development & structure of thyroid gland · pdf filehistogenesis of thyroid gland....
TRANSCRIPT


DEVELOPMENT & STRUCTURE
OF THYROID GLAND
DR TATHEER ZAHRA
ASSISTANT PROFESSOR ANATOMY

DEVELOPMENT OF THYROID
Concept of pharyngeal arch
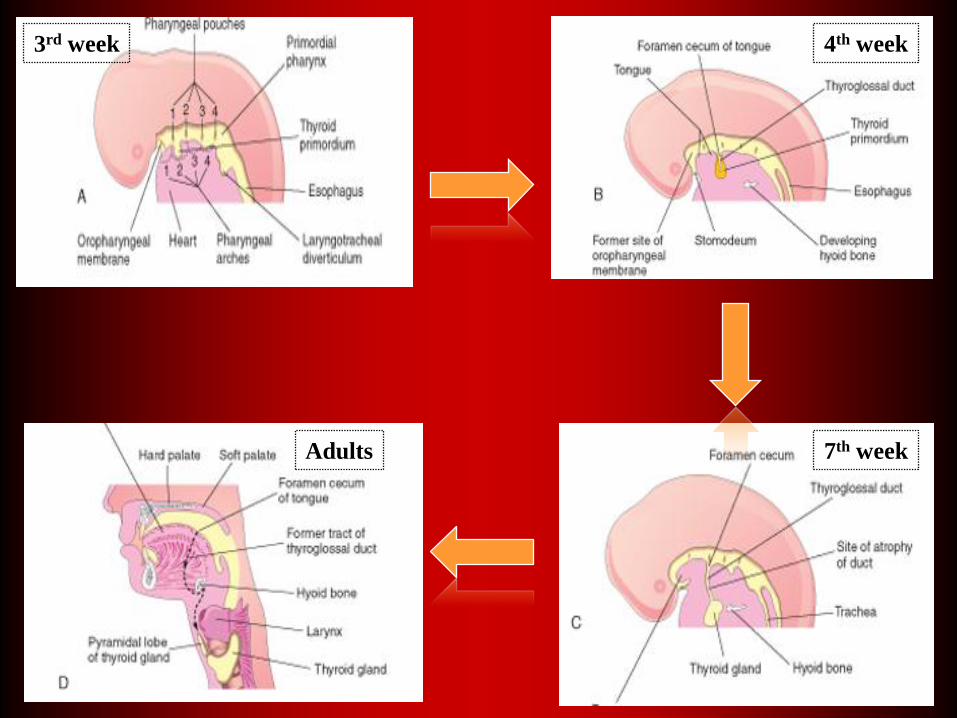
4th week
7th weekAdults
3rd week

DEVELOPMENT OF FOLLICULAR CELLS
7TH WEEK: Solid cord of cells breaks into
network of epithelial cells as invaded by vascular
mesenchyme
10TH WEEK: Cellular groups formation, Lumen
formation
11TH WEEK: Colloid formation
20TH WEEK: level of TSH ↑, Adult levels by 35th
week
HISTOGENESIS OF THYROID
GLAND

