release. N C Med J 50:390-394, 1989122. De Conno F, Ripamonti C, Saita L, et al: Role of rectal route in
treating cancer pain: A randomized crossover clinical trial of oralversus rectal morphine administration in opioid-naive cancer patientswith pain. J Clin Oncol 13:1004-1008, 1995123. Bruera E, Fainsinger R, Spachynski K, et al: Clinical efficacy
and safety of a novel controlled-release morphine suppository andsubcutaneous morphine in cancer pain: A randomized evaluation.J Clin Oncol 13:1520-1527, 1995124. Derby S, Portenoy RK: Assessment and management of
opioid-induced constipation, in Portenoy RK, Bruera E (eds): Topics inPalliative Care. New York, NY, Oxford University Press, 1997, pp95-112125. Sykes NP: The relationship between opioid use and laxative use
in terminally ill cancer patients. Palliat Med 12:375-382, 1998126. Ramesh PR, Kumar KS, Rajagopal MR, et al: Managing
morphine-induced constipation: A controlled comparison of anAyurvedic formulation and senna. J Pain Symptom Manage 16:240-244, 1998127. Sykes NP: An investigation of the ability of oral naloxone to
correct opioid-related constipation in patients with advanced cancer.Palliat Med 10:135-144, 1996128. Sykes NP: Oral naloxone in opioid-associated constipation.
Lancet 337:1475, 1991129. Culpepper-Morgan JA, Inturrisi CE, Portenoy RK, et al:
Treatment of opioid-induced constipation with oral naloxone: A pilotstudy. Clin Pharmacol Ther 52:90-95, 1992130. Daeninck PJ, Bruera E: Reduction in constipation and laxative
requirements following opioid rotation to methadone: A report of fourcases. J Pain Symptom Manage 18:303-309, 1999
2553ADVERSE EFFECTS OF ORAL MORPHINE

| 287 287Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
226
131. Forrest WH Jr, Brown BW Jr, Brown CR, et al: Dextroamphet-amine with morphine for the treatment of postoperative pain. N EnglJ Med 296:712-715, 1977132. Bruera E, Chadwick S, Brenneis C, et al: Methylphenidate
associated with narcotics for the treatment of cancer pain. Cancer TreatRep 71:67-70, 1987133. Bruera E, Brenneis C, Paterson AH, et al: Narcotics plus
methylphenidate (Ritalin) for advanced cancer pain. Am J Nurs88:1555-1556, 1988134. Bruera E, Brenneis C, Paterson AH, et al: Use of methylpheni-
date as an adjuvant to narcotic analgesics in patients with advancedcancer. J Pain Symptom Manage 4:3-6, 1989135. Bruera E, Miller MJ, Macmillan K, et al: Neuropsychological
effects of methylphenidate in patients receiving a continuous infusionof narcotics for cancer pain. Pain 48:163-166, 1992136. Bruera E, Fainsinger R, MacEachern T, et al: The use of
methylphenidate in patients with incident cancer pain receiving regularopiates: A preliminary report. Pain 50:75-77, 1992137. Wilwerding MB, Loprinzi CL, Mailliard JA, et al: A random-
ized, crossover evaluation of methylphenidate in cancer patientsreceiving strong narcotics. Support Care Cancer 3:135-138, 1995138. Yee JD, Berde CB: Dextroamphetamine or methylphenidate as
adjuvants to opioid analgesia for adolescents with cancer. J PainSymptom Manage 9:122-125, 1994139. Bruera E, Miller L, McCallion J, et al: Cognitive failure in
patients with terminal cancer: A prospective study. J Pain SymptomManage 7:192-195, 1992140. Battaglia J, Moss S, Rush J, et al: Haloperidol, lorazepam, or
both for psychotic agitation? A multicenter, prospective, double-blind,emergency department study. Am J Emerg Med 15:335-340, 1997141. Bieniek SA, Ownby RL, Penalver A, et al: A double-blind study
of lorazepam versus the combination of haloperidol and lorazepam inmanaging agitation. Pharmacotherapy 18:57-62, 1998142. Seneff MG, Mathews RA: Use of haloperidol infusions to
control delirium in critically ill adults. Ann Pharmacother 29:690-693,1995143. Foster S, Kessel J, Berman ME, et al: Efficacy of lorazepam and
haloperidol for rapid tranquilization in a psychiatric emergency roomsetting. Int Clin Psychopharmacol 12:175-179, 1997144. Lenox RH, Newhouse PA, Creelman WL, et al: Adjunctive
treatment of manic agitation with lorazepam versus haloperidol: adouble-blind study. J Clin Psychiatry 53:47-52, 1992145. Fernandez F, Holmes VF, Adams F, et al: Treatment of severe,
refractory agitation with a haloperidol drip. J Clin Psychiatry 49:239-241, 1988146. Akechi T, Uchitomi Y, Okamura H, et al: Usage of haloperidol
for delirium in cancer patients. Support Care Cancer 4:390-392, 1996147. Olofsson SM, Weitzner MA, Valentine AD, et al: A retrospec-
tive study of the psychiatric management and outcome of delirium inthe cancer patient. Support Care Cancer 4:351-357, 1996148. Potter JM, Reid DB, Shaw RJ, et al: Myoclonus associated with
treatment with high doses of morphine: The role of supplemental drugsBMJ 299:150-153, 1989149. Krames ES, Gershow J, Glassberg A, et al: Continuous infusion
of spinally administered narcotics for the relief of pain due to malignantdisorders. Cancer 56:696-702, 1985150. Parkinson SK, Bailey SL, Little WL, et al: Myoclonic seizure
activity with chronic high-dose spinal opioid administration. Anesthe-siology 72:743-745, 1990
151. Radbruch L, Zech D, Grond S: Myoclonus resulting fromhigh-dose epidural and intravenous morphine infusion [in German].Med Klin 92:296-299, 1997152. Glavina MJ, Robertshaw R: Myoclonic spasms following
intrathecal morphine. Anaesthesia 43:389-390, 1988153. De Conno F, Caraceni A, Martini C, et al: Hyperalgesia and
myoclonus with intrathecal infusion of high-dose morphine. Pain47:337-339, 1991154. Eisele JH, Jr., Grigsby EJ, Dea G: Clonazepam treatment of
myoclonic contractions associated with high-dose opioids: Case report.Pain 49:231-232, 1992155. Obeso JA: Therapy of myoclonus. Clin Neurosci 3:253-257,
1995156. Caviness JN: Myoclonus. Mayo Clin Proc 71:679-688, 1996157. Holdsworth MT, Adams VR, Chavez CM, et al: Continuous
midazolam infusion for the management of morphine-induced myoc-lonus. Ann Pharmacother 29:25-29, 1995158. Hagen N, Swanson R: Strychnine-like multifocal myoclonus
and seizures in extremely high-dose opioid administration: Treatmentstrategies. J Pain Symptom Manage 14:51-58, 1997159. Mercadante S: Dantrolene treatment of opioid-induced myoc-
lonus. Anesth Analg 81:1307-1308, 1995160. Zylicz Z, Smits C, Krajnik M: Paroxetine for pruritus in
advanced cancer. J Pain Symptom Manage 16:121-124, 1998161. Hermens JM, Ebertz JM, Hanifin JM, et al: Comparison of
histamine release in human skin mast cells induced by morphine,fentanyl, and oxymorphone. Anesthesiology 62:124-129, 1985162. Warner MA, Hosking MP, Gray JR, et al: Narcotic-induced
histamine release: A comparison of morphine, oxymorphone, andfentanyl infusions. J Cardiothorac Vasc Anesth 5:481-484, 1991163. Katcher J, Walsh D: Opioid-induced itching: morphine sulfate
and hydromorphone hydrochloride. J Pain Symptom Manage 17:70-72,1999164. Babul N, Darke AC: Disposition of morphine and its glucuro-
nide metabolites after oral and rectal administration: Evidence of routespecificity. Clin Pharmacol Ther 54:286-292, 1993165. Nelson KA, Glare PA, Walsh D, et al: A prospective, within-
patient, crossover study of continuous intravenous and subcutaneousmorphine for chronic cancer pain. J Pain Symptom Manage 13:262-267, 1997166. Kalso E, Vainio A, Mattila MJ, et al: Morphine and oxycodone in
the management of cancer pain: Plasma levels determined by chemical andradioreceptor assays. Pharmacol Toxicol 67:322-328, 1990167. Dunbar PJ, Chapman CR, Buckley FP, et al: Clinical analgesic
equivalence for morphine and hydromorphone with prolonged PCA.Pain 68:265-2670, 1996168. Miller MG, McCarthy N, O’Boyle CA, et al: Continuous
subcutaneous infusion of morphine vs. hydromorphone: A controlledtrial. J Pain Symptom Manage 18:9-16, 1999169. Bruera E, Belzile M, Pituskin E, et al: Randomized, double-
blind, cross-over trial comparing safety and efficacy of oral controlled-release oxycodone with controlled-release morphine in patients withcancer pain. J Clin Oncol 16:3222-3229, 1998170. Heiskanen T, Kalso E: Controlled-release oxycodone and
morphine in cancer related pain. Pain 73:37-45, 1997171. Fainsinger RL, Bruera E: How should we use transdermal
fentanyl (TF) for pain management in palliative care patients? J PalliatCare 12:48-53, 1996172. Hanks GW, Fallon MT: Transdermal fentanyl in cancer pain:
Conversion from oral morphine. J Pain Symptom Manage 10:87, 1995(letter)
2554 CHERNY ET AL

288 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos

| 289 289Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
227
Published online: 22 May 2001© Springer-Verlag 2001
Friedrich Stiefel, Maria Die Trill, Alexandre Berney, Juan Manuel Nunez Olarte, Darius Razavi, and the members ofthe Steering Committee of the ResearchNetwork of the European Association forPalliative Care
The named authors are the invited expertswho make up the Expert Working Groupmentioned in the title, which is chaired byF. Stiefel and co-chaired by J. Olarte
The members of the Steering Committee of the Research Network of the EuropeanAssociation for Palliative Care are: Franco De Conno (Chair), Augusto Caraceni, Nathan Cherny, Carl Johan Fürst,José Antonio Ferraz Gonçalves, Geoffrey Hanks, Stein Kaasa, Sebastiano Mercadente, Juan Manuel Nunez Olarte,Philippe Poulain, Lukas Radbruch, CarlaRipamonti, Friedrich Stiefel
Abstract Our objective in thisstudy was to summarize the relevantknowledge on depression in pallia-tive care and to provide a frame-work for clinical, scientific and edu-cational efforts at improving itsmanagement. The Research SteeringCommittee (RSC) of the EuropeanAssociation of Palliative Care(EAPC) established an ExpertWorking Group (EWG) to addressthe issue of depression in palliativecare. Each invited expert was allo-cated a specific topic and was askedto review the literature. These re-views were presented during theSixth Congress of the EAPC in 1999 and then discussed in a closedmeeting with members of the RSC.Based on these reviews, and the dis-cussions that followed their presen-tation, a first draft of the paper wasproduced and circulated among theinvited experts and members of theRSC who had been present at themeetings. After some debate themanuscript was revised, and a sec-ond draft was circulated, this timealso to RSC members who had notattended the meetings. All personsconsulted have agreed on this finalversion of the report. The EWG con-cluded that the current level of evi-dence did not lend itself to the de-velopment of clinical guidelines anddecided to publish the results oftheir work as a pragmatic report.The report is divided into four sec-tions, focusing on detection, trainingand nonpharmacological and phar-
macological treatment of depressionin palliative care. For each of thesesections, general considerations areaddressed on the basis of the litera-ture review and of clinical experi-ence and a short description of unre-solved issues and recommendationsis provided. Underdetection and un-dertreatment of depression is a seri-ous problem in palliative care.Training of the nonpsychiatric staffshould therefore have the highestpriority. A proactive, flexible andcomprehensive strategy embracingclinical, scientific, and educationalaspects is advocated.
Keywords Depression · Palliativecare · Detection · Treatment · Stafftraining
Support Care Cancer (2001) 9:477–488DOI 10.1007/s005200100244 S P E C I A L A RT I C L E
Friedrich StiefelMaria Die TrillAlexandre BerneyJuan Manuel Nunez OlarteDarius Razavi
Depression in palliative care: a pragmatic report from the Expert Working Group of the European Association for Palliative Care
F. Stiefel (✉)Psychiatry Service, University HospitalLausanne, 1011 Lausanne, Switzerlande-mail: [email protected].: +41-21-3141090Fax: +41-21-3141098M.D. TrillPsycho-Oncology Unit, University General Hospital Gregorio Maranon, Madrid, SpainA. BerneyPsychiatry Service, University Hospital,Lausanne, SwitzerlandJ.M.N. OlartePalliative Care Service, University General Hospital Gregorio Maranon, Madrid, SpainD. RazaviPsychiatric University Clinic, Hôpital St. Anne, Brussels, Belgium

290 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
228
Introduction
The European Association for Palliative Care (EAPC) isa multiprofessional association for persons involved inpalliative care. The EAPC has specific networks for is-sues related to education, ethics, policy questions and re-search. The Research Steering Committee (RSC) of theresearch network of the EAPC initiates Expert WorkingGroups (EWG) to address specific topics, to summarizerelevant knowledge, to develop recommendations, and toidentify priorities for future research. So far, the topicscovered by EWGs have been concerned with morphineadministration [38], pain assessment tools [13], break-through cancer pain [65], management of bowel obstruc-tion [83], the use of corticosteroids in palliative care[28], and strategies to manage adverse effects of oralmorphine [15].
The meetings of the EWG on Depression in PalliativeCare were held during the Sixth Congress of the EAPCin Geneva (22–24 September 1999). In four open work-shops1 the invited experts reviewed relevant aspects ofdepression in palliative care, with particular reference todetection, training, and nonpharmacological and pharma-cological treatment. A closed meeting with the expertsand members of the RSC was organized a day after thecongress to discuss these topics in detail. A first versionof this paper summarizing the presentations and the sub-sequent discussions was drafted by the Chair and circu-lated to the Co-Chair, the invited experts and the mem-bers of the RSC who attended the closed meeting. Afterrevision, a second version circulated, this time also tomembers of the RSC who had not been able to attend theclosed meeting. Only unanimous conclusions have beenincluded in this final version, which is based as far aspossible on scientific evidence. Since a large part of theknowledge on this topic is not yet supported by scientificevidence, the EWG concluded that the current level ofevidence did not lend itself to the development of clini-cal guidelines [110]. The results of the work are there-fore presented as a pragmatic report based on a literaturereview by the invited experts, their clinical experience,and the expertise of the members of the RSC. The litera-ture review was provided by the experts and completedby the Chair with the aid of such conventional sources asMedline. The review cannot therefore be regarded as ex-haustive. For each of the aspects specified above a sum-mary of relevant knowledge will be presented, followedby an account of the unresolved issues and the recom-mendations for clinical practice and future research. Theaim of the paper is to provide a framework for clinical,
scientific and educational efforts to improve the manage-ment of depression in palliative care.
Background
The topic “depression in palliative care” was chosen bythe RSC because psychiatric disorders are frequent inpalliative care, often remain undetected and untreated,and add considerably to the burden of suffering on pa-tients who are already facing severe physical and psy-chosocial problems [77, 94]. The RSC considered thetopic “psychiatric disorders in palliative care” was toobroad to be treated by an EWG and decided first to ad-dress a specific disorder and then utilize a similar ap-proach for other psychiatric disorders frequently ob-served in palliative care. Since most of the literature ondepression in palliative care is related to adult cancer pa-tients and most of the patients in palliative care sufferfrom malignant diseases (WHO [112]), this paper drawslargely on experience with adult cancer patients. Howev-er, there are many other diseases, such as cardiovascular,neurological, metabolic and rheumatological diseases, inwhich depression is also a relevant topic. The recom-mendations – with modifications where necessary –should therefore also be useful for patients with nonma-lignant diseases. In addition, this first EWG on a specificpsychiatric disorder in palliative care could serve as amodel for other EWGs addressing psychiatric disordersof pediatric and geriatric patients.
General aspects of depression in palliative care
Two major paradigms exist in current clinical practice fordefining depression: (1) the general phenomenon of de-pressive symptoms and (2) specific depressive disordersdefined by diagnostic criteria [104]. While the generalmedical sector tends to conceptualize depression accord-ing to the former definition, a large proportion of mentalhealth specialists conceptualize depression according tothe second one [82]. These two paradigms have differentimplications for clinical care and treatment response. Forexample, antidepressant treatment has proved to be bene-ficial for patients with depression, but not for those with adepressive symptomatology attributable to an adjustmentdisorder [5]. The EWG was given a mandate to focus onmajor depression in palliative care and has thereforebased its work on the established diagnostic criteria of theDiagnostic and Statistical Manual of Mental Disorders(DSM-IV) of the American Psychiatric Association [1],the most widely used diagnostic system (Table 1).
The prevalence of depression in palliative care varies,depending on type and stage of disease, setting and pop-ulation characteristics [62], and has been reported as3.7–58% [11, 21, 99]. Among hospitalized cancer pa-
478
1 The workshops were chaired by F. Stiefel and co-chaired by J.M.Nunez Olarte. “Detection of depression in palliative care” waspresented by D. Razavi, “Psychotherapeutic treatments” by M.Die Trill, and “Pharmacological treatments” by A. Berney. “Edu-cational aspects” was presented by D. Vuille (replacement) andthen discussed by F. Stiefel

| 291 291Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
229
tients with significant levels of physical impairment, atleast one quarter of patients with advanced disease sufferfrom a clinically relevant and treatable depressive illness[7, 53, 54, 75, 102]. Unfortunately, only a minority ofthese patients receive the necessary pharmacologicaltreatment [53, 59, 95]. The undertreatment of depressionhas different reasons [5, 6]. Among them are the difficul-ties of physicians to talk with patients about their emo-tions [61], or the belief – even among mental health pro-fessionals – that depression is somehow inevitable in theterminally ill [25]. It is unfortunate that health care pro-fessionals and the public agree that depressive illnessshould be treated in the physically healthy but remainskeptical about the treatment of depression in patientswith severe somatic diseases.
In the palliative care setting depression and pain oftencoexist and influence each other. A close correlation be-tween long periods of pain and depressive feelings hasbeen demonstrated, a correlation that may be due to neu-rotransmitter changes, but also to psychological exhaus-tion [93]. On the other hand, pain-free periods are knownto give patients new strength and to lower the incidenceof mood disturbances and suicidal ideation [85]. It isvery difficult to establish a diagnosis of depression in anindividual suffering from unrelieved pain, and pain per-ception on the other hand may be influenced by de-pressed mood. Many of the symptoms of depression,such as sleep and appetite disturbances or loss of energyand fatigue, are also associated with unrelieved pain anddisappear when analgesia is achieved [9]. Adequatetreatment of pain is therefore most important in the man-agement of depression in palliative care.
Detection of depression in palliative care
The undertreatment of depression in palliative care isclosely related to the fact that depression remains unde-tected in a substantial number of patients [72, 99]. Somestudies have found that depression remains unrecognizedin more than 50% of depressed medically ill patients [56,69]. The difficulty lies in differentiating depression fromother psychiatric disorders, such as acute stress reactionsor adjustment disorders and from normal reactions suchas grief, or from somatic states that may mimic depres-sion [16]. The psychiatric interview, conducted by an ex-perienced consultation-liaison mental health professionalwho is familiar with patients with advanced disease,would certainly be the gold standard for detection of de-pression in this patient population [29, 75]. However, inmost settings mental health specialists are not part of thepalliative care team or their number is very limited. De-tection of depression in palliative care by the treatingphysicians and nurses is therefore crucial.
The medical staff need specific knowledge, skills andinstruments to detect depression in palliative care. Train-ing in psychiatric issues is complex, however, and vari-ous factors hamper effective educational efforts (see sec-tion on Training, below). Most scientific approaches tothe problem have concentrated on the use of screeninginstruments to detect depression. Screening is designedto detect a given disturbance early; it picks up false-posi-tive and false-negative cases and is not diagnostic inconfirming caseness. The instrument that has been mostwidely utilized and evaluated in the palliative care set-ting is the Hospital Anxiety and Depression Scale
479
Table 1 DSM-IV criteria of major depressive episode.a Five (ormore) of the following symptomsb have been present during thesame 2-week period and represent a change from previous func-
tioning; at least one of the symptoms is either (1) depressed moodor (2) loss of interest or pleasure
– Depressed mood most of the day, nearly every day, as indicated by either subjective report (e.g. feels sad or empty) or observation made by others (e.g., appears tearful)
– Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day(as indicated by either subjective account or observations made by others)
– Significant weight loss when not dieting or weight gain (e.g., a change of more than 5% of body weight in a month),or decrease or increase in appetite nearly every day
– Insomnia or hypersomnia nearly every day– Psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings
of restlessness or being slowed down)– Fatigue or loss of energy nearly every day– Feelings of worthlessness or excessive and inappropriate guilt (which may be delusional) nearly every day
(not merely self-reproach or guilt about being sick)– Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account
or as observed by others)– Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan,
or a suicide attempt or a specific plan for committing suicide
a Adapted from the Diagnostic and Statistical Manual of MentalDisorders (DSM-IV) (APA)b The symptoms cause clinically significant distress or impairmentin social, occupational, or other important areas of functioning.
The symptoms are not due to direct physiological effects of a sub-stance or a medical condition, and are not better accounted for bybereavement

292 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
230
(HADS) [113]. This self-report scale is especially suit-able for the medically ill, since it does not include thesomatic symptoms of depression, such as fatigue, pain orinsomnia, which may also be caused by the illness or itstreatment [60]. Several studies have concluded that theHADS is a simple, sensitive and specific tool that can beused to screen for adjustment, depressive, and anxietydisorders [37, 51, 52, 79]. However, there are severalproblems associated with the use of the HADS in dailyclinical practice. First, the sensitivity and specificity ofthe instrument depends on cut-off points, which maychange in different patient populations (e.g. inpatients,outpatients, young and elderly patients, patients differingin stage and type of disease) [45, 76]. Second, as withany other instrument, higher sensitivity is associatedwith lower specificity and higher specificity with lowersensitivity. Third, the HADS is a screening instrumentfor adjustment disorders with anxious and depressedmood, as well as for major depression or dysthymic andanxiety disorders. Since the types of intervention neededto treat these disorders differ, the HADS lacks a diagnos-tic component that would allow the diagnosis of majordepression. Fourth, the HADS is an instrument based onself-report: acute stress reactions contribute to relativelyhigh rates of false-positive results and social desirability,to false-negative results [96]. Its suitability for use as ascreening instrument for depression in palliative care hastherefore been called in question [35].
There are studies comparing different screening in-struments [43, 45, 52], such as the HADS [113], theZung Self-Rating Depression Scale [24], the GeneralHealth Questionnaire (GHQ) [30], and the RotterdamSymptom Checklist (RSC) [20]. However, the aforemen-tioned problems associated with screening remain thesame. Diagnostic instruments for the detection of psychi-atric disorders, including depression, also exist. ThePrime MD – to mention one widely used and validatedinstrument – has been designed to diagnose six majorpsychiatric disorders (including depression) prevalent inprimary care and consists of a one-page patient question-naire and a structured diagnostic interview conducted bythe physician [91]. This instrument has not been adaptedand validated for palliative care. A two-step screeningand diagnostic procedure for depression in palliative carehas not yet been developed.
Unresolved issues
When all these difficulties associated with screening aretaken into account, it becomes clear that no suitable in-strument is available for the detection of depression inpalliative care. Several issues therefore remain unre-solved (Table 2). It remains unknown whether training inhow to diagnose depression may be an alternative to theuse of screening instruments or whether screening should
be implemented as an isolated act. It also remains unclearwhether screening should focus on specific disorders,how often it should be repeated over time, and how thesomatic symptoms of depression should be taken into ac-count. In addition, the screening of patients who are un-able to communicate because of language barriers, per-sonality traits or severe depressive states also remains anunresolved problem. The inter- and intraindividual varia-tions in the threshold of psychological suffering and ad-aptation make it impossible to conceive of screening as aone-point procedure [78, 79]. Finally, the roles of the spe-cialist nurse clinician [102] and of the consultation-liai-son mental health professional have to be defined. In onestudy only 3 out of 106 patients receiving antidepressantswere referred to mental health specialists [53].
Several other factors affect the diagnosis of depres-sion. Among them are the diagnostic criteria: if diagnos-tic criteria differ, prevalence rates will of necessity alsodiffer [47]. The same holds true for symptom severitythresholds, which may differ depending on instrumentsand clinical judgments [107]. In addition, inclusion andexclusion of somatic symptoms of depression or theirsubstitution with psychological symptoms affect diagno-sis prevalence rates. A flexible approach could be to ex-clude physical symptoms in the diagnosis of depressionif they are probably due to physical disease or its treat-ment and to include them if they are more likely to bepart of the depressive symptomatology [8].
Recommendations
As mentioned above, empirical studies addressing thesequestions are lacking; the following recommendationsare therefore based on the clinical experience of theEWG and the literature (Table 3). Since palliative caresettings vary widely with regard to patients and healthcare delivery characteristics, recommendations for thedetection of depression also vary. For example, ambula-
480
Table 2 Detection of depression in palliative care: unresolved is-sues
Should efforts concentrate on screening instruments or on comprehensive, educational strategies?Are specific mental disorders or “psychological distress” the focusof detection?Since detection is not a one-point procedure, how should it beconceptualized longitudinally?How can somatic symptoms of depression be taken into account in a medically ill patient population?Intra- and interindividual variations in symptom thresholds,language barriers and personality traits hamper uniform detectionproceduresThe roles of the specialized mental health professionals remainundefined

| 293 293Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
231
tory patients would have to be screened with differentthreshold levels than would inpatients, and any referralpolicy will depend on existing resources in terms ofmental health specialists. Nevertheless, the current policy of “wait and see” should be replaced by a proactive clinical, scientific and educational strategycharacterized rather by “trial and error.” All screeningprocedures should be complemented by staff training andby close cooperation with consultation-liaison psychia-try. Consultation-liaison psychiatry services are usuallystaffed by mental health specialists from different profes-sional backgrounds, such as psychiatry, psychology,nursing and social work. With regard to future research,comparison of different strategies should be favored, forexample, implementation of screening or diagnostic in-struments versus training in clinical judgement. Defini-tion of local referral policies is also recommended.
Staff training
The assessment and treatment of psychiatric disordersdepend on the ability to address sensitive issues, such asemotional states, illness representations, and relation-ships, which it may be difficult to ask about in patientswith advanced disease. The highest levels of agreementbetween patients’ self-reported depressive symptoms andstaff members’ perceptions are found when patients re-port few or no depressive symptoms, with only 14% con-cordance in the severe ranges of depression [64]. Theseresults are similar to those of studies on the correlationsbetween patients and health care professionals in theirperception of pain [93], illustrating that adequate assess-ment is based on communication and not on intuitionalone. Communication, on the other hand, is not just anatural gift, but can be influenced and improved bytraining [26, 58, 80]. Other important aspects of trainingare related to staff members’ knowledge about how todiagnose depression, how to identify underlying etiolo-
gies, including organic factors, and how to differentiatedepression from normal and other pathologic states.While the link between diagnosis and treatment of de-pression may seem obvious, clinical experience and sci-entific evidence from noncancer populations indicatethat less than a quarter of diagnosed depressed patientsreceive effective treatment [3, 67]. In advanced diseasethis percentage is probably even lower, since the reluc-tance to prescribe antidepressants seems to be evengreater in such patients [53]. Finally, monitoring of treat-ment and its adverse effects is often neglected and delaysthe reaction (changes of treatment modalities) to nonre-sponsiveness. In summary, many different factors ham-per effective management of depression in palliative careand make training of the staff necessary. They can beidentified as recognition barriers, diagnostic barriers, andtreatment barriers related to patients, physicians, orhealth care system characteristics [31].
Up to now, only a few projects and studies have ad-dressed the issue of training in the management of de-pression for nonpsychiatric health professionals [72].While physicians seem to be aware of their need for im-provement in diagnosing depression, effective strategiesare difficult to design and to evaluate [36]. In a random-ized study, a brief educational intervention did not signif-icantly improve residents’ ability to detect depressed pa-tients; nevertheless it had changed the residents’ attitudesand knowledge relevant to the care of depressed patientsby the time they were followed up 6 months later [50]. Inanother randomized controlled trial, the training of spe-cialist nurses led to a six-fold improvement in their abili-ty to recognize patients with depression compared withnurses who had not had the training; the psychiatric refer-ral rate increased five times, with a three- to four-fold re-duction in the incidence of depression in the interventiongroup [58]. However, the accumulating load on specialistnurses and the tendency to delegate psychological careare major disadvantages of such models. It has also beendemonstrated that specific interviewing behaviors, suchas posing open-ended questions, periodically summariz-ing the information supplied by the patient, and respond-ing to nonverbal and emotional cues, led to greater recog-nition of depression [2, 84]. These findings support theview that training in communication skills promotingsuch an interview behavior is important. In the GroningenPrimary Care Study recognition of psychological disor-ders was not associated with better patient outcome; theauthors concluded that recognition was necessary, but notsufficient, unless primary care physicians had the skills toprovide appropriate treatment [100]. This view has beensupported by other studies [31, 48]. Comprehensive strat-egies are therefore needed, and the provision of an antide-pressant algorithm [18] or of diagnostic criteria aloneseems not to be sufficient. First studies investigatingcomprehensive educational strategies designed to im-prove detection and treatment of depression in the physi-
481
Table 3 Detection of depression in palliative care: recommenda-tions
The setting (patient and care delivery characteristics) should influence detection strategies; flexibility is most importantThe “wait-and-see” policy should be replaced by a proactive strategy characterized by “trial and error”Implementation of screening should be complemented by trainingand a comprehensive management strategyClose collaboration with specialized mental health professionalsfrom consultation-liaison psychiatry is mandatoryComparison of different strategies should be the focus of future researchReferral policy to mental health professionals should be defineddepending on the local circumstances

