design and implementation of a portable physiologic data
TRANSCRIPT

Clinical Investigation
Design and implementation of a portable physiologic dataacquisition system*
Kevin Vinecore, BS; Mateo Aboy, PhD; James McNames, PhD; Charles Phillips, MD; Rachel Agbeko, MD;Mark Peters, MRCP, PhD; Miles Ellenby, MD; Michael L. McManus, MD, MPH; Brahm Goldstein, MD, FCCM
T he intensive care unit (ICU)has long been viewed as sim-ilar to a physiology labora-tory due to the diverse num-
ber of pathophysiologic processes thatoccur and the relative rapidity by whichthey progress. However, in order tostudy closely the pathophysiology ofcritically ill and injured patients, an
accurate physiologic data acquisitionsystem needs to be available that iscomparable to those used in experimen-tal laboratories to record both physio-logic signals and associated importantclinical events (1– 4).
To date, such a system for the simul-taneous collection of long (hours todays) annotated time series has proven
difficult (5) due to insufficient compu-tational power, inadequate specializedsoftware, difficulty in accurately anno-tating clinical events, and incompatibil-ity between data acquisition, data anal-ysis, and commercial monitoringsystems. A number of investigatorshave described their systems for physi-ologic data acquisition, archive, andanalysis (6, 7), but none have been ableto record the finely granular signal dataand clinical annotations required to ac-curately perform clinical physiologicstudies in the ICU.
We previously reported a real-time,continuous physiologic data acquisitionsystem developed for the study of dis-ease dynamics in the ICU that capturedphysiologic signal and parameter (i.e.,time averaged mean signals) data frommultiple patients simultaneously on acontinuous basis (6) and was ideal forblinded data analysis. However, thissystem was not capable of recordingtime-sensitive information aboutchanges in a patient’s clinical condi-
Objective: To describe and report the reliability of a portable,laptop-based, real-time, continuous physiologic data acquisitionsystem (PDAS) that allows for synchronous recording of physio-logic data, clinical events, and event markers at the bedside forphysiologic research studies in the intensive care unit.
Design: Descriptive report of new research technology.Setting: Adult and pediatric intensive care units in three ter-
tiary care academic hospitals.Patients: Sixty-four critically ill and injured patients were
studied, including 34 adult (22 males and 12 females) and 30pediatric (19 males and 11 females).
Interventions: None.Measurements and Main Results: Data transmission errors
during bench and field testing were measured. The PDAS wasused in three separate research studies, by multiple users, and forrepeated recordings of the same set of signals at various intervalsfor different lengths of time.
Both parametric (1 Hz) and waveform (125–500 Hz) signalswere recorded and analyzed. Details of the PDAS components are
explained and examples are given from the three experimentalphysiology-based protocols. Waveform data include electrocar-diogram, respiration, systemic arterial pressure (invasive andnoninvasive), oxygen saturation, central venous pressure, pulmo-nary arterial pressure, left and right atrial pressures, intracranialpressure, and regional cerebral blood flow. Bench and field test-ing of the PDAS demonstrated excellent reliability with 100%accuracy and no data transmission errors. The key feature ofsimultaneously capturing physiologic signal data and clinicalevents (e.g., changes in mechanical ventilation, drug administra-tion, clinical condition) is emphasized.
Conclusions: The PDAS provides a reliable tool to record phys-iologic signals and associated clinical events on a second-to-second basis and may serve as an important adjunctive researchtool in designing and performing clinical physiologic studies incritical illness and injury. (Pediatr Crit Care Med 2007; 8:563–569)
KEY WORDS: physiologic signals; waveforms; data acquisition;intensive care unit; research
*See also p. 588.From the Pulmonary and Critical Care Medicine,
Oregon Health & Science University, OR (KV, CP);Oregon Institute of Technology, Portland, OR (MA);Biomedical Signal Processing Laboratory, PortlandState University, OR (JM); Critical Care Group, PortexUnit Institute of Child Health, London, UK (RA, MP);Paediatric Intensive Care Unit, Great Ormond StreetHospital for Children NHS Trust, London, UK (MP);Division of Pediatric Critical Care, Department ofPediatrics, Oregon Health & Science University, OR(ME); Department of Anesthesia and Division ofCritical Care Medicine, Children’s Hospital, HarvardMedical School, Boston, MA (MLM); Novo Nordisk,Princeton, NJ (BG).
