depressive cognitions, maternal attitudes and postnatal depression
TRANSCRIPT

This article was downloaded by: [University of Kiel]On: 27 October 2014, At: 06:32Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Reproductive and InfantPsychologyPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/cjri20
Depressive cognitions, maternalattitudes and postnatal depressionKimberly D. Thompsona & Debra Bendellaa School of Psychology, Fielding Graduate University, SantaBarbara, California, USAPublished online: 26 Nov 2013.
To cite this article: Kimberly D. Thompson & Debra Bendell (2014) Depressive cognitions, maternalattitudes and postnatal depression , Journal of Reproductive and Infant Psychology, 32:1, 70-82,DOI: 10.1080/02646838.2013.858312
To link to this article: http://dx.doi.org/10.1080/02646838.2013.858312
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Depressive cognitions, maternal attitudes and postnatal depression
Kimberly D. Thompson* and Debra Bendell
School of Psychology, Fielding Graduate University, Santa Barbara, California, USA
(Received 18 July 2013; accepted 20 October 2013)
Objective: This study explored the relationship of depressive cognitions, sociallyprescribed perfectionism and self-silencing, to postnatal depression and women’sbeliefs about motherhood. The study aimed to replicate, with a postnatal sample,findings in the depression literature that link certain depressive cognitions withdepressive symptoms. Additionally, the study explored a proposed model inwhich these cognitions influenced the development of dysfunctional maternal atti-tudes and postnatal depressive symptoms. Background: Postnatal depression anddysfunctional maternal attitudes are situated within the interactional model ofdepression. The importance of beliefs about interpersonal relationships that arethought to lead to depressive symptoms is explored and explained theoretically.Methods: A cross-sectional design used correlational and SEM path analysis toexamine interrelationships between variables. Participants were 77 postnatalwomen from 18 to 38 years of age attending their regular gynaecological appoint-ments 4–8 weeks after childbirth. Measures used included: Edinburgh PostnatalDepression Scale, Maternal Attitudes Questionnaire, Multidimensional Perfec-tionism Scale and the Silencing the Self Scale. Results: Socially prescribed per-fectionism, externalised self-perception, self-silencing, the divided self anddysfunctional maternal attitudes were significantly correlated with postnataldepression (r = .354–.677) and with each other (r = .272–.574). SEM modelling(final model, χ2(7, 77) = .891, CFI = 1.000, RMSEA = .000) suggested that post-natal depression is most strongly related to externalised self-perception andsocially prescribed perfectionism through the mediating effects of dysfunctionalmaternal attitudes and the divided self. Conclusions: Depressive cognitions werefound to be related to postnatal depression in ways similar to depression in otherlife periods. The central finding of this study was the observation that dysfunc-tional maternal attitudes and the divided self-mediate the relationship betweendepressive cognitions and postnatal depression.
Keywords: postnatal depression; postpartum depression; socially prescribedperfectionism; silencing the self; maternal attitudes
Kelly (1963) asserted that to be human is to be motivated to predict and controlone’s experience. Past experiences are used as a template to guide predictions aboutthe future. These predictions are then used as response controls. Cognitive patternsare habitual ways of thinking about relevant situations that increase the predictabil-ity of one’s experience, guide responding and increase one’s sense of control.Double-binds, or no-win situations, occur when a person’s multiple predictions, orexpectancies, about a situation conflict with one another. This study explored the
*Corresponding author. Email: [email protected]
© 2013 Society for Reproductive and Infant Psychology
Journal of Reproductive and Infant Psychology, 2014Vol. 32, No. 1, 70–82, http://dx.doi.org/10.1080/02646838.2013.858312
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
relationship of depressive cognitions, which put the individual in double-binds, tosymptoms of depression in the postnatal period.
Socially prescribed perfectionism is the belief that others expect perfection;self-silencing is the belief that stringent self-monitoring and inhibition is necessaryto preserve interpersonal connection. These are cognitions that supply predictivepower regarding interpersonal outcomes. They also constitute double-binds, inwhich one’s abilities, inner experience, or natural inclinations conflict withperceived demands from others. Those high in socially prescribed perfectionismbelieve ‘I must be perfect in order to please others’ and ‘I cannot be perfect’.Self-silencers are aware at some level that their relationships are being preserved atthe expense of their personal authenticity. They believe both ‘I must be acceptedby others’ and ‘I cannot be accepted as I am’.
A woman high in socially prescribed perfectionism, a known predictor ofhopelessness, may become hopeless when she doubts that she can satisfy othersand does not expect their acceptance (O’Connor & O’Connor, 2003). Similarly, awoman who values relatedness and believes that self-silencing is necessary mayfeel hopeless when this strategy fails her in building meaningful relationships. Ashope goes down, symptoms of postnatal depression go up (Thio & Elliott,2008).
Depression is thought to be precipitated and maintained by interpersonal fac-tors (Coyne, 1976, 1999), in particular the quality of early significant relation-ships (Jacobovitz, Hazen, Curran, & Hitchens, 2004). In adulthood, theinterpersonal lives of depressed people differ from the non-depressed (e.g. Abelaet al., 2011). People prone to depression tend to engage in excessive reassur-ance-seeking and negative feedback-seeking, habits that others find aversive (Evr-aire & Dozois, 2011). They tend to create interpersonal stress and to havechronic insecurity, which interferes with relationships (Epkins & Heckler, 2011;Flynn & Rudolph, 2011). During the postnatal period, when a depression-pronewoman particularly needs the emotional and instrumental support of others, shemay be poorly equipped to elicit help and may be in relationships with peoplepoorly equipped to give it. Depressive behaviours may even act as a contagion,passing on depression to others in her social circle (Abela, Zinck, Kryger, Zilber,& Hankin, 2009).