294 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
232
cally ill are currently under way [72, 73]. Such compre-hensive strategies should also define referral policies formental health staff by outlining the limits of nonpsychiat-ric competence. If staff members encounter difficultcases, for example if there is diagnostic uncertainty, sui-cidality, an important psychiatric comorbidity or unre-sponsiveness to treatment, referral to specialized mentalhealth professionals should be the rule [6].
Unresolved issues
Unresolved issues in staff training are listed in Table 4and include the following. First, the lack of trained men-tal health specialists who are interested in palliative careremains a serious problem, especially with regard totraining. Historically, psychiatry and somatic medicinehave developed separately, and the emergence of psychi-atric liaison services in general hospitals is relatively re-cent. Such services exist mainly in large hospitals andthose affiliated to universities [109]. This lack of mentalhealth specialists hampers educational efforts despite thestrong support for interdisciplinarity within the palliativecare movement. Second, even in settings where mentalhealth specialists are part of the palliative care team, thechoice of training strategies for the detection and man-agement of depression are based on personal preferencesand skills. Working with personal preferences may in-volve such advantages as increased motivation of thetrainer, but they may not meet the needs of the staff, inwhich case they will be ineffective. Finally, the questionremains whether patients, family members, nurses, physi-cians or other team members should be the target of train-ing interventions. It also has to be determined whethercommunication skills, diagnostic skills or prescription be-havior should be their main focus of these interventions.Such studies are difficult to conduct, since they involveboth health care professionals and patients and outcomesare influenced by a variety of confounding variables.
Recommendations
Based on the studies reviewed and on clinical experi-ence, the transfer of knowledge (e.g. of diagnostic crite-ria) alone may be a necessary but not a sufficient condi-tion of improvement in the management of depression inpalliative care. Other important training aspects concernthe staff’s ability to develop appropriate communicationskills. The EWG therefore recommends complementingthe transfer of knowledge with training in communica-tion skills. Such training courses have proved to be ef-fective if their duration and content are adapted to thetype of work performed and if they are consolidated overtime [80]. Finally, the EWG recommends that future re-search should focus on the evaluation and comparison of
different, comprehensive training interventions. Again,close collaboration with specialized mental health pro-fessionals from consultation-liaison psychiatry (CL-Psy-chiatry) is especially crucial (Table 5).
Nonpharmacological treatments
Prior to the discussion of treatment, the issue of preven-tion will be addressed. Since depression is associatedwith different factors, such as psychological and physicalsymptom distress, ineffective coping styles, and poor so-cial support [17, 24, 37, 46, 70], preventive interventionscould possibly have an impact. Up to now such attemptshave not been very successful. In nontargeted interven-tions, a reduction in depression scores for patients inpsychoeducational groups was achieved; the reductiondid not seem to be clinically significant [27]. The sameholds true for other interventions, which failed to reducethe incidence of depression [12, 32, 105, 111]. In orderto have an impact, preventive interventions will mostprobably have to be targeted at patients at risk.
Treatment of depression should not be restricted tothe prescription of a psychotropic medication. The empa-thy and support of significant others and of the medicalteam are as important as the psychopharmacologicaltreatment [33, 77]. In addition to basic but very impor-tant nonspecific therapeutic interventions, such as sup-port and information, specific psychotherapeutic inter-ventions have been proposed for the treatment of depres-sion in patients with severe and life-threatening diseases[19, 27, 89, 90]. However, only in a few studies on psy-chotherapy in the medically ill has the methodology beencomprehensively described. Information on such impor-tant aspects as how randomization was achieved or howsample size, power and confidence intervals were calcu-lated is most often lacking [23]. It is difficult to comparethese studies, since timing and duration of interventions
482
Table 4 Staff training in the management of depression in pallia-tive care: unresolved issues
How should the “transfer of knowledge” be organized given thelack of mental health professionals working in palliative care?What are the most effective strategies for the training of nonpsychiatric staff?Who should be the main target of training interventions and whatshould be their main focus?
Table 5 Staff training in the management of depression in pallia-tive care: recommendations
Transfer of knowledge is a necessary, but not sufficient, elementEducation should also include training in communication skillsFuture research should compare different educational interventions

| 295 295Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
233
vary, description of the practitioners providing the inter-ventions is lacking, and study samples and outcomemeasures differ. Despite these difficulties, a recent meta-analysis of 30 trials of psychological interventions in de-pressed patients with cancer (10 trials were excluded be-cause of missing data) demonstrated that interventionstargeted at patients at risk or with significant psychologi-cal distress were associated with clinically powerful ef-fects; group therapy was found to be more effective thanindividual therapy [87].
Most of the studies demonstrating the efficacy of psy-chotherapeutic techniques in depressed patients withcancer are based on group formats and cognitive-behav-ioral, time-limited models that have emphasized copingstrategies, psychological strengths, personal control, re-laxation training and cognitive restructuring [19, 27, 89,90]. Some psychotherapeutic models have combinedstructured cognitive behavioral techniques with an exis-tential approach [89], while others have reported the effi-cacy of a treatment package combining behavioral andpharmacological therapies [40]. Even though structuredtreatments have proved to be more effective in the reduc-tion of depression than nonstructured treatments [68],clinical experience suggests that more psychodynamical-ly oriented treatments may also be beneficial in the pal-liative care setting [33].
Unresolved issues
Before we can rely exclusively on scientific evidencewhen implementing psychotherapeutic programs in pal-liative care, the following issues need to be considered(Table 6). First, preventive interventions cannot yet beconceptualized. Second, it is necessary to ask whetherthe quantitative approaches used for the scientific evalu-ation of psychotherapeutic interventions are optimal forstudying the complex topic of psychotherapy with pa-tients who are facing the highly individual and existen-tial issues of life and death. Outcome measures of de-pression that define the “success” of a given interventionin palliative care have yet to be defined. Third, it re-mains unknown whether psychotherapeutic interven-tions, such as group therapies and structured treatmentsimplemented by trained counsellors that have been em-pirically tested, are beneficial for the majority of patientsor whether they should be used in selected populations inspecific clinical and cultural embeddings [19]. Fourth, afinal interesting question concerns the key elements ofpsychotherapeutic interventions. It is well known frompsychotherapeutic research that many nonspecific factorscommon to different interventions, such as empathy, pro-viding information and support, and mutual emotionalinvolvement, are key elements of psychotherapeutic pro-gress [44, 86, 92]. Given all the reasons described aboveand the complexity of the palliative care patients, highly
structured treatment modalities have to be regarded withcaution despite the empirical evidence of their usefulness[97].
Recommendations
It is suggested that at this point in time, the implementa-tion of psychological treatment should not be based onscientific evidence alone, and both highly structured psy-chotherapeutic treatments and other treatment modalitiesfor which there is clinical although not yet empirical evi-dence of effectiveness can be recommended. In view ofthe persisting lack of mental health professionals work-ing in palliative care, training of the nonpsychiatric staffis currently the most effective strategy to improve non-pharmacological treatment of the depressed patient withadvanced disease. The above-mentioned training in com-munication skills is a basic requirement in reaching thisgoal; however, it is only one element in improving thepsychological care of the depressed patient in palliativecare. Future research should focus on the effectivenessand role of nonspecific elements of the psychotherapeu-tic process. Owing to the high levels of depression insignificant others of patients in palliative care [39], theytoo, should benefit from these efforts (Table 7).
483
Table 6 Nonpharmacological treatment of depression in palliativecare: unresolved issues
Preventive interventions will have to be targeted, but the profile of patients at risk for depression remains unknownMany methodological aspects (e.g., concerning outcome) of psychotherapeutic intervention studies, are still controversial, and many of the studies in the palliative care setting have methodological flawsEfficacy of psychotherapeutic interventions has been demonstrated, but effectiveness studies are still lackingNonspecific elements of psychotherapeutic interventions, such as empathy, favoring emotional expression and informationare known to be beneficial, yet remain to be evaluated
Table 7 Nonpharmacological treatment of depression in palliativecare: recommendations
Implementation of psychological treatments should be based on clinical and scientific evidence at this point in timeTraining of nonpsychiatric staff (see recommendations for training) is currently the most effective strategy to improve the situation of the depressed patient in palliative careFuture research should focus on effectiveness studies and the unspecific therapeutic elements that can be offered by nonpsychiatric staffPsychotherapeutic efforts should also include the patients’ significant others

296 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
234
Psychopharmacological treatment
In most cases, management of major depression also in-volves pharmacological treatment. There has been con-siderable progress in the development of new antidepres-sants with a more favorable side effect profile facilitatingtheir use in the medically ill and the elderly [5, 66]. De-spite these developments, clinical utilization of thesesubstances remains stable over time and is restricted to asmall minority of patients with advanced disease [95]. Arecent study on the prescription of antidepressant medi-cation in palliative care found that only 10% of the pa-tients admitted to a palliative care inpatient unit weretreated with an antidepressant. In the majority of cases,the medication was initiated during the final 2 weeks oflife, consequently leaving insufficient time for the medi-cation to have any therapeutic effect [53]. Barriers to theuse of antidepressants derive from the patient (e.g., lackof compliance, fear of side effects) or from the physician(e.g., lack of training, unfamiliarity with these sub-stances) [49].
Thus, there is a considerable gap between the pro-gress in the development of newer antidepressants andtheir utilization. Even when the diagnosis of depressionhas been established and initiation of psychopharmaco-logical treatment seems obvious, less than a quarter ofdepressed psychiatric patients receive effective treatment[31, 67]. It is difficult to imagine that the situation in thepalliative care setting is any better. Although there aremany reports on the efficacy of antidepressants in de-pressed patients with advanced somatic disease, only afew controlled studies have been conducted [5]. Theseplacebo-controlled double-blind studies support the clin-ical experience indicating that these substances improvedepressive symptoms and quality of life [41, 81, 103]. Ifsuch treatment is indicated, these medications should beprescribed in a dose that guarantees therapeutic efficacy(therapeutic range). Medications should be changed ifthere is no appropriate response after a 2- to 3-weektreatment period with a therapeutic dosage [5]. After res-olution of the depressive state, they should be continuedfor at least 4–6 months and slowly tapered [88].
The era of antidepressants started with agents with ef-fects on multiple receptor systems, then progressed to se-lective agents with single pharmacological mechanisms,and we now have drugs that again offer multiple receptoractions but also selective mechanisms, reducing side ef-fects while maintaining clinical efficacy [5]. Becauseolder and newer antidepressants are equally efficacious[88, 106], both adverse effect profiles and pharmacologi-cal properties (half-life, interactions, accumulation in he-patic and renal impairment) should determine the one se-lected. The newer (serotoninergic) agents have fewerside effects; some of them are available in liquid formsfor patients with difficulties in swallowing and can beconsidered as first-line treatment in the presence of med-
ical illness [4]. Tricyclics or tetracyclics (mianserin) maystill be useful, for example in patients with concomitantinsomnia and neuropathic pain [57]. The reader is re-minded that tricyclic agents have anticholinergic and an-tihistaminic properties and should therefore be used withcaution in the elderly, in patients with advanced or car-diovascular disease, and in those also being treated withopiates [8]. Different tricyclics and serotoninergic agentsare significant inhibitors of the isoenzyme CYP2D6[101], which catalyzes the conversion of codeine intomorphine, and thus may almost completely abolish itsanalgesic action [22]. There has been a recent interest inphytotherapeutic agents (hypericum extracts) for depres-sion of moderate intensity [74]; no studies have yet beenconducted with these substances in palliative care. Final-ly, mirtazepine, one of the newest agents with both sero-toninergic and noradrenergic actions, seems to be welltolerated in the elderly [34], but again has not been stud-ied in the palliative care setting.
Amphetamines (psychostimulants) have also beenused for the treatment of depression in palliative care.They are known to improve arousal, energy, ability toconcentrate and depressive symptoms [42]. They have arapid onset of action (within 2 days) and may thereforebe useful for patients with limited survival [71]. Severalopen trials and also randomized double-blind placebo-controlled studies in depressed medically ill patientshave led to the conclusion that amphetamines are effec-tive in relieving depressive symptoms, especially in ad-justment disorders (but also major depression) and inwomen [42, 55, 108]. They should not be prescribed toagitated or anxious patients [10, 42]. During the latentperiod before antidepressants take effect, alternativetreatments with benzodiazepines [40, 98] and neurolep-tics [63] may also be considered, especially for patientsin the terminal phase of their life.
Unresolved issues
Some of the unresolved issues are listed in Table 8. Stud-ies comparing different classes of medications for differ-ent clinical situations, such as for rapid relief of symp-toms or rapid onset of action until antidepressant treat-ment is effective, are still lacking, and clinical experienc-es remain somehow controversial. Such studies withhigher numbers of patients would be of great impor-tance, but are not easy to conduct because of recruitmentdifficulties, drop-outs and intercurrent disease and treat-ment variables [41]. Finally, various factors hamperingeffective psychopharmacological treatment remain un-known.
484

| 297 297Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
235
Recommendations
There is enough clinical and scientific evidence to justifyexploiting the benefit of these medications, even in a ter-minal stage of disease (see Table 9) [14]. Medicationshould be started without delay, like any other therapyaimed at symptom control. In patients with limited lifeexpectancy, amphetamines may be considered. For therelief of suffering until antidepressants are effective andin anxious and depressed patients, benzodiazepines andneuroleptics may also be useful. Strategies to improvepharmacological treatment cannot be conceptualizedseparately, but should be part of a comprehensive man-agement strategy based on a proactive but thoughtful ap-proach with due consideration for all aspects of depres-sion in palliative care. Future research should focus oninterventions directed at barriers that hamper adequateprescription of antidepressants.
Conclusions
Depression in palliative care is a most complex topic,being associated with many unresolved issues as well asa lack of scientific evidence. The major problem remainsthe underdetection and undertreatment of the disorder,both of which are related to a variety of different factors,only some of which have been identified (Table 10). Aproactive approach to this problem should include clini-cal, scientific and educational aspects and address detec-tion and treatment of depression in palliative care in acomprehensive manner. Such an approach would over-come the shortcomings of isolated actions, which losetheir impact in targeting the individual levels of theproblem separately. In order to achieve these objectives,interdisciplinary cooperation with specialized mentalhealth professionals from consultation-liaison psychiatryand psychooncology will be necessary.
Acknowledgment The authors wish to thank Heidi Blumhuberfor her help in organizing this expert working group and for hercontinuous support of the Research Network of the European As-sociation for Palliative Care.
485
Table 8 Psychopharmacological treatment of depression in pallia-tive care: unresolved issues
Effectiveness studies comparing different agents are still lackingThe value of alternative substances, such as amphetamines, for pa-tients with limited survival times remains unknownA variety of patient-, physician- and health care-related factorshamper effective pharmacological treatment; yet they have notbeen identified and targeted in intervention studies
Table 9 Psychopharmacological treatment of depression in pallia-tive care: recommendations
Antidepressants should be utilized without delay once the diagnosis of major depression has been establishedUntil effectiveness or if survival time is very limited, amphetamines, benzodiazepines and neuroleptics should be consideredStrategies to improve pharmacological treatment should not beconceptualized separately, but should be part of an comprehensivemanagement strategyFuture research should attempt to identify and target factors thathamper effective pharmacological treatment
Table 10 Conclusions
– Undertreatment and underdetection of depression in palliative care remains a major problem impairingthe quality of life of the patients and their significant others
– A proactive and comprehensive approach should be favored.Such an approach addresses detection and treatmentof depression in palliative care and training,and consists in clinical, scientific and educational strategies
– A flexible approach should be adopted to the implementation of general guidelines, depending on the setting
– Close collaboration with specialized mental healthprofessionals is highly recommended
– Clinical experience and scientific evidenceshould be considered when psychological treatmentmodalities are implemented
– Studies evaluating different comprehensive approachesshould be initiated
References
1. American Psychiatric Association(1994) Diagnostic and statistical manu-al of mental disorders, 4th edn. Ameri-can Psychiatric Association, Washing-ton, DC
2. Badger LW, deGiny FV, Hartman J, etal (1994) Psychosocial interest, medi-cal interviews, and the recognition ofdepression. Arch Fam Med 3:899–907
3. Ballenger JC, Davidson JR, LecrubierY et al (1999) Consensus statement onthe primary care management of de-pression from the International Con-sensus Group on Depression and Anxi-ety. J Clin Psychiatry 60 [Suppl7]:54–61
4. Beliles K, Stoudemire A (1998) Psy-chopharmacological treatment of de-pression in the medically ill. Psychoso-matics 39:2–19
5. Berney A, Stiefel F, Mazzocato C, Buclin T (2000) Psychopharmacologyin supportive care in cancer: a reviewfor the clinician. III. Antidepressants.Support Care Cancer 8:278–286

298 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
236
6. Block SD, for the ACP-ASIM End-of-life Care Consensus Panel (2000) As-sessing and managing depression in theterminally ill. Ann Intern Med132:209–216
7. Bottomley A (1998) Depression in can-cer patients: a literature review. Eur JCancer Care 7:181–191
8. Breitbart W, Passik S (1993) Psychiat-ric aspects of palliative care. In: DoyleD, Hanks GW, MacDonald N (eds) Ox-ford textbook of palliative medicine.Oxford University Press, New York, pp 609–626
9. Breitbart W, Bruera E, Cochinov H,Lynch M (1995) Neuropsychiatric syn-dromes and psychological symptoms inpatients with advanced cancer. J PainSymptom Manage 10:131–141
10. Bruera E, Miller MJ, Macmillan K, et al (1992) Neuropsychological effectsof methylphenidate in patients receiv-ing a continuous infusion of narcoticsfor cancer pain. Pain 48:163–168
11. Buckberg JB, Holland JC (1980) Aprevalence study of depression in acancer hospital population. Proc AmAssoc Cancer Res 21:382
12. Burton MV, Parker RW (1995) A ran-domised controlled trial of preopera-tive psychological preparation for mas-tectomy. Psychooncology 4:1–20
13. Caraceni A, Cherny N, Fainsinger R,Kaasa S, Poulin P, Radbruch L and theEAPC Research Network SteeringCommittee (2001) Pain measurementtools and methods in clinical research.J Pain Symptom Manage (submittedfor publication)
14. Chaturvedi SK, Maguire P, Hopwood P(1994) Antidepressant medication incancer patients. Psychooncology3:57–60
15. Cherny N, Ripamonti C, Davis C, Fallon M, McQuay H, Mercadente S,Pasternack G, Pereira J, Ventafridda Vand the EAPC Research NetworkSteering Committee (2001) Strategiesto manage the adverse effects of oralmorphine: an evidence-based report. J Clin Oncol (in press)
16. Clayton P (1974) Mourning and de-pression: their similarities and differ-ences. Can J Psychiatry 1:309–312
17. Coyle N, Adelhardt J, Foley K, Porte-noy R (1990) Character of terminal ill-ness in advanced cancer patients: painand other symptoms during the last4 weeks of life. J Pain Symptom Man-age 5:83–93
18. Crisman ML, Trivedi M, Pigott TA,Rush HJ, Hirschfeld RM, et al (1999)The Texas Medication Algorithm Pro-ject: report of the Texas ConsensusConference Panel on Medication Treat-ment of Major Depressive Disorder. JClin Psychiatry 60:142–156
19. Cunningham AJ (1995) Group psycho-logical therapy for cancer patients. Abrief discussion of indications for itsuse, and the range of interventionsavailable. Support Care Cancer3:244–247
20. De Haes F, van Knippnberg F, Neijt J(1990) Measuring psychological dis-tress in cancer patients: structure andapplication of the Rotterdam SymptomChecklist. Br J Cancer 62:1034–1038
21. Derogatis LT, Morrow GR, Fetting J,Penman D, Piasetsky S, et al (1983)The prevalence of psychiatric disordersamong cancer patients. JAMA249:751–757
22. Desmeules J, Gascon MP, Dayer P,Magistris M (1991) Impact of environ-mental and genetic factors on codeineanalgesia. Eur J Clin Pharmacol41:23–26
23. Die Trill M (2000) Los trastornos delestado de animo y el suicido en paci-ente en fase terminal. In: Die Trill M,Lopez Imedio E (eds) Aspectos psico-logicos en cuidados palliativos. ADES,Madrid, pp 189–210
24. Dugan W, McDonald MV, Passik SD,Rosenfeld BD, Theobald D, Egerton S(1998) Use of the Zung Self-RatingDepression Scale in cancer patients: fe-asability as a screening tool. Psychoon-cology 7:483–493
25. Endicott J (1984) Measurement of de-pression in patients with cancer. Can-cer 53 [10 Suppl]:2243–2249
26. Fallowfield L, Lipkin M, Hall A(1998) Teaching senior oncologistscommunication skills: results fromphase I of a comprehensive longitudi-nal program in the United Kingdom. J Clin Oncol 16:1961–1968
27. Fawzy IF, Fawzy NW, Hyun CS,Eloskoff R, Guthrie D, Fakey JL, Morton DL (1993) Effects of an earlystructured psychiatric intervention oncoping and affective state, recurrenceand survival 6 years later. Arch GenPsychiatry 50:681–689
28. Fürst CJ, Kaasa S, Andrews P, Ellershaw J, Siegel T, Stiefel F, WalshD, and the EAPC Research NetworkSteering Committee (2001) The indica-tions for and use of steroids in pallia-tive cancer. (submitted for publication)
29. Golden RN, McCartney CF, HaggertyJJ Jr, Raft D, Nemeroff CB, et al(1991) The detection of depression bypatient self-report in women with gy-necological cancer. Int J PsychiatryMed 21:17–27
30. Goldenberg D (1972) The detection ofpsychiatric illness by questionnaire.(Maudsley Monogr) Oxford UniversityPress, Oxford
31. Goldman LS, Nielsen NH, ChampionHC (1999) Awareness, diagnosis, andtreatment of depression. J Gen InternMed 14:569–580
32. Greer S, Moorey S, Baruch JD, WatsonM, Robertson BM, Bason A, RowdenL, Law M, Bliss J (1992) Adjuvantpsychological therapy for patients withcancer: a prospective randomised trial.Br Med J 304:675–680
33. Guex P, Stiefel F, Rousselle I (2000)Psychotherapy with patients with can-cer. Psychother Rev 2:269–273
34. Halikas JA (1995) Org 3770 (mirtaze-pine) versus trazodone: a placebo con-trolled trial in depressed elderly pa-tients. Hum Psychopharmacol10:125–133
35. Hall A, A’Hern R, Fallowfield L(1999) Are we using appropriate self-report questionnaires for detecting anx-iety and depression in women with ear-ly breast cancer? Eur J Cancer35:79–85
36. Hamblin J, Connor PD (1998) Cancerscreening guideline preference surveys:physicians’ perception of the AmericanCancer Society. Tenn Med 91:17–20
37. Hammerlid E, Ahlner-Elmqvist M,Bjordal K, Biorklund A, Evensen J,Boysen M, Jannert M, Kaasa S, Sullivan M, Westin T (1999) A prospec-tive multicenter study in Sweden andNorway of mental distress and psychiat-ric morbidity in head and neck cancerpatients. Br J Cancer 80:766–774
38. Hanks G, De Conno F, Cherny N, et al(1996) Morphine in cancer pain: modesof administration. BMJ 312:823–826
39. Holland JC (1989) Lung cancer. In:Holland JC, Rowland JH (eds) Hand-book of psychooncology. Oxford Uni-versity Press, New York, pp 180–187
40. Holland JC, Morrow G, Schmale A, etal (1991) A randomized clinical trial ofalprazolam versus progressive musclerelaxation in cancer patients with anxi-ety and depressive symptoms. J ClinOncol 9:1004–1011
41. Holland JC, Romano SJ, HeiligensteinJH, Tepner RG, Wilson MG (1998) Acontrolled trial of fluoxetine and desi-pramine in depressed women with ad-vanced cancer. Psychooncology7:291–300
42. Homsi J, Walsh D, Nelson KA (2000)Psychostimulants in supportive care.Support Care Cancer 8:385–397
43. Hopwood P, Howell A, Maguire P(1991) Screening for psychiatric mor-bidity in patients with advanced breastcancer: validation of two self-reportquestionnaires. Cancer 64:353–356
44. Horvath AO, Symonds BD (1991) Re-lation between working alliance andoutcome in psychotherapy: a meta-analysis. J Couns Psychol 38:139–149
45. Ibbotson T, Maguire P, Selby P, Priestman T, Wallace L (1994) Screen-ing for anxiety and depression in can-cer patients : the effect of disease andtreatment. Eur J Cancer [A] 30:37–40
486

