denver medical examiner forensic pathology fellowship in 2008, the denver office of the medical...
TRANSCRIPT

DENVER MEDICAL
EXAMINER
2014 ANNUAL REPORT

2
DENVER OFFICE OF THE MEDICAL EXAMINER
2014 Statistical Data
VISION STATEMENT: To be the premier death investigation office in the State of Colorado. By providing outstanding forensic services, OME supports other City and regional agencies such as Denver Police, Denver District Attorney, State Public Defenders and public health departments in improving the overall health and safety of the citizens of Denver MISSION STATEMENT: To serve as a guardian of the health, safety, and overall welfare of the citizens of Denver.
PREFACE
Per Colorado statute the Coroner is an elected official. In Denver, the Chief Medical Examiner is appointed as the Coroner in the City and County of Denver. State law defines the parameters of what constitutes a Coroner’s case in Section 30-10-606, Colorado Revised Statutes. By the state Constitution, Denver is a combined City and County. The City and County charter states that the position of Coroner is to be an appointed position, appointed by the Board of the Department of Environmental Health. The duties of Coroner are entrusted to the Chief Medical Examiner. In 2011, the coroner statute was revised in an attempt to improve the coroner system and to address weaknesses and inconsistencies in death investigation across the state. The main provisions included a mandate that forensic autopsies be performed by forensic pathologists; a mandate that autopsies be performed in accordance to the National Association of Medical Examiners (NAME) autopsy standards; and a mandate that transfers jurisdiction back to the County where the incident causing death occurred. The statute was revised again in 2013, this time emphasizing the partnership of the coroner’s office with law enforcement, and expanding the list of circumstances where the coroner would determine the cause and manner of death of a decedent. The revision also gives the coroner more authority in determining when a body should be removed from a scene, and clarifies the authority of the coroner to collect suicide notes, prescription medications, and any other documents or evidence they deem necessary to determine the cause and manner of death, including electronic devices such as cell phones and computers. The new version of the statute also emphasizes the working relationships between the coroner’s office and other community agencies. The revision states that the coroner and public administrator have the right to take charge of safeguarding the property of the deceased against the estate when necessary, and that the coroner shall comply with requests for information from the Department of Public Health and Environment and the Department of Transportation. (C.R.S. 30-10-606 [2013] http://www.coloradocoroners.org/CRS.html )

3
Organizational chart-2014 Office of the Medical Examiner
James Caruso, MD Chief Medical Examiner
Michelle Weiss-Samaras, Operations Manager (retired 12/2014)
Steven Castro, Operations Manager (12/2014)
Jami Milsap, ASA IV
Galena Brown, ASA IV
Cecelia Albertson, ASA III
Don Bell Investigations Manager
Tracey Balbin, Investigator
Kayla Wallace, Investigator
Harris Neil, Investigator
Kerrie Cady, Investigator
Andrea Raffauf, Investigator
Chip Whitley, Investigator
Howard Daniel, Investigator
Karen Jazowski Autopsy Support Manager
Barbara Criter, Autopsy Tech
Robert Garner, Autopsy Tech
Esperanza Ortega, Autopsy Tech
On-Call Pool, Autopsy Techs
Glenda Slade, Transcriptionist
Dawn Holmes, MD Forensic Pathologist
Garth Warren, MD Forensic Pathologist
Meredith Lann MD Forensic Pathlologist
(7/2014)
4
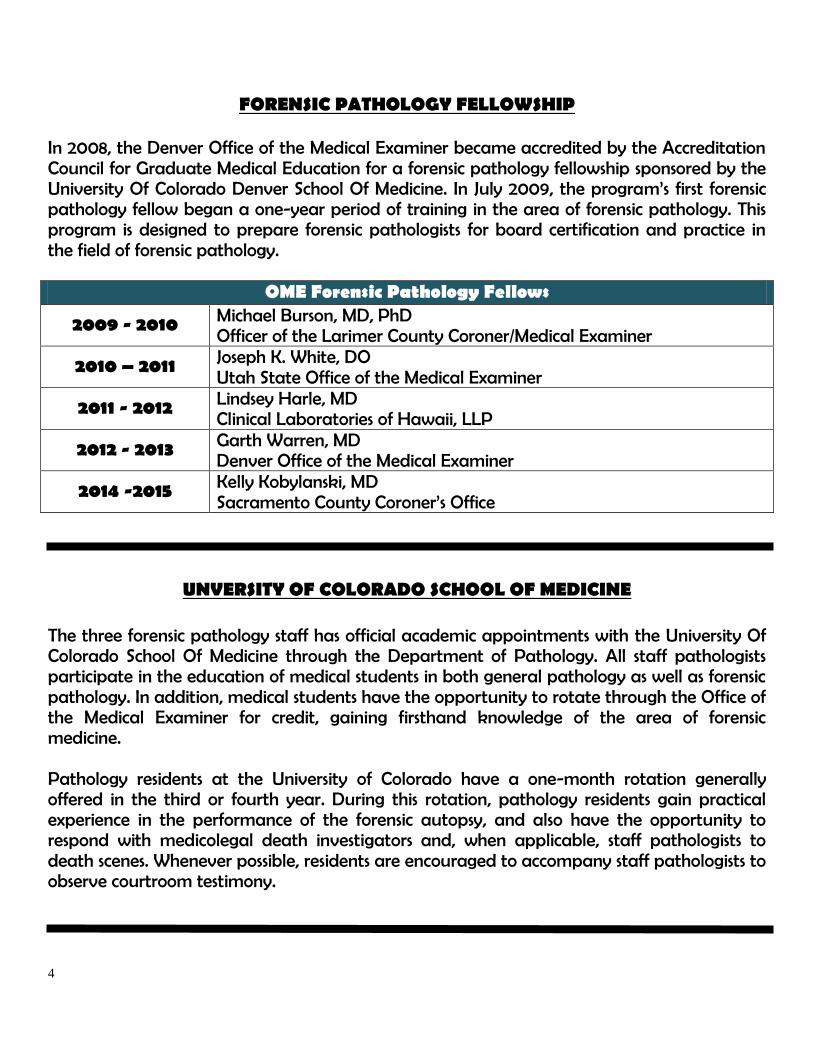
FORENSIC PATHOLOGY FELLOWSHIP
In 2008, the Denver Office of the Medical Examiner became accredited by the Accreditation Council for Graduate Medical Education for a forensic pathology fellowship sponsored by the University Of Colorado Denver School Of Medicine. In July 2009, the program’s first forensic pathology fellow began a one-year period of training in the area of forensic pathology. This program is designed to prepare forensic pathologists for board certification and practice in the field of forensic pathology. OME Forensic Pathology Fellows
2009 - 2010 Michael Burson, MD, PhD Officer of the Larimer County Coroner/Medical Examiner
2010 – 2011 Joseph K. White, DO Utah State Office of the Medical Examiner
2011 - 2012 Lindsey Harle, MD Clinical Laboratories of Hawaii, LLP
2012 - 2013 Garth Warren, MD Denver Office of the Medical Examiner
2014 -2015 Kelly Kobylanski, MD Sacramento County Coroner’s Office
UNVERSITY OF COLORADO SCHOOL OF MEDICINE
The three forensic pathology staff has official academic appointments with the University Of Colorado School Of Medicine through the Department of Pathology. All staff pathologists participate in the education of medical students in both general pathology as well as forensic pathology. In addition, medical students have the opportunity to rotate through the Office of the Medical Examiner for credit, gaining firsthand knowledge of the area of forensic medicine. Pathology residents at the University of Colorado have a one-month rotation generally offered in the third or fourth year. During this rotation, pathology residents gain practical experience in the performance of the forensic autopsy, and also have the opportunity to respond with medicolegal death investigators and, when applicable, staff pathologists to death scenes. Whenever possible, residents are encouraged to accompany staff pathologists to observe courtroom testimony.

