decreased sex hormone binding globulin (shbg) and insulin-like growth factor binding protein...
TRANSCRIPT

Clinical Endocrinology (1 990), 33,415422
DECREASED SEX HORMONE BINDING GLOBULIN (SHBG) AND INSULIN-LIKE GROWTH FACTOR BINDING
PROTEIN (IGFBP-1) IN EXTREME OBESITY
J . U . WEAVER, J. M. P. HOLLY, P. G . KOPELMAN, K. NOONAN, C . G. GIADOM, N. WHITE, S. VIRDEE AND J. A. H . WASS
Medical Unit and Department of Chemical Pathology, The London Hospital; Endocrine Department, Chelsea Hospital for Women, London S W3 and
Department of Endocrinology and Chemical Endocrinology, St Bartholomew’s Hospital, London, E C l A 7BE, UK
(Received 9 January 1990; returned,for revision I3 February 1990; .finally revised 10 April 1990: accepred 2 May I990)
SUMMARY
Obesity may be characterized by abnormal sex steroid secretion and reduced sex hormone binding globulin (SHBG) which in turn is related to fat distribution and insulin secretion. Recent in-vitro and in-vivo evidence suggests that insulin is the common mechanism regulating the secretion of SHBG and insulin-like growth factor small binding protein (IGFBP-I). IGFBP-1 appears not only to be a carrier for insulin growth factors (IGFs) but also to play an active role in growth processes, independent of growth hormone secretion. We have exam- ined the possible relationship between fasting insulin, SHBG, testosterone, IGF-1, IGFBP-I and fat distribution in 25 extremely obese, menstruating women (mean weight 107 f 3 kg) with normal glucose tolerance. Fat distribu- tion was assessed from measurements of the waist to hip ratio (W/H). The obese women showed an elevated fasting insulin (mean f SEM; 21 +2 pmol/l), a normal IGF-I, but reduced IGFBP-I (14.6f2 pg/l); in I5 women IGFBP-I levels were undetectable by the present assay. In addition, SHBG levels were reduced in the obese women (24f2 nmol/l) but total testosterone values (1.9 f 0.1 nmol/l) were normal. The elevated fasting insulin levels were positively correlated with increasing upper segment obesity as expressed by a rising W/H ratio ( P < 0.01, r2 =0.306) and inversely correlated with SHBG ( P < 0.01, r2 =0.483). Similarly, reduced SHBG values showed an inverse correlation with increasing W/H ratio ( P < 0.001, r2 =0.383). No correlation was found between IGFBP-I and W/H ratio but a strong positive correlation was seen between IGFBP-1 and SHBG (P < 0.001, r2 = 0.466). Furthermore, an equally significant inverse correlation was found between IGFBP-1 and insulin
Correspondence: Dr P. G. Kopelman, Medical Unit, The London Hospital, Whitechapel, London El IBB, UK.
415
416 J . U . Weaver et al.
levels (P<O.OOl, r2=0.474). Testosterone and fasting IGF-1 did not show any correlation with the studied variables. Multivariate analysis suggested that insulin was the strongest factor involved in the regulation of IGFBP-1 levels, whereas the level of SHBG was primarily determined by IGFBP-1 concentra- tion and W/H ratio. We conclude that reduced SHBG and IGFBP-1 found in extreme obesity are inversely correlated to the prevailing hyperinsulinaemia and to increasing upper segment obesity. These findings provide further evidence to support the hypothesis for insulin being an important regulator of both binding proteins, SHBG and IGFBP-1.
Obesity may be characterized by an elevated fasting plasma insulin concentration and an exaggerated insulin response to a glucose load which, in turn, may be correlated to the degree of obesity (Bagdade et al., 1971). The distribution of fat tissue is also important in determining the degree of hyperinsulinaemia with the highest plasma insulin concentra- tions generally being associated with upper body fatness, central obesity (Kalkoff et al., 1983).
We have previously described altered androgen secretion in obese women with reduced sex hormone binding globulin concentrations, SHBG (Kopelman et al., 1980). More recently, others have reported a linear relationship between decreased SHBG values and increasing insulin concentrations in normal peripubertal adolescents and suggested a possible role for insulin in the regulation of SHBG, independent of sex steroid secretion or metabolism (Holly et al., 1989).