One way that interpersonal factors put women at risk for postnatal depressionis low social support (e.g. Agoub, Moussaoui, & Battas, 2005; Dennis & Ross,2006). Depressed married women report poorer marital quality (Brenninkmeyer-Davis, 2007) and increased marital discord (Kendall-Tackett, 2007). Hung (2007)found that Chinese women whose mother-in-law helped in the postnatal periodwere at lower risk of becoming depressed. Social support deficits may explainwhy more children in the home increase risk (Faisal-Cury, Tedesco, Kahhale,Menezos, & Zugaib, 2004) and may increase sleep deprivation, another risk factor(Ross, Murray, & Steiner, 2005). Findings that new mothers are more likely tohave unstable mood during the neonatal period if they experienced their ownmother to be uncaring (Mayes & Leckman, 2007), and to become depressed iftheir own mothers and grandmothers experienced postnatal depression (Sejourne,Alba, Onorrus, Goutadier, & Chabrol, 2011) may reflect interpersonal difficultiesacross generations.
Journal of Reproductive and Infant Psychology 71
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
Cognitive vulnerabilities
Women at increased risk of postnatal depression tend to exhibit a depressivecognitive style, similar to patterns found in other depressed persons (Milgrom &Beatrice, 2003). They interpret negative situations in global, stable, and internalterms, and attribute positive situations to specific, unstable and external causes(Cole et al., 2008). Cognitive risk also includes perfectionistic, rigid, dependent, orself-critical traits (Mazzeo et al., 2006) and high levels of rumination (Josefsson,Larsson, Sydsjo, & Nylander, 2007). Depressed pregnant women have positivebeliefs about rumination at significantly higher rates than the controls, a finding thatunderscores the relevance of cognitive factors to depression in the perinatal period(Alfaraj, Spada, Nikcevic, Puffett, & Meer, 2013).
Socially prescribed perfectionism has been associated with depression in clinicaland nonclinical samples (Egan, Wade, & Shafran, 2011), including pregnant women(Dimitrovsky, Levy-Shiff, & Schattner-Zanani, 2002). It generates the need topresent one’s self as perfect (Hewitt et al., 2003), the inability to feel pride at one’ssuccesses (Stoeber & Yang, 2010), destructive levels of rumination (Randles, Flett,Nash, McGregor, & Hewitt, 2010), and deficits in cognitive emotional regulationstrategies (Rudolph, Flett, & Hewitt, 2007). It is inversely related to social support(Sherry, Law, Hewitt, Flett, & Besser, 2008), and may both reflect dysfunctionalpast relationships and interfere with the formation of supportive ones.
Silencing the self has been observed in women of many cultures (Jack & Ali,2010). It has been found to be related to depression in university students (Flett, Bes-ser, Hewitt, & Davis, 2007), female outpatients (Ali, Oatley, & Toner, 2002), and eth-nically diverse, low-income women (Grant, Jack, Fitzpatrick, & Ernst, 2011).Although self-silencing is thought to stem from parental criticism and rejection, cur-rent perceptions of one’s partner are also important (Thompson, Whiffen, & Aube,2001). Silencing the self is a multidimensional construct, consisting of the active inhi-bition of self-expression, belief that caring for others requires self-sacrifice, preferen-tially viewing one’s self through others’ perspectives, and experience of the self asbeing divided between inner experience and outer expression (Jack & Ali, 2010).
While self-silencing individuals may appear to be quite interpersonally passive,silencing the self requires constant active self-monitoring (Jack & Ali, 2010). Awoman high in self-silencing is likely to be distressed by any self-monitoringlapses. Ussher and Perz (2010) have described premenstrual syndrome as a rupturein self-monitoring, in which the woman temporarily loses the rigid self-controlkeeping the inner and outer selves divided. A history of premenstrual symptomsserves as a risk factor for postnatal depression (e.g. Buttner et al., 2012). Thepostnatal period may also be a phase of life in which it is difficult to silence theself. A woman who copes in relationships by silencing herself may find ruptures inself-silencing postnatally to be particularly distressing, as she is forming a newrelationship with her baby and is dependent upon the support of significant others.
Intensive self-monitoring is also a feature of socially prescribed perfectionism(Randles et al., 2010). Flett et al. (2007) found a robust relationship betweensocially prescribed perfectionism and self-silencing, and confirmed the relationshipbetween each of these and depression. This study found that while self-silencingoverall mediated the relationship between socially prescribed perfectionism anddepression, the strongest mediator was externalised self-perception, a type ofself-monitoring that is a component of silencing the self.
72 K.D. Thompson and D. Bendell
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4

Externalised self-perception, the tendency to preferentially take others’presumed viewpoint when contemplating the self, undermines a woman’sconfidence in her own perspective and is independently predictive of depression inwomen (Tan & Carfagnini, 2008). Those who believe that others expect them to beperfect and have a bias toward viewing themselves from other people’s perspectivesare relatively defenceless against unreasonable expectations, actual or perceived.
Negative expectancies toward interpersonal relationships may be carried forwardinto a woman’s relationship with her new baby. Depressed new mothers have beenfound to show a negative bias in interpreting infant facial expressions (Gil,Teissedre, Chambres, & Droit-Volet, 2011), to have more negative attitudes towardtheir baby and toward themselves as mothers (Fowles, 2010), to have lower levelsof parenting efficacy (O’Neil, Wilson, Shaw, & Dishion, 2009), to think less ofthemselves as mothers (Horowitz, Damato, Duffey, & Solon, 2005), and to havemore negative attitudes toward the mother role (Deave, 2005). Stein et al. (2012)found that anxious and depressed mothers of 10-month-old infants weresignificantly less responsive to their infants following priming with negative worryor ruminative thoughts.
