deprescribing benzodiazepine receptor agonists (bzras
TRANSCRIPT
Deprescribing benzodiazepine receptor agonists (BZRAs): evidence and practical considerations from a BZRA deprescribing guideline Wade Thompson, HBSc, BScPharm, RPh, MSc student University of Ottawa, School of Epidemiology, Public Health and Preventive Medicine Bruyère Research Institute OPEN Deprescribing Guidelines for the Elderly Project Ottawa, ON
Support provided by — • Government of Ontario • School of Pharmacy, University of Waterloo
Department of Family Medicine, McMaster University
The views expressed in this presentation are those of the presenter and do not necessarily reflect those of the Government of Ontario.
Funding/Disclaimer
Learning Objectives 1. Describe development of a BZRA deprescribing
guideline 2. Explain rationale for deprescribing BZRAs 3. Determine when a BZRA deprescribing approach is
appropriate for individual patients 4. Apply the BZRA deprescribing guideline in practice
and understand practical points
Outline • Why consider deprescribing a BZRA? • What are the benefits and risks of deprescribing
BZRAs? • When is it appropriate to deprescribe BZRAs? • How should BZRAs be deprescribed? • How to monitor patients after a BZRA is
deprescribed?
Deprescribing: background • Inappropriate medication use and polypharmacy
– Associated with nonadherence, adverse events, hospitalizations
• Older persons – Age-related changes in drug metabolism, distribution
and excretion – Increased sensitivity to CNS-active drugs – More comorbidities
Am J Geriatr Pharmacother 2007;5(4):345-51. Br J Clin Pharmacol 2005;61(2):218-23. Drugs Aging 2009;26(12):1039-48. Clin Geriatr Med 2012;28: 273–286.
Deprescribing • Tapering, stopping, discontinuing or withdrawing
drugs
• Considers evidence along with patient specific factors: – Comorbidities and function – Quality of life – Patient preference and goals
Where is this coming from? • Ontario Pharmacy Research Collaboration’s (OPEN)
Deprescribing Guidelines for the Elderly • Development and implementation of 3 deprescribing
guidelines – Led by Drs. Barbara Farrell and James Conklin – 2nd guideline is for benzodiazepine receptor agonists
(BZRAs), chosen as a priority drug class by an expert panel
Ancient Greece
https://divabetic.wordpress.com/2014/06/30/diabetes-time-machine-ancient-greece/ http://dominicus.malleotus.free.fr/rhodes/lang_en/site_asclepieion.htm Sleep Med Clin 2011;6:1–14
http://pubs.acs.org/cen/coverstory/83/8325/8325librium.html
http://www.cvs.com/drug/ http://popspiracy.blogspot.ca/2009/07/1980s.html
Evidence-Based Clinical Practice Guideline for Deprescribing Benzodiazepine Receptor Agonists
for Insomnia
Dr. Kevin Pottie, MD (lead)Dr. Barbara Farrell, PharmDDr. Anne Holbrook, MDDr. Simon Davies, MDDr. Cynthia Boyd, MDDr. Cheryl Sadowski, PharmDDr. Robert Swenson, MDDr. Jean Grenier, PhDDr. Vivian Welch, PhDWade Thompson, BScPharm
Andy Ma, BScPharmElli Polemiti, MScSonia Hussain, BSc
Guideline Development Team
GRADE Framework Question
Gather evidence
Assess quality and strength of evidence
Synthesize evidence
Consider patient values, preferences, resource implications
Recommendations
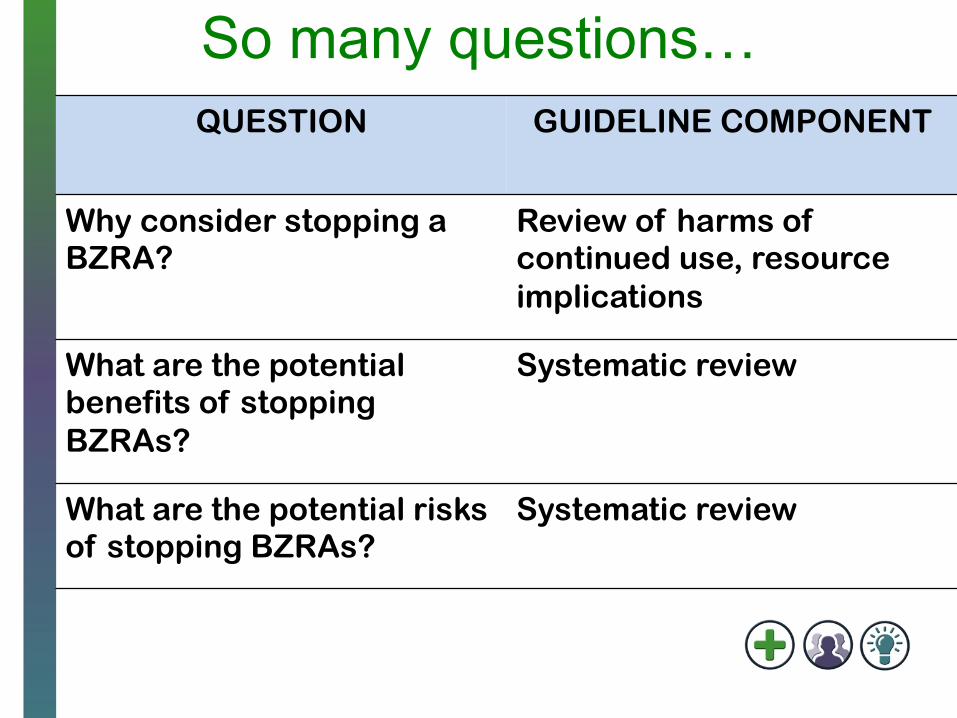
So many questions… QUESTION GUIDELINE COMPONENT
Why consider stopping a BZRA?
Review of harms of continued use, resource implications
What are the potential benefits of stopping BZRAs?
Systematic review
What are the potential risks of stopping BZRAs?
