diabetes en la adolescencia - fundación redgdps curso avanzado_valencia_2010... · • dermatitis...
TRANSCRIPT

Dr. F. Javier Ampudia-BlascoUnidad de Referencia de Diabetes
Hospital Clínico Universitario de Valencia
1er Curso Práctico Avanzado en Diabetes
Diabetes en la adolescencia
Valencia, 5 de Junio 2010

La adolescencia
“La adolescencia es la fase del desarrollo que ocurre entre la infancia y la vida adulta, y que incorpora los cambios fisiológicos y psicológicos de la pubertad”
Ampu
dia-
Blas
co F
J, M
D

Periodo de transición en muchos aspectos
• De la infancia pasa a la vida adulta
• De la Pediatría a la Medicina del adulto
• Del tratamiento controlado por los padres al control propio del tratamiento
• De la educación al trabajo
Ampu
dia-
Blas
co F
J, M
D

Aspectos a desarrollar
• Diabetes tipo 2 en la adolescencia.
• Enfermedades asociadas a la diabetes en la adolescencia
• Trastornos psicológicos en el paciente diabético adolescente
Ampu
dia-
Blas
co F
J, M
D

Diabetes tipo 1
Obesidad“Doublediabetes”
Diabetes tipo 2
Diabetes monogénica:
• Neonatal
• MODY
Clasificación de la Diabetes en la edad pediátrica (ADA)
Diabetes Care 2006; 25: 731-6
Ampu
dia-
Blas
co F
J, M
D

Prevalence of Diabetes and IFG in US Adolescents – NHANES 1999-2002
• Type 2 Diabetes
– 0.5% of adolescents have diabetes
– 71% type 1 and 29% type 2
• Determined by insulin use vs. no insulin use
– 39,005 US teens with type 2 diabetes
• Impaired Fasting Glucose (IFG)
– 11% had IFG
– 2,769,736 teens with IFG
• Diabetes increased 41% from 4.9 to 6.9/1000 from 1997 to 2003 - adults
Duncan. Arch Pediatr Adolesc Med 2006;160:523; Geiss. Am J Prevent Med 2006;30:371
Ampu
dia-
Blas
co F
J, M
D

¿Cuándo debe sospecharse una diabetes tipo 2 en la adolescencia ?
Ampu
dia-
Blas
co F
J, M
D

Type 1 diabetes Type 2 diabetes
Weight
Course
DKA
Relative with DM
Comorbid
C-peptide
Antibody
Ethnicity
20% may be overweight / obese Virtually all BMI > 85%th percentile
RapidFrom DPT-1 can be indolent
IndolentVirtually none found on screening
35%-40%Ketonuria (33%)Mild DKA (5%-25%)
5% with T1DM Up to 30% may have with T2DMFH of T2 2-3Xs in person with T1
74%-100% - 1st –2nd degree with T2DM
Thyroid, adrenal, vitiligo, celiacIncrease in polycystic ovary syndromeAcanthosis nigricans
C-peptide can be preserved at DX Normal or increased
85%
Whites predominate
15% (reported as high as 30%)
NA, AA, HA, Asian, Pacific Islander
Type 1 vs. type 2 diabetes in youth?
Kaufman. Endocrinol Metab Clin North Am 2005; 34:659-76
Ampu
dia-
Blas
co F
J, M
D
Autoantibody testing and C-Peptide when diagnosing and treating T2DM
• In all pediatric patients with the clinical diagnosis of T2DM:
– As indication of earlier need for Insulin
– As a need to check for other associated autoimmune disorders
• Should be considered in overweight/obese children > 13 years of age with a clinical picture of T1DM (weight loss, ketosis/ketoacidosis)
• C–peptide should be measured in overweight/obese children > 13 years of age, who have worsening on oral agents to confirm requiring insulin therapy
Rosenbloom AL et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Ampu
dia-
Blas
co F
J, M
D

¿Cómo debe de enfocarse este problema ?
Ampu
dia-
Blas
co F
J, M
D

Prevention Treatment–10 10 Years
Diagnosis
MacrovascularMacrovascular complicationscomplications
0
IGT/IFG Type 2 diabetes
Historia natural de la diabetes tipo 2
Blood glucose
Insulin resistance
MicrovascularMicrovascular complicationscomplications
DeFronzo RA. Med Clin N Am 2004; 88:787–835
Β-cell function
Ampu
dia-
Blas
co F
J, M
D