5
INVESTIGATIVE INTERNSHIP PROGRAM
OME offers a one-year medicolegal investigative internship program with the following schools: University of Denver Graduate Program – Masters of Forensic Psychology, Metropolitan State University of Denver, and the University of Colorado, Denver Campus. Select individuals may opt, if accepted, to continue on for an additional year. Undergraduate seniors and graduate students compete to participate in a program designed to train forensic death investigators. During the internship year, interns are expected to carry their own case load that includes gathering of information for the determination of the cause and manner of death, assisting in identification of the decedent, investigating cause and manner of death, assist in the identification of the decedent, assist in locating and notifying next of kin, and proper documentation of a death scene. Upon successful completion, participants are eligible for certification as a medicolegal death investigator by the Colorado Coroner’s Association. The program also prepares participants for eventual ABMDI (American Board of Medicolegal Death Investigation) certification after hire in a coroner or medical examiner’s office
FORENSIC AUTOPSY TECHNICIAN INTERNSHIP PROGRAM
OME offers numerous Autopsy Technician internships with the following schools: University of Colorado Experiential Learning Center, Metropolitan State University of Denver, Regis University, Denver, and Wesleyan University in Nebraska, Masters in Forensic Science. With the exception of Wesleyan University, which offers a two-week rotation, participants are offered a one-semester internship. During this internship, participants work closely with staff pathologists and Autopsy Technicians in the autopsy room, and gain experience in clinicopathologic correlation, forensic photography, fingerprinting, and evidence collection. Many graduates from this internship go on to medical school; others continue on in an alternative field of medicine such as physical therapy, pathology assistant and other forensic sciences.
COMMUNITY EDUCATION
The Denver Office of the Medical Examiner participates in a wide variety of community education through affiliations with area universities, as well as community outreach activities throughout the Denver Metropolitan area with high schools and middle schools, medical providers, and other interested parties.

6
INVESTIGATIONS
The Investigations Section of the Denver Medical Examiner responds to the scenes of deaths throughout the City and County of Denver twenty-four hours a day, seven days a week. It is the responsibility of the Medicolegal Death Investigator to function as the eyes and ears of the Medical Examiner and insure that the State law is followed with respect to the reporting and handling of deaths in Denver City and County. In addition to scene response, investigators also investigate hospital, nursing homes, and other facility deaths that fall under the Coroner statute via phone reports. When they deem it necessary, they will respond to these scenes as well. Investigators are also responsible for coordinating and facilitating identification of the decedent; locating and notifying of the next of kin; and processing some of the evidence, medication, and effects of the decedent. Investigators respond to any death scene where the body has not been removed if the death occurs outside of a healthcare facility. Investigators may also respond to select hospital deaths; for example many homicides and child deaths where the individual has been transported to an emergency room. Investigators may also respond to a hospital or healthcare facility if the death appears due to non-natural circumstances (a suicidal hanging that occurs in a psychiatric unit). There can be a great deal of month-to-month fluctuation in the number of scenes, although overall the yearly total does not vary greatly, and generally averages between 65 and 75 scenes per month.
71 51 56 57 69 45 51 49 66 82 63 60
69 78 73 75 70
62 67 62 54 62
62 85
67 81 81 54 78
79 60 67 61
93 67
95
76 65 62 56
65 65 64 69 75
71
67
68
83 73 91
73
82
66 73 61 72
73
76
81
Jan Feb March April May June July Aug Sept Oct Nov Dec
Investigative Scene Visits 2010-2014
2010 2011 2012 2013 2014

7
In 2014, Denver OME investigators responded to 904 scenes in less than 30 minutes 68% of the time, between 30 minutes and 60 minutes 28% of the time, and only over 60 minutes 4% of the time.
In September of 2014, the investigative section began a new program in cooperation with local funeral homes. In cases where scene investigation did not indicate an apparent need for examination, investigators released the deceased directly to a funeral home from the scene. The case was then put on hold for review at OME, and as determined by the investigation and OME physicians, the decedent would either be brought in for examination or released from hold so the family could then make arrangements at a mortuary of their choice. In many cases this eliminated unnecessary transport of the decedent to the medical examiner, and expedited the process for families in making final arrangements.
< 30 mins 68%
30 - 60 mins 28%
> 60 mins 4%
Investigator Response Time

8
MASS FATALITY RESPONSE
In March 2006, the Denver Office of the Medical Examiner Manager of Investigations spearheaded the establishment of the North Central Region Mass Fatalities Committee. This multi-county group was formally accepted as a joint Denver Urban Area Initiative/ North Central Region committee. The committee has drafted a regional mass fatalities plan and meets monthly to further prepare for a mass fatalities incident. The investigative unit remains very active with this organization.
COHEART In September 2008, the Denver Office of the Medical Examiner established a reserve corps. This pool of volunteers was established to support operations in the event of a mass fatality incident. These volunteers receive periodic forensic training as well as experience in death scene investigations. In November 2009, an Urban Area Security Initiative grant was received in support of this program. The reserve corps became a North Central Region Mass Fatalities response asset. The reserve corps was renamed as the Colorado Human Remains Extraction and Recovery Team (COHEART). Volunteers are recruited from a myriad of sources. All volunteers are screened and have background checks. The volunteers must participate in training throughout the year, spend time with the investigators, and observe autopsies.
ORGAN/TISSUE/CORNEAL RECOVERY OME supports organ and tissue recovery whenever possible, and works closely with local procurement agencies such as Donor Alliance and the Rocky Mountain Lions Eye Bank to facilitate recovery activities in response to the large need for both organs and tissues on a local, as well as a national level. OME follows the Colorado Organ and Tissue Donation Coroner Protocol, which is an agreement signed by the Coroners and the District Attorney for each participating county along with Donor Alliance and the Rocky Mountain Lions Eye Bank. This protocol is designed to optimize organ and tissue recovery through cooperation and communication between all signed parties. Local coroners meet with representatives from the procurement agencies on a regular basis to review the protocol and update as needed.
Colorado Violent Death Reporting System The Denver Office of the Medical Examiner compiles data on all violent deaths in the county which is then used by the Centers for Disease Control and Prevention (CDC). This grant funded program housed at Colorado Department of Public Health and Environment (CDPHE) has provided a better understanding of the drivers and risk factors associated with violent deaths. Thirteen states including Colorado participate in the National Violent Death Reporting System (NVDRS). The data collection began with cases from January 2004 to date. More information on the program is available at www.cdc.gov/ncipc/dvp/dvp.htm

9
NAME ACCREDITATION
In 2000, the Denver Office of the Medical Examiner received accreditation by NAME for the
facility. Every five years the office has applied for accreditation and on December 10, 2010,
the office received its third accreditation. This accreditation recognized that the Denver
Office of the Medical Examiner had achieved consistent performance and competency in
medicolegal death investigation, and is in compliance with standards developed by NAME.
Only a handful of ME/Coroner offices in the country hold this accreditation.
NAME PERFORMANCE MEASURES
2014 Identification and Notification of Next of Kin within 24 hours (Target 90%)
Autopsy Reports completed within 60 days
All Reports Completed within 60 days (NAME target 90%)
All Reports completed within 90 days (NAME target 90%)
Bodies ready for release to mortuary within 48 hours (Target 90%)
Non-Autopsy cause and manner of death certificates provided within 10 days (Target >80%)
Success 87% 96% 97% 100% 91% 71%

10
ANNUAL STATISTICAL REPORT 2014 TOTAL DEATHS REPORTED (All jurisdictions) 4426
Medical Examiner Cases (Jurisdiction Retained) 1104
Waived Cases (Jurisdiction Waived) 1931
( Waived Natural Deaths ) 1807
( Waived Transferred Jurisdiction ) 118
( Waived – Declined/Other) 6 Inquiries (No jurisdiction determined) 1389
(Declined) 5
(Request for Assistance ) 17
(Natural) 1367
(Transferred Jurisdiction) 0
Manner of death (ME Cases)
Accident 324
Homicide 39
Suicide 107
Traffic Accidents 58 Undetermined 24
Request for assistance (non-human bones, skeletal remains, remnant, reported asystolic deaths, outside agency assist requested etc.) 1
Natural 551
Total scene visits by ME or ME Investigators 904
Bodies transported to office by order of DOME 793
External examinations 313
Complete autopsies 612
Partial autopsies 0 Outside autopsy for other jurisdiction 2
Chart Review 176
Hospital/private autopsies retained under the ME jurisdiction 0
Cases where toxicology is performed 614
Bodies unidentified after examination 0
Organ and tissue releases
Organs 15
Tissues 34
Total percent 98%
Unclaimed bodies (Coroner rotation burials) 16
Exhumations 0

