derm 1 final - ask doctor · pdf file• tx – if necessary, for smaller lesions...
TRANSCRIPT

DERMATOLOGY
Samantha Dye &
Salwa Elmamoun

DESCRIPTIVES• ERYTHEMA ‐ Increased perfusion
• PLAQUE ‐ Flat topped disc
• MACULE ‐ Flat area of discolouration
• PAPULE ‐ <1cm of elevated skin
• NODULE ‐ >1cm palpable mass
• VESICLE ‐ Blister <5mm
• BULLA ‐ Blister >5mm
• PUSTULE ‐ Blister containing pus
• SCALE ‐ Flaky keratin
• CRUST ‐ Dried exudate
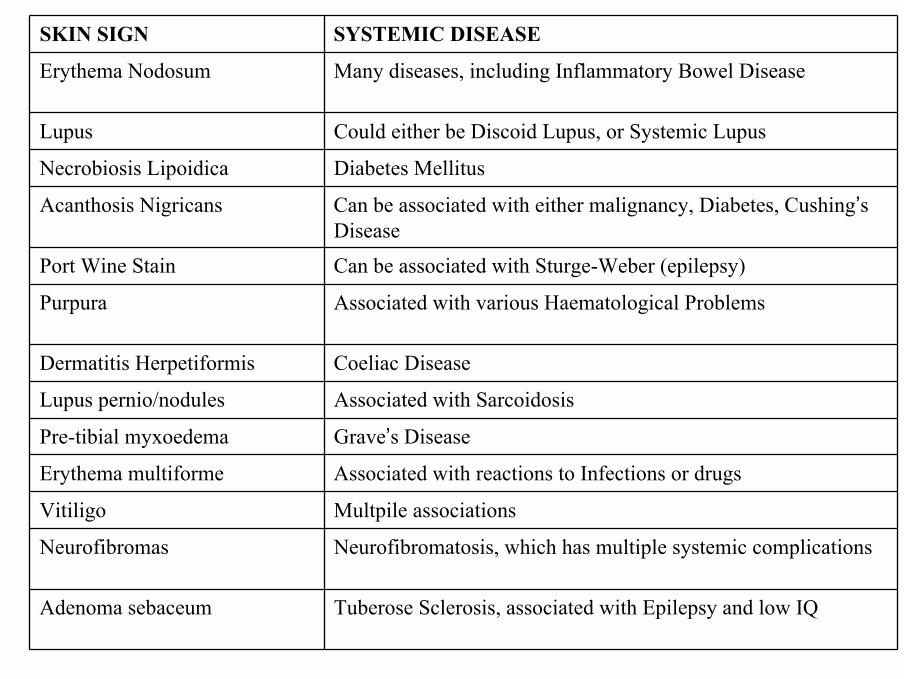
SKIN SIGN SYSTEMIC DISEASE
Erythema Nodosum Many diseases, including Inflammatory Bowel Disease
Lupus Could either be Discoid Lupus, or Systemic Lupus
Necrobiosis Lipoidica Diabetes Mellitus
Acanthosis Nigricans Can be associated with either malignancy, Diabetes, Cushing’s Disease
Port Wine Stain Can be associated with Sturge-Weber (epilepsy)
Purpura Associated with various Haematological Problems
Dermatitis Herpetiformis Coeliac Disease
Lupus pernio/nodules Associated with Sarcoidosis
Pre-tibial myxoedema Grave’s Disease
Erythema multiforme Associated with reactions to Infections or drugs
Vitiligo Multpile associations
Neurofibromas Neurofibromatosis, which has multiple systemic complications
Adenoma sebaceum Tuberose Sclerosis, associated with Epilepsy and low IQ
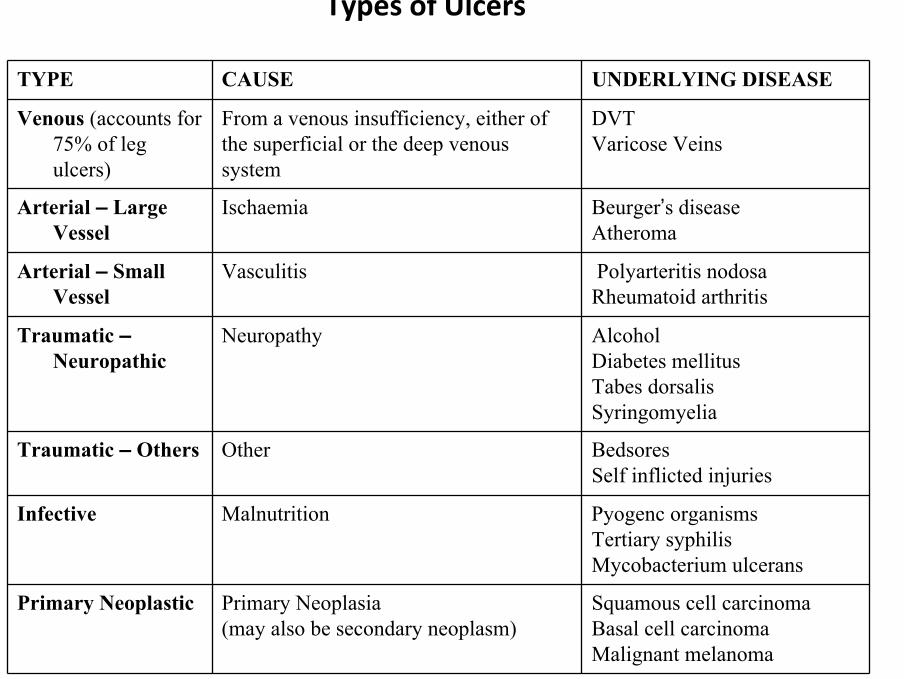
TYPE CAUSE UNDERLYING DISEASE
Venous (accounts for 75% of leg ulcers)
From a venous insufficiency, either ofthe superficial or the deep venoussystem
DVTVaricose Veins
Arterial – Large Vessel
Ischaemia Beurger’s diseaseAtheroma
Arterial – Small Vessel
Vasculitis Polyarteritis nodosaRheumatoid arthritis
Traumatic –Neuropathic
Neuropathy AlcoholDiabetes mellitusTabes dorsalisSyringomyelia
Traumatic – Others Other BedsoresSelf inflicted injuries
Infective Malnutrition Pyogenc organismsTertiary syphilisMycobacterium ulcerans
Primary Neoplastic Primary Neoplasia(may also be secondary neoplasm)
Squamous cell carcinomaBasal cell carcinomaMalignant melanoma
Types of Ulcers

