determinants of physical activity in rural african...
TRANSCRIPT
To the Graduate Council:
I am submitting herewith a dissertation written by Michael R. Bamman entitled “Determinants of physical activity in rural African-American adolescents.” I have examined the final copy of this dissertation for form and content and recommend that it be accepted in partial fulfillment of the requirements for the degree of Doctor of Philosophy, with a major in Exercise Science.
______________________________Jeffrey S. Hallam, Major Professor
We have read this thesisand recommend its acceptance:
_____________________________________Ed Acevedo Associate Professor
_____________________________________Scott Owens Assistant Professor
_____________________________________John Bentley Assistant Professor
Accepted for the Council:
____________________________ Dean of the Graduate School
DETERMINANTS OF PHYSICAL ACTIVITY IN RURAL AFRICAN-AMERICAN
ADOLESCENTS
A Dissertation
Presented for the
Doctor of Philosophy
Degree
The University of Mississippi
Michael R. Bamman
August 2004
Copyright © 2004 by Mike BammanAll rights reserved
3
DEDICATION
This work is dedicated to Joyce Bamman. Without her love and support this
would not have been possible.
4

ACKNOWLEDGMENTS
I would like to thank my parents James and Gale Bamman, and my wife Joyce
Bamman for believing in me when not many others did. I would also like to thank
my major advisor Dr. Jeff Hallam, for his help and guidance throughout my time
at The University of Mississippi, and my committee for their assistance and
direction over the past year. I would like to thank Alena Cushman for her help in
collecting data for this project. Finally, I would like to acknowledge two
classmates, Gina Blunt and Danielle Wadsworth, whose friendship and support
have made The University of Mississippi a much better place these last three
years.
v
ABSTRACT
The purpose of this study was to identify the determinants of PA of
African-American schoolchildren ages 12-18 in Tunica County, Mississippi. A
secondary purpose of this study was to determine the relationships among and
identify differences between recognized determinants of PA (age, body mass
index, perceived SE, and perceived barriers to PA) of the students. Assessment
included height and weight measurements, completion of the Physical Activity
Recall, self-efficacy and barriers to PA questionnaires. Subjects wore an MTI
accelerometer for seven consecutive days, except when sleeping or bathing.
Correlation matrices were conducted for male and female groups for the
independent variables self-efficacy, barriers to PA, BMI and age, and the
dependent variable, PA. Nonsignificant correlations in the male group were found
between PA and barriers to PA (r =-0.005, p = 0.977), and self-efficacy (r =
0.102, p = 0.0.527). Nonsignificant correlations in the female group were found
between and between PA and barriers to PA (r = 0.411, p = 0.119), and age (r =
0.101, p = 0.518). Stepwise multiple regression analyses were performed with
independent variables that were related to the dependent variable, PA. In males
(n = 41) the independent variables of age (r = 0.426, p<0.05), and BMI (r = 0.543,
p<0.05), were regressed on the dependent variable, PA. The final regression
model (with BMI and Age) accounted for 34% of the variance in PA. For females
(n = 43), the independent variables of BMI (r = 0.508, p<0.05), and self-efficacy (r
= 0.411, p<0.05), were regressed on the dependent variable, PA. It was
vi
discovered that the final regression model (with BMI and self-efficacy) accounted
for 34% of the variance in PA. The Chow test was conducted to compare the
regression equations for males and the regression equation for females. The
comparison of both male and female regression equations’ with the Chow test
results in a nonsignificant regression model (F = 2.848, Fcv = 3.564). The results
of this study demonstrate that rural African-American adolescent males’ PA is
predicted by BMI and age but not self-efficacy and that females’ PA is predicted
by BMI and self-efficacy, but not age. The results also show that barriers to PA
are not predictive of PA in rural African-American adolescents.
vii

TABLE OF CONTENTS
CHAPTER PAGE
I. INTRODUCTION................................................................................................1
PURPOSE OF STUDY.......................................................................................3 HYPOTHESES..................................................................................................4
OPERATIONAL DEFINITIONS..........................................................................4
DELIMITATIONS................................................................................................5
LIMITATIONS.....................................................................................................6
ASSUMPTIONS.................................................................................................6
SIGNIFICANCE OF THE STUDY.......................................................................6
II. REVIEW OF LITERATURE...............................................................................7
HEALTH BENEFITS OF PHYSICAL ACTIVITY.................................................7
DETERMINANTS OF PHYSICAL ACTIVITY IN ADULTS................................12
PHYSICAL ACTIVITY AMONG CHILDREN AND ADOLESCENTS.................18
CHILD AND ADOLESCENT DETERMINANTS OF PHYSICAL ACTIVITY......20
CONCLUSION..................................................................................................23
III. METHODS......................................................................................................25
DESIGN............................................................................................................25
SUBJECTS.......................................................................................................25
INSTRUMENTS................................................................................................26
PROCEDURES................................................................................................30
DATA ANALYSIS.............................................................................................33
viii
IV. RESULTS.......................................................................................................35
SUBJECTS.......................................................................................................36
CORRELATIONS OF DEPENDENT AND INDEPENDENT VARIABLES......41
COMPARISON OF PA MEASURES.................................................................45
BARRIERS AND PA LEVEL.............................................................................47
GRADE LEVEL AND PA LEVEL......................................................................48
REGRESSION ANALYSES..............................................................................49
COMPARISON OF REGRESSION EQUATIONS............................................52
HYPOTHESIS TESTING..................................................................................58
V. DISCUSSION..................................................................................................59
DESCRIPTIVES...............................................................................................59
VALIDATION OF PA MEASURE......................................................................60
EFFECT OF BARRIERS TO PA ON PA LEVEL..............................................62
EFFECT OF GRADE LEVEL ON PA LEVEL ..................................................62
DETERMINANTS OF PA IN FEMALES...........................................................63 DETERMINANATS OF PA IN MALES.............................................................66
COMPARISON OF REGRESSION EQUATIONS............................................68
SUMMARY.......................................................................................................69
CONCLUSIONS...............................................................................................71
RECOMMENDATIONS....................................................................................72
LIST OF REFERENCES.....................................................................................74
APPENDICES.....................................................................................................96
A. MEDICAL HISTORY AND DEMOGRAPHICS FORM...............................96
ix
B. MTI ACCELEROMETER..............................................................................99
C. SEVEN-DAY PHYSICAL ACTIVITY RECALL...........................................101
D. SAHHP QUESTIONNAIRE.......................................................................105
E. CAMPBELL QUESTIONNAIRE................................................................107
F. IRB APPLICATION....................................................................................109
G. PARENTAL CONSENT FORM.................................................................148
H. ORAL ASSENT FORM.............................................................................152
I. WRITTEN ASSENT FORM........................................................................155
J. LOG BOOK................................................................................................158
K. ADHERANCE FLYER...............................................................................160
L. SINGLE PROJECT ASSURANCE FORMS...............................................162
M. RAW DATA...............................................................................................175
VITA 184
x
LIST OF TABLES
TABLE PAGE
1. Females' Descriptive Data for Age, BMI, SAHHP, Barriers, PAR, and MTI.....37
2. Females' Frequency Data for Free Lunch, Current Sport Participation, and
Usual Activity Level.............................................................................................38
3. Males' Descriptive Data for Age, BMI, SAHHP, Barriers, PAR, and MTI.........39
4. Males' Frequency Data for Free Lunch, Current Sport Participation, and Usual
Activity Level........................................................................................................40
5. t-test data for Age, BMI, SAHHP, Barriers to PA, and PAR - Females and Males
42
6. Correlation Table for Females' Age, BMI, SAHHP, Barriers to PA, PAR, MTI.43
7. Correlation Table for Males' Age, BMI, SAHHP, Barriers to PA, PAR, MTI.....44
8. Correlation of PA Assessment Measures PAR (kcal/wk) and MTI (kcal/wk) - All
Subjects...............................................................................................................45
9. Correlation of PA Measures in METs and kcal/wk for PAR and MTI - All Subjects
46
10. Correlation of Barriers to PA to PAR (kcal/wk) - All Subjects........................47
11. Oneway ANOVA - Females' PAR (kcal/wk) and Grade Level.......................48
12. Oneway ANOVA - Males' PAR (kcal/wk) and Grade Level...........................48
13. Correlation of Females' PAR with Age, BMI, SAHHP, and Barriers to PA ....50
14. Females' Regression Summary.....................................................................51
15. Correlation of Males' PAR with Age, BMI, SAHHP, and Barriers to PA.........53
xi
16. Males' Regression Summary.........................................................................54
17. Formula - Chow Test ......................................................................................55
18. Chow Test of All Standard Regression Results............................................56
19. Chow Test Results for Comparison of Males’ and Females’ Regression
Equations.............................................................................................................57
xii
CHAPTER 1
INTRODUCTION
Recent findings from the Centers for Disease Control and Prevention's
(CDC) National Health and Nutrition Examination Survey (NHANES) show that
more Americans are becoming overweight and obese. Data show that the
percentage of adults classified as overweight or obese has risen from 47% in
1980 to 61% in 1999 (National Center for Health Statistics [NCHS], 2000). Also,
similar findings of increased obesity are evident in adolescents. The number of
overweight children and adolescents in the United States has almost tripled since
1980 (CDC, 2001). The 1999 NHANES results for children showed 13% of
children ages 6-11 years are overweight, up from 11% in the previous NHANES
survey concluded in 1994. The number of overweight adolescents ages 12-19
increased from 11% to 14% in the same time span. The increase in child and
adolescent obesity is greater in the state of Mississippi. Penman (2000) shows,
by comparison, 30% of adolescents in Mississippi met the criteria for being
overweight (>85 percentile BMI). In 2001, the self-reported incidence of
overweight for Mississippi middle school and high school students was 25%. This
number was significantly higher among girls (32%) when compared to boys
(20%) in the same age group (Mississippi State Department of Health [MSDH],
2001). These changes illustrate that obesity has reached epidemic proportions in
the United States and in the State of Mississippi. At this time however, there are
no data available for Tunica County, Mississippi, concerning obesity and activity
rates for the adolescent population.
1
Exercise science professionals have long emphasized the benefits of
physical activity (PA) as a key combatant of adult and childhood obesity. As
recently as 1993, evidence shows significant inverse relationship between self-
reported PA and total body weight (TBW), skin fold measurements, and body
mass index (BMI) (Williamson, et al, 1993). The importance of increasing the
level of PA is not only essential to reducing obesity, but PA also carries
significant health benefits. Key health benefits of PA include: a reduction in
overall mortality, a decreased risk of cardiovascular disease, a decreased risk of
developing hypertension (HTN) and a reduction in blood pressure levels in
individuals who have HTN, a decreased risk of developing non-insulin dependent
diabetes mellitus (NIDDM), and a decreased risk of colon cancer. Many of these
adverse health effects are also associated with overweight and obesity in
children and adolescents. Specifically, obesity in children and adolescents is
found to be related to increased morbidity and mortality later in life, an early
onset of NIDDM and HTN, a number of orthopedic complications, as well as
various negative psychosocial effects (CDC, 1996). Subsequent to these
findings, increasing PA levels in both children and adolescents has become an
integral part of recent statements and recommendations by the United States
government (HHS, 2001a; HHS, 2001b; CDC, 2001).
Identification of determinants of PA in the recent literature shows that
adolescent PA is influenced by several factors. The first population-based cohort
study to examine psychosocial predictors of PA in adolescents utilizing males
and females of multiple ethnicities across different levels of exercise intensity
2
was the Stanford Adolescent Heart Health Program (SAHHP) (Reynolds, et al,
1990). The SAHHP, as well as other studies, identified self-efficacy (SE) as the
most significant determinant of physical activity in adolescents, across ethnicity
and geographic settings (Zakarian, Hovell, Hofstetter, Salles, & Keating, 1994;
Trost, et al, 1997). Specific barriers to PA in adolescents were identified by
Allison, Dwyer, and Makin (1999b). They showed that adolescents identified
barriers that resulted in a lack of time, as most concerning. Subjects also
identified lack of energy and low motivation as other significant barriers to PA.
Levels of PA in adolescents are also determined by differences in sex,
ethnicity and age. Several studies show that males were significantly more active
than females across all intensity levels (Aaron, et al, 1993; Garcia, et al, 1995;
Trost, et al, 2002; Allison, Dwyer, & Makin, 1999a). The disparity in ethnic, sex
and age differences in PA has also been reported on two occasions in
publications by the United States government (CDC, 1992 & CDC, 2001).
Purpose of Study
The purpose of this study was to identify the determinants of PA of
African-American schoolchildren ages 12-18 in Tunica County, Mississippi. A
secondary purpose of this study was to determine the relationships among and
identify differences between recognized determinants of PA (age, body mass
index, perceived SE, and perceived barriers to PA) of the students.
3
Hypotheses
To address the purpose of the study the following null hypotheses were tested.
Ho1: There is no significant relationship between level of PA and perceived
SE, perceived barriers to PA, age, and BMI for males in this population.
Ho2: There is no significant relationship between level of PA and perceived
SE, perceived barriers to PA, age, and BMI for females in this population.
This study also considered the following alternative hypothesis.
Ha1: Males’ level of pa will be influenced by their level of perceived SE,
followed by the perceived barriers to PA, followed by age, and BMI.
Ha2: Females’ level of pa will be influenced by their level of perceived SE,
followed by the perceived barriers to PA, followed by age, and BMI.
Operational Definitions
Adolescent was defined as a person age 12 through age 19.
Risk of overweight was defined as a BMI measurement above the 85th
percentile as measured by the Halls.md BMI calculator (Rosenthal, Bain,
Bush, & Warner, 1994).
Overweight was defined as a BMI measurement above the 95th percentile
as measured by the Halls.md BMI calculator (Rosenthal, Bain, Bush, &
Warner, 1994).
Light activity was determined by 7-day Activity Recall activities of 1.0 – 2.9
METs (Sallis, et al, 1985), and MTI activity counts of less than 1952
counts per minute (Freedson, Melanson, & Sirard, 1998).
4
Moderate activity was determined by 7-day Activity Recall activities of 3-
5.0 METs. (Sallis, et al, 1985), and MTI counts between 1953 and 5724
counts per minute (Freedson, Melanson, & Sirard, 1998).
Hard activity was determined by 7-day Activity Recall activities of 5.1 – 6.9
METs (Sallis, et al, 1985), and MTI counts between 5725 and 9498 counts
per minute (Freedson, Melanson, & Sirard, 1998).
Very Hard activity was determined by 7-day Activity Recall activities of 7.0
METs or greater (Sallis, et al, 1985), and MTI counts above 9498 per
minute (Freedson, Melanson, & Sirard, 1998).
Self-efficacy was defined as an individual’s belief in his or her ability to
make changes with regard to a specific exercise behavior (Bandura,
1986).
Delimitations
This study was limited to the following restrictions:
1. Sample of students ages 12-19 were taken from Rosa Fort High School
and The North Mississippi Delta Boys and Girls Club located in Tunica
County, Mississippi.
2. Based upon the following power analysis, the acceptable sample of
students was at least 40 males and 40 females. With power set at 0.80, an
alpha level of 0.05, and an estimated effect size of 0.25 the formula to
determine the necessary number of cases (n) is written as follows (Cohen
& Cohen, 1984):
5

n = L / f2 + k + 1 where f2 = R2 / 1 – R2
n = 11.94 / f2 + 4 + 1 where f2 = 0.25 / 1 - 0.25
n = 11.94 / 0.333 + 4 + 1 n = 35.82 + 4 + 1 n = 39.82
Limitations
1. Subjects were selected from a convenience sample of the population.
Assumptions
1. All subjects followed the study protocol as it relates to the subjective
assessment and objective monitoring of physical activity.
Significance of the Study
This study allows researchers, school officials, community leaders, and
parents to better understand the possible determinants of, and barriers to PA in
African-American adolescents in Tunica County, Mississippi. This research also
made a significant contribution to the existing literature relating to determinants of
PA in African-American adolescents.
6
CHAPTER 2
REVIEW OF LITERATURE
Health Benefits of Physical Activity
In 1996, the U. S. Department of Health and Human Services released,
Physical Activity: a Report of the Surgeon General, a report of the Surgeon
General that combined and presented decades of research on adult PA and
health. The report stressed the importance of daily PA in reducing the risk of
developing or dying from some of the leading causes of morbidity and mortality in
the United States.
Overall mortality is found to be significantly lower among persons with
moderate or higher levels of both PA and cardiorespiratory fitness. When
compared with people who are most active, sedentary persons have up to a 2-
fold increased mortality risk (Slattery and Jacobs 1988; Slattery, Jacobs,
Nichaman 1989; Leon and Connett 1991; Stender et al. 1993; Sandvik et al.
1993; Chang-Claude and Frentzel-Beyme 1993; Kaplan et al., 1987; Arraiz,
Wigle, Mao 1992; Paffenbarger et al. 1993). The CDC report also illustrated that
a person’s level of PA, and its relationship to cardiovascular disease (CVD)
mortality was inversely related (Kannel & Sorlie, 1979, Paffenbarger, et al., 1984,
Kannel, et al, 1986, Ekelund, et al, 1988, Blair, et al, 1989, Lindsted, Tonstad,
Kuzma, 1991, and LaCroix, et al, 1996). Multiple studies also showed that there
is even a significant dose response relationship between PA level and overall
7
mortality (Arraiz, Wigle, & Mao, 1992, Sandvik, et al, 1993, & Blair, et al, 1995).
These data demonstrate that the protective benefits of PA occur significantly at
moderate levels of PA, with the benefits increasing with increasing levels of PA.
Other factors that affect the development of CVD, such as the presence of
low HDL cholesterol (Leon 1991a; Krummel et al. 1993; Superko 1991; Durstine
and Haskell 1994; Stefanick and Wood 1994; Leon, 1991b; Duncan, Gordon,
Scott 1991; Tsopanakis et al. 1989) are shown to improve significantly with
increased levels of PA. For persons with existing CVD, PA also influences
several of the concurrent mortality risk factors. Regular PA reduces the incidence
and severity of, and delay the onset of, myocardial ischemia by certain
physiological adaptations that together reduce myocardial oxygen demand
(Jorgensen, et al, 1977; Cohen, 1985; Smith & Leon, 1992; Laughlin, 1994; Leon
& Bloor, 1968, 1976; Scheuer, 1982; Laughlin, 1994; Tomanek, 1994;
Overholser, Laughlin, & Bhatte, 1994; Underwood, Laughlin, & Sturek, 1994).
The risk of cardiac arrhythmias may also be reduced in persons with a physically
active lifestyle (Leon, 1991; Leon, et al, 1987). In populations of cardiac
rehabilitation patients, regular exercise training reduced the overall risk of sudden
cardiac death even among persons with significant CAD (O’Connor, et al, 1989).
Evidence of PA significantly affecting the development and progression of
established CAD, as a part of comprehensive risk factor reduction programs, has
been published as well (Ornish, et al, 1990, 1998; Schuler, et al, 1992;
Hambrecht, et al, 1993; Haskell, et al, 1994).
PA also positively impacts significant independent risk factors for CVD.
8
Hypertension is a widespread health problem in the US, with over 55 million
persons ages 20-74 classified as hypertensive (National Center for Health
Statistics [NCHS], 2000). Cohort studies with both men and women show that a
sedentary lifestyle is significantly related to an increased risk of developing HTN
(Paffenbarger, et al, 1983; Blair, et al, 1984 & Folsom, et al, 1990). These studies
also showed an overall dose response relationship between PA and HTN. In
addition, a five-year trial with over 200 adults showed that sedentary control
subjects were 2.4 times more likely to develop HTN than subjects in a moderate
PA group (Stamler, et al, 1989). The control of HTN is important in lowering not
only an individual’s CVD risk, but the risk of stroke as well. Several randomized
studies show that regular aerobic exercise significantly lowers elevated diastolic
and systolic blood pressure (Arroll & Beaglehole, 1992 & Kelley & McClellan,
1994).
The prevalence of NIDDM in the United States is also important due to the
high mortality and morbidity costs associated with this condition (Rubin, et al,
1993). As of 1996, over 8 million persons in this country are currently diagnosed
with NIDDM. Not only is NIDDM an independent risk factor for CVD, but is also
linked to stroke, peripheral vascular disease, and congestive heart failure. The
relationship of physical inactivity and NIDDM has been examined in cross-
sectional, cohort, and randomized trials, in the United States, Europe, and Asia,
showing a significantly increased incidence of NIDDM in sedentary persons
(Kriska, Blair & Pereira, 1994; Zimmet, 1992; King & Kriska, 1992; Kriska &
Bennett, 1992; King, Taylor, Zimmet, et al., 1984; Dowse et al., 1991; Ramaiya et
9

al., 1991; Kriska, Gregg, et al., 1993; Chen & Lowenstein 1986; Frish et al.,
1986; Holbrook, Barrett-Connor & Wingard, 1989; Kaye et al., 1991; Uusitupa et
al., 1995; Helmrich et al., 1991; Manson et al., 1992; Eriksson & Lindgärde,
1991; Pan, Li & Hu, 1995). An inverse dose response relationship between PA
and NIDDM has also been demonstrated in population studies of both males and
females. The effects of PA have also show to be protective against the
development of NIDDM in persons with impaired glucose tolerance. Multiple
intervention studies, with follow-up durations of over five years, show that regular
exercisers have less than a 0.50 relative risk of developing NIDDM (Eriksson &
Lindgärde, 1991; Pan, Li & Hu, 1995) when compared to sedentary subjects.
Another long-standing health crisis in the United States is the increased
incidence of cancer. As a US citizen, one has a 43% chance of developing
cancer, and a 21.2% percent chance of dying from the disease (Feuer & Wun,
1999). The most widely investigated form of cancer with respects to its
relationship with PA is colon cancer. Of all the studies utilizing leisure time PA,
the majority showed an inverse dose response relationship with the risk of colon
cancer. These results were consistent across various study types and subject
groups, and utilizing different endpoints, mortality and incidence (Severson, et al,
1989; Whittenmore, et al, 1990; Kono, et al, 1991; Giovannucci, et al, 1995;
Longnecker, et al, 1995). Unfortunately, the protective benefit of PA has not been
established with great consistency in its association to all other types of cancer.
Many of these same health consequences related to overweight and
obesity are initiated in childhood or adolescence. Overweight children and
10
adolescents have show to be at increased risk for various chronic diseases later
in later life. Freedman, Dietz, Srinivasan, and Berenson (1999), found that nearly
60% of overweight children had at least one cardiovascular risk factor compared
to 10% of those with a BMI< 85th percentile for their age and sex. Of these
overweight children, 25% had two or more risk factors. Of the adverse medical
consequences of overweight and obesity that directly affect children and
adolescents, NIDDM, HTN, and dyslipidemia have the greatest impact on overall
health. Overweight and obesity are demonstrated to be independent predictors
for developing these health consequences, beginning in childhood (Berenson et
al., 1998). The development of type II diabetes among children and adolescents
is increasing at an alarming rate, accompanying the national rise in overweight
among teens (Pinhas-Hamiel, Dolan, Daniels, Standiford, Khoury, & Zeitler,
1996). Many studies have demonstrated the relationship between PA and insulin
resistance in obese youth. Significant research has also recently identified a
strong relationship between increased PA and a reduction in the risk for NIDDM
in non-diabetic, normal weight children and adolescents (Schmitz, Jacobs, Hong,
Steinberger, Moran, & Sinaiko, 2002; Quarry-Horn, et al, 2003). Persistent
hypertension does not typically occur in children. However, it has been found to
occur approximately nine times as much among children who are overweight and
obese when compared with children at normal weight (Lauer, Connor, &
Leaverton, 1975). In Lauer's study, almost 60% of children with persistent
hypertension had comparative weights >120% of the median for their sex, height
and age. Childhood blood pressure and change in BMI were consistently the two
11
most powerful predictors of adult blood pressure across all ages and both sexes.
In addition, hyperlipidemia in children is significantly related to overweight and
obesity. Freedman and colleagues (1999) showed that 90 percent of the children
with high levels of triglycerides were also overweight. While the results of the
research between PA and overall cholesterol levels in children and adolescents
have not been in agreement, a strong positive relationship has been consistently
identified between PA levels and HDL cholesterol (Armstrong & Simmons-
Morton, 1994; Riddoch & Boreham, 1995; Twisk, 2000).
Determinants of Physical Activity in Adults
Reliable assessment of PA levels among American adults was effectively
addressed in the Five-City Project (Sallis, et al, 1985). Sallis and colleagues
measured PA by questionnaire, as well as estimation of weekly kcal expended,
across several levels of intensity and activity settings. Results of the Five-City
Project showed significant relationships between exercise and various personal
characteristics, such as education level, occupation, marital status, and, within
the moderate PA subcategory only, ethnicity. These relationships remained
significant across all levels of age and sex. The Five-City Project was found to
have distinct advantages over many of the previous epidemiological studies
assessing PA. This study was able to characterize patterns of activity in a large
population, assess PA at all intensity levels, and in work and leisure settings,
provide an estimate of total caloric expenditure, specify the different types of
activities in population subgroups, had acceptable reliabilities and was
12

appropriate for evaluating changes in physical activity habits in populations.
Subsequent to a uniform assessment of PA, identification of characteristics and
traits that could predict exercise behavior became the next rational goal, in the
research on PA. Sallis, Dishman, and Orienstien (1985) reviewed previous
research on determinants of participation in supervised exercise programs and
spontaneous PA. The authors acknowledged several correlates, identified in
personal characteristics that were similar to those discussed in the Five-City
Project (Sallis, et al, 1985). Personal characteristics such as previous
participation in high school sports, education level, and occupation all have a
significant effect of the probability of exercise. Almost two-thirds of physically
active adults surveyed had participated in sports in their youth. Although a history
of participation in sports can be a strong predictor of PA, its influence may have
been overridden by other factors (Clarke, 1973). The authors show that persons
with higher levels of education had significantly higher activity levels (General
Mills, 1979; Canada fitness Survey, 1983; Harris, 1970; Sallis, et al, 1985).
Occupation type was also a strong predictor of PA level. Blue-collar workers
were less likely to engage in either leisure time activity or supervised exercise
(Oldridge, 1982; Cox, 1984). Environmental factors found to significantly affect
PA participation included weather, time constraints, and social reinforcements.
Only 10% of runners reported that weather had no impact on their activity
patterns. Changes in climate conditions are shown to influence the likelihood of
outdoor activity (Sacks & Sachs, 1981; Canada Fitness Survey) across all activity
levels. Lack of time was identified as a significant barrier to PA among exercise
13
dropouts, but was not a barrier to those surveyed that were adherent (General
Mills) to exercise. Social reinforcement was also predictive of PA participation.
The PA level of families was found to have a positive effect on its members
(Greendorfer, 1983; Butcher, 1983). In addition, adherence to clinical exercise
programs was strongly linked to reinforcement from program staff or from an
activity partner (Wankel, 1984; Stalonas, Johnson, and Christ, 1978).
Interestingly, survey results showed that membership fees are not perceived as
barriers to participation in exercise programs (Canada Fitness Survey & Iverson,
Fielding, Crow & Christenson, 1985). Only 10% of those surveyed indicated that
less expensive facilities would likely increase their levels of PA.
Other studies identified additional environmental barriers to exercise in
population samples of 3,000 women (King, et al, 2000) and of 1800 adults
(Brownson, et al, 1997). Subjects in both studies cited lack of time, lack of
energy, and being too tired, as the most important barriers to PA. Women
surveyed by King et al, also identified the burden of care-giving duties, and a lack
of a safe place to exercise as barriers to PA. Adults participating in Brownson’s
study also recognized the barriers of obtaining enough PA on one’s job and not
being motivated to exercise. When King and colleagues compared the results
across ethnicity, the authors found that, aside from lack of a safe place to
exercise, the most frequently listed barriers differed only in their rank order
across Caucasian and African-American women. For example, African-American
women listed a lack of a safe place to exercise as the top barrier to exercise,
whereas Caucasian women listed it as the 6th most frequent barrier. Caucasian
14
women listed lack of time as the most frequent barrier, while African-American
women ranked it 5th most frequently. Regression models showed that significant
predictors of PA in the Caucasian sub-group were age (older age associated with
less activity); education level (lower education level associated with less activity);
lacking energy (lower energy associated with less activity) and self-
consciousness about appearance (less confident associated with less activity).
Within the African-American sub-group, three different variables were found to be
significant. Each significant variable was a sub-category located within the
“neighborhood characteristics” category. Frequently observing others exercising
in one’s neighborhood (greater frequency associated with more activity), care-
giving duties (more time spent care giving associated with lower activity), and the
presence of unattended dogs in one’s neighborhood (more dogs associated with
less activity) were the only variables that reached significance. Neighborhood
characteristics were also found to be significant barriers to PA by Brownson et al.
This study identified neighborhood characteristics such as the presence of
sidewalks (positive), enjoyable scenery (positive), heavy traffic (negative), and
hills (positive) were significant predictors of PA levels. Across all levels of
socioeconomic status (SES), the lack of childcare and the burden of care-giving
duties were not acknowledged as significant barriers in this study. However,
care-giving duties have been cited in previous studies as a significant barrier to
exercise for women, across various minority groups and nationalities (King &
Brassington, 1997; Zunft, et al, 1999; Grassi, Gonzalez, Tello, and He, 1999).
Heesch, Brown, and Blanton (2000) compared perceived barriers to
15

exercise across ethnicity and stages of exercise adoption in women over 40
years. Pre-contemplators, both Caucasian and African-American, listed being too
tired and having a lack of energy as the leading barriers to exercise. However,
the similarities between the groups end with the pre-contemplators. In the
contemplator groups, Caucasian women listed lack of time as the leading barrier,
compared with a lack of a safe place to exercise and care-giving duties in the
African-American group. The Caucasian preparer/active group identified being
too tired while the African-American group listed a lack of time as the leading
barrier to exercise. Interestingly, the authors showed that over 55% of women
(over 40) surveyed were regular exercisers, compared with national averages
that ranged from 12-22%.
The Coronary Artery Risk Development in Young Adults (CARDIA) study
showed over 30% of African-American women and 25% of Caucasian women did
not achieve moderate exerciser status (Bild, et al, 1993). The authors assessed
physical activity, body composition, and demographic and psychosocial variables
of Caucasian and African-American women in five regional sites. The authors
found significant differences in all measured variables except the women’s
competitiveness level, their level of social support, and their level of instrumental
support. African-American women showed significantly lower participation levels
in all measured areas of PA and exercise except four: dancing, bowling, running,
and home-related exercise. The authors classified subjects in quintiles according
to activity level. There were twice as many African-American women in the
lowest quintile as Caucasian women and half as many in the highest activity
16

group. African-American women had significantly lower overall PA scores across
all ages, education levels, and all levels of SES.
Ford and colleagues (1991) assessed SES levels and their relationship to
PA behaviors. Their data show significantly lower levels of total, leisure-time, job-
related, and household PA in lower SES women when compared with higher
SES women. Each SES group reported a moderate percentage of regular
walking activity among its subjects. However, the average percentage of lower
SES women was significantly higher than the upper SES group (41% vs. 33%)
across all sub-levels of walking activity except leisure-time walking. While more
upper SES women walked for leisure (57% vs. 42%), and there was no
difference in the percentage of women in either group that walked during lunch or
other work-related breaks (24% lower vs. 17% upper), a significantly higher
percentage of lower SES women walked to school or work (25% vs. 7%) and for
errands (73% vs. 50%). The authors calculated total weekly kcal expenditure
using Paffenbarger’s physical activity index. These results were similar to those
stated above in the CARDIA study (Bild, 1993). Only 7% of lower SES women
expended >2000 kcal per week compared with 16.8% of higher SES women.
Adult PA determinants have been identified with a great amount of
success. We can clearly see that personal determinants such as education level,
marital status, ethnicity, previous sport participation, and job occupation are
significant determinants of adult PA. Additional environmental determinants such
as weather conditions, time constraints, social reinforcements, lack of energy,
17
being too tired, the burden of care-giving duties, and a lack of a safe place to
exercise also affect PA in adult populations. We have seen that these barriers
are different across many covariates such as stages of exercise adoption,
ethnicity, and SES.
Due to the alarming rise in adult obesity and reduction in PA there is a
great amount of attention being placed on adult PA levels and determinants of
physical activity. Perhaps more important to our society at this time, is that
children and adolescents in the United Sates are a part of the same crisis.
Identification of the determinants of PA, how they differ among subpopulations,
and the strategies to overcome barriers in children and adolescents is a vital
direction of research.
Physical activity among children and adolescents
The 2001 Youth Risk Behavior Survey (YRBS) shows that while 64% of
adolescents in grades 9-12 nationwide, participate in at least 20 minutes of
vigorous activity on three or more days per week, over 9% of students in this age
group are completely sedentary (CDC, 2001). Furthermore, adolescents in the
state of Mississippi show significantly lower levels of PA. Only 55% meet the
goals for vigorous activity, with females (57% nationwide versus 43% in MS)
comparing much less favorably than males (72% nationwide versus 68% in MS)
(MSDH, 2001). In MS, the percentage of sedentary adolescents almost doubles
from the nationwide prevalence, to 15.6%. The MS percentages of adolescents
who meet the guidelines for moderate PA have not changed significantly from
18

recent statistics of 52% in 1995, and 53% in 1997. However, this decrease is not
demonstrated in middle school students in MS. Over 65% of students in grades
6-8 report meeting the guidelines for vigorous activity.
Student enrollment and participation in physical education classes in MS
is also significantly lower than national norms. In MS, only 37% of high school
students are enrolled in physical education classes, compared to nationwide
participation rate of 51% (CDC 2001, MSDH, 2001). The national average of
32% of students participating in daily physical education is also significantly
higher than the MS participation rate of 23% (CDC 2001, MSDH, 2001). These
disparities are not present when comparing MS middle school students to the
national norms. Almost 40% of middle school students in the state of MS get
daily physical education (MSDH, 2001).
When examining these PA rates by sex we see an even larger gap
between national averages and MS averages. Males in the state of MS compare
satisfactorily with national rates on all of the measured PA categories (Sedentary
rates – 10.6% vs. 7.2%, PE enrollment – 47% vs. 55%), while females in MS are
well below the national averages in these areas (CDC 2001, MSDH, 2001). Over
47% of adolescent males in MS participate are enrolled in PE, which compares
favorably with national averages of 55%, and over 34% of MS students receive
daily PE compared with a national average of 36%. Only 10.6% of adolescent
males in MS report no PA, compared with 7.2%, nationally. For females, only
18% of MS high school students are enrolled in physical education and only 13%
receive daily physical education, compared with 48% and 28%, nationally (CDC,
19

