developmental delay and multiple congenital anomalies in a child with a unique combination of...
TRANSCRIPT

130 Developmental Medicine & Child Neurology 2001, 43: 130–132
Developmental delayand multiplecongenital anomaliesin a child with aunique combination ofpartial monosomy 18and partial trisomy 16
Nicole Schmidt MD, Department of Pediatrics;
Don C Van Dyke* MD, Division of Developmental
Disabilities;
Kim Keppler-Noreuil MD;
Ann Muilenburg RN MA;
Shivanand Patil PhD;
Adam B Kanis MD PhD, Division of Medical Genetics,
Children’s Hospital of Iowa, Iowa, USA.
*Correspondence to second author at Division of
Developmental Disabilities, University Hospital School, The
University of Iowa Hospitals and Clinics, 100 Hawkins Drive,
Room 213, Iowa City, IA 52242, USA.
E-mail: [email protected]
A male child with multiple congenital anomalies anddevelopmental delay is described. Cytogenetic evaluationshowed that the patient was partially monosomic for the shortarm of chromosome 18 and partially trisomic for the short armof chromosome 16: a combination of chromosomal syndromesnot previously described.
Deletion of the short arm of chromosome 18 (monosomy 18p)
was first described by de Grouchy and colleagues in 1963.
Since then, more than 100 cases of monosomy 18p have been
reported in the literature. Trisomy 16p, first described by Yunis
and coworkers (1977) and Roberts and Duckett (1978), is an
extremely rare event, but is usually compatible with life
(Golden et al. 1981). The combination of these two chromoso-
mal syndromes as presented in this case has not been previ-
ously described in the literature.
Case reportA male infant with multiple congenital anomalies was born at
37 weeks to unrelated parents who had no significant med-
ical or past family history. The couple had one previous preg-
nancy that ended in miscarriage at 4 to 6 weeks’ gestation.
The mother had a healthy 30-month-old male infant from a
previous relationship. The pregnancy was without complica-
tion. Upon spontaneous rupture of membranes the amniotic
fluid was found to be meconium-stained. The infant was
delivered by Cesarean section due to breech positioning.
Apgars were 7 at one minute and 9 at five minutes. There was
mild to moderate respiratory distress requiring continuous
positive airway pressure.
Examination revealed a 2620g appropriate-for-gestational-
age infant with an abnormal helical pattern of the pinna and
low-set ear position, syndactyly of toes 2, 3, and 4 bilaterally,
Case report
with overlapping of toes 4 and 5 on the right, and hypoplastic
nails. There was a single palmar crease on the left hand. Head
circumference was 32cm (3 to 5%) and length was 46cm (3 to
50%). There was micrognathia, midline cleft palate, sacral dim-
ple, and severe hypospadias with bifid scrotum. A heart mur-
mur was present. Echocardiogram revealed tetralogy of Fallot
with a large ventricular septal defect, overriding aorta, small
pulmonary artery, and probable valvular/subvalvular obstruc-
tion. The ophthalmology examination revealed telecanthus,
bilateral microcornea, and hyperopia. The renal ultrasound
was normal. An endocrinology evaluation revealed normal
thyroid functions, normal cortisol and insulin levels, and mild-
ly decreased growth hormone (5.1ng/mL). Head CT revealed
an abnormal gyral pattern in the cerebrum with an abnormal
amount of subarachnoid space, particularly posteriorly. MRI
was not performed.
Karyotypes by the G-banded chromosomes were prepared
from a peripheral blood sample using the standard procedure.
The patient’s karyotype (Fig.1) revealed 46, XY, der(18)t
(16;18)(p11.2; p11.2)pat. The derivative chromosome 18 was
partially monosomic for the short arm of chromosome 16 and
partially trisomic for the short arm of chromosome 18. The
mother had a normal karyotype.The father's karyotype revea-
led 46, XY, t(16;18)(p11.2; p11.2). All cells contained an appar-
ently balanced translocation between the short arm of chromo-
some 16 and the short arm of chromosome 18.
