delirium in the pediatric intensive care unit in the pediatric intensive care unit recognition,...
TRANSCRIPT

Delirium in the Pediatric Intensive Care Unit
Recognition, Prevention and Treatment
Shad Outsen, MDDirector, Pediatric Intermediate Care, Utah Valley HospitalPediatric Intensivist, Primary Children’s Hospital

Objectives
• Understand how delirium negatively impacts patients
• Use a validated score to diagnose delirium in the pediatric population
• Implement strategies to prevent and treat delirium
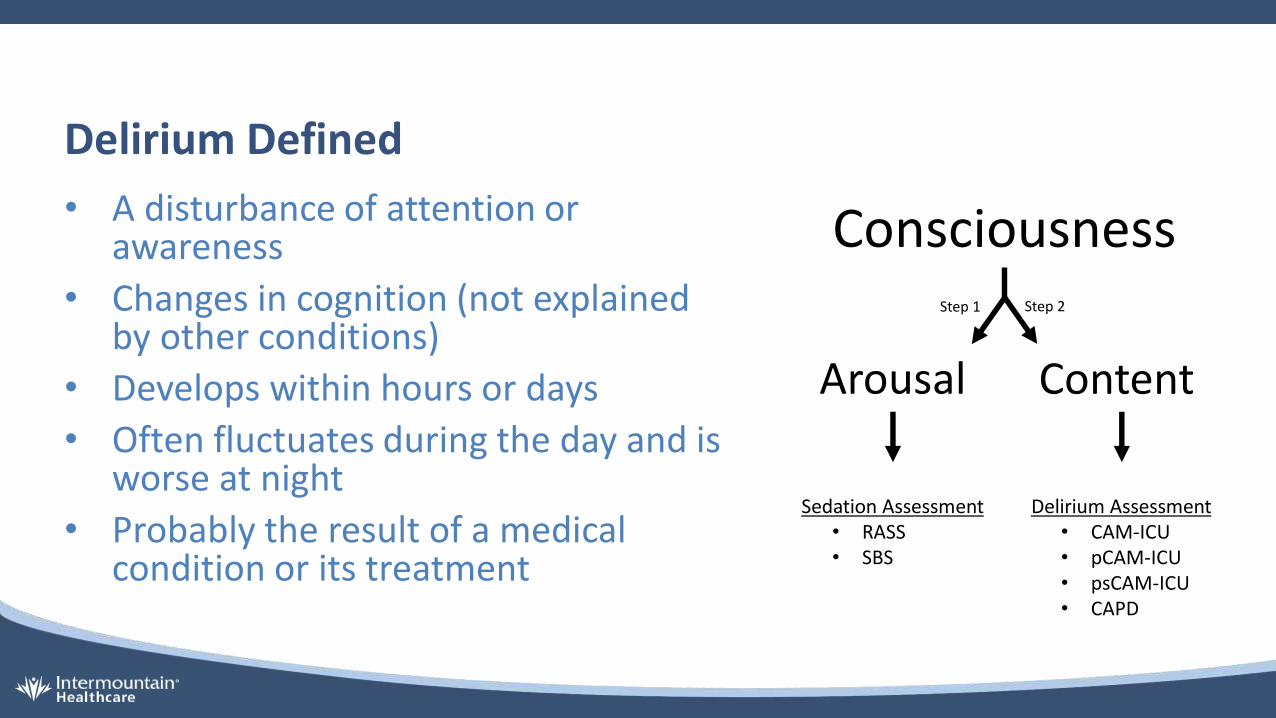
Delirium Defined
• A disturbance of attention or awareness
• Changes in cognition (not explained by other conditions)
• Develops within hours or days
• Often fluctuates during the day and is worse at night
• Probably the result of a medical condition or its treatment
Consciousness
Arousal Content
Sedation Assessment• RASS• SBS
Delirium Assessment• CAM-ICU• pCAM-ICU• psCAM-ICU• CAPD
Step 1 Step 2

In adult ICU patients…
Is independently predicted by:• Age
• Dementia
• Emergency surgery or trauma
• Severity of illness• Metabolic acidosis
• Benzodiazepines
• Coma
• Mechanical ventilation 60-80%
Independently predicts:
• Prolonged mechanical ventilation
• ↑ length of hospitalization
• ↑ 6-month mortality
• Long-term cognitive impairment
• ↑ medical costs

In pediatric ICU patients…
Independently predicted by:• Age ≤ 2 years• Developmental delay• Severity of illnesso Infectious and inflammatory disorders
• Coma status• Mechanical ventilation• Use of physical restraints• Medicationso Benzodiazepines
o Anticholinergics
o Vasopressors
o Antiepileptics
Independently predicts:• ↑ PICU LOS
• ↑ Hospital LOS
• ↑ duration of mechanical ventilation
• ↑ mortality• Posttraumatic stress symptoms
• Delusional memories or disturbing hallucinations 33%

