dementia state plan and innovations in caregiver support and dementia care
TRANSCRIPT
VIRGINIA’S DEMENTIA STATE PLAN
Ms. Courtney Tierney, MSW Director Prince William County Department of Social Services
Dr. Patricia Slattum
Director, Geriatric Pharmacotherapy Program
Virginia Commonwealth University
The Alzheimer’s Disease and Related Disorders Commission
Established in 1982 by the Virginia
General Assembly
§ 51.5-154 of the Code of Virginia
15 Members; Quarterly Meetings
Advises the Governor and
General Assembly on policy, funding,
regulatory and other issues related to
Duties and Powers1 • Examine the needs and ways that state government can most effectively and
efficiently assist in meeting those needs;
2 • Develop and promote strategies to encourage brain health and reduce cognitive
decline;
3 • Advise the Governor and General Assembly;
4 • Develop the Commonwealth's plan for meeting the needs;
5 • Submit annual reports on activities to the Governor, General Assembly, and DARS;
and
6 • Establish priorities for programs among state agencies and criteria to evaluate these
programs.

Work Groups
Training Data & Research
Coordinated CareLegislative
Timeline: Dementia State Plan2009-2010 • Review other
state plans • Five public
listening sessions + comments received 2010-2011
• Drafted DSP • Public listening
sessions + comments received
Dec 2011 • Publication of
the 2011-2015 DSP
2014-2015 • Drafted Update
to DSP • Public listening
sessions + comments receivedOctober 2015
• Publication of 2015-2019 DSP

Goal 1 • Coordinate Quality Dementia Services in the Commonwealth to Ensure Dementia
Capability
Goal 2 • Use Dementia Related Data to Improve Public Health Outcomes
Goal 3 • Increase Awareness and Create Dementia-Specific Training
Goal 4 • Provide Access to Quality Coordinated Care for Individuals with Dementia in the Most
Integrated Setting
Goal 5 • Expand Resources for Dementia-Specific Translational Research and Evidence-Based
Practices

Goal One: Tracking Progress
OBJECTIVES ACTIONS
A. Create a dementia services coordinator
1. Approved; DSC started on July 25, 2013
B. Expand availability and access of dementia capable Medicaid and other state-level services
1. 2015: Modified DMAS Alzheimer’s Assisted Living Waiver for eligibility 2. 2014: Increased public guardianship funding by $599,700 3. 2014: Amended code for ombudsman’s access to records 4. 2013: DARS receives Lifespan Respite Voucher Grant 5. 2013 GA Funding Increases or Restorations: a. Auxiliary Grant by 3% b. Medicaid adult day rates (about $10/unit increase) c. Medicaid LTC services in FY 2014 to elderly and disabled individuals with incomes up to 300% of SSI payment level
C. Review all state-funded services to ensure dementia-capable approaches and policies based on principles derived from the person-centered care and culture change movements
1. 2014 Dementia care best practices report prepared and disseminated on AlzPossible
Coordinate Quality Dementia Services in the Commonwealth to Ensure Dementia Capability

Goal One: Next Steps
OBJECTIVES ACTIONS
A. Support and maintain a dementia services coordinator
Ongoing
B. Expand availability and access of dementia capable Medicaid and other state-level services
1. ADSSP grant to advance dementia capability of the aging and disability resource network and provide caregiver support
2. Support workgroup efforts to modify or replace the AAL waiver
C. Review all state-funded services to ensure dementia-capable approaches and policies based on principles derived from the person-centered care and culture change movement
1. Commission and DSC are continuing to monitor and disseminate best practices
Coordinate Quality Dementia Services in the Commonwealth to Ensure Dementia Capability
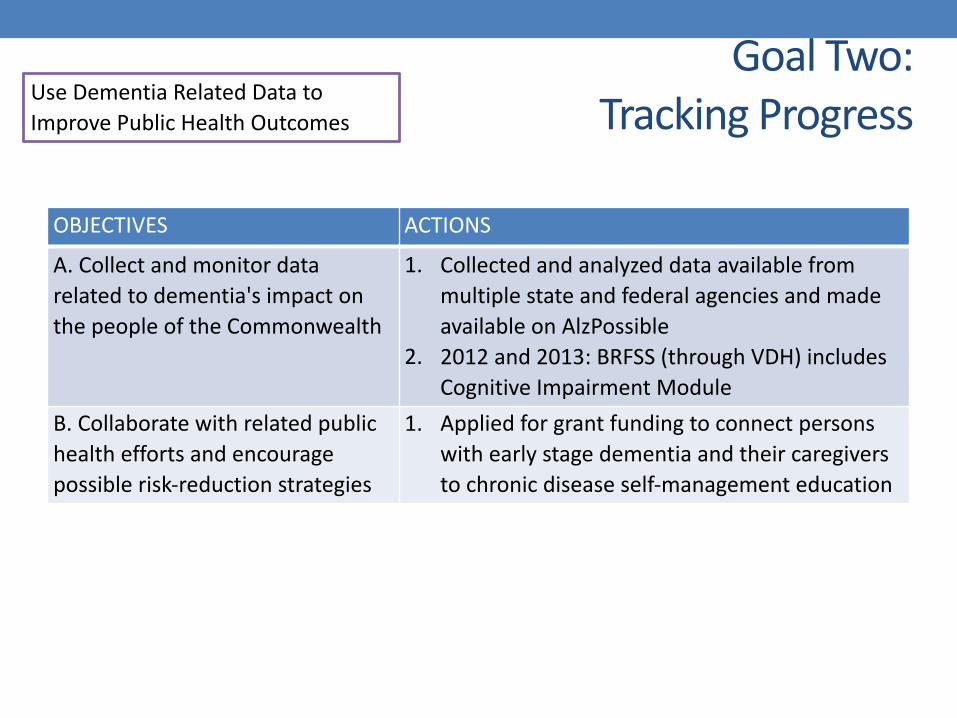
Goal Two:Tracking Progress
OBJECTIVES ACTIONS
A. Collect and monitor data related to dementia's impact on the people of the Commonwealth
1. Collected and analyzed data available from multiple state and federal agencies and made available on AlzPossible
2. 2012 and 2013: BRFSS (through VDH) includes Cognitive Impairment Module
B. Collaborate with related public health efforts and encourage possible risk-reduction strategies
1. Applied for grant funding to connect persons with early stage dementia and their caregivers to chronic disease self-management education
Use Dementia Related Data to Improve Public Health Outcomes

