diabetes melitus
TRANSCRIPT

DIABETES MELITUS BY DR.ISHTIAQ SHAFIQ (BSC PHARM D RPH CDE)

Definition Diabetes mellitus is most common
endocrine disorder . It is a chronic condition ,characterized by hyperglycemia due to impaired insulin secretion with or without insulin resistance .

Insulin β cells secrete due to
high blood glucose levels
Glucose uptake into tissues increases
Glucagon α cells secrete when
blood glucose is low Glucose is released from
tissues back into blood
Pancreatic axis

Glucose homeostasis
Figure 26.8
Insulin
Beta cellsof pancreas stimulatedto release insulin intothe blood
Bodycellstake up moreglucose
Blood glucose leveldeclines to a set point;stimulus for insulinrelease diminishes
Liver takesup glucoseand stores it asglycogen
High bloodglucose level
STIMULUS:Rising blood glucoselevel (e.g., after eatinga carbohydrate-richmeal) Homeostasis: Normal blood glucose level
(about 90 mg/100 mL) STIMULUS:Declining bloodglucose level(e.g., afterskipping a meal)
Alphacells ofpancreas stimulatedto release glucagoninto the blood
Glucagon
Liverbreaks downglycogen and releases glucoseto the blood
Blood glucose levelrises to set point;stimulus for glucagonrelease diminishes


Mechanism of Insulin Action
Insulin binds to specific high affinity membrane receptors with tyrosine kinase activity
Phosphorylation cascade results in translocation of Glut-4 (and some Glut-1) transport proteins into the plasma membrane.
It induces the transcription of several genes resulting in increased glucose catabolism and inhibits the transcription of genes involved in gluconeogenesis.
Insulin promotes the uptake of K+ into cells.

Mechanism of Insulin Release in the Pancreas

Action of Insulin on Carbohydrate, Protein and Fat Metabolism
Carbohydrate Facilitates the transport of glucose into
muscle and adipose cells Facilitates the conversion of glucose to
glycogen for storage in the liver and muscle.
Decreases the breakdown and release of glucose from glycogen by the liver

Action of Insulin on Carbohydrate, Protein and Fat Metabolism
Protein Stimulates protein synthesis Inhibits protein breakdown; diminishes
gluconeogenesis
Action of Insulin on Carbohydrate, Protein and Fat Metabolism
Fat Stimulates lipogenesis- the transport of
triglycerides to adipose tissue Inhibits lipolysis – prevents excessive
production of ketones or ketoacidosis


Epidemiology (pakistan)Prevalence of diabetes is high ranging from 7.6to 11% in Pakistan . Variations accordingto age, sex, location and urbanization havebeen noted. Reports from National diabetessurvey and National health survey differboth in observations regarding prevalence ofdiabetes and in relative burden of diabetes invarious provinces and among males andfemales.Type 2diabetes is much more common than type 1 , accounting for 80 – 85 % it usually occur in those over the age of 40 years .
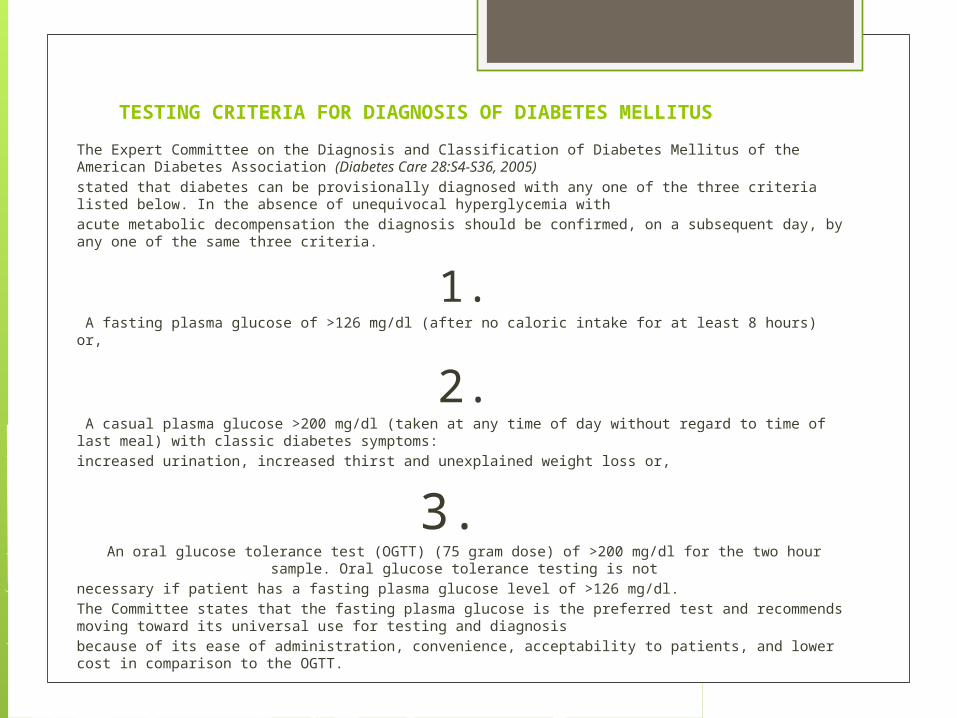
TESTING CRITERIA FOR DIAGNOSIS OF DIABETES MELLITUS
The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus of the American Diabetes Association (Diabetes Care 28:S4-S36, 2005)stated that diabetes can be provisionally diagnosed with any one of the three criteria listed below. In the absence of unequivocal hyperglycemia withacute metabolic decompensation the diagnosis should be confirmed, on a subsequent day, by any one of the same three criteria.
1. A fasting plasma glucose of >126 mg/dl (after no caloric intake for at least 8 hours) or,
2. A casual plasma glucose >200 mg/dl (taken at any time of day without regard to time of last meal) with classic diabetes symptoms:increased urination, increased thirst and unexplained weight loss or,
3. An oral glucose tolerance test (OGTT) (75 gram dose) of >200 mg/dl for the two hour sample. Oral
glucose tolerance testing is notnecessary if patient has a fasting plasma glucose level of >126 mg/dl.The Committee states that the fasting plasma glucose is the preferred test and recommends moving toward its universal use for testing and diagnosisbecause of its ease of administration, convenience, acceptability to patients, and lower cost in comparison to the OGTT.