Prior conditions associated with insulin resistance during development
• Conditions associated with insulin resistance:
– premature adrenarche in girls (pubic hair appearing before the age of 8 years)
– small for gestational age
– ovarian hyperandrogenism and PCOS
Rosenbloom AL et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Ampu
dia-
Blas
co F
J, M
D

Diabetes is only one manifestation of the insulin resistance syndrome
• Obesity
• Hypertension
• Albuminuria may be present at the time of diagnosis
• Hypertriglyceridemia and ↓ HDL cholesterol
• Ovarian hyperandrogenism and premature adrenarche
• Hepatic steatosis: 25–45% of adolescents with T2DM
• Systemic inflammation: ↑ CRP, ↑ inflammatory cytokines, ↑ white blood cell
Rosenbloom AL et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Ampu
dia-
Blas
co F
J, M
D

Tratamiento de la diabetes tipo 2
Control glucémico:Hábitos dietéticosActividad físicaTx farmacológico
Tx comorbilidades asociadas:DislipemiaHTAObesidad(Enf. Cardiovascular)
Screening/Tx complicaciones:RetinopatíaNefropatíaNeuropatíaEnf. CardiovascularOtras
Principios de la dieta en niños y adolescentes
Número de comidas:
– 3 comidas principales
– 2-3 snacks
– Adaptada a la edad, actividad física y pauta de insulina
Ingesta calórica:
– 1000 kcal + 100 kcal/año de edad (máximo de 2.200 kcal en chicas/ 2.600 kcal en chicos, que se incrementará o disminuirá en función de actividad física y peso)
– 50–55% en carbohidratos
– 30% en grasas
– 15–20% en proteínas
Ampu
dia-
Blas
co F
J, M
D

Treatment decision tree for type 2 diabetes in children and adolescents
Rosenbloom AL et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Ampu
dia-
Blas
co F
J, M
D

Key messagesand follow-up
Ampu
dia-
Blas
co F
J, M
D
Recommendation for initial medical treatment of type 2 diabetes
• Preadolescent children are unlikely to have T2DM, even if obese
• Overweight adolescents may have both T1DM and T2DM. Antibody determination is the only way to definitively differentiate both entities.
• Initial treatment modality is determined by symptoms, severity of hyperglycemia, and presence or absence of ketosis/ketoacidosis.
• Lifestyle changes in diet and exercise are essential and should be recommended for all individuals with T2DM
Rosenbloom AL et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Ampu
dia-
Blas
co F
J, M
D

Associated diseases testing, specific to T2DM in young people
• Testing for microalbuminuria at the time of diagnosis and annually thereafter
• BP should be monitored at every visit
• Testing for dyslipidemia should be performed soon after diagnosis when BG control has been achieved and annually thereafter
• Evaluation for NAFLD should be done at diagnosis and annually thereafter
• Examination for retinopathy should be performed at diagnosis and annually thereafter
Rosenbloom AL et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32
Ampu
dia-
Blas
co F
J, M
D
Aspectos a desarrollar
• Diabetes tipo 2 en la adolescencia.
• Enfermedades asociadas a la diabetes en la adolescencia
• Trastornos psicológicos en el paciente diabético adolescente
Ampu
dia-
Blas
co F
J, M
D

Otras patologías asociadas
• Diabetes mal controlada:
– Retraso de crecimiento y alteraciones puberales
• Enfermedades autoinmunes:
– Tiroiditis autoinmune (3-8%, 25% anticuerpos)
– Enf. de Graves-Basedow
– Enfermedad de Addison (2% anticuerpos)
– Enfermedad celíaca (1-10%)
– Vitíligo (6%)
• Necrobiosis lipoídica diabeticorum
• Limitación de la movilidad articular
Ampu
dia-
Blas
co F
J, M
D

