dental adhesives for direct placement composite ... · pdf filedental adhesives for direct...
TRANSCRIPT
Earn
3 CE creditsThis course was
written for dentists, dental hygienists,
and assistants.
Dental Adhesives for Direct Placement Composite Restorations: An UpdateA Peer-Reviewed Publication Written by Howard E. Strassler, DMD, FADM, FAGD and Michael Mann, DDS
Publication date: Sept. 2011Expiration date: Aug. 2014
AbstractDental adhesives used to bond composite resins to tooth structure have evolved over the last several decades. The earliest bonding systems required an acid-etch technique and were only compatible with enamel, and the challenge has always been to predictably bond to enamel and dentin simultaneously. There can be confusion as to what bonding agents are being described, because there are a number of different labeling categories. With a simplified, logical category description the clinician is better able to understand what each bonding agent is and how it is used. Bonding systems can in fact be differentiated into two distinct classes: etch-and-rinse and self-etch. Both classes of bonding systems work well as long as one understands which to use for different treatment conditions. There is no one universal bonding system that does it all, but recent advances in the chemistries of these adhesives allow many of them to be bonded to all intraoral substrates – to enamel; to dentin; and to all types of dental resins, ceramics and metals. The key to success is to provide your patients with materials and techniques that you can reproduce to achieve the best, longest-lasting clinical results.
Learning ObjectivesThe overall goal of this article is to provide the reader with information on the classifications, indications and current techniques for restorative clinical success with adhesives. After reading this article the reader should be able to:1. Describe the differences between etch-and-rinse and
self-etch adhesives and relate these categories to other naming systems
2. Discuss the current research evidence comparing etch-and-rinse and self-etch adhesives
3. List and describe the indications for etch-and-rinse and self-etch adhesives
4. Describe the clinical procedure for an etch-and-rinse and a self-etch single-step adhesive
Author ProfilesDr. Howard Strassler is professor in the department of endodontics, prosthodontics and operative dentistry at the University of Maryland School of Dentistry. He is a fellow in the Academy of Dental Materials and the Academy of General Den-tistry, a member of the the Academy of Operative Dentistry, and the International Association for Dental Research. Dr. Stras-sler has published more than 475 articles, coauthored seven chapters in texts, and lectured nationally and internationally. Dr. Strassler is a consultant to over 15 dental manufacturers and is on editorial boards for several dental journals. Dr. Michael Mann is an assistant professor in the Advanced Education in General Dentistry residency at the University of Maryland School of Dentistry. He is a member of the American Dental Association. He has lectured nationally and internation-ally. Dr. Mann has a full-time general practice with an emphasis on comprehensive dental care and aesthetics.
Author DisclosureThe author(s) of this course have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
This course has been made possible through an unrestricted educational grant.
Supplement to PennWell Publications This course was written for dentists, dental hygienists and assistants, from novice to skilled. Educational Methods: This course is a self-instructional journal and web activity. Provider Disclosure: Pennwell does not have a leadership position or a commercial interest in any products or services discussed or shared in this educational activity nor with the commercial supporter. No manufacturer or third party has had any input into the development of course content.Requirements for Successful Completion: To obtain 3 CE credits for this educational activity you must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%.
CE Planner Disclosure: Michelle Fox, CE Coordinator does not have a leadership or commercial interest with DENTSPLY Caulk, the commercial supporter, or with products or services discussed in this educational activity.
Educational Disclaimer: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
Registration: The cost of this CE course is $59.00 for 3 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
Go Green, Go Online to take your coursePennWell designates this activity for 3 Continuing Educational Credits

www.ineedce.com 2
Educational objectivesThe overall goal of this article is to provide the reader with information on the classifications, indications and current techniques for restorative clinical success with adhesives. After reading this article the reader should be able to:1. Describe the differences between etch-and-rinse and
self-etch adhesives and relate these categories to other naming systems
2. Discuss the current research evidence comparing etch-and-rinse and self-etch adhesives
3. List and describe the indications for etch-and-rinse and self-etch adhesives
4. Describe the clinical procedure for an etch-and-rinse and a self-etch single-step adhesive
AbstractDental adhesives used to bond composite resins to tooth structure have evolved over the last several decades. The earliest bonding systems required an acid-etch technique and were only compatible with enamel, and the challenge has always been to predictably bond to enamel and dentin simul-taneously. There can be confusion as to what bonding agents are being described, because there are a number of different labeling categories. With a simplified, logical category de-scription the clinician is better able to understand what each bonding agent is and how it is used. Bonding systems can in fact be differentiated into two distinct classes: etch-and-rinse and self-etch. Both classes of bonding systems work well as long as one understands which to use for different treatment conditions. There is no one universal bonding system that does it all, but recent advances in the chemistries of these adhesives allow many of them to be bonded to all intraoral substrates – to enamel; to dentin; and to all types of dental resins, ceramics and metals. The key to success is to provide your patients with materials and techniques that you can reproduce to achieve the best, longest-lasting clinical results.
IntroductionImportant advances and innovations in restorative dental treatment that have changed the way we treat patients for the better would certainly include fluorides, local anes-thesia, high-speed handpieces, dental radiography and implants. Another innovation that would be near the top of this elite list is dental resin adhesion. Little did Michael Buonocore and colleagues at the Eastman Dental Center in Rochester, New York, realize that the introduction of adhesion, first bonding to enamel, would change the way we practice dentistry. G.V. Black described the retention of restorations based upon cavity design and undercut dentin.1 Even with the caries removed, because of the limitations of the restorative materials available at the time (gold foil and dental silver amalgam), additional tooth structure needed to be removed to fulfill the requirements for retention of the restorative material. The goal of conservation of tooth
structure was limited by the materials that were available up until the late 1960s, when clinical techniques with resin adhesives bonded to etched enamel were introduced using UV-light-cured resin restoratives, a resin sealant and a com-posite resin that utilized the acid etch technique described by Buonocore.2,3
Bonding to tooth substrates is now the standard of care for single-tooth direct placement restorations and has been the driving force in changing how we prepare and restore teeth. With the use of adhesives, minimally invasive den-tistry (MID) with a more conservative, tooth-structure saving approach when treatment planning restorative dental procedures is possible. While the majority of restorations placed today are restoration replacements, minimally in-vasive adhesive restorative dentistry not only relates to the treatment of caries but also to these restoration replacements and to elective esthetic dentistry. There has been a signifi-cant change in the principles of cavity preparation design, from the traditional principles of “extension for prevention” described by G.V. Black to a more carious lesion-centered approach.4-6 This lesion-centered approach is possible through the advancements in adhesive restorative materials, as well as through the introduction of computer-assisted methods of caries detection, a better understanding of the role of magnification, digital radiography and caries risk assessment of the patient to allow for improved conserva-tive caries management.7 One of the greatest benefits of a more conservative approach is that it allows the clinician to maintain as much tooth structure as possible.
While enamel bonding and dentin bonding have been pursued in parallel paths, the goal has been to develop a uni-versal adhesive that bonds to all substrates used in dentistry: enamel, dentin, metals, ceramics and composite resin. This author remembers reading an article in 1985 written by Dr. Wayne Barkmeier on the fundamental elements for an adhesive used for bonding restorative materials to tooth structure. Recently these five key prerequisites for success-ful adhesion to tooth structure were reiterated because they have not changed since then.8 (Table 1)
Table 1. Key prerequisites for successful adhesion 1. The procedure must be safe and biologically acceptable.2. The level of bond strength must be clinically significant to avoid discoloration at the margins and secondary caries.3. The bond strength must be routinely achieved so that predictable results are obtained.4. The bond must be established quickly in order to permit immediate finishing.5. The bond must be stable in vivo for a clinically significant period of time.
Since then, significant advances in the development of dental adhesives have been accomplished. The adhesives currently available offer reliable adhesion between restor-ative materials and tooth structure.

3 www.ineedce.com
Enamel and dentin bonding: An historical perspectiveIn 1955, Buonocore described a clinical technique that uti-lized diluted phosphoric acid to etch the enamel surface and provide for retention of unfilled, self-cured acrylic resins.9 The resin mechanically locked to the microscopically rough-ened enamel surface, forming small “tags” as it flowed into the 10-to-40-micrometer-deep enamel microporosities and then polymerizing. (Figure 1) The first clinical use of this technique was for the placement of sealants.10 The combi-nation of acid etching enamel and adhesive composite resin restorations afforded the benefits of reduction or elimination of microleakage at the enamel margins with a decrease in sensitivity, less discoloration at the margins, lower rates of recurrent caries and improved retention of the restoration.11,12
The effectiveness and success of etched enamel/resin bond has been demonstrated in many reported clinical trials.13
Figure 1. SEM of etched enamel
Unlike enamel bonding, dentin bonding has seen an evolution in its viability. Effective dentin-bonding materials should fulfill several goals. (Table 2)
Table 2. Goals for effective dentin-bonding materials
• The material should be retentive to dentin at a clinically acceptable level, and it should be able to withstand intraoral forces of occlusion and mastication.
• The bond should be instantaneous once the material has set.
• The material and technique must be biocompatible.
• The material should resist the forces of polymerization shrinkage of composite resins and the coefficient of thermal expansion and contraction to eliminate microleakage.
• The material should create a long-lasting bond to dentin.
• Postoperative sensitivity must be minimized or eliminated.
The earliest research in 1956 with dentin bonding fo-cused on chemical adhesion of resins to the inorganic com-ponents of dentin.14 This created a very weak bond, the basis
for which was the presence of the dentin smear layer.15 Other attempts using similar technologies for dentin bonding were not very successful.16, 17 These products had limited success and the search for a better adhesive to dentin continued. Another research path for dentin bonding investigated the use of an etch-and-rinse (total-etch) approach by etching the enamel and dentin simultaneously with phosphoric acid.18,19 At the time, there was concern that phosphoric acid placed on dentin would cause pulpal inflammation and necrosis.20 Jennings and Ranly demonstrated that the pulpal effect of phosphoric acid on dentin for one minute was minimal.21 Early results reported with dentin etching were disappoint-ing because the adhesive resin used was the same unfilled hydrophobic Bis-GMA bonding resin used for etched enamel.19 The hydrophobic resin would not wet the moist, vital dentin and predictable adhesion could not be produced.
