diabete ed asa: cosa c è di nuovo? - benvenuti nel sito ... · università magna græcia di...
TRANSCRIPT

Università Magna Græcia di Catanzaro Dipartimento di Medicina Sperimentale e Clinica
Cattedra di Medicina Interna ed U.O. Malattie Cardiovascolari
Scuola di Specializzazione in Geriatria
Prof. Francesco Perticone [email protected]
Diabete ed ASA:
cosa c’è di nuovo?



* P<0.0001
2
4
6
8
Uri
c ac
id,
mg
/dl
0
*
2
4
6
8
Hs-
CR
P, m
g/L
*
NGT IGT DM
<155 >155
0
0
0,4
0,8
1,2
1,6
2
0 100 200 300 400 500 600 700 800 900
0.001
0.012
0.340 0.799
0.355 0.192 0.124 0.090 0.071
HR
(p
lus u
ric a
cid
1 g
/d
L in
cre
ase
)
ACh % of increase
Ac. Urico, Funzione Endoteliale e Diabete
Ac. Urico e Glicemia
Perticone F et al, Int J Cardiol 2011
Perticone F et al, Int J Cardiol 2012

Endothelial dependent vasodilation after ASA treatment in diabetics
Re
acti
ve H
ype
rem
ic In
dex
0 1 4 weeks Wash out
*
* P=<0.0001

Box and whisker plots of urinary excretion of 11-dehydro-thromboxane (TX)B2 n healthy patients and in type 2 diabetic
patients.
Santilli F. et al. J Am Coll Cardiol 2006;47:391–7.

11-dehydro-TXB2n 20 type 2 diabetic patients before and after improved metabolic control.
Santilli F. et al. J Am Coll Cardiol 2006;47:391–7.

ATC, BMJ 2002; 324: 71-86
METAANALYSIS FROM THE ANTITHROMBOTIC
TRIALISTS' COLLABORATION (2002)


— Recommendations for primary prevention of CVD in people with diabetes. Antiplatelet agents
Aspirin therapy (75–162 mg/day) should be recommended as a primary prevention strategy in those with diabetes at increased cardiovascular risk, including those who are >40 years of age or who have additional risk factors (family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria).
People with aspirin allergy, bleeding tendency, existing anticoagulant therapy, recent gastrointestinal bleeding, and clinically active hepatic disease are not candidates for aspirin therapy. Other antiplatelet agents may be a reasonable alternative for patients with high risk.
Aspirin therapy should not be recommended for patients under the age of 21 years because of the increased risk of Reye’s syndrome associated with aspirin use in this population. People under the age of 30 years have not been studied.

Ogawa, H. et al. JAMA 2008;300:2134-2141.
Participation in Japanese Primary Prevention of Atherosclerosis With Aspirin for Diabetes (JPAD) Trial

Ogawa, H. et al. JAMA 2008;300:2134-2141.
Atherosclerotic Events

Ogawa, H. et al. JAMA 2008;300:2134-2141.
Total Percentage of Atherosclerotic Events According to Treatment Group
Ogawa, H. et al. JAMA 2008;300:2134-2141.
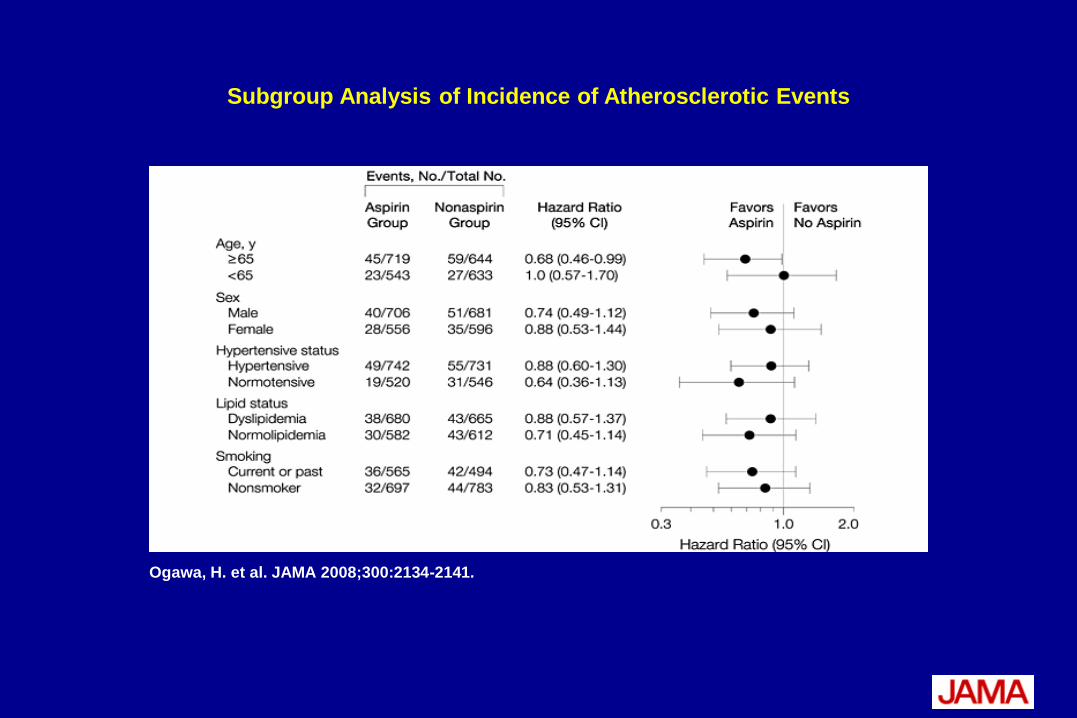
Subgroup Analysis of Incidence of Atherosclerotic Events