Systematic review
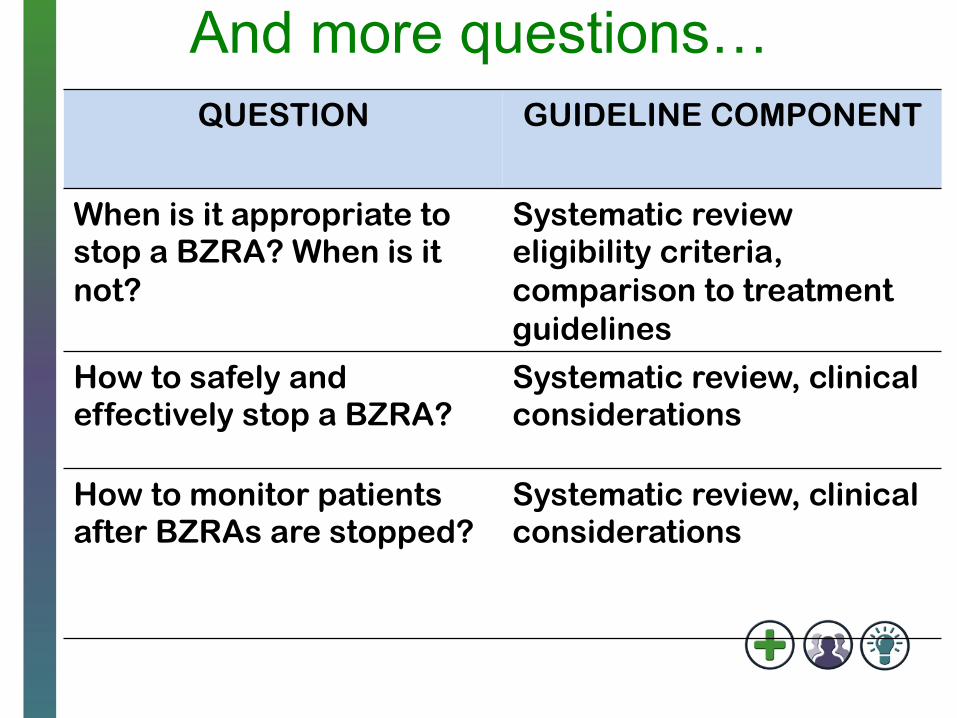
And more questions… QUESTION GUIDELINE COMPONENT
When is it appropriate to stop a BZRA? When is it not?
Systematic review eligibility criteria, comparison to treatment guidelines
How to safely and effectively stop a BZRA?
Systematic review, clinical considerations
How to monitor patients after BZRAs are stopped?
Systematic review, clinical considerations
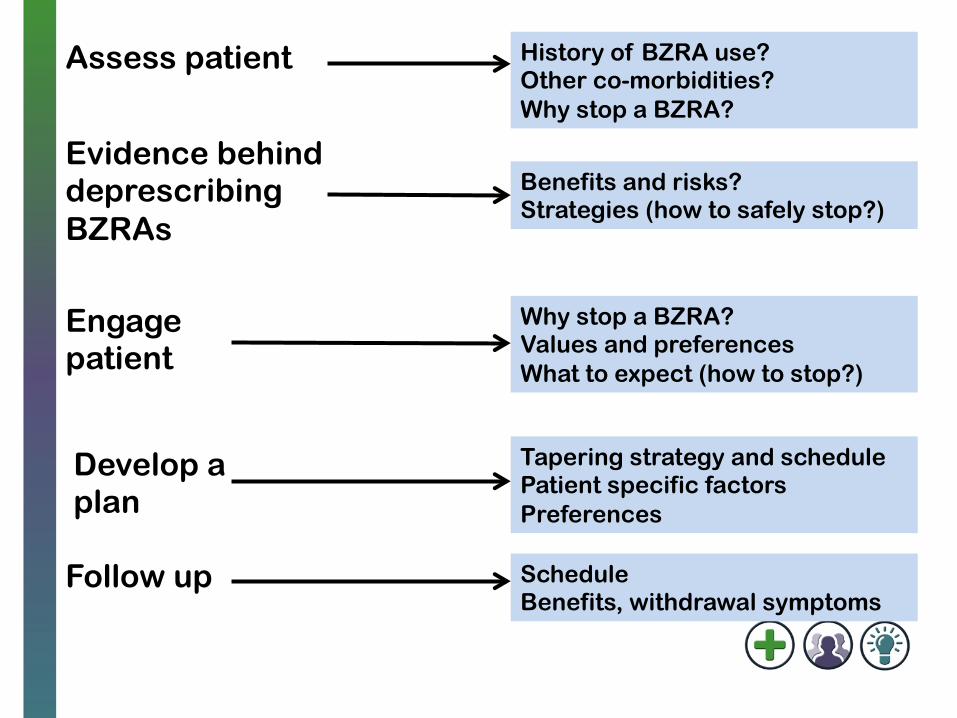
Assess patient
Engage patient
Develop a plan
Evidence behind deprescribing BZRAs
Follow up
History of BZRA use? Other co-morbidities? Why stop a BZRA?
Why stop a BZRA? Values and preferences What to expect (how to stop?)
Benefits and risks? Strategies (how to safely stop?)
Tapering strategy and schedule Patient specific factors Preferences
Schedule Benefits, withdrawal symptoms
WHY CONSIDER STOPPING A BZRA?
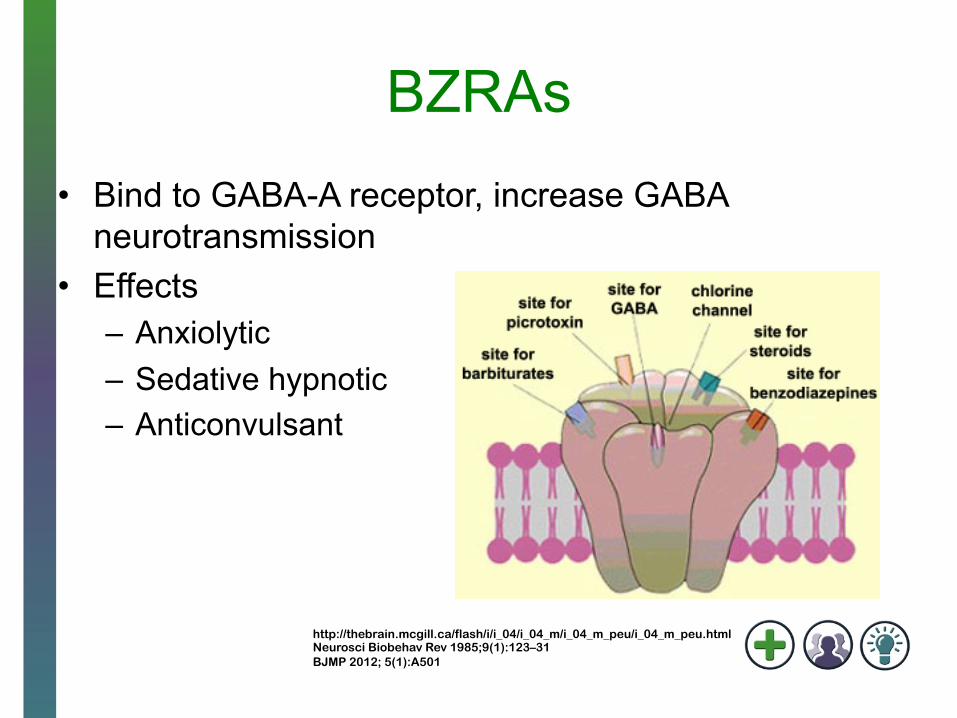
BZRAs • Bind to GABA-A receptor, increase GABA
neurotransmission • Effects
– Anxiolytic – Sedative hypnotic – Anticonvulsant
http://thebrain.mcgill.ca/flash/i/i_04/i_04_m/i_04_m_peu/i_04_m_peu.html Neurosci Biobehav Rev 1985;9(1):123–31 BJMP 2012; 5(1):A501
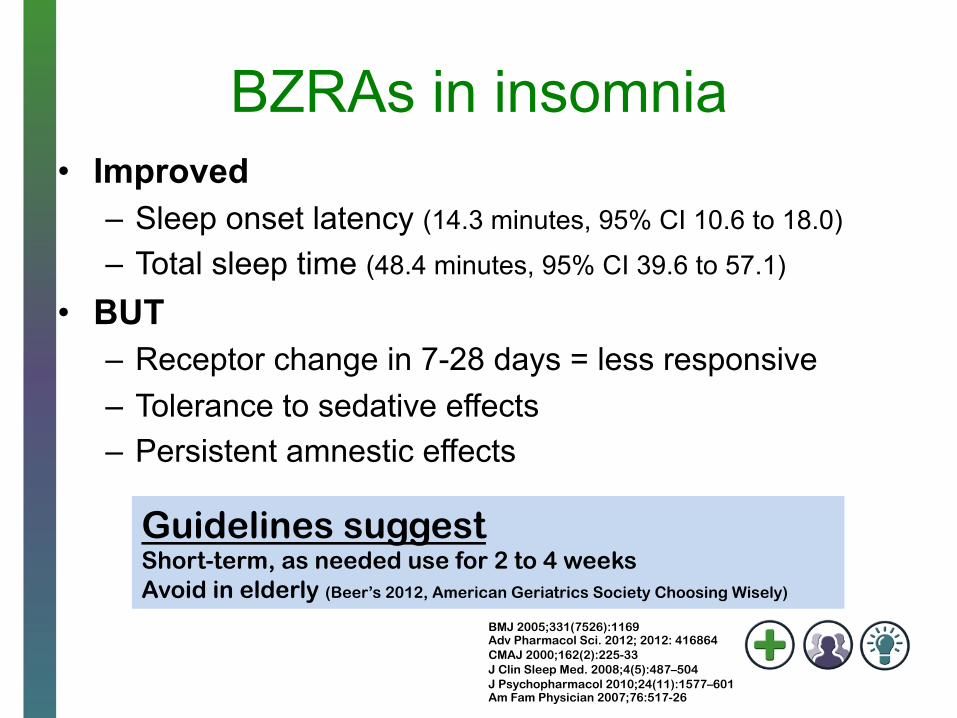
BZRAs in insomnia • Improved
– Sleep onset latency (14.3 minutes, 95% CI 10.6 to 18.0) – Total sleep time (48.4 minutes, 95% CI 39.6 to 57.1)
