dengue by dr umar draz
DESCRIPTION
DENGUETRANSCRIPT

By

Biodata
• My patient Mohammad Gulzar, 20 Years,oldresident of Jhelum, and manual worker by profession, unmarried, presented in emergency department on 9th September, 2014.

Presenting complaints
• High grade Fever for 8 days
• Bodyaches for 8 days
• Vomiting for 6 days
• Patient was in his usual state of health when he started fever.
• It was sudden in onset initially high grade, associated with rigors and chills and slightly relieved by medications from the local doctor.
• It was associated with body aches of severe degree and patient felt very weak and he was not able to continue his daily job activities.
• Fever has daily variation of less than 10C and whenever recorded with thermometer it was around 102 to 103 OF.
• Was no associated rash on the body
• He went to local doctor who gave him some open medications but those medications gave no relief to the patient.
• During his illness he has marked nausea and he was not able to take food in fact his appetite was markedly suppressed and his nausea worsens whenever he looked at or ate food.

• 6 days back he started having vomiting as well. He had 2 episodes of vomiting on first day, which were non foul smelling containing food particles which he recently took and it was non-projectile.
• On 6th day both vomiting episodes were clear and not containing the slightest of blood.
• On 7th day he again had 3 episodes of vomiting non projectile and non foul smelling and occurred after in take of food.
• But this time around all 3 vomitus contained blood (coffee ground).
• After that patient’s attendants took him to the hospital and he was admitted in emergency ward of Mayo Hospital.

Systemic review
• General: decrease sleep, decrease appetite, decrease energy.
• Git : no history of diarrhea, no history of black tarry stools, no history of yellow discoloration of eyes or sclera.
• Respiratory: no history of shortness of breath, no history of seasonal variation, no history of nose or ear discharge, no history of cough with sputum.

• CVS: no history of shortness of breath on lying flat, no history of chest pain on exertion, no history of palpitation.
• CNS: no history of focal weakness, no history of fits, no history of diplopia, no history of headache.

Past history
• No history of previous hospital admission.
• No history of hypertension, diabetes, TB, CVA, MI or meningitis.
Socio-economic history
• Patient is laborer by profession and his earning is only 6000 per month.
• He belongs to a lower socio-economic class.
Drug history
• No history of any drug allergies.
• He was not using any medications for any reason previously.
• During this illness, he used medications from local doctor but those were open medications without any labels.

Differential diagnosis
• Dengue hemorrhagic fever• Enteric fever• Aplastic anemia• Lympho-proliferative disorder• Malaria• Yellow fever• Secondary syphillis• Ebola hemorrhagic fever• Congo fever

• At presentation he was afebrile and lethargic and ill looking.
• Patient was not maintaining bp. His bp was only 70 systolic.
• He was shifted to HDU west medical ward where he was given NS 50-80ml/hr.
• His platelet count was 7000 only
• He was transfused one pint of mega platelet concentrate.
On 11th September• After that he went into overload with fine
crepts up to middle zone of both lungs.
• His JVP was raised as well. Initially dextran 40 was not available but later on it was arranged from emergency and he was given bolus of dextran 40.
• After that his BP was built up to 125/80mm of hg.

• At that point his breathing was gasping and he was not maintaining oxygen saturation even with 3l/min oxygen inhalation.
• Inj lasix 40mg was given iv stat to relieve his overload and to took him out of pulmonary edema.
• Meanwhile ventilator was arranged and ETT passed and patient was put onto ventilator on SIMV with pressure support and PEEP was kept at 5 but later on increased to 7 which helped to achieve saturation of 98%.

On 12th September • Patient was given one more shot of inj lasix
40mg iv stat. and 1 pint of pcv of blood was transfused.
• Patient developed high grade fever and injtazocin 4.5g iv tds was started to cover pseudomonas of ICU setting.
• One more PCV was arranged as HB level was falling and we were suspecting occult bleed.
• Ventilator was kept on SIMV with pressure support mode.
• Tepid water sponging were continued and only fluid to be given was dextran 40.
• Patient had three instances of fall in BP which were managed by giving dextran 40 bolus.
On 13th September
• Antibiotic was continued but fever didn’t settle so blood culture and sensitivity and urine culture and sensitivity were planned and sent.
• On examination power was 5/5 in all 4 limbs with +2 reflexes at ankle, knee, bicep and tricep.

• Patient was started NG feed and atralax was stopped and later patient was shifted to CPAP mode of ventilator.
• He was able to maintain Oxygen saturation on CPAP and bp was also stable.

On 14th September
• Patient had episode of bradycardia and neubulization with ventolin and tab theograde350mg ½ po bd was started. Soon heart rate was normalized but fever continued.
• Tepid water sponging were continued and injflagyll was added.