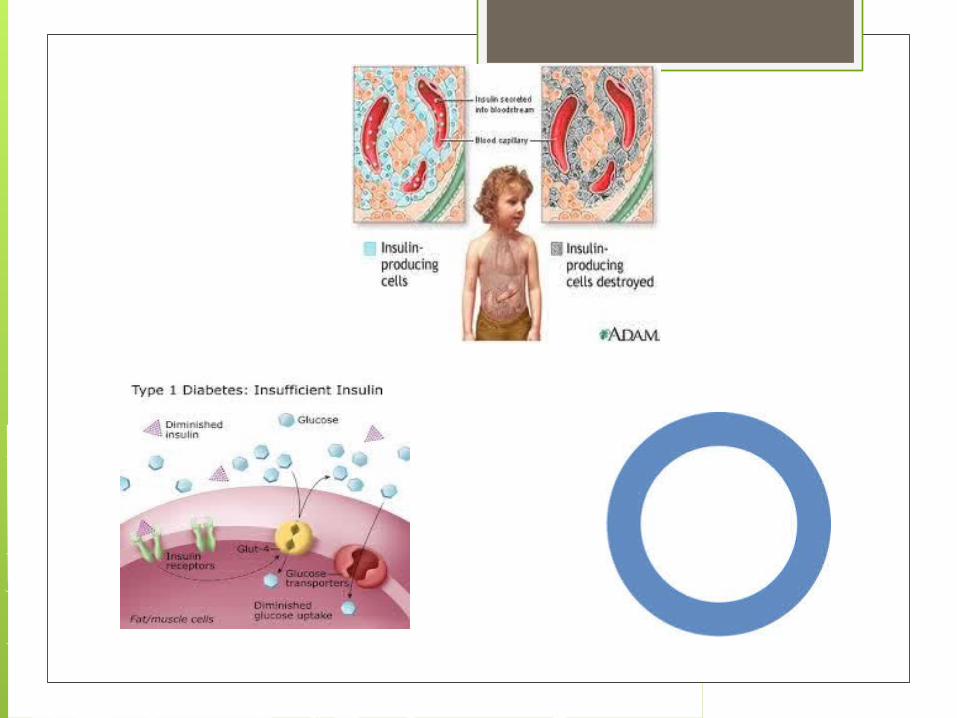
Type 1In type I (insulin-dependent diabetes mellitus [IDDM], previously called juvenile diabetes; !A) there is an absolute lack of insulin, so that the patient needs an external supply ofinsulin. The condition is caused by a lesion in the beta cells of the pancreas, as a rule produced by an autoimmune mechanism that may, in certain circumstances, have been triggered by a viral infection. The pancreatic islets are infiltrated by T lymphocytes and autoantibodies against islet tissue (islet cell antibodies[ICA]) and insulin (insulin autoantibodies [IAA]) can be detected. ICA may in some cases be detected years before the onset of the disease. After the death of the beta cells, the ICA again disappear. 80% of patients form antibodies against glutamatedecarboxylase expressed in the beta cells. Type I diabetes mellitus occurs more frequently in the carriers of certain HLA antigens (HLA-DR3 and HLADR4),i.e., there is a genetic disposition.


Type 2Type II (non-insulin-dependent diabetes mellitus [NIDDM], formerly called maturity onsetdiabetes; !B) is by far the most common form of diabetes. Here, too, genetic dispositionis important. However, there is a relative insulin deficiency: the patients are not necessarily dependent on an exogenous supply of insulin. Insulin release can be normal or even increased, but the target organs have a diminished sensitivity to insulin . Most of the patients with type II diabetes are overweight. The obesity is the result of a genetic disposition, too large an intake of food, and too little physical activity. The imbalancebetween energy supply and expenditure increases the concentration of fatty acids in the blood. This in turn reduces glucose utilization in muscle and fatty tissues. The result is a resistance to insulin, forcing an increase of insulin resistance .The resulting down-regulation of the receptors further raises insulin resistance. Obesity is an important trigger, but not the sole cause of type II diabetes. More important is the already existing genetic disposition to reduced insulin sensitivity. Frequently, insulinrelease has always been abnormal. Several genes have already been defined that promote the development to obesity and type II diabetes. Among other factors, the genetic defect of a mitochondrial decoupling protein limits substrate consumption. If there is a strong genetic disposition, type II diabetes can already occur at a young age (maturity-onset diabetes of the young [MODY]).