Contemporary adhesivesThe breakthrough in the etch-and-rinse (total-etch) ap-proach was first described in the late 1970s by Fusayama and coworkers,22 Bertolotti23 and Kanca.24 They demonstrated the success of the etch-and-rinse (total-etch) adhesive bond based upon the addition of a hydrophilic monomer, usually hydroxyethyl methylmethacrylate (HEMA), to the primer and adhesive. This hydrophilic monomer allows the adhe-sive resin to penetrate the peritubular dentin and dentinal tubules.25-27 (Figure 2) Simultaneously, Bowen was investi-gating the use of a dentin primer that in fact was a self-cure adhesive that was painted on the enamel and dentin, and that produced clinically acceptable bonds.28 In recent years self-etch adhesives for bonding to enamel and dentin have been introduced,29 and some adhesives have added fillers to improve physical properties30. While the earlier generations of adhesives to dentin were disappointing in their clinical performance, contemporary adhesives are demonstrating excellent clinical success.31-37
Figure 2. SEM of multiple-bottle etch-and-rinse adhesive infil-trated dentin hybrid zone (3-E&R) (dentin has been dissolved to demonstrate resin infiltration)

www.ineedce.com 4
Classification of bonding systemsThe development of improved adhesion systems using different chemistries with a variation in the numbers of re-agents and steps for application led to several descriptions of the categories and classification of adhesives. With no standard on how adhesives were classified and described, there was some confusion among clinicians and research-ers alike. With the development of two different classes of bonding systems that relied on the use of phosphoric acid as a surface etchant came the classification and description of bonding systems based upon generational time-line changes. Fourth-generation bonding systems were re-ferred to as total-etch multi-bottle (multi-step) systems, and fifth-generation systems were referred to as total-etch single-bottle bonding agents that contained both primer and adhesive. Both fourth- and fifth-generation products required a total-etch with phosphoric acid before adhesive placement.
It is obvious that the more steps required to bond a restoration, the greater the potential for inconsistency of timing of application, rinsing, drying, rewetting dentin and maintaining a controlled operative field during treatment.38 Manufacturers responded to this by put-ting research efforts into the development of simpli-fied adhesive systems and reduction in the number of steps required. Thus the earliest self-etching bonding systems were introduced. These did not require the ad-ditional steps of applying phosphoric acid, rinsing and drying before adhesive application. The classification system became more confusing in that bonding systems that had the additional step of phosphoric acid etching were referred to as total-etch, and those adhesives that did not require the additional step of phosphoric acid were referred to as self-etch. Other bonding systems continued with generational descriptions building on the fourth- and fifth-generation model, and the self-etching systems were referred to as sixth and seventh genera-tion. These terminologies do not adequately describe the current adhesives that are being used for composite resin bonding.
All adhesives used today exhibit the same phenomena for adhesion, i.e., micromechanical locking to the etched enamel prisms and to dentin through hybridization.38 There have been several attempts to better describe the different bonding systems based upon the steps required and the chemistry of the adhesives. In 2003, Van Meer-beek et al. proposed a rational, logical categorization and classification of the current adhesives based upon what is required to achieve the adhesive interface to enamel and dentin.39 (Table 3) Based upon the current adhesives being used in our practices, the classification of adhesives can be broken down into two distinct categories: etch-and-rinse (E&R), which is also referred to as total-etch (TE ), and self-etch (SE).
Table 3. Classification of adhesives according to Van Meerbeek et al.23
Etch-and-Rinse Adhesives (also referred to as Total-Etch)Three-step multiple-bottle etch-and-rinse adhesives (3-E&R)Two-step single-bottle etch-and-rinse adhesives (2-E&R)Self-Etch AdhesivesTwo-step multiple-bottle self-etch adhesives (2-SEA)One-step multiple-bottle mix self-etch adhesives (1-SEA)One-step no-mix self-etch adhesives (1-SEA)
Etch-and-Rinse approachThe etch-and-rinse (E&R) or total-etch (TE) adhesives can be recognized by the initial application of a 10%-40% phos-phoric acid to the enamel/dentin followed by the mandato-ry rinsing step. The enamel etching leaves a microscopically roughened surface to bond to and removes the dentin smear layer. The enamel surface can be completely dried with air, but the dentin should remain damp and glossy. To leave the dentin slightly damp, the wet dentin can be blotted dry or after air drying can be rewetted with a slightly damp cotton pellet.40-45 This will leave the dentin as a damp, glossy sur-face. An adhesive resin is then applied. The adhesive resin is provided as either two bottles, a separate dentin primer and separate adhesive (also referred to as three-step etch-and-rinse) (3-E&R) (e.g., ProBond, Dentsply-Caulk; Op-tibond FL, Kerr; ScotchBond MP, 3M-ESPE), or a single bottle that contains both primer and adhesive (also referred to as two-step etch-and-rinse) (2-E&R) (e.g., Prime and Bond NT, Dentsply-Caulk; XP Bond, Dentsply-Caulk; Optibond Solo Plus, Kerr; One Step Plus, Bisco). Many of the single-bottle etch-and-rinse systems are provided as a unit dose. Based upon the evidence to date, bonding to enamel is best accomplished with this technique. In vitro and in vivo research has demonstrated that etch-and-rinse adhesives can reliably bond to both enamel and dentin.46-48
The duration of enamel etching has been suggested as 15-30 seconds, while research has demonstrated that for most clinical situations dentin should be etched for only 15 seconds. Dentin age can also have an effect on adhesion, and it has been recommended to increase etching time to 30 sec-onds for sclerotic dentin (found in patients in the age range of 55-60 years and older), the rationale being that compared to normal dentin, sclerotic dentin exhibits hypermineraliza-tion and is resistant to phosphoric acid etching.49-51
Clinical success with etch-and-rinse adhesives is depen-dent on the basic clinical technique: 1. Prepare the tooth (all classes of cavity preparations; can be in
enamel-only Class IV, facial veneers, porcelain veneers).2. Etch with a phosphoric acid (range of concentration 10%-40%)
for 15-30 seconds (15 seconds for normal dentin and 30 seconds for sclerotic dentin).
3. Rinse with air-water spray for 10 seconds.4. Dry the tooth, leaving the enamel frosty, dentin glossy (moist).52, 53
5. Apply adhesive system of choice using a rubbing action54; light cure.6. Apply restorative material; light cure.

5 www.ineedce.com
Self-etch adhesives Self-etch adhesive systems are aqueous mixtures of acidic functional monomers, usually phosphoric acid esters with a pH value higher than that of phosphoric acid gels.55 The SE approach does not require a separate etching step because the etchant is incorporated into the adhesive (either in a separate self-etching primer or in the adhesive). Addition-ally, the step of rewetting with water is eliminated because SE adhesives contain water and are never completely dried from the tooth. SE adhesives do not remove the smear layer, instead incorporating it into the adhesive. Investigations have demonstrated that SE systems provide hybridization and infiltration of dentin similar to that seen with etch-and-rinse adhesives.56-58 There has been concern about the qual-ity of bonding of SE adhesives to enamel. If enamel is left unprepared, it is resistant to etching and adhesion with most SE adhesives.59-61 For preparations that include both dentin and enamel, it is recommended that the enamel be prepared with a bur or diamond to optimize the bond to the enamel. Currently, the use of an SE adhesive for restoring Class IV incisal edge fractures, esthetic facial veneering and diastema closures with direct composite resin and bonding porcelain veneers is contraindicated. 62
A chief complaint among practitioners has been the rate of postoperative sensitivity observed following placement of Class I, II and V composite resin restorations, especially using etch-and-rinse adhesives. However, several clinical studies have found no differences in postoperative sensi-tivity with etch-and-rinse or SE adhesives.63-67 In fact, the conclusion of one study stated that postoperative sensitivity may depend on the restorative technique and variability among operators rather than on the type of enamel-dentin adhesive used.63 Postoperative sensitivity may, however, be linked to using a TE adhesive bonding to desiccated dentin.44,45 Since SE adhesives contain water and require no rinsing or drying, the dentin remains moist, which may ac-count for reports of minimized postoperative sensitivity.68,69 Santini and coworkers investigated microleakage around Class V restorations bonded with etch-and-rinse and SE adhesives, concluding that SE systems were as reliable as TE systems.70
Clinical success with self-etch adhesives is dependent on the following basic clinical technique: 1. Prepare the tooth (preparations that are self-retentive,
e.g., box-like Class I, II, III and V, and Class V NCCL with an enamel bevel; not Class IV, not facial veneers, not porcelain veneers).
2. Apply the SE adhesive following the manufacturer’s timing and application instructions. This is very product specific.
3. DO NOT RINSE. Air-dry the tooth following the timing and intensity of air spray from the product instructions; do not take any shortcuts.
4. Light cure the adhesive.5. Apply restorative material.6. Light cure.
Adhesion to tooth structure: Clinical challengesNot all dentin and enamel is equally bondable. Factors influencing the bond include the presence of amalgam resto-rations, caries and other tooth conditions that can affect the quality of etching and the quality of adhesion to enamel and dentin. There has been a trend to replace defective amalgam restorations with composite resins. When removing an amal-gam restoration it is not unusual to find discolored enamel and dentin present due to the leaching of metallic ions and corrosion products into the dentin tubules. Harnirattisai et al. found no differences in adhesion between normal dentin and discolored amalgam-affected dentin with either an etch-and-rinse adhesive or a self-etch adhesive.71 However, bonding to caries-affected dentin has been shown to be reduced.72-74 Fluorosed enamel and dentin can also be more difficult to bond to. For enamel fluorosis, the recommendation is to prepare the enamel with a bur or diamond to improve bond-ing.75 For fluoride-rich dentin, self-etching adhesives provide better bonding.76 Of note, with the increased interest in tooth whitening and the availability of over-the-counter peroxide-based products, the clinician may not know if their patients are bleaching their teeth. Research supports waiting at least one week after bleaching before any restorative procedure with either an etch-and-rinse or SE adhesive to prevent inter-ference with bonding adhesion and material setting.77-81
An area of recent investigation has been the compatibility of TE and SE systems with self-cure and dual-cure composite resins. There is contradictory evidence on whether or not SE and TE single-bottle adhesive systems bond well to self-cure and dual-cure composite resins due to the acidity of the sin-gle-bottle primer-adhesive. Some studies have demonstrated a decreased bond and other studies have demonstrated no effect.82-84 Some recent studies evaluating TE and SE systems and their compatibility with dual-cure and self-cure compos-ite resins have demonstrated some changes in chemistry that have resulted in composite resin-adhesive compatibility.85-89 This variability requires that the clinician review the manu-facturer’s recommendations for use with self-cure and dual-cure composite resins.