Goal Two:Next Steps
Use Dementia Related Data to Improve Public Health Outcomes
OBJECTIVES ACTIONS
A. Collect and monitor data related to dementia's impact on the people of the Commonwealth
1. Review 2015 BRFSS data when available 2. Developing plan to regularly update data
reporting
B. Collaborate with related public health efforts to encourage possible risk-reduction strategies
1. Continue pursuing funding for public health-related efforts

Goal Three:Tracking Progress
OBJECTIVES ACTIONS
A. Provide standardized dementia specific training to individuals in the health-related fields and require demonstrated competency
1. 2015: ADSSP grant obtained to train options counselors, care transitions coaches and information and referral specialists
2. 2012-2013: CMS launches initiative to reduce antipsychotic medications in residents with dementia (Hand in Hand Toolkit given to all certified NFs)
3. 2012-2016: VCOA Virginia Geriatric Education Center continues with trainings under HRSA grant
4. 2011-2015: 25 webinars on dementia-related topics for over 2,000 formal and informal caregivers on AlzPossible
B. Provide dementia specific training to professional first responders (police, fire, EMS and Search & Rescue personnel), financial services personnel, and the legal profession
1. 2016: DCJS partnering with IACP to provide 5 one-day trainings for 250 first responders with $50,000 ongoing funding
2. 2010: Commission successfully advocates for the restoration of funding for First Responders Training for 2011
C. Support caregivers, family members and individuals with dementia by providing educational information about dementia and available resources and services
1. 2011-2015: Continued maintenance of the AlzPossible/VACAPI website and platform
2. 2011-2015: Continued partnership with Alzheimer’s Association Chapters and AAAs
Increase Awareness and Create Dementia Specific Training
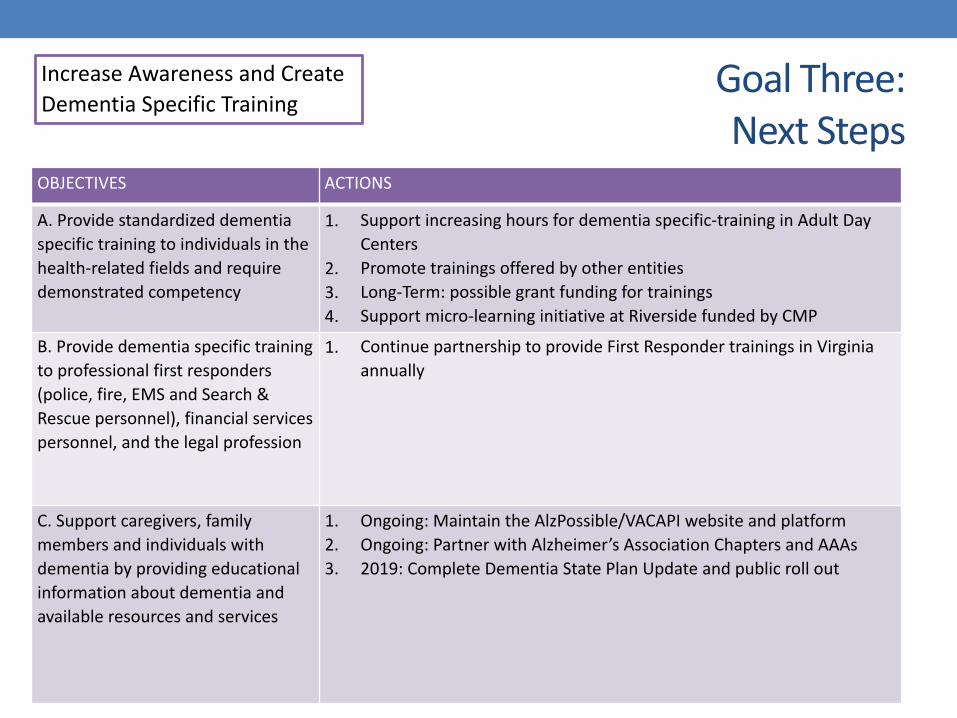
Goal Three:Next Steps
OBJECTIVES ACTIONS
A. Provide standardized dementia specific training to individuals in the health-related fields and require demonstrated competency
1. Support increasing hours for dementia specific-training in Adult Day Centers
2. Promote trainings offered by other entities 3. Long-Term: possible grant funding for trainings 4. Support micro-learning initiative at Riverside funded by CMP
B. Provide dementia specific training to professional first responders (police, fire, EMS and Search & Rescue personnel), financial services personnel, and the legal profession
1. Continue partnership to provide First Responder trainings in Virginia annually
C. Support caregivers, family members and individuals with dementia by providing educational information about dementia and available resources and services
1. Ongoing: Maintain the AlzPossible/VACAPI website and platform 2. Ongoing: Partner with Alzheimer’s Association Chapters and AAAs 3. 2019: Complete Dementia State Plan Update and public roll out
Increase Awareness and Create Dementia Specific Training
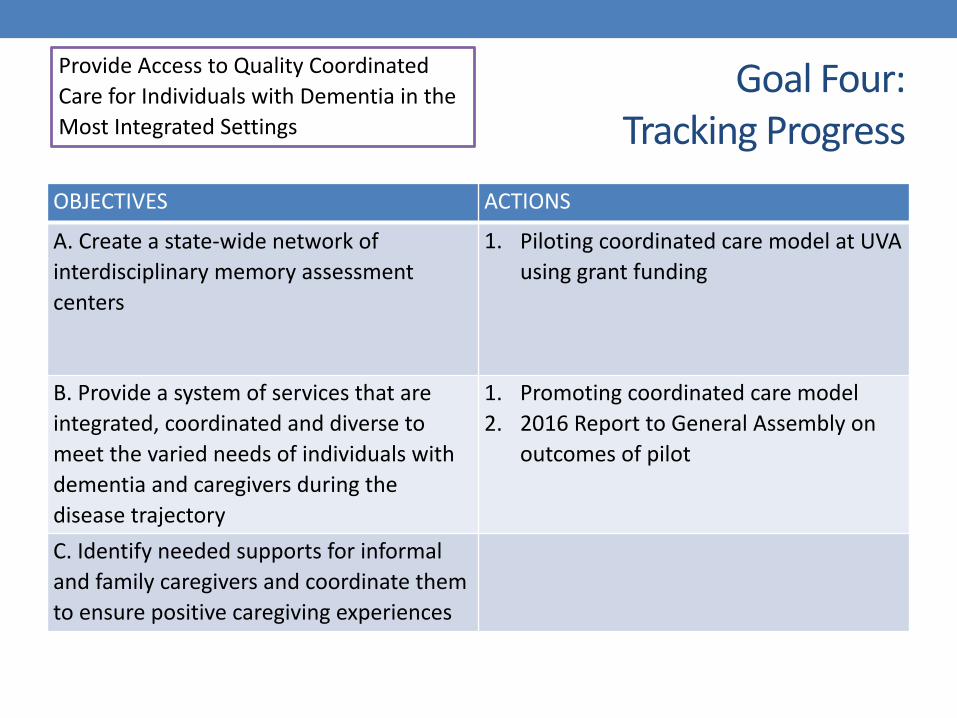
Goal Four:Tracking Progress
OBJECTIVES ACTIONS
A. Create a state-wide network of interdisciplinary memory assessment centers
1. Piloting coordinated care model at UVA using grant funding
B. Provide a system of services that are integrated, coordinated and diverse to meet the varied needs of individuals with dementia and caregivers during the disease trajectory
1. Promoting coordinated care model 2. 2016 Report to General Assembly on
outcomes of pilot
C. Identify needed supports for informal and family caregivers and coordinate them to ensure positive caregiving experiences
Provide Access to Quality Coordinated Care for Individuals with Dementia in the Most Integrated Settings