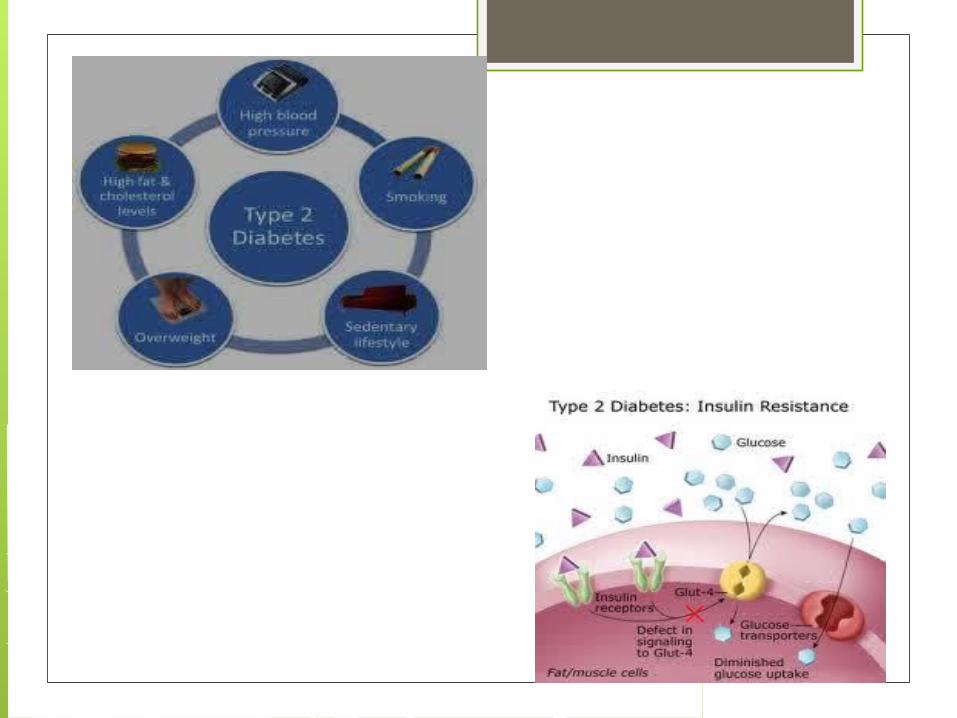

Table 24-8. Type 1 Versus Type 2 Diabetes Mellitus (DM)
Type 1 DM Type 2 DM
Clinical Onset: <20 years Onset: >30 years
Normal weight Obese
Markedly decreased blood insulin
Increased blood insulin (early);normal to moderate decreased insulin (late)
Anti-islet cell antibodies No anti-islet cell antibodies
Ketoacidosis common Ketoacidosis rare; nonketotic hyperosmolar coma
Genetics 30-70% concordance in twins 50-90% concordance in twins
Linkage to MHC Class II HLA genes
No HLA linkage Linkage to candidate diabetogenic genes (PPARγ, calpain 10)
Pathogenesis Autoimmune destruction of β-cells mediated by T cells and humoral mediators (TNF, IL-1, NO)
Insulin resistance in skeletal muscle, adipose tissue and liver β-cell dysfunction and relative insulin deficiency
Absolute insulin deficiency
Islet cells Insulitis early No insulitis
Marked atrophy and fibrosis Focal atrophy and amyloid deposition
β-cell depletion Mild β-cell depletion




MODY – Maturity Onset Diabetes of the Young
MODY is a monogenic form of diabetes with an autosomal dominant mode of inheritance:◦ Mutations in any one of several transcription factors or in the
enzyme glucokinase lead to insufficient insulin release from pancreatic ß-cells, causing MODY.
◦ Different subtypes of MODY are identified based on the mutated gene.
Originally, diagnosis of MODY was based on presence of non-ketotic hyperglycemia in adolescents or young adults in conjunction with a family history of diabetes.
However, genetic testing has shown that MODY can occur at any age and that a family history of diabetes is not always obvious.
MODY

MODY (cont.)

Within MODY, the different subtypes can essentially be divided into 2 distinct groups: glucokinase MODY and transcription factor MODY, distinguished by characteristic phenotypic features and pattern on oral glucose tolerance testing.
Glucokinase MODY requires no treatment, while transcription factor MODY (i.e. Hepatocyte nuclear factor -1alpha) requires low-dose sulfonylurea therapy and PNDM (caused by Kir6.2 mutation) requires high-dose sulfonylurea therapy.
MODY (cont.)

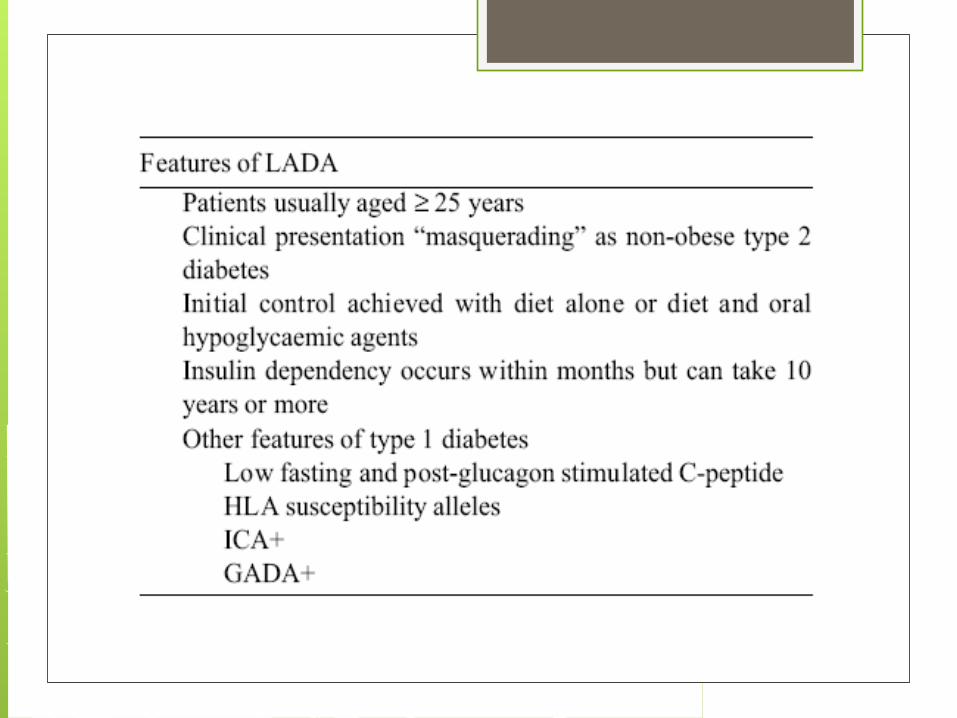
Latent Autoimmune Diabetes in Adults (LADA) is a form of autoimmune (type 1 diabetes) which is diagnosed in individuals who are older than the usual age of onset of type 1 diabetes.
Alternate terms that have been used for "LADA" include Late-onset Autoimmune Diabetes of Adulthood, "Slow Onset Type 1" diabetes, and sometimes also "Type 1.5
Often, patients with LADA are mistakenly thought to have type 2 diabetes, based on their age at the time of diagnosis.
LADA
LADA (cont.)

