defining bipolar mood states with quantitative measurement of inhibition/activation and emotional...
TRANSCRIPT

Journal of Affective Disorders 127 (2010) 300–304
Contents lists available at ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad
Brief report
Defining bipolar mood states with quantitative measurement of inhibition/activation and emotional reactivity
Chantal Henry a,b,c,d,⁎, Katia M'Bailara e,f, Jean-Pierre Lépine d,g,h,i,Mohamed Lajnef a, Marion Leboyer a,b,c,d
a INSERM, U 995, IMRB, département de Génétique, Créteil, F-94000, Franceb Université Paris 12, Faculté de Médecine, IFR10, Créteil, F-94000, Francec AP-HP, Hôpital Henri Mondor-Albert Chenevier, Pôle de Psychiatrie, Créteil, F-94000, Franced Fondation FondaMental, Fondation de coopération scientifique, Francee Hôpital Charles Perrens, Bordeaux, Francef Université de Bordeaux 2, Franceg Service de psychiatrie d'adultes, groupe hospitalier Lariboisière-Fernand-Widal, AP-HP, 75010 Paris, Franceh Inserm U705, 75010 Paris, Francei Neuropsychopharmacologie des addictions, CNRS UMR 7157, faculté de pharmacie, université Paris-Descartes et université Paris-Diderot, France
a r t i c l e i n f o
⁎ Corresponding author. Pôle de psychiatrie du CHU CrE-mail address: [email protected] (C. Henry
0165-0327/$ – see front matter © 2010 Elsevier B.V.doi:10.1016/j.jad.2010.04.028
a b s t r a c t
Article history:Received 16 December 2009Received in revised form 27 April 2010Accepted 27 April 2010Available online 9 June 2010
Objectives: Mood state heterogeneity in bipolar disorder leads to confusion in diagnosis andtherapeutic strategies. Recently, the Systematic Treatment Enhancement Program for BipolarDisorder (STEP-BD) showed that two-thirds of bipolar-depressedpatients had concomitantmanicsymptoms, these characteristics being linked to amore severe formof bipolar disorder.Moreover,manic symptoms occurring during bipolar depression are associatedwithmood switches inducedby antidepressant. It is thus important to best characterize mood episodes with mixed features inorder to improve our understanding of the etiopathology and to choose the most appropriatetreatment. As dimensional approach can better describe phenomena that are distributedcontinuously without clear boundaries, we used the MATHYS scale, constructed on adimensional approach. The aim of the study is to determine whether two dimensions(activation/inhibition and emotional reactivity) improve assessment of bipolar states in whichboth manic and depressive symptoms are associated.Methods: We included 189 bipolar patients and 90 controls. Bipolar patients were distinguishedbetween thosewith amajor depressive episodewithoutmanic symptoms, amajor depressive episodewith manic symptoms, a mixed state and a manic state. The MATHYS scale provides a total score,quantifying an inhibition/activationprocess, anda score for emotional reactivity (intensityof emotions).Results: We demonstrated that there is a continuum ranging from inhibition to activation(respectively from major depressive episodes without manic symptoms to manic states), with agradual increase in the severity of the activation. Regarding emotional reactivity, results are quietdifferent since only major depressive episodes without manic symptoms are characterized byemotional hypo-reactivity while major depressive episodes with manic symptoms, manic andmixed states exhibited emotional hyper-reactivity.Conclusions: The MATHYS scale, providing a score for inhibition/activation process and a score foremotional reactivity, is clearly useful to distinguish bipolar depressive episodes without manicsymptoms from those with manic symptoms. This last type of depression appears to belong to abroad spectrumofmixed state. To go furtherwe need to explore if these two types of depression areunderlined by different mechanisms and what is the most appropriate treatment for each of them.
© 2010 Elsevier B.V. All rights reserved.