11
Death investigations are classified in four main categories at DOME:
“ME” (Medical Examiner) cases o The Office of the Medical Examiner retains primary jurisdiction. There is an in-
depth investigation, and an Office of the Medical Examiner physician will certify the cause and manner of death.
“W” (Waived) cases o After initial investigation, some cases that are reportable by law may be
transferred to another county (if the event resulting in death occurred outside Denver), or may be released to a hospital or treating physician to certify the cause and manner of death.
“I” (Inquiry) cases o Care facilities often report deaths which do not fall into the area of a reportable
death. These cases are totally released after being documented. “OC” (Outside) cases
o Autopsies performed for other Colorado counties for a fee.
Case Number Comparisons 2009 - 2014
Medical examiner cases have averaged between 85 and 95 cases a month since 2009.
106 94 101 99 82 70 67 101 89 89 97 94
96 68
82 86 100 65 82
78 94 110 92 82
103
96 98 82 89
78 96
88 88 85 82 100
90
106 98
81 91
96 75
95 79 100
99 101
93
87 77 78
98
86 79
103 80
92 86 87
110
101 104
89
91
88 87
80 88
73 92 100
Jan Feb March April May June July Aug Sept Oct Nov Dec
2009-2014 ME Cases
2014 ME
2013 ME
2012 ME
2011 ME
2010 ME
2009 ME

12
The number of waived cases averaged 109 per month in 2009, between 130 and 135 a month from 2010 through 2013, and increased to an average 160 each month in 2014.
Documented inquiry cases have generally increased each year since 2009. The average number per month has gone up from 51 in 2009 to 116 in 2014. The highest number in the last six years was in 2013, with an average of 123 reported inquiries.
92 91 118 98 106 113 93 109 107 131 131 127
126 132 136
121 131 113 113 123 145 143 142 147
150 150 195
159 155 114
98 105
120 126 116 139
141 138
164
123 130 142
123 124
119 156 139
141
162 126
120
131 125 124
124 113
134
142 126
153
147 145
173
177 143 159
145 180
155
148 153
206
Jan Feb March April May June July Aug Sept Oct Nov Dec
2009-2014 W Cases
2009 W 2010 W 2011 W 2012 W 2013 W 2014 W
66 39 52 48 46 50 60 46 55 51 50 52
46 55 52 51 70 70 60
50 51 50 51 62
67 75 88 87 107 93 92 126 97
148 124 119
128 116 130 116
127 118 120 121 111
121 102
128
130 129
135 105
132 129 107 105
119
132 135
127
125 122
99
94
136
92 122 103 121
121 121
133
Jan Feb March April May June July Aug Sept Oct Nov Dec
2009-2014 I Cases
2009 I 2010 I 2011 I 2012 I 2013 I 2014 I

13
In cases where the Office of the Medical Examiner retains jurisdiction, one of three medical examinations will occur:
Autopsy – An examination of written documents including medical records, examination of the body externally, and opening the head, neck, chest, and abdomen at a minimum, removing and thoroughly examining the organs. A report is compiled, which is a public record in Colorado.
External examination – An examination of written documents, including medical records and an external examination of the body only (no internal intrusion). Blood/fluid or other samples are still preserved when possible.
Chart review – When a person dies of injuries that result in extensive medical treatment that is well documented, the body is not examined, but the cause of death is certified based upon review of medical records.
CAUSE OF DEATH refers to the disease or injury that sets into motion the chain of events that result in death. Causes could be from a medical condition such as coronary artery disease, or a traumatic event such as gunshot wound.
MANNER OF DEATH refers to how people die in general, if a non-natural action has a contribution to the death, it will determine the manner. There are five manners of death:
Homicide (death caused by the actions of another)
Suicide (death caused by intentional harm to self)
Accident (death caused by non-intentional injury)
Natural (death due to a natural disease process)
Undetermined (could not assign other manner due to unclear or unknown circumstances).
Request for Assistance (The Denver Office of the Medical Examiner also includes an additional sixth Manner of Death: “Request for Assistance,” which includes bones cases and other activities that do not fit neatly into the other manners.)

14
In medically examined cases, 2014 saw an increase in both traffic and non-traffic accidents compared to the previous 3 years. Homicides and suicides slightly decreased over the same time period.
Accident (nontraffic), 324
Homicide, 39
Suicide, 107 Traffic Accidents, 58
Undetermined, 24
Natural, 551
Request for Assistance, 1
2014 ME Cases by Manner of Death
Accident (nontraffic)
Homicide Suicide Traffic
Accidents Undetermined Natural
Request for Assistance
2012 304 42 109 40 40 585 1
2013 296 47 88 48 32 534 3
2011 321 49 91 50 50 521 5
2014 324 39 107 58 24 551 1
0
100
200
300
400
500
600
700
ME Cases by Manner of Death 2011 - 2014

15
2014 Medical Examiner Cases
NATURAL DEATHS
In 2014, there were 551 cases determined to be death by natural cause upon examination. In
65% of those cases, the decedent was white. Males between the ages of 61 to 70 had the
highest number of natural deaths, and the lowest number of natural deaths was among
females ages 11 to 20. Of the cases examined, males made up 70%. Cardiovascular disease
was the leading cause of death for all races and for both males and females.
143
188
27
39
52
2
39
39
4
3
8
1
2
3
0
0
1
0
Autopsies
External Examinations
Chart Reviews
Natural Deaths by Examination and Race
Other/Unidentified Race Native American Asian Hispanic Black White

16
3 1 3 0 4 6
16
6
46
17
113
31
120
49 52
23 26 24
4 7
Male Female
Natural Deaths by Age and Sex
0-10 years 11-20 years 21-30 years 31-40 years 41-50 years
51-60 years 61-70 years 71-80 years 81-90 years 91 + years
0 50 100 150 200 250 300
CARDIOVASCULAR
COMPLICATIONS OF ETOH
RESPIRATORY
INFECTIOUS DISEASE
NEOPLASTIC
METABOLIC/DIABETES
SIDS
OTHER
Natural Deaths by Category and Sex
Female
Male

17
White Black Hispanic Asian Native American Other
0-10 years 1 1 1 1 0 0
11-20 years 2 1 0 0 0 0
21-30 years 7 1 2 0 0 0
31-40 years 15 2 5 0 0 0
41-50 years 33 11 16 2 1 0
51-60 years 88 31 21 2 1 1
61-70 years 119 26 20 2 2 0
71-80 years 45 13 15 2 0 0
81-90 years 41 6 1 1 1 0
91 + years 7 1 1 2 0 0
0
20
40
60
80
100
120
140
Natural Death by Age and Race

18
UNDETERMINED MANNER OF DEATH
Undetermined manner is used to designate that a death does not fit the category of natural, suicide, homicide, or accident. This includes areas where the cause of death may have been found but the manner may not be clear. This can be due to a lack of background information, uncertainties in circumstances, or decomposition of the body related to a time delay in discovery. There are also cases where the cause of death itself cannot be determined, again possibly related to advanced decomposition of the body, the inability to obtain sufficient information for a variety of reasons, or the death may have been due to causes which leave no anatomic foot print such as certain types of heart disease (long QT syndrome e.g.), some seizure deaths, and some asphyxial deaths. In general, autopsies should be performed on cases where manner of death and cause of death are undetermined. However, in practice that is not always possible. Cases may come to the attention of OME after cremation has occurred, making autopsy impossible. In other instances, the cause of death is clear, but the determination of manner of death would not be aided by the performance of an autopsy due to insufficient investigative information in existence. This is especially true in instances where death occurs years or even decades after a traumatic injury. In these cases, an autopsy would not yield any information that would differentiate between manners of death.
3
5
11
2
2
0 0 0
0 0 1
0
Toxin Trauma Unknown/Other SUDI Autopsy 3 5 11 2 External Exam 2 0 0 0 Chart Review 0 0 1 0
Undetermined Manner by Cause of Death and Exam Type

