dentin bonding: sem comparison of the dentin surface in ... · pdf filedentin bonding: sem...
TRANSCRIPT
Dentin bonding: SEM comparison of the dentinsurface in primary and permanent teethJacques E. N6r, DDS, MS Robert J. Feigal, DDS, PhDJoseph B. Dennison, DDS, MS Chris A. Edwards BS, MS
Abstract
The literature suggest differences between primary andpermanent teeth regarding the composition and morpholoogy of the dentin. The purpose of this study was to com-pare the effect of two dentin conditioners on the micromor-phology of the dentin surface of primary and permanentteeth. Human extracted and noncarious molars were di-vided into four groups and conditioned with either 10%phosphoric acid (All-Bond 2TM) or 10% maleic acid( Scotchbond Multi-PurposeTM ) for different time periods.SEM photomicrographs (1500x) were taken from the con-ditioned dentin and evaluated blindly by three calibratedexaminers. The results indicate that the smear layer wasremoved more easily from primary teeth than from perma-nent teeth (P = 0.0001), which suggests greater reactivityto acidic dentin conditioners. We also found that the longerthe time of application of dentin conditioner the more smearlayer is removed (P = 0.0094). In comparing primary andpermanent dentin, the results of this study indicate thatless time is required for appropriate acid conditioning ofprimary dentin surfaces. Such a differentiated protocol forbonding to primary tooth dentin results in surface mor-phological characteristics similar to those found in condi-tioned permanent teeth. (Pediatr Dent 19:246-52, 1997)
C linical indications for tooth-colored restorations
have increased with the evolution of adhesiveand composite resin systems. More conserva-
tive cavity preparations, as well as increased publicconcern about esthetics, are also strong motivations forusing composite resins. However, failures of these res-torations in primary teeth are still a common problemfor pediatric dentists. The bond strength of compositeresins to the dentin surface is lower in primary teeththan in permanent teeth,1,2 leading eventually to poorerperformance of this material when used for primarydentition restorations. Two studies with similar meth-odologies can be used to illustrate differences in adhe-sion to both dentin types. When AmalgambondTM wasused in permanent teeth, it presented bond strengthsof 23.3 + 5.7 MPa and All-BondTM 19.3 + 5.6 Mpa3, whilein primary teeth Amalgambond had bond strengths of12.6 + 7.5 MPa and All-Bond 11.6 + 6.6 Mpa.4
Comparison of the composition and morphology ofdentin in primary and permanent teeth indicates somedifferences. Neutron activation analysis was used tomeasure the mineral content of dentin, and lower con-centrations of calcium and phosphorus were measuredfor primary teeth than for permanent teeth, but thisdifference was not statistically significant. 5 When en-ergy dispersive spectroscopy was used, the concentra-tions of calcium and phosphorus were shown to bedecreased in both peritubular and intertubular dentinof primary teeth, compared with permanent teeth. 6 Ina microhardness study, the dentin from the central areaof the crowns of permanent teeth was shown to beharder than dentin from the same area of primaryteeth. 7 This finding suggested that permanent toothdentin is more mineralized than primary tooth dentin.The concentration is higher and the diameter of den-tin tubules is larger close to the pulpal surface (0.4-0.5mm) in permanent teeth than in primary teeth, lead-ing to decreased dentinal permeability in primaryteeth.8 Previous work from this laboratory9 has showndifferences in resin-dentin interdiffusion zone (hybridlayer) width between primary and permanent toothdentin after treatment with two different dentin bond-ing systems. It was shown that the same protocol fordentin bonding produces a hybrid layer in primaryteeth that is comparatively thicker than in permanentteeth. We believe that this finding might be due to dif-ferences in reactivity of primary tooth dentin to theacidic solutions used for conditioning the surface priorto the application of primers and adhesive resins (asrecommended by the manufacturer).
The effects of dentin surface treatment and conse-quent characteristics of the dentinal substrate used forbonding affect the performance of composite resin res-torations.1° However, all the parameters established forpreparation of an adequate dentin substrate for bond-ing have been studied in permanent teeth, and the re-sults merely extrapolated for primary teeth withouttaking into consideration compositional and morpho-logical differences that may exist between the two den-titions. The purpose of this SEM study, therefore, wasto evaluate the impact of dentin surface treatments on
246 American Academy of Pediatric Dentistry Pediatric Dentistry - 19:4, 1997
the micromorphology of the conditioned dentin of pri-mary and permanent teeth.
Methods and materials
Specimen preparationTen primary and 10 permanent noncarious, previ-
ously erupted molars were selected for this study. Theextracted teeth were stored in a solution of 0.2% sodiumazide in distilled water at 4°C. All teeth were usedwithin 6 months of extraction. Primary teeth in finalstage of rhizolysis (old primary teeth) were paired withold permanent teeth, and primary teeth that still pre-sented complete root structure (young primary teeth)were paired with recently erupted permanent teeth.This procedure was done to avoid eventual biasescaused by age changes normally manifested throughthe biological cycle of the dentin in both primary andpermanent teeth.
