defining moments - vicki c. walker, tech writer & editor
TRANSCRIPT
D e f i n i n g M o M e n t s 20 Years of Making CFS History
Commemorating the past…The CFIDS Association of America is pleased to bring you this special magazine, which traces the journey of the CFS community and the Association through 20 years of victories and setbacks, challenges and opportunities, turmoil and hope. This journey has been filled with moments that have defined the present—and that will
help shape the future—of CFS research, advocacy, education and awareness worldwide.
We hope you enjoy this magazine, and that reflecting on past defining moments can help empower us all to create future defining moments for the CFS cause.
Defining Moments is a companion piece to the Science & Research of CFS, a special 64-page issue of the CFIDS Chronicle that covers significant research findings over the past two decades and new areas of study from around the world. This popular 2006 publication—a one-of-a-kind resource for the CFS community, health care professionals, public policy makers and the community at large—is offered in conjunction with the publication of the second magazine in the set.
D e f i n i n g M o M e n t s
Please act now!
MAKE A DONATION to help make CFS history! The progress made over the past 20 years wouldn’t have been possible without the philanthropic support of thousands of supporters. To sustain that progress and propel the CFS cause forward, we need your help.
Please consider: a gift to the CFIDS Association to support the million-dollar research initiative $ a $20 gift to help commemorate the 20th anniversary $ 20
ORDER Defining Moments and/or the Science & Research of CFS: @ $15 each ($20 for 2 copies of any combination of the 2 magazines; includes shipping and handling)
Special discount offer: Want additional copies of this magazine, or copies of the Science & Research of CFS? To commemorate the past 20 years, order 2 or more magazines (1 of each, or 2 copies of either publication) for $10 each. Call the Resource Line at 704-365-2343 for discounts on orders of 10 or more.
Look for this envelope inside.Instructions: Use the enclosed envelope to make a charitable donation or order extra copies of the companion magazines, Defining Moments: 20 Years of Making CFS History and the Science & Research of CFS.
Simply mark the appropriate box, enclose your check or credit card information and return by mail.
Proceeds support the CFIDS Association of America.
The CFIDS Association of America PO Box 220398
Charlotte, NC 28222-0398 www.cfids.org
704-365-2343
Supporting the future…With its education and public policy programs, the CFIDS Association of America has kept CFS in the spotlight for the past two decades, fostering scientific progress in understanding this complex and disabling condition. As we mark our 20-year milestone, the Association is in a unique position to accelerate the pace of progress and to channel more resources into closing the gap between knowledge about CFS and meaningful improvements in diagnosis and care.
To fuel an expanded research program, the CFIDS Association has launched a campaign to raise $1 million in 2008 for new research projects—the most ambitious campaign ever for privately funded CFS research.
Over the next year, the Association will increase funding for results-oriented research grants, host symposia to explore important scientific frontiers, and actively recruit fresh talent and build new collaborations to intensify the study of CFS.
The success of this research initiative will depend on an infusion of support from donors like you. You can make this campaign a defining moment for the entire CFS community. With your gift, you can help make CFS history.
About CFSChronic fatigue syndrome (CFS), also known as chronic fatigue and immune dysfunction syndrome (CFIDS), is a complex chronic illness that results in a constellation of debilitating symptoms, including incapacitating fatigue (experienced as profound exhaustion and extremely poor stamina), sleep difficulties, and problems with concentration and short-term memory. It’s also accompanied by flu-like symptoms, pain in the joints and muscles, tender lymph nodes, sore throat and headaches. A distinctive characteristic of the illness is postexertional malaise, a worsening of symptoms following physical or mental exertion that can require an extended recovery time.
CFS can be challenging for health care professionals to diagnose and treat—and equally chal-lenging for patients and their families to endure. Scientists still don’t know what causes CFS, and there isn’t a cure yet. However, significant progress has been made in recent years by researchers and the medical community in unraveling the mysteries of this illness. This progress has led to a greater understanding of how CFS affects the body, but current treatments are still aimed at symptom relief and improved function, and there is a critical need to develop more effective treatments.
CFS strikes people of all age, ethnic and socioeconomic groups. Research indicates that between one and four million Americans have CFS, but less than 20 percent have been diagnosed. The low rate of diagnosis shows a need for increased understanding of CFS among individuals experienc-ing symptoms of the illness, the general public and health care professionals.
About the CFIDS Association of AmericaThe CFIDS Association of America is the largest and most active charitable organization dedicated to conquering CFS. Since this organization was founded in 1987, the Association has invested more than $25 million in initiatives to bring an end to the pain, disability and suffering caused by this illness.
We are committed to providing credible, up-to-date information for patients and their caregivers, the general public and health care professionals. We have a variety of available resources. For more information about any of the resources mentioned in this publication, please contact us or visit one of the web pages listed below.
Resource Line ......................................... 704-365-2343
Fax....................................................... 704-365-9755
Our Website ......................................... www.cfids.org
Public Awareness Campaign Website ....... www.cfids.org/cfs
Donating to the CFIDS Association ........... www.cfids.org/support/default.asp
The CFIDS Chronicle ............................... www.cfids.org/archives/chronicle-issues.asp
CFIDSLink E-Newsletter ........................... www.cfids.org/archives/cfidslink.asp
CFS Research Review .............................. www.cfids.org/archives/research-review-issues.asp
Grassroots Action Center ........................ www.capwiz.com/cfids/home/
Health Care Provider Education ............... www.cfids.org/sparkcfs/health-professionals.asp
My Cause ............................................. www.cfids.org/support/donations-mycause.asp
Research Grants .................................... www.cfids.org/profresources/association-grants.asp
Science & Research of CFS ..................... www.cfids.org/special/default.asp
Support Groups ..................................... www.cfids.org/resources/support-groups.asp
Youth Information ................................... www.cfids.org/resources/youth.asp
November 2007Plans to hire a full-time scientific director come to fruition with the announcement that Dr. Suzanne Vernon, formerly of the CDC, is joining the CFIDS Association. Dr. Vernon is devoting her time and talents to fostering a more robust CFS research program and acceler-ating the pace of progress. A $1 million campaign is launched to fuel the expanded research program.
July 2007Andrew Lloyd and colleagues in Australia link 35 specific genes to CFS when the illness develops following infection with Epstein-Barr virus. The paper is published in the Journal of Infectious Disease and generates international media attention. Two months later, Dr. John Chia also garners extensive media coverage with another study related to viral infection, reporting that enteroviruses, a family of common pathogens, may be associated with CFS in patients with chronic gastro-intestinal problems.
October 2007The CFIDS Association participates in a collaborative meeting of organizations concerned with overlapping conditions such as fibromyalgia, interstitial cystitis, irritable bowel syndrome and chronic pain, providing guidance on how to expand awareness and funding that benefits patients with one or several of these disorders.
September 2007Dr. Brigitte Huber of Tufts University is awarded a research grant to study a retrovirus, HERV-K 18, as a risk factor for postviral CFS. The grant is funded by the NIH’s National Institute of Arthritis and Skin Diseases and the Office of Research on Women’s Health based on data collected during a 2004-06 pilot study funded by the CFIDS Association. It fulfills one of the main goals of the Association’s research program—to help promising investigators with pilot studies that can lead to larger studies funded by the NIH or biotech firms.
Directors with terms beginning in the 1980s
Marilyn Asbury (1988–1991) James Bavis (1989–1993) Pat Bradshaw (1988–1993) Susan Dorman (1989–1992) Alan Goldberg (1987–1996) Jonathan Goldberg (1989–1992) Betty Guthrie (1988–1994) Effie Hall (1989–1991) Jeanne Hardy (1989–1991) Mayhugh Horne (1988–1993) Kenneth Iverson (1987–1998) Marc Iverson, CPA, MBA (1987–2001; Board chairman, 1987–2000) Hal Levinson, JD (1989–1992) Richard Patterson (1989–1994) Adrienne Rosenberg, MSW (1989–1992) Kathryn Schwille (1989–1993) Cindy Teal (1989–1991) Robert Yentes (1989–1991)
Directors with terms beginning in the 1990s
Sheba Anderson (1993–1994) Debra Arnold (1993–1995) David Bell, MD (1992–1997) Jeffery Blum, MD (1993–1996) Richard Bourne, PhD (1997–1999) Coco Crum (1993–1998) Priscilla deLeon, RT (1995–2000) Thomas English, MD (1992–1994) Heather Frese (1997–1998) Bill Gareau (1993–1998) Betsy Haas, MSW (1992–1994) Bruce Hardy (1992) Barbara Hautau (1992)
Chester Helms (1991–1993) Jhan Hiber (1995–1996) Edward Isenberg (1995–1999) Wilhelmina Jenkins (1996–2000) Tim Kenny (1992–1994) Karen Lang (1997–1999) Kimberly McCleary (1996–present) Maggie McKenzie (1995–1998) Rebecca Moore Leibowitz (1995–1998) Marion Nelson (1997–1999) Allison O’Neal (1997–1998) David Patterson, CPA, MBA (1996–1998) Jane Perlmutter (1996–present) Kim Phillips (1993–1997) Lea Rhodes (1997–1999) Cathryn Rivers (1992–1994) Julia Sain (1993) Charles MacBrayer Sasser, JD (1992–2002) Patti Schmidt (1998–2004) Michael Shulimson (1992–1994) Carolyn Startsman (1992–1996) Marilyn Stewart (1994) Harriett Thompson (1992–1996) John Trussler (1997–2000 and 2002–2005; Board chairman, 2004) Marcia Wallace, MD (1998–1999) Frank Wrenn (1998–2000)
Directors with terms beginning in the 2000s
Bruce Allshouse (2005–present) Rick Baldwin (2001–2007) Lucinda Bateman, MD (2005–present) Diane Bean (2004–2005) Katrina Berne, PhD (2004–present) Barbara Comerford, JD (2003–2004) Rod Converse (2005–present) John Ginsberg, JD (2002) Terry Hedrick, PhD (2004–2007) Dennis Irwin (2001) Susan Jacobs, Esq. (2004–present; Board chairman, 2005–2007) Joseph Lane (2003–2004) Adam Lesser (2007–present) Beth Levine (2001–2003) Dimitris Papanicolaou, MD (2005–present) Mark Peterson, DDS (2003–present) Lynn Royster, PhD, JD (2004–present) Adrianne Ryan (2001–2007) Brian Smith (2007–present) Jennie Spotila, JD (2005–present; Board chairman, 2008) Amy Squires (2007–present) Jonathan Sterling (2000–2004; Board chairman, 2001–2004) Patrick Venetucci (2007–present)
1Defining Moments: 20 Years of Making CFS History
Akers, Michelle .............................................26 Allshouse, Bruce ...........................................53 Baldwin, Dr. Larry.......................................59 Bateman, Dr. Lucinda ..................................46 Bauer, Heidi ..................................................60 Becker-Bean, Rebecca ..................................44 Bell, Dr. David .............................................. 41 Blum, Dr. Jeffrey ...........................................43 Brice, Karen ....................................................8 Buchwald, Dr. Dedra ...................................28 Burlingame, Liz ............................................23 Carson, Rich ....................................................8 Casanova, Ken .............................................. 10 Cheney, Dr. Paul .............................................4 Cornell, Alan and Jane ................................ 31 Crum, Coco ................................................... 17 DeMeirleir, Dr. Kenneth ..............................30 Edwards, Blake ............................................. 10 Evengard, Dr. Birgitta ..................................54 Farmelo, Laura .............................................53 Fero, Pat ...........................................................6 Field, Carolyn .................................................9 Gee, Carolyn .................................................28 Goldberg, Alan .............................................. 13 Harmon, Marcia ...........................................58 Harris, Susan .................................................11 Hillenbrand, Laura ............................... 46, 49 Hopkins, Kris ................................................ 13 Huggins, Hosiah ...........................................52 Iverson, Marc ..................................................5
Jason, Dr. Leonard ....................................... 21 Jenkins, Wilhelmina .....................................33 Johnson, Cort ................................................32 Kaign, Elaine ................................................34 Klimas, Dr. Nancy ........................................ 12 Komaroff, Dr. Anthony ................................39 Lapp, Dr. Charles ......................................... 41 McCleary, Kimberly .............................. 20, 55 Moore, Rebecca ............................................26 Munoz, Mike ..................................................11 Natelson, Dr. Benjamin ...............................25 Perlmutter, Jane ............................................38 Peterson, Dr. Daniel .......................................4 Porter, Hon. John ..........................................40 Robinson, Mary ............................................ 21 Rowe, Dr. Peter ............................................45 Royster, Lynn ................................................ 51 Ryan, Adrianne ............................................. 15 Sasser, Mac ....................................................34 Schmidt, Patti ................................................30 Sheridan, Tom ............................................... 16 Silverman, Marla ..........................................44 Sklar, Zachary .................................................6 Sloven, Ruth ..................................................56 Small, Jennifer ..............................................40 Treves, Vivian ...............................................43 Trussler, John ................................................ 51 Walker, Vicki .................................................48 Weaver, Kim ..................................................49 Wong, Faith ...................................................50
Contributors & Profiles
Introduction .....................................................2 Defining Moments: Zachary Sklar ...............6 Grassroots Advocacy ......................................9 Support Groups ............................................. 10 CFS Literature .............................................. 14 Research ........................................................ 18 Name Change ................................................22 Staff ................................................................24 Youth Activism ..............................................27 CDC Exposed ...............................................33 Online Evolution ..........................................35 Provider Education ......................................37 Celebrities ......................................................42 Defining Moments: Laura Hillenbrand .....46 Philanthropy ..................................................52 Public Awareness Campaign.......................56 Board of Directors ........................................60
Features
Table of Contents
1
D e f i n i n g m o m e n T s
January 2008 © copyright by the CFIDS Association of America
2 The CFIDS Association of America 3Defining Moments: 20 Years of Making CFS History
“One of the things I’m most proud of is the way the CFIDS Association has leveraged the small amount of funds it has to fight such a large national problem. We are on a war footing with this disease.”MARK PETERSON, Virginia CFS patient; CFIDS Association Board of Directors, 2003–present
Defining Moments: 20 Years of Making CFS History 3
Marking the passage of time is often bittersweet, whether it’s watching a child reach certain milestones, celebrating a birthday or attending a class reunion. So how does an organization like ours recognize passing its own 20-year milestone, when we still don’t know the cause or cure for CFS? Certainly not by celebrating. Nor by touting our own accomplishments. However, there’s a shared history worthy of recognition. And there are individuals and organizations that warrant acknowledgement.
Defining Moments: 20 Years of Making CFS History is an effort to do just that. While the CFIDS Association of America has been the leading catalyst for chronic fatigue syndrome (CFS) progress since
it was founded in 1987, it’s the community of patients, support groups, philanthropists, doctors, researchers, government officials and, yes, patient advocacy organizations worldwide that col-lectively shares credit for the advances which have occurred since the Incline Village, Nevada, outbreak of 1984 that first alerted the country to this devastating condition.
While it would be impossible to mention all of the individuals, groups, organizations and events that have contributed to the CFS story over the past 20 years, we hope that Defining Moments provides insight on where we have been, as well as empowers us all with the recognition of the progress we have made together.
The theme for commemorating the Association’s 20th anniversary is “20 Years of Making CFS History.” The dual meaning of that phrase is entirely intentional. The CFIDS Association of America is extremely proud of its legacy—its principal role in the history of CFS. Our goal, however, is to eradicate CFS and the suffering it causes—in colloquial terms, to make the disease “history.”
The story of any community, individual or family is comprised of a series of defining moments—individual acts and singular events that contributed to change and progress that may not be evident until many years later. Some of the CFS community’s defining moments are evident, such as the Centers for Disease Control and Prevention (CDC) funding scandal, exposed in 1998, which ultimately resulted in the return of $12.9 million to the CDC’s CFS research program and an expansion of CDC research from 2000 to 2005.
Others are more subtle, such as the CFIDS Association’s moment of recognition in the mid-1990s that simply finding the cause of CFS would be insufficient to complete our mission—that once the cause is identified, there would still be tremendous work to develop effective treatments, teach clinicians to administer those treatments, and identify and deploy prevention mechanisms to keep others from becoming ill. This understanding reframed the CFIDS Association’s perspective on the time, resources and strategies that would be required to truly conquer CFS, and it resulted in assigning higher priority to advocacy, disability issues, medical education and public awareness, as well as taking a more strategic approach to research.
The CFIDS Association of America is extremely proud of its legacy— its principal role in the history of CFS. Our goal, however, is to eradicate CFS and the suffering it causes— in colloquial terms, to make the disease “history.”
Some of our community’s defining moments have been important events that created new chal-lenges. For instance, publication of the book Osler’s Web in 1996 was a watershed event, with its meticulous documentation of the government’s early contempt for CFS. Yet the controversies it set up fractured the patient advocacy community, as groups wrestled over different strategies and beliefs about disease etiology and epidemiology. These internal debates consumed scarce resources and, for a time, weakened the patient community’s collective call for social change.
To our entire community’s credit, however, divisions haven’t impeded positive strides made to improve the lives of people with CFS. The CDC-funded CFS provider and public education cam-paigns, lobbied for and implemented by the CFIDS Association, have greatly increased awareness of CFS and the ability for patients to find compassionate, competent medical care. The 1999 CFS Social Security ruling established a framework for CFS disability claims and made it easier for those disabled by CFS to secure benefits. Scientific research, much of it lobbied for or directly funded by the patient community, has provided incontrovertible evidence that CFS is one of the most complex and widespread illnesses of our time, and that there is a sound scientific basis for the biological origins of the disease.
Despite all of our progress, at least a million Americans remain ill with CFS. Many have been fighting the disease for as long as the CFIDS Association has. Many remain as sick as they were 5, 10 or 20 years ago. And that distressing knowledge—and the belief that we must harness the power to change it—drive the CFIDS Association every day.
Much work lies ahead, but as a community of CFS patients, advocates, organizations, doctors and philanthropists, we have proven we have the tenacity and collective commitment to see it through. Over the next 20 years, or however long it takes, we’ll continue driving toward the mission set forth when the CFIDS Association of America was founded: to conquer CFS.
Our dedication to that goal was just reinforced with the Association’s launch of the largest CFS research campaign to date in the United States. This initiative is designed to advance CFS research and accelerate progress in developing treatments for this illness, and it includes a campaign to raise one million dollars over a one-year period to fuel the program.
In our first two decades, we have been blessed by the support of thousands of contributors whose donations have sustained our work. We would like to recognize three donors whose special gifts helped make publication of Defining Moments possible and whose partnership has made some of the defining moments reported in its pages possible as well: the Sheridan Group, GMMB and Fleishman Hillard. Accelerating our progress will require the widespread support of donors whose gifts, both large and small, enable us to propel forward our mission to eradicate CFS.
And as the CFS story continues to be written, we will count on your participation in helping to achieve the singular defining moment we’re all working toward—the day we eradicate the enormous suffering that this illness has caused, the day we truly make CFS history.

4 The CFIDS Association of America 5Defining Moments: 20 Years of Making CFS History
19861985–1987Media attention on the outbreaks in Nevada and New York, as well as reports of similar symptoms appear-ing sporadically across the United States, lead to the formation of support groups and patient network-ing. The National CEBV Syndrome Association is founded in Portland, Oregon, by patient Gidget Faubion Jones, and the precursor to the Massachusetts CFIDS Association is launched by Bonnie Gorman, Gail Kansky, John Herd and others.
United Kingdom researcher Dr. Melvin Ramsay suggests that this “new” American illness seems to be the same thing that he and others had been calling myalgic encepha-lomyelitis (ME) since the 1950s. He publishes his case definition for ME in the ME Association Journal.
Patient Marc Iverson, who had been ill but undiagnosed since 1979, reads about CEBV in media reports. He is diagnosed by Dr. Paul Cheney, who has relocated to Charlotte, North Carolina. Iverson begins networking with other CFS patients, including Rich Carson, a former financial advisor in California, and Alan Goldberg, a fellow Charlotte resident who became ill after a trip to Incline Village during the height of the outbreak.
The Charlotte CEBV Association, the precursor to the CFIDS Association of America, is founded by patients Marc Iverson, Alan Goldberg and Laurel Gainer. The local support group begins meeting monthly that summer to share coping strategies and research news. Simultaneously, the Wisconsin CFS Association, the United Kingdom’s Action for ME and the Norwegian ME Association are founded as support and information networks.
1986–1987 Summer 1987
Marc Iverson: His Legacy Endures Marc Iverson never expected the CFIDS Association would be commemorating a 20th anniversary when he founded it in 1987.
“We were in business to go out of business,” he says. His plan was to fund the right kind of research, solve the mystery, get the cure and return to the high-powered life he had enjoyed until falling ill in October 1979.
At the time it seemed attainable. After years of traveling the country to numerous doctors in search of a diagnosis, he finally had one, and he was elated. He dove headfirst into the battle to regain his health and his life, talking with patients, support organizations, researchers, clinicians and anyone else who might help him on his quest.
Within months, he and fellow Charlotte patients Alan Goldberg and Laurel Gainer started a local support group. More than 150 people turned out for the group’s first meeting in the summer of 1987, resulting in a core of dedicated volunteers that helped run the organization.
Most of the volunteers helped turn out the then-monthly CFIDS Chronicle, making the photocopies and helping sort the bulk mailing. Iverson’s first wife, Valerie, “took care of everyone, feeding us, managing the process, doing whatever needed to be done,” he says, calling her one of the unsung heroes.
It was a heady, exciting time: “When you’re fighting for a cause that affects you, but people say doesn’t exist, you get ramped up,” Iverson says. But reality soon caught up with the chronically ill volunteers who were running the growing organization, and in 1998 the first staff member was hired. “It was a controversial decision among the patient community to hire healthy people, but with everything there was to do, it was impossible to accomplish those tasks any other way,” he says.
Until 2001 Iverson served as the Association’s board chair, orchestrating the growth and maturation of the group into the leading CFS research and public policy organization in the United States. His departure was an extraordinarily painful experience for him and for the Association’s staff and leadership. But he also found that leaving behind the responsibility, stress and energy he had invested into the Association gave him the opportunity to focus on his family and his own health, and also taught him to “put things into better perspective.”
That perspective has been much-needed in recent years, as he has seen both of his parents die after extended illnesses, his 23-year-old daughter, Dana, become increasingly disabled by CFS, and his wife, Karen, slowly recover from a devastating car accident. And he still remains very ill with CFS.
Although he has transitioned from being the caretaker of the CFS community to being his family’s caretaker, he remains involved in the CFS community. He donates to several CFS-related organizations, including the International Association for CFS/ME and the CFIDS Association of America. And he remains a significant supporter of CFS research.
Although his early hopes of quickly eradicating CFS didn’t pan out, Iverson seems to be at peace with this illness and his life. As he put it, “I count my blessings” while still pursuing the original dream of conquering CFS.
January 1985The first documented cluster of the illness that would eventually be named chronic fatigue syndrome, or CFS, begins when approxi-mately 200 people in Incline Village, Nevada, become ill with a prolonged flu-like illness. Local physicians Paul Cheney and Daniel Peterson can’t explain the scope of the outbreak and the similarity of the patients’ mysterious symptoms, other than to note that the patients have high levels of Epstein-Barr virus antibod-ies. The condition is dubbed chronic Epstein-Barr virus (CEBV).
Two research papers linking persis-tent fatiguing illness to Epstein-Barr virus are published in the Annals of Internal Medicine. Principal authors are Dr. Stephen Straus of the National Institutes of Health (NIH) and Denver’s Dr. James Jones.
A report from Drs. Paul Cheney and Daniel Peterson on the Nevada outbreak results in an investigation by the Centers for Disease Control and Prevention (CDC), whose rapid-response team visits Incline Village to review charts and interview local physicians, but examines few patients. The CDC is unable to confirm the EBV link or uncover any other explanation for the mysterious illness and is widely criticized in the patient community for its early dismissive posture concerning this illness.
About a year after the Incline Village outbreak, a second CFS cluster starts in tiny Lyndonville, New York. This time, most of the dozens afflicted are children and adoles-cents. Their physician, Dr. David Bell, suspects an infectious origin for the illness, possibly something in the milk the children were drink-ing, but he can’t identify a specific responsible organism.
September 1985 November 1985
In the early years it was nearly impossible to get anyone to take chronic fatigue syndrome seriously. The CDC’s initial dismissive reaction to the illness, and the careless and insensitive coverage of CFS by some media, contributed to a cultural response to this illness that became a major obstacle to effectively helping patients. I believe that this cultural response left a legacy that patients, clinicians and research-
ers interested in CFS are still dealing with today, although the situation has certainly improved.
Today there is much greater recognition that CFS is real and worthy of atten-tion, especially among patients and their families, and among researchers at the CDC and in the field. The legal system has come a long way too. I find that more disability judges are familiar with CFS and willing to grant disability benefits to patients. And there has been scientific progress in understanding this illness. We do know much more than we knew 20 years ago, and the puzzle pieces are coming together.
But 20 years is a long time, and I’m frustrated more hasn’t been done in the clinical arena. I’m still seeing some CFS patients who first came to me in the 1980s, many of whom travel great distances because there isn’t anyone in their area who will treat them. There are still too few treatment options, and many physicians are still incredibly resistant to treating CFS.
Those are the challenges for the next decade. Attracting in-the-trenches doctors to the field. Educating medical professionals about this illness. Discovering new treatment options. And all of this takes money. Finding the funds to move forward on these goals will be a challenge. After all, a lot of so-called orphan diseases aren’t well-funded. Even doctors who specialize in illnesses like multiple sclerosis are frustrated with lack of funding. In today’s managed care environment, chronic disease is a conundrum, and it will take a lot of effort for CFS to get its share of the pie.
Historical PerspectiveBy DANIEL PETERSON, MD Sierra Internal Medicine, Nevada
Fall 1984
Paul Cheney: Dedicated to CFS Fierce intellect. Powerful dedication. Deep compassion. This is the spirit of Dr. Paul Cheney, whose clinical and research skills have given CFS patients hope since 1984, when they began streaming through the Incline Village, Nevada, practice he shared with Dr. Daniel Peterson.
He has treated more than 5,000 CFS patients in his Nevada and North Carolina practices, and his reach extends to the many thousands worldwide who have followed his work through the medical literature and presentations at meetings and conferences.
Dr. Cheney has a well-deserved reputation for integrating disparate research and clinical findings to develop new models to explain chronic fatigue syndrome. Even after a serious illness that required a heart transplant in 2003, he continues his research and clinical work, now focusing on cardiac problems in CFS. He is also known for being one of the staunchest defenders of patients, never hesitating to set straight federal agencies, the media or anyone who dares question the seriousness of CFS.
6 The CFIDS Association of America 7Defining Moments: 20 Years of Making CFS History
The Charlotte CEBV Association starts a newsletter that includes cutting-edge news from a large network of researchers, clinicians and patients. The CFIDS Chronicle’s first “staff” is a group of volunteers/patients led by editor Marilyn Asbury, founders Marc Iverson and Alan Goldberg, writer Caryn Freese and other members of the support group. Graphic designer Matt Straznitskas and writers like Tara Allen, Susan Dion and Patti Schmidt are integral to the development of the Chronicle in its early years.
The CDC’s working group of experts, formed in late 1986, completes its work on a case definition for the illness. Notably, Drs. Paul Cheney, Daniel Peterson and David Bell—all of whom have been seeing CFS patients since the initial cluster outbreaks—are never asked to comment on the definition. It takes until 1989 for the CDC’s Dr. Walter Gunn to formalize the CFS Inter-agency Coordinating Committee (CFSICC) to begin to synchronize CFS activities across federal health agencies.
Fall 1987 October 1987
Zachary Sklar is a journalist, editor and screenwriter. He is best known as co-screenwriter (with Oliver Stone) of the Oscar-nominated film JFK. A former executive editor of The Nation magazine, he has taught at the Columbia University Graduate School of Journalism and served as a creative adviser at the Sundance Screenwriters’ Lab and many other workshops around the world.
Fall 1987Summer 1987Ted Van Zelst, whose adult daughter has CEBV (CFS), becomes the first person to testify before Congress about the new illness. His congressman, Rep. John Porter, becomes a strong supporter of CFS issues throughout his long tenure in the House of Representatives. CFS patient Barry Sleight of Alexandria, Virginia, joins Van Zelst’s initiative and begins advocating in Congress for CEBV issues.
The fledgling Charlotte organization spends the very first dollar it raises on research, giving a $15,000 research grant to Dr. Paul Cheney, who is trying to identify laboratory markers for CFS. This expenditure establishes the CFIDS Association’s research program, which has funded researchers or research symposia every year since then.
“The Wisconsin group was founded the same year as the CFIDS Association. The early years were rough, and many state and local organizations didn’t survive the challenges of being run by patient volunteers who were so ill, and lack of funds to operate. I’m proud that our state group has managed to serve the needs of patients all these years.”PAT FERO, Wisconsin President of Wisconsin CFS Association
D e f i n i n g m o m e n T sBy Zachary Sklar
THen The first dollar spent by the CFIDS Association of America was directed to medical research. In 1987, the year the orga-nization was founded, we funded just $15,000 in research.
noW The Association has funded more than $4.8 million in research, making our organization the largest source of CFS research money aside from the federal government. Financial contributions by individuals make this vital objective possible.
In November 1986 I went to see Dr. Shyam Singha in a cramped hotel room in mid-Manhattan. Tall and thin, he was a Sikh from India—a naturopath, osteopath, acupuncturist and nutritionist. He had a restless energy, flowing black hair and an ageless face. He could have been 40. Or 70. I had no idea.
He examined my tongue, felt my pulse and asked me what made me laugh. Then he handed me a piece of paper with a scribbled regimen. “Twelve to 16 broiled oranges per day for seven days. As much hot water as you want. Nothing else.”
I looked at him. He must be insane, I thought. For nine months I’d gone from doctor to doctor at the best hospitals in New York. I’d taken countless tests and pills. Nothing had helped. If anything, I was worse than I’d been the night I got sick. More exhausted, more fevers and night sweats, digestion hopelessly messed up, head in a 24-hour-a-day fog, skin turning a sicken-ing yellow.
“I can’t walk to the corner store,” I protested. “How am I going to survive without protein?”
“Do it!” he ordered in his Indian accent. He turned and left to see another patient.
I was scared. For 15 years I’d been a journalist and editor. Strong and healthy, I’d never been seriously sick, never missed a day of work. Now I couldn’t read more than a few minutes before my head throbbed with pain. I couldn’t concentrate to write. My savings were depleted. How was I going to pay the rent?
I was 38 back then, a rational man who believed in science and Western medicine. I distrusted anything that smacked of unquantifiable Eastern mysticism. But now I had to admit: everything I’d believed in wasn’t working.
Dr. Singha was asking me to change my diet and my habits—the way of life that had got me into this mess. He dismissed the hope that the next doctor or the next pill might magically save me. Instead, with those two words—“Do it!”—he challenged me to take control of my own health.
I decided to do it. The broiled oranges, I realize now, were a fruit fast to cleanse my overtaxed liver and digestive tract. Within two days, I started to feel better. The fog in my head lifted for a few hours and I felt more energetic. For the first time in nine months, I had hope.
After the week of oranges, Dr. Singha’s regimen continued with only raw food for a month. Then one cooked meal a day and the rest raw for five months. No meat, no alcohol, no caf-feine, no sugar. Fifteen minutes of laughter per day.
That first visit with Dr. Singha was the beginning of my long journey back to good health. Over eight years I learned some of his simple wisdom. Food is medicine, he used to say. But when you eat the wrong food, it can be poison. He modified my diet many times and added in supplements—things like
digestive enzymes, fish oil, psyllium husks, spirulina. He treated me with acupuncture and gave me breathing exercises. Occasionally he offered prescriptions that I thought were wacky: “hug a tree until you can hear it talk,” “walk in cold water for 10 minutes before bed,” “conduct the orchestra for 15 minutes a day in front of a mirror.” As it turned out, each of these helped.
But the most important thing Dr. Singha did was to empower me by giving me a vision and some tools to change my life. Over the last 21 years I have tried many things to speed my healing—homeopathic injections, colonics, low doses of doxycycline, thyroid supplements, antiyeast diets and more. I’ve eliminated much of the stress in my life. I’ve learned what’s really important to me and focused my limited energy on that. I’ve moved to a rural town with lots of trees, clean air and silence. I’ve insisted on getting a good night’s sleep and a good nap every day. I’ve exercised as my body allows—swimming, qigong and running. And I’ve been fortunate to have unwavering support and love from my life partner, Sarah Plant. Gradually, very gradually, I’ve improved. I feel far better today at the age of 59 than I did at 38.
I’ll probably never know the exact cause of my illness. From the tests, it’s clear that my immune system was unable to fight off whatever attacked it.
Why was my immune system compromised? I have my own theories. I led an extremely stressful life in New York City. For six years I missed two nights of sleep every week proofreading at Time and Life magazines. I spent my vacation time picking coffee on a peace brigade in Nicaragua and ended up with intestinal parasites.
But there’s something else. I grew up in Los Angeles during the 1950s when nuclear testing in the atmosphere was routine. On Halloween Day of 1958, wind carried a huge cloud of radiation from the Nevada test site toward southern Califor-nia. The radiation hung over the Los Angeles basin for three days in an inversion layer. Nobel Prize laureate Linus Pauling predicted that 25,000 cancer deaths would result from that one exposure over the next 30 years. I was 10 years old then, and I got sick 28 years later. I don’t know if that radiation contrib-uted to my illness. But it sure didn’t help.
I know some people suffering with CFS who cling to the hope that one day researchers will discover a viral cause for the illness and a miraculous cure—the polio model. But after I met Dr. Singha, I stopped thinking that way. Instead, I started working to heal myself.
What Dr. Singha gave me wasn’t a cure. But for me, it was a more important gift. I’m very grateful to him. With two words I’ll never forget, he helped me move on to my new life. “Do it!”
1 9 8 7