There has been concern over the durability and longevity of the bond to dentin, and the in vitro bond strength to dentin has been shown to decrease over time for some adhesives.90-94 The mechanism of bond degradation has been attributed to the loss of hybrid layer integrity, which then compromises resin-dentin bond stability. A number of researchers have focused on the matrix metalloproteinases (MMPs) within the collagen that may be partially responsible for hybrid layer degradation.95 To prevent or decrease the degradation of bonding using either TE or SE adhesives, a number of chemical reagents that are known to inhibit MMPs have been evaluated. Chlorhexidine (CHX) has been shown to have an inhibitory effect on MMPs,96 and a number of studies have evaluated the successful use of CHX to inhibit the degradation of adhesion to dentin.97-100 Other MMP
www.ineedce.com 6
inhibitors that produce results similar to those of CHX have also been investigated, including polyvinylphosphonic acid101 and quaternary ammonium methacrylates102. Another ap-proach to inhibiting bond degradation has been to use ethanol instead of water when wetting the dentin.103,104 With a better understanding of improving bond durability by using prote-ase inhibitors, there will be changes in adhesive chemistries to reflect the need to inhibit MMPs with recommendations with TE adhesives to apply CHX for one minute after etching and/or to use CHX as a primer before use of an SE.105-107 Some manufacturers are reviewing the addition of CHX or other MMP inhibitors into SE adhesives.
Clinical applicationsThe recommendations for the use of adhesive systems are product specific. A summary of the indications and clinical applications for each adhesive system is provided in Table 4, based upon the clinical evidence and clinical reports.
Table 4. Clinical applications for adhesive systems.
Etch-and-Rinse (Total-Etch) Adhesive SystemsMultiple-bottle (3-E&R): All uses including
self-cure composite resin cores and dual-cure composite resin cementation
Single-bottle (2-E&R): Direct composite resin placement and with systems that have an activator use with self-cure and dual-cure composites is acceptable
Self-Etching Adhesive Systems (not indicated with self-cure or dual-cure composites unless the manufacturer makes the recommendation and has a self-cure activator)Multiple-step systems (2-SEA): Direct placement Class I, II, III and V with prepared enamelSingle-step mix systems (1-SEA): Direct placement Class I, II, III and V with prepared enamelSingle-step no mix (1-SEA): Direct placement Class I, II, III and V with prepared enamel
Use of any adhesive is manufacturer specific for use with self-cure and dual-cure composite resin systems. Currently, self-etching systems can be used for Class IV incisal edge repair, facial veneering and porcelain veneers with a light cure cement (or flowable composite as a luting agent) with the use of a total-etch of the enamel surface with phosphoric acid etchant. As more evidence becomes available in clinical trials this recommendation may change. Also, if phosphoric acid is used with an SE adhesive, only the enamel needs to be etched.
Anterior direct composite resin restorations: Class III, IV, V and facial veneers When preparing Class III, IV and V restorations, as well as facial veneer preparations, the type of preparation will determine whether an etch-and-rinse or self-etch adhesive
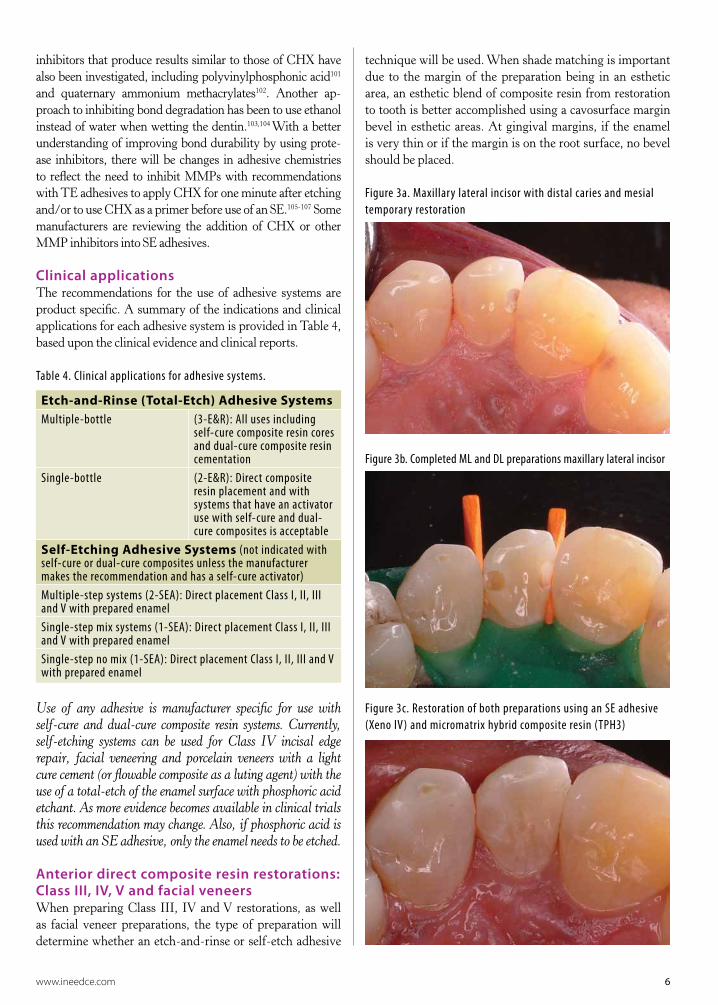
technique will be used. When shade matching is important due to the margin of the preparation being in an esthetic area, an esthetic blend of composite resin from restoration to tooth is better accomplished using a cavosurface margin bevel in esthetic areas. At gingival margins, if the enamel is very thin or if the margin is on the root surface, no bevel should be placed.
Figure 3a. Maxillary lateral incisor with distal caries and mesial temporary restoration
Figure 3b. Completed ML and DL preparations maxillary lateral incisor
Figure 3c. Restoration of both preparations using an SE adhesive (Xeno IV) and micromatrix hybrid composite resin (TPH3)
7 www.ineedce.com
Class III restorations can be required to replace a defec-tive restoration or due to initial caries. Class III prepara-tions with box-like features and retentive walls can be restored with TE or SE adhesives. (Figure 3) When using a self-etch adhesive with a Class III preparation, it is im-portant to follow the manufacturer’s directions, especially the length of time the adhesive is on the tooth as well as whether or not the self-etch adhesive needs to be agitated during placement since this is product dependent.
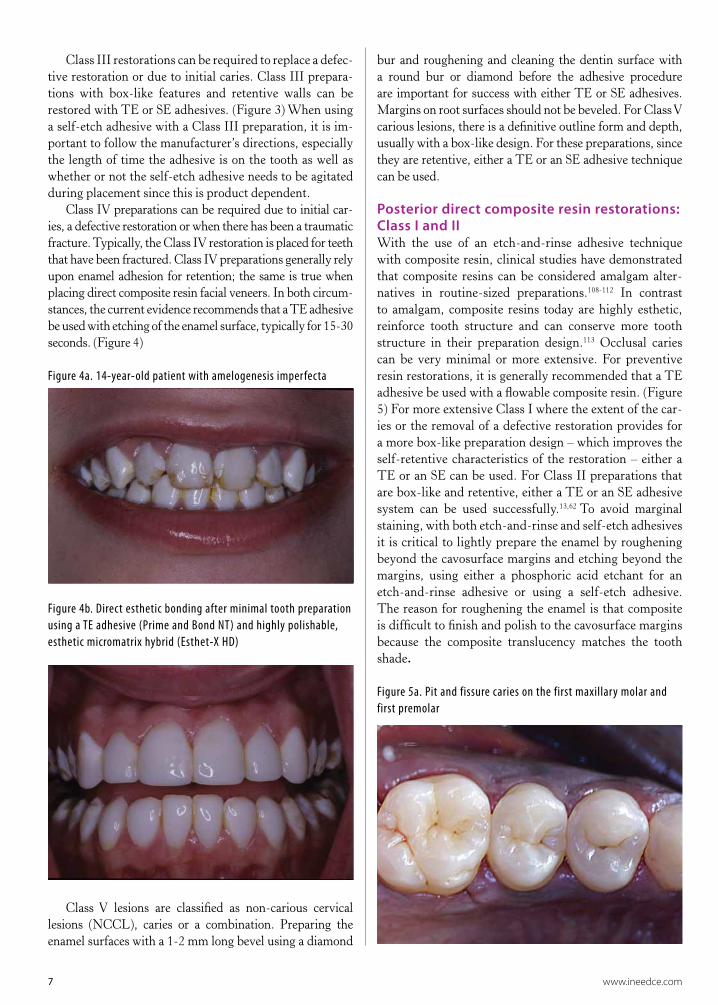
Class IV preparations can be required due to initial car-ies, a defective restoration or when there has been a traumatic fracture. Typically, the Class IV restoration is placed for teeth that have been fractured. Class IV preparations generally rely upon enamel adhesion for retention; the same is true when placing direct composite resin facial veneers. In both circum-stances, the current evidence recommends that a TE adhesive be used with etching of the enamel surface, typically for 15-30 seconds. (Figure 4)
Figure 4a. 14-year-old patient with amelogenesis imperfecta
Figure 4b. Direct esthetic bonding after minimal tooth preparation using a TE adhesive (Prime and Bond NT) and highly polishable, esthetic micromatrix hybrid (Esthet-X HD)
Class V lesions are classified as non-carious cervical lesions (NCCL), caries or a combination. Preparing the enamel surfaces with a 1-2 mm long bevel using a diamond
bur and roughening and cleaning the dentin surface with a round bur or diamond before the adhesive procedure are important for success with either TE or SE adhesives. Margins on root surfaces should not be beveled. For Class V carious lesions, there is a definitive outline form and depth, usually with a box-like design. For these preparations, since they are retentive, either a TE or an SE adhesive technique can be used.
Posterior direct composite resin restorations: Class I and II With the use of an etch-and-rinse adhesive technique with composite resin, clinical studies have demonstrated that composite resins can be considered amalgam alter-natives in routine-sized preparations.108-112 In contrast to amalgam, composite resins today are highly esthetic, reinforce tooth structure and can conserve more tooth structure in their preparation design.113 Occlusal caries can be very minimal or more extensive. For preventive resin restorations, it is generally recommended that a TE adhesive be used with a flowable composite resin. (Figure 5) For more extensive Class I where the extent of the car-ies or the removal of a defective restoration provides for a more box-like preparation design – which improves the self-retentive characteristics of the restoration – either a TE or an SE can be used. For Class II preparations that are box-like and retentive, either a TE or an SE adhesive system can be used successfully.13,62 To avoid marginal staining, with both etch-and-rinse and self-etch adhesives it is critical to lightly prepare the enamel by roughening beyond the cavosurface margins and etching beyond the margins, using either a phosphoric acid etchant for an etch-and-rinse adhesive or using a self-etch adhesive. The reason for roughening the enamel is that composite is difficult to finish and polish to the cavosurface margins because the composite translucency matches the tooth shade.