Insulin-like growth factors (IGF-I and IGF-2) are peptides with a close structural and functional resemblance to insulin. Unlike insulin the IGFs are present in the circulation largely bound to specific carrier proteins and recent evidence suggests that these proteins may not simply be carrier proteins but actively regulate the cellular actions of IGFs. Two classes of binding proteins have been identified with most of the IGF- 1 being associated in the circulation within a I50 kDa molecular weight complex which is growth hormone dependent (IGFBP-3). In contrast, the other well characterized binding protein, IGFBP- 1, with a molecular weight of 25 kDa, is largely unsaturated and accounts for most of the free IGF-I binding activity in plasma. The plasma concentration of this binding protein, which appears to have an important effect on the action of IGF-1 at the cellular level (Ooi & Herington, 1988), may also be regulated by plasma insulin concentrations (Holly et al., 1988; Suikkari et al., 1988); there is no information presently on IGFBP-I in obesity. We have measured IGFBP-1 levels in obese women and investigated a possible role for insulin in the regulation of SHBG and IGFBP-1 and its relationship to the distribution of fat.
METHODS
Details of the obese women studied are given in Table 1. Body mass index (BMI) was defined as kg/m2 (normal range 20-25). All the subjects were attending the Obesity Clinic at the London Hospital for management of their weight problem and had normal glucose tolerance by WHO criteria. All subjects were studied in the follicular phase of their menstrual cycle and none was receiving any medication at the time of the investigation. The subjects had been eating a weight-maintaining diet for several weeks prior to the study. Blood samples for analysis of insulin, IGF-1, IGFBP-I, testosterone and SHBG were taken at 0900 h after an overnight fast. The study was approved by the London
SHBG, IGFBP-1, insulin in extreme obesity 417
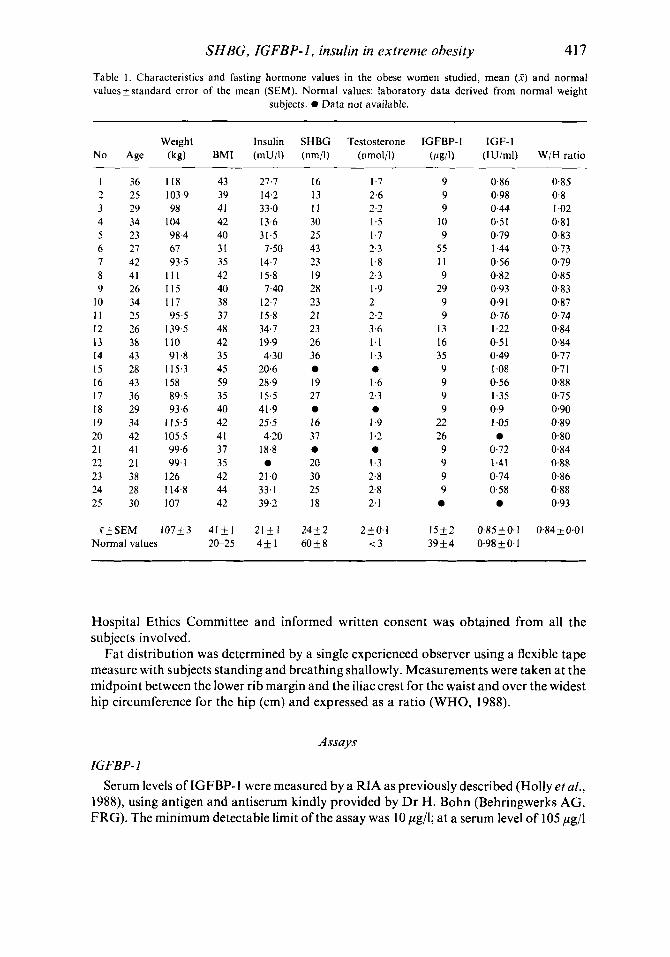
Table 1. Characteristics and fasting hormone values in the obese women studied, mean (2) and normal valuesf standard error of the mean (SEM). Normal values: laboratory data derived from normal weight
subjects. 0 Data not available.
