diabetes and ckd - cannt steel diabetes and ckd.pdfdiabetes and ckd andrew steele md, ... much of...
TRANSCRIPT

Diabetes and CKD
Andrew Steele MD, FRCPC
Chief and Medical Director Nephrology
and Diabetes, Lakeridge
Lead Nephrologist, Central East LHIN
May 29, 2013

Overview
Diabetes epidemiology
CKD in Diabetes
Diabetic Kidney Disease and CV Risk
CDA Guidelines and Recommendations
Issues with glycemic control in CKD
Safety Issues and Hypoglycemia
Emerging therapies for glycemic control


Proportion of Adult Ontarians with Diabetes 2003 to 2009: ICES
1,044,622 people with Diabetes have been identified in Ontario by 2009

Adapted from IDF Diabetes Atlas, 4th ed. International Diabetes
Federation, 2009.
Diabetes, a growing global epidemic likely to
affect ~500 million people by 2030
>90% of diabetic patients have type 2 diabetes1
EU: 10.1%
+17% North America: 13.6%
+16%
China: 14.1%
+45%
*All cases of diabetes, including type 1 and type 2 diabetes, and impaired glucose tolerance (IGT), in patients aged 20-79 years.
aAbsolute number of cases and national prevalence 1International Diabetes Federation. IDF Diabetes Atlas, 4th ed. Brussels, Belgium: International Diabetes Federation, 2009. http://www.idf.org/diabetesatlas accessed July 6th 2011.
Prevalence (%) estimates of diabetes* (age 20-79 years, 2030)1a
5
73
2H
Q1
1N
P0
68

Public Health Agency of Canada. Diabetes in Canada: Facts and figures from a public health perspective. Ottawa, 2011.
Prevalence of diagnosed diabetes among individuals aged ≥ 1 year, by age group
and sex, 2008/09
Diabetes in Canada: Prevalence of Diagnosed
Diabetes by age and sex
Prevalence increased with age. The sharpest increase occurred after age 40 years. The highest prevalence was in the 75-79 year age group.
Pre
va
len
ce
(%
)
0
10
15
25
30
1-19
5
20
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 ≥85 Canada Age group (years)
Females
Males
Total
Overall Prevalence
6.4%
7.2%
6.8%

Patients with DM are more likely to be hospitalized
for many conditions
Public Health Agency of Canada (August 2011); using 2008/09 data from the Canadian Chronic Disease Surveillance System (Public Health Agency of Canada).

Diabetic Nephropathy
“ Progressive increase in proteinuria in people with
longstanding diabetes, followed by declining function
which can eventually lead to End-Stage Renal Disease
(ESRD)”

Importance of the Problem
Diabetic Nephropathy From the perspective of diabetes – One of the most frequent vascular
complications
Type 1 diabetes 30%
Type 2 diabetes 40%
From the perspective of kidney disease – The most common cause of end-stage renal disease (ESRD)
Incident patients 45%
Prevalent patients 55%
From the perspective of cardiovascular disease (CVD) - Progressive risk amplifier
Much of the excess CVD risk in diabetes occurs in the subset of those with diabetic kidney disease (DKD)

lla
illi
lla
illi
Incidence of Diabetic ESRD: Whites,
1992
USRDS 2004

lla
illi
lla
illi
Incidence of Diabetic ESRD: Whites,
2002
USRDS 2004

Diabetes is #1 Cause of New Cases of ESRD
Public Health Agency of Canada (August 2011); using 2008/09 data from the Canadian Chronic Disease Surveillance System (Public Health Agency of Canada).

CKD
in Diabetes
ACR ≥2.0 mg/mmol
and / or
eGFR <60 mL/min
2013

Stages of Diabetic Nephropathy
Note: change in definition of microalbuminuria
ACR ≥2.0 mg/mmol
2013


Chronic Kidney Disease (CKD)
Checklist
SCREEN regularly with random urine albumin creatinine ratio
(ACR) and serum creatinine for estimated glomerular filtration rate
(eGFR)
DIAGNOSE with repeat confirmed
ACR ≥2.0 mg/mmol and/or eGFR <60 mL/min
DELAY onset and/or progression with glycemic and blood pressure
control and ACE-inhibitor or Angiotensin Receptor Blocker (ARB)
PREVENT complications with “sick day management” counselling
and referral when appropriate
2013

Hemmelgarn, JAMA 2010

CV Risk Factors in Diabetes and CKD
CV risk factors should be treated as aggressively in patients with T2DM as in those with a prior myocardial infarction (MI)
Increased CV Risk in CKD and Proteinuria!
11