Hipotiroidismo primario autoinmune
Ampu
dia-
Blas
co F
J, M
D

Tiredness
Forgetfulness/Slower Thinking
Moodiness/ Irritability
Depression
Inability to Concentrate
Thinning Hair or Hair LossLoss of Body Hair
Dry, Patchy Skin
Muscle Weakness or Cramps
Constipation
Infertility
Menstrual Irregularities/Heavy Period
Slower Heartbeat
Difficulty Swallowing
Persistent Dry or Sore Throat
Hoarseness/Deepening of Voice
Swelling (Goiter)
Puffy Eyes
Weight Gain
Cold Intolerance
Elevated Cholesterol
Signs and Symptoms of Hypothyroidism
Ampu
dia-
Blas
co F
J, M
D

Diagnosing Hypothyroidism
• Family and personal medical history• Hypothyroidism may be
Hereditary
• Physical exam• MD Observes the Patient• Palpates the thyroid• Interviews patient
• Laboratory Tests• TSH Test• Free T4
Ampu
dia-
Blas
co F
J, M
D
Hypothyroidism associated with type 1 diabetes in young people
• Primary hypothyroidism is due to autoimmune thyroiditis(3–8%)
• Antithyroid antibodies (in up to 25%) are predictive for the development of clinical or compensated hypothyroidism
• Thyroid antibodies are observed more frequently in girls than in boys, often emerging along with pubertal maturation
Kordonouri O et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 204–10
Ampu
dia-
Blas
co F
J, M
D

Enfermedad celíacao intolerancia al gluten
Ampu
dia-
Blas
co F
J, M
D

Why screening for celiac disease in type 1 diabetes?
Significant health problem, multi-organ morbidity:
– Intestinal: diarrhea, distention, vomiting, abdominal pain, weight loss
– Extra-intestinal: pubertal/growth delay, anemia, osteopenia, etc.
– In type 1 diabetes: unexplained hypoglycemia, poor HbA1c
Ampu
dia-
Blas
co F
J, M
D

T T cell
ab TCR
APC
HLA-DQ2or -DQ8
Pathomechanism of Celiac Disease
TG
Gluten
Transaminatedgluten peptides
T
T T
T T
T
TG

Old paradigm Celiac disease as a disease of small intestine
Celiac disease• villous atrophy • malnutrition
London, year 1938
Ampu
dia-
Blas
co F
J, M
D

New paradigm: multi-organ autoimmune disease
Celiac disease• villous athrophy• malnutrition• malignancies
Bone• osteoporosis, fractures• arthritis• dental anomalies
HepatitisCholangitis
Skin & mucosa• dermatitis herpetiformis• aphtous stomatitis• hair loss
Reproductive• miscarriage, infertility• delayed puberty
Central nervous system• ataxia, seizures• depression
Carditis, cardiomyopathy
Anemia
Ampu
dia-
Blas
co F
J, M
D

Dermatitis Herpetiformis
• Erythematous macule > urticarial papule > tense vesicles
• Severe pruritus
• Symmetric distribution
• 90% no GI symptoms
• 75% villous atrophy
• Gluten sensitive
Ampu
dia-
Blas
co F
J, M
D
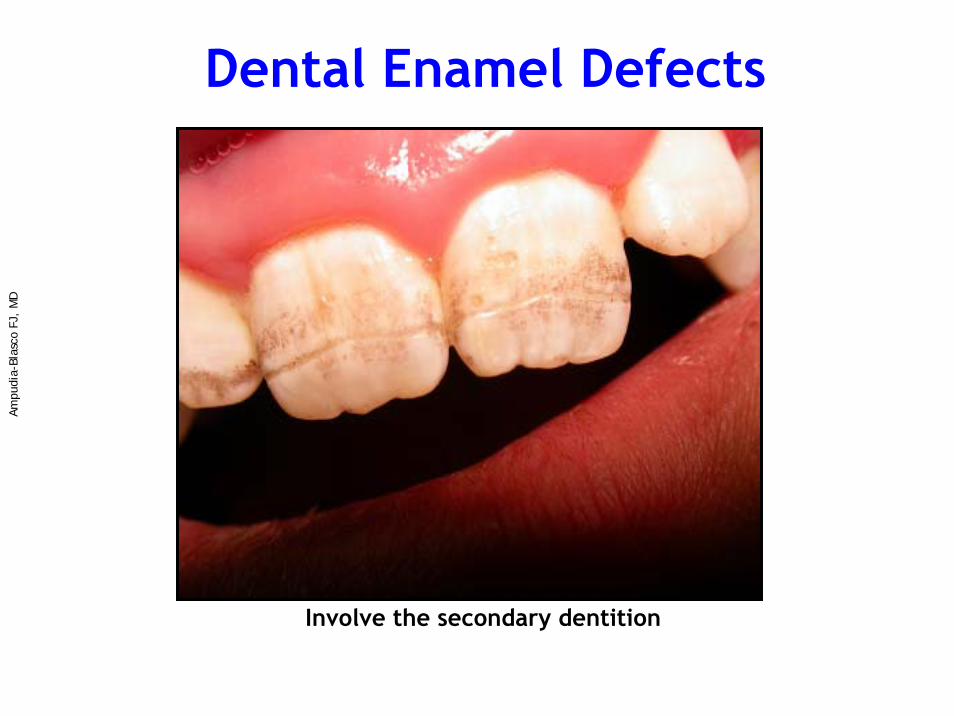
Involve the secondary dentition
Dental Enamel DefectsAm
pudi
a-Bl
asco
FJ,
MD