Figure 5a. Pit and fissure caries on the first maxillary molar and first premolar
www.ineedce.com 8
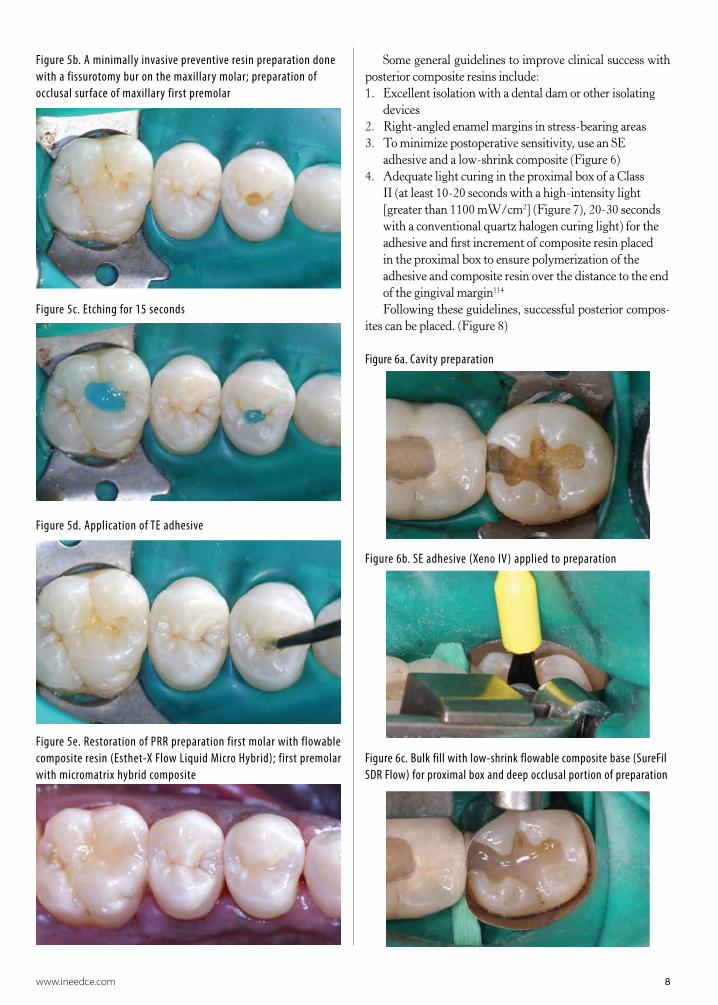
Figure 5b. A minimally invasive preventive resin preparation done with a fissurotomy bur on the maxillary molar; preparation of occlusal surface of maxillary first premolar
Figure 5c. Etching for 15 seconds
Figure 5d. Application of TE adhesive
Figure 5e. Restoration of PRR preparation first molar with flowable composite resin (Esthet-X Flow Liquid Micro Hybrid); first premolar with micromatrix hybrid composite
Some general guidelines to improve clinical success with posterior composite resins include:1. Excellent isolation with a dental dam or other isolating
devices2. Right-angled enamel margins in stress-bearing areas3. To minimize postoperative sensitivity, use an SE
adhesive and a low-shrink composite (Figure 6) 4. Adequate light curing in the proximal box of a Class
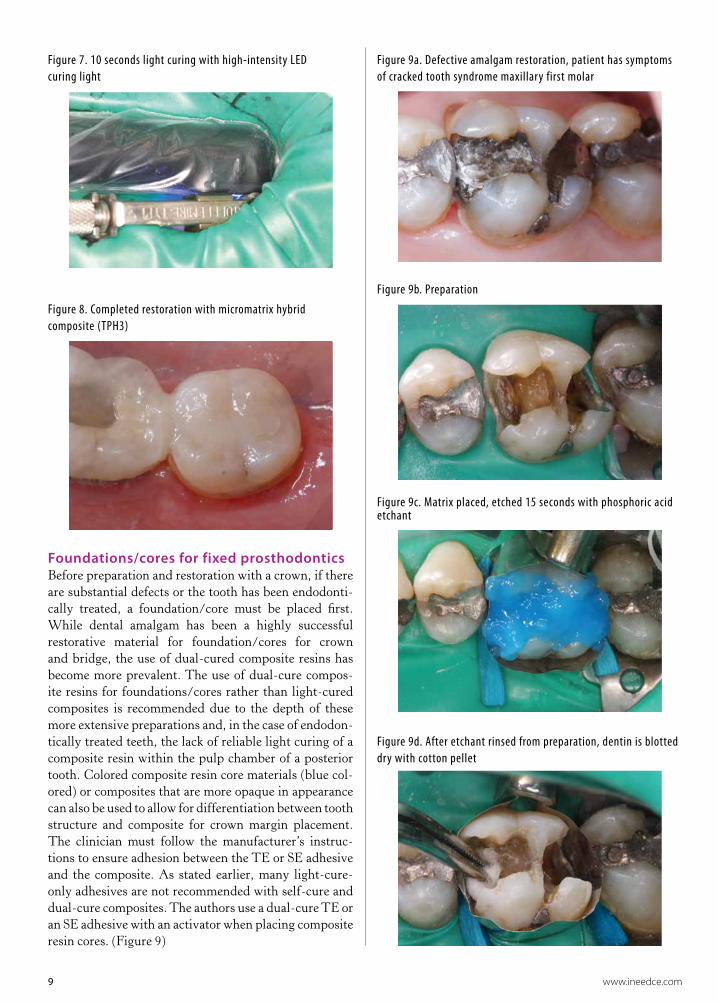
II (at least 10-20 seconds with a high-intensity light [greater than 1100 mW/cm2] (Figure 7), 20-30 seconds with a conventional quartz halogen curing light) for the adhesive and first increment of composite resin placed in the proximal box to ensure polymerization of the adhesive and composite resin over the distance to the end of the gingival margin114
Following these guidelines, successful posterior compos-ites can be placed. (Figure 8)
Figure 6a. Cavity preparation
Figure 6b. SE adhesive (Xeno IV) applied to preparation
Figure 6c. Bulk fill with low-shrink flowable composite base (SureFil SDR Flow) for proximal box and deep occlusal portion of preparation
9 www.ineedce.com
Figure 7. 10 seconds light curing with high-intensity LED curing light
Figure 8. Completed restoration with micromatrix hybrid composite (TPH3)
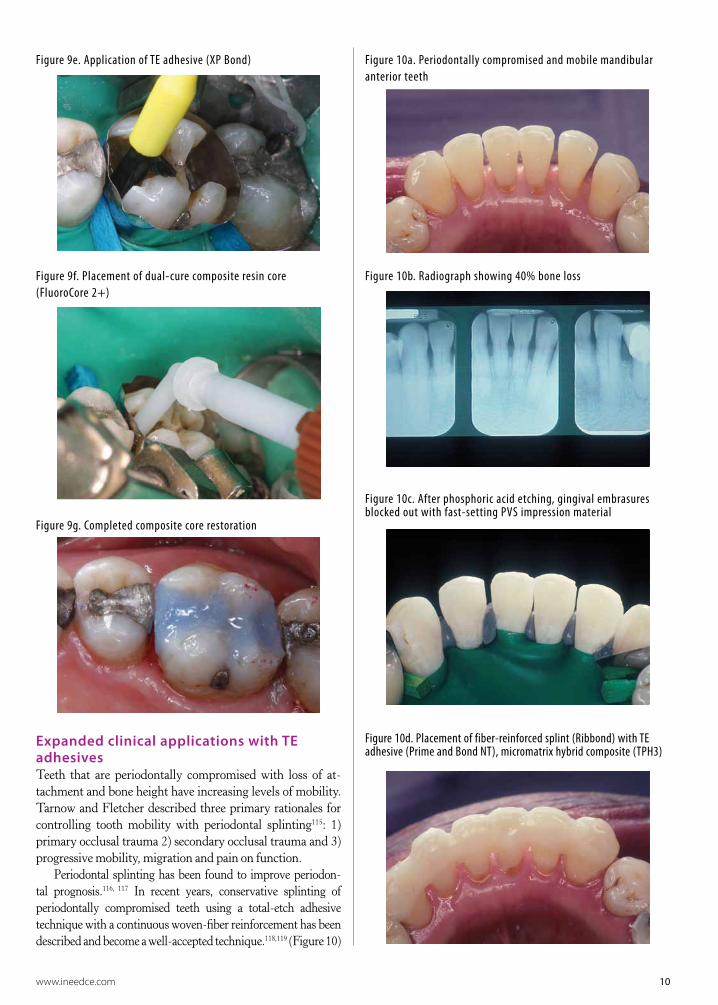
Foundations/cores for fixed prosthodonticsBefore preparation and restoration with a crown, if there are substantial defects or the tooth has been endodonti-cally treated, a foundation/core must be placed first. While dental amalgam has been a highly successful restorative material for foundation/cores for crown and bridge, the use of dual-cured composite resins has become more prevalent. The use of dual-cure compos-ite resins for foundations/cores rather than light-cured composites is recommended due to the depth of these more extensive preparations and, in the case of endodon-tically treated teeth, the lack of reliable light curing of a composite resin within the pulp chamber of a posterior tooth. Colored composite resin core materials (blue col-ored) or composites that are more opaque in appearance can also be used to allow for differentiation between tooth structure and composite for crown margin placement. The clinician must follow the manufacturer’s instruc-tions to ensure adhesion between the TE or SE adhesive and the composite. As stated earlier, many light-cure-only adhesives are not recommended with self-cure and dual-cure composites. The authors use a dual-cure TE or an SE adhesive with an activator when placing composite resin cores. (Figure 9)
Figure 9a. Defective amalgam restoration, patient has symptoms of cracked tooth syndrome maxillary first molar
Figure 9b. Preparation
Figure 9c. Matrix placed, etched 15 seconds with phosphoric acid etchant
Figure 9d. After etchant rinsed from preparation, dentin is blotted dry with cotton pellet
www.ineedce.com 10
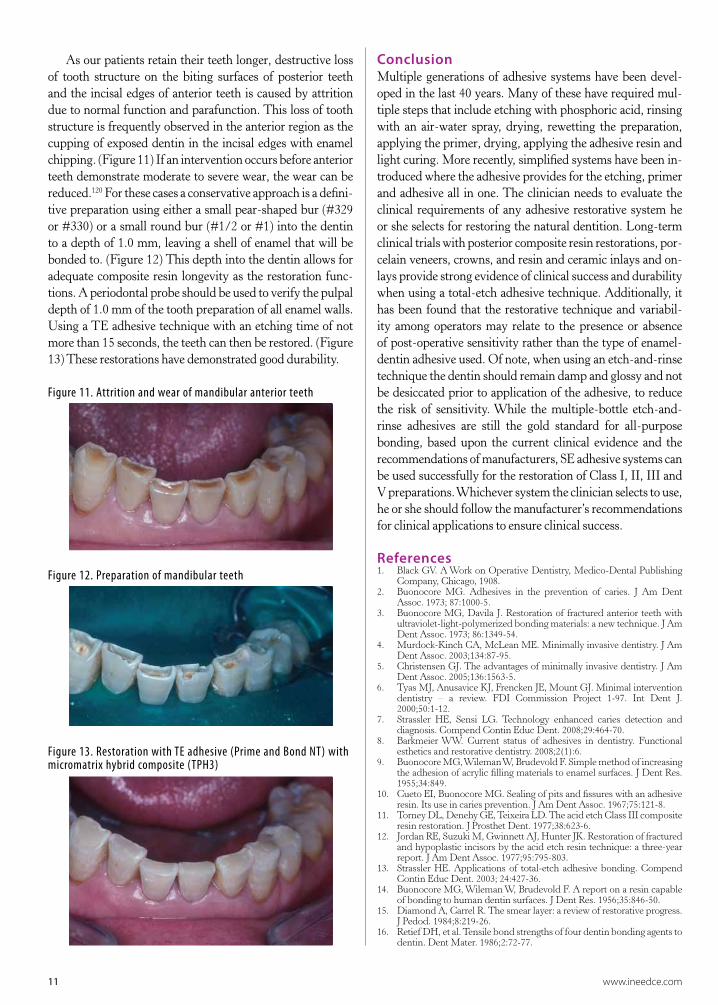
Figure 9e. Application of TE adhesive (XP Bond)
Figure 9f. Placement of dual-cure composite resin core (FluoroCore 2+)
Figure 9g. Completed composite core restoration
Expanded clinical applications with TE adhesivesTeeth that are periodontally compromised with loss of at-tachment and bone height have increasing levels of mobility. Tarnow and Fletcher described three primary rationales for controlling tooth mobility with periodontal splinting115: 1) primary occlusal trauma 2) secondary occlusal trauma and 3) progressive mobility, migration and pain on function.