Keywords:Bipolar disorderDepressive stateMixed stateDSM-VEmotional reactivityDimensional approachMATHYS Scale
éteil, Hôpital A. Chenevier, 40 rue deMesly 94000 Créteil, France. Tel.: +33 1 49 81 32 31; fax+33 1 49 81 30 99).
All rights reserved.
.

301C. Henry et al. / Journal of Affective Disorders 127 (2010) 300–304
1. Introduction
Mood state heterogeneity in bipolar disorders has led toconfusion in diagnosis and therapeutic strategies. Contraryto Kraepelin (Kraepelin, 1899), who described six mixedstates, DSM-IV (Diagnostic and Statistical Manual of MentalDisorders, 1994) narrowly defines mixed episodes on thebasis of full manic and full depressive syndromes beingpresent at the same time, for at least one week, in onlybipolar I patients. However, recent studies highlight thediversity of mood states in which both manic and depressivesymptoms are associated. Koukopoulos was the first to drawattention to the need to recognize manic or hypomanicfeatures that may arise in conjunction with bipolar depres-sive episodes (Koukopoulos and Koukopoulos, 1992).Benazzi (Benazzi, 2002) suggested defining “depressivemixed states” by the presence of three manic symptomsduring bipolar II depressive episodes. Based on a broaderICD-10 (WHO, 1993) definition of amixed episode, Suppes etal (Suppes et al., 2005) described “mixed hypomania” forepisodes simultaneously presenting hypomanic and depres-sive features. More recently, the Systematic TreatmentEnhancement Program for Bipolar Disorder (STEP-BD) hasshown that two-thirds of bipolar-depressed patients hadconcomitant manic symptoms (Goldberg et al., 2009). In theSTEP-BD study, patients with mixed features had moresevere characteristics, such as illness onset at an early age,more bipolar I subtype, more rapid cycling in the past year,and a more frequent history of suicide attempts. Moreover,Frye et al. (Frye et al., 2009) showed that minimal manicsymptoms at baseline coexisting with an otherwise fullsyndromal form of bipolar depression are associated withantidepressant treatment-emergent mania or hypomania. Abetter assessment of the differences between pure andmixed bipolar depression is of a great clinical significance, asit may offer potential indicators of short-term prognosis andmay help in the prescription of psychotropic drugs.
On the other hand, Kraemer et al. (2004) have defined adimensional approach, in which clinical presentations areclassified based on quantitative attributes rather than theassignment to categories. It should work best if describingphenomena that are distributed continuously without clearboundaries. Thus, a dimensional approach appears to beappropriate for defining the spectrum of mixed episodes. Toapply this concept to mixed states, we built and validated theMATHYS (Multidimensional Assessment of Thymic States)scale to define mood states as a function of a dimensionalapproach assessing symptoms on their quantitative aspects(acceleration/retardation; increase/decrease) (more detailsin the Method section) (Henry et al., 2008). This scaleprovided a total score quantifying an overall level ofinhibition/activation and a score of emotional reactivity(hypo versus hyper). We have previously shown that(Henry et al., 2003) emotional hyper-reactivity (feelingemotions with a higher intensity than usual) characterizesmixed and manic states.
Weaimed1) todeterminewhether onlyone scale (MATHYS)could be used to assess all bipolar mood episodes, and 2) todetermine whether two dimensions (activation/inhibition;emotional reactivity) can help defining bipolar states in whichboth manic and depressive symptoms are associated.
2. Method
2.1. Participants
Participants included control subjects and bipolar patients.Control subjects were recruited through advertisements inshopping areas and in sportive associations. Bipolar patientswere in and outpatients recruited in a setting specialized inbipolar consultations or patients hospitalized in a departmentcorresponding to a catchment area in Bordeaux (France). Allpatients had bipolar disorder, type I or II, and at the time ofentry met the DSM-IV criteria for a full episode (depressed,manic or mixed). All subjects gave written informed consent,and the protocol was approved by the local ethics committee.