Aphtous StomatitisAm
pudi
a-Bl
asco
FJ,
MD

Osteopenia/OsteoporosisLow bone mineral density by DEXA in a child with untreated CD
Ampu
dia-
Blas
co F
J, M
D

Entheropathy-Associated T-cell Lymphoma
Ampu
dia-
Blas
co F
J, M
D
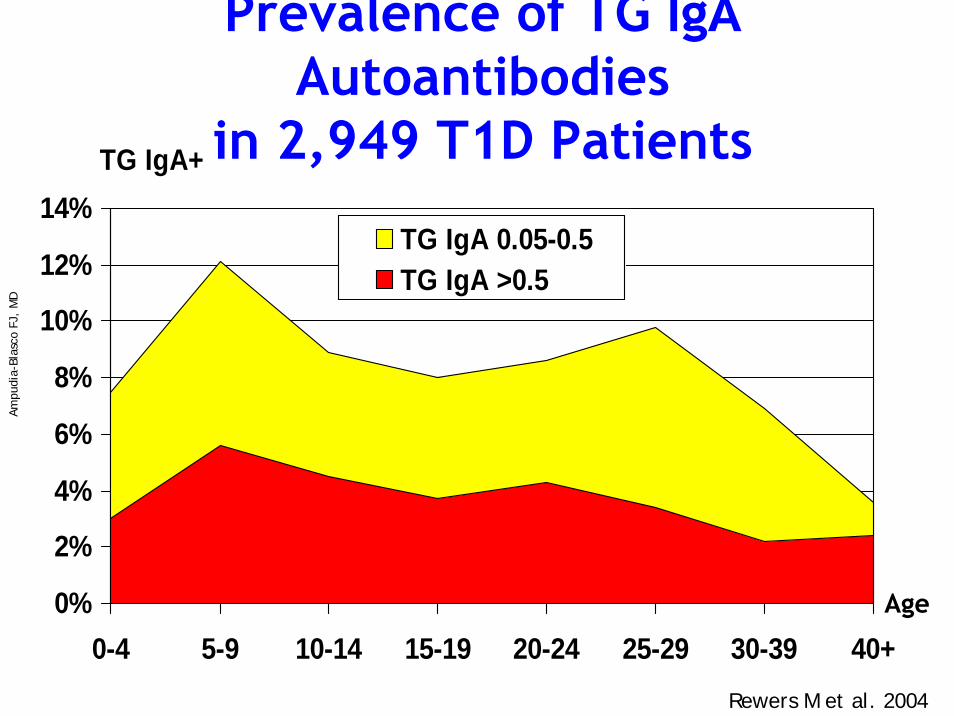
Prevalence of TG IgA Autoantibodies
in 2,949 T1D Patients
0%
2%
4%
6%
8%
10%
12%
14%
0-4 5-9 10-14 15-19 20-24 25-29 30-39 40+
TG IgA+
TG IgA 0.05-0.5TG IgA >0.5
Age
Rewers M et al. 2004
Ampu
dia-
Blas
co F
J, M
D

