dermatology quiz and case discussion gloves and socks synd
DESCRIPTION
MedicalTRANSCRIPT
7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 1/21
Dermatology Quiz and Case Discussion
From The Child's Doctor, Fall 2004
Anthony J. Mancini, MD
Head, Dermatology, Ann & Robert H. Lurie Children's Hospital of Chicago; Professor of
Pediatrics and Dermatology, Northwestern University Feinberg School of MedicineDisclosure: Dr. Mancini has no industry relationships to disclose and does not refer to products that are still
investigational or not labeled for the use in discussion.
Daniela Russi, MD
Fellow, Pediatric Dermatology, Children's Memorial HospitalDisclosure: Dr. Russi has no industry relationships to disclose and does not refer to products that are still
investigational or not labeled for the use in discussion.
Other Disclosure Information
Educational objectives
At the conclusion of this activity, participants will be able to:
Recognize the exanthematous disorder presented in the photographs
Describe the epidemiologic concerns associated with the causative agent
Evaluate the associated findings and relate the course of the disease
CME credit
Credit statement
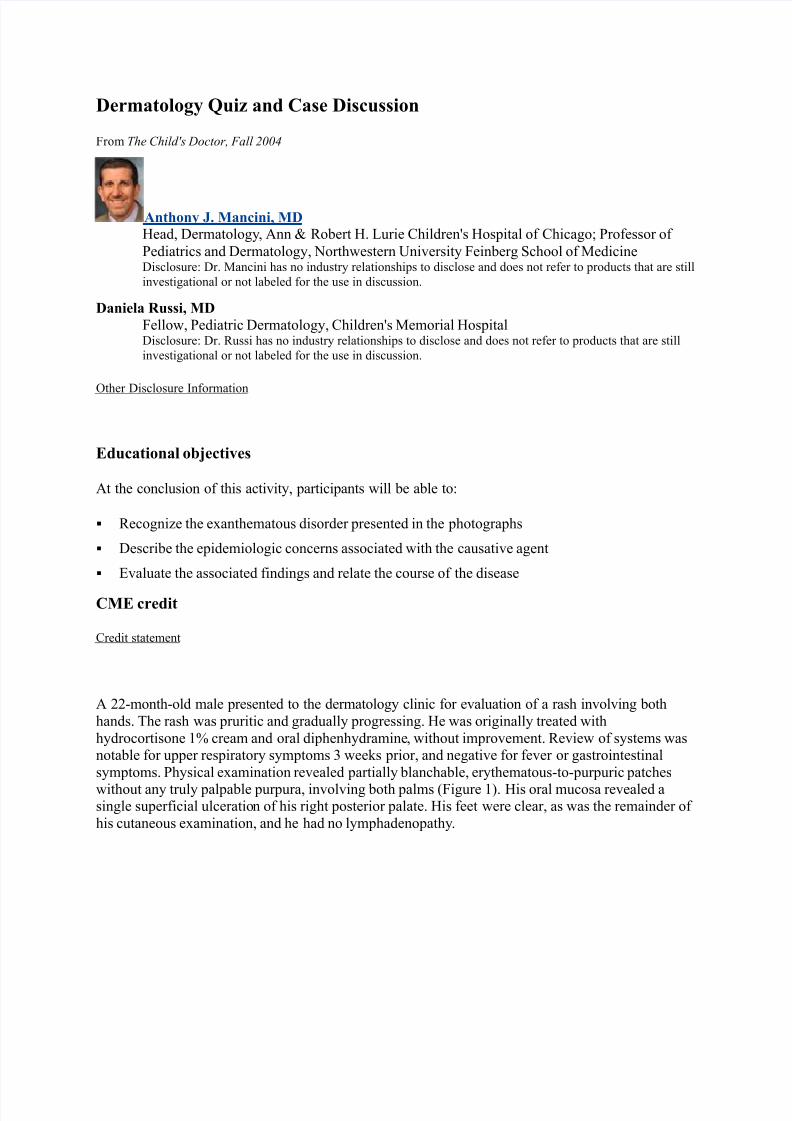
A 22-month-old male presented to the dermatology clinic for evaluation of a rash involving both
hands. The rash was pruritic and gradually progressing. He was originally treated with
hydrocortisone 1% cream and oral diphenhydramine, without improvement. Review of systems wasnotable for upper respiratory symptoms 3 weeks prior, and negative for fever or gastrointestinal
symptoms. Physical examination revealed partially blanchable, erythematous-to-purpuric patches
without any truly palpable purpura, involving both palms (Figure 1). His oral mucosa revealed asingle superficial ulceration of his right posterior palate. His feet were clear, as was the remainder of
his cutaneous examination, and he had no lymphadenopathy.