Supported, in part, by a grants from the ThrasherResearch Fund, the Oregon Child Health ResearchCenter (HD33703, NICHHD), the Oregon Opportunity,
and the Center for Excellence in Human ResearchGrant. Research at the Institute of Child Health andGreat Ormond Street Hospital for Children NHS Trustbenefits from R&D funding received from the NHSExecutive.
Drs. Ellenby, Goldstein, McNames, and Phillips andMr. Vinecore have no financial interest in PDAS andhave no plans for commercial development. The re-maining authors were not involved in PDAS develop-ment.
For information regarding this article, E-mail:[email protected]
Copyright © 2007 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/01.PCC.0000288715.66726.64
563Pediatr Crit Care Med 2007 Vol. 8, No. 6

tion, timing of drug administration, oc-currence of noxious environmentalstimuli (such as noise and light), and amultitude of other important variables.
This article describes the next gener-ation of the physiologic data acquisitionsystem (PDAS) that allows for synchro-nous recording of physiologic data, clin-ical events, event markers, and notationat the bedside of experimental clinicalprotocols designed for studies of criticallyill and injured patients. To date, thePDAS described in this manuscript hasbeen used in four ICUs: the adult andpediatric ICUs at Oregon Health and Sci-ence University, the pediatric ICU atGreat Ormond Street Hospital, London,UK, and the medical/surgical intensivecare unit at Children’s Hospital, Boston,MA.
METHODS
Institutional Review Board and ResearchEthics Committee Approvals. Three study pro-tocols have been used to date. The Pulse Pres-sure Variation and Fluid Responsiveness Pro-tocol was approved by the Institutional ReviewBoard of Oregon Health and Science Univer-sity; the Physiologic Challenge Protocol in Pe-diatric Traumatic Brain Injury (TBI) Protocolwas approved by both the Institutional ReviewBoard of Oregon Health and Science Univer-sity and the Institute of Child Health/GreatOrmond Street Hospital Research EthicsCommittee; and the Characterization of Re-gional Cerebral Blood Flow in Patients withMoyamoya Disease Undergoing Pial Synangio-sis Protocol was approved by Children’s Hos-pital Boston Committee on Clinical Investiga-tion.
Study Protocol Summaries. Table 1 brieflysummarizes the study protocols referred to inthe manuscript. Table 2 lists the subject demo-graphics, diagnoses, and waveforms recorded us-ing the PDAS for each study protocol.
PDAS Hardware and Software. The PDASconsists of a laptop computer, a standard PC-MCIA serial card (Socket Communications,Newark, CA), RS232 serial interface cables
(Oregon Electronics, Portland, OR), and cus-tom software that continuously acquires andstores physiologic signals from the ICU mon-itoring devices. The laptop is a Gateway M675with a 3.0-GHz P4 processor (Gateway, Irvine,CA) running Microsoft Windows XP (MicrosoftCorporation, Redmond, WA) although anysimilarly equipped laptop computer will per-form adequately. Serial ports were added tothe laptop with a dual high-speed serial I/OPCMCIA card. The serial card is connected toRS232 communication ports on the medicaldevices with custom-built T25-pin serial inter-face cables. Data are exported from a PhilipsComponent Monitoring System or Intellivue(Philips Medical Systems, N.A. Bothell, WA)patient monitor through the RS232 serial portcard. The PCMCIA serial adapter card providesaccess to up to four physical serial ports fordata from secondary monitoring devices, suchas continuous cardiac output monitors(PiCCO, Pulsion Medical Systems AG, Munich,Germany), transonic flow meters, and near-infrared spectroscopy perfusion monitors(Hutchinson Technology, Hutchinson, MN).
The PDAS software, developed at OregonHealth and Science University in collaborationwith Portland State University, is the heart ofthe data collection system. The PDAS softwaremanages the communications with the mon-itoring devices and coordinates the incomingdata flow from each of the physiologic signalswhile presenting an intuitive graphical userinterface to the PDAS operator. The PDASgraphical user interface is customizable to addclinical annotation pages for existing or newstudies. All recorded data are transferred totext files that can be easily imported into anyoff-line analysis tool, such as MATLAB (TheMathWorks, Natick, MA), for post hoc signalprocessing, waveform analysis, and statisticalanalysis.