8 The CFIDS Association of America 9Defining Moments: 20 Years of Making CFS History
The work of early advocates like Ted Van Zelst and Barry Sleight pays off when Congress directs the NIH and the CDC to study CFS and the Social Security Administration (SSA) to update its disability guidelines on CFS. This is the first inclusion of chronic fatigue syndrome in report language; it has been included every year since.
Fall 1988
Administration (SSA) with letters and phone calls that influenced policy change. Grassroots advocates are largely responsible for the bipartisan support that CFS has in Congress and the federal policy decisions that have benefited CFS patients.
The CFIDS Association has always made it a priority to help CFS patients become effective advocates. In the earliest years, it took the form of supporting and promoting the activities of the first CFS lobbyist, Barry Sleight, and joining the leadership circle of the CACTUS coalition of advocacy organizations. When the Associa-tion assumed responsibility for federal CFS activism in 1992, one of its first steps was to form the CFIDS Activist (C-ACT) program, which gave supporters the tools, including background information and sample letters, to make effective contact with officials about CFS-related issues. In 2004 the web-based Grassroots Action Center (GAC) was launched, making it even easier for advocates to contact legislators, federal officials and the media about CFS. More than 40,000 messages have been sent by advocates through the GAC since then.
The CFIDS Association’s Lobby Day is another important tool in the grassroots advocacy arsenal, giving advocates the opportunity to meet in person with elected officials in Washington, D.C. It has grown considerably from the three participants at the first event in 1992. In 2007 a record 80 advocates met with representatives of 94 congressional offices about CFS-related policy. “Virtual lobbyists” also played an important role in this May’s event, sending nearly
6,200 messages about CFS to Congress members, federal officials and reporters.
In 2007 the Association also helped advocates make contact with members of Congress during the August recess, arming them with materials and talking points for local Town Hall meetings held by their congressional representatives, creating hundreds of individual “lobby days” around the country.
Your voice is more powerful than you know. Visit the Grassroots Action Center at
www.capwiz.com/cfids/home/ to lend your voice to the
CFS advocacy movement.
Throughout 1988November 1987The National CEBV Syndrome Association holds the first CFS conference in the United States. Researcher Seymour Grufferman proposes chronic fatigue and immune dysfunction syndrome (CFIDS) as the condition’s new name. Many organizations quickly jump on Dr. Grufferman’s suggestion; for example, the Charlotte organization becomes the CFIDS Association of Charlotte and the Portland group becomes CFIDS Society International.
New national organizations are founded to join the fight against CFS. The CFS Research Foundation starts raising funds for research. Rich Carson opens ProHealth and the CFIDS Buyers Club, selling nutritional supplements and directing funds toward CFS research. And the CFS Information Institute is launched in Washington, D.C., to support Barry Sleight’s legislative work, which he had been doing as a volunteer.
March 1988February 1987The NIH issues its first CFS program announcement, soliciting applications for research grants to join the two CFS grants it’s already funding.
The CDC publishes its first research case definition for CFS in the Annals of Internal Medicine. The case definition states that a person must have new onset of fatigue, at least a 50 percent reduction in function and 8 of 11 listed symptoms (or 6 of the 11 symptoms and 2 of 3 physical criteria) for 6 months or more to be diagnosed with the illness. This complex case definition is criticized for its “Chinese menu” approach. Two other definitions of CFS would follow—Lloyd in 1998 and Oxford in 1991.
Rich Carson: Making a Difference Rich Carson was just 23 years old when CFS sidelined his sales career and sent him in search of researchers and clinicians who might explain the chronic EBV diagnosis he received in 1981, before there was anything called chronic fatigue syndrome. After leading a local support group, Carson put his sales skills to use, founding a nutritional supplement company, ProHealth.
Over the years, ProHealth grew under Carson’s entrepreneurial direction. And he became a vocal activist and advocate for the CFS community, developing the immunesupport.com section of the ProHealth website into a widely used resource for information about CFS and fibromyalgia (FM). ProHealth has reportedly raised and donated more than $2.6 million to support CFS and FM research through various organizations, including the CFIDS Association of America and the National Fibromyalgia Association.
In 2006 he received the annual Outstanding Advocate award from the Whittemore-Peterson Institute for Neuroimmune Research, an honor he accepted by saying, “Much of our work is still ahead of us, but the incredible achievements of organizations such as the institute are clear signs that progress is inevitable with dedication and perseverance of people who care.”
“For 13 years CFS has intruded on my life, and my family’s life. We are all its victims, even though it is my husband, Jim, who has the illness. Many patients have lost jobs, families, homes and friends because people don’t understand how debilitating this illness can be. People don’t understand that CFS is more than being tired; it’s like carrying around a crushing weight or wearing a cement overcoat.”KAREN BRICE, Pennsylvania Wife of CFS patient
Grassroots Advocacy
It’s a story that’s been told so often, it has taken on legendary status. Unlike many legends, this one is true and, like all such stories, it holds a powerful message.
In 1987 Illinois’ Ted Van Zelst, whose adult daughter was disabled by CFS, became the first person to testify before Congress about CFS. His congressman, Rep. John Porter, was at the time a low-ranking member of the health appropriations subcommittee, but within a few years rose to become the subcommittee’s chair. Van Zelst’s relationship with Porter led the congressman to champion CFS issues in Congress until his retirement in 2000, illustrating the power of relationship-building that guides all successful activism.
At the same time that Van Zelst was building a relationship with Porter, patients who became ill in the 1984-85 Nevada CFS cluster, including Jerry Crum, were building a similarly strong relationship with their senator, Harry Reid. Reid has continued to support CFS issues today, even as Senate Majority Leader.
Grassroots activism is the foundation on which all of CFS advocacy is built. The power of concerned, individual voters dem-onstrating their interest and demanding change on an issue like CFS is considerable. On health issues like CFS, a representative’s decision to initiate or support a change rarely hinges on campaign contributions. Very often, it’s either the number of voters who contact him or her about the issue, or the relationship with the petitioner that makes the difference.
Hundreds of CFS patients and activists have found this to be true over the years. For example, Maggie McKenzie and Rep. Rosa DeLauro; the Iverson family and Sen. Lauch Faircloth; Jan Montgomery and Rep. Nancy Pelosi; Jane Perlmutter and Rep. Nita Lowey; Jonathan and Rachel Stein and Sen. Arlen Specter; Dr. Lucinda Bateman and Sen. Orrin Hatch; the hundreds who have flooded agencies like the CDC and the Social Security
“In August I spoke about CFS research at a Town Hall meeting held by my congressman, Mike Honda. I was stunned when the audience broke into applause when I finished! I was also surprised when Honda said he definitely supported CFS research at NIH. And I feel like I brought awareness to the hundreds of people sitting in the auditorium. When I was leaving, I had three different people come up to me to share their story or congratulate me. It was such an empowering experience; I can’t wait to do it again.”CAROLYN FIELD, California CFS patient
10 The CFIDS Association of America 11Defining Moments: 20 Years of Making CFS History
September 1989April 1989The name chronic fatigue syndrome continues to elicit strong patient protest. The San Francisco CFIDS Association conference includes the first official name-change forum.
Hit TV show The Golden Girls opens the season with a two-part episode detailing lead character Dorothy’s battle with chronic fatigue syndrome. The episode closely mirrors series creator Susan Harris’s own experience as a person with CFS. The program concludes with the telephone number of the CFIDS Association, which is flooded with 10,000 requests for information.
Spring 1990February 1990Los Angeles clinician Dr. Jay Goldstein holds his first CFS research conference. This confer-ence becomes a regular event over the next several years, highlighting cutting-edge CFS findings. Goldstein focuses on a “limbic hypothesis” for CFS and publishes several books, but few peer-reviewed articles.
The CFIDS Action Campaign for the United States (CACTUS) is founded as a collaborative advocacy group by the CFIDS Association, San Francisco CFIDS Foundation, Massachusetts CFIDS Association, CFS Information Institute and 10 other groups. Duties are divided among the collaborators: the CFIDS Chronicle serves as its publication arm, the CFS Information Institute leads the legislative charge and the San Francisco CFIDS Foundation manages publicity.
“Support groups have strengthened advocacy on the local, grassroots level where national organizations can’t specifically focus. They also give patients a local connection with other patients.”MIKE MUNOZ, Colorado President of Rocky Mountain CFIDS/FMS Association
“My hope in writing those Golden Girls episodes was to bring this illness to the attention of as many people as I could, and there’s no greater device for that than television. It did bring an overwhelming response from viewers, people who felt understood for the first time. But I don’t think it changed the minds of very many doctors, and the skepticism in the medical community is still a problem today.”SUSAN HARRIS, California Creator of The Golden Girls and Soap
September 1988September 1988The NIH and the University of Pittsburgh collaborate on a CFS research conference called “Considerations in the Design of Studies of CFS.” Interest in CFS continues to grow. The NIH reports that 25 percent of the calls taken by its National Institute of Allergy and Infectious Diseases (NIAID) communications office are about chronic fatigue syndrome.
The National Institute of Allergy and Infectious Diseases (NIAID) announces three-year, $1 million center grants to Drs. Dedra Buchwald and Anthony Komaroff to research CFS.
February 1989December 1988The newly renamed CFIDS Association of Charlotte receives its first major donation from someone other than the organization’s founders or their family members: a $10,000 gift earmarked for research from film director Blake Edwards, who has CFS.
The National CFS Advisory Council, the precursor to the American Asso-ciation for CFS (AACFS) is organized by Dr. Dharam Ablashi and others. This organization continues to serve the international CFS research and medical community today as the International Association for CFS/ME (IACFS/ME).
Even before CFS was formally defined, support groups began forming to provide an environment where patients could find validation for their illness, share experiences and identify ways of coping with a poorly understood chronic illness. By the mid-1990s there were more than a thousand CFS support groups in the United States, and the CFIDS Association had formed the CFIDS Support Network as a resource for group leaders around the country.
Today there are fewer groups, as the Internet and other forms of communication have made it easier for disabled and housebound individuals to find “virtual communities” without leaving home. But support groups continue to play a vital role not just in sup-porting individual patients, but as forces for change.
Early on, patients who met in living rooms, church halls or hospital community rooms to support one another also took on the roles of educators, advocates and marketers. Support groups acted as local repositories of information about CFS for health care professionals, patients, the media and the general public. Leaders and groups found these roles to be empowering.
Some groups transformed from having a traditional support ori-entation to becoming advocacy organizations. A North Carolina support group, the Charlotte CEBV Association, became the CFIDS Association of America. Several support groups meeting across New Jersey joined to form the New Jersey CFS Associa-tion. The Wisconsin CFS Association was created to foster the work of 30 groups across that state and to take on larger educa-tion and advocacy initiatives. The same story played out around the world with groups such as the United Kingdom’s Action for ME, the ME/CFS Society of South Australia, the Allison Hunter Memorial Foundation (Australia), Norway’s ME Association and FM-CFS Canada.
In fact, nearly every advance in awareness, advocacy, research and provider education can trace its roots to these support and advocacy organizations. It’s not possible to list all the groups
that have made notable contributions over the past 20 years, but a few of those vital to progress include the CFIDS Action Campaign for the United States (CACTUS), CFIDS Action Network, CFIDS Society International, CFIDS Youth Alliance, Connecticut CFIDS Association, Dallas/Fort Worth CFS/FM Association, Houston CFIDS Association, Lehigh Valley CFIDS (Pennsylvania), Manasota CFIDS (Florida), Mas-sachusetts CFIDS Association, Northern Virginia CFS/FM Support Group, OFFER (Utah), Oregon CFIDS Association, PANDORA (Florida), Rhode Island CFIDS Association, Rocky Mountain CFIDS/FM Association, San Francisco CFIDS Foundation and Vermont CFIDS Association. Many of these organizations are still active today, but others have ceased operation.
No discussion of support groups would be possible without hailing the support group leaders themselves. Most also have CFS; most don’t have a background in counseling, health care, science or advocacy, but learn to be conversant in all these areas; and most sacrifice their own health and finances to help their fellow patients and to spur progress in the understanding of CFS. We salute them all.
“Mass CFIDS was one of the first organizations to push the government for more research funding. Without such patient advocacy, recognition of this illness and subsequent research would’ve been nearly impossible.”KEN CASANOVA, Massachusetts President of Massachusetts CFIDS Association
“I found it very hard to articulate it or explain chronic fatigue syndrome except to say that my whole body was just one big boil, that I ached in every joint every second of the day and night.”BLAKE EDWARDS CFS patient; director of such films as Breakfast at Tiffany’s, Victor/Victoria and the Pink Panther detective spoofs
Support Groups

