dermatology: challenges for primary care nurses · dermatology: challenges for primary care nurses...
TRANSCRIPT

Dermatology: Challenges for primary care nurses
Karen Stephen
Lead Dermatology Nurse
NHS Tayside

Declaration of interests
I have received fees from:
• GSK
• Bayer Healthcare
• Abbvie Ltd
• Janssen-Cilag Ltd
• Celgene Ltd
• Leo Pharma

What are the Dermatology challenges in primary care? • >2000 Dermatology diseases
• Each year 54% of the population is affected by skin disease
• Skin diseases represent 34% of disease in children
• Atopic Eczema affects 20% of infants
• Hand eczema is one of the most common reasons for disablement benefit in the UK
(www.bad.org.uk. Kings fund press release 30/4/15)
• Approximately 13million GP consultations for skin conditions a year in England and Wales
(Kings Fund Dermatology report 2015)
Aim
• Identify the diagnosis criteria for different types of eczema
• Discuss practical tips for topical treatments for eczema
• Explore how to ensure a consistent approach to this long term condition

Eczema
• “Eczema’ is a term which comes from the Greek word ‘to boil’ and is used to describe red, dry, itchy skin which can sometimes become weeping, blistered, crusted, scaling and thickened. The words eczema and dermatitis mean the same thing”
(http://www.bad.org.uk/shared/get-file.ashx?id=69&itemtype=document)

Types of Eczema/Dermatitis
• Atopic Eczema
• Discoid Eczema
• Sebhorrhoeic Eczema
• Contact Eczema
• Hand Eczema
• Pompholyx excema
• Varicose Eczema

Atopic Eczema
• Atopic Eczema is the most common form of Eczema
• Can affect people at any age but most common in children
• Affects 1 in 5 children in the UK
• The term ‘atopic’ is used to describe a group of conditions which include asthma, eczema and hay-fever.
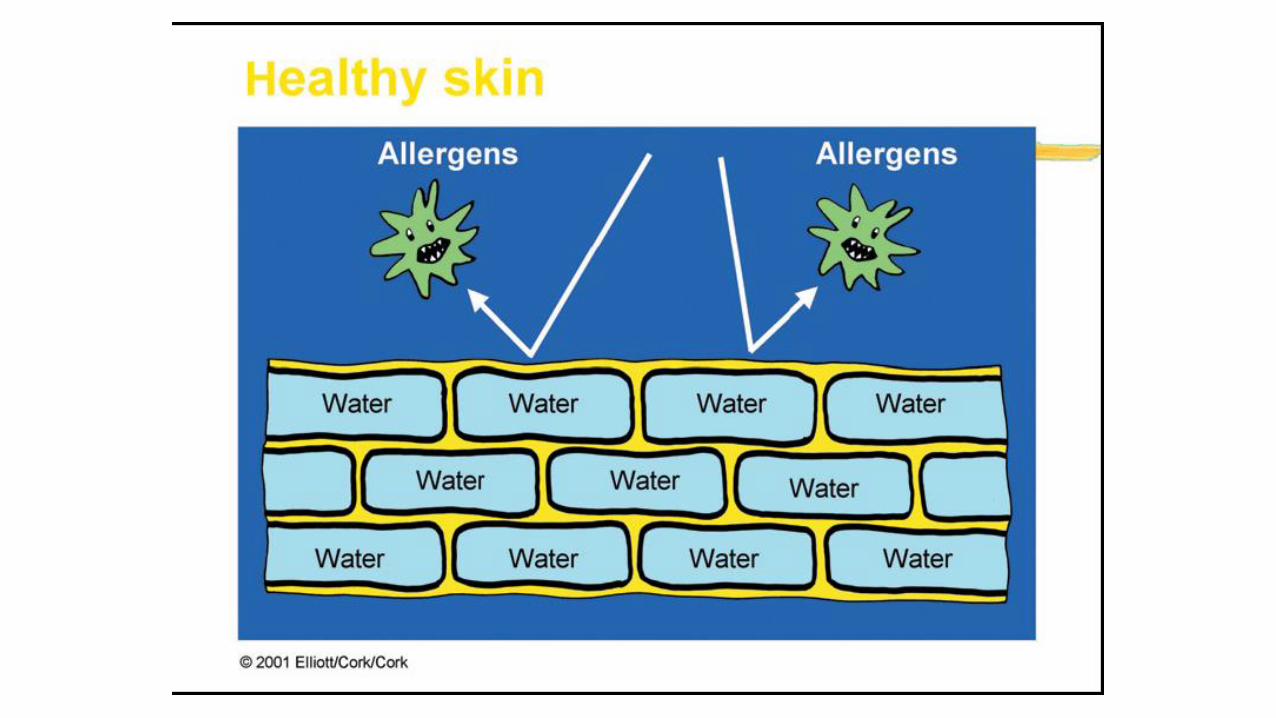
• The cause is complex but includes: • Defect in skin barrier
• Abnormalities in the normal inflammatory and allergy responses