Histology of intestinal biopsy in celiac disease
Ampu
dia-
Blas
co F
J, M
D

Recommendations for celiac disease
• All patients with type 1 diabetes should be screened for TG IgA at onset and at least bi-annually until age 10, or if symptomatic
• In asymptomatic cases, intestinal biopsy should be recommended if TG levels are positive (predictive in over 90%)
• Biopsy should be done after at least 1-2 weeks on a high-wheat diet
• Persistent TG IgA and HLA-DQA1*0501/B1*0201 predict progression to celiac disease even if the initial biopsy is negative
• Gluten-free diet should be recommended to all Bx+ patients
• Insulin dose usually needs to be increased when gluten-free diet is started
Ampu
dia-
Blas
co F
J, M
D

Screening and diagnosis of CD in diabetic patients and their relatives
Biopsy negative:Biopsy positive: GFD monitor TG,
repeat biopsy
Biopsyrecommended
TG IgA > 0.5
or symptoms
Biopsy likely negrepeat TG in 6-12 months
TG IgA < 0.5 and
asymptomatic
TG Positive > 0.05
TG negative, no symptomsrepeat every 1-2 yrs if HLA-DQB1*0201
until age 10?
Biopsyrecommended
IgA <10 mg/dl
TG negative, symptomaticrepeat in 3-6 months
check IgA levels, HLA,other causes?
All patients TG IgA
Rewers et al. EMCNA 2004
Ampu
dia-
Blas
co F
J, M
D

A girl that refuses pasta and breadFemale Type 1 diabetes diagnosed by age 3.9 yr HLA-DR3/4 DQB1*0201/0302
Height Weight
GFD ?
M3b
TG>0.5
TG 0.05-0.05
•TG<0.05
Ampu
dia-
Blas
co F
J, M
D

A girl that is trying to catch upFemale Type 1 diabetes diagnosed by age 5.3 yr HLA-DR3/4 DQB1*0201/0302
Height Weight
GFD
M3c
TG>0.5
TG 0.05-0.05
•TG<0.05
Ampu
dia-
Blas
co F
J, M
D

With gluten free diet1 in 10
TG IgA +++
Biopsy
M1
M2
M3
Ampu
dia-
Blas
co F
J, M
D

Aspectos a desarrollar
• Diabetes tipo 2 en la adolescencia.
• Enfermedades asociadas a la diabetes en la adolescencia
• Trastornos psicológicos en el paciente diabético adolescente
Ampu
dia-
Blas
co F
J, M
D

Causes of deterioration of metabolic control in adolescents with diabetes
• Erratic meal and exercise patterns
• Poor adherence to treatment regimens
• Hazardous and risk taking behaviours
• Eating disorders
• Endocrine changes associated with puberty, leading to greater insulin resistance
Court JM et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 185–94
Ampu
dia-
Blas
co F
J, M
D

Adolescencia vs. diabetes
¿Qué exige la diabetes?
Grandes cambios físicos, psicológicos y sociales.
Transgresión de las normas
Necesidad de libertad independencia,
Inconstancia
Falta de madurez para asumir responsabilidades totales.
Afirmación con el grupo
Problema de salud
Vida ordenada (horarios, dieta sana...)
Limites
Autocontrol, sobreprotección
Asumir la diabetes para responsabilizarse en el aprendizaje y manejo
Posicionarse ante los demás
¿Cómo es la adolescencia?
Grandes cambios físicos, psicológicos y sociales.
Transgresión de las normas
Necesidad de libertad independencia,
Inconstancia
Falta de madurez para asumir responsabilidades totales.
Afirmación con el grupo
Ampu
dia-
Blas
co F
J, M
D
Eating disorders and diabetes in adolescence
• Insulin omission for weight control has been reported in 12–15% of adolescents
• Rebellion, binges and erratic eating behavior are frequent during adolescence
• Poor glycemic control may reflect insulin omission in association with disordered eating
• Eating disorders in adolescents and young adults with diabetes are associated with poor metabolic control and diabetic complications
Smart C et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 100–17
Ampu
dia-
Blas
co F
J, M
D