• BUT – Receptor change in 7-28 days = less responsive – Tolerance to sedative effects – Persistent amnestic effects
Guidelines suggest Short-term, as needed use for 2 to 4 weeks Avoid in elderly (Beer’s 2012, American Geriatrics Society Choosing Wisely)
BMJ 2005;331(7526):1169 Adv Pharmacol Sci. 2012; 2012: 416864 CMAJ 2000;162(2):225-33 J Clin Sleep Med. 2008;4(5):487–504 J Psychopharmacol 2010;24(11):1577–601 Am Fam Physician 2007;76:517-26
Harms of BZRAs • Commonly reported adverse effects
– Daytime drowsiness, balance issues, dizziness, and memory disturbance
• >60 years of age: number needed to harm = 6 (95 % CI 4.7-7.1)
• Physical dependence • Older persons at increased risk of adverse effects
BMJ 2005;331(7526):1169 CMAJ 2000;162(2):225-33
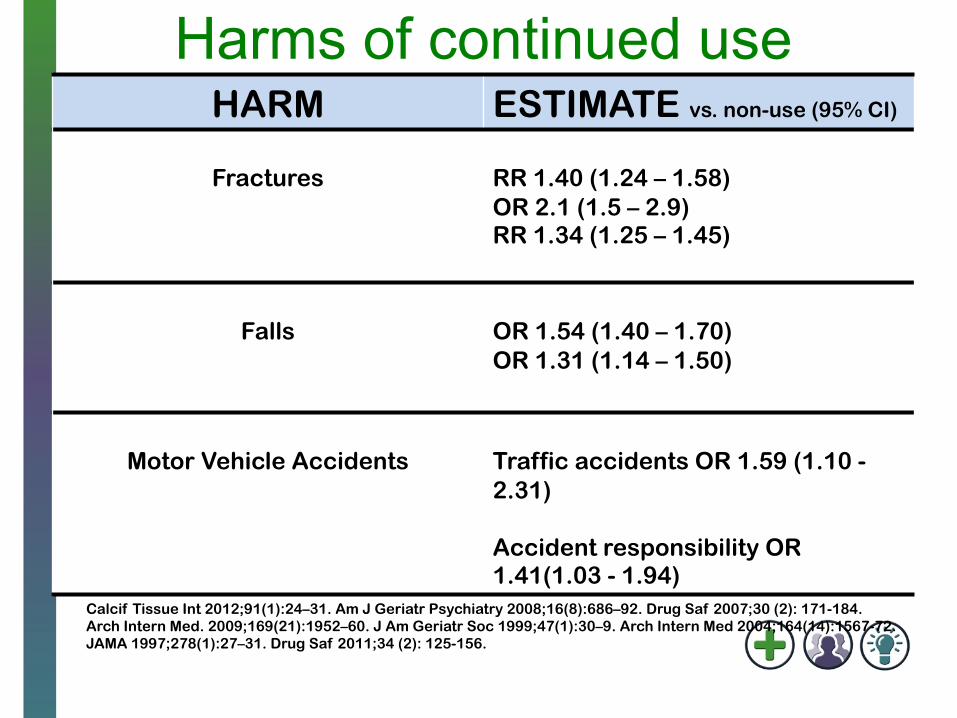
Harms of continued use HARM ESTIMATE vs. non-use (95% CI)
Fractures
RR 1.40 (1.24 – 1.58) OR 2.1 (1.5 – 2.9) RR 1.34 (1.25 – 1.45)
Falls
OR 1.54 (1.40 – 1.70) OR 1.31 (1.14 – 1.50)
Motor Vehicle Accidents
Traffic accidents OR 1.59 (1.10 - 2.31) Accident responsibility OR 1.41(1.03 - 1.94)
Calcif Tissue Int 2012;91(1):24–31. Am J Geriatr Psychiatry 2008;16(8):686–92. Drug Saf 2007;30 (2): 171-184. Arch Intern Med. 2009;169(21):1952–60. J Am Geriatr Soc 1999;47(1):30–9. Arch Intern Med 2004;164(14):1567-72. JAMA 1997;278(1):27–31. Drug Saf 2011;34 (2): 125-156.