Goal Four:Next Steps
OBJECTIVES ACTIONS
A. Create a state-wide network of interdisciplinary memory assessment centers
1. Obtain funding to replicate memory assessment centers
B. Provide a system of services that are integrated, coordinated and diverse to meet the varied needs of individuals with dementia and caregivers during the disease trajectory
1. Continue monitoring best practices and identify opportunities to enhance current efforts
C. Identify needed supports for informal and family caregivers and coordinate them to ensure positive caregiving experiences
1. Pursuing grant funding to expand the FAMILIES program
Provide Access to Quality Coordinated Care for Individuals with Dementia in the Most Integrated Settings

Goal Five:Tracking Progress
OBJECTIVES ACTIONS
A. Increase funding for the ARDRAF
1. 2013: GA provides ARDRAF & Palliative Care Program an increase of $175,000, with $125,000 going to ARDRAF
B. Provide support to researchers across the Commonwealth through data sources and networking opportunities
1. 2011-2016: AlzPossible platform posts information on ARDRAF applications and deadlines
C. Promote research participation in Virginia
1. 2015: Amended state code to clarify language around informed consent for persons with dementia in research
2. 2012: Commission promotes Alzheimer’s Association Trial Match Program on AlzPossible
Expand Resources for Dementia Specific Translational Research and Evidence-Based Practices
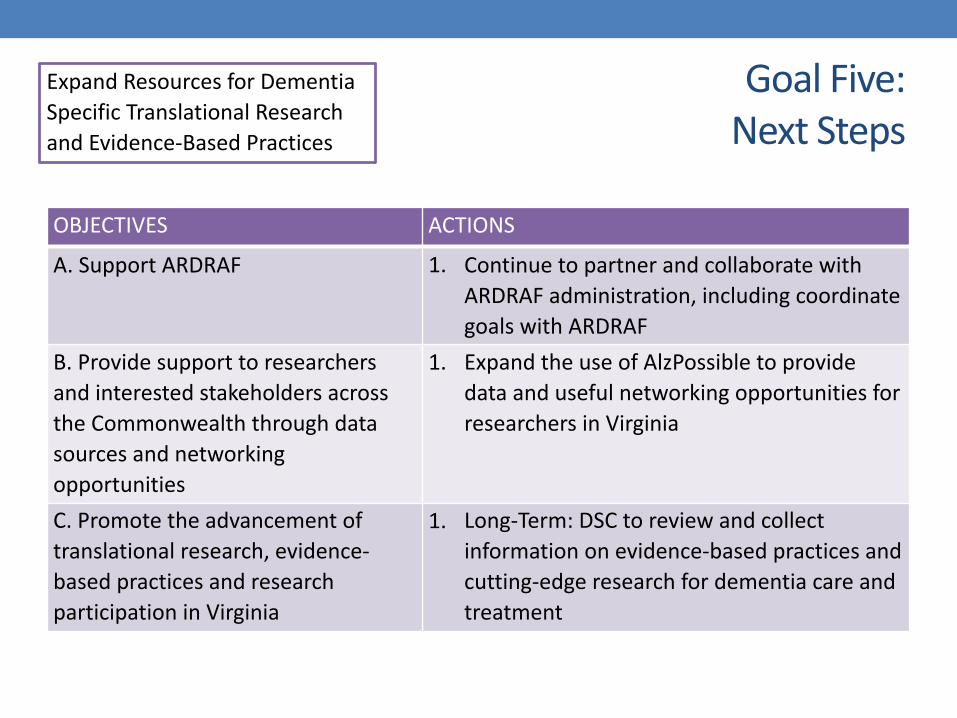
Goal Five:Next Steps
OBJECTIVES ACTIONS
A. Support ARDRAF 1. Continue to partner and collaborate with ARDRAF administration, including coordinate goals with ARDRAF
B. Provide support to researchers and interested stakeholders across the Commonwealth through data sources and networking opportunities
1. Expand the use of AlzPossible to provide data and useful networking opportunities for researchers in Virginia
C. Promote the advancement of translational research, evidence-based practices and research participation in Virginia
1. Long-Term: DSC to review and collect information on evidence-based practices and cutting-edge research for dementia care and treatment
Expand Resources for Dementia Specific Translational Research and Evidence-Based Practices

RESOURCESDementia State Plan
http://alzpossible.org/dementia-state-plan/
Webinars http://alzpossible.org/webinars-2/
Links http://alzpossible.org/tools/links/
Research Support http://alzpossible.org/tools/links/
VA Research Funding http://alzpossible.org/ardraf-reports/
Data & Data Sets http://alzpossible.org/tools/data/
Memory Assessment Centers http://alzpossible.org/tools/memory-centers/
Elder Abuse http://alzpossible.org/tools/elder-abuse/
Best Practices Report http://alzpossible.org/tools/best-practices-report/

Short Question and Answer Session

VIRGINIA’S INNOVATIONS IN CAREGIVER SUPPORT AND
DEMENTIA CARE
Dr. Christine Jensen
Director, Health Services Research
Riverside Center for Excellence in Aging and Lifelong Health
IMPLEMENTING THE FAMILIES PROGRAM TO SUPPORT CAREGIVERS
Partners:
Funded by:

Dementia in Virginia• Number of persons aged 65+ with Alzheimer’s disease
• Percentage of adults 45+ experiencing memory loss or confusion
• 11% or 1 in 9 9% are receiving help from family and friends
• 452,000 caregivers provide unpaid care for individuals with dementia
Alzheimer’s Association, 2015 and BRFSS, 2013
2015 2025 Increase130,000 190,000 46%
Background
• Adapted from the New York University Caregiver Intervention (NYUCI) model
• Implemented in Virginia in 2014 • Funding through ACL • Technical assistance through NYU
School of Medicine
FAMILIES = Family Access to Memory Impairment and Loss Information, Engagement and Supports
Purpose and Overview
• Caregiver intervention program via specially certified counselors
• Counseling support over 7 sessions
• Ease caregiver stress by involving family and friends in 4 of the sessions

Recruitment Partners
• Alzheimer’s Association (Central and Western VA, Southeastern VA, and Greater Richmond Chapters)
• Peninsula Agency on Aging (Newport News, VA)
• Jefferson Area Board on Aging (Charlottesville, VA)
Goals
• 120 caregivers to complete the program
• To demonstrate the impact in Virginia
• To relieve caregiver stress through counseling sessions and family/friend involvement
• To prolong independence and time until admittance to nursing home
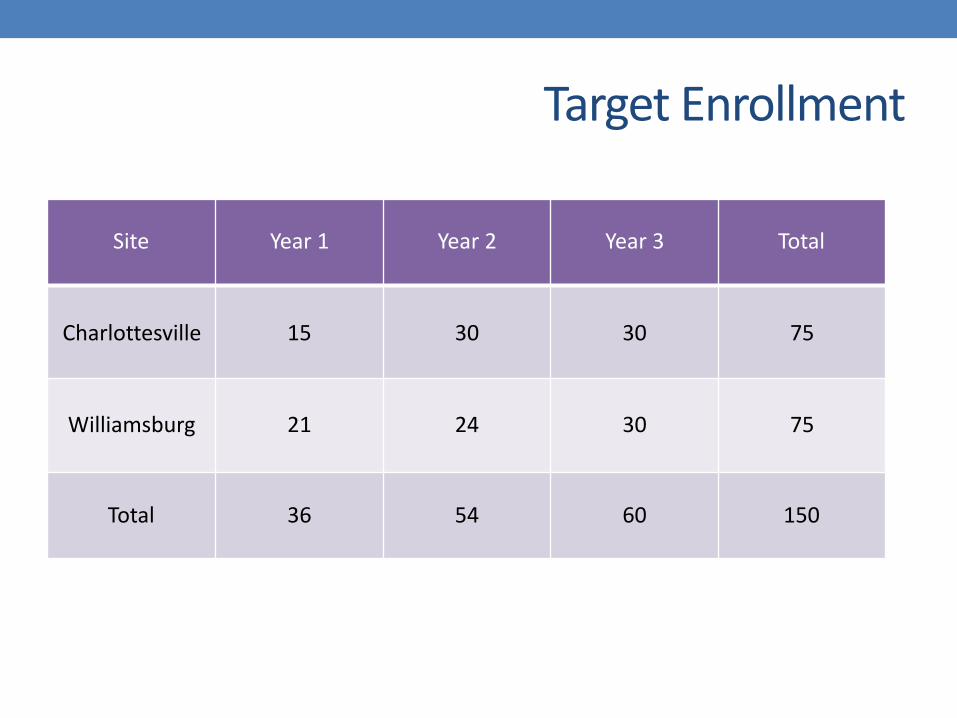
Target Enrollment
Site Year 1 Year 2 Year 3 Total
Charlottesville 15 30 30 75
Williamsburg 21 24 30 75
Total 36 54 60 150

Timeline
September 2014 August 2017


Outreach
• Governor’s Press Release
• Support groups
• Health Fairs
• Radio Interviews
• PACE Newsletter
• Promotion among religious groups
• Adult Protective Services
• Riverside Health Systems Intranet
• Riverside Senior Care Navigators
• Alzheimer’s Association Walks
• Health Department Distribution List
• Health Journal
• Local Senior Living Providers

Challenges and Benefits
Challenges
• Maintaining steady recruitment
• Caregiver has difficulty identifying their support network
• Family’s willingness to engage
• Travel to site • Sandwich generation
caregivers
Benefits
• Participants established a strong rapport with counselor
• Participants encouraged other caregivers to enroll
• Counselors expanded their knowledge and strategies in dementia care
• Grant-funded respite care

“… [it gave me] the opportunity to discuss ‘feelings’ about my situation that I would not normally do.”
-Participant 1034
“Made me understand that I was not in this thing alone.”
-Participant 1019
Participant Feedback
“This program has been a blessing. Nothing I would change.” -Participant 1041
“Good advice and friendship. A safe, supportive space.” -Participant 1058
Lessons Learned
• Translating NYUCI to Virginia
• Role of Riverside Senior Care Navigators
• Bi-monthly supervisory calls with counselors
• Orientation and timely updates for counselors
• Significance of Master Tracking Sheet
• Supporting data collection through counselors

Combined Demographics
UVA & Williamsburg
Enrolled / Completed • Baseline: 61 people • 6th Session: 34 people • 6 Month: 16
Age: • Mean: 64.7 +SD 10.1 • Range: 44-89 years old
Gender 12 males (19.7%) 46 females (75.4%)