2.2. Assessments
All subjects (controls and bipolar patients) were assessedusing the mood section of the French version of DIGS(Diagnostic Interview for Genetic studies), a structuredinterview providing DSM-IV diagnosis criteria (Nurberger etal., 1994). Severity of depressive and manic symptoms wasfurther rated using theMontgomery–AsbergDepression RatingScale (MADRS) (Montgomery and Asberg, 1979) and the Bechand Rafaelsen Manic scale (MAS) (Bech et al., 1978).
As there was no clinical tool to assess bipolar mood statesdimensionally, we developed and validated a dimensionalself-rated scale: MATHYS (Multidimensional Assessment ofThymic States). This scale was built a priori, with fivequantitative dimensions, which vary from inhibition toactivation. The goal was to generate a total score indicativeof the overall level of inhibition/activation. Thus, classicdimensions, such as cognition, motivation, psychomotoragitation or retardation and sensory perception, wereassessed quantitatively (i.e., racing thoughts or subjectivelyfeeling that their thoughts occur slower, physical agitation orretardation, and increase or decrease in sense perception)(Example: My brain never stops/My brain seems to befunctioning in slow motion). We applied a similar conceptto evaluate emotion, focusing only on the quantitative aspect(i.e., whether the patient felt emotion with normal intensity,greater intensity, or less intensity) (Example: My emotionsare very intense/My emotions are attenuated).
The concept behind this scale involved exploring allbipolar mood states on a continuum using a score forinhibition/activation and exploring emotional reactivityrather than tonality of affect (euphoria/sadness). Manic andmixed states were better characterized by emotional hyper-reactivity, suggesting that all patients felt emotions with anunusual intensity, irrespective of the emotion (sadness,irritability, euphoria, and anxiety) (Henry et al., 2003). Thescale is composed of a visual analog scale comprising 20 itemsrelated to how the individual feels during the previous week.Statistical analyses demonstrated a good validity for thisscale, and a good internal consistency (Cronbach's alphacoefficient=0.95). The MATHYS scale is moderately corre-lated of both the MADRS scale (depressive score; r=−0.45)and the MAS scale (manic score; r=0.56).
This scale gives a total score assessing the activation/inhibition level and a score for emotional reactivity (hyper/hypo-reactivity) (the English version of the scale can be
302 C. Henry et al. / Journal of Affective Disorders 127 (2010) 300–304
found by following this link: [http://www.biomedcentral.com/content/supplementary/1471-244X-8-82-S1.doc](Henry et al., 2008).
2.3. Statistical analyses
Groups (bipolar mood episodes and control) were com-pared based on MATHYS, MADRS and MAS scales. Statisticalmethods consisted of Chi-square tests for comparisons ofcategorical variables (sex) andanalysis of variance (ANOVA) forcontinuous variables: [MATHYS (total score and score ofemotional reactivity), age, MADRS, MAS]. The score foremotional reactivity was obtained by adding items 3, 7, 10and 18 (define by a principal component analysis, Henry et al.,2008). Post-hoc analysis using Tukey's procedure was used tocalculate mean differences and to determine which meanswere significantly different from one another. Finally, weanalyzed whether there was a trend in the mean differencesbetween bipolar mood episodes. Testing was 2-sided, with asignificance level of 5%. Two-sided p values of 0.05 wereconsidered statistically significant. We used SAS software(version 9.1; SAS Institute) for the analysis.
3. Results
3.1. Characteristics of the groups
The total sample of 279 subjects (189 bipolar patients and90 controls) was composed of 92 (33%) men and 187 (67%)women, with a mean age at interview of 39.3 (±13.1) [14–72]years. There is no difference between control subjects andbipolar patients for age and gender. A total of 54.9% of patients(n=96) met the criteria for bipolar type I disorder. Accordingto DSM-IV criteria, 51 patients (18.3%) had a major depressiveepisode without manic symptoms, 21 (7.5%) had mixedepisodes, and 54 (19.5%) had hypomanic or manic episodes.As defined by STEP-BD (Goldberg et al., 2009), 63 (22.6%)patients presented a major depressive episode associated withmanic symptoms, but these patients did not fulfil the DSM-IVcriteria for a mixed episode.