Atopic eczema
•Eczema can be acute or chronic
•weeping
•crusting
•scaling
•lichenification
•excoriated (scratched)
•inflammation

Discoid Eczema (nummular)
• Discoid means disc-shaped, nummular meaning coin-shaped
• Slightly more common in men than in women
• Can affect any age but more commonly seen in adults
• Intensely itchy condition
• Often becomes infected
• Mostly affect limbs but can be seen on the trunk
• Unknown cause

Discoid eczema – differential diagnosis
Psoriasis
Tinea Corpis

Seborrhoeic eczema
• ‘Seborrhoeic’ means that this type of eczema affects greasy (sebaceous) skin zones such as the face, scalp and centre of the chest
• About 4% of the population are affected
• Dandruff (which is mild seborrhoeic dermatitis of the scalp) can affect almost half of all adults.
• Cradle cap in babies is a type of Seborrhoeic eczema
• In adults it is slightly more common in men
• Sometimes associated with Psoriasis and is then known as Sebopsoriasis
Seborroeic Eczema
• Thought to be triggered by an overgrowth of a harmless yeast called Malassezia that lives on the skin, or an overreaction by the skin’s immune system to this yeast.
Contact Eczema
• Caused by the skin being in contact with something in the environment
• Allergic contact eczema
• Irritant contact eczema (most commonly seen on hands)
• More commonly seen in patients who are Atopic
• Often a clear cut off
• Can cause pompholyx eczema

Patch testing
• Test for allergic contact eczema
• Patches applied usually to the back
• Left in place for 48hrs
• Initial readings at 48hrs
• Final readings at 96hrs

Hand Eczema
• Hand eczema is very common, can affect 1 in 20 people
• Can start at any age but more common in adults
• More common in those with atopic eczema
• Can be irritant, allergic or unknown cause
• Often becomes infected
• Hyperkeratotic eczema can look very similar to Psoriasis
• If affecting only one hand test for tinea infection
• Fissures can be very painful
• More common in healthcare professionals, hairdressers, catering etc

Pompholyx eczema
• A type of eczema affecting hands and/or feet
• Characterized by tiny vesicles or bullae (blisters)
• Intensely itchy
• Usually affects adults
• More common in women
• 50% have atopic eczema
• Many possible causes – heat, stress, irritants, allergy, infecion

Varicose/venous/gravitational eczema
• Affects one or both lower legs
• Associated with venous insufficiency
• More common in middle and older age
• Can be associated with: • History of deep venous thrombosis in affected limb
• History of cellulitis in affected limb
• Chronic swelling of lower leg, aggravated by hot weather and prolonged standing
• Varicose veins
• Venous leg ulcers

Varicose/venous/gravitational eczema
• Treatment should always include treatment of venous insufficiency as well as skin treatment

Eczema Treatments • Avoid irritants and allergens
• Emollients
• Topical steroids
• Bandages
• Education/advice
• (Immunomodulators, Antihistamines, Phototherapy, Systemic therapies)

Emollients
• Soap substitutes – bars, creams, lotions, ointments, washes
• Bath/shower additives – oils, gels, lotions
• Topical substances – lotions, creams, ointments, gels
Enhanced emollients
For very dry skin •Urea – e.g. Eucerin, calmurid, Hydromol intensive To reduce secondary infection •Antimicrobial agents – e.g. Dermol Anti-itch •Laurylmacrogol – e.g. Balneum plus
Why do we use emollients?
• To restore the barrier function
• Reduce itch
• Soothe the skin
• Moisturise and lubricate
• Reduce Steroid Use

Practical tips
• Use a complete emollient regime
Bath/shower, Soap Substitute, Topical Preparations
• Choose preparations to suite body site, lifestyle, skin dryness
• After bathing, pat dry and apply emollient immediately to trap water
Practical Tips
• Apply in a downward direction with hair growth do not rub
• Apply regular topical emollients at least twice daily, more frequently if skin very dry
• Use generously - approximately 500gms per week for an adult, 250-500gms for a child
Practical tips
• Ointments – more moisturising, can be messy, good for very dry skin, use tubular bandage to cover
• Creams – less moisturising need to be applied more regularly, good for
hot, inflamed skin (can be kept in fridge), less messy • Lotions – least moisturising, good for hairy areas or as soap substitute