Parenting a neonate with an irritable temperament and poor motor control,characteristics that tend to inhibit a child’s interpersonal responsiveness, has beenassociated with postnatal depression (Murray, 2006). Women with maladaptiveexpectancies about close relationships may interpret low infant responsivenessmuch more negatively than women with more adaptive ones. As early as 48 hoursafter childbirth, the degree to which a woman perceives her infant to be ‘difficult’has been found to predict the intensity of her depressive symptoms (Denis, Ponsin,& Callahan, 2013).
Hypotheses
This study examined the interrelationships between the four dimensions ofself-silencing, socially prescribed perfectionism, postnatal depression and dysfunc-tional maternal attitudes, and hypothesised that all study variables would besignificantly and positively correlated with one another. Exploration was conductedin the second phase of data analysis, in which a model was built, tested andmodified based on the theory that externalised self-perception and sociallyprescribed perfectionism are early-developing cognitive patterns that make specificpredictions and provoke particular types of responses. They were conceptualised aspreconditions for the coping strategies of care as self-sacrifice and self-silencing,the experience of the divided self, and the development of dysfunctional maternalattitudes and postnatal depression. We predicted that the data would supportpathways between these externalised self-perception and socially prescribedperfectionism, to the other dimensions of self-silencing, resulting in dysfunctionalmaternal attitudes and postnatal depression symptoms.
Methods
Procedure
Participants included women that were 4–8 weeks postnatal at the time of datacollection, and were patients of participating private-practice obstetricians in a ruralarea of Texas. Participating physicians included a clause in their informed consent
Journal of Reproductive and Infant Psychology 73
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4

documents that allowed patients to give or deny consent for their de-identifiedclinical information to be used in professional research.
Referring physicians administered the study measures as part of the routineinformation-gathering at the patient’s postnatal appointment. Patients completed themeasures while waiting for their appointment. The data obtained from theadministration of these measures remained a part of the medical record, for use atthe discretion of the referring physician. No items on any of the measures werealtered for this study.
Ethical approval
The proposal for this study was examined by the Internal Review Board of theinstitution with which the investigators are associated. Ethical approval wasobtained prior to the beginning of data collection.
A-priori power analysis
A-priori power analysis, conducted using the G Power 3 program, downloaded fromhttp://www.psycho.uni-duesseldorf.de/abteilungen/aap/gpower3/download-and-register,suggested that the minimum number of participants in this study should be 75.A-priori power analysis was computed using the parameters of: 10 variables (all MPSsubscales, all silencing the self subscales and silencing the self total score,dysfunctional maternal attitudes scores, and postnatal depression scores), p = .05,power = .80 and effect size estimated from r values from previous studies(Dimitrovsky et al., 2002; Flett et al., 2007; Hewitt & Flett, 1991; Hewitt et al., 1998;Warner, Appleby, Whitton, & Faragher, 1997). Effect sizes between dysfunctionalmaternal attitudes scores and perfectionism and silencing the self subscale scorescould not be computed because prior studies with these variables had not beenpreviously conducted.
Measures
Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987)The EPDS is a 10-item questionnaire created to identify postnatal depression andto avoid confounding factors that are observed when postnatal women completeother more general depression measures. The authors report that, in the initial study,the EPDS had 86% sensitivity to cases, and 78% specificity in screening out non-cases, and had good internal consistency (α = .87), using a cut-off score of 12. Thesensitivity increased to more than 90% when the cut-off was lowered to 9 (Coxet al., 1987). In this study, EPDS scores were used as continuous data, and there-fore a cut-off score was not used.
Multidimensional Perfectionism Scale (MPS; Hewitt & Flett, 1991)The MPS is a 45-item scale that measures 3 dimensions of perfectionism. Thesubscale of interest to this study, socially prescribed perfectionism, has been shownto have a test-retest reliability coefficient of .60, which is significant at the p < .05level. Additionally, it has been found to have good construct validity, asdemonstrated by associations at the p < .001 level, with measures of parental
74 K.D. Thompson and D. Bendell
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
expectations, parental criticism, and self-punitiveness (Hewitt & Flett, 1991). In thisstudy, no cut-off scores were used, as scores were used as continuous data.
Maternal Attitudes Questionnaire (MAQ; Warner et al., 1997)The MAQ is a 14-item questionnaire designed to evaluate attitudes toward mother-hood in the postnatal period. No significant changes were observed between thefirst and second administrations of the questionnaire during test construction pilottesting. Internal reliability was observed to be r = .84. Because the scale wasconstructed by extensive review of the literature and by extensive clinicalexperience with depressed postnatal women, it has good face validity. Concurrentvalidity was tested and confirmed by the scale’s ability to discriminate betweenwomen with and without depression (r = .60, p < .0001; Warner et al., 1997). Inthis study, MAQ scores were used as continuous data; therefore, a cut-off scorewas not utilised.
Silencing the Self Scale (STSS; Jack & Dill, 1992)The Silencing the Self Scale is a 31-item quantitative measure of self-silencing. Itwas found to have good internal consistency, good test–retest reliability, and goodconstruct validity as indicated by its high correlations (r = .50 to .52, p < .0001)with Beck Depression Inventory scores. The STSS is made up of four theoreticallydriven subscales, including External Self-Perception, Care as Self-Sacrifice,Silencing the Self and the Divided Self. Psychometric testing for the STSS wasconducted with three samples: undergraduate females, residents of a batteredwomen’s shelter, and new mothers at 4 months postnatal (Jack & Dill, 1992).Previous use of this scale with postnatal women yielded subscale internalconsistency coefficients of .78 for Silencing The Self, .85 for ExternalisedSelf-Perception, .79 for Care As Self-Sacrifice, and .81 for Divided Self (Jack &Dill, 1992).
