demystifying screening and brief advice in clinical settings for alcohol and tobacco north east...
TRANSCRIPT

Demystifying screening and brief advice in clinical settings for alcohol and tobacco
North East Parity of Esteem conference Sunderland, 15th October 2014
Martyn Willmore – Fresh
Dr Dorothy Newbury-Birch, Institute of Health & Society, Newcastle University
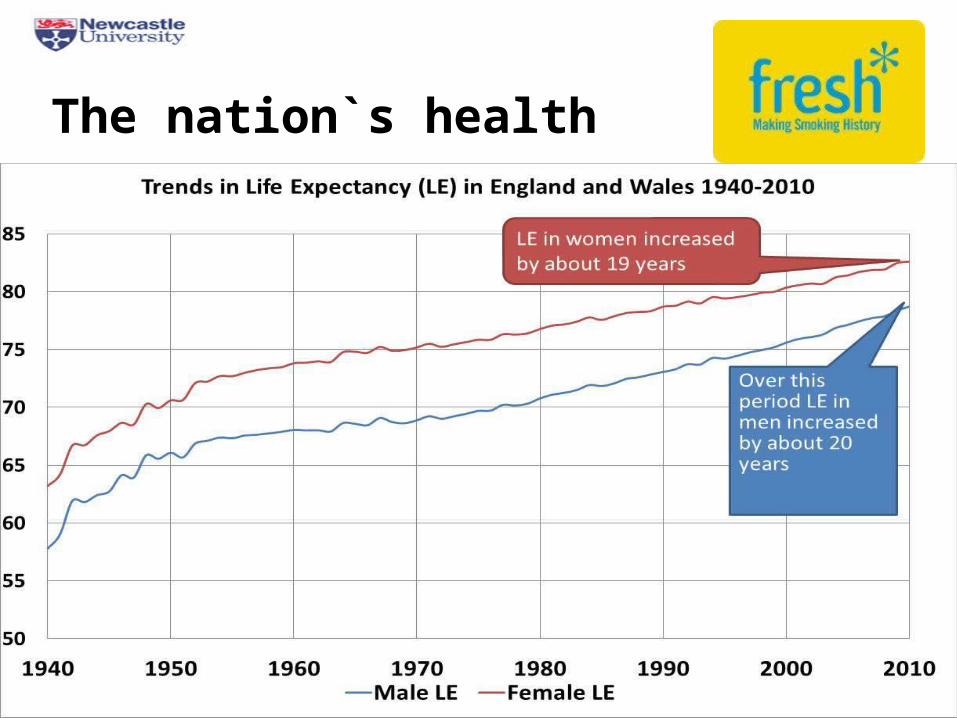
The nation`s health

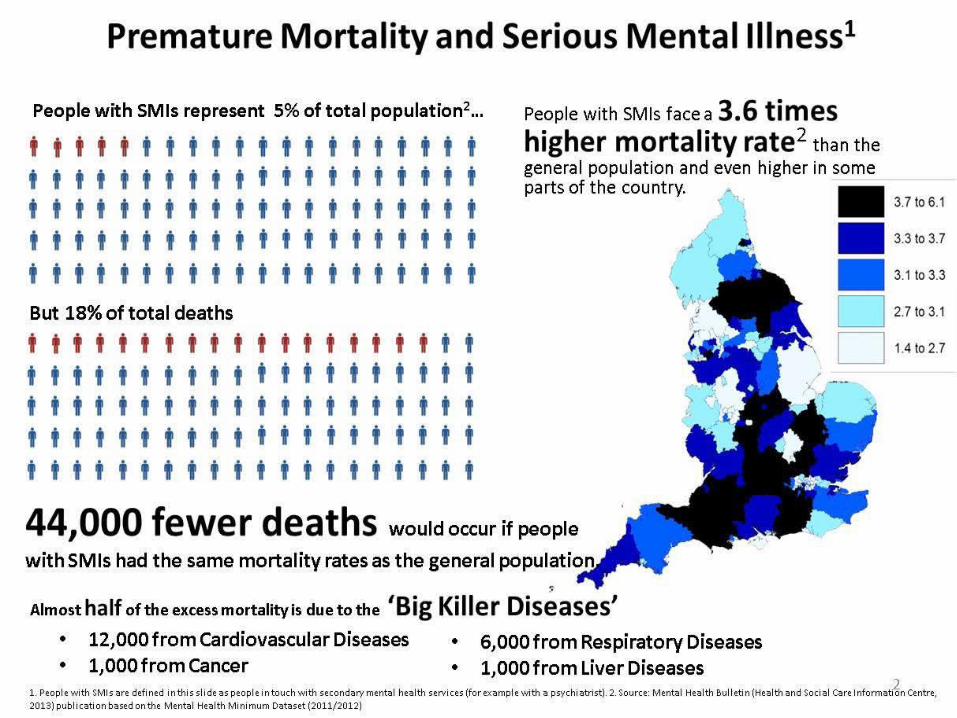
Life expectancy of people living with mental illness