12 The CFIDS Association of America 13Defining Moments: 20 Years of Making CFS History
April 1991January 1991The CFIDS Association’s national agenda continues to grow, but the paid staff is still limited to editor Caryn Freese, controller David Patterson and office manager Diane Pritchard. So Marc Iverson expands the paid staff to meet the organization’s important objectives. Kris Hopkins comes on board as an office assistant, then Kimberly McCleary is hired as executive director.
To deal with the increasing number of information requests, the CFIDS Association establishes a toll-free 800 number. By 1993 the Association is responding to more than 60,000 calls annually. Every year the Association receives thousands of calls and requests for information and responds by mailing out packets on topics such as choosing a doctor, finding a support group, qualifying for Social Security disability and coping with pediatric CFS.
The CFIDS Action Campaign for the United States (CACTUS) advocacy coalition hires Joan Sutherland as its executive director and engages lobbyist Tom Sheridan of the newly formed Sheridan Group to provide strategic guidance. That fall a handful of CACTUS leaders meets in Washington to lobby for CFS funding. A direct-mail appeal to patients to support CACTUS falls short of expectations.
The NIH convenes a meeting to debate the CFS case definition. The amendments, published in 1992, are known as the “Schleuderberg definition” after Dr. Ann Schleuderberg, a National Institute of Allergy and Infectious Diseases (NIAID) administrator and the meeting’s organizer.
Early 1991 March 1991
In the early years of the CFIDS Association, we were such a small staff that just getting day-to-day matters handled was a challenge. So little was known about the illness, and we were all facing a steep learning curve together. How to decipher conflicting research and theories about CFS. How—and what—to tell the public about the illness to get people to take it seriously. How to work with researchers and clinicians. How to deal with media myths and misunderstanding about the illness. How to get federal officials and legislators, most of whom had never heard of CFS, to pay attention to it. We were learning as we went.
Back then there were so few resources available for patients, family members and even health care professionals. This was before the Internet revolutionized how society gathers and dissemi-nates information, so patients turned to the Association for everything. We often spent so much time answering patient phone calls, putting out the CFIDS Chronicle, sending out information packets and giving other organizations the day-to-day assistance they needed that it was nearly impossible to lift our heads from the tasks at hand and take a look ahead at the future.
Today, with the addition of more staff members with so much talent and expertise, and the vision of a Board of Directors focused on the long-term view, we make the time for strategic planning and for routinely assessing the Association’s work in terms of resources, programs and long-range goals. This is a critical step in the Association’s evolution and its maturation. Stepping back to see the big picture has not only made us better stewards of our financial resources, it has positioned us to make even more contributions to the fight to conquer CFS in the years ahead.
I’m so grateful that our donors and members recognize the value of having a talented professional staff with the expertise to move us forward and an unwavering commitment to the CFS commu-nity we serve.
Historical PerspectiveBy KRIS HOPKINS Chief Financial Officer, CFIDS Association of America
“After two of the early advocacy organizations closed in late 1991, the CFIDS Association was asked to take responsibility for leading national policy efforts. Although two donors had pledged to support costs for the public policy program, I wasn’t sure that this was the right direction for us to take. But at our first meeting with lobbyist Tom Sheridan, he made a persuasive argument about how advocacy could augment research, so we cautiously moved forward. That decision—and the work that Tom and Kim McCleary have done together—have transformed this organization.”
ALAN GOLDBERG, North Carolina CFS patient; CFIDS Association Board of Directors, 1987–1996
June 1990June 1990A double-blind study of the experimental drug Ampligen starts in four cities: Incline Village, Charlotte, Houston and Portland. A total of 92 patients are enrolled in the study sponsored by the manufacturer, Human Ethical Medical, or HEM (later called Hemispherx Biopharma). Half of the patients receive Ampligen and half placebo. Study subjects are told that after the trial, HEM will give them all Ampligen free of charge; when the company reneges on its oral promises, lawsuits are filed.
Dr. Nancy Klimas publishes her first paper linking CFS to low natural killer cell function, a key component of the immune system’s defense mechanism. Klimas stays in the field and earns a reputation as one of America’s foremost authorities on CFS.
Dr. Elaine DeFreitas presents the preliminary results of her CFIDS Association-funded research linking CFS to a novel retrovirus similar to human T-cell leukemia virus type II. The data is presented at an international virology meeting in Kyoto, Japan, and then published in the Proceedings of the National Academy of Sciences in 1991. Sadly, her research is never completed due to lingering disability from a car accident in the early 1990s, and remains unconfirmed due to the inability of other investigators to replicate her findings.
Newsweek publishes a cover story on chronic fatigue syndrome, which becomes the year’s top-selling issue of the magazine. The story coincides with a CFS research conference in Charlotte, which highlights the latest findings in immunology, virology and other disciplines from the day’s leading investigators, including Drs. Elaine DeFreitas, John Martin, Jay Levy, Andrew Lloyd, Harvey Moldofsky and Nancy Klimas.
September 1990 November 1990
Over the years, people have often asked me if CFS is an immune disorder, a brain disease or a dysfunction of the endocrine system. Scientists working within their own disciplines have tended to see CFS through a narrow lens. As an immunologist, I once would have said CFS is clearly an immune dysfunction state, while an endocrinologist would call attention to the adrenal gland irregularities, and a specialist in the autonomic nervous system would be convinced CFS is all about blood pressure abnormalities.
Given what we’ve discovered about the illness, I now tell people CFS is all of these things. We
know that chronic fatigue syndrome has identifiable biologic underpinnings because we now have research documenting a number of underlying pathophysiologic processes involving the brain, the immune system, the neuroendocrine system and the autonomic nervous system.
Many researchers are starting to question whether CFS is caused by one trigger or agent, or whether multiple triggers may lead to this disease state, with similar but not identical sympto-mology and illness course. Increasingly, scientists are adopting
Historical PerspectiveBy NANCY KLIMAS, MD University of Miami; Miami VA Medical Center
a more multidisciplinary approach and promoting scientific exchange and collaboration. We are finally interested in integrating disciplines, and we have the tools to accomplish this. It’s an exciting time for CFS research.
While there continue to be scientific advances in our understanding of this illness, there is less enthusiasm about our progress in the clinical care of CFS patients. Chronic fatigue syndrome is still challenging to treat, creating a cycle of frustration for patients and physicians alike. We need more work to discover treatments that address the true biologic underpinnings of this illness. We need clini-cal trials data with patient groups that are large enough to answer questions about the efficacy and safety of various clinical approaches. We need disability insurance carriers to recognize this condition. And we need to educate physicians and other health care workers about this illness until every doctor, nurse practitioner and physician assistant knows what the current standard of care and treatment strategies are for chronic fatigue syndrome.
What we know about CFS today has been fueled by activism, and the important questions we have yet to answer warrant our sustained commitment to those efforts.
D e f i n i n g m o m e n T
14 The CFIDS Association of America 15Defining Moments: 20 Years of Making CFS History
Fall 1991Summer 1991The CFIDS Association formalizes its research grant-making process by instituting a formal peer-review body, the Scientific Advisory Committee. The Association also raises $150,000 from donors in 1991 to support research grants. This sets the stage for a significant increase in the amount of funds raised for research in the 1990s.
The NIH funds its first three CFS Cooperative Research Centers. Drs. James Jones in Denver, Anthony Komaroff in Boston and Benjamin Natelson in Newark are the grant recipients. The centers had been directed by Congress in its 1990 annual health appropriations legislation, the work of advocates Barry Sleight and Ted Van Zelst.
The NIH’s Mark Demitrack reports low cortisol levels in CFS patients, indicating an abnormality in patients’ endocrine systems, in the Journal of Clinical Endocrinology and Metabolism. This finding helps establish that CFS is different from primary depression, which is characterized by high cortisol levels.
CFIDS Action Campaign for the United States (CACTUS) folds due to lack of financial support, and the CFIDS Association assumes responsibility for national CFS advocacy efforts. The Public Policy Advisory Committee is formed to oversee the Association’s advocacy efforts. With earmarked financial contributions from advocates Ed Taylor and Ted Van Zelst, the Association takes on financial support for lobbyist Tom Sheridan’s work at the federal level.
December 1991 June 1992
“One of the most valuable lessons I’ve learned as a board member of the CFIDS Association has been the importance of advocacy. Whether you lend your time or support to a grassroots letter-writing campaign or you visit legislators on Capitol Hill, every effort has the potential to change hearts and minds, forever altering the way this disease is viewed in the public eye, in your doctor’s office and in the halls of Congress. Advocacy translates into very tangible benefits for people with this disease.”ADRIANNE RYAN, New York CFS patient; CFIDS Association Board of Directors, 2001–2007’87 ’88 ’89 ’90 ’91 ’92 ’93 ’94 ’95 ’96 ’97 ’98 ’99 ’00 ’01 ’02 ’03 ’04 ’05
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
$400,000
$450,000
$500,000
Grants Research Symposia
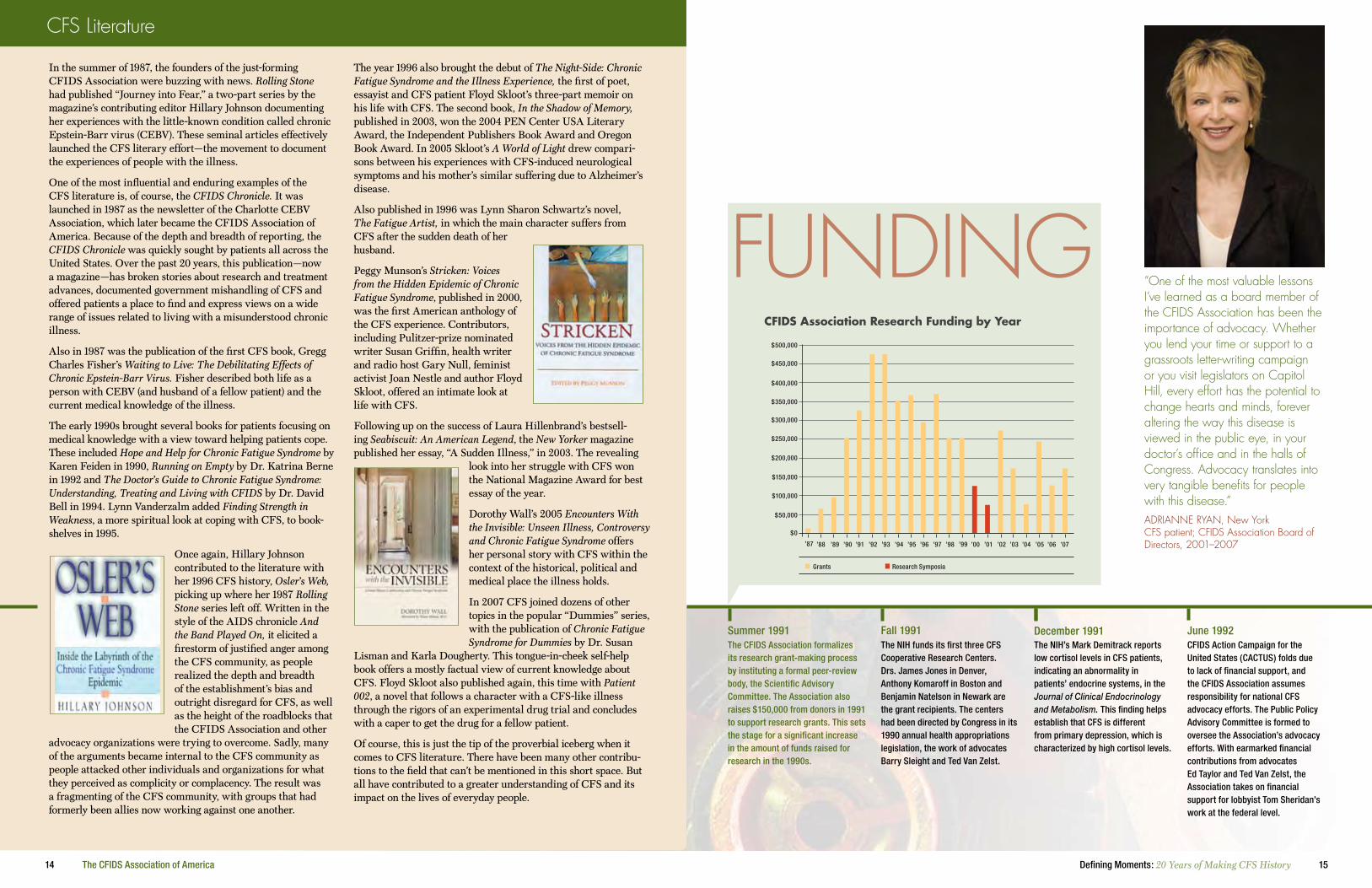
CfiDs Association Research funding by Year
’06 ’07
FUNDING
In the summer of 1987, the founders of the just-forming CFIDS Association were buzzing with news. Rolling Stone had published “Journey into Fear,” a two-part series by the magazine’s contributing editor Hillary Johnson documenting her experiences with the little-known condition called chronic Epstein-Barr virus (CEBV). These seminal articles effectively launched the CFS literary effort—the movement to document the experiences of people with the illness.
One of the most influential and enduring examples of the CFS literature is, of course, the CFIDS Chronicle. It was launched in 1987 as the newsletter of the Charlotte CEBV Association, which later became the CFIDS Association of America. Because of the depth and breadth of reporting, the CFIDS Chronicle was quickly sought by patients all across the United States. Over the past 20 years, this publication—now a magazine—has broken stories about research and treatment advances, documented government mishandling of CFS and offered patients a place to find and express views on a wide range of issues related to living with a misunderstood chronic illness.
Also in 1987 was the publication of the first CFS book, Gregg Charles Fisher’s Waiting to Live: The Debilitating Effects of Chronic Epstein-Barr Virus. Fisher described both life as a person with CEBV (and husband of a fellow patient) and the current medical knowledge of the illness.
The early 1990s brought several books for patients focusing on medical knowledge with a view toward helping patients cope. These included Hope and Help for Chronic Fatigue Syndrome by Karen Feiden in 1990, Running on Empty by Dr. Katrina Berne in 1992 and The Doctor’s Guide to Chronic Fatigue Syndrome: Understanding, Treating and Living with CFIDS by Dr. David Bell in 1994. Lynn Vanderzalm added Finding Strength in Weakness, a more spiritual look at coping with CFS, to book-shelves in 1995.
Once again, Hillary Johnson contributed to the literature with her 1996 CFS history, Osler’s Web, picking up where her 1987 Rolling Stone series left off. Written in the style of the AIDS chronicle And the Band Played On, it elicited a firestorm of justified anger among the CFS community, as people realized the depth and breadth of the establishment’s bias and outright disregard for CFS, as well as the height of the roadblocks that the CFIDS Association and other
advocacy organizations were trying to overcome. Sadly, many of the arguments became internal to the CFS community as people attacked other individuals and organizations for what they perceived as complicity or complacency. The result was a fragmenting of the CFS community, with groups that had formerly been allies now working against one another.
The year 1996 also brought the debut of The Night-Side: Chronic Fatigue Syndrome and the Illness Experience, the first of poet, essayist and CFS patient Floyd Skloot’s three-part memoir on his life with CFS. The second book, In the Shadow of Memory, published in 2003, won the 2004 PEN Center USA Literary Award, the Independent Publishers Book Award and Oregon Book Award. In 2005 Skloot’s A World of Light drew compari-sons between his experiences with CFS-induced neurological symptoms and his mother’s similar suffering due to Alzheimer’s disease.
Also published in 1996 was Lynn Sharon Schwartz’s novel, The Fatigue Artist, in which the main character suffers from CFS after the sudden death of her husband.
Peggy Munson’s Stricken: Voices from the Hidden Epidemic of Chronic Fatigue Syndrome, published in 2000, was the first American anthology of the CFS experience. Contributors, including Pulitzer-prize nominated writer Susan Griffin, health writer and radio host Gary Null, feminist activist Joan Nestle and author Floyd Skloot, offered an intimate look at life with CFS.
Following up on the success of Laura Hillenbrand’s bestsell-ing Seabiscuit: An American Legend, the New Yorker magazine published her essay, “A Sudden Illness,” in 2003. The revealing
look into her struggle with CFS won the National Magazine Award for best essay of the year.
Dorothy Wall’s 2005 Encounters With the Invisible: Unseen Illness, Controversy and Chronic Fatigue Syndrome offers her personal story with CFS within the context of the historical, political and medical place the illness holds.
In 2007 CFS joined dozens of other topics in the popular “Dummies” series, with the publication of Chronic Fatigue Syndrome for Dummies by Dr. Susan
Lisman and Karla Dougherty. This tongue-in-cheek self-help book offers a mostly factual view of current knowledge about CFS. Floyd Skloot also published again, this time with Patient 002, a novel that follows a character with a CFS-like illness through the rigors of an experimental drug trial and concludes with a caper to get the drug for a fellow patient.
Of course, this is just the tip of the proverbial iceberg when it comes to CFS literature. There have been many other contribu-tions to the field that can’t be mentioned in this short space. But all have contributed to a greater understanding of CFS and its impact on the lives of everyday people.
CFS Literature
16 The CFIDS Association of America 17Defining Moments: 20 Years of Making CFS History
January 1993Early to mid-1990sBetween 1991 and 1995, the CFIDS Association’s research funding priorities are driven by intense interest in viruses as causative or contributing factors in CFS. During this period, the Association raises nearly $2 million from donors to fund research grants for investigators examining the role of known or novel viruses in CFS, as well as immune studies that suggest assault by an outside invader. Frequent reassessment of research priorities in the years since has broadened our research portfolio, as the graph above shows.
Research confirming immune abnormalities in CFS is published in the Journal of Clinical Immunology by the NIH’s Dr. Stephen Straus.
The CFIDS Association launches the CFIDS Activist (C-ACT) program to teach and encourage advocates to get involved in grassroots public policy activities. One of the program’s early successes is the mass protesting of misinformation in the CDC’s pamphlet, The Facts About CFS.
The CFIDS Association adds “of America” to its title, officially acknowledging the national scope of its work. Coco Crum is the first board member recruited from outside the Charlotte area. Two years later leaders from California, Connecticut, New Mexico, New York and Pennsylvania join the Board of Directors.
January 1993 January 1993
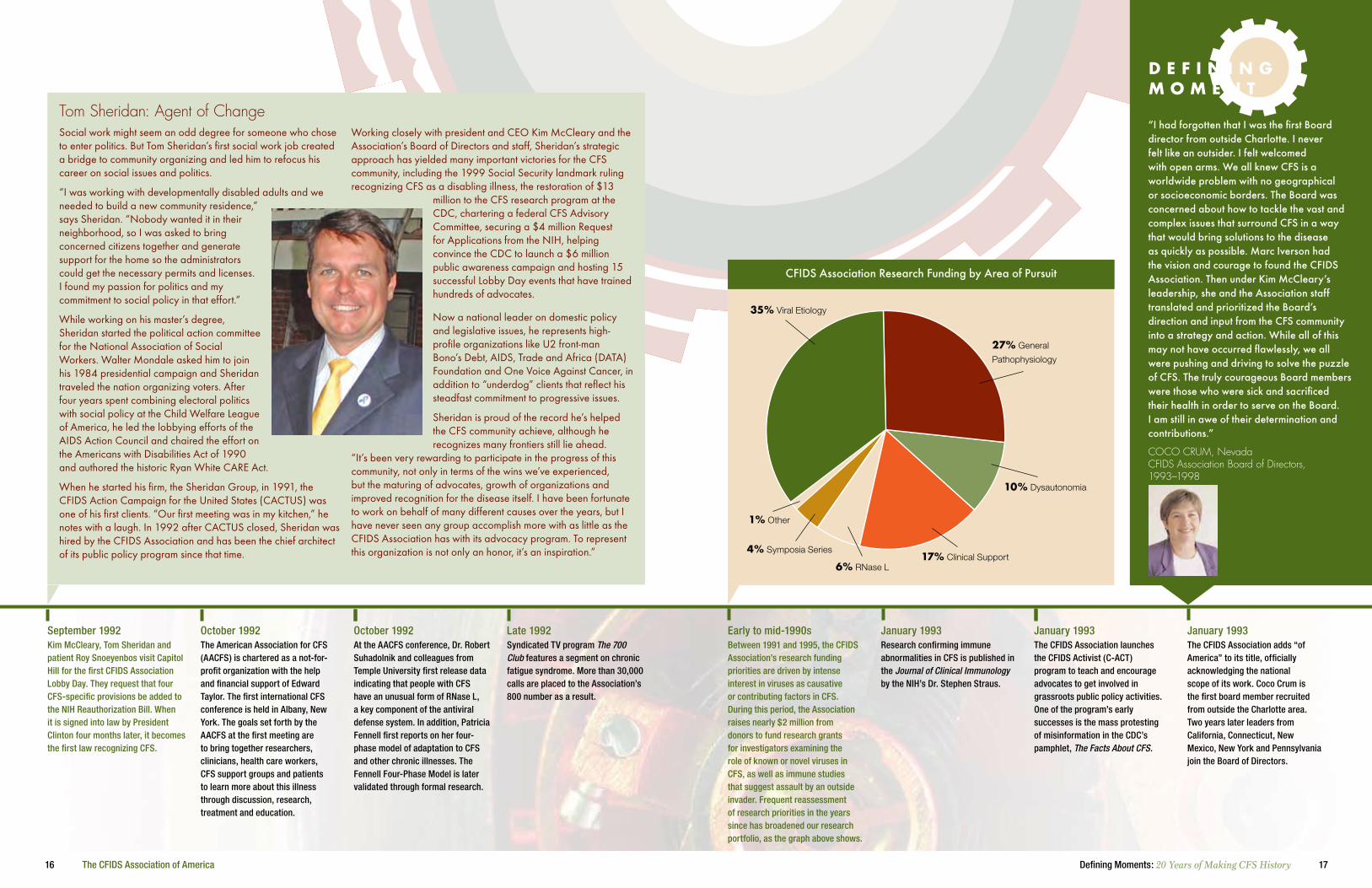
CFIDS Association Research Funding by Area of Pursuit
27% General
Pathophysiology
10% Dysautonomia
17% Clinical Support6% RNase L
4% Symposia Series
1% Other
35% Viral Etiology
“I had forgotten that I was the first Board director from outside Charlotte. I never felt like an outsider. I felt welcomed with open arms. We all knew CFS is a worldwide problem with no geographical or socioeconomic borders. The Board was concerned about how to tackle the vast and complex issues that surround CFS in a way that would bring solutions to the disease as quickly as possible. Marc Iverson had the vision and courage to found the CFIDS Association. Then under Kim McCleary’s leadership, she and the Association staff translated and prioritized the Board’s direction and input from the CFS community into a strategy and action. While all of this may not have occurred flawlessly, we all were pushing and driving to solve the puzzle of CFS. The truly courageous Board members were those who were sick and sacrificed their health in order to serve on the Board. I am still in awe of their determination and contributions.”
COCO CRUM, Nevada CFIDS Association Board of Directors, 1993–1998
1% Other
October 1992September 1992Kim McCleary, Tom Sheridan and patient Roy Snoeyenbos visit Capitol Hill for the first CFIDS Association Lobby Day. They request that four CFS-specific provisions be added to the NIH Reauthorization Bill. When it is signed into law by President Clinton four months later, it becomes the first law recognizing CFS.
The American Association for CFS (AACFS) is chartered as a not-for-profit organization with the help and financial support of Edward Taylor. The first international CFS conference is held in Albany, New York. The goals set forth by the AACFS at the first meeting are to bring together researchers, clinicians, health care workers, CFS support groups and patients to learn more about this illness through discussion, research, treatment and education.
At the AACFS conference, Dr. Robert Suhadolnik and colleagues from Temple University first release data indicating that people with CFS have an unusual form of RNase L, a key component of the antiviral defense system. In addition, Patricia Fennell first reports on her four-phase model of adaptation to CFS and other chronic illnesses. The Fennell Four-Phase Model is later validated through formal research.
Syndicated TV program The 700 Club features a segment on chronic fatigue syndrome. More than 30,000 calls are placed to the Association’s 800 number as a result.
October 1992 Late 1992
Tom Sheridan: Agent of Change Social work might seem an odd degree for someone who chose to enter politics. But Tom Sheridan’s first social work job created a bridge to community organizing and led him to refocus his career on social issues and politics.
“I was working with developmentally disabled adults and we needed to build a new community residence,” says Sheridan. “Nobody wanted it in their neighborhood, so I was asked to bring concerned citizens together and generate support for the home so the administrators could get the necessary permits and licenses. I found my passion for politics and my commitment to social policy in that effort.”
While working on his master’s degree, Sheridan started the political action committee for the National Association of Social Workers. Walter Mondale asked him to join his 1984 presidential campaign and Sheridan traveled the nation organizing voters. After four years spent combining electoral politics with social policy at the Child Welfare League of America, he led the lobbying efforts of the AIDS Action Council and chaired the effort on the Americans with Disabilities Act of 1990 and authored the historic Ryan White CARE Act.
When he started his firm, the Sheridan Group, in 1991, the CFIDS Action Campaign for the United States (CACTUS) was one of his first clients. “Our first meeting was in my kitchen,” he notes with a laugh. In 1992 after CACTUS closed, Sheridan was hired by the CFIDS Association and has been the chief architect of its public policy program since that time.
Working closely with president and CEO Kim McCleary and the Association’s Board of Directors and staff, Sheridan’s strategic approach has yielded many important victories for the CFS community, including the 1999 Social Security landmark ruling recognizing CFS as a disabling illness, the restoration of $13
million to the CFS research program at the CDC, chartering a federal CFS Advisory Committee, securing a $4 million Request for Applications from the NIH, helping convince the CDC to launch a $6 million public awareness campaign and hosting 15 successful Lobby Day events that have trained hundreds of advocates.
Now a national leader on domestic policy and legislative issues, he represents high-profile organizations like U2 front-man Bono’s Debt, AIDS, Trade and Africa (DATA) Foundation and One Voice Against Cancer, in addition to “underdog” clients that reflect his steadfast commitment to progressive issues.
Sheridan is proud of the record he’s helped the CFS community achieve, although he recognizes many frontiers still lie ahead.
“It’s been very rewarding to participate in the progress of this community, not only in terms of the wins we’ve experienced, but the maturing of advocates, growth of organizations and improved recognition for the disease itself. I have been fortunate to work on behalf of many different causes over the years, but I have never seen any group accomplish more with as little as the CFIDS Association has with its advocacy program. To represent this organization is not only an honor, it’s an inspiration.”
D e f i n i n g m o m e n T

18 The CFIDS Association of America 19Defining Moments: 20 Years of Making CFS History
scientific gatherings Key to Building momentum
Some of the most important contributions toward advancing research have been the multidisciplinary scientific gatherings and collaborations over the past 20 years. These events, sponsored and organized by groups including the International Association for CFS/ME, the CFIDS Association of America, the CDC and the NIH, have inspired ideas and partnerships that have broadened knowledge about CFS. One of the chief successes of these events has been in expanding the number, depth and breadth of scientists involved in CFS research and bringing new perspectives to the study of the cause(s) of and the objective diagnosis, effective therapeutic interventions and cure for CFS.
By the early 1990s research enthusiasm moved from pathogen identification to immune system dysfunction that could be caused by different infectious agents. This “final common pathway” theory was supported by studies published in the late 1980s by Drs. Nancy Klimas and Anthony Komaroff, who reported that natural killer cells that destroy virally infected cells didn’t function properly in people with CFS. HIV pioneer Dr. Jay Levy reported in 1991 that he had found CFS-associated immune abnormalities consistent with exposure to an infectious agent. In a similar study, the NIH’s Dr. Stephen Straus published findings of abnormal lymphocyte function in CFS patients.
In 1992 Dr. Robert Suhadolnik first reported that the activity of RNase L, an enzyme necessary for inducing interferon production in response to viral infection, was defective in immune cells from CFS patients. With funding from the CFIDS Association and the NIH, Dr. Suhadolnik discovered a new and unusual form of RNase L in people with CFS. RED Labs in Belgium later developed a commer-cial test for this novel form of RNase L.
Even with substantial high-quality scientific evidence of immune system abnormalities, in the absence of a known cause, the search continued and branched out into new areas. Dr. Mark Demitrack’s 1991 study showing that levels of the stress-response associated hormone cortisol were low in CFS brought attention to the endo-crine system and differentiated CFS from depression, which is characterized by high cortisol. In 1998 Dr. Peter Rowe established that many people with CFS have orthostatic intolerance, a type of autonomic nervous system dysfunction. Clinical-care pioneer Dr. David Bell found vestibular dysfunction in CFS. Neuroimaging studies by Drs. Benjamin Natelson, Ismael Mena and Irving Salit reported differences in brain blood flow. Cognitive function and exercise physiology studies by Dr. John DeLuca and Staci Stevens documented the CFS-related “brain fog” and symptom exacerba-tions following mental and physical activity.
These studies helped to further define the clinical spectrum of CFS. At the same time, the fact that differences were found in multiple systems throughout the body reflected the enigmatic and complex nature of this illness and how challenging it is to understand, diagnose and treat.
An important advance in the biologic and medical understanding of CFS came with the publication of the Human Genome Project in the early 2000s. Knowledge of the human genome sequence allowed investigators an “inside-out” approach to generating medical
diagnostics and therapeutics even without knowledge of a lesion, a target organ or a cause of a disease, as in CFS.
Using some of the new molecular tools generated by the human genome revolution, investigators including Drs. Suzanne Vernon of the CDC, Jonathan Kerr of London and Jonathan Gow of Glasgow demonstrated in 2005 that gene activity in blood cells from people with CFS is different from that of healthy controls. Importantly, these studies substantiated the earlier immune dysfunc-tion findings and implicated genes important for proper immune function. Genes important in the normal function of the hypothalamic-pituitary-adrenal (HPA) axis and cell metabolism also contained variations that weren’t found in healthy controls.
Investigations by Drs. Andrew Lloyd in Australia, Peter White in London and others across the globe also used the new molecular techniques, combined with basic epidemiology, to validate the early theories of postviral CFS, finding that infections with EBV, Ross-River virus and other pathogens are potent risk factors for developing CFS. In late 2006 Dr. Jose Montoya of Stanford linked CFS to HHV-6 and EBV infection and began a treatment study using a powerful antiviral, Valcyte. September 2007 brought a report from California infectious disease special-ist Dr. John Chia showing that 80 percent of CFS patients with chronic gastrointestinal symptoms have enterovirus present in stomach tissue. Yet, since all cases of CFS can’t yet be tied to an infectious onset, and effective treatment and a cure remain elusive, the research pursuit continues to move forward.
As we sit in the third decade of the CFS era, it’s almost as though the CFS research path has taken a circular course, as modern tools bring new evidence supporting the earliest theories of immune dysfunction and viral involvement. Infectious disease, immune, clinical, epidemiologic and genomic studies have provided a clearer view of CFS and its risk factors and precipitating triggers. This wouldn’t have been possible without the scientific advances of the 21st century—or without the concerted effort of a relatively small group of investigators who, even in the face of skepti-cism and ridicule from their peers, have dedicated their careers to understanding CFS.
May 1993March 1993Dr. Philip Lee, who is sympathetic to CFS because of patients he treated in his San Francisco practice, is installed as the country’s assistant secretary for health. He and his staff help advance CFS-related policy issues across the Department of Health and Human Services through the department’s CFS Coordinating Committee. Lee makes sure that patient advocates have a voice at the table, chartering the committee until his retirement in 1997.
The first CFIDS/ME Awareness Day is organized by patient advocate Tom Hennessey on May 12. The second CFS Lobby Day is held in conjunction with a meeting of the Association’s Public Policy Advisory Committee. The focus of the meeting is a report from the Sheridan Group detailing discrepancies in federal funding reports for CFS research.
Patients, doctors, advocates and researchers have consistently seen research as the path toward the grand prize: a cure for CFS supported by knowledge of the cause(s) and its pathophysi-ology and prevention. Like many such roads, the CFS research trail is riddled with gridlock, wrong turns and dead ends, but hope is high that, after 20-plus years of study and significant breakthroughs, scientists are on a clearer path toward under-standing this mysterious illness.
In 1984 and 1985 there were nearly simultaneous outbreaks of what is now known as CFS across the United States. In addi-tion to the highly publicized clusters in Incline Village, Nevada, and Lyndonville, New York, clinicians across the country were seeing an increased number of people with debilitating, fatiguing illness. In January 1985 Drs. James Jones and Stephen Straus each published articles in the Annals of Internal Medicine that described Epstein-Barr virus (EBV), the pathogen that causes infectious mononucleosis, as the cause of persistent illness and fatigue in adults.
When researchers couldn’t definitively link the common EBV to this new chronic illness, the CDC organized an international group that, in 1988, quickly published the first working case definition for CFS. Although the definition wasn’t perfect, it provided researchers with a valuable tool and a system-atic approach for identifying and characterizing patients for research studies.
Because these mid-1980s outbreaks had the characteristics of an infectious disease (and likely also because CFS emerged in the shadow of another prominent immune-related disease, HIV/AIDS), the early research course was set toward identifying CFS-associated pathogens. In 1987 the CFIDS Association wrote its first check—a $15,000 research grant made to Dr. Paul Cheney, allowing him to hire staff so that patient specimens could be collected and used to identify pathogens and to study immune function.
Most of the early research funds granted by the CFIDS Asso-ciation went toward identifying pathogens, particularly retro-viruses, through large grants to investigators including Drs. Elaine DeFrietas, Sidney Grossberg and John Martin. Human herpesvirus 6 (HHV-6) was also suspected and investigated as an etiologic agent of CFS. However, because HHV-6 (like EBV) is common in the general population and most infected people aren’t sick, it has been challenging to demonstrate a causal link with CFS.
Research
20 The CFIDS Association of America 21Defining Moments: 20 Years of Making CFS History
February 1994January 1994A supplement in the peer-reviewed journal Clinical Infectious Diseases is dedicated to CFS, with more than a dozen research papers by Drs. Robert Suhadolnik, Benjamin Natelson, Dedra Buchwald and others.
The CFIDS Support Network is established by the CFIDS Association to provide information and services to CFS support groups nationwide. The group holds its first meeting in October at the American Association for CFS (AACFS) conference in Ft. Lauderdale. By 1995 the network grew to include 280 member groups.
Early 1994February 1994Ann Landers responds to a question about CFS in her syndicated advice column, listing the CFIDS Association as an information source. The Association receives (and replies to) more than 50,000 requests for information from readers of her column.
Rebecca Moore, a 17-year-old from New York, forms the Youth Campaign for CFIDS Awareness. Later, she also forms the Pediatric Network for CFS with Mary Robinson, a parent activist with two children who have CFS.
THenSince the early years, the CFIDS Association has served as a government watchdog. In 1993 we led a six-year effort to document and hold the CDC accountable for funding des-ignated for CFS research. The effort paid off in 1999 when federal investigators reported that $12.9 million of the $22.7 million allocated to CFS between 1995 and 1998 had been diverted to other agency programs.
noWThe Association has been visionary enough to transform its adversarial relationship with the CDC into a more collab-orative one. This led to a giant leap forward in our efforts to educate physicians and other health care professionals about this disease when in 2002 we secured funding from the CDC for a five-year Provider Education Project whose curriculum was developed by CFS experts from around the country. Another huge victory was achieved in 2005 when we secured CDC funding to launch the first-ever national CFS public awareness campaign.
“In the late 1980s and early 1990s, many thought CFS was a yuppie flu-like illness, and early epidemiologic research by the CDC suggested that the illness was relatively uncommon. With funds from the CFIDS Association, my team was able to collect pilot data suggesting that the illness affected hundreds of thousands of people. That pilot study eventually enabled our group to receive NIH funding to do a large community-based study of the prevalence of CFS. We are very appreciative of the early funding support we received from the CFIDS Association.”DR. LEONARD JASON, Illinois DePaul University Center for Community Research
“It can be exhausting to educate all the teachers, school counselors, coaches and administrators your child comes in contact with about CFS, especially since the cast of characters changes each new school year, but the effort usually pays off. After all, it’s hard for school personnel to understand why your child needs special accommodations if they know nothing about the illness and its impact on cognitive and physical functionality.”MARY ROBINSON, New York Co-author of A Parents’ Guide to CFIDS
September 1993August 1993The CDC concludes its “four-city” surveillance study after four years. The study, which relies on physicians in four American cities to report diagnosed cases, grossly underestimates the number of people with CFS, suggesting that, at most, 20,000 people in the United States have the condition.
At a public meeting held at the CDC, the CFIDS Association begins publicly questioning the CDC’s use of its CFS budget. It would take five years, an agency whistleblower and dogged research by Kim McCleary to prove that the agency was diverting millions of CFS funds to other areas. At this meeting advocates also vocalize opposition to dropping symptom criteria from the CFS case definition as researchers begin work on a new definition.
Late 1993November 1993The NIH convenes a two-day workshop on CFS treatment. Patient advocate Wilhelmina Jenkins speaks eloquently about the lack of attention paid to racial minorities with CFS and to children with CFS; her daughter became ill at age 14.
The CFIDS Association provides grant funding to Dr. Leonard Jason of DePaul University to conduct a community-based study to estimate how many people have CFS. Jason’s study, published in 1995, finds that at least 400,000 Americans have CFS. This grant to Jason, like all the Association’s research grants, is funded through designated gifts from individual donors.
I’m often asked what drew me to the CFIDS Association. It was the fall of 1990, and I was pursuing a career change that would allow me the opportu-nity to do something more meaningful than contribute to corporate profits. I learned from a friend about the Association’s work and its search for someone to run the day-to-day operations. She also told me that chronic fatigue syn-drome was on the cover of Newsweek that week. Reading about the medical mystery CFS presented, and being introduced through that article to people whose lives were completely derailed by this condition, definitely piqued my interest.
But it was two meetings with Marc Iverson that instilled a passion for the cause I hadn’t anticipated. My own encounters with arrogant medical profes-sionals struck a chord of familiarity with the stories I heard from him and other CFS patients who had been treated dismissively during their search for a diagnosis. My communications training gave me an academic foundation in social policy change that I was eager to put to use in helping the Association
change how CFS was viewed by the public, the media, the medical community and scientists. And I wanted to give a voice to the many people too debilitated by CFS to advocate for themselves.
In spite of many demanding and trying times over the past 17 years, I have never looked back with regret on the job change that forever changed my life—and me. In the earliest days of my tenure, being a “healthy” person caused many within the community to question my credibility as an advocate for the cause. Conflict over research and media strategies, funding priorities, policy initiatives and name change made navigation difficult, but my resolve never wavered. During one such turbulent time, Board member Coco Crum insisted we ignore the roar and “keep our eyes on the prize”—the Association’s mission. Her sage advice still resonates today.
Another question I’m asked is why I stay. In part, it’s because I feel a commitment to finish what was begun in 1987 when this organization was created. But it’s mostly because of the people I’ve met through this organization whom I’d like to know healthy and restored. The courage and absolute determination I’ve witnessed in people whose lives have been affected by CFS is a con-stant inspiration in the work I’m honored to do on their behalf. To me, there’s no more important calling in the world.
Historical PerspectiveBy K. KIMBERLY McCLEARY President and CEO, CFIDS Association of America