2001, MSDH, 2001). Worse yet, over 20% of MS female adolescents surveyed
are completely sedentary. This is almost double the national rate for females of
11.6%.
Activity objectives of Healthy People 2010 (CDC, 2001) relevant to
children and adolescents seek to increase the proportion of adolescents who
engage in moderate PA for at least 30 minutes on 5 or more of the previous 7
days (Objective 22-6), increase the proportion of adolescents who engage in
vigorous PA that promotes cardiorespiratory fitness 5 or more days per week for
20 or more minutes per occasion (Objective 22-7) and increase the proportion of
adolescents who spend at least 50 percent of school physical education class
time being physically active (Objective 22-8). These objectives were adjusted
from healthy people 2000 recommendations that 30% of adolescents participate
in regular moderate PA and 75% participate in regular vigorous PA.
Child and adolescent determinants of physical activity
The Stanford Adolescent Heart Health Study (Reynolds, et al, 1990) was
the first population-based cohort study to examine psychosocial predictors of PA
in adolescents utilizing males and females of multiple ethnicities. The authors
established the importance of SE (i.e., confidence in one’s abilities to overcome
perceived and actual barriers to PA) as an exercise determinant in adolescents.
After controlling for pre-test PA level and subject’s BMI, SE shows to be the most
significant predictor of PA at all stages of follow-up (4 and 16 months).
Furthermore, SE shows to be a significant predictor of vigorous PA in groups of
20

lower SES and minority adolescents (Zakarian, Hovell, Hofstetter, Salles, &
Keating, 1994), and in rural 5th grade children (Trost, et al, 1997), even when
controlled for age and sex.
Dwyer and colleagues (1998) measured SE of high school students
across a broad range of perceived barriers and showed that levels of SE differed
according to whether barriers to PA were perceived as more external (i.e.,
environmental) or internal (i.e., motivation). With each type of perceived barrier
(positive association with external barriers and a negative association with
internal barriers), level of SE was a significant predictor of PA. Allison, Dwyer and
Makin (1999a) studied this relationship of SE and PA by separating possible
vigorous PA settings into three subcategories, physical education classes; other
school-related activity; and out of school activity. The authors found that the
significant relationship of PA and SE was maintained across two of the three
settings, other school-related activity, and out of school activity. Specific barriers
to PA in a high school population were also studied by Allison, Dwyer, and Makin
(1999b). They discovered that subjects were most concerned about barriers that
resulted in a lack of time (time consumed by schoolwork as well as other
interests). To a lesser extent, the subjects identified lack of energy and low
motivation as other significant barriers to PA. The authors also found that the
perceived barriers to PA were not constant across all grade levels. Perceived
barriers were only predictive of PA in subjects in grade 9.
In 1993, Aaron et al., identified significant differences in PA levels across
sex, ethnicity and age while establishing a standardized, reliable self-report
21
questionnaire to track PA in children and adolescents. The authors showed that
males were significantly more active than females (22.5 hr/wk vs. 6.6 hr/wk),
across all intensity levels. Similar sex differences have been demonstrated since.
Notably, Garcia et al (1995), showed sex as a significant predictor of PA in a
multi-racial cohort study. In addition, Trost and colleagues (2002) demonstrated
significant differences in levels of vigorous PA in boys (2.03 bouts/wk) and girls
(0.70 bouts/wk) across all grade levels assessed (1-12).
Data from Aaron (1993) also showed that PA levels of females
significantly decreased from ages 12-15+. Prior to Aaron (1993), it was
demonstrated that PA level decreases with age in children 6-18 (Saris, Elvers,
Van’t Hof & Binkhorst, 1986 & Verschuur & Kemper, 1985). The significance of
age has continued to be noteworthy, whether measured as vigorous PA (Allison,
Dwyer, & Makin, May, 1999; Trost, et al, 2002), or through daily moderate
physical activity (Trost, et al).
In both males and females, Aaron (1993) showed Caucasian adolescents
had a significantly higher PA level than African-Americans and Hispanics (15.2
hrs/wk vs. 11.9 hrs/wk). This difference supports previous reports by Gottlieb and
Chen (1985), who showed that Caucasian adolescents were more likely to
engage in PA than either African-American or Hispanic youth. The disparity in
ethnic differences in PA has been reported on several occasions by the United
States government (CDC, 1992 & CDC, 2001). This disparity is greater among
girls, with Caucasian girls participating in regular moderate PA at a remarkably
higher rate (27.5%), compared with Latino girls (20.3%), and African-American
22
girls (17.4%). African-American and Latino schoolchildren cited a dislike of their
physical education classes, an unpleasant association with sweating or
perspiring, and a lack of opportunity to participate in their PA classes, as the
main barriers to physical activity. Many of the girls surveyed stated that a fair
opportunity to participate in physical education class would greatly increase their
PA (Taylor, et al, 1999). These subjects also identified peer and family support
as significant predictors of PA.
Zakarian and colleagues (1994) also found social support to be an
important correlate of PA in minority adolescent subjects. For male subjects, peer
support was identified, while female subjects identified family support as
significant predictors of PA. Much of the literature shows that parents and family
play important roles to their children and are the major sources of reinforcement
and modeling when it comes to PA. In 1992, Sallis and colleagues discovered no
association with children’s PA and parent characteristics (PA level, with how
much they played with the child, hours the parents worked, number of parents in
the household [one or two], or parental education). The authors did find
significant relationships between children’s PA and the parents as a source of
transportation to the children’s activities. For male subjects, amount of parental
encouragement was also significant in predicting PA. In contrast, Stuckey-Ropp
and DiLorenzo (1993) found that 5th and 6th grade subjects’ (both boys and girls’)
physical activity level was significantly influenced by their mothers’ perception of
activity barriers and parental modeling of PA.
23
Conclusion
Determinants of PA in adolescents differ from that of adults in many ways.
The influence of age on child and adolescent PA, as well as sex differences in
PA has been well established through the recent literature. Similarly, the impact
of SE on PA across all levels of age and sex has been well known for many
years. While researchers differ on the impact of parental and peer support and
their effects on PA levels, they agree that there are significant ethnic disparities
in child and adolescent PA. It has been demonstrated repeatedly that minority
adolescents participate in recommended levels of moderate and vigorous PA at a
far lower percentage than Caucasian youth belonging to the same age groups. In
addition, it has recently been publicized that minority adolescents are the fastest-
growing group of obese youth in the United States (NCHS, 2000). The literature
reviewed on PA determinants, shows no assessment of rural African-American
adolescents. Identification of any determinants of PA, would allow researchers to
develop strategies to increase the levels of PA in minority populations, or to
adjust current policies in order to create “culturally appropriate” programs for
increasing PA in minority populations.
24
CHAPTER 3
METHODS
Design
This study was designed as a causal comparative study. The research
tested the hypotheses of no relationship between the continuous criterion
variable and multiple predictor variables in both male and female adolescents.
This research identified the unique contribution of age, BMI, perceived SE, and
perceived barriers to PA to both male and female adolescent populations in
Tunica County, Mississippi.
Subjects
This project took place in Tunica County, Mississippi. Tunica County is a
rural (20.3 persons per square mile versus 79.6 [US average]), predominantly
African-American (70.2% versus 12.3% [US average]) county in the Mississippi
delta with a total population of 9,227 persons. The county population is largely
impoverished (median household income of $19,300 versus $37,000 [US
average]; 26.6% of the population below poverty level versus 13.3% [US
25
average]) and undereducated (24.2% county population over 25 yrs old with high
school diploma or greater versus 53.9% of US population with same). The
segment of Tunica County under the age of 18 is 31.7% (US average 25.7%). As
previously demonstrated, approximately 30% of Tunica County adolescents meet
the criteria for overweight. According to Mississippi census data (2000) there
were 975 African-American adolescents between the ages of 12-18 enrolled in
Tunica County public schools.
Subjects for this study (n=84) were recruited through Rosa Fort High
School and The North Mississippi Delta Boys and Girls Club. Permission to
assess adolescents ages 12-19 was obtained from the Tunica County School
Board, and the Director of the North Mississippi Delta Boys and Girls Club, from
each student, and from his or her parents/guardians. Subject recruitment at Rosa
Fort High School was limited to students enrolled in physical education classes.
Adolescents with orthopedic/musculoskeletal conditions or chronic
diseases that prevent them from participating in any regular PA as identified by
the health history form (Appendix A) were excluded from the study.
Instruments
Activity levels were assessed by two measures. All subjects wore a
physical activity monitor for seven consecutive days and completed the 7-day
physical activity recall questionnaire for the previous seven-day period (PAR).
The MTI model WAM 7164 activity monitor (Manufacturing Technology
Inc., Fort Walton Beach, FL) (Appendix B) is a measurement device that tracks
26
PA by measuring accelerations from 0.05 to 2.1 G. The MTI is equipped with a
0.1 to 3.6-passband filter, which discriminates human movement from vibrations.
Output from the MTI is sampled 10 times per second and summed over user-
defined time intervals. The MTI is capable of 22 days continuous recording.
Accelerometery, in general, has been established as a reliable and valid
means of activity assessment in children (Coleman, Saelens, Wiedrich-Smith,
Finn, & Epstein, 1997; Matthews & Freedson, 1995; Yngve et al, 2003). The
authors show significant correlations between accelerometry and adjusted heart
rates in a sample of 8-12 year old obese children (r = 0.71) (Coleman, Saelens,
Wiedrich-Smith, Finn, & Epstein). Specifically, the MTI was validated against
energy expenditure measured by indirect calorimetery (Freedson, Melanson, &
Sirand, 1998). The data show the MTI to be a valid instrument for quantifying
energy expenditure in 10-14 year old children during treadmill exercise. Ekelund
(2001) and colleagues found activity counts from the MTI to contribute
significantly to the explained variation in total energy expenditure (R2 = 0.54) and
was found, in combination with sex, to be the best predictor of activity energy
expenditure (R2 = 0.45) in a sample of 9 year old children.
Data taken as part of the Amherst Health and Activity Study (Trost, Pate,
Freedson, Sallis & Taylor, 2000) show that the optimal duration for PA monitoring
with the MTI is 7 days. Researchers found that a 7-day protocol in school-age
children (grades 1-12) resulted in acceptable estimation of moderate to vigorous
PA (R2 = 0.76 – 0.87).
27
While the MTI is an objective tool for assessing PA, there is however, a
limited ability to assess cycling, ambulation on a grade or other arm-intensive
activities. Furthermore, converting MTI counts to units of energy expenditure may
provide inaccurate estimates due to additional measurement error (Sirard & Pate,
2001; Sallis et al, 1990).
The MTI accelerometer provides an output file that contains daily
kilocalories expended and daily METS accumulated. These kcal/d and MET
results were calculated by the MTI software using a combination of the Freedson
equation and the Work Energy Theorem.
The PAR (Appendix C) is a widely used PA instrument in exercise science
and epidemiological research. In recent years, the PAR has been used in several
intervention studies including Project Active (Dunn, et al., 1997; Dunn et al.,
1999), the Stanford Five City Project (Blair 1984; Sallis, et al., 1985), and Project
PACE (Calfas et al., 1996). The validity of the PAR has been established in
comparisons with objective fitness measures such as VO2 and percent body fat
(Blair et al., 1985; Jacobs, Ainsworth, Hartman, & Leon, 1993). Further studies
showed convergent validity with the PAR and direct observation (Wallace,
McKenzie & Nader, 1985) as well as with activity monitors (Rauh, Hovell, Sallis &
Hofstetter, 1992; Matthews & Freedson, 1995). Washburn and colleagues (2003)
assessed the accuracy of the PAR in measuring total daily energy expenditure
and PA energy expenditure by comparing the PAR with doubly labeled water.
The authors found no difference in total daily energy expenditure or PA energy
expenditure as measured by doubly labeled water when compared to PAR. No
28

differences were detected in the overall sample of men and women or for each
sex separately. The PAR is also found to be a valid and reliable instrument with
adolescents. Sallis, Buono, Roby, Micale, & Nelson, (1993) report a test-retest
reliability of the PAR of r = 0.81 in a large sample of schoolchildren. Very hard PA
shows good reliability (r = 0.53) when correlated with direct heart rate
measurements above 160 bpm.
The popularity of this measure stems largely from its versatility and
relative ease of use in research applications. The PAR provides detail regarding
the duration, intensity, and volume (energy expenditure) of PA and can therefore
be used for a variety of applications. Because it utilizes a one-week time frame,
data from the PAR are often considered representative of typical PA patterns
(Blair et al., 1998; Dunn et al., 1997). Results for the PAR (kcal/wk) are
calculated using the following steps. Intensity categories were based on
metabolic equivalents (METs) that are multiples of resting metabolic rate. For
each of the seven previous days, subjects reported time in sleep (1.0 METs), at
moderate (4.0 METs), at hard (6.0 METs), and at very hard (10 METs) activities.
Time in light activities (1.5 METs) was estimated by subtraction. Procedures for
estimating total kilocalories of expenditure per week (kcal/wk) are as follows.
Time (in hours) spent in each activity level, is multiplied by the appropriate MET
value and then all products are summed, to produce total kcal per day per
kilogram of bodyweight. That value (kcal/d/kg), is then multiplied by the subjects’
bodyweight in kg, and then by 7, to yield total kcal of energy expenditure per
week (Sallis, Haskell, Fortmann, Vranizan, Taylor & Solomon, 1986). Data from
29
the MTI (kcal/wk) was used to validate the data obtained from the PAR (kcal/wk).
The expression of PA in the analysis was reported as a result of the PAR
questionnaire.
SE was assessed through the questionnaire utilized in the Stanford
Adolescent Heart Health Program (SAHHP) (Reynolds et al, 1990). The SAHHP
(Appendix D) is a multiple risk factor intervention program that involved over 740
adolescents in northern California. After controlling for baseline levels of PA and
BMI associations were found between physical activity and SE (r = (-0.28) – (-
0.46), p>0.001). Self-efficacy responses were measured on a Likert scale by
using a series of statements that will be rated from 1 (strongly agree) to 6
(strongly disagree). Subjects rated how confident they felt about their ability to
exercise regularly despite a series of obstacles. Self-efficacy scores are
expressed as an aggregate score ranging from a possible minimum of eight to a
possible maximum of forty-eight (8-48). Cronbach’s alpha generated for the SE
scale in this study was 0.89 (Reynolds, et al).
Subject’s perceived barriers to PA were assessed with a subset of
Campbell’s Study of Well Being (Stephens & Craig, 1990) (Appendix E). These
items, also scored on a Likert scale, asked the subject to rate the importance of
14 factors in preventing them from participating in regular PA. The possible range
of aggregate scores from the Campbell questionnaire is fourteen to seventy (14-
70). These measures of barriers to PA in adolescents have been previously
utilized effectively (Allison, Dwyer, & Makin, 1999).
Body Mass Index was determined by measurements and formulas set
30
forth by the by the Halls.md BMI calculator (Rosenthal, Bain, Bush, & Warner,
1994).
For descriptive purposes, subjects were asked if they are currently
participating in school-sponsored sports, and if they are currently enrolled in the
school lunch program. Both questions were located on the health history form
(Appendix A).
Procedures
This study received the approval of the University of Mississippi
Institutional Review Board for the protection of human subjects (Protocol number:
04-081). An application for research with human subjects along with a
child/classroom IRB checklist and guide was submitted and was approved
(Appendix F). Permission was obtained from the Tunica County School Board,
the principal of Rosa Fort High School, and the director of the North Mississippi
Delta Boys and Girls Club.
The initial session with the subjects began with a program description and
orientation. Subjects were given informational handouts on the study, the MTI
accelerometer, and an IRB-approved informed parental consent to participate in
the study (Appendix G). Consent forms included contact e-mail address and
phone numbers for parents/guardians with questions or comments about the
study.
The second session began with collection of completed parental consent
31

forms. Subject assent was then obtained based upon the University of
Mississippi’s child/classroom IRB checklist and guide. Subjects 12-13 years of
age gave oral assent with the responses recorded by the technician (Appendix
H). Subjects age 14-17 years gave assent using the written assent form
(Appendix I). Subjects were then given a detailed description and demonstration
of the study procedures and instrumentation. Subjects then completed medical
history and demographic data form (Appendix I).
The subjects’ BMI was then measured. Subjects were weighed, with
weight recorded to the nearest 0.10 lb. and converted to kilograms. Height was
recorded in inches to the nearest 0.10-inch and converted to centimeters.
Subjects were provided with written and oral instructions on the use and care of
the MTI. At this time, the MTI was attached to the right hip with an elastic belt.
The MTI was initialized according to manufacturer specifications and activated.
Subjects then received individual oral instruction relating to the proper
procedures for wearing the MTI. Written information was also provided for the
subject and their parent/guardian relating to the use and care of the MTI. The
subject was then instructed to wear the MTI during waking hours except during
water activities or during bathing. Subjects were given a log book (Appendix J) in
order to record the times when the MTI is removed and attached each day, which
allowed for the calculation of sleep and active hours. Subjects were instructed to
wear the MTI for seven consecutive days and were encouraged to contact the
investigator with any questions regarding the MTI. Subjects were also given an
adherence flyer (Appendix K) to post at home in a conspicuous place for the
32

seven days of monitoring. Upon completion of the MTI procedures, the subjects
completed all paper and pencil questionnaires. Each subject was given the PAR,
the modified Campbell’s questionnaire and the SAHHP questionnaire. Subjects
were given oral and written instructions concerning the proper completion of the
questionnaires, and encouraged to ask questions. Subjects then completed the
self-administered questionnaires at that time.
On the morning of the fourth day of their participation in the study, each
subject received a personal telephone communication from the investigator or a
technician as a reminder to wear the MTI accelerometer. On the fifth day of their
participation in the study, the investigator met with the subjects during their
school day, and presented each with a water bottle (donated by the Tunica
County Recreation Commission) as an incentive to continue with the study
protocol.
The third assessment session consisted of MTI collection and analyses.
Subjects were then given the opportunity to receive feedback concerning their
PA and questionnaire data. Any subject that requested feedback was instructed
to make an appointment with the investigator at their convenience within 30 days
of the completion of their participation in the study. When analysis of the MTI
data was complete and showed full adherence to the study protocol by the
participant, the investigator provided the subjects with t-shirts.
Upon completion of the overall data analysis, an aggregate report was
mailed to Rosa Fort High School and to The North Mississippi Delta Boys and
Girls Club with detailed explanations of the results.
33

Data Analysis
SPSS 11.0 statistical package was used to analyze all data. All data are
reported using means and standard errors. Initial analysis included correlation of
the PAR and MTI data. The results of the PAR were validated against the results
of the MTI. If the instruments did not correlate significantly, regression equations
were run using both instruments and results of both were to be reported.
Correlation of the MTI and PAR data expressed in kcals and METs was also
conducted in order to determine any artificial relationship between kcals
measured by the MTI, which contained a component of BMI measurement, and
the independent variable, BMI.
Correlation matrices for each group were conducted to identify any
significant relationships between the independent variables (perceived SE
(SAHHP), barriers to PA, age and BMI) and the dependent variable, PA level.
Backward stepwise multiple regression was then performed to determine the
factors that predict both male and female African-American adolescents’ PA
levels. The dependent variable physical activity, expressed as kcals per week
from PAR, for each sex was regressed on any significantly correlated
independent variables of perceived SE, perceived barriers to PA, age, and BMI.
To test whether the regression equation for males and the regression equation
for females are the similar, the Chow test (Chow, 1960; Chinaburapa, Larson,
Bootman, McGhan & Nicholson, 1987; Kohli, 1989) was performed with the two
equations.
34
CHAPTER 4
RESULTS
The purpose of this study was to identify the determinants of PA of
African-American schoolchildren ages 12-18 in Tunica County, Mississippi. A
secondary purpose of this study was to determine the relationships among and
identify differences between determinants of PA (age, body mass index, SE, and
perceived barriers to PA) of the students. Results are presented in the following
sequence. Female subjects’ descriptive data and frequencies precede male
subjects’ descriptive and frequency data. Comparison of female and male data
for each variable follows the descriptive data. Correlation data, for all subjects,
between subjective and objective measures of PA are presented next, followed
35
by correlations between PA measures expressed as kcal/wk and as METs.
These data are followed by correlations of all subjects’ barriers to PA to PAR by
grade level. Next ANOVA results for female subjects’ PAR compared with grade
level. These data are followed by correlations for female subjects’ comparing
PAR to the four independent variables. Then regression results for significant
predictors of females’ PA level are presented. Next, male subjects’ correlation
results, comparing PAR to the independent variables are presented, followed by
the regression results for significant predictors of males’ PA level. Finally, results
of the Chow test and hypotheses results are provided.
Subjects
One hundred and fifty-nine adolescents returned parental consent forms
to participate in this study. Of these, 141 adolescents began the study protocol,
with 84 completing the protocol requirements (43 females, 41 males). All 141
students that began the study protocol completed the PAR, SAHHP, barriers to
PA, demographic, and medical history forms. Fifty-seven students that began the
study did not complete the study protocol due to incomplete MTI data. Over 50%
of the 57 students completed less than three days of the 7-day MTI protocol.
Mean age of female subjects (n = 43) was 16.2 + 0.21 years, with a range
of ages 14-19. Mean BMI for females was 25.1 + 0.97 kg/m2. Females had a
mean aggregate SAAHP score of 31.7 + 1.32. Barrier scores for females showed
a mean aggregate score of 47.3 + 1.47. Mean calories expended per week (PAR
36
kcal/wk) as measured by PAR questionnaire in females was 6,303.4 + 351.2
kcal/wk. Analysis of MTI data show mean calories expended in females as
2,818.5 + 182.7 kcal/wk. Demographic data for females for age, BMI, SAHHP,
barriers to PA, PAR, and MTI are displayed in Table 1. Raw data are in Appendix
M. Of 43 female subjects, 35 were enrolled in the free lunch program. Only eight
females were currently participating in school-sponsored athletic programs, while
35 were not. Twenty-three females described their current activity level
measured with the SAHHP questionnaire as about the same as the previous
three months. Only 11 females described their activity level as less, and nine
described their activity level as more than usual. Frequency data for females
(free lunch data, current sport participation data, and previous PA level data) are
shown in Table 2.
Table 1
Females’ Descriptive Data for Age, BMI, SAHHP, Barriers, PAR, and MTI.
Mean SE Min Max
Age 16.2 0.21 14 19
BMI (kg/m2) 25.1 0.97 18.2 54.8
SAHHP 31.7 1.32 8 48
Barriers to PA 47.3 1.47 28 66
PAR (kcal/wk) 6,303.4 351.2 3,548.5 14,046.8
MTI (kcal/wk) 2,818.5 182.7 1,127.7 6,352.3
n = 43
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
37
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
energy expenditure, MTI = Accelerometer energy expenditure
Table 2
Females’ Frequency Data for Free Lunch, Current Sport Participation, and Usual
Activity Level
Free Lunch Frequency Percent of Total
Yes 35 81.4
No 8 18.6
Current Sport Participation Frequency Percent of Total
Yes 8 18.6
No 35 81.4
Usual Activity Level Frequency Percent of Total
More 9 20.9
Less 11 25.6
About the same 23 53.5
38
n = 43
Mean age of male subjects (n = 41) was 15.4 + 0.24 years, with a range of
12-18. Mean BMI for males was 24.9 + 0.93 kg/m2. Males had a mean aggregate
SAAHP score of 32.9 + 1.31. Barriers to PA scores for males showed a mean of
39.8 + 2.17. Mean calories expended per week as measured by PAR
questionnaire for males was 6,894.7 + 328.2 kcal/wk. Analysis of MTI data show
mean calories expended for males as 4,593.8 + 410.8 kcal/wk. Demographic
data for males for age, BMI, SAHHP, barriers to PA, PAR, and MTI are shown in
Table 3.
Table 3
Males’ Descriptive Data for Age, BMI, SAHHP, Barriers to PA, PAR, and MTI
Mean SE Min Max
Age 15.4 0.25 12 18
BMI (kg/m2) 24.9 0.93 16.6 46.4
39
SAHHP 32.9 1.31 8 48
Barriers to PA 38.8 2.17 15 70
PAR (kcal/wk) 6,894.7 328.2 3,645.8 12,942.6
MTI (kcal/wk) 4,593.8 410.8 1,148.4 14,002.9
n = 41
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
energy expenditure, MTI = Accelerometer energy expenditure
Of 41 males, 29 were enrolled in the free lunch program. Seventeen
males were currently participating in school-sponsored athletic programs, while
24 were not. Twenty-five males described their current activity level, measured
with the SAHHP questionnaire, as about the same as the previous three months.
Only six males described their current activity level as less, and ten described
their activity level as more than usual. Frequency data (free lunch data, current
sport participation data, and previous activity level data) for males are shown in
Table 4.
Table 4
Males’ Frequency Data for Free Lunch, Current Sport Participation, and Usual
Activity Level
Free Lunch Frequency Percent of Total
Yes 29 70.7
40
No 12 29.3
Current Sport Participation Frequency Percent of Total
Yes 17 41.5
No 24 58.5
Usual Activity Level Frequency Percent of Total
More 10 24.4
Less 6 14.6
About the same 25 61
n = 41
Mean scores for the dependent variable (PAR), and each independent
variable (SAHHP, barriers to PA, age, BMI) from each group of subjects were
compared using independent samples t-tests. Significant differences were found
between mean scores of age and barriers to PA. Females mean age was
significantly higher than mean age for male subjects [16.2 + 0.21, 15.4 + 0.24 (t =
-2.56, p<0.05)]. Mean barrier score for females was also significantly higher than
males’ mean barrier score [47.3 + 1.47, 39.8 + 2.17 (t = -2.870, p<0.05)]. Mean
kcal/wk from MTI assessment for females was significantly lower than males’ MTI
results [2,818.5 + 182.7, 4,593.8 + 410.8 (t = 4.01, p<0.05)]. Independent
samples t-test for SAHHP, BMI and PAR showed no significant differences
between the groups. Females’ mean SAHHP score was 31.7 + 1.32, while males’
mean SAHHP score was 32.9 + 1.31 (t = 0.647, p = 0.519). For females, BMI
was 25.1 + 0.97, while BMI for male subjects was 24.9 + 0.93 (t = -0.104 p =
41
0.92). Finally, mean PAR score for female subjects was 6,303.4 + 351.2 kcal/wk
and mean PAR score for males was 6,894.7 + 328.2 kcal/wk (t = 1.227, p =
0.223). Independent samples data is shown in Table 5.
Correlations of Dependent and Independent Variables
Correlations for females and males are found in Tables 6 and 7. For
females, a significant correlation was found between age and BMI (r = 0.372,
p<0.05). Other correlations among the independent variables, age, BMI, SAHHP,
and barriers to PA were nonsignificant. For males, there were no significant
correlations between the independent variables.
Table 5
t-test Data for Age, BM, SAHHP, Barriers to PA, and PAR – Females and Males
Mean SE
t pFemale Male Female Male
Age 16.2 15.4 0.21 0.24 -2.56 0.012*
BMI 25.1 24.9 0.97 0.93 -0.104 0.920
SAHHP 31.7 32.9 1.32 1.31 0.647 0.519
Barriers to PA 47.3 39.8 1.47 2.17 -2.870 0.005*
PAR 6,303.4 6,894.7 351.2 328.2 1.227 0.223
MTI 2,818.5 4,593.8 182.7 410.8 4.012 0.000*
Females n = 43, Males n = 41
*p<0.05
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
42
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
energy expenditure, MTI = Accelerometer energy expenditure
Table 6
Correlation table for Females’ Age, BMI, SAHHP, Barriers to PA, PAR, MTI
Age BMI
(kg/m2)
SAHHP Barriers
to PA
PAR MTI
Age -------
BMI (kg/m2) 0.372 -------
SAHHP -0.056 0.148 -------
Barriers to PA 0.070 0.154 0.179 -------
PAR 0.101 0.508a 0.411a 0.241 -------
MTI 0.151 0.203 0.137 0.064 0.412a -------
n = 43
ap<0.05
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
43

energy expenditure, MTI = Accelerometer energy expenditure
Table 7
Correlation table for Males’ Age, BMI, SAHHP, Barriers to PA, PAR, MTI
Age BMI
(kg/m2)
SAHHP Barriers
to PA
PAR MTI
r r r r r r
Age -------
BMI (kg/m2) 0.289 -------
SAHHP -0.014 0.085 -------
Barriers to PA 0.226 -0.137 0.050 -------
PAR 0.426a 0.543a 0.102 -0.005 -------
MTI 0.387a 0.360 0.096 0.093 0.735a -------
n = 41
ap<0.05
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
44
energy expenditure, MTI = Accelerometer energy expenditure
Comparison of PA Measures
Total weekly physical activity, measured by the PAR (mean = 6,592
kcal/wk) for both groups showed a significant positive correlation when compared
with total weekly physical activity as measured by the MTI accelerometer (mean
= 3,685 kcal/wk) (r = 0.57, p<0.05) for both groups. Correlation of the MTI and
PAR data expressed in kcal/wk and METs showed significant correlations
between MTI data expressed in kcal/wk and in METs (r = 0.67, p<0.05), and
between PAR data expressed in kcal/wk and in METs (r = 0.90, p<0.05).
Correlation data are shown in Tables 8 and 9.
Table 8
Correlation of PA Assessment Measures PAR (kcal/wk) and MTI (kcal/wk) – All
Subjects
Instrument N Mean SE Pearson r
PAR 84 6,592 241.54 0.57a
MTI 84 3,685 240.47
45
ap<0.05
Note: PAR = 7-day Physical Activity Recall energy expenditure; MTI=
Accelerometer energy expenditure
Table 9
Correlation of PA Measures in METS and kcal/wk for PAR and MTI – All Subjects
Instrument N Mean SE Pearson r
PAR (kcal/wk) 84 6,592.04 241.56 0.90a
PAR (METs) 84 10,137.12 382.85
MTI (kcal/wk) 84 3,685.01 240.47 0.67a
MTI (METs) 84 5,582.63 367.66
ap<0.05
Note: PAR = 7-day Physical Activity Recall energy expenditure; MTI =
Accelerometer energy expenditure
46
Barriers and PA Level
Correlation of barriers to PA and PAR for both males and females in each
grade level (9-12) showed no significant correlations. Pearson product moment
correlations ranged from 0.505 (p = 0.385) in 8th grade students to -0.296 (p =
0.266) in 10th grade students. Correlations of barriers to PA by grade level are
shown in Table 10.
Table 10
Correlation of Barriers to PA to PAR (kcal/wk) – All Subjects
Grade N Mean SE Pearson r p
8th PAR 5 6,355.46 532.41 0.505 0.385
Barriers to PA 5 32.4 2.09
9th PAR 35 6,417.98 369.50 0.255 0.139
Barriers to PA 35 43.6 2.31
10th PAR 16 6,861.81 629.11 -0.296 0.266
Barriers to PA 16 42.81 2.96
11th PAR 11 5,700.04 304.13 -0.237 0.482
47
Barriers to PA 11 50.27 2.32
12th PAR 17 7,343.32 643.53 0.124 0.636
Barriers to PA 17 43.35 3.09
N = 84
Note: PAR = 7-day Physical Activity Recall energy expenditure (kcal/wk); Barriers
to PA = barriers scale of Campbell’s Well-Being Questionnaire
Grade Level and PA Level
Oneway ANOVA of females’ PAR by grade level did not show
significant differences between grade levels (9-12) in female subjects (F (2, 39) =
0.740, p = 0.534). The Levene’s statistic for the ANOVA conducted with female
subjects on grade level and PA level, was significant (LS = 3.240, p<0.05).
Results for females’ PAR by grade level are shown in Table 11. Oneway ANOVA
of males’ PAR by grade level demonstrated a significant difference between
grade levels (8-12) in male subjects (F (3, 36) = 3.508, p = 0.025). However, the
Levene’s statistic for the ANOVA conducted with male subjects on grade level
and PA level was also significant (LS = 5.873, p<0.05), Results for males’ PAR
by grade level are shown in Table 12.
Table 11
Oneway ANOVA – Females’ PAR (kcal/wk) and Grade Level
PAR (kcal/wk) df SS MS F p
Between Groups 3 12,001,398.9 4,000,433.3 0.740 0.534
Within Groups 39 222,750,499.8 5,403,823.1
48
N = 43
Note: PAR = 7-day Physical Activity Recall energy expenditure
Table 12
Oneway ANOVA – Males’ PAR (kcal/wk) and Grade Level
PAR (kcal/wk) df SS MS F p
Between Groups 3 39,963,736 13,321,245.3 3.508 0.025
Within Groups 36 136,698,397 3,797,177.7
N = 43
Note: PAR = 7-day Physical Activity Recall energy expenditure
Regression Analyses
Correlation matrices were created for both female and male groups. The
correlation for females showed a significant relationship between PAR and
SAHHP (r = 0.411, p<0.05) and between PAR and BMI (r = 0.508, p<0.05). The
independent variables of age (r = 0.101, p = 0.518) and barriers to PA (r = 0.411,
p = 0.119) were not significantly correlated with the dependent variable, PAR.
The initial regression model for female subjects included BMI and the
dependent variable, PAR. This analysis resulted in a significant model with an R2
of 0.258 [F (1, 41) = 14.23, p<0.05], with BMI accounting for 24% of the variance
in PA for this sample. SAHHP was entered along with BMI for the final model,
49
contributing significantly to the predictive power of the model with an R2 increase
of 0.115 [F (2, 40) = 11.89, P<0.05]. The addition of SAHHP to BMI results in a
model that accounts for 34% of the variance in PA in this sample of female
adolescents. Correlation data for females are shown in Table 13. Summary data
for the regression analysis for females are shown in Table 14.
Table 13
Correlation of Females’ PAR with Age, BMI, SAHHP, and Barriers to PA
PAR (kcal/wk)
Pearson r p
Age 0.101 0.518
BMI (kg/m2) 0.508 0.001
SAHHP 0.411 0.006
Barriers to PA 0.411 0.119
n = 43
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
energy expenditure, MTI = Accelerometer energy expenditure
50

Table 14
Females’ Regression Summary
PAR (kcal/wk)
Variable βa βb R2 F p R2 ∆
Step 1
BMI (kg/m2) 0.508 184.394 0.258 14.23 0.001 ------
Step 2
BMI (kg/m2) 0.457 165.981
SAHHP 0.343 91.537 0.373 11.89 0.001 0.115
n = 43
aStandardized Beta Coefficient
bUnstandardized Beta Coefficient
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
energy expenditure
51

The correlations for males showed a significant relationship between PAR
and BMI (r = 0.543, p<0.05), and between PAR and age (r = 0.426, p<0.05).
Independent variables SAHHP (r = 0.102, p = 0.527) and barriers to PA (r = -
0.005, p = 0.977) were not correlated with PAR. The initial regression model for
male subjects included BMI and the dependent variable, PAR. This analysis
resulted in a significant model with an R2 = 0.295 [F (1, 39) = 16.307, p<0.05],
with BMI accounting for 28% of the variance in PA for this sample. Age was then
entered along with BMI for the final model, contributing significantly to the
predictive power of the model with an R2 change = 0.079 [F (2, 38) = 11.349,
p<0.05]. The addition of SAHHP to BMI results in a model that accounts for 34%
of the variance in PA in this sample of male adolescents. Correlation data for
males are shown in Table 15. Summary data for the regression analysis for
males are shown in Table 16.
Comparison of Regression Equations
The Chow test (Chow, 1960) was used to compare the regression
equation for males with the regression equation for females. In order to perform
the Chow test, three regression equations must be performed, the first for all
subjects, and one for each group of subjects (males and females). Each
regression equation includes each independent variable. The F value is then
52
calculated using the Chow test. Formula for the Chow test is shown in Table 17.
The comparison of both male and female groups’ equations with the Chow Test,
results in a non-significant regression model (F (5, 74) = 1.849, Fcv = 2.37).
Results of each regression analysis are shown in Table 18 and results of the
Chow test are shown in Table 19.
Table 15
Correlation of Males’ PAR with Age, BMI, SAHHP, and Barriers to PA
PAR (kcal/wk)
Pearson r p
Age 0.426 0.005
BMI (kg/m2) 0.543 0.000
SAHHP 0.102 0.527
Barriers to PA -0.005 0.977
n = 41
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
energy expenditure
53
Table 16
Males’ Regression Summary
PAR (kcal/wk)
Variable βa βb R2 F p R2 ∆
Step 1
BMI 0.543 192.555 0.295 16.307 0.000 ------
Step 2
BMI (kg/m2) 0.458 162.442
Age 0.294 394.557 0.374 11.349 0.000 0.097
n = 41
aStandardized Beta Coefficient
bUnstandardized Beta Coefficient
Note - PAR = 7-day Physical Activity Recall energy expenditure, BMI = Body
Mass Index
54

Table 17
Formula - Chow Test
F = [SSe (Both Groups) a – SSe (Males) b – SSe (Females) c ] / p [SSe (Males)b + SSe (Females)c] / (n + m – 2p)
p = parameters (IV + 1)
n = female n
m = male n
aFrom standard regression analysis , both groups
bFrom standard regression analysis, males
cFrom standard regression analysis, females
55
Table 18
Chow Test of All Standard Regression Results
Predictors - All subjects N = 84 βa βb t p
SAHHP 0.222 58.00 2.36 0.021
Barriers to PA 0.025 4.48 0.262 0.794
Age 0.069 101.46 0.681 0.498
BMI (kg/m2) 0.469 170.08 4.718 0.000
Predictors - Female Subjects n = 43 βa βb t p
SAHHP 0.317 84.63 2.425 0.020
Barriers to PA 0.117 27.94 0.901 0.373
Age -0.063 -
106.54
-0.457 0.650
BMI (kg/m2) 0.466 169.34 3.335 0.002
Predictors Male Subjects n = 41 βa βb t p
SAHHP 0.069 17.18 0.518 0.608
Barriers to PA -0.014 -2.183 -0.104 0.917
Age 0.301 404.09 2.101 0.043
BMI (kg/m2) 0.448 158.94 3.170 0.003
aStandardized Beta Coefficients
bUnstandardized Beta Coefficients56

Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire, PAR = 7-day Physical Activity Recall
energy expenditure, MTI = Accelerometer energy expenditure
Table 19
Chow Test Results for Comparison of Males’ and Females’ Regression
Equations
Group R2 Standardized Beta Coefficients Chow Test Fcv
Age BMI SAHHP Barriers
to PA
Males 0.38 0.30a 0.45a 0.07 -0.01
Females 0.39 -0.06 0.47a 0.32a 0.12 1.849 2.37
Males n = 41
Females n = 43
ap<0.05
Note - BMI = Body Mass Index, SAHHP = self-efficacy scale of the Stanford
Adolescent Heart Health Program questionnaire, Barriers to PA = barriers scale
of Campbell’s Well-Being Questionnaire
57
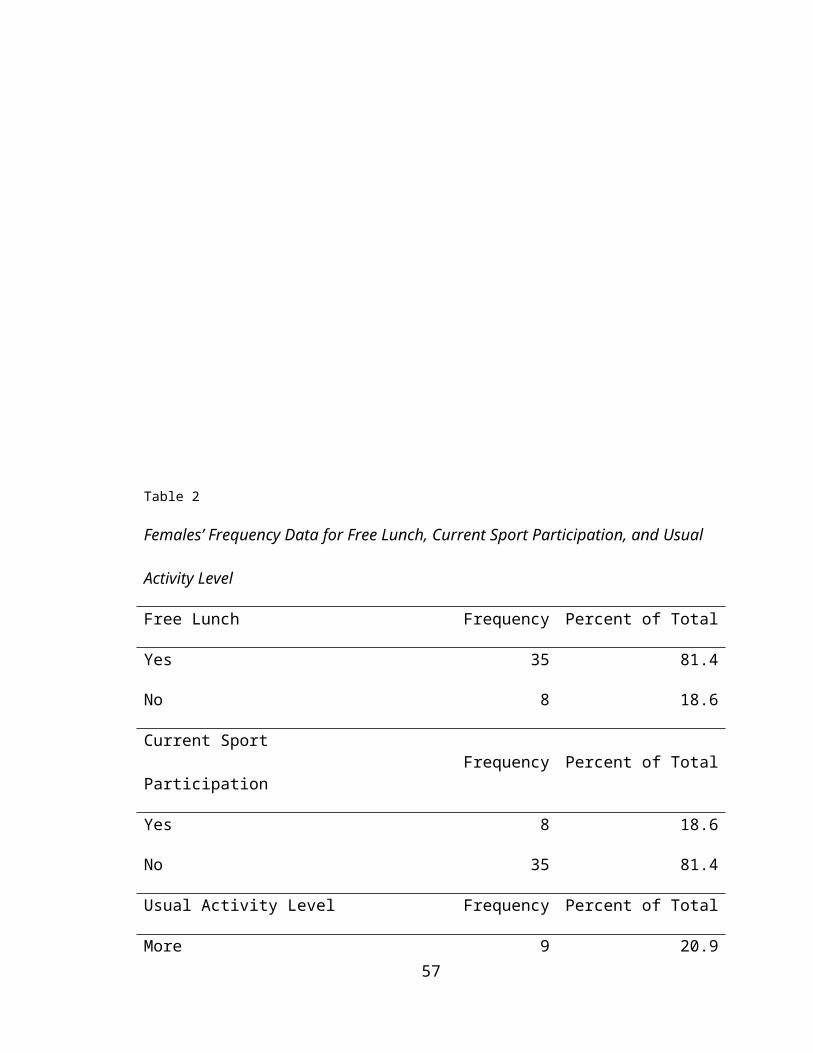
Outlier Scores
Using the SPSS default formula with box plot analysis, all univariate
outliers from the dependent variable and from each independent variable for both
males and females were removed from the data set. The identification of outliers
was assessed for each variable until no outliers existed in the box plot analyses.
For male subjects, 21 scores were removed. Fifteen male subjects achieved
these 21 outlier scores. For female subjects, 8 outlier scores were identified and
removed. Seven female subjects achieved these 8 scores.
After removal of outliers, the mean of each variable for each group was
compared with the original data. The t-test results for each variable were
nonsignificant, except for the difference in males PAR. The only variable that was
significant after removal of outlier scores was PAR in male subjects. However,
when outlier scores were removed after the first iteration, the difference in the
means was not yet significant for this variable.
Due to the nonsignificance of 9 of 10 variables after removal of outlier scores
from the data set, it was recommended that outlier data be included in the data
analyses.
Hypothesis Testing
58