About 80% of adults apparently with recently diagnosed Type 2 diabetes but with GAD auto-antibodies (i.e. LADA) progress to insulin requirement within 6 years.
The potential value of identifying this group at high risk of progression to insulin dependence includes: the avoidance of using metformin treatment the early introduction of insulin therapy
LADA (cont.)



Long term complications of Diabetes
Increasing numbers of deaths from cardiovascular and renal complications
Renal (microvascular) disease is more common in type 1 diabetics
Cardiovascular disease (macrovascular) complications are more common in type 2 diabetics

Diabetic Vascular Diseases Chronic hyperglycemia causes
irreversible structural changes in the basement membranes of vessels. Result is thickening and organ damage.
Glucose toxicity affects cellular integrity Chronic ischemia in microcirculatory
brances>>cause connective tissue hypoxia and microischemia
Diabetic Vascular Diseases Up to 21% of diabetics have retinopathy
at time of diagnosis

Macrovascular Complications Coronary artery disease Cerebrovascular disease Peripheral arterial disease

Management of Macrovascular Diseases
Modify/reduce risk factors Meds for hypertension and
hyperlipidemia Smoking cessation Control of blood sugars

Microvascular Complications--Retinopathy
Diabetic retinopathy-leading cause of blindness in those 20-74
Blood vessel changes—worst case scenario, proliferative retinopathy. Also an increased incidence of cataracts and glaucoma in diabetics.
Need regular eye exams Control BP, control BS and cessation
of smoking can help
Microvascular complications-Nephropathy
Accounts for 50% of patients with ESRD Earliest clinical sign of nephropathy is
microalbuminuria. Warrants frequent periodic monitoring
for microalbuminuria—if exceeds 30mg/24h on two consecutive random urines, need 24h urine sample

Nephropathy Diabetes causes hypertension in renal
vessels which cause leaking glomeruli, deposits in narrow vessels, scarring and vascular damage

Microvascular disease-Nephropathy
Medical management: control BP (ACE or ARB)
Tx of UTIs Avoid nephrotoxic agents, contrast dyes Low sodium diet Low protein diet Tight glycemic control

Nephropathy May require dialysis May have co-existent retinopathy Kidney transplantation—success now
75-80% for 5 years Pancreas transplantation may also be
performed at time of kidney transplantation

Neuropathies Group of diseases that affect all types of
nerves. Includes peripheral, autonomic and
spinal nerves. Prevalence increases with duration of
the disease and degree of glycemic control

Neuropathies Capillary basement membrane
thickening and capillary closure may be present.
May be demyelination of the nerves, nerve conduction is disrupted.
Two most common types of neuropathy are: sensorimotor polyneuropathy and autonomic neuropathy.
Peripheral neuropathy Manifestations:paresthesias, burning
sensations, numbness, decrease in proprioception.
Charcot foot can result from abnormal weight distribution on joints secondary to lack of proprioception

Management of Peripheral Neuropathies
Pain management in the form of TCAs, Dilantin, Tegretol, Neurontin, mexilitene, and TENS. Cymbalta has been recommended. Also, the drug Lyrica (pregabalin)

Autonomic Neuropathies Cardiac, gastrointestinal and renal
systems Cardiac—myocardial ischemia may be
painless GI—delayed gastric emptying with early
satiety, nausea, bloating, diarrhea or constipation
Urinary retention—decreased sensation of bladder, neurogenic bladder

Autonomic neuropathy—hypoglycemia unawareness
No longer feel shakiness, sweating, nervousness and palpitations associated with hypoglycemia
The inability to detect warning signs of hypoglycemia can place the patient at very high risk

Autonomic neuropathy-sudomotor neuropathy
Patient will have a decrease or absence of sweating of the extremities with compensatory increase in upper body sweating.