22 The CFIDS Association of America 23Defining Moments: 20 Years of Making CFS History
Summer 1994Spring 1994The CFS Interagency Coordinating Committee (CFSICC), created in 1989, meets in Washington, D.C., this time with four “consultants” appointed by Assistant Secretary for Health Philip Lee. Kim McCleary, Marya Grambs, Orvalene Prewitt and Judy Basso gain a seat at the table with federal officials, but not a vote.
The CDC launches its San Francisco prevalence study, which ultimately gives the first evidence that certain racial minorities and those at lower income levels are at increased risk for CFS.
Spring 1995December 1994The CDC publishes its second case definition of CFS in the Annals of Internal Medicine. Led by CDC author Keiji Fukuda, the new definition provides more straightforward symptom criteria and acknowledges that CFS is an inadequate term, but the international working group that developed the definition fails to offer an alternative.
The CFIDS Association launches the CFIDS Public Relations (CPR) Team, organizing advocates to promote good press—and respond to bad press—about CFS.
“In the recent, often heated debate over the proposed name change, I’ve been heartened to hear thoughtful reasoning on both sides. I’ve been equally saddened when the debate degenerates into pointless attacks on the character of the debaters. As a disabled CFS patient of 15 years, I adamantly refuse to be counted among the mudslingers of CFS activism. If a person is angry about being incurably sick, I share that frustration; but when that anger is channeled into mudslinging and blame, then count me out. I am too weary and too sick to be involved in anything but intelligent, constructive dialogue.”LIZ BURLINGAME, Georgia CFS patient
How many Americans have CFS? Knowing how many people have an illness is a relevant factor in establishing the burden of a disease on the population and, hopefully, in determining the level of resources dedicated to combating it.
The first CFS prevalence estimates were based on asking doctors to report cases of CFS to the CDC, but since few doctors were making the diagnosis in the late 1980s and early 1990s, the official rate was pegged at 3,000 to 10,000 cases in the United States, considerably underestimating the public health impact of CFS.
The next wave of studies (in the mid-1990s) used a “community-based” model, where researchers, including Drs. Leonard Jason and Dedra Buchwald and CDC researchers, contacted a randomly selected group of people and asked them questions to determine whether they had symptoms of CFS, then conducted medical exams to rule out other possible causes. These studies suggested that between 200,000 and 800,000 American adults have CFS.
The most recent head-counting effort by the CDC, a study of CFS in Georgia, may increase the prevalence significantly—to four million Americans. But, while earlier studies were criticized for using a too-stringent definition of CFS and underestimating its magnitude, this latest study, released in summer 2007, has taken fire for using very loose criteria and diluting CFS by including people with other illnesses, including primary psychiatric disorders.
One thing is certain. CFS is not a rare disorder, as once was thought. And, as measurement methods continue to improve and efforts to expand awareness gain steam, the level of resources dedicated to fighting CFS should grow as well.Cf
s
Of the many debates associated with CFS—cause, treatments, cure, even its very existence—the issue that has generated the most controversy is the name of the illness. Patients, clinicians, researchers, even politicians, have weighed in on the debate. Although there has been wide recognition that the name chronic fatigue syndrome doesn’t adequately describe the sever-ity and complexity of the condition, the challenge has been in finding an alternative term embraced by the patient community, medical professionals and researchers—not just in the United States but around the world.
Because high levels of Epstein-Barr virus (EBV) were initially found in most of the ill patients in the Incline Village, Nevada, outbreak of 1984-85, the disease was first called chronic EBV (CEBV). Soon it was recognized that EBV failed to explain many cases of the illness in Nevada or in other parts of the United States, where it was being reported. A new way to define the illness was published in 1988 by researchers at the CDC, which coined the term chronic fatigue syndrome.
Even before this name was made official in 1988, it was controversial. United Kingdom researcher Dr. Melvin Ramsay pointed out that this “new” illness seemed to be the same thing that he and others had been calling myalgic encephalomyelitis (ME) since the 1950s. In November 1987 researcher Seymour Grufferman proposed the term chronic fatigue and immune dysfunction syndrome (CFIDS). Patient organizations, such as the Charlotte CEBV Association (precursor to the CFIDS Association of America), quickly instituted Dr. Grufferman’s recommendation in hopes of preempting the singular focus on fatigue.
The first official name change forum was held in 1989 at a conference hosted by the San Francisco CFIDS Foundation. The foundation was a member of the CFIDS Action Campaign for the United States (CACTUS), which made name change one of its top advocacy priorities in 1990. No CFS research confer-ence since has neglected to address the issue.
Politicians and federal appointees have also tried to shape the debate. The 1994 international case definition led by the CDC acknowledged the inadequacy of the name, but didn’t propose a new one. In 1996 Congress advised the secretary for health to consider renaming CFS. In 1998 Assistant Secretary for Health Phillip Lee announced at the American Association for CFS conference that he supported a name change.
The chief battleground for the name change issue, however, has been the Department of Health and Human Services’ CFS coordinating and advisory committees. Advocates, such as Roger Burns, who organized many name change initiatives in the 1990s, brought the issue before the committees on a regular basis, and the committees attempted to be responsive by forming multiple workgroups and subcommittees. In 2001 one such workgroup proposed the name neuroendocrineimmune dysfunction syndrome (NDS). A CFSCC workgroup survey of patients and health care professionals showed that 91 percent of
survey respondents favored a name change in general and two-thirds supported the NDS name. This overwhelming support for a name change was consistent with earlier surveys by Burns, the CFIDS Association and other groups.
The CFSCC was dissolved prior to submitting the name change committee’s recommendations, but the concept for NDS was presented to the new CFS Advisory Committee (CFSAC) at its first meeting in September 2003. The CFSAC responded by agreeing that CFS is a poor name, but declined to rename the illness in absence of a better understanding of its pathophysiol-ogy. The CFSAC’s response was loudly decried and many, including longtime patient advocates Tom Hennessey and John Herd, continued to work toward a name change.
Names such as Nightingale syndrome (after Florence Nightin-gale, who was reported to have a CFS-like illness) and Peter-son-Cheney-Bell disease (after the physicians who demanded recognition of clusters of CFS in their practices) have won favor among some patients. However, myalgic encephalomyelitis and myalgic encephalopathy have been the most popular.
Historically, doctors have been less supportive of the ME titles, saying there isn’t enough evidence to support terms that indicate muscle weakness or central nervous system disease, although this is changing as more studies of the central nervous system detect abnormalities. In addition, there is concern because many countries—and researchers—define ME differ-ently than CFS and may select a different patient population for research groups. Some argue that unless one of the definitions for ME is adopted with the name, and the CFS name disap-pears altogether, that ME and CFS should not be merged under one term.
CFS patient and entrepreneur Rich Carson convened a CFS Name Change Advisory Board of recognized CFS doctors and researchers in January 2007. The Advisory Board recommended use of the combined term CFS/ME, preferring the “encephal-opathy” variation of ME. At the same time, the International Association for CFS (IACFS), the scientific organization concerned with the illness, also adopted a new name to reflect its international scope, becoming IACFS/ME. A pediatric case definition published in early 2007 also used the term ME/CFS.
Following these announcements, disputes continue over which version of ME is most appropriate and how the combined term will affect (and be affected by) the different definitions for CFS and ME. And some advocates oppose time and energy being spent on the name change issue when two decades of work have failed to resolve the issue and diverted much-needed efforts from other important issues. Others believe the issue isn’t as critical as it once was, with initiatives like the national CFS public awareness campaign making inroads into how the public and health care professionals view the illness.
Time will be the real measure of how this challenging issue is ultimately resolved.
Name Change

24 The CFIDS Association of America 25Defining Moments: 20 Years of Making CFS History
Fall 1995June 1995The CDC links Gulf War illness to CFS, reporting that veterans of the first Gulf War have at least a four-fold higher rate of CFS compared to the general population. Also this year, the CDC includes CFS on its list of “priority one new and reemerging infectious diseases.” Ten years later, in June 2005, an Annals of Internal Medicine article reports that veterans of the 1991 Gulf War are 16 times more likely to develop CFS than nondeployed veterans.
The NIH’s National Institute of Allergy and Infectious Diseases (NIAID) renews funding for Dr. Benjamin Natelson’s CFS Cooperative Research Center and announces funding for a center led by Dr. Dedra Buchwald at the University of Washington. Funding for the Boston and Denver centers is not renewed.
September 1995Fall 1995Volunteers, including Roger Burns and Matt Strasnitskas, create the first CFIDS Association website.
Johns Hopkins researcher Peter Rowe and his colleagues publish a groundbreaking study in the Journal of the American Medical Association linking CFS to neurally mediated hypotension, a type of orthostatic intolerance involving a miscommunication between the brain and the heart with regard to blood flow. The finding generates considerable media attention, most of it acknowledging the seriousness of the illness, and provides a new way of looking at the science of CFS.
NIAID’s decision to establish three CFS Cooperative Research Centers was a tremendous stimulus to broad areas of research on the pathophysiology of CFS. Prior to our getting the New Jersey center, I was able to do limited research based on my clinical practice. After establishing the center, I was able to develop a broad research program that integrated work on autonomic and cardiovascular physiology with other work on cytokines and cognitive functioning.
A fabulous advantage of our center was that we were awarded $50,000 a year for innovative pilot projects. Every one of the mini-projects we funded ended up with data that appeared in the scientific literature, and about one third of them ended up with additional NIH funding.
I view NIAID’s decision to stop funding these centers as a disastrous moment for the goal of better understanding this disabling illness. Now CFS researchers have to compete for NIH funding against researchers studying cancer, AIDS and heart disease. Needless to say, this has impacted negatively on research output. Taking our center apart was one of the hardest things I have ever had to do. Many of my former colleagues are no longer CFS researchers, and the well-oiled machine I had built for CFS research is much smaller and operates with squeaks. However, I remain 100 percent committed to my patients and to continuing research to understand causes and to establish cures for this hard-to-treat illness.
Historical PerspectiveBy BENJAMIN NATELSON, MD UMDNJ–New Jersey Medical School
A lot of snail mail and e-mail is sent to the CFIDS Associa-tion every week. Address changes, support group referral requests, ideas for research or media initiatives, suggestions for what we should tell health care professionals about CFS, requests for information and help. The Association is lucky to have a dedicated staff to help address these tasks, execute long-term projects and maintain communication with all the people the organization serves.
The Association hired its first employee in 1989. When Kris Hopkins and Kim McCleary joined the staff in early 1991, there were four staffers who came into the office every day and one other person who worked mostly from home because she had CFS. The decision to hire McCleary as executive director was a controversial one. There were strong expectations that the novel retrovirus linked by Dr. Elaine DeFreitas to CFS would quickly lead to advances to solve the “bug and a drug” model of disease most embraced at the time. The Board questioned whether there would be a need for someone to help founder Marc Iverson run things if this research rapidly translated to treatment and wellness. There were also concerns that hiring someone who didn’t have the illness (or a family member with the illness) would weaken the reputation of this patient-led organization.
Over time, those concerns proved unfounded and the Association slowly added to its staff and replaced individu-als who moved on to other challenges. In all, there have been 58 employees of the CFIDS Association over the past 20 years; just 14 are on staff today. No one on staff has CFS, and McCleary is the only staff member who has family with CFS, an outcome of her marriage to Kofi McCleary, whose mother, Wilhelmina Jenkins, and sister, Kamilah Konrad, both have the illness.
April 1995Spring 1995By 1995 the CFIDS Association employs eight staff members to execute plans approved by the Board of Directors, and the Resource Line (704-365-2343) is established by the Association to give people a way to talk directly to a staff person. The new phone number addresses a common patient frustration about the voice-mail-only 800 number—“How can I talk to a real person?” The Resource Line is still functioning today, thanks to contributions from donors.
The Food and Drug Administration (FDA) and the NIH co-sponsor a workshop on clinical endpoints in treatment research, working to determine ways of measuring the effectiveness of CFS treatments.
May 1995May 1995On May 12 the CFIDS Association hosts the first congressional briefings about CFS with sponsorship from Sen. Harry Reid (Nevada) and Rep. John E. Porter (Illinois). Patients Wilhelmina Jenkins and Sean Tracy and researchers Drs. Mark Loveless and Anthony Komaroff testify. Dr. William Reeves of the CDC also testifies, reporting that new CFS prevalence data shows the “yuppie flu” label is inaccurate. The third Lobby Day is held with 16 advocates meeting with staff of 58 congressional offices.
The Youth Campaign for CFIDS Awareness comes under the CFIDS Association umbrella and is renamed CFIDS Youth Alliance. Its newsletter, Youth Allied by CFIDS, publishes its first issue in September.
One of the strengths of our staff is the tremendous sense of commitment to the mission that each member feels, and that they collectively share. This is demonstrated in many differ-ent ways, but certainly one measure is the combined years of service to this community—more than 107 years of Association experience are represented among these 14 people. Remarkably in such a small staff, 7 individuals have served the Association for 10 years or more. They are acknowledged below:
• Nova Bouknight (1993-present) • Jamie Davis Giuliani (1994-2007) • Kristina Hopkins (1991-present) • Lois Infanti (1997-present) • Kimberly McCleary (1991-present) • Gloria Smith (1996-present) • Vicki Walker (1993-2003 and 2007)
The Staff
THen In the beginning, the CFIDS Association operated out of a room above Marc Iverson’s garage. It was a big moment when we moved into a “real” office, which was modest rental space. By 1991, when there were only 5 paid staffers, that office was already filled to capacity.
noW It still surprises visitors to see just how modest our offices are. Although we’ve moved into larger rental space than we had in 1991, our facility is hardly luxurious. The carpet is threadbare, the walls could use a coat of paint, and we are once again at capacity, with every nook and cranny filled with people, boxes, supplies and all the essentials of running the organization. We have 14 people on staff now instead of 5, but our philosophy is the same. Just like in the early days, we’d rather spend our limited resources on programs and people than on expensive “corporate digs.”
THen In 1995 when the first CFIDS Association website was developed, the site was very small. It was largely comprised of Association brochures and flyers posted on the Internet, making it easier for people to access the Association’s materials and for the Association to connect with people with CFS. In 2001 the Association revamped its website to better serve the information needs of patients, their families and health care professionals.
noW Today, more than 1,500 pages of information about CFS are available at www.cfids.org. In 2006 alone, 1.56 million people visited our site, a fraction of the millions of individuals who have visited the site since it was first posted more than a decade ago.

26 The CFIDS Association of America 27Defining Moments: 20 Years of Making CFS History
March 1996December 1995The San Francisco CFIDS Foundation closes. The foundation was one of the first CFS advocacy groups; its leaders, Marya Grambs and Jan Montgomery, were instrumental in the formation of the CFIDS Action Campaign for the United States (CACTUS) and in guiding the CFIDS Association’s early public policy activities. The organization also was responsible for creating the first CFS clinic at the University of California-San Francisco with help from clinicians Jonathan Rest and Dan Peterson and researcher Jay Levy.
Osler’s Web is published, completing a nine-year effort by author Hillary Johnson to document the early history of CFS, particularly focusing on the government’s paltry response to the illness. Johnson promotes the book, which was partially funded by the CFIDS Association, on ABC’s Good Morning America and other national media outlets. Johnson’s assertion that CFS is a “contagious brain disease” elicits deep worry from patients, who fear that they will be ostracized by family and friends, and from doctors, who find no scientific evidence for her statements.
May 1996May 1996Michelle Akers testifies before Congress, eloquently describing the life-altering impact of CFS. Three months later, in August, Akers and the U.S. Women’s Soccer Team win Olympic Gold in Atlanta. Beginning in 1995, Akers had publicly disclosed her battle with CFS and her extraordinary efforts to continue playing in spite of its disabling effects. She became the first star athlete and celebrity widely associated with CFS.
Youth activist Rebecca Moore and Dr. Peter Rowe of Johns Hopkins provide testimony about pediatric CFS at the CFIDS Association’s second congressional briefings. The briefings are held in conjunction with the fifth CFIDS Lobby Day.
“In the early 1990s, most people thought that pediatric CFS, if it existed at all, was rare. Many of the kids with CFS were isolated from their peers, dependent on parents and unable to pursue independence the way a typical teen would do. Then we found each other and stood up to say, ‘We exist and we speak for ourselves and for those who are too ill to participate.’”REBECCA MOORE, New York CFS activist
“My name is Michelle Akers. I am 51́0˝ and weigh 150 pounds. I am muscular. I am tan. I love to laugh. On vacations, I love to hike in the Cascade Mountains near Seattle with my dad and brother. I am the starting center forward for the world-class American soccer women’s team . . . and soon to be a 1996 Olympian. If you saw me today, you would see a healthy, physically fit, elite athlete.
“But I’m not. I am sick. Some days it is all I can do just to get through the day. On the very bad days . . . I drag myself off the field, my legs and body like lead. My breathing is labored. It is all I can do to get to the locker room, change my clothes and keep from crying in utter exhaustion and weariness. I am light-headed and shaky. My vision is blurred.
“I tell you these things not to gain sympathy, but so that you too can experience a day in the life of someone with this illness . . . CFS is a devastating disease.”MICHELLE AKERS, Florida Olympic Gold Medalist, taken from her 1996 testimony to Congress
Youth Activism
Twenty years ago, you might have expected that children and youth with CFS wouldn’t have had trouble being noticed, given that most of the patients in the 1985 Lyndonville, New York, outbreak were children.
However, despite the diligent efforts of their doctor, David Bell, and physicians like Dr. Charles Lapp in other areas of the United States, the notion that children and adolescents got CFS was often met with skepticism. Even more than the adults struggling for recognition, they were called school phobic, “just depressed” or shirkers. Their parents were sometimes accused of Munchausen syndrome by proxy, a psychiatric condition in which parents deliberately make their children ill, or of pushing their children so hard that they faked illness to escape the pressure.
In 1994 this began to change, thanks to the Herculean efforts of a girl with CFS. Rebecca Moore, 17 years old and virtually homebound with CFS, launched the Youth Campaign for CFIDS Awareness with a letter-writing campaign to President Clinton, asking for his help for young people with CFS. She used the CFIDS Chronicle, pen-pal organizations and local support groups to spread information about the letter-writing campaign, gaining participation from people across the United States.
Moore’s persistence, earnestness and intelligence, as well as her talent for drawing people to her, made the campaign blossom. In 1995 the Youth Campaign came under the CFIDS Associa-tion’s umbrella, becoming the CFIDS Youth Alliance, with its own newsletter, Youth Allied by CFIDS. Moore and other talented youth leaders, notably Sandy Becker, Sharon Walk, Heather Freese, Emilie Sutterlin, Jenn Waterman, Catherine Matheny and Connie Howard, as well as parent leaders Karen Lang, Michelle Banks, Mary Robinson, Lynn Vanderzalm and Frank Albrecht, produced the newsletter; ran websites, chat rooms and a pen-pal program; managed advocacy campaigns; and challenged the medical establishment, government officials and popular opinion.
In April 1996 more than 100 members of the CFIDS Youth Alliance and their supporters gathered in Washington, D.C.,
Rebecca Moore, Jenny Luray, Suzanne Connelly-Myers, Dr. Peter Rowe, Jerry Crum, Dr. Nancy Klimas and Kim McCleary on Capitol Hill in April 1996.
to attend a federal CFS Interagency Coordinating Committee (CFSICC) meeting. Six youth and parents testified before the CFSICC, shining a spotlight on the unique issues facing them. They also brought dozens of letters written to Assistant Secre-tary for Health Dr. Philip Lee in support of their cause.
These and other efforts led directly to scientific meetings about pediatric CFS held by the CDC in February 1998 and by the (renamed) CFS Coordinating Committee (CFSCC) in April 1998. The daylong “State of the Art Workshop on CFS in Adolescents” hosted by the CFSCC attracted participation by
dozens of federal, university and private-sector scientists and clini-cians. These included Dr. Peter Rowe, whose research on orthos-tatic intolerance in CFS had been a groundbreaking finding for all people with CFS, and particularly adolescents, who were a major focus of his research and clinical practice.
In 1998, citing the difficulty of engaging children and adoles-cents, most of whom were too sick to help run the organization and/or who wanted to be considered as “normal” as possible by their healthy peers, the CFIDS Youth Alliance ceased to exist as a sepa-rate organization and its activities were integrated into the CFIDS Association umbrella.
The impact of the CFIDS Youth Alliance has been significant, even a decade later. As a result of their pressure, more research-ers, such as Drs. Leonard Jason and Renee Taylor, have joined the field. The early battles among scientists about whether children and adolescents can even get CFS are long past, and in 2007 the International Association for CFS/ME published a clinical definition for pediatric ME/CFS, recognizing some of the ways the illness differs in kids compared to adults.
Today young patients like 13-year-old Brian Bernard, a partici-pant in the CFIDS Association’s national CFS public awareness campaign photo exhibit, have taken up where the early youth advocate leaders left off. And groups like the Pediatric Network for CFS, Fibromyalgia and Orthostatic Intolerance, New Jersey CFS Association, Connecticut CFIDS Association, the United Kingdom’s Association of Youth for ME and the CFIDS Association of America continue to provide support, advocacy and information for children with CFS and their families.

28 The CFIDS Association of America 29Defining Moments: 20 Years of Making CFS History
May 1997April 1997The Social Security Administration (SSA) reports to a joint SSA-CFIDS Association study group that its own internal investigation shows it has mishandled CFS disability claims. Work begins on a new policy that will more effectively guide the review process for applicants disabled by CFS.
The first-ever Capitol Hill rally for CFS is organized on May 12, CFIDS Awareness Day, by patient advocate Mary Schweitzer. Lobby Day attendance this year jumps three-fold, with 65 advocates finding overwhelming support in the 75 congressional offices they visit on May 15. Congressional briefings on May 16 include presentations from pediatric researcher Dr. Karen Jordan, RNase L investigator Dr. Robert Suhadolnik, patient and parent Karen Lang, patient Iris Ramer and the NIH’s Dr. John LaMontagne.
May 1997May 1997The first meeting of the CFS Coordinating Committee (CFSCC), convened by the Department of Health and Human Services the prior September, is held. Public members of the CFSCC, which replaced the CFSICC that had operated since 1989, were CFIDS Association head Kim McCleary, patients Jerry Crum and Kristin Thorson, attorney Aba Heiman, and researchers Dedra Buchwald, Nancy Klimas and Anthony Komaroff.
After nearly eight years of study, Ampligen receives “cost recovery” status from the FDA, allowing patients to pay to receive the drug. The cost is reported to be $20,000 per patient for the 40-week open-label trial. The following summer the FDA approves both an expansion of the cost-recovery trial and a new double-blind, placebo-controlled phase III trial for Ampligen. AIDS activists petition for approval of Ampligen in hopes of getting access to it. Ten years later, Ampligen still hasn’t been approved for the treatment of CFS.
Still No FDA-Approved Drug for CFS In contrast to the important scientific advances made in understanding CFS, development of effective pharmaceutical treatments lags significantly. In fact, there is still no FDA-approved drug for the treatment of CFS, although many drugs are used to manage symptoms.
Several drugs have been tested in CFS, but none have proven to be very effective in eliminating CFS symptoms. The drug that has undergone the most clinical study is the immunomodulator Ampligen, which has been under investigation in CFS since 1988. It was submitted for marketing approval in 2007 and awaits a decision by the FDA. There have been experiments with other drugs, notably fludrocortisone (Florinef), hydrocortisone, modafinil (Provigil) and several antidepressants, on the basis that CFS shares symptoms with the conditions the treatments were designed for, like orthostatic intolerance, low cortisol, daytime sleepiness, fatigue, low mood and poor sleep quality. Some of these drugs also act on the immune system and hormones, contributing to researchers’ desire to study them as CFS treatments.
One issue that has hindered treatment studies is the difficulty in establishing accurate endpoints for measuring whether a treatment is effective. Some treatment studies use criteria such as ability to work, quality of life or immune function, but it’s arguable whether any single measure—or even a combination of measures—can accurately assess recovery or improvement in a complex, multisystem illness like CFS. Without knowing the underlying cause or pathophysiology of CFS, it’s very difficult to determine whether a treatment is positively (or negatively) impacting the disease itself.
Research advances from gene studies conducted in the last five years, and recent data showing that CFS affects at least one million Americans—and is therefore a larger (and potentially more lucrative) market than previously recognized—provide hope that scientists will discover more effective treatments (or combination of treatments) for CFS within the next several years. Until that time, patients and their clinicians remain dependent upon a variety of symptom-based treatments and lifestyle modifications to improve their health.
“The 1997 Washington rally was held to honor the request of CFS patient Joan Irvine, who committed suicide because she didn’t think she could bear the physical pain she was in, given the years that stretched in front of her with continued public ignorance and dismissal of this illness. And we were frustrated because we felt invisible—invisible within our communities, invisible in the medical world, even invisible to our patient advocacy organizations.”MARY SCHWEITZER, Delaware CFS patient and advocate
Fall 1996August 1996CFS patient Judith Curran commits an assisted suicide with Dr. Jack Kevorkian, launching a firestorm of controversy and a story on Dateline NBC. Her death is followed by the June 1997 Kevorkian-assisted death of CFS patient Janis Murphy.
The name-change debate continues. Congress directs the secretary for health to consider renaming CFS in its annual fall appropriations bill.
Spring 1997Noted feminist Elaine Showalter publishes Hystories: Hysterical Epidemics and Modern Culture, in which she claims CFS, Gulf War illness (GWI) and other conditions are forms of “mass cultural hyste-ria” caused by media coverage. Her thesis doesn’t, however, stop her from seeking media attention; she promotes her book in news outlets such as Good Morning America, Newsweek and Rolanda. Her book fuels myths about CFS and makes the task of increasing public under-standing even harder.
Late 1996Dr. Dedra Buchwald reports that patients with both CFS and fibromyalgia (FM) are substantially more disabled than patients with either condition alone. During the 1990s, research from multiple investigators shows that CFS shares symptoms with other syndromes that overlap with CFS, including FM, irritable bowel syndrome (IBS) and multiple chemical sensitivity (MCS). This not only complicates research, it makes diagnosis and management of these illnesses more difficult for medical professionals.
“Personally, I have no problem with the term CFS. I think the way the media, medical practitioners and other professional bodies portray the illness is more important than giving it a serious-sounding medical name. I refer to the illness as CFS rather than ME, although I have friends who insist on the name ME. I have found that most people have at least heard of CFS and have some limited understanding that it’s a nasty illness.”CAROLYN GEE, Australia CFS patient
“Federal support is crucial for CFS research, not only because progress cannot be made without it, but because research underscores the credibility and rigor of the CFS research enterprise. Support for CFS research also lends credibility to the disease itself. Perhaps most importantly, in a disease without a marker or uniformly effective treatment, patients’ future health is inextricably linked to the hope held by new and better science.”DR. DEDRA BUCHWALD, Washington University of Washington
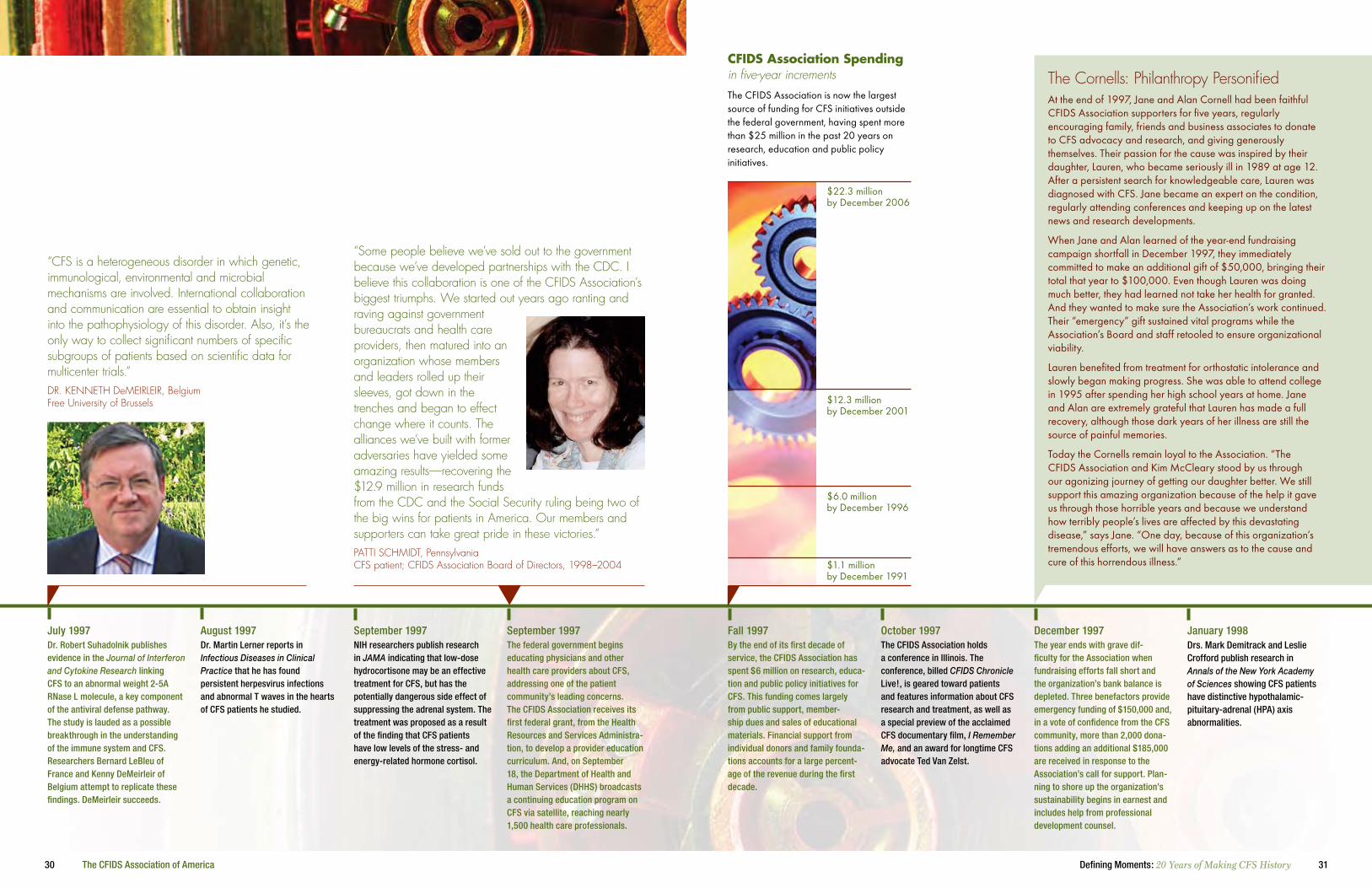
30 The CFIDS Association of America 31Defining Moments: 20 Years of Making CFS History
October 1997Fall 1997By the end of its first decade of service, the CFIDS Association has spent $6 million on research, educa-tion and public policy initiatives for CFS. This funding comes largely from public support, member-ship dues and sales of educational materials. Financial support from individual donors and family founda-tions accounts for a large percent-age of the revenue during the first decade.
The CFIDS Association holds a conference in Illinois. The conference, billed CFIDS Chronicle Live!, is geared toward patients and features information about CFS research and treatment, as well as a special preview of the acclaimed CFS documentary film, I Remember Me, and an award for longtime CFS advocate Ted Van Zelst.
January 1998December 1997The year ends with grave dif-ficulty for the Association when fundraising efforts fall short and the organization’s bank balance is depleted. Three benefactors provide emergency funding of $150,000 and, in a vote of confidence from the CFS community, more than 2,000 dona-tions adding an additional $185,000 are received in response to the Association’s call for support. Plan-ning to shore up the organization’s sustainability begins in earnest and includes help from professional development counsel.
Drs. Mark Demitrack and Leslie Crofford publish research in Annals of the New York Academy of Sciences showing CFS patients have distinctive hypothalamic-pituitary-adrenal (HPA) axis abnormalities.
The Cornells: Philanthropy Personified At the end of 1997, Jane and Alan Cornell had been faithful CFIDS Association supporters for five years, regularly encouraging family, friends and business associates to donate to CFS advocacy and research, and giving generously themselves. Their passion for the cause was inspired by their daughter, Lauren, who became seriously ill in 1989 at age 12. After a persistent search for knowledgeable care, Lauren was diagnosed with CFS. Jane became an expert on the condition, regularly attending conferences and keeping up on the latest news and research developments.
When Jane and Alan learned of the year-end fundraising campaign shortfall in December 1997, they immediately committed to make an additional gift of $50,000, bringing their total that year to $100,000. Even though Lauren was doing much better, they had learned not take her health for granted. And they wanted to make sure the Association’s work continued. Their “emergency” gift sustained vital programs while the Association’s Board and staff retooled to ensure organizational viability.
Lauren benefited from treatment for orthostatic intolerance and slowly began making progress. She was able to attend college in 1995 after spending her high school years at home. Jane and Alan are extremely grateful that Lauren has made a full recovery, although those dark years of her illness are still the source of painful memories.
Today the Cornells remain loyal to the Association. “The CFIDS Association and Kim McCleary stood by us through our agonizing journey of getting our daughter better. We still support this amazing organization because of the help it gave us through those horrible years and because we understand how terribly people’s lives are affected by this devastating disease,” says Jane. “One day, because of this organization’s tremendous efforts, we will have answers as to the cause and cure of this horrendous illness.”
The CFIDS Association is now the largest source of funding for CFS initiatives outside the federal government, having spent more than $25 million in the past 20 years on research, education and public policy initiatives.
CfiDs Association spending in five-year increments
$22.3 million by December 2006
$12.3 million by December 2001
$6.0 million by December 1996
$1.1 million by December 1991
August 1997July 1997Dr. Robert Suhadolnik publishes evidence in the Journal of Interferon and Cytokine Research linking CFS to an abnormal weight 2-5A RNase L molecule, a key component of the antiviral defense pathway. The study is lauded as a possible breakthrough in the understanding of the immune system and CFS. Researchers Bernard LeBleu of France and Kenny DeMeirleir of Belgium attempt to replicate these findings. DeMeirleir succeeds.
Dr. Martin Lerner reports in Infectious Diseases in Clinical Practice that he has found persistent herpesvirus infections and abnormal T waves in the hearts of CFS patients he studied.
September 1997September 1997NIH researchers publish research in JAMA indicating that low-dose hydrocortisone may be an effective treatment for CFS, but has the potentially dangerous side effect of suppressing the adrenal system. The treatment was proposed as a result of the finding that CFS patients have low levels of the stress- and energy-related hormone cortisol.
The federal government begins educating physicians and other health care providers about CFS, addressing one of the patient community’s leading concerns. The CFIDS Association receives its first federal grant, from the Health Resources and Services Administra-tion, to develop a provider education curriculum. And, on September 18, the Department of Health and Human Services (DHHS) broadcasts a continuing education program on CFS via satellite, reaching nearly 1,500 health care professionals.
“Some people believe we’ve sold out to the government because we’ve developed partnerships with the CDC. I believe this collaboration is one of the CFIDS Association’s biggest triumphs. We started out years ago ranting and raving against government bureaucrats and health care providers, then matured into an organization whose members and leaders rolled up their sleeves, got down in the trenches and began to effect change where it counts. The alliances we’ve built with former adversaries have yielded some amazing results—recovering the $12.9 million in research funds from the CDC and the Social Security ruling being two of the big wins for patients in America. Our members and supporters can take great pride in these victories.”PATTI SCHMIDT, Pennsylvania CFS patient; CFIDS Association Board of Directors, 1998–2004
“CFS is a heterogeneous disorder in which genetic, immunological, environmental and microbial mechanisms are involved. International collaboration and communication are essential to obtain insight into the pathophysiology of this disorder. Also, it’s the only way to collect significant numbers of specific subgroups of patients based on scientific data for multicenter trials.”DR. KENNETH DeMEIRLEIR, Belgium Free University of Brussels

