defining response & reducing harms from clinical therapies ... · defining response &...
TRANSCRIPT
Defining response & reducing
harms from clinical therapies:
Lessons from CRT
Dr David Warriner BSc MRCP DipSEM
Cardiology Registrar, UK
@DrDavidWarriner
#PODC2016
Conflicts of interest
I refuse all meals, gifts or payments from
any industry representative.
For my full disclosure see:
http://www.whopaysthisdoctor.org
UK Drs - please consider signing up too!
@DrDavidWarriner
#PODC2016

Who am I?
Cardiology Registrar in Sheffield, South Yorkshire, UK
PhD: “The HF syndrome & predicting response to CRT”
Passionate about preventing overdiagnosis
Empowering patients, championing common sense
Not bowing to those with vested interests
@DrDavidWarriner
#PODC2016

Why am I here?
Attended PODC 2014, 2015 and 2016 (?2017)
Cardiologists were noticeable in their absence (n = 2)
But, cardiologists MUST be part of the solution
Based AoMRC for 12/12 on #choosingwisely in UK
Written, blogged & tweeted – too much medicine
Original member of Overdiagnosis UK group
@DrDavidWarriner
#PODC2016
@DrDavidWarriner
#PODC2016
Preventing Overdiagnosis
Cardiology
Heart Failure
CRT
Response
Vested interests Overtreatment Harm Guidelines Industry Decision making

Objectives
@DrDavidWarriner
#PODC2016
Learn little about heart failure and CRT
Consider problem of defining CRT response
Apply the concepts of Preventing Overdiagnosis to CRT

Cardiology
Cardiac devices e.g. pacemakers & defibrillators
Devices market worth £9 billion (€13 billion) globally in 2015
1 million devices implanted yearly (2011) & increasing
In 2014, CRT-P £8k (€9.5k) and CRT-D £18k (€22k)
R&D is important, as are devices and manufacturers
BUT - wary of influence of industry & opinion leaders
@DrDavidWarriner
#PODC2016
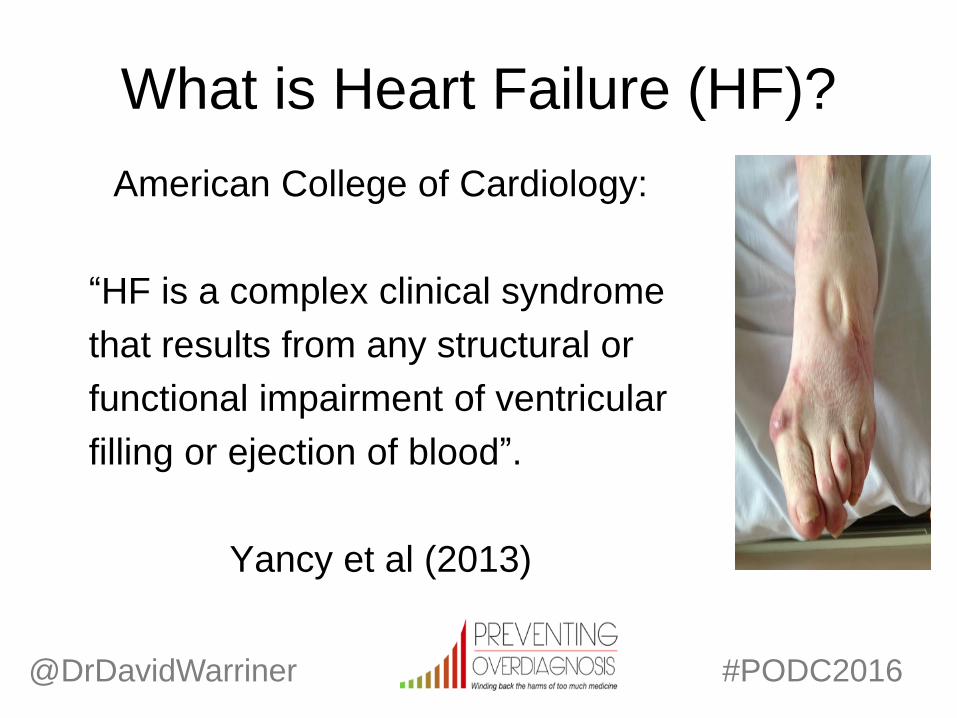
What is Heart Failure (HF)?
American College of Cardiology:
“HF is a complex clinical syndrome
that results from any structural or
functional impairment of ventricular
filling or ejection of blood”.
Yancy et al (2013)
@DrDavidWarriner
#PODC2016