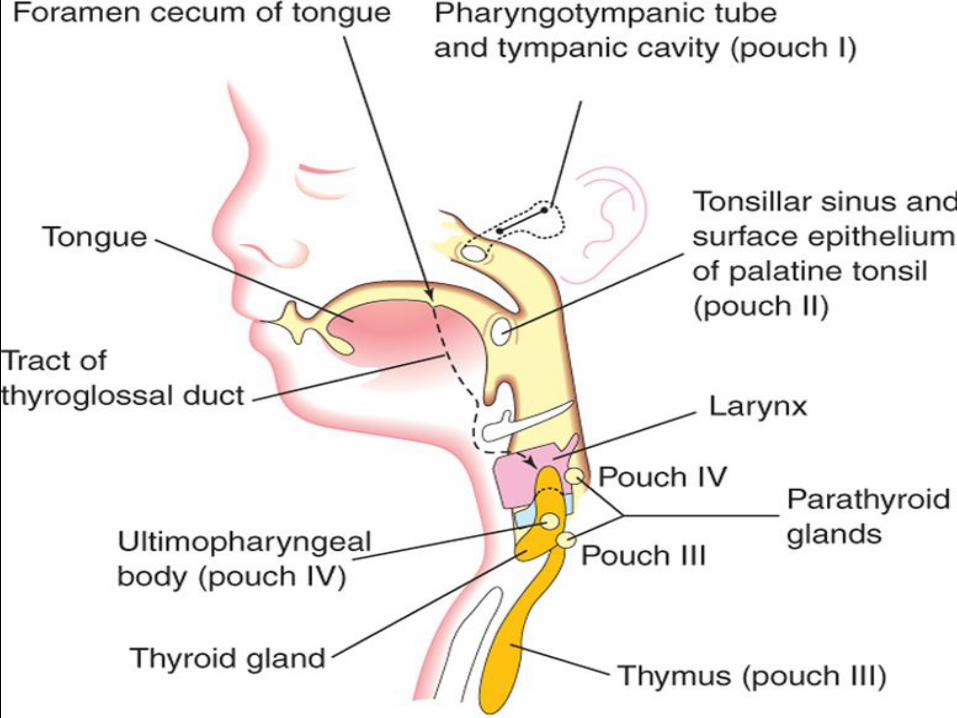
DEVELOPMENT OF
PARAFOLLICULAR CELLS
4th or 5th
pharyngeal pouch
Ultimobranchial
body
Neural crest cells
origin

Ultimopharyngeal body / Ultimobranchial body

AGENESIS OF THE
THYROID GLANDDefective development of thyroid gland ~
Congenital hypothyroidism i.e. Cretinism
No central cause related to Hypothalamic-Pituitary
axis
Absence of gland or one of its lobes ~ Rare
anomaly
Thyroid Hemiagenesis ~ Left lobe most commonly
Mutations in the receptors for TSH is involved in
some cases

PYRAMIDAL LOBE
40% population
Usually to the left of
midline
Levator glandulae
thyroideae
Innervated by branch
of external laryngeal
nerve


THYROGLOSSAL DUCT
CYSTSAsymptomatic ~ unless the
lesion become infected
Painless, progressively
enlarging swelling
Appear in childhood,
adolescence or young
adults
Treatment: Surgery with
removal of hyoid bone

POSSIBLE LOCATIONS OF
THYROGLOSSAL CYSTS

THYROGLOSSAL SINUS &
FISTULA

ABERRANT/ ECTOPIC THYROID
GLAND

ACCESSORY THYROID TISSUE

GROSS STRUCTURE OF
THYROID
Only endocrine gland to
store its secretions
Location & extent
Shape
Length: 5 cm
Width: 2.5 cm
Weight: 25-30 g
True Capsule
Pretracheal fascia covering

RELATIONS OF THE LOBES
ANTEROLATERALLY
POSTEROLATERALLY
MEDIALLY


RELATIONS OF THE ISTHMUS
ANTERIORLY
POSTERIORLY

WHY SWELLINGS OF THYROID
GLAND MOVE WITH SWALLOWING?

THYROID GLAND & AIRWAY

ARTERIAL SUPPLY
Superior thyroid
artery (Anterior &
posterior branches)
Inferior thyroid
artery
Stroma richly
vascularized
Vessels lie between
true & false capsule



RELATIONSHIP OF NERVES WITH
THYROID ARTERIES & THEIR DAMAGE
Superior Thyroid Artery Ligation: Close to gland
Inferior Thyroid Artery Ligation: Lateral to gland

INJURY TO THE RECURRENT & NON
RECURRENT LARYNGEAL NERVES
Blood accumulation and serous exudate after the operation ~ Pressure
effects & nerve compression
Non-recurrent laryngeal nerve (due to lack of normal subclavian
artery) 1% incidence ~ Possible hazard in thyroidectomy

A:Weakness of voice
B: Speech not greatly
affected; Hoarseness of
voice; temporary aphonia or
disturbance of phonation
(voice production) and
laryngeal spasm
C: Impaired breathing,
speech lost
D: Greater degree of
paralysis of abductors
E: Dyspnea & stridor; Needs
cricothyroidotomy or
tracheostomy