Results
Participants
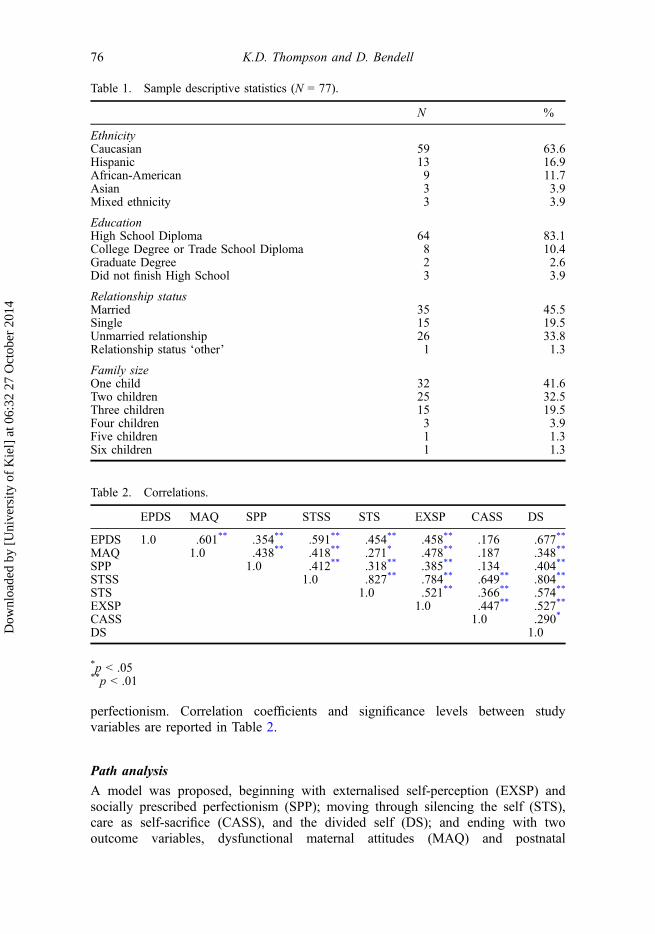
Participants were women attending their scheduled postnatal obstetricalappointments. After packets were screened for incomplete data, the final N = 77.The mean age of the sample is 24.6, with a standard deviation of 4.72. Allparticipants were between the ages of 18 and 38, and were between 4 and 8 weekspostnatal. Sample descriptive statistics are reported in Table 1.
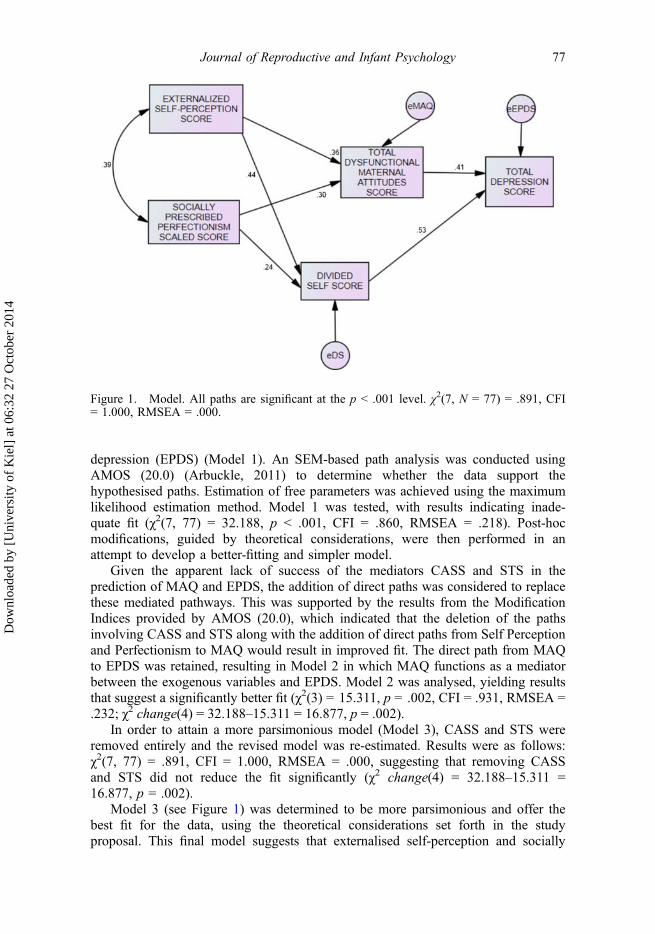
Correlational analysis
Using correlational analysis, the hypotheses that study variables, including postnataldepression (EPDS) scores, dysfunctional maternal attitudes (MAQ) scores, sociallyprescribed perfectionism (SPP) scores, and scores on silencing the self subscalesexternalised self-perception (EXSP), silencing the self per se (STS), the divided self(DS) and care as self-sacrifice (CASS) would be significantly correlated with oneanother were supported for the most part. The only variable examined that was notsignificantly correlated with all other variables was care as self sacrifice (CASS),which had positive relationships that did not achieve statistical significance withpostnatal depression, dysfunctional maternal attitudes and socially prescribed
Journal of Reproductive and Infant Psychology 75
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
perfectionism. Correlation coefficients and significance levels between studyvariables are reported in Table 2.