| 299 299Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
237
46. Kaasa S, Malt U, Hagen S, Wist E,Moum T, Kvikstad A (1993) Psycho-logical distress in cancer patients withadvanced disease. Radiother Oncol27:193–197
47. Kathol RG, Mutgi A, Williams J, Clamon G, Noyes R (1990) Diagnosisof major depression in cancer patientsaccording to four sets of criteria. Am JPsychiatry 147:1021–1024
48. Katon W, Gonzales J (1994) A reviewof randomized trials of psychiatric con-sultation-liaison studies in primarycare. Psychosomatics 35:268–278
49. Keller MB (1999) The long-term treat-ment of depression. J Clin Psychiatry60 [Suppl 17]:41–48
50. Kick SD (1999) An educational inter-vention using the agency for healthcare policy and research depressionguidelines among internal medicineresidents. Int J Psychiatry Med29:47–61
51. Kugaya A, Akechi T, Okuyama T, Okamura H, Uchitomi Y (1998)Screening for psychological distress inJapanese cancer patients. Jpn J ClinOncol 28:333–338
52. Le Fevre P, Deveneux J, Smith S,Lawnie SM, Cornbleet M (1999)Screening for psychiatric illness in thepalliative care inpatient setting: a com-parison between the Hospital Anxietyand Depression Scale and the GeneralHealth Questionnaire-12. Palliat Med13:399–407
53. Lloyd-Williams M, Friedman T, RuddN (1999) A survey of antidepressantprescribing in the terminally ill. PalliatMed 13:243–248
54. Lynch ME (1995) The assessment andprevalence of affective disorders in ad-vanced cancer. J Palliat Care 11:10–18
55. Macleod AD (1998) Methylphenidatein terminal depression. J Pain Symp-tom Manage 16:193–198
56. Maekin C (1992) Screening for depres-sion in the medically ill. The future ofpaper and pencil tests. Br J Psychiatry160:212–216
57. Magni G, Conlon P, Arsie D (1987)Tricyclic antidepressants in the treat-ment of cancer pain: a review. Pharma-copsychiatry 20:160–164
58. Maguire GP, Tait A, Brooke M, Thomase C, Sellwood R (1980) Effectsof counselling on the psychiatric mor-bidity associated with mastectomy. BrMed J 281:1454–1456
59. Maguire P (1997) Depression and can-cer. In: Robertson MM, Katona CLE(eds) Depression and physical illness.Wiley, Chichester, pp 429–441
60. Maguire P, Selby P (1989) Assessingquality of life in cancer patients. Br JCancer 60:437–440
61. Maguire P, Faulkner A, Booth K, Elliott C, Hillier V (1996) Helping can-cer patients disclose their concerns.Eur J Cancer [A] 32:78–81
62. Massie MJ (1989) Depression. In: Holland JC, Rowland JH (eds) Hand-book of psychooncology. Oxford Uni-versity Press, New York, pp 273–290
63. Mazzocato C, Stiefel F, Berney A, Buclin T (2000) Psychopharmacologyin supportive care in cancer: a reviewfor the clinician. II. Neuroleptics. Support Care Cancer 8:89–97
64. McDonald MV, Passik SD, Dugan W,Rosenfeld B, Theobald DE, Egerton S(1999) Nurses’ recognition of depres-sion in their patients with cancer. On-col Nurs Forum 26:593–599
65. Mercadente S, Radbruch L, CaraceniA, et al and the EAPC Research Net-work Steering Committee (2001)Breakthrough pain – episodic pain.(submitted for publication)
66. Montgomery SA (1999) New developments in the treatment of depression. J Clin Psychiatry 60 [Suppl 14]:10–15
67. Montgomery SA, Kasper S (1998) Depression: a long-term illness and itstreatment. Int Clin Psychopharmacol13 [Suppl 6]:S23–S26
68. Moorey S, Greer S, Bliss JM, Law M (1989) A comparison of adjuvant psychological therapy and supportive counselling in patientswith cancer. Psychooncology7:218–228
69. Newell S, Sanson-Fisher RW, Girgis A,Bonaventura A (1998) How well domedical oncologists’ perception reflecttheir patients’ reported physical andpsychosocial problems? Data from asurvey of five oncologists. Cancer83:1640–1651
70. Nordin K, Berglund G, Glimelius B,Sjödén PO (1999) Predicting anxietyand depression among cancer patients(abstract 104). Psychooncology 8 [6 Suppl]:28
71. Olin J, Masand P (1996) Psychostimu-lants for depression in hospitalised can-cer patients. Psychosomatics 37:57–62
72. Passik SD, Dugan W, McDonald MV,Rosenfeld B, Theobald DE, Egerton S(1998) Oncologists’ recognition of de-pression in their patients with cancer. JClin Oncol 16:1594–1600
73. Passik S, Theobald D, Lundberg J,Donaghy K, Holtsclaw E. Kirsk K(1999) The initial experience with anti-depressant algorithm in a communitybased oncology clinic (abstract 70).Psychooncology 8 [6 Suppl)]:20
74. Philipp M, Kohnen R, Hiller K (1999)Hypericum extract versus imipramineor placebo in patients with moderatedepression: randomized multicentrestudy of treatment for eight weeks.BMJ 319:1534–1539
75. Power D, Kelly S, Gilsenan J, et al(1993) Suitable screening tests for cog-nitive impairment and depression in theterminally ill – a prospective study.Palliat Med 7:213–218
76. Ramirez AJ, Richards MA, Jarrett SR,Fentiman IS (1995) Can mood disor-ders be identified preoperatively? Br JCancer 72:1509–1512
77. Razavi D, Stiefel F (1994) Commonpsychiatric disorders in cancer patients:adjustment disorders and depressivedisorders. Support Care Cancer2:223–232
78. Razavi D, Delvaux N, Farvacques C,Robaye E (1990) Screening for adjust-ment disorders and major depressivedisorders in cancer inpatients. Br J Psy-chiatry 156:79–83
79. Razavi D, Delvaux N, Bredart A, Paesmans N, Debusscher L, Bron D,Stryckmans P (1992) Screening forpsychiatric disorders in a lymphomaoutpatient population. Eur J Cancer [A]28:1869–1872
80. Razavi D, Delvaux N, Marchal S, Bredart A, Farvacques C, Paesmans M(1993) The effect of a 24-h psychologi-cal training program on attitudes, com-munication skills and occupationalstress in oncology: a randomised study.Eur J Cancer [A] 29:1858–1863
81. Razavi D, Alliaire JF, Smith M, Salimpour A, Verra M, et al (1996) Theeffect of fluoxetine on anxiety and de-pression symptoms in cancer patients.Acta Psychiatr Scand 94:205–210
82. Regier DA, Kessler LG, Burns BJ,Goldberg ID (1979) The need for apsychosocial classification system inprimary-care settings. Int J MentHealth 8:16–29
83. Ripamonti C, Twycross R, Baines M,Bozzetti F, Capri S, et al (2001) Clini-cal-practice recommendations for themanagement of bowel obstruction.Support Care Cancer (in press)
84. Robbins JM, Kirmayer LJ, Cathbras P,et al (1994) Physician characteristicsand the recognition of depression andanxiety in primary care. Med Care32:795–812
85. Saltzburg D, Breitbart W, Fishman B,Stiefel F, Holland J, Foley K (1989)The relationship of pain and depressionto suicidal ideation in cancer patients(abstract). Proc Am Soc Clin OncolAnnual Meeting 8:312
86. Sexton HC, Hembre K, Kvarme G(1996) The interaction of the allianceand therapy microprocess: a sequentialanalysis. J Couns Clin Psychol64:471–480
87. Sheard T, Maguire P (1999) The effectof psychological interventions on anxi-ety and depression in cancer patients:results of two meta-analyses. Br J Can-cer 80:1770–1780
487

300 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
238
88. Snow V, Lascher S, Mottur-Pilson C,for the American College of Physicians/ American Society of Internal Medi-cine (2000) Pharmacological treatmentof acute major depression and dysthy-mia. Ann Intern Med 132:738–742
89. Spiegel D (1995) Essentials of psycho-therapeutic intervention for cancer pa-tients. Support Care Cancer 3:252–256
90. Spiegel D, Bloom JR, Yalom ID (1981)Group support for patients with meta-static breast cancer. Arch Gen Psychia-try 38:527–533
91. Spitzer RL, Kroenke K, Linzer M,Hahn SR, Williams JB, deGruy FV3rd, Brody D, Davies M (1995)Health-related quality of life in primarycare patients with mental disorders.Results from the PRIME-MD 1000Study [see comments]. JAMA274:1557
92. Stern DN, Sander LW, Nahum JP, Harrison AM, Lyons-Ruth K, et al(1998) Non-interpretive mechanisms inpsychoanalytic therapy – the “some-thing more” than interpretation. Int JPsychoanal 79:903–921
93. Stiefel F (1993) Psychosocial aspectsof cancer pain. Support Care Cancer1:130–134
94. Stiefel F, Razavi D (1994) Commonpsychiatric disorders in cancer patients:anxiety and acute confusional states.Support Care Cancer 2:233–237
95. Stiefel F, Kornblith A, Holland J(1990) Changes in the prescription pat-terns of psychotropic drugs for cancerpatients during a 10-year period. Can-cer 65:1048–1053
96. Stiefel F, Glaus A, Morant R, Senn HJ(1994) Advanced cancer patients in apalliative care unit: how prevalent arepsychiatric disorders and how shouldthey be screened? Paper presented atthe 8th Congress of the Society ofPsychosocial Oncology, Budapest,1–3 September 1994
97. Stiefel F, Guex P, Real O (1998) Anintroduction to psycho-oncology withspecial emphasis on its developmentin the historical and cultural context.In: Portenoy RK, Bruera E (eds) Top-ics in palliative care, vol 3. OxfordUniversity Press, New York, pp175–190
98. Stiefel F, Berney A, Mazzocato C(1999) Psychopharmacology in sup-portive care in cancer: a review forthe clinician. I. Benzodiazepines.Support Care Cancer 7:379–385
99. Swire N, George RJD (1997) Depres-sion in palliative care. In: RobertsonMM, Katona CLE (eds) Depressionand physical illness. Wiley, Chiches-ter, pp 443–464
100. Tiemens BG, Ormel J, Simon GE(1996) Occurrence, recognition, andoutcome of psychological disorder inprimary care. Am J Psychiatry153:636–644
101. Touw DJ (1997) Clinical implicationsof genetic polymorphisms and druginteractions mediated by cytochromeP-450 enzymes. Genet Metab DrugInteract 14:55–82
102. Valente SM, Saunders JM (1997) Diagnosis and treatment of major de-pression among people with cancer.Cancer Nurs 20:168–177
103. Van Heering K, Zivkov M (1996)Pharmacological treatment of depres-sion in cancer patients. A placebo-controlled study of mianserin. Br JPsychiatry 169:440–443
104. Wells KB, Stewart A, Hays RD, Burnam MA, Rogers W, et al (1989)The functioning and well-being of de-pressed patients. JAMA 262:914–919
105. Wilkinson S, Maguire P, Tait A(1988) Life after breast cancer. NursTimes 54:34–37
106. Williams JW, Mulrow D, Chiquette E,Hitchcock Noël P, Aguilar C, CornellJ (2000) A systematic review of new-er pharmacotherapies for depressionin adults: evidence report summary.Ann Intern Med 132:743–756
107. Wilson KG, Enus M, Lander S (1994)The prevalence of depression in theterminally ill: effects of diagnosticcriteria and symptom threshold judg-ments. Am J Psychiatry 151:537–540
108. Wilwerding MB, Loprinzi CL, Mail-lard JA, et al (1995) A randomizedcross-over evaluation of methylpheni-date in cancer patients receivingstrong narcotics. Support Care Cancer3:135–138
109. Wise MG, Rundell JR (eds) (1994)Concise guide to consultation psychi-atry, 2nd edn. American PsychiatricPress, Washington, DC
110. Woolf SH (1999) Clinical guidelines:potential benefits, limitations, andharms of clinical guidelines. BMJ318:527–530
111. Worden JW, Weisman AD (1984) Pre-ventive psychological interventionwith newly diagnosed cancer patients.Gen Hosp Psychiatry 6:243–249
112. World Health Organization (1990)Cancer pain relief and palliative care.(Technical report series 804) WHO,Geneva
113. Zigmond A, Snaith R (1983) TheHospital Anxiety and DepressionScale. Acta Psychiatr Scand67:361–370
488

| 301 301Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
239
© U.S. Cancer Pain Relief Committee, 2002 0885-3924/02/$–see front matterPublished by Elsevier, New York, New York PII S0885-3924(01)00409-2
Vol. 23 No. 3 March 2002 Journal of Pain and Symptom Management 239
Special Article
Pain Measurement Tools and Methods in Clinical Research in Palliative Care: Recommendations of an Expert Working Group of the European Association of Palliative Care
Augusto Caraceni, MD, Nathan Cherny, MBBS, FRACP, Robin Fainsinger, MD, Stein Kaasa, MD, Philippe Poulain, MD, Lukas Radbruch, MD,Franco De Conno, MD, and the Steering Committee of theEAPC Research Network
Rehabilitation and Palliative Care Unit (A.C., F.D.C.), National Cancer Institute of Milan, Milan, Italy; Pain & Palliative Medicine Service (N.C.), Shaare Zedek Medical Center, Jerusalem, Israel; Palliative Care Program (R.F.), Royal Alexandra Hospital, Edmonton, Alberta, Canada; Palliative Medicine Unit (S.K.), University Hospital of Trondheim, Trondheim, Norway; Analgesia Consult Service (P.P.), Institut Gustave-Roussy, Paris, France; and Anesthesiology Clinic (L.R.), University of Cologne, Cologne, Germany
Abstract
An Expert Working Group was convened under the auspices of the Steering Committee of the Research Network of the European Association of Palliative Care to review the status of the use of pain measurement tools (PMTs) in palliative care research conducted in a multilingual-multicenter setting. Based on a literature review and on the experts’ opinion, the present work recommends that standardized methods should be applied for the use of PMTs in research in palliative care. Visual analogue scales, numerical rating scales, and verbal rating scales are considered valid to assess pain intensity in clinical trials and in other types of studies. Among the multidimensional questionnaires designed to assess pain, the McGill Pain Questionnaire and Brief Pain Inventory are valid in many multilingual versions. Specific recommendations for PMT use and administration, depending on the study type and aim, are reviewed. Special population requirements specific of clinical situations encountered in palliative care (elderly, terminal, cognitively impaired patients, pediatric patients) are also considered.
J Pain Symptom Manage 2002;23:239–255.
©
U.S. Cancer Pain Relief Committee
,
2002
.
Key Words
Palliative care, pain, pain measurement, clinical trials
Introduction
Pain is among the most common and distress-ing symptoms encountered by patients with ad-vanced cancer and other terminal illnesses. Therelief of pain is a clinical task at the very heart ofthe endeavor of palliation. The challenge of
Address reprint requests to:
Augusto Caraceni, MD, Neu-rology Unit, Rehabilitation and Palliative Care Unit,National Cancer Institute of Milan, via Venezian 1,20133 Milan, Italy.
Accepted for publication: June 19, 2001.

302 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
240
240 Caraceni et al. Vol. 23 No. 3 March 2002
this task is to achieve effective relief with mini-mal side effects and to deliver this service to allpatients in need of these interventions. Successin meeting this challenge requires delineationof the scope of the problem, characterization ofthe pain syndromes, determination of optimaltherapeutic strategies, identification of barriersto implementation of effective strategies, deter-mination of strategies to overcome these ob-structions, and the monitoring of outcomes forpurposes of continual quality improvement.
Evidence-based medicine requires the testingand evaluation of strategies to assure their effec-tiveness and to define optimal approaches forall contingent indications. Through this ap-proach, ineffective strategies are to be discardedand effectual strategies are submitted to trialsagainst competing options to determine thebest approach to serve as the standard for futurecomparison. It is incumbent upon palliativecare practitioners to participate in the challengeof clinical research to enhance the efficacy ofpalliative practices to the benefit of our pa-tients and their families.
1
Interpretation of re-search data requires that the data be valid andrecorded in an interpretable format. In clinicalstudies on pain, valid and reliable outcomesshould be used. Furthermore, in order to com-pare data between studies, a standardization ofoutcomes, namely, pain measures, will increasethe validity of the comparisons.
Many approaches to the measurement ofpain attributes have evolved over the past fourdecades. Some of them have been applied tocancer pain and palliative care,
2
but the selec-tion and application of these approaches inpalliative care has often been capricious andidiosyncratic. The lack of uniformity in the ap-proach to outcome measurement in evaluatingchronic pain conditions has diminished fromthe ability to draw meaningful conclusionsfrom much of the published literature.
3–5
This article reports the results of the work ofan Expert Working Group which was convenedunder the auspices of the European Associa-tion of Palliative Care (EAPC) Research Net-work to prepare recommendations for the mea-surement of pain in palliative care research.
Research Issues in Palliative Medicine
The patient populations that are the focus ofpalliative medicine are often frail, and have de-
teriorating health and multiple symptoms. Atthe end of life, cognitive impairment of vari-able severity is common. These factors impactboth the ability to extrapolate pain manage-ment data derived from other clinical contextswith relatively healthy patient populations andthe ability to conduct clinical research. Theyspecifically influence the processes of data col-lection necessary for prospective studies. Re-search methodologies must be sensitive to theseconsiderations. Specific recommendations willbe made for approaches suitable for patientswith cognitive impairment and for children.
No valid instrument is applicable at the mo-ment for the assessment of pain in the cogni-tively impaired. A behavioral scale has been re-cently designed for pain assessment in thecognitively impaired patient and its validationis ongoing (DOLOPLUS, Bernard Wary, per-sonal communication).
Study Types
The working group defined six types of painstudies in palliative care, three descriptivestudy designs and three intervention designs(Table 1).
Descriptive Studies
Descriptive studies of pain are needed to de-fine the prevalence and severity and scope ofpain in various patient populations encoun-tered in palliative care. These studies are per-formed to clarify clinical variability, paincourse and prognosis, quality of care, and ser-vices. Depending upon the epidemiologicalmethod used, the results of these studies giveinformation of varied generalizability.
1. Prevalence/severity studies: Pain is evalu-ated in a specific patient population todefine its prevalence and severity.
6–10
Table 1
Study Types
Descriptive Studies
Prevalence/severity studiesTrajectory studiesPain syndrome characterization
Intervention Studies
Phase IPhase IIPhase III

| 303 303Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
241
Vol. 23 No. 3 March 2002 Pain Measurement Tools in Palliative Care 241
2. Trajectory studies: Pain is evaluated at re-peated intervals in a defined patient pop-ulation over time.
11
3. Pain syndrome characterization: The clin-ical characteristics of pain and its rela-tionship to clinical and investigation find-ings are collated to define and to describespecific pain syndromes.
12
Intervention Studies
Intervention studies are needed to evaluatethe effect of a therapeutic strategy. Pain man-agement interventions may include primarytherapies against the underlying pathology, an-algesic drug therapy, invasive interventions,and psychological or social interventions.
1. Phase I studies: This term typically refersto drug interventions with new agents. Theaim of the study is to define the maximaldose range that can be administered with-out excessive toxicity and to determine theacute toxicity profile of the agent.
2. Phase II studies: This term refers to pro-spective studies aimed at evaluating theimpact of a study intervention with regardto the primary outcome, pain; secondaryoutcomes, such as quality of life and satis-faction; and costs, such as adverse effectsand treatment-related resource utilization.
In the evaluation of analgesic drugs, Phase Iand II studies are often combined. In additionto essential pharmacokinetic data, pharmacody-namic effects including analgesia and adverseeffects are measured. Pharmacokinetic/phar-macodynamic (PK/PD) studies correlate drugeffects with measurement of plasma concentra-tion in blood or other relevant compartments,such as cerebrospinal fluid. PK/PD studies maybe performed with a single administration of astudy drug or prolonged administration.
3. Phase III studies: This term refers to stud-ies comparing the relative efficacy of twoor more treatment approaches with a viewto determining an optimal approach.These studies typically evaluate drugs withsimilar outcomes in phase II studies.
Pain evaluation approaches must be appro-priate for the study type and patient popula-tion that will constitute the subjects of thestudy.
Covariates
A list of the covariates that are most relevantto pain studies in palliative care is provided inTable 2.
Description of Pain MeasurementTools (PMTs)
Pain is a subjective sensation which can bedescribed according to several relevant fea-tures or attributes (quality, location, intensity,aversiveness, emotional impact, frequency, etc.).Among these attributes, intensity is recognizedas one of the most relevant clinical dimensionof the pain experience.
13
Being a subjective ex-perience, there is no objective method to mea-sure pain. However, pain intensity can be mea-sured in patients in a reliable and valid way byrecording the self-rating of the sensation ondifferent types of scales.
14–20
When consideringpain assessement limited to the intensity di-mension, PMTs should have a unidimensionalstructure.
Since clinical pain is not only the product ofa primary sensory modality, but rather, a com-plex human experience with functional, emo-tional, social, and spiritual components, multi-dimensional PMTs and health-related qualityof life measures are also appropriate to addressspecific research questions related to the mea-surement of pain intensity.
The measurement of pain for purposes ofclinical research demand that the selected toolis valid and appropriate to the patient popula-tion and the study design. The Expert WorkingGroup reviewed unidimensional and multidi-mensional pain measurement tools suitable forthis purpose.
Unidimensional Pain Measurement Tools
Three types of unidimensional pain mea-surement tools were considered, visual ana-logue scales (VAS), categorical verbal ratingscales (VRS), and categorical numerical ratingscales (NRS). All of these approaches are com-monly used to measure pain intensity and arewell validated in the cancer population.
21–27
VAS, VRS, and NRS are also commonly used tomeasure pain relief.
25,27
When applied in the chronic nonmalignantpain or cancer pain populations, the unidi-mensional pain scales—VAS, NRS and VRS canbe considered equivalent. The choice should

304 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
242
242 Caraceni et al. Vol. 23 No. 3 March 2002
be influenced by practical considerations basedon available knowledge (see also Table 3).
28
Numerous verbal rating scales exist and usedifferent words in different languages. The ver-bal 15-level scale developed by Gracely et al.for rating experimental pain can be consid-ered a ratio scale,
14,15
but this is not proven forthe many scales available in the literature. Af-ter much discussion of the issues related totranslational validity of verbal rating scales, theExpert Working Group recognized that a sim-ple intensity scale of “none, mild, moderate,and severe” is the most widely used in the clini-cal context, but also that scales with a largernumber of intervals are more desirable, bothin research and in clinical practice, because ofhigher sensitivity to treatment effects.
15
A vali-dated multilingual translation of the more sim-ple VRS does not exist, but a valid multilingualsix-level VRS is presented in Appendix 1.
29
The VAS has been studied and is often con-sidered an ideal scale, because it is continuous,approximates a ratio scale, and is more inde-pendent from language than verbal scales (al-though the choice of the extreme anchor wordsor end-phrases can be relevant).
16,19,20,30
On theother hand, its validity more strongly depends onthe appropriateness of administration methodand of the instructions given to the study sub-jects.
19,20
It is, therefore, more difficult to usethan other scales.
Evidence suggests that numeric rating scalesare easier to apply and are associated with bet-ter compliance than the VAS.
28,31
Based on theavailable evidence,
17,28,32
the use of a standard0–10 numeric rating scale and 100-mm horizon-
tal visual analogue scale can be recommended.Although these are typically administered withpen and paper, other valid approaches includethe use of touch screens for VAS and NRS, slid-ing scales, and verbally administered numericrating scales.
20
For purposes of intervention studies, both painintensity and pain relief can be measured.
21,22
Pain relief can be measured by asking the pa-tients to compare pain now with previous painexperiences. Pain relief measurement validityis limited to short-term intervention studies(24 hours or less); in chronic studies, its valid-ity has been seriously questioned
33
and theconstruct underlying its meaning in descriptivestudies is uncertain.
5,6,34,35
Multidimensional Pain Measuring Tools
Three multidimensional scales were consid-ered, the McGill Pain Questionnaire, the BriefPain Inventory, and the Memorial Pain Assess-ment Card. Although recognizing that otherinstruments exist
36
or are under study,
37,38
theExpert Working Group recommends the use ofthe Short form of the Brief Pain Inventory orthe McGill Pain Questionnaire. Both of thesetools are well validated in multiple languagesand are thus suitable for application in an in-ternational setting. The Expert Working Groupwithheld recommendation of the MemorialPain Assessment Card
35
because it is not vali-dated in languages other than English.
The Brief Pain Inventory (BPI)
39
is a simpleand easy to administer tool that provides infor-mation about the history, intensity, location,and quality of pain. Numeric scales (range 0 to 10)
Table 2
Recommendations for Clinical and Pain-Related Covariates to be Documented in Pain-Related Studies
Basic demographic data to be collected for all studies1. Age2. Sex3. Disease diagnosis4. Predominant pain mechanism: neuropathic, nociceptive (visceral or somatic), idiopathic5. Performance status6. Cognitive function: normal or impaired7. Current analgesic therapy: Drug(s), dose(s), non-drug therapies
Other covariates that may be relevant to specific study designs1. Stage of disease at time of study2. Sites of metastases3. Place of care4. Specific pain syndrome5. Primary therapies (i.e., antitumor treatments among patients with cancer)6. Co-existing psychological disorder (present vs. absent, specific diagnoses)7. Measure of cognitive function (i.e., Mini Mental Status Examination Score)

| 305 305Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
243
Vol. 23 No. 3 March 2002 Pain Measurement Tools in Palliative Care 243
indicate the intensity of pain in general, at itsworst, at its least, and right now. A percentagescale quantifies relief from current therapies. Afigure representing the body is provided forthe patient to shade the area corresponding tohis or her pain. Seven questions determine thedegree to which pain interferes with function,mood, and enjoyment of life. The BPI is self-administered and easily understood, and hasbeen translated and validated in many differ-ent languages.
40–48
A Norwegian (S. Kaasa, per-sonnal communication), and Spanish (J.M.Nunez-Olarte, personal communication) vali-dation are ongoing. It is suitable for repeatedevaluation of pain—that is, weekly or bi-weekly—but its use for this purpose needs fur-ther study.
49
The McGill Pain Questionnaire (MPQ)
50
is aself-administered questionnaire that providesglobal scores and subscale scores that reflect
the sensory, affective, and evaluative dimen-sions of pain. It has been validated in cancerpain.
51
A short form of the MPQ (SF-MPQ) wasdeveloped for use in research settings.
52,53
TheSF-MPQ consists of 15 representative wordsfrom the sensory (
n
�
11) and affective (
n
�
4)categories of MPQ. The Present Pain Index,verbal rating scale, and a visual analogue scale(VAS) measuring pain intensity is included.The 15 words are scored using a 4-point verbalrating scale, ranging from none, mild, moder-ate, to severe pain. The SF-MPQ correlateshighly with the MPQ. Whereas the MPQ isavailable in many languages, the SF-MPQ is not.
Health-Related Quality of Life Measures
Several measures of health-related quality oflife (HRQL) have been developed and interna-tionally validated during the last decade.
54
These measures are multi-dimensional and in-
Table 3
Evidence-Based Criteria Adopted for Recommending Pain Measurement Tools
Scale Ease of Administration ValiditySensitivity to
Treatment EffectValidated in
Palliative CareMultilingual
Validity
VAS
�
Kremer et al. 1981
31
�
Briggs et al. 1999
60
�
Scott & Huskinsson1976
16
�
Price et al. 1994
20
�
Jensen et al.1986
28
�
Littmann et al.1985
27
�
Joyce et al.1975
64
�
De Conno et al. 1994
61
NA
NRS 0-10
�
Kremer et al. 1981
30
�
Jensen et al. 1986
28
�
Jensen et al. 1986
28
�
Jensen et al.1993
18
�
Jensen et al.1994
32
�
Farrar et al.2000
66
�
De Conno et al.1994
61
�
Serlin et al.1995
40
VRS
�
Jensen et al. 1986
28
�
Jensen et al.1986
28
�
Gracely et al.1978
14
�
/
�
Littman et al.1985
27
�
De Conno et al.1994
61
�
Bullinger et al.1998
29
Relief NA
�
/
�
De Conno et al.1994
61
�
Wallenstein et al.1980
25
�
Fishman et al.1987
35
�
Feine et al.1998
33
�
Littman et al.1985
27
�
Farrar et al.2000
66
�
De Conno et al.1994
61
NA
BPI
�
/
�
Twycross et al. 1996
48
�
Serlin et al.1995
40
�
/
�
Twycross et al.1996
49
? Twycross et al.1996
49
�
Twycross et al.1996
49
�
a
McGill NA. The expert consensuswas that this instrumentis more demanding thanothers
�
Melzack 1975, 1985
50, 52
�
/
�
Holroyd et al.1992
62
�
Melzack 1985
52
�
De Conno et al.1994
61
�
Graham et al. 1980
51
�
Dudgeon et al.1993
53
�
De Conno et al.1994
61
�
/
�
NA
�
not available;
�
Studies providing evidence for validity;
�
Studies not providing evidence of validity;
�/� Studies offering mixed resultsa See text for full list.