The crowns were divided from the roots using ahigh-speed diamond bur just apical to thecementoenamel junction, and the pulp tissue was re-moved using a stainless steel hand instrument. Labialsurfaces were used in order to have a homogeneousdepth of the dentin in relation to the pulp chamber. Thepreparation was done with a conical carbide bur # 7664in high speed with copious water spray, parallel to thelong axis of the tooth, exposing an area of superficialdentin within 1 mm of the dentinoenamel junction.11
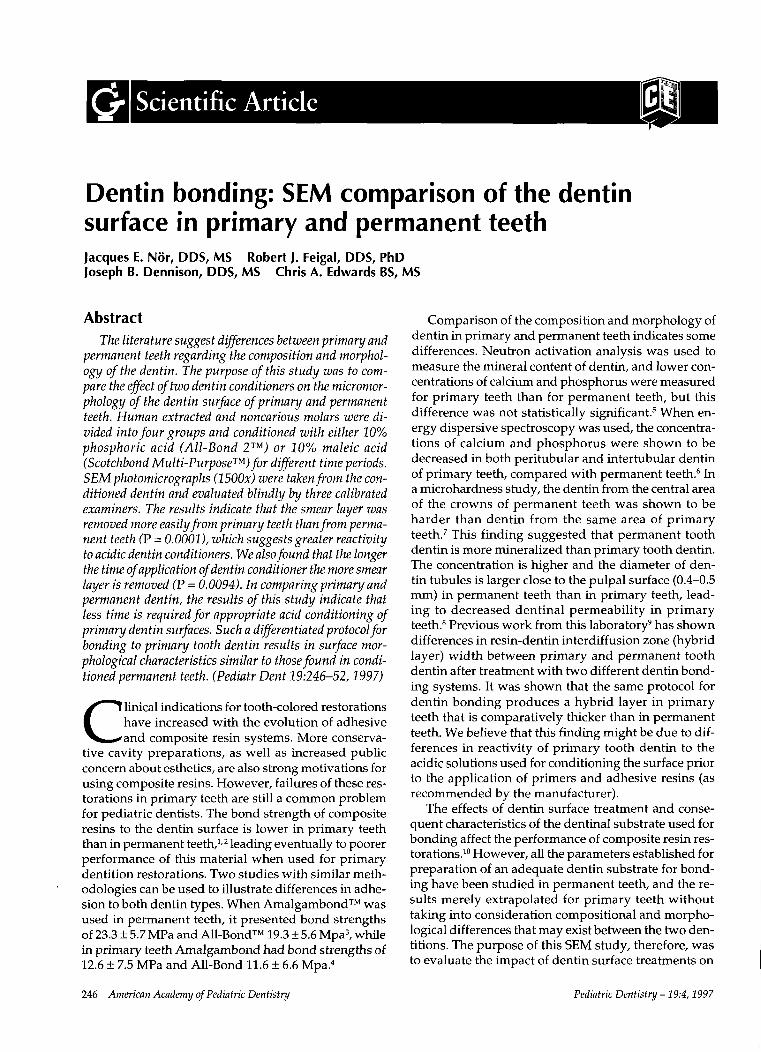
The dentin was then divided into four distinct zonesin order to obtain a separate area for each dentin con-ditioning time protocol (Fig 1).
Dentin conditioningHydrostatic intrapulpal pressure was used in all
samples to simulate the average tissue pressure ofhealthy pulps (about 25 mmHg).12 Each crown was
~ T|me2 :’ i :’ i:’i :’ !:’! i ! :" :" ! ii~i "~i iii T|m.O ~
/ /--x xFig 1. Schematic representation explaining themethodology used for evaluating the dentin surface. Allphotomicrographs were taken from the l-ram~ shadedareas at the center of the labial surface.
fixed to an acrylic platform penetrated in its center bya tube to connect the pulpal chamber to a pressure ap-paratus. Physiological intrapulpal pressure was repro-duced by filling the pulp chambers with distilled wa-ter and connecting the mounted teeth to a 34-cm-highand 1-cm-diameter column.13 All teeth were kept un-der positive hydrostatic intrapulpal pressure for 12 hrprior to dentin conditioning in order to establish anequilibrium between external (dentin surface) and in-ternal (pulp chamber) pressures and also to achieve homogeneous baseline pressure for all samples. Up tonine teeth were placed at each time on the intrapulpalpressure apparatus. These teeth were mounted in sucha way that primary and permanent teeth were alter-nated on the table, resulting in an equal distributionthrough the platform to avoid biases caused by minorpressure differences that might have occurred in dif-ferent locations on the table.
Intrapulpal pressure then was reduced to zero inorder to simulate effects of application of an anestheticwith vasoconstrictor (commonly used in clinical situa-tions). The dentin was conditioned after 15 min witheither 10% phosphoric acid gel (All-Bond 2TM, BiscoDental Products, Itasca, IL) or 10% maleic acid gel(Scotchbond Multi-PurposeTM, 3M Co, St Paul, MN) forfour different time periods: 0 sec (control), 7 sec (halfof the manufacturer’s recommended conditioningtime), 15 sec (recommended time), and 30 sec (twice recommended time). These four areas in the labial sur-face were assigned randomly to the different etchingtimes so that each tooth presented a different configu-ration in the relation of etching time to quadrant at thelabial surface.
The conditioning of the experimental areas wasdone in a standardized sequence: the first area to beetched was the one that received the longest etchingtime (30 sec). When the first area had 15 sec of etching,acid was applied to the second area (the one to receive15 sec total of acid etch). Finally, after 23 sec of etchingtime in the first area (and consequently, 8 sec in thesecond), the third area was conditioned for 7 sec. Thenall samples were rinsed with 180 cc of distilled waterfor 30 sec with a hypodermic syringe. By doing thissequence, all etching procedures were done at once,and consequently, all areas received the same amountof water irrigation, including the control sites (no acidetch). After irrigation, all teeth were air dried for 5 secand then stored in a desiccation cabinet (The Chemi-cal Rubber Co, Cleveland, OH) for 24 hr.