Dependent in Basic ADLs
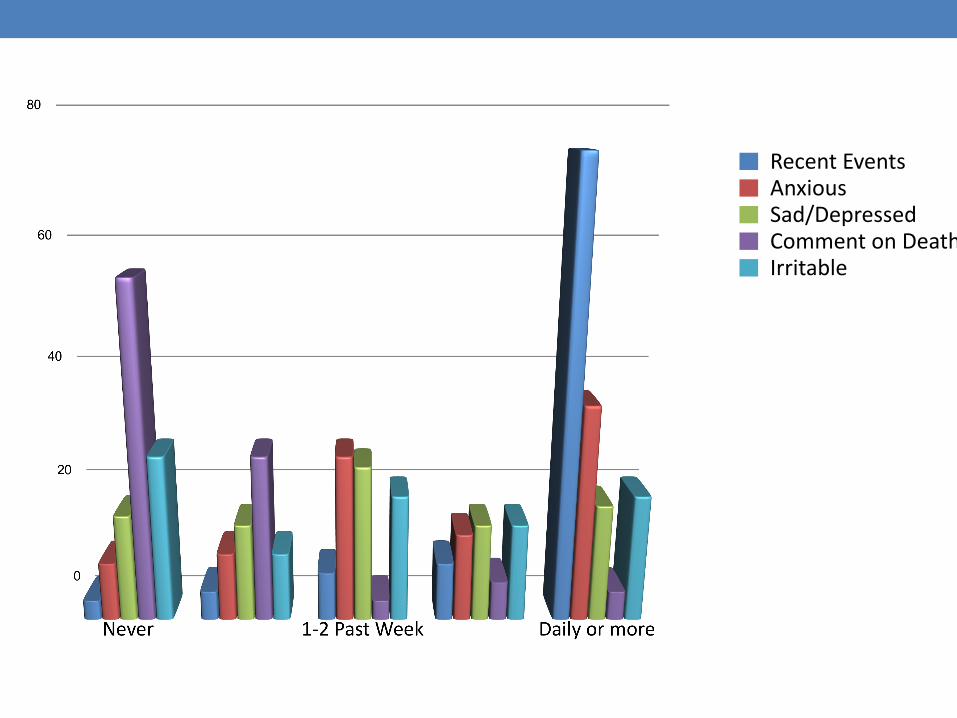
Recent EventsAnxiousSad/DepressedComment on DeathIrritable
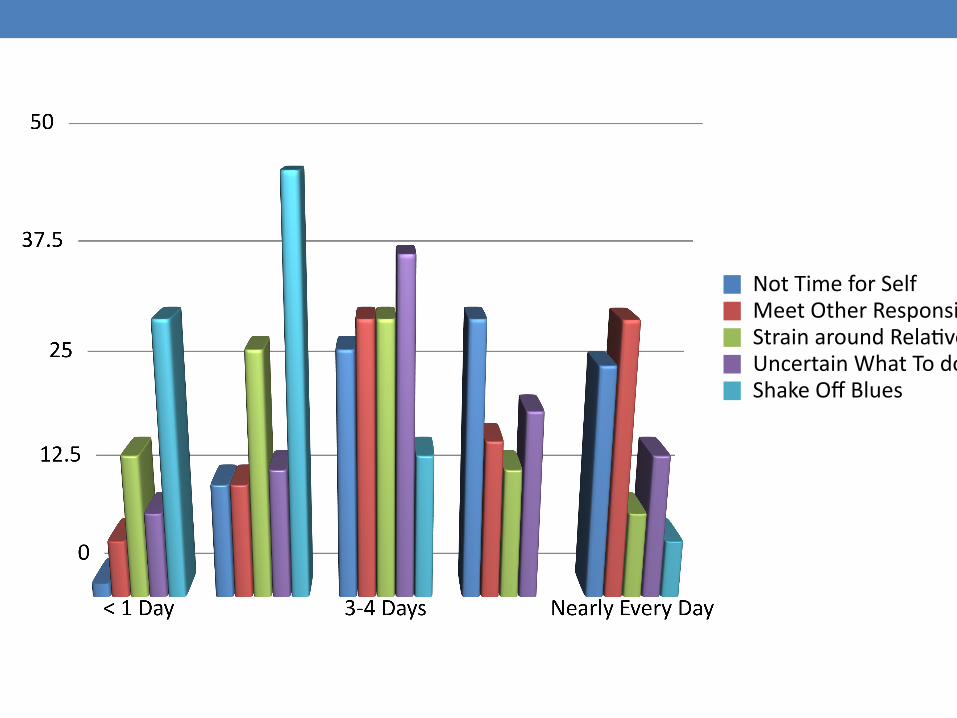
Not Time for SelfMeet Other ResponsibilitesStrain around RelatveUncertain What To doShake Off Blues
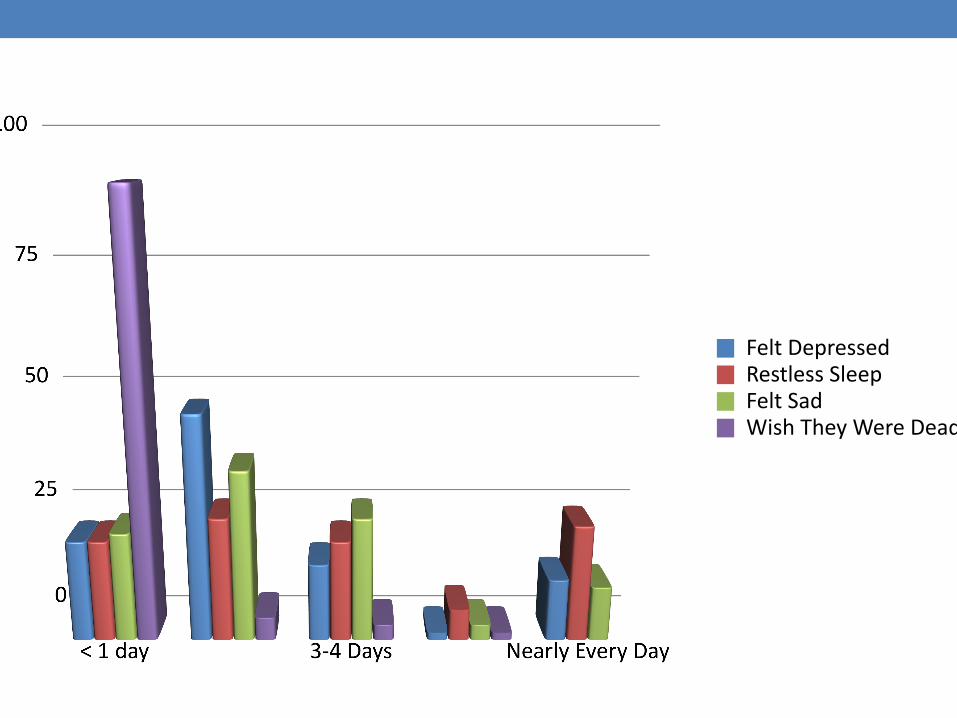
Felt DepressedRestless SleepFelt SadWish They Were Dead
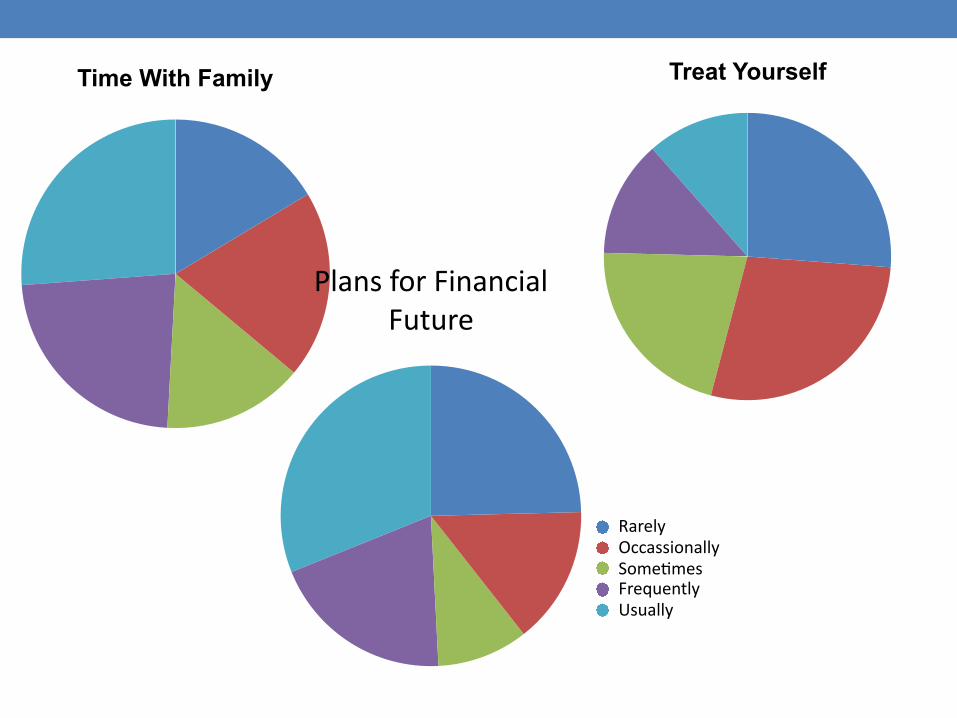
Time With Family Treat Yourself
Plans for Financial Future
RarelyOccassionallySometmesFrequentlyUsually
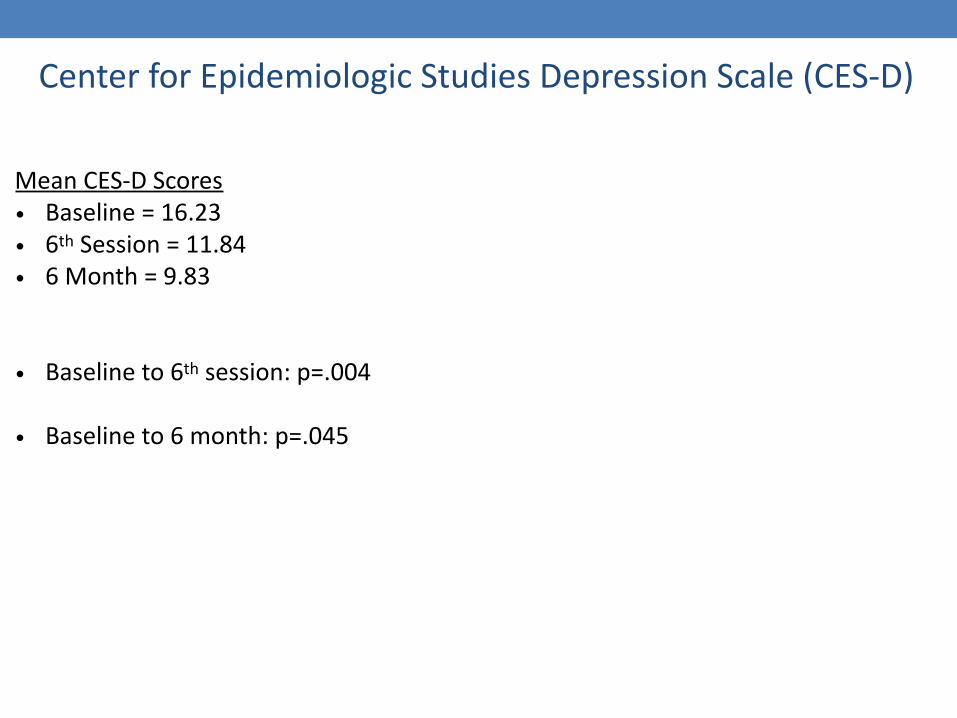
Center for Epidemiologic Studies Depression Scale (CES-D)
Mean CES-D Scores • Baseline = 16.23 • 6th Session = 11.84 • 6 Month = 9.83
• Baseline to 6th session: p=.004
• Baseline to 6 month: p=.045