The problem of HF
Prevalence - 1-2% Europe* (>10% if >70 years)
Aetiology - 62% coronary artery disease
Physiology - 50% LV systolic dysfunction (LVSD)
Symptoms - Fatigue, breathlessness & swelling
Treatment - Diuretics, β-blockers, ACE-I & MRA
*Slides prepared pre-Brexit – 1% of UK population
@DrDavidWarriner
#PODC2016
The problem of HF
Most common cause of hospitalisation > 65 years
6 month re-admission rate is 50%
Average length of inpatient stay is 2 weeks
2% of the annual NHS budget (£2 billion/€2.5 billion)
Average 5 year survival is only 50%
In short, HF is common, costly and deadly
@DrDavidWarriner
#PODC2016
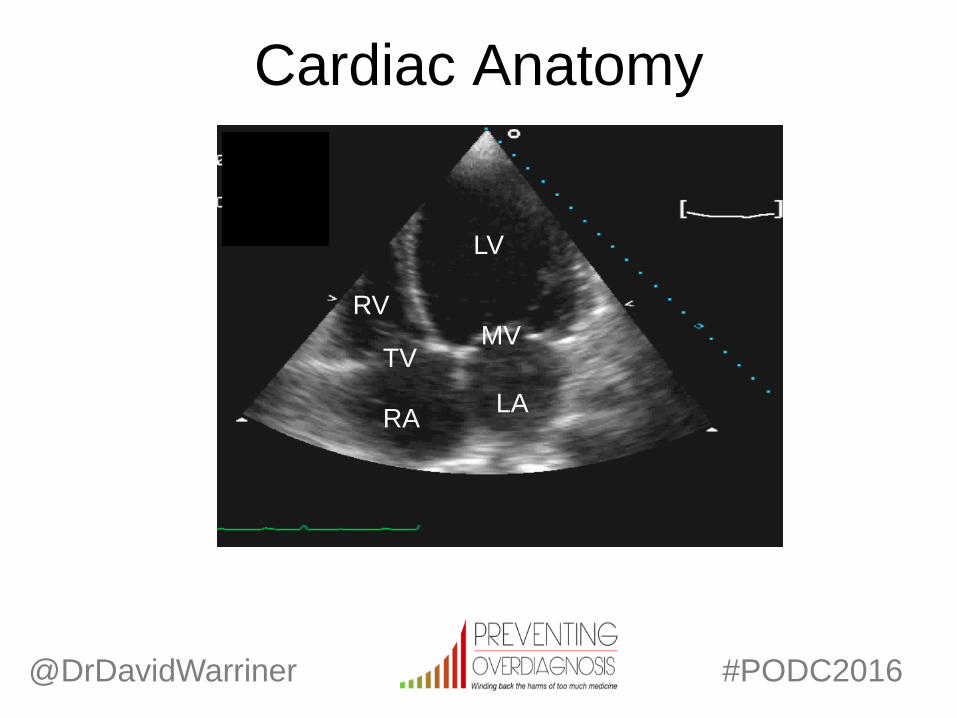
Cardiac Anatomy
LV
RV
RA LA
@DrDavidWarriner
#PODC2016
TV MV
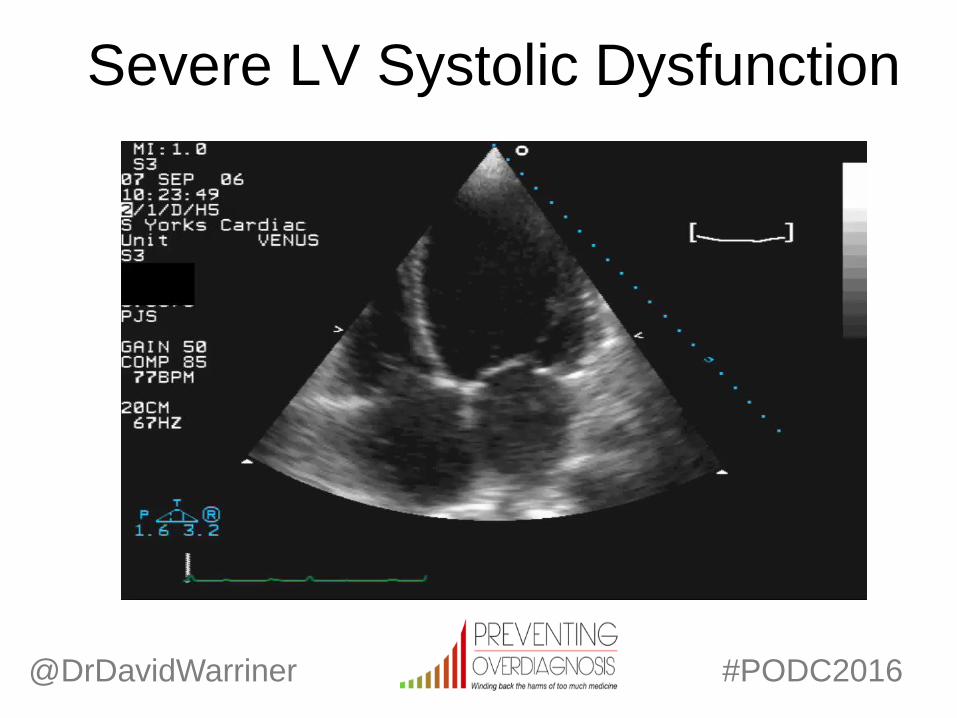
Severe LV Systolic Dysfunction
LV
RV
RA LA
@DrDavidWarriner
#PODC2016
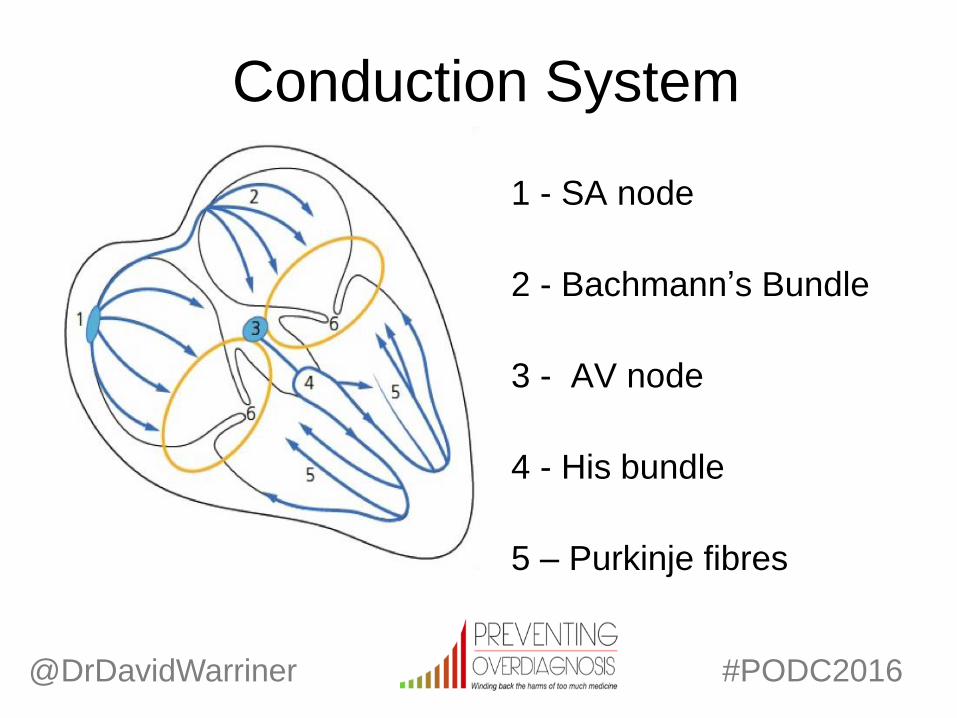
Conduction System
1 - SA node
2 - Bachmann’s Bundle
3 - AV node
4 - His bundle
5 – Purkinje fibres
@DrDavidWarriner
#PODC2016