Microscopic evaluationAll samples were mounted in metal stubs and coated
with gold in a Sputter Coater TM, Model S 150B(Edwards Co, West Sussex, England), during twocycles of 45 sec each, as a preparation for SEM. Eachsample was then analyzed in a scanning electron mi-croscope (Model 1000B, Amray, Bedford, MA) with accelerating voltage of 8.0 Kv. All photomicrographs were
Pediatric Dentistry - 19:4, 1997 American Academy of Pediatric Dentistry 247
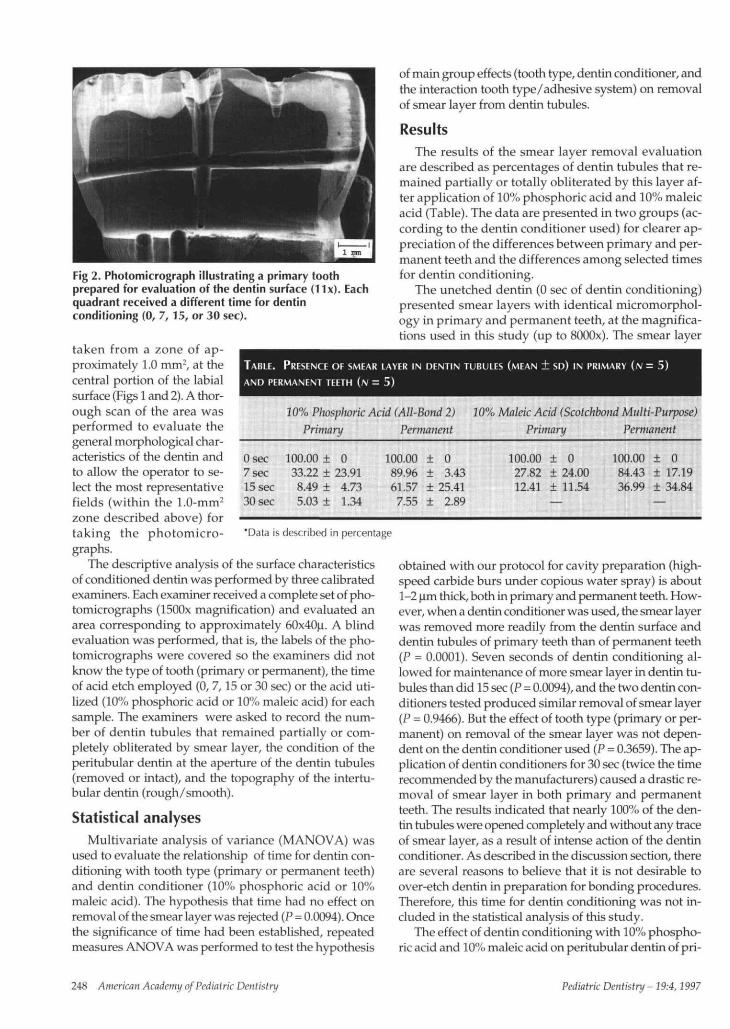
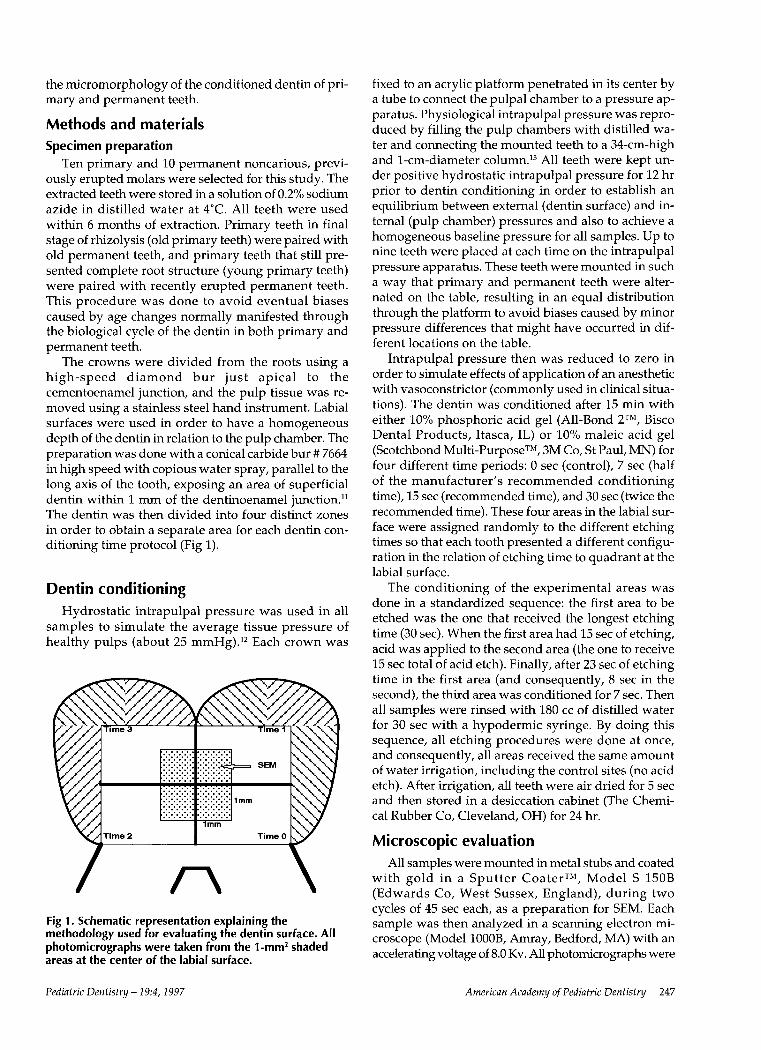
Fig 2. Photomicrograph illustrating a primary toothprepared for evaluation of the dentin surface (11x). Eachquadrant received a different time for dentinconditioning (0, 7,15, or 30 sec).
10% Phosphoric Add (All-Bond 2)Primary Permanent
'Data is described in percentage
taken from a zone of ap-proximately 1.0 mm2, at thecentral portion of the labialsurface (Figs 1 and 2). A thor-ough scan of the area wasperformed to evaluate thegeneral morphological char-acteristics of the dentin andto allow the operator to se-lect the most representativefields (within the 1.0-mm2
zone described above) fortaking the photomicro-graphs.