Autonomic neuropathy—sexual dysfunction
Decreased libido in women Anorgasmia ED in men UTI and vaginitis Retrograde ejaculations

Management of neuropathies Early detection, periodic f/u on patient’s
with cardiac disease Monitor BP frequently for s/s orthostatic
hypotension Low fat diet, frequent small meals, close
BS monitoring and use of prokinetic medications
Meticulous skin care
Foot and Leg Problems Sensory loss Sudomotor neuropathy leads to dry,
cracking feet PAD—so poor wound healing/gangrene Lowered resistance to infection

Management of Foot and Leg Problems
Teaching patient foot care-inspect feet and shoes daily
Examine feet every time goes to doctor See podiatrist at least annually Closed toe shoes Trimming toenails Good foot hygiene Glycemic control is the key to
preventing complications


Management of Diabetes Mellitus

The major components of the treatment of diabetes are:
Management of DM
• Diet and ExerciseA
• Oral hypoglycaemic therapy
B
• Insulin TherapyC

Diet is a basic part of management in every case. Treatment cannot be effective unless adequate attention is given to ensuring appropriate nutrition.
Dietary treatment should aim at:◦ ensuring weight control◦ providing nutritional requirements◦ allowing good glycaemic control with blood
glucose levels as close to normal as possible◦ correcting any associated blood lipid abnormalities
A. Diet

The following principles are recommended as dietary guidelines for people with diabetes:
Dietary fat should provide 25-35% of total intake of calories but saturated fat intake should not exceed 10% of total energy. Cholesterol consumption should be restricted and limited to 300 mg or less daily.
Protein intake can range between 10-15% total energy (0.8-1 g/kg of desirable body weight). Requirements increase for children and during pregnancy. Protein should be derived from both animal and vegetable sources.
Carbohydrates provide 50-60% of total caloric content of the diet. Carbohydrates should be complex and high in fibre.
Excessive salt intake is to be avoided. It should be particularly restricted in people with hypertension and those with nephropathy.
A. Diet (cont.)

Physical activity promotes weight reduction and improves insulin sensitivity, thus lowering blood glucose levels.
Together with dietary treatment, a programme of regular physical activity and exercise should be considered for each person. Such a programme must be tailored to the individual’s health status and fitness.
People should, however, be educated about the potential risk of hypoglycaemia and how to avoid it.
Exercise

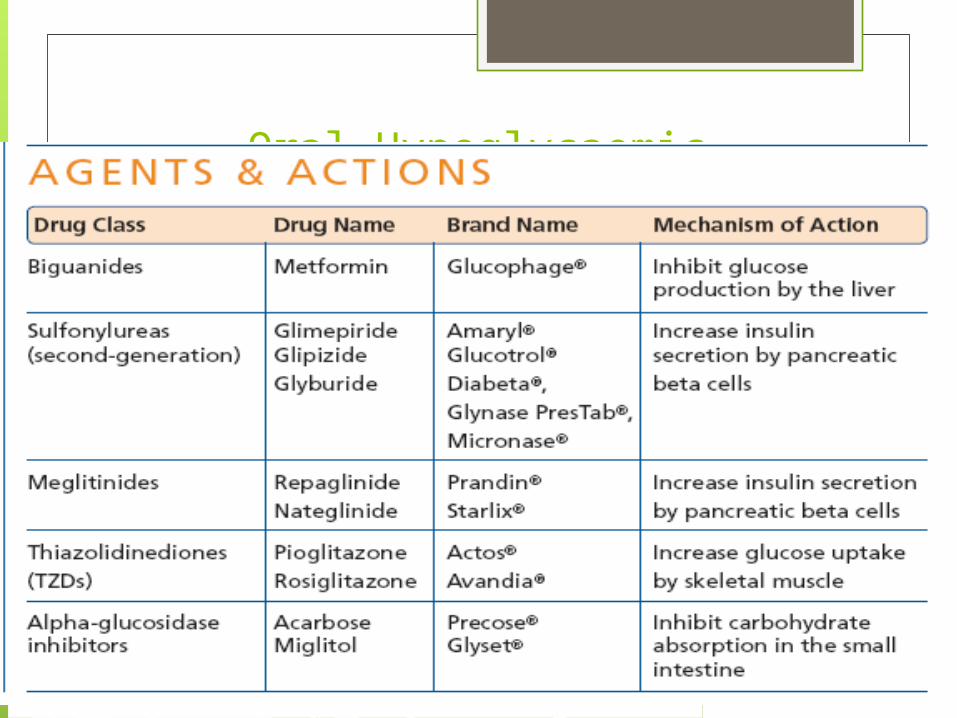
There are currently four classes of oral anti-diabetic agents:
i. Biguanidesii. Insulin Secretagogues – Sulphonylureasiii. Insulin Secretagogues – Non-
sulphonylureasiv. α-glucosidase inhibitorsv. Thiazolidinediones (TZDs)
B. Oral Anti-Diabetic Agents

SulfonylureasThese agents promote the
release of insulin from β-cells (secretogogues); tolbutamide, glyburide, glipizide and glimepiride.
Mechanism: These agents require
functioning β-cells, they stimulate release by blocking ATP-sensitive K+ channels resulting in depolarization with Ca2+ influx which promotes insulin secretion.
They also reduce glucagon secretion and increase the binding of insulin to target tissues.
They may also increase the number of insulin receptors
Pharmacokinetics: These agents bind to plasma proteins, are metabolized in the liver and excreted by the liver or kidney. Tolbutamide has the shortest duration of action (6-12 hrs) the other agents are effective for ~24 hrs.

