development of a pediatric trigger tool to identify ...development of a pediatric trigger tool to...
TRANSCRIPT

1
Development of a Pediatric Trigger Tool to Identify Adverse Drug Events
Pediatric Safety Surveillance WorkshopCritical Path InstituteSeptember 13, 2010
Glenn Takata, MD, MSChildrens Hospital Los Angeles
2
Abbreviations
ADE = Adverse Drug Event
CHAI = Child Health Accountability Initiative
CHCA = Child Health Corporation of America
IHI = Institute for Healthcare Improvement
ME = Medication Error

3
Outline
1. Why Measure?
2. ADE Trigger Tool Origins
3. Development of a Pediatric ADE Trigger Tool
4. Is the Outcome the Trigger Tool?
5. ADE Trigger Tool Challenges

4
Why Measure?
Accountability versus Improvement?
↓For the Child Health Accountability Initiative
Improvement = Measurement Purpose!

5
A trigger is defined as an “occurrence,
prompt, or flag found on review of the
medical chart that ‘triggers’ further
investigation to determine the presence
or absence of an adverse event.
Classen, 1991
ADE Trigger Tool Origins

6
Trigger Example:
• Naloxone (Narcan) Trigger:
“This is a powerful narcotic antagonist. If it has been used,overdosage of narcotics is a frequent finding. If it was used and the patient's condition didn't change, doubt excessive narcotic administration.”
• Review medical record for naloxone use.
• If found, e.g. morphine order, review medical record for ADE associated with naloxone use, e.g. respiratory arrest in child who received morphine.
ADE Trigger Tool Origins

7
Classen’s (1991) Trigger Tool
• Computerized monitorSudden medication order stopsAntidote orderingAbnormal laboratory values
• Computer identified trigger• Pharmacist identified ADE
ADE Trigger Tool Origins
IHI ADE Trigger Tool (Rozich, 2003)
• Chart Review monitorSudden medication order stopsAntidote orderingAbnormal laboratory valuesOversedation, rash, transferCustomized to individual institution
• Reviewer identified trigger• Reviewer identified ADE

8
ADE Trigger Tool Origins
ElectronicDatabase
TriggerInvestigator
ADETriggerList
Classen’s (1991) Trigger Tool36,653 Primarily Adult Patients over 18 months
Trigger Tool 631 ADEsVoluntary Report 92 ADEs

9
TriggerList
Chart ReviewTrigger
InvestigatorADE
IHI ADE Trigger Tool (2003)Total: 2,837 Patients in 86 hospitals
Trigger Tool 720 ADEsSubset: 1,040 Patients in 9 hospitals
Trigger Tool 274 ADEsVoluntary Report 5 ADEs
ADE Trigger Tool Origins

10
Purpose:
• Develop and test a pediatric-focused trigger tool.
• Determine the rate of adverse drug events (ADEs) in hospitalized children at 12 freestanding children’s hospitals in the United States
• Identify characteristics of ADEs in children’s hospitals to provide the basis for developing a strategy to prevent drug-related harm in hospitalized children.
CHAI/CHCA Pediatric ADE Trigger Tool