To address the purpose of the study the following null hypotheses were
tested with stepwise multiple regression analysis.
Ho1: There is no significant relationship between level of PA and perceived
SE, perceived barriers to PA, age, and BMI for males.
Ho2: There is no significant relationship between level of PA and perceived
SE, perceived barriers to PA, age, and BMI for females.
This study also considered the following alternative hypothesis.
Ha1: Males’ level of PA will be influenced by their level of perceived SE,
followed by the perceived to PA, followed by age, and BMI.
Ha2: Females’ level of PA will be influenced by their level of perceived SE,
followed by the perceived barriers to PA, followed by age, and BMI.
Based upon the data for rural African-American adolescent males, we fail to
reject null hypothesis one (Ho1), based upon the lack of significance in the
correlations for the independent variables barriers to PA and SE to the
dependent variable, PAR. Even though we failed to reject Ho1, the independent
variables age and BMI were significantly correlated with the dependent variable
PAR.
Based upon the data for rural African-American adolescent females, we also
fail to reject null hypothesis two (Ho2) based upon the lack of significance
demonstrated in the correlations for the independent variables barriers to PA and
age to the dependent variable, PAR. Even though we failed to reject Ho1, the
independent variables age and BMI were significantly correlated with the
dependent variable PAR.
59
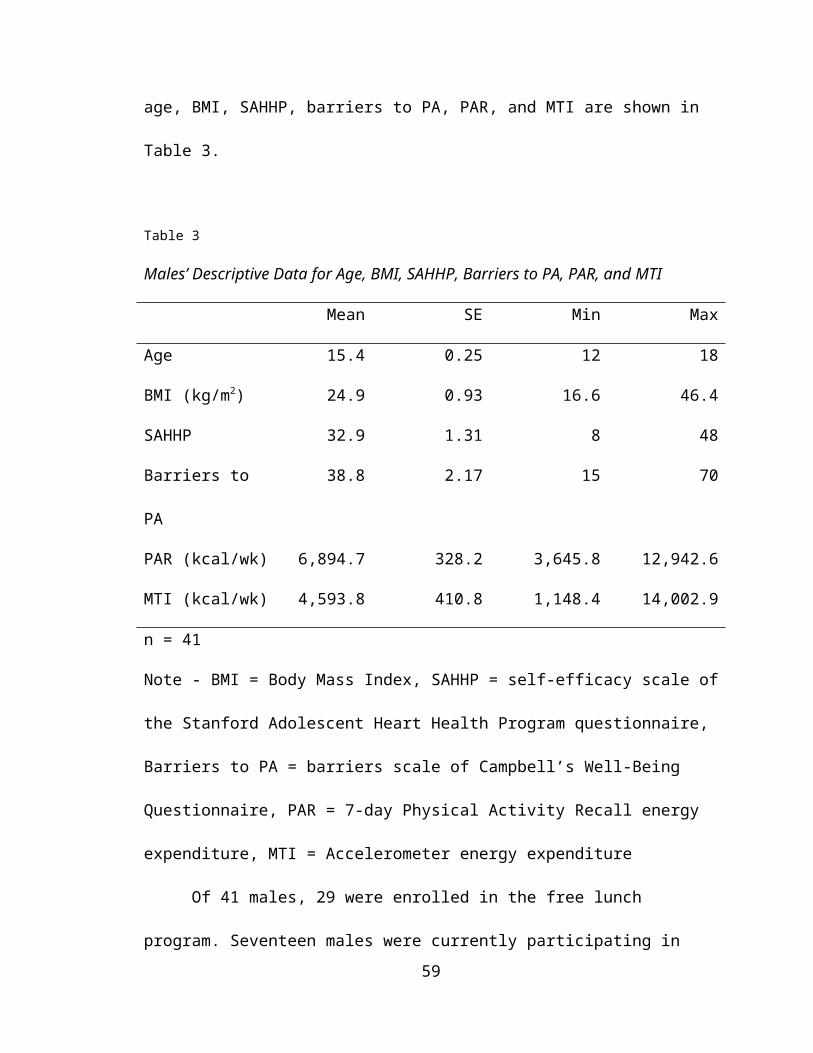
Furthermore, based upon the results of regression analysis for male
subjects, we reject alternative hypothesis one (Ha1). We also reject alternative
hypothesis two (Ha2) based upon the results of regression analysis of female
subjects in this sample.
CHAPTER 5
DISCUSSION
The purpose of this study was to identify the determinants of PA of
African-American schoolchildren ages 12-18 in Tunica County, Mississippi. A
secondary purpose of this study was to determine the relationships among and
identify differences between recognized determinants of PA (age, body mass
index, perceived SE, and perceived barriers to PA) of the students.
Descriptives
For descriptive purposes, subjects were asked to indicate if they were
enrolled in the school lunch program or if they were currently a member of a
school-sponsored athletic team. Forty-three female subjects completed the study
protocol. Of these, 81.4% were enrolled in the school lunch program. This
percentage is similar for the forty-one males that completed the study. Of the
forty-one males, 65% were enrolled in the school lunch program. Only 11.6% of
the female subjects were currently a member of a school-sponsored athletic
program. The number of males currently participating in school-sponsored sports
60
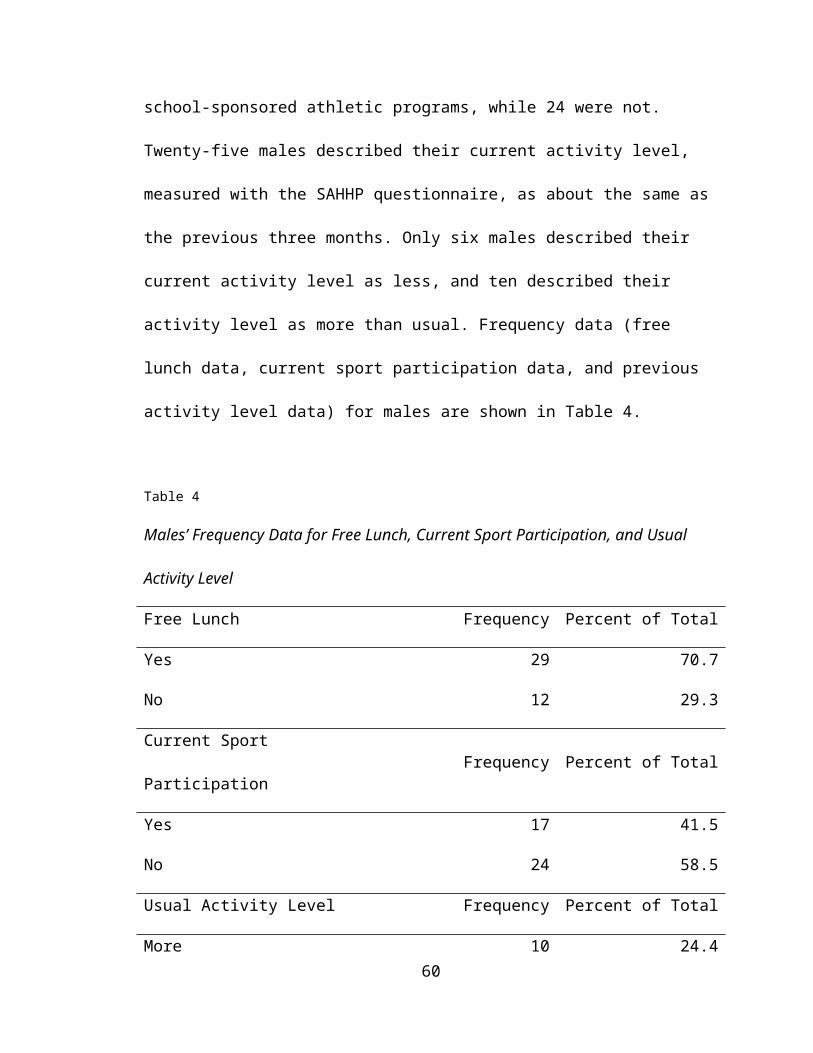
was higher. Twenty percent of males were also participating in sports during the
time of the study protocol. As part of the PAR, each subject was asked if their PA
level was more, less, or about the same as their typical PA level over the past
three months. Over half (51.2%) of female subjects and 60% of male subjects
described their recent activity levels as about the same as the previous three
months. Over twenty-five percent of females and 14.6% of males rated their
previous week’s PA level as less than the previous three months. Over twenty-
four percent of males and 20.9% of females described their previous week’s PA
as more than usual when compared to their previous three months PA levels.
The mean kcal/wk for female subjects (2,818 kcal/wk) measured by the
MTI accelerometer is less than half of that estimated by the PAR (6,303 kcal/wk).
This difference in male subjects is over 33% (MTI = 4,593 kcal/wk, PAR = 6,894
kcal/wk). By comparison, assessment of PA methodology in the five-city project
(N = 1,120, ages 20 – 74), showed an average PAR kcal/wk of over 18,000
kcal/wk in both male and female adults (Sallis, et al, 1985). In young adults (18-
25), assessment of PA by PAR shows a weekly energy expenditure of 11,825
kcal/wk (Washburn, Jacobson, Sonko, Hill, & Donnely, 2003). In a sample of
middle school students, total energy expenditure assessed by accelerometry was
1,941 kcal/wk (McMurray, Harrell, Bradley, Webb & Goodman, 1998). When
compared to adults (11,852 kcal/wk), the PA level of this sample of adolescents
(6,592 kcal/wk), assessed by PAR, was significantly lower (t = -21.77, p<0.05).
However, the PA level measured by MTI in this sample of African-American
adolescents (2,264 kcal/wk) was significantly higher than the sample of middle
61
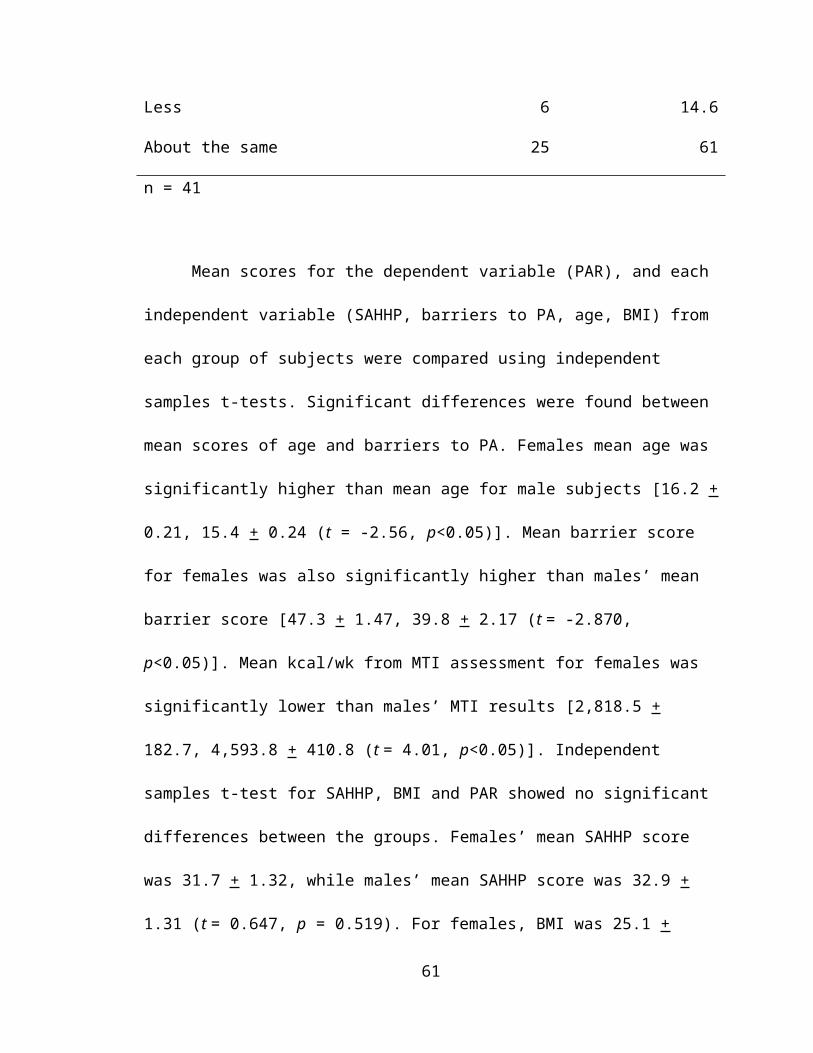
school students (1,941: t = 2.64 p<0.05)(McMurray, Harrell, Bradley, Webb &
Goodman).
Validation of PA Measure
Physical activity measurement using accelerometry and physical activity
recall has been established as a reliable and valid means of activity assessment
in the adolescent population. Several studies show significant correlations
between accelerometry and exercise heart rate, activity energy expenditure, and
treadmill exercise (Coleman, Saelens, Wiedrich-Smith, Finn, & Epstein, 1997;
Matthews & Freedson, 1995; Yngve et al, 2003; Freedson, Melanson, & Sirand,
1998; Ekelund, 2001). The PAR has been validated against objective fitness
measures such as VO2, direct observation, activity energy expenditure and
accelerometers (Blair et al., 1985; Jacobs, Ainsworth, Hartman, & Leon, 1993;
Wallace, McKenzie & Nader, 1985; Rauh, Hovell, Sallis & Hofstetter, 1992;
Matthews & Freedson, 1995; Washburn 2003; Sallis, Buono, Roby, Micale, &
Nelson, 1993).
In order to validate the use of the subjective measure of PA (PAR) as our
dependent variable in this sample, the results of all subjects’ energy expended
(kcal/wk) as estimated by the PAR, were correlated with the objective measure of
physical activity (MTI [kcal/wk]). The results of the correlation showed that the
PAR and MTI results were significantly related (r = 0.57, p<0.05). This significant
relationship allowed for regression equations of physical activity to be analyzed
using kcal/wk estimated from the PAR instrument as the dependent variable.
62

Correlations found in the literature from adult samples between the PAR and
accelerometer instruments (N = 33) show Pearson product moment correlations
ranging from 0.41(Hayden-Wade, Coleman, Sallis, & Armstrong, 2003) to 0.79
(Miller, Freedson & Kline, 1994) Furthermore, in a sample of middle school
students, authors found a correlation of 0.51 between PAR and accelerometry
(McMurray, et al. 1998).
In order to control for any artificial effect of BMI, which is not only an
independent variable, but also contains a component in estimation of kcal/wk in
the dependent variable (PAR), correlations were calculated between the MTI and
PAR data expressed in kcal/wk and expressed in METs. Significant positive
correlations were found between both measurements (kcal, METs) of PA using
the PAR (r = 0.90, p<0.05) and both measurements (kcal, METs) of PA using the
MTI (r = 0.67, p<0.05). The significant correlations between each PA instrument
expressed in both kcal/wk and METs show a significant relationship between the
instruments after the removal of body weight, which is a factor in the calculation
of BMI and kcal/wk, from the measurement of PA by PAR.
Effect of Barriers to PA on PA Level
The effect of barriers to PA in adolescents were recently reported by
Allison, Dwyer, and Makin (1999b). The authors found that the perceived barriers
to PA were not constant across all grade levels. Allison, Dwyer and Makin found
that perceived barriers to PA were predictive in subjects in grade 9 only. In this
63
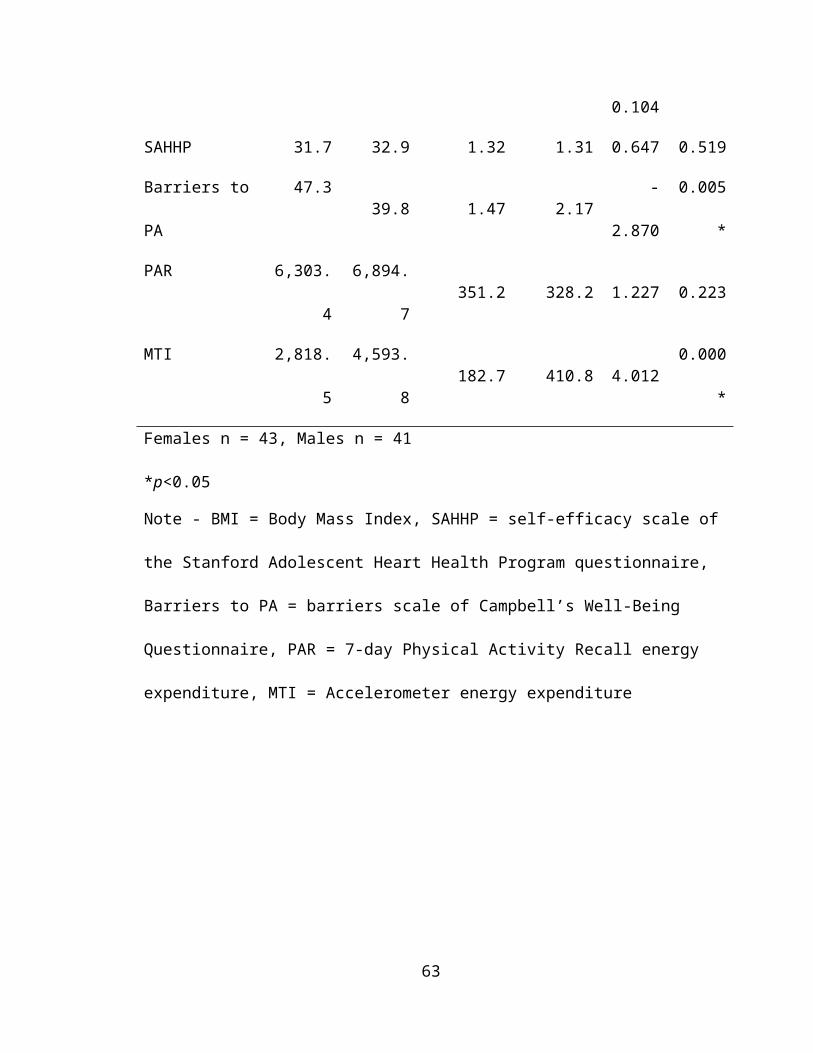
sample of male and female adolescents, no significant correlations were found
between barriers to PA and level of PA, regardless of grade (r = 0.255 – (-
0.139), p = 0.255 – 0.636). A number of possible reasons for the nonsignificant
interaction of barriers to PA and PA in this sample of adolescents are discussed
in both the determinants of PA in females’ and in the determinants of males’ PA
sections.
Effect of Grade Level on PA Level
Data from Aaron (1993) show that PA levels of females significantly
decreased from ages 12-15+. Prior to Aaron (1993), it was demonstrated that PA
level decreases with age in children 6-18 (Saris, Elvers, Van’t Hof & Binkhorst,
1986). Physical activity is demonstrated to decrease across age, whether PA
was measured as vigorous PA or as daily moderate PA (Allison, Dwyer, & Makin,
May, 1999; Trost, et al, 2002).
In this sample of female adolescents, no differences were found between
the different grade levels as they relate to daily PA (F = 0.740, p = 0.534).
Female students in grade nine, as measured by PAR, expended 6,863.9
kcal/wk. Tenth grade females expended less kcal/wk (5,872.5) followed by 11 th
grade girls (5,577.2). The pattern is then reversed with 12th grade girls burning
6,533.7 kcal/wk. The Levene’s statistic for the ANOVA conducted with female
subjects on grade level and PA level was significant (Levene’s Statistic = 3.240,
p<0.05), meaning that the variances of all the grade levels on the dependent
64
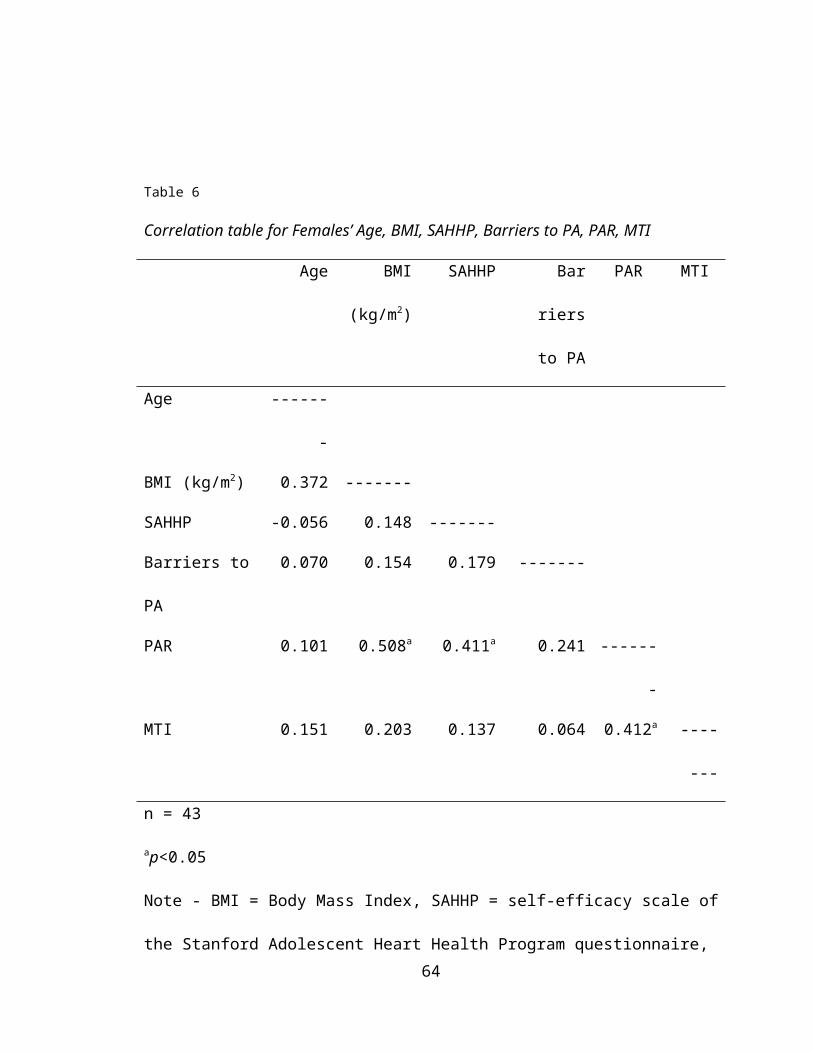
variable are significantly different. Therefore, since we have violated the second
assumption of ANOVA, no interpretations can be made about the ANOVA
results. Furthermore, the sample of females in the study by Aaron was primarily
Caucasian females from a metropolitan area, whereas the current sample was
exclusively African-American females from a rural setting.
In this sample of male adolescents, differences were found in PA levels
across each grade level (F = 3.508, p = 0.25). However, the Levene’s statistic for
the ANOVA conducted with male subjects on grade level and PA level was also
significant (Levene’s Statistic = 5.873, p<0.05), indicating that the variances of all
the grade levels on the dependent variable are significantly different. Therefore,
any further analysis of males’ PA level and grade is unwarranted. As is the case
with females, the data available from previous research on age and PA level in
adolescents were gathered using Caucasian subjects (Saris, Elvers, Van’t Hof &
Binkhorst, 1986; Allison, Dwyer, & Makin, May, 1999; Trost, et al, 2002) in a
urban setting.
Determinants of PA in Females
It was hypothesized that both males’ and females’ levels of PA would be
influenced by their level of perceived SE, followed by their perceived barriers to
PA, followed by age, and BMI. However, data analysis for females shows that
BMI and SAHHP are the only significant predictors of PA in this sample (F (2, 40)
= 11.896, p = 0.05). The amount of variance in PA explained by BMI for this
sample of female adolescents is 26%. The addition of SAHHP to the regression
65
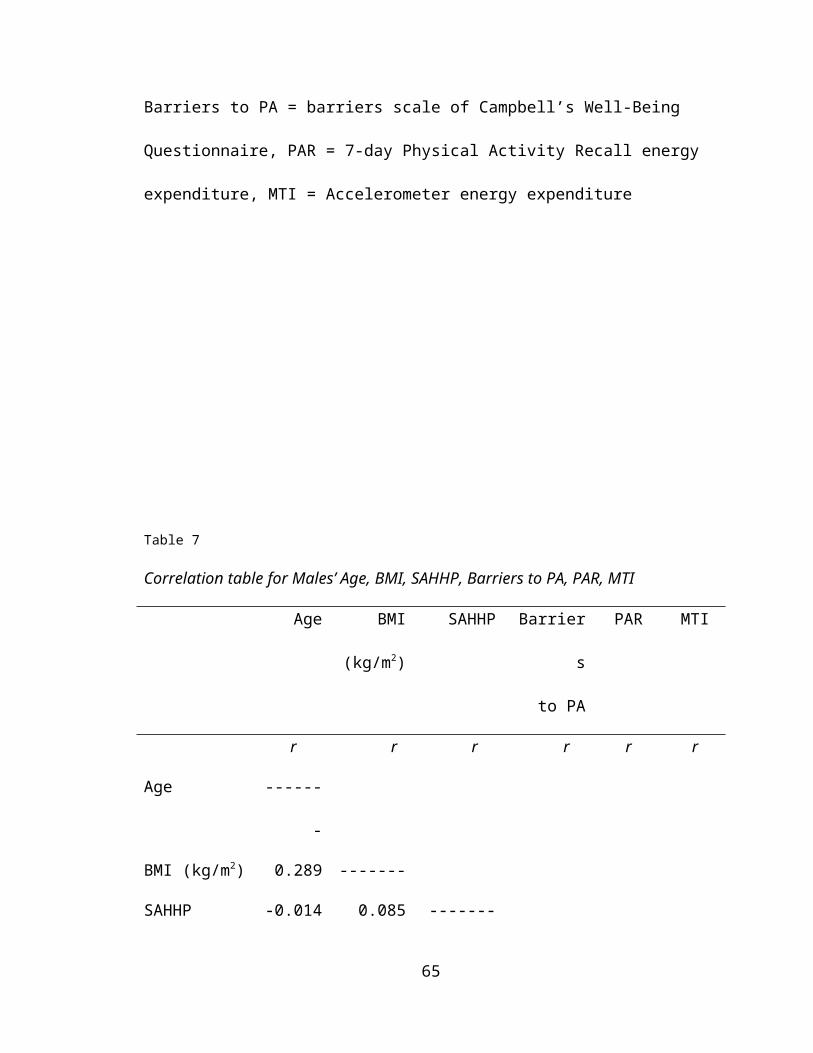
model results in an R2 change of 0.115, increasing the amount of variance in PA
explained by BMI and SAHHP to 34%. Independent variables that were
hypothesized to influence female subjects’ levels of PA that did not show
significance were barriers to PA (r = 0.411, p = 0.119), and age (r = 0.101, p =
0.518).
Barriers to PA are significant in a high school population (Allison, Dwyer,
and Makin, 1999b). However, these results have not been consistent across all
grade levels. It was demonstrated that perceived barriers to PA were only
predictive of PA in subjects in grade 9. In this sample of female adolescents,
barriers to PA are not significantly related to PA level (r = 0.241, p = 0.119).
Also, analysis showed that the Pearson product moment correlation coefficient
for barriers to PA, while not significant, were positively correlated (r = 0.241) with
the dependent variable, PAR. It would be expected, that as levels of PA
increased, barriers to PA would decrease, thus resulting in a negative
relationship, which is not the case with this sample of adolescent females. In
recent literature, barriers to PA are inversely correlated, not only with PA, but
with SE and age as well. In this sample of female adolescents, however, barriers
to PA are not correlated with either SE (r = 0.179, p = 0.250) or age (r = 0.070, p
= 0.657). Specific barriers and their relationship to sex and PA were not
examined as part of this study. Analysis of these data in future projects may be
helpful in identifying particular barriers to PA that affect a similar sample of
adolescent females.
Previous studies with adolescents that have addressed barriers to PA
66
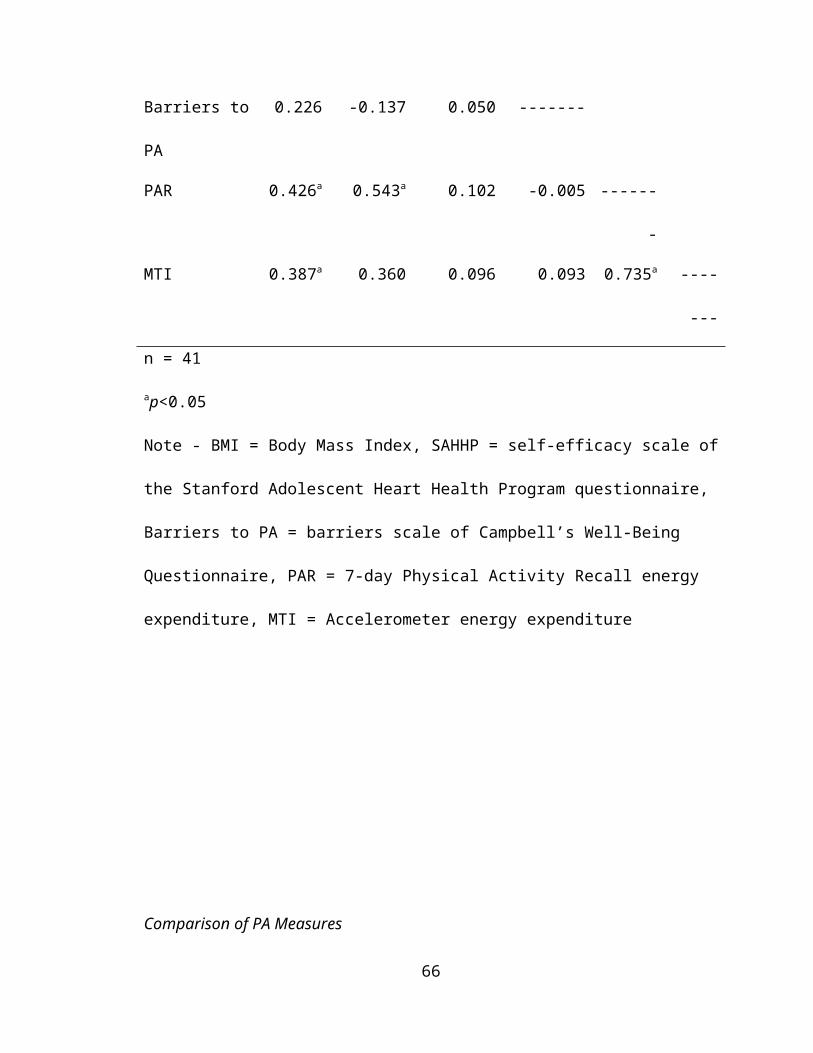
have been conducted in an urban population. This research with rural African-
American adolescents may represent a unique situation where barriers to PA
most common in urban adolescents, do not affect the PA levels of adolescents in
a rural setting. Also, according to a review of the literature, this is the first study
examining determinants of PA in an exclusively African-American adolescent
population. Other studies conducted with minority adolescents, have utilized
Hispanic and African-American subjects. Those studies, much like studies
conducted with urban adolescents, may not have assessed barriers to PA that
would be applicable in this sample of adolescents. Various barriers that have
been identified in studies with rural adults, African-American adults, and with
other minority females that were not assessed with this instrument that could
affect the females’ level of PA include appearance, self-image, condition of
sidewalks and quality of street lighting, and weather (Richter, Wilcox, Graney,
Henderson, & Ainsworth, 2002; Eyler, et al., 2002; Sanderson, Littleton, & Pulley,
2002). Also, barriers to PA exclusive to physical education classes (opportunities
to participate, lack of dressing/showering facilities, and lack of equipment) show
significance in other samples of minority female adolescents (Taylor, et al., 1999)
It is demonstrated that PA level significantly decreases with age in
children 6-18 (Saris, Elvers, Van’t Hof & Binkhorst, 1986 & Verschuur & Kemper,
1985). The significant impact of age on PA has been noteworthy, whether
measured as vigorous PA (Allison, Dwyer, & Makin, May, 1999; Trost, et al,
2002), or through daily moderate physical activity (Trost, et al). While the range
of ages in this sample of female adolescents is limited, and the standard error is
67