Approach to CV Risk Reduction:
CDA 2013 Guidelines
All individuals with diabetes (T1D or T2D) should follow a comprehensive,
multifaceted approach to CV risk including:
*Statins, ACEIs/ARBs, and/or ASA as indicated.
CDA: Canadian Diabetes Association.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
Healthy weight Healthy Diet Physical activity Smoking cessation
Glycemic control BP control Additional vascular
protective medications*
Control of lipids
19

Optimal glycemic control in type 1 and type 2 diabetes has
been shown to reduce the development and progression of
nephropathy
Glucose Control and Diabetic
Nephropathy

Reducing Progression of Diabetic
Nephropathy
Optimal glycemic control
Optimal blood pressure control (< 130/80)
ACE-inhibitor (ACEi) or Angiotensin Receptor Blocker (ARB)
Optimize Cardiovascular Risk Factors
Safety concerns – K+, ARF, hypoglycemia....
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
Reducing Progression of Diabetic
Nephropathy
Optimal glycemic control
Optimal blood pressure control (< 130/80)
ACE-inhibitor (ACEi) or Angiotensin Receptor Blocker (ARB)
Optimize Cardiovascular Risk Factors
Safety concerns – K+, ARF, hypoglycemia....
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
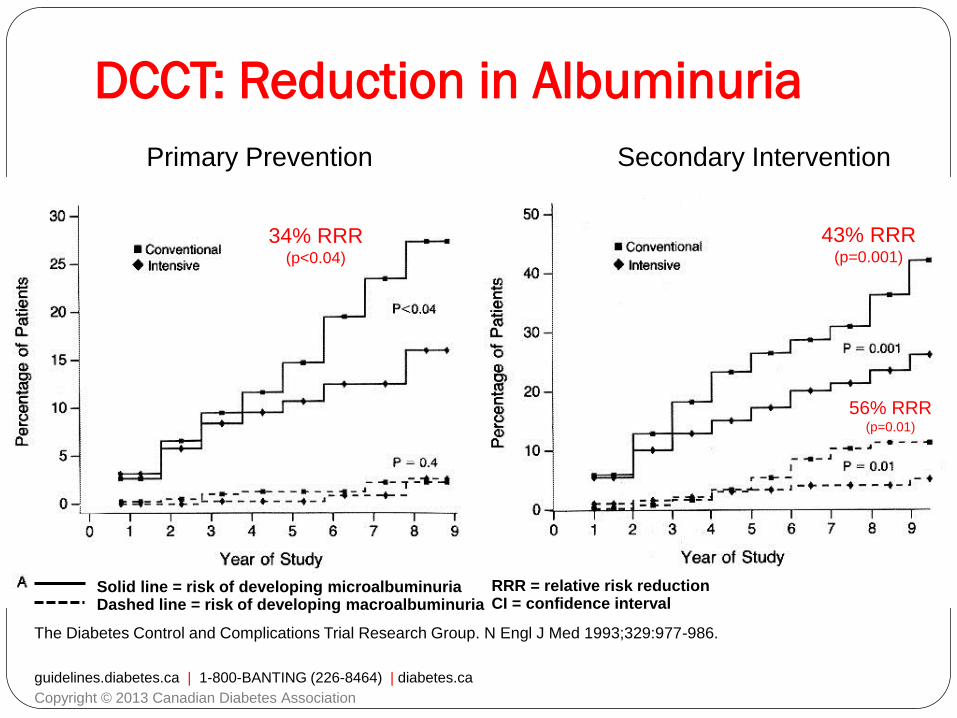
The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977-986.
34% RRR (p<0.04)
43% RRR (p=0.001)
56% RRR (p=0.01)
Primary Prevention Secondary Intervention
Solid line = risk of developing microalbuminuria Dashed line = risk of developing macroalbuminuria
DCCT: Reduction in Albuminuria
RRR = relative risk reduction CI = confidence interval
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association

deBoer IH et al. Arch Intern Med 2011;171(5):412-420.
HR 1.92 (p<0.05)
HR 0.64 (95% CI 0.40-1.02)
Return to normoalbuminuria Macroalbuminuria
HR = hazard ratio CI = confidence interval
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
EDIC: Continued Reduction in
Albuminuria

EDIC: Early Glycemic Control Reduces
Long-term Risk of Impaired GFR
Risk reduction with intensive therapy
50% (95% CI 18-69; p=0.006)
DCCT/EDIC Research Group. N Engl J Med 2011;365:2366-76.