11
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 1Antidote Use• Diphenhydramine• Vitamin K• Flumazenil• Antiemetic• Naloxone• Sodium polystyrene
DroperidolAnti-diarrheals
Other• Oversedation/lethargy/
fall/hypotension• Rash
Abnormal Lab Value• PTT > 100 seconds• Rising Serum Creatinine
HypoglycemiaC. difficile (+) stoolINR > 6LeukopeniaThrombocytopenia↑ Digoxin↑ Lidocaine↑ Gentamicin or Tobramycin↑ Amikacin↑ Vancomycin level
• Abrupt medication stopTransfer to higher level of care
12
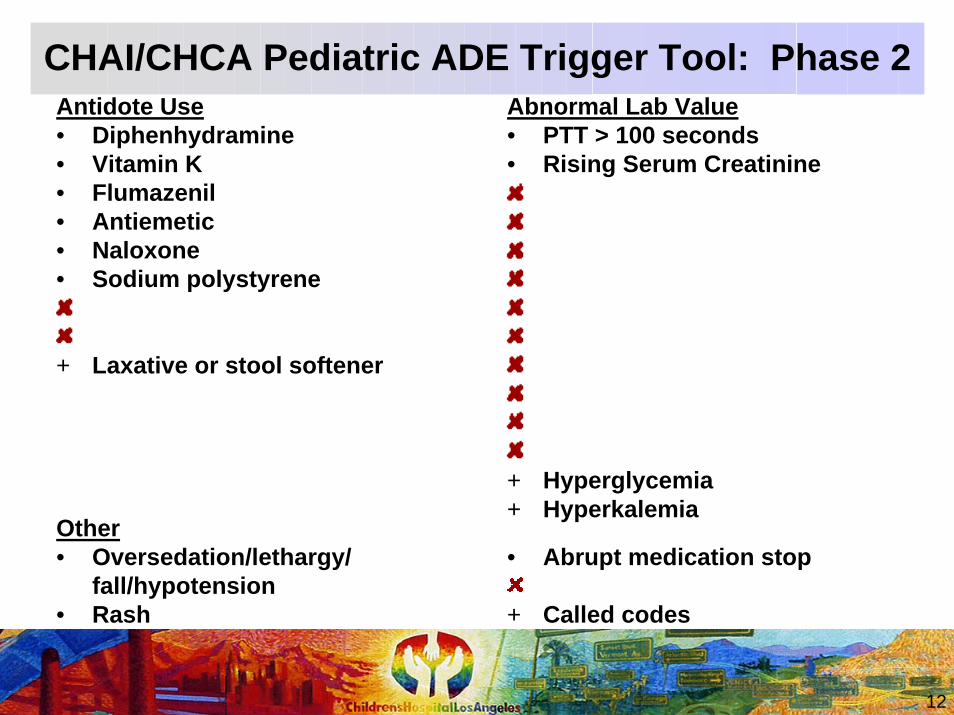
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 2Antidote Use• Diphenhydramine• Vitamin K• Flumazenil• Antiemetic• Naloxone• Sodium polystyrene
+ Laxative or stool softener
Other• Oversedation/lethargy/
fall/hypotension• Rash
Abnormal Lab Value• PTT > 100 seconds• Rising Serum Creatinine
+ Hyperglycemia+ Hyperkalemia
• Abrupt medication stop
+ Called codes

13
• 12 Free-Standing Children’s Hospitals• Training• Random Chart Selection
4 consecutive two-week periods20 charts randomly selected each two-week period at each hospital
• Exclusion CriteriaHospital stay <2 daysNewborn nursery stayObstetrics serviceDay hospital or observation unit
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 2

14
960 Patients in 12 Children’s Hospitals
Trigger Tool 89 ADEsVoluntary Report* 4 ADEs
Total† 107 ADEs*All 4 voluntary report ADEs were identified by the Trigger Tool.†18 additional ADEs not associated with a trigger were identified
while using the Trigger Tool.
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 2
7.29% of all patients experienced an ADE.
Trigger Tool 13.1 ADEs/1000 pt-daysVoluntary Report 0.59 ADEs/1000 pt-days
Total 15.7 ADEs/1000 pt-days

15
The rate of adverse drug events experienced by hospitalized children is higher than previously reported.
Medication-Related Harm in US Children’s Hospitals
Study Year ADE Detection Method
ADEsper 100
admissions
Takata(2008)
2002 Manual Pediatric ADE Trigger & Incident Reports
11.1
Kaushal(2001)
1999 Chart Review & Incident Reports
2.3
Holdsworth(2003)
2000-2001 Chart Review & Staff Interviews
6.4

16
Trigger Positive Predictive Values
All Triggers 3.73%
Polystyrene 20.0% Serum creatinine 3.8%Medication stop 19.7% Hyperkalemia 3.6%
PTT 16.7% Laxative 2.8%Oversedation 14.9% Vitamin K 1.8%
Codes 14.3% Antiemetic 1.5%Rash 12.7% Hyperglycemia 0.6%
Naloxone 12.1% Flumazenil 0.0%Diphenhydramine 8.4%
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 2
17
Chronic DiagnosesPrinciple DiagnosisAdmission DateDischarge DateGestational AgeDate of BirthInitial UnitCommunication BarrierTotal Transfers between Units
In addition:Number of TriggersNumber of ADEsTotal MedicationsTotal DosesTime to Review ChartChart Reviewer Type
Patient-Level Characteristics
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 2