Weight Insulin SHBG Testosterone IGFBP-I IGF-I No Age (kg) BMI (mU/l) (nm/I) (nmol/l) (pgll) (IUjml) W/H ratio
I 2 3 4 5 6 7 8 9
10 I 1 12 13 14 15 16 17 18 19 20 21 22 23 24 25
36 25 29 34 23 27 42 41 26 34 25 26 38 43 28 43 36 29 34 42 41 21 38 28 30
.f & SEM
I18 103.9 98
104 98.4 67 93.5
I l l 115 1 I7 95-5
139.5 110 91.8
115.3 158 89.5 93.6
115.5 105.5 99.6 99. I
I26 114.8 I07
107+3 Normal values
43 39 41 42 40 31 35 42 40 38 37 48 42 35 45 59 35 40 42 41 37 35 42 44 42
4151 20-25
27.7 14.2 33.0 13.6 31.5 7.50
14.7 15.8
12.7 15.8 34.7 19.9
7.40
4.30 20.6 28.9 15.5 41.9 25.5 4.20
18.8 a
21.0 33. I 39.2
2 1 + 1 4$ 1
16 I .7 13 2.6 I 1 2.2 30 1.5 25 I .7 43 2-3 23 1.8 19 2.3 28 1.9 23 2 21 2.2 23 3.6 26 1.1 36 I .3
0 19 1.6 27 2.3 a 0
16 1.9 37 1.2 0 0 20 1.3 30 2.8 25 2.8 18 2. I
2 4 k 2 2+0.I 60$8 < 3
9 9 9
10 9
55 I I 9
29 9 9
13 16 35 9 9 9 9
22 26 9 9 9 9 0
15T2 3 9 k 4
0.86 0.85 0.98 0.8 0.44 1.02 0.51 0.8 1 0.79 0.83 1.44 0.73 0.56 0.79 0.82 0.85 0.93 0.83 0.9 I 0.87 0.76 0.74 I ,22 0.84 0.51 0.84 0.49 0.77 I .08 0.7 1 0.56 0.88 1.35 0.75 0.9 0.90 I .05 0.89 a 0.80
0.72 0.84 1.41 0.88 0.74 0.86 0.58 0.88 a 0.93
0.85 f 0. I 0.98 $ 0. I
0.84 & 0.0 I
Hospital Ethics Committee and informed written consent was obtained from all the subjects involved.
Fat distribution was determined by a single experienced observer using a flexible tape measure with subjects standing and breathing shallowly. Measurements were taken at the midpoint between the lower rib margin and the iliac crest for the waist and over the widest hip circumference for the hip (cm) and expressed as a ratio (WHO, 1988).
Assays
IGFBP-I Serum levels of IGFBP- I were measured by a RIA as previously described (Holly et al.,
1988), using antigen and antiserum kindly provided by Dr H. Bohn (Behringwerks AG, FRG). The minimum detectable limit of the assay was 10 pg/l; at a serum level of 105 pg/l
41 8 J. U. Weauer et at.
the intra-assay coefficient of variation (CV) was 4% and interassay CV was 5.7% at 60 pg/l. The control range in our laboratory drawn from 19 normal weight volunteers is 18-82 /.ig/l.
IGF-I Serum IGF-1 levels were measured by a well characterized RIA using a rabbit
antiserum developed by L. Underwood and J. J. Van Wyk (University of North Carolina, Chapel Hill) and distributed by the Hormone Distribution Program of NIDDK through the National Institute of Health, Bethesda. The assay was standardized against a pool of normal adult human serum which was defined as containing 1.0 U IGF-l/ml; this was equivalent to 159 ng/ml of a highly purified preparation of IGF-1 (Morrell et al., 1986). The control range for IGF-1 in samples drawn from our normal volunteers is 0.61 - 2-25 U/ml.
Insulin Serum immunoreactive insulin was determined by a double antibody RIA, using
Guildhay antisera. The interassay CV was 10% and intra-assay CV 7% with a minimal detectable limit of 3 pmol/l.