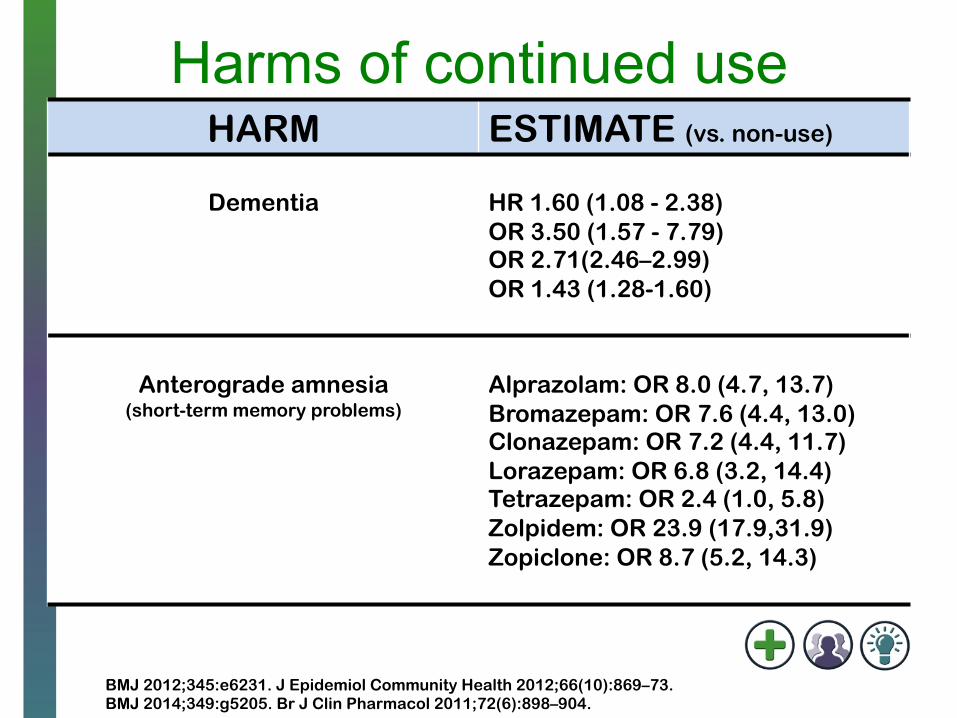
Harms of continued use HARM ESTIMATE (vs. non-use)
Dementia
HR 1.60 (1.08 - 2.38) OR 3.50 (1.57 - 7.79) OR 2.71(2.46–2.99) OR 1.43 (1.28-1.60)
Anterograde amnesia
(short-term memory problems)
Alprazolam: OR 8.0 (4.7, 13.7) Bromazepam: OR 7.6 (4.4, 13.0) Clonazepam: OR 7.2 (4.4, 11.7) Lorazepam: OR 6.8 (3.2, 14.4) Tetrazepam: OR 2.4 (1.0, 5.8) Zolpidem: OR 23.9 (17.9,31.9) Zopiclone: OR 8.7 (5.2, 14.3)
BMJ 2012;345:e6231. J Epidemiol Community Health 2012;66(10):869–73. BMJ 2014;349:g5205. Br J Clin Pharmacol 2011;72(6):898–904.
Mr. Twillie
• 82 years of age, Hx of hypertension and osteoarthritis – On ramipril 5 mg once daily, acetaminophen
500 mg TID • Prescribed temazepam 15 mg qhs to help him
sleep following death of wife 2 years ago • Five falls in the last 3 months • Diagnosed with mild cognitive impairment at last
clinic visit 2 weeks ago
http://wc-fields.info/movies/little-chickadee-w-c-fields-mae-west/
WHEN IS IT APPROPRIATE TO CONSIDER DEPRESCRIBING
A BZRA?
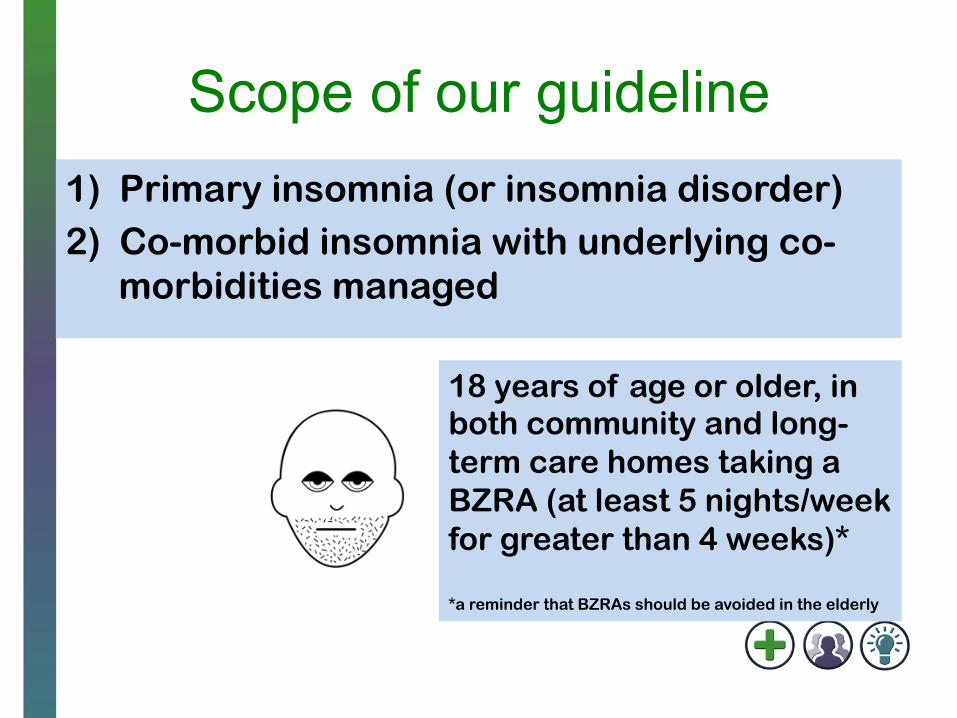
Scope of our guideline 1) Primary insomnia (or insomnia disorder) 2) Co-morbid insomnia with underlying co-
morbidities managed
18 years of age or older, in both community and long-term care homes taking a BZRA (at least 5 nights/week for greater than 4 weeks)* *a reminder that BZRAs should be avoided in the elderly
When our guideline does not apply Other sleep disorders (e.g. sleep apnea)
Underlying depression or anxiety not optimally managed
Physical conditions aggravating or causing insomnia (e.g. COPD)
Use of BZD specifically for anxiety disorder, seizure disorder
Alcohol withdrawal
Appropriate treatment of underlying/primary condition before consideration of deprescribing BZRAs
J Clin Sleep Med. 2008;4(5):487–504 J Psychopharmacol 2010;24(11):1577–601
Consider…
Mrs. Moone • 63 years of age • Generalized anxiety
disorder, major depressive disorder
• Incomplete response to SSRI for anxiety disorder, responded to and stabilized on clonazepam 1 mg TID 6 months ago
Mr. O’Dowd • 73 years of age • Depression managed
with citalopram 20 mg once daily x 2 years
• Complaint of difficulty sleeping 4 months ago, prescribed lorazepam 1 mg qhs
WHAT ARE THE POTENTIAL BENEFITS AND HARMS OF DEPRESCRIBING BZRAs?