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 2/21
One week later, a 9-month-old male was referred to the dermatology clinic for a rash involving his
hands and feet. His skin eruption was associated with pruritus, and he had had low grade fevers andupper respiratory symptoms for 2 days. Physical examination revealed petechial, erythematous patches of the palms and soles (Figure 2). The remainder of his physical examination wasunremarkable, including a normal oral mucosal examination and the absence of lymphadenopathy.
What is the most likely diagnosis in both patients?
a. Palmoplantar hidradenitis
b. Hand-foot-and-mouth disease
c. Papular-purpuric gloves and socks syndrome
d. Rocky Mountain spotted fever
Answer: C
Discussion:
Papular-purpuric gloves and socks syndrome (PPGSS) is an acute, self-limited condition initially
described in 1990. The characteristic features include purpuric erythema involving the hands and feet
(especially palms and soles) in a “glove and stocking” distribution. It is occasionally associated with

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 3/21
fever and oral lesions. Serological studies have revealed that the vast majority of patients withPPGSS have IgM antibodies to parvovirus B19 (B19). Other infectious agents that have been
proposed in association with PPGSS include human herpesvirus 6 (HHV6), human herpesvirus 7
(HHV7), measles virus and cytomegalovirus. PPGSS occurs most often during the spring andsummer months.
The incubation period in PPGSS is around 10 days. Skin manifestations are quite characteristic, and
begin with edema and erythema symmetrically localized to the hands and feet. Subsequently, petechial and purpuric changes appear, and vary from a few millimeters in diameter to larger,
confluent patches. Pruritus, tingling, and pain may be reported by the patient. Polymorphous lesions(usually small erosions) of the oral cavity may be present, affecting the hard and soft palate, pharynx,
tongue, and inner aspects of the lips. Other occasionally reported signs and symptoms include fatigue, headache, anorexia, arthralgias and lymphadenopathy. Low grade fever is common, often
developing 2 to 4 days following the onset of the rash, and usually not exceeding 38.5 degreesCelsius.
Laboratory findings in patients with PPGSS are variable, and depend upon the specific etiologic
agent. Hematologic findings may include mild and transient abnormalities, including anemia,neutropenia, eosinophilia, monocytosis and thrombocytopenia. In addition, elevation of hepatic
transaminases, C-reactive protein, and erythrocyte sedimentation rate have been observed. Skin biopsies, which are rarely necessary, have revealed nonspecific histopathologic features, includinglymphocytic perivascular infiltrates, edema, and erythrocyte extravasation within the papillarydermis. Direct immunofluorescence studies have shown deposits of immunoglobulin and C3 in a
granular pattern within papillary dermal vessel walls, and B19 DNA has been demonstrated in skin biopsy specimens by polymerase chain reaction (PCR) analysis. These findings suggest that PPGSSmay result from a direct viral effect, as well as an immune-mediated vascular response to infection.
The timing of the antibody response to B19 in PPGSS appears to differ from that seen in erythema
infectiosum (EI). Patients with PPGSS may develop mucocutaneous lesions during the period of
viremia (and hence while still considered infectious), and subsequently develop a humoral immuneresponse. In contrast, in patients with EI, development of the skin exanthem coincides with the
appearance of antibody and disappearance of viremia.
The course of PPGSS is one of spontaneous involution. Resolution of the exanthem occurs over 1 to
2 weeks, during which time desquamation may occur. No residual sequelae are usually found.Treatment is generally supportive, and includes cool fluids and analgesics for oral mucosal
discomfort, if necessary. The affected skin surfaces can be treated with cool compresses and oralantihistamines in symptomatic patients.
For Further Reading:
[1.] Aractingi S, Bakhos D, Flageul B, et al. Immunohistochemical and virological study of skin in the papular-purpuric gloves and socks
syndrome. British Journal of Dermatology 1996;135:599-602.
[2.] Larralde M, Enz PA, Sanchez Gomes A, Corbella MC. Papular-purpuric “gloves and socks” syndrome due to parvovirus B19 infection in
childhood. Pediatr Dermatol 1998 Sep-Oct;15(5):413-414.
[3.] Messina MF, Ruggeri C, Rosano M, et al. Purpuric gloves and socks syndrome caused by parvovirus B19 infection. Pediatr Infect Dis J 2003
Aug;22(8):755-756.
7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 4/21
[4.] Pavlovic MD. Papular-purpuric “gloves and socks” syndrome caused by parvovirus B19. Vojnosanit Pregl 2003 Mar-Apr;60(2):223-225.
[5.] Smith PT, Landry ML, Carey H, et al. Papular-purpuric gloves and socks syndrome associated with acute parvovirus B19 infection: case
report and review. Clin Infect Dis 1998;27:164-168.
[6.] Vargas-Diez E, Buezo GF, Aragues M, et al. Papular-purpuric gloves-and-socks syndrome. Int J Dermatol 1996;35:626-632.
[7.] Veraldi S, Rizzitelli G, Scarabelli G, et al. Papular-purpuric “gloves and socks” syndrome. Arch Dermatol 1996;132:975-977.