Practical Tips
• Pump dispensers are more hygienic and avoid unnecessary waste through disposal – Use until finished
• Single patient use for all topical therapies
• Aqueous cream should be avoided due to potential irritation (SLS)

Topical Steroid Therapy
• SAFE WHEN USED APPROPRIATELY
• Come in different potency
• Only mild steroids to face or flexures
• Should only be used for short periods
• Should only be used when skin is inflamed or itchy
• Follow steroid dosage charts

Topical Corticosteroids
Mild
Moderate
Potent
Very Potent
1% Hydrocortisone Modrasone,
Clobetasone Butyrate
0.05%
Mometasone Furoate
0.1%, Betamethasone
Valerate 0.1%
Clobetasol Propionate
0.05%
To reduce
inflammation
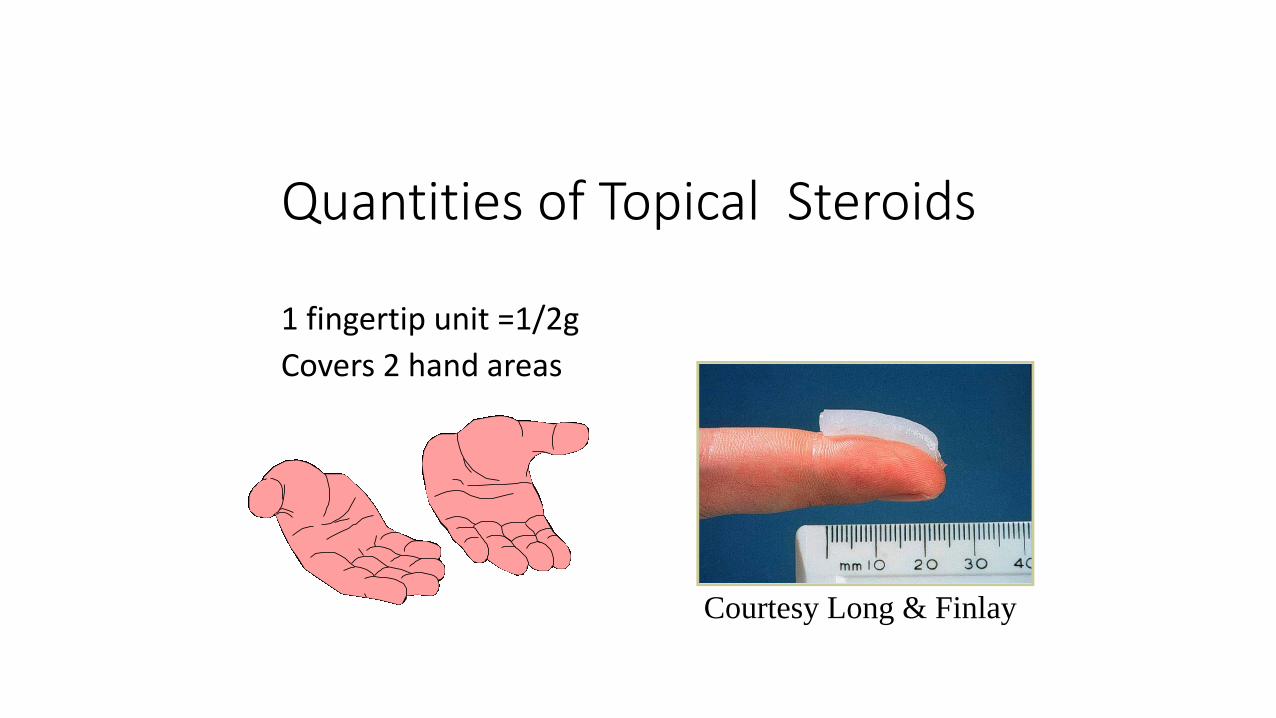
Quantities of Topical Steroids
1 fingertip unit =1/2g
Covers 2 hand areas
Courtesy Long & Finlay

Medicated Bandages

Tubular bandages

How do we ensure consistency
• Education and support
• Use of information leaflets e.g. National Eczema Society (NES), BAD, Dermnet
• Individualised treatment plans
• Refer to local and national guidelines • NICE guideline 57 – Eczema in under 12s
• Sign 125 – Management of Atopic Eczema in Primary care
• PCDS – Guideline for the management of Atopic Eczema

Useful websites
• www.bdng.org.uk – British Dermatological Nursing Group membership,journals, sub-group, study days
• www.bad.org.uk - British Association of Dermatologists information leaflets
• www.dermnetnz.org – New Zealand Dermatologist Association information leaflets
• www.eczema.org – national Eczema Society
• www.pcds.org.uk – Primary Care Dermatology Society

Thank you