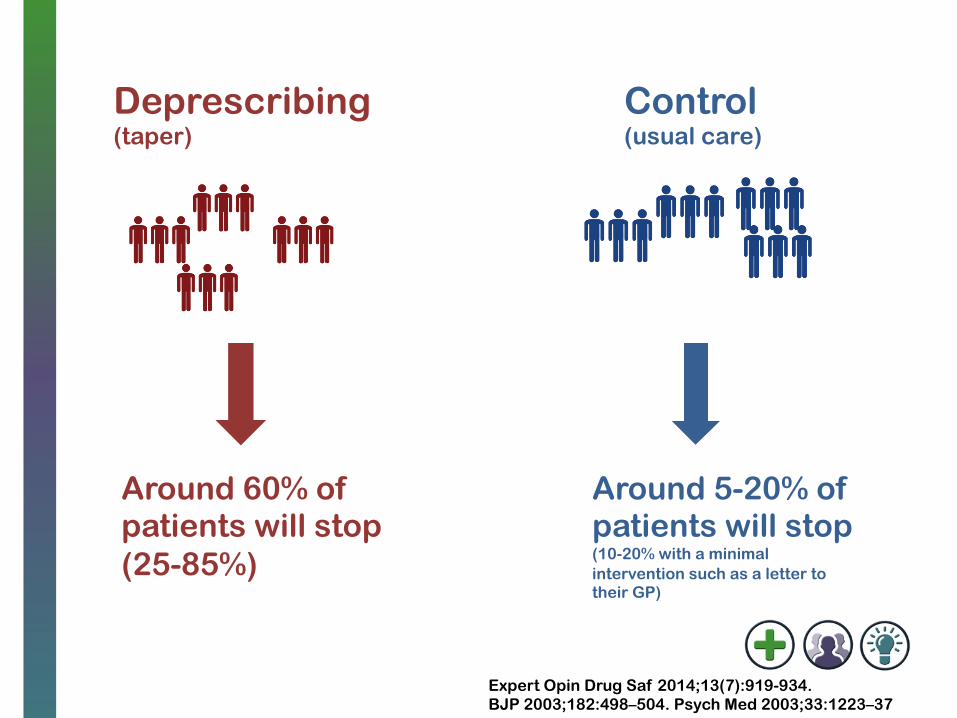
Deprescribing (taper)
Control (usual care)
Around 5-20% of patients will stop (10-20% with a minimal intervention such as a letter to their GP)
Around 60% of patients will stop (25-85%)
Expert Opin Drug Saf 2014;13(7):919-934. BJP 2003;182:498–504. Psych Med 2003;33:1223–37
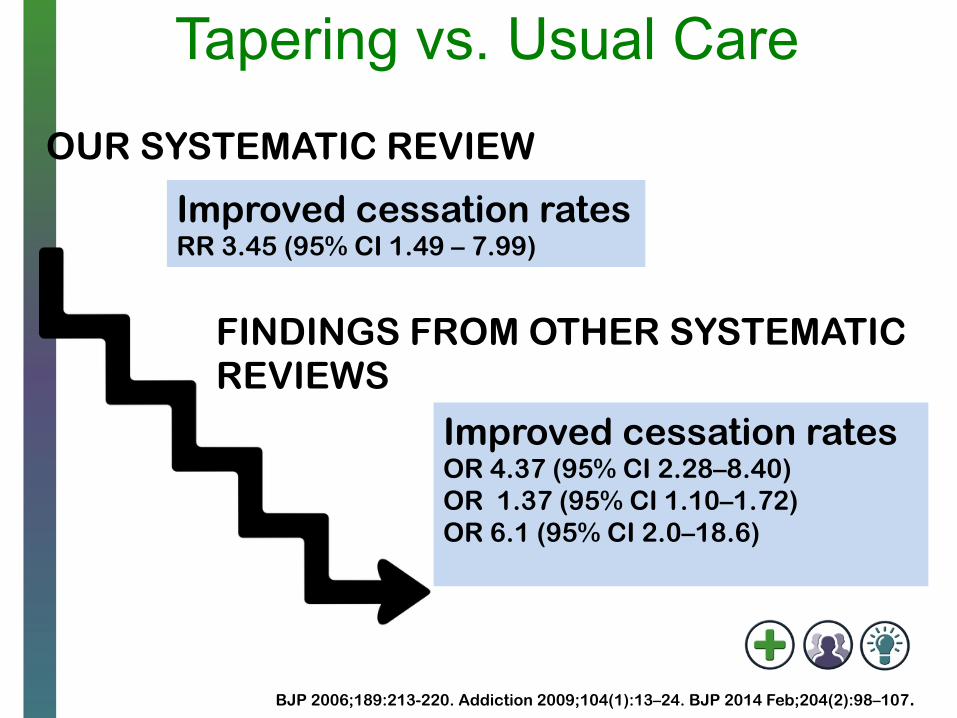
Tapering vs. Usual Care
Improved cessation rates RR 3.45 (95% CI 1.49 – 7.99)
OUR SYSTEMATIC REVIEW
FINDINGS FROM OTHER SYSTEMATIC REVIEWS
Improved cessation rates OR 4.37 (95% CI 2.28–8.40) OR 1.37 (95% CI 1.10–1.72) OR 6.1 (95% CI 2.0–18.6)
BJP 2006;189:213-220. Addiction 2009;104(1):13–24. BJP 2014 Feb;204(2):98–107.
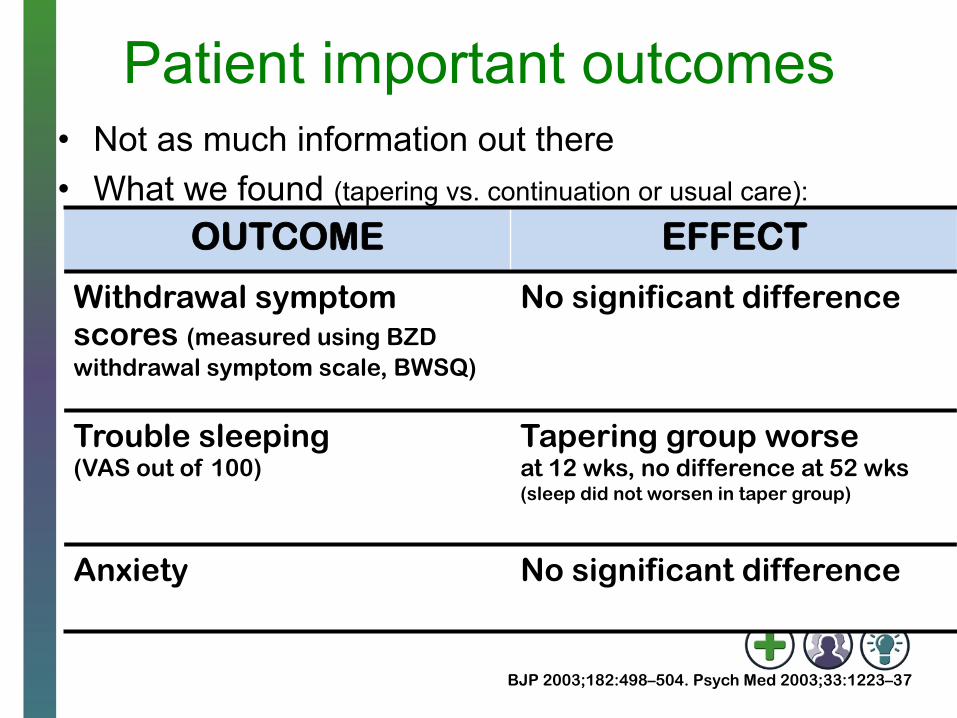
Patient important outcomes • Not as much information out there • What we found (tapering vs. continuation or usual care):
OUTCOME EFFECT
Withdrawal symptom scores (measured using BZD withdrawal symptom scale, BWSQ)
No significant difference
Trouble sleeping (VAS out of 100)
Tapering group worse at 12 wks, no difference at 52 wks (sleep did not worsen in taper group)
Anxiety No significant difference
BJP 2003;182:498–504. Psych Med 2003;33:1223–37
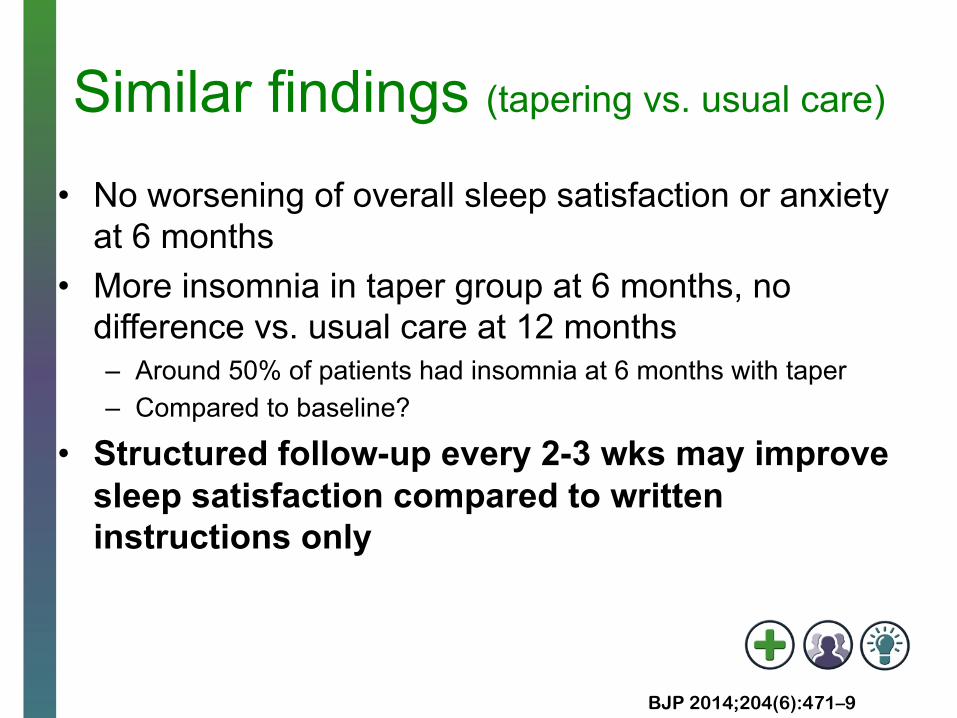
Similar findings (tapering vs. usual care)
• No worsening of overall sleep satisfaction or anxiety at 6 months
• More insomnia in taper group at 6 months, no difference vs. usual care at 12 months – Around 50% of patients had insomnia at 6 months with taper – Compared to baseline?
• Structured follow-up every 2-3 wks may improve sleep satisfaction compared to written instructions only
BJP 2014;204(6):471–9
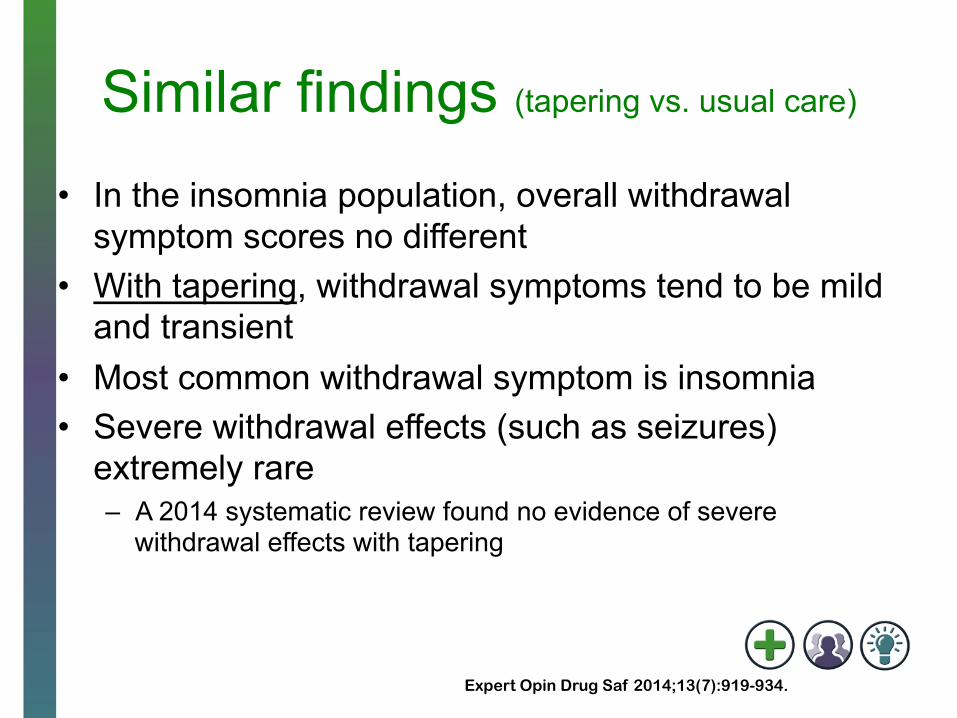
Similar findings (tapering vs. usual care)
• In the insomnia population, overall withdrawal symptom scores no different
• With tapering, withdrawal symptoms tend to be mild and transient
• Most common withdrawal symptom is insomnia • Severe withdrawal effects (such as seizures)
extremely rare – A 2014 systematic review found no evidence of severe
withdrawal effects with tapering
Expert Opin Drug Saf 2014;13(7):919-934.