Accreditation Statement
The Northwestern University Feinberg School of Medicine is accredited by the Accreditation
Council for Continuing Medical Education to provide continuing medical education for physicians.
Credit Designation Statement
The Northwestern University Feinberg School of Medicine designates this enduring material for amaximum of 2 AMA PRA Category 1 Credit(s)™ . Physicians should claim only the creditcommensurate with the extent of their participation in the activity.
Gloves and Socks Syndrome

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 5/21
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Gloves and Socks Syndrome back of the hands erythema
http://www.dermis.net/dermisroot/en/12018/image.htm
Gloves and socks syndrome caused by parvovirus B19 infection
M Carlesimo1, E Palese1, E Mari 1, V Panasiti 1, A Picarelli 2 , A Rossi 1, G Camplone1 Dermatology Online Journal 12 (6): 19
1. Department of Dermatology, University of Rome "La Sapienza" 2. Department of Clinical Sciences,
University of Rome "La Sapienza"
Abstract
The papular purpuric gloves and socks syndrome (PPGSS) is an uncommon dermatosis with a typicalpurpuric exanthem limited to hands and feet; it occurs mainly in young adults. We report a case of a 19-year-old man with an acute febrile illness accompanied by purpuric and papular lesions located mostly onthe dorsal areas of his hands and feet. Serologic analysis for parvovirus B19 yielded positive results. Thediagnosis of PPGSS was made. The eruption cleared without therapy in 12 days with plantar and palmardesquamation. Parvovirus B19 and some other viral infections have been proven to be causative agentsof this syndrome.
Introduction
The papular purpuric gloves and socks syndrome (PPGSS) is an uncommon dermatosis described for thefirst time by Harms et al. in 1990 [1]. They named this entity gloves and socks syndrome for the typicaldisposition of the exanthem.
In 1991 Bagot and Revuz observed the association between PPGSS and infection by human parvovirusB19 [2], supporting the hypothesis of a viral etiology. Papular purpuric gloves and socks syndrome isclinically characterized by a monomorphic eruption of purpuric macules and papules that is accompaniedby pruritic and painful edema involving the distal extremities in a peculiar gloves and socks distribution.

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 6/21
Some authors report symptoms and signs that occur during the course of this disease such as fever,asthenia, anorexia, arthralgia, lymphadenopathy, mucosal erosions, and perineuritis [3, 4, 5]. Theexanthem is self-limited and clears within a period of 1 or 2 weeks [6].
Clinical synopsis
In March 2004 a 19-year-old man was seen in our department for a 6-day history of papular purpuric lesions located exclusively on the hands(Fig. 1) and feet with a sharp demarcation at the wrists and the ankles.Edema, itching, and pain were also present. The eruption waspreceded by fever, abdominal pain, anorexia, and asthenia. Neitheroral lesions nor lymphadenopathy were present. Laboratory studieswere within normal limits with the exception of a mildly elevated whiteblood cell count, erythrocyte sedimentation rate at 22 mm/h, andprotein C reactive at 2 mg/dl.
Serologic markers for Epstein Barr virus, parvovirus, measles virus,cytomegalovirus, hepatitis B and C virus, Rickettsia, HIV, herpessimplex virus 1 and 2 were tested with an indirect enzyme linkedimmunosorbent assay on the sixth day and on the eleventh day afteronset of the clinical eruption. The results were within normal limits withthe exception of assays for parvovirus B19 IgG and IgM confirmingacute infection in the second week. The diagnosis of acute parvovirusB19 infection was made on the basis of the presence of specific IgM antibodies in serum samplesassayed at two different times during the patient's illness. Based on the clinical picture and the laboratorydata the diagnosis of PPGSS was made. The eruption cleared after palmoplantar desquamation in 12days.
Discussion
PPGSS is an acute self-limited acral dermatosis that affects children or young adults. Edema anderythema appear on the hands and feet in a "gloves and socks" distribution, followed by the appearanceof pruritic or painful purpuric macules and papules on the same sites [3, 4]. Sometimes similar lesionsmay also be observed on other sites and a variety of oral or genital manifestation have been described [6, 7].
Systemic involvement that may precede or accompany skin manifestations include flu-like symptomssuch as fever, asthenia, anorexia, arthralgia, lymphadenopathy, myalgia, respiratory or gastrointestinalsymptoms [3, 7, 8].
Laboratory data are nonspecific with occasional leukopenia, neutropenia, eosinophilia, and mild elevationof transaminase levels and erythrocyte sedimentation rate [4, 8].
Histologic findings are non-specific and include necrotic keratinocytes, erythrocyte extravasion, and asuperficial and mild-dermal perivascular lymphocytic infiltrate.
The illness is self limited, lasting 1-2 weeks; usually the eruption clears with palmar and plantardesquamation.