small (14-19, 0.25), age does not correlate significantly with PA (r = 0.241, p =
0.119). Based on previous literature, it would be expected that as age increases,
level of PA would decrease, resulting in a negative Pearson product moment
correlation, which is not the case in this sample of female adolescents.
Interestingly, several subjects at higher ages were also some of the most active
females in the study. Of all female subjects ages 17-19, 30% (6 of 18) had PAR
scores at or above +1 SD above the mean. Also, the two most active female
subjects were in the top half of the age range (12,041.5 and 14,046.8 kcal/wk; 17
and 18 years old, respectively) and neither of the subjects were currently a
member of a school-sponsored athletic team. A possible reason for the increase
in PA level in 12th grade females (PAR = 6,533.7 kcal/wk) from 10th (PAR =
5,872.5 kcal/wk) and 11th grade (PAR = 5,577.2 kcal/wk) females could have
been due to a larger percentage currently participating in school-sponsored
athletic teams. It was found, however that 50% of the eight females that were
currently participating in sports were 15 years old, while two were 17 years old,
and two were 18 and 19 years old.
Determinants of Physical Activity in Males
Data analysis for males show that BMI and age are the only significant
predictors of physical activity in this sample (F (2, 38) = 11.35, p <0.05). The
amount of variance in PA explained by BMI for this sample of male adolescents
is 29.5%. The addition of age to the regression model results in an R2 change of
0.097, increasing the amount of variance in PA explained by BMI and age to
68
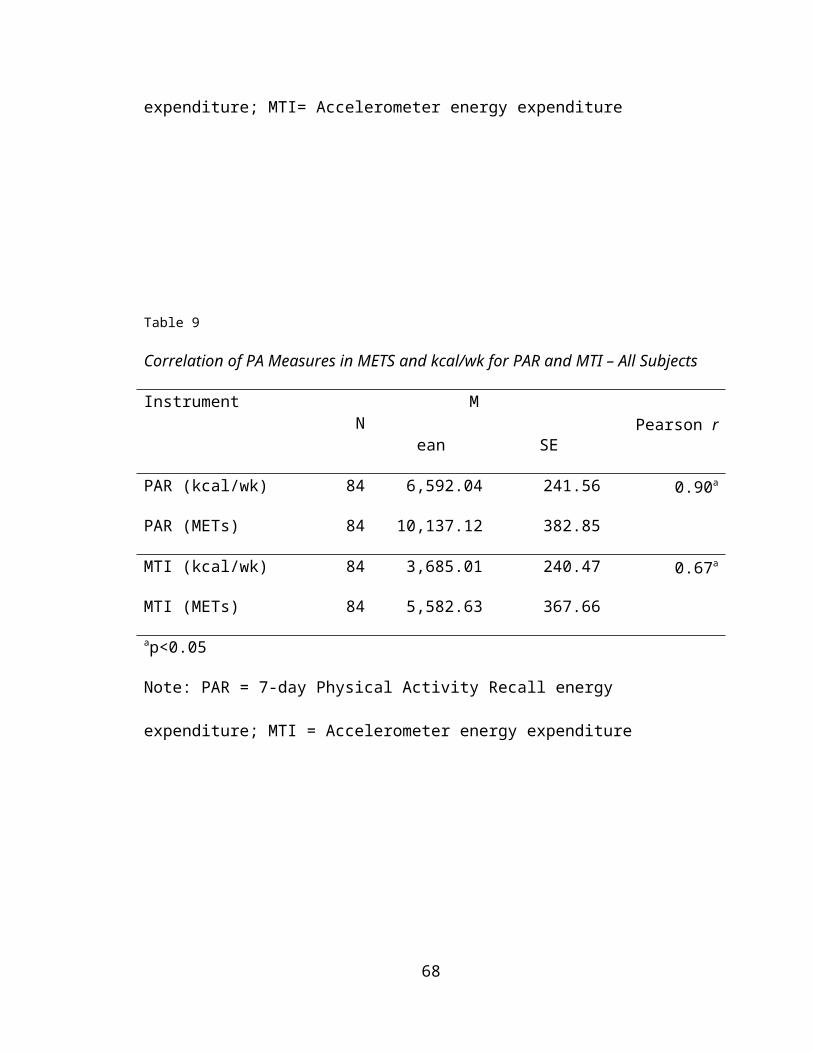
34%. Independent variables that were hypothesized to influence male subjects’
levels of PA that did not show significance were SE (r = 0.102, p = 0.527) and
barriers to PA (r = -0.005, p = 0.977).
The importance of SE as a determinant of PA in adolescents has been
well established in the recent literature. Several studies show SE to be the
strongest predictor of PA, regardless of BMI, socioeconomic status, and age
(Reynolds, et al, 1990; Zakarian, Hovell, Hofstetter, Salles, & Keating, 1994;
Trost, et al, 1997). In this sample of male adolescents, SE was not significantly
related to PA (r = 0.102, p = 0.527). A minimum aggregate score on the SAHHP
of eight by one subject and a maximum aggregate score of 48 by another subject
could indicate set responses by those subjects. However, these scores remained
in the analysis along with other outlier scores. Removal of outlier scores from the
dependent variable and from the independent variables in each group of subjects
did not result in significantly different means for those variables, therefore the
outlier scores for both groups remained in the analysis. Physical Education
classes at Rosa Fort High School are elective courses, not required by the state
of Mississippi. Therefore, it could be possible that students enrolling in physical
education courses already possess a higher level of exercise SE than others in
the student body, therefore resulting in increased SE scores, regardless of PA
level. Furthermore, 20% of male subjects were currently a member of a school–
sponsored athletic team, which could have also produced a SE score that is not
indicative of the population.
Barriers to PA are significant in a high school population (Allison, Dwyer,
69
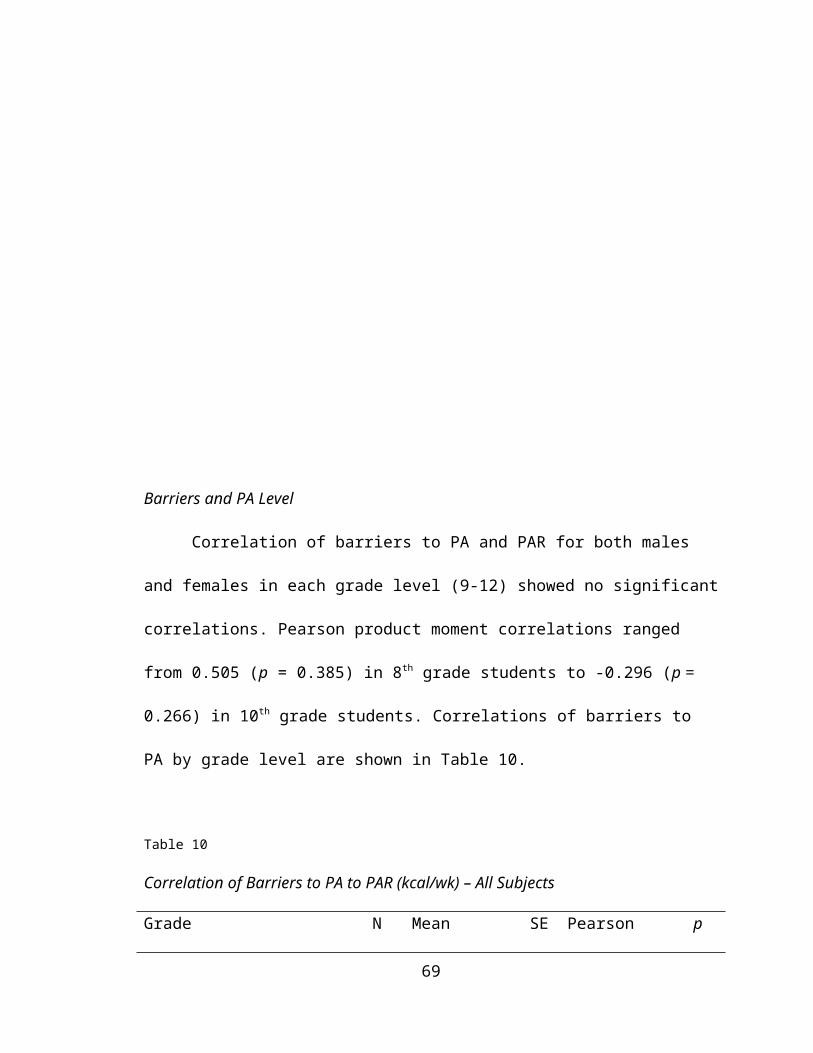
and Makin, 1999b). However, past studies found perceived barriers to PA were
not constant across all grade levels, that they are only predictive of PA in
subjects in grade 9. In this sample of male adolescents, barriers to PA are not
significantly related to PA level (r = -0.005, p = 0.977). Also, barriers to PA do not
correlate with any other independent variable. Furthermore, in this sample of
male adolescents, the result of the correlation between barriers to PA and
SAHHP is unexpected. It would be expected that as barrier scores decrease, SE
would increase, resulting in a negative correlation. However, in this sample of
male adolescents, this is not the case (r = 0.050, p = 0.755).
This study did not examine the effect of specific barriers on PA. Future
studies with this population may consider examining barrier types and their effect
on PA in this sample of male adolescents. Included in the barriers to PA listed for
this study, were cost and lack of facilities. In recent studies of adult barriers to
PA, these two barriers to PA were the most common listed. However, in Tunica
County, MS access to facilities and cost are issues that are addressed effectively
by the Parks and Recreation department. Furthermore, previous studies with
adolescents that have addressed barriers to PA have been conducted in an
urban population. This research with rural African-American adolescents may
represent a unique situation where barriers to PA most common in urban
adolescents, do not affect the PA levels of adolescents in a rural setting. Barriers
to PA that have been identified in the recent literature that were not assessed by
the current instrument include weather problems, safety of both the
70

neighborhood and route to facilities, and the presence of sidewalks (Richter,
Wilcox, Greaney, Henderson, & Ainsworth, 2002; Sharpe, Granner, Hutto, &
Ainsworth, 2004).
Comparison of Regression Equations
Originally developed for use in economics, the Chow test (Chow, 1960)
assesses the equality between sets of coefficients in two linear regression
equations. This test was conducted to examine whether the relationship between
SE, barriers to PA, age, BMI and PAR were the same across both female and
male samples. In order to test this possible equality in our sample of adolescents,
the Chow test obtains the sum of squares of the residuals assuming equality
(SSe – both groups) and the sum of squares without assuming the equality (SSe
– M, SSe – F). The ratio of the difference between these two sums to the latter
sum (SSe – M, SSe – F), adjusted for the corresponding degrees of freedom (5,
74), will be distributed as the F ratio under the null hypothesis. The comparison
of the regression equation for females and the regression equation for males in
this sample results in a non-significant F ratio (F (5, 74) = 1.848, Fcv = 2.37). A
non-significant F ratio for the Chow test indicates that quantitatively, separate
regression equations for female and male subjects are not statistically different.
Results for each regression equation however, show that males and females
share only a significant coefficient between BMI and PAR (Females: β = 0.47,
p<0.05; Males: β = 0.45, p<0.05), and a non-significant coefficient between
barriers to PA and PAR (Females: β = 0.12, p = 0.37; Males: β = -0.01, p = 0.92).
71
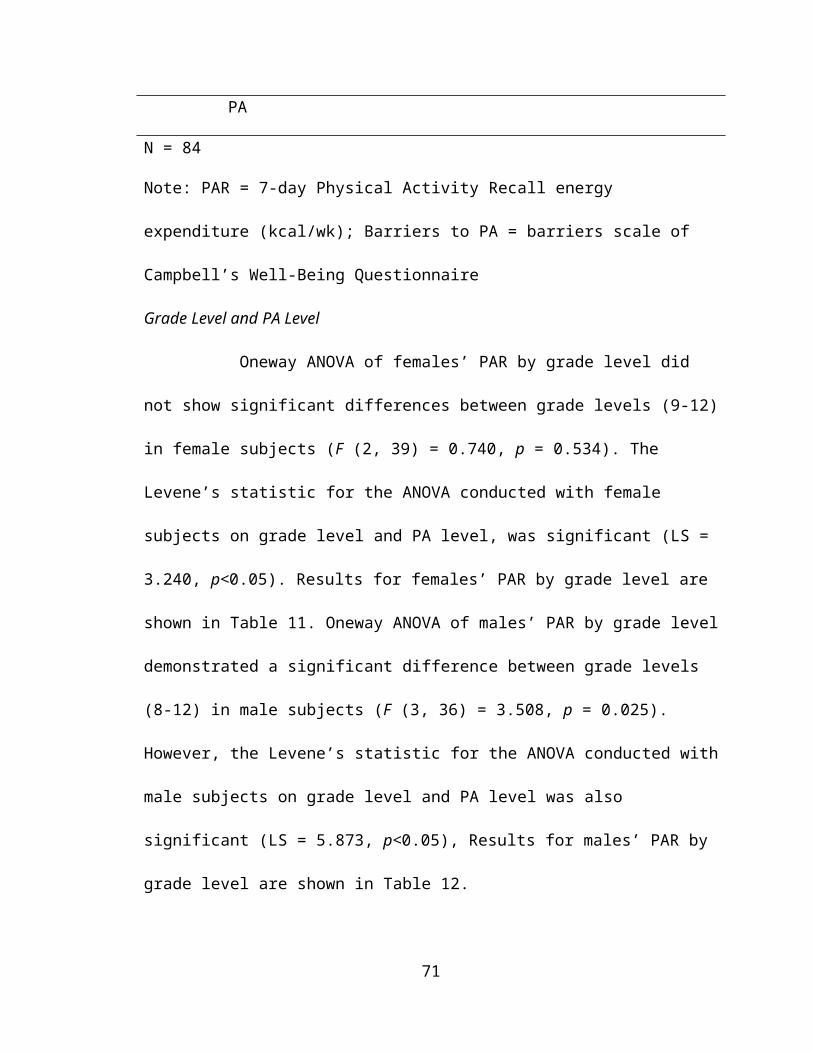
Female regression equation also shows a significant coefficient between SAAHP
and PAR (β = 0.32, p<0.05), as well as a non-significant coefficient between age
and PAR (β = -0.06, p = 0.650). Conversely, the regression equation for males
shows a significant coefficient between age and PAR (β = 0.49, p<0.05) and a
non-significant coefficient between SHAAP and PAR (β = 0.07, p = 0.608).
Summary
The purpose of this study was two-fold. First, this study was to identify the
determinants of PA of African-American schoolchildren ages 12-19 in Tunica
County, Mississippi. A secondary purpose of this study was to determine the
relationships among and identify differences between recognized determinants of
PA (age, body mass index, SE, and perceived barriers to PA) of the students.
The data show that female subjects’ PA level was accounted for by BMI
followed by SE. Correlation matrices showed no relationship between females’
PA level and barriers to PA or age. The regression model for female subjects
showed that BMI accounted for 24% of the variance in PA level, with the addition
of SE resulting in a regression model that accounted for 34% of the variance in
PA level, in this sample of female adolescents.
Data for male subjects show that PA level was accounted for by BMI
followed by age. Correlation of PA level with independent variables showed no
relationship between the dependent variable and barriers to PA and SE in this
sample of male adolescents. Regression analysis showed that BMI accounted for
28% of the variance in PA level. The addition of age resulted in a regression
72
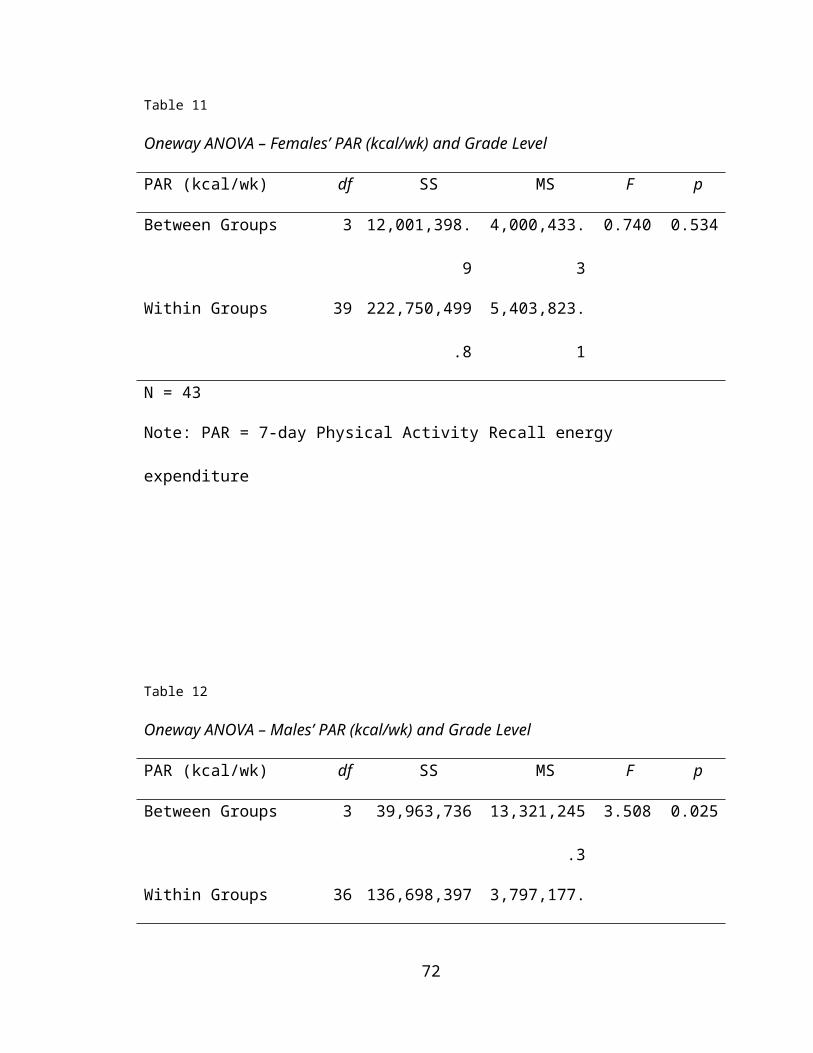
model that accounted for 34% of the variance in PA level, in this sample of male
adolescents.
Also, the Chow test was conducted to compare regression equations for
both female and male groups of subjects. Results of the Chow test show that the
regression equations for female and male adolescents in this sample results in a
non-significant F ratio (F (5, 74) = 1.848, Fcv = 2.37), which indicates that
quantitatively, separate regression equations for female and male subjects are
not statistically different. Therefore, based upon the data presented, it is
concluded that for both females and males in this sample of rural African-
American adolescents BMI is a recognized determinant of PA, and that barriers
to PA are not related to PA level. Furthermore, for male subjects, in addition to
BMI, age is also a predictor of PA level, and that SE has a nonsignificant
relationship to PA level. For female subjects, SE was also found to be a
significant predictor of PA level, and age was found to have a nonsignificant
relationship to PA in this sample. Finally, results of the Chow test show that
regression equations for females and males are not significantly different.
Conclusions
Based upon correlation and regression analyses and the Chow test, the
following conclusions are warranted. In rural African-American adolescent
females, BMI and SE predict subjectively measured PA. Other hypothesized
predictors of PA, barriers to PA and age show nonsignificant relationships to PA
level. Therefore we fail to reject null hypothesis one, based upon the lack of
73

significance in the correlations for the independent variables barriers to PA and
age with the dependent variable, PAR.
In rural African-American adolescent males, subjectively measured PA is
predicted by BMI and age. Other hypothesized predictors of PA, barriers to PA
and SE show non-significant relationships to PA level. Therefore we fail to reject
null hypothesis two based upon the lack of significance in the correlations for the
independent variables barriers to PA and age with the dependent variable PAR.
Based on the results of the Chow test, regression equations for males and
females are not statistically different.
The results of this study allow researchers, school officials, community
leaders, and parents to better understand the possible determinants of PA in this
sample of African-American adolescents. The significant relationship of SE and
PA in this sample of females, demonstrates the need for programs and
interventions designed to enhance the SE of female adolescents. This research
also adds significantly to the existing data relating to determinants of PA in
African-American adolescents. The existing literature relating to determinants of
PA in an adolescent population has dealt primarily with urban, Caucasian
adolescents. Previous research with both rural and lower socioeconomic status
adolescents have also examined determinants of PA in Caucasian subjects.
Furthermore, studies examining determinants of PA in minority adolescents
utilized Hispanic subjects as the largest segment of their sample.
Recommendations
The following are the recommendations for further research based on this
74
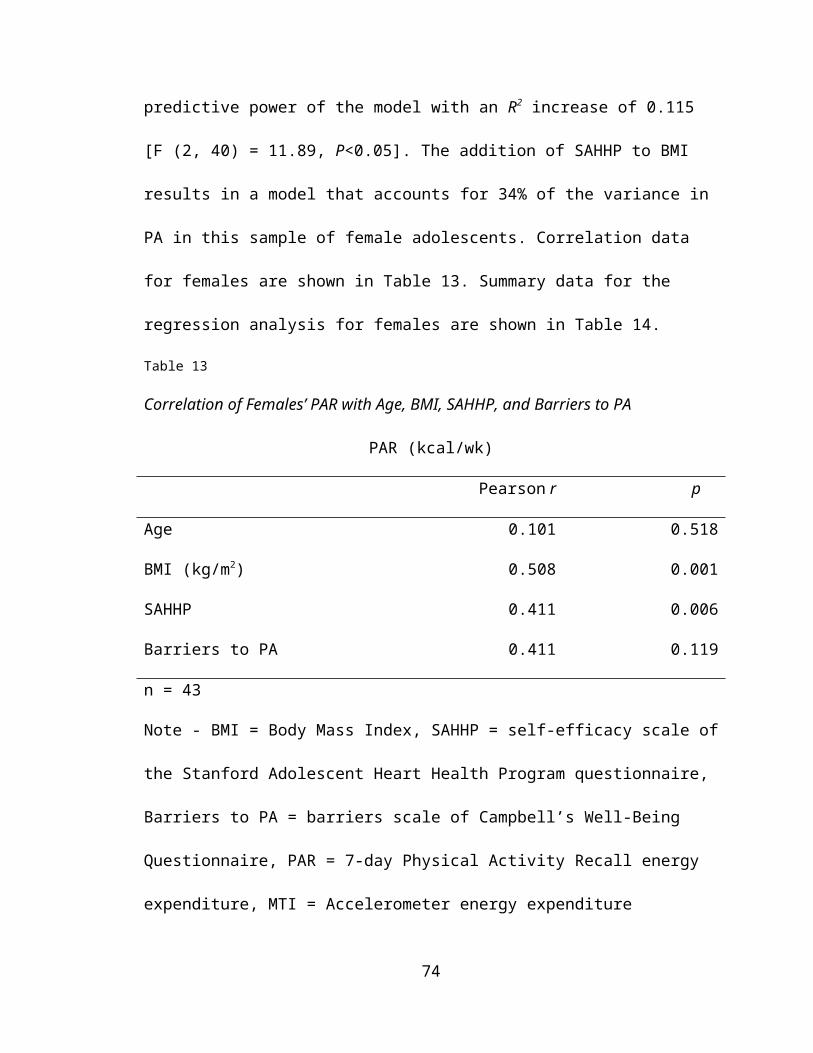
study. Random selection of rural African-American adolescents for participation
in future research. The current study drew from subjects from physical education
classes at Rosa Fort High School and from the Boys and Girls Club of the North
Mississippi Delta. Physical education is not a required course at the high school
and students that were enrolled in the class may have had an increased
perceived SE for PA, reduced barriers to PA, and may have been more active
than the normal population of students.
Another recommendation for further research in this population is to employ
an interview processes for completion of the seven-day PAR. The PAR has been
utilized effectively in an interview setting as well as a self-administered
questionnaire. While the PAR was significantly correlated with the objective
measure of PA, MTI, the minimum and maximum scores for both (N = 84)
instruments in this study were as follows; PAR (kcal/wk) mean = 6,592, min. =
3,548.5, max. = 14,046.8, MTI (kcal/wk) mean = 3,685, min. = 1,127.7, max. =
14,002.9. Although the maximum score for each instrument was within 50
kcal/wk of one another (PAR – 14,046.8, MTI – 14,002.9), the difference in the
minimum scores (kcal/wk) was over 60% (PAR – 3,548.5, MTI – 1,127.7) and the
difference in the mean scores (kcal/wk) was over 45% (PAR – 6,592, MTI –
3,685).
Further research with this population could also make use of additional
measures of SE and barriers to PA. Previous research with the adolescent
population utilized the SAHHP and the Campbell’s questionnaire, exclusively.
The questionnaire used to measure SE in this sample consisted of only eight
75
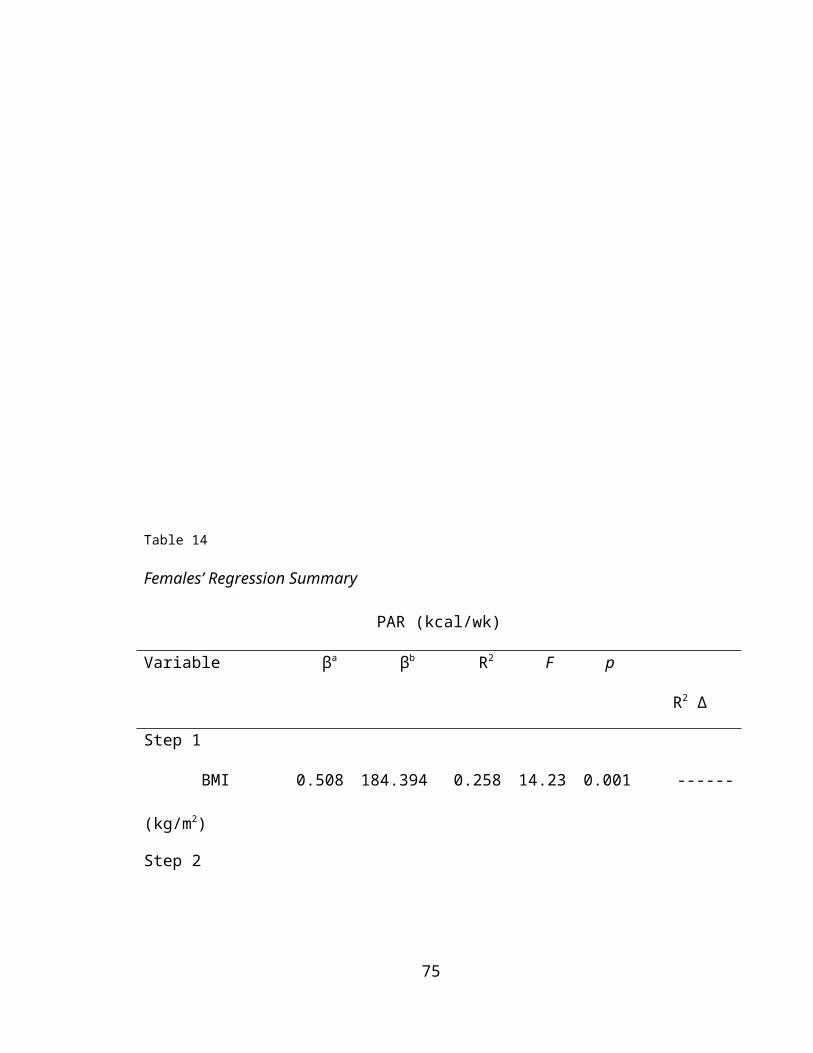
questions, which may not have accurately measured the SE of the sample. The
specific barriers to PA assessed in this study may have been inappropriate for a
rural, lower SES population. Also, previous studies examining barriers to PA in
adolescents have been set in an urban environment.
In both the male and female groups only 34% of the variance in PAR is
accounted for by the independent variables. Other studies with this population of
adolescents should seek to identify additional variables, not assessed in the
current project that may account for additional variance in PAR. This study
assessed four independent variables (BMI, age, SE, and barriers to PA). Future
studies should assess other variables that have been examined in previous
research such as type of PA (physical education class activity, extracurricular
school activity, out of school activity), parental PA levels, parental support, and
specific barriers to PA. Other studies have also given the subjects an opportunity
to allow subjects to list specific barriers, which may be useful for future studies
with similar samples of adolescents. Professionals developing intervention
programs for this sample of adolescent females are encouraged to create
programs and activities that attempt to improve SE. Programs for males should
utilize enjoyable and effective activities that can increase PA levels among all
ages of the current sample.
76
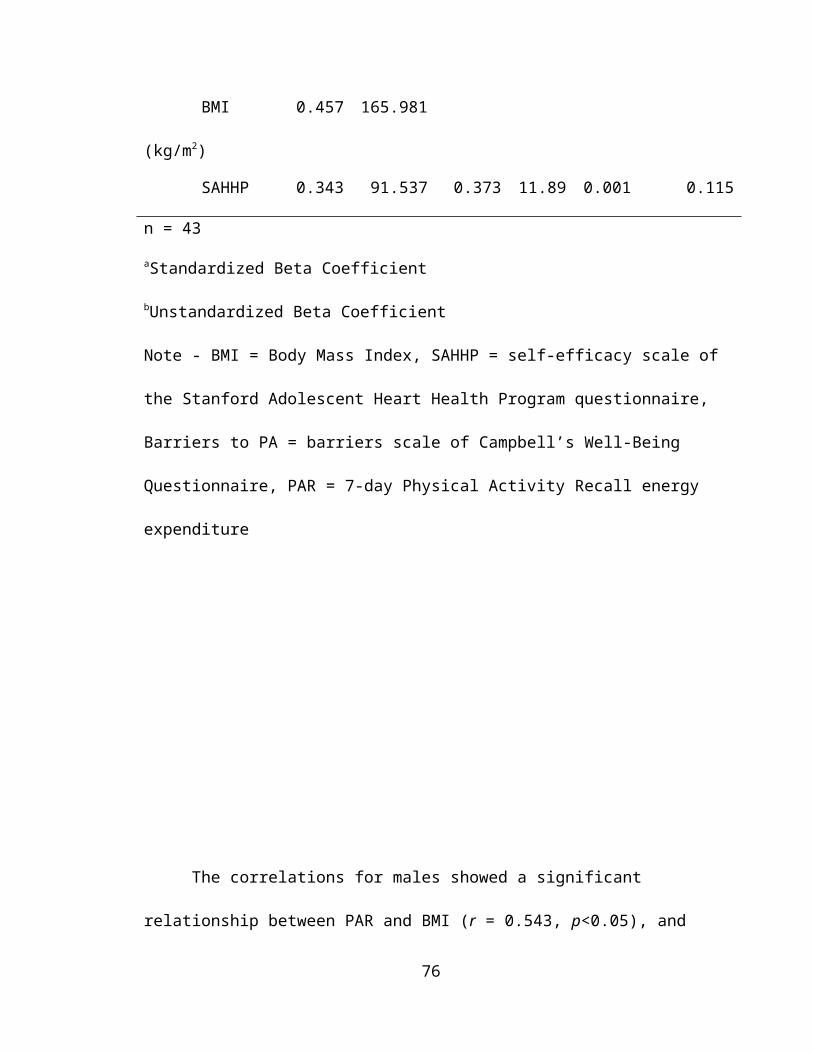
77
LIST OF REFERENCES
Aaron, D.J., Kriska, A.M., Dearwater, S.R., Anderson, R.L., Olsen, T.L., Cauley,
J.A., et al. (1993). The epidemiology of leisure physical activity in an
adolescent population. Medicine and Science in Sports and Exercise. 25,
847-53.
Allison, K.R., Dwyer, J.J., & Makin, S. (1999a). Perceived barriers to physical
activity among high school students. Preventive Medicine. 28, 608-15.
Allison, K.R., Dwyer, J.J., & Makin, S. (1999b). Self-efficacy and participation in
vigorous physical activity by high school students. Health Education
Behavior. 26, 12-24.
Armstrong, N., & Simons-Morton, B. (1994). Physical activity and blood lipids in
78
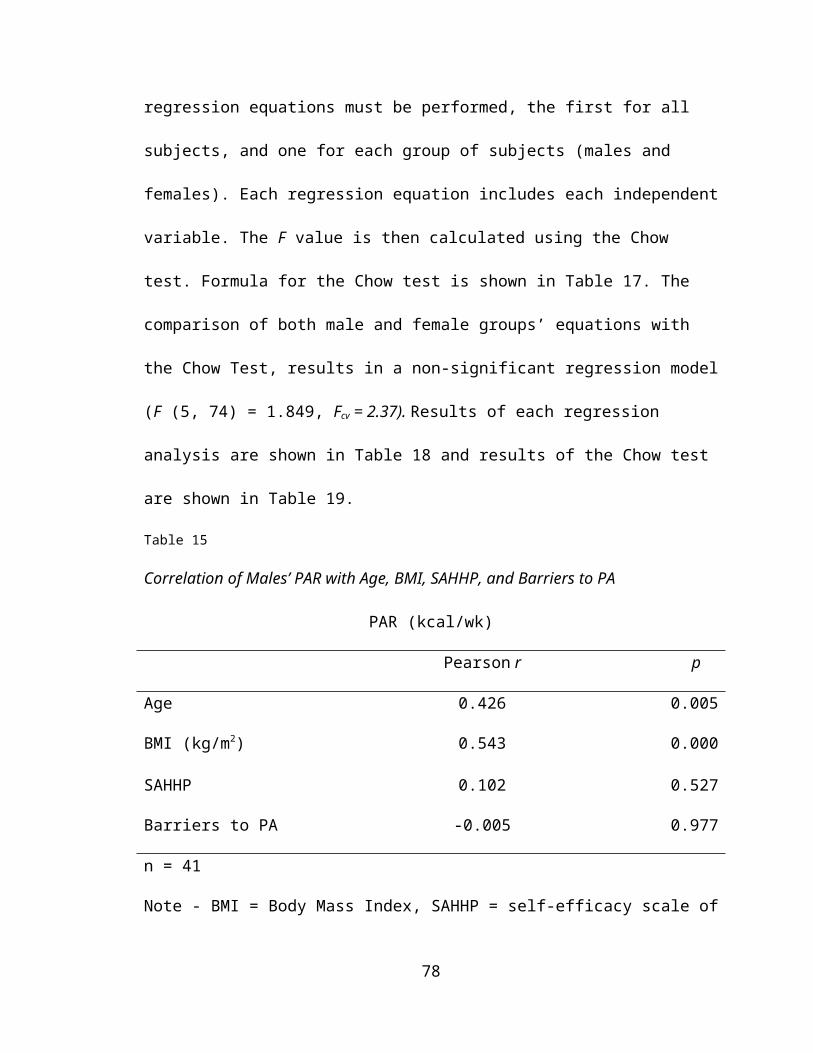
adolescents. Pediatric Exercise Science, 6, 381–405.
Arraiz, G.A., Wigle, D.T., & Mao, Y. (1992). Risk assessment of physical activity
and physical fitness in the Canada Health Survey Mortality Follow-up Study.
Journal of Clinical Epidemiology, 45, 419-28.
Arroll, B., & Beaglehole, R. (1992). Does physical activity lower blood pressure?
A critical review of the clinical trials. Journal of Clinical Epidemiology, 45,
439–447.
Bandura, A. Social foundations of thought and action: a social-cognitive theory.
Englewood Cliffs, NJ: Prentice-Hall, 1986.
Berenson, G., Srinivasan, S. & Nicklas, T. (1998). Atherosclerosis: a nutritional
disease of childhood. American Journal of Cardiology, 26, 22T-29T.
Bild, D.E., Jacobs, D.R., Sidney, S., Haskell, W.L., Anderssen, N., & Oberman,
A. (1993). Physical activity in young black and white women. The CARDIA
study. Annals of Epidemiology, 3, 636-644.
Blair, S.N., Goodyear, N.N., Gibbons, L.W., & Cooper, K.H. (1984). Physical
fitness and incidence of hypertension in healthy normotensive men and
women. Journal of the American Medical Association, 252, 487–490.
Blair ,S.N., Kohl, H.W. III, Barlow, C.E., Paffenbarger, R.S. Jr, Gibbons, L.W., &
Macera, C.A. (1995). Changes in physical fitness and all-cause mortality: a
prospective study of healthy and unhealthy men. Journal of the American
Medical Association, 273, 1093–1098.
Blair, S.N., Kohl, H.W. III, Paffenbarger, R.S. Jr, Clark, D.G., Cooper, K.H., &
Gibbons L.W. (1989). Physical fitness and all cause mortality: a prospective
79
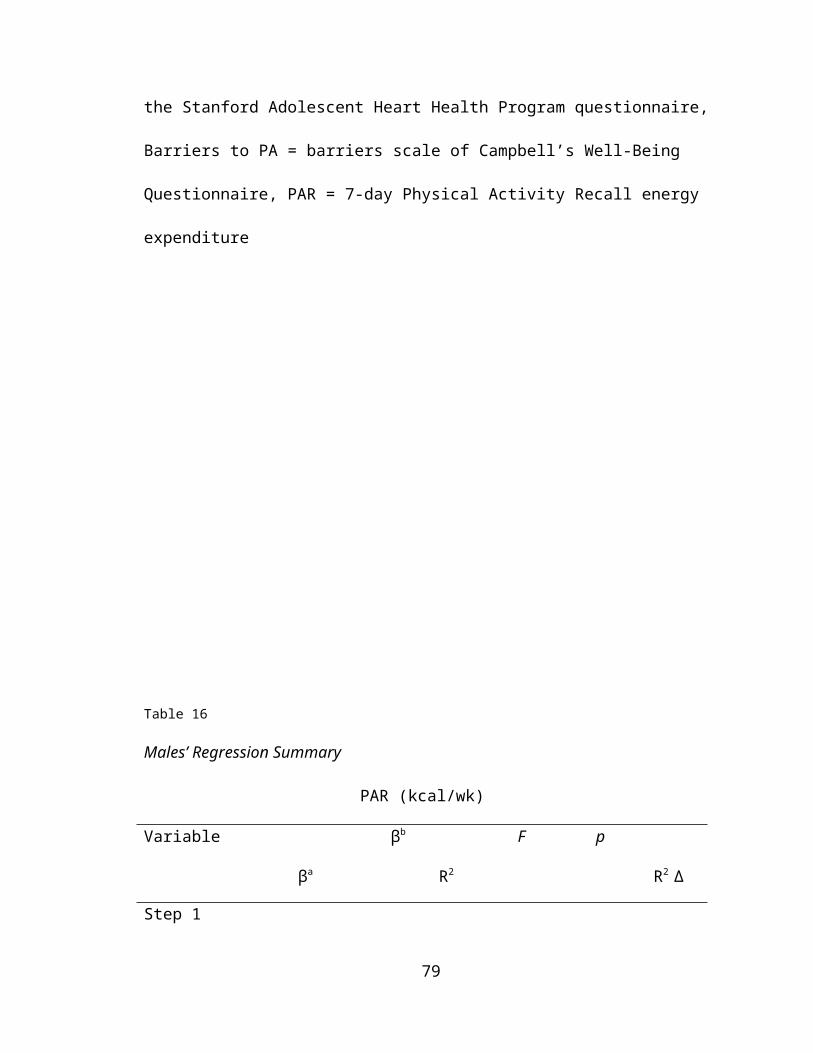
study of healthy men and women. Journal of the American Medical
Association, 262, 2395–2401.
Blair, S.N., Haskell, W.L., Ho, P., Paffenbarger, R., Vranizan, K., Farquar, J., et
al. (1985). Assessment of habitual physical activity by a seven-day recall in
a community survey and controlled experiments. American Journal of
Epidemiology, 122, 794-804.
Blair, S.N., Applegate, W., Dunn, A., Ettinger, W., Haskell, W.L., King, A., et al.
(1998). Activity counseling trial (ACT): rationale, design, and methods.
Activity Counseling Trial research Group. Medicine and Science in Sports
and Exercise, 30, 1097-106.
Body Mass Index Calculator, http://www.halls.md/body-mass-index/bmi.htm.
2000.
Brownson, R.C., Baker, E.A., Housemann, R.A., Brennan, L.K., & Bacak, S.J.
(1997). Environmental and policy determinants of physical activity in the
United States. American Journal of Public Health. 91, 1995-2003.
Butcher, J. (1983). Socialization of adolescent girls into physical activity.
Adolescence. 18, 753-766.
Calfas, K, & Long, B. (1996). A controlled trial of physician counseling to promote
the adoption of physical activity. Preventive Medicine, 25, 225-233.
Canada Fitness Survey. Fitness and lifestyle in Canada. (1983). Fitness Canada,
Ottawa.
Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance
System Survey Data. Atlanta, Georgia: U.S. Department of Health and
80
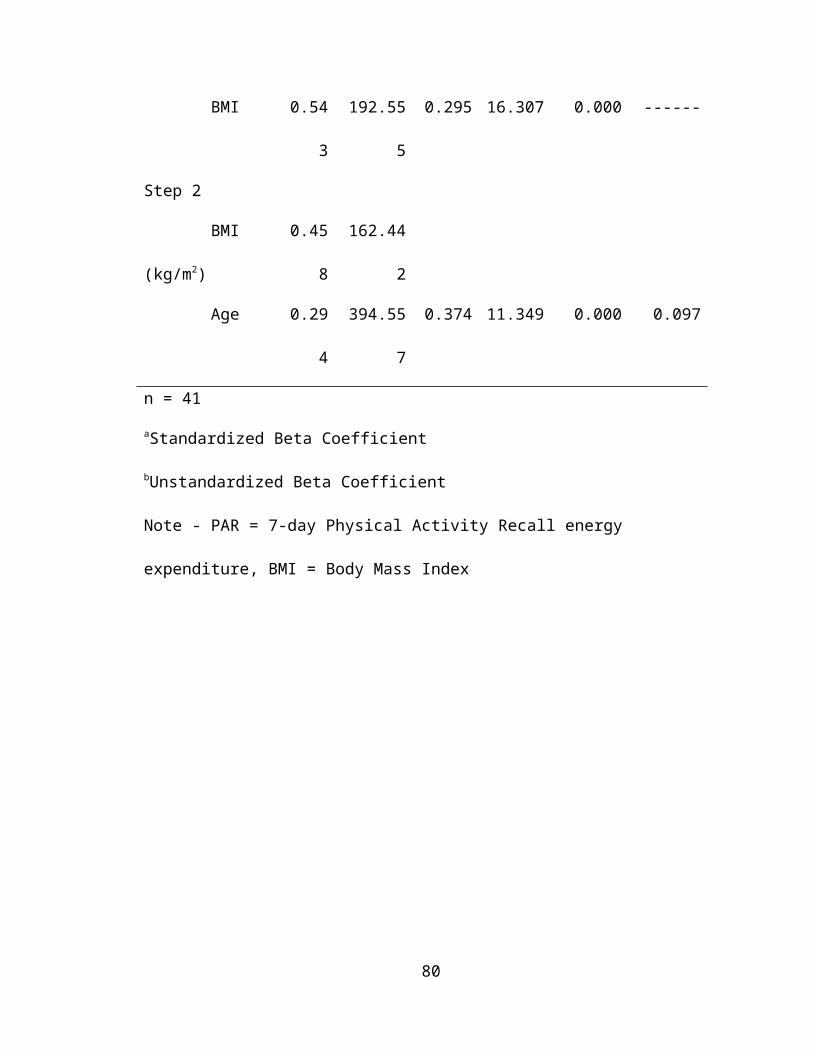
Human Services, Centers for Disease Control and Prevention, 1996.
Centers for Disease Control and Prevention. Increasing physical activity: a report
on recommendations of the Task Force on Community Preventive Services.
MMWR 2001; 50(No. RR-18).
Chang-Claude, J., & Frentzel-Beyme, R. (1993). Dietary and lifestyle
determinants of mortality among German vegetarians. International Journal
of Epidemiology, 22, 228–236.
Chen, M. & Lowenstein, F. (1986). Epidemiology factors related to self-reported
diabetes among adults. American Journal of Preventive Medicine, 2, 14-9.
Chinburapa, V., Larson, L.N., Bootman, J.L., McGhan, W. & Nicholson, G.
(1987). Prescribing intention and the relative importance of drug attributes: a
comparative study of HMO and fee-for-service physicians. Journal of
Pharmaceutical Marketing and Management, 2, 89-105.
Chow, G.C. (1960). Tests of equality between sets of coefficients in two linear
regressions. Econometrica, 28, 291-605.
Clarke, H.H. ed. (1973). National adult physical fitness survey. President’s
Council on Physical Fitness and Sports Newsletter. Washington DC.
Cohen, A. & Cohen, P. (1984). Applied Multiple Regression/Correlation Analysis
for the Behavioral Sciences. (2nd ed.). Mahwah, NJ: Lawrence Erlbaum and
Associates, Inc.
Cohen, M.V. Coronary collaterals: clinical and experimental observations. Mount
Kisco, NY: Futura Publishing Company, 1985.
Coleman, K., Saelens, B., Wiedrich-Smith, M., Flinn, J., & Epstein L. (1997).
81
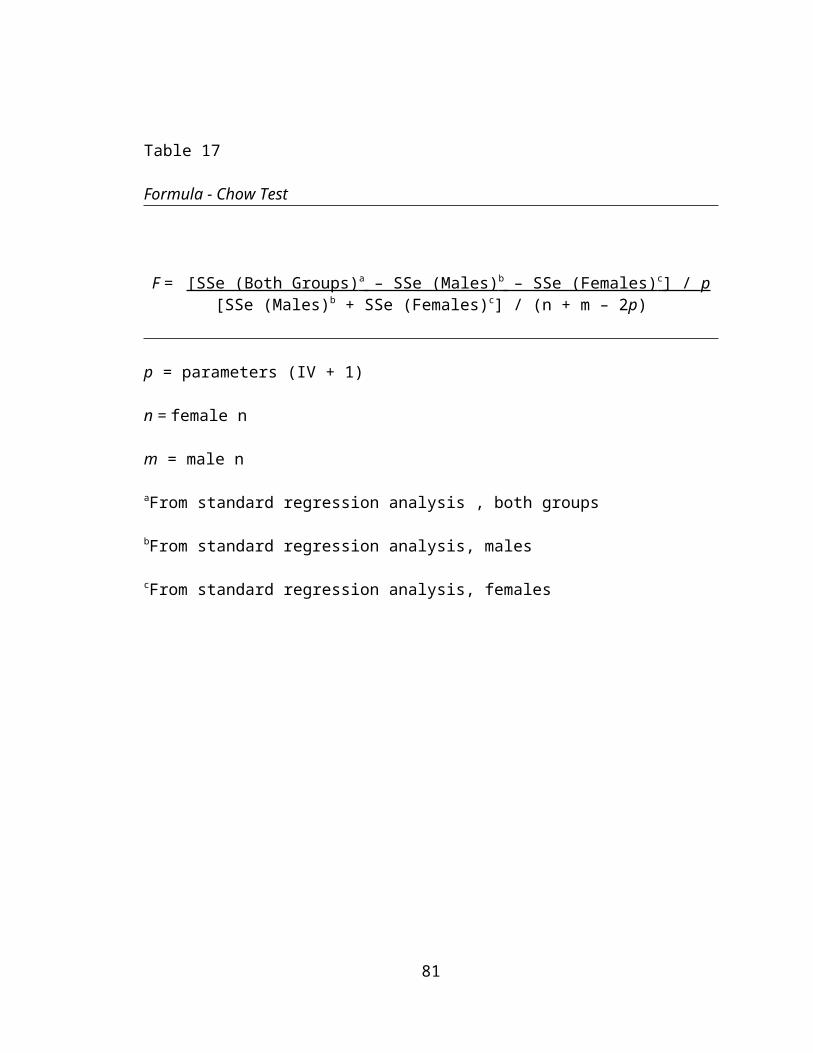
Relationships between TriTreac-R3D vectors, heart rate and self-report in
obese children. Medicine and Science in Sports and Exercise, 29, 1535-
1542.
Conway, J.M., Seale, J., Jacobs, D, & Irwin, M., Ainsworth, B. (2002).
Comparison of energy expenditure estimates from doubly labeled water, a
physical activity questionnaire, and physical activity records. American
Journal of Clinical Nutrition, 75, 519-525.
Cox, M.H. (1984). Fitness and lifestyle programs for business and industry:
problems in recruitment and retention. Journal of Cardiac rehabilitation. 4,
136-142.
Dishman, R.K., Sallis, J.F., & Orenstein, D.R. (1985). The determinants of
physical activity and exercise. Public Health Report, 100, 158-71.
Dowse, G., Zimmet, P. & King, H. (1991). Relationship between prevalence of
impaired glucose tolerance and NIDDM in a population. Diabetes Care. 14,
968-74.
Dunn, A., Marcus, B, Kampert, J., Garcia, M., Kohl, H., & Blair, S. (1997).
Reduction in cardiovascular risk disease factors: 6-month results from
Project Active. Preventive Medicine, 26, 883-892.
Dunn, A.L., Marcus, B.H., Kampert, J.B., Garcia, M.E., Kohl, H.W., & Blair, S.N.
(1999). Comparison of lifestyle and structured interventions to increase
physical activity and cardiorespiratory fitness. Journal of American Medical
Association, 281, 327-334.
Durstine, J.L., & Haskell, W.L. (1994). Effects of exercise training on plasma
82
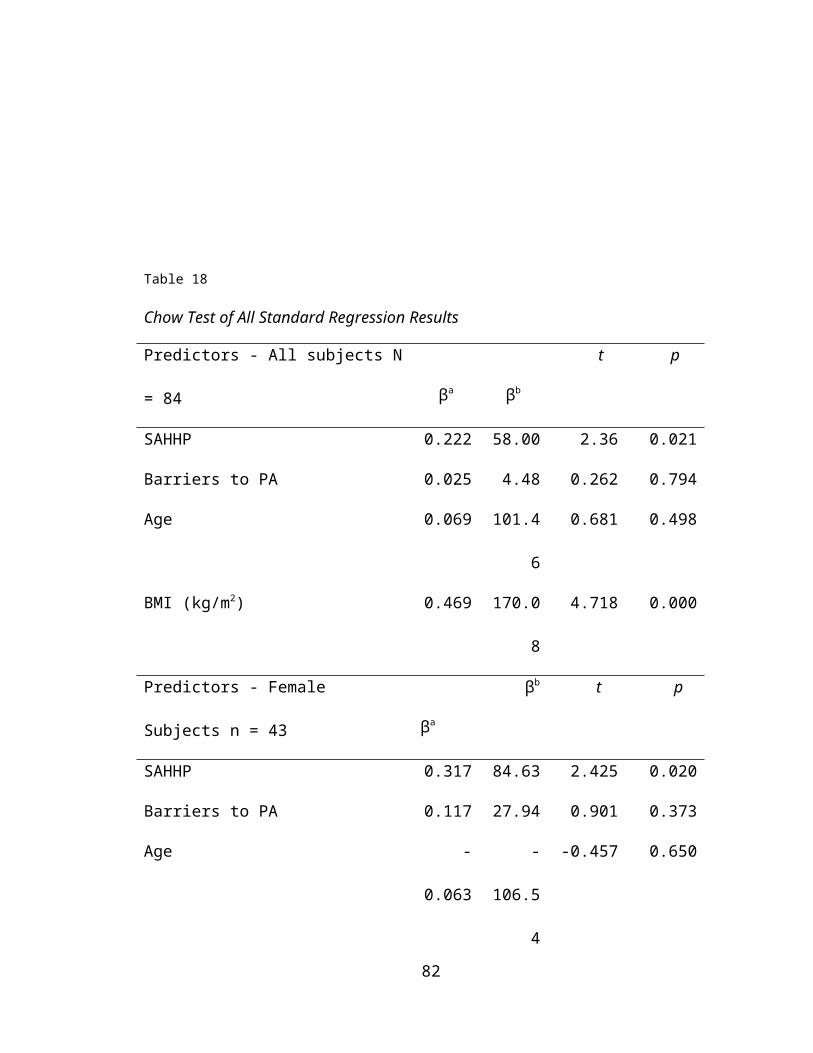
lipids and lipoproteins. Exercise and Sport Sciences Reviews, 22, 477–521.
Dwyer, J., Allison, K., & Makin, S. (1998). Internal structure of a measure of self-
efficacy in physical activity among high school students. Social Science and
Medicine, 9, 1175-1182.
Ekelund, L.G., Haskell, W.L., Johnson, J.L., Whaley, F.S., Criqui, M.H., & Sheps,
D.S. (1988). Physical fitness as a predictor of cardiovascular mortality in
asymptomatic North American men. The Lipid Research Clinics Mortality
Follow-up Study.
New England Journal of Medicine, 319, 1379-84.
Ekelund U., Sjostrom, M., Yngve, A., Poortvliet, E., Nilsson, A., Froberg, K., et al.
(2001). Physical activity assessed by activity monitor and doubly labeled
water in children. Medicine and Science in Sports and Exercise, 33, 275-81.
Eriksson, K.F., & Lindgärde, F. (1991). Prevention of type 2 (noninsulin-
dependent) diabetes mellitus by diet and physical exercise. Diabetologia,
34, 891–898.
Eyler, A., Matons-Koffman, D., Vest, J., Evensong, K., Sanderson, B.,
Thompson, J, et al. (2002). Environmental, policy, and cultural factors
related to physical activity in a diverse sample of women: The Women’s
Cardiovascular Health Network Project – summary and discussion. Women
and Health, 36, 123-134.
Feuer, E., Merrill, R., Kessler, L., Udler, J. & Rasband, G. (1999). Comparison or
risk estimates for selected diseases and causes of death. Preventive
Medicine, 28, 179-93.
83
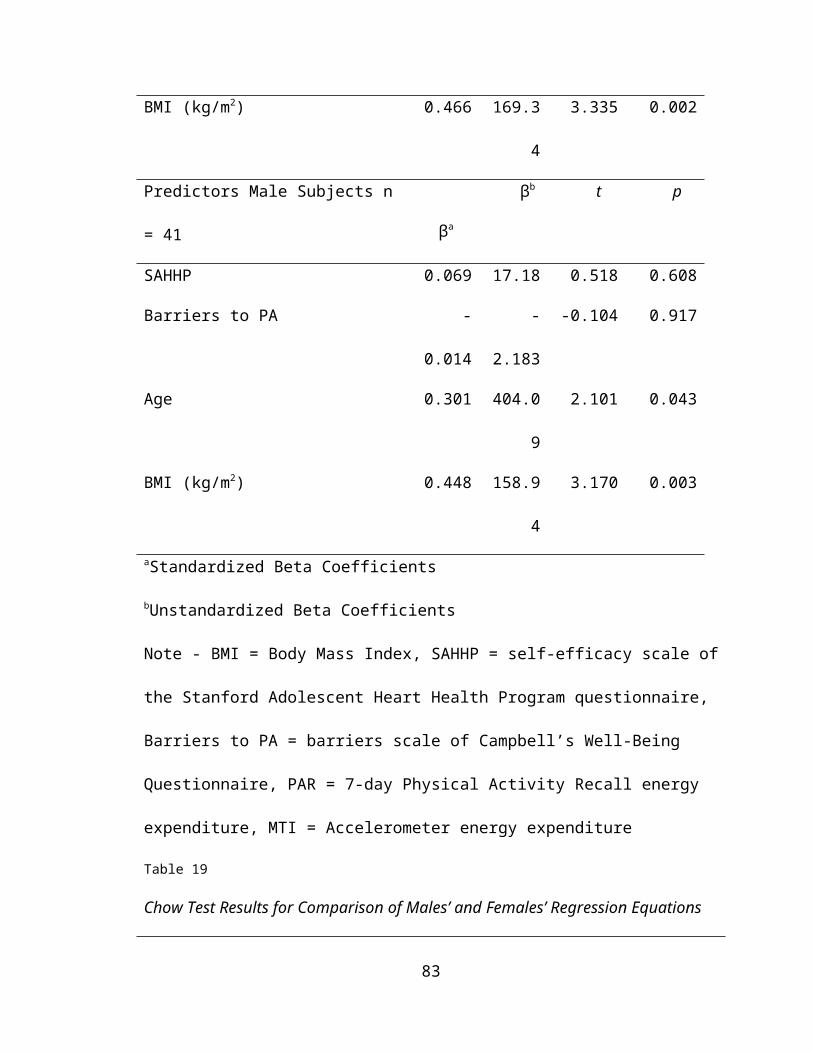
Folsom, A.R., Prineas, R.J., Kaye, S.A., & Munger, R.G. (1990). Incidence of
hypertension and stroke in relation to body fat distribution and other risk
factors in older women. Stroke, 21, 701–706.
Ford, E.S., Merritt, R.K., Heath, G.W., Powell K.E., Washburn, R.A., et al. (1991).
Physical activity behaviors in lower and higher socioeconomic status
populations. American Journal of Epidemiology, 133, 1246-1255.
Freedman, D.S., Dietz, W.H., Srinivasan, S.R., & Berenson, G.S. (1999). The
relation of overweight to cardiovascular risk factors among children and
adolescents: The Bogalusa Heart Study. Pediatrics, 103, 1175-1182.
Freedson, P., Melanson, E. & Sirard, J. (1998). Calibration of the Computer
Science and Applications, Inc. accelerometer. Medicine and Science in
Sports and Exercise, 30, 777-81.
Frisch, R.E., Wyshak, G., Albright, T.E., Albright, N.L., & Schiff, I. (1986). Lower
prevalence of diabetes in female former college athletes compared with
nonathletes. Diabetes, 35, 1101–1105.
Garcia, A.W., Broda, M.A., Frenn, M., Coviak, C., Pender, N.J., & Ronis, D.L.
(1995). Gender and developmental differences in exercise beliefs among
youth and prediction of their exercise behavior. Journal of School Health.
65, 6, 213-9.
Giovannucci, E., Ascherio, A., Rimm, E.B., Colditz, G.A., Stampfer, M., & Willett,
W.C. (1995). Physical activity, obesity, and risk for colon cancer and
adenoma in men. Annals of Internal Medicine, 22, 327-34.
Gottlieb, N.H., & Chen, M.S. (1985). Sociocultrual correlates of childhood
84
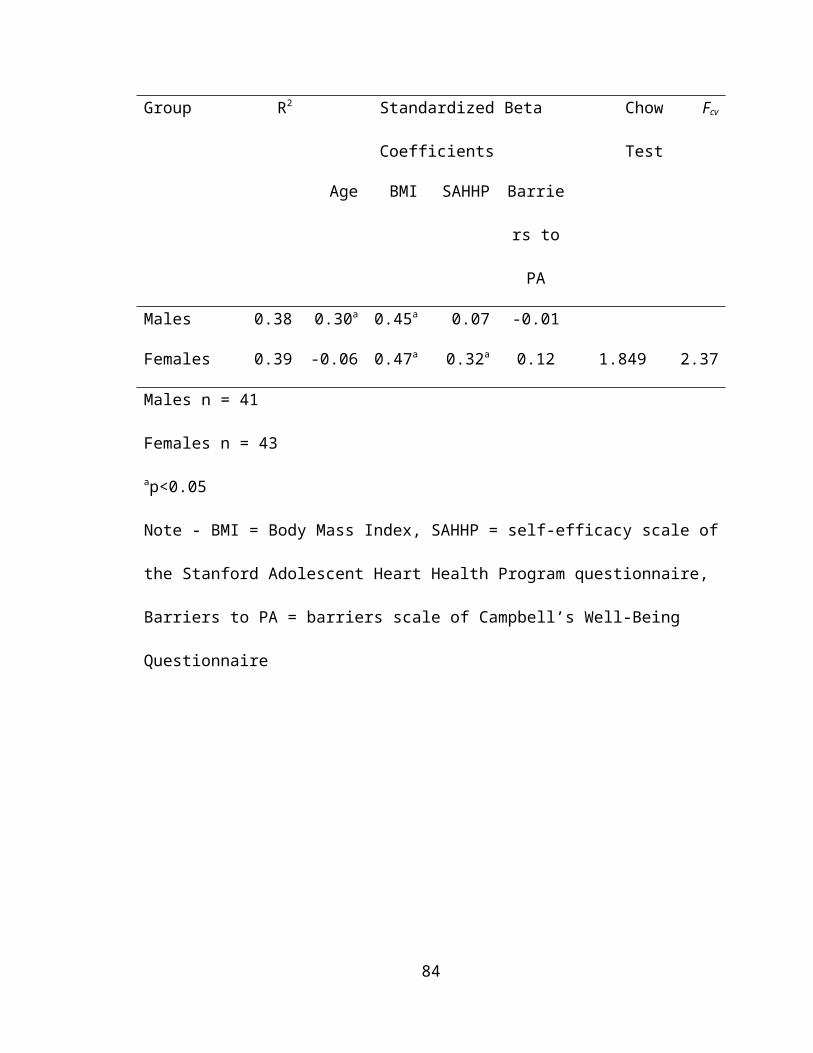
sporting activities: their implications for heart health. Social Science and
Medicine, 21, 533-539.
Grassi, K., Gonzalez, M.G., Tello, P., & He, G. (1999). La Vida Caminando: a
community-based physical activity program designed by and for rural Latino
families. Journal of Health Education, 30 (Suppl), S13-S17.
Greendorfer, S.L. (1983). Shaping the female athlete: the impact of the family. In,
The Sporting Woman, Boutsleier, M. & Giovani, S., Eds. Human kinetics
Publishers, Champaign, 135-155.
Hambrecht, R., Niebauer, J., Marburger, C., Grunze, M., Kälberer, B., Hauer, K.,
et al. (1993). Various intensities of leisure-time physical activity in patients
with coronary artery disease: effects on cardiorespiratory fitness and
progression of coronary atherosclerotic lesions. Journal of the American
College of Cardiology, 22, 468–477.
Harris, D.V. (1970). Physical activity history and attitudes of middle-aged men.
Medicine and science in Sports and Exercise. 2, 203-208.
Haskell, W.L., Alderman, E.L., Fair, J.M., Maron, D.J., Mackey, S.F., Superko,
H.R., et al. (1994). Effects of intensive multiple risk factor reduction on
coronary atherosclerosis and clinical cardiac events in men and women with
coronary artery disease: the Stanford Coronary Risk Intervention Project
(SCRIP). Circulation, 89, 975–990.
Hayden-Wade, H., Coleman, K., Sallis, J., & Armstrong, C. (2003). Validation of
the telephone and in-person interview versions of the 7-day PAR. Medicine
and Science in Sports and Exercise, 35, 801-809.
85
Heesch, K.C., Brown, D.R., & Blanton, C.J. (2000). Perceived barriers to
exercise and stage of exercise adoption in older women of different
racial/ethnic groups. Women and Health. 30, 61-76.
Helmrich, S.P., Ragland, D.R., Leung, R.W., & Paffenbarger, R.S. Jr. (1991).
Physical activity and reduced occurrence of noninsulin-dependent diabetes
mellitus. New England Journal of Medicine, 325, 147–152.
Holbrook, T.L., Barrett-Connor, E., & Wingard, D.L. (1989). The association of
lifetime weight and weight control patterns with diabetes among men and
women in an adult community. International Journal of Obesity, 13, 723–
729.
Irwin, M, Ainsworth, B., & Conway, J. (2001). Estimation of energy expenditure
from physical activity measures: determinants of accuracy. Obesity
Research, 9, 517-525.
Iverson, D.C., Feilding, J.E. Crow, R.S. & Christenson, G.M. (1985). The
promotion of physical activity in the U.S. population: the status of programs
in the medical, worksite, community, and school settings. Public Health
Reports. 100, 212-224.
Jacobs, D., Ainsworth, B., Hartman, T., & Leon, A. (1993). A simultaneous
evaluation of 10 commonly used physical activity questionnaires. Medicine
and Science in Sports and Exercise, 25, 81-91.
Janz, K., Witt, J., & Mahoney, L. (1995). The stability of children’s physical
activity as measured by accelerometry and self-report. Medicine and
Science in Sports and Exercise, 27, 1326-1332.
86