32 The CFIDS Association of America 33Defining Moments: 20 Years of Making CFS History
July 1998July 1998CFS patients Wilhelmina Jenkins and her daughter, Kamilah Neal, appear on the Oprah show on July 28 as part of a program on “hard to diagnose conditions.” They talk about their battles with the illness and help raise awareness of CFS. But for patients who believe that “just getting CFS on Oprah” would magically transform the public’s understanding of the illness, it was a lesson in the realities of modern media. One show, no matter how influential, isn’t enough. It takes sustained, positive media coverage to change hearts and minds.
National Public Radio’s Diane Rehm devotes a show to CFS. Guests include the NIH’s Stephen Straus, CDC’s William Reeves, Drs. Paul Levine and Marsha Wallace, and patients Terry Hedrick and John Ginsberg.
October 1998October 1998A highlight of the American Association for CFS (AACFS) conference in Boston is Assistant Secretary for Health Philip Lee declaring his support for a CFS name change. Also, the CDC reports on its research showing that CFS is 20 times more common than its previous studies found, a story covered nationally by Reuters.
The United States medical coding system, ICD-9CM, creates a code for CFS under the category “Signs and Symptoms.” Advocates protest that the National Center for Health Statistics, which oversees the American system, should have adopted the international code in ICD-10, which places CFS with ME in the nervous system diseases category.
In 1998 years of questioning and research into CFS spending at the Centers for Disease Control and Prevention (CDC) reached a flash point. A series of public meetings provided opportunities to document conflicting answers to detailed questions about funding practices. At an April 29 meeting of the CFS Coordinating Com-mittee, CFIDS Association president and CEO Kim McCleary asked the CDC’s Brian Mahy about reported 1996 expenditures for lab studies, a year when no lab studies were conducted. Mahy called on his subordinate, William Reeves, to back his story that lab studies had been done that year, but Reeves refused.
Three months later Reeves, who was protected under the Whistle-blower Protection Act, and McCleary went to Capitol Hill and Health and Human Services auditors with documentation showing that actual spending for CFS research was less than what the CDC had reported to Congress.
Dr. Terry Hedrick, former assistant comptroller for the govern-ment’s General Accountability Office and later a member of the Association’s Board, recalls the era. “By 1998 we had collected enough documentation to warrant formal investigation by authori-ties, but would they believe us? Dr. Reeves came forward with his internal records and it seemed impossible that the federal watch-dogs could ignore such major discrepancies. Fortunately, when we presented all the evidence together, the appropriate investigations were launched.”
An Inspector General (IG) investigation followed immediately and a Government Accountability Office (GAO) audit commenced a year later. The IG report released on May 12, 1999, documented $12.9 million in funds spent on other diseases but reported to Congress as CFS expenditures. Congress directed the CDC to restore all the funds to the CFS program over a five-year period beginning in 2000.
The budget expansion enabled broader studies of prevalence, new clinical investigations, enhanced lab studies and activities dedi-cated to educating health care professionals about the diagnosis and management of CFS. Just as important was the enhanced clout of McCleary and other CFS advocates, both on Capitol Hill and the CDC campus, as vigilant watchdogs over federal funds.
“My daughter, Kamilah Konrad, and I were anxious about presenting CFS accurately to a huge viewing audience, especially after the tiring trip from Atlanta to Chicago. But Oprah and her staff were very reassuring and sympathetic to our needs, and we had one another to lean on—literally and figuratively! Dr. Nancy Snyderman, who also appeared on the show, helped explain the reality of CFS. It was very empowering for both of us to be taken seriously by such influential media personalities, and I hope we did a service for all patients.”
WILHELMINA JENKINS, Georgia CFS patient; spokesperson for the CFS public awareness campaign; CFIDS Association Board of Directors, 1996–2000
February 1998February and April 1998As a result of effective advocacy by CFIDS Youth Alliance members and CFIDS Association leaders, government agencies turn to the science of pediatric CFS. The CDC does so with a February panel discussion featuring some of the nation’s top experts, and the CFS Coordinating Committee (CFSCC) follows up with an April workshop with 21 scientists participating.
“Dear Abby” includes a letter in her advice column from a woman whose sister committed suicide because of chronic fatigue syndrome. Many CFS patients and supporters replied to Abby after reading the column, and she publishes a follow-up letter from CFS patient Thomas Smith in April 1998.
April 1998Spring 1998Studies of the link between CFS and orthostatic intolerance (OI) gain steam. Dr. David Bell and the “father of orthostatic intolerance research,” Dr. David Streeten, link low blood volume to CFS. And NIH and Johns Hopkins researchers collaborate on a study of fludrocortisone treatment for CFS. Fludrocortisone is a steroidal treatment for OI.
The CDC is formally accused of misappropriating CFS research funds after a historic showdown at a CFSCC meeting, in which Kim McCleary accuses CDC administrator Brian Mahy of reporting to Congress CFS expen-ditures that were never made. His subordinate, CFS research group head Dr. William Reeves, denies that Mahy’s statements are accurate. In July Dr. Reeves brings evidence to Congress of the diversion of funds, seeking protection under the Whistleblower Protection Act. The story is covered by the Associated Press and Congressional Quarterly.
In some ways the high-water mark of CFS advocacy was the CDC funding scandal. That scandal really rocked the CDC’s world; nothing of that sort had ever happened to that respected institution before. By the time it was over, the CFS research program was put on tight oversight and CFS got an enormous amount of publicity. The scandal wasn’t all good news; it apparently generated a lot of bad blood. Some people there will never forgive Dr. Bill
Reeves for the embarrassment his testimony caused. But it was a remarkable achievement.
Ironically, one could make the argument that the shenanigans of the late 1990s helped CFS more than they hurt it. They got CFS into the news in a big way, we got all the money back that was taken from us, and the program was put under the direc-tion of a vigorous researcher who took advantage of technology not available during the late 1990s. Dr. Bill Reeves may or may not be right in his approach, only time will tell, and he definitely ruffles feathers from time to time, but he is undoubt-edly engaged and interested in the subject—something we did not have before. One could also argue that the current national public awareness/media campaign would never have taken place without the CDC scandal.
Historical PerspectiveBy CORT JOHNSON CFS Phoenix (http://phoenix-cfs.org)
Dr. William Reeves of the CDC
CDC Exposed
D e f i n i n g m o m e n T
The CDC/CFIDS Association press conference that jump-started the CFS media campaign in November 2006 may turn out to be a watershed moment in the history of CFS. There can’t be many more impactful ways for CFS to gain legitimacy than having the director of the CDC and the assistant secretary for health stand up and announce to the world that CFS is a real and serious disease. The fact that this came just six or seven years after the CDC was taken to the mat by Congress for lying about its misuse of CFS funds only helped matters. To go from chief skeptic to promoter in this amount of time is little short of amazing.
Kimberly McCleary of the CFIDS Association
34 The CFIDS Association of America 35Defining Moments: 20 Years of Making CFS History
Since the dawn of the CFS era, computers have been vital to keeping people with CFS in touch with one another and engaged in the world. For those who are often bed- or home-bound due to their illness, electronic communication makes it possible to keep up with friends and colleagues, stay aware of local, national and world news events, and even work and shop without expending the energy they would need to go out into the world.
The people involved in the earliest days of CFS online networking—such as John Kossowan, Molly Holzschlag, Roger Burns, John (Friedlich) Herd, Maryka Ford and Marc-Alex-ander Fluks—became some of the most vocal early activists. They launched and propagated many of the earliest advocacy initiatives, banging the drum for more research, a new name for CFS and better understanding of the illness that had taken so much of their lives away.
The evolution started on September 1, 1988, when SYSOP (system operator) John Kossowan and a small group of his fellow patients launched the CFIDS Computer Bulletin Board, a plain-text discussion and information board. During prearranged times several days each week, they would dial their modems into the bul-letin board to chat with one another, comparing notes on the latest treatment strategy or research finding.
By the early 1990s, CFS chat rooms were springing up on commercial online services like CompuServe, Genie, Prodigy, Delphi and, later, America Online, and e-mail was starting to find wider use. This led to the growth of Usenet listservs, notably Roger Burns’s CFS-L, launched in 1992, which used e-mail to disseminate general CFS-related information, and CFIDS-L, which focused on advocacy. As CFS online com-munication became more common, people like Patti Schmidt, Gayle Babykin, Ray Colliton, Mary Schweitzer, Ed Isenberg, Rona Halpern and others joined (and, in some cases, replaced) the early online leaders, helping run the existing groups and forming new groups such as WE-CAN, CPAR, ME-Web and Co-Cure.
A group of volunteers created the first CFIDS Association website in 1995, making it easier for people to access the Association’s materials and for the Association to connect with people with CFS. By the late 1990s, the Association began transitioning its CFIDS Activist (C-ACT) program from a mail-based to an e-mail alert system because of the speed and pervasiveness of e-mail, not to mention the increasing cost of postal mail. A similar media alert system, CFIDS Public Rela-tions (CPR) Team, was launched to engage activists in respond-ing to bad press or applauding the rare (in that era) positive news story about CFS.
The turn of the century brought further maturation in the online effort, particularly for the CFIDS Association. Until the late 1990s, the Association had been hesitant to embrace the Internet revolution. The reason was simple and sound: many people with CFS didn’t have (at the time) computers and Internet access in their homes and Association leaders believed it was unfair for people with computers to have access to more information than those without Internet access.
As computers became mainstream household appliances, the Association started a major online initiative. A redesign of www.cfids.org launched in 2001, with new Web-specific infor-mation and interactive features, including a quiz to help visitors determine whether they might have CFS. In late 2002 the monthly e-newsletter CFIDSLink debuted and now reaches more than 20,000 subscribers. In 2003 the Association’s Provider Education Project, a collaborative effort with the CDC, started training medical professionals and created an online self-study course with continuing medical education credits.
In April 2004 the CFIDS Association launched the Grassroots Action Center, a place for CFS activists to easily and effectively communicate with elected officials, federal agency representa-
tives and the media about CFS-related issues. Through the Grassroots Action Center, advocates can also register to receive regular updates and Action Alerts for timely oppor-tunities to express concern or thanks to decision makers and thought leaders.
My Cause, an online tool people can use to create their own web pages, tell friends and family members about CFS and to raise funds for the Association’s programs, started in 2006. To date, nearly $45,000 has been raised with My Cause.
And 2007 brought the first CFIDS Association webinars, offering real-time virtual education seminars over the Internet.
Nowadays online support groups have largely taken on the role of the local support group. Websites, including Phoenix Rising, Co-Cure, ImmuneSupport and www.cfids.org,
provide information and understanding 24/7 to people who often can’t leave their homes due to CFS.
Twenty years ago it would have been impossible to imagine how the Internet has changed how we communicate today. Today it’s impossible to think of living without it. The achievements of the CFS community and the progress in research, understanding and awareness likely would have been unattainable without the ability to rapidly engage thousands of concerned people. Whether used to examine how the government spends its CFS dollars, communicate the latest research or clinical advance, facilitate action or reach out for understanding, the Internet has both informed and trans-formed the CFS community.
Early 1999Late 1998The CFIDS Association starts the Founder’s Circle (later renamed the Chairman’s Circle), a monthly giving program allowing support-ers to donate money each month through automatic credit card charges. Chairman’s Circle members also receive a special newsletter in thanks for their ongoing support.
The CFIDS Association ramps up its efforts to stop deceptive tactics of long-term disability carriers in unfairly denying or terminating benefits to CFS patients by providing testimony on ERISA reform to Con-gress and the Department of Labor. ERISA is the federal law governing employee benefits programs.
April 1999Spring 1999Information linking CFS and fibromyalgia to Chiari malformation, a compression of the spinal cord, is publicized by researchers and support organizations, including the National Fibromyalgia Research Association. Many patients undergo radical neurosurgery; most report less-than-ideal results.
The Social Security Administration (SSA) legitimizes disability associated with CFS with its ruling clarifying how CFS claims should be decided. The ruling, SSR 99-2p, creates a clearer path for people disabled by CFS to obtain benefits and charts new ground when the agency closely involves the CFIDS Association in its development. The agency’s initiatives to train its thousands of staff about the new ruling include a satellite-delivered training session in July.
“Sometimes I feel like such a deadbeat, and like I’m not contributing to society. I’d much rather still be a bank vice president than spend my life in bed. Working was much more fun! People like me with CFS want to work and do our part. I can’t work anymore, but I can contribute to my own cause. Making monthly gifts to the CFIDS Association is my small way of doing so. If it weren’t for the Association, I wouldn’t know what’s going on with this illness, nor would I feel as if anyone’s
working toward finding a cure. That’s the bottom line for all of us. I’ve been a Chairman’s Circle member for many years now, and it’s an absolutely empowering thing.”ELAINE KAIGN, Oklahoma CFS patient; Chairman’s Circle member
Defining moments
“Of all the CFS milestones, the 1999 Social Security Administration (SSA) policy ruling on CFS may be the one that’s had the most direct, positive impact on the daily lives of severely ill patients. Special rulings by the SSA on specific diseases are somewhat unusual. The CFIDS Association and advocates throughout the CFS community fought hard for this victory. And they won.
“The ruling, SSR 99-2p, was a huge milestone for those of us who have advocated for people with CFS. Before it, there were no universally accepted guidelines and precious little precedent for judges to follow when evaluating disability cases involving CFS. SSR 99-2p has been remarkably effective in providing legitimacy for the diagnosis and acknowledgement of the disease’s impact. As a lawyer representing people with CFS in a broad range of legal matters, I’ve also found 99-2p useful in providing practical
and persuasive support for my advocacy in other types of CFS cases, including those involving private disability insurance or employer provided benefits, even though it’s not legally binding in those areas.
“The SSA was among the first government agencies to work collaboratively with CFS advocates and clinicians, resulting in a policy that met the agency’s criteria, while also reflecting the reality of the disease as experienced by patients, their doctors and their lawyers.”
MAC SASSER, North Carolina Attorney; CFIDS Association Board of Directors, 1992–2002VI
CTO
RY
D e f i n i n g m o m e n T
Online Evolution

36 The CFIDS Association of America 37Defining Moments: 20 Years of Making CFS History
One of the CFS community’s top priorities is expanding the number of health care professionals who can confidently diagnose and manage CFS, treating patients with respect and compassion. Many obstacles have hampered progress, not the least of which are physician attitudes about CFS and the lack of a diagnostic marker or singularly effective treatment. But progress is occurring.
With CFS absent from most traditional medical curricula, local support groups initiated early education efforts. Armed with copies of research papers, CFIDS Chronicle articles and CFS booklets from the NIH and CDC, patient advocates approached their own doctors, medical societies, hospitals and clinics. They sponsored speakers and conferences, hoping to engage the local medical community. A key success occurred in 1999 when the New Jersey CFS Association secured state funding for publica-tion of a primary care manual on CFS. In partnership with the New Jersey Academy of Medicine and state health department, the manual was written and distributed in 2002 to all health care providers in the state.
Another excellent model has been established by the Organiza-tion for Fatigue and Fibromyalgia Education and Research (OFFER), founded by Dr. Lucinda Bateman in Utah in 2001. Focused on educating the area’s primary and allied health care professionals about CFS and fibromyalgia, OFFER sponsored its first conference in May 2003 with more than 150 physicians, nurses, social workers, physician assistants, psychologists and other medical professionals in attendance. Conferences held in 2005 and 2007, plus monthly educational meetings, have also informed the region’s providers.
The best-established conference series for professionals was initiated in 1992 by the American Association for CFS (AACFS, now the International Association for CFS/ME). The organiza-tion has now sponsored eight biennial research and clinical conferences, bringing together researchers, clinicians and patients to hear the latest in research and clinical practice. It has become a forum for experts to present cutting-edge data and for newcomers to learn from veterans.
Efforts to formalize CFS medical education began in 1997 when federal public health agencies hosted a satellite training program on CFS. The CFIDS Association helped arrange 78 downlink sites across the country with support from Area Health Education Centers (AHEC) and a small grant from the Health Resources and Services Administration (HRSA).
In 1999 HRSA and the CDC jointly sponsored the CFS Provider Education Project (PEP) and contracted with the CFIDS Association to manage it. The PEP is a multidimen-sional program that promotes awareness and information about the diagnosis and management of CFS for primary care providers and allied health care professionals. In 2002 the CDC became the sole funder of the project and awarded a competitive contract to the CFIDS Association to administer the PEP through December 2007.
The core of the PEP is the course curriculum, developed by a consortium of CFS experts and health educators from across the United States. Training methods have included Train-the-Trainer, in which 78 “core trainers” learned CFS fundamentals and tools to conduct peer-trainings in their own communities. A Grand Rounds component, with presentations for residents and medical staff at universities and medical centers, was added in 2005. Grand Rounds presentations have been given at 12 institutions so far, and more than 4,200 providers have heard live presentations about CFS through the project.
The PEP’s exhibit booth, featuring the message “Help the Person Behind the Symptoms,” has been displayed at 67 health care conferences to date, raising awareness and providing evidence-based
information to nearly 14,000 health care professionals through face-to-face interactions. Partnership activities with organiza-tions, including the American Academy of Family Practice, American Academy of Physician Assistants and American Academy of Nurse Practitioners, have extended the reach of CFS information to these important audiences.
A CDC-accredited self-study continuing education course for primary care provid-ers made its debut in February 2002 and was updated in 2006. Available in a variety of formats, including the popular online module, the course has been distributed to more than 7,000 health care professionals.
The national CFS public awareness cam-paign launched in 2006 included a new resource for the medical community, the CFS Toolkit for Health Care Professionals. Offered in both print and electronic formats, it covers evidence-based approaches to the diagnosis and treatment of CFS. The toolkit is being distributed through the
awareness campaign and by the PEP at health care conferences. The awareness campaign’s “Faces of Chronic Fatigue Syndrome” photo exhibit was also displayed alongside the PEP booth at several major medical conferences in 2006 and 2007.
Efforts over the past two decades to inform health care providers about CFS have begun to make a difference, as evidenced by changing attitudes and increased requests for clinical information. But much more work lies ahead
to improve the care available to people affected by CFS. The CFIDS Association will work to strengthen existing collabora-tions and forge new ones to accelerate progress in building a larger network of knowledgeable health care professionals.
“Although initially intended to be a resource for educating physicians in New Jersey, our CFS manual quickly became the CFS patient’s bible. Patients regularly take it to their physicians’ offices and discuss its content with them. And now, the manual is serving a far greater patient population: it has been adopted by the Vermont state health department and will soon be available in Florida. It is available in Japanese to patients and doctors in Japan and we are also discussing a Spanish-language version for use in the United States and South America.”DR. KENNETH FRIEDMAN, New Jersey UMDNJ–New Jersey Medical School
April 1999April 1999The New Jersey legislature passes a bill directing the state to educate medical professionals about CFS. The initiative is launched—and suc-cessfully lobbied for—by the New Jersey CFS Association, resulting in the creation of A Consensus Manual for the Primary Care and Manage-ment of CFS, a provider education resource released in 2002 that is distributed to 14,000 health care providers across the state.
As the CFIDS Association matures, its Board of Directors reexamines the organization mission and expands it to reflect the many needs and challenges of the broader CFS community. While reaffirming the Association’s commitment to research and to providing informa-tion and resources for the CFS com-munity, the new mission reflects the need to also focus on educating the medical community and the public about the illness.
Fall 1999May 1999The Inspector General’s report documenting the CDC’s misspend-ing of $12.9 million in CFS funds is released on May 12, CFIDS Aware-ness Day and the CFIDS Association’s eighth Lobby Day. The 67 advocates on Capitol Hill bring the news to 84 House and Senate members that, of the $23.3 million reportedly spent by the CDC on CFS, only $9.8 million went to studying the illness. The CDC issues a public apology and—most importantly—agrees to restore the $12.9 million, significantly increasing the productivity of the agency’s CFS research group in future years.
The Health Resources and Services Administration (HRSA) and the Illinois Area Health Education Center (AHEC) provide grant funding to the CFIDS Association to develop a health care provider training curriculum. In February 2000 the CDC joins with HRSA and the Illinois AHEC to co-fund this CFS Provider Education Project (PEP), managed by the CFIDS Association. That same year the PEP develops an exhibit about CFS that has now been displayed at 67 medical conferences around the country.
Our MissionThe mission of the CfiDs Association of America is to conquer Cfs. The Association works toward its mission by:
• Building recognition of Cfs as a serious widespread medical disorder
• securing a meaningful response to Cfs from the federal government
• stimulating high-quality Cfs research
• improving health care providers’ abilities to detect, diagnose and manage Cfs
• Providing information to persons with Cfs and enabling the Cfs community to speak with a collective voice
Provider Education

38 The CFIDS Association of America 39Defining Moments: 20 Years of Making CFS History
February and October 2000January 2000Researchers at UMDNJ publish a study finding that significantly more cases of CFS start during the winter months, providing more support for the theory that an infection underlies the onset of the illness. This finding is echoed by British researchers, who report in March that the majority of children with CFS developed the illness at the start of the school year, when they were more likely to be exposed to new infectious agents.
The NIH holds two scientific meetings on CFS—a February “consultation” organized by NIH staff and an October “State of the Science” conference, headed by Harvard’s Dr. Anthony Komaroff. In addition, the NIH moves coordination of the CFS research program from the National Institute of Allergy and Infectious Diseases (NIAID), where it had been located since the 1980s, to the NIH Office of the Director.
June 2000March 2000A “CFS think tank” meeting in Reno, Nevada, is the first major initiative by the group that would years later create the Whittemore-Peterson Institute for Neuro-Immune Disease at the University of Nevada–Reno, tentatively scheduled to open in 2010.
Deficiencies in the CDC and NIH CFS research programs are documented by the government’s General Accountability Office (GAO), which also recommends remedial measures for the agencies. The 57 CFIDS Association Lobby Day participants deliver the GAO report to Congress on June 22. The GAO also recommends changes to the CFS Coordinating Committee, and plans are made to elevate it to full formal advisory committee status.
Historical PerspectiveBy ANTHONY KOMAROFF, MD Harvard Medical School
Many people seem surprised that after 20 years of research, doctors still don’t know the cause of CFS. They shouldn’t be surprised. The causes of an illness—any illness—are complex. Scientists never make a sudden breakthrough that moves us from complete ignorance to total enlighten-ment. Understanding proceeds in very small steps, one foot in front of the other, and the journey is a long one.
In fact, we don’t really understand the central causes of most major diseases, including almost all forms of cancer, diabetes and atherosclerosis (the cause of heart attacks and strokes). But we do know vastly more about all of these major diseases—and about CFS—than we did decades ago because we have invested public and private funds in research.
Take cancer, for example. About 30 years ago the federal government decided to wage a “war on cancer” and began investing much more heavily in research because—after thousands of years of recognizing and trying to treat cancer—doctors knew next to nothing about it. Thirty years later we still don’t know the fundamental cause of most forms of cancer. But we do know vastly more than we did, and the knowledge is already leading to much-improved diagnostic testing and treatments.
Have we cured cancer? No. Are we close to curing most types of cancer? No. But some types have been cured, and others are now a chronic disease, whereas 30 years ago they were a death sentence.
Twenty years ago at the beginning of the latest wave of interest in CFS, we had limited tools for understanding an illness like this. Today we have powerful new research technologies. Newer brain imaging modalities allow us to study brain activity better than ever before. New molecular biology technologies allow us to study gene activity inside circulating immune system cells and to look for infectious agents with an accuracy that wasn’t possible two decades ago.
When a patient has been suffering with a debilitating illness like CFS for many years, but scien-tists still don’t know what causes it and medical professionals still can’t cure it, it’s understandable that the patient is frustrated. But that doesn’t mean the CFS community—including patients, researchers, clinicians and advocates—don’t have cause for celebration and optimism.
We’re still a long way from understanding the causes of CFS. On the other hand, we have come a long way in 20 years. In 1987 most researchers and physicians had never heard of CFS, and the few who had knew little about it. The research of the past 20 years, in part supported by the CFIDS Association, has demonstrated that the illness is real and has shown us where to look for the causes of the illness. That’s a significant accomplishment.
October 1999Fall 1999The CFIDS Association receives donations totaling more than $700,000 in its annual fundrais-ing campaign, the most successful fundraiser in Association history. Such funding allows the organiza-tion to continue funding research, a priority since the beginning, as well as important advocacy and educa-tion programs.
DePaul University researchers publish a study in Archives of Internal Medicine reporting that as many as 800,000 adults nationwide may suffer from CFS, twice the number previously estimated by the CDC. The study data shatters the previously held “yuppie flu” myth by confirming the CDC’s earlier finding from its San Francisco study that minorities and low-income Americans are at higher risk for CFS.
January 2000December 1999Dr. Garth Nicolson publishes data suggesting that a new form of mycoplasma is responsible for CFS. Studies like these keep the concept of infectious agents as triggers for CFS alive. Other groups report finding chlamydia pneumoniae in a large percentage of CFS patients tested, but results aren’t confirmed by other researchers.
The CFS Research Review is published for the first time by the CFIDS Association to educate health care professionals about CFS. Another Association publication, Snapshots of CFIDS, puts a personal face on the CFS experience by profiling people with CFS from all walks of life.
“In 1999 the CFIDS Association’s executive committee of the Board made a landmark decision: to return a donor’s gift earmarked for a particular research application that didn’t survive peer review. Although we can look back today and reflect on how this decision demonstrated the growing maturity of the Association’s research program, I remember wrestling with it at the time. Our program was evolving from a pass-through account for
individuals to support a favored researcher to a source of funding for scientifically sound proposals. We were at a crossroads. It took courage to refund a five-figure donation, but the integrity of our program hinged on us following through. I’m proud that we stood up to the challenge.”
JANE PERLMUTTER, New York CFIDS Association Board of Directors, 1996–present
THen In the beginning, there were few pioneering doctors and researchers studying CFS. In those early days, decisions about which studies the CFIDS Association would fund were rather simple because the field was so small. Hopes and dollars were invested in projects that promised to uncover the cause and the cure. Needless to say, these efforts fell short of delivering either one.
noW Over the years the purpose of our research program has evolved. As our organization has grown, decisions about which projects to fund have been made with greater care. Not only are there more people researching CFS, but the shift from narrowly focused single-agent hunting expeditions to multidisciplinary studies of numerous out-of-kilter body systems makes the granting process more complex. We’ve modeled our program after those of other health charities funding research, blending peer-review systems with patient-based needs and concerns. And instead of funding multiyear open-ended grants, we now fund pilot studies, helping investigators refine their hypotheses and accumulate data in hopes they can then compete successfully for larger sums available from the NIH or biotech firms. We’re trying to shift the funding burden from those least able to afford supporting expensive medical research—people with CFS—to government and cor-porate institutions and philanthropic foundations. This will take some of the funding burden for the most expensive research off the patient community, but still allow CFIDS Association supporters to fill the vital role of funding less expensive pilot studies.
D e f i n i n g m o m e n T