The viral etiology is well documented in the literature [9,10]. B19 is the most frequently reported etiologicagent of PPGSS, whereas occasional cases are associated with Coxsackie B virus, Epstein Barr virus,
Figure 1
Figure 1: Papular purpuric
lesions presented exclusively
on the hands with a sharp
demarcation at the wrists

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 7/21
Measles virus, Cytomegalovirus, Hepatitis B virus, and Herpes virus 6 infection. These data suggest thatPPGSS could be a non- specific manifestation of a viral infection.
The pathogenesis of this syndrome is still not completely understood. Parvovirus B19 is a member of theerythrovirus family and is the only parvovirus known to cause disease in humans. Infection withparvovirus B19 during pregnancy can cause several serious complications in the fetus, such as fetal
anemia, neurological anomalies, hydrops fetalis, and fetal death because of viral inhibition oferythropoiesis and cytolysis of erythroid progenitor cells [11].
A receptor for Parvovirus B19 is present on bone marrow erythroid precursor cells, endothelial cells ofdermal vessels, and keratinocytes. An immunohistochemical study with specific anti-B19V antibodiesshowed the presence of viral antigens on both epidermal and endothelial cells [12]. Therefore, themucocutaneous lesions could be virus-mediated, through cytotoxicity, and not antibody-mediated.Cutaneous lesions generally develop on days 10 to 13 after infection [13-15].
In the literature there are some sero-negative cases, perhaps because testing for IgM antibodies wasdone during the first week of clinic eruption when sometimes antibodies are not yet detectable. Indeed,we perform this test during the second week of clinical eruption.
Many clinical entities have been strongly associated with B19 infection such as erythema infectiosum,transient aplastic crisis, arthralgias, rheumatoid-like arthritis, spontaneous abortions, hydrops fetalis, andPPGSS.
In a recent paper, however, the sera of 110 children with cutaneous eruptions and an acute systemicillness were analyzed to evaluate the presence of antibodies against parvovirus B19. Specific IgMantibodies to Parvovirus B19 were found in only 3 cases. This data indicates that Parvovirus B19 is notone of the most common causes of acute illness and rash in children [16].
We report this case because of the importance of recognizing Parvovirus B19 illness due to theoccasional serious sequelae and because of the increased frequency of this presentation in young adultsin recent years [17].
References
1. Harms M, Feldmann R, Saurat JH . Papular-purpuric "gloves and socks" syndrome. J Am Acad
Dermatol 1990 Nov;23: 850-854.
2. Bagot M, Revuz J. Papular-purpuric "gloves and socks" syndrome: primary infection with parvovirus
B19? J Am Acad Dermatol. 1991 Aug;25(2 Pt 1):341-2.
3. Borradori L, Cassinotti P, Perrenoud D, Frenk E. Papular-purpuric "gloves and socks" sindrome. Int J
Dermatol. 1994 Mar;33(3):196-7.
4. Halasz CL, Cormier D, Den M. Petechial glove and sock sindrome caused by parvovirus B19. J Am
Acad Dermatol. 1992 Nov;27(5 Pt 2):835-8.
5. Aguilar-Bernier M, Bassas-Vila J, Torne-Gutierrez J.I, Martinez-Garcia G, Aragoneses-Fraile H,
Miranda-Romero A. Presence of perineuritis in a case of papuar purpuric gloves and socks syndrome
associated with mononeuritis multiplex attributable to B19 parvovirus. J Am Acad Dermatol. 2006;
54:896-899.
6. Smith SB, Libow LF, Elston DM, Bernert RA, Warschaw KE Gloves and socks syndrome: early and late
histopathologic features. J Am Acad Dermatol. 2002 Nov; 47(5):749-54.

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 8/21
7. Grilli R, Izquierdo MJ, Farina MC, Kutzner H, Gadea I, Martin L, Requena L. Papular-purpuric "gloves
and socks" sindrome: polymerase chain react demonstration of parvovirus B19 DNA in cutaneous lesions
and sera. J Am Acad Dermatol. 1999 Nov; 41(5 Pt):793-6.
8. Smith Pt, Landry ML, Carey H, Krasnoff J, Cooney E. Papular-purpuric gloves and socks syndrome
associated with acute parvovirus B19 infection: case report and review. Clin Infect Dis. 1998Jul;27(1):164-8.
9. Vargas-Diez E, Buezo GF, Arageus M, Dauden E, De Ory F. Papular-purpuric gloves-and-socks
syndrome. Int J Dermatol. 1996 Aug;132(8):975-7.
10. Stone MS, Murph JR. Papular-purpuric gloves and socks syndrome: a characteristic viral exanthema.
Pediatrics. 1993 Dec;92(6):864-5.
11. de Jong EP, de Haan TR, Kroes AC, Beersma MF, Oepkes D, Walther FJ. Parvovirus B19 infection in
pregnancy. J Clin Virol. 2006 May;36(1):1-7.