19
2
1 1 1 1 1
2
1
6
2
1 1
2
0-10 years 11-20
years
21-30
years
31-40
years
41-50
years
51-60
years
61-70
years
71-80
years
81-90
years
91 + years
Undetermined by Age and Method
Toxin Trauma Unknown/Other SUDI
7
2 1
1
1
1
4
2
1
1
1
1
1
Male
Female
Undetermined by Age and Sex 91 + years 81-90 years 71-80 years 61-70 years 51-60 years 41-50 years 31-40 years 21-30 years 11-20 years 0-10 years
0-10 years
11-20
years
21-30
years
31-40
years
41-50
years
51-60
years
61-70
years
71-80
years
81-90
years
91 + years
Native American 0 0 0 0 0 0 0 0 0 0
Asian 0 0 0 0 0 0 0 0 0 0
Hispanic 2 0 0 3 0 0 0 0 0 0
Black 5 0 0 1 0 0 0 0 0 0
White 2 1 2 1 3 1 2 1 0 0
0 1 2 3 4 5 6 7 8 9
10
Undetermined by Age and Race

20
SUDDEN UNEXPECTED DEATHS IN INFANCY (SUDI)
The Office of the Medical Examiner certifies sleep associated deaths in infants as undetermined in manner rather than natural, following evolving practice changes in the field of forensic medicine recognizing the uncertainties and multi-factorial issues related to these deaths. In the past, these deaths might have been called "SIDS" or Sudden Infant Death Syndrome. More recent forensic literature uses the term "Sudden Unexplained Death in Infancy" or SUDI. Recognized risk factors include external factors that could contribute to asphyxia in these children, for example bed sharing with an adult and unsafe sleep surfaces. OME feels these deaths are best certified as undetermined in manner for these reasons. For this reason, most of these deaths are also certified as undetermined in cause. In 2014, there were two SUDI deaths reported to the Denver Medical Examiner; both were male, one Hispanic and one black; both were in the evening to overnight hours, and one death occurred in January, the other in October. One of the infants was 2 days old, the other was 4 months. From 2009 to 2014, only 23 infant deaths have been determined as SUDI, 12 males and 11 females. The greatest number occurred in babies over 3 months old, but less than 1 year.
2009 2010 2011 2012 2013 2014
Male 4 2 2 2 0 2
Female 5 3 1 1 1 0
SUDI by Sex 2009 - 2014
< 1 month 1 month 2 months 3 months > 3 mo < 1
yr > 1 year
2009 1 2 1 3 2 0
2010 0 1 1 0 2 1
2011 0 0 0 0 3 0
2012 1 0 1 1 0 0
2013 0 0 0 1 0 0
2014 1 0 0 0 1 0
SUDI by Age 2009 - 2014

21
4 2 1
2
2
1
3 1
3
1
1
1
1
2009 2010 2011 2012 2013 2014
SUDI by Race 2009-2014
All Other
Hispanic
Black
White
Jan
Mar
May
Jul
Sep
Nov
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
2014 1 0 0 0 0 0 0 0 0 1 0 0
2013 0 0 0 0 0 1 0 0 0 0 0 0
2012 0 0 0 1 0 1 0 0 0 0 1 0
2011 0 0 0 1 0 0 0 1 0 0 0 1
2010 0 1 0 0 0 0 1 0 0 2 1 0
2009 1 1 1 0 2 1 0 0 0 1 1 1
SUDI by Months of the Year 2009-2014
0
2
4
6
8
10
2009 2010 2011 2012 2013 2014
SUDI by Time of Day 2009-2014
morning (8:01 am-12:14pm) afternoon (12:15 pm-6:00 pm)
evening (6:01 pm-8:00 am)
The 23 SUDI deaths from 2009-2014 were pretty evenly distributed among Hispanic, black, and white infants.
There was no great differentiation by month of the year, but a great difference in time of day, with evening/overnight hours being the most prevalent time for SUDI deaths to occur.
70% of SUDI deaths occurred between the hours of 6:00 pm and 8:00 am from 2009 to 2014.

22
HOMICIDES
Homicides have markedly declined in Denver over the last 10 years, with the number of homicides down by nearly one-third over that time.
OME almost universally performs autopsies on victims of homicide. Rarely, there is a significant delay between injury and the death, and all investigative and legal activities have been exhausted by the time the death occurs. In these situations, the pathologist reviewing the case may opt to perform a more limited examination. Occasionally, a homicide is made known to OME after the remains have been cremated, sometimes several years later. In cases such as these, the pathologist may only be able to review available medical records.
60 60 56 55
48
41
49 42
47
39
200
5
200
6
200
7
200
8
200
9
2010
2011
2012
2013
2014
Homicide Trends 2005-2014
Autopsies External Examinations
Chart Review
31
0 1
7
0 0
2014 Homicide Examinations
Male Female

23
Female Male TOTAL Race:
Asian 0 1 1 Black 1 12 13 Hispanic 1 10 11 American Indian 0 1 1
White 5 8 13 Other 0 0 0 TOTAL 7 32 39
Asian 0%
Black 14%
Hispanic 14%
American Indian
0%
White 72% Other
0%
Female Homicides by Race
Asian 3%
Black 38%
Hispanic 31%
American Indian
3%
White 25%
Other 0%
Male Homicides by Race

24
1 1 2
1
4 4
0
4
3
4
1
1
2
2
3
1
2
1
1
1
0-10 years 11-20 years
21-30 years
31-40 years
41-50 years
51-60 years
61-70 years
70+ years
Homicides by Age and Race
White Black Hispanic Asian Native American
Male
Female
0
1
2
1
8
1
7
1
7
2
7
0
1
1
0
0
Homicides by Age and Sex
70 + years
61-70 years
51-60 years
41-50 years
31-40 years
21-30 years
11-20 years
0-10 years

25
0
1 1
2 2
0
1
6
4 4
5
4
5
4 S
un
da
y
Mo
nd
ay
Tu
esd
ay
We
dn
esd
ay
Th
urs
da
y
Fri
da
y
Sa
turd
ay
Homicides by day of the week
Female
Male
0 0
3 4
11
2
8
11
12:01 AM - 6:00 AM 6:01 AM - NOON 12:01 PM - 6:00 PM 6:01 PM - MIDNIGHT
Homicides by Time of Day
Female Male
7
3
3
1
5
9
3
5
2
1
Alley
Other's Residence
Outdoors/Public Area
Parking Lot
Residence
Retail Business
Roadway/Street
Unknown
Vacant Building
Homicides by Setting
Male Female

26
Drug and alcohol testing is performed on all homicide deaths where feasible e.g. where death occurs shortly after the injury was inflicted and/or in hospitalized individuals when adequate antemortem blood samples can be obtained: These samples are not always available and so in some cases testing is not possible. In 2014, 34 out of 39 cases were tested. While drug or alcohol use is not usually the cause of death in a homicide, it can contribute to the manner of death (homicide) if it causes an individual to act irrationally. One example could be if a person is under the influence of a substance and causes an argument or fight that ultimately leads them to being killed by another. This is why, in part, a forensic pathologist and/or other investigator will take into consideration the level of substances in a victim’s blood.
4
9
2 2 1
2 3
4 4
1 2
Male Female
Drug/Alcohol Tested Homicides by Sex
Alcohol with Other Drugs Alcohol Only
Amphetamine/Methamphetamine Cocaine/Metabolites
Morphine/Heroin Multiple Drugs
No Drugs/Alcohol Other
THC
2
1 1
6
1
3
1 1 1 1
2 2
1
3
2
3
1
2
White Black Hispanic Asian Native American
Drug/Alcohol Tested Homicides by Race
Alcohol with Other Drugs Alcohol Only
Amphetamine/Methamphetamine Cocaine/Metabolites
Morphine/Heroin Multiple Drugs
No Drugs/Alcohol Other
THC

