derek martinig suzanne lane julia barnscher. fdg (18-fluoro-2-deoxyglucose) – radioactive f in...
TRANSCRIPT

Derek MartinigSuzanne Lane Julia Barnscher
REGULATIONS AND PET TECHNOLOGY


POSITRON EMISSION TOMOGRAPHY
FDG (18-fluoro-2-deoxyglucose) – Radioactive F in place of O in glucose
Fluoride decays back to Oxygen and emits positrons
Cellular consumption of glucose molecules can be observed using a PET scanner
Used for research, cancer, blood clots, Alzheimers

BACKGROUND
1952 – First positron imaging device Mid 70s – First PET scanners using
Fluoride Late 70s – first PET scanners using in
clinical settings 1980s – Research showing clinical utility 1988- U.S.A – Medicare funded first PET
Scan 1992 – Australia’s first PET Facility

BARRIERS
Lack of Personnel High Costs Accessibility of FDG Lack of Standardized Protocols Government Regulations

FDG Radiopharmaceutical drug -
Investigation drug - Biologics and Genetic Therapies Directorate (BGTD) branch of Health Canada
Over 5,000 studies demonstrating safety and benefits of FDG
Support from: Canadian Association of Radiologists Canadian Society of Nuclear Medicine European Association of Nuclear Medicine American Society of Nuclear Medicine

The power of PET over traditional imaging modalities
CASE STUDIES

CASE STUDY #1
72 year old Male Diagnosed with
Esophageal Tumor CT scan revealed
abnormality in distal esophagus
Treatment Plan: radiation & chemo. then Surgery

PET/CT Imaging revealed two undiagnosed lymph nodes
Staging and treatment volume were both altered.
Studies found that up to 62% of treatments were adjusted as a result of a PET Scan

CASE STUDY #2
•82 year old female with Rectal Bleed•Mass found in Right transverse colon during colonscopy•CT performed and revealed mass in presacral area•Liver was unremarkable on CT Scan•Patient underwent colectomy and 8 out of 9 nodes tested were positive for metastases
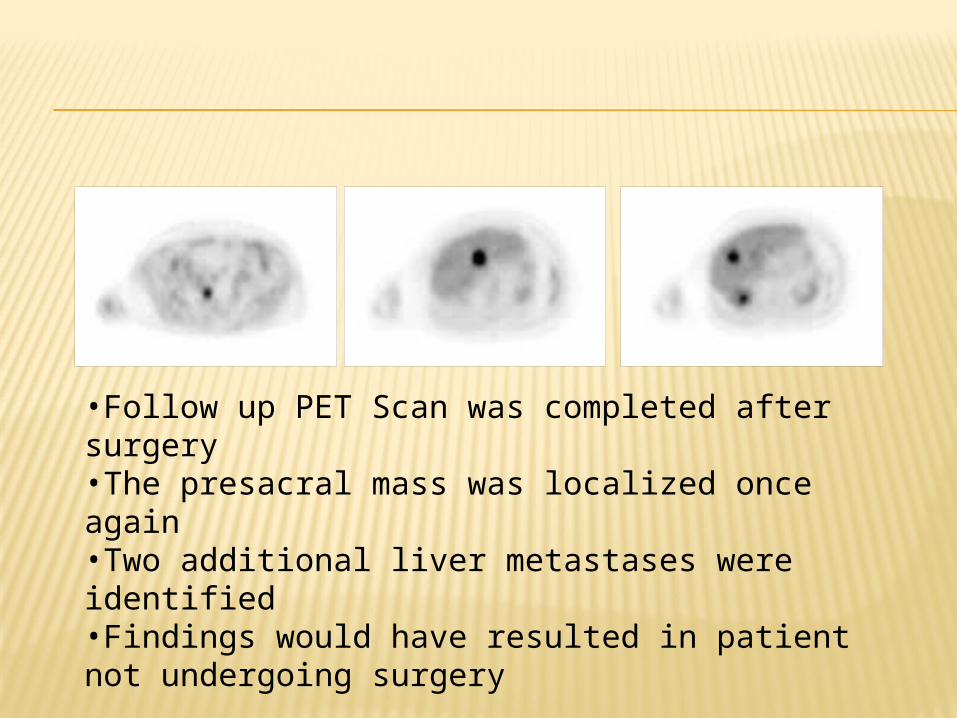
•Follow up PET Scan was completed after surgery•The presacral mass was localized once again•Two additional liver metastases were identified•Findings would have resulted in patient not undergoing surgery

REGULATION OF FDG IN CANADA

REGULATION OF FDG
Regulations changed in 2003
Approval for production and use of FDG by BGTD New drug submission 4 manufacturers
approved for limited uses Non approved uses
must be carried out under clinical trial applications

PET SCANNING IN CANADA
Limited number of funded scans per province Not related to size of population or
availability of scanning facilities Not available in all provinces Public and private not equivalent Up to 6 week waiting period

PET SCANNING IN CANADA
Canada approves scans for fewer conditions than other countries US, European Union, Australia Lung, breast, colorectal cancers
Revisions suggested as of March 2009 Will not have any rapid effect to increase
availability of FDG

Those impacted by the Current Regulations on PET in Canada
WINNERS AND LOSERS


RESEARCHERS
Pros:Still Pending....
Cons:-”Brain Drain” still exists as a result of limitations on research(6 months in US, 3 years in Canada)
-Costly and time consuming clinical trials
-Redundancy of research
-Lack of motivation to continue with research in the field.

PROVINCIAL GOVERNMENTPros:-Limit initial healthcare spending-Capital Investments-Exam Reimbursement
Cons:-Less cost-effective-Reduction in Surgeries-More effective treatment regiments-Perception of not providing best possible care.

MANUFACTURERS
Pros: Monopoly Power....really?Cons: Expensive licensing costs & Low demand lead to Inability to control pricing

PATIENTS


DOESN’T MATTER HOW YOU SPIN IT...

.... EVERYONE’S STILL A LOSER

What needs to be done to fix this problem...
REGULATION REFORM

THREE STEP PROCESS

STEP ONE
Remove the Clinical Trial Label
Eliminate Redundancy of NDS
Provide Guidelines for Production of FDG
_____________________ Result in Increased
Provision!

STEP TWO
Collaboration of College of Physicians and Government
Set Fee Structure Cover cost of PET
under provincial health plans
_____________________ Resulting in Increased
Utilization and Provision

STEP THREE
Advertising and Promotion of PET
Increase Physician Awareness
Increase Patient Awareness
Increase Research_____________________ Optimal Utilization
of PET


QUESTIONS??