As expected, all groups had different MADRS scores(F=152.4; ddl=4; pb0.0001). The highest score wasobserved for patients in a major depressive episode withoutmanic symptoms and manic patients exhibited the lowestscore. All groups had also different scores on the manic scale(MAS) (F=142.9; ddl=4; pb0.0001). The highest score wasfound in the manic group 17.6 (±6.8) while the group with amajor depressive episode exhibited 1.3 (±2.1) and patients
Table 1Socio-demographic characteristics of subjects andmean scores on the depressive scathe total score and the score for emotional reactivity.
Controls MDE MDE‡
N(%) 90 (32.3) 51 (18.3) 63 (22.6)Sex(%) 31 (34.4) 18 (35.3) 19 (30.2)Age[M(SD)] 37.8(14.2) 42.1 (13) 41.2 (11.1)Madrs[M(SD)] 0.31 (1.5) 25.3 (9.8) 15.3 (6.4)Mas[(M(SD)] 0.2 (0.6) 1.3 (2.1) 7.6 (4.3)MATHYS total[M(SD)] 104.5(8.4) 58.6 (27.0) 111.1 (24.1)Emotional reactivity [M(SD)] 21.7 (2.6) 13.9 (10.3) 31.2 (7.5)
with a major depressive episode associated with manicsymptoms had a mean score at 7.6 (±4.3).
3.2. Dimensional characterization
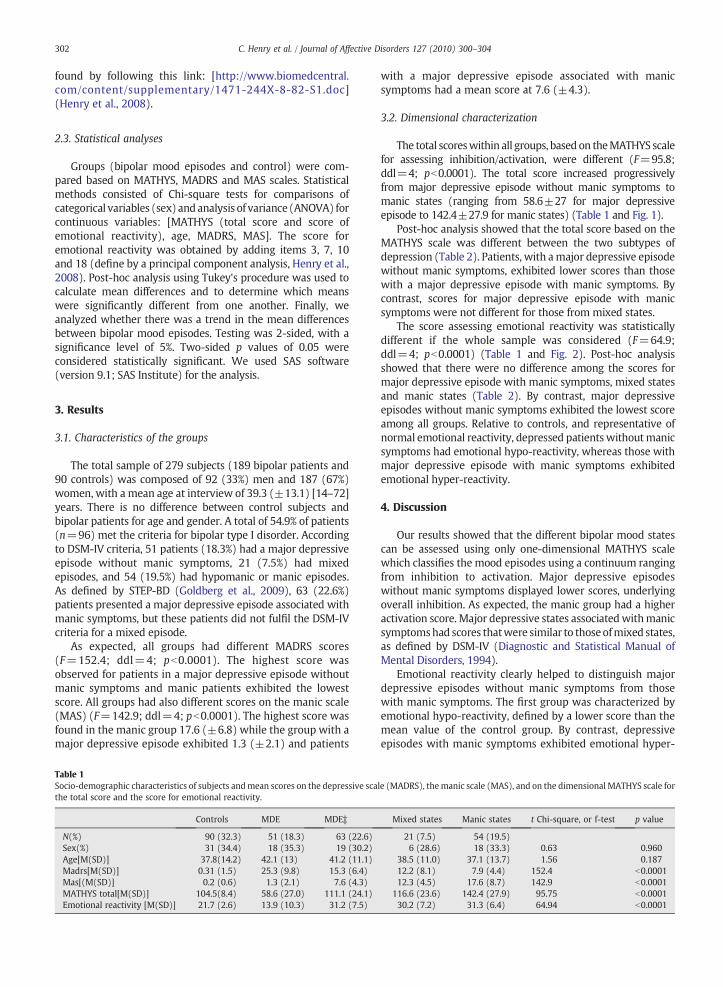
The total scoreswithin all groups, based on theMATHYS scalefor assessing inhibition/activation, were different (F=95.8;ddl=4; pb0.0001). The total score increased progressivelyfrom major depressive episode without manic symptoms tomanic states (ranging from 58.6±27 for major depressiveepisode to 142.4±27.9 for manic states) (Table 1 and Fig. 1).