CBT + taper vs. taper alone Improves cessation rates post-intervention, benefit may not be sustained long-term
5-6 sessions, focused on behavioural management (stimulus control, relaxation training, tolerating temporary discomfort)
May improve anxiety scores compared to tapering alone
Behav Res Ther 2005;43(1):1–14. Consult Clin Psychol 2007;75(2):325–35. CMAJ 2003;169(10):1015-20. BJP 2003;182:498–504.
HOW ARE BZRAs DEPRESCRIBED?
Engage patients Discuss reasons behind deprescribing: harms of continued use, receptor changes, tapering plan, potential withdrawal symptoms & duration
Consider patient values and preferences, patient factors such as age & duration of use
Use of educational tools such as pamphlets or brochures have demonstrated success
JAMA Intern Med 2014;174(6):890–8. BJP 2014;204(6):471–9
Engaging patients
Patients succeed in deprescribing BZRAs when: 1) They understand the risks of continued BZRA use 2) They know what to expect from deprescribing
JAMA Intern Med 2014;174(6):890–8. BJP 2014;204(6):471–9.
http://www.criugm.qc.ca/fichier/pdf/BENZOeng.pdf
TAPERING OFF
BENZODIAZEPINE RECEPTOR
AGONISTS
•
• • • •
May experience insomnia following deprescribing, but usually short-term (days – weeks) and no difference vs. usual care at 12 months
Likely no increase in anxiety (if occurs, usually mild, short-term and transient)
Overall withdrawal symptom scores no different with tapering vs. usual care
• Sensitivity to light • Loss of appetite • Dizziness, muscle twitching • Perceptual disturbance
No evidence of severe withdrawal symptoms in tapering studies
Expert Opin Drug Saf 2014;13(7):919-934. BJP 2014;204(6):471–9. BJP 2003;182:498–504. Psych Med 2003;33:1223–37 http://www.dvdsreleasedates.com/movies/5404/What-to-Expect-When-Youre-Expecting-2012.html
Tapering strategies • No head-to-head comparisons in literature • Switching to equivalent dose of diazepam is one
approach, no evidence that this is more effective or safer compared to tapering shorter half-life BZRAs
We suggest reducing dose by approximately 25% every 2 weeks, with 12.5% reductions near end, and gradual introduction of drug free days
J Psychiatry Neurosci 2015;40(3):E27.