Summary
o Majority of people living with a mental health condition will die from one of the five big killers
o We know that people from the most deprived communities are more likely to have mental illness and likely to die younger
o “Better health, fairer health”?? We have made least progress in outcomes for those with mental illness

Smoking

Supporting smokers to stop
o For people living with mental illness who smoke, stopping smoking will have the greatest positive impact on their physical health
o Very Brief Advice on smoking is a life-saving intervention, and takes 30 seconds….
o Mental health staff (both inpatient and community) are ideally placed to identify those that smoke, and offer advice on stopping
What are the perceptions?
o Those with mental health issues don’t want to stop /cannot stop
o Smoking is one of very few pleasures in life
o Tobacco/nicotine helps to relieve stress
o Cessation will negatively impact on mental health

Very Brief Advice on Smoking
VBA for smoking follows 3 simple steps:
ASK(and record smoking status)
Is the patient a smoker, ex-smoker, or non-smoker
ADVISE(on the best way of quitting)
Best way of stopping is with a combination of support and product
ACT(on the patient`s response)
Give information, refer to service, prescribe
o Vital that MH staff use every contact as a health improvement opportunity
o Staff already have the skills to engage patients in conversations in behaviour change. Easily applied to smoking
o Raising the issue re-enforces that stopping smoking is integral to overall health of patient
ASK and record
Do you smoke?
Have you recently stopped
smoking?

o Once smoking status confirmed, follow up with advice/offer of support to quit
o Most effective way of quitting is a combination of stop smoking product, and behavioural support
o You are up to four times more likely to quit with SSS support than trying to quit unaided
ADVICE
Did you know that stopping smoking is the
best thing you can do for your health?
Support and medication really improves your chances of quitting
Would you like for me to arrange for a stop smoker advisor to chat with you?

o Act upon the patient`s response:o If interested in quitting, make a referral to local SSSo Encourage/Build up their self-confidenceo If inpatient, but not looking to quit, ensure access to
NRT or medication to help with nicotine managemento Be proactive about possible impact on dosage of
associated medicationso Record actions taken
o Majority of smokers say they want to stop, but lack confidence or impetus to access proper support
ACT
Key role of mental health staff
o Trained SSS advisors will offer clients a 12-week programme of support and medication
o But MH staff can support patients too by encouraging correct use of medications, and helping to re-enforce positive messages
o Motivation to quit can be easily undermined by staff:o Offering cigarettes/purchasing them on behalfo Smoking in front of themo Conveying negative messages about chances to quit

Managing nicotine withdrawal
o Nicotine has a very short half-life, and so smokers will begin to suffer withdrawal within 1-2 hours
o Withdrawal symptoms could include irritability and low mood, and are easily misinterpreted as signs of worsening mental health. Important to understand alternative options
o There are currently three main types of licensed product to help with cravings from tobacco withdrawal:• Nicotine Replacement Therapy• Varenicline (Champix)• Buproprion (Zyban)
Effect of cessation on metabolism
o Tobacco (specifically tar) speeds up the metabolism of some antipsychotic medications, anti-depressants and benzodiazepines
o Therefore some smokers need higher doses of these drugs than non-smokers
o Blood levels of medication can be impacted by many things, but stopping smoking likely to increase it within 7 days
o Doses of medicines may need to be reduced by 25%-50% once someone stops smoking
Summary
o Tobacco dependence is a chronic relapsing condition – may take a number of attempts to quit successfully
o MH staff have a vital role in supporting patients
o Normalising VBA is pivotal in prompting quit attempts
o Online VBA training available. Staff can also acquire skills from local SSS to become advisors if they wish
o Smoking remains our biggest preventable cause of premature mortality

VBA Smoking Resources
Online NCSCT Training module
http://elearning.ncsct.co.uk/vba-launch
Short film on VBA
http://elearning.ncsct.co.uk/vba-stage_1

Alcohol

Is IBA effective?