The descriptive analysis of the surface characteristicsof conditioned dentin was performed by three calibratedexaminers. Each examiner received a complete set of pho-tomicrographs (1500x magnification) and evaluated anarea corresponding to approximately 60x40|i. A blindevaluation was performed, that is, the labels of the pho-tomicrographs were covered so the examiners did notknow the type of tooth (primary or permanent), the timeof acid etch employed (0, 7,15 or 30 sec) or the acid uti-lized (10% phosphoric acid or 10% maleic acid) for eachsample. The examiners were asked to record the num-ber of dentin tubules that remained partially or com-pletely obliterated by smear layer, the condition of theperitubular dentin at the aperture of the dentin tubules(removed or intact), and the topography of the intertu-bular dentin (rough/smooth).
Statistical analysesMultivariate analysis of variance (MANOVA) was
used to evaluate the relationship of time for dentin con-ditioning with tooth type (primary or permanent teeth)and dentin conditioner (10% phosphoric acid or 10%maleic acid). The hypothesis that time had no effect onremoval of the smear layer was rejected (P = 0.0094). Oncethe significance of time had been established, repeatedmeasures ANOVA was performed to test the hypothesis
of main group effects (tooth type, dentin conditioner, andthe interaction tooth type/adhesive system) on removalof smear layer from dentin tubules.
ResultsThe results of the smear layer removal evaluation
are described as percentages of dentin tubules that re-mained partially or totally obliterated by this layer af-ter application of 10% phosphoric acid and 10% maleicacid (Table). The data are presented in two groups (ac-cording to the dentin conditioner used) for clearer ap-preciation of the differences between primary and per-manent teeth and the differences among selected timesfor dentin conditioning.
The unetched dentin (0 sec of dentin conditioning)presented smear layers with identical micromorphol-ogy in primary and permanent teeth, at the magnifica-tions used in this study (up to SOOOx). The smear layer
TABLE. PRESENCE OF SMEAR LAYER IN DENTIN TUBULES (MEAN ± SD) IN PRIMARY (N - 5)AND PERMANENT TEETH (N = 5)
10% Maleic Acid (Scotchbond Multi-Purpose)Primary Permanent
0 sec 100.00 ± 07 sec 33.22 + 23.9115 sec 8.49 + 4.7330 sec 5.03 + 1.34
100.00 ± 089.96 ± 3.4361.57 ± 25.41
7.55 ± 2.89
100.00 + 027.82 ± 24.0012.41 + 11.54
—
100.00 ± 084.43 ± 17.1936.99 ± 34.84
—
obtained with our protocol for cavity preparation (high-speed carbide burs under copious water spray) is about1-2 Lim thick, both in primary and permanent teeth. How-ever, when a dentin conditioner was used, the smear layerwas removed more readily from the dentin surface anddentin tubules of primary teeth than of permanent teeth(P = 0.0001). Seven seconds of dentin conditioning al-lowed for maintenance of more smear layer in dentin tu-bules than did 15 sec (P = 0.0094), and the two dentin con-ditioners tested produced similar removal of smear layer(P = 0.9466). But the effect of tooth type (primary or per-manent) on removal of the smear layer was not depen-dent on the dentin conditioner used (P = 0.3659). The ap-plication of dentin conditioners for 30 sec (twice the timerecommended by the manufacturers) caused a drastic re-moval of smear layer in both primary and permanentteeth. The results indicated that nearly 100% of the den-tin tubules were opened completely and without any traceof smear layer, as a result of intense action of the dentinconditioner. As described in the discussion section, thereare several reasons to believe that it is not desirable toover-etch dentin in preparation for bonding procedures.Therefore, this time for dentin conditioning was not in-cluded in the statistical analysis of this study.
The effect of dentin conditioning with 10% phospho-ric acid and 10% maleic acid on peritubular dentin of pri-
248 American Academy ofPediatric Dentistry Pediatric Dentistry - 19:4,1997
Permanent-10% maleic acid
Permanent-10% phosphoric acid
Primary-10% maleic acid
Primary-10% phosphoric acid
0 10 20 30 40 50 60 70 80 90 100
* Results are described in percentages.
Fig 3. Effect of the dentin conditioners on the peritubular dentin of primary (N = 10)and permanent teeth (/v= 10).
ing intertubular dentin topogra-phy.