Post-hoc analysis showed that the total score based on theMATHYS scale was different between the two subtypes ofdepression (Table 2). Patients, with amajor depressive episodewithout manic symptoms, exhibited lower scores than thosewith a major depressive episode with manic symptoms. Bycontrast, scores for major depressive episode with manicsymptoms were not different for those from mixed states.
The score assessing emotional reactivity was statisticallydifferent if the whole sample was considered (F=64.9;ddl=4; pb0.0001) (Table 1 and Fig. 2). Post-hoc analysisshowed that there were no difference among the scores formajor depressive episode with manic symptoms, mixed statesand manic states (Table 2). By contrast, major depressiveepisodes without manic symptoms exhibited the lowest scoreamong all groups. Relative to controls, and representative ofnormal emotional reactivity, depressed patients withoutmanicsymptoms had emotional hypo-reactivity, whereas those withmajor depressive episode with manic symptoms exhibitedemotional hyper-reactivity.
4. Discussion
Our results showed that the different bipolar mood statescan be assessed using only one-dimensional MATHYS scalewhich classifies the mood episodes using a continuum rangingfrom inhibition to activation. Major depressive episodeswithout manic symptoms displayed lower scores, underlyingoverall inhibition. As expected, the manic group had a higheractivation score. Major depressive states associatedwithmanicsymptomshad scores thatwere similar to thoseofmixed states,as defined by DSM-IV (Diagnostic and Statistical Manual ofMental Disorders, 1994).
Emotional reactivity clearly helped to distinguish majordepressive episodes without manic symptoms from thosewith manic symptoms. The first group was characterized byemotional hypo-reactivity, defined by a lower score than themean value of the control group. By contrast, depressiveepisodes with manic symptoms exhibited emotional hyper-
le (MADRS), themanic scale (MAS), and on the dimensional MATHYS scale for
Mixed states Manic states t Chi-square, or f-test p value
21 (7.5) 54 (19.5)6 (28.6) 18 (33.3) 0.63 0.960
38.5 (11.0) 37.1 (13.7) 1.56 0.18712.2 (8.1) 7.9 (4.4) 152.4 b0.000112.3 (4.5) 17.6 (8.7) 142.9 b0.0001
116.6 (23.6) 142.4 (27.9) 95.75 b0.000130.2 (7.2) 31.3 (6.4) 64.94 b0.0001
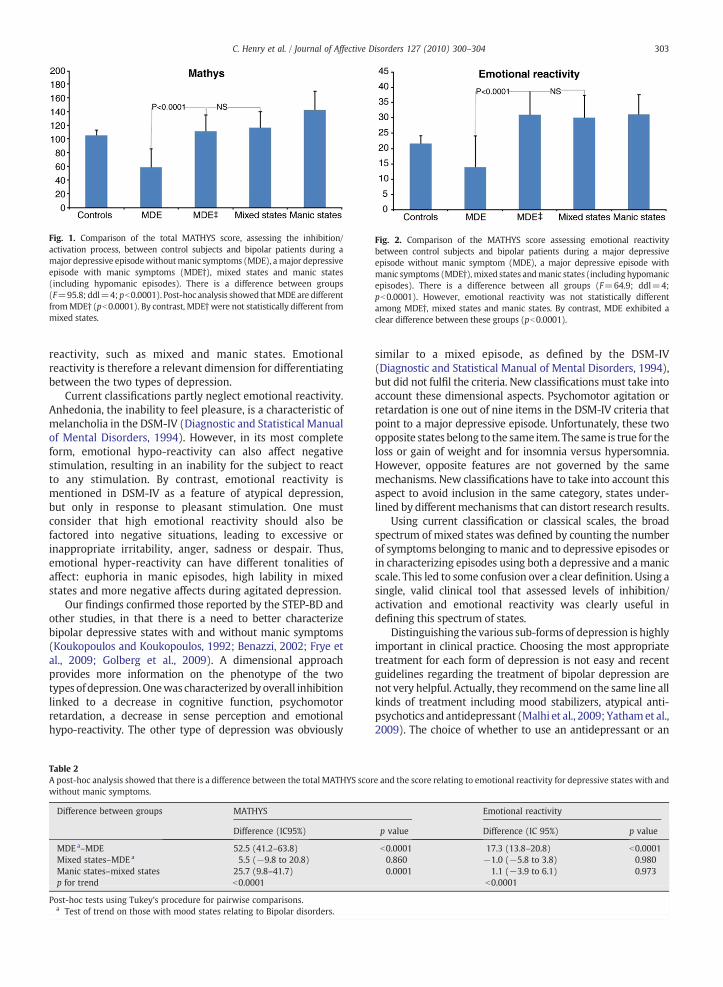