• CK MB report was sent which was found to be raised 57.
• Call to cardiology was attended and they said its sinus arrhythmia and advised to repeat call on Monday for consultant opinion.
• Patient was still kept on CPAP mode of ventilator and he was maintaining oxygen saturation and bp.

On 15th September
• Patient was weaned off from ventilator and kept under observation for 2hrs he was maintaining oxygen saturation and he was then extubated as well.
• Echocardiography and repeat cardiac enzymes were planned.
• Patient is fully conscious and oriented and he was able to take his food as well without NG tube

A young male ill looking lying on bed with ETT passed and on
ventilator
General physical examination
PALLOR +VE• CYANOSIS -VE• CLUBBING -VE• JAUNDICE -VE• PALMAR ERYTHEMA -VE• PEDAL EDEMA +VE• LYMPH NODES -VE• THYROID -VE• JANEWAY LESIONS -VE• KOILONYCHIA -VE• LEUKONYCHIA -VE

RESPIRATORY SYSTEMINSPECTION
• Respiratory rate 34/min
• Abdomino-thoracic type
• Pattern of respiration is shallow rapid breathing
• No scar mark
• Chest seems to be moving equally on inspection
• Trachea is central

PALPATION• Chest movements are equal bilaterally• Chest expansion is 5cm• Vocal fremitus is normal and bilaterally equal.
PERCUSSION• Liver upper border is in fifth intercostal space• Percussion note is resonant all over and bilaterally equal
AUSCULTATION• NVB • Fine end inspiratory crepts at bases bilaterally and
extending upto middle zone.• No rhonchi, no coarse crepts, no pleural rub

GASTRO-INTESTINAL SYSTEM
INSPECTION
• Flat abdomen moving with respiration, no fullness in flanks, umbilicus central and inverted, no scar mark.
PALPATION
• On superficial palpation , slight tenderness in epigastric and right hypochondrial area. No palpable mass
• On deep palpation liver is not enlarged and span is 13 cm. spleen is 1 finger breath enlarged
• Kidneys are not palpable.

PERCUSSION
• Shifting dullness is negative.
• Fluid thrill is negative.
AUSCULTATION
Bowel sounds are audible.
CARDIO VASCULAR SYSTEMINSPECTION• NO VISIBLE PULSATIONS
• NO SCAR MARK
PALPATION• TRACHEA IS CENTRAL
• APEX BEAT IS IN 5TH INTERCOSTAL SPACE JUST MEDIAL TO MID-CLAVICULAR LINE OF NORMAL CHARACTER
• NO PALPABLE THRILL
• NO PARASTERNAL HEAVE.
AUSCULTATIONS1+S2 and no added sounds

CENTRAL NERVOUS SYSTEM
• GCS is 14/15
• Patient was on ventilator hence speech and higher mental functions can not be assessed.
• Bulk and tone both are normal in all 4 limbs.
• Power and reflexes in all 4 limbs are 5/5 and +2 respectively.
• Planters bilaterally down going

9/9/2014 10/9/2014
11/9/2014
12/9/2014
13/9/2014
14/9/2014
15+16/9/2014
HBHCT
11.632
1129
8.723
8.5,9.322 ,27
8.5,8.823.1 ,25
8.8,9.726.3,29.8
10.8,,10.331,,,,32.4
TLC 1,000 1.1,000 1.6 2.8,3.1 2.7,2.1 1.9,3.1 3.2,,,,,2.8
NEUTROPHILS
47% 65% 37% 68% 73% 52 75,,,,65
LYMPHOS 44% 30% 51% 30% 26% 46 22,,,,,34
PLATELETS
7000 6000 4000 29000,32000
31000,,,71000
21000,,19000
29000,,34000
ABGS PHHCO3O2 SATPCO2
7.26146132
7.46239932
7.50249931
7.51249930
7.5,7.5126,,2898,,9533,,36
LFTSRFTS
ALT-AST-ALBUMUREA-70
751872.741 70
25173.486
872502.795
601582.791
57,,,863.170
CT scan

X-RAY CHEST PA VIEW

Why patient went into fluid overload?

• Why patient was put on ventilator?

• Why higher PEEP was used?

• Why CK MB was raised?

• Why patient developed bradycardia?
• Why dextran 40 and inj lasix were used?