DISTINGUISHING BETWEEN ISCHAEMIC AND NEUROPATHIC ULCERS
ISCHAEMIC ULCER NEUROPATHIC ULCER
PAINFUL? Painful Painless
ASSOCIATED BLACK ESCHAR?
Present Absent
TEMPERATURE? Cold Warm
SENSATION? Intact Lost
DISTINGUISHING BETWEEN RAISED EDGED/NEOPLASIC ULCERS
BASAL CELL CARCINOMA
SQUAMOUS CELL CARCINOMA
EDGE Raised Usually everted as well as raised
COLOUR Described as a pink, pearly glistening colour. (due to the fine telangiectasia)
Reddy-brown colour (due to vascularity)
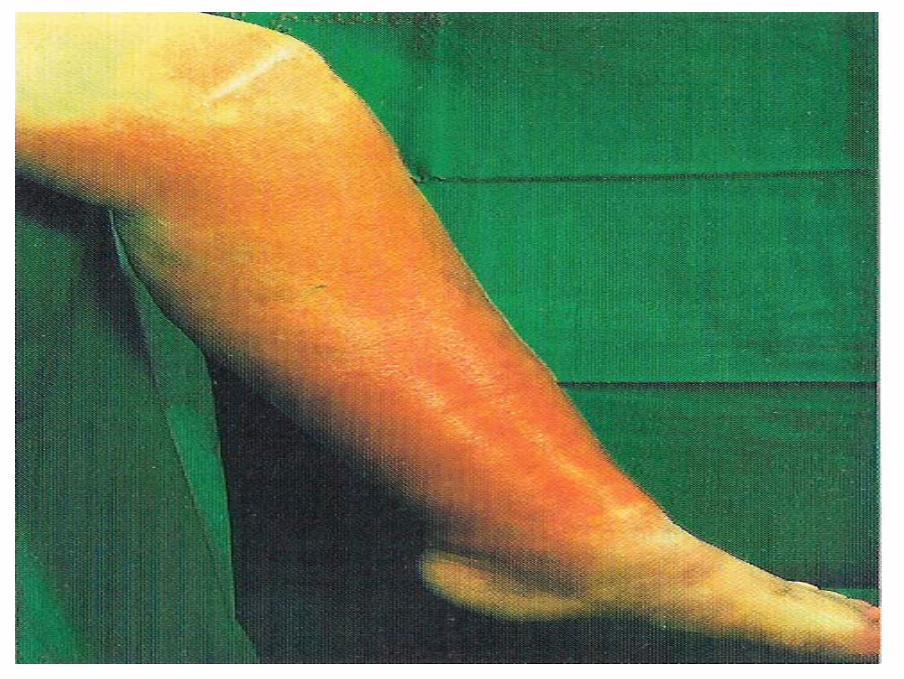
CELLULITIS• INFECTION OF SKIN AND SUBCUTANEOUS TISSUES
• Caused by Streptococcus Pyogenes
• Predisposing factor – leg oedema
• The effected area – Erythematous, hot, swollen, occasionally with blisters and necrosis
• Patient – pyrexial, unwell, with rigors in elderly (toxic confused state)
• Treatment ‐ strict bed rest
‐ parental Penicillin
‐ recurrent episodes and oedmea – prophylactic Penicillin V or Erythromycin