Fig. 1. Comparison of the total MATHYS score, assessing the inhibition/activation process, between control subjects and bipolar patients during amajor depressive episodewithoutmanic symptoms (MDE), amajor depressiveepisode with manic symptoms (MDE†), mixed states and manic states(including hypomanic episodes). There is a difference between groups(F=95.8; ddl=4; pb0.0001). Post-hoc analysis showed thatMDE are differentfromMDE† (pb0.0001). By contrast, MDE†were not statistically different frommixed states.
Fig. 2. Comparison of the MATHYS score assessing emotional reactivitybetween control subjects and bipolar patients during a major depressiveepisode without manic symptom (MDE), a major depressive episode withmanic symptoms (MDE†),mixed states andmanic states (including hypomanicepisodes). There is a difference between all groups (F=64.9; ddl=4;pb0.0001). However, emotional reactivity was not statistically differentamong MDE†, mixed states and manic states. By contrast, MDE exhibited aclear difference between these groups (pb0.0001).
303C. Henry et al. / Journal of Affective Disorders 127 (2010) 300–304
reactivity, such as mixed and manic states. Emotionalreactivity is therefore a relevant dimension for differentiatingbetween the two types of depression.
Current classifications partly neglect emotional reactivity.Anhedonia, the inability to feel pleasure, is a characteristic ofmelancholia in the DSM-IV (Diagnostic and Statistical Manualof Mental Disorders, 1994). However, in its most completeform, emotional hypo-reactivity can also affect negativestimulation, resulting in an inability for the subject to reactto any stimulation. By contrast, emotional reactivity ismentioned in DSM-IV as a feature of atypical depression,but only in response to pleasant stimulation. One mustconsider that high emotional reactivity should also befactored into negative situations, leading to excessive orinappropriate irritability, anger, sadness or despair. Thus,emotional hyper-reactivity can have different tonalities ofaffect: euphoria in manic episodes, high lability in mixedstates and more negative affects during agitated depression.
Our findings confirmed those reported by the STEP-BD andother studies, in that there is a need to better characterizebipolar depressive states with and without manic symptoms(Koukopoulos and Koukopoulos, 1992; Benazzi, 2002; Frye etal., 2009; Golberg et al., 2009). A dimensional approachprovides more information on the phenotype of the twotypes of depression.Onewas characterized byoverall inhibitionlinked to a decrease in cognitive function, psychomotorretardation, a decrease in sense perception and emotionalhypo-reactivity. The other type of depression was obviously
Table 2A post-hoc analysis showed that there is a difference between the total MATHYS scorwithout manic symptoms.