Delirium in Pediatric ICU Patients
• Overall 17-25%oMedian duration 2 days
o78% develop delirium within first 3 PICU days• 20% in first 5 PICU days
• 38% after day 5
oMechanical ventilation 53%
• 3 typesoHypoactive 46%
oMixed 45%
oHyperactive 8%

Screening for DeliriumThe Cornell Assessment of Pediatric Delirium (CAPD)• Done at least one time per shifto At end of shifto Takes less than 2 minutes
• CAPD score ≥ 9 is a positive screen
• Sensitivity 94%, specificity 79%o Without developmental delay, 92%
and 87%o With delay, 96% and 51%

Anchors


Preventing Delirium
• Reduce medication exposureo Sedate as lightly as possible• Measure sedation levels
oAnalgesia first sedation
oAvoid benzodiazepines and anticholinergics
o Intermittent rather than continuous
o Spontaneous awake trials
• Protect sleepo Cluster cares!
oMinimizing overhead pages
o Turn off TV’s, soothing music
oDim hallway lights and darken room
o Earplugs and eye masks
oNoise reduction
oAvoid caffeine
oMelatonin or Ambien

Treating Delirium
• Investigate for underlying illness
• Investigate for iatrogenic causeso Iatrogenic Withdrawal Syndrome
• Investigate for abnormal environment
• Pharmacological treatmentoQuetiapine (Seroquel)
oRisperidone
oHaloperidol

Summary
• Delirium is an acute alteration in awareness, attention and cognition.• Pediatric delirium is associated with increased morbidity and mortality. • Pediatric delirium occurs in as many as 25% of critically ill children and in as many as
50% of mechanically ventilated children.• The CAPD score effectively screens for delirium at any age in pediatric patients with or
without developmental delay and should be performed one time per shift.• Preventing delirium includes reducing exposure to medications, particularly
benzodiazepines, and maintaining normal circadian rhythms.• When delirium is diagnosed, caregivers should investigate for underlying illness,
iatrogenic causes and environmental causes.• Certain antipsychotic medications have been used safely to treat pediatric delirium.

ReferencesTraube, C., Silver, G., Gerber, L. M., Kaur, S., Mauer, E. A., Kerson, A., et al. (2017). Delirium and Mortality in Critically Ill Children: Epidemiology and Outcomes of Pediatric Delirium. Critical Care Medicine, 45(5), 891–898.
Traube, C., Silver, G., Reeder, R. W., Doyle, H., Hegel, E., Wolfe, H. A., et al. (2017). Delirium in Critically Ill Children: An International Point Prevalence Study. Critical Care Medicine, 45(4), 584–590.
Harris, J., Ramelet, A.-S., van Dijk, M., Pokorna, P., Wielenga, J., Tume, L., et al. (2016). Clinical recommendations for pain, sedation, withdrawal and delirium assessment in critically ill infants and children: an ESPNIC position statement for healthcare professionals. Intensive Care Medicine, 42(6), 972–986.
Silver, G., Traube, C., Gerber, L. M., Sun, X., Kearney, J., Patel, A., & Greenwald, B. (2015). Pediatric Delirium and Associated Risk Factors. Pediatric Critical Care Medicine, 16(4), 303–309.
Weinhouse, G. L. (2015). When Perception May Not Meet Reality. Critical Care Medicine, 43(1), 248–249.
Zaal, I. J., Devlin, J. W., Peelen, L. M., & Slooter, A. J. C. (2015). A Systematic Review of Risk Factors for Delirium in the ICU*. Critical Care Medicine, 43(1), 40–47.
Kamdar, B. B., Niessen, T., Colantuoni, E., King, L. M., Neufeld, K. J., Bienvenu, O. J., et al. (2015). Delirium transitions in the medical ICU: exploring the role of sleep quality and other factors. Critical Care Medicine, 43(1), 135–141.
Kudchadkar, S. R., Yaster, M., & Punjabi, N. M. (2014). Sedation, Sleep Promotion, and Delirium Screening Practices in the Care of Mechanically Ventilated Children: A Wake-Up Call for the Pediatric Critical Care Community*. Critical Care Medicine, 42(7), 1592–1600.
Traube, C., Silver, G., Kearney, J., Patel, A., Atkinson, T. M., Yoon, M. J., et al. (2014). Cornell Assessment of Pediatric Delirium. Critical Care Medicine, 42(3), 656–663.
Kamdar, B. B., King, L. M., Collop, N. A., Sakamuri, S., Colantuoni, E., Neufeld, K. J., et al. (2013). The effect of a quality improvement intervention on perceived sleep quality and cognition in a medical ICU. Critical Care Medicine, 41(3), 800–809.
Barr, J., Fraser, G. L., Puntillo, K., Ely, E. W., Gélinas, C., Dasta, J. F., et al. (2013). Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. Critical Care Medicine, 41(1), 278–280.
Smith, H. A. B., Boyd, J., Fuchs, D. C., Melvin, K., Berry, P., Shintani, A., et al. (2011). Diagnosing delirium in critically ill children: Validity and reliability of the Pediatric Confusion Assessment Method for the Intensive Care Unit*. Critical Care Medicine, 39(1), 150–157.