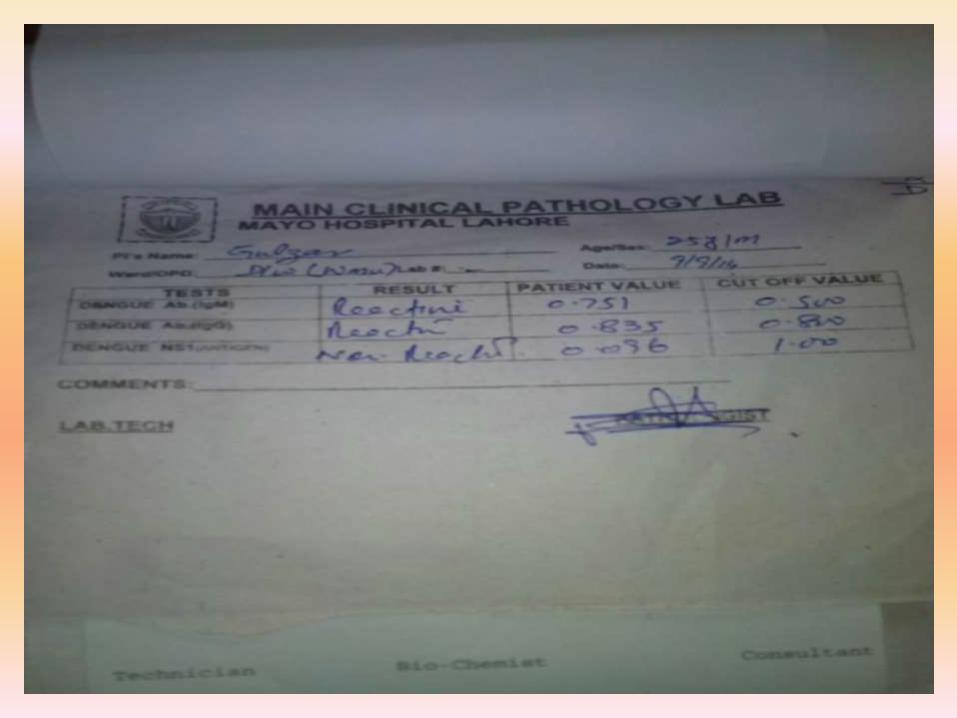
Diagnosis for Dengue
• Travel history and symptom profile
• Detection of antibodies against the virus
• Complete blood count
• Chemistry panel
• Liver function test
• Occult blood in stool
• DIC panel

Recognize the Stage of the Disease
►Febrile phase
►Critical phase
►Convalescent phase
►Day of the illness ?
►Evidence of plasma leakage ?
►Convalescent rash ?
HOW

Fluid Therapy“No Fixed Regime”
►Cornerstone of management
►Dynamic approach
►Be fully aware of the dynamics of the disease
►Mode of intervention depends on:► Phase
► Clinical type
►Type of fluid►Oral fluids
►Crystalloid
►Colloid

Fluid Shifts
►N.Saline – 1 hour
►Colloids – 4 to 6 hours
Febrile Phase
►Oral fluids only►Electrolyte solutions
►IV fluids are not mandatory►Undue vomiting or diarrhea
►Oral fluids not tolerated
►Quantity:►1500ml – 2500ml/24Hrs
►Both oral & IV
►Type:►N.Saline

Critical Phase of DHF Without Shock
► Objective:► Prevent progression to shock► Avoid fluid overloading
► Judicious fluid therapy- Fluid restriction
► Quantity – calculated► M+5% = 4600 ml / 48 hrs (50Kg)► Full quota for entire critical phase 48 hrs► Approximately 90 ml/hr► Adjust infusion rate to match the dynamics of plasma leakage
► Type:► N.Saline
MonitorHRPP > 20 mm HgCRFT < 2 secsU.O.P. 0.5-1ml/kg/hrHCTRR <20/mt
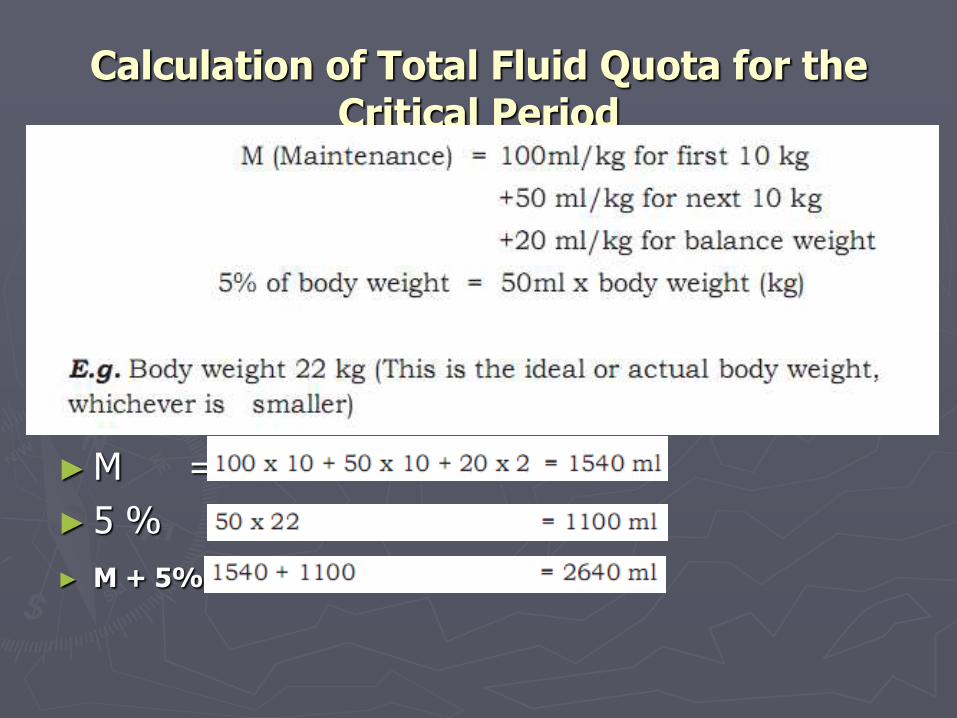
Calculation of Total Fluid Quota for the Critical Period
►M =
► 5 % =
► M + 5% =