Difference between groups MATHYS
Difference (IC95%)
MDE a–MDE 52.5 (41.2–63.8)Mixed states–MDE a 5.5 (−9.8 to 20.8)Manic states–mixed states 25.7 (9.8–41.7)p for trend b0.0001
Post-hoc tests using Tukey's procedure for pairwise comparisons.a Test of trend on those with mood states relating to Bipolar disorders.
similar to a mixed episode, as defined by the DSM-IV(Diagnostic and Statistical Manual of Mental Disorders, 1994),but did not fulfil the criteria. New classifications must take intoaccount these dimensional aspects. Psychomotor agitation orretardation is one out of nine items in the DSM-IV criteria thatpoint to a major depressive episode. Unfortunately, these twoopposite states belong to the same item. The same is true for theloss or gain of weight and for insomnia versus hypersomnia.However, opposite features are not governed by the samemechanisms. New classifications have to take into account thisaspect to avoid inclusion in the same category, states under-lined by different mechanisms that can distort research results.
Using current classification or classical scales, the broadspectrum of mixed states was defined by counting the numberof symptoms belonging tomanic and to depressive episodes orin characterizing episodes using both a depressive and a manicscale. This led to some confusion over a clear definition. Using asingle, valid clinical tool that assessed levels of inhibition/activation and emotional reactivity was clearly useful indefining this spectrum of states.
Distinguishing the various sub-forms of depression is highlyimportant in clinical practice. Choosing the most appropriatetreatment for each form of depression is not easy and recentguidelines regarding the treatment of bipolar depression arenot very helpful. Actually, they recommend on the same line allkinds of treatment including mood stabilizers, atypical anti-psychotics and antidepressant (Malhi et al., 2009; Yathamet al.,2009). The choice of whether to use an antidepressant or an
e and the score relating to emotional reactivity for depressive states with and
Emotional reactivity
p value Difference (IC 95%) p value
b0.0001 17.3 (13.8–20.8) b0.00010.860 −1.0 (−5.8 to 3.8) 0.9800.0001 1.1 (−3.9 to 6.1) 0.973
b0.0001

304 C. Henry et al. / Journal of Affective Disorders 127 (2010) 300–304
atypical antipsychotic in bipolar depression would be facilitat-ed by distinguishing inhibited/emotional hypo reactive depres-sion from activated/emotional hyper reactive depression.
This study is the first one using a new dimensional scalethat compares all bipolar mood states as a function of a levelof activation/inhibition and emotional reactivity. To gofurther we need to perform a follow up in order to assess ifrecurrences of mood states and more particularly depressiveepisodes exhibit the same characteristics in a same patient.Moreover, further studies are needed to find biomarkers thatcharacterize each group.
Role of funding sourceThis research was supported by grants from the Institut National de la
Santé et de la Recherche Médicale (INSERM), the Programme Hospitalier deRecherche Clinique (PHRC) and by the French Ministry of Research (RTRSSanté Mentale) and attributed to the French national science foundationFondaMental (Journal official de la République française, 17 juin 2007).
Conflict of interestAuthors have no actual or potential conflict of interest including financial,
personal or other relationshipswith other people or organizationswithin threeyears of beginning the work submitted that could inappropriately influence, orbe perceived to influence, their work.
AcknowledgmentWe thank M.J. Pereira Gomes for technical assistance.
References
Bech, P., Rafaelsen, O.J., Kramp, P., Bolwig, T.G., 1978. The mania rating scale:scale construction and inter-observer agreement. Neuropharmacology17, 430–431.
Benazzi, F., 2002. Depressive mixed state frequency: age/gender effects.Psychiatry Clin. Neurosci. 56, 537–543.
Diagnostic and Statistical Manual of Mental Disorders, 1994. Fourth Edition.American Psychiatric Association, Washington, DC.