Path analysis
A model was proposed, beginning with externalised self-perception (EXSP) andsocially prescribed perfectionism (SPP); moving through silencing the self (STS),care as self-sacrifice (CASS), and the divided self (DS); and ending with twooutcome variables, dysfunctional maternal attitudes (MAQ) and postnatal
Table 1. Sample descriptive statistics (N = 77).
N %
EthnicityCaucasian 59 63.6Hispanic 13 16.9African-American 9 11.7Asian 3 3.9Mixed ethnicity 3 3.9
EducationHigh School Diploma 64 83.1College Degree or Trade School Diploma 8 10.4Graduate Degree 2 2.6Did not finish High School 3 3.9
Relationship statusMarried 35 45.5Single 15 19.5Unmarried relationship 26 33.8Relationship status ‘other’ 1 1.3
Family sizeOne child 32 41.6Two children 25 32.5Three children 15 19.5Four children 3 3.9Five children 1 1.3Six children 1 1.3
Table 2. Correlations.
EPDS MAQ SPP STSS STS EXSP CASS DS
EPDS 1.0 .601** .354** .591** .454** .458** .176 .677**
MAQ 1.0 .438** .418** .271* .478** .187 .348**
SPP 1.0 .412** .318** .385** .134 .404**
STSS 1.0 .827** .784** .649** .804**
STS 1.0 .521** .366** .574**
EXSP 1.0 .447** .527**
CASS 1.0 .290*
DS 1.0
*p < .05**p < .01
76 K.D. Thompson and D. Bendell
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
depression (EPDS) (Model 1). An SEM-based path analysis was conducted usingAMOS (20.0) (Arbuckle, 2011) to determine whether the data support thehypothesised paths. Estimation of free parameters was achieved using the maximumlikelihood estimation method. Model 1 was tested, with results indicating inade-quate fit (χ2(7, 77) = 32.188, p < .001, CFI = .860, RMSEA = .218). Post-hocmodifications, guided by theoretical considerations, were then performed in anattempt to develop a better-fitting and simpler model.
Given the apparent lack of success of the mediators CASS and STS in theprediction of MAQ and EPDS, the addition of direct paths was considered to replacethese mediated pathways. This was supported by the results from the ModificationIndices provided by AMOS (20.0), which indicated that the deletion of the pathsinvolving CASS and STS along with the addition of direct paths from Self Perceptionand Perfectionism to MAQ would result in improved fit. The direct path from MAQto EPDS was retained, resulting in Model 2 in which MAQ functions as a mediatorbetween the exogenous variables and EPDS. Model 2 was analysed, yielding resultsthat suggest a significantly better fit (χ2(3) = 15.311, p = .002, CFI = .931, RMSEA =.232; χ2 change(4) = 32.188–15.311 = 16.877, p = .002).
In order to attain a more parsimonious model (Model 3), CASS and STS wereremoved entirely and the revised model was re-estimated. Results were as follows:χ2(7, 77) = .891, CFI = 1.000, RMSEA = .000, suggesting that removing CASSand STS did not reduce the fit significantly (χ2 change(4) = 32.188–15.311 =16.877, p = .002).
Model 3 (see Figure 1) was determined to be more parsimonious and offer thebest fit for the data, using the theoretical considerations set forth in the studyproposal. This final model suggests that externalised self-perception and socially
Figure 1. Model. All paths are significant at the p < .001 level. χ2(7, N = 77) = .891, CFI= 1.000, RMSEA = .000.
Journal of Reproductive and Infant Psychology 77
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
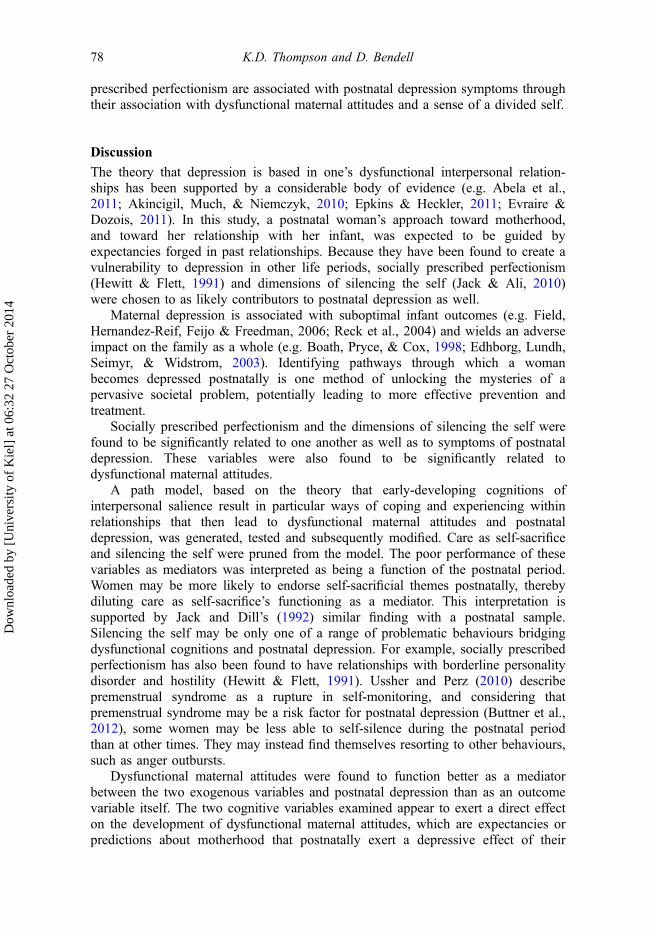
prescribed perfectionism are associated with postnatal depression symptoms throughtheir association with dysfunctional maternal attitudes and a sense of a divided self.