After median 8.5 years post-trial follow-up
Aggregate Endpoint 1997 2007
Any diabetes related endpoint RRR: 12% 9%
P: 0.029 0.040
Microvascular disease RRR: 25% 24%
P: 0.0099 0.001
Myocardial infarction RRR: 16% 15%
P: 0.052 0.014
All-cause mortality RRR: 6% 13%
P: 0.44 0.007
Holman R, et al. N Engl J Med 2008;359.
UKPDS: Post-trial Monitoring “Legacy Effect”
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association

New/worsening nephropathy, retinopathy
66
Cumulative
incidence (%)
Follow-up (months)
HR 0.86 (0.77-0.97)
p = 0.01 Standard
control
Intensive
control
25
20
15
10
5
0 0 6 12 18 24 30 36 42 48 54 60
Intensive Standard HR p
Nephropathy/retinopathy (%) 9.4 10.9 0.86 0.01
Nephropathy (%) 4.1 5.2 0.79 0.006
Retinopathy (%) 6.0 6.3 0.95 NS
Adapted from:
ADVANCE Collaborative Group. N Engl J Med 2008;358:2560-72. ADVANCE Collaborative Group. N Engl J Med 2008;358:24.
ADVANCE: Primary Microvascular
Outcomes

Leon
70 year old hypertensive for 10 years with type
2 diabetes for 8 years
Presents to emergency with acute
hypoglycemia
His blood sugar is 2.8

What we know…..
eGFR 40 ml/min
Blood Pressure 132/82 mmHg
Waist Circumference 104 cm
ACR 44 mg/mmol
A1c 0.080
Lipids Optimal

Leon’s Medications
Metformin 1000 mg BID
Glyburide 10 mg BID
Ramipril 10 mg OD
Atorvastatin 10 mg OD

Etiology of hypoglycemic events in ESRD
patients hospitalized due to hypoglycemia
46%
39%
7%2% 2% 2% Hypoglycemic agents
SepsisSevere MalnutritionLiver FailureAlcohol
Renal Failure, 22(2), 219-223 (2000)
Hypoglycemia often caused by drugs in CKD patients

Summary hypoglycemia in CKD patients:
1. Loss of renal cortical gluconeogenesis
2. Malnutrition
3. Decreased insulin clearance
4. Failure to adjust dose of AHA

Reducing Progression of Diabetic
Nephropathy
Optimal glycemic control
Optimal blood pressure control (< 130/80)
ACE-inhibitor (ACEi) or Angiotensin Receptor Blocker (ARB)
Optimize Cardiovascular Risk Factors
Safety concerns – K+, ARF, hypoglycemia....
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association

Counsel all
Patients
About
Sick Day
Medication
List
2013

When to Refer…..
Chronic, progressive loss of kidney function
ACR persistently >60 mg/mmol
eGFR <30 mL/min
Unable to remain on renal-protective therapies due to
adverse effects such as hyperkalemia or a >30% increase in
serum Cr within 3 months of starting ACEi or ARB
Unable to achieve target BP (could be referred to any
specialist in hypertension)
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association

What we know…..Leon
eGFR 40 ml/min
Blood Pressure 132/82 mmHg
Waist Circumference 104 cm
ACR 44 mg/mmol
A1c 0.080 Lipids Optimal
Metformin 1000 mg BID
Glyburide 10 mg BID
Ramipril 10 mg OD
Atorvastatin 10 mg OD

Glycemic Targets: CDA
2013 Clinical Practice Guidelines
*Examples are shown on next slide.
CDA: Canadian Diabetes Association.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
≤ 7.0% Most people with T1DM or T2DM
≤ 6.5%
May be considered to further reduce the risk of nephropathy or retinopathy, but must be balanced against the risk of hypoglycemia
7.1 - 8.5% May be considered in select situations*
A1C Target
23