40 The CFIDS Association of America 41Defining Moments: 20 Years of Making CFS History
January 2001January 2001Founder Marc Iverson resigns as chairman of the CFIDS Association, a position he has held since the organization was founded. Jon Sterling, former president of the New Jersey CFS Association, becomes the second chairman of the Association. Jon brings to the post his experience as a CFS patient, his interest in research and advocacy, and his extensive network of contacts inside and outside the CFS community.
The AACFS holds its biennial conference in Seattle. Genetic research is a major focus of the meeting; Dr. Dedra Buchwald’s University of Washington research group discusses the results of its NIH-funded study of CFS in twins, finding that genes play a role in the development of the illness. Also, the University of Miami’s Dr. Kevin Maher reports on low concentrations of the immune protein perforin in CFS patients’ NK and cytotoxic T cells, providing the first evidence suggesting a T cell-associated cytotoxic deficit in CFS.
May 2001April 2001 The CFS Provider Education Project holds its first Train the Trainer session, teaching 15 “core trainers” to deliver the continuing education course in their own communities. Physician Charles Lapp and researcher Leonard Jason conduct this training, which is designed to deliver credible scientific information about CFS to medical professionals across the country. At subsequent sessions that year, an additional 40 medical professionals are trained.
Dr. David Bell publishes his 13-year follow-up on the children from the Lyndonville, New York, cluster outbreak that occurred between 1985 and 1987. His Pediatrics article is one of the first longitudinal studies of pediatric CFS. Bell, one of the foremost authorities on CFS in children and adolescents, concludes that CFS “may result in persistent somatic symptoms and disability in a minority of those affected.” A majority of the children had mild to moderate symptoms 13 years after first becoming ill, and 20 percent remained significantly ill.
Historically, one of the myths about chronic fatigue syndrome that has had the most adverse affect on patients—and patient care—is the idea that CFS is a form of depression or a psycho-logical illness. The idea that CFS is “all in your head” was perpetuated for years, doing a great deal of damage not only to the public’s understanding of this illness, but also to the medical profession’s response to CFS patients in a clinical care setting.
Mistakenly attributing the symptoms of CFS to depression causes unwarranted delay in proper diagnosis and manage-ment, leads to unnecessary medications and potentially drives the patient—who is certain that it’s an organic problem and not a psychiatric one—to distrust the medical profession and seek alternative care. For the patient, such alternative care can be expensive, unhelpful and sometimes even dangerous.
I conducted a study in 1993 of 11 new CFS patients who came to the Hunter-Hopkins Center to consult me. I found that their diagnosis had been delayed for more than two years, and the patients had spent an average of $26,000, excluding hospitaliza-tion, seeking the correct diagnosis. This is totally unnecessary and unacceptable because we have a body of scientific research that’s pretty clear in showing that CFS is not a psychological illness and that it can be differentiated from depression not only in a research setting, but in a clinical setting.
All of the wasted time and money, and the potential harm to patients, can be avoided when medical professionals understand how to distinguish CFS from depression.
Historical PerspectiveBy DR. CHARLES LAPP, MD Hunter-Hopkins Center, Charlotte, North Carolina “The state of research into
pediatric CFS is abysmal. The lack of pediatric diagnostic criteria has hampered efforts, and it took until January 2007 for a pediatric case definition for ME/CFS to be published. Progress has also been slowed because the American Academy of Pediatrics and others have largely ignored this illness and because of a dire lack of funding for research on pediatric CFS. Still, there have been isolated studies that have been extraordinary considering the challenges.”DR. DAVID BELL, New York Primary Care Pediatrics
November 2000October 2000Dr. David Torpy and his Australian research group present data on a genetic mutation they discover in CFS. The mutated gene regulates production of cortisol, a hormone that affects immune and stress response.
CFS patient Jennifer Small becomes the first donor to the CFIDS Association whose gifts total more than one million dollars. In March 2002, CFS patient Elena Ditemoveev also makes Association donor history, leaving $300,000 to the Association in her will, marking the first bequest received by the Association.
December 2000December 2000The CFIDS Association holds the first of three research symposia designed to reinvigorate research on CFS and draw new investigators into the field. The first meeting examines the role of the autonomic nervous system in CFS. The second and third meetings, held in 2001, focus on the neuroendocrine and immune systems in CFS. Three resulting peer-reviewed papers outlining promising avenues of research are published in the journal Neuroim-munomodulation in 2003 and 2004.
U.S. Representative John Porter, a longtime champion of CFS issues who was crucial to getting the $12.9 million restored to the CDC’s CFS research program, retires from Congress. Porter becomes chairman of Research!America, an influential coalition of academic, biomedical and health advocacy organizations. The CFIDS Association joins Research!America in spring 2005.
“As chair of the subcommittee funding CDC, I asked Dr. Jeff Koplan, the director, to meet with me. He was very concerned and embarrassed for the agency, and promised to and did take immediate corrective actions. Kim McCleary’s testimony before Congress, her strong behind-the-scenes leadership, and her tenacity until the problem was solved helped to secure the positive outcome for the CFS community.”HON. JOHN PORTER, Illinois Former U.S. congressman
Jennifer Small: Generosity Unmatched None of the CFIDS Association’s accomplishments would have been possible without the generosity of donors who have entrusted their funds to the CFIDS Association to invest in the battle against CFS. Jennifer Small holds an important place in CFS history as the CFIDS Association’s most generous benefactor, with donations totaling $1,337,810. A person with CFS, she first learned of the CFIDS Association in 1994 through Ann Landers’s advice column and quickly became a key supporter of the Association’s mission to conquer CFS. Her gifts have supported virtually every aspect of Association programming, from research to advocacy to capacity building. Jennifer was also instrumental in supporting the production of Kim Snyder’s documentary, I Remember Me.
The CFIDS Association is deeply grateful to Jennifer and thousands of other donors who have expressed their commitment to the mission to conquer CFS by making gifts of all sizes over the past 20 years.

42 The CFIDS Association of America 43Defining Moments: 20 Years of Making CFS History
September 2001September 2001On September 10, Kim McCleary is honored by Redbook magazine as a “Mother and Shaker” for her role in exposing the CDC’s misspending of CFS research funds. She is introduced at the Lincoln Center event by Sarah Ferguson. Other honorees are Hillary Clinton, Marlo Thomas and Christy Turlington. McCleary is forced to leave a related interview with Self magazine on September 11 following the terrorist attacks on the World Trade Center, which lead to the evacuation of most high-rise buildings in lower Manhattan.
The Agency for Healthcare Research and Quality releases a report examining studies of the treatment of CFS. Its support for cognitive behavioral therapy and graded exercise as the most promising treatments for CFS is widely contested, particularly given the high rates of dropouts in studies of these therapies (which the agency acknowledges).
November 2001September 2001While the Department of Health and Human Services reorganizes its committees after a challenging change of administrations and new priorities following 9-11, the CFSCC name change workgroup proposes renaming CFS as neuroendocrine-immune dysfunction syndrome and solicits input from the patient community and health care providers. The survey results, released in 2002, indicate that two-thirds of respondents find the new name acceptable and 91 percent support a name change in general.
I Remember Me, a critically acclaimed documentary film on CFS written, produced and directed by CFS patient Kim Snyder, opens in a Manhattan theater. Between 2000 and 2002, the film wins awards at several film festivals, receives critical praise from film critic Roger Ebert, is broadcast on the Sundance Channel and is released on home video. The film includes interviews with celebrity CFS patients Blake Edwards and Michelle Akers.
“The culture of an organization starts at the top. I have to give Kim McCleary the credit: the CFIDS Association is an incredible organization because of Kim’s leadership and integrity. I’m one of the lucky ones with CFS; I’m still able to work and earn a living. I feel so fortunate I can contribute to the Association and all the excellent work Kim does. I have so much respect for her, and for the Board and the staff throughout these 20 years. It’s a great organization because of their strong principles and vision.”DR. JEFFREY BLUM, North Carolina CFS patient; CFIDS Association Board of Directors, 1993–1996
“The release of I Remember Me is still among the most important moments of the past two decades. It has had an incredible impact, not only validating the experience of patients but increasing public understanding of CFS.
“I still don’t know how Kim Snyder ever managed to complete the film. She was so sick that there were times during the filming and production I
thought she’d drop. But when it was finally released to critical acclaim and she heard how much the film meant to so many patients, I think it made it all worthwhile. She still gets hundreds of e-mails every year about I Remember Me from all over the world.”
VIVIAN TREVES, New York CFS patient; spokesperson for the CFS public awareness campaign
A popular actor, musician, athlete or other celebrity can bring credibility, awareness and public and government concern to an issue. Most people concerned with CFS—observing celebrities like Michael J. Fox, Lance Armstrong and Christopher Reeve using their celebrity to raise awareness and funds for their own medical conditions—have hoped for a star to take up the CFS cause and bring media and popular attention to the illness.
The notion of celebrity, however, is difficult to reconcile with the debilitating effects of CFS, and this may explain some of the tension that many celebrities with CFS have elicited when they talk about their illness. To maintain their status, celebri-ties must be consistently in the public eye, doing whatever it is that brought them into the limelight in the first place—acting, writing, playing a sport, attending parties and premieres and projecting a glamorous image. Otherwise, they risk losing their appeal to the media and the public.
Susan Harris, writer/creator of popular 1980s sitcom The Golden Girls, was the first to use her platform in popular entertainment to talk about CFS. In 1989 she wrote a CFS plotline for the show’s character Dorothy. A seminal two-part episode described Dorothy’s difficulty in gaining credibility and medical attention for her illness.
Possibly because of the extreme physical stress of high-level athletic training, athletes seem to be one of the hardest-hit celebrity professions. But athletes with CFS have also generated some of the most controversy among patients. If it’s hard to reconcile the notion of an actor or singer with the devastation of CFS, it’s even harder with a person who makes his or her living doing physical activity.
Michelle Akers, one of the world’s greatest soccer players, was one of the first to feel that tension. In 1995 she began using her significant public platform to talk eloquently and honestly about how CFS had affected her. She continued speaking out about CFS while still playing on the 1996 Olympic and 1999 World Cup teams that won gold medals.
After Akers’s disclosure, other Olympic athletes with CFS began speaking out. Swimmers Tom Dolan and Anita Nall and speedskater Amy Peterson continued to compete as they talked
publicly about their battles with CFS. In 2000 longtime CFS patient and Charlotte, North Carolina, support group leader Kebbie Cannon competed in the Sydney, Australia, International Paralympics in equestrian dressage.
Keith Jarrett, a superstar jazz musician known for his improvi-sational genius, went public in 1998, telling reporters that the only way he could describe the mysterious illness he had
“If you want to give the average person an idea of what this illness feels like to many sufferers, it’s like the last four months of an AIDS patient’s life, but it lasts forever.”KEITH JARRETT CFS patient; legendary musician
contracted two years earlier was, “It was like aliens were invading my body. I felt completely drained of energy. It felt like forced cessation. No one knows how debilitating this sickness is unless they have it. I’ve met people who have had it for 10 years, 25 years. Some are bedridden, some can’t walk across the street. If you want to give the average person an idea of what this illness feels like to many sufferers, it’s like the last four months of an AIDS patient’s life—but it lasts forever.”
Other celebrities with CFS who made their illnesses known were legendary film director Blake Edwards; musicians Randy Newman, Cher and Dennis DeYoung; actors Morgan Fairchild, James Garner, Alana Stewart and Kathy Crosby; and philoso-pher Ken Wilbur.
Possibly the best-known celeb-rity with CFS is Laura Hillen-brand, author of the best-seller Seabiscuit: An American Legend. Because writing is a sedentary profession, Hillenbrand has escaped some of the criticism others have attracted. She has also been very clear about the fact that her illness often prevents her from leaving her home, but she’s willing to do media interviews either at her home or by telephone. Her New Yorker piece, “A Sudden Illness,” eloquently revealed her personal battle with CFS and won the 2004 National Magazine Award for best essay of the year.
Although CFS hasn’t yet garnered the degree of celebrity involvement and fundraising as many other conditions, the disclosures of stars like Akers, Hillenbrand and others have made it more acceptable for celebrities and noncelebrities to talk publicly about the illness. Their efforts have helped pave the way for the type of star-driven positive media and public attention that CFS patients and advocates have long dreamed of to help bring attention to the illness and to augment other kinds of media coverage about CFS.
Celebrities
D e f i n i n g m o m e n T

44 The CFIDS Association of America 45Defining Moments: 20 Years of Making CFS History
December 2002September 2002Johns Hopkins investigators, including Dr. Peter Rowe, find that adolescents with CFS are 3.5 times more likely to have joint hypermobility, which may be associated with the orthostatic intolerance found more often in children and adolescents with CFS. This finding receives little attention. But other physicians also report joint hypermobility in their patients, including Dr. Alan Pocinki, who later writes an article about the link between CFS and joint hypermobility for the summer 2004 CFIDS Chronicle.
CFIDSLink, a free monthly e-mail newsletter, is introduced by the CFIDS Association to provide the community with news in between quarterly issues of the CFIDS Chronicle. The electronic publication proves popular, with thousands of subscribers quickly signing up to have the Link sent to their in-boxes each month.
February 2003January 2003A consortium of Canadian doctors and researchers publish a clinical case definition for ME/CFS in the Journal of CFS. The so-called Canadian case definition generates excitement in the patient community because it’s created for practicing health care professionals to diagnose the condition, in contrast to other definitions that were developed to select cases for research studies.
The American Association for CFS (AACFS) holds its biennial conference near Washington, D.C. A highlight of the meeting is a session on genetic research, where the CDC reports it can distinguish people with CFS from healthy controls based on their gene profiles.
Historically, understanding of pediatric CFS has been hampered by several key factors. First, there has been marked reluctance by some in the medical community even to accept that children and adolescents can get CFS. Second, there have been only a handful of published pedi-atric research studies on CFS, largely due to the lack of enough federal research funding to draw young research-ers into the field and to sustain those who made a commit-ment to this line of inquiry. Third, the variability of the disorder—in the mode of onset and in the symptoms— has made it more difficult than usual to define which treatments are truly beneficial, and which treatments should be tailored to which subgroup of patients. And fourth, attributing the symptoms of pediatric CFS exclusively to anxiety or depression rather than looking at
a wider range of other contributing biological problems has limited the scope of research and clinical progress.
Yet when the illness is studied in children, remarkable progress can be made. For instance, studies have confirmed that there is a strong association between CFS and related circulatory disorders that are characterized by intolerance of prolonged upright posture. The most common of these circulatory problems is neurally mediated hypotension, but postural tachycardia syn-drome is also common. Exciting work by Wyller and colleagues in Norway published in the last year has extended the earlier observations and confirmed the presence of abnormal cardiovascu-lar regulation in adolescents with CFS. These disorders are treatable, which has opened up new avenues for the rehabilitation of patients with CFS.
Research has also confirmed that adolescents with CFS are more likely to have joint hypermobil-ity, a physical trait that is present before they become ill. In fact, I find that the physical examina-tion is not normal in people with CFS, as was once claimed.
As we move into the future, I would emphasize the importance of individualized care in the short term and the need for a much larger research initiative in the long run if we are to improve rates of disability from pediatric CFS
“Investigators like Dr. Peter Rowe and the late Dr. David Streeten have made enormous contributions to our understanding of orthostatic intolerance and joint hypermobility, conditions I see in many of my CFS patients.”DR. ALAN POCINKI, Washington, D.C. CFS clinician
Historical PerspectiveBy PETER ROWE, MD Johns Hopkins Children’s Center
Summer 2002May 2002The NIH closes its CFS Cooperative Research Centers program and terminates funding to the three centers at the University of Medicine & Dentistry of New Jersey, the University of Miami and the University of Washington. The CFIDS Association ramps up its public policy initiatives directed toward boosting the NIH’s anemic research portfolio.
PANDORA, a Florida-based nonprofit supporting neuroendocrineimmune disorders, is founded by Marla Silverman. Under the leadership of Silverman and Rebecca Artman, PANDORA sponsors the annual Neuroendocrine Disorders Confer-ence, provides support for CFS and FM patients in Florida, starts the Pediatric Pennies campaign to raise funds to increase awareness of pediatric CFS, lobbies for a Florida Neuroendocrineimmune Center of Excellence and co-hosts the 2007 biennial IACFS conference in Ft. Lauderdale.
November 2001Summer 2002The CFIDS Association faces the same financial difficulties plaguing many nonprofits in the wake of 9-11. For the first time ever, the Association is forced to lay off staff and cut programming expenses. Efforts begin to overhaul operations to weather the initial crisis and build a stronger, more effective organization for future sustainability.
The CFIDS Association is selected by the CDC to partner in the Provider Education Project (PEP), aimed at teaching health care providers how to diagnose and manage CFS. The PEP soon releases its CFS self-study course, augmenting the efforts of the program’s core trainers. For each of the next five years the Association hosts trainings, exhibits at health care conferences, sponsors educational events and promotes understanding of CFS in the medical community. The multiyear award represents the largest grant ever made for CFS povider education.
Marla Silverman: Advocate ExtraordinaireFall 1998 was the bittersweet mark of a new beginning for Marla Silverman. That’s when she finally was correctly diagnosed with CFS and fibromyalgia (FM), ending 13 months of doctors’ visits and uncertainty about what was causing a litany of debilitating symptoms.
Although Silverman felt relieved with the confirmation that she wasn’t a hypochondriac, as her disability insurance company suggested, she was devastated over the loss of her health and the limitations placed on her by severe illness. She says, “I cried for the life I left behind and for fear of the unknown.”
Before becoming so ill, Silverman was an assistant vice president for a large American bank, representing the bank in Brazil and Portugal. As her health permitted, she rechanneled the skills and business acumen developed in her previous career into a new path. “I knew I needed to figure out a way to face the future. So in 2002 I founded PANDORA, the Patient Alliance for Neuroendocrineimmune Disorders Organization for Research and Advocacy, a nonprofit organization that addresses the issues of people with these disorders.”
In five short years PANDORA has developed into one of the most active state CFS/FM patient organizations in the country, vigorously advocating for services for Florida patients in the state legislature and on Capitol Hill. “Empowerment, respect, dignity and safety—the life net to a very unkind world that doesn’t embrace CFS and other neuroendocrine disorders in the way it should. That’s what organizations like ours provide,” Silverman declares.
When I was diagnosed with CFS nearly 12 years ago, only 2 of the 16 physicians I consulted were knowledgeable about this illness. The others viewed my symptoms with reactions ranging from indifference to skepticism to ridicule. Recently I had a two-week hospital stay during which 9 physicians and specialists examined me. Although none of them had much experience treating CFS, they each interacted with me attentively and with respect. None questioned the validity of my symptoms, and some reviewed my CFS and fibromyalgia books with great interest. I’m very grateful to the Association for the great programs you’ve introduced in the provider education area. You are making a difference!”REBECCA BECKER-BEAN CFS patient

46 The CFIDS Association of America 47Defining Moments: 20 Years of Making CFS History
D e f i n i n g m o m e n T sBy Laura Hillenbrand
July 2003Laura Hillenbrand’s essay about her experience with CFS, “A Sudden Illness,” is published in the New Yorker. Publication coincides with the release of Seabiscuit, a film based on Hillenbrand’s best-selling book. To commemorate the movie’s release, the CFIDS Association hosts a special screening in Washington, D.C., for nearly 400 celebrities, politicians, scientists and friends of the Association, including Hillenbrand, who is too ill to travel to the movie’s Hollywood premiere. Among the luminaries in attendance are Sen. Harry Reid, CDC Director Dr. Julie Gerberding, and media personalities Bob Costas, Tony Kornheiser, Diane Rehm and Michael Wilbon. The event is covered by TV program Inside Edition and the Washington Post. Hillenbrand is also invited to a special White House screening with director Steven Spielberg and leading actor Toby McGuire. She takes the opportunity to inform President Bush, Mrs. Bush and other guests about CFS.
Laura Hillenbrand is the author of Seabiscuit: An American Legend, a book she wrote lying in her bed, too ill with CFS to remain upright. She is also the author of a New Yorker essay detailing her experience with CFS, which went on to win the 2004 National Magazine Award for the best essay of the year. Hillenbrand was named one of Glamour magazine’s 12 Women of the Year for 2003, while Vogue named her one of its Extraordinary Women of 2003. She is currently working on another book.
May 2003Winter 2003The CDC begins releasing enormous amounts of data generated by research funded with its “payback” of $12.9 million. An Archives of Internal Medicine paper from CDC investigators increases prevalence estimates. Other papers show that relapses and remissions are common; that CFS is as disabling as AIDS, cancer and multiple sclerosis; and that people with sudden onset of CFS have different genetic profiles than those with gradual onset.
Dr. Lucinda Bateman, a physician who specializes in the care of patients with CFS and fibromyalgia (FM), organizes the first conference of the Organization for Fatigue and Fibromyalgia Education and Research (OFFER). The Salt Lake City conference draws 150 health care professionals and 250 patients, setting a standard for subsequent OFFER conferences, which contribute immensely to provider and patient education in the region.
“There is a huge difference in the way CFS is regarded by medical professionals since the late 1980s when patients used to be diverted to me by local and regional doctors who just didn’t want to deal with them. Today, there’s more acceptance of CFS as a legitimate medical condition. But much more work remains. That’s why the CFIDS Association’s provider education programs are so important. And it’s why OFFER sponsors conferences on CFS and FM. We want to give physicians, psychologists, nurse practitioners, physician assistants and other professionals overviews of the best treatment practices and clinical research so they can handle day-to-day management for CFS and FM patients.”DR. LUCINDA BATEMAN, Utah Fatigue Consultation Clinic; CFIDS Association Board of Directors, 2005–present
impossibility of traveling even very short distances. Interviewers would have to come to me. My publicist said that the media was going to need
an explanation. Was I willing to go public with my illness?
The prospect was terrifying. It seemed possible, even likely, that I would meet with the same derision that I had faced from the beginning, only this time it would be public, and on a far greater scale. But as scary as it was, it was also a golden opportunity to educate the world about a disastrously misunderstood disease. I had to say yes. I penned a short essay explaining my illness and the obstacles it had created as I wrote my book, and my publicist included it in my press packet. I held my breath.
The next three years were a whirlwind. I did hundreds of interviews, and it seemed that every journalist wanted to talk as much about CFS as about Seabiscuit. At first, telling my story was intensely uncomfortable. But my perspective quickly changed. I began to focus on the fact that I was speaking not for myself, but for countless other people who were enduring CFS. Though I was bedeviled by the sense that my own illness was unseemly, when I thought of all the other people whose lives had been stolen from them through no fault of their own, and whose suffering was exacerbated by an unjustified stigma, all I felt was compassion. That change in perspective freed me, and suddenly all I wanted to do was fight for understanding. I became more and more involved with CFS advocacy. I spent a full year writing a lengthy article for the New Yorker, telling my story with a raw honesty that I had never been able to muster before. The experience was transforming. All of my useless years of suffering now had a meaning, a purpose. I could use them to help someone else.
The epiphany came in an unlikely way. My struggle with CFS was the subject of a story on 20/20. Just after the show aired, a couple of “shock jock” radio deejays in a major city mocked my illness on the air, suggesting that it was faked. Here was the thing I had feared, but my reaction startled me. I didn’t feel humiliated. To my astonishment, I didn’t even feel the slightest bit ruffled. I thought the deejays foolish and depraved, but the derision no longer found a home in me. I shrugged it off and forgot about it.
The sense that my illness was disgraceful was finally gone, thanks to the work of advocacy. It is the greatest paradox of my experience with CFS that public exposure, the very thing that I had avoided because of the shame it triggered, turned out to be the one thing I needed to shed that shame forever.
When CFS came crashing down on me in 1987, it seemed that there was nothing it did not take. But for me, the cruel-est twist was not what it stole, but what it left behind.
Virtually unstudied, invisible to standard diagnostic tests, CFS existed in a vacuum of understanding. In the absence of easy answers, an arrogant, irrational assumption was made. If extant tests revealed nothing, the problem wasn’t that medical knowledge was limited, it was that patients weren’t really sick. CFS, it was decided, was simply hypochondria or fakery. In that horrifying spring of 1987, I learned that I was facing not only a catastrophic disease, but a poisonous stigma as well.
Like so many other patients, I felt the stigma every day. I was called “lazy” and “a deadbeat” and accused of playing for attention and pretending to be ill. From doctors, acquain-tances, even relatives, I received not compassion and care, but hostility, derision, disgust, dismissal. When I asked for help, I was excoriated for troubling other people just so I could enjoy being waited on. Intellectually, I understood that my illness was real, and that I was blameless. But emotionally, it was impossible to be steeped in scorn without absorbing it. CFS took everything from me, and in its place left grinding, relentless shame. I was ashamed of myself, ashamed of the failure of my body, ashamed of my helplessness.
That shame was ruinous. I became so afraid of encountering contempt that I avoided seeking help even when I desper-ately needed it, compounding my suffering exponentially and leading me into relapses. When I couldn’t avoid asking for help, I felt overwhelmed by guilt, especially when the assistance I requested was given with bitterness. Over and over again, I drove myself to collapse to prove that I wasn’t malingering. Worst of all, I felt so suffused with shame that I couldn’t offer my body the compassion that it needed to heal.
My disease became my dirty little secret. Whenever I could hide it, I did, fearing that disclosure would bring humiliation. When I began to write professionally, working almost entirely from bed, I hid my illness from all but my most trusted editors. I revealed it to only one interviewee, a woman whom I trusted enough to explain why I couldn’t accept her invitation to ride her horse. “CFS?” she said. “I thought that was all just made up.” When I first spoke to the man who would become my editor at Random House, I said nothing about my disease, sure that he would never agree to work with me if he knew my secret. It was my literary agent, who knew I had nothing to be ashamed of, who eventually told him.
In 2001 as I prepared for the release of my book, Seabis-cuit: An American Legend, I stood at a crossroads. A book tour was customary, but far beyond my capabilities. I told Random House’s publicist about my disease and the