DiscussionThis study was designed to
evaluate the morphologicalcharacteristics of the condi-tioned dentin used as a sub-strate for bonding compositeresin restorations to primaryand permanent teeth. The threeaspects evaluated were the re-sponsiveness of the smear layerto the use of acidic solutions fordentin conditioning, the mor-phology of peritubular dentin,and the topography of the inter-tubular dentin after acidic con-
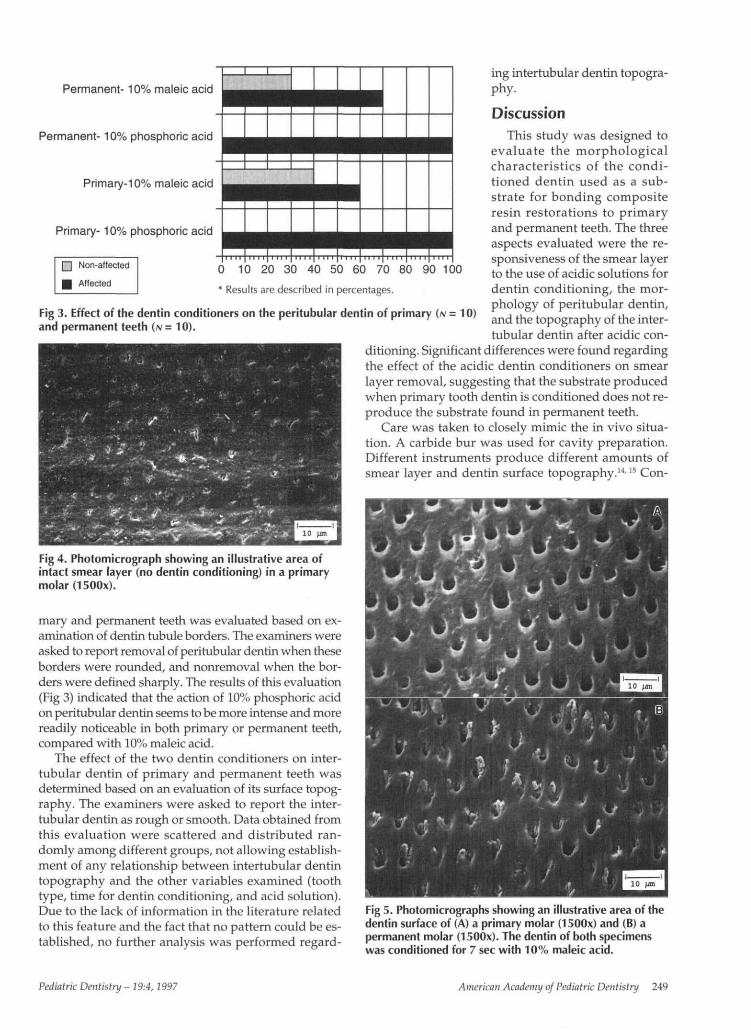
Fig 4. Photomicrograph showing an illustrative area ofintact smear layer (no dentin conditioning) in a primarymolar (1500x).
mary and permanent teeth was evaluated based on ex-amination of dentin tubule borders. The examiners wereasked to report removal of peritubular dentin when theseborders were rounded, and nonremoval when the bor-ders were defined sharply. The results of this evaluation(Fig 3) indicated that the action of 10% phosphoric acidon peritubular dentin seems to be more intense and morereadily noticeable in both primary or permanent teeth,compared with 10% maleic acid.
The effect of the two dentin conditioners on inter-tubular dentin of primary and permanent teeth wasdetermined based on an evaluation of its surface topog-raphy. The examiners were asked to report the inter-tubular dentin as rough or smooth. Data obtained fromthis evaluation were scattered and distributed ran-domly among different groups, not allowing establish-ment of any relationship between intertubular dentintopography and the other variables examined (toothtype, time for dentin conditioning, and acid solution).Due to the lack of information in the literature relatedto this feature and the fact that no pattern could be es-tablished, no further analysis was performed regard-
ditioning. Significant differences were found regardingthe effect of the acidic dentin conditioners on smearlayer removal, suggesting that the substrate producedwhen primary tooth dentin is conditioned does not re-produce the substrate found in permanent teeth.
Care was taken to closely mimic the in vivo situa-tion. A carbide bur was used for cavity preparation.Different instruments produce different amounts ofsmear layer and dentin surface topography.14'15 Con-
Fig 5. Photomicrographs showing an illustrative area of thedentin surface of (A) a primary molar (1500x) and (B) apermanent molar (1500x). The dentin of both specimenswas conditioned for 7 sec with 10% maleic acid.
Pediatric Dentistry - 19:4, 1997 American Academy of Pediatric Dentistry 249
sequently, attention should be given to this step in or-der to use an instrument for cavity preparation that hasclinical relevance, as it is in the case of carbide burs.
Another attempt to simulate the in vivo conditionwas the use of hydrostatic intrapulpal pressure.16'17 Thepresence of fluids under physiological pressure insidethe dentin tubules alters the pattern of demineraliza-tion caused by dentin conditioners by diluting the ac-ids and, consequently, decreases their action on re-moval of peritubular dentin. It may also influence theextension of the dentin that is etched on the lateral wallsof the dentin tubules and, consequently, the area avail-able for primer/adhesive resin diffusion among the col-lagen fibers resulting in the formation of a hybrid layer.So, the use of physiological intrapulpal pressure allowsfor a more reliable system to evaluate, in vitro, the ac-tion of dentin conditioners.
Every time tooth structure is cut, a smear layer is cre-ated (Fig 4).15 This layer of debris has important impli-cations for restorative procedures. It has the protectiveeffect of reducing the diffusion of elements from the re-storative material to the pulp18 and of limiting bacte-rial invasion.19 It also decreases the fluid flow withinthe dentin tubules after restorative procedures, a factthat may have a positive impact on reducing postop-erative sensitivity.20
On the other hand, the smear layer must be removed
from the intertubular dentin and the opening of the den-tin tubules to allow for the establishment of a hybrid layer,which ultimately is responsible for a strong and stableadhesion to dentin.21'24 The extent to which smear layeris ideally removed from permanent teeth is already es-tablished. Each manufacturer indicates a time for dentinconditioning that is determined specifically for its adhe-sive system, but the protocol for removing smear layerfrom primary teeth is yet to be established.