SulfonylureasAdverse Effects: These agents tend to
cause weight gain, hyperinsulinemia and hypopglycemia. Hepatic or renal insufficiency causes accumulation of these agents promoting the risk of hypoglycemia. There are a number of drug-drug interactions. Elderly patients appear particularly susceptible to the toxicities of these agents.
Tolbutamide is asociated with a 2.5X ↑ in cardiovascular mortality.
Onset and Duration Short acting: Tolbutamide (Orinase) Intermediate acting: Tolazamide
(Tolinase), Glipizide (Glucotrol), Glyburide (Diabeta)
Long acting: Chloropropamide, Glimerpiride

Meglitinide analogsThese agents (repaglinide (Prandin) and nateglinide (Starlix))
act as secretogogues. Mechanism: These agents bind to ATP sensitive
K+channels like sulfonylureas acting in a similar fashion to promote insulin secretion however their onset and duration of action are much shorter. They are particularly effective at mimicking the prandial and post-prandial release of insulin. When used in combination with other oral agents they produce better control than any monotherapy.
Pharmacokinetics: These agents reach effective plasma levels when taken 10-30 minutes before meals. These agents are metabolized to inactive products by CYP3A4 and excreted in bile.
Adverse Effects: Less hypoglycemia than sulfonylureas; drugs that inhibit CYP3A4 (ketoconozole, fluconazole, erythromycin, etc.) prolong their duration of effect. Drugs that promote CYP3A4 (barbiturates, carbamazepine and rifampin) decrease their effectiveness. The combination of gemfibrozil and repaglinide has been reported to cause severe hypoglycemia.

Insulin SensitizersTwo classes of oral hypoglycemics work by improving insulin
target cell response; the biguanides and thiazolidinediones.Biguanides: Metformin is classified as an insulin sensitizer, it increases
glucose uptake and utilization by target tissues. It requires the presence of insulin to be effective but does not promote insulin secretion. The risk of hypoglycemia is greatly reduced.
Mechanism: Metformin reduces plasma glucose levels by inhibiting hepatic gluconeogenesis. It also slows the intestinal absorption of sugars. It also reduces hyperlipidemia (↓LDL and VLDL cholesterol and ↑ HDL). Lipid lower requires 4-6 weeks of treatment. Metformin also decreases appetite. It is the only oral hypoglycemic shown to reduce cardiovascular mortality. It can be used in combination with other oral agents and insulin.
Adverse effects: Hypoglycemia occurs only when combined with other agents. Rarely severe lactic acidosis is associated with metformin use particularly in diabetics with CHF. Drug interactions with cimetidine, furosemide, nifedipine and others have been identified.

Insulin SensitizersThiazolidinedion
es (Glitazones)
These agents are insulin sensitizers, they do not promote insulin secretion from β-cells but insulin is necessary for them to be effective. Pioglitazone and rosigglitazone are the two agents of this group.

Mechanism of Action: These agents act through the activation of peroxisome proliferator-activated receptor-γ (PPAR-γ). Ligands for PPAR-γ regulate adipocyte production, secretion of fatty acids and glucose metabolism. Agents binding to PPAR-γ result in increased insulin sensitivity is adipocytes, hepatocytes and skeletal muscle. Hyperglycemia, hypertriglyceridemia and elevated HbA1c are all improved. HDL levels are also elevated. Accumulation of subcutaneous fat occurs with these agents.

In the liver: ↓glucose output In muscle: ↑glucose uptake In adipose: ↑glucose uptake , ↓FA release Only pioglitazone may be used in combination with
insulin; the insulin dose must be modified. Rosiglitazone may be used with other hypoglycemic but severe edema occurs when combined with insulin.
Pharmacokinetics: Both are extensively bound to albumin. Both undergo extensive P450 metabolism; metabolites are excreted in the urine the primary compound is excrete unchanged in the bile.
Adverse Effects: Fatal hepatotoxicity has occurred with these agents; hepatic function must be monitored. Oral contraceptives levels are decreased with concomitant administration, this has resulted in some pregnancies.

α-Glucosidase InhibitorsThis enzyme hydrolyses
oligosaccharides to monosaccharides which are then absorbed. Acarbose also inhibits pancreatic amylase. The normal post-prandial glucose rise is blunted, glucose levels rise modestly and remain slightly elevated for a prolonged period, less of an insulin response is required and hypoglycemia is avoided; use with other agents may result in hypoglycemia. Sucrase is also inhibited by these drugs.

α-Glucosidase Inhibitors
Acarbose and miglitol are two agents of this class used for type 2 diabetes.
Mechanism of action: These agents are oligosaccharide derivatives taken at the beginning of a meal delay carbohydrate digestion by competitively inhibiting α-glucosidase, a membrane bound enzyme of the intestinal brush border.
Pharmacokinetics: Acarbose is poorly absorbed remaining in the intestinal lumen. Migitol is absorbed and excreted by the kidney. Both agents exert their effect in the intestinal lumen.
Adverse Effects: GUESS (flatulence, diarrhea, cramping). Metformin bioavailability is severely decreased when used concomitantly. These agents should not be used in diabetics with intestinal pathology.

If glycaemic control is not achieved (HbA1c > 6.5% and/or; FPG > 7.0 mmol/L or; RPG >11.0mmol/L) with lifestyle modification within 1 –3 months, ORAL ANTI-DIABETIC AGENT should be initiated.
In the presence of marked hyperglycaemia in newly diagnosed symptomatic type 2 diabetes (HbA1c > 8%, FPG > 11.1 mmol/L, or RPG > 14 mmol/L), oral anti-diabetic agents can be considered at the outset together with lifestyle modification.
B.1 Oral Agent Monotherapy

As first line therapy:
Obese type 2 patients, consider use of metformin, acarbose or TZD.
Non-obese type 2 patients, consider the use of metformin or insulin secretagogues
Metformin is the drug of choice in overweight/obese patients. TZDs and acarbose are acceptable alternatives in those who are intolerant to metformin.
If monotherapy fails, a combination of TZDs, acarbose and metformin is recommended. If targets are still not achieved, insulin secretagogues may be added
B.1 Oral Agent Monotherapy (cont.)