Other considerations
• May consider slower taper in some patients – Long duration of use, high disease burden,
previous unsuccessful attempts • Set goal and develop taper plan at outset • Decide on thresholds for symptom relapse AND
withdrawal symptoms (see paper below for examples of scales)
Expert Opin Drug Saf 2014; 13(7):919-934. J Psychiatry Neurosci 2015;40(3):E27.
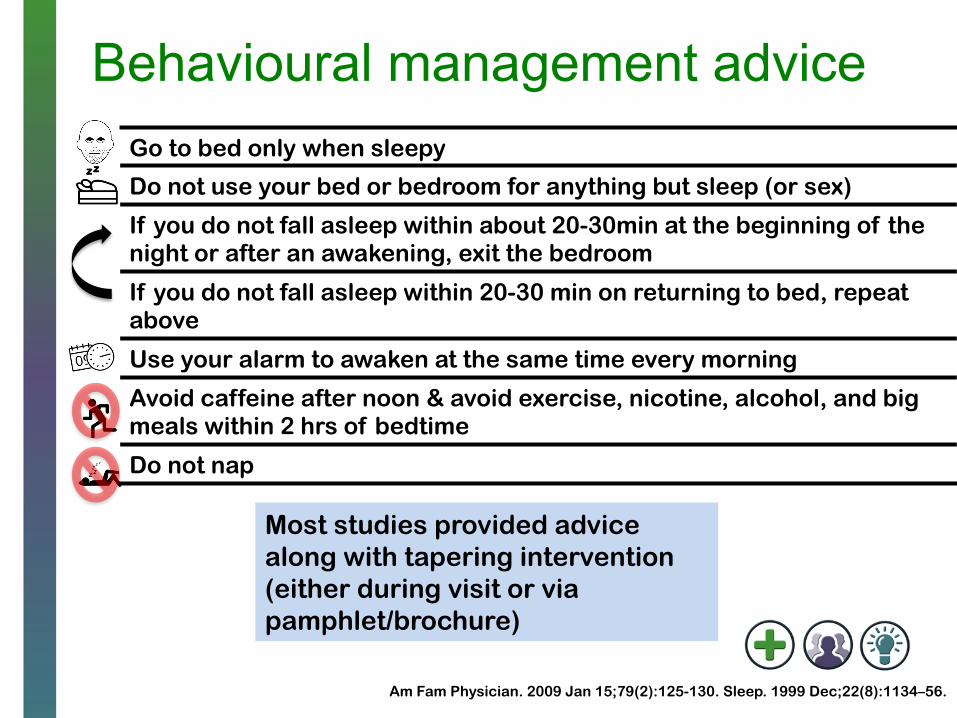
Behavioural management advice Go to bed only when sleepy
Do not use your bed or bedroom for anything but sleep (or sex)
If you do not fall asleep within about 20-30min at the beginning of the night or after an awakening, exit the bedroom
If you do not fall asleep within 20-30 min on returning to bed, repeat above
Use your alarm to awaken at the same time every morning
Avoid caffeine after noon & avoid exercise, nicotine, alcohol, and big meals within 2 hrs of bedtime
Do not nap
Most studies provided advice along with tapering intervention (either during visit or via pamphlet/brochure)
Am Fam Physician. 2009 Jan 15;79(2):125-130. Sleep. 1999 Dec;22(8):1134–56.
HOW TO MONITOR PATIENTS AFTER STOPPING BZRAs
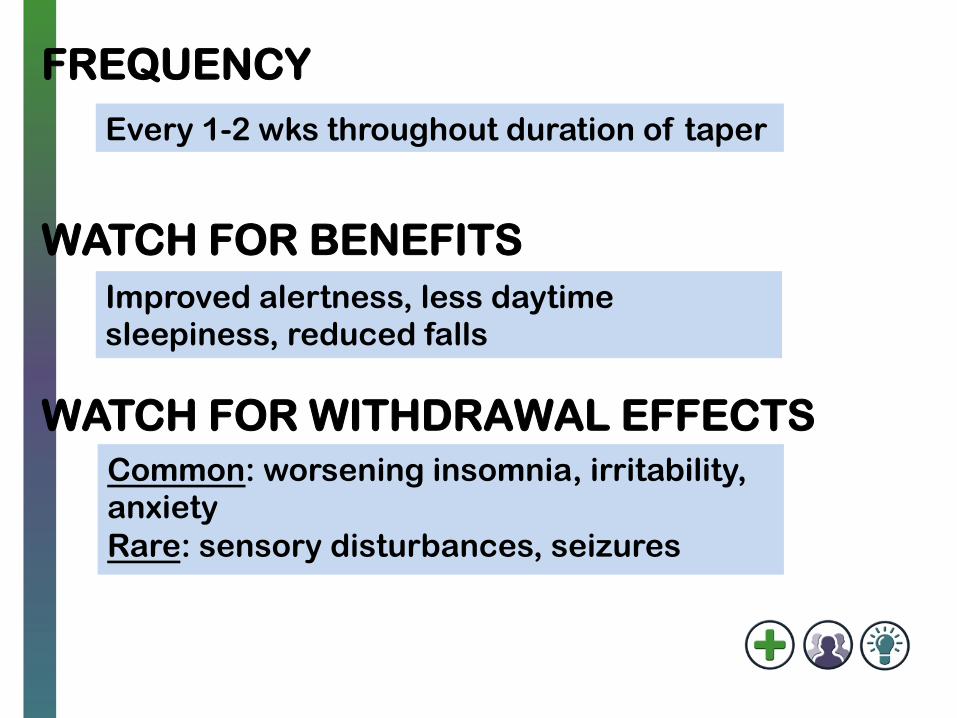
Every 1-2 wks throughout duration of taper
Improved alertness, less daytime sleepiness, reduced falls
Common: worsening insomnia, irritability, anxiety Rare: sensory disturbances, seizures
FREQUENCY
WATCH FOR BENEFITS
WATCH FOR WITHDRAWAL EFFECTS
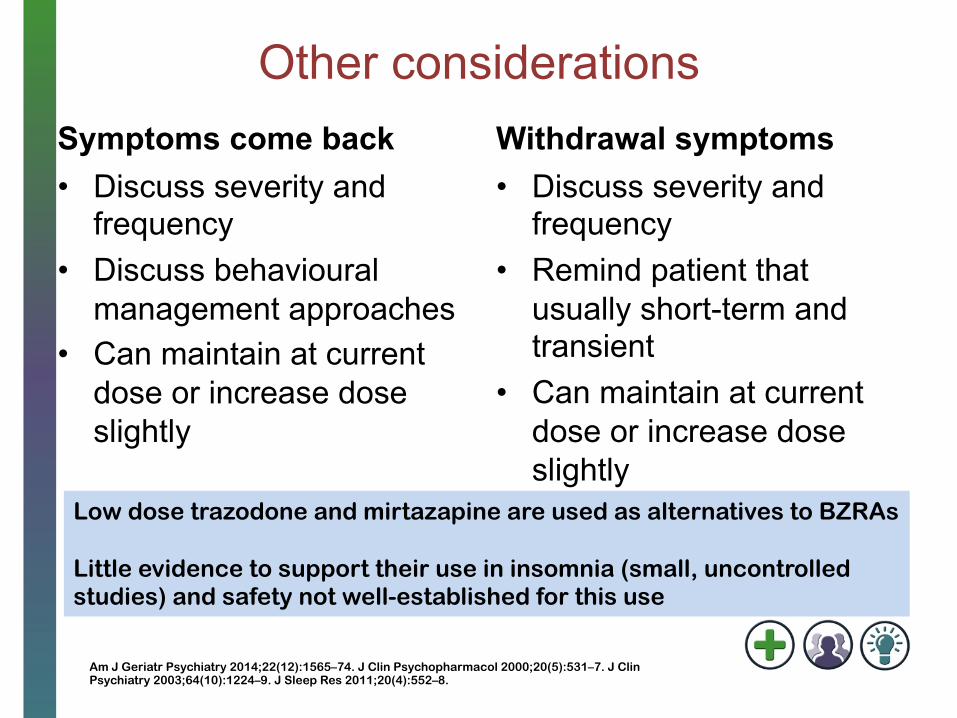
Other considerations Symptoms come back • Discuss severity and
frequency • Discuss behavioural
management approaches • Can maintain at current
dose or increase dose slightly
Withdrawal symptoms • Discuss severity and
frequency • Remind patient that
usually short-term and transient
• Can maintain at current dose or increase dose slightly
Low dose trazodone and mirtazapine are used as alternatives to BZRAs Little evidence to support their use in insomnia (small, uncontrolled studies) and safety not well-established for this use
Am J Geriatr Psychiatry 2014;22(12):1565–74. J Clin Psychopharmacol 2000;20(5):531–7. J Clin Psychiatry 2003;64(10):1224–9. J Sleep Res 2011;20(4):552–8.