Discussion
The theory that depression is based in one’s dysfunctional interpersonal relation-ships has been supported by a considerable body of evidence (e.g. Abela et al.,2011; Akincigil, Much, & Niemczyk, 2010; Epkins & Heckler, 2011; Evraire &Dozois, 2011). In this study, a postnatal woman’s approach toward motherhood,and toward her relationship with her infant, was expected to be guided byexpectancies forged in past relationships. Because they have been found to create avulnerability to depression in other life periods, socially prescribed perfectionism(Hewitt & Flett, 1991) and dimensions of silencing the self (Jack & Ali, 2010)were chosen to as likely contributors to postnatal depression as well.
Maternal depression is associated with suboptimal infant outcomes (e.g. Field,Hernandez-Reif, Feijo & Freedman, 2006; Reck et al., 2004) and wields an adverseimpact on the family as a whole (e.g. Boath, Pryce, & Cox, 1998; Edhborg, Lundh,Seimyr, & Widstrom, 2003). Identifying pathways through which a womanbecomes depressed postnatally is one method of unlocking the mysteries of apervasive societal problem, potentially leading to more effective prevention andtreatment.
Socially prescribed perfectionism and the dimensions of silencing the self werefound to be significantly related to one another as well as to symptoms of postnataldepression. These variables were also found to be significantly related todysfunctional maternal attitudes.
A path model, based on the theory that early-developing cognitions ofinterpersonal salience result in particular ways of coping and experiencing withinrelationships that then lead to dysfunctional maternal attitudes and postnataldepression, was generated, tested and subsequently modified. Care as self-sacrificeand silencing the self were pruned from the model. The poor performance of thesevariables as mediators was interpreted as being a function of the postnatal period.Women may be more likely to endorse self-sacrificial themes postnatally, therebydiluting care as self-sacrifice’s functioning as a mediator. This interpretation issupported by Jack and Dill’s (1992) similar finding with a postnatal sample.Silencing the self may be only one of a range of problematic behaviours bridgingdysfunctional cognitions and postnatal depression. For example, socially prescribedperfectionism has also been found to have relationships with borderline personalitydisorder and hostility (Hewitt & Flett, 1991). Ussher and Perz (2010) describepremenstrual syndrome as a rupture in self-monitoring, and considering thatpremenstrual syndrome may be a risk factor for postnatal depression (Buttner et al.,2012), some women may be less able to self-silence during the postnatal periodthan at other times. They may instead find themselves resorting to other behaviours,such as anger outbursts.
Dysfunctional maternal attitudes were found to function better as a mediatorbetween the two exogenous variables and postnatal depression than as an outcomevariable itself. The two cognitive variables examined appear to exert a direct effecton the development of dysfunctional maternal attitudes, which are expectancies orpredictions about motherhood that postnatally exert a depressive effect of their
78 K.D. Thompson and D. Bendell
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
own. In the final model (Model 3), socially prescribed perfectionism and externa-lised self-perception develop early in life, leading to a sense of a divided self anddysfunctional attitudes toward motherhood, and culminate in depressive symptomsin the postnatal period (see Figure 1).
The central finding of this study was to provide an extension to the interactionaltheory of depression (Coyne, 1976, 1999), by the observation that dysfunctionalmaternal attitudes and the divided self mediate the relationship between depressivecognitions and postnatal depression. This suggests that the adverse outcomesprecipitated by maternal postnatal depression could be mitigated by targeting themother’s dysfunctional cognitions as early as possible, through therapy andpsychoeducation. Because it appears that postnatal depression is psychologicallysimilar to depression throughout life, these findings support the postnatal use ofestablished depression-focused therapies. The development of new therapies toassist women in creating more adaptive expectations of themselves and their infantsis also recommended, in order to improve interpersonal patterns, depressivesymptoms, and adverse infant outcomes.
Limitations and directions for future research
The creation of the model, while based on theoretical considerations, wasexploratory in nature. The final model has some distinct differences from the modeloriginally proposed. These differences, as well as the cross-sectional nature of thisstudy, suggest that conclusions should be drawn cautiously and that replication isnecessary for full confidence in the findings. In particular, longitudinal studies areneeded to test the appropriateness of the model.
The care as self-sacrifice dimension of self-silencing was not as stronglyassociated with depression as has been found in non-postnatal research. This hasbeen interpreted as postnatal women being generally more likely to endorseself-sacrificial themes. However, this should be interpreted with caution. Futureresearch should keep in mind how sample characteristics may influence thisvariable.
Future research would do well to explore maternal attitudes in multidimensionaland idiographic ways that capture the richness of this construct more fully, and toexplore more fully what types of relational interactions tend to produce maladaptivecognitions.
ReferencesAbela, J., Zinck, S., Kryger, S., Zilber, I., & Hankin, B. (2009). Contagious depression:
Negative attachment cognitions as a moderator of the temporal association betweenparental depression and child depression. Journal of Clinical Child and AdolescentPsychology, 38, 16–26.
Abela, J., Stolow, D., Mineka, S., Yao, S., Zhu, X., & Hankin, B. (2011). Cognitivevulnerability to depressive symptoms in adolescents in urban and rural Hunan, China: Amultiwave longitudinal study. Journal of Abnormal Psychology, 120, 765–778.
Agoub, M., Moussaoui, D., & Battas, O. (2005). Prevalence of postnatal depression in aMoroccan sample. Archives of Women’s Mental Health, 8, 37–43.
Akincigil, A., Much, S., & Niemczyk, K. (2010). Predictors of maternal depression in thefirst year postnatal: Marital status and mediating role of relationship quality. Social Workin Health Care, 49, 227–244.