Physiologic data from the Philips patientmonitors are downloaded at sampling rates of500 Hz for electrocardiogram (ECG) wave-forms and 125 Hz for pressures and mostother waveforms. Both waveform signals andparametric data are displayed on the PDASscreen. Since the data transmission rate of theComponent Monitoring System patient mon-itor is 38,400 bps, a maximum of one 500-HzECG signal and four additional 125-Hz signals
can be recorded and displayed for each RS232connection. The Intellivue has a throughputof 115,200 bps, which permits up to two ECGwaveforms sampled at 500 Hz and five otherwaveforms sampled at 125 Hz to be acquiredfor each RS232 connection.
Collected data are stored in an organized,logical, protected, and accessible manner foranalysis or presentation by other software ap-plications. The data acquisition software han-dles file organization with an automatic filename generation scheme that allows for mul-tiple research studies, multiple users, and re-peated recording of the same set of signals atarbitrary intervals for arbitrary lengths oftime. Data are stored on the laptop’s harddrive in a hierarchical structure based on thespecific research study, the study-specific pa-tient identification number, the recording ses-sion number, and the source of the signalbeing recorded. Data are stored in ASCII textformat files with one data point per line. Thispermits data to be easily imported into com-mon statistical analysis and digital signal pro-cessing packages as well as desktop publishingprograms. Signal-specific information, such asscaling values, units, and study start and stoptimes, for each of the signals recorded is col-lected into a single information file. Diskspace consumption varies depending on thenumber and type of signals being recorded,but simultaneous acquisition of five waveformsignals with associated parametric values re-quires �45 MB/hr.
Clinical or study annotations and text com-ments are entered as free-form text or specifi-cally designed data sets for a particular researchstudy protocol and are stored in a separate ACSIItext file with all of the fields for a particularannotation separated by commas and stored on asingle line. The file is structured to indicatewhen the annotation was made and is indexed toboth the 125-Hz and 500-Hz data files. Indicesinto data files recorded at other sampling ratesare calculated using the annotation time stamp,the sample rate, and the start time of the re-corded data file.
RESULTS
We have successfully recorded physio-logic signals with synchronous clinicalannotations from 44 subjects under threedifferent research protocols using thePDAS.
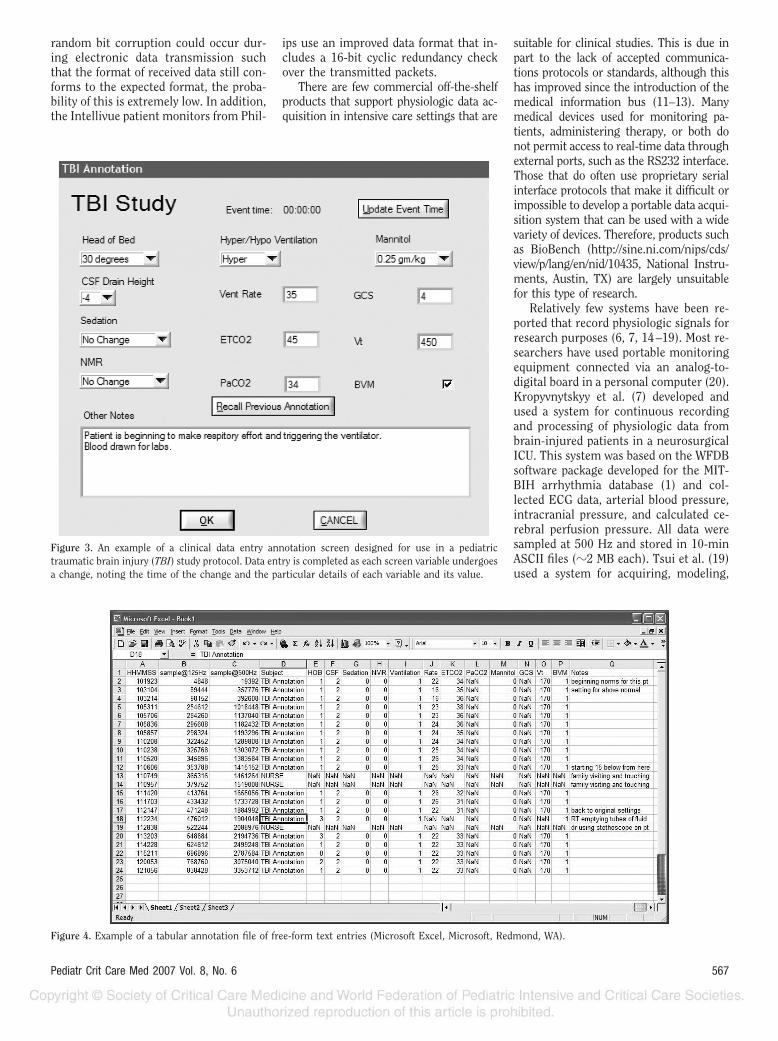
Figure 1 is a screen shot of the PDASmain data acquisition screen with the ac-quired physiologic signal waveforms andparametric values displayed in real time.Figure 2 is an example of a clinical anno-tation screen designed specifically for thepulse pressure variation study protocol.Figure 3 is an example of the clinicalannotation entry page that is used for thepediatric TBI study protocol. Figure 4shows PDAS fields for free-form text
Table 1. Subject demographics, diagnoses, and waveforms recorded using the physiologic dataacquisition system
StudyNo. of
SubjectsMean Age,
yrsGender,
Male/Female Waveforms
Pulse pressure variation 34 45 22/12 ECG, RESP, ABP, SpO2, CVPPediatric TBI 11 8 8/3 ECG, RESP, Pairway, ABP, ICPPial synangiosis for