Dyssynchrony
Atrio-ventricular, inter-ventricular & intra-ventricular
ECG – measure conduction delay e.g. PRd, QRSd
Common in LVSD-heart failure, ≥ 30% of patients
Due to ischaemia, scar and adverse dilation
Impairs cardiac filling and cardiac function
@DrDavidWarriner
#PODC2016

Conduction delay
@DrDavidWarriner
#PODC2016
Cardiac Resynchronisation
Therapy (CRT)
First introduced in early 1990’s
Patients with refractory heart failure
Already taking optimal medical therapy
RV apical pacing alone led to LVSD
Heart transplants are a scarce resource
Where next for these breathless patients?
@DrDavidWarriner
#PODC2016

CRT
A pacemaker with 3 leads - RA, RV and LV
Electrically ‘rewires’ a dysynchronous heart
Improves symptoms, morbidity and mortality
Patients must fulfill specific pre-implantation criteria
Efficacy proven in many trials & NICE/AHA/ESC approved
CRT-P = pacemaker only vs CRT-D = defibrillator function
@DrDavidWarriner
#PODC2016

CRT implantation
The procedure takes between 1 – 3 hours
Aseptic technique under LA and sedation
Incision in left pectoral region and subcutaneous pocket made
Venous access gained to cephalic, axillary or subclavian vein
Leads then passed to RA, RV and LV (via CS)
Screwed into generator and skin sutured close
@DrDavidWarriner
#PODC2016
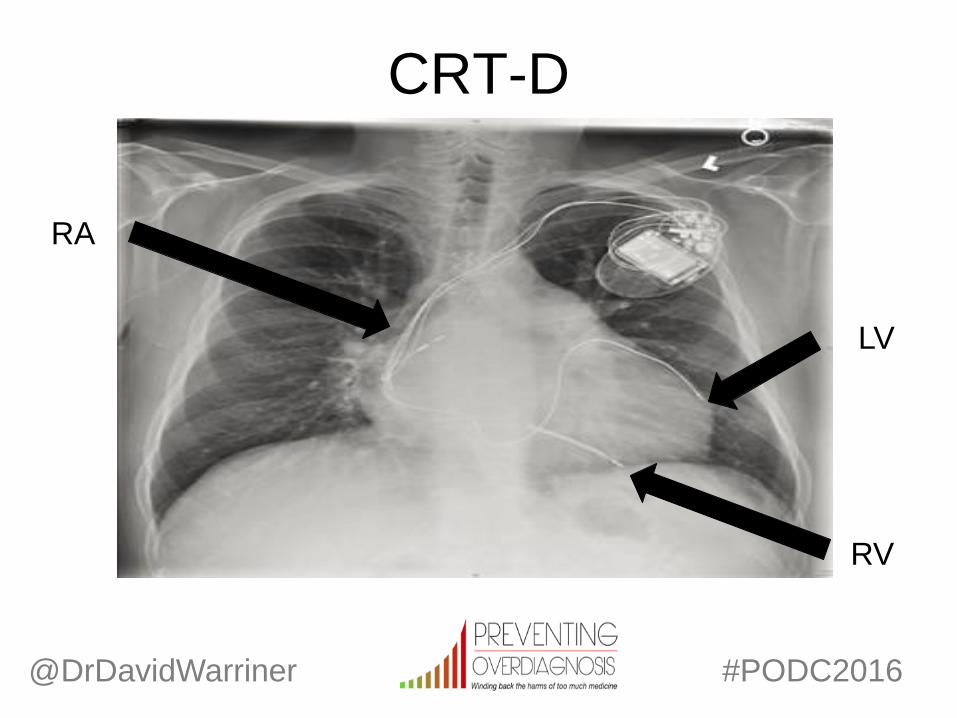
CRT-D
RA
RV
LV
@DrDavidWarriner
#PODC2016
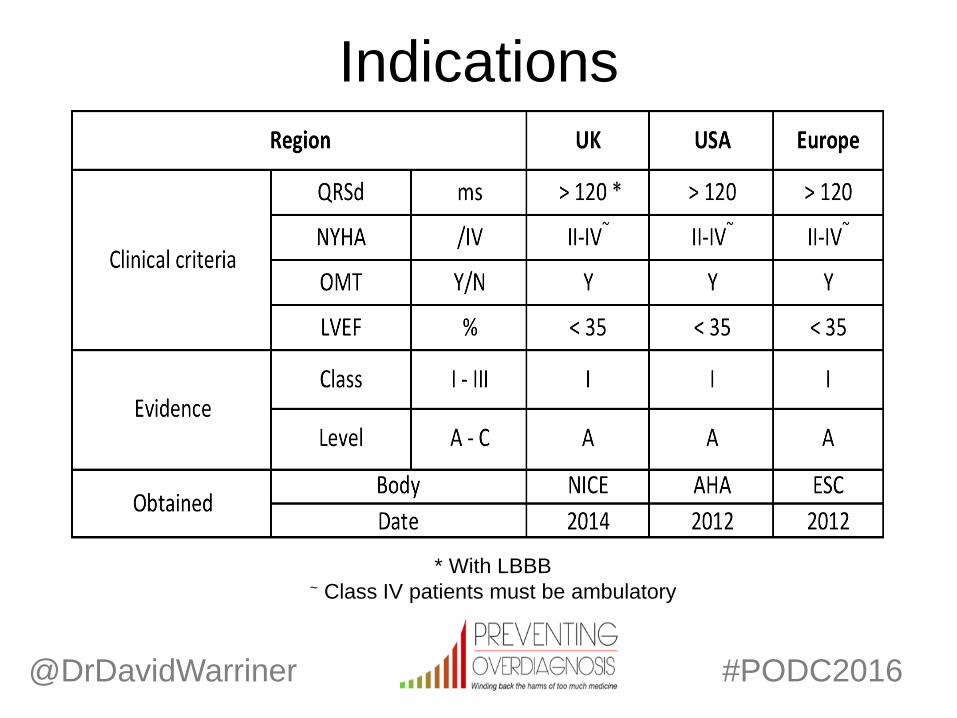
Indications
@DrDavidWarriner
#PODC2016
* With LBBB ~ Class IV patients must be ambulatory