18
TriggerADE DateHow ADE IdentifiedUnit of ADE OccurrenceADE OutcomeMedication InvolvedIntervention
ADE SeverityPreventable?Identified Earlier?Mitigated Better?ADE ProcessMedication Error Type
ADE Characteristics
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 2

19
Conclusions
• The Pediatric ADE Trigger Tool identified more ADEs than voluntary reporting 22 times more.
• 1 of 15 hospitalized children experienced an ADE.
• 1 of 5 ADEs were preventable.
• Opportunities for Improvement:Narcotics & antibiotic usageMonitoring & prescribing/ordering
CHAI/CHCA Pediatric ADE Trigger Tool: Phase 2

20
An Intervention to Decrease Narcotic-Related Adverse Drug Events in Children’s Hospitals (Sharek, 2008):
Interventions Narcotic-related ADE rates ↓ 67%Based on Narcotic-Related ADE Trigger Tool
Antiemetic useNaloxone useOversedation, lethargy, fallsAbrupt cessation of narcoticAdministration of laxatives or enemasAdministration of diphenhydramineIntubation/respiratory arrestCombination of ≥3 narcotics ordered
Is the Outcome the Trigger Tool? No!

21
Measurement ChallengesWhat is the gold standard for ADE detection? Sensitivity? Specificity?Optimal thresholds?Are positive predictive values enough? (Handler, 2007)Cost-effectiveness?
How dependent are ADE trigger tools on the operator?Phansalkar (2007): 0.23 ADEs identified/admit by pharmacists versus 0.12 ADEs identified/admit by non-pharmacists
Resources to utilize ADE TriggersFerranti (2008): 2 dedicated clinical pharmacists to follow-up 57 automated ADE triggers at an academic medical centerJha (1998): voluntary report 5 h/wk 23 ADEs; chart review 55 h/wk 398 ADEs; computer monitoring 11 h/wk 275 ADEs
ADE Trigger Tool Challenges

22
How do we automate triggers, in particular those not related to medication use or laboratory values? Will natural language triggers work?
Melton (2005): sensitivity 25% and specificity 99.96%Cantor (2007): sensitivity 31% and specificity 98%CHLA (2010): testing prohibited abbreviation triggers in EMR
Real-time trigger interventionRaschke (1998): Physicians notified for increased ADE risk situations 53% true positive 44% unrecognized by MDJha (2008): High-priority ADE alerts 38% true positive 11.3% MDs contacted & all unaware of event.Duncan (2006): PEWS (Pediatric Early Warning System) triggers Rapid Response Team
ADE Trigger Tool Challenges

23
*Ferranti, Horvath, Cozart, et al., 2008: Duke Children’s Hospital†Takata, Taketomo, Waite, 2008: California Pediatric Patient Safety
Initiative
Pediatric ADE Trigger Tool: Postlude
Study Year Manual or Automated
ADEsper 100
admissions
Takata(2008)
2002 Manual Pediatric ADE Trigger & Incident Reports
11.1
Ferranti* (2008)
2004-2006 Automated ADE Trigger & Incident Reports
3.5
Takata†
(2008)2003-2004 Automated Pediatric ADE
Trigger11.2
Automated ADE Trigger

24
5 California Children’s Hospitals (CHCF): Pediatric Patient Safety Surveillance SystemAutomated ADE Triggers: antidote and lab valuesPatients with Trigger: 53.9%Trigger Rate: 2.3 triggers/patientsPatients with ADE: 9.1%Trigger ADE Rate: 11.2 ADEs/100 patients
11 times higher than voluntary ADE rate
Positive Predictive Value (all triggers): Trigger level: 4.7% Patient level: 16.8%
CaPPSI Findings, Takata (AJHP 2008): Postlude