SHBG
was 1 1 %. The laboratory control mean -t SEM for women is 60 & 8 nmol/l.
Testosterone Total testosterone level was measured using a double antibody RIA; intra and inter-
assay variability were 1-7 and 3.4% respectively. The control laboratory range for women was less than 3 nmol/l.
SHBG was determined using the method of Iqbal and Johnson (1 977); intra-assay CV
Statistical analysis
Univariate, multivariate regression (backward stepwise regression analysis) were used to analyse any association between the studied variables in the obese group (Kleinbaum et al., 1988). Serum fasting insulin and IGFBP-1 values were both log normally distributed. In the analysis, levels of IGFBP-1 undetected by the present assay were included as a value of 9 pg/l.
RESULTS
The mean fasting insulin level + SEM (21 1 pmol/l) was elevated whereas SHBG (24+ 2 mmol/l) and IGFBP- 1 (1 5.0 f 2 pg/1) values were markedly reduced in the obese women studied. The mean testosterone (2 f 0.1 mmol/l) and IGF- 1 (0.85 f 0. I U/1) levels in the obese women were within the normal range.
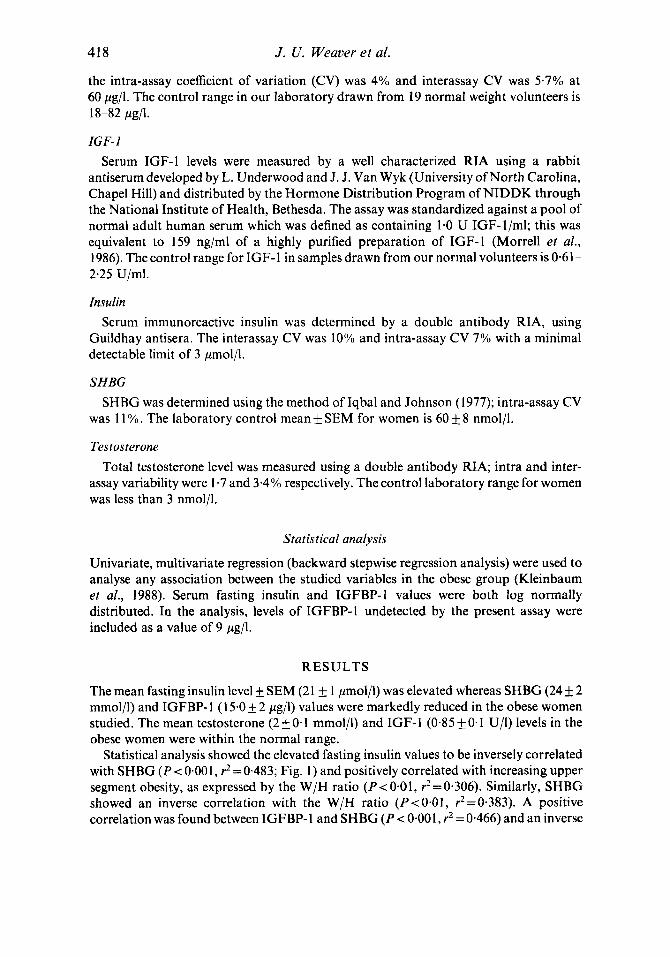
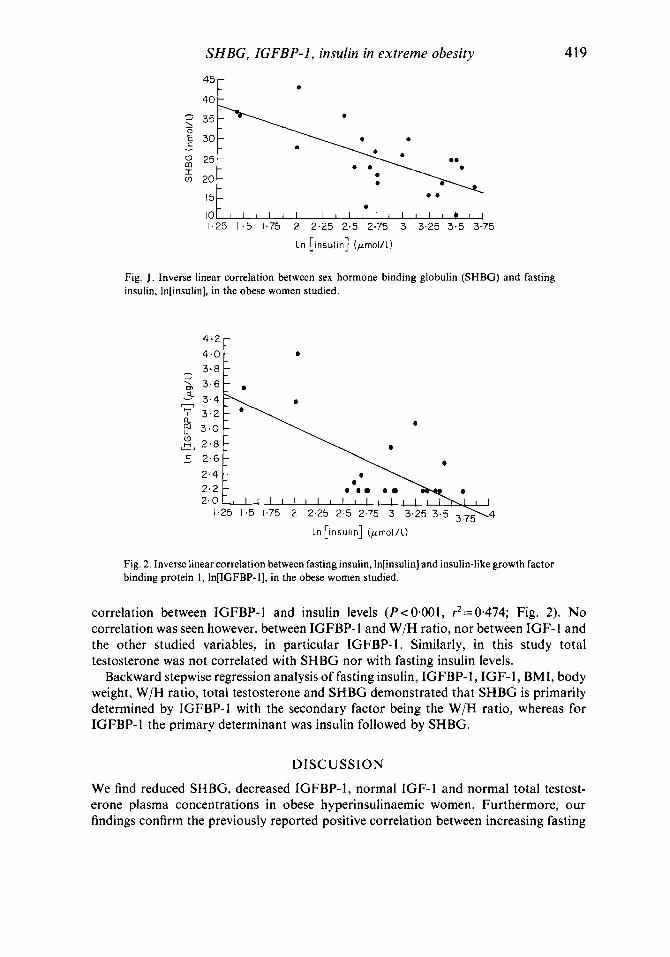
Statistical analysis showed the elevated fasting insulin values to be inversely correlated with SHBG (P < 0.001, r2 = 0,483; Fig. 1) and positively correlated with increasing upper segment obesity, as expressed by the W/H ratio (P<O.Ol, r2=0.306). Similarly, SHBG showed an inverse correlation with the W/H ratio (P<O4l1, r2=0*383). A positive correlation was found between IGFBP- 1 and SHBG ( P < 0.00 1, rz = 0.466) and an inverse
SHBG, IGFBP-1, insulin in extreme obesity
- 0
419
40
Fig. J . Inverse linear correlation between sex hormone binding globulin (SHBG) and fasting insulin, In[insulin], in the obese women studied.