Guide to rate of fluid intake in Critical Phase
PulseBPPulse PressureCRFTWarmth / ColdnessUOP – ml/kg/hrEvidence of Bleeding

DHF with ShockAggressive Fluid Therapy
► Objective
►Resuscitate
►Prevent further shock
►Anticipate & prevent complications of shock►GIT bleeding & DIC
► Intervention depends on:► Compensated shock
►Systolic pressure maintained but signs of reduced perfusion
►Narrow Pulse Pressure
►Cold extremities
► Low volume pulse
► Hypotensive shock
►Unrecordable BP & Pulse

Compensated Shock
► N.Saline 10ml/kg (approx 500 ml) IV – 1Hr► No improvement
► Collect blood► venous BGA
► Calcium HCT before & after fluid bolus► Sugar
Sodium ► Grouping & DT
► Colloid bolus 10ml/kg IV over 1 hr► Colloid boluses
► Haemodynamically unstable► HCT drops
► Blood transfusion

Hypotensive ShockHCT before & after fluid bolus
►N.Saline 10ml/kg IV bolus over 15 mts►2nd bolus 10 ml/kg over 60 mts►Collect blood
►Blood gas analysis►Calcium►Electrolytes►Sugar►Grouping & cross matching
►Colloid 10 ml/kg IV bolus over 1 hr

Choice of ColloidBoluses NOT infusions
►Dextran 40►3 boluses over 24 hours
►6 boluses over 48 hours
►6% starch-Heta starch(Voluven)►5 boluses over 24 hours
►10 boluses over 48 hours
►Fresh Frozen Plasma►1 bolus
►3 units approximately 450 – 600 ml

Monitoring & Documentation
► Early detection of shock►Pulse pressure < 20 mm Hg►CRFT > 2 secs►HCT increase of 20% or more from baseline
► Judge the efficacy of IV fluid therapy►PP , CRFT, No postural hypotension►Hourly UOP 0.5 – 1.0 ml/kg/hr
► Early detection of complications of fluid therapy►Respiratory rate > 20/mt ►Lung bases►SaO2 < 92% ►CXR

0 Hr 24 Hr
48 Hr
Time of Presentation and Management
F C R
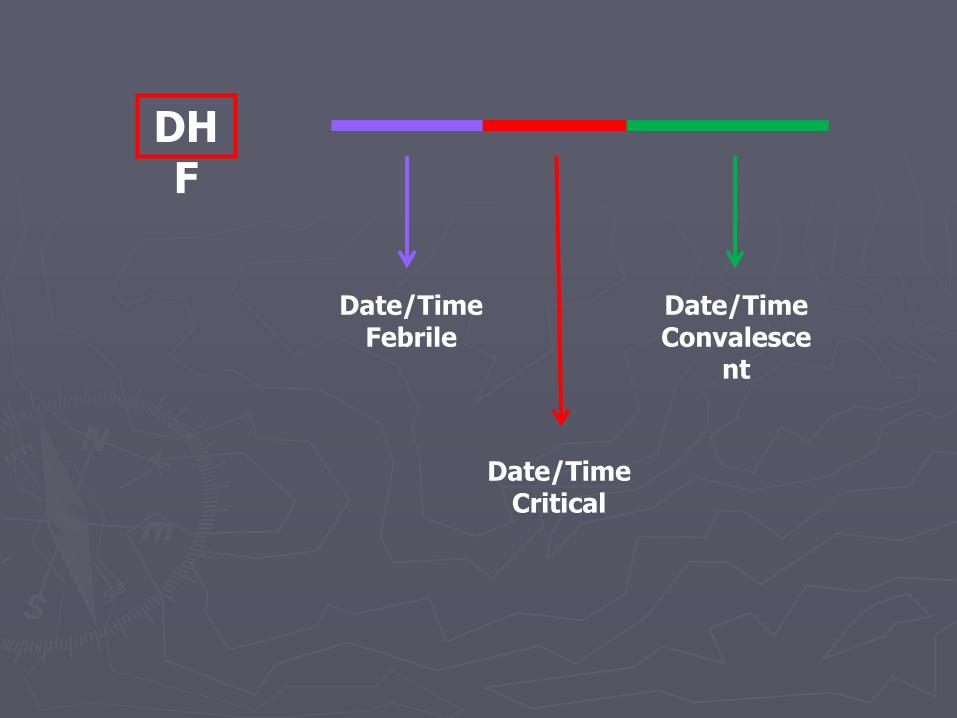
DHF
Date/TimeFebrile
Date/TimeCritical
Date/TimeConvalesce
nt
Basic MonitoringAll Patients
►Pulse rate►Pulse pressure►CRFT►Respiratory rate►FBC - HCT►Intensity of monitoring depends on
►Phase of the illness►Severity►Aggressiveness of fluid therapy
►Accurate fluid balance charts