moyamoya disease19 9 11/8 ECG, ABP, ETCO2, SpO2,
CBF
TBI, traumatic brain injury; ECG, electrocardiogram; RESP, respiration; ABP, arterial bloodpressure; SpO2, pulse oximetry; CVP, central venous pressure; Pairway, airway pressure; ICP, intracranialpressure; CBF, cerebral blood flow; ETCO2, end-tidal carbon dioxide.
564 Pediatr Crit Care Med 2007 Vol. 8, No. 6

annotations displayed in a spreadsheetformat.
Bench and field testing of the PDASdemonstrated excellent reliability. If adata transmission error is detected by thePDAS software, a warning is displayed forthe operator and the event is time-stamped, tagged with a subject, and thenlogged along with the clinical annota-tions. During analysis, error-free datacollection can then be confirmed witheither a visual inspection of the log file ora simple automated search for the subjecttag. Validation of PDAS error detectionwas performed by replacing live inputwith specially crafted data packets con-taining errors. V1.2 of the software hasperformed �100 recording sessions ofbetween 2 to 24 hrs each without anydata transmission errors entered into theevent log.
DISCUSSION
The PDAS is a sophisticated, user-friendly, physiologic data acquisition sys-tem specifically developed for clinical re-search in the ICU environment. Data
acquisition systems intended for researchpurposes must meet several importantspecifications. The system must be ableto interface with many commercial phys-iologic monitoring devices from differentmanufacturers and be capable of contin-uously acquiring and storing every typeof physiologic signal with 100% accuracy.The system also needs to include a mech-anism for researchers to make time-stamped clinical annotations that are pre-cisely synchronized with the collectedsignals. Protocol-specific pull-downmenus for rapid clinical data entry arealso needed. And finally, the system mustbe reliable, versatile, easy to use, cost-effective, and compliant with the HealthInsurance Portability and AccountabilityAct (8–10).
We have shown that the PDAS meetsthe preceding requirements. It is user-friendly, portable, accurate, and adapt-able to multiple ICU clinical trial designs.Operators, including bedside ICU nursingstaff without prior research or specificcomputer expertise, have used the systemand were easily able to acquire up to four
continuous physiologic signals (125–500Hz) simultaneously with parametric datawhile detailing important clinical eventsthrough the time-stamped PDAS annota-tion software. With the addition of a sec-ond dual high-speed serial I/O PCMCIAcard, eight physiologic signals and asso-ciated parametric data are possible.
The accuracy of the transmitted datato the PDAS is equal to the accuracy ofthe patient monitor itself. In other words,the transcription and recording error iszero so the only source of error in posthoc physiologic analysis would comefrom nonstationary sources related to thepatient or the external ICU environment(e.g., movement artifact, 60-Hz interfer-ence). Because the patient monitor digi-tizes data as they come in from the vari-ous data collection modules andtransmits the data in a very precise for-mat with extensive header and trailer in-formation, any corruption of data or lossof signal is immediately recognized andreported by the PDAS software.