Glycemic Targets: CDA
2013 Clinical Practice Guidelines
CDA: Canadian Diabetes Association.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
A less stringent A1C target (7.1% - 8.5)
may be appropriate in people with:
Limited life expectancy
High level of functional dependency
Extensive CAD at high risk of ischemic events
Multiple comorbidities
Recurrent severe hypoglycemia
Hypoglycemia unawareness
Longstanding diabetes for whom it is difficult to achieve A1C
≤ 7.0% despite effective doses of multiple antihyperglycemic
agents, including intensified basal-bolus insulin regimen
24

aRosiglitazone vs. other treatments.
Kahn SE et al. N Engl J Med 2006; 355:2427-43.
Time (years)
A1
C (
%)
0
Rosiglitazone, 0.07 (0.06 to 0.09)
Metformin, 0.14 (0.13 to 0.16)a
Glyburide, 0.24 (0.23 to 0.26)a
No. of patients
Treatment difference
(95% CI)
Rosiglitazone vs.
metformin,
0.13 (0.22 to 0.05);
p = 0.002
Rosiglitazone vs.
glyburide,
0.42 (0.50 to 0.33);
p < 0.001
Annual curve (95% CI)
6.0
6.4
6.8
7.2
7.6
8.0
0 1 2 3 4 5
4012 3308 2991 2583 2197 822
ADOPT
It is Hard to Treat T2DM Adequately…
Because T2DM is a Progressive Disease
33

Increased
glucagon
secretion
Islet-α cell
Increased
lipolysis
Decreased
incretin effect
Neurotransmitter
dysfunction
DeFronzo R. Diabetes 2009; 58:773-85.
Hyperglycemia
Decreased
insulin secretion
Increased
glucose
reabsorption
Increased
hepatic glucose
production
Decreased
glucose
uptake
It is Hard to Treat T2DM Adequately…
Because T2DM has Multiple Pathophysiologic
Abnormalities
34

Lack of Improvement in A1C
in Canada Over Time
1. Harris SB, et al. Diabetes Res Clin Pract 2005; 70(1):90-7.
2. Braga M, et al. Can J Cardiol 2010; 26(6):297-302.
Pro
po
rtio
n w
ith
A1C
< 7
.0%
100
0
60
20
80
40
DICE Study (2005)1 DRIVE Survey (2010)2
Proportion of Subjects with T2DM and A1C Control
53% 51%
31

QUESTION
Which currently available classes of
glucose-lowering medications have been shown to
definitively reduce the risk for CVD in patients with
T2DM?
1. Alpha-glucosidase inhibitor (Acarbose)
2. Biguanides (Metformin)
3. Dipeptidyl peptidase-4 (DPP-4) inhibitors
4. Glucagon-like peptide 1 (GLP-1) receptor agonists
5. Sulfonylureas (SUs)
6. Thiazolidinedione (TZD; pioglitazone)
7. None of the above
41

Conflicting Evidence: Glycemic Control and
Reductions in Risk for CVD
Long-term follow-up of the
UKPDS study
benefit of metformin
> SU / insulin
Meta-analyses of individual
studies
CVD = cardiovascular disease.
1. UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352:837-53. 2. The ACCORD Study Group. N Engl J Med 2011; 364:818-28.
3. The ADVANCE Collaborative Group. N Engl J Med 2008; 358:2560-72. 4. Duckworth W, et al. N Engl J Med 2009; 360:129-39.
5. Holman RR, et al. N Engl J Med 2008; 359:1577-89. 6. Boussageon R, et al. BMJ 2011; 343:d4169. 7. Hemmingsen B, et al. BMJ 2011; 343:d6898.
• Original UKPDS study
• ACCORD
• ADVANCE
• VADT
Evidence
of Benefit
No Evidence
of Benefit
42

UKPDS:
Metformin in Overweight Patients
Compared with conventional policy:
*p < 0.02
UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352:837-53.
BUT: N = just 342
risk reduction
in MI*
42%
32%
39%
36% risk reduction
in all cause
mortality*
risk reduction in any
diabetes-related
endpoints*
risk reduction in
diabetes-related
deaths*
43

Controversies: Glucose Control for
Prevention of CV Events
If you start treating too late,
do you lose CV benefit?
UKPDS vs. ACCORD, ADVANCE, VADT
Do some treatments produce side-effects
that counteract CV benefit?
? certain SUs1,2
? thiazolidinediones (TZDs)3-6
Do we need longer follow-up to see benefit?
1. Tzoulaki I, et al. BMJ 2009; 339:b4731. 2. Schramm TK, et al. Circulation 2008; 117:1945-54.
3. Nissen SE, et al. N Engl J Med 2007; 356:2457-71. 4. Home PD, et al. Lancet 2009; 373:2125-35.
5. Dormandy JA, et al. Lancet 2005; 366:1279-89. 6. Wilcox R, et al. Am Heart J 2008; 155:712-7.
44