FOLLICULITIS
• STAPHYLOCOCCAL INFECTION
• Infection of superficial part of hair follicle, with Staph. Aureus
• Description – small pustule on an erythematous base, centred on a follicle

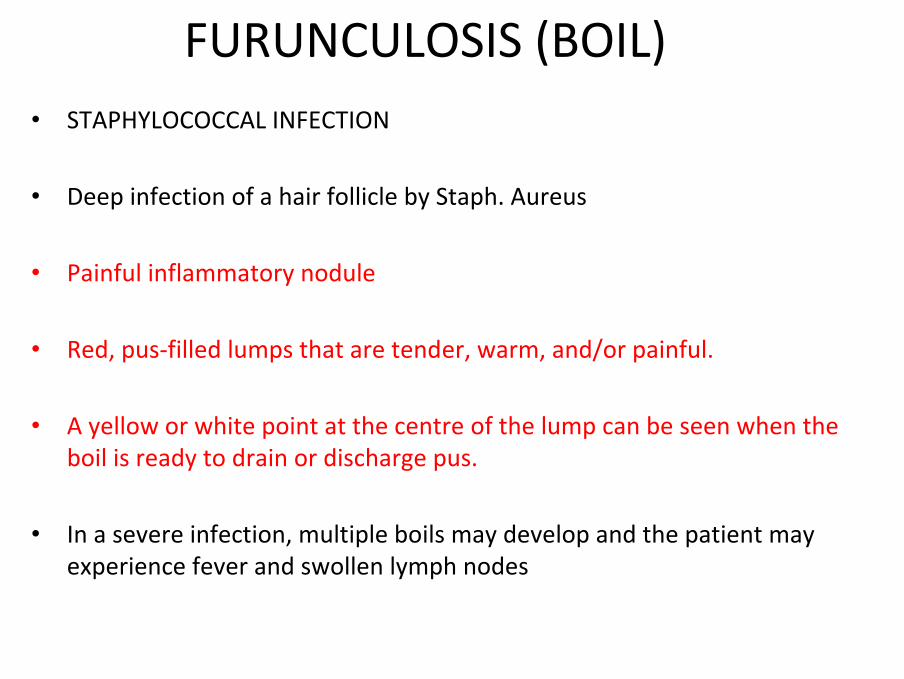
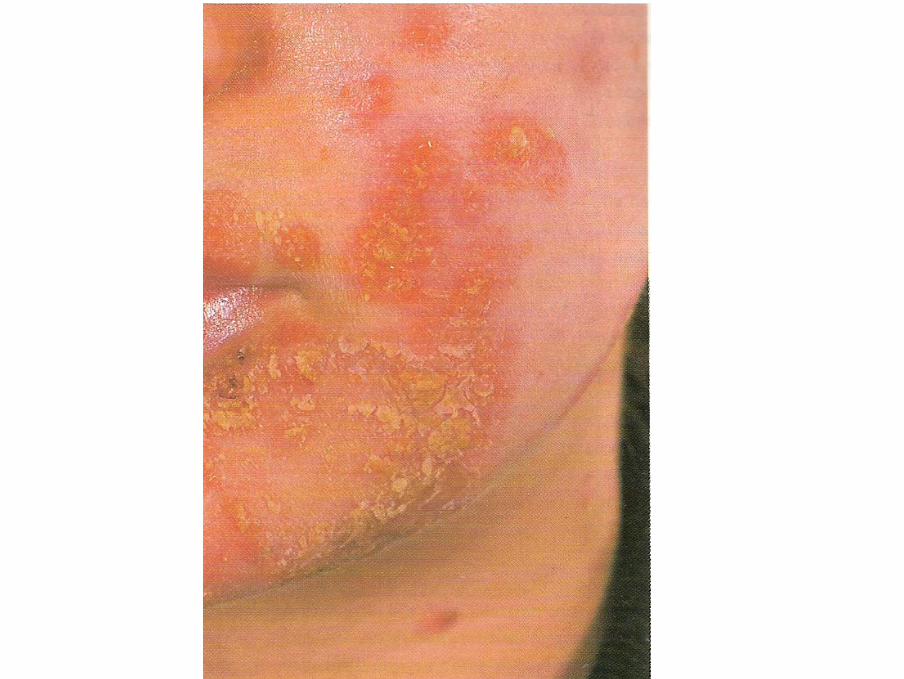
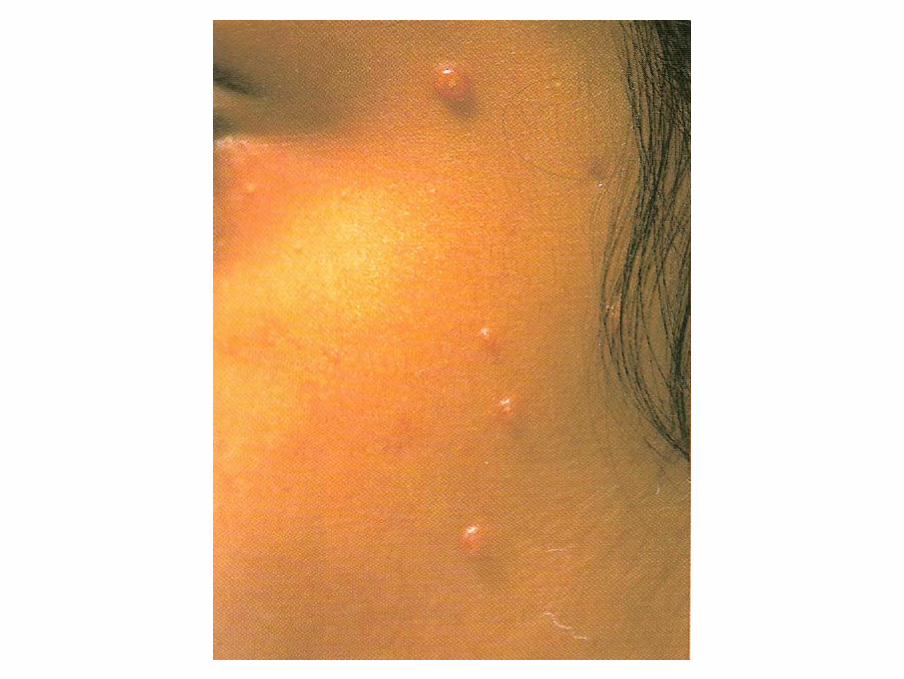
FURUNCULOSIS (BOIL)• STAPHYLOCOCCAL INFECTION
• Deep infection of a hair follicle by Staph. Aureus
• Painful inflammatory nodule
• Red, pus‐filled lumps that are tender, warm, and/or painful.
• A yellow or white point at the centre of the lump can be seen when the boil is ready to drain or discharge pus.
• In a severe infection, multiple boils may develop and the patient may experience fever and swollen lymph nodes

CARBUNCLE• STRAPHYLOCOCCUS
• Deep infection of a group of adjacent hair follicles with Staph. Aureus
• Dome shaped area of tender erythema
• Pus discharging from multiple follicular orifices after a few days