Zarit Burden Interview (Revised)
Mean Zarit Scores • Baseline = 9.15 • 6th Session = 7.77 • 6 Month = 6.6
• Baseline to 6 session: p =.037
• Baseline to 6 month: p =.173
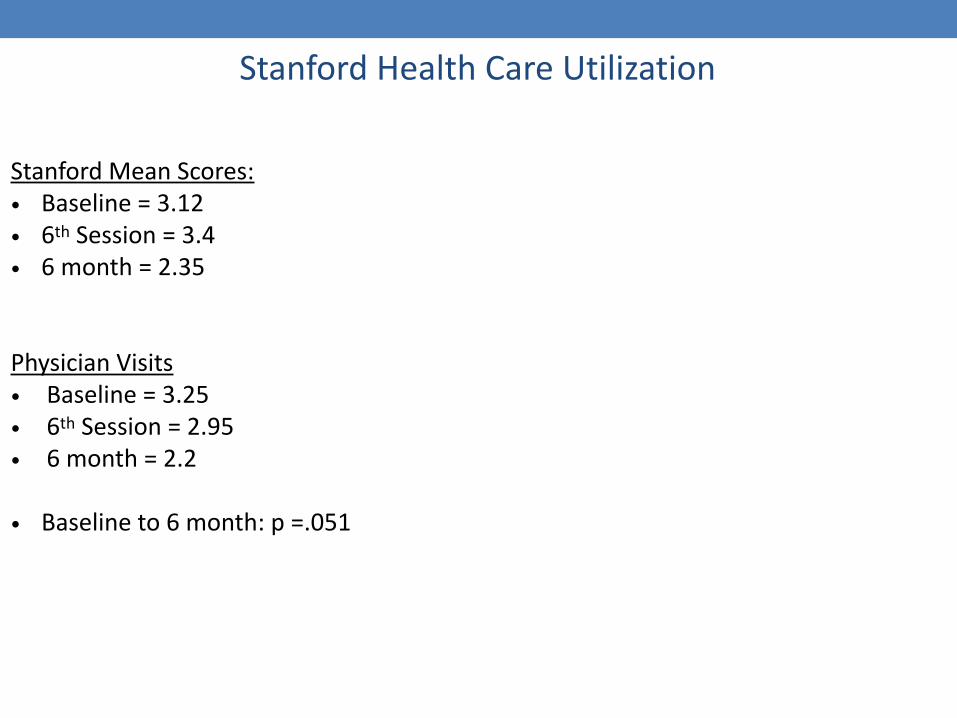
Stanford Health Care Utilization
Stanford Mean Scores: • Baseline = 3.12 • 6th Session = 3.4 • 6 month = 2.35
Physician Visits • Baseline = 3.25 • 6th Session = 2.95 • 6 month = 2.2
• Baseline to 6 month: p =.051
Caregiver Well-Being Scale (CWBS)
“Feeling good about yourself” • Baseline to 6 month: p =.051
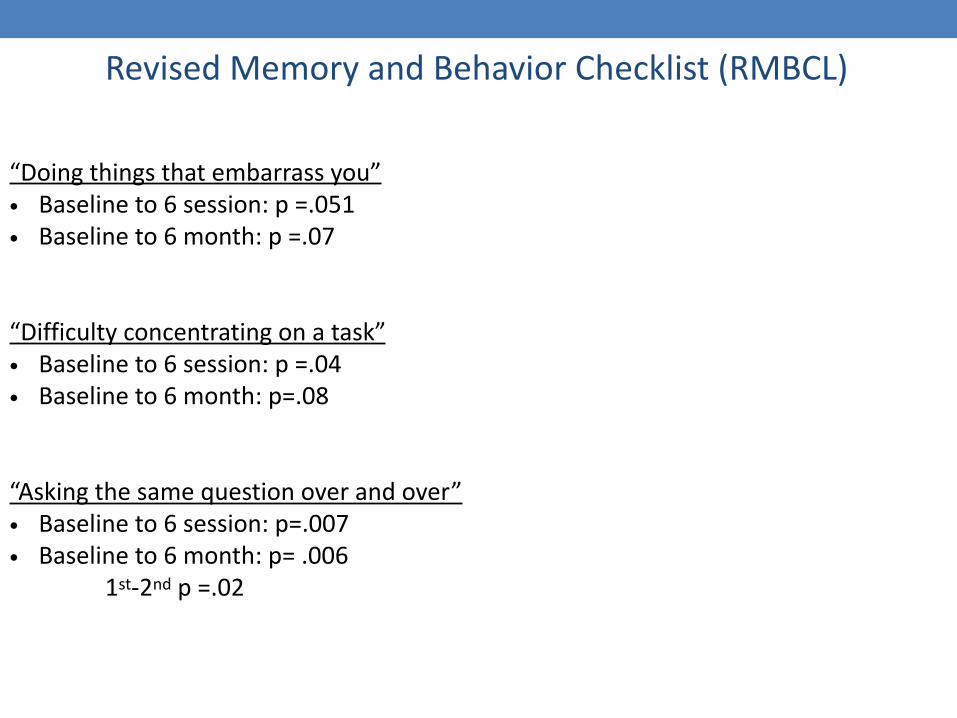
Revised Memory and Behavior Checklist (RMBCL)
“Doing things that embarrass you” • Baseline to 6 session: p =.051 • Baseline to 6 month: p =.07
“Difficulty concentrating on a task” • Baseline to 6 session: p =.04 • Baseline to 6 month: p=.08
“Asking the same question over and over” • Baseline to 6 session: p=.007 • Baseline to 6 month: p= .006 1st-2nd p =.02