12. Alfadey A, Alijubran A, Hainau B, Alhokail A. Papular-purpuric"gloves and socks" syndrome in amother and daughter. J Am Acad Dermatol. 2003 Jun; 48(6):941-4.
13. Feldmann R, Harms M, Borradori L, Saurat JH. "Gloves and socks" papulo-purpuric syndrome. Ann
Dermatol Venereol. 1993;120(11):810-2.
14. Aractingi S, Bakhos D, Flageul B, Verola O, Brunet M, Dubertret L, Morinet F. Immunohistochemical
and virological study of skin in the popular-purpuric gloves and socks syndrome. Br J Dermatol. 1996
Oct;135(4):599-602.
15. Nelson JS, Stone MS. Update on selected viral exanthems. Curr Opin Pediatr. 2000 Aug;12(4):359-
64.
16. Pruksachatkunakorn C, Apichartpiyakul N, Kanjanaratanakorn K. Parvovirus B19 infection in children
with acute illness and rash. Pediatric Dermatology. 2006; 23:216-218.
17. Hsieh MY, Huang PH. The juvenile variant of papular-purpuric gloves and socks syndrome and its
association with viral infections. Br J Dermatol. 2004 Jul;151(1):201-6.
© 2006 Dermatology Online Journal
http://escholarship.org/uc/item/41s0b467
7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 9/21
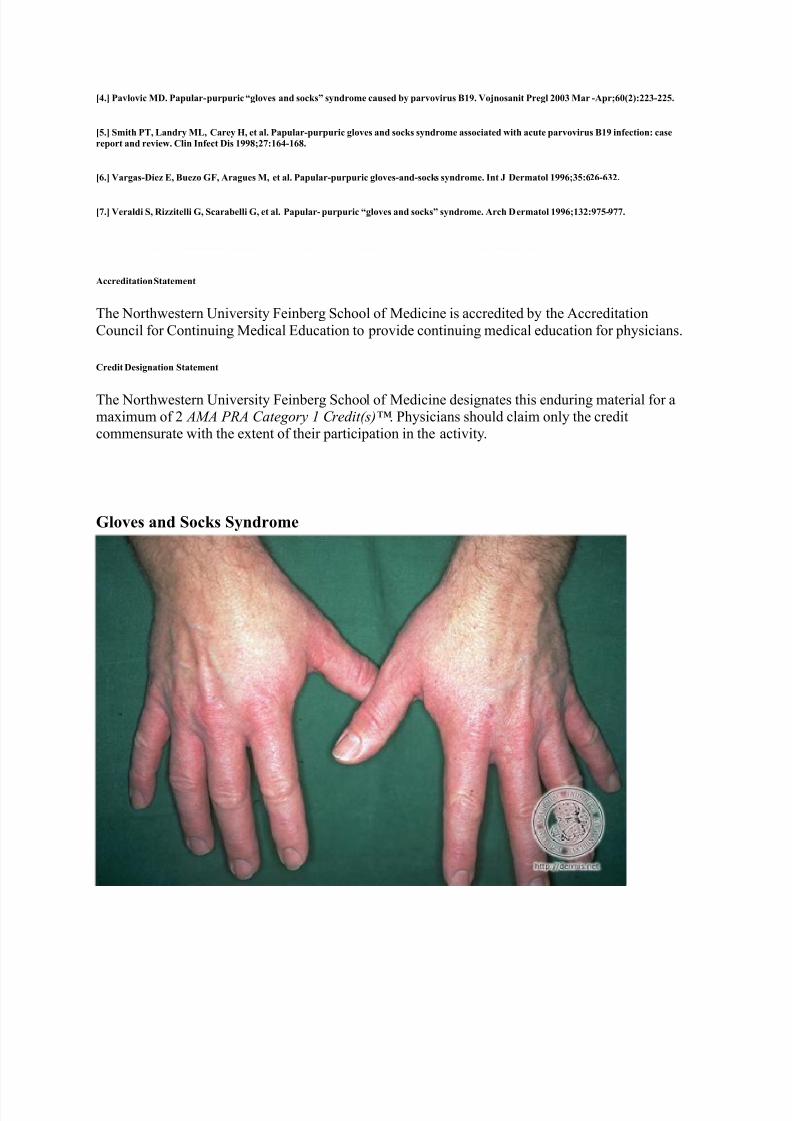
Gloves and Socks Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Gloves and Socks Syndrome feet petechiae
patient information