To date, no errors have been detected.Although it is theoretically possible that a
Table 2. Three experimental clinical protocols using the physiologic data acquisition system
Protocol Title Background Main Objective
PPV responsiveness in adultpatients with shock
The effects of positive pressure mechanical ventilation on cardiacfilling (preload) can be used to determine fluid responsiveness(27). If the patient has low venous return and is thus preloaddependent, cardiac output and thus arterial pulse pressure willsignificantly vary with respirations (i.e., PPV).
1. To record cardiorespiratory signals withclinical annotations to determine PPV asa predictor of intravenous fluidresponsiveness.
2. To determine if the pulse oximetrysignal can be substituted for arterialpressure in calculation of PPV.
Physiologic challenge inpediatric TBI
Therapy for TBI is largely unsupported by clinical evidence. Thisstudy uses a randomized protocol that records physiologicsignals and clinical events during changes in three standardtherapies for elevated ICP:
1. Elevating the head of bed between 0° and 40° in 10° randomincrements
1. To analyze each physiologic challengeand characterize the dynamicphysiologic responses.
2. Inducing mild hypo- and hyperventilation (decreasing orincreasing the end-tidal CO2 by 4 mm Hg from baseline)
2. To develop an in silico computer modelthat allows for virtual testing oftherapeutic options for elevated ICPbefore actual treatment is administered.
3. Changing the resistance to cerebral spinal fluid drainage(altering the height of the drainage bag between �8 and �8cm in 4-cm increments from baseline)
Characterization of regionalcerebral blood flow inpatients with moyamoyadisease undergoing pialsynangiosis
Moyamoya disease is characterized by progressive stenosis of theintracranial internal carotid arteries and compensatoryproliferation of dilated collateral arteries at the base of thebrain. Pial synangiosis is a surgical procedure that augmentssurface collateral blood flow to the brain by using the externalcarotid circulation (28, 29) and suturing the superficialtemporal artery to the pial surface. As a consequence ofcompromised rCBF, measured by the Bowman PerfusionMonitor (Hemedex, Cambridge, MA), and abnormal cerebralautoregulation, patients are at risk for stroke in theperioperative period (30–32).
1. To detect episodes of regional cerebraloligemia and ischemia in thepostoperative period from variousphysiologic signals and clinicalannotations.
2. To test the ability of two noninvasivemodalities (near-infrared spectroscopyand electroencephalogram) to detectcerebral ischemia, and to correlate rCBFwith mean arterial pressure and end-tidal carbon dioxide values.
PPV, pulse pressure variation; TBI, traumatic brain injury; ICP, intracranial pressure; rCBF, regional cerebral blood flow.
565Pediatr Crit Care Med 2007 Vol. 8, No. 6
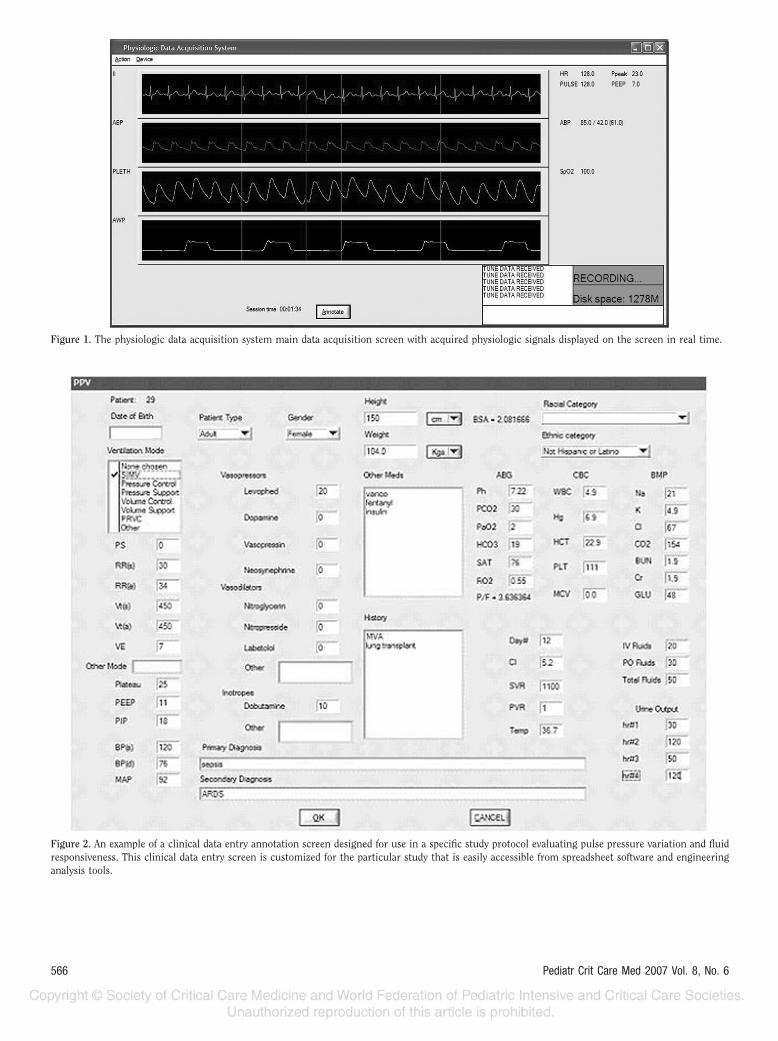
Figure 1. The physiologic data acquisition system main data acquisition screen with acquired physiologic signals displayed on the screen in real time.