Monitoring Platelet Count Drops Below 100,000
►FBC- twice daily►Vital parameters- four hourly
Pulse rate Blood pressure (both systolic and diastolic), Respiratory rate, Capillary refill time
►Detailed fluid balance chart- Type and route of fluid hourly, Urine output four hourly
MonitoringEvidence of Plasma Leakage
Escalate ►Vital signs - hourly►HCT - 8 hourly►Fluid intake & the balance left from the
calculated quota ►Temporal relationship ►Critical phase►In hours
►Detailed fluid balance chart

MonitoringIV Fluid Therapy
Phase of the illness – be fully aware►Adequacy of fluid therapy
►Pulse Pressure >20 mmHg►CRFT <2 sec►Pulse Rate <80/mt►UOP > 0.5 ml/Kg/hr►HCT
►Early detection of fluid overloadingRespiratory rate > 20/mt
►Lung bases►SaO2 < 92% ►CXR
Shift toICU
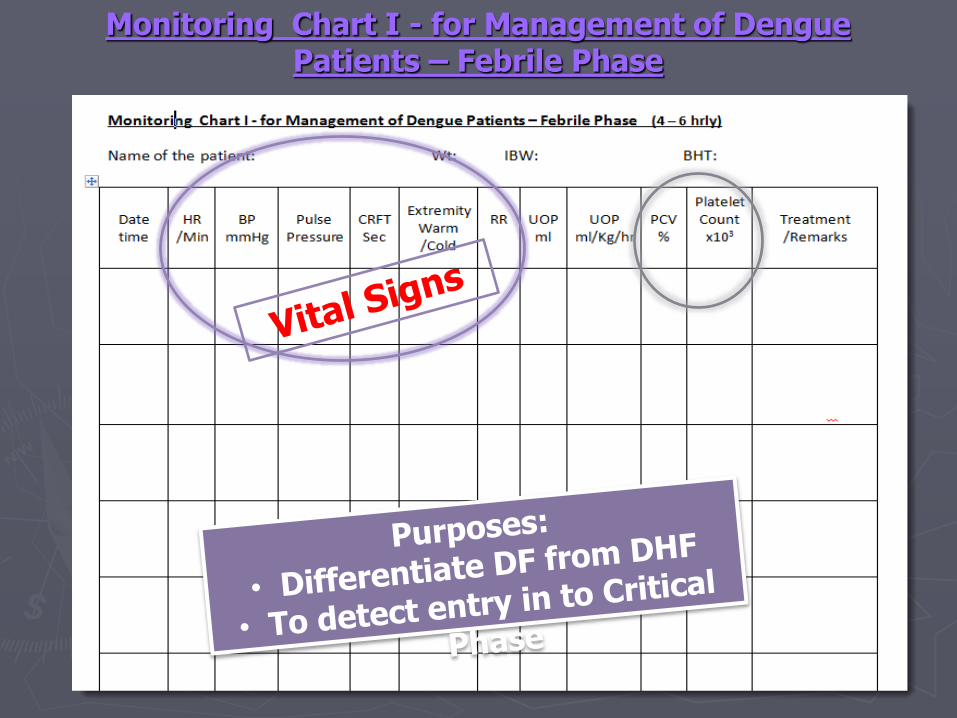
Monitoring Chart I - for Management of Dengue Patients – Febrile Phase

Monitoring Chart I - for Management of Dengue Patients – Febrile Phase
D4 without Fever
D3 with FeverWBC<5000/mm3
N-40% L-58%TT + ve