Frye, M.A., Helleman, G., McElroy, S.L., Altshuler, L.L., Black, D.O., Keck Jr, P.E.,Nolen, W.A., Kupka, R., Leverich, G.S., Grunze, H., Mintz, J., Post, R.M.,
Suppes, T., 2009. Correlates of treatment-emergent mania associated withantidepressant treatment in bipolar depression. Am. J. Psychiatry 166,164–172.
Goldberg, J.F., Perlis, R.H., Bowden, C.L., Thase,M.E.,Miklowitz, D.J.,Marangell, L.B.,Calabrese, J.R., Nierenberg, A.A., Sachs, G.S., 2009. Manic symptoms duringdepressive episodes in 1, 380 patients with bipolar disorder: findings fromthe STEP-BD. Am. J. Psychiatry 166, 173–181.
Henry, C., Swendsen, J., Van Den Bulke, D., Sorbara, F., Leboyer, M., 2003.Emotional hyper-reactivity as the fundamental mood characteristic ofmanic and mixed states. Eur. Psychiatry 18, 124–128.
Henry, C., M'Baïlara, K., Mathieu, F., Poinsot, R., Falissard, B., 2008. Constructionand validation of a dimensional scale exploring mood disorders: MAThyS(Multidimensional Assessment of Thymic States). BMC Psychitry 8, 82.
Koukopoulos, A., Koukopoulos, A., 1999. Agitated depression as a mixed stateand the problem of melancholia. Psychiatr. Clin. N. Am. 22, 547–564.
Kraemer, H.C., Noda, A., O'Hara, R., 2004. Categorical versus dimensionalapproaches to diagnosis: methodological challenges. J. Psychiatr. Res. 38,17–25.
Kraepelin, E., 1899. Manic Depressive Insanity and Paranoia. E.S. Livingston,Edinburgh.
Malhi, G.S., Adams, D., Lampe, L., Paton, M., O'Connor, N., Newton, L.A., Walter, G.,Taylor, A., Porter, R., Mulder, R.T., Berk, M., 2009. Northern Sydney CentralCoastMental HealthDrug&Alcohol; NSWHealth Clinical Redesign Program;CADE Clinic, University of Sydney. Clinical practice recommendations forbipolar disorder. Acta Psychiatr. Scand. Suppl. 439, 27–46.
Montgomery, S., Asberg, A., 1979. A new depression scale designed to besensitive to change. Br. J. Psychiatry 134, 382–389.
Nurnberger Jr, J.I., Blehar,M.C., Kaufmann, C.A., et al., 1994. Diagnostic interviewfor genetics studies. Rationale, unique features, and training. NIMHGenetics Initiative. Arch. Gen. Psychiatry 51, 849–859 discussion 863-4.
Suppes, T., Mintz, J., McElroy, S.L., et al., 2005. Mixed hypomania in 908 patientswith bipolar disorder evaluated prospectively in the Stanley FoundationBipolar Treatment Network: a sex-specific phenomenon. Arch. Gen.Psychiatry 62, 1089–1096.
WHO., 1993. The ICD-10 Classification of Mental and Behavioural Disorders.Diagnostic Criteria for Research. WHO, Geneva.
Yatham, L.N., Kennedy, S.H., Schaffer, A., Parikh, S.V., Beaulieu, S., O'Donovan, C.,MacQueen, G., McIntyre, R.S., Sharma, V., Ravindran, A., Young, L.T., Young,A.H., Alda, M., Milev, R., Vieta, E., Calabrese, J.R., Berk, M., Ha, K., Kapczinski,F., 2009. Canadian Network for Mood and Anxiety Treatments (CANMAT)and International Society for Bipolar Disorders (ISBD) collaborative updateof CANMAT guidelines for the management of patients with bipolardisorder: update 2009. Bipolar Disord. 11, 225–255.