Fig. 2. Inverse linear correlation between fasting insulin, In[insulin] and insulin-like growth factor binding protein I , In(1GFBP-I], in the obese women studied.
correlation between IGFBP-1 and insulin levels (P< 0.001, r2=0.474; Fig. 2). No correlation was seen however, between IGFBP- 1 and W/H ratio, nor between IGF- 1 and the other studied variables, in particular IGFBP-1. Similarly, in this study total testosterone was not correlated with SHBG nor with fasting insulin levels.
Backward stepwise regression analysis of fasting insulin, IGFBP-1, IGF- 1, BMI, body weight, W/H ratio, total testosterone and SHBG demonstrated that SHBG is primarily determined by IGFBP-1 with the secondary factor being the W/H ratio, whereas for IGFBP- 1 the primary determinant was insulin followed by SHBG.
DISCUSSION
We find reduced SHBG, decreased IGFBP-I, normal IGF-1 and normal total testost- erone plasma concentrations in obese hyperinsulinaemic women. Furthermore, our findings confirm the previously reported positive correlation between increasing fasting
420 J . U . Weaver et al.
insulin concentrations and increasing upper body segment obesity (central obesity) and an inverse correlation between fasting insulin and SHBG values. We now additionally report an inverse correlation between fasting insulin and IGFBP- 1 in obese women, which strengthens the evidence for insulin being an important determinant of both IGFBP- 1 and SHBG plasma concentrations. We suspect that the lack of correlation between IGFBP-1 and W/H ratio is explained by fatness per se having a stronger influence on IGFBP-1 levels rather than its distribution. It is of interest that despite the alterations in binding proteins, plasma testosterone and IGF- 1 levels were within the normal laboratory range in the obese women studied.