Monitoring Chart I - for Management of Dengue Patients – Febrile Phase
D4 with FeverTT + ve, WBC<5000/mm3
N-40% L-58%Tender Liver

Monitoring Chart II for Management of DHF Patients during Critical Phase Patient to be monitored hourly
Name of the patient ………………………………………………………BHT……………………………….Date and time of admission ………………………………ward -…………………
Critical Phase Commencing date and time -…………………………………………………….. End date and time …………………………………
10
9
8
7
6
5
4
3
2
1.5
1
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
PCV
Fluids
HR
BP
Pulse Pressure
RR
CRFT extremities
UOP UOP
ml/Kg/hr
Platelet count
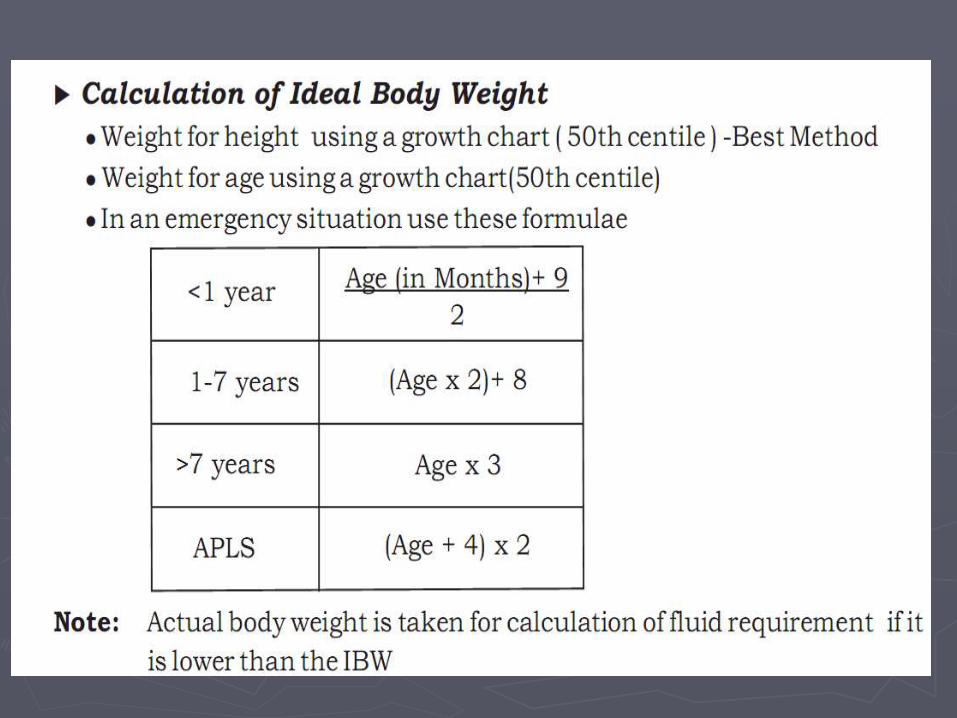
Weight - …………………………………
Height - ……………………………
Ideal body weight - …………… M- ………………………………… M+ 5% = …………………………ml
Annexure II
Used
Remaining
Monitoring Chart II for Management of DHF Patients during Critical Phase

0 Hr 24 Hr
48 Hr
Date/Time Scale 2 Hrs
Date/Time Scale 20 Hrs
Date/Time Scale 36 Hrs

Monitoring Chart II for Management of DHF Patients during Critical Phase

Monitoring Chart II for Management of DHF Patients during Critical Phase
Summary – Febrile Patient
►Dengue or not?
Clinical
FBC
►Leucopaenia + thrombocytopaenia
►DF or DHF ?
Plasma leakage + or –
►If DHF – what is the phase ?

Summary
►In Critical phase
Time of entry
Predicted time of end
►Aggressive monitoring
►Calculate the fluid quota
►Dynamic approach to fluid therapy
►Final diagnosis – precise (DF or DHF & grade)