@DrDavidWarriner
#PODC2016
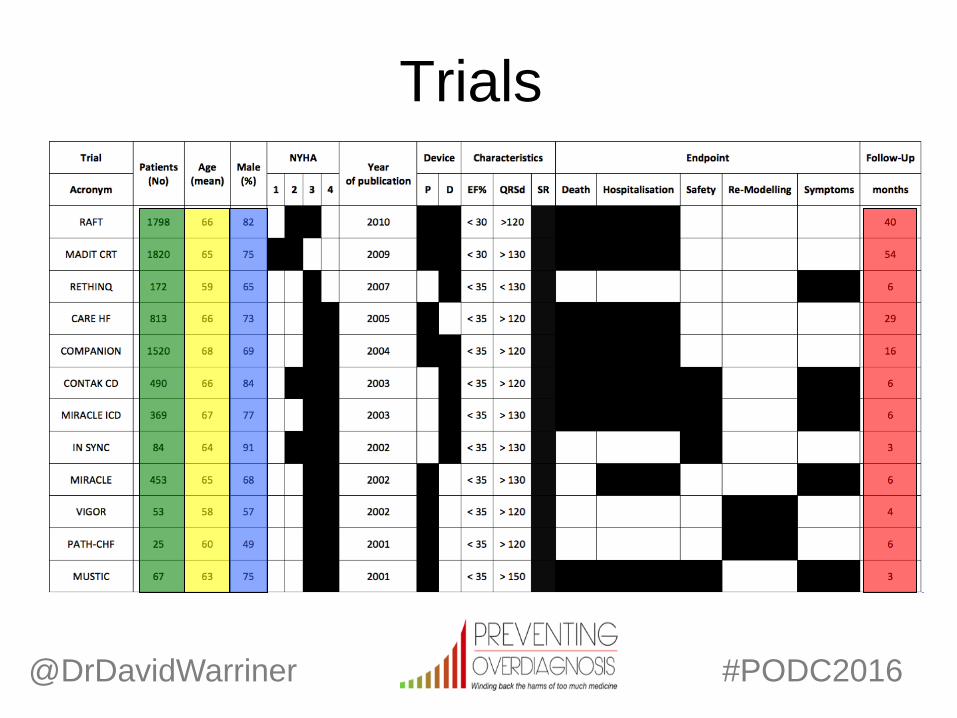
Trials
@DrDavidWarriner
#PODC2016
Trials
Response
~70% of patients “respond” to CRT
Definition of response is very variable
Therefore, how can you tell if a patient has got better?
Must define response, in order to predict it
Subjective e.g. functional class or quality of life
Objective e.g. imaging, biomarker or exercise capacity
@DrDavidWarriner
#PODC2016
Preventing overdiagnosis
Majority of trials industry funded
Majority of trials positive
Majority of trials exclude significant comorbidity
No universal consensus on “response”
Response is not just a one-off biomarker
1/3 patients risk of harm w/o likelihood of benefit
@DrDavidWarriner
#PODC2016