VENOUS DRAINAGE


LYMPHATIC DRAINAGE
DEEP CERVICAL
NODES
PRELARYNGEAL
PRETRACHEAL
PARATRACHEAL
THORACIC
DUCT
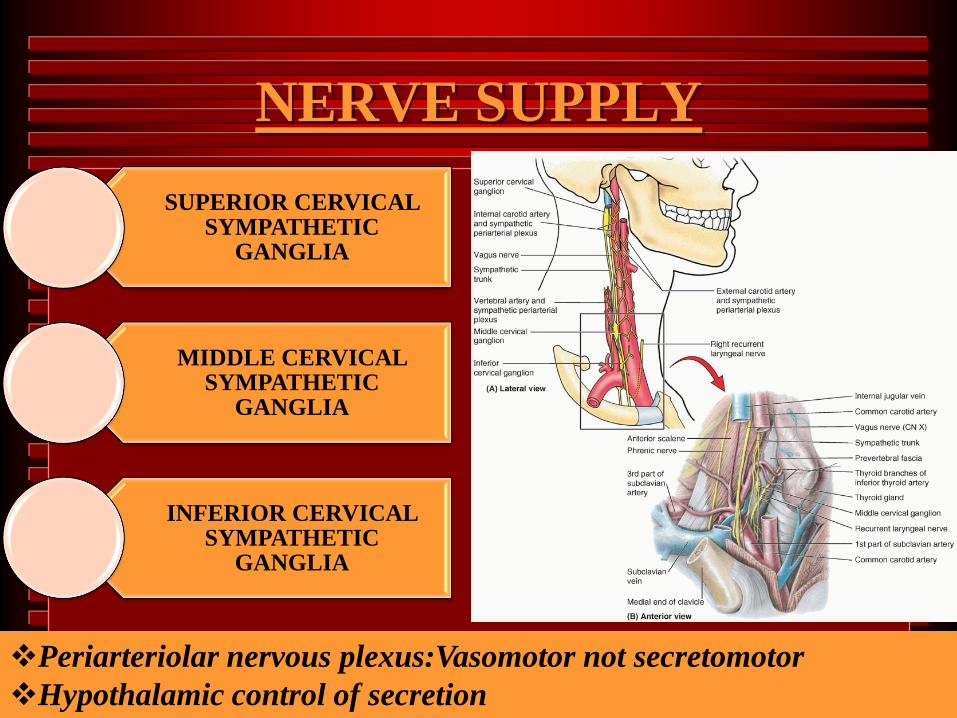
NERVE SUPPLY
SUPERIOR CERVICAL SYMPATHETIC
GANGLIA
MIDDLE CERVICAL SYMPATHETIC
GANGLIA
INFERIOR CERVICAL SYMPATHETIC
GANGLIA
Periarteriolar nervous plexus:Vasomotor not secretomotor
Hypothalamic control of secretion

FUNCTIONS & REGULATION OF
SYNTHESIS OF THYROID HORMONES


ENLARGEMENT OF
THYROID GLAND
PHYSIOLOGICAL(e.g., during
menstruation & pregnancy)
PATHOLOGICAL e.g., GOITER
(HYPOTHYROIDISM/ HYPERTHYROIDISM)

HYPOTHYROIDISM
CONGENITAL HYPOTHYROIDISM/
CRETINISM
IODINE DEFICIENCY GOITER/ ENDEMIC
THYROID
AUTOIMMUNE/ HASHIMOTO’S THYROIDITIS
ADULT HYPOTHYROIDISM/
MYXEDEMA

HYPERTHYROIDISM/ TOXIC
GOITER/ GRAVES’ DISEASE
Exophthalamic goiter
Autoantibodies
Treatment options:
Surgery
Radiotherapy
Radioactive iodine
ingestion

EXTENT & MECHANICAL EFFECTS OF
GOITER
Attachment of sternothyroid muscle
Limits upward extension
No limit to downward expension behind sternum
Enlarges anteriorly, posteriorly, inferiorly, or
laterally
Retrosternal or substernal more common
Compression of trachea ~ Dyspnea
Severe venous compression

SURGICAL APPROACH OF
THYROID GLAND
TRANSVERSE INCISION IN A LOW SKIN CREASE ON THE FRONT OF NECK
VERTICAL DIVISION OF INVESTING FASCIA
RETRACTION / DIVISION OF STERNOHYOID & STERNOTHYROID MUSCLES
DIVISION OF PRETRACHEAL FASCIA TO EXPOSE GLAND PROPER