We have previously described an association between reduced SHBG levels and altered sex steroid secretion in obesity (Kopelman et al., 1980). We considered the decreased SHBG primarily reflected altered androgen production and clearance found in obesity and this, in turn, was influenced by the effect of fat tissue on the peripheral metabolism of androstenedione to oestrone and testosterone. There has been considerable recent interest in the shape of fatness (fat distribution) and several reports confirm that the accumulation of fat in the upper body segment is a better predictor for hyperinsulinaemia, hyperlipidaemia and cardiovascular disease (Kissebah et al., 1982; Kalkoff et al., 1983; Krotkiewski et al., 1983), than either excess body weight or body mass index. In-vitro studies suggest insulin controls SHBG production in human hepatoma cells (Plymate et al., 1988) and our results from hyperinsulinaemic obese women (with normal glucose tolerance) support the hypothesis for a similar role for insulin in oivo. The proposed action of insulin on the hepatic production of SHBG would explain both the lowered SHBG levels found in obese men (which cannot be accounted for by increased androgen production) and the normal testosterone values found in the obese women in the present study.
Insulin-like growth factors constitute an important family of (skeletal) growth regulatory peptides which may play a vital autocrine and paracrine role in cellular growth. IGF-I is growth hormone dependent and is thought to mediate most of the somatotrophic actions of G H in peripheral tissues, but i t is uncertain whether its secretion is altered by obesity per se. Recent reports indicate that circulating IGFBP-1 levels undergo a marked circadian variation unrelated to growth hormone secretion but apparently regulated by the circadian variation of insulin. Holly and colleagues (1988) have shown the levels of IGFBP-1 in insulin-treated diabetics and non-diabetics follow a similar pattern with a nocturnal peak appearing in the early hours of the morning when insulin levels were at their lowest, but disappearing with the morning dose of insulin or postprandial endogenous rise. Such a circadian pattern was independent of changes in growth hormone secretion and not accompanied by any consistent change in IGF-1 levels. Thus the finding of reduced IGFBP-1 unrelated to IGF-I levels in obese hyperinsulinaemic women provides additional evidence for insulin being an important modulator of IGFBP-1.
What possible biological role does circulating IGFBP- 1 play in obesity? Dietary intake influences insulin secretion, IGF-1 and IGFBP-1 levels and it seems likely that previous eating patterns may be one of the explanations for the variable levels of IGF- 1 reported in obesity (Loche et al., 1987). Prolonged fasting results in a fall in IGF-1 whereas refeeding leads to a rapid rise (Clemmons et al., 1981; Davenport et al., 1988). In the present study care was taken to ensure that all the obese subjects had eaten a weight-maintaining diet for several weeks prior to study. Since diet and insulin secretion both influence the secretion

SHBG, IGFBP-I, insulin in extreme obesity 42 1
of IGFBP-I, this carrier protein could serve as an important link between nutritional intake, insulin action and IGF activity at the cellular level and thereby coordinate the growth response to IGF-1 by the cell. It seems possible that biological activity of IGF-I is enhanced at the tissue level in obesity in the presence of reduced IGFBP-1 despite normal plasma immunoreactive IGF-I concentrations. Fine tuning of mechanisms controlling adipocyte growth could be regulated by insulin controlling the levels and distribution of IGFBP- 1 and the latter peptide modulating the actions of IGF in tissues. Our findings suggest that long-term overnutrition and hyperinsulinaemia of obesity alters this mechanism by suppressing IGFBP- I circulating levels.
We conclude that obesity is characterized by reduced levels of circulating IGFBP- 1 and SHBG. I t seems likely that these changes are modulated by insulin whose secretion, in turn, is influenced by body fat distribution.
R E F E R E N C E S
BAGDADE, J.D., BIERMAN. E.L. & PORTE, D. (1971) Influence of obesity on the relationship between insulin and triglyceride level in endogenous hypertrigliceridemia. Diabetes, 20, 664-670.
CLEMMONS, D.R., KLIBANSKI, A., UNDERWOOD, L.E., MCARTHUR, J.W., RIDGEWAY, E.C.. BEITINS, I.Z. & V A N WYK, J.J. (1981) Reduction of plasma immunoreactive Somatomedin C during fasting in humans. Journal of Clinical Endocrinology and Metabolism, 53, 1247-1 250.
DAVENPORT, M.L., SVOBODA, M.E., KOERBER, K.L., VAN WYK, J.J., CLEMMONS, D.R. & UNDERWOOD, L.E. (1988) Serum concentrations of Insulin-like growth factor I1 are not changed by short term fasting and re feeding. Journal of Clinical Endocrinology and Metabolism, 67, 123 1 - 1236.