306 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
244
244 Caraceni et al. Vol. 23 No. 3 March 2002
clude several domains, such as physical func-tion, psychological function, social function,and various symptoms which are prevalent inadvanced medical illnesses. Pain is included asa single item or as a dimension in many ofthese measures. The European Organizationfor Research and Treatment of Cancer (EORTC)quality-of-life questionnaire has been specifi-cally designed for the use in oncology clinicaltrials in a multicenter multilingual setting55,56
and has a pain-related scale.57
By using a measure of HRQL, a more com-prehensive picture of the patient’s total symp-tom burden and function might be obtained.This may be favorable when compared to usingone scale or one measure for pain. However,HRQL instruments are long and can be diffi-cult to complete for patients with reduced per-formance status. HRQL should be included indescriptive studies and in prospective phase IIIstudies. At the moment, research in HRQLmeasures and pain is still insufficient to makespecific recommendations on which toolshould be used in pain-related studies.54,58,59
Summary of Criteria Adoptedfor Recommendation
Table 3 summarizes some of the evidencethat can be used to support the appropriate-ness of the PMTs considered. The use of ascale can be recommended according to sev-eral criteria. Practicality and appropriatenessfor palliative care studies were emphasized.
1. Ease of administration. This criterion has ob-vious practical implications. Between two in-struments sharing all other psychometric prop-erties the choice should favor the one thatmaximizes patients’ compliance. In this re-spect, the VAS may have disadvantages whencompared with other instruments, especially inthe elderly,31,60 although some have found thatthe percentage of incorrect responses with theVAS is higher but comparable with those ob-tained with other instruments.28 The BPI isusually considered easy to complete, but in onestudy that employed this questionnaire for clin-ical purposes, the percentage of missing re-sponses and of noncompliant patients in re-peated administration was relatively high.49
2. Validity. This criterion is fundamental andguarantees that the instrument measures what
it is meant to measure (within the limited aimsof our review, pain intensity). Human sensa-tion has no external “gold standard” withwhich to compare empirical measures, and in-direct methods of inferring validity are neces-sary. These may include concurrent validitywith other supposedly valid measures,16,20,25,61
crossmodality matching,14,15 matching of ex-perimentally-administered pain stimuli withclinical pain,19 and factor analysis.28,39,61,62
The pain intensity measures obtained withVAS, VRS, and NRS are valid; the assessment ofpain relief has been demonstrated to be validin the short-term assessment of analgesics25
and when used over intermediate periods oftime,61 but it is problematic in longer-termevaluation.33,35
3. Sensitivity to treatment effect. Sensitivity tochange can be considered one aspect of valid-ity. The measure must be shown to be valid forthe use for which it is recommended.63 For theuse of PMTs in clinical trials, a scale shouldshow changes in pain intensity when a changeis expected. Sensitivity to treatment effects ofVAS, NRS, and VRS for pain intensity and short-term relief is well demonstrated.27,52,61,64–66 Theonly study49 that evaluated repeated adminis-tration of the BPI in a clinical context demon-strated that clinical changes can be detected bythis instrument, but did not specifically addresssensitivity (for this reason, this point is associ-ated with a question mark in Table 3). Data onthe McGill Pain Questionnaire are variable.52,61
4. Validation studies in palliative care. Data on thevalidity and reliability of an instrument in thespecific area of interest are relevant to establishits specific value and recommended use.51,53
5. Multilingual validity. The availability of multi-lingual and multicultural validity and reliabilitydata is particularly relevant because these rec-ommendations are made also to allow multi-center international trials. The specific use ofdifferent words as end-phrases or anchorpoints for the VAS has been shown to changethe distribution of patient responses.30 Nostudy is available that assesses how the transla-tion of intensity describing words in anotherlanguage may affect the VAS and NRS measur-ing properties. It is advisable that the wordsused are strictly intensity descriptors and repre-

| 307 307Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
245
246 Caraceni et al. Vol. 23 No. 3 March 2002
rating scale (none, mild, moderate, se-vere). Additional desired data include sat-isfaction with pain relief and whether ornot pain level is acceptable.
3. Adult patients who are unable to commu-nicate: Observer rating using 4-point VRSfor pain now.
Pain Syndrome Characterization
1. Adult patients with no cognitive impair-ment: Co-administration of both the BriefPain Inventory-Short Form and the shortform of McGill Pain Questionnaire is rec-ommended. Together, these tools pro-vide excellent coverage of quantitativeand qualitative pain characteristics. Thesedata should be integrated with detailedrecording of the clinical narrative, paincharacteristics, exacerbating and relievingfactors, response to previous trials of anal-gesic therapies, findings of physical exam-ination, and relevant imaging studies.
2. Adult patients with cognitive impairmentor unable to communicate: The nature ofthe data needed for characterization ofpain syndromes requires a level of detailthat cannot be derived from these patientpopulations. The Expert Working Grouprecommends that adequate cognitive func-tion should be an inclusion criteria forstudies of pain syndrome characterization.
Pharmacokinetic/Pharmacodynamic(PK/PD) Studies
1. Adult patients with no cognitive impair-ment: The primary pain measures inthese studies are pain intensity and painrelief; pain unpleasantness has also beenstudied.71 Both pain intensity and reliefshould be measured by using a standardVAS or 0–10 NRS. In general, the work-ing group recommends the NRS over theVAS because of data on better compli-ance. These measures should be appliedwith a frequency appropriate to the agentunder investigation.70,72–74
2. Adult patients with cognitive impairmentor unable to communicate: The nature ofthe data needed for PK/PD studies re-quires a level of compliance that can notbe derived from these patient popula-
tions. Adequate cognitive function andability to communicate should be inclu-sion criteria for PK/PD studies.
Phase I and II Studies
1. Adult patients with no cognitive impair-ment: Repeated measurement of pain atboth long-term and short-term intervals isneeded. Long-term changes in pain andpain-related interference with functioncan be measured using the Brief Pain In-ventory-Short Form at intervals of 3 daysto 2 weeks. Short-term changes in painand pain relief should be measured usinga standard VAS or 0–10 NRS adminis-tered at least three times daily for 4days.18 Although data specific to the pal-liative care population are lacking, thisrecommendation is based on the evi-dence that averaging multiple measuresof pain intensity across time maximizesthe reliability and validity of pain assess-ments and is preferred to assessment ofaverage pain over last 24 hours.18 In gen-eral, the working group recommends theNRS over the VAS because of data on bet-ter compliance. These measures shouldbe applied more frequently dependingon the study aim and on the agent underinvestigation.70,74,75
2. Multiple dose Phase II studies should in-corporate measures of adverse effects andthe impact of the intervention on qualityof life. For Phase I and single dose studies,quality-of-life evaluation is not needed.There are inadequate data to make firmrecommendations regarding the choiceof measure to record data regarding ad-verse effects and quality of life. However,the EORTC QLQ-C30 is the only validHRQL instrument available in a signifi-cant number of different languages.56
3. Adult patients with cognitive impair-ment: The Expert Working Group didnot recommend that patients with cogni-tive impairment be candidates for PhaseI/Phase II studies. The development ofbehavioral scales (Bernard Wary, per-sonal communication), or simplified pro-rated scales to measure pain, satisfaction,distress, and adverse outcomes might pro-vide valid assessments to obtain useful in-

308 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
246
Vol. 23 No. 3 March 2002 Pain Measurement Tools in Palliative Care 247
formation from this population in inter-vention studies, but trial development is,at the moment, not recommended.
Phase III Analgesic Studies
1. These studies should be restricted to pa-tients who are cognitively intact.
2. Repeated measurement of pain at bothlong-term and short-term intervals shouldbe performed. Long-term changes in painand pain-related interference with func-tion should be measured using the BriefPain Inventory-Short Form at intervals of3 days to 2 weeks. Short-term changes inpain and pain relief should be measuredusing a standard VAS or 0–10 NRS admin-istered at least three times daily for 4 days.In general, the Expert Working Grouprecommends the NRS over the VAS be-cause of data on better compliance.
3. The Expert Working Group recommendsthat all Phase III studies incorporate mea-sures of adverse effects, quality of life, andmeasure of satisfaction. The same obser-vations on the instrument of choice madefor Phase II studies apply.
When a crossover design is incorporated, pa-tient preference between the treatment armsshould be ascertained.76
Pain Measurement Tools for ChildrenThe following recommendations concerning
pain assessment in children reflect the contri-bution of a separate study group organized bythe EuroPain group. (List of EuroPain Collab-orators: P. Poulain, MD, Chair, E. Pichard-Léandri, MD, C. Wood, MD, M. Vieyra, PhD,H. H. Abu-Saad, MD, RN, G. Schaffer Vargas,MD.) Evaluation of pain in children is alwaysdelicate and notoriously difficult, because itdepends on the level of cognitive developmentand psychological condition of the child. Thereactions to prolonged pain, as seen in pallia-tive care, may be characterized by withdrawaland are similar to depression in its manifesta-tions. Pain measurement tools used in childrenmust determine the presence and the severityof pain in various conditions.
Most pain scales used in adults can also beused in children, provided they can be under-
stood. Pain should be assessed from a multidi-mensional perspective by combining subjectiveand objective measurement tools, includingself-report,77 behavioral measures, and physio-logic indicators. Physiologic measures alonecannot be interpreted simply as pain, as theyare also signs of stress.78 In children under theage of 5 and in those with developmental defi-cits, self-assessment is limited.79 In older chil-dren, the correlation between self-assessmentand behavioral methods is variable.77 False re-plies and underrating are possible. As a result,a multidimensional approach is, in general,warranted.
Unidimensional Pain Measurement ToolsThe VAS is generally the “gold standard” for
children, as it is for adults. The scale has beenadapted for children and is usually presentedvertically. Particularly in the setting of pallia-tive care, reliability of self-assessment will de-pend on the care with which it is applied to ob-tain measurements. NRS is used in childrenbut they have to be old enough to count up to10, which means they have to be school-agedchildren. Other tools are more useful in thepreschool child. A VAS score can be obtainedfrom a 3-year-old child, but the reply can bemisleading, as at that age the child does nothave the same abstract capacities of older chil-dren. They have a tendency to choose the ex-tremities of the scale, whether for the VAS oranother tool (such as the “algocube”). TheBieri Face Scale can be recommended80,81 as itis sensitive to pain intensity and less to emotionsin comparison with the Smiley AnalogueScale.82,83 Indeed, recently it has been shown84
that scales with smiles or tears show higher rat-ing scores than scales with “neutral” faces (asthe Bieri scale). The number of faces is also im-portant. Although some scales show up to 9faces, the best choice may be a scale using from5 to 6 faces, because of the child’s cognitive ca-pacities. The Bieri scale has a shorter version(Carl Von Baeyer, personal communication).The Poker Chip Tool representing four piecesof hurt has been used in acute pain.85
Multidimensional Pain Measurement ToolsThe McGill Pain Questionnaire and the
McGill Pain Questionnaire-Short Form can beproposed to children over approximately 9years of age. Drawings and body outlines are

| 309 309Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
247
248 Caraceni et al. Vol. 23 No. 3 March 2002
specific methods for communicating with chil-dren, useful for diagnosis and followup.86 ThePediatric Pain Assessment Tool has establishedcontent, convergent, discriminant, and con-struct validity.87 The tool has been validated foruse in children with cancer and is being cur-rently used to assess the effectiveness of painmanagement in pediatric palliative care.
Behavioral pain assessment tools. Few behavioralmeasurement tools have been evaluated fortheir response to medication, and insufficientattention has been paid to the significance ofbehaviors in terms of level of pain.88 In youngerchildren or in children with handicaps andcommunication problems, these are, nonethe-less, the preferred tools. Various scales havebeen developed for postoperative pain, butpain behavior can be different in advanced dis-ease. Scales that have been validated for use inchronic pain conditions include the DEGRscale for cancer pain89 and San SalvadourScales90 for cognitively delayed children.
The San Salvadour Scales90 has 22 items.Many of them depend on the child’s responseto manipulation during physical examination,basal state, and sleep. It is correlated with thelevel of autonomy. It has never been used inpalliative care but the relevance of palliativecare in neurologically disabled children cansuggest its use in special populations.
The DEGR scale89 consists of ten indicatorsdivided into three subgroups, voluntary expres-sion of pain, direct signs of pain and psycho-motor alterations. Observation of the child iscarried out at rest, on movement, and duringsocial interaction and play. It has been vali-dated in French for children with cancer aged2 to 6 years. Translations in English and Span-ish are available. At the moment, it is the onlyavailable measurement tool for prolongedpain in young children. It is appropriate foryounger children in palliative care but lacksthe benefit of self-report.
Practical RecommendationsRecommendations for children are more
difficult because of the paucity of studies ad-dressing pain in the palliative care of pediatricpatients. As a result, the recommendationshere below must be adapted to the study de-sign with the same criteria used in adults, with
specific attention to the more difficult and eth-ically demanding situation.
1. Children with no cognitive impairmentand old enough to understand: VAS, Facesscale, Poker Chip tool, MPQ, drawings.
2. Children with cognitive impairment: SanSalvadour is a possibility in the absence ofanother tool that might apply to palliativecare in the neurologically disabled child.To confirm this recommendation, fur-ther validation studies are necessary.
3. Children unable to communicate becauseof their age and poor physical status: DEGR.
4. For the younger children (�2 years), theDEGR should be tried as no other scale isavailable or adapted.
ConclusionsThe measurement of pain is a cardinal activ-
ity in palliative care research. The members ofthe Expert Working Group hope that theserecommendations may assist researchers inproject development. It is acknowledged thatsome of the recommendations address areasthat have not been formally studied or vali-dated, and are, therefore, open to study andcriticism. The Expert Working Group did notattempt a systematic literature review but useda critical approach to give substantial examplesfor all the statements provided. All statementslacking specific references reflect the opinionof the expert consensus. When sufficient evi-dence existed, the recommendations under-line that they should be used to implementstate-of-the-art research in palliative care. Thewidespread application of these recommenda-tions will facilitate greater standardization ofoutcomes and presentations of data, and willenhance the applicability and relevance of ac-cumulated data to the palliative care patientpopulation. These recommendations shouldalso help in evaluating critically the availableliterature on the use of PMTs in research inpalliative care.
The Expert Working Group acknowledgesthat other study designs and methods are feasi-ble beyond the ones reviewed. The present rec-ommendations will be relevant to pain mea-surement in most study designs. Specific study

310 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
248
Vol. 23 No. 3 March 2002 Pain Measurement Tools in Palliative Care 249
requirements may necessitate research ap-proaches that are not covered by our work.
AcknowledgmentsEAPC Research Network Steering Committee
members: Franco De Conno (Chair), AugustoCaraceni, Rehabilitation and Palliative CareUnit, Istituto Nazionale Dei Tumori, Milan, It-aly; Nathan Cherny, Pain and Palliative Medi-cine Service, Shaare Zedek Medical Center,Jerusalem, Israel; José António S. FerrazGonçalves, Unidade de Cuidados Continuados,Instituto Português de Oncologia Porto, Portu-gal; Carl Johan Fürst, Palliative Care Unit, Stock-holm, Sweden; Geoffrey Hanks, Department ofPalliative Medicine, Bristol Oncology CentreBristol, Great Britain; Stein Kaasa, PalliativeMedicine Unit University Hospital of Trond-heim, Trondheim, Norway; Sebastiano Mer-cadante, Palliative Care Unit, Ospedale La Mad-dalena, Palermo, Italy; Juan Manuel NuñezOlarte, Unidad de Cuidados Paliativos, HospitalGeneral Univ. Gregorio Marañon, Madrid,Spain; Philippe Poulain, Consultation D`Anal-gésie France Institut Gustave Roussy, Paris,France; Lukas Radbruch, Anesthesiologie,Klinik Universität zu Köln, Cologne, Germany;Carla Ripamonti, Rehabilitation and PalliativeCare Unit, Istituto Nazionale Dei Tumori, Mi-lan, Italy; Friedrich Stiefel Service de Psychiatriede Liaison, Lausanne, Switzerland.
The authors wish to thank Heidi Bulmhuberfor her help in organizing this expert workinggroup and for her continuous support of theResearch Network of the European Associationfor Palliative Care.
References1. Sauders C. Foreword. In: Doyle D, Hanks GWC,
eds. Oxford textbook of palliative medicine, 2nd ed.Oxford: Oxfor University Press, 1998:V–IX.
2. Deschamps M, Band PR, Coldman AJ. Assess-ment of adult cancer pain shortcoming of currentmethods. Pain 1988;32:133–139.
3. Rinck GC, van den Bos AM, Kleijnen J, et al.Methodologic issues in effectiveness research onpalliative cancer care: a systematic review. J Clin On-col 1997;15:1697–1707.
4. McQuay H, Moore A. An evidence-based re-source for pain relief. Oxford: Oxford UniversityPress, 1998.
5. de Wit R, Huijer Abu-Saad H, Loonstra S, et al.
Empirical comparison of commonly used measuresto evaluate pain treatment in cancer patients withchronic pain. J Clin Oncol 1999;17:1280–1287.
6. Daut RL, Cleeland CS. The prevalence and se-verity of pain in cancer. Cancer 1982;50:1913–1918.
7. Greenwald HP, Bonica JJ, Bergner M. The prev-alence of pain in four cancers. Cancer 1987;60:2563–2569.
8. Greenwald HP. Interethnic differences in painperception. Pain 1991;44:157–163.
9. Portenoy RK, Miransky J, Thaler HT, et al. Painin ambulatory patients with lung and colon cancer.Prevalence, characteristics, and effect. Cancer 1992;70:1616–1624.
10. Portenoy RK, Kornblith AB, Wong G, et al. Painin ovarian cancer patients. Prevalence, characteristics,and associated symptoms. Cancer 1994;74:907–915.
11. Ingham J, Seidman A, Yao TJ, et al. An explor-atory study of frequent pain measurement in a can-cer clinical trial. Qual Life Res 1996;5:503–507.
12. Caraceni A, Portenoy RK, and a Working Groupof the IASP Task Force on Cancer Pain. An interna-tional survey of cancer pain characteristics and syn-dromes. Pain 1999;82:263–274.
13. Clark CW, Ferrer-Brechner T, Janal MN, et al.The dimensions of pain: a multidimensional scalingcomparison of cancer patients and healthy volun-teers. Pain 1989;37:23–32.
14. Gracely RH, McGrath PA, Dubner R. A ratioscales of sensory and affective verbal pain descrip-tors. Pain 1978;5:5–18.
15. Gracely RH, McGrath PA, Dubner R. Validityand sensitivity of ratio scale of sensory and affectiveverbal pain descriptors: manipulation of affect by di-azepam. Pain 1978;5:19–29.
16. Scott J, Huskinsson EC. Graphic representationof pain. Pain 1976;2:175–184.
17. Jensen MP, Karoly K. Measurement of cancerpain by self report. In: Chapman CR, Foley KM, eds.Current and emerging issues in cancer pain: researchand practice. New York: Raven Press, 1993:193–218.
18. Jensen MP, McFarland CA. Increasing the reli-ability and validity of pain intensity measurement inchronic pain patients. Pain 1993;55:195–203.
19. Price DD, McGrath PA, Rafii A, Buckingham B.The validation of visual analogue scales as ratio scalemeasures for chronic and experimental pain. Pain1983;17:45–56.
20. Price DD, Bush FM, Long S, Harkins SW. Acomparison of pain measurement characteristics ofmechanical visual analogue and simple numericalrating scales. Pain 1994;56:217–226.
21. Houde RW, Wallenstein SL, Beaver WT. Clinicalmeasurement of pain. In: de Stevens G, ed. Analge-sics. New York: Academic Press, 1965:75–122.
22. Houde RW, Wallenstein SL, Beaver WT. Evalua-tion of analgesics in patients with cancer pain. In:Lasagna L, ed. International encyclopedia of phar-
| 311 311Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
249
250 Caraceni et al. Vol. 23 No. 3 March 2002
macology and therapeutics, vol 1. New York: Perga-mon Press, 1966:59–67.
23. Wallenstein SL. Analgesic studies of aspirin incancer patients. Proceedings of the Aspirin Sympo-sium. London: Aspirin Foundation, 1975:5–10.
24. Wallenstein SL, Houde RW. The clinical evalua-tion of analgesic effectiveness. In: Ehrenpreis S, Hei-dle A, eds. Methods of narcotic research. New York:Marcel Dekker, 1975:127–145.
25. Wallenstein SL, Heidrich GI, Kaiko R, HoudeRW. Clinical evaluation of mild analgesics: the mea-surement of clinical pain. Br J Clin Pharmacol 1980;10:319S–327S.
26. Wallenstein SL. Commentary: the VAS relief scaleand other analgesic measures: carryover effect in par-allel and crossover studies. In: Max MB, Portenoy RK,Laska EM, eds. The design of analgesic clinical trials,vol 18. New York: Raven Press, 1991:97–104.
27. Littmann GS, Walker BR, Schneider BE. Reas-sessment of verbal and visual analog ratings in anal-gesic studies. Clin Pharmacol Ther 1985;38:16–23.
28. Jensen MP, Karoly P, Braver S. The measure-ment of clinical pain intensity: a comparison of sixmethods. Pain 1986;27:117–126.
29. Bullinger M, Alonso J, Apolone G, et al. Translatinghealth status questionnaires and evaluating their qual-ity: the IQOLA Project approach. International qualityof life assessment. J Clin Epiderm 1998;51:913–923.
30. Seymour RA, Simpson JM, Charlton JE, PhilipsME. An evaluation of the length and end-phrase ofvisual analogue scales in dental pain. Pain 1985;21:177–185.
31. Kremer EF, Atkinson JH, Ignelzi RJ. Meaure-ment of pain: patient preferences does not con-found pain meausurement. Pain 1981;12:153–163.
32. Jensen MP, Turner JA, Romano JM. What is themaximum number of level needed in pain intensitymeasurement. Pain 1994;58:387–392.
33. Feine JS, Lavigne GJ, Thuan Dao TT, et al.Memories of chronic pain and perception of relief.Pain 1998;77:137–141.
34. Cleeland CS. The impact of pain on the patientwith cancer. Cancer 1984;54:2635–2641.
35. Fishman B, Pasternak S, Wallenstein SL, et al.The Memorial Pain Assessment Card: a valid instru-ment for the evaluation of cancer pain. Cancer1987;60:1151–1158.
36. Kerns RD, Turk DC, Rudy TE. The West HavenYale multidimensional pain inventory (WHYMPI).Pain 1985;23:345–356.
37. Galer BS, Jensen MP. Development and prelimi-nary validation of a pain measure specific to neuro-pathic pain. Neurology 1997;48:332–338.
38. Winer RT, Clark WC, Keohan ML, et al. Valida-tion of the multidimensional affect and pain ques-tionnaire (MAPS) in cancer patients. 9th WorldCongress on pain. Vienna: IASP Press, 1999:214.
39. Cleeland CS. Measurement of pain by subjective re-port. In: Chapman CR, Loeser JD, eds. Advances in painresearch and management, vol 12. Issues in pain man-agement. New York: Raven Press, 1989 pp. 391–403.
40. Serlin RC, Mendoza TR, Nakamura Y, et al.When is cancer pain mild moderate or severe? Grad-ing pain severity by its interference with function.Pain 1995;61:277–284.
41. Larue F, Colleau SM, Brasseur L, Cleeland CS.Multicentre study of cancer pain and its manage-ment in France. Br Med J 1995;310:1034–1037.
42. Caraceni A, Mendoza T, Mencaglia E, et al. Avalidation study of the Italian version of the BriefPain Inventory (Breve Questionario per la Valutazi-one del Dolore). Pain 1996;65:87–92.
43. Wang XZ, Mendoza TR, Gao SZ, Cleeland CS.The Chinese version of the Brief Pain Inventory.Pain 1996;67:407–416.
44. Uki J, Mendoza T, Cleeland CS, et al. A briefcancer pain assessment tool in Japanese: the utilityof the Japanese Brief Pain Inventory. J Pain Symp-tom Manage 1998;16:364–373.
45. Radbruch L, Loick P, Kiencke P, et al. Valida-tion of the German version of the Brief Pain Inven-tory. J Pain Symptom Manage 1999;18:180–187.
46. Mistakidou K, Mendoza T, Befon S, et al. Greekbrief pain inventory (BPI-G): validation and utilityin cancer pain. Proceedings of the 9th World Con-gress on Pain. Vienna: IASP Press, 1999:214.
47. Saxena A, Mendoza T, Cleeland CS. The assess-ment of cancer pain in north India: the validation ofthe Hindi Brief Pain Inventory—BPI-H. J PainSymptom Manage 1999;17:27–41.
48. Ger LP, Ho ST, Sun WZ, et al. Validation of thebrief pain inventory in a Taiwanese population. JPain Symptom Manage 1999;18:316–322.
49. Twycross R, Harcourt J, Bergl S. A survey of painin patients with advanced cancer. J Pain SymptomManage 1996;12:273–282.
50. Melzack R. The McGill pain questionnaire: ma-jor properties and scoring methods. Pain 1975;1:277–299.
51. Graham C, Bond S, Gerkovich M, Cook MR.Use of the McGill Pain Questionnaire in the assess-ment of cancer pain: replicability and consistency.Pain 1980;8:377–387.
52. Melzack R. The short-form McGill Pain Ques-tionnaire. Pain 1987;30:191–197.
53. Dudgeon D, Raubertas RF, Rosenthal SN. Theshort-form McGill pain questionnaire in chronic can-cer pain. J Pain Symptom Manage 1993;8:191–195.
54. Hearn J, Higginson I. Outcome measures in pal-liative care for advanced cancer patients: a review. JPublic Health Med 1997;19:193–199.
55. Aaronson NK, Ahmedzai S, Bergman B, et al.The European Organization for Research andTreatment of Cancer QLQ-C30: a quality-of-life in-

312 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
250
Vol. 23 No. 3 March 2002 Pain Measurement Tools in Palliative Care 251
strument for use in international clinical trials in on-cology. J Natl Cancer Inst 1993;85:365–376.
56. Kaasa S, Bjordal K, Aaronson N, et al. TheEORTC core quality of life questionnaire (QLQ-C30): validity and reliability when analysed with pa-tients treated with palliative radiotherapy. Eur J Can-cer 1995;31A:2260–2263.
57. Klepstadt P, Borgchgrevink PC, Kaasa S. Effects oncancer patients health-related quality of life from start ofmorphine. J Pain Symptom Manage, 2000;20:19–26.
58. Osoba D, Rodrigues D, Myles J, et al. Interpret-ing the significance of changes in health-relatedquality-of-life scores. J Clin Oncol 1998;16:139–144.
59. Sloan JA, Loprinzi CL, Kuross SA, et al. Ran-domized comparison of four tools measuring overallquality of life in patients with advanced cancer. JClin Oncol 1998;16:3662–3673.
60. Briggs M, CLoss JS. A descriptive study of the useof visual analogue scales and verbal rating scales forthe assessment of postoperative pain in othopedicpatients. J Pain Symptom Manage 1999;18:438–446.
61. De Conno F, Caraceni A, Gamba A, et al. Painmeasurement in cancer patients: a comparison ofsix methods. Pain 1994;57:161–166.
62. Holroyd KA, Holm JE, Keefe FJ, et al. A multi-center evaluation of the McGill Pain Questionnaire:results from more than 1700 chronic pain patients.Pain 1992;48:301–311.
63. American Educational Research AssociationAPA, National Council on Measurement in Educa-tion. Standards or educational and psychologicaltesting. Washington DC: American Psychological As-sociation, 1985:98.
64. Joyce CRB, Zutshi DW, Hrubes V, Mason RM.Comparison of fixed interval and visual analoguescales for rating chronic pain. Eur J Clin Pharmacol1975;8:415–420.
65. Jensen MP, Turner JA, Romano JM, Fisher LD.Comparative reliability and validity of chronic painintensity measures. Pain 1999;83:157–162.
66. Farrar JT, Portenoy RK, Berlin JA, Kinman JL,Strom BL. Defining the clinically important differencein pain outcome measure. Pain 2000;88:287–294.
67. Maiani G, Sanavio E. Semantics of pain in Italy:the Italian version of the McGill Pain Questionnaire.Pain 1985;22:399–405.
68. De Benedittis G, Massei R, Nobili R, Pieri A. TheItalian pain questionnaire. Pain 1988;33:53–62.
69. Portenoy RK, Payne D, Jacobsen P. Break-through pain: characteristics and impact in patientswith cancer pain. Pain 1999;81:129–134.
70. Portenoy RK, Payne R, Coluzzi P, et al. Oraltransmucosal fentanyl citrate (OTFC) for the treat-ment of breakthrough pain in cancer patients: a con-trolled dose titration study. Pain 1999;79:303–312.
71. Price DD, von der Gruen A, Miller J, et al. A psy-chophysical analysis of morphine analgesia. Pain1985;22:261–269.
72. Inturrisi CE, Colburn WA, Kaiko RF, et al. Phar-macokinetics and pharmacodynamics of methadonein patients with chronic pain. Clin Pharmacol Ther1987;41:392–401.
73. Inturrisi CE, Portenoy RK, Max MB, et al. Phar-macokinetic-pharmacodynamic (PK-PD) relation-ships of methadone infusions in patients with can-cer pain. Clin Pharmacol Ther 1990;47:565–570.
74. Farrar JT, Cleary J, Rauck R, et al. Oral transmu-cosal fentanyl citrate: randomized, double-blinded,placebo-controlled trial for treatment of break-through pain in cancer patients. J Natl Cancer Inst1998;90:661–666.
75. Max MB, Laska EM. Single-dose analgesic com-parisons. In: Max MB, Portenoy RK, Laska EM, eds.The design of analgesic clinical trials, vol 18. NewYork: Raven Press, 1991:55–95.
76. Max M, Portenoy RK. Pain research: designingclinical trials in palliative care. In: Doyle D, HanksGWC, eds. Oxford textbook of palliative medicine, 2nded. Oxford: Oxford University Press, 1998:167–178.
77. Champion GD, Goodenough B, Von Baeyer CL,Thomas W. Measurement of pain by self-report. In:Finley GA, McGrath PJ, eds. Measurement of pain ininfants and children, vol 10. Seattle: IASP Press, 1998.
78. Sweet SD, McGrath PJ. Physiological measuresof pain. In: Finley GA, McGrath PJ, eds. Measure-ment of pain in infants and children, vol 10. Seattle:IASP Press, 1998:59–81.
79. Hammers JP, Abu-Saad HH, Van Den Hout MA,et al. The influence of children’s vocal expressions,age, medical diagnosis and information obtainedfrom parents on nurses’ pain assessment and deci-sions regarding interventions. Pain 1996;65:53–61.
80. Hicks CL, Von Baeyer CL, Spafford PA, van Kor-laar I, Goodenough B. The Faces pain scale—re-vised: toward a common metric in pediatric painmeasurement. Pain 2001;93:173–183.
81. Bieri D, Reeve RA, Champion GD, et al. Thefaces pain scale for the self-assessment of pain expe-rienced by children. Pain 1990;41:139–150.
82. Wong DL, Baker CM. Pain in children: compari-son of assessment scales. Ped Nurs 1988;14:9–17.
83. Pothmann R. Comparison of visual analoguescale (VAS) and a Smiley analogue scale (SAS). In:Tyler DC, ed. Advances in pain research and ther-apy. New York: Raven Press, 1990:95–99.
84. Chambers CT, Giesbrecht K, Craig KD, et al. Acomparison of faces scales for the measurement ofpediatric pain: children’s and parents’ ratings. Pain1999;83:25–35.
85. Hester NK. The preoperational child’s reactionto immunization. Nurs Res 1979;28:250–255.
86. Poulain P, Pichard-Leandri E, Gauvain-PiquardA. Assessment and treatment of pain in children inpalliative care. Eur J Palliative Care 1994;1:31–35.
87. Abu-Saad HH, Pool H, Tulkens B. Further test-