IMPETIGO• Superficial infection by Staphylococcal Aureus with or without haemolytic
streptococci
• Initial lesion – small pustule which rapidly increases in size and ruptures to leave a raw exuding surface
• GOLDEN CRUSTED LESIONS / RASH
• Tx – Flucloxicillin or Erythromycin, and antibacterial agents on localised areas


LUPUS VULGARIS• Due to Mycobacterium infection
• Lesions typically found on head and neck
• Red/brown, nodular plaque with a scaly surface
• When pressed with a glass slide the brown nodules more easily seen as ‘apple‐jelly nodules’
• Tx – standard anti‐tuberculosis therapy (Rifampicin, Isoniazid, Pyrazinamide)
• Risk of Squamous Cell Carcinoma with long‐standing Lupus Vulgaris

LEPROSY (Hansen’s Disease)• Disease of peripheral nerves that affects the skin and possibly the eyes, URT
mucosa, bones and testis.
• Caused by Mycobacterium Leprae (leprosy bacillus)
• Skin lesions are single, or few in number well defined,macules or papules which are hypopigmented in dark skin
• Lepromin test is strongly positive
• Bacilli not seen on modified Ziehl‐Nielsen straining
• SPECTRUM – Lepromatius (extensive lesions and involvement of organs, negative lepromin test, Tx‐ Dapsone, Rifampicin, Clofazimine)
‐ Borderline (scattered lesions)‐ Tuberculoid (1 or 2 skin lesions, good cell mediated immune
response, +ve Lepromin test, Tx – Dapsone and Rifampicin)


WARTS• Raised, cauliflower‐like lesions which occur most frequently on the hands
• Scattered, grouped or periungual (around the nail, involving the nail folds) in distribution
• Tx – resolve spontaneously, but can used wart paints or Cryotherapy


GENITAL WARTS• CAUSED BY THE HUMAN PAPILLOMA VIRUS
• Increased risk of Penile and Cervical Cancer
• Lesions vary from tiny flat patches on vulval skin to small papilliform (cauliflower like) swellings
• Usually multiple and may affect the cervix – CIN?
• Treatment through GUM to detect coexisting STIs and trace contacts and examine them
• Tx ‐ Topical Podophyllin (not on cervix as possibly teratogenic)‐ Cryotherapy‐ Electrocautery for resistant warts
Recurrence rates up to 25%

MOLLUSCUM CONTAGIOSUM• Caused by POX virus
• Pearly pink papules with central umbilication (pit or naval like depression)filled with a horny plug
• Can affect anywhere but more common on head and neck and trunk
• Tx – resolve spontaneously• Children – parents can squeeze each lesion to express central plug to help speed the
resolution
• Adults – Cryotherapy
• No anti‐viral agent
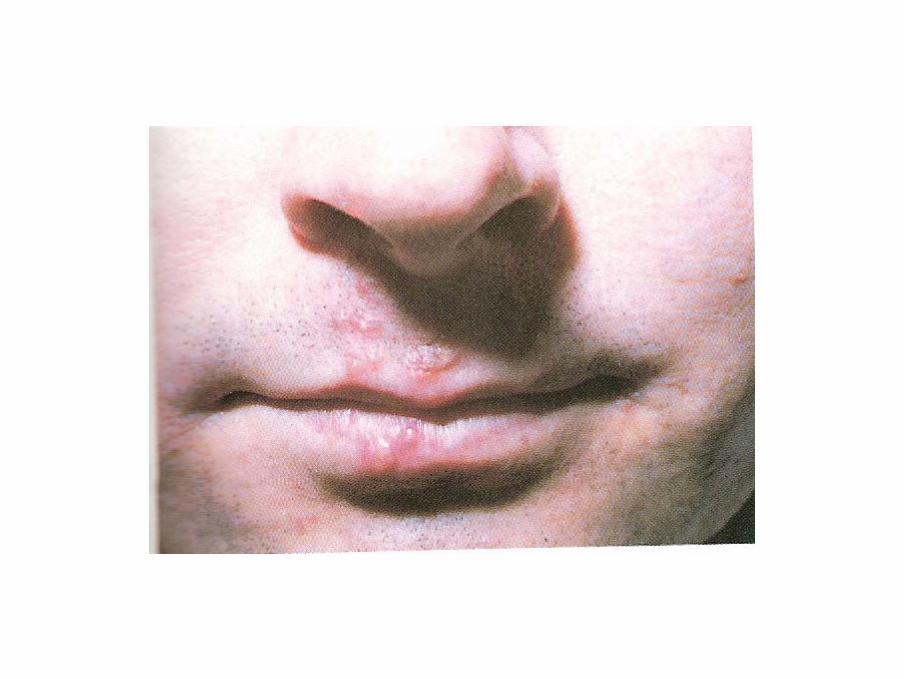
HERPES SIMPLEX• TYPE 1 – ‘Cold sore on lips and face’
• TYPE 2 – Genital herpes
• Initial contact with virus usually in early childhood, lesions usually mild and not noticed
• Following primary infection the virus settles in sensory ganglia and may be triggered to produce recurrent lesions by a variety of stimuli
• Recurrent cold sores in lips are common and resolve spontaneously or helped by topical Aciclovir
• Small vesicle preceded by itching and discomfort, the vesicles burst and the lesion crusts over and resolves within 10‐14 days