WASS, J.A.H. (1988) Circadian variation of GH-independent IGF-binding protein in diabetes mellitus and its relation to insulin. A new role for insulin? Clinical Endocrinology, 29, 667-675.
HOLLY. J.M.P., SMITH, C.P., DUNGER, D.B., HOWELL, R.J.S., CHARD, T., PERRY, L.A., SAVAGE, M.O., CIANFARANI, S., REES, L.H. & WASS, J.A.H. (1989) Relationship between the pubertal fall in sex hormone binding globulin and insulin-like growth factor binding protein-I. A synchronized approach to pubertal development? Clinical Endocrinology, 31,277- 284.
IQBAL, M.J. &JOHNSON, M.W. (1977) Study of steroid-protein binding by a novel ‘two-tier’ column employing Cibacron Blue F3G-A-Sepharose 4B. I Sex hormone binding globulin, Journal of Steroid Biochemistry, 8, 977-983.
KALKOFF, R.K., HARTZ, A.H., RUPLEY, D. KISSEBAH, A.H. & KELBER, S. (1983) Relationship of body fat distribution to blood pressure, carbohydrate tolerance and plasma lipids in healthy obese women. Journal qf Laboratory and Clinical Medicine, 102, 62 1-627.
KISSEBAH, A.H., VYDELINGUM, R.M., EVANS, D.J., MURRAY, R., HARTZ, A.J., KALKOFF, K . & ADAMS, P. (1982) Relation of body fat distribution to metabolic complications of obesity. Journal of Clinical Endocrinology and Metabolism. 54,254-260.
KLEINBAUM, D.G., KUPPER, L.L. & MULLER, K.E. (1988) Applied Regression Analysis and other Mullivariable Methods. PWS-Kent Publishing Company, Boston.
KOPELMAN, P.G., PILKINGTON, T.R.E., WHITE, N. & JEFFCOATE, S.L. (1980) Abnormal sex steroid secretion and binding in massively obese women. Cliical Endocrinology, 12, 363-369.
KROTKIEWSKI, M.. BJORNTDRP, P., SJOSTROM, L. & SMITH, U. (1983) Impact of obesity on metabolism in men and women: importance of regional adipose tissue distribution. Journalof Clinical Investigations, 72,1150- 1162.
LOCHE, S., CAPPA, M., BORRELLI, P., FAEDDA, A., CRINO, A,, CELLA, S.G., CORDA, A., MULLER, E.E. & PINTOR, C. (1987) Reduced growth hormone response to growth hormone-releasing hormone in children with simple obesity: evidence for somatomedin-C mediated inhibition. Clinical Endocrinology, 27, 145- 153.
MORRELL, D.J., RAY, K.P., HOLDER, A.T., TAYLOR, A.M., BLOWS, J.A., HILL, D.J., WALLIS, M. & PREECE, M.A. (1986) Somatomedin C insulin-like growth factor I . Simplified purification procedure and biological activities of purified growth factor. Journal of Endocrinofogy, 110, 151-158.
001, G.T. & HERINGTON, A.C. (1988) The biological and structural characterization of specific serum binding proteins for the insulin-like growth factors. Journal sf Endocrinology, 118,7718.
HOLLY, J.M.P., BIDDLECOMBE, R.A., DUNGER, D.B., EDGE, J., AMIEL. S.A., HOWELL, R., CHAD, T., REEs, L.H. &
422 J . U. Weaver et al.
PLYMATE, S.R., MATEJ, L.A., JONES, R.E. & FRIEDL, K.E. (1988) Inhibition of sex hormone-binding globulin production in the human hepatoma (Hep G2) cell line by insulin and prolactin. Journal of Clinical Endocrinology and Metabolism, 67,460-464.
SUIKKARI, A-M., KOIVISTO, V.A., RUTANEN, E-M., YKI-JARVINEN, H., KARONEN, S-L. & SEPPALA, M. (1988) Insulin regulates the serum levels of low molecular weight insulin-like growth factor-binding protein. Journal of Clinical Endocrinology and Metabolism, 66, 266-272.