QUESTION
Assuming you consider Leon's hypoglycemia is AHA
related –What would you do?
Stop SU and add Acarbose
Stop SU and add bedtime insulin
Stop DU and add dipeptidyl peptidase (DPP-4) inhibitor
Stop DU and add glucagon-like peptide 1 (GLP-1) agonist
Continue the Sulfonylurea (SU) at lower dose
Stop SU and add thiazolidinedione (TZD; pioglitazone)
None of the above
45

Glycemic
control
Drug
toxicity
Hypoglycemia
Hyperglycemia

Individualizing Pharmacologic Therapy in
T2DM: CDA 2013 Clinical Practice Guidelines
CDA: Canadian Diabetes Association.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
Patient-related
Factors
Hyperglycemia
Hypoglycemia
Weight
Comorbidities
Preferences
Access to treatment
Other
Agent-related
Factors
Glucose-lowering efficacy/durability
Hypoglycemia
Effect on weight
Contraindications and side effects
Cost and coverage
Other
25

CPG
- therapeutic
considerations for
renal impairment
2013

T2DM Treatment Options (1 of 4)
*In alphabetical order.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
Class* Drug
(brand name)
Expected
decrease in
A1C with
monotherapy
Hypoglycemia Other therapeutic
considerations
Alpha-
glucosidase
inhibitor
acarbose Rare
• Improved postprandial control
• GI side effects
• Weight: neutral to
• Cost: $$
DPP-4
inhibitors
linagliptin
saxagliptin
sitagliptin
Rare • Weight: neutral to
• Cost: $$$
GLP-1
agonists
exenatide
liraglutide
to
Rare
• GI side effects
• Weight:
• Cost: $$$$
46

T2DM Treatment Options (2 of 4)
Class* Drug (brand name)
Expected
decrease in
A1C with
monotherapy
Hypoglycemia Other therapeutic
considerations
Insulin
Rapid-acting analogues
- aspart
- glulisine
- lispro
Short-acting
- regular
Intermediate-acting
- NPH
Long-acting basal
analogues
- detemir
- glargine
Premixed
- premixed regular-NPH
(30/70 40/60, 50/50)
- biphasic insulin aspart
- insulin lispro/lispro
protamine
Yes
• No dose ceiling
• Flexible regimens
• Weight:
• Cost: $ to $$$$
*In alphabetical order, continued from previous slide.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
47
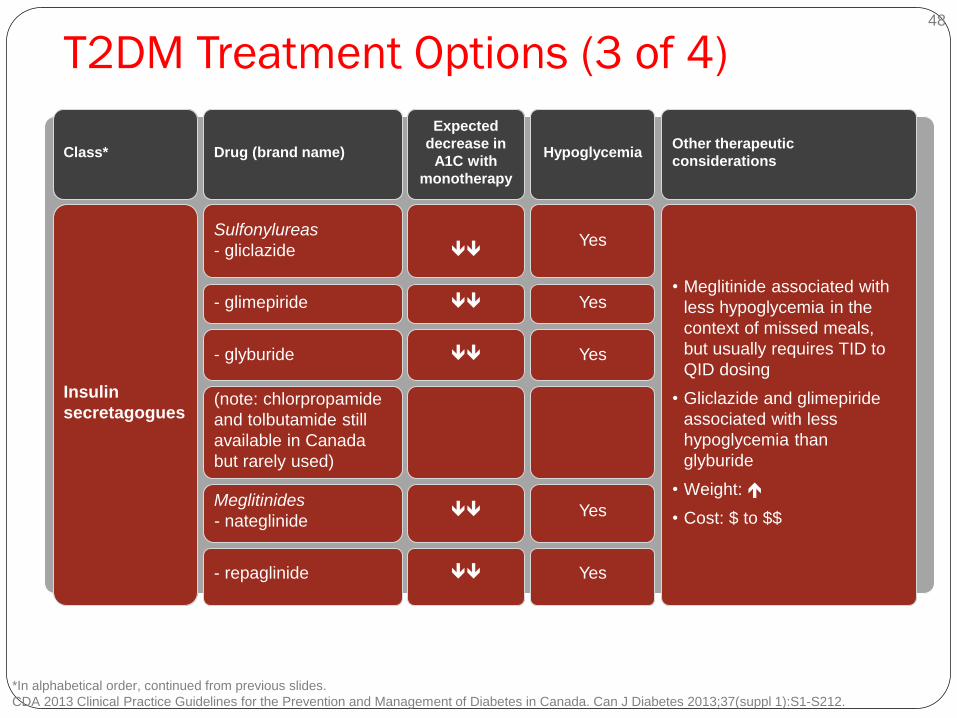
T2DM Treatment Options (3 of 4)
*In alphabetical order, continued from previous slides.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
Class* Drug (brand name)
Expected
decrease in
A1C with
monotherapy
Hypoglycemia Other therapeutic
considerations
Insulin
secretagogues
Sulfonylureas
- gliclazide
Yes
• Meglitinide associated with
less hypoglycemia in the
context of missed meals,
but usually requires TID to
QID dosing
• Gliclazide and glimepiride
associated with less
hypoglycemia than
glyburide
• Weight:
• Cost: $ to $$
- glimepiride Yes
- glyburide Yes
(note: chlorpropamide
and tolbutamide still
available in Canada
but rarely used)
Meglitinides
- nateglinide Yes
- repaglinide Yes
48