HERPES ZOSTER (Shingles)• Chicken pox and shingles caused by the VARICELLA ZOSTER virus
• Following chicken pox the virus remains dormant in dorsal root ganglia until some stimulus activates it and causes shingles attack
• Usually affects and single dermatone
• Eruptions may be preceded by pain in region of dermatone
• Lesions – unilateral band of grouped vesicles on an erythematous base, contents of vesicles are clear but subsequently become cloudy
• Tx ‐ resolve spontaneously (after an few days the vesicles dry up and formcrusts)
‐ In elderly takes longer to heal due to erosive changes‐ Persistence of pain after resolution is termed Post‐Herpetic Neuralgia


TRIGEMINAL ZOSTER
• HERPES ZOSTER AFFECTING A DIVISION OF THE TRIGEMINAL NERVE
• Unilateral band of grouped vesicles on an erythematous base, contents of vesicles is clear but subsequently become cloudy; if affecting the eye, causing peri‐orbital oedema
• Most commonly the Ophthalmic Zoster
• Can present with Conjuncitivits, Keratitis and / or Iridocyclitis if nasocilliary branch of ophthalmic division affected
• Need to refer to eye clinic


SCABIES• Caused by the mite SARCOPTES SCABIE through physical contact
• The female scabies mite burrows in the epidermis and lays eggs in the burrow behind her
• After 4‐6 weeks hypersensitivity to the mite faeces develops and itching begins –the burrow excoriates and mites and eggs destroyed
• Burrows characteristically on hands and feet, sides of fingers and toes, web spaces, wrists and insteps
• Rash – tiny inflammatory papular rash grouped together, with excoriations secondary to bacterial infection
• Tx – Benzylbenzoate emulsion, Lindane lotion, Monosulfiram solution, Aqueous Malathion, 5% Permethrin cream, topical anti‐pruiritc cream for residual itchy areas
• Explain also need for family members and close physical contacts tx


SEBORRHOEIC KERATOSES• Flat topped area of skin with a stuck‐on appearance
• May be pale, but are often pigmented, some deeply
• Surface is often greasy, with small surface pits and irregularities, giving the surface a granular look
• Sites – head, neck, back of hands, forearms, trunk
• Usually a straight forward diagnosis but sometimes mistaken for malignant melanomas
• Tx – If necessary, for smaller lesions cryotherapy, for larger lesions curettage and cautery or excision
With thanks to the authors and publishers:
Robin Graham‐Brown, Tony Burns. Lecture Notes on Dermatology, 7th Ed. UK: Blackwell Publishing Ltd, 1996 – (Images from pages 26, 30, 40, 57, 80, 90, 120, 123, 126, 127,133, 135, 136, 138, 139, 153, 154, 162, 197, 201, plus purple tables and boxes from pages 130, 140, 137, 138, 140, 203)
JAA Hunter, JA Savin, MV Dahl. Clinical Dermatology, 2nd Ed. UK: Blackwell Publishing Ltd, 1996 – (Images from pages 68, 110, 152, 153, 157, 160,162, 173, 174, 179,180, 198, 199, 221, 222, 223, 227, 230, 232, 242, 243, 130)
All images are copyright and reproduced by kind permission of the authors and publishers