Jorgensen, C.R., Gobel, F.L., Taylor, H.L., & Wang, Y. (1977). Myocardial blood
flow and oxygen consumption during exercise. Annals of the New York
Academy of Sciences, 301, 213–223.
Kannel, W.B., Belanger, A., D’Agostino, R., & Israel, I. (1986). Physical activity
and physical demand on the job and risk of cardiovascular disease and
death: the Framingham Study. American Heart Journal, 112, 820-5.
Kannel, W.B., & Sorlie, P. (1979). Some health benefits of physical activity: the
Framingham study. Archives of Internal Medicine, 139, 857–861.
Kaplan, G.A., Seeman, T.E., Cohen, R.D., Knudsen, L.P., & Guralnik, J. (1987).
Mortality among the elderly in the Alameda County Study: behavioral and
demographic risk factors. American Journal of Public Health, 77, 307–312.
Kaye, S.A., Folsom, A.R., Sprafka, J.M., Prineas, R.J., & Wallace, R.B. (1991).
Increased incidence of diabetes mellitus in relation to abdominal adiposity in
older women. Journal of Clinical Epidemiology, 44, 329–334.
Kelley, G., & McClellan, P. (1994). Antihypertensive effects of aerobic exercise: a
brief meta-analytic review of randomized controlled trials. American Journal
of Hypertension, 7, 115–119.
King, A.C., & Frederiksen, L.W. (1984). Low-cost strategies for increasing
exercise behavior; relapse preparation training and social support. Behavior
Modification, 8, 3–21.
King, H., & Kriska, A.M. (1992). Prevention of type II diabetes by physical
training: epidemiology considerations and study methods. Diabetes Care,
15, 1794–1799.
87
King, A.C. & Brassington, G. (1997). Enhancing physical and psychological
functioning g in older family caregivers: the role of regular physical activity.
Annals of Behavioral Medicine, 19, 91-100.
King, A.C., Castro, C., Wilcox, S., Eyler, A.A., Sallis, J.F., & Brownson, R.C.
(2000). Personal and environmental factors associated with physical
inactivity among different racial-ethnic groups of U.S. middle-aged and
older-aged women. Health Psychology, 19, 354-64.
Kohli, A. (1989). Determinants of influence in organizational buying: a
contingency approach. Journal of Marketing, 53, 50-65.
Kono, S., Sinchi, K., Ikeda, N., Yanai, F. & Imanishi, K. (1991). Physical activity,
dietary habits and adenomatous polyps of the sigmoid colon: a study of self-
defense officials in Japan. Journal of Clinical Epidemiology, 44, 1255-61.
Kriska, A.M, & Bennett, P.H. (1992). An epidemiological perspective of the
relationship between physical activity and NIDDM: from activity assessment
to intervention. Diabetes/Metabolism Reviews, 8, 355–372.
Kriska, A.M., Blair, S.N., & Pereira, M.A. (1994). The potential role of physical
activity in the prevention of noninsulin dependent diabetes mellitus: the
epidemiological evidence. Exercise and Sport Sciences Reviews, 22, 121–
143.
Kriska, A.M., Gregg, E.W., Utter, A.C., Knowler, W.C., Narayan, V., & Bennett,
P.H. (1993). Association of physical activity and plasma insulin levels in a
population at high risk for NIDDM. Medicine and Science in Sports and
Exercise, 26, S121.
88
LaCroix, A.Z., Leveille, S.G., Hecht, J.A., Grothaus, L.C., Wagner, E.H. (1996).
Does walking decrease the risk of cardiovascular disease hospitalizations
and death in older adults? Journal of the American Geriatrics Society, 44,
113–120.
Landgraf, J.M. & Abetz, L.N. (1997). The physical and psychosocial well being of
children representing three cultural groups: Initial self-reports using the
Child Health Questionnaire (CHQ-CF87). Psychology and Health, Quality of
Life: Recent Advances in Theory and Methods, 12, 839-854.
Lauer, R.M., Connor, W.E., & Leaverton, P.E. (1975). Coronary heart disease
risk factors in school children: the Muscatine study. Journal of Pediatrics,
86, 697-706.
Laughlin, M.H. (1994). Effects of exercise training on coronary circulation:
introduction. Medicine and Science in Sports and Exercise, 26, 1226–1229.
Leon, A.S., Bloor, C.M. (1968). Effects of exercise and its cessation on the heart
and its blood supply. Journal of Applied Physiology, 24, 485–490.
Leon, A.S., Bloor, C.M. (1976). The effect of complete and partial deconditioning
on exercise-induced cardiovascular changes in the rat. Advances in
Cardiology, 18, 81–92.
Leon, A.S. (1991). Effects of exercise conditioning on physiologic precursors of
coronary heart disease. Journal of Cardiopulmonary Rehabilitation, 11, 46–
57.
Leon, A.S. (1991). Recent advances in the management of hypertension. Journal
of Cardiopulmonary Rehabilitation, 11, 182–191.
89
Leon, A.S., & Connett, J. (1991). Physical activity and 10.5 year mortality in the
Multiple Risk Factor intervention Trial (MRFIT). International Journal of
Epidemiology, 20, 690-7.
Leon, A.S. (1987). Age and other predictors of coronary artery disease. Medicine
and Science in Sports and Exercise, 19, 159-67.
Lindsted, K.D., Tonstad, S., & Kuzma, J.W. (1991). Self-report of physical activity
and patterns of mortality in Seventh-day Adventist men. Journal of Clinical
Epidemiology, 44, 355–364.
Longnecker, M.P., De Verdier, M.G., Frumkin, H., & Carpenter, C. (1995). A
case-control study of physical activity in relation to risk of cancer of the right
colon and rectum in men. International Journal of Epidemiology, 24, 42–50.
Manson, J.E., Nathan, D.M., Krolewski, A.S., Stampfer, M.J., Willett, W.C., &
Hennekens, C.H. (1992). A prospective study of exercise and incidence of
diabetes among U.S. male physicians. Journal of the American Medical
Association, 268, 63–67.
Matthews, C., & Freedson, P. (1995). Field trial of a three-dimensional activity
monitor: comparison with self-report. Medicine and Science in Sports and
Exercise, 27, 1071-1078.
McMurray, R., Harrell, J., Bradley, C., Webb, J., & Goodman, E. (1998).
Comparison of physical activity recall with a triaxial motion sensor in middle-
school youth. Medicine and Science in Sports and Exercise, 30, 1238-1245.
Miller, D, Freedson, P., & Kline, G. (1994). Comparison of activity levels using
the Caltrac accelerometer and five questionnaires. Medicine and Science in
90

Sports and Exercise, 26, 349-382.
Mississippi State Department of Health. Youth Risk Behavior Survey-Mississippi.
Mississippi State Department of Health, Jackson, Mississippi. 2001.
National Center for Health Statistics, Centers for Disease Control and
Prevention, Health E-Stats, 2001. (2000). Prevalence of Overweight Among
Children and Adolescents: United States, 2000.
O’Connor, G.T., Buring, J.E., Yusuf, S., Goldhaber, S.Z., Olmstead, E.M.,
Paffenbarger, R.S. Jr, et al. (1989). An overview of randomized trials of
rehabilitation with exercise after myocardial infarction. Circulation, 80, 234–
244.
Oldridge, N.B. (1982). Compliance and exercise in preliminary and secondary
prevention of coronary heart disease: a review. Preventive Medicine, 11, 56-
70.
Ornish, D., Brown, S.E., Scherwitz, L.W., Billings, J.H., Armstrong, W.T., Ports,
T.A., et al. (1990). Can lifestyle changes reverse coronary heart disease?
The Lifestyle Heart Trial. Lancet, 336, 129–133.
Ornish, D., Scherwitz, L.W., Billings, J.H., Gould, K.L., Merritt, T.A., Sparler, S.,
et al. (1998). Intensive lifestyle changes for reversal of coronary heart
disease. Journal of the American Medical Association, 280, 3, 2001-2007.
Overholser, K.A., Laughlin, M.H., & Bhatte, M.J. (1994). Exercise training-
induced increase in coronary transport capacity. Medicine and Science in
Sports and Exercise, 26, 1239–1244.
Paffenbarger, R.S. Jr, Hyde, R.T., Wing, A.L., Lee, I.M., Jung, D.L., & Kampert,
91
J.B. (1993). The association of changes in physical activity level and other
lifestyle characteristics with mortality among men. New England Journal of
Medicine, 328, 538–545.
Paffenbarger, R.S. Jr, Hyde, R.T., Wing, A.L., & Steinmetz, C.H. (1984). A
natural history of athleticism and cardiovascular health. Journal of the
American Medical Association, 252, 491–495.
Paffenbarger, R.S. Jr, Jung, D.L., Leung, R.W., & Hyde, R.T. (1991). Physical
activity and hypertension: an epidemiological view. Annals of Medicine, 23,
319–327.
Paffenbarger, R.S. Jr, Wing, A.L., Hyde, R.T., & Jung, D.L. (1983). Physical
activity and incidence of hypertension in college alumni. American Journal
of Epidemiology, 117, 245–257.
Pan, X., Li, G., & Hu, Y. (1995). Effect of dietary and/or exercise intervention on
incidence of diabetes in 530 subjects with impaired glucose tolerance from
1986–1992. Chinese Journal of Internal Medicine, 34, 108–112.
Penman, A.D. (2000). Overweight and obesity in Mississippi: a growing problem.
Journal of the Mississippi State Medical Association, 41,785-9.
Pinhas-Hamiel, O., Dolan, L.M., Daniels, S.R., Standiford, D., Khoury, P.R., &
Zeitler, P. (1996). Increased incidence of non-insulin-dependent diabetes
mellitus among adolescents. Journal of Pediatrics, 128, 608-615.
Quarry-Horn, J., Evans, B. & J Kerrigan. (2003). Type two diabetes mellitus in
youth. Journal of School Nursing. 19, 195-203.
Ramaiya, K., Swai, A., McLarty, D., Bhopal, R. & Alberti, K. (1991). Prevalence of
92
diabetes and cardiovascular disease risk factors in Hindu Indian
subcommunitites in Tanzania. British Medical Journal, 303, 271-6.
Rauh, M., Hovell, M., Sallis, J., & Hofstetter, C. (1992). Reliability and validity of
self-reported physical activity in Latinos. International Journal of
Epidemiology, 21, 966-971.
Reynolds, K., Killne, H., Bryson, S., Maron, D., Taylor, C, Maccoby, N., et al.
(1990). Psychosocial predictors of physical activity in adolescents.
Preventive Medicine, 19, 541-51.
Richter, D., Wilcox, S., Greaney, M., Henderson, K., & Ainsworth, B. (2002).
Environmental, policy, and cultural factors related to physical activity in
African American women. Women and Health, 36, 91-109.
Riddoch, C. & Boreham, C. (1995). The health-related physical activity of
children. Sports Medicine, 19, 86-102.
Rosenthal, M., Bain, S.H., Bush, A., & Warner, J.O. (1994). Weight/height 2.88
as a screening test for obesity or thinness in school-age children. European
Journal of Pediatrics, 153, 876-83.
Rubin, K., Schirduan, V., Gendreau, P., Sarfarazi, M., Mendola, R., & Dalsky, G.
(1993). Predictors of axial and peripheral bone mineral density in healthy
children and adolescents, with special attention to the role of puberty.
Journal of Pediatrics, 123, 863–870.
Sacks, M.H., & Sachs, M.L., Eds. (1981). Psychology of running. Human Kinetics
Publishers. Champaign, IL.
Sallis, J.F., Haskell, W.L., Fortmann, S., Vranizan, K.M., Taylor, C.B., &
93

Solomon, D.S. (1986). Predictors of adoption and maintenance of physical
activity in a community sample. Preventive Medicine, 15, 331-341.
Sallis, J.F., Haskell, W.L., Wood, P., Fortmann, S., Rogers, T., Blair, S.N., et al.
(1985). Physical activity assessment methodology in the five-city project.
American Journal of Epidemiology, 121, 91-106.
Sallis, J.F., Dishman, R.K., & Orenstein, D.R. (1985). Determinants of physical
activity and exercise. Public Health Reports, 100, 158-171.
Sallis, J.F., Buono, M.J., Roby, J.J., Carlson, D., & Nelson, J.A. (1990). The
Caltrac accelerometer as a physical activity monitor for school-age children.
Medicine and Science in Sports and Exercise. 22, 5, 698-703.
Sallis, J.F., Buono, M.J., Roby, J.J., Micale, F.G., & Nelson, J.A. (1993). Seven-
day recall and other physical activity self-report in children and adolescents.
Medicine and Science in Sports and Exercise, 25, 99-108.
Sallis, J.F., Simons-Morton, B.G., Stone, E.J., Corbin, C.B., Epstein, L.H.,
Faucette, N., et al. (1992). Determinants of physical activity and
interventions in youth. Medicine and Science in Sports and Exercise. 24,
S248-57.
Sanderson, B., Littleton, M., & Pulley, L. (2002). Environmental, policy, and
cultural factors related to physical activity among rural, African American
women. Women and Health, 36, 75-90.
Sandvik, L., Erikssen, J., Thaulow, E., Erikssen, G., Mundal, R., & Rodahl, K.
(1993). Physical fitness as a predictor of mortality among healthy, middle-
aged Norwegian men. New England Journal of Medicine, 328, 533–537.
94
Saris, J.F., Elvers, J.W., Van’t Hof, M.A., & Binkhorst, J. L. (1988). Changes in
physical activity of children ages 6-18 years. In: Children and Exercise XII.
Rutenfranz, J & Kilmt, F. (Eds.). Human Kinetics: Champaign, IL, 121-130.
Scheuer, J. (1982). Effects of physical training on myocardial vascularity and
perfusion. Circulation, 66, 491–495.
Schmitz, K.H., Jacobs, D.R., Hong, C.P., Steinberger, J., Moran, A. & Sinaiko,
A.R. (2002) Association of physical activity with insulin sensitivity in children.
International Journal of Obesity and Related Metabolic Disorders, 26, 1310-
6.
Schuler, G., Hambrecht, R., Schlierf, G., Niebauer, J., Hauer, K., Neumann, J, et
al. (1992). Regular physical exercise and low fat diet: effects on progression
of coronary artery disease. Circulation, 86, 1–11.
Severson, R.K., Nomura, A.M., Grove, J.S., & Stemmermann, G.N. (1989). A
prospective analysis of physical activity and cancer. American Journal of
Epidemiology, 130, 522–529.
Sharpe, P., Granner, M., Hutto, B., & Ainsworth, B. (2004). Association of
environmental factors to meeting physical activity recommendations in two
South Carolina counties. American Journal of Health Promotion, 18, 251-
257.
Sirard, J. & Pate, R. (2001). Physical activity assessment in children and
adolescents. Sports Medicine, 31, 439-454.
Slattery, M.L., Jacobs, D.R. Jr, & Nichaman, M.Z. (1989). Leisure-time physical
activity and coronary heart disease death: the U.S. Railroad Study.
95