The initial hospital course was complicated by episodes of
respiratory distress and cyanosis, and significant gastroe-
sophageal reflux with aspiration. The patient had bilateral
inguinal hernias that required surgical repair. He underwent a
tracheotomy for airway management. A Nissen fundoplica-
tion and gastrostomy tube placement were performed. He
failed his hearing screen. Later evaluation showed moderate
to severe hearing loss in the left ear and moderate hearing loss
in the right ear. Baseline oxyhemoglobin saturation in room
air was 70 to 80%, with intermittent self-limited cyanotic
episodes during which oxyhemoglobin saturation dropped to
50%. At the time of discharge the patient was on total gastros-
tomy tube feedings with stable respiratory status on room air.
DiscussionThis infant has monosomy for most of the short arm of chromo-
some 18 and trisomy for most of the short arm of chromosome
16 (Fig. 1). Both trisomy 16p and monosomy 18p have been
reported separately in the literature (de Grouchy et al. 1963,
Uchida et al. 1965, de Grouchy 1969, Schinzel et al. 1974, de
Grouchy and Turleau 1976, Rethore 1977, Yunis et al. 1977,
Roberts and Duckett 1978, Dallapiccola et al. 1979, Leschot et
al. 1979, Golden et al. 1981). The combination of trisomy 16
and monosomy 18p has not been previously reported.
The primary clinical features of individuals with 16p trisomy
are a small round skull, prominent maxilla, low-set ears,
micrognathia, thumb abnormalities, and overlapping fingers
and toes (de Grouchy and Turleau 1976, Leschot et al. 1979,
Golden et al. 1981). Three cases of congenital heart disease
have been described including two cases of tetratology of
Fallot (Leschot et al. 1979). Mental impairment is usually very
severe (Dallapiccola et al. 1979, Leschot et al. 1979). Autistic
features and tics have also been described (Hebebrand et al.
1994). Feeding difficulties, seizures, abnormal tone, and
poor reflexes are reported in the postnatal period (Roberts
and Duckett 1978, Leschot et al. 1979). In half of the cases
the infants die within the first year of life, with the oldest
reported child being over 11 years of age (de Grouchy and
Turleau 1976, Leschot et al. 1979).
Over 100 cases of monosomy 18p have been reported, most
of which occur de novo. The phenotype of ‘18p– syndrome’
varies widely, but usually includes failure to thrive, mental
retardationa, and some characteristic dysmorphisms as
reviewed in Table I (Uchida et al. 1965, de Grouchy and
Turleau 1976, Zumel et al. 1989, Telvi et al. 1995). Other