Ogawa, H. et al. JAMA 2008;300:2134-2141.
Adverse Effects

Belch, J. et al. BMJ 2008;337:a1840
POPADAD trial: Progress of participants in trial

0,0
5,0
10,0
15,0
20,0
25,0
Composite end point
Aspirin
No Aspirin
%
PRIMARY END POINTS:
0,05,0
10,015,020,025,0
Death from coronary heart disease or stroke
Aspirin
No Aspirin%
Variables Aspirin (n=638) No aspirin (n=638) Effect estimate* (95% CI)
P value
Composite end point
116 (18.2) 117 (18.3) 0.98 (0.76 to 1.26) 0.86
Death from coronary heart disease or stroke
43 (6.7) 35 (5.5) 1.23 (0.79 to 1.93) 0.36
*
*Death from coronary heart disease or stroke, non-fatal myocardial infarction or stroke, or above
ankle amputation for critical limb ischaemia.

%
SECONDARY END POINTS:
0,02,04,06,0
Coronary Heart Disease Death
Aspirin
No Aspirin%
0,0
0,5
1,0
1,5
2,0
Stroke Death
Aspirin
No Aspirin%
0,02,04,06,08,0
10,0
Non-fatal myocardial infarction
Aspirin
No Aspirin% 0,02,04,06,0
Non-fatal stroke
Aspirin
No Aspirin%
Variables Aspirin (n=638)
No aspirin (n=638)
Effect estimate* (95% CI)
P value
Death (any cause) 94 (14.7) 101 (15.8) 0.93 (0.71 to 1.24) 0.63
Coronary heart disease death 35 (5.5) 26 (4.1) 1.35 (0.81 to 2.25) 0.24
Stroke death 8 (1.3) 9 (1.4) 0.89 (0.34 to 2.30) 0.80
Non-fatal myocardial infarction 55 (8.6) 56 (8.8) 0.98 (0.68 to 1.43) 0.93
Non-fatal stroke 29 (4.6) 41 (6.4) 0.71 (0.44 to 1.14) 0.15

Belch, J. et al. BMJ 2008;337:a1840
Causes of death Aspirin plus antioxidant
(n=56)
Aspirin plus placebo (n=38)
Placebo plus antioxidant
(n=59)
Placebo plus placebo (n=42)
Myocardial infarction
11 10 8 5
Other coronary heart disease
4 10 7 6
Stroke:
Ischaemic 3 0 3 2
Haemorrhagic 2 0 1 2
Unknown cause 3 0 0 1
Other cardiac 5 0 4 1
Other vascular 3 1 2 2
Cancer 16 9 18 13
Trauma 0 0 2 0
Other 9 8 14 10
Cause of death in patients with diabetes according to
treatment group.

Belch, J. et al. BMJ 2008;337:a1840
Kaplan-Meier estimates in aspirin and no aspirin groups of proportion of patients who
experienced the composite end point of death from coronary heart disease or stroke, non-fatal myocardial infarction or stroke, or above ankle amputation for critical limb ischaemia;
and death from coronary heart disease or stroke.

Belch, J. et al. BMJ 2008;337:a1840
Kaplan-Meier estimates for aspirin and no aspirin groups of proportion of patients who
died from any cause, compared with proportion expected based on age and sex specific population rates for Scotland, 2002

Neri Serneri et al. EHJ 2004; 25:1845–1852
Picotamide, a combined inhibitor of thromboxane A2 synthase and receptor, reduces 2-year mortality in diabetics with peripheral arterial disease: the DAVID study
Randomised
n=1209
Assigned aspirin
n=606 (50.1%)
Assigned picotamide
n=603 (49.9%)
Lost to follow-up
n=26 (4.3%)
Lost to follow-up
n=32 (5.3%)
Completed trial
n=571 (94.7%)
Completed trial
n=580 (95.7%)
Study profile

DAVID t
rial: 2
-year
mor
tality
bene
fit
of
pico
tamide v
s ASA
Kaplan-Meier analysis of the time-to-death according to treatment assignment
Neri Serneri et al. EHJ 2004; 25:1845–1852

Type of event
Picotamide (n = 603) Aspirin
(n = 606)
n Cumulative
incidence (%) n
Cumulative incidence (%)
Myocardial infarction
(fatal and non-fatal) 15 2.9 19 3.6
Stroke (fatal and non-fatal) 14 2.7 12 2.2
Amputation 4 0.8 4 0.8
Other deaths 12 2.2 19 3.8
At least one event 43 53
Mortality and morbidity events by treatment groups: the DAVID Study
Neri Serneri et al. EHJ 2004; 25:1845–1852

PLA2
F2-Isoprostanes
TxA2
Gp IIb/IIIa
O2-
COX1
O2-
AA

PLA2
F2-Isoprostanes
TxA2
Gp IIb/IIIa
O2-
COX1
ASA
O2-
AA

Oxidative stress and platelet activation in diabetic patients
Diabetes 2012 C T2DM
ASA - + - + ASA - + - +
ASA - + - + ASA - + - +

PLA2
F2-Isoprostanes
TxA2
Gp IIb/IIIa
O2-
COX1
ASA
O2-
AA

Oxidative stress and platelet activation in diabetic patients
Diabetes 2012

Diabetes 2012
Platelet recruitment in diabetic patients

Conclusion
• Aspirin treatment alone is not sufficient to reduce cardiovascular events in diabetes mellitus
• This lack of efficacy may be dependent upon NOX2-dependent platelet isoprostane over-production
• Down-regulation of isoprostanes may represent a new avenue to optimize antithrombotic treatment