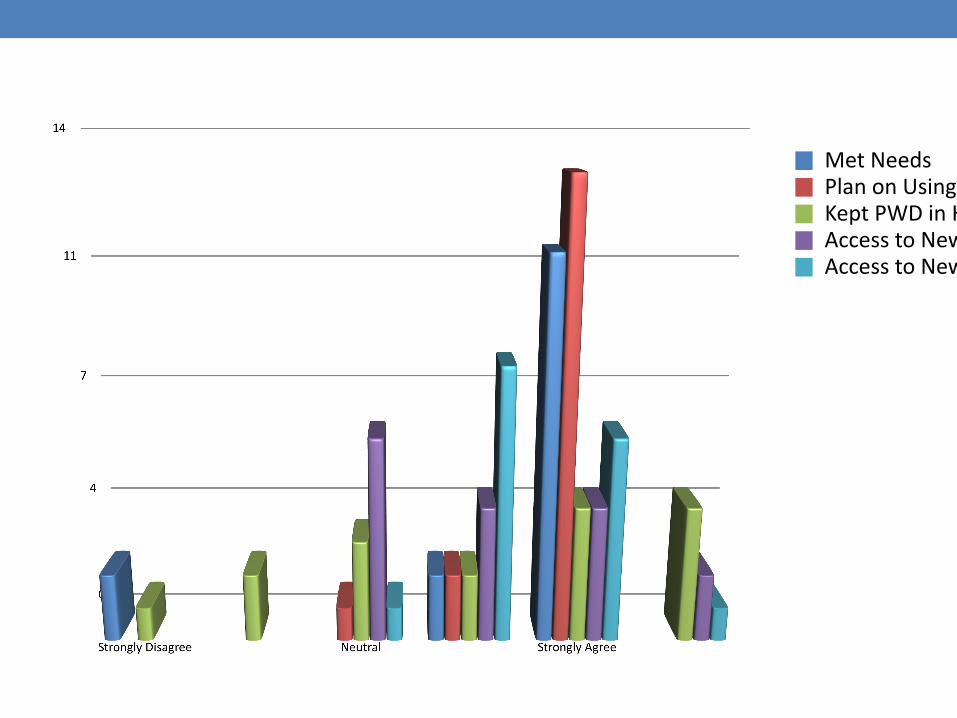
Met NeedsPlan on Using InformatonKept PWD in HomeAccess to New Services for PWDAccess to New Services for Self


Learned Coping SkillsMood ImprovedHealth ImprovedHave More SupportPositve Impact on MeRecommend Program

Short Question and Answer Session
IMPLEMENTING THE CARE COORDINATION PROGRAM AND EFFECTIVE STRATEGIES PROGRAMDr. Carol Manning
Director, Memory Disorders Clinic
University of Virginia