Journal of Reproductive and Infant Psychology 79
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
Alfaraj, A., Spada, M., Nikcevic, A., Puffett, A., & Meer, S. (2009). Positive beliefs aboutrumination in depressed and non-depressed pregnant women: A preliminary investigation.Journal of Reproductive and Infant Psychology, 27, 54–60.
Ali, A., Oatley, K., & Toner, B. (2002). Life stress, self-silencing, and domains of meaningin unipolar depression: An investigation of an outpatient sample of women. Journal ofSocial and Clinical Psychology, 21, 669–685.
Arbuckle, J.(2011). Amos (Version 20.0) [Computer Program]. Chicago, IL: SPSS.Boath, E., Pryce, A., & Cox, J. (1998). Postnatal depression: The impact on the family.
Journal of Reproductive and Infant Psychology, 16, 199–203.Brenninkmeyer-Davis, C.(2007). Effects of mood states on decision-making and social
perception. Dissertation Abstracts International: Section B: The Sciences andEngineering, 1296.
Buttner, M., Mott, S., Pearlstein, T., Stuart, S., Zlotnick, C., & O’Hara, M. (2012).Examination of premenstrual symptoms as a risk factor for depression in postpartumwomen. Archives of Women’s Mental Health, 16, 219–225.
Cole, D., Ciesla, J., Dallaire, D., Jacquez, F., Pineda, A., LaGrange, B., et al. (2008).Emergence of attributional style and its relation to depressive symptoms. Journal ofAbnormal Psychology, 117, 16–31.
Cox, J., Holden, J., & Sagovsky, R. (1987). Detection of postnatal depression: Developmentof the 10-item Edinburgh Postnatal Depression Scale. British Journal of Psychiatry,150, 782–786.
Coyne, J. (1976). Depression and the response of others. Journal of Abnormal Psychology,85, 186–193.
Coyne, J. (1999). Thinking interactionally about depression: A radical restatement. In T.Joiner, & J. Coyne (Eds.), The interactional nature of depression: Advances in interper-sonal approaches (pp. 365–392). Washington, DC: American Psychological Association.
Deave, T. (2005). Associations between child development and women’s attitudes topregnancy and motherhood. Journal of Reproductive and Infant Psychology, 23, 63–75.
Denis, A., Ponsin, M., & Callahan, S. (2012). The relationship between maternalself-esteem, maternal competence, infant temperament and post-partum blues. Journal ofReproductive and Infant Psychology, 30, 388–397.
Dennis, C., & Ross, L. (2006). Depressive symptomatology in the immediate postnatalperiod: Identifying maternal characteristics related to true- and false-positive screeningscores. Canadian Journal of Psychiatry, 51, 265–273.
Dimitrovsky, L., Levy-Shiff, R., & Schattner-Zanani, I. (2002). Dimensions of depression andperfectionism in pregnant and nonpregnant women: Their levels and interrelationshipsand their relationship to marital satisfaction. The Journal of Psychology, 136, 631–646.
Edhborg, M., Lundh, W., Seimyr, L., & Widstrom, A. (2003). The parent–child relationshipin the context of maternal depressive mood. Archives of Women’s Mental Health, 6,211–216.
Egan, S., Wade, T., & Shafran, R. (2011). Perfectionism as a transdiagnostic process: Aclinical review. Clinical Psychology Review, 31, 203–212.
Epkins, C., & Heckler, D. (2011). Integrating etiological models of social anxiety anddepression in youth: Evidence for a cumulative interpersonal risk model. Clinical Childand Family Psychology Review, 14, 329.
Evraire, L., & Dozois, D. (2011). An integrative model of excessive reassurance seeking andnegative feedback seeking in the development and maintenance of depression. ClinicalPsychology Review, 31, 1291–1303.
Faisal-Cury, A., Tedesco, J., Kahhale, S., Menezes, P., & Zugaib, M. (2004). Postpartumdepression: In relation to life events and patterns of coping. Archives of Women’s MentalHealth, 7, 123–131.
Field, T., Hernandez-Reif, M., Feijo, L., & Freedman, J. (2006). Prenatal, perinatal, and neo-natal stimulation: A survey of neonatal nurseries. Infant Behavior and Development, 29,24–31.
Flett, G., Besser, A., Hewitt, P., & Davis, R. (2007). Perfectionism, silencing the self, anddepression. Personality and Individual Differences, 43, 1211–1222.
Flynn, M., & Rudolph, K. (2011). Stress generation and adolescent depression: Contributionof interpersonal stress responses. Journal of Abnormal Child Psychology, 39, 1187–1198.
80 K.D. Thompson and D. Bendell
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4

Fowles, E. (2010). The relationship between maternal role attainment and postnataldepression. Healthcare for Women International, 19, 83–94.
Gil, S., Teissedre, F., Chambres, P., & Droit-Volet, S. (2011). The evaluation of emotionalfacial expressions in early postnatal depression mood: A difference between adult andbaby faces? Psychiatry Research, 186, 281–286.
Grant, T., Jack, D., Fitzpatrick, A., & Ernst, C. (2011). Carrying the burdens of poverty,parenting, and addiction: Depression symptoms and self-silencing among ethnicallydiverse women. Community Mental Health Journal, 47, 90–98.
Hewitt, P., & Flett, G. (1991). Dimensions of perfectionism in unipolar depression. Journalof Abnormal Psychology, 100, 98–101.
Hewitt, P., Flett, G., Sherry, S., Habke, M., Parkin, M., Lam, R., et al. (2003). Theinterpersonal expression of perfection: Perfectionistic self-presentation and psychologicaldistress. Journal of Personality and Social Psychology, 84, 1303–1325.