27
In over half of the tested cases, alcohol was not present. In cases that tested positive for alcohol, 6 homicide victims had alcohol levels higher than 0.2% With a BAC level between .06 and .09% an individual can have dulled feeling, become disinhibited, have impaired reasoning, depth perception, and peripheral vision. With a BAC over 0.2% an individual can be in a stupor, have loss of understanding, and possibly lose consciousness. (http://en.wikipedia.org/wiki/Blood_alcohol_content)
Blood Alcohol SEX RACE Male Female White Black Hispanic Asian Native American TOTAL Not Done/Negative
15 4 5 8 6 0 0 19
Less than 0.050% 0 1 1 0 0 0 0 1 0.051% - 0.1% 3 0 1 1 1 0 0 3 0.101% - 0.150% 2 0 0 1 1 0 0 2 0.151% - 0.2% 2 1 1 0 1 1 0 3 0.201% - 0.25% 2 0 1 0 0 0 1 2 0.251% - 0.3% 3 0 1 1 1 0 0 3 0.301% - 0.350% 1 0 1 0 0 0 0 1 > 0.351% 0 0 0 0 0 0 0 0 TOTAL 28 6 11 11 10 1 1 34
15
0 3 2 2 2 3
0
4
0 1
BAC levels by Sex (Homicides)
Male Female
0
2
4
6
8
10
12
White Black Hispanic Asian Native American
BAC levels by Race (Homicides)
Not Done/Negative Less than 0.050% 0.051% - 0.1%
0.101% - 0.150% 0.151% - 0.2% 0.201% - 0.25%
0.251% - 0.3% 0.301% - 0.350% > 0.351%
28
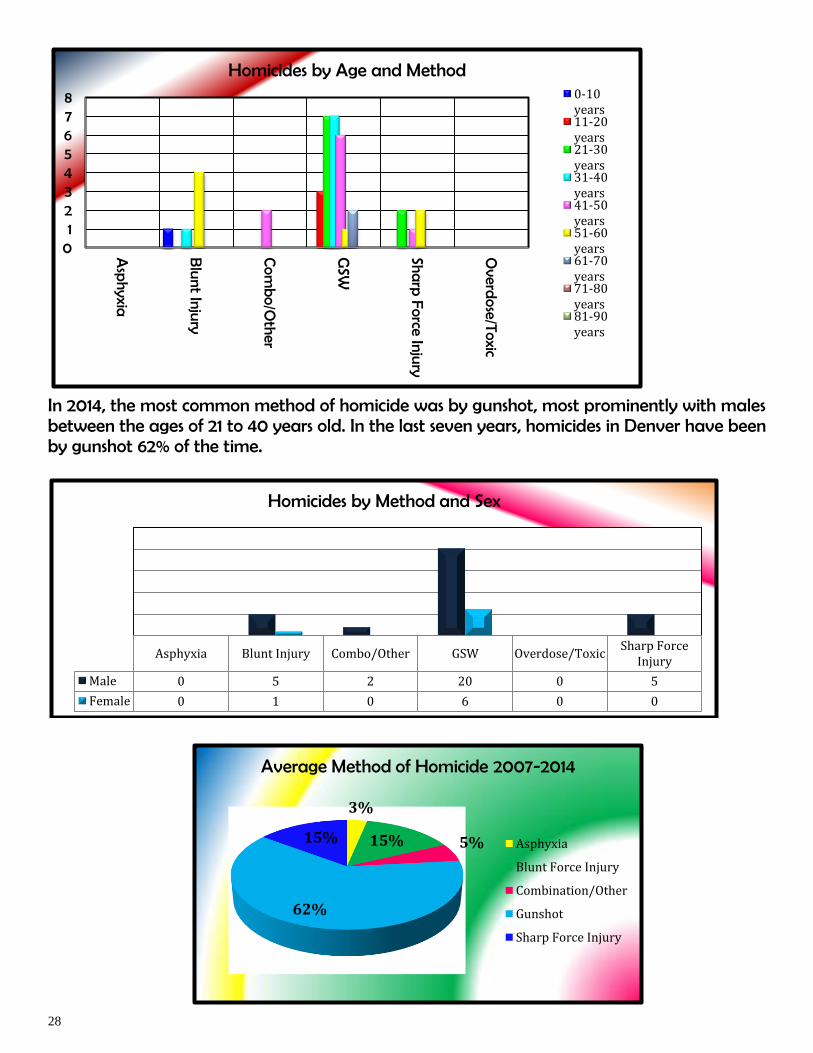
In 2014, the most common method of homicide was by gunshot, most prominently with males between the ages of 21 to 40 years old. In the last seven years, homicides in Denver have been by gunshot 62% of the time.
0 1 2 3 4 5 6 7 8
Asp
hyxia
Blu
nt Injury
Com
bo/O
ther
GSW
Sharp
Force Injury
Overd
ose/Toxic
Homicides by Age and Method 0-10 years 11-20 years 21-30 years 31-40 years 41-50 years 51-60 years 61-70 years 71-80 years 81-90 years
Asphyxia Blunt Injury Combo/Other GSW Overdose/Toxic Sharp Force
Injury
Male 0 5 2 20 0 5
Female 0 1 0 6 0 0
Homicides by Method and Sex
3%
15% 5%
62%
15%
Average Method of Homicide 2007-2014
Asphyxia
Blunt Force Injury
Combination/Other
Gunshot
Sharp Force Injury

29
3
8
4
4 1 1
2
6
2
2
3
3
Number of 2014 Homicides by Zip Code
80014
80204
80205
80207
80210
80211
80216
80219
80220
80223
80239
Unknown
30
SUICIDES
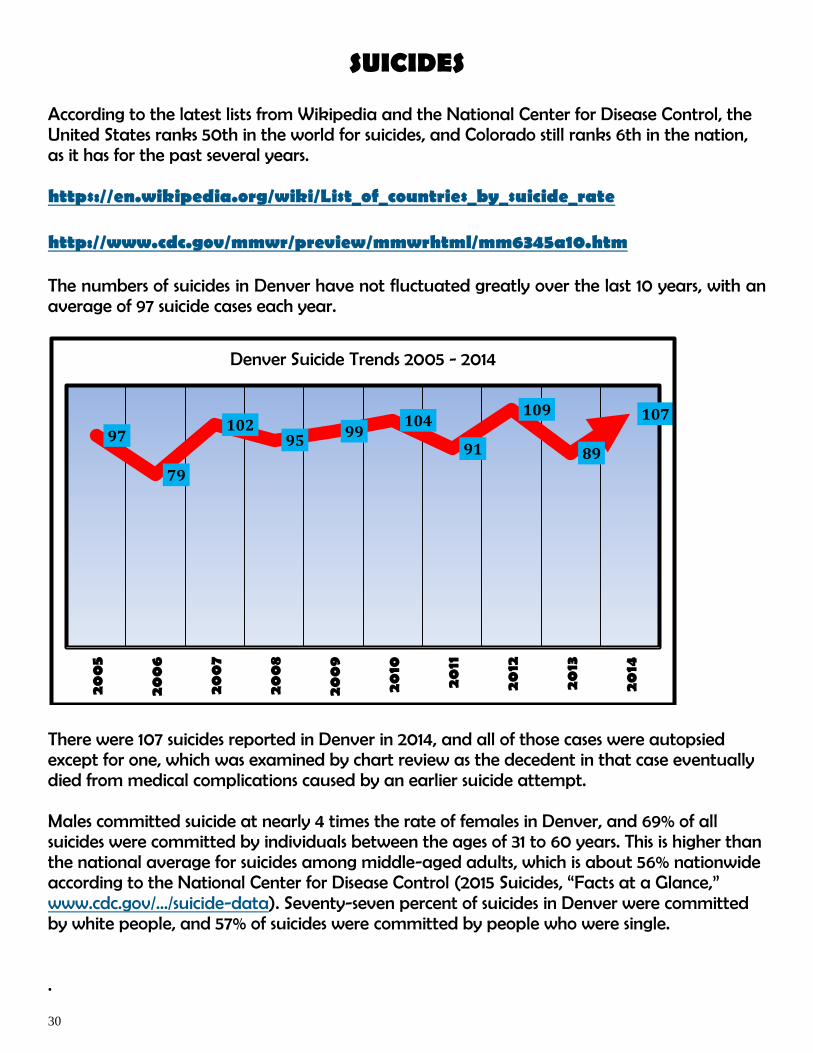
According to the latest lists from Wikipedia and the National Center for Disease Control, the United States ranks 50th in the world for suicides, and Colorado still ranks 6th in the nation, as it has for the past several years. https://en.wikipedia.org/wiki/List_of_countries_by_suicide_rate http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6345a10.htm The numbers of suicides in Denver have not fluctuated greatly over the last 10 years, with an average of 97 suicide cases each year.
There were 107 suicides reported in Denver in 2014, and all of those cases were autopsied except for one, which was examined by chart review as the decedent in that case eventually died from medical complications caused by an earlier suicide attempt. Males committed suicide at nearly 4 times the rate of females in Denver, and 69% of all suicides were committed by individuals between the ages of 31 to 60 years. This is higher than the national average for suicides among middle-aged adults, which is about 56% nationwide according to the National Center for Disease Control (2015 Suicides, “Facts at a Glance,” www.cdc.gov/.../suicide-data). Seventy-seven percent of suicides in Denver were committed by white people, and 57% of suicides were committed by people who were single. .
97
79
102 95
99 104
91
109
89
107
200
5
200
6
200
7
200
8
200
9
2010
2011
2012
2013
2014
Denver Suicide Trends 2005 - 2014