http://www.dermis.net/dermisroot/en/12022/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 10/21
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Gloves and Socks Syndrome feet macula / patch petechiae
http://www.dermis.net/dermisroot/en/12025/image.htm
7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 11/21
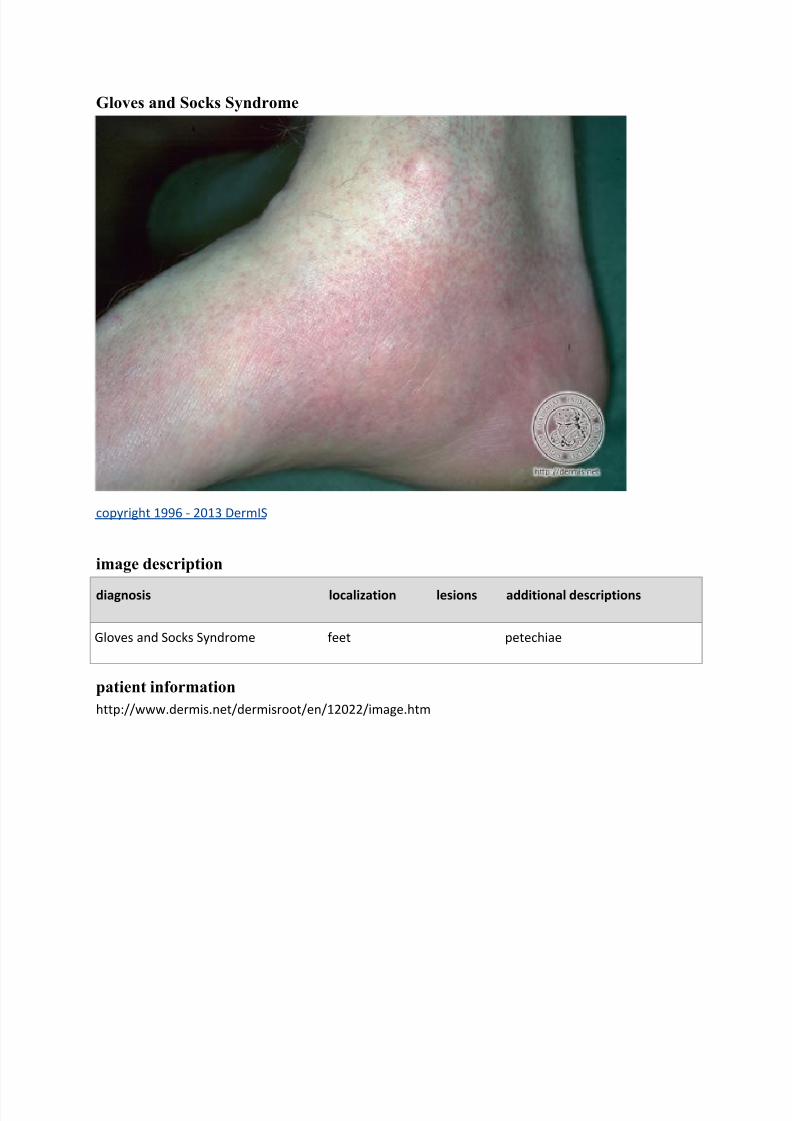
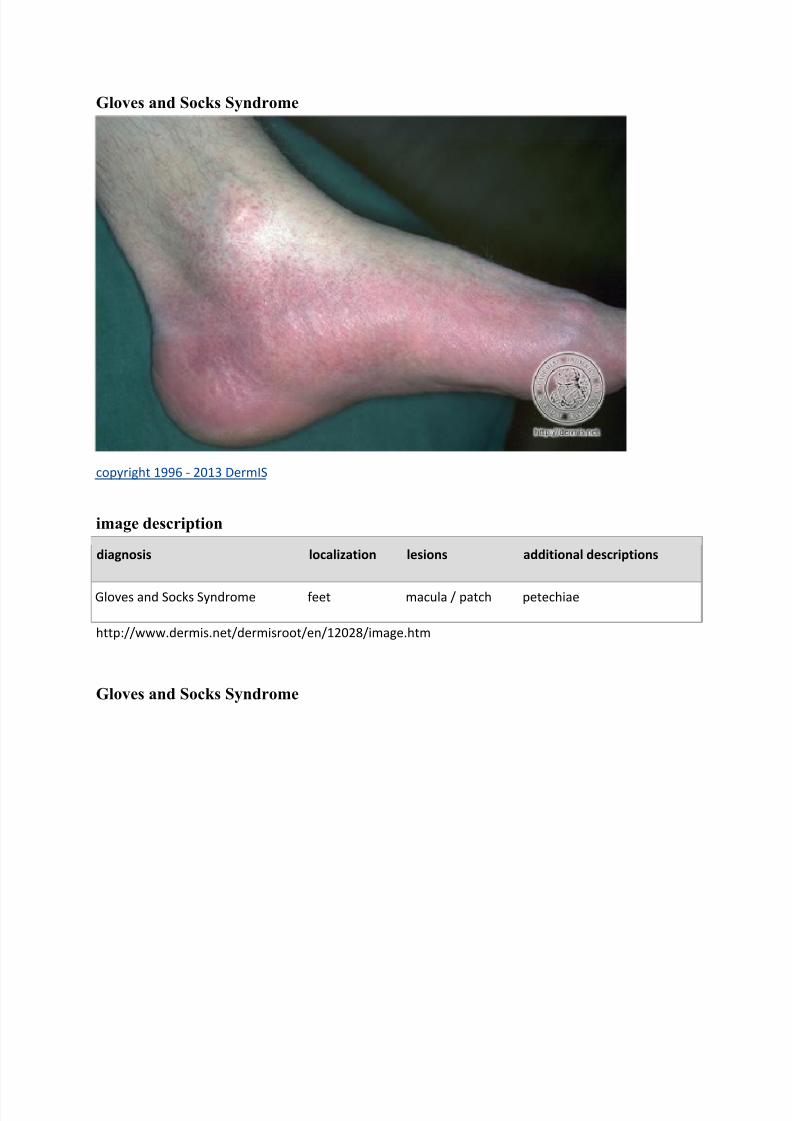
Gloves and Socks Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Gloves and Socks Syndrome feet macula / patch petechiae
http://www.dermis.net/dermisroot/en/12028/image.htm
Gloves and Socks Syndrome
7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 12/21
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
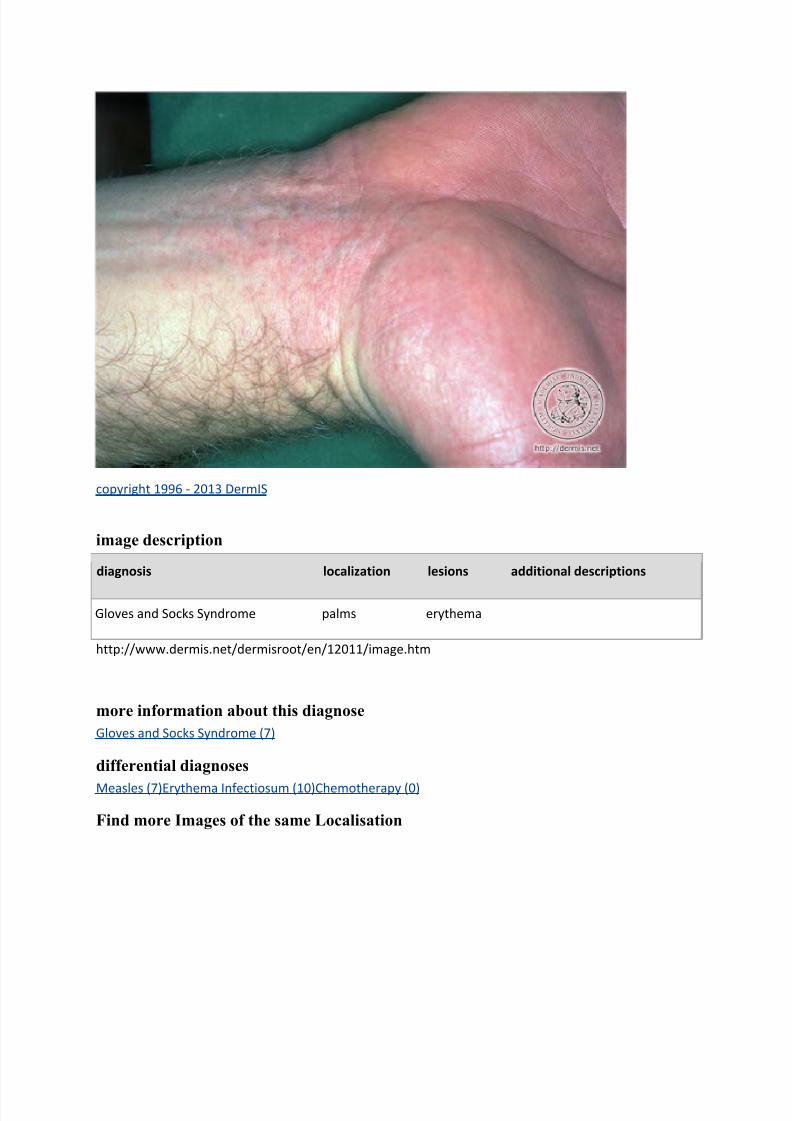
Gloves and Socks Syndrome palms erythema
http://www.dermis.net/dermisroot/en/12011/image.htm
more information about this diagnose
Gloves and Socks Syndrome (7)
differential diagnoses
Measles (7)Erythema Infectiosum (10)Chemotherapy (0)
Find more Images of the same Localisation

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 13/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome palms plaque
Stevens-Johnson Syndrome palms vesicle