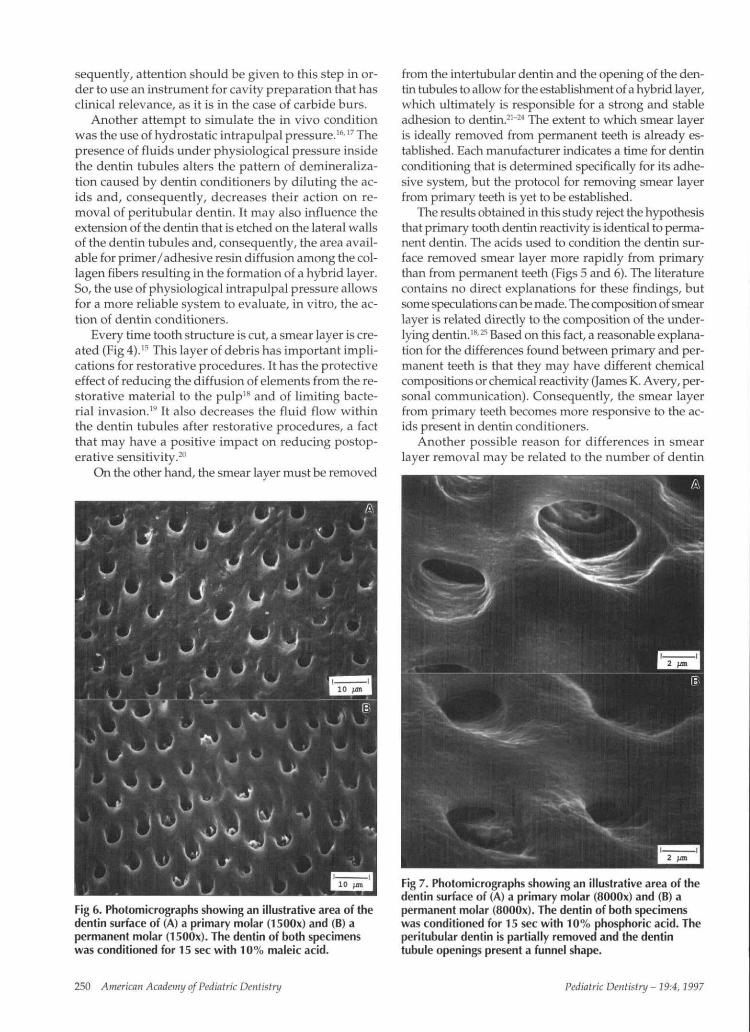
The results obtained in this study reject the hypothesisthat primary tooth dentin reactivity is identical to perma-nent dentin. The acids used to condition the dentin sur-face removed smear layer more rapidly from primarythan from permanent teeth (Figs 5 and 6). The literaturecontains no direct explanations for these findings, butsome speculations can be made. The composition of smearlayer is related directly to the composition of the under-lying dentin.'8'25 Based on this fact, a reasonable explana-tion for the differences found between primary and per-manent teeth is that they may have different chemicalcompositions or chemical reactivity (James K. Avery, per-sonal communication). Consequently, the smear layerfrom primary teeth becomes more responsive to the ac-ids present in dentin conditioners.
Another possible reason for differences in smearlayer removal may be related to the number of dentin
Fig 6. Photomicrographs showing an illustrative area of thedentin surface of (A) a primary molar (1500x) and (B) apermanent molar (1500x). The dentin of both specimenswas conditioned for 15 sec with 10% maleic acid.
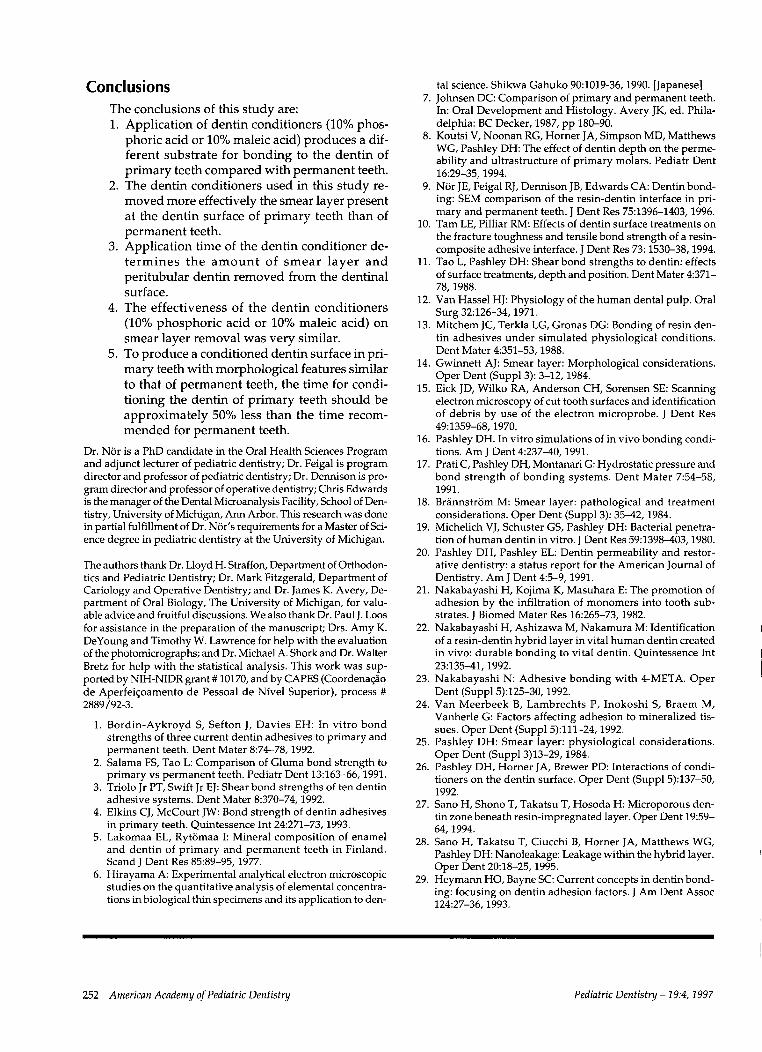
Fig 7. Photomicrographs showing an illustrative area of thedentin surface of (A) a primary molar (SOOOx) and (B) apermanent molar (SOOOx). The dentin of both specimenswas conditioned for 15 sec with 10% phosphoric acid. Theperitubular dentin is partially removed and the dentintubule openings present a funnel shape.