Periodontal splinting has been found to improve periodon-tal prognosis.116, 117 In recent years, conservative splinting of periodontally compromised teeth using a total-etch adhesive technique with a continuous woven-fiber reinforcement has been described and become a well-accepted technique.118,119 (Figure 10)
Figure 10a. Periodontally compromised and mobile mandibular anterior teeth
Figure 10b. Radiograph showing 40% bone loss
Figure 10c. After phosphoric acid etching, gingival embrasures blocked out with fast-setting PVS impression material
Figure 10d. Placement of fiber-reinforced splint (Ribbond) with TE adhesive (Prime and Bond NT), micromatrix hybrid composite (TPH3)
11 www.ineedce.com
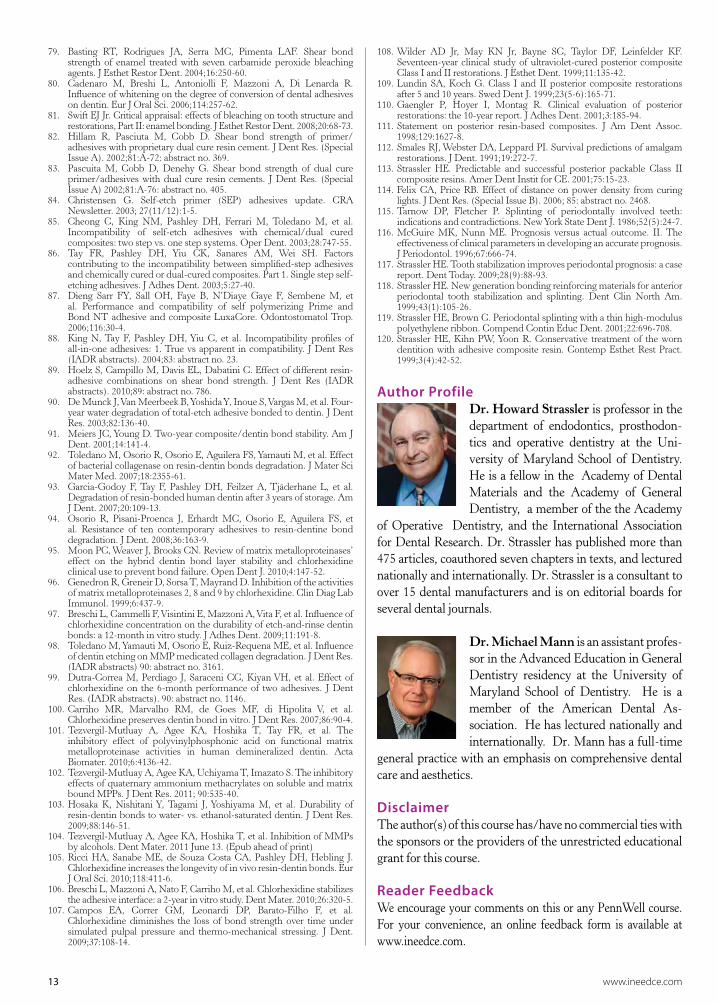
As our patients retain their teeth longer, destructive loss of tooth structure on the biting surfaces of posterior teeth and the incisal edges of anterior teeth is caused by attrition due to normal function and parafunction. This loss of tooth structure is frequently observed in the anterior region as the cupping of exposed dentin in the incisal edges with enamel chipping. (Figure 11) If an intervention occurs before anterior teeth demonstrate moderate to severe wear, the wear can be reduced.120 For these cases a conservative approach is a defini-tive preparation using either a small pear-shaped bur (#329 or #330) or a small round bur (#1/2 or #1) into the dentin to a depth of 1.0 mm, leaving a shell of enamel that will be bonded to. (Figure 12) This depth into the dentin allows for adequate composite resin longevity as the restoration func-tions. A periodontal probe should be used to verify the pulpal depth of 1.0 mm of the tooth preparation of all enamel walls. Using a TE adhesive technique with an etching time of not more than 15 seconds, the teeth can then be restored. (Figure 13) These restorations have demonstrated good durability.
Figure 11. Attrition and wear of mandibular anterior teeth
Figure 12. Preparation of mandibular teeth
Figure 13. Restoration with TE adhesive (Prime and Bond NT) with micromatrix hybrid composite (TPH3)
ConclusionMultiple generations of adhesive systems have been devel-oped in the last 40 years. Many of these have required mul-tiple steps that include etching with phosphoric acid, rinsing with an air-water spray, drying, rewetting the preparation, applying the primer, drying, applying the adhesive resin and light curing. More recently, simplified systems have been in-troduced where the adhesive provides for the etching, primer and adhesive all in one. The clinician needs to evaluate the clinical requirements of any adhesive restorative system he or she selects for restoring the natural dentition. Long-term clinical trials with posterior composite resin restorations, por-celain veneers, crowns, and resin and ceramic inlays and on-lays provide strong evidence of clinical success and durability when using a total-etch adhesive technique. Additionally, it has been found that the restorative technique and variabil-ity among operators may relate to the presence or absence of post-operative sensitivity rather than the type of enamel-dentin adhesive used. Of note, when using an etch-and-rinse technique the dentin should remain damp and glossy and not be desiccated prior to application of the adhesive, to reduce the risk of sensitivity. While the multiple-bottle etch-and-rinse adhesives are still the gold standard for all-purpose bonding, based upon the current clinical evidence and the recommendations of manufacturers, SE adhesive systems can be used successfully for the restoration of Class I, II, III and V preparations. Whichever system the clinician selects to use, he or she should follow the manufacturer’s recommendations for clinical applications to ensure clinical success.
References 1. Black GV. A Work on Operative Dentistry, Medico-Dental Publishing
Company, Chicago, 1908.2. Buonocore MG. Adhesives in the prevention of caries. J Am Dent
Assoc. 1973; 87:1000-5.3. Buonocore MG, Davila J. Restoration of fractured anterior teeth with
ultraviolet-light-polymerized bonding materials: a new technique. J Am Dent Assoc. 1973; 86:1349-54.
4. Murdock-Kinch CA, McLean ME. Minimally invasive dentistry. J Am Dent Assoc. 2003;134:87-95.
5. Christensen GJ. The advantages of minimally invasive dentistry. J Am Dent Assoc. 2005;136:1563-5.
6. Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry – a review. FDI Commission Project 1-97. Int Dent J. 2000;50:1-12.
7. Strassler HE, Sensi LG. Technology enhanced caries detection and diagnosis. Compend Contin Educ Dent. 2008;29:464-70.
8. Barkmeier WW. Current status of adhesives in dentistry. Functional esthetics and restorative dentistry. 2008;2(1):6.
9. Buonocore MG, Wileman W, Brudevold F. Simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955;34:849.
10. Cueto EI, Buonocore MG. Sealing of pits and fissures with an adhesive resin. Its use in caries prevention. J Am Dent Assoc. 1967;75:121-8.
11. Torney DL, Denehy GE, Teixeira LD. The acid etch Class III composite resin restoration. J Prosthet Dent. 1977;38:623-6.
12. Jordan RE, Suzuki M, Gwinnett AJ, Hunter JK. Restoration of fractured and hypoplastic incisors by the acid etch resin technique: a three-year report. J Am Dent Assoc. 1977;95:795-803.
13. Strassler HE. Applications of total-etch adhesive bonding. Compend Contin Educ Dent. 2003; 24:427-36.
14. Buonocore MG, Wileman W, Brudevold F. A report on a resin capable of bonding to human dentin surfaces. J Dent Res. 1956;35:846-50.
15. Diamond A, Carrel R. The smear layer: a review of restorative progress. J Pedod. 1984;8:219-26.
16. Retief DH, et al. Tensile bond strengths of four dentin bonding agents to dentin. Dent Mater. 1986;2:72-77.

www.ineedce.com 12
17. Eliades GC, Caputo AA, Vougionklakis A. Composition, wetting properties and bond strength with dentin of six new dentin adhesives. Dent Mater. 1985;1:170-6.
18. Lee HL, et al. Effects of acid etchants on dentin. J Dent Res. 1973;52:1228-33.
19. Torney DL. The retentive ability of acid-etched dentin. J Prosthet Dent. 1978;39:169-72.
20. Skinner EW, Phillips RW. The Science of Dental Materials. 5th ed. Philadelphia, PA: WB Saunders; 1960;277.
21. Jennings RF, Ranly DM. Autoradiographic studies of P32 penetration into enamel and dentin during acid etching. J Child Dent. 1972;39:69-71.
22. Fusayama T, Nakamura M, Kurosaki N, Iwaku M. Non-pressure adhesion of a new adhesive restorative system. J Dent Res. 1979;58:1364-1370.
23. Bertolotti RL. Acid etching of dentin. Quintessence Int. 1990;21:77-8.24. Kanca J III. One year evaluation of a dentin-enamel bonding system. J
Esthet Dent. 1990;2:100-3.25. Van Meerbeek B, Inoue S, Perdigão J, Lambrechts P, Vanherle G. Enamel
and dentin adhesion. In Fundamentals of Operative: A Contemporary Approach. 2nd edition. Ed. Summitt JB, Robbins JW, Schwartz RS. Quintessence Books, 2001, 178-235.