31
0
5
10
15
20
25
30
0-10 years
11-20 years
21-30 years
31-40 years
41-50 years
51-60 years
61-70 years
71-80 years
81-90 years
91 + years
Suicides by Race and Age
White Black Hispanic Asian Native American Other
0
5
9
16
26
18
6
2
3
0
1
4
4
2
8
0
2
1
0-10 years
11-20 years
21-30 years
31-40 years
41-50 years
51-60 years
61-70 years
71-80 years
81-90 years
91 + years
Suicides by Age and Sex
Female
Male
32
Div
orced
Married
Single
Un
determ
ined
Wid
ow
ed
0 5
10 15 20 25 30 35 40 45 50
Female
Male
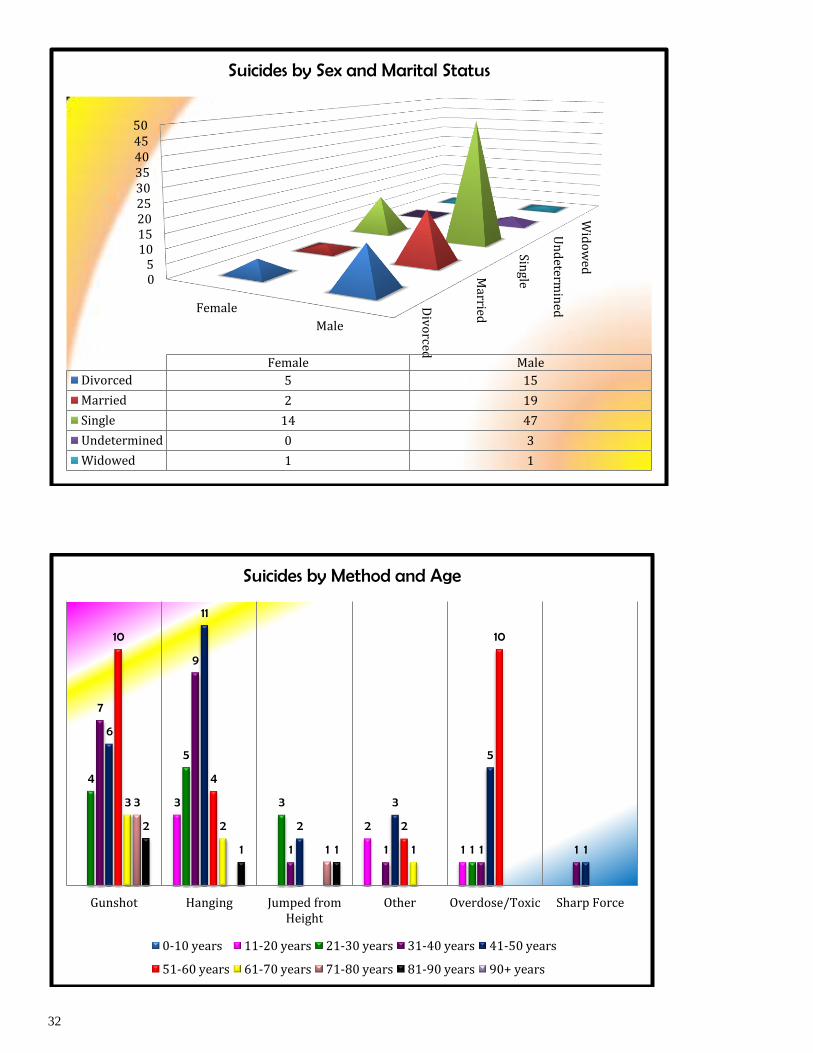
Female Male
Divorced 5 15
Married 2 19
Single 14 47
Undetermined 0 3
Widowed 1 1
Suicides by Sex and Marital Status
3
2
1
4
5
3
1
7
9
1 1 1 1
6
11
2
3
5
1
10
4
2
10
3
2
1
3
1
2
1 1
Gunshot Hanging Jumped from Height
Other Overdose/Toxic Sharp Force
Suicides by Method and Age
0-10 years 11-20 years 21-30 years 31-40 years 41-50 years
51-60 years 61-70 years 71-80 years 81-90 years 90+ years

33
In 2014, suicides were committed equally by gunshot and hanging. Over the past five years, those two methods have been used the most, with gunshot being the more prevalent. Overdose is the third method of suicide most used. Beginning in 2009, the Denver Medical Examiner began more aggressively tracking risk factors for suicide in order to identify any trends. The purpose of tracking suicide trends is to expand understanding and knowledge, hopefully pointing to prevention measures. Below shows the risk factors noted in Denver suicides. Most people exhibit more than one risk factor, and suicide usually involves a combination of these factors.
Gunshot Hanging Jumped from
Height Other Overdose/Toxic Sharp Force
2010 32 39 5 6 21 1
2011 31 32 8 0 18 2
2012 38 28 12 2 26 3
2013 32 18 9 2 27 0
2014 35 35 8 9 18 2
Suicides by Method 2010 - 2014
Alcohol Abuse
8%
Drug Problems 4% Family Member/Close
Friend Died 2%
Financial Problems 9%
Friend Attempted Suicide
1% Illness of Another
1% Illness of Self 6%
Legal/Disciplinary Problems
4%
Loss of Loved One 3%
Loss of Significant
Relationship 9% Marital
Problems 6%
Other/Mental Health Issues 2%
Previous Threats/Attempts
10% Prior Suicide in Family
0%
Recent Period of Despondency
12%
Recent Period of Rage 3%
Relationship Problems
9%
Suicide Note Left 11%
Unknown/Other Reason
2% Suicides by Risk Factors