| 313 313Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
251
252 Caraceni et al. Vol. 23 No. 3 March 2002
ing of the Abu-Saad pediatric pain assessment tool. JAdvanced Nurs 1994;19:1063–1071.88. McGrath PJ. Behavioral measure of pain. In:Finley GA, McGrath PJ, eds. Measurement of pain ininfants and children, vol 10. Seattle: IASP Press,1998:83–102.89. Gauvain-Piquard A, Rodary C, Rezvani A, Ser-
bouti S. The development of the DEGR: a scale toassess pain in young children with cancer. Eur J Pain1999;3:165–176.
90. Collignon P, Giusano B, Boutin AM, CombesJC. Utilisation d’une echelle d’heteroevaluation dela douleur chez le sujet severement handicape. Doulet Analg 1997;1:27–32.
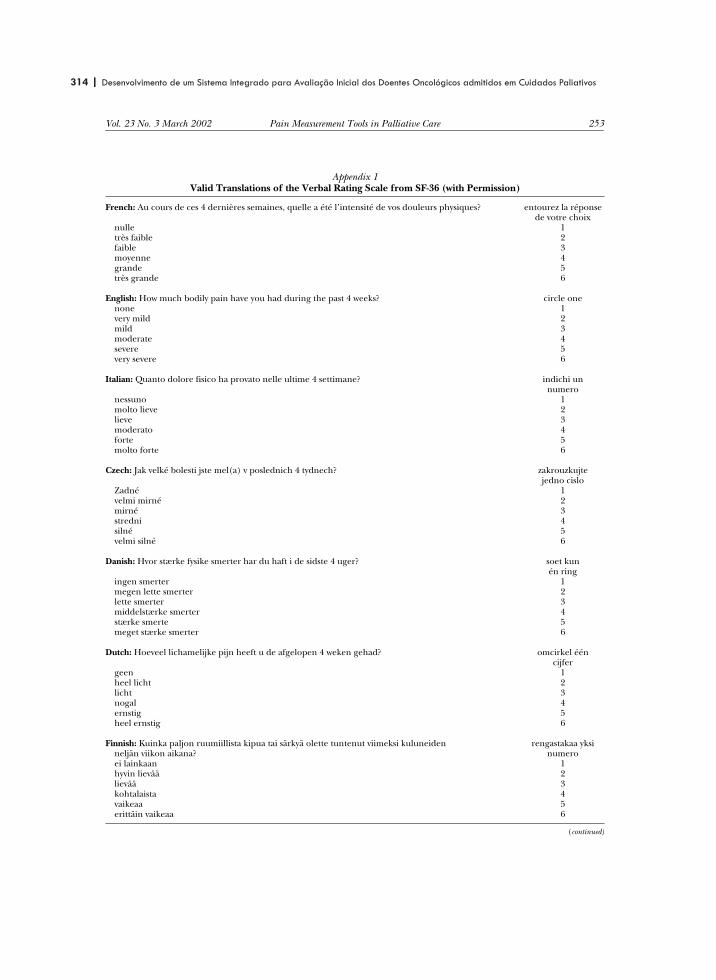
314 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
252
Vol. 23 No. 3 March 2002 Pain Measurement Tools in Palliative Care 253
Appendix 1Valid Translations of the Verbal Rating Scale from SF-36 (with Permission)
French: Au cours de ces 4 dernières semaines, quelle a été l’intensité de vos douleurs physiques? entourez la réponsede votre choix
nulle 1très faible 2faible 3moyenne 4grande 5très grande 6
English: How much bodily pain have you had during the past 4 weeks? circle onenone 1very mild 2mild 3moderate 4severe 5very severe 6
Italian: Quanto dolore fisico ha provato nelle ultime 4 settimane? indichi unnumero
nessuno 1molto lieve 2lieve 3moderato 4forte 5molto forte 6
Czech: Jak velké bolesti jste mel(a) v poslednich 4 tydnech? zakrouzkujtejedno cislo
Zadné 1velmi mirné 2mirné 3stredni 4silné 5velmi silné 6
Danish: Hvor stærke fysike smerter har du haft i de sidste 4 uger? soet kunén ring
ingen smerter 1megen lette smerter 2lette smerter 3middelstærke smerter 4stærke smerte 5meget stærke smerter 6
Dutch: Hoeveel lichamelijke pijn heeft u de afgelopen 4 weken gehad? omcirkel één cijfer
geen 1heel licht 2licht 3nogal 4ernstig 5heel ernstig 6
Finnish: Kuinka paljon ruumiillista kipua tai särkyä olette tuntenut viimeksi kuluneidenneljän viikon aikana?
rengastakaa yksinumero
ei lainkaan 1hyvin lievää 2lievää 3kohtalaista 4vaikeaa 5erittäin vaikeaa 6
(continued)

| 315 315Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
253
254 Caraceni et al. Vol. 23 No. 3 March 2002
Appendix 1Continued
German: Wie stark waren Ihre Schmerzen in den vergangenen 4 Wochen? Bitte kreuzen Sie nureine Zahl an
Ich hatte keine Schmerzen 1Sehr leicht 2Leicht 3Mäßig 4Stark 5Sehr stark 6
Hungarian: Milyen erõs testi fájdalmai voltak az elmúlt 4 hébten? csak egy számotjelöljön meg!
nem voltak 1nagyon enyhe 2enyhe 3közepes 4erõs 5nagyon erõs 6
Norwegian: Hvor sterke kroppslige smerter har du hatt løpet av de siste 4 ukene? sett ring rundtett tall
ingen 1meget svake 2svake 3moderate 4sterke 5meget sterke 6
Polish: Jak bardzo odczuwali Panstwo w ciagu ostanich 4 tygodni ból fizyczny? zakresl jednoZadnego 1bardzo lagodny 2lagodny 3sredni 4silny 5bardzo silny 6
Portuguese: Durante as ultimas 4 semanas teve dores? circule umanenhumas 1muito fracas 2ligeiras 3moderadas 4fortes 5muito fortes 6
Serbian: Da li ste osecali telesni bol, i ako jeste u kolikoj meri, tokom poslednje 4 nedelje? zaokruzitijedan broj
bez bola 1vro blag bol 2blag bol 3umeren bol 4tezak bol 5vrlo tezak bol 6
Slovak: Aké vel’ ké telesné bolesti ste mali v piebehu poslednych 4 tyzdnov? zakrúzkujte jednu moznost’
ziadne 1vel’ mi mierne 2mierne 3stredné 4väcsie 5t’azké 6
(continued)

316 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
254
Vol. 23 No. 3 March 2002 Pain Measurement Tools in Palliative Care 255
Appendix 1Continued
Spanish: ¿Tuvo dolor en alguna parte del curpo durante las 4 últimas semanas? marque unsolo número
no ninguno 1sì, muy poco 2sì, un poco 3sì, moderado 4sì, mucho 5sì, muchissimo 6
Swedish: Hur mycket värk eller smärta har Du haft under de senaste fyre veckorna? sätt en ring runten siffra
ingen 1mycket lätt 2lätt 3måttlig 4svår 5mycket svår 6
Turkish: Gectigimiz bir ay (4 hafta) içerisinde ne kada bedensel agrilariniz oldu? birinin etrafinadaire cizin
hiç 1çok hafif 2hafif 3orta hafiflikte 4asiri derecede 5çok asiri derecede 6
In this questionnaire the scale is intended to evaluate pain during the previous 4 weeks. Different time frames can be chosen depending on thestudy requirements and aims.

| 317 317Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
255
Episodic (Breakthrough) PainConsensus Conference of an Expert Working Group of the European Associationfor Palliative Care
Sebastiano Mercadante, M.D.1
Lukas Radbruch, M.D.2
Augusto Caraceni, M.D.3
Nathan Cherny, M.D.4
Stein Kaasa, M.D., Ph.D.5
Friedemann Nauck, M.D.6
Carla Ripamonti, M.D.3
Franco De Conno, M.D.3
the Steering Committee of theEuropean Association for PalliativeCare (EAPC) Research Network
1 Pain Relief and Palliative Care Unit, La Mad-dalena Cancer Center, Palermo, Italy.
2 Klinik fur Anasthesiologie und Operative Intensiv-medizin, University of Koln, Koln, Germany.
3 Department of Rehabilitation and Palliative Care,National Cancer Institute, Milan, Italy.
4 Cancer Pain and Palliative Medicine, ShareZedek Medical Center, Jerusalem, Israel.
5 Palliative Medicine Unit, Trondheim UniversityHospital, Trondheim, Norway.
6 Palliative Medicine Unit, University of Bonn,Bonn, Germany.
Members of the Research Steering Committee ofthe EAPC: Franco De Conno (Chair), Augusto Cara-ceni, Nathan Cherny, Carl Johan Furst, Jose FerrazGoncalves, Geoffrey Hanks, Stein Kaasa, Sebas-tiano Mercadante, Juan Manuel Nunez Olarte, Phil-ippe Poulain, Lukas Radbruch, Carla Ripamonti,and Friedrich Stiefel.
Address for reprints: Sebastiano Mercadante,M.D., Pain Relief and Palliative Care Unit, LaMaddalena Cancer Center, Via S. Lorenzo 312,90146 Palermo, Italy; Fax: 39-091-6806909;E-mail: [email protected]
Received July 11, 2001; revision received July 11,2001; accepted October 15, 2001.
BACKGROUND. Breakthrough pain is transitory exacerbation of pain that occurs in
addition to otherwise stable persistent pain. The wide differences in estimation of
incidence reported in literature are probably because of different settings and
meanings attributed to the definition of breakthrough pain.
METHODS. A panel of experts met to establish the actual knowledge on break-
through pain, according to the evidence in literature and experience. They agreed
that episodic or transient pain could be a more simple and adequate term in most
languages, including English, French, Italian, and Spanish.
RESULTS. A specific assessment and precise pain characterization are essential to
plan the most appropriate treatments. Despite the relevance of this temporal pain
pattern for the influence on the outcome and quality of life, few controlled studies
have been performed to give evidence of a specific approach. Several experiences
have reported the possible efficacy of different drugs, route of administration, and
modalities of administration in different circumstances.
CONCLUSIONS. Prospective studies with previous treatments using similar termi-
nologies are necessary to find the most convenient therapeutic intervention, ac-
cording to the temporal pattern characteristics and the pain mechanism involved.
Cancer 2002;94:832–9. © 2002 American Cancer Society.
DOI 10.1002/cncr.10249
KEYWORDS: cancer pain, breakthrough pain, incident pain, transient pain, opioids,nonsteroidal antiinflammatory drugs (NSAIDs), pamidronate, transmucosal fentanyl,radiotherapy, spinal opioids.
Pain relief usually is achieved in most cancer patients using theWorld Health Organization guidelines for cancer pain manage-
ment. However, it is well acknowledged that many patients continueto suffer from difficult pain syndromes with a typical temporal pat-tern.1,2 Breakthrough pain has been associated with a reduced likeli-hood for adequate pain control in some groups of cancer patients.3– 6
The incidence of breakthrough pain has been estimated to be high(approximately 40 – 80% depending on the setting) in various sur-veys.2,7–11 The differences reported are probably because of differentsettings and meanings attributed to the definition of breakthroughpain. In an international survey of cancer pain characteristics andsyndromes, large differences in the diagnosis of breakthrough pain byclinicians of different countries have been found, suggesting that thisphenomenon is diagnosed differently in various countries.5 Thesecontroversial aspects, both semantic and clinical, were discussed in aconsensus meeting of an expert working group from the ResearchNetwork of the European Association for Palliative Care during the2nd International and Hellenic Conference on Pain Relief and Pallia-
832
© 2002 American Cancer Society

318 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
256
tive Care held in Athens in March 1999. The selectedmembers of the expert panel were required to havespecific clinical and research interests relating to thetopic and to have published significant articles onpatients with cancer pain. Before the meeting, eachselected expert prepared a report on various aspects,including epidemiology, definition, assessment, paincategorization, and treatment, according to the exist-ing literature and his or her own experience. The ma-terial drawn from a systematic review of the variousaspects was discussed. The chairs of this group weresolicited to refine a draft. In the subsequent year, theposition paper was circulated and then debated andextended to other external referees belonging to thesteering committee of the research network, and fur-ther changes were made, according to new sugges-tions until a final agreement was achieved in Decem-ber 2000.
TERMINOLOGYBreakthrough pain is defined as transitory exacerba-tion of pain that occurs in addition to otherwise stablepersistent pain.2 This suggests a high pain intensitylimited in time, that means a transient episode ofuncontrolled pain. The definition of breakthroughpain is not agreed on among various researchers.2,12
For example, in the United Kingdom this term often isused as a sign of end-of-dose failure during dose ti-tration. A relation between transient pain and baselineregimen has been found. End-of-dose pain occurswhen the effect of opioids does not last until the nextdose is scheduled. Moreover, the term is typically En-glish and does not have any correspondent in otherlanguages in Europe, especially in Latin countries,where patients and untrained physicians may havemisconception of the definition of breakthrough pain.To increase the relevance in the clinical setting, abroader and less burdened term should be preferred,such as episodic or transient pain. These terms seemto be more simple and adequate in most languages,including English, French, Italian, and Spanish.
In Table 1, typical episodic pain mechanisms are
listed. These could be useful for education and forestablishing a common language among researchers;clinical conditions with varying underlying mecha-nisms requiring various approaches could be used toillustrate each mechanism.
ASSESSMENTPatients with episodic pain and their treatment fre-quently have been described as a common group. Thetherapeutic approach, however, can change consider-ably according to the phenomenology and the patho-physiology of the episodic pain. An assessment algo-rithm is useful to categorize patients in groupsaccording to the background pain conditions (Fig. 1).Patients with background pain that was described asunusually severe are considered to have uncontrolledbackground pain. Patients with controlled back-ground pain who experienced one or more severe orexcruciating episodes of pain during the past day maybe classified as having controlled background painand episodic pain (Fig. 2).
A temporal distribution of opioid doses as neededhas been reported. It has been attributed to a moreintense diurnal activity.13 Conversely, an intraindi-
FIGURE 1. Algorithm for treatment of episodic (breakthrough) pain. WHO:
World Health Organization.
TABLE 1Differentiation of Episodic Pain
Episodic pain with significant baseline pain(inadequate pain management)
Episodic pain without significant baseline pain (difficult pain problem)
Movement-related episodic pain Nonmovement-related episodic pain
Any kind of pain Bone painNeuropathic pain Neuropathic painVisceral pain Visceral painSomatic soft tissue pain Somatic soft tissue pain
Episodic Pain in Cancer/Mercadante et al. 833

| 319 319Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
257
vidual variation in the absorption of morphine orchanges in volume of distribution during the day havebeen demonstrated, and there is a potential for amismatch between fluctuations in pain intensity andmorphine blood concentration, as a consequence of achronopharmacokinetic variability.14
This suggests a more accurate assessment, includ-ing not only intensity, frequency, and duration of ep-isodic pain, but also quality of pain and alleviating orprecipitating factors. The characteristics of this kind ofpain suggest that it needs to be assessed with instru-ments aiming at measuring pain intensity over shortperiods of time.
Although the traditional measures of pain inten-sity, including visual analog scales, numericl ratingscales, and verbal rating scales, most likely are equiv-alent for this purpose, measurements should be per-formed frequently, at the onset and then at intervalsuntil the episode evanishes spontaneously or after aspecific treatment. The use of analgesics, the relationbetween the occurrence of the episode and the admin-istration of drugs, and the onset of effect should berecorded.9 Onset and peak intensity, location, qualityand predictability, and factors that precipitated themor provided relief once they occurred or able to pre-vent them also should recorded. An additional ques-tion should determine whether the episode representan acute worsening of the chronic pain or was anentirely distinct phenomenon.
The Brief Pain Inventory (BPI) is a useful tool to
evaluate the degree to which pain interferes with func-tion and quality of life.5 It offers useful information forepisodic pain, including several questions on painintensity differentiating between average pain andworst pain as an indicator of episodic pain intensity.The Beck Depression Inventory, the Beck Anxiety In-ventory, and performance status measures such asEastern Cooperative Oncology Group and Karnofsky,are other well recognized instruments, which includephysical and psychologic symptoms and the ability tofunction physically, although they do not assess spe-cific questions on episodic pain.
PAIN CATEGORIZATIONThe concluded pathophysiology can be categorized asthe following:
1. Nociceptive if the pain is related to injured somaticor visceral structures, and is usually described asaching, sharp, or throbbing;
2. Neuropathic if the pain was related to an injury ofa neural structure with a typical neuropathic pat-tern or aberrant characteristics (Fig. 3).
Given the broad scope of pain syndromes thatmay be hidden under the cover of episodic pain, theimportance of a differentiated diagnosis must bestressed. The most striking distinction could be madein movement-related pain and nonmovement-relatedpain (Table 1). The former case typically is associatedto bone metastases. Patients have pain well controlled
FIGURE 2. Different temporal patterns
of episodic pain and continuous pain.
Examples on the left side should be
interpreted as inadequate pain manage-
ment, whereas those on the right side as
difficult pain problems. In the middle is
an example of a mixed pattern.
834 CANCER February 1, 2002 / Volume 94 / Number 3

320 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
258
at rest and tend to prevent pain by limiting theirmovements, depending on the site of the painful bonemetastases. As a consequence, autonomy and qualityof life are highly compromised by this status. Incidentpain usually has a sudden onset reaching a peak painintensity within few minutes. Because the onset isquite predictable and can be considered volitional,these episodes are associated with a functional im-pairment on measures of mood and anxiety, and onscales of pain interferences with function.9
Nonvolitional movements, such as laughing,sneezing, coughing, or myoclonus, may also exacer-bate skeletal pain. A Valsalva maneuver induced bycoughing and sneezing can precipitate transient ele-vations in intracranial or spinal cord pressure. Be-cause of the proximity of neural and somatic struc-tures, neuropathic radicular pain often is exacerbatedby volitional or nonvolitional movements, as typicallyobserved in situations of epidural compression of thecord or nerve roots.
Some other pains should be considered volitionalrather than induced by a specific movement. Paininduced by swallowing or chewing in patients withmucositis or touching some hyperesthetic skin areasin patients with neuropathic or somatic pain condi-tions may precipitate a pain crisis.
Mucositis renders patients unable to take oralmedication or to swallow, inducing a decrease in foodand fluid intake. Tenesmus of colon and bladder areinduced by attempts in defecation and micturition.
Finally, episodic pain may be independent of themovement or volitional conditions.
Transient episodes of spontaneous lancinating orburning pain are a common manifestation of neuro-pathic pain syndromes. These paroxysmal episodescommonly present with a short onset and duration
(seconds or minutes) and require a preventive therapyrather than an as-needed medication.15 Spontaneousmuscular contractions of hollow organs (including theesophagus, intestine, gall bladder and their ducts, theurinary bladder, and the ureters) commonly result inparoxysmal transient pain exacerbations. Irritant fac-tors or the obstruction of any hollow viscus may gen-erate such pain with the typical colic pattern. Specificepisodic pain mechanisms are listed in Table 2.
TREATMENTAny temporal increase in pain intensity should becarefully considered, because it may be just a sign ofinadequate pain management due to a wrong opioiddose or schedule. Treatment with adjuvant drugsshould be optimized because they may be useful inimproving basal analgesia and in preventing episodicpain. When exacerbations of pain occur or markedlyworsen predictably before next scheduled dose of opi-oid, pain can be managed by increasing the basal doseor decreasing the interval between dosing until eitherfavorable effects occur or intolerable and unmanage-able adverse effects supervene. Dosing on an as-needed basis may be beneficial for an appropriateincrement in the regularly scheduled dose, when thetransient events are attributable to a low daily basaldosage, for example, when rapid escalation is needed.The quantity of rescue medication can be summed tothe previous 24 hours’ consumption to find out themore appropriate dosage to prevent new episodes inthe following days.16
Once an effective background has been provided,precipitating factors and measures able to preventthem, as well as palliative factors should be found,although this often results in a limitation in movement(Fig. 1).
Primary TherapiesThe value of primary therapies, such as hormonalmanipulation and chemotherapy, remains to be es-tablished. In patients with very advanced cancer, thereis little justification for using chemotherapy, becauseof its toxicity. Orthotic devices, such as lightweight
FIGURE 3. Algorithm for treatment of neuropathic breakthrough pain.
TABLE 2Specific Episodic Pain Problems
With (incident) movement-relatedpain
Oversedation at rest
With neuropathic pain Paroxysmal pain with very short durationWith visceral pain Tenesmus of colon or bladderWith somatic soft tissue pain
(mucositis)Inability to take oral medication, inability to
swallow
Episodic Pain in Cancer/Mercadante et al. 835

| 321 321Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
259
functional bracing, may be useful with upper extrem-ity bone lesions, and surgical stabilization of the spineand extremities may substantially improve the qualityof life, although the potential benefits of surgical in-tervention must be tempered with patient survival. Ifsuitable, surgical abdominal interventions may behelpful in resolving bowel obstruction and, as a con-sequence, colics associated with a difficult transit.
Radiotherapy is a well recognized method to re-duce pain from bone metastases. However, no studiesto our knowledge have analyzed specifically the effecton episodic pain.17
Nonopioid Analgesic RegimensDifferent drugs have been used in controlling episodicpain according to specific pain mechanisms.
Some algorithms have been designed as a way tofacilitate the approach to patients with episodic pain(Figs. 2 and 3).
Antiinflammatory drugsAdditive or synergic analgesia produced by nonsteroi-dal antiinflammatory drugs (NSAIDs) and steroidalantiinflammatory drugs can be useful in painful bonemetastases or mucosal and skin lesions. The specificusefulness in bony pain has not been addressed ap-propriately. The chances of good pain control untildeath were high, and the negative influence of inci-dental pain was lower when patients achieved a goodresponse using NSAIDs, according to an individualvariability in response to analgesics.6 Whereas long-acting NSAIDs facilitating once- or twice-daily dosingshould be favored in patients already taking multipledrugs, rescue doses of particular formulations (fastrelease, sublingually, or parenterally) of NSAIDs maybe useful in controlling incidental pain when sideeffects from opioids administered as needed can beexpected once the episodic pain disappears. Guide-lines in the management of NSAIDs in the patient withcancer pain are largely empiric, drawn from clinicalexperience. Anecdotal experience has been reportedon the use of steroids for this indication as well as forconditions of edema and swelling surrounding periph-eral nervous structures.18
Other drugsVarious classes of drugs have been used in episodicpain according to the pain mechanism involved.These treatments have a rationale from the patho-physiologic point of view. However, to our knowledge,no controlled studies have been performed to gainscientific evidence.
Spasmolytics such as butylscopolamine or oct-reotide also may be useful in abdominal colic super-
imposed to visceral pain, often associated with ob-struction of the intestinal or urinary tract.
Bisphosphonates represent a new class of drugswith inhibitory activity on bone resorption and oninflammatory process. Recently, a review of Phase IIIstudies and an evidence-based review have under-lined that bisphosphonates are able to reduce bothskeletal events and pain in metastatic bone diseasewithout determining relevant adverse effects.19 A re-duction in bone pain might potentially result in areduction of incidental pain. Anecdotal experience re-ports that bisphosphonate cycles may be useful inreducing movement-related pain.20 However, to ourknowledge to date no prospective studies have as-sessed the role of this class of drugs in preventing orreducing movement-related pain nor the number ofrescue doses required with respect to placebo or othertreatments.
Predictable movement-related pain, such as thoseoccurring with dressing changes or skin toilette, maybe prevented with a light sedation using midazolam orketamine. Ketamine has been found to be useful inneuropathic pain conditions poorly responsive tomorphine21 and potentially may prevent pain exacer-bations. However, psychomimetic effects are of con-cern.
The regular use of some adjuvants, including an-tidepressants, antiarrhythmics, and anticonvulsants,have been used to prevent or alleviate paroxysmalburning or lancinating neuropathic pain, although toour knowledge controlled studies in this context arenot available. In a recent review, the pain character-istics did not appear to predict the response to specificagents. However, studies were performed in noncan-cer patients.22,23 Some topical drugs, including capsa-icin, aspirin, or a cream of eutectic mixture of localanesthetics, may reduce the input from peripheralnerve lesions.18 Topical application of opioids or localanesthetics is another option in pain due to mucositisor skin ulcers in which pain is precipitated with con-tact.24
Nitrous oxide has properties that might enableprompt control of episodic pain. It has been safely andeffectively used with a 50:50 mixture of nitrous oxideand oxygen by a patient-controlled mechanism bymask in advanced cancer patients with episodic painfrom bone metastases.25
The use of psychostimulant drugs such as meth-ylphenidate has been demonstrated to allow patientsto tolerate higher doses of opioids during the periodbetween incident pain episodes.26 However, it shouldbe used cautiously, especially in the first 48 hours oftreatment.
836 CANCER February 1, 2002 / Volume 94 / Number 3