Figure 2. An example of a clinical data entry annotation screen designed for use in a specific study protocol evaluating pulse pressure variation and fluidresponsiveness. This clinical data entry screen is customized for the particular study that is easily accessible from spreadsheet software and engineeringanalysis tools.
566 Pediatr Crit Care Med 2007 Vol. 8, No. 6
random bit corruption could occur dur-ing electronic data transmission suchthat the format of received data still con-forms to the expected format, the proba-bility of this is extremely low. In addition,the Intellivue patient monitors from Phil-
ips use an improved data format that in-cludes a 16-bit cyclic redundancy checkover the transmitted packets.
There are few commercial off-the-shelfproducts that support physiologic data ac-quisition in intensive care settings that are
suitable for clinical studies. This is due inpart to the lack of accepted communica-tions protocols or standards, although thishas improved since the introduction of themedical information bus (11–13). Manymedical devices used for monitoring pa-tients, administering therapy, or both donot permit access to real-time data throughexternal ports, such as the RS232 interface.Those that do often use proprietary serialinterface protocols that make it difficult orimpossible to develop a portable data acqui-sition system that can be used with a widevariety of devices. Therefore, products suchas BioBench (http://sine.ni.com/nips/cds/view/p/lang/en/nid/10435, National Instru-ments, Austin, TX) are largely unsuitablefor this type of research.
Relatively few systems have been re-ported that record physiologic signals forresearch purposes (6, 7, 14–19). Most re-searchers have used portable monitoringequipment connected via an analog-to-digital board in a personal computer (20).Kropyvnytskyy et al. (7) developed andused a system for continuous recordingand processing of physiologic data frombrain-injured patients in a neurosurgicalICU. This system was based on the WFDBsoftware package developed for the MIT-BIH arrhythmia database (1) and col-lected ECG data, arterial blood pressure,intracranial pressure, and calculated ce-rebral perfusion pressure. All data weresampled at 500 Hz and stored in 10-minASCII files (�2 MB each). Tsui et al. (19)used a system for acquiring, modeling,
Figure 3. An example of a clinical data entry annotation screen designed for use in a pediatrictraumatic brain injury (TBI) study protocol. Data entry is completed as each screen variable undergoesa change, noting the time of the change and the particular details of each variable and its value.
Figure 4. Example of a tabular annotation file of free-form text entries (Microsoft Excel, Microsoft, Redmond, WA).
567Pediatr Crit Care Med 2007 Vol. 8, No. 6

and predicting intracranial pressure inthe ICU. The IBIS data library (15) con-tains continuous electroencephalographysignals, multimodal evoked potential re-cordings, and diagnostic ECG recorded inthe ICU and operating room. The dataacquisition system also allows for trenddata (i.e., parametric data) from patientmonitors, laboratory data, and clinicalannotations. Each of these systems wasmore limited than the PDAS in terms ofeither number of waveforms recorded,length of the recording, number and typeof compatible monitoring devices, pro-scribed clinical research data entryscreens, and/or ability for time-stampedclinical and study annotations.