78
Pts with complications ....
Usually due to
• PROLONG SHOCK• FLUID OVERLOAD

Fluid overload– Too much fluids in febrile phase
– Calculation of fluids in obese pt-ABW vsIBW
– Use of hypotonic saline
– Given excess fluids
– Given more than time of leakage
– Not using colloidal solution when indicates
– Not giving blood when there is concealed bleeding
– Inappropriate IV Fluids for “severe bleeding”
Eg: FFP, platelets & cryo 79
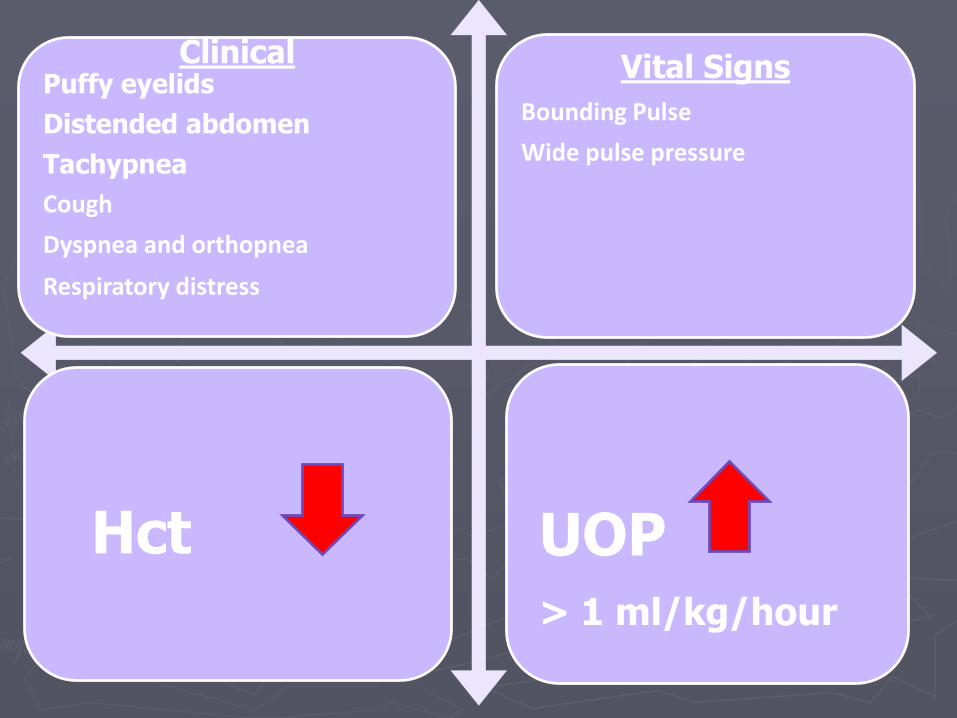
ClinicalPuffy eyelids
Distended abdomen
Tachypnea
Cough
Dyspnea and orthopnea
Respiratory distress
Vital Signs
Bounding Pulse
Wide pulse pressure
Hct UOP> 1 ml/kg/hour

Management of fluid overload
Frusemide 1 mg/kg
Critical Phase

Indications for IV Frusemide
► Midway in the infusion of colloids when colloids are given to patients who are already fluid overloaded or who are likely to be overloaded depending on the fluids already given.
► Midway between blood transfusions.
► In patients passing less than 0.5ml/kg/hr of urine despite receiving adequate fluids and having stable BP, pulse, Hctto improve the UOP.
► During recovery phase when there is suggestion of pulmonary oedema or fluid overload.
82

Prolonged shock
– Delayed diagnosis/ delayed resuscitation
– Late presentation
– Fluid restriction without monitoring
83

ClinicalRestless
Irritable
Behaviour changes e.g. –Confusion, speak fowl language
Vital Signs
Tachycardia
Pulse Pressure - < 20
CRFT - > 2 sec
Cold Extremities
Hct UOP< 0.5 ml/kg/hour

> 4 hours untreated Liver failure- prognosis 50%
Liver + Renal failure - prognosis10%
3 organs failure (+respiratory failure) – Prognosis is a miracle!!!
> 10 hours untreated - Death!!!
85

Complicated DHF►When a pt is deteriorating with no
response to fluid therapy….
A: AcidosisB: BleedingC: CalciumS: Sugar
86

A : Acidosis
►Acidosis is common in profound shock
►Prolonged acidosis makes patients more prone to DIC
►Correct acidosis if pH is <7.35 together with HCO3- level <15 mmol/l
►One may use empirical NaHCO3 1ml/kgsslow bolus (max 10ml) diluted in equal volume
87
B : Bleeding
►Significant overt bleeding - >6-8ml/kg BW
►Concealed bleeding
88
When to suspect bleeding ?
• When PCV drop without clinical improvement
Even with bleeding the PCV drop may take time(4-5hrs). When the pt does not show improvement important to do repeat PCVs frequently!
• Haematocrit not as high as expected for the degree of shock to be explained by plasma leakage alone. (Hypotensive shock with low or normal HCT)
• Severe metabolic acidosis and end-organ dysfunction despite adequate fluid replacement
89

Massive bleeding
Not given blood transfusion
Delayed blood transfusion
90
Remember!!!
In DHF Bleeding could be concealed

How to manage bleeding
►Use PRC or WB
►If there is fluid overload(most frequently) use PRC as 5ml/kg at once and repeat only if needed depending on the response
►If there is no fluid overload use 10ml/kg of WB
►Even if bleeding is likely and if PCV is >45% do not give blood without bringing down the PCV first by giving a colloid.
91
• 5ml/kg of PRC or 10ml/kg of WB will increase PCV by 5%
– Eg.10 year old girl with PCV of 26% in shock..
– Base line PCV in a 10 yr old 36% but if in shock it will be up by 20% 43%. There is 17% deficit which need 3 PRC transfusuions
92