WHO (1988) Measuring obesity-classification and description of anthropometric data. WHO, Regional Office for Europe, Copenhagen.
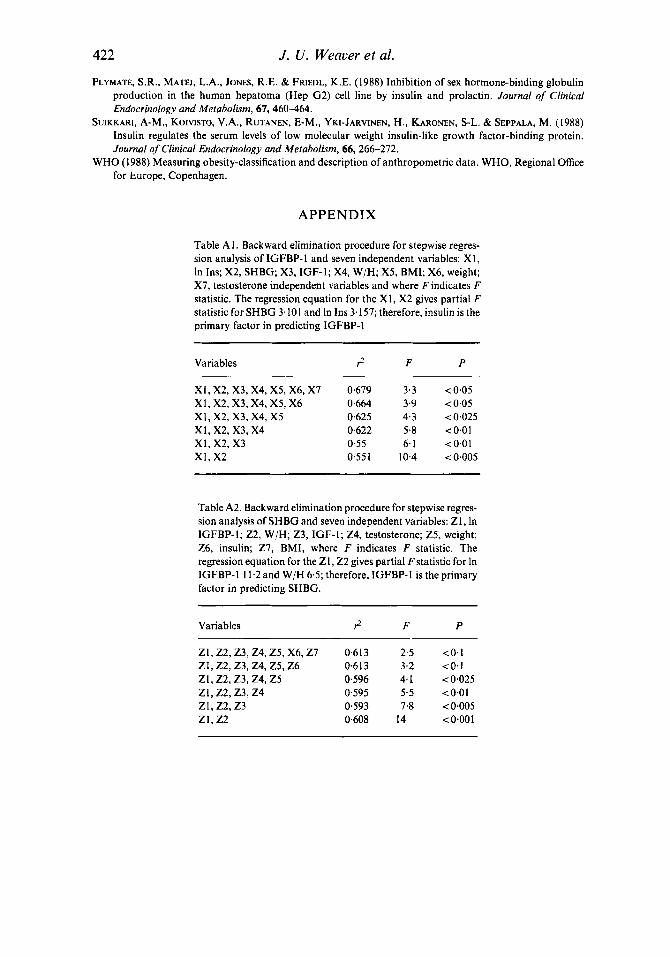
APPENDIX
Table A 1. Backward elimination procedure for stepwise regres- sion analysis of IGFBP-I and seven independent variables: XI, In Ins; X2, SHBG; X3, IGF-1; X4, W/H; X5, BMI; X6, weight; X7, testosterone independent variables and where F indicates F statistic. The regression equation for the XI, X2 gives partial F statistic for SHBG 3.101 and In Ins 3.157; therefore, insulin is the primary factor in predicting IGFBP-I
Variables
~~
rz F P
XI, X2, X3, X4, X5, X6, X7 0.679 3.3 <0.05 XI, X2, X3, X4, X5, X6 0.664 3.9 <0,05 XI, x2 , x3 , x4 , x 5 0,625 4.3 <0.025 XI, x2, x3 , x 4 0.622 5.8 <0.01 XI, x2, x 3 0.55 6.1 <0.01 x1, x 2 0.551 10.4 <0.005
Table A2. Backward elimination procedure for stepwise regres- sion analysis of SHBG and seven independent variables: Z 1, In IGFBP-I; 22, W/H; 23, IGF-I; 24, testosterone; 25, weight; 26, insulin; 27, BMI, where F indicates F statistic. The regression equation for the ZI, 22 gives partial Fstatistic for In IGFBP-I 11.2 and W/H 6.5; therefore, IGFBP-I is the primary factor in predicting SHBG.
Variables rz F P
ZI, 22 ,23 ,24 ,Z5, X6,Zl 0.613 2.5 <0.1 21, 22,23 ,24 ,Z5,26 0.6 13 3.2 <O-1 z I , z2 ,23 ,24 , z5 0,596 4.1 <0.025 ZI, z 2 , 2 3 , z 4 0.595 5.5 <0.01 21, z 2 , z 3 0.593 7.8 <0.005 ZI, 22 0.608 14 <0.001