Horowitz, J., Damato, E., Duffey, M., & Solon, L. (2005). The relationship of maternalattributes, resources, and perceptions of postnatal experiences to depression. Research inNursing and Health, 28, 159–171.
Hung, C. (2007). Postpartum stress as a predictor of women’s minor psychiatric morbidity.Community Mental Health Journal, 43, 1–12.
Jack, D., & Ali, A. (2010). Silencing the self across cultures: Depression and gender in thesocial world. New York, NY: Oxford University Press.
Jack, D., & Dill, D. (1992). The Silencing the Self Scale: Schemas of intimacy associatedwith depression in women. Psychology of Women Quarterly, 16, 97–106.
Jacobovitz, D., Hazen, N., Curran, M., & Hitchens, K. (2004). Observations of early triadicfamily interactions: Boundary disturbances in the family predict symptoms in depression,anxiety, and attention-deficit/hyperactivity disorder in middle childhood. Developmentand Psychopathology, 16, 577–592.
Josefsson, A., Larsson, C., Sydsjo, G., & Nylander, P. (2007). Temperament and characterin women with postpartum depression. Archives of Women’s Mental Health, 10, 3–7.
Kelly, G. (1963). A theory of personality: The psychology of personal constructs. Oxford:W.W. Norton.
Kendall-Tackett, K. (2007). Violence against women and the perinatal period: The impact oflifetime violence and abuse on pregnancy, postnatal, and breastfeeding. Trauma,Violence, & Abuse, 8, 344–353.
Mayes, L., & Leckman, J. (2007). Parental representations and subclinical changes inpostnatal mood. Infant Mental Health Journal, 28, 281–295.
Mazzeo, S., Landt, M., Jones, I., Mitchell, K., Kendler, K., Neale, M., et al. (2006).Associations among postpartum depression, eating disorders, and perfectionism in apopulation-based sample of adult women. International Journal of Eating Disorders, 39,202–211.
Milgrom, J., & Beatrice, G. (2003). Coping with the stress of motherhood: Cognitive anddefence style of women with postnatal depression. Stress and Health, 19, 281–287.
Murray, L. (2006). The impact of postnatal depression on infant development. Journal ofChild Psychology and Psychiatry, 33, 543–561.
O’Connor, R., & O’Connor, D. (2003). Predicting hopelessness and psychological distress:The role of perfectionism and coping. Journal of Counselling Psychology, 50, 362–372.
O’Neil, J., Wilson, M., Shaw, D., & Dishion, T. (2009). The relationship between parentalefficacy and depressive symptoms in a diverse sample of low income mothers. Journalof Child and Family Studies, 18, 643–652.
Randles, D., Flett, G., Nash, K., McGregor, I., & Hewitt, P. (2010). Rumination andinterpersonal functioning in perinatal depression. Journal of Social and ClinicalPsychology, 29, 646–667.
Reck, C., Hunt, A., Fuchs, T., Weiss, R., Noon, A., Moehler, E., … Mundt, C. (2004).Interactive regulation of affect in postpartum depressed mothers and their infants: Anoverview. Psychopathology, 37, 272–280.
Ross, L., Murray, B., & Steiner, M. (2005). Sleep and perinatal major depressive disorders:A critical review. Journal of Psychiatry and Neuroscience, 30, 247–256.
Rudolph, S., Flett, G., & Hewitt, P. (2007). Perfectionism and deficits in cognitive emotionregulation. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 25, 343–357.
Journal of Reproductive and Infant Psychology 81
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4
Sejourne, N., Alba, J., Onorrus, M., Goutadier, N., & Chabrol, H. (2011). Intergenerationaltransmission of postpartum depression. Journal of Reproductive and Infant Psychology,29, 115–124.
Sherry, S., Law, A., Hewitt, P., Flett, G., & Besser, A. (2008). Social support as a mediatorof the relationship between perfectionism and depression: A test of the socialdisconnection model. Personality and Individual Differences, 45, 339–344.
Stein, A., Craske, M., Lehtonen, A., Harvey, A., Savage-McGlynn, E., Davies, B., et al.(2012). Maternal cognitions and mother–infant interaction in postnatal depression andgeneralized anxiety disorder. Journal of Abnormal Psychology, 121, 795–809.
Stoeber, J., & Yang, H. (2010). Perfectionism and emotional reactions to perfect and flawedachievements: Satisfaction and pride only when perfect. Personality and IndividualDifferences, 49, 246–251.
Tan, J., & Carfagnini, B. (2008). Self-silencing, anger and depressive symptoms in women:Implications for prevention and intervention. Journal of Prevention and Intervention inthe Community, 35(2), 5–18.
Thio, I., & Elliott, T. (2008). Hope, social support, and postpartum depression:Disentangling the mediating effects of negative affectivity. Journal of ClinicalPsychology in Medical Settings, 12, 293–299.
Thompson, J., Whiffen, V., & Aube, J. (2001). Does self-silencing link perceptions of carefrom parents and partners with depressive symptoms? Journal of Social and PersonalRelationships, 18, 503–518.
Ussher, J., & Perz, J. (2010). Gender differences in self-silencing and psychological distressin informal cancer carers. Psychology of Women Quarterly, 34, 228–242.
Warner, R., Appleby, L., Whitton, A., & Faragher, B. (1997). Attitudes toward motherhoodin postnatal depression: Development of the Maternal Attitudes Questionnaire. Journalof Psychosomatic Research, 43, 351–358.
82 K.D. Thompson and D. Bendell
Dow
nloa
ded
by [
Uni
vers
ity o
f K
iel]
at 0
6:32
27
Oct
ober
201
4