*Pause*
@DrDavidWarriner
#PODC2016
EXPERTS HOLD SUMMIT

NEWS FLASH! NEW “LIVE SAVING” CRT DEVICE
IN SMALL GROUPS YOU’LL BE GIVEN A SERIES
OF TASKS TO WORK ON OVER NEXT 60 MIN.
DICUSSING HOW TO MEASURE
RESPONSE FROM SUCH A HEART FAILURE
DEVICE
Preventing Overdiagnosis does...
….. defining response.
@DrDavidWarriner
#PODC2016
Task No. 1
How would you define
response to a
treatment and why?
@DrDavidWarriner
#PODC2016
Defining response
Halting disease progression and sequelae
Reducing admissions & mortality is important
But patients also want to feel better
Doctors also want patients to feel better
If the patient feels no better – why was this implanted?
Is response even the right word….
@DrDavidWarriner
#PODC2016
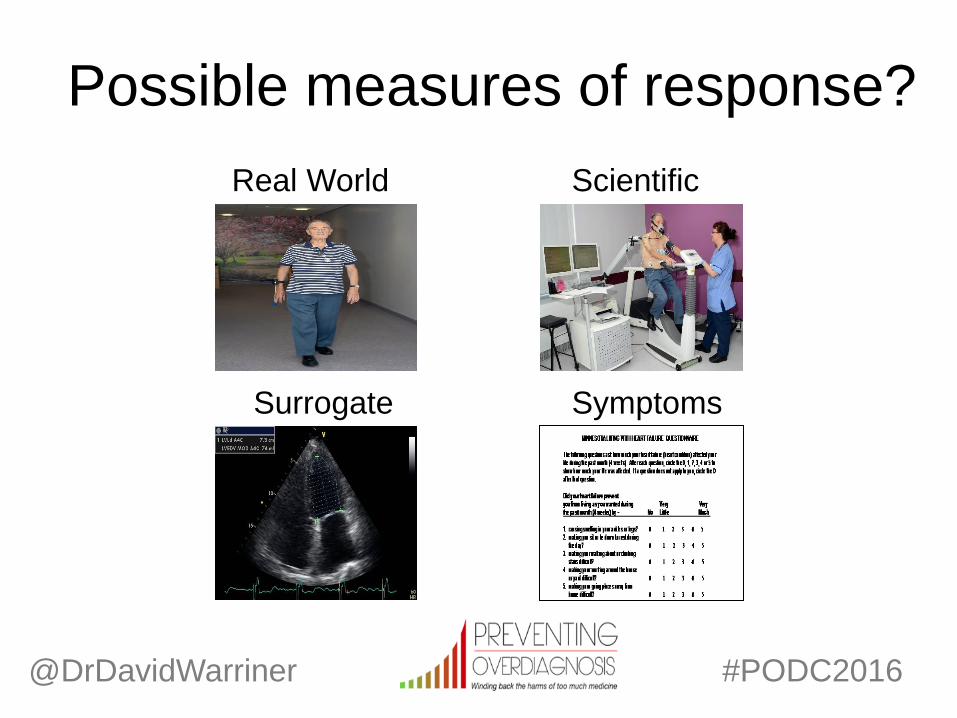
Possible measures of response?
@DrDavidWarriner #PODC2016
Scientific Real World
Surrogate Symptoms
Task No. 2
Which would be the
best measure of
response and why?
@DrDavidWarriner
#PODC2016

Rank these in order (1-4)
Real World e.g. 6WMD
Exercise -
Scientific e.g. CPET
Surrogate e.g. LV volumes or EF%
Symptoms e.g. NYHA, MLWHFQ
@DrDavidWarriner
#PODC2016
Defining response
In research, usually a combination of measures
In clinic, usually only symptom based
@DrDavidWarriner
#PODC2016
Response isn’t Black and
Super-responders Responders Non-responders ???
Much better Better No better Worse
@DrDavidWarriner
#PODC2016

A combination e.g. research
Which combination?
How many?
How measured?
By whom?
What if mixed results?
What is the key measure?
@DrDavidWarriner
#PODC2016
Combination. Sure?
Bleeker et al (2006) 70% of CRT
responders improved by at least one
NYHA functional class but only 56% of
patients had >15% reduction in LVEDV
and 51% met both criteria
@DrDavidWarriner
#PODC2016
Symptoms alone e.g. clinic
Single clinic visit post implant
Usually assessed by the implanting physician
If feel better – discharged back to referrer
If not – look at reasons why
May look at device optimisation
@DrDavidWarriner
#PODC2016