Circulation, 79, 304–311.
Slattery, M.L., & Jacobs, D.R. Jr. (1988). Physical fitness and cardiovascular
disease mortality: the U.S. Railroad Study. American Journal of
Epidemiology, 127, 571–580.
Smith, T.W., & Leon, A.S. (1992). Coronary heart disease: a behavioral
perspective. Champaign, IL: Research Press.
Stalonas, P.M. Johnson, W.G. & Christ, M. (1978). Behavior modification for
obesity: the evaluation of exercise, contingency management, and program
adherence. Journal of Counseling Clinical Psychology, 46, 463-469.
Stamler, R., Stamler, J., Gosch, F.C., Civinelli, J., Fishman, J., McKeever, P., et
al. (1989). Primary prevention of hypertension by nutritional-hygienic
means: final report of a randomized, controlled trial. Journal of the American
Medical Association, 262, 1801–1807.
Stefanick, M.L., & Wood, P.D. Physical activity, lipid and lipoprotein metabolism,
and lipid transport. In: Bouchard C, Shephard RJ, Stephens T, editors.
Physical activity, fitness, and health: international proceedings and
consensus statement. Champaign, IL: Human Kinetics, 1994: 417–431.
Stender, M., Hense, H.W., Döring, A., & Keil, U. (1993). Physical activity at work
and cardiovascular disease risk: results from the MONICA Augsburg Study.
International Journal of Epidemiology, 22, 644–650.
Stephens, T., & Craig, C. (1990). The Well-Being of Canadians: Highlights of the
1988 Campbell’s Survey. Ottawa, Canadian Fitness and Lifestyle Research
Institute.
96
Stucky-Ropp, R.C., & DeLorenzo, T.M. (1993). Determinants of exercise in
children. Preventive Medicine, 22, 880-889.
Superko, H.R. (1991). Exercise training, serum lipids, and lipoprotein particles: is
there a change threshold? Medicine and Science in Sports and Exercise,
23, 677–685.
Taylor, W.C., Yancey, A.K., Leslie, J., Murray, N.G., Cummings, S.S., Sharkey,
S.A., et al. (1999). Physical activity among African American and Latino
middle school girls: consistent beliefs, expectations, and experiences across
two sites. Women and Health. 30, 2, 67-82.
The General Mills American Family Report, 1978-1979. (1979). Family health in
an era of stress. Yankelovich, Skelly and White, Inc., New York.
Tomanek, R.J. (1994). Exercise-induced coronary angiogenesis: a review.
Medicine and Science in Sports and Exercise, 26, 1245–1251.
Trost, S.G., Pate, R.R., Freedson, P.S., Sallis, J.F., & Taylor, W.C. (2000). Using
objective physical activity measures with youth: how many days of
monitoring are needed? Medicine and Science in Sports and Exercise. 32,
2, 426-31.
Trost, S.G., Pate, R.R., Sallis, J.F., Freedson, P.S., Taylor, W.C., Dowda, M., et
al. (2002). Age and gender differences in objectively measured physical
activity in youth. Medicine and Science in Sports and Exercise. 34, 2, 350-5.
Trost, S.G., Pate, R.R., Saunders, R., Ward, D.S., Dowda, M., & Felton, G.
(1997). A prospective study of the determinants of physical activity in rural
fifth-grade children. Preventive Medicine. 26, 257-63.
97
Tsopanakis, A.D., Sgouraki, E.P., Pavlou, K.N., Nadel, E.R., & Bussolari, S.R.
(1989). Lipids and lipoprotein profiles in a 4-hour endurance test on a
recumbent cycle ergometer. American Journal of Clinical Nutrition, 49, 980–
984.
Twisk, J., Kemper, H., & van Mechelen, W. (2000). Tracking of activity and
fitness and the relationship with cardiovascular disease risk factors.
Medicine and Science in Sports and Exercise, 32, 1455-61.
U.S. Department of Health and Human Services. (1992). Assessing Health Risk
Behaviors Among Young People: Youth Risk Behavior Surveillance System.
Atlanta, GA: U.S. Centers for Disease Control and Prevention, National
Center for Chronic Disease Prevention and Health Promotion.
U.S. Department of Health and Human Services. (2001). Assessing Health Risk
Behaviors Among Young People: Youth Risk Behavior Surveillance System.
Atlanta, GA: U.S. Centers for Disease Control and Prevention, National
Center for Chronic Disease Prevention and Health Promotion.
U.S. Department of Health and Human Services. (2001). Healthy People 2010.
[Rockville, MD]: U.S. Department of Health and Human Services Office of
Disease Prevention and Health Promotion.
U.S. Department of Health and Human Services. (1996). Physical Activity and
Health: A Report of the Surgeon General. Atlanta, GA: U.S. Department of
Health and Human Services, Centers for Disease Control and Prevention,
National Center for Chronic Disease Prevention and Health Promotion.
U.S. Department of Health and Human Services. (2001). Promoting Better Health
98

for Young People Through Physical Activity and Sports A Report to the
President From the Secretary of Health and Human Services and the
Secretary of Education. [Rockville, MD]: U.S. Department of Health and
Human Services, Public Health Service, Office of the Secretary of Health
and Human Services.
U.S. Department of Health and Human Services. (2001). The Surgeon General's
call to action to prevent and decrease overweight and obesity. Rockville,
MD: U.S. Department of Health and Human Services, Public Health Service,
Office of the Surgeon General.
Underwood, F., Laughlin, M. & Sturek, M. (1994). Altered control of calcium in
coronary smooth muscle cells by exercise training. Medicine and Science in
Sports and Exercise, 26, 1230-8.
Uusitupa, M., Siitonen, O., Pyörälä, K., Aro, A., Hersio, K., Penttilä, I., &
Voutilainen, E. (1995). The relationship of cardiovascular risk factors to the
prevalence of coronary heart disease in newly diagnosed type 2 (non-insulin
dependent) diabetes. Diabetologia, 28, 653–659.
Wallace, J.P., McKenzie, T.L., & Nader, P.R. (1985). Observed vs. recalled
exercise behavior: a validation of a seven-day recall for boys 11 to 13 years
old. Research Quarterly in Exercise and Sport, 56, 161-165.
Wankel, L.M. (1984). Decision-making and social support strategies for
increasing exercise involvement. Journal of Cardiac Rehabilitation. 4, 124-
135.
Washburn, R., Jacobsen, D., Sonko, B., Hill, J., & Donnelly, J. (2003). The
99
validity of the Stanford seven-day physical activity recall in young adults.
Medicine and Science in Sports and Exercise, 35, 1374-1380.
Whittemore, A.S., Wu-Williams, A.H., Lee, M., Shu, Z., Gallagher, R.P., Dengao,
J., et al. (1990). Diet, physical activity, and colorectal cancer among
Chinese in North America and China. Journal of the Cancer Institute, 82,
915–926.
Williamson, D.F., Madans, J., Anda, R.F., Kleinman, J.C., Kahn, H.S., & Byers,
T. (1993). Recreational physical activity and ten-year weight change in a US
national cohort. International Journal of Obesity Related Metabolic
Disorders, 17, 279–286.
Yngve, A., Nilsson, Sjostrom, M., & Ekelund, U. (2003). Effect of monitor
placement and of activity setting on the MTI accelerometer output. Medicine
and Science in Sports and Exercise, 35, 320-326.
Zakarian, J.M., Hovell, M.F., Hofstetter, C.R., Sallis, J.F., & Keating, K.J. (1994).
Correlates of vigorous exercise in a predominantly low SES and minority
high school population. Preventive Medicine, 23, 314-321.
Zimmet, P.Z. (1992). Kelly West Lecture 1991 challenges in diabetes
epidemiology—from West to the rest. Diabetes Care, 15, 232–252.
Zunft, H.F., Friebe, D., Seppelt, B., Winhalm, B., ReMaut de Winter, A.M., Vaz de
Almeida, M.D., et al. (1999). Perceived benefits and barriers to physical
activity in a nationally representative sample in the European Union. Public
Health Nutrition, 2, 153-160.
100
101

APPENDIX A
Medical History and Demographics Form
The University of Mississippi
246 Turner Center University, MS 38677
Abbreviated Medical History Questionnaire
Directions. Please answer the following questions to the best of your
102
knowledge. All information given is CONFIDENTIAL.
Name of Subject: ____________________________________
Age: ______ Date of Birth: _____________ Grade: _________
Sex: ______ male _______ female
Home Phone Number: ________________________
Are you currently playing on any school-sponsored sports teams?
___ Yes ___ No
Do you currently take part in the school lunch program? ___ Yes ___ No
Do you have any form of respiratory (breathing) ailments?
___ Yes ___ No
If yes, please check all that apply:
__Asthma ___Emphysema ___Bronchitis
___COPD ___Unusual fatigue ___Common cold
Other (list)______________________________________________________Do you have any form of metabolic disorder? ___ Yes ___ No
If yes, please check all that apply
___Diabetes ___hyperthyroidism ___hypothyroidism
Other (list) _______________________________________________________________________________________________________________________
103
________________________________________________________________
Have you had any previous injuries that prevent you from performing any physical activity? ___ Yes ___ No
If yes, please list:__________________________________________________________________________________________________________________________________________________________________________________
Have you had any previous surgeries that prevent you from performing any physical activity? ___ Yes ___ No
If yes, please list:__________________________________________________________________________________________________________________________________________________________________________________
Are you currently taking any medications or supplements? ___Yes ___No
If yes, please list:______________________________________________________________
________________________________________________________________
104
APPENDIX B
MTI Accelerometer
MTI Health Services Users Manual Actisoft Analysis Software 3.2
TECHNICAL INFORMATION
The MTI ActiGraph has a built-in single axis accelerometer designed to measure and record time varying accelerations ranging in magnitude from approximately 0.05 to 2 G's. The accelerometer is band limited with a frequency response from 0.25 to 2.5 hertz. These parameters have been carefully chosen to detect normal human motion and to reject motion from other sources. The acceleration signal is filtered by an analog bandpass filter and digitized by an 8-bit Analog to Digital Converter (A/D) at 10 samples per second. The A/D quantizes the magnitude of the
105
acceleration giving a linear response to accelerations within the passband. Each A/D value is summed over a user specified interval of time called an ‘cycle’.
The hardware in the ActiGraph includes an 8 bit microcontroller with on chip 8 bit A/D, 64K of nonvolatile RAM in the AM7164-2.2 and 256K in AM71256, a low power operational amplifier, an accelerometer built from a cantilevered rectangular piezoelectric bimorph plate and seismic mass, a charge amplifier, analog bandpass filters, and a voltage regulator. The circuitry is surrounded in a metal shield and packaged into a plastic enclosure measuring 2.0 x 1.6 x 0.6 inches. The ActiGraph weight is 1½ ounces. A 3V (2430) coin cell lithium battery supplies power. Battery life is in excess of 4000 hours. The case is transparent to infrared light. Communications with the ActiGraph is via coded infrared light using a Reader Interface Unit (RIU) connected to a PC serial port. Microsoft Windows compatible software is supplied with the RIU to support PC communications with the MTI ActiGraph.
Cycles can be from one second to several minutes. When using a one-minute cycles and collecting Activity data only, the MTI ActiGraph AM7164-2.2 can collect 22 consecutive days of data. At the end of each cycle, the summed value is stored in memory and the numerical integrator is reset. This process repeats until memory is filled at which point the ActiGraph stops collecting data for that session and waits for the data to be downloaded or to be reinitialized. The data collected by the ActiGraph is a series of numbers representing the level or intensity of movement for each cycle. The first number in the data series represents the activity measured for the first cycle, which starts at the user specified start time and date. The numbers that follow in the series represent activity over each cycle in chronological order.
For AM71256-T ActiGraph: The AM71256-T measures skin temperature in addition to Activity. The probe is located flush on the back of the ActiGraph and must be worn against bare skin. The probe is an epoxy coated NTC Thermistor, type MS. Its operating range is 0oC to 50oC, +/- 1oC @ 25oC. It Dissipation Constant is 1.4 mW/oC.
For AM71256-L ActiGraph: The AM71256-L measures ambient light in addition to Activity. The sensor, a planar silicon photodiode, is located inside the ActiGraph to the right of the notch. The operating range is from 0-3000 Lux with 12 Lux Resolution.
For further information contact: MTI Health Services
709 Anchors Street, NW Fort Walton Beach, Florida 32548 USA
Tel: (850)-244-7211 Fax: (850)-664-5349 www.mtiactigraph.com
106
APPENDIX C
Seven-day Physical Activity Recall
INSTRUCTIONS: the questions in this section ask about your physical activity
participation.
We are going to ask you questions about your physical activities from the past 7
days, but first we would like to know about your sleep habits.
107
1. On the average, how many hours did you sleep each night during the last
five weekday nights (Sunday – Thursday)?
_______ hours
2. On the average how many hours did you sleep each night last Friday and
Saturday nights?
_______ hours
We would now like to ask you about your physical activity during the past 7 days,
that is the last 5 weekdays, and last Saturday and Sunday. We are not going to
list light activities such as slow walking, light housework, or unstrenuous sports
such as bowling, archery, or softball. Please look at the provided list, which
shows some examples of what we consider moderate, hard, and very hard
activities. If you are not sure where one of your activities fits, please ask the
instructor.
3. Moderate activities. What activities did you do and how many total hours
did you spend during the last 5 weekdays doing these moderate activities
or others like them? Please add them to the nearest half hour.
_______ hours
4. Last Saturday and Sunday, how many hours did you spend on moderate
activities and what did you do? Please add them to the nearest half hour.
_______ hours
5. Hard activities. What activities did you do and how many total hours did
you spend during the last 5 weekdays doing these hard activities or others
like them? Please add them to the nearest half hour.
_______ hours
108
6. Last Saturday and Sunday, how many hours did you spend on hard
activities and what did you do? Please add them to the nearest half hour.
_______ hours
7. Very hard activities. What activities did you do and how many total hours
did you spend during the last 5 weekdays doing these very hard activities
or others like them? Please add them to the nearest half hour.
_______ hours
8. Last Saturday and Sunday, how many hours did you spend on very hard
activities and what did you do? Please add them to the nearest half hour.
_______ hours
9. Compared with your physical activity over the past 3 months, was last
week’s physical activity more, less, or about the same?
_____ a. More
_____ b. Less
_____ c. About the same
EXAMPLE OF ACTIVITES IN EACH CATEGORYModerate Activity
1. Raking the lawn
2. sweeping and mopping
3. mowing the lawn
109
4. cleaning windows
5. volleyball
6. ping pong
7. callisthenic exercises
8. brisk walking (3 miles per hour)
Hard Activity
1. heavy carpentry
2. construction work
3. scrubbing floors
4. dancing
5. tennis doubles
6. half court basketball
Very Hard Activity
1. digging or chopping with heavy tools
2. jogging or swimming
3. singles tennis
4. racquetball
5. soccer
6. full court basketball
110
APPENDIX D
SAHHP Questionnaire
INSTRUCTIONS: The questions in this section ask you about your feelings and
attitudes concerning exercise. Please read each question carefully and circle the
answer that best describes how you feel. There are no right or wrong answers.
1 2 3 4 5 6
111
Strongly Slightly Slightly Strongly disagree disagree disagree agree agree agree
1. I am confident that I can exercise consistently 1 2 3 4 5 6 three times per week for the next 6 months.
2. I am confident that I can exercise consistently 1 2 3 4 5 6five times per week for the next 6 months.
3. I am confident that I can make time for 1 2 3 4 5 6exercise no matter how busy my day.
4. I am confident that I can motivate myself to 1 2 3 4 5 6exercise no matter how tired I may feel.
5. I am confident that I can motivate myself to 1 2 3 4 5 6exercise no matter how stressed I feel.
6. I am confident that I can motivate myself to 1 2 3 4 5 6exercise even when Id rather be doing something else.
7. I am confident that I can motivate myself to 1 2 3 4 5 6exercise if my friends criticize me for it.
8. I am confident that I can motivate myself 1 2 3 4 5 6to exercise even when I am feeling down.
112

APPENDIX E
Campbell Questionnaire
INSTRUCTIONS: The questions in this section ask you about barriers to physical
activity. Please read each question carefully and circle the answer that best
describes how you feel.
How important are each of the following in preventing you from being more
113
physically active?
not at all important Very important
Lack of time due to school or work 1 2 3 4 5
Lack of time due to family obligations 1 2 3 4 5
Lack of time due to other interests 1 2 3 4 5
Lack of energy, too tired 1 2 3 4 5
Lack of athletic ability 1 2 3 4 5
Lack of programs, leaders or accessible facilities 1 2 3 4 5
Lack of a partner 1 2 3 4 5
Lack of support from family or friends 1 2 3 4 5
Lack of babysitting services 1 2 3 4 5
Cost 1 2 3 4 5
Lack of self-discipline or willpower 1 2 3 4 5
Self-consciousness, ill at ease 1 2 3 4 5
Long-term illness, disability or injury 1 2 3 4 5
Fear of injury 1 2 3 4 5
Thank you for your participation
114
APPENDIX F
IRB Application
115
APPLICATION PACKET FOR
RESEARCH WITH HUMAN SUBJECTS
This packet includes all forms and instructions needed for an IRB application for research with human subjects. Please indicate on the checklist below which items are included (or explain why they are not necessary for your study). The review process will not be initiated until the complete application is on file with the IRB, and research may not begin until approval has been granted.
Please submit the original and one copy of this form tothe Office of Research and Sponsored Programs at the above
address.Faxes are not acceptable.
CHECKLIST Completed CHECKLIST and application (with appropriate
signatures) Copies of all instruments/questionnaires Informed Consent form(s) – modeled after standard form on the
IRB website Recruitment notices/announcements Debriefing statement and summary of procedure If conducting research off-campus, approval letter from other
IRB(s) or Single Project Assurance(s) signed by the appropriate parties
THE UNIVERSITY OF MISSISSIPPI Institutional Review Board for the Protection of
Human Subjects
125 Old ChemistryP. O. Box 907
University, MS 38677662-915-7482 662-915-7577 (fax)
www.olemiss.edu/depts/research/irb
OFFICE USE ONLY:
Date Received Protocol No.
Investigator(s)
Title ______________________________________________________________________________
116
Application to Conduct Research with Human Subjects 1. Title of Project: Determinants of Physical Activity in Rural African-American Adolescents______ If Student Project: Dissertation Thesis Class Project Other
2. Principal Investigator: Mike Bamman Department Health, Exercise Science, and Recreation Management Work Phone 662-363-4019 Mailing Address 1241 Pendulum Drive __________________ Home Phone 662-429-3514
___Hernando________________MS__________38632__________ City State Zip Code
E-Mail Address [email protected] ___ Fax Number 662-363-4059
Co-Investigator(s): ___ _______
3. Research Advisor (for student researchers): Jeffrey S. Hallam, PhD
Department __Health, Exercise Science and Recreation Management Work Phone 662-915-5140 E-Mail Address [email protected] Fax Number 662-915-5525 4. Funding Source (if grant or contract):
5. Anticipated Beginning and Ending Dates Beginning Date (mm/dd/yy) 02/01 /04
of Human Subjects Contact: Ending Date (mm/dd/yy) 03/15/ 04
6. Subject Characteristics: Number _80_ Age Range 12-18 (If under 18, parental consent required)
7. Briefly describe subject population:Participants for this study will be recruited in Tunica County MS, at Rosa Fort High School.
Permission has been obtained from the Tunica County School Assistant Superintendent, Fernando Bearden
117
and from Rosa Fort High School Principal, Larry Ball, and will be obtained from each student and from his or her parents/guardians, to assess all county students ages 12-18.
8. Special Risk Subjects Involved: (Check all applicable groups) Pregnant Females Prisoners Elderly Fetal Tissue/Fetuses Mentally Ill Cognitively Impaired HIV+ Children/Adolescents Other Use of blood, other bodily fluids, or tissues (IBC approval needed. See Instructions.)
9. Recruitment Procedures:
a. How will subjects be recruited? Copy of the recruitment notice/announcement attached?
Subjects will be recruited for this study via permission that has been obtained from the Tunica County School Board, and the principal of Rosa Fort High School. Permission has been given to the researcher to utilize children enrolled in Physical Education classes at Rosa Fort High School. All students enrolled in Physical Education classes will be given the consent forms and information about the study. Students that decline to be included in the study will continue to take part in normal class activities, while students in the study will be excused from class work during study times.
b. Describe compensation or incentives for subjects, if any.
On the fifth day of their participation in the study, the investigator will meet with the subjects during their school day, and present each with a water bottle (donated by the Tunica County Recreation Commission) as an incentive to continue with the study protocol. Upon completion of the study, when the data shows full adherence to the study protocol by the participant, the investigator will provide the subjects with t-shirts donated by the Tunica County Recreation Commission.
10. Consent Procedures Information letter (attached)
Informed Consent form (attached)
An information packet will be distributed to all eligible students to take to their parents. The packet will include a cover letter, an informational page concerning the study design, technical information concerning the MTI accelerometer and the parental informed consent.
The informational packet is attached, which includes:1. Cover letter2. Study information page3. MTI Technical information page
There are 3 informed consent forms attached.1. Parental/guardian consent for participation by a child2. Child ages 12-13 oral assent script3. Child ages 14-18 written assent
11.Where will the study be conducted?
This study will take place in Tunica County Mississippi. Permission to utilize existing classroom space at Rosa Fort High School has been obtained.
Approval letter from another IRB attached
118
Single Project Assurance from cooperating organization attached
One Single Project Assurance forms is attached.1. Rosa Fort High School
If survey research, will surveys be mailed or distributed in another way? Give details.
Surveys consisting of Medical history questionnaire, Seven-day physical Activity Recall, modified Stanford Adolescent Heart Health Program Questionnaire, and modified Campbell’s Questionnaire will be administered to students in a classroom setting at Rosa Fort High School. Each student will have access to the investigator and a technician in order to answer any questions or provide any guidance required to complete the surveys.
1. Copies of each questionnaire are attached.
The MTI has been shown to be a valid measure of PA in adolescents (.71) against energy expenditure measured by indirect calorimetery (Freedson, Melanson, & Sirand, 1998). Ekelund (2001) and colleagues found activity counts from the MTI to contribute significantly to the explained variation in total energy expenditure (R2 = 0.54) and was found, in combination with sex, to be the best (compared with VO2 and anthropometric data) predictor of activity energy expenditure (R2 = 0.45) in a sample of 9 year old children. Data taken as part of the Amherst Health and Activity Study (Trost, Pate, Freedson, Sallis & Taylor, 2000) show that the optimal duration for PA monitoring with the MTI is 7 days. Researchers found that a 7-day protocol in school-age children (grades 1-12) resulted in acceptable estimation of moderate to vigorous PA (R2 = 0.76 – 0.87).The physical activity recall has been validated in comparisons with objective fitness measures such as VO2max and percent body fat (..33-.50) (Blair et al., 1985) direct observation (.64) (Wallace, McKenzie & Nader, 1985) as well as with activity monitors (.40) (.77-.82)(Rauh, Hovell, Sallis & Hofstetter, 1992; Matthews & Freedson, 1995). Sallis, Buono, Roby, Micale, & Nelson, (1993) report a test-retest reliability of the PAR of (.81) in a large sample of elementary and secondary schoolchildren. Very hard PA is shows good reliability (.53) when correlated with direct heart rate measurements above 160 beats per minute.
Self-efficacy will be assessed through the questionnaire utilized in the Stanford Adolescent Heart Health Program (SAHHP) (Reynolds et al, 1990). After controlling for baseline levels of physical activity and BMI, associations were found between physical activity levels and self-efficacy ((-.46) – (-.51)). Cronbach’s alpha generated for the self-efficacy scale in this study was 0.89.
Subject’s perceived barriers to exercise will be assessed with a subset of Campbell’s Study of Well Being (Stephens & Craig, 1990). This measure has been shown to be reliable in an adolescent population (.60-.79) (Allison, Dwyer, & Makin, 1999).
12.What are the possible risks (physical, psychological, social, work-related, financial, etc.) that might be experienced by the subject?
MTI health services lists no physical risks from the MTI accelerometer. However, misuse, disassembly, or destruction of the MTI accelerometer may pose physical risks such as bruises, cuts and abrasions. There will be no financial risks assumed by the subjects in this study. Psychological and social risks in this study may be a result of subjects’:
o ‘Competing’ with other subjects to accumulate as much or as little physical activity as possible.
o Disappointment when the results of their MTI physical activity log are discussed when the study is completed.
119
o Disappointment and/or teasing by other adolescents or subjects if MTI accelerometer malfunctions, is worn improperly, is damaged or is lost.
Specify the precautions that will be taken to minimize any risks.
Subjects will be informed as a group and individually that they are to maintain a normal physical activity schedule, and that their results are not a comparison to other subjects in the study. Subjects will be informed both as a group and individually of the proper care and use of the MTI accelerometer and given contact information in case of malfunction, loss, or damage to the MTI accelerometer.
13.What are the potential benefits, if any, to the subject? [Potential benefits do not include incentives offered for participation.] Explain:
Subjects will be eligible receive information regarding their Body Mass Index, their activity level, their physical activity self-efficacy, and their perceived barriers to exercise.
14.What are the penalties, if any, the subject can experience from participation in the study?
There are no penalties associated with this study.
15.How will you maintain subject confidentiality?
Include a statement regarding where data will be kept, who will have access to it, how you will ensure confidentiality, and what will be done with the data when the study is finished.
NOTE: Federal law requires de-linking identifying information from the data as soon as identifiers are no longer needed for analysis.
Original hard copies of the completed Medical History Questionnaire, completed consent/assent forms, completed questionnaires, MTI ActiGraph printouts will be kept in a locked file cabinet in Mr. Bamman’s office at the G.W. Henderson Health and Wellness Pavilion (1165 Abbay Drive, Tunica, MS). Electronic data generated by the MTI ActiGraph, Excel spreadsheets, and SPSS data analysis files will be downloaded to removable disks and stored in the locked file cabinet in Mr. Bamman’s. Only Mr. Bamman and Dr. Hallam will have access to the locked file cabinet in his office. Confidentiality will be maintained by assigning a random 4-digit number for each subject. No identifiers such as name or social security number will be used. In addition, confidentiality will be maintained by de-linking the identifying information from the files as soon as identifiers are no longer needed for analysis. Data, but no identifiers will be shared with Dr. Hallam. Original hard copy data will be kept on file for a period of one year and then shredded. De-linked electronic data will be kept indefinitely.
16. Please attach a Project Description. Include a ٱ problem statement , ٱ brief literature review citing evidence for need of research, ٱ research design, ٱ data
120
collection method, ٱ data analysis methods, and ٱ debriefing procedure and statement (if applicable).
A project Description is attached to the document. Included with the project description is a copy of the adherence flyer that will be handed out to the subjects.
INVESTIGATOR ASSURANCE
Please read and sign below. Obtain signatures of your research advisor and co-investigators, if applicable, and of your department chair. Return this original and one copy, along with any attachments, to the Office of Research and Sponsored Programs. Please allow up to four weeks for a response from the Office of Research and Sponsored Programs and/or the IRB. You will be contacted for any modifications and/or clarifications needed, and once approval is granted, you will be notified in writing. Approvals under the Expedited and Full Review categories are subject to continuing review by the IRB.
I understand that no research activities should be conducted with human participants prior to obtaining the required approvals from the IRB. I will inform the IRB at the earliest possible date of (1) any significant changes in the project with respect to human subject participation, (2) any adverse reactions or unexpected responses observed involving human subjects, and
121
(3) any need for continuation of the project activities beyond the approval date.
Failure to comply with Federal Regulations (45 CFR 46) can result in confiscation and possible destruction of data, suspension of all current and future research involving human subjects, or other institutional sanctions, until compliance is assured.
__________________________ ________ _______________________________ _________Principal Investigator Date Research Advisor (if student project) Date
__________________________ _______ ________________________________ _________Co-Investigator Date Department Chair Date
OFFICE USE ONLY:
Administrative Review
Office of Research Representative Date
Expedited Review* Full Review*
IRB Chair Date
Dear Parents:
My name is Mike Bamman. I am the manager of the fitness center here in Tunica. I am also a student at the University of Mississippi. I am doing a study in Tunica County looking at exercise and county teen-agers.
The Principal at Rosa Fort High School, Mr. Ball has approved the study. The University of Mississippi’s Institutional Review Board has also approved the study. Your child can be in this study if your child wants to. Your child will not be punished in any way if your child does not want to be included in the study.
122
There is a consent form for you to sign in this packet. Your child can start the study after you sign this form and it is returned to the school. After we get the form, we will ask your child if he/she wants to be in the study.
Also in this packet is information about the study and about the piece of equipment that your child will be using. I ask that you please read the packet before signing the form.
After the study is over you will have a chance to see you child’s results if you wish. Just get in touch with me and we will get together to discuss them. Please contact me if you have any questions about anything in this packet.
Sincerely,
Mike Bamman
662-363-4019 office 662-363-4059 fax 901-277-8014 cell [email protected]
Study Information
This study will help us learn about the amount of exercise teen-agers get in Tunica County. We feel that learning more about this can help us offer better programs for your children.
After you say its okay and your child says its okay, your child will be in the study. We will only work with your child during their PE class at school. The first time will take about 30 minutes and the second time will take no more than 5 minutes.
123

If your child is in the study, he or she will be asked to fill out a survey. The survey will be about how your child feels about exercise. They will also be asked to wear a small device that measures how much exercise they do. Your child will be asked to wear this device for seven days in a row.
On the first visit we will measure your child’s height and weight. We will then ask them to fill out the survey. We will then tell your child about the exercise device. We will also describe the study. We will also give them written directions about the exercise device. Each child will be given directions on how to use the device and take care of the device. This device measures exercise by measuring the movements that your child makes. To help you we have put more information about this device in the packet.
The device will be attached to your child’s hip with an elastic belt. Each child will then get instructions on how to wear the device. We will give each child a small notebook. We will ask them to write down the times when they take it off each day. Each child will be given a flyer to hang up in a place that they see all the time (like the refrigerator or the door to go outside) to remind it to wear the device.
On the fourth day, Mr. Bamman will call each student to remind them to wear the device. On the fifth day, Mr. Bamman will visit the school and hand out water bottles to the children that are wearing the device.
On the second visit, each child will turn in their device and their notebook. If your child has worn the device every day, they will receive a free t-shirt.
If you have any questions about the study or the device, please contact Mr. Bamman.
MTI Health Services Users Manual Actisoft Analysis Software 3.2
TECHNICAL INFORMATION
The MTI ActiGraph has a built-in single axis accelerometer designed to measure and record time varying accelerations ranging in magnitude from approximately 0.05 to 2 G's. The accelerometer is band limited with a frequency response from 0.25 to 2.5 hertz. These parameters have been carefully chosen to detect normal human motion and to reject motion from other sources. The acceleration signal is filtered by an analog bandpass filter and digitized by an 8-bit Analog to Digital Converter (A/D) at 10 samples per second. The A/D quantizes the magnitude of the
124
acceleration giving a linear response to accelerations within the passband. Each A/D value is summed over a user specified interval of time called an ‘cycle’.
The hardware in the ActiGraph includes an 8 bit microcontroller with on chip 8 bit A/D, 64K of nonvolatile RAM in the AM7164-2.2 and 256K in AM71256, a low power operational amplifier, an accelerometer built from a cantilevered rectangular piezoelectric bimorph plate and seismic mass, a charge amplifier, analog bandpass filters, and a voltage regulator. The circuitry is surrounded in a metal shield and packaged into a plastic enclosure measuring 2.0 x 1.6 x 0.6 inches. The ActiGraph weight is 1½ ounces. A 3V (2430) coin cell lithium battery supplies power. Battery life is in excess of 4000 hours. The case is transparent to infrared light. Communications with the ActiGraph is via coded infrared light using a Reader Interface Unit (RIU) connected to a PC serial port. Microsoft Windows compatible software is supplied with the RIU to support PC communications with the MTI ActiGraph.
Cycles can be from one second to several minutes. When using a one-minute cycles and collecting Activity data only, the MTI ActiGraph AM7164-2.2 can collect 22 consecutive days of data. At the end of each cycle, the summed value is stored in memory and the numerical integrator is reset. This process repeats until memory is filled at which point the ActiGraph stops collecting data for that session and waits for the data to be downloaded or to be reinitialized. The data collected by the ActiGraph is a series of numbers representing the level or intensity of movement for each cycle. The first number in the data series represents the activity measured for the first cycle, which starts at the user specified start time and date. The numbers that follow in the series represent activity over each cycle in chronological order.
For AM71256-T ActiGraph: The AM71256-T measures skin temperature in addition to Activity. The probe is located flush on the back of the ActiGraph and must be worn against bare skin. The probe is an epoxy coated NTC Thermistor, type MS. Its operating range is 0oC to 50oC, +/- 1oC @ 25oC. It Dissipation Constant is 1.4 mW/oC. For AM71256-L ActiGraph: The AM71256-L measures ambient light in addition to Activity. The sensor, a planar silicon photodiode, is located inside the ActiGraph to the right of the notch. The operating range is from 0-3000 Lux with 12 Lux Resolution. For further information contact:
The University of Mississippi246 Turner CenterUniversity, MS 38677
125
Parental/Guardian Consent for Child to Participate in an Experimental Study
Title of Investigation: Determinants of physical activity in rural African-American adolescents
Principal Investigator: Mike BammanDepartment of HESRMUniversity of MississippiUniversity, MS 38677
Description:
This study will help us learn more about physical activity of teen-agers in Tunica County. If your child takes part in this study he or she will be asked to complete a short survey. The survey will measure how they feel about exercise. Your child will also be asked to wear a small exercise device that measures exercise. The device is the size of a watch.
We ask that you complete this consent form about your child. After you return the consent form, we will ask your child if he or she wants to be in the study. We will give your child all the details of the study before we ask his or her permission.
Then we will work with your child on two different times during their PE class. The first time will take about 30 minutes and the second time will be about 5 minutes.
On the first visit we will measure your child’s height and weight. We will then ask your child to fill out the survey. We will also give your child directions about the device. We will also tell them about the study. Each child will be given directions on the use and care of the activity device. We will then place the device around their hips with an elastic belt. Each child will then receive directions about how to wear and care for the device. We will then give your child a small notebook. We will ask them to write down when they take off the device each day. Each child will then be given a flyer to post in a highly visible place at home to remind them to wear the device.
On the fourth day, Mr. Bamman will call your child to remind him or her to wear the device. On the fifth day of the study, Mr. Bamman will visit the school and hand out water bottles to the children that are wearing the device.
126
On the second visit, each child will turn in his or her device and logbook. If your child has worn the device every day, they will receive a free t-shirt.
Risks and Benefits:
The risks to your child of taking part in this study are minimal. The use of the physical activity device is a safe method of measuring physical activity.
The benefits to your child for taking part in this study include gaining information about his or her physical activity level. After we get the data you and your child will have a chance to discuss the results with Mr. Bamman.
Costs and Payments:
Participation in this project will incur no cost to you or your child. As a benefit to your child for participation, they may receive a water bottle and a t-shirt.
Confidentiality/Privacy:
Any information obtained about your child from this research, including any medical history or findings on physical measures will be kept confidential. If the study results are published in a science journal, the data will be presented so that no one can identify your child.
Protected Health Information: Protected health information is any personal health information through which you can be identified. The data collected in this study includes: medical history, body mass index, and physical activity level. A decision to participate in this research means that you agree to the use of your health information for the study described in this form. This information will not be released beyond the purposes of conducting this study. The information collected for this study will be kept indefinitely. While this study is ongoing you may not have access to the research information, but you may request it after the research is completed.
Right to Withdraw:
You or your child are free to refuse to take part in this study or to withdraw from this study at any time by simply informing Mr. Bamman in person, by letter (1165 Abbay Drive, Tunica, MS 38676) or by telephone (363-4019). If you decide to withdraw your child from the study, you will not upset us. Whether or not you and your child choose to participate will not affect your standing with the Department of Health, Exercise Science and Recreation Management, with the University, or with the Tunica County Recreation Commission, and it will not cause you or your child to lose any benefits to which you are entitled.
Compensation for Illness or Injury:
127
"I understand that I am not waiving any legal rights or releasing the institution or their agents from liability for negligence. I understand that in the event of physical injury resulting from a research procedure, the University of Mississippi does not have the funds budgeted for compensation either for lost wages or medical treatment or reimbursement for such injuries. The University will help, however, obtain any medical attention which my child may require while involved in the study by securing transportation to the nearest medical facility."
IRB Approval:
The University of Mississippi’s Institutional Review Board (IRB) has reviewed this study. The IRB has determined that this study meets the ethical obligations required by federal and university standards. If you have any questions, concerns or reports regarding this study, please contact the IRB at 915-7482.
Statement of Consent:
I have read the above information. I have been given a copy of this form. I have had an opportunity to ask questions, and I have received answers. I consent to have my child participate in the study.
Please Print Child’s Name
_________________________________________ Date: ________________Signature of Parent/Guardian
__________________________________________ Date: ________________Signature of Investigator
128
The University of Mississippi 246 Turner Center University, MS 38677
Oral Assent Script for Child (ages under 14) to Participate in an Experimental
Study
Title of Investigation: Determinants of physical activity in rural African-American adolescents
Principal Investigator: Mike BammanDepartment of HESRMUniversity of MississippiUniversity, MS 38677
Script to be read to child by experimenter:
Description:
“This study is going to help us find out more about how physically active a person is. If you decide to take part in this study, we will meet with you two times. Each time will be during your PE class.
On the first visit, after we collect the forms signed by your parents, we will tell everything about the study. Then we will check your height and your weight. We will ask you to complete a short survey for us at this time. This survey takes about 15 minutes to fill out. Then you will be given an activity device to wear for 7 days. We will show you how to wear it and we will tell you the proper use of the device. We will also give you a notebook to write down the times when you take the device off and put it back on every day.
On the final visit, we will take the activity device back and if it shows that you have worn if everyday, you will get a free t-shirt.”
129
Risks and Benefits:
“All the tests you will do in this study are safe and easy to do. They do not involve any pain or discomfort. For being in this study you will learn how many calories your body uses during a week. Costs and Payments:
“It will not cost you or your family anything to be in this study. By participating in this study you may receive a water bottle and a t-shirt if you wear the device every day.”
Confidentiality/Privacy:
“The only people who will ever see the results of your measurements will be you, your parents or guardian, and the people who record the measurements. “
Right to Withdraw:
“You do not have to be in this study if you do not want to be. And, once you start this study, you can stop before you finish if you want to. If you want to stop being in the study all you or your parent or guardian needs to do is tell Mr.Bamman. Whether or not you choose to participate will not affect your standing with the Department of Health, Exercise Science and Recreation Management, with the University of Mississippi or with the Tunica County Recreation Commission, and it will not cause you to lose any benefits to which you are entitled.”
IRB Approval:
“All the measurements we will make in this study are safe and have been reviewed and approved by doctors, professors, and other people associated with the university. The group of people who have reviewed and approved all the measurements are known as the University of Mississippi's Institutional Review Board (IRB). If you or your parents or guardians have any questions, concerns or reports regarding this study you can call the IRB at 915-7482.”
Voluntary Assent: “Do you have any questions? Do you want to be in this study?”
Child’s Response: Yes________ No ________
______________________________________ Date ______________
Print child’s name
130
______________________________________ Date _______________
Witness
The University of Mississippi 246 Turner Center University, MS 38677
Child (ages 14-18) Written Assent to Participate in an Experimental Study
Title of Investigation: Determinants of physical activity in rural African-American adolescents
Principal Investigator: Mike BammanDepartment of HESRMUniversity of MississippiUniversity, MS 38677
Description:
This study is going to help us find out more about how physically active a person is. If you decide to take part in this study, we will meet with you two times. Each time will be during your PE class.
On the first visit, after we collect the forms signed by your parents, we will tell everything about the study. Then we will check your height and your weight. We will ask you to complete a short survey for us at this time. This survey takes about 15 minutes to fill out. Then you will be given an activity device to wear for 7 days. We will show you how to wear it and we will tell you the proper use of the device. We will also give you a notebook to write down the times when you take the device off and put it back on every day.
131
On the final visit, we will take the activity device back and if it shows that you have worn it everyday, you will get a free t-shirt.
Risks and Benefits:
All the tests you will do in this study have been reviewed and approved and are safe and easy to do. For being in this study you will learn how many calories your body uses during a week.
Costs and Payments:
It will not cost you or your family anything to be in this study. As part of this study, you may receive a water bottle or a t-shirt.
Right to Withdraw:
You do not have to be in this study if you do not want to be. And, once you start this study, you can stop before you finish if you want to. If you want to stop being in the study all you or your parent or guardian needs to do is tell Mr. Bamman in person, send him a letter (Tunica County Recreation, 1165 Abbay Drive, Tunica, MS 38632) or call Mr. Bamman (363-4019). Whether or not you choose to participate will not affect your standing with the Department of Health, Exercise Science and Recreation Management, with the University of Mississippi or with the Tunica County Recreation Commission, and it will not cause you to lose any benefits to which you are entitled.
IRB Approval:
All the measurements we will make in this study are safe and have been reviewed and approved by doctors, professors, and other people associated with the university. The group of people who have reviewed and approved all the measurements are known as the University of Mississippi's Institutional Review Board (IRB). If you or your parents or guardians have any questions, concerns or reports regarding this study you can call the IRB at 915-7482.
Statement of Assent:
I have read the above information. I have been given a copy of this form. I have had an opportunity to ask questions, and I have received answers. I assent to participate in the study.
Signature: _____________________________________ Date: ____________
132
Signature of Investigator: _________________________ Date: ____________
Assurance of Compliance with DHHS Regulations for
Protection of Human Research Subjects
Rosa Fort High School , hereinafter known as the "institution," hereby gives assurance that it will comply with the Department of Health and Human Services (DHHS) regulations for the protection of human research subjects (45 CFR 46) as specified below.
Part I
Ethical Principles and Institutional Policies Governing
Research Involving Human Subjects
I. Applicability
Except for research exempted or waived under the DHHS regulations 45 CFR 46.101, Part I of this Assurance applies to all research involving human subjects, and all other activities which even in part involve such research, regardless of whether the research is otherwise subject to federal regulation, if:
a. the research is sponsored by this institution, orb. the research is conducted by or under the direction of any employee or agent of this institution in
connection with institutional responsibilities, orc. the research is conducted by or under the direction of any employee or agent of this institution using
any property or facility of this institution, ord. the research involves the use of this institution's nonpublic information to identify or contact human
research subjects or prospective subjects.
II. Ethical Principles Governing Human Subjects Research
This institution is guided by the ethical principles regarding all research involving humans as subjects as set forth in the report of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research entitled, Ethical Principles and Guidelines for theProtection of Human Subjects of Research (the "Belmont Report") and as specified below.
A. This institution recognizes the principles of respect for persons, beneficence (including
133
minimization of harms and maximization of benefits), and justice as stated in the Belmont Report and will apply these principles in all research covered by this Assurance.
B. This institution acknowledges and accepts its responsibilities for protecting the rights and welfare of human research subjects.
III. Policies
A. This institution acknowledges that it and its investigators bear full responsibility for the performance of all research covered by this Assurance, including full responsibility for complying with federal, state, and local laws as they may relate to such research.
B. This institution assures that before human subjects are involved in research, proper consideration will be given to:
(1) the risks to the subjects,(2) the anticipated benefits to the subjects and others,(3) the importance of the knowledge that may reasonably be expected to result,(4) the informed consent process to be employed,(5) the provisions to protect the privacy of subjects, and(6) the additional safeguards for vulnerable populations.
C. This institution recognizes the need for appropriate additional safeguards in research involving subjects who are likely to be vulnerable to coercion or undue influence, such as children, prisoners, pregnant women, mentally disabled persons, or economically or educationally disadvantaged persons.
D. This institution encourages and promotes constructive communication among the institutional officials, research administrators, department heads, research investigators, clinical care staff, human subjects, and all other relevant parties as a means of maintaining a high level of awareness regarding the safeguarding of the rights and welfare of the subjects.
E.This institution will exercise appropriate administrative overview carried out at least annually to assure that its practices and procedures designed for the protection of the rights and welfare of human subjects are being effectively applied.
134
Part 2
IRB, Institution, and Investigator Compliance with 45 CFR 46
I. Applicability
Part 2 of this Assurance applies to the following research project which is conducted or sponsored by this institution in collaboration with The University of Mississippi.
Project title Determinants of Physical Activity in Rural African-American Adolescents
Project Investigator Mike Bamman
Research Advisor (if applicable) Jeffrey S. Hallam, PhD
II. Institutional Responsibilities
A. This institution has complied and will continue to comply with the requirements of 45 CFR 46 as specified below.
B. This institution has reviewed and sponsors the project referenced above, and is responsible for continuing review of this project in conjunction with the Institutional Review Board at The University of Mississippi.
III. IRB Review
A. The IRB at The University of Mississippi shall review, and have the authority to approve, require modification in, or disapprove this research activity or proposed changes in it before human subjects become involved.
B. The convened IRB reviewed and approved the above project.
C. The IRB determined, in accordance with the criteria found at 45 CFR 46.111, and where applicable, 45 CFR 46 Subparts B, C, and D, that protections for human research subjects are adequate.
D. The IRB has the authority to suspend or terminate approval of the above referenced research in accordance with 45 CFR 46.113 for (1) noncompliance with 45 CFR 46, and this Assurance document or the IRB's requirements, and (2) for elimination of unexpected serious harm to subjects.
135