322 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
260
OpioidsPatients with severe episodic pain typically are treatedwith an opioid drug. When baseline pain is well con-trolled, eventual increases in opioid dosage will resultin oversedation at rest. The use of as-needed analgesiaeither to prevent an anticipated flair of pain or to treatan established episode of pain is the standard symp-tomatic treatment. A “rescue dose” must have a rapid-ity of onset appropriate to the specific pain presenta-tion, appropriate potency, and easy administration.Despite the large clinical experience on the use ofopioids, there is limited scientific evidence becausefew randomized studies have dealt with this subject.
Routes of AdministrationOral routeTypically, the rescue doses consist of an immediaterelease opioid preparation that is usually the samedrug as that being administered on an around-the-clock basis. The most effective dose remains un-known. Titration of the rescue dose according to thecharacteristics of the event should be attempted in anindividual way to identify the most appropriate dose,although some clinicians suggest a dose roughlyequivalent to 5–10% of the total opioid dose adminis-tered as needed every 2–3 hours.2 The time to peakeffect for orally administered opioids is approximately60 minutes and is not suitable for pains with a shortonset and duration. Methadone may have a shorterpeak effect.
SublingualThis alternative route of opioid administration haslimited value due to a lack of formulations, poor orirregular absorption of most drugs, and the inability todeliver high doses that are prevented by swallowing.Potent drugs such as sufentanil may be useful to de-livery higher doses in lower volumes.27 When com-pared with morphine, lipophilic drugs such as bu-prenorphine, fentanyl, sufentanil, and methadone arerelatively well absorbed through the buccal mucosa.28–30
RectalRectal administration potentially offers the possiblepharmacokinetic advantage of bypassing first-passmetabolism by entering the system circulation vialower rectal veins. Rectal morphine is absorbed intothe systemic circulation to an extent at least that oforal morphine.30
The use of small amount of liquid may prevent thediffusion into sigmoid colon and avoid the drainage bythe superior rectal vein into the portal system. There-fore, the avoidance of first-pass metabolism is depen-
dent on the level of absorption within the rectum.However, there is no clear anatomic demarcation be-tween the portal and systemic drainage because of thepresence of extensive anastomoses, and this may ren-der the proportion of drug absorbed via portal veindifficult to predict. The absorption also depends onthe preparation (aqueous or alcoholic solutions, sup-positories, use of surfactants), bowel movements, pHof solutions used, and the presence of feces in rectalampulla. As expected, considerable interindividualvariation in bioavailability of morphine administeredrectally have been reported. Whereas suppositoriesgenerally achieve peak effect within 60 –90 minutes,liquid rectal formulations seem to have a shorter peakeffect.31
TransmucosalAn oral transmucosal formulation of fentanyl in a ma-trix that dissolves when rubbed against the buccalmucosa has been developed recently. Transmucosalfentanyl provides a rapid onset of pain relief within5–10 minutes,32 comparable to parenterally adminis-tered fentanyl. In controlled studies, most patientsfound this approach safe and effective for episodicpain.33–36 Formulations incorporating 200, 400, andmore will be available soon in Europe. Dose titrationshould be individualized, because there is a lack ofrelation between the effective dose of transmucosalfentanyl and fixed schedule of opioids.34,35 Somno-lence, nausea, and dizziness are the most commonadverse effects associated with this fentanyl formula-tion. Transmucosal fentanyl was used safely and ef-fectively during long-term treatment of episodic painfor cancer patients at home.37 In a recent pilot study,intranasal fentanyl in doses of 20 �g recently has beenreported to be effective in the management of epi-sodic pain.38
Subcutaneous and intravenous routeThe onset of action of noninvasive administration maybe too slow, and better results may be obtained with aparenteral rescue dose. Subcutaneous administrationis associated with a slower onset of effect than intra-venous administration, but it should be consideredequivalent in terms of efficacy, unless when high vol-umes are required.39 Opioids are commonly adminis-tered via a subcutaneous or intravenous cannula.Repetitive intramuscular injections are not recom-mended, because they are painful and do not offerpharmacokinetic advantages.
Opioids suitable for subcutaneous infusion mustbe soluble, well absorbed, and nonirritant. Injectionsite should be changed every 3–7 days, depending onthe type of needle used. Teflon cannulas are better
Episodic Pain in Cancer/Mercadante et al. 837

| 323 323Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
261
tolerated. Among opioids, methadone appears to berelatively irritating.40
More often, these approaches are used in con-junction with simple or sophisticated devices that thepatients control to deliver a bolus “on demand,” set byphysicians. The optimal candidates for intravenous orsubcutaneous patient-controlled analgesia (PCA) arepatients with intravenous or subcutaneous accesswith irregular or rapidly accelerating pain requiring animmediate treatment.41 The PCA device should be setinitially to deliver a continuous infusion with the bolusdose at 25% of the hourly dose and with a lockoutintervals of 2 hours. The bolus dose should be ad-justed to provide supplementary analgesia to counteror minimize episodic pain.42,43 Cognitive impairment,technical expertise, drug-seeking behavior, and costsare the major drawbacks of this technique.41
Invasive TechniquesPain syndromes with episodic somatic and neuro-pathic mechanism have been resolved by intermittentor continuous administration of local anesthetic by acatheter. This is because of the finding that somelocations are more readily accessible with respect toother areas receiving a significant overlap in sensoryinnervation.
The spinal administration of local anestheticswith an opioid may provide additional analgesia inpatients unresponsive to systemic therapies. Individ-ual titration seems to be mandatory to preventthe adverse effects of local anesthetics.42 Epiduralclonidine is an important alternative. The benefitseems to be more evident in patients with neuropathicpain.43
A percutaneous cordotomy may be indicated in aselected group of patients with refractory incidentpain from bone metastases. However, the risk of seri-ous complications, including mirror pain, general fa-tigue or hemiparesis, and respiratory depression, ishigh. Intrathecal phenol block, chemical neurolysis ofintercostal nerves, and pituitary ablation have beenused for cancer pain. The results of these invasiveprocedures are often suboptimal when consideringthe risk of serious side effects.17
CONCLUSIONEpisodic pain, that is, a transitory exacerbation of painthat occurs in addition to otherwise stable persistentpain, has been associated with a reduced likelihoodfor adequate pain control. Despite the variable inci-dence of this condition reported in several surveys,probably because this phenomenon is diagnosed dif-ferently in various countries, few prospective con-trolled study have assessed the efficacy of a treatment
with traditional drugs commonly used for cancer pain,including opioids, anticonvulsants, antidepressants,and NSAIDs, unless for transmucosal fentanyl. An at-tempt to clarify the cultural aspects between Euro-pean and American people could contribute in ho-mogenizing the language and definition of thisphenomenon. Further prospective studies using sim-ilar terminologies are necessary to find the therapeuticintervention, according to the temporal pattern char-acteristics and the pain mechanism involved.
REFERENCES1. Hanks GW, Portenoy RK, MacDonald N. Difficult pain prob-
lems. In: Doyle D, Hanks GW, MacDonald N, editors. Oxfordtextbook of palliative medicine. Oxford, UK: Oxford MedicalPublications, 1993:257–74.
2. Portenoy RK, Hagen NA. Breakthrough pain: definition,prevalence, and characteristics. Pain 1990;41:273– 81.
3. Banning A, Sjogren P, Henriksen H. Treatment outcome in amultidisciplinary cancer pain clinic. Pain 1991;47:129 –34.
4. Bruera E, Schoeller T, Wenk R, et al. A prospective multi-center assessment of the Edmonton staging system for can-cer pain. J Pain Symptom Manage 1995;10:348 –55.
5. Caraceni A, Portenoy RK, et al An international survey ofcancer pain characteristics and syndromes. Pain 1999;82:263–74.
6. Mercadante S, Maddaloni S, Roccella S, Maddaloni S, Sal-vaggio L. Predictive factors in advanced cancer pain treatedonly by analgesics. Pain 1992;50:151–5.
7. Fine PG, Busch MA. Characterization of breakthrough painby hospice patients and their caregivers. J Pain SymptomManage 1998;16:179 – 83.
8. Petzke F, Radbruck L, Zech D, Loick G, Grond S. Temporalpresentation of chronic cancer pain: transitory pains onadmission to a multidisciplinary pain clinic. J Pain SymptomManage 1999;17:391– 401.
9. Portenoy RK, Payne D, Jacobsen P. Breakthrough pain: char-acteristics and impact in patients with cancer pain. Pain1999;81:129 –34.
10. Fine PG, Busch MA. Characterization of breakthrough painby hospice patients and their caregivers. J Pain SymptomManage 1998;16:179 – 83.
11. Zeppetella G, O’Doherty CA, Collins S. Prevalence and char-acteristics of breakthrough pain in cancer patients admittedto a hospice. J Pain Symptom Manage 2000;20:87–92.
12. Mercadante S. What is the definition of breakthrough pain?Pain 1991;45:107.
13. Bruera E, MacMillian K, Kuehn N, et al. Circadian distribu-tion of extra doses of narcotic analgesics in patients withcancer pain: a preliminary report. Pain 1992;49:311– 4.
14. Gourlay GK, Plummer JL, Cherry DA. Chronopharmacoki-netic variability in plasma morphine concentrations follow-ing oral doses of morphine solution. Pain 1995;61:375– 81.
15. MacFarlane BV, Wright A, Benson HA. Chronic neuropathicpain and its control by drugs. Pharmacol Ther 1997;75:1–19.
16. Portenoy RK. Treatment of temporal variations in chroniccancer pain. Semin Oncol 1997;243(Suppl.16):7–12.
17. Mercadante S. Malignant bone pain: pathophysiology andtreatment. Pain 1997;69:1– 8.
18. Portenoy RK. Adjuvant analgesic agents. Hematol Oncol ClinNorth Am 1996;10:103–19.
838 CANCER February 1, 2002 / Volume 94 / Number 3

324 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
262
19. Fulfaro F, Casuccio A, Ticozzi C, Riupamonti C. The role ofbisphosphonates in the treatment of painful metastatic dis-ease: a review of phase III trials. Pain 1998;78:157– 69.
20. Mercadante S, Villari P, Ferrera P, Dabbene M. Pamidronatein incident pain due to bone metastases. J Pain SymptomManage 2001;22:630 –1.
21. Mercadante S, Arcuri E, Tirelli W, Casuccio A. The analgesiceffect of intravenous ketamine in cancer patients on morphinetherapy: a randomized controlled double-blind cross-overdouble dose study. J Pain Symptom Manage 2000;20:246–52.
22. McQuay HJ, Moore RA. An evidence based resource for painrelief. Oxford, UK: Oxford University Press, 1998.
23. Sindrup SH, Jensen TS. Efficacy of pharmacological treat-ment of neuropathic pain: an update and effect related tomechanism of action. Pain 1999;83:389 – 400.
24. Krajnik M, Zylicz Z, Finlay I, Luczak J, van Sorge AA. Poten-tial uses of topical opioids in palliative care—report of 6cases. Pain 1999;80:121–5.
25. Keating HJ, Kundrat M. Patient-controlled analgesia withnitrous oxide in cancer pain. J Pain Symptom Manage 1996;11:126 –30.
26. Bruera E, Fainsinger R, MacEachern T, et al. The use of meth-ylphenidate in patients with incident cancer pain receivingregular opiates. A preliminary report. Pain 1992;50:75–7.
27. Kunz KM, Theisen JA, Schoeder ME. Severe episodic pain:management with sublingual sufentanil. J Pain SymptomManage 1993;8:189.
28. Coluzzi PH. Sublingual morphine: efficacy reviewed. J PainSymptom Manage 1998;16:184 –92.
29. Mercadante S, Arcuri E. Breakthrough pain in cancer pa-tients. Pathophysiology and treatment. Cancer Treat Rev1998;24:425–32.
30. Ripamonti C, Bruera C. Rectal, buccal, and sublingual nar-cotics for the management of cancer pain. J Palliat Care1991;7:30 –5.
31. De Conno F, Ripamonti C, Saita L, et al. Role of rectal routein treating cancer pain: a randomized crossover trial of oralversus rectal morphine administration in opioid-naive can-cer patients with pain. J Clin Oncol 1995;13:1004 – 8.
32. Cleary JF. Pharmacokinetic and pharmacodynamic issues inthe treatment of breakthrough pain. Semin Oncol 1997;24(Suppl.16):S16 –39.
33. Christie JM, Simmonds M, Patt R, et al. Dose-titration, mul-ticenter study of oral transmucosal fentanyl citrate for the
treatment of breakthrough pain in cancer patients usingtransdermal fentanyl for persistent pain. J Clin Oncol 1998;16:3238 – 45.
34. Farrar JT, Cleary J, Rauck R, Busch M, Nordbrock E. Oraltransmucosal fentanyl citrate: randomized, double-blinded,placebo-controlled trial for treatment of breakthrough painin cancer patients. J Natl Cancer Inst 1998;90:611– 6.
35. Portenoy RK, Payne R, Coluzzi P, et al. Oral transmucosalfentanyl citrate (OTFC) for the treatment of breakthroughpain in cancer patients: a controlled dose titration study.Pain 1999;79:303–12.
36. Coluzzi PH, Schwartzberg L, Conroy JD, Chaparata S, GayM, Busch MA, et al. Breakthrough cancer pain: a random-ised trial comparing oral transmucosal fentanyl citrate(OTFC) and morphine sulphate immediate release (MSIR).Pain 2001;91:123–30.
37. Payne R, Coluzi P, Hart L, Simmonds M, Lyss A, Rauck R, etal. Long-term safety or oral transmucosal fentanyl citrate forbreakthrough cancer pain. J Pain Symptom Manage 2001;22:575– 83.
38. Zeppetella G. An assessment of the safety, efficacy, andacceptability of intranasal fentanyl citrate in the manage-ment of cancer-related breakthrough pain: a pilot study. JPain Symptom Manage 2000;20:253– 8.
39. Nelson KA, Glare A, Walsh D, Groh ES. A prospective, with-in-patient, crossover study of continuous intravenous andsubcutaneous morphine for chronic cancer pain. J PainSymptom Manage 1997;13:262–7.
40. Bruera E, Fainsinger R, Moore M, et al. Local toxicity withsubcutaneous methadone. Experience of two centers. Pain1991;45:141–3.
41. Mercadante S. Alternatives to oral opioids for cancer pain.Oncology 1999;13:215–25.
42. Ripamonti C, Bruera E. Current status of patient-controlledanalgesia in cancer patients. Oncology 1997;11:373– 80.
43. Walsh T, Smith EM, Currie K, et al. A pilot study, review ofliterature, and dosing guidelines for patient-controlled an-algesia using subcutaneous morphine sulphate for chroniccancer pain. Palliat Med 1992;6:217–26.
44. Mercadante S. Problems of long-term spinal opioid treat-ment in advanced cancer patients. Pain 1999;79:1–13
45. Eisenach JC, Du Pen S, Dubois M, et al. Epidural clonidineanalgesia for intractable cancer pain. Pain 1995;61:391–9.
Episodic Pain in Cancer/Mercadante et al. 839

| 325 325Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
263
Pain and pain treatments in European palliative care units.A cross sectional survey from the European Association forPalliative Care Research NetworkPal Klepstad Department of Circulation and Medical Imaging, Norwegian University of Science and Technology,
Stein Kaasa Department of Clinical and Molecular Medicine, Norwegian University of Science and Technology,
Trondheim, Norway, Nathan Cherny Pain and Palliative Medicine, Shaare Zedek Medical Center, Jerusalem,
Israel, Geoffrey Hanks Department of Palliative Medicine, Bristol Oncology Centre, Bristol, UK, Franco deConno Istituto Nazionale dei Tumori, Milan, Italy and the Research Steering Committee of the EAPC+
The Research Network of the European Association for Palliative Care (EAPC) performed a
survey of 3030 cancer patients from 143 palliative care centres in 21 European countries.
The survey addressed pain intensity and the use of non-opioid analgesics, adjuvant
analgesics and opioids.
Patients were treated with analgesics corresponding to the WHO pain ladder step I
(n�/855), step II (n�/509) and step III (n�/1589). The investigators assessed 32% of the
patients as having moderate or severe pain. In general there were small differences
between pain intensities across different countries. Cancer primary sites and the presence
of metastasis had only minor influences on pain intensity. The most frequently used non-
opioid analgesics were NSAIDs (26%) and paracetamol (23%). Adjuvant analgesics or co-
analgesics used by �/1% of the patients were corticosteroids (39%), tricylic antidepres-
sants (11%), gabapentin (5%), bisphosphonates (4%), clonazepam (2%), carbamazepine
(4%) and phenytoin (2%). The use of non-opioid analgesics and co-analgesics varied widely
between countries. Opioids administered for mild to moderate pain were codeine (8%),
tramadol (8%), dextropropoxyphene (5%) and dihydrocodeine (2%). Morphine was the
most frequently used opioid for moderate to severe pain (oral normal release morphine:
21%; oral sustained-release morphine: 19%; iv or sc morphine: 10%). Other opioids for
moderate to severe pain were transdermal fentanyl (14%), oxycodone (4%), methadone
(2%), diamorphine (2%) and hydromorphone (1%). We observed large variations in the use
of opioids across countries. Finally, we observed that only a minority of the patients who
used morphine needed very high doses. Palliative Medicine 2005; 19: 477�/484
Key words: analgesics; cancer; opioid; pain; palliative care; survey
Introduction
Pain is one of the most frequent symptoms among cancer
patients with metastatic disease. The prevailing principle
for treatment of cancer pain is the WHO three-step pain
ladder in which pain treatment is escalated from the use
of non-opioids as the first step, through a second step
using opioids for mild to moderate pain, up to the third
step applying opioids for moderate and severe pain.1
Based on the WHO pain ladder, a more detailed
European recommendation for the use of morphine and
alternative opioids has been published by an expert
committee of the European Association for Palliative
Care (EAPC),2 which parallels its US counterpart’s
guidelines for the treatment of cancer pain.3
Despite the widespread use and recognition of recom-
mendations for the treatment of cancer pain, results from
retrospective and prospective surveys consistently show
that pain is still prevalent in patients with malignant
disease. Cleeland et al . surveyed the intensity of pain in
1308 outpatients with metastatic cancer and observed
that 42% of those with pain were not given adequate
analgesic therapy.4 The inadequacy of cancer pain
treatment was also demonstrated by an IASP Task Force
on Cancer Pain survey which reported that among 1095
patients treated by pain specialists, 20% reported average
pain intensity of ]/7 on a 10-point numerical rating
scale and 67% reported worse pain of ]/7.5 A recent
*At the time of this study the members of the ResearchCommittee of the EAPC were Franco de Conno (chair),Augusto Caraceni, Nathan Cherny, Jose Antonio FerrazGoncalves, Carl Johan Furst, Geoffrey Hanks, Stein Kaasa,Sebastiano Mercadante, Juan Manuel Nunez Olarte, LukasRadbruch, Carla Ripamonti and Frederic Stiefel.Address for correspondence: Pal Klepstad, Department ofAnaesthesiology and Acute Medicine, St. Olavs UniversityHospital, 7006 Trondheim, Norway.E-mail: [email protected]
Palliative Medicine 2005; 19: 477�/484
# 2005 Edward Arnold (Publishers) Ltd 10.1191/0269216305pm1054oa

326 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
264
Norwegian survey observed that 13% of cancer patients
on ongoing morphine treatment reported an average pain
score of ]/7. These data suggest that there has been littleimprovement in pain treatment since the IASP task force
project was completed.6
In 2000, the Research Network of the EAPC initiated a
questionnaire survey among 141 palliative care centres in
21 European countries. One of the main objectives of the
survey was to provide detailed information on the use of
strong opioids and other key drugs by specialist palliative
care services. This was a select sample of patients in thecare of palliative care services, but the data provide some
insights into the epidemiology of symptoms and the use
of non-opioid and opioid analgesic drugs in a palliative
care patient population across European countries.
Methods
Palliative care centresThe project was organized by the Research Network of
the EAPC. Palliative care centres were recruited from 15
states in the European Union (in June 2000), as well as
Norway, Switzerland, Iceland, Israel, Romania and
Cyprus. In each country a national co-ordinator
recruited individual centres with a maximum of ten in
each country. In the countries where the national co-
ordinators identified more than ten palliative carecentres, a representative selection based upon the dis-
tribution of palliative care programmes in that country
was identified. Data on contributing centres, patient
demographics and symptoms will be reported in a
separate paper.
Study period
This was a cross-sectional survey performed during week
23 of the year 2000. All patients treated in the palliativecare programme, either as in-patients or out-patients,
during this week were eligible.
Study procedure
A physician or other health care professional completed a
questionnaire for each patient currently in the care of the
palliative care service. The questionnaire included the
demographics, age, gender, cancer diagnosis and presence
of metastasis. Current medications used for pain control
at the time of inclusion into the study were recorded asyes or no in respect of predefined categories of medica-
tions. These categories included the non-opioid drugs:
paracetamol, dipyrone, aspirin, NSAIDs, dexametha-
sone, prednisolone, other corticosteroids, amitriptyline,
other antidepressants, gabapentin, carbamazepine, phe-
nytoin and clonazepam. The opioid drugs recorded were
codeine, tramadol, dextropropoxyphene, dihydrocodeine,
morphine, fentanyl, methadone, oxycodone, diamor-
phine, hydromorphone and hydrocodone. Doses were
registered for those patients who used morphine. The
investigators assessed the patients’ symptom severity over24 hours applying a 4-point verbal rating scale with the
descriptors none, mild, moderate or severe. The symp-
toms rated were pain, fatigue, generalized weakness, focal
weakness, anxiety, anorexia, depression, confusion, con-
stipation, diarrhoea, nausea, vomiting, sleep disturbance,
dyspnoea, itching, hallucination and hiccups.
Statistics
All data are descriptive in character. Collection and
organization of the data were performed at the Unit forApplied Clinical Research, Norwegian University of
Science and Technology. The SPSS statistical software
for Windows v.10.07 was used for all statistical analyses.
Results
PatientsReports were submitted on 3030 patients from 143
centres located in 21 countries. The patients were
admitted to cancer hospital departments (8%), general
hospital departments (28%), hospices (39%) or treated as
outpatients (26%). The patients mean age was 66 years
(0�/19 years: 24 patients; 20�/39 years: 127 patients;
40�/59 years: 798 patients; 60�/79 years: 1555 patients;
80�/99 year: 504 patients, �/100 years: three patients).The majority of patients suffered from a malignant
disease (94%). Other diseases were neurological (3%),
respiratory (0.5%), cardiac (0.5%), renal (0.3%) or AIDS
(0.3%).
Among those patients with cancer, breast cancer was
the most prevalent malignant diagnosis with lung cancer
and colorectal cancer as the second and third most
prevalent cancer diagnosis (Table 1). Some 30% of thepatients had bone metastases. Liver and lung were the
two other sites of metastasis observed in more than
one-tenth of the patients (Table 2).
Pain and other symptoms
A total of 32% of the patients had pain of intensity that
was moderate or severe (Table 3). The reported pain
intensity varied between countries: on a 4-point scale, the
lowest mean score of 1.6 was reported from Austria and
the highest mean score of 2.6 was reported fromRomania. However, in general there were small differ-
ences in pain intensity across different countries (data can
be supplied from the first author).
The percentage of patients who were considered to
have moderate or severe pain were 11% of those receiving
WHO pain ladder step I treatment (n�/855), 30% for
step II treatment (n�/509) and 43% for step III treatment
(n�/1589). Overall, there were only minor differences in
478 P Klepstad et al.

| 327 327Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
265
pain intensities between different cancer diagnoses (data
can be supplied from the first author). The only notable
exception was for primary brain tumours, which wereassociated with reports of lower pain intensity than other
sites. Pain severity was not influenced by the presence of
bone, liver, lung or brain metastases (data can be
supplied from the first author).
Symptoms other than pain were prevalent in this
population. Commonly reported symptoms of moderate
or greater severity were generalized weakness (53%),
fatigue (51%), anxiety (30%), anorexia (27%), constipa-tion (20%), mood disorder (19%), lack of sleep (17%),
dyspnoea (16%) and nausea (10%) (Table 3).
Non-opioid analgesics
NSAIDS and paracetamol were the most frequently used
non-opioid analgesics. Acetylsalicylic acid (1%) anddipyrone (2%) were given only to a small number of
patients.
Use of adjuvant analgesics was commonplace. Various
types of corticosteroids were used by 39% of the patients
and dexamethasone was the most frequent choice. Less
commonly used adjuvant analgesics were tricylic anti-
depressants, most often amitriptyline (11%), gabapentin
(5%), bisphosphonates (pamidronate and clodronate)
(4%), clonazepam (2%), phenytoin (2%), carbamazepine
(4%), sodium valproate (1%), baclofen (1%), calcitonin(0.4%) and sodium channel blockers (lidocaine and
mexiletine) (0.2%). The use of non-opioid analgesics
and adjuvant analgesics varied widely between countries
(Table 4).
Opioid analgesics
The opioids administered for mild to moderate pain were
codeine (8%), tramadol (8%), dextropropoxyphene (5%)and dihydrocodeine (2%). Morphine was the most fre-
quently used opioid for moderate to severe pain (oral
normal release morphine: 21%; oral sustained-release
morphine: 19%; iv or sc morphine: 10%). Other opioids
used in the management of severe pain were transdermal
fentanyl (14%), oxycodone (normal release oxycodone:
2%; sustained release oxycodone: 2%), methadone (2%),
diamorphine (2%) and hydromorphone (1%).Of those patients receiving morphine, approximately
three-quarters were treated with doses B/150 mg/24
hours, and only a very small minority used a dose
�/1000 mg (Table 5). Similar sets of data were not
reported for the other opioids.
The use of step II opioids varied across countries
(Table 6). Codeine was not given to cancer patients in
Austria and Portugal, while 25% of the patients fromGreece received this drug. The Greek patients, however,
did not use tramadol, a drug used frequently in Romania
(23%), Italy (23%), Finland (17%), Portugal (14%) and
Spain (13%). Also the prescription practice of another
WHO step II drug, dextropropoxyphene, varied between
countries. One quarter of Romanian patients received
dextropropoxyphene, a drug not used at all in nine of the
countries.
Table 1 Malignant diagnosis
Primary site Number of patients %
Breast 471 17Lung 395 14Colorectal 349 12Prostate 214 8Female reproductive organs 201 7Head and neck 189 7Stomach 134 5Pancreas 121 4Haematological malignancy 114 4Bladder 87 3Renal 71 3Skin (including malignant melanoma) 54 2Oesophagus 44 2Sarcoma 37 1Brain 32 1Liver 25 1Thyroid 18 1Others 228 8Unknown 59 2
Total 2843 100
Table 2 Localization of metastases
Site Number of patients %
Bone 901 30Liver 605 20Lung 450 15Peritoneum 283 9Brain 231 8Skin 124 4Pleural 119 7Others 325 11
Table 3 Symptom severity: clinician assessment*
Severity None(%)
Mild(%)
Moderate(%)
Severe(%)
Pain 31 37 24 8Fatigue 16 33 33 18Generalized weakness 17 30 33 20Anxiety 40 30 21 9Anorexia 43 30 18 9Depression 52 28 14 5Constipation 54 27 14 6Poor sleep 57 27 13 4Dyspnoea 65 20 12 4Focal weakness 70 10 11 9Nausea 70 21 8 2Confusion 79 11 6 3Vomiting 84 10 5 2Diarrhoea 91 5 3 1Itch 92 5 2 1Hallucination 95 3 1 1Hiccups 96 2 1 0.5
*Overall severity for the past 24 hours.
Cross sectional survey from the European Association 479

328 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
266
Table
4Useofnon-opioidsbycountry(No.ofpatients
(%ofpatients))
Total
(n�
/3030)
Austria
(n�
/59)
Belgium
(n�
/109)
Cyprus
(n�
/133)
Denmark
(n�
/88)
Finland
(n�
/139)
France
(n�
/160)
Germ
any
(n�
/101)
UK
(n�
/783)
Greece
(n�
/72)
Iceland
(n�
/72)
Paracetamol
700(23)
016(15)
60(45)
38(43)
8(6)
28(18)
2(2)
261(33)
11(15)
7(10)
NSAIDs
792(26)
11(19)
9(8)
38(29)
13(15)
40(29)
23(14)
33(33)
222(28)
28(39)
20(28)
Acetylsalicylic
acid
43(1)
00
00
2(1)
1(1)
037(5)
00
Dipyrone
66(2)
6(10)
1(1)
00
03(2)
30(30)
1(0.1)
00
Corticosteroids
1179(39)
27(46)
36(24)
30(23)
57(65)
51(37)
68(43)
41(41)
228(29)
20(28)
30(42)
TCA
337(11)
4(7)
5(5)
5(4)
19(22)
11(8)
37(23)
23(23)
89(11)
16(22)
11(15)
Gabapentin
152(5)
1(2)
2(2)
1(1)
15(17)
6(4)
11(7)
4(4)
30(4)
4(6)
0Bisphosphonates
132(4)
3(5)
01(1)
2(2)
6(4)
9(6)
5(5)
30(4)
1(1)
0Clonazepam
57(2)
1(2)
1(1)
00
1(1)
29(18)
4(4)
1(0.1)
01(1)
Phenytoin
64(2)
02(2)
9(7)
02(1)
01(1)
16(2)
2(3)
1(1)
Carbamazepine
108(4)
5(9)
3(3)
2(2)
09(7)
3(2)
6(6)
24(3)
3(4)
3(4)
Ireland
(n�
/205)
Israel
(n�
/107)
Italy
(n�
/269)
Luxembourg
(n�
/5)
Netherlands
(n�
/42)
Norw
ay
(n�
/121)
Portugal
(n�
/43)
Romania
(n�
/94)
Spain
(n�
/195)
Sweden
(n�
/168)
Switzerland
(n�
/65)
Paracetamol
27(18)
6(6)
10(4)
5(100)
15(36)
47(39)
12(28)
11(12)
32(16)
82(49)
22(34)
NSAIDs
79(37)
8(8)
94(35)
3(60)
13(31)
16(13)
11(26)
41(44)
42(21)
33(20)
15(32)
Acetylsalicylic
acid
1(0.5)
00
00
1(1)
00
00
1(2)
Dipyrone
014(13)
00
00
00
11(6)
00
Corticosteroids
93(44)
41(38)
206(54)
4(80)
11(25)
38(31)
21(49)
30(32)
85(44)
90(54)
32(49)
TCA
13(6)
5(5)
32(2)
1(20)
1(2)
9(7)
7(16)
30(22)
9(5)
9(5)
1(2)
Gabapentin
21(10)
016(6)
1(20)
2(5)
5(4)
2(5)
9(10)
14(7)
5(3)
3(5)
Biphosphonates
5(5)
11(10)
20(8)
2(40)
1(2)
05(12)
5(5)
7(4)
9(5)
4(6)
Clonazepam
2(1)
7(7)
00
00
00
6(3)
04(6)
Phenytoin
10(5)
3(3)
00
2(5)
02(5)
1(1)
9(5)
2(1)
2(3)
Carbamexapine
3(1)
2(2)
9(3)
00
5(4)
2(5)
13(14)
6(3)
8(5)
2(3)
Distributionbycountriesfornon-opioid
analgesic
drugsandco-analgesicsusedby�
/1%
ofthepatients.Somepatients
mayhavereceivedanon-opioid
drugoraco-
analgesic
drugforindicationsotherthanpain.
480 P Klepstad et al.