Symptoms alone. Sure?
MIRACLE-ICD Trial (CRTD vs ICD)
62% vs 46% improved ≥ 1 NYHA class
CONTAK CD TRIAL (CRT on vs CRT off)
73% vs 53% improved ≥ 1 NYHA class
MIRACLE Trial (CRT vs OMT)
68% vs 38% improved ≥ 1 NYHA class
@DrDavidWarriner
#PODC2016
Threshold of response
Low e.g. 1% improvement
Clinically Meaningless
Most will be responders
Scientifically unsound
High e.g. 99% improvement
Clinically Implausible
Few will be responders
Scientifically unsound
@DrDavidWarriner
#PODC2016
Task No. 3
What threshold of improvement should
define response and why?
@DrDavidWarriner
#PODC2016
0% 100%
Definitions of response in CRT
Subjective
Symptoms – 1 point in NYHA functional class
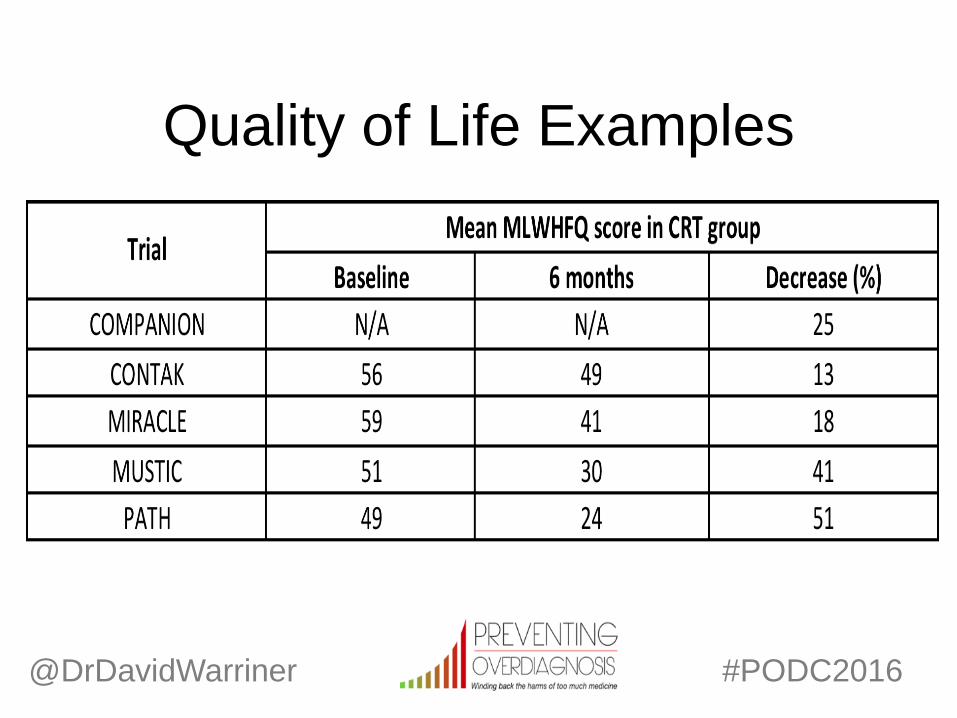
Quality of Life – 10% in MLWHFQ score
Objective
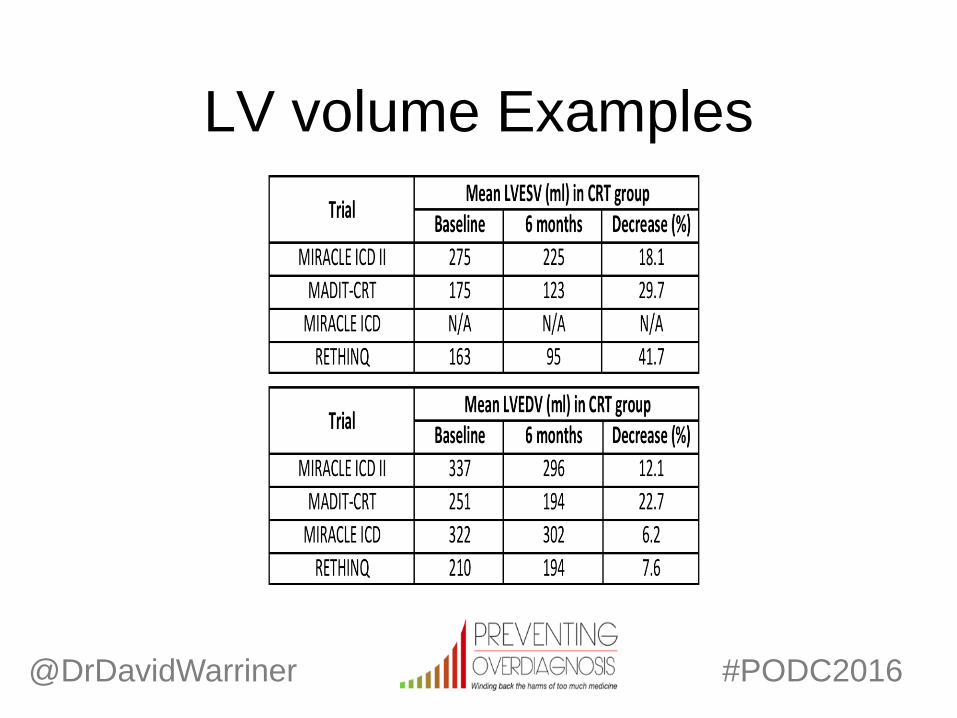
Imaging – 10-15% in LV volumes
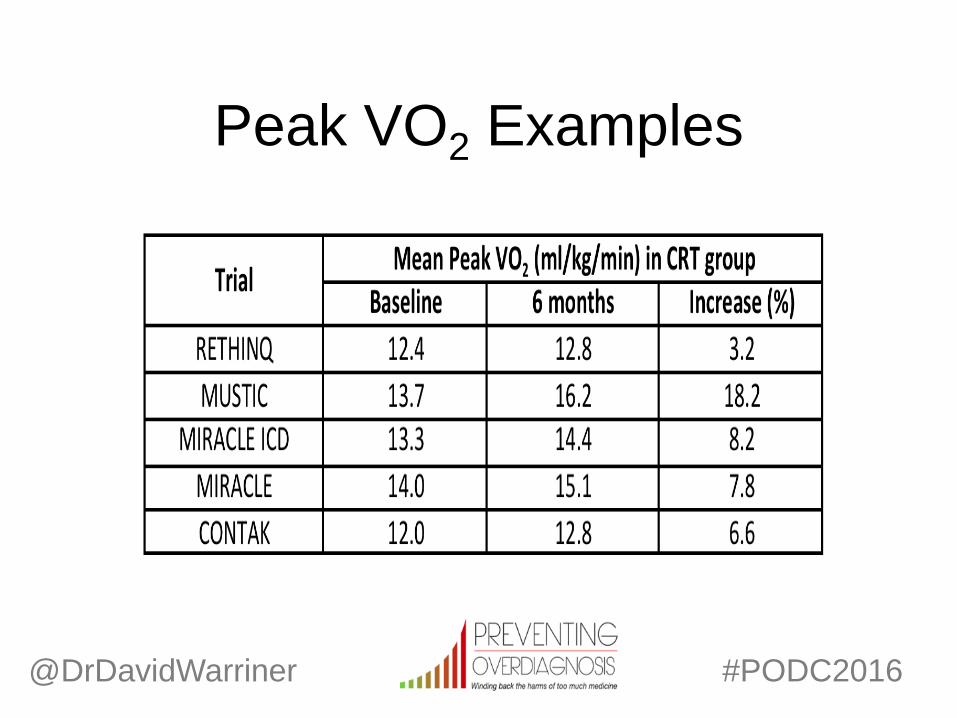
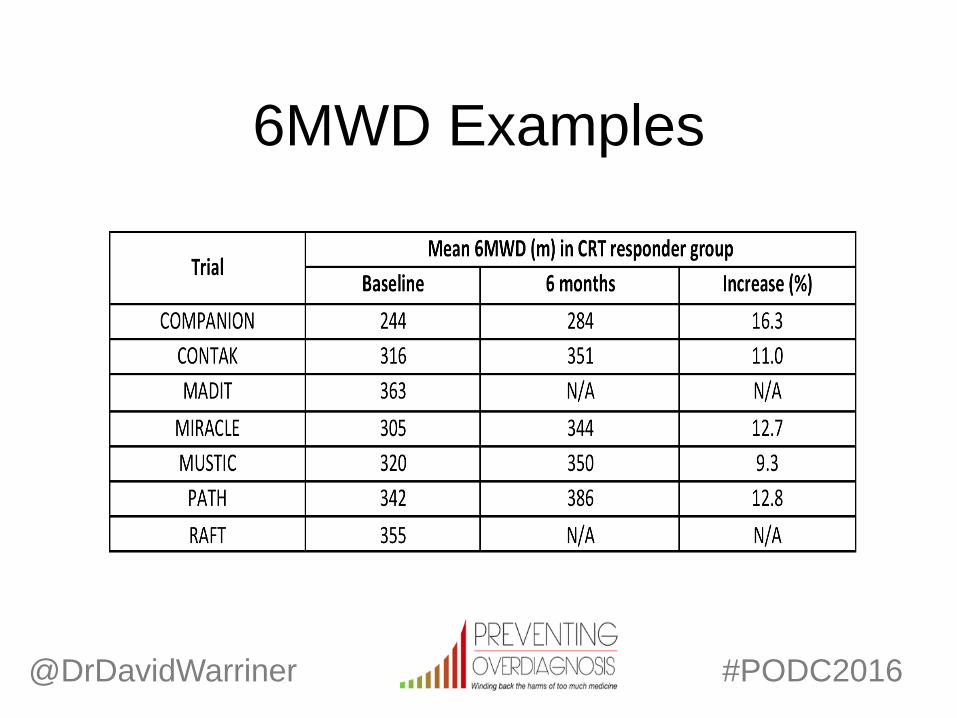
Exercise - 1.0 ml/kg/min in peak VO2 or 10% in 6MWD
@DrDavidWarriner
#PODC2016
@DrDavidWarriner
#PODC2016
Quality of Life Examples
@DrDavidWarriner
#PODC2016
Peak VO2 Examples
@DrDavidWarriner
#PODC2016
6MWD Examples
@DrDavidWarriner
#PODC2016
LV volume Examples