T2DM Treatment Options (4 of 4)
Class* Drug
(brand name)
Expected
decrease in
A1C with
monotherapy
Hypoglycemia Other therapeutic
considerations
Biguanides metformin Rare
• Improved CV outcomes in overweight
subjects
• Contraindicated if CrCl/eGFR
< 30 mL/min or hepatic failure
• Caution if CrCl/eGFR < 60 mL/min
• Weight: neutral as monotherapy;
promotes less weight gain when
combined with other antihyperglycemic
agents including insulin
• B12 deficiency
• GI side effects
TZDs pioglitazone
rosiglitazone Rare
• CHF, edema, fractures, rare bladder
cancer (pioglitazone), CV controversy
(rosiglitazone),
• 6-12 weeks required for maximal effect
• Weight:
• Cost: $$
*In alphabetical order, continued from previous slides.
CDA 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212.
49

Glucose Control in CKD/ESRD Intensive Glycemic Control and End-Stage Renal Disease
in Type 2 Diabetes : ADVANCE
N = 11,140 T2DM 5 Yrs
A1c 7.35% vs 6.6%
ESRD 20 vs 7
Nephropathy 4.1% vs. 5.2%
HR =0.79; 95% CI ( 0.66 to 0.93, P=0.006)
NNT = 430 to prevent one ESRD
Not felt to be worth it
Kidney Int 2013 Mar; 83:517.

Glucose Control in ESRD: Excellent glycemic control has not been emphasized as much in
diabetic dialysis patients than in those without renal failure.
Some possible reasons for this practice include the following [21]:
Lack of macrovascular or survival benefit
precipitation of severe hypoglycemia
lack of symptoms with hyperglycemia
The perceived inability to significantly alter progressive damage in
organs other than the kidney.
The perceived lack of accuracy of the glycated hemoglobin level

Glucose Control in ESRD:
Asia N= 150 diabetic subjects
with ESRD starting HD
treatment.
60.5 ± 10.2 years
2.8 years, 76% of the
patients died;
HbA1c < 7.5%), mortality
was lower than in those
with poor glycaemic
control (HbA1c ≥ 7.5%).
Morioka et al. Diabetes Care. Vol. 24. 2001.
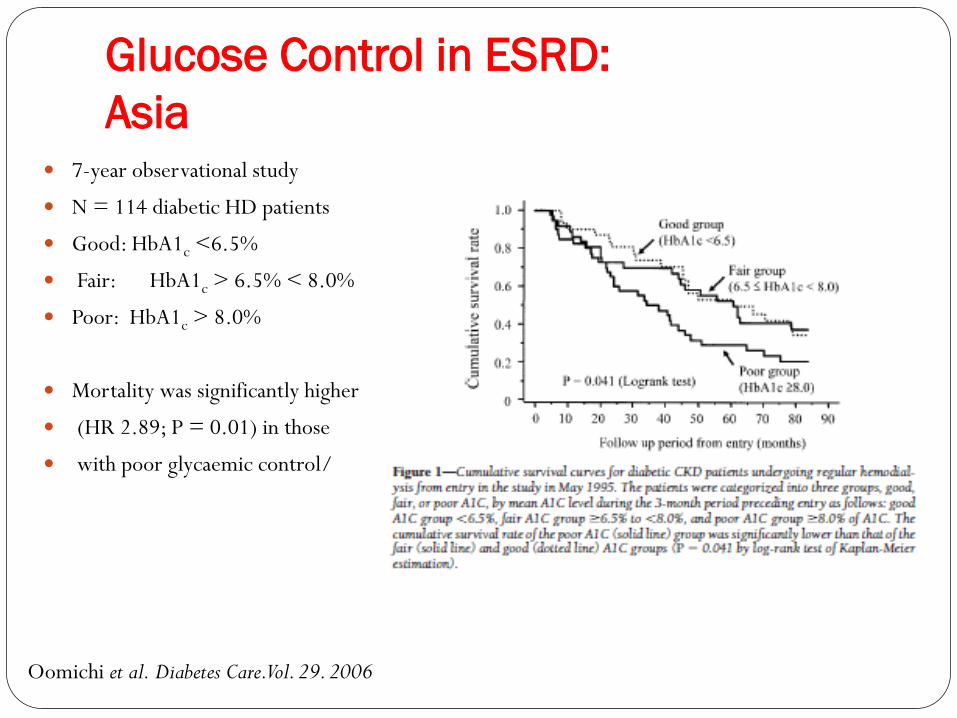
Glucose Control in ESRD:
Asia 7-year observational study
N = 114 diabetic HD patients
Good: HbA1c <6.5%
Fair: HbA1c > 6.5% < 8.0%
Poor: HbA1c > 8.0%
Mortality was significantly higher
(HR 2.89; P = 0.01) in those
with poor glycaemic control/
Oomichi et al. Diabetes Care. Vol. 29. 2006