26. Van Meerbeek B, Yoshihara K, Yoshida Y, Mine A, De Munck J, et al. State of the art of self-etch adhesives. Dent Mater. 2011;27:17-28.
27. Pashley DH. The effects of acid etching on the pulpodentin complex. Oper Dent. 1992;17:229-42.
28. Bowen RL, Cobb EN. A method for bonding to dentin and enamel. J Am Dent Assoc. 1983;107:734-6.
29. Strassler HE. Self-etching resin adhesives. Inside Dentistry. 2007;3(2):50-4.
30. Giannini M, Mettenburg D, Arrais CA, Rueggeberg FA. The effect of filler addition on biaxial flexural strength and modulus of commercial dentin bonding systems. Quintessence Int. 2011;42:e39-43.
31. van Dijken JW, Sunnegårdh-Grönberg K, Lindberg A. Clinical long-term retention of etch-and-rinse and self-etch adhesive systems in non-carious cervical lesions. A 13 years evaluation. Dent Mater. 2007;23:1101-7.
32. Peumans M, Kanumilli P, De Munch J, Van Landuyt K, et al. Clinical effectiveness of contemporary adhesives: a systematic review of current clinical trials. Dent Mater. 2005;21:864-81.
33. van Kijken JW, Pallesen U. Long-term dentin retention of etch-and-rinse and self-etch adhesives and a resin modified glass ionomer cement in non-carious cervical lesions. Dent Mater. 2008;24:915-22.
34. Dunn J Arambula M, Wilson AC, Santucci E. 18-month clinical evaluation of Xeno IV in cervical lesions. J Dent Res (Special Issue IADR Abstracts). 2007;86: abstract no. 900.
35. van Dijken JW. A prospective 8-year evaluation of mild two-step self-etching adhesive and a heavily filled two-step etch and rinse system in non-carious cervical lesions. Dent Mater 2010; 26:940-6.
36. van Dijken JW, Pallesen U. Four-year clinical evaluation of Class II nano-hybrid resin composite restorations bonded with a one-step self-etch and a two-step etch-and-rinse adhesive. J Dent. 2011;39:16-25.
37. Peumans M, de Munck J, Van Landuyt K, Lambrechts P, Van Meerbeek B. Five-year clinical effectiveness of a two-step self-etching adhesive. J Adhes Dent. 2007;9:7-10.
38. Van Meerbeek B. Mechanism of resin adhesion: dentin and enamel bonding. Functional Esthet Restor Dent. 2008;2(1):18-25.
39. Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, et al. Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent. 2003;28:215-35.
40. Xu C, Wang Y. Collagen cross linking increases its biodegradation resistance in wet dentin bonding. J Adhes Dent. 2011;May 13. (Epub ahead of print).
41. Hashimoto M, Jujita S, Endo K. Bonding of self-etching adhesives on dehydrated dentin. J Adhes Dent. 2011;13:49-54.
42. Walter R, Miguez PA, Swift EJ Jr, Pereira PN. Long-term bond strengths to dentin treated with different re-wetting solutions. Am J Dent. 2008;21:143-7.
43. Hegde M, Manjunath J. Bond strength of newer dentin bonding agents in different clinical situations. Oper Dent. 2011;June 24. (Epub ahead of print).
44. Kanca J. Improved bond strength through acid etching of dentin and bonding to wet dentin surfaces. J Am Dent Assoc. 1996;123:35-43.
45. Gwinnett AJ. Moist versus dry dentin: its effect on shear bond strength. Am J Dent. 1992;5:127-9.
46. De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, et al. A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res. 2005;84:118-32.
47. Inoue S, Vargas MA, Abe Y, Yoshida Y, Lambrechts P, et al. Microtensile bond strength of eleven contemporary adhesives to enamel. Am J Dent. 2003;16:329-34.
48. Shirai K, De Munck J, Yoshida Y, Inoue S, Lambrechts P, et al. Effect of cavity configuration and aging on the bonding effectiveness of six adhesives to dentin. Dent Mater. 2005;21:110-24.
49. Lopes GC, Baratieri CM, Baratieri LN, Monteiro S Jr, Cardoso Vieira
LC. Bonding to cervical sclerotic dentin: effect of acid etching time. J Adhes Dent. 2004;6:19-23.
50. Lopes GC, Vieira LC, Monteiro S Jr, Caldeira de Andrada MA, Baratieri CM. Dentin bonding: effect of degree of mineralization and acid etching time. Oper Dent. 2003;28:429-39.
51. Lopes GC, Vieira LC, Araujo E, Bruggmann T, Zucco J, et al. Effect of dentin age and acid etching time on dentin bonding. J Adhes Dent. 2011;13:139-45.
52. Manso AP, Marquezini L Jr, Silva SM, Pashley DH, Tay FR, et al. Stability of wet versus dry bonding with different solvent based adhesives. Dent Mater. 2008; 24:476-82.
53. Orellana N, Ramirez R, Roiq M, Giner L, Mercade M, et al. Comparative study of the microtensile bond strength of three different total-etch adhesives with different solvents to wet and dry dentin (in vitro test). Acta Odontol Latinoam. 2009;22:47-56.
54. Zander-Grande C, Ferreira SQ, da Costa TR, Loguercio AD, Reis A. Application of etch-and-rinse adhesives on dry and rewet dentin under rubbing action: a 24-month clinical evaluation. J Am Dent Assoc. 2011;142:828-35.
55. Tay FR, Sano H, Carvalho R, Pashley EL, Pashley DH. An ultrastructural study of the influence of acidity on self-etching primers and smear layer thickness on bonding to intact dentin. J Adhes Dent. 2000;2:83-98.
56. Hegde M, Manjunath J. Bond strength of newer dentin bonding agents in different clinical situations. Oper Dent. 2011;June 24. (Epub ahead of time)
57. Hashimoto M, Fujita S, Endo K, Ohno H. Effect of dentinal water on bonding of self-etch adhesives. Dent Mater. 2009;28:634-41.
58. Bernasconi C, Romano S, Alonso Muruaga G, Garcia D. Evaluation of microleakage between two adhesives: self-etch adhesive and total-etch adhesive. J Dent Res. (Argentine Division Abstracts). 2004;83: abstract no. 129.
59. Perdigao J, Geraldeli S. Bonding characteristics of self-etching adhesives to intact versus prepared enamel. J Esthet Restor Dent. 2003;5:32-42.
60. Brackett WW, Ito S, Nishitani Y, Haisch LD, Pashley DH. The microtensile bond strength of self-etching adhesives to ground enamel. Oper Dent. 2006;31:332-7.
61. Di Hipolita V, de Goes MF, Carrilho MR, Chan DC, Daronch M, et al. SEM evaluation of contemporary self-etching primers applied to ground and unground enamel. J Adhes Dent. 2005;7:203-11.
62. Strassler HE. Self-etch adhesives. Inside Dentistry 2006;3(6).63. Perdigao J, Geraldeli S, Hodges JS. Total-etch versus self-etch adhesive
effect on postoperative sensitivity. J Am Dent Assoc. 2003;134:1621-9.64. Akpata ES, Behbehani J. Effect of bonding systems on post-operative
sensitivity from posterior composites. Am J Dent. 2006;19:151-4.65. Perdigao J, Anauate-Netto C, Carmo AR, Hodges JS, Cordeiro HJ,
et al. The effect of adhesive and flowable composite on postoperative sensitivity: 2 week results. Quintessence Int. 2004;35:777-84.
66. Unemori M, Matsuya Y, Akashi A, Goto Y, Akamine A. Self-etching adhesives and postoperative sensitivity. Am J Dent. 2004;17:191-5.
67. Browning WD, Myers M, Downey M, Schull GF, Davenport MB. Reduction in post-operative sensitivity: a community based study. J Dent Res. (Special Issue B) 2006;85: abstract no. 1151.
68. Lee R, Blank JT. Simplify bonding with a single step: one component, no mixing. Contemp Esthet Rest Practice. 2003;7(5):45-6.
69. Van Meerbeek B, Kanumilli P, De Munck J, Van Landuyt K, Lambrechts P, et al. A randomized controlled study evaluating the effectiveness of a two-step self-etch adhesive with and without selective phosphoric-acid etching of enamel. Dent Mater. 2005;21:375-83.
70. Santini A, Ivanovic V, Ibbetson R, Milia E. Influence of cavity configuration on microleakage around Class V restorations bonded with seven self-etching adhesives. J Esthet Restor Dent. 2004;16:128-36.
71. Harnirattisai C, Senawongse P, Tagami J. Microtensile bond strengths of two adhesive resins to discolored dentin after amalgam removal. J Dent Res. 2007; 86:232-6.
72. Ceballos L, Camego DG, Victoria Fuentes M, Osorio R, Toledano M, et al. Microtensile bond strength of total-etch and self-etching adhesives to caries-affected dentine. J Dent. 2003;31:469-77.
73. Say EC, Nakajima M, Senawongse P, Soyman M, Ozer F, et al. Bonding to sound vs caries-affected dentin using photo- and dual-cure adhesives. Oper Dent. 2005;30:90-8.
74. Omar H, El-Badrawy W, El-Mowafy O, Atta O, Saleem B. Microtensile bond strength of resin composite bonded to caries-affected dentin with three adhesives. Oper Dent. 2007;32:24-30.
75. Waidyasekera PG, Nikaido T, Weerasinghe DD, Tagami J. Bonding of acid-etch and self-etch adhesives to human fluorosed dentin. J Dent. 2007;35:915-22.
76. Ermis RB, De Munck J, Cardoso MV, Coutinho E, Van Landuyt KL, et al. Bonding to ground versus unground enamel in fluorosed teeth. Dent Mater. 2007; 23:1250-5.
77. Godwin JM, Barghi N, Berry TG, et al. Time duration for dissipation of bleaching effects before enamel bonding. J Dent Res. 1992;71:179(Abstr 590).
78. Cvitko E, Denehy GE, Swift Jr EJ, Pires JA. Bond strength of composite resin to enamel bleached with carbamide peroxide. J Esthet Dent 1991;3:100-2.
13 www.ineedce.com
79. Basting RT, Rodrigues JA, Serra MC, Pimenta LAF. Shear bond strength of enamel treated with seven carbamide peroxide bleaching agents. J Esthet Restor Dent. 2004;16:250-60.
80. Cadenaro M, Breshi L, Antoniolli F, Mazzoni A, Di Lenarda R. Influence of whitening on the degree of conversion of dental adhesives on dentin. Eur J Oral Sci. 2006;114:257-62.
81. Swift EJ Jr. Critical appraisal: effects of bleaching on tooth structure and restorations, Part II: enamel bonding. J Esthet Restor Dent. 2008;20:68-73.