250 American Academy ofPediatric Dentistry Pediatric Dentistry - 19:4, 1997

Fig 8. Photomicrographs showing the depth of demineral-ization of the dentin and hybrid layer thickness in (A)permanent tooth (13000x) and in (B) primary tooth(13000x). The dentin was conditioned for 15 sec with10% maleic acid, and the Scotchbond Multi-Purpose/Z100 system™ was used in both teeth. AR = adhesiveresin; H = hybrid layer; D = dentin.
tubules present. The decreased dentin permeability ofprimary teeth is caused by smaller tubule concentra-tion and diameter.8 Thus, it can be hypothesized thatprimary teeth present less moisture on the dentin sur-face, thereby altering the effectiveness of the dentinconditioners on smear layer removal. Well-controlledstudies of the consequences of a differentiated concen-tration and diameter of dentin tubules and a compara-tive analysis of the dentin and smear layer constituentsin both dentitions may provide the necessary informa-tion for better understanding the mechanisms involvedin smear layer removal and the reasons for the signifi-cant differences found in this research.
When the removal of smear layer was analyzed un-der the perspective of the dentin conditioner used, both10% phosphoric acid and 10% maleic acid presentedvery similar results. The results also indicated that bothprimary and permanent teeth had their peritubulardentin affected by the use of these two dentin condi-tioners, even in short periods of time (7 sec). This ac-tion ultimately results in funnel-shaped openings of thedentin tubules at the surface level (Fig 7). The most no-ticeable feature regarding peritubular dentin removalobserved in our study was the fact that 10% phospho-ric acid seemed to have a more intense action onperitubular dentin than 10% maleic acid.
Another perspective of peritubular dentin removalwas observed by the authors during a previously re-ported evaluation of the resin-dentin interface in pri-mary and permanent teeth.9 The cross-sections ob-tained for that SEM study showed clear enlargementof the opening ends of the dentin tubules of both pri-mary and permanent teeth, compared with deeper ar-eas in the dentin (not affected by the acid). The extentof this effect seems to be related to the duration of thedentin conditioning step (i.e., the longer the acid isapplied to the dentin, the more significant is the re-
moval of peritubular dentin).It is clear that even short periods of dentin condition-
ing can potentially promote significant alterations inthe structure of the dentin. Acidic dentin conditioningshould be evaluated seriously since there are indica-tions that dentin conditioning should be effective butnot excessive. Conditioning the dentin is fundamentalto remove the smear layer, partially deminerali/e theintertubular dentin, and expose the collagen fibers toallow the establishment of a hybrid layer.26 However,when the depth of demineralization of the intertubu-lar dentin is excessive, the collagen fibers collapse andform a dense layer that may not be fully impregnatedby the primer and adhesive resin.17 In these circum-stances, the mineral matrix removed is not replacedfully by the primer, leaving a weaker area at the bot-tom of the hybrid layer, which potentially becomes apathway for microleakage27'28 or a site for bonding fail-ure.10
Removal of smear layer is related directly to the con-centration of acid and time of contact.29 Based on thefindings of this study, either shorter times for applica-tion of dentin conditioner or use of weaker concentra-tions should be considered for primary teeth. Thisstudy supports the concept that it is possible to controlthe amount of smear layer removed from the dentinsurface by controlling the application time of the den-tin conditioner. The clinical application of the knowl-edge generated by this work is that a shorter time forconditioning primary tooth dentin is indicated to pro-mote a removal of smear layer and surface morphol-ogy similar to that observed in conditioned permanenttooth dentin.
The authors have found that the hybrid layer createdat the resin-dentin interface of primary teeth is thickerthan the one observed in permanent teeth, as demon-strated in cross-sectional views of dentin used as sub-strate for bonding (Fig 8).9 We have also shown that aporosity can be seen at the bottom of the hybrid layerin primary teeth that were conditioned for 15 sec.9
These results, combined with the observations of ourstudy, offer a possible explanation for the problematicparadigm of bonding to primary tooth dentin. The useof the same protocol for bonding to primary and per-manent teeth may be the reason why primary teethconsistently exhibited lower values in shear bondstrength tests with dentin bonding systems.1-2 Estab-lishing a differentiated protocol for dentin condition-ing primary teeth creates a dentinal substrate that re-sembles more closely the one found in permanent teeth.The findings of this work show that time for condition-ing primary teeth dentin should be approximately 50%less than the time recommended for permanent tooth.However, well-designed clinical trials and reliableshear bond strength studies using the criteria estab-lished by Pashley16 for in vitro simulation of in vivoconditions should be performed before this techniquecan be considered clinically acceptable.
Pediatric Dentistry - 19:4,1997 American Academy of Pediatric Dentistry 251
ConclusionsThe conclusions of this study are:1. Application of dentin conditioners (10% phos-
phoric acid or 10% maleic acid) produces a dif-ferent substrate for bonding to the dentin ofprimary teeth compared with permanent teeth.
2. The dentin conditioners used in this study re-moved more effectively the smear layer presentat the dentin surface of primary teeth than ofpermanent teeth.
3. Application time of the dentin conditioner de-termines the amount of smear layer andperitubular dentin removed from the dentinalsurface.
4. The effectiveness of the dentin conditioners(10% phosphoric acid or 10% maleic acid) smear layer removal was very similar.
5. To produce a conditioned dentin surface in pri-mary teeth with morphological features similarto that of permanent teeth, the time for condi-tioning the dentin of primary teeth should beapproximately 50% less than the time recom-mended for permanent teeth.
Dr. N6r is a PhD candidate in the Oral Health Sciences Programand adjunct lecturer of pediatric dentistry; Dr. Feigal is programdirector and professor of pediatric dentistry; Dr. Dennison is pro-gram director and professor of operative dentistry; Chris Edwardsis the manager of the Dental Microanalysis Facility, School of Den-tistry, University of Michigan, Ann Arbor. This research was donein partial fulfillment of Dr. N6r’s requirements for a Master of Sci-ence degree in pediatric dentistry at the University of Michigan.