Glucose Control in ESRD:
USA
A. N = 24 875 US diabetic dialysis patients HgbA1c <5.0 % 11.3%
HgbA1c 5.1 – 7.0% 40.7%
HgbA1c > 7.0% 35%
HgbA1c > 8.5% 14%.
No correlation between HbA1c and survival was found at 12 months in
B. N = 23 618 US diabetic HD patients
HbA1c values were incrementally associated with higher mortality.
HbA1c in the range of 5–6% vs. HbA1c >10% Adjusted all-cause HR = 1.41 (P < 0.001)
CV death HR = 1.73 (P < 0.001)
Kidney Int 2006;70:1503-1509.
Diabetes Care. Vol. 30. 2007

Glucose Control in ESRD: However since diabetes-related damage is likely to present in varying degrees among
different organs, good glycemic control should be a significant treatment goal for diabetic patients with end-stage renal disease.
1. A1c is probably less informative
2. Aim for A1c < 7% if possible
3. A1c < 8.5% for long standing DM, elderly, frail, established CVD
4. Difficult to achieve in PD
5. Avoid Hypoglycemia is paramount
6. Avoid symptomatic hyperglycemia
7. Choosing safe drugs
In conclusion, there is an urgent need for large prospective RCTs in diabetic patients with CKD / ESRD with the following goals:
different approaches of antidiabetic treatment
efficacy and safety of different levels of glycaemic control

Glucose Control in CKD and ESRD:
LH KCC
<.07 = 65.5%
<0.084 =23.9% (89.4%)
Home HD
<0.07% =60.6%
<0.084 =21.2% (81.8%)
PD
<0.07 = 38.1%
<0.084= 34.9% (73 %)
ICHD
<0.07=44.2%
<0.084=18.4% (62.6%)
Possible Benefits of Newer Classes
of AHA
Incretin Therapy

ADVANCE:
Severe Hypoglycemia Associated with Adverse Clinical
Endpoints and Death
Numbers above sets of bars are HR (95% CI). aAdjusted for multiple baseline covariates. bPrimary endpoints. Major macrovascular event = CV death, nonfatal myocardial infarction,
or nonfatal stroke; major microvascular event = new or worsening nephropathy or retinopathy.
Zoungas S, et al. N Engl J Med 2010; 363:1410–8.
b b
25
0
15
5
20
10
Severe Hypoglycemia
(n = 231)
No Severe Hypoglycemia
(n = 10,909)
3.53
(2.41–5.17)a
Major
macrovascular
eventb
15.9
10.2
2.19
(1.40–3.45)a
Major
microvascular
eventb
11.5
10.1
3.27
(2.29–4.65)a
Death from
any cause
19.5
9.0
3.79
(2.36–6.08)a
CV disease
9.5
4.8
2.80
(1.64–4.79)a
Non-CV disease
10.0
4.3
Pa
tie
nts
wit
h ≥
1
hyp
og
lyc
em
ic e
ve
nts
(%
)
54

Some Antihyperglycemic Therapies
May Have Adverse CV Effects
Data suggest an increase in CV risk with certain oral antihyperglycemic agents
Certain sulfonylureas1,2 — possibly mediated by:
increased CV risks associated with hypoglycemia
effects on cardiac potassium ATP channels (loss of beneficial ischemic pre-conditioning)
Thiazolidinediones3-6
increased risk of edema, CHF
1. Tzoulaki I, et al. BMJ 2009; 339:b4731. 2. Schramm TK, et al. Circulation 2008; 117:1945-54.
3. Nissen SE, Wolski K. N Engl J Med 2007; 356:2457-71. 4. Home PD, et al. Lancet 2009; 373:2125-35.
5. Dormandy JA, et al. Lancet 2005; 366:1279-89. 6. Wilcox R, et al. Am Heart J 2008; 155:712-17.
52