Timing of response
Early – low dropout, acute response, delayed effect?
Late – higher dropout, all responders, confounders
Single – definitive, simpler stats, binary, chance
Multiple – progressive, ecological validity, richer data
@DrDavidWarriner
#PODC2016
Task No. 4
What time interval(s) should be used to
measure response and why?
@DrDavidWarriner
#PODC2016
Baseline Hours Days Weeks Months Years

Timing interval
Complex.
Arguably, a higher frequency of sampling
over a longer time period, more likely to
equate to “response means response”
@DrDavidWarriner
#PODC2016
Timing interval Hauptman et al (2004): Variation in clinical HF status
116 patients with NYHA 3-4 class LVSD-HF over 6 weeks
30% better, 53% unchanged, 17% worse (statistically significant)
Better – 148m in 6MWD & 17 point in KCCQ
Worse - 107m in 6MWD & 7 point in KCCQ
Random variation – 30% patients improve w/o intervention
@DrDavidWarriner
#PODC2016
The problem of syndromes
ACC: “HF is a complex clinical syndrome”
Yancy et al (2013)
It is not a single disease, like hypertension for
example, measuring BP, prescribing a single
drug and then remeasuring BP
@DrDavidWarriner
#PODC2016

AHA Guidelines 2009
Cardiac factors influencing
symptoms, including “ventricular
distensibility, valvular regurgitation,
pericardial restraint, conduction
disturbance, cardiac rhythm and right
ventricular function.”
@DrDavidWarriner
#PODC2016

AHA guidelines 2009 cont.
Non-cardiac factors influencing
symptoms such as “abnormal
peripheral vascular function, skeletal
muscle physiology, pulmonary dynamics,
neurohormonal and reflex autonomic
activity, and renal sodium handling.”
@DrDavidWarriner
#PODC2016
Task No. 5
Is measuring response be a
challenge and why?
@DrDavidWarriner
#PODC2016
Yes.
Brand new, innovative, expensive device
To improve LV systolic function
BUT
LVSD-HF isn’t a simple, single organ disease
It’s a complex, multi-organ syndrome
Therefore, not just LV systolic function that determines symptoms
@DrDavidWarriner
#PODC2016