The authors thank Dr. Lloyd H. Straffon, Department of Orthodon-tics and Pediatric Dentistry; Dr. Mark Fitzgerald, Department ofCariology and Operative Dentistry; and Dr. James K. Avery, De-partment of Oral Biology, The University of Michigan, for valu-able advice and fruitful discussions. We also thank Dr. Paul J. Loosfor assistance in the preparation of the manuscript; Drs. Amy K.DeYoung and Timothy W. Lawrence for help with the evaluationof the photomicrographs; and Dr. Michael A. Shork and Dr. WalterBretz for help with the statistical analysis. This work was sup-ported by NIH-NIDR grant # 10170, and by CAPES (Coordena~aode Aperfei~oamento de Pessoal de Nivel Superior), process 2889/92-3.
1. Bordin-Aykroyd S, Sefton J, Davies EH: In vitro bondstrengths of three current dentin adhesives to primary andpermanent teeth. Dent Mater 8:74-78, 1992.
2. Salama FS, Tao L: Comparison of Gluma bond strength toprimary vs permanent teeth. Pediatr Dent 13:163-66, 1991.
3. Triolo Jr PT, Swift Jr EJ: Shear bond strengths of ten dentinadhesive systems. Dent Mater 8:370-74, 1992.
4. Elkins CJ, McCourt JW: Bond strength of dentin adhesivesin primary teeth. Quintessence Int 24:271-73, 1993.
5. Lakomaa EL, Ryt6maa h Mineral composition of enameland dentin of primary and permanent teeth in Finland.Scand J Dent Res 85:89-95, 1977.
6. Hirayama A: Experimental analytical electron microscopicstudies on the quantitative analysis of elemental concentra-tions in biological thin specimens and its application to den-
tal science. Shikwa Gahuko 90:1019-36, 1990. [Japanese]7. Johnsen DC: Comparison of primary and permanent teeth.
In: Oral Development and Histology. Avery JK, ed. Phila-delphia: BC Decker, 1987, pp 180-90.
8. Koutsi V, Noonan RG, Horner JA, Simpson MD, MatthewsWG, Pashley DH: The effect of dentin depth on the perme-ability and ultrastructure of primary molars. Pediatr Dent16:29-35, 1994.
9. N6r JE, Feigal RJ, Dennison JB, Edwards CA: Dentin bond-ing: SEM comparison of the resin-dentin interface in pri-mary and permanent teeth. J Dent Res 75:1396-1403, 1996.
10. Tam LE, Pilliar RM: Effects of dentin surface treatments onthe fracture toughness and tensile bond strength of a resin-composite adhesive interface. J Dent Res 73: 1530-38, 1994.
11. Tao L, Pashley DH: Shear bond strengths to dentin: effectsof surface treatments, depth and position. Dent Mater 4:371-78, 1988.
12. Van Hassel HJ: Physiology of the human dental pulp. OralSurg 32:126-34, 1971.
13. Mitchem JC, Terkla LG, Gronas DG: Bonding of resin den-tin adhesives under simulated physiological conditions.Dent Mater 4:351-53, 1988.
14. Gwinnett AJ: Smear layer: Morphological considerations.Oper Dent (Suppl 3): 3-12, 1984.
15. Eick JD, Wilko RA, Anderson CH, Sorensen SE: Scanningelectron microscopy of cut tooth surfaces and identificationof debris by use of the electron microprobe. J Dent Res49:1359-68, 1970.
16. Pashley DH. In vitro simulations of in vivo bonding condi-tions. Am J Dent 4:237-40, 1991.
17. Prati C, Pashley DH, Montanari G: Hydrostatic pressure andbond strength of bonding systems. Dent Mater 7:54-58,1991.
18. Br~innstr6m M: Smear layer: pathological and treatmentconsiderations. Oper Dent (Suppl 3): 35-42, 1984.
19. Michelich VJ, Schuster GS, Pashley DH: Bacterial penetra-tion of human dentin in vitro. J Dent Res 59:1398-403, 1980.
20. Pashley DH, Pashley EL: Dentin permeability and restor-ative dentistry: a status report for the American Journal ofDentistry. Am J Dent 4:5-9, 1991.
21. Nakabayashi H, Kojima K, Masuhara E: The promotion ofadhesion by the infiltration of monomers into tooth sub°strates. J Biomed Mater Res 16:265-73, 1982.
22. Nakabayashi H, Ashizawa M, Nakamura M: Identificationof a resin-dentin hybrid layer in vital human dentin createdin vivo: durable bonding to vital dentin. Quintessence Int23:135-41, 1992.
23. Nakabayashi N: Adhesive bonding with 4-META. OperDent (Suppl 5):125-30, 1992.
24. Van Meerbeek B, Lambrechts P, Inokoshi S, Braem M,Vanherle G: Factors affecting adhesion to mineralized tis-sues. Oper Dent (Suppl 5):111-24, 1992.
25. Pashley DH: Smear layer: physiological considerations.Oper Dent (Suppl 3)13-29, 1984.
26. Pashley DH, Horner JA, Brewer PD: Interactions of condi-tioners on the dentin surface. Oper Dent (Suppl 5):137-50,1992.
27. Sano H, Shono T, Takatsu T, Hosoda H: Microporous den-tin zone beneath resin-impregnated layer. Oper Dent 19:59-64, 1994.
28. Sano H, Takatsu T, Ciucchi B, Horner JA, Matthews WG,Pashley DH: Nanoleakage: Leakage within the hybrid layer.Oper Dent 20:18-25, 1995.
29. Heymann HO, Bayne SC: Current concepts in dentin bond-ing: focusing on dentin adhesion factors. J Am Dent Assoc124:27-36, 1993.
252 American Academy of Pediatric Dentistry Pediatric Dentistry - 19:4, 1997