abnormalities include nystagmus, cataracts, patent ductus
arteriosus, aortic stenosis and ventricular hypertrophy (de
Grouchy and Turleau 1976), neonatal hypotonia, torsion
Case Report 131
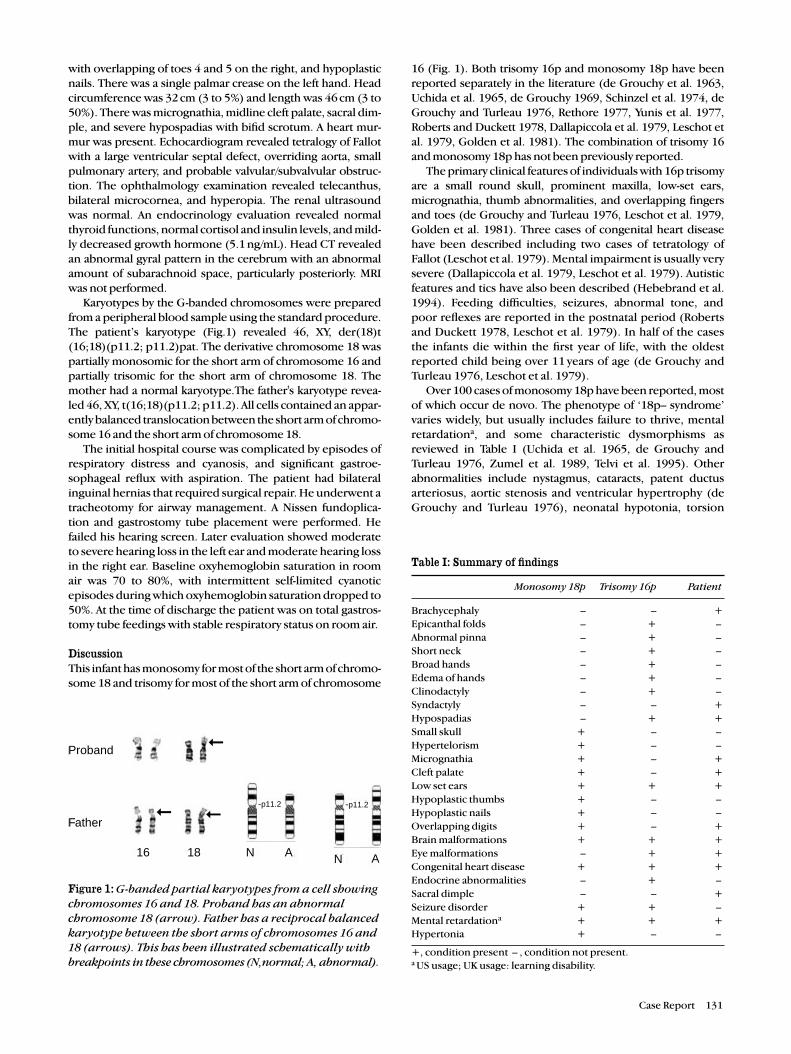
Figure 1: G-banded partial karyotypes from a cell showingchromosomes 16 and 18. Proband has an abnormalchromosome 18 (arrow). Father has a reciprocal balancedkaryotype between the short arms of chromosomes 16 and18 (arrows). This has been illustrated schematically withbreakpoints in these chromosomes (N,normal; A, abnormal).
Table I: Summary of findings
Monosomy 18p Trisomy 16p Patient
Brachycephaly – – +
Epicanthal folds – + –
Abnormal pinna – + –
Short neck – + –
Broad hands – + –
Edema of hands – + –
Clinodactyly – + –
Syndactyly – – +
Hypospadias – + +
Small skull + – –
Hypertelorism + – –
Micrognathia + – +
Cleft palate + – +
Low set ears + + +
Hypoplastic thumbs + – –
Hypoplastic nails + – –
Overlapping digits + – +
Brain malformations + + +
Eye malformations – + +
Congenital heart disease + + +
Endocrine abnormalities – + –
Sacral dimple – – +
Seizure disorder + + –
Mental retardationa + + +
Hypertonia + – –
+, condition present – , condition not present.a US usage; UK usage: learning disability.
Proband
Father
16 18 N A N A
-p11.2 -p11.2➞
➞
➞

dystonia (Awaad et al. 1999, Klein et al. 1999), autoimmune
endocrinopathy complex and serum IgA deficiency (Artman
et al. 1992), hypogonadism, and skeletal malformations (de
Grouchy and Turleau 1976, Telvi et al. 1995). Although cogni-
tive deficits are usually in the moderate range, many affected
individuals have only mild mental retardation, with 10% of
individuals sustaining severe brain malformations such as
holoprosencephaly, agenesis of the corpus callosum, and
hydrocephalus (de Grouchy et al. 1969). The life expectancy
of these individuals is not markedly diminished, with one per-
son in the literature as old as 61 years (de Grouchy and
Turleau 1976).
The present patient shows major abnormalities as might be
expected of both monosomy 18p and trisomy 16p. Findings
such as midfacial hypoplasia and low-set ears, though sugges-
tive of monosomy 18p, are seen in many chromosomal anom-
alies. Other common findings with monosomy 18p are hypo-
spadias, congenital heart disease, eye and brain malforma-
tions, and developmental delay. Features seen in this infant
which are strongly suggestive of those found in trisomy 16 are
micognathia, overlapping digits, congenital heart disease, cleft
palate, and developmental delay.