http://www.dermis.net/dermisroot/en/30351/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 14/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome palms plaque
Stevens-Johnson Syndrome palms vesicle
http://www.dermis.net/dermisroot/en/30348/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 15/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome lower arms plaque
Stevens-Johnson Syndrome lower arms vesicle
http://www.dermis.net/dermisroot/en/30345/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 16/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome lower arms plaque
Stevens-Johnson Syndrome lower arms vesicle
http://www.dermis.net/dermisroot/en/30342/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 17/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome lower arms erythema
Stevens-Johnson Syndrome lower arms plaque
Stevens-Johnson Syndrome lower arms vesicle
http://www.dermis.net/dermisroot/en/30337/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 18/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome lower arms plaque
Stevens-Johnson Syndrome lower arms vesicle
http://www.dermis.net/dermisroot/en/30333/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 19/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome lips (skin) erosion
Stevens-Johnson Syndrome lips (skin) crust
http://www.dermis.net/dermisroot/en/30355/image.htm
7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 20/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
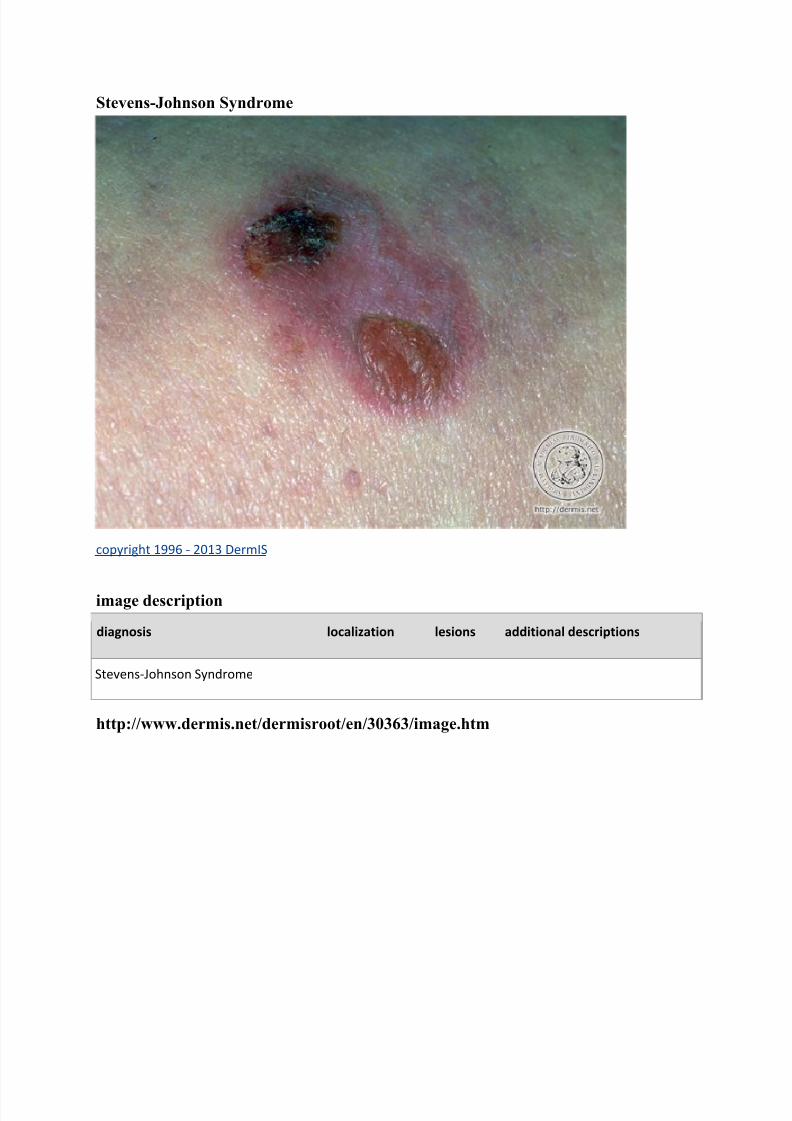
Stevens-Johnson Syndrome
http://www.dermis.net/dermisroot/en/30363/image.htm

7/18/2019 Dermatology Quiz and Case Discussion Gloves and Socks Synd
http://slidepdf.com/reader/full/dermatology-quiz-and-case-discussion-gloves-and-socks-synd 21/21
Stevens-Johnson Syndrome
copyright 1996 - 2013 DermIS
image description
diagnosis localization lesions additional descriptions
Stevens-Johnson Syndrome lower arms plaque
Stevens-Johnson Syndrome lower arms vesicle
http://www.dermis.net/dermisroot/en/30329/image.htm
more information about this diagnose
Stevens-Johnson Syndrome (55)
differential diagnoses
Gingivostomatitis Herpetica (2)Gingivostomatitis Herpetica Gravis (0)Pemphigus, Paraneoplastic (0)Drug
Eruption (43)Lyell Syndrome (20)Pemphigus Vulgaris (43)Pemphigus Mucosae (44)Bullous Pemphigoid
(71)Linear IgA Dermatosis (3)Erythema Exsudativum Multiforme, Minor Form (12)Acute Cutaneous
Graft-versus-Host Reaction (0)Lichen Planus of the Mucosa, Erosive (30)Lupus Erythematosus Mucosae
Oris (8)Epidermolysis Bullosa Hereditaria (36)
Find more Images of the same Localisation