Recent advances in medical informaticsand data information protocols have led toelectronic medical records and real-timedecision support systems that permit ac-cess to virtually all of the disparate patientdata (21, 22). These systems often are ca-pable of automatic reports and analysis tohelp clinicians integrate all of the availableinformation (23). These systems are able tocollect data from a wide variety of intensivecare devices but typically do so automati-cally for analysis that is not at the bedside.These are insufficient for many clinicalstudies because they do not permit eventannotation through an interface that issuitable for clinical research. There appearsto be insufficient market demand to de-velop this type of system commercially.
Limitations. Signal artifact remains asubstantial but not insurmountable prob-lem for any data acquisition system. Wepreviously presented a discussion of thetypes and character of signal artifact inthe ICU setting (6). Although there is noperfect technique for isolating artifact,clinical annotations by an observer sta-tioned in the patient’s room, as incorpo-rated with the PDAS, is probably the mostaccurate. The IMPROVE database used asimilar technique with detailed timed an-notations regarding patient state, nurs-ing actions, and other patient distur-bances by a team of physicians whoremained at the bedside throughout the�24-hr recording (15, 24). Annotation ofthe recording during data collection pro-vided for comparison of any changes inthe recorded waveforms or measure-ments against physician observations.The PDAS works in essentially the samemanner. Although PDAS was developedto record data from Philips monitors andstand-alone devices via a PCMCIA serialadapter card, it could be easily be adaptedto interface with ICU monitors from
other manufacturers, such as SpaceLabs(OSI Systems, Hawthorne, CA) andWelchAllynProtocol (Beaverton, OR).
CONCLUSION
The PDAS may significantly contrib-ute to critical care research in three ways.First, the PDAS may provide a tool toimprove our understanding of the patho-physiology of critical illness by closelyexamining physiologic changes in rela-tion to clinical events on a second-to-second time frame, including detailedpharmacodynamic studies heretofore notpractical. Second, patterns of physiologicvariability or organ system interactionsmay be identified that may yield physio-logic markers of impending clinical dete-rioration (25). And third, the PDAS mayaid the development of patient-specificmathematical models representing criticalillness that can be shared across differentcomputer formats or via a database such asPhysionet (www.physionet.org) (2, 3). Infact, physiologic data from the current pe-diatric traumatic brain injury project haveled to development of a novel dynamicmodel of intracranial pressure (26).
The PDAS offers a gateway to synthesisof clinical research and the complexities ofICU patient care. There are significant op-portunities to perform detailed pharmaco-dynamic studies not possible with earliertechnology and to delineate on a second-to-second basis the natural course andcomplications from critical illness and in-jury. Measuring the signals that patientsemit continuously and translating them tomeaningful physiologic information give usa powerful tool to understand, predict, andeventually influence the course of criticalillness (27–32).
REFERENCES
1. Moody G, Mark R: The MIT-BIH arrhythmiadatabase on CD-ROM and software for usewith it. Comput Cardiol 1990; 17:185–188
2. Moody GB, Mark RG, Goldberger AL: Phys-ioNet: A research resource for studies ofcomplex physiologic and biomedical signals.Comput Cardiol 2000; 27:179–182
3. Moody GB, Mark RG, Goldberger AL: Phys-ioNet: A Web-based resource for the study ofphysiologic signals. IEEE Eng Med Biol Mag2001; 20:70–75
4. Saeed M, Lieu C, Raber G, et al: MIMIC II: Amassive temporal ICU patient database tosupport research in intelligent patient mon-itoring. Comput Cardiol 2002; 29:641–644
5. Belair J, Glass L, An Der Heiden U, et al:Dynamical disease: Identification, temporal
aspects and treatment strategies of humanillness. Chaos 1995; 5:1–7