| 329 329Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
267
The formulation of morphine varied between coun-
tries. Oral normal release morphine is most frequently
used in Ireland, Denmark and Norway, while Romania,Luxembourg, Iceland and Italy rarely use this formula-
tion. The use of sustained release morphine varied from
3% in Greece to 43% in Iceland. The use of sc or iv
morphine varied from B/5% in several countries (Cyprus,
Finland, UK, Greece) to �/30% in Austria and Portugal.
Fentanyl was the most used opioid for moderate or
severe pain in Belgium, Denmark, Greece and Nether-
lands. Oxycodone was most used in Denmark, Finlandand Israel, hydromorphone most often used in Germany,
Ireland and Switzerland and diamorphine was used only
in Belgium and the UK.
Opioids for severe pain were often combined with a
non-opioid analgesic drug. Of the 1416 patients treated
with a WHO step III opioid analgesic, 334 received
paracetamol and 504 received a NSAID.
Discussion
This paper presents a cross-sectional survey of the
incidence and intensity of pain and of the use of analgesic
medications prescribed for pain in European palliative
care units. The principal findings of the survey are that
most patients are treated with moderate doses of
morphine, that there is considerable variability betweencountries in the use of non-opioids, and a similar large
variability between countries in the selection of opioids.
In this survey about one-third of the patients were
assessed as having moderate or severe pain. This result
confirms that pain is still prevalent in cancer patients.
The number of patients with pain observed in this
palliative care patient population was similar to reported
incidences of pain in other cancer patient populations,such as those treated as out-patients,4 or those admitted
to a general hospital.6 The reasons why such a high
proportion of patients had moderate or severe pain are
not clear. Potential causes are lack of knowledge of
adequate pain treatment,7,8 fear of prescribing opioids,9
or patient related barriers towards the use of opioids.10,11
Lack of compliance may cause inferior pain treatment,
especially if opioids are prescribed on an ‘as required’
basis.12 Lack of treatment success may also be caused by
failure to recognize specific cancer pain syndromes
needing differential pain treatments. An IASP Task Force
on Cancer Pain identified 22 pain syndromes as prevalent
and observed that 40% of patients had some pain of
neuropathic origin.5 These findings indicate that in some
cases poor pain control is a result of inaccurate or
inadequate diagnosis.
The pain intensities were in general rather uniform
across the different countries and were also similar to
results obtained in US surveys.4 However, the pain
ratings were slightly higher in some countries of which
Romania had the highest pain scores. It is not clear why
this should be, but potential explanations are differences
in the availability of opioids because of legislative or
economic restrictions, doctor or patient barriers against
opioid use, differences in pain assessment or different
expectations about acceptable pain relief.
Patients with brain cancer had less pain compared to
the other patients. For all other cancer diseases, the
difference in pain from the lowest ratings (gastric and
liver cancer) to the highest ratings (sarcoma and head
and neck cancer) was only 0.5 on the 4-point pain verbal
rating scale. Thus, cancer primary site had no major
influence on pain intensities. This finding was surprising
since it is assumed that highly invasive cancers generally
cause a more intense pain stimulus. Previous studies have
also reported that patients with bone metastases are
subject to more intense pain.13 No association was
observed between the presence of bone metastases and
pain intensity in this survey. The explanation may be that
increased pain caused by a more invasive cancer or by a
metastasis is simply counterbalanced with higher opioid
doses. Another explanation not addressed in this survey
may be that pain related to bone metastases is more
associated with breakthrough pain,13 which is not
adequately assessed using a global pain assessment. The
findings of only minor associations between pain inten-
sity and cancer primary site suggest that clinicians should
not over emphasize the implications of a particular
cancer diagnosis or the presence of metastasis when
considering the expected success of pain treatment.
An interesting finding of this survey is the wide
variation in use of analgesics across countries. This
variability is evident for non-opioids, opioids for mild
to moderate pain, and opioids for moderate and severe
pain. The EAPC guidelines recommend morphine as
the first choice step III opioid.2 Despite the EAPC
recommendation, some countries such as Belgium (fen-
tanyl), Finland (oxycodone), Greece (fentanyl) and Israel
(fentanyl) do not use morphine as the opioid of first
choice. Another interesting opioid in terms of differences
in use between countries is diamorphine, which is
exclusively used in Belgium and the UK. In the UK,
diamorphine is the most frequently used opioid for
Table 5 Distribution of daily doses of morphine
Dose (mg) Morphine oral (%) Morphine parenteral (%)
B/30 28 32�/30�/60 26 26�/60�/150 22 19�/150�/300 13 11�/300�/600 6 6�/600�/1000 3 3�/1000�/1500 1 2�/1500 0.2 0.5
Cross sectional survey from the European Association 481
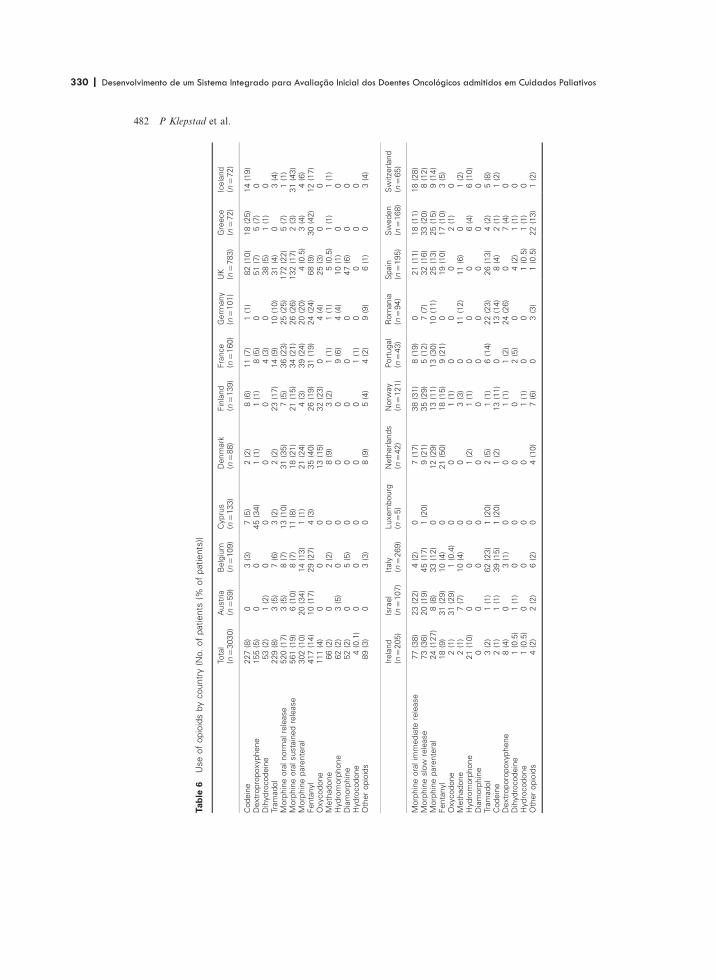
330 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
268
Table
6Useofopioidsbycountry(No.ofpatients
(%ofpatients))
Total
(n�
/3030)
Austria
(n�
/59)
Belgium
(n�
/109)
Cyprus
(n�
/133)
Denmark
(n�
/88)
Finland
(n�
/139)
France
(n�
/160)
Germ
any
(n�
/101)
UK
(n�
/783)
Greece
(n�
/72)
Iceland
(n�
/72)
Codeine
227(8)
03(3)
7(5)
2(2)
8(6)
11(7)
1(1)
82(10)
18(25)
14(19)
Dextropropoxyphene
155(5)
00
45(34)
1(1)
1(1)
8(5)
051(7)
5(7)
0Dihydrocodeine
53(2)
1(2)
00
00
4(3)
038(5)
1(1)
0Tramadol
229(8)
3(5)
7(6)
3(2)
2(2)
23(17)
14(9)
10(10)
31(4)
03(4)
Morphineoralnorm
alrelease
520(17)
3(5)
8(7)
13(10)
31(35)
7(5)
36(23)
25(25)
172(22)
5(7)
1(1)
Morphineoralsustainedrelease
561(19)
6(10)
8(7)
11(8)
18(21)
21(15)
34(21)
26(26)
132(17)
2(3)
31(43)
Morphineparenteral
302(10)
20(34)
14(13)
1(1)
21(24)
4(3)
39(24)
20(20)
4(0.5)
3(4)
4(6)
Fentanyl
417(14)
10(17)
29(27)
4(3)
35(40)
26(19)
31(19)
24(24)
68(9)
30(42)
12(17)
Oxycodone
111(4)
00
013(15)
32(23)
04(4)
25(3)
00
Methadone
66(2)
02(2)
08(9)
3(2)
1(1)
1(1)
5(0.5)
1(1)
1(1)
Hydromorphone
62(2)
3(5)
00
00
9(6)
4(4)
10(1)
00
Diamorphine
52(2)
05(5)
00
00
047(6)
00
Hydrocodone
4(0.1)
00
00
01(1)
00
00
Otheropioids
89(3)
03(3)
08(9)
5(4)
4(2)
9(9)
6(1)
03(4)
Ireland
(n�
/205)
Israel
(n�
/107)
Italy
(n�
/269)
Luxembourg
(n�
/5)
Netherlands
(n�
/42)
Norw
ay
(n�
/121)
Portugal
(n�
/43)
Romania
(n�
/94)
Spain
(n�
/195)
Sweden
(n�
/168)
Switzerland
(n�
/65)
Morphineoralim
mediate
release
77(38)
23(22)
4(2)
07(17)
38(31)
8(19)
021(11)
18(11)
18(28)
Morphineslow
release
73(36)
20(19)
45(17)
1(20)
9(21)
35(29)
5(12)
7(7)
32(16)
33(20)
8(12)
Morphineparenteral
24(127)
8(8)
33(12)
012(29)
13(11)
13(30)
10(11)
25(13)
25(15)
9(14)
Fentanyl
18(9)
31(29)
10(4)
021(50)
18(15)
9(21)
019(10)
17(10)
3(5)
Oxycodone
2(1)
31(29)
1(0.4)
00
1(1)
00
02(1)
0Methadone
2(1)
7(7)
10(4)
00
3(3)
011(12)
11(6)
01(2)
Hydromorphone
21(10)
00
01(2)
1(1)
00
06(4)
6(10)
Diamorphine
00
00
00
00
00
0Tramadol
3(2)
1(1)
62(23)
1(20)
2(5)
1(1)
6(14)
22(23)
26(13)
4(2)
5(8)
Codeine
2(1)
1(1)
39(15)
1(20)
1(2)
13(11)
013(14)
8(4)
2(1)
1(2)
Dextroporopoxyphene
8(4)
03(1)
00
1(1)
1(2)
24(26)
07(4)
0Dihydrocodeine
1(0.5)
1(1)
00
00
2(5)
04(2)
1(1)
0Hydrocodone
1(0.5)
00
00
1(1)
00
1(0.5)
1(1)
0Otheropioids
4(2)
2(2)
6(2)
04(10)
7(6)
03(3)
1(0.5)
22(13)
1(2)
482 P Klepstad et al.

| 331 331Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
269
sc opioid infusions. Diamorphine is preferred to mor-
phine for parenteral administration because of its greater
solubility. Few patients received methadone. The excep-
tion was observed in Romania, where methadone was the
most used opioid for moderate to severe pain, however
this may be related to the low cost of methadone in
Romania. Methadone is a drug in which there has
recently been much renewed interest and is recommended
by several authorities as an alternative opioid in cases not
successfully treated with morphine, especially for patients
suffering from neuropathic pain.14
The use of step II opioids also varied considerably
between countries. For example, the use of tramadol and
dextropropoxyphene varied from no use in some coun-
tries to being the most frequently prescribed opioid drug
in other countries (dextropropoxyphene: Cyprus and
Romania; tramadol: Italy).
The reasons for these large variations in the use of
opioids for cancer pain across Europe are unclear.
Potential factors are clinical traditions, price, education
and legal or cultural barriers to the use of opioids. There
also remains little available data from high quality
studies �/ randomized controlled trials (RCTs) �/ in which
head to head comparisons of opioids have been made.
This lack of formal evidence,15 may be a cause of the
variability in cancer pain treatment between countries.
Another finding in the subsample of patients using
morphine was that relatively few patients needed very
high doses of morphine (Table 4). This observation may
reflect that most patients are adequately treated with low
or moderate doses of opioids, and similar experience has
been reported before.16 However, the number of patients
who still reported moderate or severe pain despite
treatment with step III opioids suggests the possibility
that some, at least, were receiving inadequate doses.Adjuvant analgesics were used in about one-fifth of the
patients. Those used in �/1% of patients were tricyclic
antidepressants, bisphosphonates and anticonvulsants.
The findings in this survey indicate that palliative care
physicians in general apply the recommended co-analge-
sics for selected cases. The choice of adjuvant (i.e.,
gabapentin versus tricyclic antidepressant) varies between
countries.
All patients included in this study were in the care of a
palliative care specialist service. Therefore, this study
represents specialist practice in different European coun-
tries and it is not possible to draw inferences from these
data about non-specialist practice in these countries.
We recognize some limitations in this cross-sectional
study. First, this study used observer ratings for symptom
assessments. Observer assessments are known to under-
estimate pain intensity.17 If present, an under report of
pain should result in a systematic error and therefore not
jeopardize the validity of comparisons across countries,
diagnoses, or different groups of medications. Second, in
this survey we did not obtain data on the number of
patients who refused inclusion or on the number of
eligible patients who were not approached for studyinclusion. Finally, we do not know if all non-opioids or
adjuvant analgesics were prescribed with the intention of
achieving improved pain control. For example, some
patients may have been prescribed paracetamol for fever,
corticosteroids for other diseases or anticonvulsants for
prevention of epileptic seizures.
In conclusion, this survey presents the first European
epidemiological study on palliative care patients’ symp-toms, use of non-opioid analgesics and use of opioids. We
observed that one-third of the individual patients had
clinically significant pain. There were large variations in
the use of both non-opioids and opioids across countries,
but the intensities of pain were still relatively evenly
distributed across the participating countries. Cancer
primary site and the presence of metastases had minor
influence on pain intensity. Finally, we observed that forpatients who used morphine, only a minority needed very
high doses.
Acknowledgements
The study was performed within the Research Network
of the European Association for Palliative Care. In
addition to the authors the following investigators
participated in the study: study coordinator : K Torvik
(Norway). National coordinators : R Likar (Austria),
J Menten, (Belgium), J Kakas (Cyprus), L Pedersen
(Denmark), E Kalso (Finland), P Poulain (France),L Radbruch (Germany), K Mystakidou (Greece),
V Sigurdardottir (Iceland), T O’Brien (Ireland), B Thill
(Luxembuourg), B Zylics (Netherlands), J Ferraz
Goncalves (Portugal), L Ionescu-Calinesti (Romania),
JM Nunes (Spain), CJ Furst (Sweden), F Porchet
(Switzerland), K Done (UK). Coordinators at clinical
sites : Austria: G Forche, JP Zoidl, H Retschitzegger,
M Werni-Kourik, B Stapel, C Stabel. Belgium:A Verhoeve, P Cornil, M Faignaert, T van Iersel,
J Menten, K Sterckx, R Veekhoven, K Claassens,
C Bieke, J Indirjian, S Michael, B Pitsillides, R Christou,
N Koupi. Denmark: M Mørk, A Bonde, L Pedersen,
B Enig. Finland: T Saarto, J Hanninen, T Leino. France:
B Veronique, R Duclos, L Hacpille, G Laval,
MHH Salamagne, P Vinan. Germany: M Cremer,
F Nauck, G Hanekop, L Latasch, W Diemer, M Kloke,L Radbruch, C Bausewein, C Muller-Busch. UK: J Dale,
D Alison, M Fallon, L Forman, C Sinnott, AWilcock, C
Regnard, M Nugent, K Forbes, C Higgs. Greece:
K Mystakidou, E Tsiouri, A Kritikou, E Argiraki,
T Christos, G Evgenia, E Kosmidou, M Tsitoura.
Iceland: V Sigurdardottir, S Bjornsson, N Fredriksdottir,
G Thorsdottir, H Helgadottir, E Hjorleifsdottir. Ireland:
L O’Siorain, S Kingston, J Flemming, R McQuillan,
Cross sectional survey from the European Association 483

332 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
270
M Kearney, S Donelly, T McCormack, T O’Brien. Israel:
Y Zinger, R Gassner, M Bercovitch. Italy: E Arcuri, R
Bortolussi, O Corli, M Gallucci, A Gottlieb, M Maltoni,M Visentin, G Zaninetta, F Zucco. Luxembourg: B Thill.
Netherlands: AJM Wolf, RJ van Boxtel, Z Zylicz, R
Voskamp, J Koningswoud-ten Hove, F Baar. Norway: N
Magerøy, S Ottesen, S Jørgensen. Portugal: F Goncalves,
AL Marques Goncalves, I Galrica Neto. Romania:
C Bogdan, G Popescu, M Daniela, H Cristina. Spain:
JM Nunez Olarte, G Maranon, A Tuca i Rodriguez,
J Porta i Sales, C Centeno Cortes, M Nabal Vicuna,J Sanz Ortiz, N Peraz de Lucas, R Rodeles del Pozo,
L Azuara Rodriguez. Sweden: G Eckerdal, I Fridegren,
I Underskog, CJ Furst, A Janson, A-M Graavgaard,
M Fahlstrom. Switzerland: A Levorato, D Anwar,
S Pautex, G Gremaud, S Eychmuller, H Gudat.
References
1 World Health Organisation. Cancer pain relief. Geneva:WHO, 1996.
2 Hanks GW, De Conno F, Cherny N, et al . Morphine andalternative opioids in cancer pain: the EAPC recommen-dations. Br J Cancer 2001; 84: 587�/93.
3 Jacox A, Carr DA, Payne R, et al . Management of cancerpain: adults quick reference guide, Volume 9. Rockville, MD.Agency for Health Care Policy and Research, US Depart-ment of Health and Human Services Publication, 1994.
4 Cleeland CS, Gonin R, Hatfield AK, et al . Pain and itstreatment in outpatients with metastatic cancer. N Engl JMed 1994; 330: 592�/96.
5 Caraceni A, Portenoy RK and a Working Group of theIASP Task Force on Cancer Pain. An international
survey of cancer patients characteristics and syndromes.Pain 1999; 82: 263�/74.
6 Klepstad P, Loge JH, Borchgrevink PC, Mendoza TR,Cleeland CS, Kaasa S. The Norwegian Brief Pain Inven-tory questionnaire: translation and validation in cancerpain patients. J Pain Symptom Manage 2001; 24: 517�/25.
7 Warncke T, Breivik H, Vainio A. Treatment of cancerpain in Norway. A questionnaire study. Pain 1994; 57:109�/16.
8 Sloan PA, Donelly MB, Scwartz RW, Sloan DA. Cancerpain assessment and management by housestaff. Pain1996; 67: 475�/81.
9 Zenz M, Willweber-Strumpf A. Opiophobia and cancerpain in Europe. Lancet 1993; 341: 1075�/76.
10 Paice JA, Toy C, Shott S. Barriers to cancer pain relief:fear of tolerance and addiction. J Pain SymptomManage1998; 16: 1�/9.
11 Weiss SC, Emanuel LL, Fairclough DL, Emanuel EJ.Understanding the experience of pain in terminally illpatients. Lancet 2001; 357: 1311�/15.
12 Miaskowski C, Dodd MJ, West C, et al . Lack ofadherence with the analgesic regimen: a significantbarrier to effective cancer pain management. J ClinOncol 2001; 19: 4275�/79.
13 Mercadante S. Malignant bone pain: pathophysiologyand treatment. Pain 1997; 69: 1�/18.
14 Ripamonti C, Zecca E, Bruera E. An update on theclinical use of methadone for cancer pain. Pain 1997; 70:109�/15.
15 Jadad AR, Browman GP. The WHO analgesic ladder forcancer pain management. Stepping up the quality of itsevaluation. JAMA 1995; 274: 1870�/73.
16 Hanks GW, Twycross RG. Pain, the physiologicalantagonist of opioid analgesics. Lancet 1984; 1: 1477�/78.
17 Zalon ML. Nurses’ assessment of postoperative patients’pain. Pain 1993; 54: 329�/34.
484 P Klepstad et al.

| 333 333Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
271
SAGEPubl icat ionsPatient demographics and centre description in European
palliative care unitsA cross sectional survey of the European Association for Palliative Care (EAPC)Research Network1
Stein Kaasa Faculty of Medicine, Norwegian University of Science and Technology, Trondheim and Department
of Oncology, St. Olavs University Hospital, Trondheim, Karin Torvik Department of Nursing, College of Higher
Eduction, Oslo, Nathan Cherny Department of Oncology, Shaare Zedek Medical Center, Jerusalem,
Geoffrey Hanks Department of Palliative Medicine, Bristol Haematology and Oncology Centre, Bristol and
Franco de Conno Rehabilitation and Palliative Care, Istituto Nazionale Dei Tumori, Milano
Patients in palliative care are elderly, frail and in decline with multisystem disease. These
and other factors make palliative care research particularly challenging, and has been one of
several reasons why relatively little systematic research has been performed. The European
Association for Palliative Care (EAPC) is seeking to emphasise the importance of research.
The present project is the first empirical multicentre study organised by the EAPC Research
Network, with the aim of identifying the patient population using specialised palliative care,
and identifying a network of palliative care services across Europe, able to participate in a
multicentre collaboration for research.
During a designated week in the autumn of 2000, data on patients were recorded from 143
centres. The survey was carried out by means of two questionnaires, one centre
questionnaire and one patient questionnaire.
Data were submitted on 3013 patients from 22 different European countries. Almost all
patients had cancer (94%), while some had neurological disease (3%). The majority (75%)
had been referred to a palliative care service during the six to seven months before the
survey was performed. Very few patients had less than one week of expected survival
(6%), the majority were expected to live one to six months, while as many as 16% were
expected to live more than one year. The majority of the patients (27%) were fully
ambulatory � the ability to walk independently without any assistance. The majority of the
patients (60%) received care as an outpatient, either at a traditional clinic in an outpatient
cancer hospital (12%), in home-care programs from a specialised advisory service (24%), or
external nursing care (24%).
The population of patients included in this survey was not a sample of dying patients. There
were a substantial number of patients with an anticipated life expectancy of more than six
months. The study demonstrated a considerable enthusiasm for research in the palliative
care community across Europe. The heterogeneity of the sample is evident, and this will
need careful consideration for future clinical trials. This calls for an international consensus
on how to report on patient characteristics within palliative care research. This is necessary
in order to be able to evaluate the representativity of the study population, as well as to
compare data between studies. The range of services encountered in the survey highlights
the need for the organisational and clinical standards for palliative care, which can be
audited. Palliative Medicine 2007; 21: 15�22
Key words: organisation; palliative care; research
1 The members of the Research Steering Committee of theEAPC at the time of the study were Franco de Conno (chair),Augusto Caraceni, Nathan Cherny, Jose Antonio FerrazGoncalves, Carl Johan Furst, Geoffrey Hanks, Stein Kaasa,Sebastiano Mercadante, Juan Manuel Nunez Olarte, LukasRadbruch, Carla Ripamonti and Frederic Stiefel.
Address for correspondence: Stein Kaasa, Pain and PalliationResearch Group, Faculty of Medicine, Norwegian University ofScience and Technology, 7006 Trondheim, Norway.E-mail: [email protected]
Palliative Medicine 2007; 21: 15�22
# 2007 SAGE Publications 10.1177/0269216306072086

334 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
272
SAGEPubl icat ions
Introduction
Palliative care is a relatively young discipline, and
epidemiological data are essential in order to provide a
credible evidence-base for clinical practice.1,2
There are particular difficulties in conducting clinical
research in a palliative care environment. Patients are
elderly, frail and in decline with multisystem disease �patients are usually severely ill with a progressive condi-
tion and limited survival time; they may have many
symptoms for which they will be receiving several drugs
concurrently; and environmental and psychological fac-
tors have a variable, but potentially great effect on
physical well being.3�5
All of these factors make palliative care research
particularly challenging, and is one reason why relatively
little systematic research had been carried out in this
area. The European Association for Palliative Care
(EAPC) has recognised these difficulties, but at the
same time seeks to emphasise the importance of
research.6 The EAPC has set up a Research Network
(RN), whose main objective is to encourage and facilitate
research in palliative care.7
The present project is the first empirical multicentre
study organised by the RN of the EAPC. A secondary
objective of the investigation was to identify a collabora-
tive group of palliative care services across Europe with
the ability to provide epidemiological and clinical data
for this and future studies.The study was a cross-sectional survey, carried out in
2000, and encompassed 143 palliative care centres in 21
European countries. The project included all 15 member
states (at the time of the research) of the European
Union, as well as Norway, Switzerland, Iceland, Israel,
Romania and Cyprus.
The aims of the study were:
1) To identify patient populations using specialist
palliative care services in terms of demographic
data, diagnostic groups, social circumstances
and performance status in 21 different European
countries.
2) To provide detailed information on the use of strong
opioid analgesics and some other key drugs by
specialist palliative care services.3) To identify a network of palliative care services
across Europe with the ability to participate in
collaborative research.
In this paper, the demographics of the palliative care
survey are presented together with basic patient char-
acteristics.
Material and methods
Palliative care centres
One national co-ordinator in each country recruited a
maximum of 10 eligible centres in that country. We did
not attempt to collect a representative sample of patients
and centres according to strict scientific principles.
However, in the countries where the national co-ordina-
tors identified more than 10 centres, he/she was asked toidentify a representative selection based upon his/her own
experience and knowledge of the centres and of the range
and distribution of palliative care programmes in that
country.
Study period
The study was performed during a designated week in
Autumn 2000. All patients who were actively receiving
care from the palliative care programme on one specific
day in the designated week were to be included.
The questionnaires
The survey was carried out by means of two question-
naires. One ‘centre’ questionnaire to be completed foreach centre/programme, and a patient questionnaire to be
completed for every patient. The patient questionnaires
were completed by the doctor, nurse or other health
professionals who was the ‘primary carer’ or who knew
the medical and social details of the patient.
The following information was collected.
Patient data
Anticipated life expectancy (on a categorical scale ran-
ging from ‘B/24 hours’, one to six days’, ‘one week to one
month’, ‘one to six months’, ‘six months to one year’ to‘�/1 year’), mobility (ranging from ‘fully ambulatory’,
‘able to walk independently, but at an impaired level’,
‘needs assistance with walking’, ‘bed- or chair-bound,
able to get to toilet’ to ‘bed- or chair-bound, unable to get
to the toilet’).
Centre data
Type of service provided by the centre categorised as:
‘hospice (freestanding)’, ‘hospital palliative care ward
(inpatient)’, ‘day hospital’, ‘ambulatory service (outpa-
tient)’, ‘palliative care consultation service in a hospital’,‘home care service’, ‘telephone consultation service
(patient follow up)’, ‘telephone consultation service for
community doctors and nurse’, and ‘other’. If more than
one service was provided more than one box could be
ticked off.
Place of palliative care service delivery
Place of palliative care delivery, categorised as: ‘cancer
hospital’, ‘general hospital’, ‘hospice’, ‘ambulatory/out-
patient-based service’, ‘day care’, ‘home care (specialist
16 S Kaasa et al.