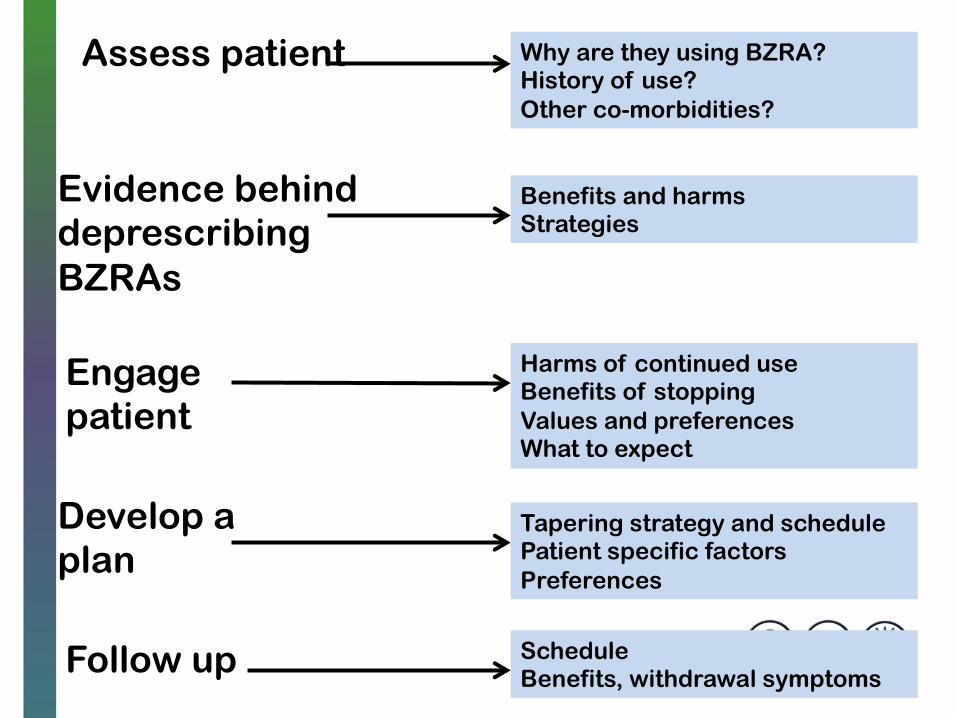
Assess patient
Engage patient
Develop a plan
Evidence behind deprescribing BZRAs
Follow up
Why are they using BZRA? History of use? Other co-morbidities?
Harms of continued use Benefits of stopping Values and preferences What to expect
Benefits and harms Strategies
Tapering strategy and schedule Patient specific factors Preferences
Schedule Benefits, withdrawal symptoms
Key points • Assess which patients deprescribing may be
appropriate for • Engage patients in discussion about harms of
continued BZRA use, goals of deprescribing • Collaborate with patient to develop goals and plan • Provide behavioural management advice (even if
brief) • Monitoring and follow-up is extremely important
PUTTING IT ALL TOGETHER: A BZRA DEPRESCRIBING
ALGORITHM
Mr. Jeeves • 86 years of age • Hx: hypertension, hyperlipidemia, MI 7 yrs ago
– ASA 81 mg once daily, rosuvastatin 10 mg once daily, bisoprolol 2.5 mg once daily, losartan 100 mg once daily, lorazepam 1 mg qhs
• On discussion with patient, find out: – Has been on lorazepam for ~7 yrs for sleep in
hospital – No history of anxiety or depression
Mr. Jeeves (continued) ENGAGE PATIENT • Discuss potential harms of BZRA use (especially in
older persons) • Discuss potential benefits of stopping • What to expect during taper (potential for withdrawal
symptoms, example tapering plan, frequency of follow-up)
• Suggest deprescribing
Mr. Jeeves (continued) • Develop a tapering plan together
1. reduce dose to 0.75 mg qhs x 2 wks 2. reduce dose to 0.5 mg qhs x 2 wks 3. reduce dose to 0.25 mg qhs x 2 wks 4. introduce 2 drug-free days each week until stopped
• Decide on frequency of follow-up • Remind pt of potential withdrawal symptoms, and
that short-term and transient • Discuss thresholds for symptom return and
withdrawal effects (how much discomfort pt can tolerate)

Contact and More Information
[email protected] @Deprescribing & @open_pharmacy www.open-pharmacy-research.ca www.deprescribing.org (coming soon) Join our e-newsletter list
All icons courtesy of the Noun Project https://thenounproject.com/