Dementia
• There are ~900 million people aged 60 years and over living worldwide
• Today: Between 35.6 and 47.5 million people with dementia
• 2030: Between 63 and 74.7 million
• 2050: Between 114 and 131.5 million

Dementia
• U.S. population-based studies: 28% of community-dwelling older adults have MCI • 19% over 65 • 29% over 85 years
• Annual conversion rate from MCI to AD is 3%–13% • 1% for the rest of the population
• 11% of older adults are living with Alzheimer’s disease and other types of dementia
Dementia
• Incidence of dementia increases exponentially with increasing age, doubling every year
• 3.9 per 1000 person-years at age 60-64
• A new case of AD is diagnosed about every minute • 2015 : over 9.9 million new cases of dementia each year worldwide
• Number of persons over 65 with AD in US will nearly triple from 2014 to 2050 • 5.1 million to a projected 13.8 million

Costs of Dementia
• Compared with other long-term care users, PWDs have higher costs of care • Personal care • Supervision • Assistance with ADLs
• Costs are expected to increase by 85% by 2030, making dementia the most expensive disease in our society
Caregiving
• 65.7 million informal caregivers in the US
• Over 90% of older adults with chronic disabilities receive some care support • 2/3 receive only informal care
• 43.5 million family members provide informal care for older adults • 15.5 million are caring for a PWD

Caregiving
• Approximately 2/3 of caregivers are women
• 34% are 65 or older
• 41% of caregivers have a household income of $50,000 or less
• Over ½ of primary caregivers take care of parents
• ~250,000 children and young adults between ages 8 and 18 provide help for a PWD
Caregiving
• 17.9 billion hours of unpaid care • Valued at $217.7 billion • ~46 percent of the net value of Walmart sales in 2013 • Nearly 8 times the total revenue of McDonald's in 2013

Caregiving
• Nearly 60 percent of dementia caregivers rate the emotional stress of caregiving as high or very high
• 40 percent suffer from depression
• $9.7 billion in additional health care costs of their own in 2014
Virginia Dementia Specialized Supportive Services Project
• A collaborative study designed to address Goals 4 & 5 of the Virginia State Dementia Plan through • Care Coordination Program • Effective Strategies Program
Goal 4: Provide access to quality coordinated care for individuals with dementia in the most integrated setting Goal 5: Expand resources for dementia specific translational research and evidence-based practices
Overall Goal - Enhance Virginia’s dementia-capability by providing efficient, effective coordination of services and promoting education and well-being to individuals and care partners

Partners:
Funded by:
UVA’s Memory and Aging Care Clinic
• A model multidisciplinary clinic providing • diagnosis • treatment • care coordination
Care team consisting of • neurologists • neuropsychologists • nurse practitioner • social workers • research coordinators • care coordinators

Care Coordination Program (CCP) • A model program of coordinated care for individuals and their
primary care partners
• Goal – To provide coordination of services, education about dementia, and emotional support to patients with Mild Cognitive Impairment (MCI) or dementia, and care partners
• Participants access services • Mainly through University of Virginia’s Memory and Aging Care Clinic
(MACC)
• Can also be referred from partner agency JABA and outside sources
• Through referral from Effective Strategies Program
Open to all Virginians with a recent diagnosis of Mild Cognitive Impairment (MCI) or dementia
Care Coordination Program (CCP) • Innovative services aimed at improving the quality of dementia
care in Virginia • Care Coordinators help with
• Navigating the health system
• Education and information about the individual’s diagnosis
• Helping individuals and their care partners access services in the community
• Discussions about future planning, such as ensuring legal and financial
safeguards
Care Coordination Program (CCP) • Innovative services aimed at improving dementia care in
Virginia • Unique collaboration between UVA Health System and Jefferson Area
Board for Aging (JABA)
• Care Coordinators Tracee Jones and George Worthington
• Promotes knowledge of community services within MACC and UVA Health
System
• Enhances cooperation and cross-referrals (e.g., respite care
available at JABA’s Adult Day Centers)
• Allows for seamless connection between individual and
multiple agencies

Effective Strategies Program (ESP)• A model program of education for individuals and their primary
care partner
• Goals – To educate people with dementia/MCI and care partners about dementia, provide strategies for anticipating and coping with changes, provide emotional support, and aid in the development of a support system
• Participants access services • Through referral from participating sites
• Through referral from Care Coordination Program
Effective Strategies Program (ESP)• Group educational program for individual and care partner • 20 sessions over 10 weeks • 1 hour interactive presentations followed by ½ hour of
socializing • Topics include: - education about dementia and memory - speech, language and memory strategies - exercises - developing and practicing an exercise program - home safety - planning and participating in outside activities - emotional adjustment
Measurable outcomes for CCP & ESPMeasured using validated tools
• at enrollment and after 12 months in CCP • at start and finish of ESP
And satisfaction surveys created specifically for both programs
Outcome 1: Individuals and care partners receiving care coordination will feel more supported in their abilities to meet the challenges of dementia as evidenced by
(1) Fewer symptoms of depression; (2) More steps taken to prepare for the dementia; and
(3) Satisfaction with the Care Coordination Program
Outcome 2: Participation in the Care Coordination Program will result in decreased use of emergency or unplanned health care
Measurable outcomes for CCP & ESP
Outcome 3: Individuals who participate in the ESP will report
(1) Increased understanding of strategies to cope with memory change; and
(2) Satisfaction with the ten week program
Outcome 4: The implementation of the Care Coordination Program and the ESP will provide a new model of support that can be readily replicated through creation of manuals:
• Manuals for both programs will facilitate implementation throughout Virginia
• Manuals will be created as collaboration between UVA and JABA demonstrating commitment between the groups
Future Replication Manual for state- and nation-wide replication by end of three-year grant
• Documented comprehensive training program for Care Coordinators • Using existing on-line materials and in-person training supporting Dementia Capability
• AlzPossible (Virginia Alzheimer’s Commission AlzPossible Initiative) webinars and materials
• Alzheimer’s Association Education Center webinars and materials
• State certification as Options Counselors, training in Person-Centered Care
• Recognizing and Reporting Abuse, Neglect and Exploitation of Adults (VDSS)
• VICAP Insurance Counselor education
• Community networking and outreach to enhance knowledge and awareness of available resources
• Fully-developed procedures and best practice for reproducing • Care Coordination Program • Effective Strategies Program

Short Question and Answer Session

Contact us…
Carol Manning
Courtney Tierney [email protected]
Patricia Slattum
Christine Jensen
Please complete the half page survey.