Combination oral agents is indicated in:
Newly diagnosed symptomatic patients with HbA1c >10
Patients who are not reaching targets after 3 months on monotherapy
B.2 Combination Oral Agents

If targets have not been reached after optimal dose of combination therapy for 3 months, consider adding intermediate-acting/long-acting insulin (BIDS).
Combination of insulin+ oral anti-diabetic agents (BIDS) has been shown to improve glycaemic control in those not achieving target despite maximal combination oral anti-diabetic agents.
Combining insulin and the following oral anti-diabetic agents has been shown to be effective in people with type 2 diabetes:◦ Biguanide (metformin)◦ Insulin secretagogues (sulphonylureas)◦ Insulin sensitizers (TZDs)(the combination of a TZD plus insulin is not
an approved indication)◦ α-glucosidase inhibitor (acarbose)
Insulin dose can be increased until target FPG is achieved.
B.3 Combination Oral Agents and Insulin

Diabetes Management
Algorithm
Oral Hypoglycaemic Medications

In elderly non-obese patients, short acting insulin secretagogues can be started but long acting Sulphonylureas are to be avoided. Renal function should be monitored.
Oral anti-diabetic agent s are not recommended for diabetes in pregnancy
Oral anti-diabetic agents are usually not the first line therapy in diabetes diagnosed during stress, such as infections. Insulin therapy is recommended for both the above
Targets for control are applicable for all age groups. However, in patients with co-morbidities, targets are individualized
When indicated, start with a minimal dose of oral anti-diabetic agent, while reemphasizing diet and physical activity. An appropriate duration of time (2-16 weeks depending on agents used) between increments should be given to allow achievement of steady state blood glucose control
General Guidelines for Use of Oral Anti-Diabetic Agent in Diabetes

The Goal of Insulin TherapyAdministration of insulins are arranged to mimic the normal basal, prandial and post-prandial secretion of insulin. Short acting forms are usually combined with longer acting preparations to achieve this effect.
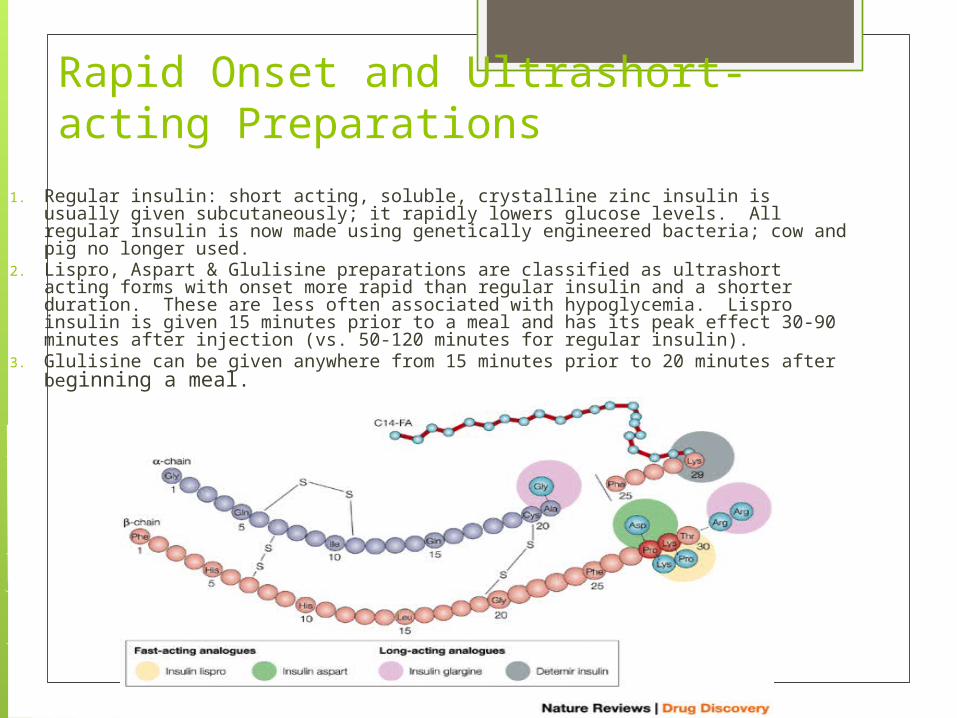
Rapid Onset and Ultrashort-acting Preparations
1. Regular insulin: short acting, soluble, crystalline zinc insulin is usually given subcutaneously; it rapidly lowers glucose levels. All regular insulin is now made using genetically engineered bacteria; cow and pig no longer used.
2. Lispro, Aspart & Glulisine preparations are classified as ultrashort acting forms with onset more rapid than regular insulin and a shorter duration. These are less often associated with hypoglycemia. Lispro insulin is given 15 minutes prior to a meal and has its peak effect 30-90 minutes after injection (vs. 50-120 minutes for regular insulin).
3. Glulisine can be given anywhere from 15 minutes prior to 20 minutes after beginning a meal.

Intermediate –acting Insulin Preparations
1. Lente insulin: This is a amorphous precipitate of insulin with zinc ion combined with 70% ultralente insulin. Onset is slower but more sustained than regular insulin. It cannot be given IV ( this has not been produced since 2005).
2. Isophane NPH insulin: Neutral protamine Hagedorn insulin is a suspension of crystalline zinc insulin combined with protamine (a polypeptide). The conjugation with protamine delays its onset of action and prolongs it effectiveness. It is usually given in combination with regular insulin.