C : Hypocalcaemia
►Every patient with complicated DHF has hypocalcaemia.
►Dengue patients who develop convulsions are likely to have hypocalcaemia.(may give them empirical calcium)
►Detection of hypocalcaemia:
Measure serum Ca2+ level
Corrected QT interval in ECG
93

When to give calcium?
94

Treat if blood sugar below 4 mmol/lt
Give 10% dextose 3-5ml/kg bolus followed by an infusion
S : Hypoglycaemia
95
Platelet transfusion-
►when platelets are low may need but only in very exceptional circumstances
(Thailand only in <0.4% of pts with DHF)
Each platelet pack is 50-150ml contribute
to fluid overload
No prophylaxis platelet transfusion
96

Why do you do platelet counts?
To recognize the beginning of critical stage-YES
To decide on platelet transfusion- NO
As a prognostic indicator- YES
97

Recombinant factor VII
►1 dose = 1,500 USD in a 10-kgs patient
►No use in cases with prolonged shock and multiple organs failure
►Consider in cases with bleeding where the cause is not prolonged shock BUT other reason: peptic ulcer, trauma etc
98
Place of dopamine and dobutamine...
►Very limited in DHF
►May do harm than good by giving a false impression about BP
►When using1st make sure that there is enough intravascular volume shown by increased CVP
99
No Place For Steroids And Iv Immunoglobulins In Dengue
100
101
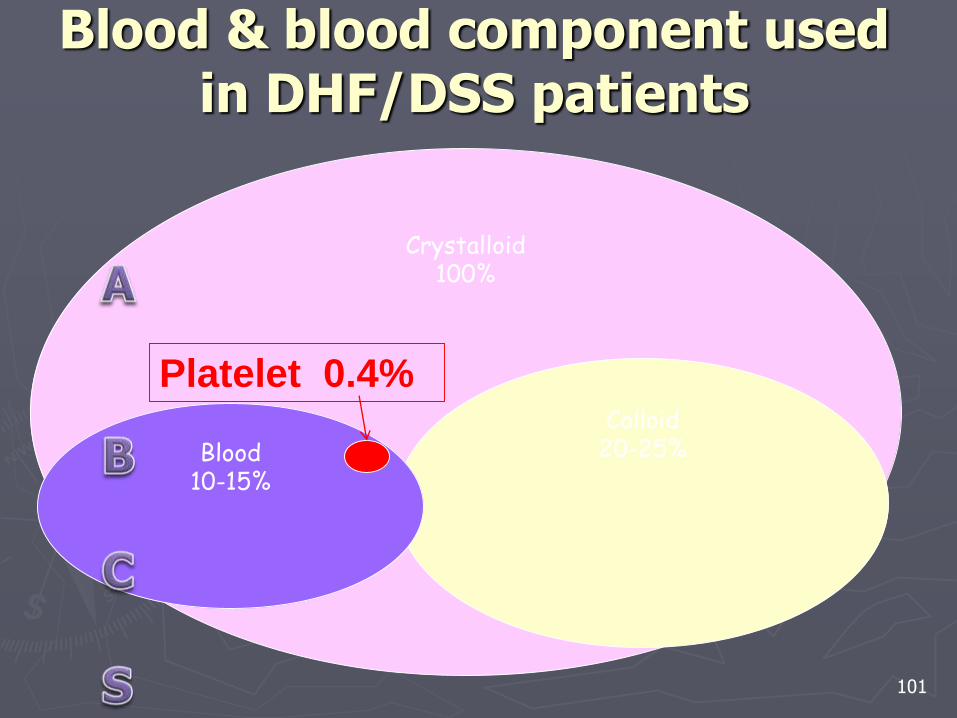
Crystalloid100%
Colloid20-25%Blood
10-15%
Blood & blood component used in DHF/DSS patients
Platelet 0.4%

Myocardial involvement in Dengue
►Global dysfunction of myocardial contractility seen in prolonged shock
►Due to, metabolic acidosis, Hypocalcaemia
►Unlikely to cause death
►If myocarditis is suspected fluid should be given very carefully
►Rx- Symptomatic
102

Causes of death in DHF patients
• Prolonged shock– Delayed diagnosis/ delayed resuscitation – Late presentation
• Fluid overload– Use of hypotonic saline– Given excess fluids– Given more than time of leakage
• Massive bleeding– Not given blood transfusion– Delayed blood transfusion
• Unusual manifestations– Encephalopathy– Underlying co-morbidity– Dual infection
103