34
The date and time of death of a decedent reflects when the person was found/pronounced. Usually in suicide cases the victim is found/pronounced sometime after they actually committed the act of suicide.
0 8 10 4
8
25 28 24
12:01 AM - 6:00 AM 6:01 AM - NOON 12:01 PM - 6:00 PM 6:01 PM - MIDNIGHT
Time of Day Suicide Victim Found/Pronounced
Female Male
6 5
2 2
3 2 2
15 15
12 11
16
6 10
Day of Week Suicide Victim Found/Pronounced
Female Male
9
11
6 5 5
8
6 6
9
7 6
7
1 0
2 2 2 2 1
2
5
3 2
0
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Month of the Year Suicide Victim Found/Pronounced
Male Female
35
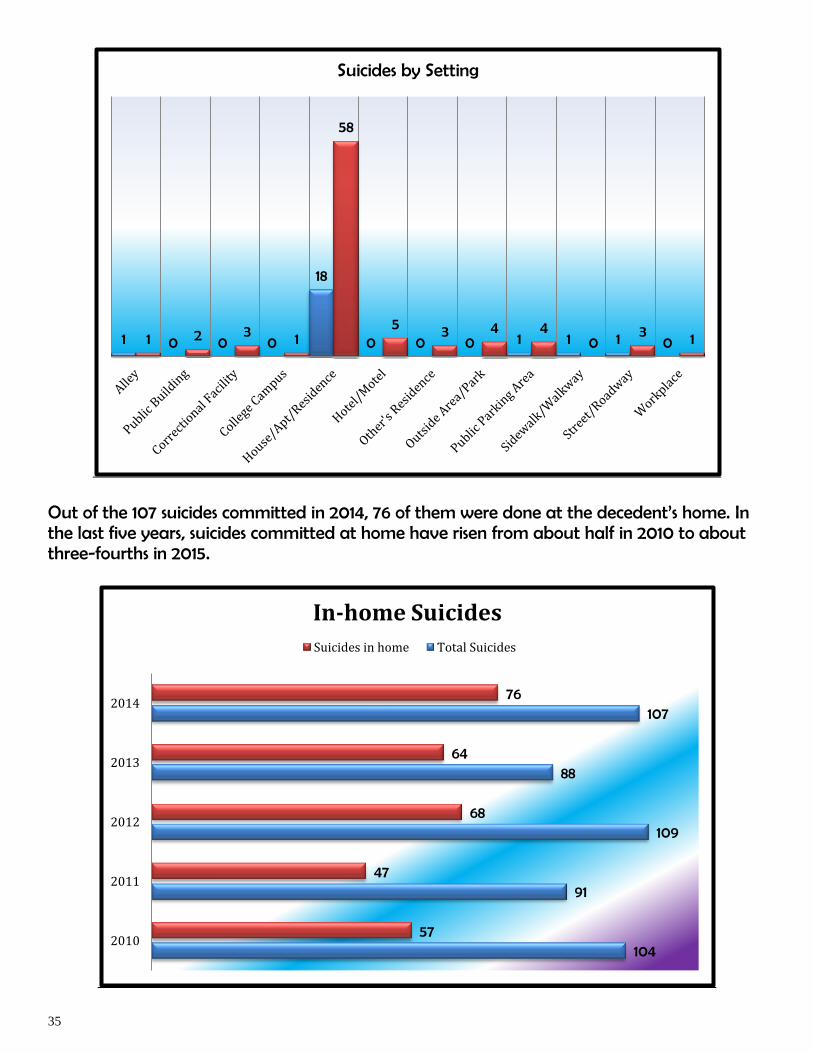
Out of the 107 suicides committed in 2014, 76 of them were done at the decedent’s home. In the last five years, suicides committed at home have risen from about half in 2010 to about three-fourths in 2015.
1 0 0 0
18
0 0 0 1 1 1 0 1 2 3 1
58
5 3 4 4 0
3 1
Suicides by Setting
104
91
109
88
107
57
47
68
64
76
2010
2011
2012
2013
2014
In-home Suicides
Suicides in home Total Suicides

36
DRUG RELATED DEATHS
In 2008, OME partnered with the Denver Office of Drug Strategy to gather data on drug-related fatalities in Denver from 2003 to present. The compilation of data is part of a bigger work group, which brings representatives from law enforcement, OME, DODS, Denver Police Crime Laboratory, Rocky Mountain Poison and Drug Center, Denver Health and Hospitals, and several drug abuse treatment providers. This workgroup will continue to examine drug use/abuse trends and determine effectiveness of treatment and prevention efforts. Drug deaths include not only accidental deaths related to recreational abuse of drugs, but also other accidental toxic effects, suicidal overdoses, and deaths with undetermined manner.
2005 2006 2007 2008 2009 2010 2011 2012 2013 Cocaine 82 85 75 60 53 41 58 50 15 Morphine 60 64 43 48 26 18 55 69 51 Alcohol 44 65 66 75 72 52 58 26 58 Codeine 36 36 18 19 11 3 18 20 15 Heroin 18 17 18 27 49 35 40 7 7 Methadone 17 16 14 15 15 11 19 11 11 Oxycodone 12 7 38 33 48 24 35 37 40 Methamphetamine 12 9 12 15 10 14 24 34 35 Acetaminophen 11 2 14 13 4 8 5 7 4 Diazepam 10 11 19 16 23 19 19 24 16 Alprazolam 10 5 13 15 20 12 18 14 11 Hydrocodone 7 10 8 22 18 10 19 16 5 Diphenhydramine 7 1 11 11 3 9 5 12 13 Clonazepam 2 0 1 4 8 7 8 8 7 Fentanyl 3 3 5 5 13 5 5 7 8 Decedents* 170 169 189 212 207 152 223 205 201 *Drug totals won't sum to decedents because more than one drug may be found in individual's toxicology
0
10
20
30
40
50
60
70
80
90
Drugs contributing to cause of death 2005-2014
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014

37
In 2014, there were 201 decedent deaths that were suicides, accidents, or were undetermined in which drugs were contributing factors. The drugs most often found in toxicology results on these cases were pain medications. Alcohol was the next most common drug found.
8%
46%
9%
11%
1%
4%
21%
Percentage of drugs by type contributing to death - 2014
Antidepressant
Pain Medication (Analgesic/Opioid)
Stimulant
Tranquilizer (Benzodiazepines)
Histamine
Anesthetic (Cocaine)
Alcohol
17
44
83
24
47
8
32
34
5
23
11
14
5
11
10
Cocaine
Morphine
Alcohol
Codeine
Heroin
Methadone
Oxycodone
Methamphetamine
Acetaminophen
Diazepam
Alprazolam
Hydrocodone
Diphenhydramine
Clonazepam
Fentanyl
Drugs contributing to cause of death 2014

38
NON-TRAFFIC ACCIDENTS
An accidental death that is not related to a traffic accident includes asphyxia (choking), drowning, falls, fire, overdose of drugs, death by another toxic substance, death in another type of motorized vehicle (airplane, motor boat, dirt bike, etc.), and “other” causes of accident that have no specific category (such as being trampled by a herd of cattle.)
9 22 2
137
14 5 11 1
112
1 6 4
Asphyxia/drowning Falls Fire/burn Overdose/toxic Other
Non-traffic accident examinations
Autopsies External Examination Chart Review
0-10 years
11-20
years
21-30
years
31-40
years
41-50
years
51-60
years
61-70
years
71-80
years
81-90
years
91 + years
Asphyxia/drowning 3 0 1 0 1 4 1 0 0 0
Falls 0 1 1 2 3 10 12 15 58 36
Fire/burn 0 0 0 0 1 2 0 0 0 0
Overdose/toxic 1 1 28 28 36 42 13 4 1 0
Other 1 0 1 3 5 3 2 1 0 3
0
10
20
30
40
50
60
70
Non-Traffic Accidents by Category and Age