Prolonged-acting insulin preparations1.Ultralente: a
suspension of zinc insulin forming large particles which dissolve slowly, delaying onset and prolonging duration of action.
2.Insulin glargine: Precipitation at the injection site extends the duration of action of this preparation.
3. Detemir insulin: has a FA complexed with insulin resulting in slow dissolution.
Pump vs. Standard Insulin Therapy

Insulin Preparations and TreatmentVarious types of insulin are characterized
by their onset and duration of action

Insulin Combinations
Various premixed combinations of various preparations of insulin are available to ease administration. Standard combination use should follow establishment of an acceptable regime of individual
preparations.

Action of Insulin on Various Tissues
Liver Muscle Adipose↓ glucose production ↑ Glucose transport ↑ glucose transport
↑ glycolysis ↑ glycolysis ↑ lipogenesis& lipoprotein lipase activity
↑ TG synthesis ↑ glycogen deposition ↓ intracellular lipolysis
↑ Protein synthesis ↑ protein synthesis

Adverse Effects of Insulin1. Hypoglycemia may occur due to insulin
overdose, insufficient caloric intake (missed meal, improper meal content, delayed meal, etc.). Ethanol consumption promotes hypoglycemic response. Symptoms: ↑ HR, diaphoresis, MS changes, anything (diabetics are usually really good at recognizing hypoglycemic symptoms).
2. Hypokalemia: insulin draws K+ into the cell with glucose (hyperglycemia with normal K+).
3. Anaphylaxis: when sensitized to non-human insulin gets non-human insulin (now rare).
4. Lipodystrophy at injection site5. Weight gain6. Injection complications

The majority of patients will require more than one daily injection if good glycaemic control is to be achieved. However, a once-daily injection of an intermediate acting preparation may be effectively used in some patients.
Twice-daily mixtures of short- and intermediate-acting insulin is a commonly used regimen.
In some cases, a mixture of short- and intermediate-acting insulin may be given in the morning. Further doses of short-acting insulin are given before lunch and the evening meal and an evening dose of intermediate-acting insulin is given at bedtime.
Other regimens based on the same principles may be used.
A regimen of multiple injections of short-acting insulin before the main meals, with an appropriate dose of an intermediate-acting insulin given at bedtime, may be used, particularly when strict glycaemic control is mandatory.
Insulin regimens

Overview of Insulin and Action


Patients should be educated to practice self-care. This allows the patient to assume responsibility and control of his / her own diabetes management. Self-care should include:
◦ Blood glucose monitoring◦ Body weight monitoring◦ Foot-care◦ Personal hygiene◦ Healthy lifestyle/diet or physical activity◦ Identify targets for control◦ Stopping smoking
Self-Care
Hypoglycemia Caused by too much insulin or oral
agents, too little food or excessive physical activity
Surge in epinephrine and norepinephrine results in sweating, tremors, tachycardia, palpitations, nervousness and hunger

Hypoglycemia CNS effects—inability to concentrate,
headache, lightheadedness, confusion, memory problems, slurred speech, incoordination, double vision, seizures and even loss of consciousness.

Hypoglycemic unawareness Related to autonomic neuropathy Will not experience the sympathetic
surge—with sweating, shakiness, HA, etc.


Treatment for hypoglycemia 2-3 tsp. of sugar or honey 6-10 hard candies 4-6oz. of fruit juice or soda 3-4 commercially prepared glucose
tablets Recheck BS 15 minutes, same s/s, repeat
treatment. After improvement, then cheese and crackers or milk.
Extreme situations, give glucagon. (can cause n/v). D50W.

Diabetic Ketoacidosis
Clinical features are:1. Hyperglycemia2. Dehydration and electrolyte loss3. acidosis

DKA Three main causes: illness, undiagnosed
and untreated and decreased insulin Other causes: patient error, intentional
skipping of insulin
Presentation of DKA 3 P’s Orthostatic hypotension Ketosis GI s/s Acetone breath hyperventilation
Diagnostic Findings of DKA BS between 300-800 Acidosis Electrolyte abnormalities Elevated BUN, creatinine and hct r/t
dehydration
Medical Management of DKA Rehydrate with normal saline, then
follow with .45% NaCl then D5.45NS (or other)
Restore electrolytes ECGs Hourly blood sugars IV insulin Avoid bicarbonate as can affect serum
K+

Nursing Management Administer fluids Insulin Prevent fluid overload Strict I&O Follow lytes ECG monitoring Vital signs Monitor patient responses to treatments

Hyperglycemic Hyperosmolar Nonketotic Syndrome
Predominated by hyperosmolarity and hyperglycemia
Minimal ketosis Osmotic diuresis Glycosuria and increased osmolarity Occurs over time Blood sugar is usually over 600
HHNS Occurs more often in older people Type 2 diabetes mellitus No ketosis Do not usually have the concomitant n/v Hyperglycemia, dehydration and
hyperosmolarity may be more severe than in DKA

Medical Management Similar treatment as seen in DKA Watch fluid resuscitation if history of
heart failure ECG Lytes monitoring Fluids with potassium replacement

Nursing Management of HHNS
Monitor neurologically Monitor ECG Monitor vital signs Labs Hourly blood glucose monitoring Insulin IV Cautious correction of hyperglycemia to
avoid cerebral edema

thanks


DIABETES EDUCATIONJOIN US ON FACEBOOK FOR DIABETES EDUCATION