The IBA evidence base• Over 30 years of research examining
impact of IBA in primary care and (more recently) other settings.
• 24 systematic reviews covering at least 56 high quality studies in primary care alone (O’Donnell et al 2014).
• Consistent message IBA is effective at reducing the quantity, frequency and intensity of drinking when delivered in primary healthcare.
• Evidence more equivocal in other settings (A&E, workplace, criminal justice).
Impact on alcohol consumption
For every eight people who receive simple alcohol advice, one will reduce their drinking to within lower-risk levels (Moyer et al., 2002).
Kaner et al (2007) showed that IBA reduced the quantity of alcohol drunk by an average 38 g per week.
Varies by age Jonas et al (2012) suggested effects may be lesser in older adults aged 65 and over (23g) and for young adults / college students aged 18-30 (23g).

Wider health impacts
Other positive outcomes include:– Reduction in alcohol-related problems;– Reduced health-care utilization;– Improved mortality outcomes.
A reduction from 50 units/week to 42 units/week will reduce the relative risk of alcohol-related conditions by some 14%, the attributable fractions by some 12%, and the absolute risk of lifetime alcohol-related death by some 20% (Anderson 2008).

Cost-effectiveness of IBA
• Estimated quality-adjusted life-year (QALY) gain associated with IBA ranges from 4-19 per 1000 (Anderson 2009)
• IBA based on new patient registrations and delivered by a practice nurse provides modest cost savings to the health care system of £120m over 30 years and health gains over the same period amount to 32,000 QALYs, at £6900 per QALY gained (Purshouse et al 2009).
• Doctor-delivered IBA would be more expensive but result in incremental health gains equivalent to 92,000 QALYs, at £1175 per QALY gained (Purshouse et al 2009).

1. To identify the most efficient and acceptable screening strategy and tool to detect hazardous and harmful drinking
2. To evaluate the effectiveness and cost effectiveness of different intensities of BI
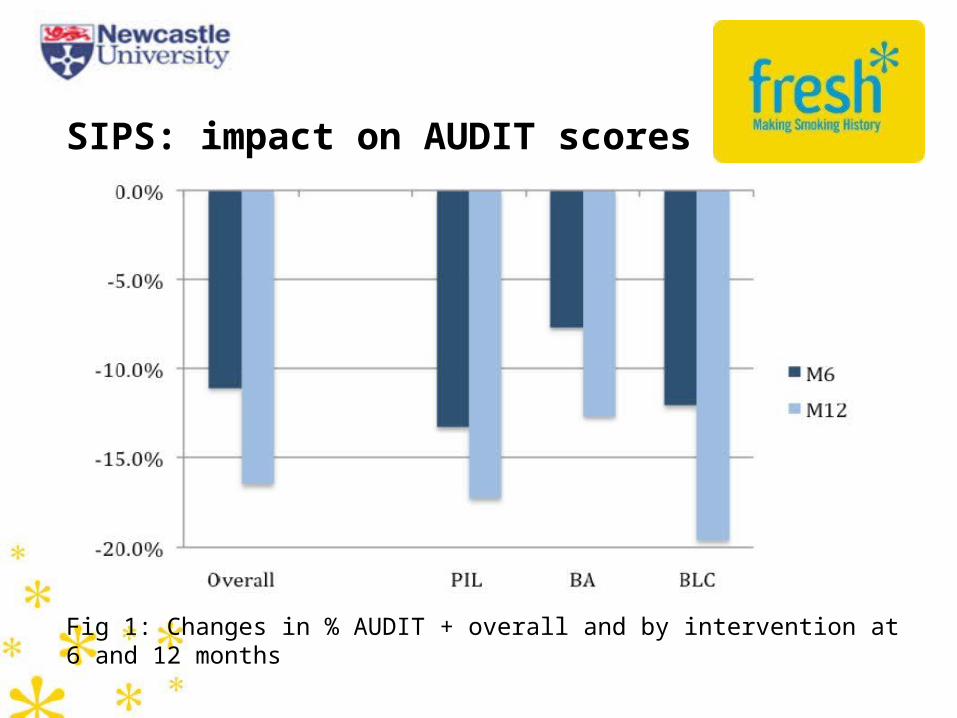
Fig 1: Changes in % AUDIT + overall and by intervention at 6 and 12 months
SIPS: impact on AUDIT scores

SIPS: Key findings
High overall recruitment and follow-up rates in PHC
High BI delivery immediately after screening
BI delivery drops if subsequent visit is needed
Risk drinking fell between baseline & follow-up
No significant differences between the 3 conditions
Gender and AUDIT score at outset predict outcome
(Kaner et al 2013)

IBA in practice……
http://www.alcohollearningcentre.org.uk/Topics/Browse/BriefAdvice/SIPS/BriefAdviceTrainingandTools/?
parent=4449&child=5186
http://www.alcohollearningcentre.org.uk/Topics/Latest/Resource/?cid=5184