Effects of Incretin Agents on CV Events
in T2DM: Risk Reduction for MACE in
Meta-analyses
MACE = CV death, MI, stroke, hospitalization for ACS or HF.
Monami M, et al. Exp Diab Res 2011; doi:10.1155/2011/215764.
Lamanna C, et al. EASD Annual Meeting, September 2011.
-60
-45
-30
-15
0
Ris
k r
ed
ucti
on
fo
r M
AC
E (
%)
-31%
p = 0.006
-26%
p = 0.121
GLP-1R agonists vs.
all comparators
(20 trials)1
-54%
p = 0.009
GLP-1R agonists
vs. placebo
(13 trials)1
DPP-4 inhibitors vs.
all comparators
(43 trials)2
DPP-4 inhibitors
vs. placebo
(25 trials)2
-29%
p = 0.045
68

Ongoing CV Outcome Trials:
DPP-4 Inhibitors
CVD = cardiovascular.
Adapted from:
1. Golden SH. Am J Cardiol 2011; 108(Suppl):59B-67B.
2. Fonseca V. Am J Cardiol 2011; 108(Supp):52B–58B.
3. www.clinicaltrials.gov
Trial Therapies # Population Primary endpoint End Date
CAROLINA Linagliptin/
Glimepiride
6000 CVD or ≥ 2 RF Non-inferiority: time to
first occurrence of any
component of MACE
composite outcome
Sept 2018
EXAMINE Alogliptin/
Placebo
5400 ACS 15-90 days
before
Non-inferiority: time to
occurrence of MACE
Dec 2014
SAVOR-TIMI 53 Saxagliptin/
Placebo
16,500 CVD or ≥ 2 RF Superiority efficacy,
non-inferiority safety:
composite CV death, NF
MI, NF stroke
July 2013
TECOS Sitagliptin/
Placebo
14,000 Established CVD Non-inferiority: time to
first occurrence of
composite CV outcome
Dec 2014
72

Ongoing CV Outcome Trials:
GLP-1 Agonists
CVD = cardiovascular.
Adapted from:
1. Golden SH. Am J Cardiol 2011; 108(Suppl):59B-67B.
2. Fonseca V. Am J Cardiol 2011; 108(Supp):52B–58B.
3. www.clinicaltrials.gov
Trial Therapies # Population Primary endpoint End Date
ELIXA Lixisenatide/
Placebo
6000 ACS leading to
hosp ≤ 180 days
before
Non-inferiority:
CV death, NF MI,
NF stroke, UA
hospitalization.
Oct 2013
EXSCEL Exenatide
LAR/
Placebo
9500 T2DM, A1C of
7.0-10.0%
Non-inferiority:
Time to primary
composite CV endpoint
Mar 2017
LEADER Liraglutide/
Placebo
8754 CVD, PAD, CKD,
CHF or RF if age
> 60 years
Superiority:
Time to composite CV
death, NF MI, NF stroke
Jan 2016
REWIND Dulaglutide/
Placebo
9622 CVD or ≥ 2 RF if
age ≥ 60 years
Superiority:
Time to composite CV
death, NF MI, NF stroke
Apr 2019
73

Leon
Goals:
1. Optimal glycemic control
2. Optimal blood pressure control (< 130/80)
3. ACE-i or ARB
4. Optimize Cardiovascular Risk Factors
5. Safety concerns – K+, ARF, hypoglycemia....
70 y.o.
HT 15 years
T2DM 10 years
CKD Stage 3
ER: Severe Hypoglycemia

Overall Conclusions
T2DM is over 10% of population and growing
DM Nephropathy is # 1 cause of ESRD
CDA recommends vascular protection in T2DM patients
Multi-risk factor intervention is necessary, including glycemic control
No prospective evidence yet of CV benefit with any antihyperglycemic therapy
Individualized goals of therapy are now the recommended, beware safety issues including hypoglycemia and increased morbidity and mortality
Newer agents may offer some benefit over traditional agents, especially in CKD and high risk patients
Large prospective RCTs are ongoing and needed to answer the question of targets, safety and optimal agents in CKD/ESRD
78