E. The IRB has determined that legally effective informed consent [copy of document must be attached unless specified otherwise by the IRB Chair] will be obtained in a manner and method which meets the requirements of 45 CFR 46.116 and 46.117.
F. Continuing reviews by the IRB shall be conducted at intervals appropriate to the degree of risk, but not less than once per year (45 CFR 46.109[e]). The IRB may be called into an interim review session by the Chairperson at the request of any IRB member or Institutional Official to consider any matter concerned with the rights and welfare of any subject.
G.The IRB shall prepare and maintain adequate documentation of its activities with respect to this project in accordance with 45 CFR 4.115.
H.The IRB shall report promptly to institutional officials:
(1) any serious or continuing noncompliance by investigators with the requirements of the IRB,
(2) any suspension or termination of IRB approval,(3) any unanticipated problems or injuries involving risks to subjects or others, and(4) any changes in this research activity which are reviewed and approved by the IRB.
I. Where appropriate, the IRB will determine that adequate additional protections are ensured for fetuses, pregnant women, prisoners, and children as required under Subparts B, C, and D of 45 CFR 46.
J. The IRB will comply fully with the requirements of all applicable Federal policies and guidelines, including those concerning notification of sero-positivity, counseling, and confidentiality of subjects.
IV. Research Investigator Reporting Responsibilities
A.Investigators acknowledge and accept their responsibility for protecting the rights and welfare of human research subjects and for complying with all applicable provisions of this Assurance and 45 CFR 46.
B. Research investigators shall report promptly to the IRB proposed changes in this research activity and the changes shall not be initiated without IRB review and approval except where necessary to eliminate apparent immediate hazards to the subjects.
C. Research investigators shall report promptly to the IRB any unanticipated problems involving risks to subjects and others.
136
Part 3
Certification of IRB Approval and Institutional Endorsement
Project Title Determinants of Physical Activity in Rural African-American Adolescents
IRB Project number
Project Investigator/Research Advisor Mike Bamman Date of IRB approval Date of Next Scheduled IRB Review
The officials signing below assure that the project referenced above was approved by the IRB on the date indicated and that the project will be conducted in accordance with the requirements of Part 46, Title 45 of the Code of Federal Regulations and this Assurance document.
I. Authorized Official of the Institution Providing This Assurance
Signature Date
Name and Title: Larry Ball, Principal – Rosa Fort High School
Address: 1100 Rosa Fort Drive Tunica, MS 38676
Telephone: 662-363-1343 FAX: 662-357-4222
II. Authorized Official of the Institution with the IRB or IRB Chairperson
This institution authorizes the designation of its IRB for review of the project referenced in this Assurance.
Signature Date
Name and Title: Diane W. Lindley, Coordinator, Institutional Review BoardAddress: The University of Mississippi
Office of Research and Sponsored ProgramsP.O. Box 907University, MS 38677
Telephone: 662-915-7482FAX: 662-915-7577
137

III. Responsible Project Investigator or Director at Institution Providing this Assurance
I have attached copies of all IRB requested documents and approved Informed Consent Documents to be used in this project.
Signature Date
Name and Title: Mike Bamman, Project Investigator
Address: 1241 Pendulum Drive Hernando, MS 38632
Telephone: 662-363-4019 FAX: 662-363-4059
138

The University of Mississippi
246 Turner Center University, MS 38677
Abbreviated Medical History Questionnaire
Directions. Please answer the following questions to the best of your knowledge. All information given is CONFIDENTIAL. Name of Subject: ____________________________________
Age: ______ Date of Birth: _____________ Grade: _________
Sex: ______ male _______ female
Home Phone Number: ________________________
Are you currently playing on any school-sponsored sports teams?
___ Yes ___ No
Do you currently part of the school lunch program? ___ Yes ___ No
Do you have any form of respiratory (breathing) ailments?
___ Yes ___ No
139
If yes, please check all that apply:
__Asthma ___Emphysema ___Bronchitis
___COPD ___Unusual fatigue ___Common cold
Other (list)______________________________________________________
Do you have any form of metabolic disorder? ___ Yes ___ No
If yes, please check all that apply
___Diabetes ___hyperthyroidism ___hypothyroidism
Other (list) _______________________________________________________________________________________________________________________________________________________________________________________
Have you had any previous injuries that prevent you from performing any physical activity? ___ Yes ___ No
If yes, please list:__________________________________________________________________________________________________________________________________________________________________________________
Have you had any previous surgeries that prevent you from performing any physical activity? ___ Yes ___ No
If yes, please list:__________________________________________________________________________________________________________________________________________________________________________________
140
Are you currently taking any medications or supplements? ___Yes ___No
If yes, please list:______________________________________________________________
________________________________________________________________
INSTRUCTIONS: the questions in this section ask about your physical activity
participation.
We are going to ask you questions about your physical activities from the past 7
days, but first we would like to know about your sleep habits.
10.On the average, how many hours did you sleep each night during the last
five weekday nights (Sunday – Thursday)?
_______ hours
11.On the average how many hours did you sleep each night last Friday and
Saturday nights?
_______ hours
We would now like to ask you about your physical activity during the past 7 days,
that is the last 5 weekdays, and last Saturday and Sunday. We are not going to
list light activities such as slow walking, light housework, or unstrenuous sports
such as bowling, archery, or softball. Please look at the provided list, which
shows some examples of what we consider moderate, hard, and very hard
activities. If you are not sure where one of your activities fits, please ask the
instructor.
141
12.Moderate activities. What activities did you do and how many total hours
did you spend during the last 5 weekdays doing these moderate activities
or others like them? Please add them to the nearest half hour.
_______ hours
13.Last Saturday and Sunday, how many hours did you spend on moderate
activities and what did you do? Please add them to the nearest half hour.
_______ hours
14.Hard activities. What activities did you do and how many total hours did
you spend during the last 5 weekdays doing these hard activities or others
like them? Please add them to the nearest half hour.
_______ hours
15.Last Saturday and Sunday, how many hours did you spend on hard
activities and what did you do? Please add them to the nearest half hour.
_______ hours
16.Very hard activities. What activities did you do and how many total hours
did you spend during the last 5 weekdays doing these very hard activities
or others like them? Please add them to the nearest half hour.
_______ hours
17.Last Saturday and Sunday, how many hours did you spend on very hard
activities and what did you do? Please add them to the nearest half hour.
_______ hours
18.Compared with your physical activity over the past 3 months, was last
week’s physical activity more, less, or about the same?
_____ a. More
_____ b. Less
_____ c. About the same
142
EXAMPLE OF ACTIVITES IN EACH CATEGORY
Moderate Activity
9. Raking the lawn
10.sweeping and mopping
11.mowing the lawn
12.cleaning windows
13.volleyball
14.ping pong
15.callisthenic exercises
16.brisk walking (3 miles per
hour)
Hard Activity
1. heavy carpentry
2. construction work
3. scrubbing floors
4. dancing
5. tennis doubles
6. half court basketball
Very Hard Activity
7. digging or chopping with
heavy tools
8. jogging or swimming
9. singles tennis
10. racquetball
11.soccer
12. full court basketball
143
INSTRUCTIONS: The questions in this section ask you about your feelings and
attitudes concerning exercise. Please read each question carefully and circle the
answer that best describes how you feel. There are no right or wrong answers.
1 2 3 4 5 6
Strongly Slightly Slightly Strongly disagree disagree disagree agree agree agree
1. I am confident that I can exercise consistently 1 2 3 4 5 6 three times per week for the next 6 months.
2. I am confident that I can exercise consistently 1 2 3 4 5 6five times per week for the next 6 months.
3. I am confident that I can make time for 1 2 3 4 5 6exercise no matter how busy my day.
4. I am confident that I can motivate myself to 1 2 3 4 5 6exercise no matter how tired I may feel.
5. I am confident that I can motivate myself to 1 2 3 4 5 6exercise no matter how stressed I feel.
6. I am confident that I can motivate myself to 1 2 3 4 5 6exercise even when Id rather be doing something else.
7. I am confident that I can motivate myself to 1 2 3 4 5 6exercise if my friends criticize me for it.
8. I am confident that I can motivate myself 1 2 3 4 5 6to exercise even when I am feeling down.
INSTRUCTIONS: The questions in this section ask you about barriers to physical
activity. Please read each question carefully and circle the answer that best
describes how you feel.
How important are each of the following in preventing you from being more
physically active?
not at all important Very important
Lack of time due to school or work 1 2 3 4 5
Lack of time due to family obligations 1 2 3 4 5
Lack of time due to other interests 1 2 3 4 5
Lack of energy, too tired 1 2 3 4 5
Lack of athletic ability 1 2 3 4 5
Lack of programs, leaders or accessible facilities 1 2 3 4 5
Lack of a partner 1 2 3 4 5
Lack of support from family or friends 1 2 3 4 5
Lack of babysitting services 1 2 3 4 5
Cost 1 2 3 4 5
Lack of self-discipline or willpower 1 2 3 4 5
Self-consciousness, ill at ease 1 2 3 4 5
Long-term illness, disability or injury 1 2 3 4 5
Fear of injury 1 2 3 4 5
Thank you for your participation
Problem Statement
This study will allow researchers, school officials, community leaders, and
parents to better understand the possible determinants of, and barriers to
physical activity (PA) in African-American adolescents in Tunica County,
Mississippi. This research will also make a significant contribution to the existing
literature relating to determinants of PA in the African-American adolescent
population.
The purpose of this study is to identify the determinants of PA of African-
American adolescent schoolchildren ages 12-18 in Tunica County, Mississippi. A
secondary purpose of this study will be to determine the relationships among and
identify any differences between recognized determinants of PA (age, body mass
index, self-efficacy, and perceived barriers to exercise) of the students.
Brief Literature Review
There have been several significant determinants of PA identified in the
recent literature. The Stanford Adolescent Heart Health Study (Reynolds, et al,
1990) was the first population-based cohort study to examine psychosocial
predictors of PA in adolescents utilizing males and females of multiple ethnicities.
The authors established the importance of self-efficacy as a PA in adolescents.
Furthermore, self-efficacy has been shown to be a significant predictor of
vigorous PA in groups of lower SES and minority adolescents (Zakarian, Hovell,
Hofstetter, Sallis, & Keating, 1994), and in rural 5th grade children (Trost, et al,
1997), even when controlled for age and sex.
Specific barriers to PA in a high school population were studied by Allison,
Dwyer, and Makin (August 1999). They discovered that subjects were most
concerned about barriers that resulted in a lack of time (time consumed by
schoolwork as well as other interests). To a lesser extent, the subjects identified
lack of energy and low motivation as other significant barriers to PA.
In 1993, Aaron et al., identified significant differences in PA levels across
sex, ethnicity and age while establishing a standardized, reliable self-report
questionnaire to track PA in children and adolescents. The authors showed that
males were significantly more active than females (22.5 hr/wk vs. 6.6 hr/wk),
across all intensity levels. Similar sex differences have been publicized since.
Notably, Garcia et al (1995), showed sex as a significant predictor of PA in a
multi-racial cohort study.
The significance of age has also shown to be noteworthy, whether
measured as vigorous PA (Allison, Dwyer, & Makin, May, 1999; Trost, et al,
2002), or through daily moderate physical activity (Trost, et al).
In both males and females, Aaron (1993) showed Caucasian subjects’
had a significantly higher PA level than African-Americans and Hispanics (15.2
hrs/wk vs. 11.9 hrs/wk). This difference supports previous reports by Gottlieb and
Chen (1985), who showed that Caucasian adolescents were more likely to
engage in PA than either African-American or Hispanic youth. The disparity in
ethnic differences in PA has been reported on several occasions by the United
States government (CDC, 1992 & CDC, 2001). This disparity is more significant
among girls, with Caucasian girls participating in regular moderate PA at a
remarkably higher rate (27.5%), compared with Latino girls (20.3%), and African-
American girls (17.4%). In addition, it has recently been publicized that the
minority children and adolescents are the fastest-growing group of obese youth
in the United States (NCHS, 2000).
The literature reviewed on PA determinants, shows no assessment of
rural African-American adolescents and sex, self-efficacy, barriers to PA, age,
and BMI. Identification of any determinants to PA, would allow researchers to
develop strategies to increase the levels of PA in minority populations, or to
adjust current policies in order to create “culturally appropriate” programs for
increasing PA in minority populations.
Research Design
This cohort study will be designed as a causal comparative study. The
research will test the hypotheses of no relationship between the continuous
criterion variable and multiple predictor variables in both male and female
adolescents. This research will identify the unique contribution of age, BMI,
perceived self-efficacy, and perceived barriers to exercise to both male and
female adolescent populations in Tunica County, Mississippi.
Data Collection Method
The initial session with the subject population will begin with a program
description and orientation. Subjects will be given informational handouts on the
study, and on the MTI accelerometer, and an IRB-approved informed parental

consent to participate in the study (Appendix G). Consent forms will include
contact e-mail address and phone numbers for parents/guardians with questions
or comments about the study.
The second session will begin with collection of completed parental
consent forms. Subject assent will then be obtained based upon the University of
Mississippi’s child/classroom IRB checklist and guide. Subjects 12-13 years of
age will give oral assent with the responses recorded by the technician
(Appendix H). Subjects age 14-17 years will give assent using the written assent
form (Appendix I). Subjects will then be given a detailed description and
demonstration of the study procedures and instrumentation. Subjects will then
complete medical history and demographic data form (Appendix I).
The subjects’ BMI will then be measured. Subjects will be weighed, with
weight being recorded to the nearest 0.10 lb. and converted to kilograms. Height
will be recorded in inches to the nearest 0.10-inch and converted to centimeters.
Subjects will be provided with written and oral instructions on the use and care of
the MTI. At this time, the MTI will be attached to the right hip with an elastic belt.
The MTI will be initialized according to manufacturer specifications and activated.
Subjects will then receive individual oral instruction relating to the proper
procedures for wearing the MTI. Written information will also be provided for the
subject and their parent/guardian relating to the use and care of the MTI. The
subject will be instructed to wear the MTI during waking hours except during
water activities or during bathing. Subjects will be given a log book in order to
record the times when the MTI is removed and attached each day, which will

allow for the calculation of sleep and active hours. Subjects will be instructed to
wear the MTI for 7 consecutive days and will be encouraged to contact the
investigator with any questions regarding the MTI. Subjects will also be given an
adherence flyer (Appendix J) to post at home in a conspicuous place for the
seven days of monitoring. Upon completion of the MTI procedures, the subjects
will complete all paper and pencil questionnaires. Each subject will be given the
PAR, the modified Campbell’s questionnaire and the SAHHP questionnaire.
Subjects will be given oral and written instructions concerning the proper
completion of the questionnaires, and encouraged to ask questions. Subjects will
complete the self-administered questionnaires at that time.
On the morning of the fourth day of their participation in the study, each
subject will receive a personal telephone communication from the investigator or
a technician as a reminder to wear the MTI accelerometer. On the fifth day of
their participation in the study, the investigator will meet with the subjects during
their school day, and present each with a water bottle (donated by the Tunica
County Recreation Commission) as an incentive to continue with the study
protocol.
The third assessment session will consist of MTI collection and analyses.
Subjects will then be given the opportunity to receive feedback concerning their
physical activity and questionnaire data. Any subjects that request feedback will
be instructed to make an appointment with the investigator at their convenience
within 30 days of the completion of their participation in the study. When analysis
of the MTI data is complete and shows full adherence to the study protocol by the
participant, the investigator will provide the subjects with t-shirts donated by the
Tunica County Recreation Commission.
Upon completion of the overall data analysis, an aggregate report will be
mailed to the school, with detailed explanations of the results.
Data Analysis Method
SPSS 11.0 statistical package will be used to analyze all data. Data
will be reported using means and standard errors. Initial analysis will include
correlation of the PAR and MTI data. The results of the PAR will be validated
against the results of the MTI. If the instruments do not correlate significantly,
then regression equations will be run using both instruments and results of both
will be reported. Correlation of the MTI and PAR data expressed in kcals and
METs will also be conducted in order to determine any artificial relationship
between kcals measured by the MTI, which contain a component of BMI
measurement, and the independent variable, BMI.
Backward stepwise multiple regression will then be performed to
determine the factors that predict both male and female African-American
adolescents’ PA levels. The dependent variable physical activity, expressed as
kcals per week from PAR, for each sex will be regressed on the independent
variables of perceived self-efficacy, perceived barriers to exercise, age, and BMI.
To test whether the regression equation for males and the regression equation
for females are the same, the Chow test (Chow, 1960; Chinaburapa, Larson,
Bootman, McGhan & Nicholson, 1987; Kohli, 1989) will be performed with the
two equations.
REFERENCES
For IRB Application
Aaron, D.J., Kriska, A.M., Dearwater, S.R., Anderson, R.L., Olsen, T.L., Cauley,
J.A., et al. (1993). The epidemiology of leisure physical activity in an
adolescent population. Medicine and Science in Sports and Exercise. 25, 7,
847-53.
Allison, K.R., Dwyer, J.J., & Makin, S. (1999). Perceived barriers to physical
activity among high school students. Preventive Medicine. 28, 6, 608-15.
Allison, K.R., Dwyer, J.J., & Makin, S. (1999). Self-efficacy and participation in
vigorous physical activity by high school students. Health Education
Behavior. 26, 1, 12-24.
Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance
System Survey Data. Atlanta, Georgia: U.S. Department of Health and
Human Services, Centers for Disease Control and Prevention, 1996.
Centers for Disease Control and Prevention. Increasing physical activity: a report
on recommendations of the Task Force on Community Preventive Services.
MMWR 2001; 50(No. RR-18).
Chinburapa, V., Larson, L.N., Bootman, J.L., McGhan, W. & Nicholoson, G.
(1987). Prescribing intention and the relative importance of drug attributes: a
comparative study of HMO and fee-for-service physicians. Journal of
Pharmaceutical Marketing and Management, 2, 89-105.
Chow, G.C. (1960). Tests of equality between sets of coefficients in two linear
regressions. Econometrica, 28, 291-605.
Garcia, A.W., Broda, M.A., Frenn, M., Coviak, C., Pender, N.J., & Ronis, D.L.
(1995). Gender and developmental differences in exercise beliefs among
youth and prediction of their exercise behavior. Journal of School Health.
65, 6, 213-9.
Gottlieb, N.H. & Chen, M.S. (1985). Sociocultrual correlates of childhood sporting
activities: their implications for heart health. Soc. Sci. and Med, 21, 533-539.
Kohli, A. (1989). Determinants of influence in organizational buying: a
contingency approach. Journal of Marketing, 53, 50-65.
National Center for Health Statistics, Centers for Disease Control and
Prevention, Health E-Stats, 2001. (2000). Prevalence of Overweight Among
Children and Adolescents: United States, 2000.
Reynolds, K., Killne, H., Bryson, S., Maron, D., Taylor, C, Maccoby, N., et al.
(1990). Psychosocial predictors of physical activity in adolescents.
Preventive Medicine, 19, 541-51.
Trost, S.G., Pate, R.R., Sallis, J.F., Freedson, P.S., Taylor, W.C., Dowda, M., et
al. (2002). Age and gender differences in objectively measured physical
activity in youth. Medicine and Science in Sports and Exercise. 34, 2, 350-5.
Trost, S.G., Pate, R.R., Saunders, R., Ward, D.S., Dowda, M., & Felton, G.
(1997). A prospective study of the determinants of physical activity in rural
fifth-grade children. Preventive Medicine. 26, 257-63.
Zakarian, J.M., Hovell, M.F., Hofstetter, C.R., Sallis, J.F., & Keating, K.J. (1994).
Correlates of vigorous exercise in a predominantly low SES and minority
high school population. Preventive Medicine, 23, 314-321.
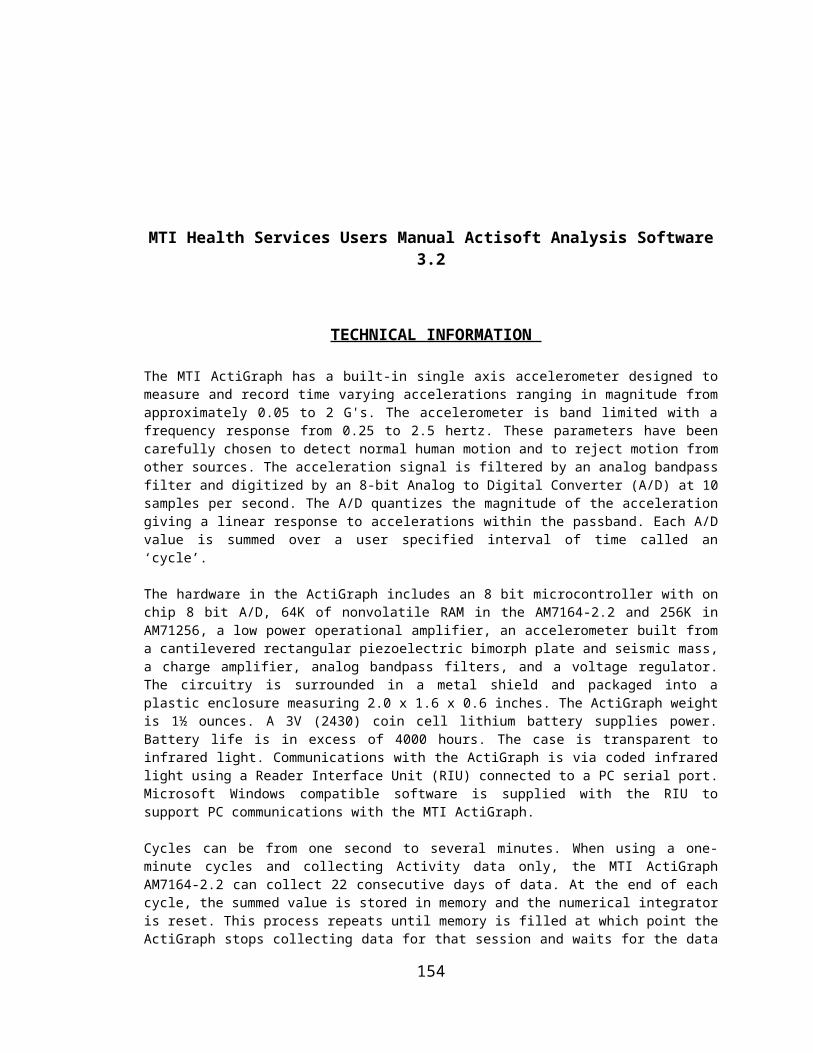
APPENDIX G
Parental Consent Form

The University of Mississippi
246 Turner CenterUniversity, MS 38677
Parental/Guardian Consent for Child to Participate in an Experimental Study
Title of Investigation: Determinants of physical activity in rural African-American adolescents
Principal Investigator: Mike BammanDepartment of HESRMUniversity of MississippiUniversity, MS 38677
Description:
This study will help us learn which, of several factors significantly determines the amount of physical activity children in Tunica County, Mississippi accumulate in a one week time period. If your child takes part in this study he or she will be required to complete a short questionnaire concerning their attitudes toward exercise, their recent exercise history, and their perceived barriers to physical activity. He or she will also be required to wear the MTI accelerometer for 7 consecutive days. You will be asked to complete this consent form about your child. Upon return of this parental consent form, each child must then give its verbal or written assent to participate in the study.
Subjects ages 7-13 years of age will give oral assent with the responses recorded by a qualified technician. Subjects age 14-17 years will give assent using a separate written assent form. Subjects will then be given a detailed description and demonstration of the study procedures and instrumentation.
The initial assessment will include BMI measurements, paper and pencil questionnaire and instrumentation instructions and procedures. Each child will be weighed, with weight being recorded to the nearest 0.10 lb. and converted to kilograms. Height will be recorded in inches to the nearest 0.10-inch and converted to centimeters. Each child will be provided with written and oral

instructions on the use and care of the MTI accelerometer. At this time, the MTI accelerometer will be attached to the right hip with an elastic belt. The MTI accelerometer will be initialized and activated. Each child will then receive individual oral instruction relating to the proper procedures for wearing the MTI accelerometer. Written information will also be provided for your child yourself relating to the use and care of the MTI accelerometer. Each child will be instructed to wear the MTI during waking hours except during water activities or during bathing. Each child will be given a log book in order to record the times when the MTI accelerometer is removed and attached each day, which will allow for the calculation of sleep and active hours. Each child will be instructed to wear the MTI accelerometer for 7 consecutive days and will be encouraged to contact Mr. Bamman with any questions regarding the MTI accelerometer. Each child will then be given a handout to post in a highly visible place at home to remind them to wear their accelerometer daily. Each child will then complete the paper and pencil questionnaire.
On the final sessions, each child will turn in their MTI accelerometer and logbook. If the data shows full cooperation with the study procedures, your child will receive a free t-shirt.
Risks and Benefits:
The risks to your child of taking part in this study are minimal. The use of the MTI accelerometer has been shown to a safe method of measuring physical activity.
The benefits to your child for taking part in this study include gaining information about his or her body mass index, physical activity level, physical activity self-efficacy and barriers to physical activity. After data collection is complete, you and your child will have a chance to discuss the results with Mr. Bamman.
Costs and Payments:
Participation in this project will incur no cost to you or your child.
Confidentiality/Privacy:
Any information obtained about your child from this research, including medical history or findings on physical measures will be kept confidential. If the study results are published in a science journal, the data will be presented so that no one can identify your child.
Protected Health Information: Protected health information is any personal health information through which you can be identified. The data collected in this study includes: medical history, body mass index, and physical activity level. A decision to participate in this research means that you agree to the use of your health information for the study described in this form. This information will not be released beyond the purposes of conducting this study. The information collected for this study will be kept indefinitely. While this study is ongoing you
may not have access to the research information, but you may request it after the research is completed.
Right to Withdraw:
You or your child are free to refuse to take part in this study or to withdraw from this study at any time by simply informing Mr. Bamman in person, by letter (1165 Abbay Drive, Tunica, MS 38676) or by telephone (363-4019). If you decide to withdraw your child from the study, you will not upset us. Whether or not you and your child choose to participate will not affect your standing with the Department of Health, Exercise Science and Recreation Management, with the University, or with the Tunica County Recreation Commission, and it will not cause you or your child to lose any benefits to which you are entitled.
Compensation for Illness or Injury:
"I understand that I am not waiving any legal rights or releasing the institution or their agents from liability for negligence. I understand that in the event of physical injury resulting from the research procedures, the University of Mississippi does not have the funds budgeted for compensation either for lost wages or medical treatment or reimbursement for such injuries. The University will help, however, obtain any medical attention which my child may require while involved in the study by securing transportation to the nearest medical facility."
IRB Approval:
The University of Mississippi’s Institutional Review Board (IRB) has reviewed this study. The IRB has determined that this study meets the ethical obligations required by federal and university standards. If you have any questions, concerns or reports regarding this study, please contact the IRB at 915-7482.
Statement of Consent:
I have read the above information. I have been given a copy of this form. I have had an opportunity to ask questions, and I have received answers. I consent to have my child participate in the study.
_________________________________________ Date: ________________Signature of Parent/Guardian
__________________________________________ Date: ________________
Signature of Investigator
APPENDIX H
Oral Assent Form

The University of Mississippi
246 Turner Center University, MS 38677
Oral Assent Script for Child (ages under 14) to Participate in an Experimental Study
Title of Investigation: Determinants of physical activity in rural African-American adolescents
Principal Investigator: Mike BammanDepartment of HESRMUniversity of MississippiUniversity, MS 38677
Script to be read to child by experimenter:
Description:
“This study will help us learn more about what helps determine how physically active a person is. If you decide to take part in this study you will fill out a questionnaire, and wear a small device, called an accelerometer, for 7 days.
On the first day, after we collect the consent forms signed by your parents, we will explain everything about the study to you. Then we will measure your height and your weight. You will then be given an accelerometer to wear for 7 days. We will show you how to wear it and we will tell you the proper use of the accelerometer. We will give you a logbook to write down the times when you take the device off and put it back on every day. You will also complete a short questionnaire for us at this time. This questionnaire takes about 15 minutes to fill out.
On the final session, we will take the accelerometer back and if it shows that you have worn if everyday, you will get a free t-shirt.”
Risks and Benefits:
“All the tests you will do in this study have been reviewed and approved by a board of doctors and are safe and easy to do. They do not involve any pain or discomfort. For being in this study you will learn how many calories your body uses during a week.
Costs and Payments:
“It will not cost you or your family anything to be in this study.”
Confidentiality/Privacy:
“The only people who will ever see the results of your measurements will be you, your parents or guardian, and the people who record the measurements. “
Right to Withdraw:
“You do not have to be in this study if you do not want to be. And, once you start this study, you can stop before you finish if you want to. If you want to stop being in the study all you or your parent or guardian needs to do is tell Mr. Bamman in person, send him a letter (Tunica County Recreation, 1165 Abbay Drive, Tunica, MS 38632) or call Mr. Bamman (363-4019). Whether or not you choose to participate will not affect your standing with the Department of Health, Exercise Science and Recreation Management, with the University of Mississippi or with the Tunica County Recreation Commission, and it will not cause you to lose any benefits to which you are entitled.”
IRB Approval:
“All the measurements we will make in this study are safe and have been reviewed and approved by doctors, professors, and other people associated with the university. The group of people who have reviewed and approved all the measurements are known as the University of Mississippi's Institutional Review Board (IRB). If you or your parents or guardians have any questions, concerns or reports regarding this study you can call the IRB at 915-7482.”
Voluntary Assent: “Do you have any questions? Do you want to be in this study?”
Child’s Response: Yes________ No ________
______________________________________ Date ______________
Print child’s name
______________________________________ Date _______________
Witness
APPENDIX I
Written Assent Form
The University of Mississippi 246 Turner Center University, MS 38677
Child (ages 14-18) Written Assent to Participate in an Experimental Study
Title of Investigation: Determinants of physical activity in rural African-American adolescents
Principal Investigator: Mike BammanDepartment of HESRMUniversity of MississippiUniversity, MS 38677
Description:
This study will help us learn more about what helps determine how physically active a person is. If you decide to take part in this study you will fill out a questionnaire, and wear a small device, called an accelerometer, for 7 days.
On the first day, after we collect the consent forms signed by your parents, we will explain everything about the study to you. Then we will measure your height and your weight. You will then be given an accelerometer to wear for 7 days. We will show you how to wear it and we will tell you the proper use of the accelerometer. We will give you a logbook to write down the times when you take the device off and put it back on every day. You will also complete a short questionnaire for us at this time. This questionnaire takes about 15 minutes to fill out.
On the final session, we will take the accelerometer back and if it shows that you have worn if everyday, you will get a free t-shirt.
Risks and Benefits:
All the tests you will do in this study have been reviewed and approved by a board of doctors and are safe and easy to do. They do not involve any pain or discomfort. For being in this study you will learn how many calories your body uses during a week.
Costs and Payments:It will not cost you or your family anything to be in this study.
Confidentiality/Privacy:
The only people who will ever see the results of your measurements will be you, your parents or guardian, and the people who record the measurements. Protected Health Information: Protected health information is any personal health information through which you can be identified. The data collected in this study includes: medical history, and body mass index. A decision to participate in this research means that you agree to the use of your health information for the study described in this form. This information will not be released beyond the purposes of conducting this study. The information collected for this study will be kept indefinitely. While this study is ongoing you may not have access to the research information, but you may request it after the research is completed.
Right to Withdraw:
You do not have to be in this study if you do not want to be. And, once you start this study, you can stop before you finish if you want to. If you want to stop being in the study all you or your parent or guardian needs to do is tell Mr. Bamman in person, send him a letter (Tunica County Recreation, 1165 Abbay Drive, Tunica, MS 38632) or call Mr. Bamman (363-4019). Whether or not you choose to participate will not affect your standing with the Department of Health, Exercise Science and Recreation Management, with the University of Mississippi or with the Tunica County Recreation Commission, and it will not cause you to lose any benefits to which you are entitled.
IRB Approval:
All the measurements we will make in this study are safe and have been reviewed and approved by doctors, professors, and other people associated with the university. The group of people who have reviewed and approved all the measurements are known as the University of Mississippi's Institutional Review
Board (IRB). If you or your parents or guardians have any questions, concerns or reports regarding this study you can call the IRB at 915-7482.
Statement of Assent:
I have read the above information. I have been given a copy of this form. I have had an opportunity to ask questions, and I have received answers. I assent to participate in the study.
Signature: _____________________________________ Date: ____________
Signature of Investigator: _________________________ Date: ____________
APPENDIX J
Log Book