| 335 335Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
273
SAGEPubl icat ions
advisory service)’, ‘home care (extended nursing care, or
‘hospice at home’)’ and other. More than one category
could be ticked when care was delivered at several placessimultaneously.
Ethics
Ethical approval was obtained at each centre according
to national and/or regional recommendations.
Statistics
Descriptive statistics only are presented. Collection and
organisation of the data was performed at the Unit for
Applied Clinical Research, Norwegian University of
Science and Technology. The statistical software SPSS
for Windows v. 12 was used for all statistical analyses.
Results
Patients
Data were submitted on 3013 patients from 143 centres
(Table 1). In most countries, with the exception of
France, Ireland, Italy and Spain, the majority of the
patients in this survey were female (56%), and the meanage for the total sample was 66 years (range 2�103 years)
(Table 1). The majority of patients were married (54%),
and the remaining were either widowed (25%), single
(11%), divorced (7.5%), or living with a partner (3%).
Most patients were living with a spouse or other relative
in good health (59%). Almost all the patients had cancer
(94%), while some had a neurological diagnosis (3%),respiratory disease (0.5%), cardiac disease (0.5%), or
AIDS (0.3%). The majority (75%) had been referred to
the palliative care service during the six to seven months
before the survey was performed; 16% had been referred
during the year 1999, while 4% were referred before 1998.
Very few patients had less than one week of expected
survival (6%), the majority were expected to live one to
six months, while as many as 16% were expected to livemore than one year (Figure 1).
The majority of the patients were fully ambulatory
(27%) or able to walk independently (28%), while 21%
were bed- or chair-bound unable to get to the toilet
(Figure 2).
Service characteristics
The number of centres per country varied from one to 13,and the number of patients per country varied from five
to 778 (Table 2). As shown in Table 2, the median number
of patients per centre varied considerably from seven in
Greece and the Netherlands, to 30 and 40 in Norway and
the UK, respectively.
Looking at the range, a substantial number of centres
(48/143) hadB/10 patients included in the study. The
majority of the centres were either based upon a generalhospital (33%), hospice (25%) or cancer hospital (8%),
while a minority of the services were based upon home
care (Table 3). Consequently as many as 2171 (74%) of
the patients were recruited from inpatient-based services.
The type of service provided per centre is presented in
Table 4. In the questionnaire, it was possible to check off
more than one type of service per centre. In order to give
a general overview, the raw scores are expressed inTable 4. In all countries, except Cyprus, all services
provided at least day hospital care and/or ambulatory
Table 1 Patient characteristics
No. %
Age, years (mean; range)Male (66; 2�98) 1320 44Female (66; 3�103) 1693 56
Marital statusSingle 316 10.5Married 1625 54Unmarried with partner 80 3Widows 759 25Divorced 227 7.5Home circumstancesLives alone 851 28Lives with spouse who is in good health 1320 44Lives with spouse who is not in good health 317 10.5Lives with other relative who is In good health 467 15.5Missing home circumstances 58 2
Date of first referral to palliative care2000 2239 741999 472 161998 138 5
DiagnosisCancer 2831 94Neurological 90 3Respiratory 16 0.5Cardiac 15 0.5AIDS 10 0.3Other 43 1.5
Anticipated life expectancy
> 1
yea
r
6 m
onth
s to
1 y
ear
1 to
6 m
onth
s
1 w
eek
to 1
mon
th
1 -
6 da
ys
Les
s th
an 2
4 ho
urs
Perc
ent
50
40
30
20
10
0
Figure 1 Anticipated life expectancy estimated by thehealth care provider (physician)
Patient demographics and centre description in European palliative care units 17

336 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
274
SAGEPubl icat ions
services. Palliative care services within hospitals were
established in most countries. It should be noted that the
sample includes more hospital palliative care wards
(n�/49) than free-standing hospices (n�/35).
Place of care delivery
Place of palliative care delivery was reported for each
patient and included eight categories. More than one
category could be ticked when care was delivered at
several places simultaneously. The majority of the
patients (60%) (Figure 3) received care as an ‘outpatient’,
either at a traditional clinic in an outpatient cancerhospital (12%) or in home care programmes, and received
care from a specialist advisory service (24%) or extended
nursing care (24%). Less than one-quarter of the patients
received care in a hospice.
Discussion
One of the objectives of this project was to identify a
collaborative group of investigators in palliative care
across Europe. The EAPC RN succeeded by recruiting
143 centres from 22 countries, and collected data on a
total of 3013 patients. One reason for the successful
outcome was the establishment of a data co-ordinating
centre at the Palliative Medicine Unit in Trondheim,
Norway. The need for such an organisation has long been
recognised by other groups conducting clinical research
in cancer patients, such as the EORTC, and by research
funding bodies in many countries.
The data collection was successful in spite of severe
constraints on the budget. The national co-ordinators
organised the study in their countries without any
financial reimbursement from the EAPC RN. Clearly,
this reflects the considerable enthusiasm generated by the
project and the keenness of the palliative care services in
so many countries to be involved in research. This
experience contradicts the scepticism, raised by many
palliative care providers, about the willingness of pallia-
tive care centres to participate in research. Several
countries in Europe have identified a need for research
in palliative care. For example, a recent report from the
National Cancer Research Institute in the UK points out
that the organisation of research is fragmented, and that
the challenge is to achieve genuine collaborative work.8
In a Norwegian report, it is recommended that a Chair in
Palliative Medicine should be established at all univer-
sities in the country in order to organise, regionally and
05
101520253035404550
Fully ambulatory Able to walkindependently, butat an impaired level
Needs assistancewith walking
Bed or chair bound,able to get to toilet
Bed or chairbound, unable to
get to toilet
Mobility
Perc
ent
Figure 2 Mobility evaluated by the health care provider(physician)
Table 2 Distribution of centres, patients, gender per country and patients per centres
Country No. of centres No. of patients Gender per country No. of patients per centres
Male (%) Female (%) Median Range (min�max)
Austria 7 58 29 71 10 2�17Belgium 10 109 49 51 9 1�27Cyprus 5 132 36 64 21 15�56Denmark 5 88 36 64 17 8�25Finland 5 139 37 63 20 3�51France 13 160 56 44 10 2�36Germany 9 101 37 63 11 2�23Greece 8 70 43 57 7 2�19Iceland 7 72 39 61 8 1�33Ireland 8 203 53 47 20 8�53Israel 4 104 40 60 22 14�47Italy 10 267 52 48 26 6�50Luxembourg 1 5 20 80 � �Netherlands 6 42 31 69 7 4�10Norway 4 121 39 61 30 20�40Portugal 3 43 39 60.5 10 8�25Romania 5 93 40 60 15 2�43Spain 10 195 51 49 17 6�37Sweden 7 168 42 58 16 5�48Switzerland 6 65 43 57 11 6�20UK 10 778 43 57 40 5�299Total 143 301 44 56 13 1�299
18 S Kaasa et al.

| 337 337Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
275
SAGEPubl icat ions
nationally, education and research within this field.9 The
poor evidence-base for much clinical practice in palliativecare highlights the urgent need for well-conducted
prospective studies, preferably randomised controlled
trials.10 There is no doubt that one common recommen-
dation is the need for national and international colla-
boration in order to perform large enough studies with a
representative sample of patients. Recent Cochrane re-
views evaluating ‘oral morphine for cancer pain’,11 and
‘hydromorphone for acute and chronic pain,12 conclude
that too many small, non-conclusive, studies have been
performed, the heterogeneity of the studies is enormous,
and the possibility to perform meta-analysis is limited.
One interesting finding in this survey is the hetero-geneity of the sample. However, it needs to be taken into
consideration when the data are discussed that the
sample is not representative of centres providing care at
either a national or international level. The number of
centres per country and number of patients per centre
varied considerably. Furthermore, palliative care was
delivered in cancer hospitals and general hospitals, as
well as hospices. The type of services differed somewhat
between countries, however, in most countries both in-
patients, consultation services and home care services
were provided. Such a heterogeneity of palliative care was
also found in a recent report, which assessed the
development of palliative care services.13 Within the
seven countries studied, UK, Sweden, Italy, Germany,
Spain, Belgium and The Netherlands, the ‘founding’
initiative of palliative care took place over a period of 14
years, from 1967 to 1991. The ‘founding’ services varied
from inpatient hospice and hospital inpatient units, to
home care services and palliative care units within
departments of medical oncology. In 1999, the number
of inpatient hospice/palliative care units varied from 219
in the UK, to 18 in the Netherlands and three in Italy. A
similar wide variation was found in the ratio of the
inpatient hospice and palliative care beds to populations.
In the UK, the number of beds per person was 1:17 866,
in Spain 1:49 261 and in Italy 1:1 913 332. These numbers
reflect, to some extent, the different periods of time
during which palliative care has developed in different
countries (with the UK being the longest, starting in
1967), but also differences in the way in which healthcare
is organised and delivered in different countries. Another
problem is related to differences between centres and/or
Table 3 Centre identification ‘What is your centre basedupon?’
No. of patients(%)
No. of centres(%)
Cancer hospital 227 (7.5) 12 (8)General hospital 808 (27) 47 (33)Hospice 1137 (38) 36 (25)Ambulatory/outpatient hospital-based service
39 (1) 1 (0.7)
Day care 7 (0.2) 1 (0.7)Home care (special advice service) 74 (2.5) 7 (5)Home care � ‘hospice at home’ 380 (13) 17 (12)Other 260 (9) 19 (13)Missing centre identification 81 (3) 3 (2)
Table 4 Type of services provided per centre
Country No. of centres Hospice(free-standing)
Hospitalpalliativecare ward(Inpatient)
Day hospitaland/orambulatoryservice(Outpatients)
PC consultationservice in ahospital
Home careservice
Telephoneconsultationservice
Austria 7 2 4 1 1 1 5Belgium 10 2 1 3 2 5 5Cyprus 5 1 4Denmark 5 4 2 3 1 4 4Finland 5 3 3 3 1 3 3France 13 5 9 10 11Germany 9 7 6 5 6 7Greece 8 1 5 1 6 3Iceland 7 3 3 2 5 2Ireland 8 4 4 5 6 8Israel 4 1 1 2 1 3 1Italy 10 2 3 7 6 7 5Luxembourg 1 1 1Netherlands 6 3 2 2 4Norway 4 2 4 2 1 3Portugal 3 2 1 1 2 2Romania 5 2 1 2 3 2Spain 10 5 6 5 5 8Sweden 7 5 1 3 5 3Switzerland 6 1 3 3 3 2UK 10 5 3 8 6 3 5Total 143 35 49 75 54 69 83
Patient demographics and centre description in European palliative care units 19

338 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
276
SAGEPubl icat ions
countries on how the various types of facilities are
defined according to the type of their actual care delivery.
To our knowledge, there is no consensus internationally
on this issue.
Most palliative care patients reported by the partici-
pating services were not imminently dying. One of the
striking, and encouraging, findings of this survey was the
number of patients with an anticipated life expectancy of
more than six months. Indeed, the overwhelming major-
ity of patients had been referred at least six months prior,
and had an anticipated life expectancy of more than a
month. These findings reflect referral and practice
patterns that are in keeping with the WHO recommenda-
tions that palliative care be started relatively early in the
trajectory of incurable illness.
The models of service delivery to palliative care varies
considerably, with regard to the type of facility (inpatient
units, hospice, day care, out patient clinics and home care
services) and also the staffing. There are major national
and international idiosyncrasies which have influenced
the types of service which have been developed and the
involvement and medical and nursing staff, social work-
ers and rehabilitation staff. There are important differ-
ences even within individual countries in the availability
of medical and paramedical staff to multidisciplinary
palliative care teams. In a British survey performed in the
Thames region, access to doctors was only provided in
some centres, and some services describe themselves as
more medically oriented, while other centres describe
themselves as mostly socially oriented.14 In Spain, there
are no free standing hospices, and many home care teams
consist of a core team of a physician and a nurse and,
frequently, a psychologist.15 During the last decade,
palliative care has, in many countries, been incorporated
into the public health care system with public
funding.16�18
In this study, the majority of the centres were general
or cancer hospitals; hospices were in a minority. This
highlights the fact that, in many countries, ‘hospices’ do
not exist, but palliative care is still widely provided within
the secondary care sector. It is not necessary to have a
hospice in order to provide high quality palliative care.
An encouraging finding is that palliative care seems to be
embedded in many countries into the mainstream of
health care delivery. On the other hand, these data may
reflect recruitment bias. We did not attempt to obtain a
representative sample and it is not possible to draw firm
conclusions about all of the issues raised. However, the
data certainly present some interesting trends which need
to be followed up.
Many centres reported on 10 patients. These centres
are clearly very small services or presumably have very
little infrastructure particularly to support research. The
participation of such services in this study indicates a
considerable enthusiasm to further research in palliative
care. The small numbers again emphasise the need to be
cautious in interpreting the data.
The national co-ordinators were asked to include all
palliative care programmes in their country, up to a
maximum of 10 centres. In five countries, the maximum
of 10 centres was reached; Belgium, France, Italy, Spain
and UK. In all other countriesB/10 centres were in-
cluded, which may indicate either that very few palliative
care programmes are developed in that country or that
few are able to participate in such a study. Clearly, there
remains an unmet need for specialist palliative care and
the establishment of new palliative care centres in most
European countries.
There are major differences between countries, even in
Europe, in the way in which health care is organised and
delivered, and for this reason alone it would be very
difficult to produce guidelines on service delivery for
specialist palliative care which would be widely applic-
able. A Task Force of the EAPC is now systematically
collecting information on how palliative care is delivered
in most European countries, and another group is
working on Centres of Excellence in palliative care. The
aim is to improve the understanding of how palliative
care is and should be delivered, and ultimately, this
should lead to international definitions and standards for
palliative care.7
We believe that the data from the present survey
together with the work performed by the EAPC groups
and the political initiatives taken in many countries, will
improve the quality of palliative care and identify
palliative care as a speciality in other countries than the
UK. With different types of palliative care services in
hospitals, or dedicated beds and/or specialist units in
nursing homes/hospices at the community level and home
care programmes, a comprehensive national network of
0
5
10
15
20
25
30
Can
cer
hosp
itals
Gen
eral
hos
pita
ls
Hos
pice
Day
care
Out
pat
ient
sho
spita
l ser
vice
Hom
e ca
re: S
pec.
advi
sory
ser
vice
Hom
e ca
re: E
xt.
nurs
ing
care
Place of palliative caredelivery
Per
cent
Figure 3 Place of palliative care delivery reported by eachcentre, more than one alternative could be ticked
20 S Kaasa et al.

| 339 339Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
277
SAGEPubl icat ions
services will provide care for patients, wherever their
preference is for this care.
Palliative care is assumed by many health careproviders, politicians and the lay public to focus on
terminal care, that is care of the dying patient. It is
noteworthy that the population of patients included in
this survey was not a sample of dying patients. There
were a substantial number of patients with an anticipated
life expectancy of more than six months, and only a
minority was identified as dying patients. This empha-
sises that a palliative care approach may be applicableearly in the disease trajectory, a concept incorporated in
the EAPC definition of palliative care.18
Conclusions
This study has demonstrated a considerable enthusiasm
for research in the palliative care community across
Europe. However, it has also highlighted the fact that
many palliative care services, whilst they may be inter-
ested in carrying out research, do not have the infra-
structure to support it. It seems clear that, in terms of
multicentre clinical trials, the EAPC has access topotentially very large numbers of healthcare workers
who could participate in research and, thus, access to
potentially large numbers of patients.
The heterogeneity of the sample is evident, and this
would need careful considerations for future clinical
trials. We have no doubt that prospective identification
of suitable patients would be possible for a particular
study.The range of services encountered in the different
countries highlights the need for organisational and
clinical standards for palliative care which can be
audited. These are already available in some countries,
such as the UK, but need to be modified to make them
applicable to other European countries. Finally, it is clear
that palliative care services are serving a population of
patients who may not necessarily be in the terminal phaseof their illness. It is appropriate that the principles of
palliative care be applied to the care of cancer patients,
at whatever stage of their illness, when their needs
demand it.
AcknowledgementsThis project was organised by the Research Network
Steering Committee of the EAPC. Data collection was
performed at the Pain and Palliation Research Group at
the Norwegian University of Science and Technology
(NTNU), Trondheim, Norway.
Study coordinator: K Torvik (Norway). National co-
ordinators: R Likar (Austria), J Menten, (Belgium), J
Kakas (Cyprus), L Pedersen (Denmark), E Kalso
(Finland), P Poulain (France), L Radbruch (Germany),
K Mystakidou (Greece), V Sigurdardottir (Iceland), TO’Brien (Ireland), B Thill (Luxembourg), B Zylics
(Netherlands), J Ferraz Goncalves (Portugal), L Iones-
cu-Calinesti (Romania), JM Nunes (Spain), CJ Furst
(Sweden), F Porchet, K Done (UK). Co-ordinators at
clinical sites: Austria: G Forche, JP Zoidl, H Retschit-
zegger, M Werni-Kourik, B Stapel, C Stabel. Belgium: A
Verhoeve, P Cornil, M Faignaert, T van Iersel, J Menten,
K Sterckx, R Veekhoven, K Claassens, C Bieke, JIndirjian, S Michael, B Pitsillides, R Christou, N Koupi.
Denmark: M Mørk, A Bonde, L Pedersen, B Enig.
Finland: T Saarto, J Hanninen, T Leino. France: B
Veronique, R Duclos, L Hacpille, G Laval, MHH.
Salamagne, P Vinan. Germany: M Cremer, F Nauck, G
Hanekop, L Latasch, W Diemer, M Kloke, L Radbruch,
C Bausewein, Harlaching, C Muller-Busch, Havelhohe.
UK: J Dale, D Alison, M Fallon, L Forman, C Sinnott,A Wilcock, C Regnard, M Nugent, K Forbes, C Higgs.
Greece: K Mystakidou, E Tsiouri, A Kritikou, E
Argiraki, T Christos, G Evgenia, E Kosmidou, M
Tsitoura. Iceland: V Sigurdardottir, S Bjornsson,
N Fredriksdottir, G Thorsdottir, H Helgadottir, E
Hjorleifsdottir. Ireland: L O’Siorain, S Kingston, J
Flemming, R McQuillan, M Kearney, S Donelly, T
McCormack, T O’Brien. Israel: Y Zinger, R Gassner,M Bercovitch. Italy: E Arcuri, R Bortolussi, O Corli,
M Gallucci, A Gottlieb, M Maltoni, M Visentin, G
Zaninetta, F Zucco. Luxembourg: B Thill. Netherlands:
AJM Wolf, RJ van Boxtel, Z Zylicz, R Voskamp, J
Koningswoud-ten Hove, F Baar. Norway: N Magerøy, S
Ottesen, S Jørgensen. Portugal: F Goncalves, AL
Marques Goncalves, I Galrica Neto. Romania: C
Bogdan, G Popescu, M Daniela, H Cristina. Spain: JMNunez Olarte, G Maranon, A Tuca i Rodriguez, J Porta i
Sales, C Centeno Cortes, M Nabal Vicuna, J Sanz Ortiz,
N Peraz de Lucas, R Rodeles del Pozo, L Azuara
Rodriguez. Sweden: G Eckerdal, I Fridegren, I Under-
skog, CJ Furst, A Janson, A-M Graavgaard, M Fahl-
strom. Switzerland: A. Levorato, D Anwar, S Pautex, G
Gremaud, S Eychmuller, H Gudat.
References
1 McQuay HJ, Moore A, Wiffen P. The principles ofevidence-based medicine. In Doyle D, Hanks G, ChernyN, Calman K eds. Oxford textbook of palliative care,third edition. 2004: 119�28.
2 Hanks G, Kaasa S, Robbins M. Research in palliativecare: getting started. In Doyle D, Hanks G, Cherny N,Calman K eds. Oxford textbook of palliative care, thirdedition. 2004: 128�38.
3 Jordhøy M, Kaasa S, Fayers P, Ovreness T, UnderlandG, Ahlner-Elmqvist M. Challenges in palliative care
Patient demographics and centre description in European palliative care units 21

340 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
278
SAGEPubl icat ions
research; recruitment, attrition and compliance: experi-
ence from a randomised controlled trial. Palliat Med
1999; 13: 299�310.4 Grande G, Todd C. Why are trials in palliative care so
difficult? Palliat Med 2000; 14: 69�74.5 Cook AM, Finlay IG, Butler-Keating RJ. Recruiting into
palliative care trials: lessons learnt from a feasibility
study. Palliat Med 2002; 16: 163�65.6 Blumhuber H, Kaasa S, De Conno F. The European
Association for Palliative Care. J Pain Symptom Manage
2002; 24: 124�27.7 Available at www. eapcnet.org8 Partners in Cancer Research. Supportive and palliative
care research in the UK: report of the NCRI Strategic
Planning Group on supportive and palliative care.
National Cancer Research Institute, July 2004.9 Norges offentlige utredninger. Livshjelp. Behandling,
pleie og omsorg for uhelbredelig syke og døende. NOU
1999:2.10 Kaasa S, Dale O; Pain and Palliation Research Group.
Building up research in palliative care: an historical
perspective and a case for the future. Clin Geriatr Med
2005; 21: 81�92.11 Wiffen PJ, Edwards JE, Barden J, McQuay HJM.
Oral morphine for cancer pain (Review). The Co-
chrane Collaboration . The Cochrane Library, 2005(Issue 1).
12 Quigley C. Hydromorphone for acute and chronic pain(Review). The Cochrane Collaboration . The CochraneLibrary, 2005 (Issue 1).
13 Clark D, ten Have H, Janssens R. Common threads?Palliative Care Service developments in seven Europeancountries. Palliat Med 2000; 14: 479�90.
14 Higginson IJ, Hearn J, Myers K, Naysmith A. Palliativeday care: what do services do? Palliative Day CareProject Group. Palliat Med 2000; 14: 277�86.
15 Centeno C, Arnillas P, Hernansanz S, Flores LA, GomezM, Lopez-Lara F. The reality of palliative care in Spain.Palliat Med 2000; 14: 387�94.
16 Jordhoy MS, Fayers P, Saltnes T, Ahlner-Elmqvist M,Jannert M, Kaasa S. A palliative-care intervention anddeath at home: a cluster randomised trial. Lancet 2000;356: 888�93.
17 DL. 28 dicembre 1998 n8 450 convertito nella legge(converted in the law) n8 39/99 del 26/2/99 (programmanazionale per la realizzazione di strutture per CurePalliative) (National Programme for the Realization ofStructure of Palliative Care).
18 German Hospice Association (Bundesarbeitsgemein-schaft Hospiz). Available at www.hospiz.net/gesetze/index.html;http://www.eapcnet.org/about/definition.html
22 S Kaasa et al.

| 341 341Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
279

342 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
280
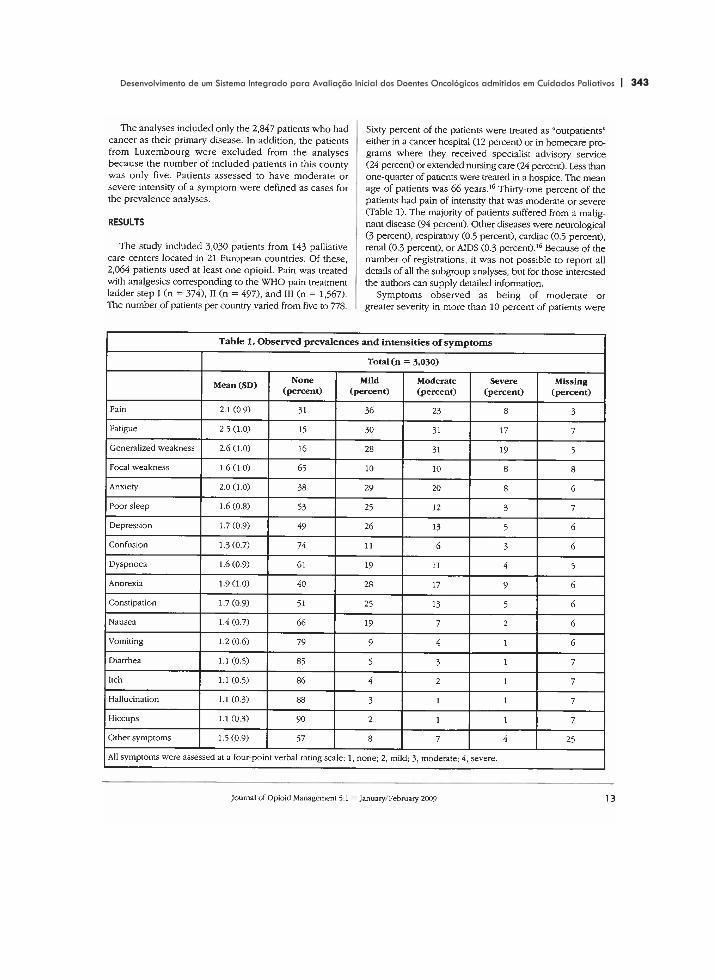
| 343 343Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
281

344 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
282
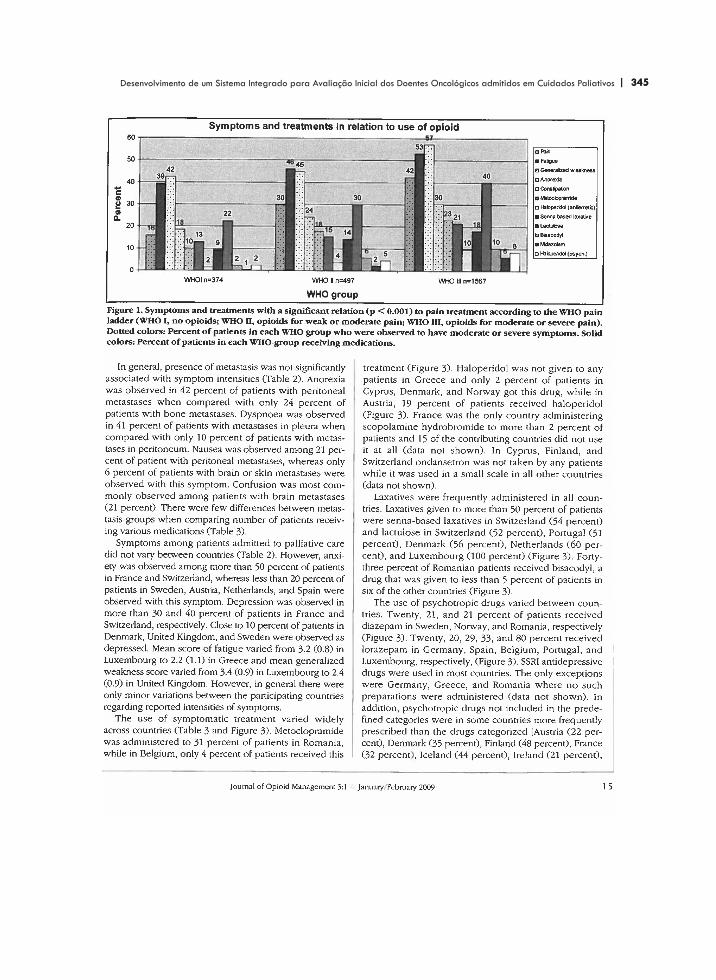
| 345 345Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
283

346 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
284
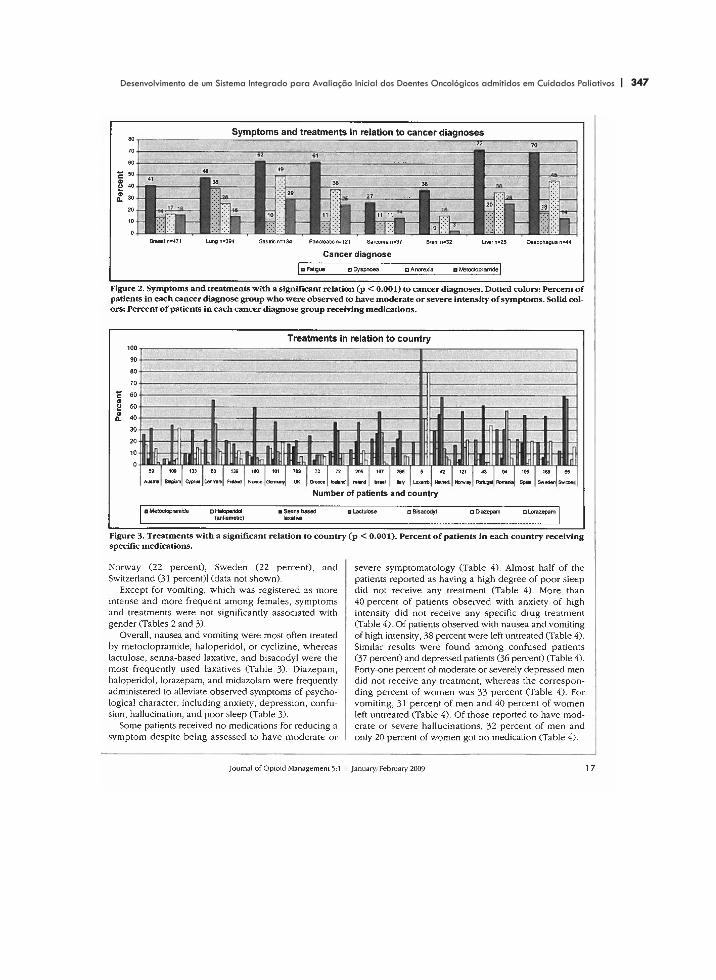
| 347 347Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
285

348 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
286

| 349 349Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
287
350 | | Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
288

| 351 351Desenvolvimento de um Sistema Integrado para Avaliação Inicial dos Doentes Oncológicos admitidos em Cuidados Paliativos
289