82. Hillam R, Pasciuta M, Cobb D. Shear bond strength of primer/adhesives with proprietary dual cure resin cement. J Dent Res. (Special Issue A). 2002;81:A-72: abstract no. 369.
83. Pascuita M, Cobb D, Denehy G. Shear bond strength of dual cure primer/adhesives with dual cure resin cements. J Dent Res. (Special Issue A) 2002;81:A-76: abstract no. 405.
84. Christensen G. Self-etch primer (SEP) adhesives update. CRA Newsletter. 2003; 27(11/12):1-5.
85. Cheong C, King NM, Pashley DH, Ferrari M, Toledano M, et al. Incompatibility of self-etch adhesives with chemical/dual cured composites: two step vs. one step systems. Oper Dent. 2003;28:747-55.
86. Tay FR, Pashley DH, Yiu CK, Sanares AM, Wei SH. Factors contributing to the incompatibility between simplified-step adhesives and chemically cured or dual-cured composites. Part 1. Single step self-etching adhesives. J Adhes Dent. 2003;5:27-40.
87. Dieng Sarr FY, Sall OH, Faye B, N’Diaye Gaye F, Sembene M, et al. Performance and compatibility of self polymerizing Prime and Bond NT adhesive and composite LuxaCore. Odontostomatol Trop. 2006;116:30-4.
88. King N, Tay F, Pashley DH, Yiu C, et al. Incompatibility profiles of all-in-one adhesives: 1. True vs apparent in compatibility. J Dent Res (IADR abstracts). 2004;83: abstract no. 23.
89. Hoelz S, Campillo M, Davis EL, Dabatini C. Effect of different resin-adhesive combinations on shear bond strength. J Dent Res (IADR abstracts). 2010;89: abstract no. 786.
90. De Munck J, Van Meerbeek B, Yoshida Y, Inoue S, Vargas M, et al. Four-year water degradation of total-etch adhesive bonded to dentin. J Dent Res. 2003;82:136-40.
91. Meiers JC, Young D. Two-year composite/dentin bond stability. Am J Dent. 2001;14:141-4.
92. Toledano M, Osorio R, Osorio E, Aguilera FS, Yamauti M, et al. Effect of bacterial collagenase on resin-dentin bonds degradation. J Mater Sci Mater Med. 2007;18:2355-61.
93. Garcia-Godoy F, Tay F, Pashley DH, Feilzer A, Tjäderhane L, et al. Degradation of resin-bonded human dentin after 3 years of storage. Am J Dent. 2007;20:109-13.
94. Osorio R, Pisani-Proenca J, Erhardt MC, Osorio E, Aguilera FS, et al. Resistance of ten contemporary adhesives to resin-dentine bond degradation. J Dent. 2008;36:163-9.
95. Moon PC, Weaver J, Brooks CN. Review of matrix metalloproteinases’ effect on the hybrid dentin bond layer stability and chlorhexidine clinical use to prevent bond failure. Open Dent J. 2010;4:147-52.
96. Genedron R, Greneir D, Sorsa T, Mayrand D. Inhibition of the activities of matrix metalloproteinases 2, 8 and 9 by chlorhexidine. Clin Diag Lab Immunol. 1999;6:437-9.
97. Breschi L, Cammelli F, Visintini E, Mazzoni A, Vita F, et al. Influence of chlorhexidine concentration on the durability of etch-and-rinse dentin bonds: a 12-month in vitro study. J Adhes Dent. 2009;11:191-8.
98. Toledano M, Yamauti M, Osorio E, Ruiz-Requena ME, et al. Influence of dentin etching on MMP medicated collagen degradation. J Dent Res. (IADR abstracts) 90: abstract no. 3161.
99. Dutra-Correa M, Perdiago J, Saraceni CC, Kiyan VH, et al. Effect of chlorhexidine on the 6-month performance of two adhesives. J Dent Res. (IADR abstracts). 90: abstract no. 1146.
100. Carriho MR, Marvalho RM, de Goes MF, di Hipolita V, et al. Chlorhexidine preserves dentin bond in vitro. J Dent Res. 2007;86:90-4.
101. Tezvergil-Mutluay A, Agee KA, Hoshika T, Tay FR, et al. The inhibitory effect of polyvinylphosphonic acid on functional matrix metalloproteinase activities in human demineralized dentin. Acta Biomater. 2010;6:4136-42.
102. Tezvergil-Mutluay A, Agee KA, Uchiyama T, Imazato S. The inhibitory effects of quaternary ammonium methacrylates on soluble and matrix bound MPPs. J Dent Res. 2011; 90:535-40.
103. Hosaka K, Nishitani Y, Tagami J, Yoshiyama M, et al. Durability of resin-dentin bonds to water- vs. ethanol-saturated dentin. J Dent Res. 2009;88:146-51.
104. Tezvergil-Mutluay A, Agee KA, Hoshika T, et al. Inhibition of MMPs by alcohols. Dent Mater. 2011 June 13. (Epub ahead of print)
105. Ricci HA, Sanabe ME, de Souza Costa CA, Pashley DH, Hebling J. Chlorhexidine increases the longevity of in vivo resin-dentin bonds. Eur J Oral Sci. 2010;118:411-6.
106. Breschi L, Mazzoni A, Nato F, Carriho M, et al. Chlorhexidine stabilizes the adhesive interface: a 2-year in vitro study. Dent Mater. 2010;26:320-5.
107. Campos EA, Correr GM, Leonardi DP, Barato-Filho F, et al. Chlorhexidine diminishes the loss of bond strength over time under simulated pulpal pressure and thermo-mechanical stressing. J Dent. 2009;37:108-14.
108. Wilder AD Jr, May KN Jr, Bayne SC, Taylor DF, Leinfelder KF. Seventeen-year clinical study of ultraviolet-cured posterior composite Class I and II restorations. J Esthet Dent. 1999;11:135-42.
109. Lundin SA, Koch G. Class I and II posterior composite restorations after 5 and 10 years. Swed Dent J. 1999;23(5-6):165-71.
110. Gaengler P, Hoyer I, Montag R. Clinical evaluation of posterior restorations: the 10-year report. J Adhes Dent. 2001;3:185-94.
111. Statement on posterior resin-based composites. J Am Dent Assoc. 1998;129:1627-8.
112. Smales RJ, Webster DA, Leppard PI. Survival predictions of amalgam restorations. J Dent. 1991;19:272-7.
113. Strassler HE. Predictable and successful posterior packable Class II composite resins. Amer Dent Instit for CE. 2001;75:15-23.
114. Felix CA, Price RB. Effect of distance on power density from curing lights. J Dent Res. (Special Issue B). 2006; 85: abstract no. 2468.
115. Tarnow DP, Fletcher P. Splinting of periodontally involved teeth: indications and contradictions. New York State Dent J. 1986;52(5):24-7.
116. McGuire MK, Nunn ME. Prognosis versus actual outcome. II. The effectiveness of clinical parameters in developing an accurate prognosis. J Periodontol. 1996;67:666-74.
117. Strassler HE. Tooth stabilization improves periodontal prognosis: a case report. Dent Today. 2009;28(9):88-93.
118. Strassler HE. New generation bonding reinforcing materials for anterior periodontal tooth stabilization and splinting. Dent Clin North Am. 1999;43(1):105-26.
119. Strassler HE, Brown C. Periodontal splinting with a thin high-modulus polyethylene ribbon. Compend Contin Educ Dent. 2001;22:696-708.
120. Strassler HE, Kihn PW, Yoon R. Conservative treatment of the worn dentition with adhesive composite resin. Contemp Esthet Rest Pract. 1999;3(4):42-52.
Author ProfileDr. Howard Strassler is professor in the department of endodontics, prosthodon-tics and operative dentistry at the Uni-versity of Maryland School of Dentistry. He is a fellow in the Academy of Dental Materials and the Academy of General Dentistry, a member of the the Academy
of Operative Dentistry, and the International Association for Dental Research. Dr. Strassler has published more than 475 articles, coauthored seven chapters in texts, and lectured nationally and internationally. Dr. Strassler is a consultant to over 15 dental manufacturers and is on editorial boards for several dental journals.
Dr. Michael Mann is an assistant profes-sor in the Advanced Education in General Dentistry residency at the University of Maryland School of Dentistry. He is a member of the American Dental As-sociation. He has lectured nationally and internationally. Dr. Mann has a full-time
general practice with an emphasis on comprehensive dental care and aesthetics.
DisclaimerThe author(s) of this course has/have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
Reader FeedbackWe encourage your comments on this or any PennWell course. For your convenience, an online feedback form is available at www.ineedce.com.
www.ineedce.com 14
Questions
Online CompletionUse this page to review the questions and answers. Return to www.ineedce.com and sign in. If you have not previously purchased the program select it from the “Online Courses” listing and complete the online purchase. Once purchased the exam will be added to your Archives page where a Take Exam link will be provided. Click on the “Take Exam” link, complete all the program questions and submit your answers. An immediate grade report will be provided and upon receiving a passing grade your “Verification Form” will be provided immediately for viewing and/or printing. Verification Forms can be viewed and/or printed anytime in the future by returning to the site, sign in and return to your Archives Page.
1. _________ have improved the way we treat patients.a. Fluoridesb. Local anestheticsc. Dental resin adhesion innovationsd. all of the above
2. _________ described the retention of restorations based upon cavity design and undercut dentin.a. Buonocoreb. Blackc. Ferranted. all of the above
3. _________ has been the driving force in changing how we prepare and restore teeth.a. Fluoride-releasing cementb. The electric handpiecec. Bonding to tooth substratesd. all of the above
4. _________ has/have contributed to the ability to have a lesion-centered approach to restorative treatment.a. Advancements in adhesive restorative materialsb. Caries risk assessmentc. The introduction of computer-assisted methods of
caries detectiond. all of the above
5. _________ is a key prerequisite for suc-cessful adhesion to tooth structure.a. A safe and biologically acceptable procedureb. Bond strength that is clinically significant c. A bond that is stable in vivo for a clinically
significant period of timed. all of the above
6. _________ wrote an article in 1985 on the fundamental elements for an adhesive used for bonding restorative materials to tooth structure.a. Dr. Wayne Swiftb. Dr. Wayne Barkmeier c. Dr. Dwayne Smithd. none of the above
7. Establishing a bond slowly _________.a. is essential for bond strengthb. is essential for adequate finishing c. a and bd. none of the above
8. _________ is a phenomenon for all adhesives used today.a. Micromechanical locking to the etched enamel
prismsb. Bonding to dentin through hybridizationc. Micromechanical locking to etched dentin