APPENDIX K
Adherence Flyer
170
APPENDIX L
Single Project Assurance Forms
171

Assurance of Compliance with DHHS Regulations for
Protection of Human Research Subjects
Rosa Fort High School , hereinafter known as the "institution," hereby gives assurance that it will comply with the Department of Health and Human Services (DHHS) regulations for the protection of human research subjects (45 CFR 46) as specified below.
Part I
Ethical Principles and Institutional Policies Governing
Research Involving Human Subjects
I. Applicability
Except for research exempted or waived under the DHHS regulations 45 CFR 46.101, Part I of this Assurance applies to all research involving human subjects, and all other activities which even in part involve such research, regardless of whether the research is otherwise subject to federal regulation, if:
a. the research is sponsored by this institution, orb. the research is conducted by or under the direction of any employee or agent of this institution in
connection with institutional responsibilities, orc. the research is conducted by or under the direction of any employee or agent of this institution using
any property or facility of this institution, ord. the research involves the use of this institution's nonpublic information to identify or contact human
research subjects or prospective subjects.
II. Ethical Principles Governing Human Subjects Research
This institution is guided by the ethical principles regarding all research involving humans as subjects as set forth in the report of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research entitled, Ethical Principles and Guidelines for theProtection of Human Subjects of Research (the "Belmont Report") and as specified below.
A. This institution recognizes the principles of respect for persons, beneficence (including minimization of harms and maximization of benefits), and justice as stated in the Belmont Report and will apply these principles in all research covered by this Assurance.
B. This institution acknowledges and accepts its responsibilities for protecting the rights and welfare of human research subjects.
III. Policies
A. This institution acknowledges that it and its investigators bear full responsibility for the performance of all research covered by this Assurance, including full responsibility for complying with federal, state, and local laws as they may relate to such research.
172
B. This institution assures that before human subjects are involved in research, proper consideration will be given to:
(1) the risks to the subjects,(2) the anticipated benefits to the subjects and others,(3) the importance of the knowledge that may reasonably be expected to result,(4) the informed consent process to be employed,(5) the provisions to protect the privacy of subjects, and(6) the additional safeguards for vulnerable populations.
C. This institution recognizes the need for appropriate additional safeguards in research involving subjects who are likely to be vulnerable to coercion or undue influence, such as children, prisoners, pregnant women, mentally disabled persons, or economically or educationally disadvantaged persons.
D. This institution encourages and promotes constructive communication among the institutional officials, research administrators, department heads, research investigators, clinical care staff, human subjects, and all other relevant parties as a means of maintaining a high level of awareness regarding the safeguarding of the rights and welfare of the subjects.
E.This institution will exercise appropriate administrative overview carried out at least annually to assure that its practices and procedures designed for the protection of the rights and welfare of human subjects are being effectively applied.
173
Part 2
IRB, Institution, and Investigator Compliance with 45 CFR 46
I. Applicability
Part 2 of this Assurance applies to the following research project which is conducted or sponsored by this institution in collaboration with The University of Mississippi.
Project title Determinants of Physical Activity in Rural African-American Adolescents
Project Investigator Mike Bamman
Research Advisor (if applicable) Jeff Hallam, PhD
II. Institutional Responsibilities
A. This institution has complied and will continue to comply with the requirements of 45 CFR 46 as specified below.
B. This institution has reviewed and sponsors the project referenced above, and is responsible for continuing review of this project in conjunction with the Institutional Review Board at The University of Mississippi.
III. IRB Review
A. The IRB at The University of Mississippi shall review, and have the authority to approve, require modification in, or disapprove this research activity or proposed changes in it before human subjects become involved.
B. The convened IRB reviewed and approved the above project.
C. The IRB determined, in accordance with the criteria found at 45 CFR 46.111, and where applicable, 45 CFR 46 Subparts B, C, and D, that protections for human research subjects are adequate.
D. The IRB has the authority to suspend or terminate approval of the above referenced research in accordance with 45 CFR 46.113 for (1) noncompliance with 45 CFR 46, and this Assurance document or the IRB's requirements, and (2) for elimination of unexpected serious harm to subjects.
E. The IRB has determined that legally effective informed consent [copy of document must be attached unless specified otherwise by the IRB Chair] will be obtained in a manner and method which meets the requirements of 45 CFR 46.116 and 46.117.
F. Continuing reviews by the IRB shall be conducted at intervals appropriate to the degree of risk, but not less than once per year (45 CFR 46.109[e]). The IRB may be called into an interim review session by the Chairperson at the request of any IRB member or Institutional Official to consider any matter concerned with the rights and welfare of any subject.
G.The IRB shall prepare and maintain adequate documentation of its activities with respect to this
174

project in accordance with 45 CFR 4.115.
H.The IRB shall report promptly to institutional officials:
(1) any serious or continuing noncompliance by investigators with the requirements of the IRB,
(2) any suspension or termination of IRB approval,(3) any unanticipated problems or injuries involving risks to subjects or others, and(4) any changes in this research activity which are reviewed and approved by the IRB.
I. Where appropriate, the IRB will determine that adequate additional protections are ensured for fetuses, pregnant women, prisoners, and children as required under Subparts B, C, and D of 45 CFR 46.
J. The IRB will comply fully with the requirements of all applicable Federal policies and guidelines, including those concerning notification of sero-positivity, counseling, and confidentiality of subjects.
IV. Research Investigator Reporting Responsibilities
A.Investigators acknowledge and accept their responsibility for protecting the rights and welfare of human research subjects and for complying with all applicable provisions of this Assurance and 45 CFR 46.
B. Research investigators shall report promptly to the IRB proposed changes in this research activity and the changes shall not be initiated without IRB review and approval except where necessary to eliminate apparent immediate hazards to the subjects.
C. Research investigators shall report promptly to the IRB any unanticipated problems involving risks to subjects and others
175
Part 3
Certification of IRB Approval and Institutional Endorsement
Project Title Determinants of Physical Activity in Rural African-American Adolescents
IRB Project number 04-081
Project Investigator/Research Advisor Mike Bamman Date of IRB approval 02-25-2004 Date of Next Scheduled IRB Review
The officials signing below assure that the project referenced above was approved by the IRB on the date indicated and that the project will be conducted in accordance with the requirements of Part 46, Title 45 of the Code of Federal Regulations and this Assurance document.
I. Authorized Official of the Institution Providing This Assurance
Signature Date
Name and Title: Larry Ball, Principal – Rosa Fort High School
Address: 1100 Rosa Fort Drive Tunica, MS 38676
Telephone: 662-363-1343 FAX: 662-357-4222
II. Authorized Official of the Institution with the IRB or IRB Chairperson
This institution authorizes the designation of its IRB for review of the project referenced in this Assurance.
Signature Date
Name and Title: Diane W. Lindley, Coordinator, Institutional Review BoardAddress: The University of Mississippi
Office of Research and Sponsored ProgramsP.O. Box 907University, MS 38677
Telephone: 662-915-7482FAX: 662-915-7577
176
III. Responsible Project Investigator or Director at Institution Providing this Assurance
I have attached copies of all IRB requested documents and approved Informed Consent Documents to be used in this project.
Signature Date
Name and Title: Mike Bamman, Project Investigator
Address: 1241 Pendulum Drive Hernando, MS 38632
Telephone: 662-363-4019 FAX: 662-363-4059
177

Assurance of Compliance with DHHS Regulations for
Protection of Human Research Subjects
North Mississippi Delta Boys and Girls Club , hereinafter known as the "institution," hereby gives assurance that it will comply with the Department of Health and Human Services (DHHS) regulations for the protection of human research subjects (45 CFR 46) as specified below.
Part I
Ethical Principles and Institutional Policies Governing
Research Involving Human Subjects
I. Applicability
Except for research exempted or waived under the DHHS regulations 45 CFR 46.101, Part I of this Assurance applies to all research involving human subjects, and all other activities which even in part involve such research, regardless of whether the research is otherwise subject to federal regulation, if:
a. the research is sponsored by this institution, orb. the research is conducted by or under the direction of any employee or agent of this institution in
connection with institutional responsibilities, orc. the research is conducted by or under the direction of any employee or agent of this institution using
any property or facility of this institution, ord. the research involves the use of this institution's nonpublic information to identify or contact human
research subjects or prospective subjects.
II. Ethical Principles Governing Human Subjects Research
This institution is guided by the ethical principles regarding all research involving humans as subjects as set forth in the report of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research entitled, Ethical Principles and Guidelines for theProtection of Human Subjects of Research (the "Belmont Report") and as specified below.
A. This institution recognizes the principles of respect for persons, beneficence (including minimization of harms and maximization of benefits), and justice as stated in the Belmont Report and will apply these principles in all research covered by this Assurance.
B. This institution acknowledges and accepts its responsibilities for protecting the rights and welfare of human research subjects.
178

III. Policies
A. This institution acknowledges that it and its investigators bear full responsibility for the performance of all research covered by this Assurance, including full responsibility for complying with federal, state, and local laws as they may relate to such research.
B. This institution assures that before human subjects are involved in research, proper consideration will be given to:
(1) the risks to the subjects,(2) the anticipated benefits to the subjects and others,(3) the importance of the knowledge that may reasonably be expected to result,(4) the informed consent process to be employed,(5) the provisions to protect the privacy of subjects, and(6) the additional safeguards for vulnerable populations.
C. This institution recognizes the need for appropriate additional safeguards in research involving subjects who are likely to be vulnerable to coercion or undue influence, such as children, prisoners, pregnant women, mentally disabled persons, or economically or educationally disadvantaged persons.
D. This institution encourages and promotes constructive communication among the institutional officials, research administrators, department heads, research investigators, clinical care staff, human subjects, and all other relevant parties as a means of maintaining a high level of awareness regarding the safeguarding of the rights and welfare of the subjects.
E.This institution will exercise appropriate administrative overview carried out at least annually to assure that its practices and procedures designed for the protection of the rights and welfare of human subjects are being effectively applied.
179
Part 2
IRB, Institution, and Investigator Compliance with 45 CFR 46
I. Applicability
Part 2 of this Assurance applies to the following research project which is conducted or sponsored by this institution in collaboration with The University of Mississippi.
Project title Determinants of Physical Activity in Rural African-American Adolescents
Project Investigator Mike Bamman
Research Advisor (if applicable) Jeff Hallam, PhD
II. Institutional Responsibilities
A. This institution has complied and will continue to comply with the requirements of 45 CFR 46 as specified below.
B. This institution has reviewed and sponsors the project referenced above, and is responsible for continuing review of this project in conjunction with the Institutional Review Board at The University of Mississippi.
III. IRB Review
A. The IRB at The University of Mississippi shall review, and have the authority to approve, require modification in, or disapprove this research activity or proposed changes in it before human subjects become involved.
B. The convened IRB reviewed and approved the above project.
C. The IRB determined, in accordance with the criteria found at 45 CFR 46.111, and where applicable, 45 CFR 46 Subparts B, C, and D, that protections for human research subjects are adequate.
D. The IRB has the authority to suspend or terminate approval of the above referenced research in accordance with 45 CFR 46.113 for (1) noncompliance with 45 CFR 46, and this Assurance document or the IRB's requirements, and (2) for elimination of unexpected serious harm to subjects.
E. The IRB has determined that legally effective informed consent [copy of document must be attached unless specified otherwise by the IRB Chair] will be obtained in a manner and method which meets the requirements of 45 CFR 46.116 and 46.117.
F. Continuing reviews by the IRB shall be conducted at intervals appropriate to the degree of risk, but not less than once per year (45 CFR 46.109[e]). The IRB may be called into an interim review session by the Chairperson at the request of any IRB member or Institutional Official to consider any matter concerned with the rights and welfare of any subject.
G.The IRB shall prepare and maintain adequate documentation of its activities with respect to this
180
project in accordance with 45 CFR 4.115.
H.The IRB shall report promptly to institutional officials:
(1) any serious or continuing noncompliance by investigators with the requirements of the IRB,
(2) any suspension or termination of IRB approval,(3) any unanticipated problems or injuries involving risks to subjects or others, and(4) any changes in this research activity which are reviewed and approved by the IRB.
I. Where appropriate, the IRB will determine that adequate additional protections are ensured for fetuses, pregnant women, prisoners, and children as required under Subparts B, C, and D of 45 CFR 46.
J. The IRB will comply fully with the requirements of all applicable Federal policies and guidelines, including those concerning notification of sero-positivity, counseling, and confidentiality of subjects.
IV. Research Investigator Reporting Responsibilities
A.Investigators acknowledge and accept their responsibility for protecting the rights and welfare of human research subjects and for complying with all applicable provisions of this Assurance and 45 CFR 46.
B. Research investigators shall report promptly to the IRB proposed changes in this research activity and the changes shall not be initiated without IRB review and approval except where necessary to eliminate apparent immediate hazards to the subjects.
D. Research investigators shall report promptly to the IRB any unanticipated problems involving risks to subjects and others
181

Part 3
Certification of IRB Approval and Institutional Endorsement
Project Title Determinants of Physical Activity in Rural African-American Adolescents
IRB Project number 04-081
Project Investigator/Research Advisor Mike Bamman Date of IRB approval 02-25-204 Date of Next Scheduled IRB Review
The officials signing below assure that the project referenced above was approved by the IRB on the date indicated and that the project will be conducted in accordance with the requirements of Part 46, Title 45 of the Code of Federal Regulations and this Assurance document.
I. Authorized Official of the Institution Providing This Assurance
Signature Date
Name and Title: Yolanda Kemp, Director North MS Delta Boys and Girls Club
Address: 1165 Abbay Drive Tunica, MS 38676
Telephone: 662-357-0523 FAX: 662-363-2242
II. Authorized Official of the Institution with the IRB or IRB Chairperson
This institution authorizes the designation of its IRB for review of the project referenced in this Assurance.
Signature Date
Name and Title: Diane W. Lindley, Coordinator, Institutional Review BoardAddress: The University of Mississippi
Office of Research and Sponsored ProgramsP.O. Box 907University, MS 38677
Telephone: 662-915-7482FAX: 662-915-7577
182
III. Responsible Project Investigator or Director at Institution Providing this Assurance
I have attached copies of all IRB requested documents and approved Informed Consent Documents to be used in this project.
Signature Date
Name and Title: Mike Bamman, Project Investigator
Address: 1241 Pendulum Drive Hernando, MS 38632
Telephone: 662-363-4019 FAX: 662-363-4059
183
APPENDIX M
Raw Data
184

ID # Age Grade SexFree
LunchCurrent Sport
Usual Act Lvl Ht Wt
mw4990 16 11 2 1 2 3 63.8 155mp1004 17 12 2 1 2 2 64.3 113xlb4997 18 10 1 2 1 1 68.5 181.4mb79531 17 11 2 1 1 1 62.7 107.2mb4190 15 10 2 1 2 2 66 129.8xxb0404 15 9 1 1 1 1 71 217xlb1499 17 11 2 2 2 3 64 156.4mp1496 15 9 2 1 1 2 62 126.8xxb7695 17 12 1 1 2 1 71.3 188.2xb7422 15 9 1 1 2 2 68.3 157lb1478 15 9 2 1 2 3 64.8 154.4lg4249 15 10 2 2 2 3 63.5 112mr7172 14 9 1 1 1 2 67.2 147bl010 17 10 2 2 2 2 62.7 132xlw0505 15 9 1 1 2 3 71.2 156.6mr1669 16 10 2 1 2 3 63.4 122.6xp1717 17 11 2 1 2 3 62 187.2xb5477 15 9 2 1 1 3 70.7 206.2lp2498 17 9 2 1 2 2 63.5 148.6xlr8101 15 9 2 1 1 3 66 147.4mb1386 13 8 1 2 2 3 64 130.6xlp41168 18 12 2 1 2 3 61.8 221m6410 15 10 2 1 2 2 70.3 127.8lb3963 16 9 2 1 2 1 63.3 133mb2506 13 8 1 1 2 3 62 119.5mp24141 18 12 2 2 2 3 60.3 145mb79123 18 12 2 1 2 1 67.7 149.4xxxlp12156 18 12 2 1 2 3 65 328.6pm1474 18 12 2 1 2 3 63.2 147.4xb1498 16 10 1 1 1 3 68.5 166.8lb1246 15 10 1 1 1 3 66.2 123.6mb2020 19 12 2 1 1 3 64.5 156.4mr1799 17 11 2 1 2 1 60 104xb6943 15 9 1 1 1 1 67.8 168.4mb1624 17 12 1 1 2 3 66.4 152.4xr6423 18 12 2 1 2 3 65 169xxo3030 18 12 1 1 1 3 71.5 263.8mp1982 16 11 2 1 2 3 60.3 110.8so4114 15 9 2 1 2 2 64 118mb6344 14 9 1 1 2 3 63.8 123.7sg4229 12 7 1 2 2 2 61.5 125.6
185
xb7944 17 10 1 2 2 2 70 204.8
ID # Age Grade SexFree
LunchCurrent Sport
Usual Act Lvl Ht Wt
5sk4 16 10 1 1 2 3 72 165.8lb1496 14 9 1 2 2 1 66.5 149.6xm8970 16 10 2 1 2 2 64 136xb7644 18 12 1 2 2 3 71.8 146.4sr6498 15 9 2 1 2 3 63 114.6xb6416 15 9 1 2 2 2 69.2 146.6mb7466 16 11 2 2 2 1 66 138.8xb2934 17 10 1 2 2 3 65.5 161mp24996 17 11 2 1 2 2 65.5 142.4sb4728 14 9 2 1 2 2 60 111.2xxxlb2927 17 10 1 1 2 3 68 304.6mb2978 15 9 1 1 1 3 65 129.6xb97428 16 9 1 1 1 1 67.8 163.6sb3114 15 9 2 2 1 3 63.5 107.2mp6061 15 9 2 1 1 3 59 119.6xxb9125 17 18 1 2 1 1 73 198.8xlb8396 13 8 1 1 1 3 62.8 184.6xb1956 19 12 2 1 1 3 66.6 140.2xlr7718 18 12 1 1 1 1 71.2 176.2xlg8212 15 9 1 1 1 3 68.7 134xb14785 18 12 1 1 2 1 71.5 150mp41020 15 9 2 1 2 1 60.5 133xxlb1123 16 10 1 1 1 3 70.5 265lb04598 17 11 2 1 2 2 64 157.8mb3994 15 10 2 1 2 3 65 151.8mb8406 15 9 1 1 1 3 62.2 112mp14986 17 11 2 2 2 3 59.3 104.8lb12457 14 9 1 2 2 3 63 119xr69428 15 9 1 1 2 1 64.5 137.2xxb5791 16 11 1 1 2 3 63.3 215.6lb4996 15 9 1 1 1 3 69.25 130.6mp1552 15 9 2 2 2 1 62 130.4sb1364 13 8 1 1 2 3 62 132.6lb7987 16 9 1 1 2 3 68 138.5sg6633 15 9 1 2 2 3 70.2 179.4xlb6211 15 9 1 2 1 3 68 153mr6143 15 10 2 1 2 3 66.3 138mb6432 14 9 1 1 2 2 68.5 127.8lr9462 15 9 1 1 2 3 68.3 109.6xb79642 18 12 2 1 2 1 62 172.6xb9874 15 9 2 1 2 1 65 165.4
186
lr49873 14 9 2 1 2 3 59 134.4
ID # Wt BMI SAHHP Barrier
Q Kcal Light
Q Kcal Mod
Q Kcal Hard
Q Kcal V Hard
mw4990 155 26.8 40 43 172.5 12 0 0mp1004 113 19.3 25 41 144 68 0 0xlb4997 181.4 27.2 27 47 138 16 60 150mb79531 107.2 19.2 33 50 148.5 28 18 30mb4190 129.8 21.0 27 33 103 40 90 140xxb0404 217 30.3 48 63 108 64 114 50xlb1499 156.4 26.9 26 62 78 24 30 100mp1496 126.8 23.2 45 56 105 80 24 80xxb7695 188.2 26.1 19 24 144 52 18 0xb7422 157 23.7 26 35 168 48 0 0lb1478 154.4 25.9 44 28 153 18 12 0lg4249 112 19.6 23 37 141 48 42 10mr7172 147 22.9 11 39 147.75 22 18 50bl010 132 23.7 8 50 150 0 0 0xlw0505 156.6 21.8 31 15 129 0 116 0mr1669 122.6 21.5 26 49 94.5 60 90 150xp1717 187.2 34.3 48 50 180 8 12 20xb5477 206.2 29.1 39 57 144 52 66 50lp2498 148.6 26.0 48 57 69 152 150 170xlr8101 147.4 23.8 40 49 158.25 12 18 40mb1386 130.6 22.5 30 29 148.5 24 36 60xlp41168 221 40.8 27 46 162 40 0 0m6410 127.8 18.2 24 33 163.5 36 0 0lb3963 133 23.4 30 37 102 24 60 180mb2506 119.5 21.9 28 33 163.5 16 54 40mp24141 145 28.1 40 48 154.5 36 42 20mb79123 149.4 23.0 26 39 114 20 60 80xxxlp12156 328.6 54.8 35 50 159.75 48 12 0pm1474 147.4 26.0 29 28 159 18 15 40xb1498 166.8 25.0 37 70 177.75 10 18 40lb1246 123.6 19.9 20 43 152.3 6 18 100mb2020 156.4 26.5 35 66 133.5 32 48 70mr1799 104 20.4 34 56 145.5 12 30 70xb6943 168.4 25.8 25 41 100.5 80 30 60mb1624 152.4 24.4 30 27 144.5 38 72 10xr6423 169 28.2 32 45 139.5 12 12 0xxo3030 263.8 36.4 38 37 84 112 60 100mp1982 110.8 21.5 19 56 125.5 28 24 40so4114 118 20.3 29 47 165 20 18 0mb6344 123.7 21.4 33 39 114 80 90 10sg4229 125.6 23.4 37 34 144 24 18 30
187
xb7944 204.8 29.4 45 20 115.5 12 120 140
ID # Wt BMI SAHHP Barrier
Q Kcal Light
Q Kcal Mod
Q Kcal Hard
Q Kcal V Hard
5sk4 165.8 22.5 33 45 133.58 20 24 70lb1496 149.6 23.8 36 21 154.5 36 24 30xm8970 136 23.4 37 46 138 24 20 0xb7644 146.4 20.0 33 44 168.75 30 18 160sr6498 114.6 20.3 26 44 165 42 48 20xb6416 146.6 21.6 39 32 136.5 36 84 40mb7466 138.8 22.4 24 53 115.5 28 30 90xb2934 161 26.4 46 42 154.5 20 6 10mp24996 142.4 23.4 32 44 168 4 12 40sb4728 111.2 21.8 31 58 183 16 0 0xxxlb2927 304.6 46.4 30 41 153 20 0 0mb2978 129.6 21.6 35 54 171.75 24 48 40xb97428 163.6 25.1 43 18 169.5 4 12 20sb3114 107.2 18.7 47 49 144 32 36 60mp6061 119.6 24.2 36 42 100.5 40 150 100xxb9125 198.8 26.3 8 29 94.5 64 102 160xlb8396 184.6 33.0 29 27 148.5 16 0 30xb1956 140.2 22.3 32 40 151.5 24 18 20xlr7718 176.2 24.5 32 70 81 52 78 180xlg8212 134 20.0 40 36 109.5 48 48 150xb14785 150 20.7 36 54 138 24 96 50mp41020 133 25.6 32 53 148.5 48 24 0xxlb1123 265 37.6 36 40 162 36 60 40lb04598 157.8 27.1 34 47 133.5 16 90 0mb3994 151.8 25.3 31 60 147 24 90 0mb8406 112 20.4 34 49 147 40 60 110mp14986 104.8 21.0 36 57 118.5 20 57 50lb12457 119 21.1 38 31 148.5 24 60 110xr69428 137.2 23.2 33 54 139.5 20 30 50xxb5791 215.6 37.9 37 35 144.75 26 12 0lb4996 130.6 19.2 30 46 120 52 36 40mp1552 130.4 23.9 15 33 136.5 12 24 0sb1364 132.6 24.3 36 39 165 8 48 120lb7987 138.5 21.1 30 70 132 4 18 60sg6633 179.4 25.6 43 26 136.5 40 30 20xlb6211 153 23.3 30 32 114 32 48 60mr6143 138 22.1 34 29 151.5 16 30 160mb6432 127.8 19.2 44 39 90 44 108 120lr9462 109.6 16.6 31 61 155.25 28 12 25xb79642 172.6 31.6 17 49 120.2 16 12 0xb9874 165.4 27.6 36 65 93 72 21 215
188
lr49873 134.4 27.2 29 50 142.5 8 12 20
ID #Total
kcal/wkDay 1
KalDay 2 Kcal
Day 3 Kcal
Day 4 Kcal
Day 5 Kcal
mw4990 4949.9 330.5 377.4 249.3 284.8 252mp1004 4082.3 197.4 133.4 184.9 173.6 159.4xlb4997 9914.4 1277.9 1929.5 2267.8 652.4 812.1mb79531 4313.1 210.6 310.3 224.4 249.7 319.8mb4190 7830.8 513.3 631.9 1144.6 359.9 325.6xxb0404 10190.4 992.6 860.3 608.2 900.7 461.1xlb1499 6241.3 390.5 575.33 378.12 381.33 570.99mp1496 6716.5 201.29 227.15 235.32 324.4 484.9xxb7695 5581.7 520.5 1478.1 953.9 523.3 1035.7xb7422 5121.8 579.8 994.4 608.6 890.13 1056.2lb1478 4740.9 586.21 679.5 731.7 443.12 839.6lg4249 4716.3 202.1 232.9 270.5 286.4 269.6mr7172 5452.7 402.7 442.5 641.9 730.4 1116.8bl010 3548.5 716.66 866.3 278.9 254.1 648.2xlw0505 5332.2 724.4 574.1 271.2 186.9 329.8mr1669 8477.5 409.6 448.8 340.86 130.8 440.2xp1717 7548.4 246.3 235.1 609.1 358.4 352.7xb5477 9068.1 693.8 935.7 912.7 627 500lp2498 14046.8 465.6 547.5 436.7 475.2 357.4xlr8101 5441.6 496.3 668.9 833.8 434.4 839.6mb1386 6031.7 286.1 249.9 318.4 194.3 172.4xlp41168 8235.2 159.4 189.7 148.4 154.3 238.3m6410 3634.7 253.1 294.3 645.9 347.2 213.7lb3963 8559.2 212.8 310.3 424 497.6 687.3mb2506 5990.3 489.7 442.8 375.3 343.5 466.4mp24141 7094.2 231.1 289.7 495.8 520.4 485.1mb79123 6292.7 697.3 631.7 551.6 463.4 554.9xxxlp12156 12041.5 657.5 855.3 270.6 413.6 624.7pm1474 6032.0 164.3 523.3 631.4 410.8 722.1xb1498 6154.9 462.8 848.1 742.2 106.1 363.3lb1246 5490.3 359.2 508.5 1265.4 176.5 222.3mb2020 7509.0 897.34 1266.3 1290.45 773.48 880.4mr1799 5241.0 201.1 200.7 195.2 156.6 101.3xb6943 6981.7 551.6 535.3 636.1 494.6 372.5mb1624 6441.5 639.7 484.8 477.5 499.6 563.4xr6423 4607.7 290.5 575.3 378.12 381.33 570.99xxo3030 12942.6 704.96 1205.9 1861.6 1450.9 1602.4mp1982 4669.5 137.6 140.9 212.9 226.9 374.2so4114 4120.3 238.8 285.1 545.02 405.2 409.9mb6344 6294.9 612.5 388.3 356.8 743.7 428.6sg4229 5053.6 337.1 482.6 421.3 346.8 521.7
189
xb7944 11410.8 2392.8 2492.6 2392.1 2992.2 2806.3
ID #Total
kcal/wkDay 1 Kal
Day 2 Kcal
Day 3 Kcal
Day 4 Kcal
Day 5 Kcal
5sk4 5578.9 942.7 727.2 1182.4 585.2 533.5lb1496 5827.4 277.8 296.3 321.1 265.7 462.8xm8970 4257.6 404.2 662.5 954.5 273.3 324.7xb7644 7538.0 187.9 369.74 384.93 102.8 205.7sr6498 5594.3 161.7 222.6 206.2 289.7 312.7xb6416 6395.2 232.8 302.3 554.9 431.1 385.4mb7466 5915.5 436.4 328 413.3 304.6 423.1xb2934 5036.7 574.4 431.3 332.1 459.4 482.3mp24996 5238.2 478.3 209.5 391.3 367.6 328.1sb4728 4330.8 171.5 235.1 275.5 184.1 306.6xxxlb2927 8029.1 678.1 599.1 312.1 380.6 622.1mb2978 6132.3 536.4 441.8 291.7 409 507.3xb97428 5152.8 730.4 951 300.6 459.7 694.8sb3114 5094.8 197.4 175.1 116.8 166.1 144.9mp6061 9452.7 617.2 720.8 667 949.2 1042.4xxb9125 11052.1 977.1 941.1 428.6 782.5 658.3xlb8396 6414.2 949.4 1491.5 336.4 684.5 1034.6xb1956 4754.5 499.6 507.5 463.7 553.8 520.4xlr7718 9574.9 1897.5 1966.3 2290.3 1377.9 1480.4xlg8212 7111.2 617.4 720.8 667 949.2 1042.4xb14785 6367.1 753.5 639.7 790.9 1020.2 812.7mp41020 5644.9 859.9 431.3 637.6 296.3 169.6xxlb1123 11194.2 1231.6 1330.8 1746.1 645.8 579.7lb04598 6500.7 214.7 482.99 139.54 420.37 361.3mb3994 6606.9 156.9 228.1 398.9 159.5 272.8mb8406 7281.4 577.4 562.4 683.9 489.4 1151.5mp14986 5154.8 246.3 632.6 206.8 334.6 226.6lb12457 7235.0 139.9 299.6 387.1 247.6 219.2xr69428 5564.8 895.1 489.6 201.6 647.2 1906.3xxb5791 6928.0 245.1 376.6 279.9 123.1 410.66lb4996 4758.4 310.6 156.6 180.4 346.8 404.8mp1552 4122.8 173.5 375.3 297.5 328.1 296.3sb1364 8287.5 744.9 1012.45 1168.4 1566.2 1349.5lb7987 4516.0 522.9 617.2 664.7 654.9 963.5sg6633 5809.3 397.4 329.7 324.4 402.3 436.4xlb6211 5921.3 183.2 409 631.7 572.1 456.8mr6143 7907.5 344.5 394.2 469.8 390.1 430.6mb6432 6946.5 591 896.2 241 135.5 256.9lr9462 3645.8 170.8 145.3 105.5 120.1 143.9xb79642 4688.3 116.9 866.5 270.5 201.8 261.1xb9874 11060.2 237.6 780.5 1051.1 1046.6 783.8
190
lr49873 4964.4 165.4 284.8 214.2 177.5 238.8
ID #Day 6 Kcal
Day 7 Kcal
Total 7d
KcalMETS MTI
METS PAR
mw4990 302.3 232.5 2028.9 4137.5 8380.145mp1004 232.6 270.5 1351.8 3174.75 5850.524xlb4997 431.5 908.5 8279.7 7810.4 17537.09mb79531 131.1 189.7 1635.6 3227.73 6385.222mb4190 711.5 639.2 4326 6271.03 11398.8xxb0404 2218.8 1512.1 7553.8 4651.1 14118.41xlb1499 241.17 265.72 2803.16 3065.95 9530.732mp1496 239.9 262.3 1975.26 2407.8 8714.618xxb7695 583.35 279.9 5374.75 11442.97 9657.74xb7422 607.5 505.9 5242.53 4150.7 8919.884lb1478 403.2 322.1 4005.43 8358.89 7675.645lg4249 632.6 436.4 2330.5 5180.73 6157.964mr7172 484.4 819.4 4638.1 4111.8 9564.087bl010 794.2 721.8 4280.16 7528.3 6048xlw0505 296.7 190.3 2573.4 2382 7557.801mr1669 225.5 213.3 2209.06 3031.8 11122.27xp1717 309.4 320.7 2431.7 4757.31 11836.49xb5477 294.3 326.2 4289.7 8470.7 14643.95lp2498 591.6 664.3 3538.3 5226.6 15523.57xlr8101 503.6 672.1 4448.7 3699.6 9421.272mb1386 387 296.5 1904.6 3436.08 9155.297xlp41168 272.3 159.4 1321.8 2682.81 11948.47m6410 287.7 221.8 2263.7 4696.33 6909.565lb3963 131.1 189.7 2452.8 4635.14 12797.02mb2506 404.8 512.4 3034.9 6068.73 8212.909mp24141 634.1 544.3 3200.5 7213.5 8836.036mb79123 562.4 494.8 3956.1 8960.91 10062.5xxxlp12156 632.8 489.5 3944 6881.53 18142.3pm1474 700.8 472.1 3624.8 7878.34 9522.576xb1498 634.4 376.3 3533.2 6422.25 11616.56lb1246 384.3 522.8 3439 4213.5 9968.992mb2020 684.6 559.7 6352.27 9685.95 11035.58mr1799 232.9 183.2 1271 2045.2 7338.24xb6943 214.9 516.8 3321.8 2883.54 10339.15mb1624 434.8 428.6 3528.4 9722.25 8716.726xr6423 241.17 265.72 2703.13 2465.23 7588.407xxo3030 1396.9 799 9021.66 3585.95 19822.41mp1982 178 152.6 1423.1 5285.25 6227.363so4114 381.02 405.9 2670.94 3429.14 6379.724mb6344 196.6 356.5 3083 3316.28 6687.897sg4229 364.6 319.7 2793.8 4835.41 7251.002
191

xb7944 615.4 311.5 14002.9 9000.65 18579.46
ID #Day 6 Kcal
Day 7 Kcal
Total 7d
KcalMETS MTI
METS PAR
5sk4 477.5 638.6 5087.1 4210.16 11171.13lb1496 476.2 428.4 2528.3 4680.98 9390.528xm8970 272.4 104.7 2996.3 3393.59 6314.356xb7644 350.8 230.91 1832.78 3797 15763.29sr6498 122.9 189.3 1505.1 2320.6 7482.338xb6416 301.6 266.5 2474.6 5066.73 9538.063mb7466 289.3 300.9 2495.6 3588.61 9666.537xb2934 522.4 463.4 3265.3 6610.89 8557.004mp24996 299.9 346.1 2420.8 4992.12 9330.048sb4728 332.1 165.2 1670.1 2599.41 6419.677xxxlb2927 651.1 697.3 3940.4 7157.33 14933.15mb2978 441.8 339.7 2967.7 3197.08 9293.027xb97428 632.1 543.8 4312.4 4993.65 9744.611sb3114 165.5 161.9 1127.7 1680.31 7465.798mp6061 620.7 739.3 5356.6 6510.2 9425.35xxb9125 1044.2 1151.7 5983.2 11600.8 18946xlb8396 757.9 829.4 6083.7 7224.25 10487.97xb1956 169.1 212.6 2926.7 5740.11 7965.399xlr7718 684.6 559.7 10256.7 21836.55 16630.72xlg8212 620.7 739.31 5356.81 6482.76 12156.48xb14785 428.6 747.2 5192.8 4798.46 10240.36mp41020 733.1 599.7 3727.3 7358.9 7007.891xxlb1123 1294.5 1174.5 8003 13327.58 18819.82lb04598 315.5 146 2080.4 1939.6 7808.518mb3994 502.3 421.9 2140.4 3677.3 8276.688mb8406 995.2 730.8 5190.6 6807.3 10006.69mp14986 333.4 653.6 2633.9 4203.1 6170.243lb12457 391.7 238.8 1923.9 4704.88 10468.54xr69428 374.1 859.5 5373.4 11017.28 8675.031xxb5791 105.9 277.8 1819.06 1305.23 10372.32lb4996 373.1 330.5 2102.8 4208.15 7599.495mp1552 423.9 409.3 2303.9 2640.95 5855.197sb1364 1199.6 710.85 7751.9 15789.82 12394lb7987 1158.6 330.9 4912.7 11014.5 8503.396sg6633 441.8 541.6 2873.6 5817.88 9863.738xlb6211 523.9 196.4 2973.1 5632.72 9393.644mr6143 211.6 304.9 2545.7 2755.12 14036.86mb6432 569.7 974.4 3664.7 6078.2 10130.13lr9462 231.1 231.7 1148.4 1708.17 6528.175xb79642 360.9 228.3 2306 4778.3 6811.612xb9874 339.1 458.1 4696.8 7438.11 17733.29
192
lr49873 206.1 137.9 1424.7 2724.75 6958.499
VITA
Michael R. Bamman was born in Chattanooga, Tennessee August 1,
1968. He graduated from Tennessee State University in May of 1994 with a
Bachelor of Science in Health, Physical Education, and Recreation. Mike
received his Masters of Education from Auburn University in Health Promotion in
August 1995. After graduation, Mike worked as a clinical exercise physiologist
with Vanderbilt University Medical Center in Nashville, Tennessee until 2000,
when he took a similar position with Methodist Healthcare in Memphis,
Tennessee. In May of 2001, Mike was named Director of the G.W. Henderson,
Sr. Health and Wellness Pavilion in Tunica, Mississippi, just before he began his
doctoral work at the University of Mississippi in August of 2001.
193