48 The CFIDS Association of America 49Defining Moments: 20 Years of Making CFS History
February 2004December 2003The CDC publishes its influential paper on ambiguities in the 1994 case definition in BMC Health Service Research. The paper is based on the work of the Inter-national CFS Study Group, which participated in a series of CDC-sponsored workshops. The paper recommends revisions for applying the definition in research, offers suggestions about utilizing several standardized classification instru-ments and recommends a study of “patients with chronic unexplained fatigue from which a definition of CFS can be empirically derived.”
A CFIDS Association benefit gala on Oscar night in Manhattan honors Laura Hillenbrand, the author of best picture nominee Seabiscuit, and generates nearly $100,000 for the CFIDS Association’s research program.
April 2004March 2004Attention, information processing speed and motor speed are found to be impaired in CFS patients in an NIH-funded study at the University of Medicine and Dentistry of New Jersey. A possible explanation for the memory and concentration problems is offered by a separate Belgian study, which finds impairments on functional MRI scans of brain activity of people with CFS during cognitive tasks.
The CFIDS Association launches the Grassroots Action Center, an online tool to increase the CFS community’s communication with legislators, federal officials and the media. In a two-month period, more than 10,000 messages are sent to lawmakers, public officials and journalists in conjunction with a “virtual Lobby Day” surrounding CFIDS Awareness Day on May 12. Funding for this new advocacy tool is provided by donor gifts.
“When I was very, very sick the CFIDS Association was my lifeline. I ponied up my $35 a year for membership and got acceptance and information and all the things you need to survive with this illness. And I got hope from the CFIDS Association because they were the advocates I had prayed for. They were the ones who were going out to try and find a cure and raise money and lobby Congress and do all the nitty-gritty work you have to do to beat an illness. I’m with this cause until the end, until everyone who is lying in bed somewhere in America right now, and who is feeling like dying because they have such a severe illness, is out of bed and living their lives, and CFS is a thing of the past.”LAURA HILLENBRAND, District of Columbia CFS patient (in a message to guests at the CFIDS Association benefit)
“I want to commend the CFIDS Association for bringing to patients and their families the Grassroots Action Center and awareness efforts. Those of us who serve as advocates have never had such a wonderfully useful tool! You have made participating in advocacy so very easy! Thank you!”KIM WEAVER CFS patient
August 2003July 2003The NIH hosts a scientific conference on Neuroimmune Mechanisms and CFS, promising to follow up with a special Request for Applications to stimulate CFS research. The agency’s CFS funding fell from $7.1 million to $5.9 million from 2002 to 2003—a 17 percent drop—after CFS Cooperative Research Centers were discontinued in an effort to retool the CFS portfolio.
New Jersey researchers report that people with severe CFS have significantly lower cardiac output (the amount of blood pumped by the heart each minute).
Fall 2003September 2003The federal CFS Advisory Committee holds its first meeting two years after its predecessor, the CFS Coordinating Committee, last met. The CFSAC considers the CFSCC’s proposal to rename CFS neuroendocrineimmune dysfunction syndrome, but responds in December that until the illness is better understood, it would not support a name change.
The CFIDS Association commissions an independent research firm to conduct qualitative and quantitative research to measure the attitudes of the American public and primary care physicians regarding CFS. Research confirms that skepticism about whether CFS is physical or mental in origin affects the way the general public perceives not only the illness itself but the patients who have it. This research helps make the case for a national public awareness campaign to educate the public and health care professionals about CFS.
Although the National Institutes of Health (NIH) is the world’s top funder of CFS research, with a reported $93.9 million invested in CFS research from 1990 to 2006, the federal agency’s relationship with patients and researchers has been tumultuous.
The NIH is largely structured by body systems, with a few diseases hosting dedicated insti-tutes. The early link to Epstein-Barr virus (EBV) focused the NIH’s CFS research within the National Institutes of Allergy and Infec-tious Diseases (NIAID), where an on-campus researcher, Dr. Stephen Straus, was among those who showed EBV wasn’t the cause of CFS. Straus later linked CFS to psychological factors when his own theories didn’t pan out, and advocates fought back against this char-acterization, with attacks escalating on both sides.
Under the 1993 NIH Reauthorization Act, the agency was required to fund Cooperative Research Centers on CFS and provide a special review section for CFS grant applications—one of the first victories achieved by the Association’s advocacy program. The first center grants were awarded to researchers who had studied patients in the Incline Village cluster, as were several other NIH grants at the time. Leonard Jason’s study of prevalence was the first of several Association pilot projects picked up for funding by NIH; Brigitte Huber’s is the latest.
By the late 1990s interest in the viral hypothesis had waned significantly. Research was expanding to studies of abnormali-ties in the HPA axis and autonomic nervous system. Expertise
Historical PerspectiveBy VICKI WALKER CFIDS Association of America staff member
from other disciplines was warranted, so advocates pushed to transfer responsibility for CFS from NIAID to the Office of the NIH Director. Under Donna Dean’s leadership, a State of the Science conference in 2000 helped identify promising direc-tions, but funding levels suffered when NIAID discontinued
support for the CFS research centers.
All along, researchers reported that reviewers selected for their proposals had little, if any, real CFS expertise and that funding levels suffered as a result. Advocates provided docu-mentation that reported funding levels were being inflated through the inclusion of studies not directly related to CFS. And NIH program officers said that researchers seeking support for CFS projects had difficulty translating their ideas into coherent proposals that met rigorous funding standards. It was a standoff of sorts.
Beginning in 2003 an emphasis on neuroim-mune mechanisms of CFS was fostered by Drs. Vivian Pinn and Eleanor Hanna of the Office of Research on Women’s Health (ORWH) with a conference that year, then a 2005 special Request for Applications and $4 million in new awards announced in late 2006. A grantsmanship workshop sponsored by ORWH in September 2007 highlighted numerous funding opportunities for CFS studies in the highly visible trans-NIH initiatives advanced by NIH Director Elias Zerhouni.
Time will tell if this new approach benefits CFS research, but it’s clear that keeping the NIH engaged requires both strong science and responsible advocacy.
Actors Toby McGuire, Chris Cooper and Jeff Bridges in Seabiscuit
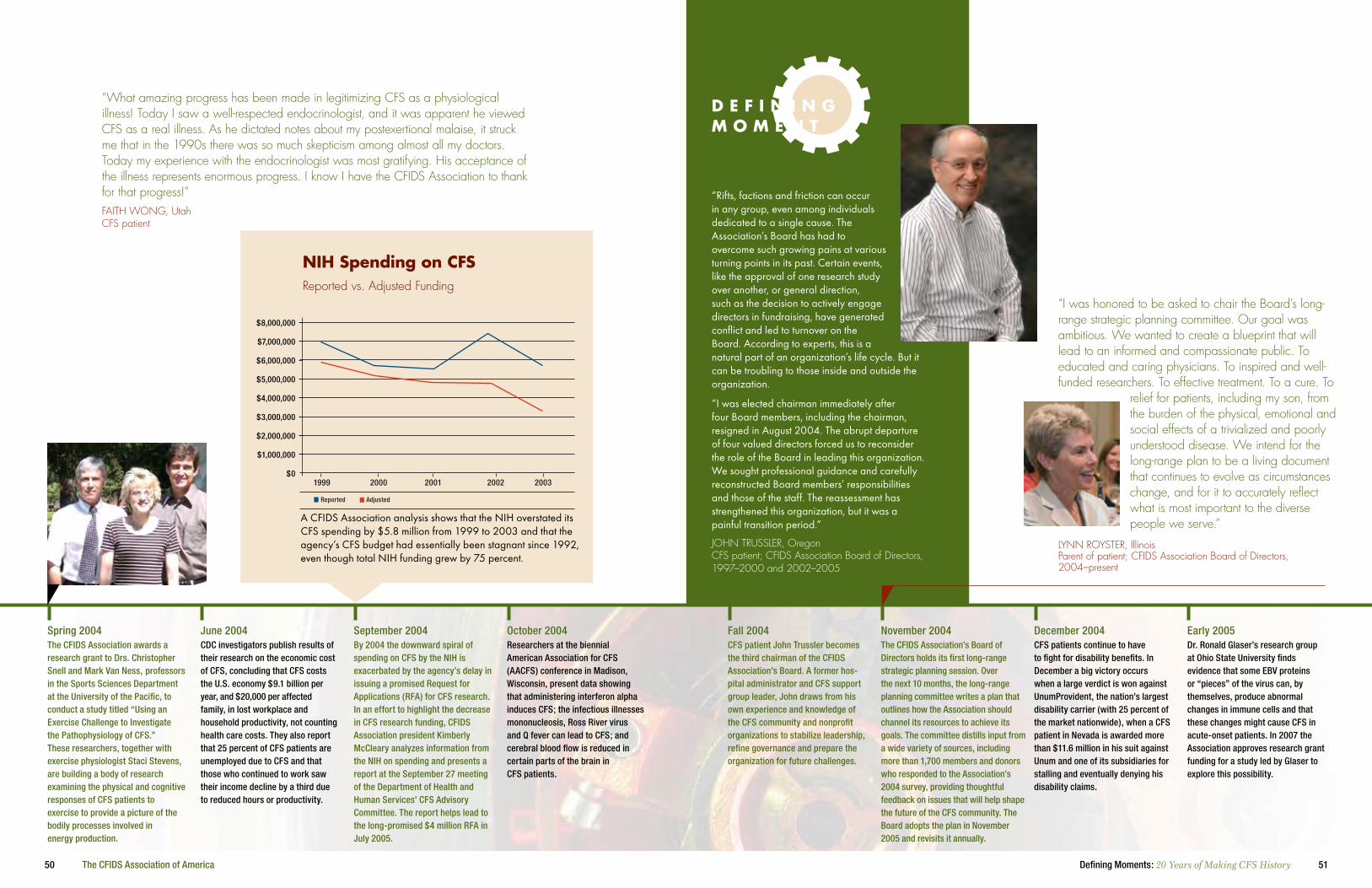
50 The CFIDS Association of America 51Defining Moments: 20 Years of Making CFS History
November 2004Fall 2004CFS patient John Trussler becomes the third chairman of the CFIDS Association’s Board. A former hos-pital administrator and CFS support group leader, John draws from his own experience and knowledge of the CFS community and nonprofit organizations to stabilize leadership, refine governance and prepare the organization for future challenges.
The CFIDS Association’s Board of Directors holds its first long-range strategic planning session. Over the next 10 months, the long-range planning committee writes a plan that outlines how the Association should channel its resources to achieve its goals. The committee distills input from a wide variety of sources, including more than 1,700 members and donors who responded to the Association’s 2004 survey, providing thoughtful feedback on issues that will help shape the future of the CFS community. The Board adopts the plan in November 2005 and revisits it annually.
Early 2005December 2004CFS patients continue to have to fight for disability benefits. In December a big victory occurs when a large verdict is won against UnumProvident, the nation’s largest disability carrier (with 25 percent of the market nationwide), when a CFS patient in Nevada is awarded more than $11.6 million in his suit against Unum and one of its subsidiaries for stalling and eventually denying his disability claims.
Dr. Ronald Glaser’s research group at Ohio State University finds evidence that some EBV proteins or “pieces” of the virus can, by themselves, produce abnormal changes in immune cells and that these changes might cause CFS in acute-onset patients. In 2007 the Association approves research grant funding for a study led by Glaser to explore this possibility.
“Rifts, factions and friction can occur in any group, even among individuals dedicated to a single cause. The Association’s Board has had to overcome such growing pains at various turning points in its past. Certain events, like the approval of one research study over another, or general direction, such as the decision to actively engage directors in fundraising, have generated conflict and led to turnover on the Board. According to experts, this is a natural part of an organization’s life cycle. But it can be troubling to those inside and outside the organization.
“I was elected chairman immediately after four Board members, including the chairman, resigned in August 2004. The abrupt departure of four valued directors forced us to reconsider the role of the Board in leading this organization. We sought professional guidance and carefully reconstructed Board members’ responsibilities and those of the staff. The reassessment has strengthened this organization, but it was a painful transition period.”
JOHN TRUSSLER, Oregon CFS patient; CFIDS Association Board of Directors, 1997–2000 and 2002–2005
“I was honored to be asked to chair the Board’s long-range strategic planning committee. Our goal was ambitious. We wanted to create a blueprint that will lead to an informed and compassionate public. To educated and caring physicians. To inspired and well-funded researchers. To effective treatment. To a cure. To
relief for patients, including my son, from the burden of the physical, emotional and social effects of a trivialized and poorly understood disease. We intend for the long-range plan to be a living document that continues to evolve as circumstances change, and for it to accurately reflect what is most important to the diverse people we serve.”
LYNN ROYSTER, Illinois Parent of patient; CFIDS Association Board of Directors, 2004–present
June 2004Spring 2004The CFIDS Association awards a research grant to Drs. Christopher Snell and Mark Van Ness, professors in the Sports Sciences Department at the University of the Pacific, to conduct a study titled “Using an Exercise Challenge to Investigate the Pathophysiology of CFS.” These researchers, together with exercise physiologist Staci Stevens, are building a body of research examining the physical and cognitive responses of CFS patients to exercise to provide a picture of the bodily processes involved in energy production.
CDC investigators publish results of their research on the economic cost of CFS, concluding that CFS costs the U.S. economy $9.1 billion per year, and $20,000 per affected family, in lost workplace and household productivity, not counting health care costs. They also report that 25 percent of CFS patients are unemployed due to CFS and that those who continued to work saw their income decline by a third due to reduced hours or productivity.
October 2004September 2004By 2004 the downward spiral of spending on CFS by the NIH is exacerbated by the agency’s delay in issuing a promised Request for Applications (RFA) for CFS research. In an effort to highlight the decrease in CFS research funding, CFIDS Association president Kimberly McCleary analyzes information from the NIH on spending and presents a report at the September 27 meeting of the Department of Health and Human Services’ CFS Advisory Committee. The report helps lead to the long-promised $4 million RFA in July 2005.
Researchers at the biennial American Association for CFS (AACFS) conference in Madison, Wisconsin, present data showing that administering interferon alpha induces CFS; the infectious illnesses mononucleosis, Ross River virus and Q fever can lead to CFS; and cerebral blood flow is reduced in certain parts of the brain in CFS patients.
“What amazing progress has been made in legitimizing CFS as a physiological illness! Today I saw a well-respected endocrinologist, and it was apparent he viewed CFS as a real illness. As he dictated notes about my postexertional malaise, it struck me that in the 1990s there was so much skepticism among almost all my doctors. Today my experience with the endocrinologist was most gratifying. His acceptance of the illness represents enormous progress. I know I have the CFIDS Association to thank for that progress!”FAITH WONG, Utah CFS patient
Reported Adjusted
niH spending on Cfs Reported vs. Adjusted Funding
1999 2000 2001 2002 2003
A CFIDS Association analysis shows that the NIH overstated its CFS spending by $5.8 million from 1999 to 2003 and that the agency’s CFS budget had essentially been stagnant since 1992, even though total NIH funding grew by 75 percent.
$8,000,000
$7,000,000
$6,000,000
$5,000,000
$4,000,000
$3,000,000
$2,000,000
$1,000,000
$0
D e f i n i n g m o m e n T

52 The CFIDS Association of America 53Defining Moments: 20 Years of Making CFS History
August 2005June 2005The Association launches the “kNOw MORE CFS” Education and Empowerment program, a regional seminar series, with the first two meetings in Reston, Virginia, in June and in Charlotte, North Carolina, in November. In 2006 the seminar series expands to Akron, Ohio, in May and to Sacramento, California, in October. These programs are part of the Association’s commitment to patient education. Although small attendance fees are charged, charitable donations supply almost half of the funding needed to conduct these seminars across the country.
Twelve members of the House of Representatives sign a letter asking the country’s secretary of health to implement a set of recommen-dations made by the CFS Advi-sory Committee (CFSAC), including advancing research, implementing public and health care education programs, and classifying CFS as a nervous system disease.
December 2005Fall 2005 Dr. Leonard Jason and his DePaul University colleagues are awarded an NIH grant to revisit their 1995-98 community-based Chicago cohort to conduct a follow-up study of CFS progression and prognosis. Research begins in the fall of 2005 on this first-ever large study to focus specifically on the long-term course of CFS.
A study implementing recommendations of the International CFS Study Group is undertaken by the CDC and published in 2005 in BMC Medicine. It is here that the new empirical case definition is first used. Importantly, this study classifies subjects by both the surveillance criteria of the 1994 case definition and the clinically empirical criteria using standardized and validated instruments that assess the major dimensions of the illness.
“We value our members, and membership fees cover the cost of important membership benefits like the CFIDS Chronicle and Research Review. However, these fees don’t make it possible for the Association to organize educational seminars, lobby on Capitol Hill, conduct outreach to health care professionals or perform any of the other myriad activities we rely on the organization to do for us. Donor support funds all these critically important programs.”BRUCE ALLSHOUSE, Delaware CFIDS Association Board of Directors, 2005–present
“I left the seminar educated and empowered. It was so encouraging to hear from practitioners who understand CFS and the challenges it presents. There were so many things said by both speakers—some of them major points, but many of them quite subtle—that almost took my breath away because of the knowledge and awareness they reflected. It is encouraging to know that this kind of progress is being made, and that there are more and more practitioners out there who truly understand CFS.”LAURA FARMELO, Maryland CFS patient; 2005 seminar participant
there are Joy Laube, Janet Moxley, Ed Taylor and his late wife Nancy, Tom Wickenhauser, Sara Wilkinson and Rich Carson, who have given during 17 of the past 20 years.
There are also the many donors who contribute at a sacrificial level. For someone no longer working and on disability because of CFS, that might be just $10. For others, a sacrificial gift might be $100, $1,000, $10,000 or even $100,000.
And there are those individuals who have reached out to family and friends, asking them to provide financial support through the Association’s online giving program, My Cause. In its first year, $45,000 has been donated through My Cause.
Vivian Treves, one of the greatest champions of My Cause and of philanthropic support of the Association, says, “I think of it as a responsibility and a privilege to help the CFIDS Association with its work. It costs money to send out informa-tion packets to patients around the country, to maintain the websites, to organize Lobby Day, to pay talented staff to do vital work that patients can’t do for themselves. In my bleakest years, I got most of my information and inspiration from the CFIDS Association. It’s important for that work to continue for others.”
The CFIDS Association is a voluntary, nonprofit organization that exists because a handful of generous individuals had a common vision—to conquer chronic fatigue syndrome. In the beginning, there were no government funds, no corporate spon-sors, no pipelines to wealthy foundations. Just individuals with a dream of being healthy again.
The CFIDS Association seems so established that it’s hard for many people to remember that in the early years our continued existence was not a sure thing. In fact, without the financial safety net provided by the Iverson family and a few other key donors, there were times when the doors would have closed—and the services the Association provides to the CFS commu-nity would have ended.
It’s also hard for many people to realize just how far the Association has come from that young organization of the 1980s, when activities were largely funded by membership dues and sales of educational materials. The picture is far brighter today, as the number of donors has expanded. Member dues represent a proportionately small income stream. In fact, today those monies only account for 17 percent of the Association’s
March 2005January 2005Attorney Susan Jacobs becomes the fourth chairperson of the CFIDS Association’s Board, and the first chairperson who doesn’t have CFS. Jacobs is drawn to the cause by a college friend whose early career was derailed by CFS. Her passion for the organization’s work is matched by considerable experience on boards of other nonprofits. Her leadership brings changes to the workings of the Association’s Board, yielding a productive, enriching environment.
The CFS Computational Challenge is convened by CDC researcher Suzanne Vernon to examine the large, multifactorial data set from the agency’s clinical study of CFS in Wichita, Kansas. Their findings point to a genetic basis for CFS and lead to 14 research papers, which are published in the April 2006 issue of Pharmacogenomics. The publica-tion is accompanied by a special media briefing by CDC Director Dr. Julie Gerberding, garnering positive coverage in lay and science press.
May 2005March 2005By 2005 many researchers believe that for CFS research purposes, people with CFS should be subtyped. In March Dr. Leonard Jason and col-leagues at DePaul and the University of Illinois at Chicago publish a paper in Neuropsychology Review sug-gesting that “subtyping individuals with CFS on sociodemographic, functional disability, viral, immune, neuroendocrine, neurology, auto-nomic and genetic biomarkers can provide clarification for researchers and clinicians.”
CFIDS Awareness Day is marked with the 13th CFIDS Association Lobby Day, with 58 advocates visiting 80 congressional offices in Washington and more than 3,000 letters sent from the Grassroots Action Center’s online “virtual Lobby Day.”
“I’ve had CFS since 1985, although it wasn’t diagnosed until 1996. I feel like it was important to be at Lobby Day so legislators could see people who look like a cross section of America who are affected by this illness. And it was important for them to see men, who often don’t step forward and admit they have a chronic illness. I was there to educate and advocate, and to paint a picture they could emotionally connect to. I tried to be conversational and build a relationship with the people we met with on Capitol Hill.”HOSIAH HUGGINS, Ohio CFS patient, 2005 Lobby Day participant
unrestricted income, excluding government grants for specific projects. The other 83 percent comes from donations from individual donors and family foundations. It is still individuals on whom we depend.
Over the past 20 years, we have succeeded in gaining cred-ibility for CFS; in providing more funding for CFS research than any other American organization; in improving govern-ment programs, policies and funding for CFS; in gaining better understanding of CFS by health care professionals and the public; and in achieving other important objectives. But none of these accomplishments would have been possible without the generosity of donors who have entrusted their money to the CFIDS Association to invest in the battle against CFS.
There’s Jennifer Small, whose cumulative gifts of $1,337,810 make her the largest donor in Association history. There are hundreds of Chairman’s Circle members, whose monthly dona-tions of $10, $50 or more have collectively added up to hundreds of thousands of dollars over time. There are long-term donors, like Allen Barss and Dr. Jeffrey Blum and his wife Linda, who have contributed to the Association every year since 1989. And
Philanthropy

54 The CFIDS Association of America 55Defining Moments: 20 Years of Making CFS History
May 2006Spring 2006Work begins on the first professional television public service announce-ment (PSA) on CFS when actress Jo McGinley portrays a patient moving slowly through her day. With creative direction from GMMB, the Pictures in a Row crew shoots the “Missing My Life” spot in Los Angeles, and the CFIDS Association and the CDC prepare for distributing the PSA nationwide to 800 TV stations and the networks as part of the national CFS public awareness campaign.
Japanese scientists report on a potential diagnostic blood test for CFS using a method called visible/near-infrared (Vis/NIR) spectroscopy, a high-tech process that displays molecular energy. Later that month, immunologists and infectious disease specialists report a link between human herpesvirus 6 (HHV-6) and CFS at the International HHV-6 and -7 Conference in Spain hosted by the HHV-6 Foundation. The CFIDS Association is a meeting sponsor.
June 2006May 2006Participants in Duke University’s annual Critical Assessment of Microarray Data Analysis (CAMDA) meeting analyze CFS data from CDC’s Wichita clinical study, proposing candidates for a CFS biomarker. The CFIDS Association helps sponsor this event, recruiting new groups to the study of CFS.
A curriculum for allied health professionals such as nurses, counselors and rehabilitation professionals is created by the Association’s CFS Provider Education Project and accredited by the CDC. In 2006 alone, more than 1,300 health care professionals are provided credible, up-to-date information about CFS through the project’s self-study continuing education courses, and 3,200 health care professionals visit the program’s booth at 11 conferences across the country.
In 1981 the first magnetic resonance imaging (MRI) scans were performed on people with multiple sclerosis (MS). By the end of the decade, MRI was used to prove that MS was an ongoing disease process even when symptoms weren’t appar-ent. With this evidence, new clinical trials were launched that yielded the first drugs shown to affect the course of the disease. MS was first described by Dr. Jean-Martin Charcot in 1868, so
the time from definition to the first specific MS treatment was more than 120 years.
I use this example not to suggest that targeted treatment for CFS is a century away, but to put the history of CFS in context. Based on my 17 years working on the front lines of CFS educa-tion and advocacy, I believe we have compressed the work done by MS activists over the first 120 years of their battle into the first 20 of ours. For CFS, the 1980s was a period of identifica-tion and definition. In the 1990s patients organized for action and respect. The 2000s have been dedicated to awareness and validation. By the end of this decade, I believe that technology will be the same kind of catalyst for CFS that it was for MS in the 1980s—and that all the research up to now will be vaulted forward with the help of a new genomics test or imaging tech-nique, something that will reveal the stealth-like markers of disease that have defied detection for two decades.
Historical PerspectiveBy K. KIMBERLY McCLEARY President and CEO, CFIDS Association of America
At the same time, it seems unlikely to me that CFS will be found to have a single cause and a single effective treatment. This condition is just too complex, and the definition (any one of them so far) yields a patient group that someday may be shown to represent several variations on a common theme, but not one uniform disease. Like many others, I believe a crucial next step is to develop consistent subtypes of CFS and criteria for the various stages of illness to help refine research until technology gives us the MRI-like catapult that MS got in 1981.
But as imperfect as the definition and nomenclature of CFS is today, the illness has given us a concept to organize around, a construct to study and begin to understand, and a label to use as we educate the public, the media and the medical community. Together we’ve transformed that label to represent something derided as “yuppie flu” and “affluenza” to something increasingly accepted as real, serious and severely life-altering. It’s taken longer than anyone thought possible when this organization was formed 20 years ago. But compared to MS, once called “hysteri-cal paralysis,” our journey has progressed relatively rapidly. We will not rest until we achieve the mission that drives our work—fully conquering CFS.
December 2005December 2005The Association’s advocacy program continues to focus on increased federal funding for CFS. Modest investments in the Association’s advocacy program, begun in 1992, spurred federal spending of $85 million in CFS research by the end of 2005. Association-sponsored research spending, which supports pilot programs and novel theories, helps seed the field, but is dwarfed by government funding. Fueling research through direct grants and sound advocacy produces a high yield for total dollars spent.
While much of the early research on CFS was concentrated in the United States, by the close of 2005, many CFS research initiatives are being led by other countries. For instance, London’s Dr. Jonathan Kerr, Glas-gow’s Dr. Jonathan Gow and CDC researchers in the United States all release data in 2005 showing CFS patients have gene expression abnormalities. And Japan estab-lishes a Society of Fatigue Science to focus attention on CFS and other fatiguing illnesses, which are a major societal, health and economic concern in that country.
Spring 2006January 2006The CFIDS Association publishes a special 68-page issue of the CFIDS Chronicle documenting the science and research of CFS, as well as promising avenues of future study. This magazine, which involves contributions from researchers and clinicians around the world, is a product of the Association’s com-mitment to educate people about the state of the science and research of CFS. This major publishing project was partially funded by philan-thropic support from donors.
In 2006 the CFIDS Association’s focus on responsible financial stewardship keeps the organization’s supporting services ratio at 8 percent. In 2007 this record of financial stewardship earns the Association the highest rating—four stars—from Charity Navigator, the nation’s largest charity watchdog. This rating is earned by fewer than 28 percent of the more than 5,000 nonprofit agencies monitored by the group through intense scrutiny of financial documents that reveal how well nonprofit organizations steward their donors’ resources.
“Chronic fatigue syndrome is a disease that affects people in every corner of the world. As a result, not only is CFS research being done outside the United States, but leading research efforts are being spearheaded by other nations. In fact, some of the more recent developments in treatment, brain study and the search for a biological marker have come from ‘across the pond.’”DR. BIRGITTA EVENGARD, Sweden Karolinska Institute
1990 1992 1994 1996 1998 2000 2002 2004
$18,000,000
$16,000,000
$14,000,000
$12,000,000
$10,000,000
$8,000,000
$6,000,000
$4,000,000
$2,000,000
$0
NIH CDC CFIDS ASSOCIATION
Advocacy’s impact on Research funding Federal funding grows in response to pressure from advocates
THen In the CFIDS Association’s first few years, operations were mainly funded by member-ship fees, sales of educational materials and “emergency gifts” from several major donors when funds were urgently needed to keep the doors open or fulfill commit-ments made to research projects. Gradu-ally, the organization matured, placing greater emphasis on fundraising, resource planning and financial stewardship to build a solid foundation for service to the CFS community.
noW Careful stewardship of our financial resources is a top priority for us. That’s why the Association has a stellar record in recent years of keeping our overhead, management and development expenses considerably below the national average for nonprofit organizations. The best-run nonprofits keep their administrative costs below 25 percent. In 2003 our supporting services ratio was 14.3 percent—well under that threshold. In 2006 that ratio was 8 percent. And in 2007 the Association earned Charity Navigator’s highest rating because of our financial efficiency and stewardship of donors’ contributions.
56 The CFIDS Association of America 57Defining Moments: 20 Years of Making CFS History
November 2006On November 3, the official launch of the CFS public awareness campaign is held at the National Press Club in Washington, D.C. Speakers are Kim McCleary; CDC Director Dr. Julie Gerberding; Assistant Secretary for Health Dr. John Agwunobi; the CDC’s CFS program chief, Dr. William Reeves; CFS experts Dr. Nancy Klimas and Dr. Anthony Komaroff; and patient Adrianne Ryan. Reporters and film crews from many major news outlets—including NBC, CBS, CNN, Fox News, NPR, C-SPAN, Associated Press, UPI, Reuters, WebMD, HealthDay and International Medical News Group—cover the press conference, resulting in worldwide media coverage of CFS and the awareness campaign. The campaign is funded by the CDC through a $6 million, multiyear contract to the CFIDS Association to conduct public opinion research, create print and online ads, produce and disseminate television and radio public service announcements, develop and distribute tools to educate health care professionals, create and manage a traveling photo exhibit, update the CFS content on the CDC website and conduct ongoing media outreach.
October 2006Summer 2006The national CFS public awareness campaign kicks off unofficially with a full-page color ad in the July and August issues of Ladies’ Home Journal and Better Homes & Gardens, educating millions of Americans about the debilitating effects of CFS. The ad continues to run in these magazines, as well as in People, throughout the following year. By October 2007 the ad has appeared 17 times in the three magazines, which have a combined readership of 44 million. Online banner ads about CFS also run on various websites, including WebMD.
My Cause, an online tool that helps individuals raise money for the CFIDS Association’s CFS programs, is launched. More than 180 people participate in the first few months alone, harnessing the power of the Internet to create personal web pages that share their stories, educate people about CFS and raise money online to fight this illness. In the first year, participants raise more than $45,000 through My Cause.
“I am especially appreciative of the collaborative efforts of the CFIDS Association and the Centers for Disease Control and Prevention to launch the public awareness campaign. Listening to a segment on NBC Nightly News convinced my parents, after 25 years, that I really was sick and had a legitimate illness.”RUTH SLOVEN, Minnesota CFS patient
The seeds of the national CFS public awareness campaign were actually planted years before they bore fruit. Myths and misun-derstanding about CFS were still too common in the early 2000s, in spite of years of work to change the social, medical and media landscape for CFS and its sufferers. The CFIDS Association believed that a major initiative was needed to catapult chronic fatigue syndrome to a new level of public recognition.
In 2003, with funding from the CDC, the Association commis-sioned an independent research firm to measure the attitudes of the American public and physicians regarding CFS. The results were not surprising to us, but they were eye-opening to federal officials. Research confirmed that skepticism about whether CFS is physical or mental in origin affects the way the general public perceives not only the illness itself, but the patients who have it. Although 64 percent of Americans believed chronic fatigue syndrome is a serious illness, only 53 percent perceived CFS as a real, physical condition.
This research—combined with earlier findings that less than 20 percent of Americans with CFS have been diagnosed and that CFS is as debilitating as MS, heart disease, lupus and end-stage renal disease—helped make the case for a national health campaign to educate the public and medical professionals about CFS. The Department of Health and Human Services and the CDC funded the campaign in 2005, and the CFIDS Association was selected to work with the CDC to design and implement the first-ever national public awareness campaign for CFS. With the help of two commu-nication firms, Fleishman Hillard and GMMB, both of which have top-notch health marketing teams, the CFIDS Association and the CDC developed an integrated, multicomponent campaign.
The November 2006 press conference announcing the campaign was a crucial element, providing a national forum not only to launch the campaign but to educate the media about the basics of CFS—symptoms, diagnosis, treatment options—as well as about recent research findings that demonstrate the genetic and physiological underpinnings of the illness. CDC Director Julie Gerberding went in front of the cameras to declare that the CDC is “committed to improving awareness that this is a real disease” and that “early diagnosis and treatment are important for recovery.” Speaker after speaker reinforced the messages that CFS is real and it’s serious, and this critical validation was echoed in print, broadcast and online stories not only in this country, but across the world.
By the time of the press conference, television and radio public service announcements (PSAs) had begun airing across the country, educating people about how to recognize the symptoms of CFS and where to go for information about the illness. The 30-second TV spot, which was distributed to all the major networks and more than 800 stations nationwide, has already aired more than 11,000 times. And the radio PSAs—which consist of a 60-second spot, 30-second spot and four versions of “live read” copy for the disc jockey or announcer to read—were distributed to major radio networks and more than 2,500 local stations. So far, the radio PSAs have aired more than 25,000 times across the country.
A full-page color print ad depicting the impact of CFS and educat-ing readers about symptoms was also developed to run in selected national magazines. The ad introduces the campaign slogan—“Get informed. Get diagnosed. Get help.”—and points people to the CDC campaign website at www.cdc.gov/cfs, where new content about CFS is available for consumers and health care professionals.
A traveling photo exhibit called “The Faces of Chronic Fatigue Syndrome” made its pubic debut at the Mall of America in Minneapolis, the largest mall in the United States, and contin-ues to tour in public venues and national medical conferences throughout the country. The photo exhibit features portraits and accompanying quotes from eight patients and two CFS experts to educate viewers about the illness, its life-altering impact and the importance of seeking diagnosis and treatment. The por-traits, taken by well-known fashion and celebrity photographer George Lange, are both compelling and dramatic, printed on huge banners that tower over visitors and give them a glimpse
of ordinary people whose lives have been impacted by CFS.
The campaign also includes printed and download-able materials for CFS patients, the public and medical professionals. So far, more than 70,000 copies of the patient brochure, the quick-read CFS brochure for medical profession-als and the CFS Toolkit for Health Care Professionals have been down-loaded, distributed at the photo exhibit and at medical conferences, and mailed to consum-ers and providers who request them.
Campaign outreach to health care professionals also includes both formal and informal alliances with health care organiza-tions like the American Academy of Nurse Practitioners, American Academy of Physician Assistants, Society for Women’s Health Research, American Academy of Family Physicians and other organizations that are helping distribute educational information about CFS to their members. Outreach to the medical press has so far resulted in articles in Internal Medicine News, the AMA’s American Medical News, JAMA, ACP Observer, WebMD and many other print and online journals and newsletters.
And the campaign media coverage—which began so successfully at the press conference—continues with new stories each week that validate the illness and the experiences of CFS patients everywhere.
Campaign brochures for patients and health care professionals, the photo exhibit schedule, fact sheets about the illness and much more information can be found at www.cfids.org/cfs. Many of these resources are downloadable. Materials can also be found on the CDC website at www.cdc.gov/cfs.
Public Awareness Campaign