6. Goldstein B, McNames J, McDonald BA, et al:Physiologic data acquisition system and da-tabase for the study of disease dynamics inthe intensive care unit. Crit Care Med 2003;31:433–441
7. Kropyvnytskyy I, Saunders F, Schierek P, etal: A computer system for continuous long-term recording, processing, and analysis ofphysiological data of brain injured patients inICU settings. Brain Inj 2001; 15:577–583
8. Artnak KE, Benson M: Evaluating HIPAAcompliance: A guide for researchers, privacyboards, and IRBs. Nurs Outlook 2005; 53:79–87
9. Erlen JA: HIPAA—Implications for research.Orthop Nurs 2005; 24:139–142
10. Pace WD, Staton EW, Holcomb S: Practice-based research network studies in the age ofHIPAA. Ann Fam Med 2005; 3(Suppl 1):S38–S45
11. Garnsworthy J: Standardizing medical devicecommunications: The Medical InformationBus. Med Device Technol 1998; 9:18–21
12. Gass M: Medical Information Bus (MIB).Health Informatics J 1998; 4:72–83
13. Kennelly RJ: Improving acute care throughuse of medical device data. Int J Med Inform1998; 48:145–149
14. Cohen A, Korhonen I: Biomedical signals data-bases. IEEE Eng Med Biol Mag 2001; 20:23–24
15. Gade J, Korhonen I, van Gils M, et al: Tech-nical description of the IBIS data library.Improved Monitoring for Brain Dysfunctionin Intensive Care and Surgery. ComputMethods Programs Biomed 2000; 63:175–186
16. Mandersloot GF, Pottinger RC, Weller PR, etal: The IBIS project: Data collection in Lon-don. Improved Monitoring for Brain Dys-function during Intensive Care and Surgery.Comput Methods Programs Biomed 2000;63:167–174
17. Penzel T, Kemp B, Klosch G, et al: Acquisi-tion of biomedical signals databases. IEEEEng Med Biol Mag 2001; 20:25–32
18. Thomsen CE, Gade J, Nieminen K, et al: Col-lecting EEG signals in the IMPROVE Data Li-brary. IEEE Eng Med Biol Mag 1997; 16:33–40
19. Tsui FC, Ching-Chung L, Sun M: Acquiring,modeling, and predicting intracranial pres-sure in the intensive care unit. Biomed Eng1996; 8:96–108
20. Goldstein B, Woolf PD, DeKing D, et al:Heart rate power spectrum and plasma cate-cholamine levels after postural change andcold pressor test. Pediatr Res 1994; 36:358–363
21. Imhoff M: Acquisition of ICU data: conceptsand demands. Int J Clin Monit Comput 1992;9:229–237
22. Langenberg CJ: Implementation of an elec-tronic patient data management system(PDMS) on an intensive care unit (ICU). IntJ Biomed Comput 1996; 42:97–101
23. East TD: Computers in the ICU: Panacea orplague? Respir Care 1992; 37:170–180
568 Pediatr Crit Care Med 2007 Vol. 8, No. 6

24. Jakob S, Korhonen I, Ruokonen E, et al:Detection of artifacts in monitored trends inintensive care. Comput Methods ProgramsBiomed 2000; 63:203–209
25. McNames J, Crespo C, Bassale J, et al: Sen-sitive precursors to acute episodes of intra-cranial hypertension. In: The 4th Interna-tional Workshop in Biosignal Interpretation.Como, Italy, June 22–24, 2002, pp 303–306
26. Wakeland W, Goldstein B: A computer modelof intracranial pressure dynamics duringtraumatic brain injury that explicitly modelsfluid flows and volumes. Acta NeurochirSuppl 2005; 95:321–326
27. Michard F: Relation between respiratorychanges in arterial pulse pressure and fluidresponsiveness in septic patients with acutecirculatory failure. Am J Respir Crit CareMed 2000; 162:134–138
28. Scott RM, Smith JL, Robertson RL, et al:Long-term outcome in children with moya-moya syndrome after cranial revasculariza-tion by pial synangiosis. J Neurosurg 2004;100:142–149
29. Adelson PD, Scott RM: Pial synangiosis formoyamoya syndrome in children. PediatrNeurosurg 1995; 23:26–33
30. Ogawa A, Nakamura N, Yoshimoto T, et al:
Cerebral blood flow in moyamoya disease.Part 2: Autoregulation and CO2 resp-onse. Acta Neurochir (Wien) 1990; 105:107–111
31. Ogawa A, Yoshimoto T, Suzuki J, et al: Ce-rebral blood flow in moyamoya disease. Part1: Correlation with age and regional distri-bution. Acta Neurochir (Wien) 1990; 105:30–34
32. Yusa T, Yamashiro K: Local cortical cere-bral blood flow and response to carbondioxide during anesthesia in patients withmoyamoya disease. J Anesthesiol 1990; 13:131–135
569Pediatr Crit Care Med 2007 Vol. 8, No. 6