@DrDavidWarriner
#PODC2016
Comorbidity in HF is common
“Over 40% of patients will have 5 or more
comorbidities accounting for 80% of total inpatient
episodes” Braunstein et al (2003)
AF (30%)
Chronic kidney disease (50%)
Chronic lung disease (20%)
OSA/CSA (10/30%)
Sarcopenia (10%)
Anaemia (20%)
Chronic liver disease (50%) Diabetes (20%)
Endothelial dysfunction (30%) Cerebrovascular disease (9%)
Thyroid disease (14%)
Osteoporosis (5%)
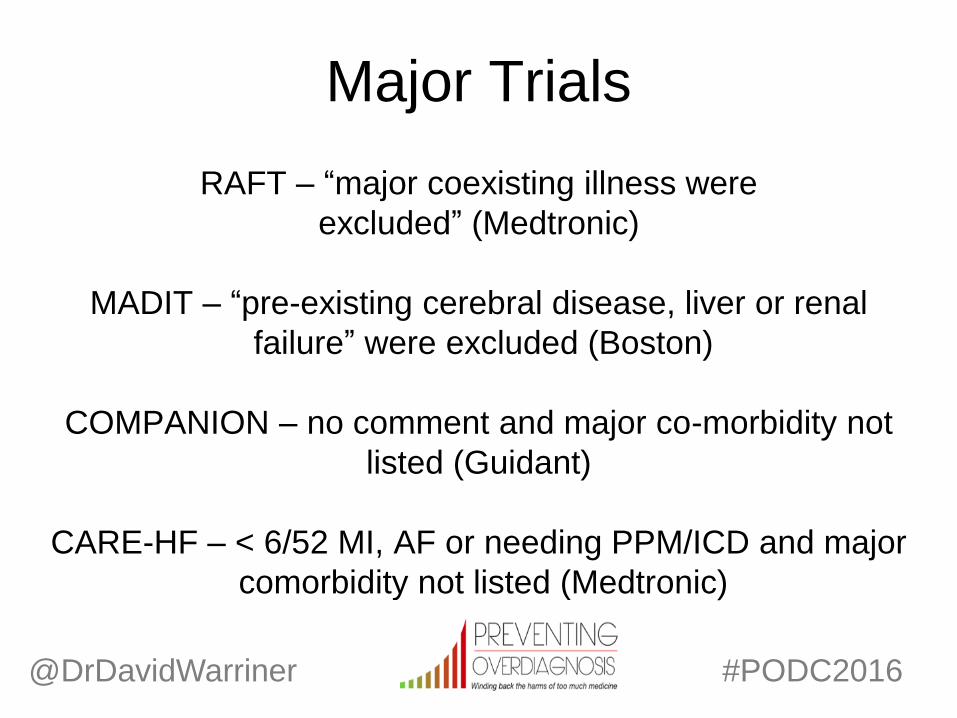
Major Trials
RAFT – “major coexisting illness were
excluded” (Medtronic)
MADIT – “pre-existing cerebral disease, liver or renal
failure” were excluded (Boston)
COMPANION – no comment and major co-morbidity not
listed (Guidant)
CARE-HF – < 6/52 MI, AF or needing PPM/ICD and major
comorbidity not listed (Medtronic)
@DrDavidWarriner
#PODC2016
@DrDavidWarriner
#PODC2016
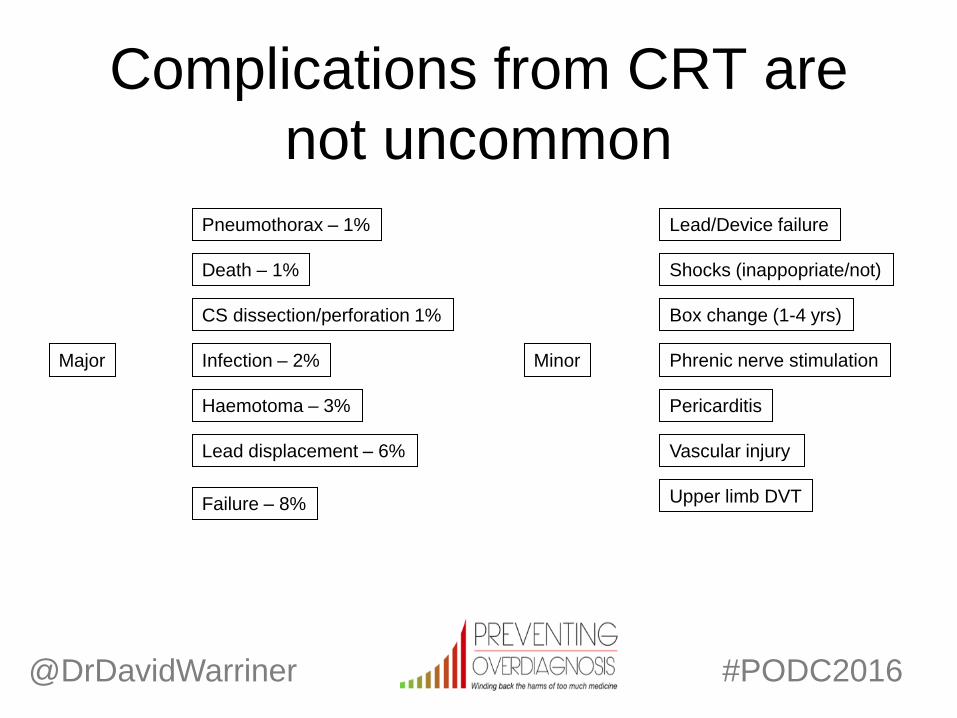
Major Infection – 2%
Pneumothorax – 1%
Haemotoma – 3%
Death – 1%
Lead displacement – 6%
Failure – 8%
CS dissection/perforation 1%
Complications from CRT are
not uncommon
Phrenic nerve stimulation
Pericarditis
Vascular injury
Minor
Box change (1-4 yrs)
Shocks (inappopriate/not)
Lead/Device failure
Upper limb DVT
Objectives
Learn little about heart failure and CRT
Consider problem of defining CRT response
Apply the concepts of Preventing Overdiagnosis to CRT
@DrDavidWarriner
#PODC2016

Balance of probabilities
@DrDavidWarriner
#PODC2016
70% Response
90% Caucasian
75% Male
No comorbidity
30% Non-response
10% Complications
40% ≥ 5 Co-morbidities
Ethnic minority
Female
Summary
Defining response to treatments is problematic
We want our patients to feel better, as do they
Not just improve abstract imaging or biomarkers
Need a open conversation on what we define as better
Otherwise comparing and applying data is meaningless
Response = significant, sustained, multifactorial, specific
@DrDavidWarriner
#PODC2016

Conclusions
1/3 of patients don’t derive benefit from CRT
This is overtreatment
But…
Because we are unable agree on “response”
Therefore we are unable to predict “response”
Unable to identify a priori and prevent possible harm
@DrDavidWarriner
#PODC2016