The infant's medical condition has been stable for the last 10
months, and at age 13 months he demonstrates developmental
delays but requires no major medical interventions. This is
more compatible with monosomy 18p than with trisomy 16p
in which half of the children die in the first year of life. How-
ever, the infant's respiratory status, heart disease, brain malfor-
mations, and risk of seizures place him at risk for complications
and early death.
Accepted for publication 25th August 2000.
ReferencesArtman HG, Morris CA, Stock AD. (1992) 18p– syndrome and
hypopituitarism. Journal of Medical Genetics 29: 671–2.Awaad Y, Munoz S, Nigro M. (1999) Progressive dystonia in a child
with chromosome 18p deletion, treated with intrathecalbaclofen. Journal of Child Neurology 14: 75–7.
Dallapiccola B, Curatolo P, Balestrazzi P. (1979) ‘De novo’ trisomy16q11 to pter. Human Genetics 49: 1–6.
de Grouchy J. (1969) The 18p–, 18q–, and 18r syndromes. BirthDefects Original Articles Series 5: 74–87.
— Turleau C. (1976) Clinical Atlas of Human Chromosomes, 2ndEdn. New York: John Wiley.
— Lamy M, Thieffry S, Arthuis M, Salmon C. (1963) Dysmorphiecomplexe avec oligophrenie: deletion des bras courts d’unchromosome. Comptes Rendus de l’Academie des Sciences256: 1028–9. (In French).
Golden NL, Bilenker R, Johnson WE, Tischfield JA. (1981)Abnormality of chromosome 16 and its phenotypic expression.Clinical Genetics 19: 41–5.
Hebebrand J, Marin M, Korner J, Roitzheim B, de Braganca K,Werner W, Remschmidt H. (1994) Partial trisomy 16p in anadolescent with autistic disorder and Tourette’s syndrome.American Journal of Medical Genetics 54: 268–70.
Klein C, Page CE, LeWitt P, Gordon MF, de Leon D, Awaad Y,Breakefield XO, Brin MF, Ozelius LJ. (1999) Genetic analysis ofthree patients with an 18p– syndrome and dystonia. Neurology52: 649–51.
Leschot NJ, De Nef JJ, Geradets JPM, Becker-Bloemkok MJ, Talma A,Bijsma JB, Verjaal M. (1979) Five familial cases with trisomy 16psyndrome due to translocation. Clinical Genetics 16: 205–14.
Rethore MO. (1977) Chromosome deletions and ring chromosomessyndrome. In: Myrianthopoulos ND, editor. Handbook ofClinical Neurology. Vol. 31, Part II. Amsterdam: North Holland.p 549–620.
Roberts SH, Duckett DP. (1978) Trisomy 16p in a liveborn infant anda review of partial and full trisomy 16. Journal of MedicalGenetics 15: 375–81.
Schinzel A, Schmid W, Luscher U, Naer M, Brook C, Steinmann B.(1974) Structural aberrations of chromosome 18: I. The 18p–syndrome. Archiv für Genetik 47: 1–15.
Telvi L, Bernheim A, Ion A, Fouquest F, LeBouc Y, Chaussain JL.(1995) Gonadal dysgenesis in del(18p) syndrome. AmericanJournal of Medical Genetics 57: 598–600.
Uchida IA, McGae KN, Want HC, Ray M. (1965) Familial short armdeletions of chromosome 18 concomitant with arrhinencephalyand alopecia congenitalis. American Journal of Human Genetics17: 410–9.
Yunis E, Gonzalez JT, Torres de Caballero OM. (1977) Partial trisomy16q–. Human Genetics 38: 347–50.
Zumel RM, Darnaud MT, Delicado A, Diaz de Bustamante A, deTorres ML, Lopez-Pajares I. (1989) The 18p– syndrome. Report offive cases. Annales de Genetique 32: 160–3.
132 Developmental Medicine & Child Neurology 2001, 43: 130–132