LOBECTOMY &
ISTHUMUSECTOMY

TOTAL THYROIDECTOMY

NEAR TOTAL & SUBTOTAL
THYROIDECTOMY

SURFACE ANATOMY OF
THYROID GLAND
Extent of gland: C5-T1 Vertebrae
Isthmus: 2nd, 3rd & 4th tracheal rings
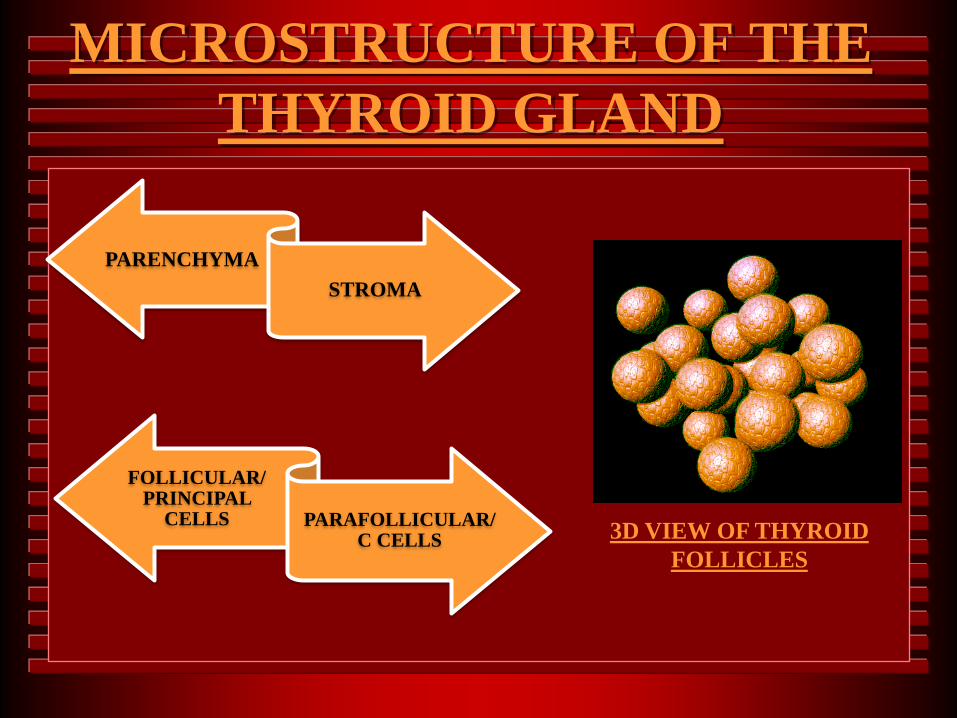
MICROSTRUCTURE OF THE
THYROID GLAND
PARENCHYMA
STROMA
3D VIEW OF THYROID
FOLLICLES
FOLLICULAR/ PRINCIPAL
CELLS PARAFOLLICULAR/ C CELLS

PARENCHYMA & STROMA

FOLLICULAR CELLS
PRINCIPAL/ CHIEF CELLS

PARAFOLLICULAR CELLS
C CELLS/ CALCITONIN CELLS

HYPOACTIVE & HYPERACTIVE
VS. EUTHYROID STAGE
Hypoactive stage: Simple squamous
epithelium lined follicle filled with colloid
Hyperactive stage: Simple columnar
epithelium lined follicle with ↓ in colloid
Euthyroid stage: Simple cuboidal
epithelium + colloid
The height of the follicular cells is directly
proportional to the glandular activity.

REFERENCES
The Developing Human, Clinically Oriented Embryology,
By KEITH L. MOORE - Latest Edition
LANGMAN’S Embryology, By T.W.SADLER - Latest
Edition
LAST’S Anatomy Regional & Applied, By CHUMMY S.
SINNATAMBY - Latest Edition
Clinically Oriented Anatomy, By KEITH L. MOORE -
Latest Edition
Clinical Anatomy By Regions, By RICHARD S. SNELL -
Latest Edition
Basic Histology Text & Atlas, By LUIZ CARLOS
JUNQUEIRA & JOSé CARNEIRO - Latest Edition