58 The CFIDS Association of America 59Defining Moments: 20 Years of Making CFS History
June 2007The CFIDS Association’s Education and Empowerment seminars, featur-ing nationally known physicians and researchers, continue with a program in Houston on June 9 with Drs. Christopher Snell and Morris Papernik and a program on October 13 in Denver featuring Drs. Suzanne Vernon and Steven Goodman. Physi-cians like Drs. Larry Baldwin and Lucinda Bateman also contribute to the CFIDS Association’s educational initiatives with CFS presentations at universities and medical schools.
April 2007Webinar technology is first used to educate advocates about the CFIDS Association’s public policy program and how they can become involved. Two Lobby Day preview programs are held in April; a webinar instruct-ing advocates how to use Town Hall meetings with Congress inspires several to attend local events and puts CFS on the record.
Summer 2007Six months after the launch of the national CFS public awareness campaign, media coverage of CFS is setting new records. More than 5,000 newspaper, magazine, TV, radio and online stories have appeared in outlets as diverse as the New York Times, NBC Nightly News, WebMD, O magazine (Oprah), Woman’s Day, First for Women, the Sacramento Bee, the Washington Post, CBS 3 in Philadelphia, the Louisville Courier Journal, Voice of America TV, Lou Adler’s Medical Journal, CNN, FOX TV and Parade magazine.
May 2007The CFIDS Association organizes the 15th Lobby Day, which sets records for both participation and the number of meetings attended, with 80 advocates meeting with 94 representatives of Congress. Materials distributed to Congress include summaries of the November 2006 press conference and a special CFS briefing insert produced by Research!America, an influential Washington-based coalition of health and research organizations.
Larry Baldwin: Helping Other Doctors Understand CFS In 1993 Dr. Larry Baldwin, a Minnesota surgeon, found himself sitting on the other side of the doctor-patient relationship when he became severely ill with CFS. Relatively speaking, he was one of the lucky ones: he was diagnosed quickly and has had excellent medical care throughout the 14 years of his illness. Although he remains very ill, his doctors have worked closely with him to treat
the basic symptoms of CFS to the point where, over the last year he says he has been “lifted up out of inactivity.”
Although still severely ill, Dr. Baldwin is now able to use his medical training to do something he is deeply passionate about: giving other CFS patients the chance to get the high-quality medical care he receives. He is an advisor to the CFS Provider Education Project and, in August 2007, did something that would have been impossible just a few years ago: he gave a CFS Grand Rounds lecture to medical school students and faculty at the University of North Dakota.
“I went to medical school to be a helper. Doctors want to help, but sometimes they need to be taught how to help. By showing that we gain life-uplifting things by treating the basic symptoms of CFS—like sleep, pain, orthostatic intolerance and energy depletion—doctors can understand how to help,” says Dr. Baldwin. “If I can help doctors learn how to help us patients, that’s what I want to see happen.”
CFS has taught him some important lessons, and he has learned to integrate the illness into his life. He plans for energy-intensive activities, like lecturing, by “banking” energy in advance and arranging his schedule for the inevitable payback that will follow. He also makes sure to enjoy his family, including his grandchildren who live nearby. As he says, “I still have CFS, but I’m no longer captured by CFS. I revel in whatever I’m able to do and I enjoy what is enjoyable.”
January 2007December 2006A campaign media audit of all the media coverage on CFS in the one-month period following the press conference finds that 82 percent of the stories include the message that CFS is serious and real. And the CDC reports that almost 12,000 people downloaded campaign materials from the CDC’s CFS website from October 1 to November 6, 2006, and visits to the CDC’s CFS site increased 39 percent after the press conference.
Members of the International Association for CFS (IACFS) vote to adopt a new name, and the organization becomes the IACFS/ME to reflect the growing international nature of the research effort, as well as to acknowledge efforts to rename CFS by appending ME to the name. The same month, a pediatric case definition for ME/CFS is published in the Journal of CFS, authored by a working group from the IACFS/ME.
January 2007The IACFS/ME holds its biennial conference in Ft. Lauderdale. Among the highlights are CFIDS Associa-tion-funded studies at Weill Cornell University showing energy conver-sion abnormalities in the brains of CFS patients, and at the University of the Pacific documenting biological and biochemical evidence of the physical and cognitive decline that is characteristic of CFS following exertion. Other important findings include potential infectious origins for CFS, unique gene expression and function abnormalities, and brain structure and chemistry differences.
January 2007Stanford researcher Dr. Jose Montoya reports that a subset of CFS patients with high levels of HHV-6 or Epstein-Barr virus and a flu-like onset improve significantly on the antiviral drug valganciclovir, leading the drug manufacturer, Roche, to award him a $1.3 million grant to expand his study. Interest in the study allows Montoya to enroll subjects quickly, accelerating the timeline for this clinical trial, with results expected in mid-2008.
Historical PerspectiveBy MARCIA HARMON Director of Communications, CFIDS Association of America
The mass media exercises an extraordinary amount of influence over opinions on social, health, political and lifestyle issues. This was true when the term mass media was coined in the 1920s with the advent of nationwide radio networks, mass-circulation newspapers and magazines. It was true in the 1950s when American households began filling up with televisions. And it’s true today, with a revolution in communications technology
having brought the World Wide Web, Blackberries and iPODs into almost every home and office in the country.
Historically, understanding of CFS in this country has been alternately helped and harmed by the power of mass media. Between 1987 and 1995, much of the time spent on media rela-tions by organizations like CACTUS and the CFIDS Associa-tion was spent responding to negative portrayals of patients and misrepresentation of facts about the illness. Trying to educate the media about CFS, so they in turn could educate the public, was an uphill battle, with frequent slides back downhill. Media relations efforts were often more reactive than proactive.
Although it was tempting for patients to blame the media, the reasons for the “bad press” were complex. Sure, there were
some lax reporters, and some who brought their own biases about “yuppie flu” or “lazy malingerers” into the story. But most editors and reporters tried to be accurate and get the story right. However, when physicians they called as sources wouldn’t validate the illness, or opined that “most CFS patients are actually depressed or have another undiagnosed illness,” and when most federal officials wouldn’t go on record about CFS, it made it harder for the media to get a clear, unequivocal handle on this illness.
There was some progress in the mid- to late 1990s, with celebrities like Michelle Akers and Amy Peterson stepping up to put the media spotlight on CFS and personalize the illness, and with the July 1998 coverage of CFS on Oprah. Then Laura Hillenbrand published Seabiscuit and her award-winning essay in the New Yorker in 2003, and there was another step forward. And recent research contributed to a clearer picture of the biological underpinnings of this illness, providing a stronger “science” foundation for journalists.
But it has been the public awareness campaign that is finally— and we hope irrevocably—transforming the way CFS is discussed in the American mass media, and in American households. At the November 2006 press conference launching the campaign, when CDC Director Dr. Julie Gerberding firmly declared that CFS is real, that it’s a public health concern, and that patients are suffering, it validated the illness for the media in a way nothing before that moment has. It was a defining moment that is still reverberating, and resulting in unprec-edented media coverage of CFS.
60 The CFIDS Association of America 61Defining Moments: 20 Years of Making CFS History
November 2007Plans to hire a full-time scientific director come to fruition with the announcement that Dr. Suzanne Vernon, formerly of the CDC, is joining the CFIDS Association. Dr. Vernon is devoting her time and talents to fostering a more robust CFS research program and acceler-ating the pace of progress. A $1 million campaign is launched to fuel the expanded research program.
July 2007Andrew Lloyd and colleagues in Australia link 35 specific genes to CFS when the illness develops following infection with Epstein-Barr virus. The paper is published in the Journal of Infectious Disease and generates international media attention. Two months later, Dr. John Chia also garners extensive media coverage with another study related to viral infection, reporting that enteroviruses, a family of common pathogens, may be associated with CFS in patients with chronic gastro-intestinal problems.
October 2007The CFIDS Association participates in a collaborative meeting of organizations concerned with overlapping conditions such as fibromyalgia, interstitial cystitis, irritable bowel syndrome and chronic pain, providing guidance on how to expand awareness and funding that benefits patients with one or several of these disorders.
September 2007Dr. Brigitte Huber of Tufts University is awarded a research grant to study a retrovirus, HERV-K 18, as a risk factor for postviral CFS. The grant is funded by the NIH’s National Institute of Arthritis and Skin Diseases and the Office of Research on Women’s Health based on data collected during a 2004-06 pilot study funded by the CFIDS Association. It fulfills one of the main goals of the Association’s research program—to help promising investigators with pilot studies that can lead to larger studies funded by the NIH or biotech firms.
Directors with terms beginning in the 1980s
Marilyn Asbury (1988–1991) James Bavis (1989–1993) Pat Bradshaw (1988–1993) Susan Dorman (1989–1992) Alan Goldberg (1987–1996) Jonathan Goldberg (1989–1992) Betty Guthrie (1988–1994) Effie Hall (1989–1991) Jeanne Hardy (1989–1991) Mayhugh Horne (1988–1993) Kenneth Iverson (1987–1998) Marc Iverson, CPA, MBA (1987–2001; Board chairman, 1987–2000) Hal Levinson, JD (1989–1992) Richard Patterson (1989–1994) Adrienne Rosenberg, MSW (1989–1992) Kathryn Schwille (1989–1993) Cindy Teal (1989–1991) Robert Yentes (1989–1991)
Directors with terms beginning in the 1990s
Sheba Anderson (1993–1994) Debra Arnold (1993–1995) David Bell, MD (1992–1997) Jeffery Blum, MD (1993–1996) Richard Bourne, PhD (1997–1999) Coco Crum (1993–1998) Priscilla deLeon, RT (1995–2000) Thomas English, MD (1992–1994) Heather Frese (1997–1998) Bill Gareau (1993–1998) Betsy Haas, MSW (1992–1994) Bruce Hardy (1992) Barbara Hautau (1992)
Chester Helms (1991–1993) Jhan Hiber (1995–1996) Edward Isenberg (1995–1999) Wilhelmina Jenkins (1996–2000) Tim Kenny (1992–1994) Karen Lang (1997–1999) Kimberly McCleary (1996–present) Maggie McKenzie (1995–1998) Rebecca Moore Leibowitz (1995–1998) Marion Nelson (1997–1999) Allison O’Neal (1997–1998) David Patterson, CPA, MBA (1996–1998) Jane Perlmutter (1996–present) Kim Phillips (1993–1997) Lea Rhodes (1997–1999) Cathryn Rivers (1992–1994) Julia Sain (1993) Charles MacBrayer Sasser, JD (1992–2002) Patti Schmidt (1998–2004) Michael Shulimson (1992–1994) Carolyn Startsman (1992–1996) Marilyn Stewart (1994) Harriett Thompson (1992–1996) John Trussler (1997–2000 and 2002–2005; Board chairman, 2004) Marcia Wallace, MD (1998–1999) Frank Wrenn (1998–2000)
Directors with terms beginning in the 2000s
Bruce Allshouse (2005–present) Rick Baldwin (2001–2007) Lucinda Bateman, MD (2005–present) Diane Bean (2004–2005) Katrina Berne, PhD (2004–present) Barbara Comerford, JD (2003–2004) Rod Converse (2005–present) John Ginsberg, JD (2002) Terry Hedrick, PhD (2004–present) Dennis Irwin (2001) Susan Jacobs, Esq. (2004–present; Board chairman, 2005–2007) Joseph Lane (2003–2004)
Adam Lesser (2007–present) Beth Levine (2001–2003) Dimitris Papanicolaou, MD (2005– present) Mark Peterson, DDS (2003–present) Lynn Royster, PhD, JD (2004–present) Adrianne Ryan (2001–2007) Brian Smith (2007–present) Jennie Spotila, JD (2005–present; Board chairman, 2008) Amy Squires (2007–present) Jonathan Sterling (2000–2004; Board chairman, 2001–2004) Patrick Venetucci (2007–present)
June 2007June 2007In the most detailed prevalence study to date, CDC researchers report that 2.54 percent of people in Georgia aged 18-59 meet the clinical definition for CFS. This rate is 10 times higher than the rate CDC researchers found in the 1990s when they surveyed residents of Wichita, Kansas, and 6 times higher than the rate found in Chicago by Dr. Leonard Jason’s research team. Those earlier studies used a more restrictive research definition for the illness, and the Georgia study gener-ates controversy for employing the “looser” empirical case definition.
The FDA approves Lyrica (pregabalin) as the first drug to treat fibromyalgia, which many CFS patients suffer from as a comorbid condition. The drug decreases the pain of fibromyalgia and is approved for adults 18 years or older. Pfizer, the drug manufacturer, agrees to perform a study of the drug in children with fibromyalgia and a study in breastfeeding women. There is still no FDA-approved drug to treat CFS.
“I wanted to show the television PSA to several friends and family because it is exactly my feelings and experiences with CFS. I’m only 36 with 3-year-old triplets, and I feel terrible about what I miss out with them. Thank you so much for creating such a perfect PSA that fits my life. I almost cried when I saw it.”HEIDI BAUER CFS patient
June 2007In response to Lobby Day advocates’ requests, 49 members of Congress write to NIH Director Elias Zerhouni asking for expanded research into CFS under new authority granted by the 2006 NIH Reform Act.
July 2007By July the campaign photo exhibit has traveled to public venues and medical conferences in San Francisco, Sacramento, Houston, Minneapolis, Ft. Lauderdale, San Diego, Boston, Philadelphia, Dallas, Washington, D.C., Indianapolis and other cities. More than five million consumers and health care professionals have been exposed directly to CFS education at the photo exhibit so far, and millions more have been exposed indirectly to CFS information through related media coverage.
Boards of nonprofit organizations serve an essential role in our society. They act as stewards and visionaries for such diverse entities as schools, hospitals, libraries, arts organizations, shelters for the abused and homeless, places of worship and health-related charities, including the CFIDS Association of America, Inc. Over the past 20 years, the Association has been enriched by the leadership provided by 80 individuals who have contributed their “time, talent and treasure” to shape and build this organization. They have brought varied perspectives, as people with CFS, parents, close friends and professionals in fields relevant to the Association’s work.
The Board’s role has evolved as the Association has grown. In the early years, Board members were called upon to run support group meetings, produce the CFIDS Chronicle, field phone calls and govern. By the mid-1990s, a small staff was handling most of the day-to-day functions and the organiza-tion was broadening its local focus to provide more national leadership. Directors were recruited from around the country
Board of Directors
to strengthen the Association’s outreach and engagement with a broader array of issues.
A financial shortfall in 1997 forced the Board to examine its role in raising and protecting the assets of the organization in order to sustain operations. Founder Marc Iverson stepped down as chairman at the end of 2000, ushering in a new leader-ship era. This transition, while difficult, was important to the maturation of the organization and demonstrated its viability beyond the vision of one individual. The maturing process continued during the mid-2000s, when Board governance was refined to more clearly distinguish roles of the Board and staff in accomplishing the Association’s work. The first formal long-range strategic plan was adopted in 2005 and now guides every action taken by the Board and the staff.
As the Association’s leadership continues to evolve to meet present and future challenges, we pay tribute to the people who have served so admirably through every stage of growth.
About CFSChronic fatigue syndrome (CFS), also known as chronic fatigue and immune dysfunction syndrome (CFIDS), is a complex chronic illness that results in a constellation of debilitating symptoms, including incapacitating fatigue (experienced as profound exhaustion and extremely poor stamina), sleep difficulties, and problems with concentration and short-term memory. It’s also accompanied by flu-like symptoms, pain in the joints and muscles, tender lymph nodes, sore throat and headaches. A distinctive characteristic of the illness is postexertional malaise, a worsening of symptoms following physical or mental exertion that can require an extended recovery time.
CFS can be challenging for health care professionals to diagnose and treat—and equally chal-lenging for patients and their families to endure. Scientists still don’t know what causes CFS, and there isn’t a cure yet. However, significant progress has been made in recent years by researchers and the medical community in unraveling the mysteries of this illness. This progress has led to a greater understanding of how CFS affects the body, but current treatments are still aimed at symptom relief and improved function, and there is a critical need to develop more effective treatments.
CFS strikes people of all age, ethnic and socioeconomic groups. Research indicates that between one and four million Americans have CFS, but less than 20 percent have been diagnosed. The low rate of diagnosis shows a need for increased understanding of CFS among individuals experienc-ing symptoms of the illness, the general public and health care professionals.
About the CFIDS Association of AmericaThe CFIDS Association of America is the largest and most active charitable organization dedicated to conquering CFS. Since this organization was founded in 1987, the Association has invested more than $25 million in initiatives to bring an end to the pain, disability and suffering caused by this illness.
We are committed to providing credible, up-to-date information for patients and their caregivers, the general public and health care professionals. We have a variety of available resources. For more information about any of the resources mentioned in this publication, please contact us or visit one of the web pages listed below.
Resource Line ......................................... 704-365-2343
Fax....................................................... 704-365-9755
Our Website ......................................... www.cfids.org
Public Awareness Campaign Website ....... www.cfids.org/cfs
Donating to the CFIDS Association ........... www.cfids.org/support/default.asp
The CFIDS Chronicle ............................... www.cfids.org/archives/chronicle-issues.asp
CFIDSLink E-Newsletter ........................... www.cfids.org/archives/cfidslink.asp
CFS Research Review .............................. www.cfids.org/archives/research-review-issues.asp
Grassroots Action Center ........................ www.capwiz.com/cfids/home/
Health Care Provider Education ............... www.cfids.org/sparkcfs/health-professionals.asp
My Cause ............................................. www.cfids.org/support/donations-mycause.asp
Research Grants .................................... www.cfids.org/profresources/association-grants.asp
Science & Research of CFS ..................... www.cfids.org/special/default.asp
Support Groups ..................................... www.cfids.org/resources/support-groups.asp
Youth Information ................................... www.cfids.org/resources/youth.asp
November 2007Plans to hire a full-time scientific director come to fruition with the announcement that Dr. Suzanne Vernon, formerly of the CDC, is joining the CFIDS Association. Dr. Vernon is devoting her time and talents to fostering a more robust CFS research program and acceler-ating the pace of progress. A $1 million campaign is launched to fuel the expanded research program.
July 2007Andrew Lloyd and colleagues in Australia link 35 specific genes to CFS when the illness develops following infection with Epstein-Barr virus. The paper is published in the Journal of Infectious Disease and generates international media attention. Two months later, Dr. John Chia also garners extensive media coverage with another study related to viral infection, reporting that enteroviruses, a family of common pathogens, may be associated with CFS in patients with chronic gastro-intestinal problems.
October 2007The CFIDS Association participates in a collaborative meeting of organizations concerned with overlapping conditions such as fibromyalgia, interstitial cystitis, irritable bowel syndrome and chronic pain, providing guidance on how to expand awareness and funding that benefits patients with one or several of these disorders.
September 2007Dr. Brigitte Huber of Tufts University is awarded a research grant to study a retrovirus, HERV-K 18, as a risk factor for postviral CFS. The grant is funded by the NIH’s National Institute of Arthritis and Skin Diseases and the Office of Research on Women’s Health based on data collected during a 2004-06 pilot study funded by the CFIDS Association. It fulfills one of the main goals of the Association’s research program—to help promising investigators with pilot studies that can lead to larger studies funded by the NIH or biotech firms.
Directors with terms beginning in the 1980s
Marilyn Asbury (1988–1991) James Bavis (1989–1993) Pat Bradshaw (1988–1993) Susan Dorman (1989–1992) Alan Goldberg (1987–1996) Jonathan Goldberg (1989–1992) Betty Guthrie (1988–1994) Effie Hall (1989–1991) Jeanne Hardy (1989–1991) Mayhugh Horne (1988–1993) Kenneth Iverson (1987–1998) Marc Iverson, CPA, MBA (1987–2001; Board chairman, 1987–2000) Hal Levinson, JD (1989–1992) Richard Patterson (1989–1994) Adrienne Rosenberg, MSW (1989–1992) Kathryn Schwille (1989–1993) Cindy Teal (1989–1991) Robert Yentes (1989–1991)
Directors with terms beginning in the 1990s
Sheba Anderson (1993–1994) Debra Arnold (1993–1995) David Bell, MD (1992–1997) Jeffery Blum, MD (1993–1996) Richard Bourne, PhD (1997–1999) Coco Crum (1993–1998) Priscilla deLeon, RT (1995–2000) Thomas English, MD (1992–1994) Heather Frese (1997–1998) Bill Gareau (1993–1998) Betsy Haas, MSW (1992–1994) Bruce Hardy (1992) Barbara Hautau (1992)
Chester Helms (1991–1993) Jhan Hiber (1995–1996) Edward Isenberg (1995–1999) Wilhelmina Jenkins (1996–2000) Tim Kenny (1992–1994) Karen Lang (1997–1999) Kimberly McCleary (1996–present) Maggie McKenzie (1995–1998) Rebecca Moore Leibowitz (1995–1998) Marion Nelson (1997–1999) Allison O’Neal (1997–1998) David Patterson, CPA, MBA (1996–1998) Jane Perlmutter (1996–present) Kim Phillips (1993–1997) Lea Rhodes (1997–1999) Cathryn Rivers (1992–1994) Julia Sain (1993) Charles MacBrayer Sasser, JD (1992–2002) Patti Schmidt (1998–2004) Michael Shulimson (1992–1994) Carolyn Startsman (1992–1996) Marilyn Stewart (1994) Harriett Thompson (1992–1996) John Trussler (1997–2000 and 2002–2005; Board chairman, 2004) Marcia Wallace, MD (1998–1999) Frank Wrenn (1998–2000)
Directors with terms beginning in the 2000s
Bruce Allshouse (2005–present) Rick Baldwin (2001–2007) Lucinda Bateman, MD (2005–present) Diane Bean (2004–2005) Katrina Berne, PhD (2004–present) Barbara Comerford, JD (2003–2004) Rod Converse (2005–present) John Ginsberg, JD (2002) Terry Hedrick, PhD (2004–2007) Dennis Irwin (2001) Susan Jacobs, Esq. (2004–present; Board chairman, 2005–2007) Joseph Lane (2003–2004) Adam Lesser (2007–present) Beth Levine (2001–2003) Dimitris Papanicolaou, MD (2005–present) Mark Peterson, DDS (2003–present) Lynn Royster, PhD, JD (2004–present) Adrianne Ryan (2001–2007) Brian Smith (2007–present) Jennie Spotila, JD (2005–present; Board chairman, 2008) Amy Squires (2007–present) Jonathan Sterling (2000–2004; Board chairman, 2001–2004) Patrick Venetucci (2007–present)
D e f i n i n g M o M e n t s 20 Years of Making CFS History
Commemorating the past…The CFIDS Association of America is pleased to bring you this special magazine, which traces the journey of the CFS community and the Association through 20 years of victories and setbacks, challenges and opportunities, turmoil and hope. This journey has been filled with moments that have defined the present—and that will
help shape the future—of CFS research, advocacy, education and awareness worldwide.
We hope you enjoy this magazine, and that reflecting on past defining moments can help empower us all to create future defining moments for the CFS cause.
Defining Moments is a companion piece to the Science & Research of CFS, a special 64-page issue of the CFIDS Chronicle that covers significant research findings over the past two decades and new areas of study from around the world. This popular 2006 publication—a one-of-a-kind resource for the CFS community, health care professionals, public policy makers and the community at large—is offered in conjunction with the publication of the second magazine in the set.
D e f i n i n g M o M e n t s
Please act now!
MAKE A DONATION to help make CFS history! The progress made over the past 20 years wouldn’t have been possible without the philanthropic support of thousands of supporters. To sustain that progress and propel the CFS cause forward, we need your help.
Please consider: a gift to the CFIDS Association to support the million-dollar research initiative $ a $20 gift to help commemorate the 20th anniversary $ 20
ORDER Defining Moments and/or the Science & Research of CFS: @ $15 each ($20 for 2 copies of any combination of the 2 magazines; includes shipping and handling)
Special discount offer: Want additional copies of this magazine, or copies of the Science & Research of CFS? To commemorate the past 20 years, order 2 or more magazines (1 of each, or 2 copies of either publication) for $10 each. Call the Resource Line at 704-365-2343 for discounts on orders of 10 or more.
Look for this envelope inside.Instructions: Use the enclosed envelope to make a charitable donation or order extra copies of the companion magazines, Defining Moments: 20 Years of Making CFS History and the Science & Research of CFS.
Simply mark the appropriate box, enclose your check or credit card information and return by mail.
Proceeds support the CFIDS Association of America.
The CFIDS Association of America PO Box 220398
Charlotte, NC 28222-0398 www.cfids.org
704-365-2343
Supporting the future…With its education and public policy programs, the CFIDS Association of America has kept CFS in the spotlight for the past two decades, fostering scientific progress in understanding this complex and disabling condition. As we mark our 20-year milestone, the Association is in a unique position to accelerate the pace of progress and to channel more resources into closing the gap between knowledge about CFS and meaningful improvements in diagnosis and care.
To fuel an expanded research program, the CFIDS Association has launched a campaign to raise $1 million in 2008 for new research projects—the most ambitious campaign ever for privately funded CFS research.
Over the next year, the Association will increase funding for results-oriented research grants, host symposia to explore important scientific frontiers, and actively recruit fresh talent and build new collaborations to intensify the study of CFS.
The success of this research initiative will depend on an infusion of support from donors like you. You can make this campaign a defining moment for the entire CFS community. With your gift, you can help make CFS history.