25
Patient safe practices
are
the right thing to do.

26
Cantor MN, Feldman HJ, Triola MM. Using trigger phrases to detect adverse drug reactions in ambulatory care notes. Qual Saf Health Care 2007;16:132-134.Classen DC, Pestotnik SL, Evans RS, et al. Computerized surveillance of adverse drug events in hospital patients. JAMA 1991;266:2847-2851.Ferranti J, Horvath MM, Cozart H, et al. Reevaluating the safety profile of pediatrics: a comparison of computerized adverse drug event surveillance and voluntary reporting in the pediatric environment. Pediatrics 2008;121:e1201-e1207.Jha AK, Kuperman GJ, Teich JM, Leape L, Shea B, Rittenberg E, Burdick E, Seger DL, Vliet MV, Bates DW. Identifying adverse drug events: development of a computer-based monitor and comparison with chart review and stimulated voluntary report. J Am Med Inform Assoc 1998;5:305-314.Jha AK, Laguette J, SegerA, Bates DW. Can surveillance systems identify and avert adverse drug events? A prospective evaluation of a commercial application. J Am Med Inform Assoc 2008;15:647-653.Handler SM, Altman RL, Perera S, Hanlan JT, Studenski SA, Bost JE, Saul MI, Fridsma DB. A systematic review of the performance characteristics of clinical event monitor signals used to detect adverse drug events in the hospital setting. J Am Med Inform Assoc 2007;14:451-458.Holdsworth MT, Fichtl RE, Behta M, et al. Incidence and impact of adverse drug events in pediatric inpatients. Arch Pediatr Adolesc Med 2003;157:60-65.Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA 2001;285:2114-2120.Larsen GY, Donaldson AE, Parker HB, Grant MJC. Preventable harm occurring to critically ill children. Pediatr Crit Care Med 2007;8:331-336.Matlow A, Flintoft V, Orrbine E, et al. The development of the Canadian paediatric trigger tool for identifying potential adverse events. Healthcare Quarterly 2005;8(special issue):90-93.Duncan H, Hutchison J, Parshuram CS. The pediatric early warning system score: a severity of illness core to predict urgent medical need in hospitalized children. Journal of Critical Care 2006;21:271-279.Melton GB, Hripcsak G. Automated detection of adverse events using natural language processing of discharge summaries. J Am Med Inform Assoc 2005;12:448-457.
References

27
Muething SE, Conway PH, Klonnenborg E, Lesko A, Schoettker PJ, Seid M, Kotagal U. Identifying causes of adverse events detected by an automated trigger tool through in-depth analysis. Qual Saf Health Care2010Aug 25 [Epub ahead of print].Phansalkar S, Hoffman JM, Nebeker JR, Hurdle JF. Pharmacists versus nonpharmacists in adverse drug event detection: a meta-analysis and systematic review. Am J Health-Syst Pharm 2007;64:842-849.Raschke RA, Gollihare B, Wunderlich TA, Guidry JR, Leibowitz AI, Peirce JC, Lemelson L, Heisler MA, SusonC. A computer alert system to prevent injury from adverse drug events: development and evaluation in a community teaching hospital. JAMA 1998;280:1317-1320.Rozich JD, Haraden CR, Resar RK. Adverse drug event trigger tool: a practical methodology for measuring medication related harm. Qual Saf Health Care 2003;12:194-200.Sharek PJ, Horbar JD, Mason W, et al. Adverse events in the neonatal intensive care unit: development, testing, and findings of an NICU-focused trigger tool to identify harm in North American NICUs. Pediatrics 2006;118:1332-1340.Sharek PJ, McClead RE, Taketomo C, et al. An intervention to decrease narcotic-related adverse drug events in children's hospital. Pediatrics 2008;122:e861-e866.Sikdar KC, Alaghehbandan R, MacDonald D, Barrett B, Collins KD, Gadag V. Adverse drug events among children presenting to a hospital emergency department in Newfoundland and Labrador, Canada. Pharmacoepidemiolgoy and Drug Safety 2010;19:132-140.Stockwell DC, Kane-Gill SL. Developing a patient safety surveillance system to identify adverse events in the intensive care unit. Crit Care Med 2010;38[Suppl.]:S117-S125.Takata GS, Mason W, Taketomo C, et al. Development, testing, and findings of a pediatric-focused trigger tool to identify medication-related harm in US children’s hospitals. Pediatrics 2008;121:e927-e935.Takata GS, Taketomo CK, Waite S. Characteristics of medication errors and adverse drug events in hospitals participating in the California Pediatric Patient Safety Initiative. Am J Health-Syst Pharm 2008;65:2036-2044.Wang X, Hripcsak G, Markatou M, Friedman C. Active computerized pharmacoviligance using natural language processing, statistics, and electronic health records: a feasibility study. J Am Med Inform Assoc. 2009;16:328 –337.
References