crystalsd. a and b
9. For successful dentin bonding, the bond should _________.
a. mature graduallyb. snap-set and then mature graduallyc. be instantaneousd. none of the above
10. _________ is a goal for an effective dentin bonding material.a. Retention at a clinically acceptable levelb. Biocompatibilityc. A long-lasting bond to dentind. all of the above
11. The success of the etch-and-rinse adhe-sive bond was demonstrated by several researchers, based upon the addition of a _________.a. hydrophilic monomerb. hydrophobic monomerc. hydrophilic polymerd. hydrophobic polymer
12. Some adhesives have added _________ to improve physical properties.a. fluorideb. fillersc. carbonited. none of the above
13. The etch-and-rinse adhesives can be recognized by the initial application of a _________ to the enamel/dentin.a. 10%-20% phosphoric acidb. 10%-40% phosphoric acidc. 10%-20% acetic acidd. 10%-40% hydrochloric acid
14. The etch-and-rinse technique is also known as the _________ technique.a. self-etchb. total-etchc. no-etchd. none of the above
15. With the etch-and-rinse technique, prior to bonding the enamel surface can be _________ with air, and the dentin should remain _________.a. completely dried; dryb. partially dried; dryc. completely dried; damp and glossyd. none of the above
16. Based upon the evidence to date, bond-ing to enamel is best accomplished with the _________ technique.a. self-etchb. no-etchc. etch-and-rinsed. none of the above
17. The etch-and-rinse technique involves the use of a ___________ adhesive resin.a. one-bottleb. one- or two-bottlec. three-bottled. none of the above
18. ___________ is a requirement for clinical success with etch-and-rinse adhesives.a. Rinsing with air-water spray for 10 seconds after
etchingb. Drying the tooth after rinsingc. Leaving the enamel frosty and dentin glossy
(moist) after drying d. all of the above
19. The self-etch technique involves the use of _________.a. a separate etchantb. a four-bottle techniquec. a one-step or two-step techniqued. a and c
20. Self-etch adhesive systems are aqueous mixtures of _________.a. acidic functional polymersb. acidic functional monomersc. alkaline functional polymersd. alkaline functional monomers
21. The self-etch approach _________.a. requires a separate etching step b. does not require a separate etching step or rewettingc. requires an additional rewetting stepd. a and c
22. Currently, the use of an self-etch adhesive for direct composite restoration _________ is contraindicated.a. of Class IV incisal edge fracturesb. of esthetic facial veneering c. for diastema closuresd. all of the above
23. Sclerotic dentin _________.a. exhibits hypermineralizationb. is resistant to phosphoric acid etchingc. is found in patients age 55 and aboved. all of the above
24. It has been recommended to increase etching time to _________ for sclerotic dentin.a. 20 secondsb. 30 secondsc. 40 secondsd. 50 seconds
25. Several clinical studies have found _________ differences in postoperative sensitivity with etch-and-rinse or self-etch adhesives.a. majorb. minimalc. nod. none of the above
26. When using a self-etch adhesive, the area _________ after adhesive application.a. must be rinsedb. must not be rinsedc. must be light-curedd. b and c
Questions Continued
15 www.ineedce.com
27. _________ is more difficult to bond to.a. Caries-affected dentinb. Fluorosed enamelc. Fluorosed dentind. all of the above
28. _________ is a matrix metalloproteinase inhibitor that has been used to decrease or prevent bond degradation.a. Chlorhexidineb. Quaternary ammonium methacrylatec. Polyvinylphosphonic acidd. all of the above
29. When preparing Class III, IV and V restorations, the type of _________ will determine whether an etch-and-rinse or self-etch adhesive technique will be used.a. etchantb. lesionc. preparationd. a and b
30. Research supports waiting at least _________ after bleaching before any restorative procedure with an etch-and-rinse or self-etch adhesive.a. one weekb. two weeksc. three weeksd. one month
31. Class III preparations with box-like features and retentive walls can be restored with _________.a. self-etch adhesives onlyb. total etch adhesives onlyc. self-etch or total-etch adhesivesd. none of the above
32. A minimally invasive preventive resin preparation can be performed with a _________ bur.a. large carbideb. large pear-shaped diamondc. end-cuttingd. fissurotomy
33. The mechanism of dentin bond degradation has been attributed to the loss of _________.a. hybrid layer integrityb. prismsc. the sealed surfaced. all of the above
34. For preventive resin restorations, it is generally recommended that a ________ adhesive be used with a flowable composite resin.a. self-etchb. total-etchc. self-etch or total-etchd. none of the above
35. To avoid _________, with both etch-and-rinse and self-etch adhesives it is critical to lightly prepare the enamel.a. dentin discolorationb. marginal stainingc. fractured. none of the above
36. One approach to inhibiting bond degradation has been to use _________ instead of water when wetting the dentin.a. acetylamideb. ethanolc. essential oilsd. fluoride rinse
37. Postoperative sensitivity _________.a. may be linked to using total-etch adhesive bonding
to desiccated dentinb. may depend on the restorative technique rather
than the type of adhesive system usedc. is a chief complaint among practitioners following
placement of Class I, II and V restorationsd. all of the above
38. With the use of an etch-and-rinse adhesive technique, clinical studies have demonstrated that composite resins can be considered _________.a. inferior alternatives to amalgamb. amalgam alternatives in routine-sized preparationsc. equivalent to cast gold crownsd. a or b
39. An esthetic blend of composite resin from restoration to tooth is better ac-complished using a _________ in esthetic areas.a. line angle bevelb. cavosurface levelc. cavosurface margin beveld. none of the above
40. The use of _________ composite resin is recommended for foundations/cores.a. light-curedb. dual curec. light-cured or dual cured. none of the above
41. _________ described three primary rationales for controlling tooth mobility with periodontal splinting.a. Fletcher and Langb. Tarnow and Fletcherc. Tarnow and Langd. Tarnow and Buser
42. If phosphoric acid is used with a self-etch adhesive, _________ need(s) to be etched.a. only the enamelb. only the dentinc. both the dentin and the enameld. none of the above
43. If phosphoric acid is used with an etch-and-rinse adhesive, _________ be etched.a. only the enamel mayb. only the dentin mayc. both the dentin and the enamel cand. none of the above
44. Colored (blue) composite resin is used for _________.a. Class I restorationsb. sealantsc. foundations/coresd. all of the above
45. Conservative splinting of periodontally compromised teeth using a _________ adhesive technique with a(n) _________ woven-fiber reinforcement has been described.a. self-etch; intermittentb. self-etch; continuousc. total-etch; continuousd. none of the above
46. Destructive loss of tooth structure on the biting surfaces of posterior teeth and the incisal edges of anterior teeth is caused by _________.a. attrition due to normal functionb. attrition due to parafunctionc. periodontal diseased. a and b
47. Anterior teeth with incisal edge tissue loss can be restored using a _________ adhesive technique with an etching time of not more than _________.a. self-etch; 10 secondsb. total-etch; 10 secondsc. self-etch; 15 secondsd. total-etch; 15 seconds
48. _________ clinical trials with posterior composite resin restorations provide strong evidence of clinical success and durability when using a total-etch adhesive technique.a. Short-termb. Long-termc. Nod. none of the above
49. _________ adhesives are still the gold standard for all-purpose bonding.a. Single-bottle self-etchb. Single-bottle etch-and-rinsec. Multiple-bottle self-etchd. Multiple-bottle etch-and-rinse
50. Based upon the current clinical evidence, self-etch adhesive systems can be used successfully for the restoration of _________ preparations.a. Class I and IIb. Class IIIc. Class Vd. all of the above
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
If not taking online, mail completed answer sheet to
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O. Box 116, Chesterland, OH 44026 or fax to: (440) 845-3447
For iMMEDiATE results, go to www.ineedce.com and click on the button “Take Tests Online.” Answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
Payment of $59.00 is enclosed. (Checks and credit cards are accepted.)
If paying by credit card, please complete the following: MC Visa AmEx Discover
Acct. Number: ______________________________
Exp. Date: _____________________
Charges on your statement will show up as PennWell
CEDADH911DE
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification of Participation forms will be mailed within two weeks after taking an examination.
PROVIDER INFORMATIONPennWell is an ADA CERP Recognized Provider. ADA CEROP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, not does it imply acceptance of credit hours by boards of dentistry.
Concerns or complaints about a CE Provider may be directed to the provider or to ADA CERP ar www.ada.org/cotocerp/
COURSE CREDITS/COSTAll participants scoring at least 70% on the examination will receive a verification form verifying 3 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 4527. The cost for courses ranges from $29.00 to $110.00.
RECORD KEEPINGPennWell maintains records of your successful completion of any exam for a minimum of six years. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
© 2011 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
Educational Objectives1. Describe the differences between etch-and-rinse and self-etch adhesives and relate these categories to other naming systems
2. Discuss the current research evidence comparing etch-and-rinse and self-etch adhesives
3. List and describe the indications for etch-and-rinse and self-etch adhesives
4. Describe the clinical procedure for an etch-and-rinse and a self-etch single-step adhesive
Course Evaluation1. Were the individual course objectives met? Objective #1: Yes No Objective #3: Yes No
Objective #2: Yes No Objective #4: Yes No
Please evaluate this course by responding to the following statements, using a scale of Excellent = 5 to Poor = 0.
2. To what extent were the course objectives accomplished overall? 5 4 3 2 1 0
3. Please rate your personal mastery of the course objectives. 5 4 3 2 1 0
4. How would you rate the objectives and educational methods? 5 4 3 2 1 0
5. How do you rate the author’s grasp of the topic? 5 4 3 2 1 0
6. Please rate the instructor’s effectiveness. 5 4 3 2 1 0
7. Was the overall administration of the course effective? 5 4 3 2 1 0
8. Please rate the usefulness and clinical applicability of this course. 5 4 3 2 1 0
9. Please rate the usefulness of the supplemental webliography. 5 4 3 2 1 0
10. Do you feel that the references were adequate? Yes No
11. Would you participate in a similar program on a different topic? Yes No
12. If any of the continuing education questions were unclear or ambiguous, please list them. ___________________________________________________________________
13. Was there any subject matter you found confusing? Please describe. ___________________________________________________________________ ___________________________________________________________________
14. How long did it take you to complete this course? ___________________________________________________________________ ___________________________________________________________________
15. What additional continuing dental education topics would you like to see? ___________________________________________________________________ ___________________________________________________________________
ANSWER SHEET
Dental Adhesives for Direct Placement Composite Restorations: An Update
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP: Country:
Telephone: Home ( ) Office ( ) Lic. Renewal Date:
Requirements for successful completion of the course and to obtain dental continuing education credits: 1) Read the entire course. 2) Complete all information above. 3) Complete answer sheets in either pen or pencil. 4) Mark only one answer for each question. 5) A score of 70% on this test will earn you 3 CE credits. 6) Complete the Course Evaluation below. 7) Make check payable to PennWell Corp. For Questions Call 216.398.7822
AGD Code 253
www.ineedce.com Customer Service 216.398.7822 16