39
Falling was the number one non-traffic accident fatality for people over 80 years old in 2014, more so for females than males. Overdose was the number one fatality for people between the ages of 21 and 60, this time with males more than females.
Male Female
10 0
59
79
1 2
94
60
12 7
Non-Traffic Accidents by Category and Sex
Asphyxia/drowning
Falls
Fire
Overdose/toxic
Other
0-10 years
11-20 years
21-30 years
31-40 years
41-50 years
51-60 years
61-70 years
71-80 years
81-90 years
91 + years
Other 1 0 0 1 1 0 0 0 0 0
White 3 0 21 22 26 37 16 12 53 36
Native American 0 0 0 0 2 0 0 0 0 0
Hispanic 1 1 7 6 15 17 8 4 4 0
Black 0 1 3 4 2 7 3 2 0 1
Asian 0 0 0 0 0 0 1 1 3 2
0 10 20 30 40 50 60 70
Non-Traffic Accidents by Race and Age
5 2
19
12
23
10
31
15
39
22
14
14
9
11
22
37
12
27
Male
Female
Non-traffic accidents by Sex and Age
91 + years 81-90 years 71-80 years 61-70 years 51-60 years
41-50 years 31-40 years 21-30 years 11-20 years 0-10 years

40
Single males and widowed females had the highest numbers, respectively, of non-traffic accidents. Fifty-eight percent of all non-traffic accident fatalities happened in the home.
Non-Traffic Accidents by Setting
Male Female TOTAL Alley 5 1 6 Assisted Living/Nursing Home 9 27 36 Business 9 3 12 Health Care Facility/Hospital 2 3 5 Hotel/Motel 11 4 15 Motor Vehicle 2 0 2 Other's Residence 4 6 10 Outside Area/Park 6 2 8 Public Parking Area 4 0 4 Public Transportation Vehicle/Station 1 0 1 Residence 93 94 187 River/Lake/Creek 2 0 2 Shelter/Temporary Housing 0 1 1 Sidewalk/Street/Roadway 7 1 8 Unknown 21 6 27 TOTAL 176 148 324
Divorced Married Single Unknown Widowed
28 43 79 4
22
26 34 28 2
58
Non-Traffic Accidents by Marital Status
Male Female

41
TRAFFIC ACCIDENTS
Traffic fatalities in Denver had a 3-year decline in numbers, but in 2014 the number of traffic deaths increased again. Out of 58 traffic fatality cases in 2014, 39 autopsies were performed, 3 external examinations, and 16 cases were determined by chart review.
2008 2009 2010 2011 2012 2013 2014 # of fatalities 63 46 54 50 42 48 58
Traffic Fatalities 2008 - 2014
30
3
10 9
6
Autopsy External Examination Chart Review
Traffic Accidents by Examination
Male
Female

42
The majority of 2014 traffic accidents happened in the afternoon/evening, and on weekends. Eight of the fatalities were from traffic accidents that had taken place prior to 2014, where the victims lived with their injuries for a time, but eventually died as a result of them.
AM, 15, 26%
PM, 33, 57%
UNKNOWN, 10, 17%
Traffic Accidents by Time of Day
Sun
day
, 13
Mo
nd
ay, 4
Tu
esd
ay, 5
Wed
nes
day
, 6
Th
urs
day
, 5
Fri
day
, 6
Satu
rday
, 11
Un
kn
ow
n/R
emo
te, 8
Traffic Accidents by Day of the Week

43
In Denver, white males between the ages of 41 to 50 had the most traffic fatalities.
1
0
6
1
7
2
3
1
10
0
5
4
6
4 4
1 1
2
Male Female
Traffic Accidents by Sex and Age
0-10 years 11-20 years 21-30 years 31-40 years 41-50 years
51-60 years 61-70 years 71-80 years 81-90 years
0 5 10 15 20 25 30
Asian
Black
Hispanic
White
Native American
Other
Asian Black Hispanic White Native
American Other
Female 1 0 3 10 1 0 Male 2 2 10 28 1 0
Traffic Accidents by Sex and Race

44
Pedestrians being struck by vehicles and at-fault driving was the two leading causes of traffic deaths in 2014. Motorcycle accidents were third. Since 2007, an average of 17 pedestrians per year are struck and killed by vehicles in Denver.
19 19
12 11
20 20
17 17
2007 2008 2009 2010 2011 2012 2013 2014
Pedestrians struck by vehicles 2007-2014
2
10
0
3 4
13
3
8
2
4
2
4 3
Driver - Victim Vehicle
Driver - At Fault
Vehicle
Passenger - Victim Vehicle
Passenger - At Fault Vehicle
Bicycle Pedestrian Unknown Motorcycle
Traffic Accidents - Decedent Position
Male Female

45
Out of the 58 traffic accident-related fatalities, 39 of the decedents were tested for both drugs and alcohol. In Colorado, there are two levels of alcohol-related driving offenses, both based on the measurement of blood alcohol concentration (BAC) in the body. A DUI (Driving Under the Influence of Alcohol or Drugs) can be charged if the driver is over 21 years old and their BAC is 0.08% or above: Under 21 years the legal BAC level is 0.02%. A DWAI (Driving While Ability is Impaired) can be charged if the driver’s BAC level is 0.05% or above. Although marijuana has been legalized in Colorado, just as with alcohol, driving while impaired by any drug is illegal. Colorado law specifies that drivers with five nanograms of active tetrahydrocannabinol (THC) in their whole blood can be prosecuted for driving under the influence of drugs (DUID). However, no matter the level of THC, law enforcement officers base arrests on observed impairment. (Source: www.dmv.org/co)
AT FAULT DRIVERS Blood alcohol/drugs Totals No toxicology ordered 3 Negative 5 BAC range 0 - 0.214% 7 THC 0 % BAC at or above 0.08% 43% Total At-Fault Drivers 14
MOTORCYCLE Blood alcohol/drugs Totals No toxicology ordered 4 Negative (drugs only) 4 Negative (ETOH) 2 BAC range 0 - 0.260% 3 THC 0 % BAC at or above 0.08% 2 Total Motorcycle Accidents 8
PEDESTRIANS Blood alcohol/drugs Totals No toxicology ordered 4 Negative 9 BAC range 0 - 0.440% 11 Alcohol and/or THC 7 Benzodiazepines, Opiates,
Cocaine/cocaine metabolites 2
Total Pedestrian – Traffic Accidents 17

46
13 18
3 3 3 2 1 6 7
0 1 1 0
Not
don
e/N
ot a
vaila
ble
Neg
ati
ve
Less
tha
n 0
.050
%
0.0
51 -
0.10
0%
0.10
1 - 0
.20
0%
0.2
01 -
0.2
50%
0.2
51 -
0.3
00
%
0.3
01 -
0.3
50%
> 0
.351
%
Blood Alcohol Levels by Sex
Male Female
Asian Native
American Black Hispanic White
Not done/Not available 0 1 0 1 17 Negative 3 1 0 5 16 Less than 0.050% 0 0 0 1 2 0.051 - 0.100% 0 0 0 0 0 0.101 - 0.200% 0 0 0 4 0 0.201 - 0.250% 0 0 1 1 1 0.251 - 0.300% 0 0 1 0 1 0.301 - 0.350% 0 0 0 1 0 > 0.351% 0 0 0 0 1
Blood Alcohol Levels by Race

47
13
3
8
0
4 5
1 3
1 1
Not Done/Available Negative THC and/or Alcohol Benzodiazepines Multiple Drugs
Detected Drugs by Sex
Male Female
Not Done/Available
Negative THC and/or
Alcohol Benzodiazepines Multiple Drugs
White 17 0 1 0 0 Black 0 0 0 3 1 Hispanic 4 2 5 0 0 Asian 1 0 0 0 0 Native American 3 0 2 0 0
Detected Drugs by Race

48
Denver has a diverse cultural composition, and continues to grow in population;
Growth is comprised of a spectrum of racial and ethnic groups represented.
The Denver Office of the Medical Examiner feels it is particularly important to be
sensitive to others and respects, and appreciates all cultures and religious beliefs.
If an autopsy is required, the office strives to adhere to as many cultural and
religious beliefs as possible, though the office must complete its statutory duty
and determine the cause and manner of death.
The office continually strives to help the friends and families understand the
duties of the office and the need for our involvement in the investigation of the
death of their loved one. Contact with clergymen is encouraged, when
appropriate, and attempts are made to locate a professional that is bilingual
when needed.