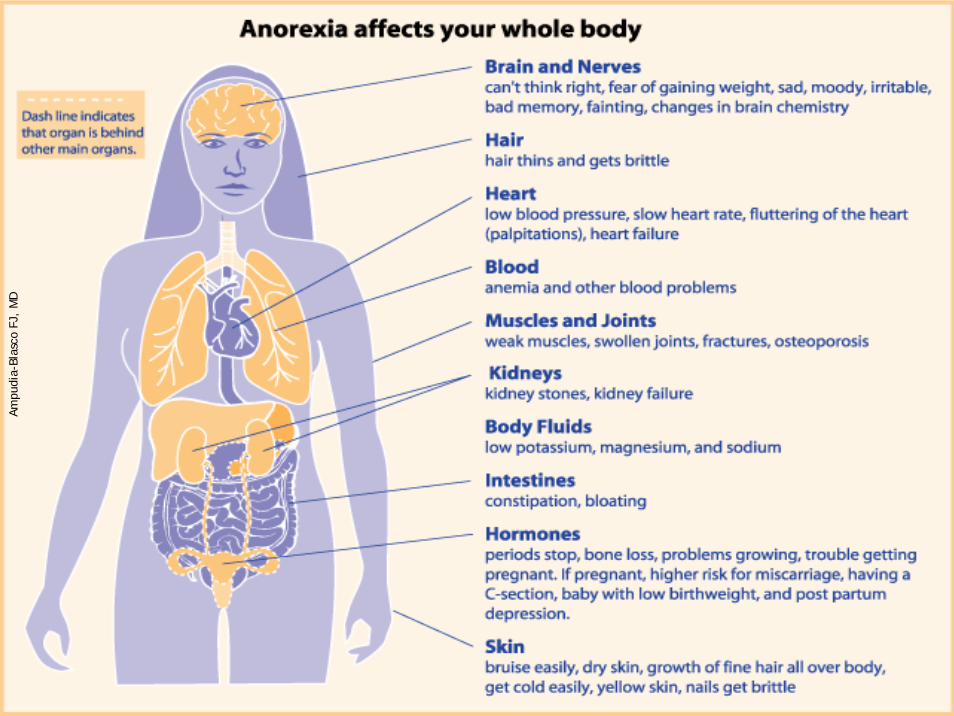
Anorexia nerviosa
1. Pérdida deliberada de peso
2. Distorsión de la imagen corporal
Ampu
dia-
Blas
co F
J, M
D

• Negativa a mantener un peso por encima del 85% de su peso ideal.
• Intenso miedo a ganar peso y a la obesidad, a pesar de estar malnutrido.
• Distorsión de la imagen corporal
• En mujeres postmenárquicas, amenorrea durante al menos tres ciclos consecutivos.
Ampu
dia-
Blas
co F
J, M
D
Criterios diagnósticos de anorexia nerviosa

Bulimia nerviosa
Atracones
Preocupación excesiva por el peso
Conductas compensadoras
Ampu
dia-
Blas
co F
J, M
D

1. Episodios recurrentes de atracones caracterizados por la ingesta en un periodo corto de tiempo de una gran cantidad de alimentos con sensación de pérdida de control.
2. Comportamientos compensadores para evitar ganar peso como el uso de diuréticos, laxantes, enemas u otras medicaciones, vómitos autoinducidos, ayuno o ejercicio exagerado.
Criterios diagnósticos de bulimia nerviosa
Ampu
dia-
Blas
co F
J, M
D

3. Tanto los atracones como los comportamientos compensadores ocurren al menos dos veces a la semana durante tres meses.
4. La autovaloración está claramente influenciada por la imagen corporal y el peso.
5. Los alteraciones no ocurren exclusivamente durante los episodios de anorexia nerviosa.
Criterios diagnósticos de bulimia nerviosa (cont.)
Ampu
dia-
Blas
co F
J, M
D

Etiopatogenia de la anorexia y de bulimiaAm
pudi
a-Bl
asco
FJ,
MD
Ampu
dia-
Blas
co F
J, M
D

Ampu
dia-
Blas
co F
J, M
D

Ampu
dia-
Blas
co F
J, M
D

Recommendations for health care teams dealing with adolescents
• Understand the physiological and psychosocial developmental changes of adolescence
• Develop a consistent trusting and motivating relationship with the adolescent
• Develop communication skills to facilitate teaching and education
• Enable the adolescent to learn from mistakes
• Recognize the signs of mental health problems (depression, eating disorders, illicit drug usage, etc.) and the occasional need for psychiatric treatment
Court JM et al. Pediatric Diabetes 2009: 10 (Suppl. 12): 185–94
Ampu
dia-
Blas
coFJ
, M
D