diabetes mellitus in children - university of nevada, reno · 2020-05-23 · diabetes mellitus in...
TRANSCRIPT

Diabetes Mellitus in Children-Some Basics-
Anamaria Manea, MDPediatric Endocrinology
01/10/2020
Objectives Identify the symptoms of diabetes mellitus across the lifespan Review type 1 DM and type 2 DM Describe pertinent physical exam findings Review the labs used to confirm the diagnosis Discuss complications and screening labs Review management options

Diabetes Classification Type 1
– failure of beta cells resulting in insulin deficiency Type 2
– Insulin resistance + failure of beta cells to compensate – ‘relative’ insulin deficiency
Genetic defects in beta cell function– MODY (maturity onset diabetes of youth)
• AD; Single gene defect (MODY 1- 6)– Mitochondrial
Drug induced – Glucocorticoids– L-Asparaginase– Newer antipsychotics
Diseases affecting pancreatic function– CF, pancreatitis, hemolytic uremic sydrome
Genetic syndromes

Normal Fasting Blood Sugar <100
Impaired Glucose Tolerance >100 but <126 Fasting
Diabetes Fasting >126Random >2002 hr postprandial glucose>200HbA1c >=6.5%
Defining diabetes
Type I DM
Autoimmune destruction of pancreatic beta cells Insulin deficiency
– Deficient glucose utilization– Cells use alternate sources of fuel (fats ketones)– Hyperglycemia glucosuria polyuria
polydipsia
Type I DM: Epidemiology Most common cause of diabetes in children
– 80% of all diabetes 9 yrs old and younger
Incidence increasing– ~1-2 per 10,000 per year– Peak incidence is early adolescence
More common in Caucasian Less common in Asian and African American

Type I DM: Epidemiology
New onset T1DM: 30% in DKA at presentation - age 0–4: 37.5%- age 15-19: 14.7%

Type I DM: Etiology
Genetic susceptibility– monozygotic twins 40% risk– Siblings 5% risk
Environmental trigger– Infectious trigger? Incidence more common in
fall and winter– Possibly multiple potential triggers in early
infancy: viruses, cow’s milk, toxins
T1DM Management
Glucose Monitoring:
Check blood sugars 4 times/day– before breakfast, lunch, dinner, and bedtime – +/- in the middle of the night

Types of insulinInsulin
Onset(min)
Peak(hr)
Duration(hr)
Lispro/Humalog5 1 ½ 3
Aspart/Novolog 5 1 ½ 3Apidra 5 1- 1 ½ 3Regular 30 1-5 6-10NPH 120 6-8 8-20Levemir/Detemir 120 Dose
dependentDose
dependentGlargine/Lantus 180 No peak 24
Fast acting
Long acting

Glargine/Lantus
Bed timeB L D
Basal bolus insulin regimenLispro/Humalog or Aspart/Novolog and Glargine/Lantus
Hypoglycemia
Symptoms– Shaky, sweaty, hungry, weak, mood and
behavior changes– Waking up with HA, nightmares, restless sleeper
Treat with fast acting sugars– Recheck blood sugar in 15 minutes
Basal Insulin Typically lasts 24 hours in the body Important to give at the same time every
day Approx 50% of TDD (total daily dose) Given with or without food Same dose everyday – not dependent on
food intake or blood sugars

Bolus insulin
Used to cover the carbohydrate in food consumed
Utilize an insulin:carb ratio Correction doses used at meals and often
during illness and when ketones are present
Challenges for families Set doses

Hypoglycemia
After exercise, extra insulin doses If severe: seizures or altered mental status,
brain damage AMS/LOC: Glucagon IM, Basqimi Nasal
Glucagon

Sick Day Management
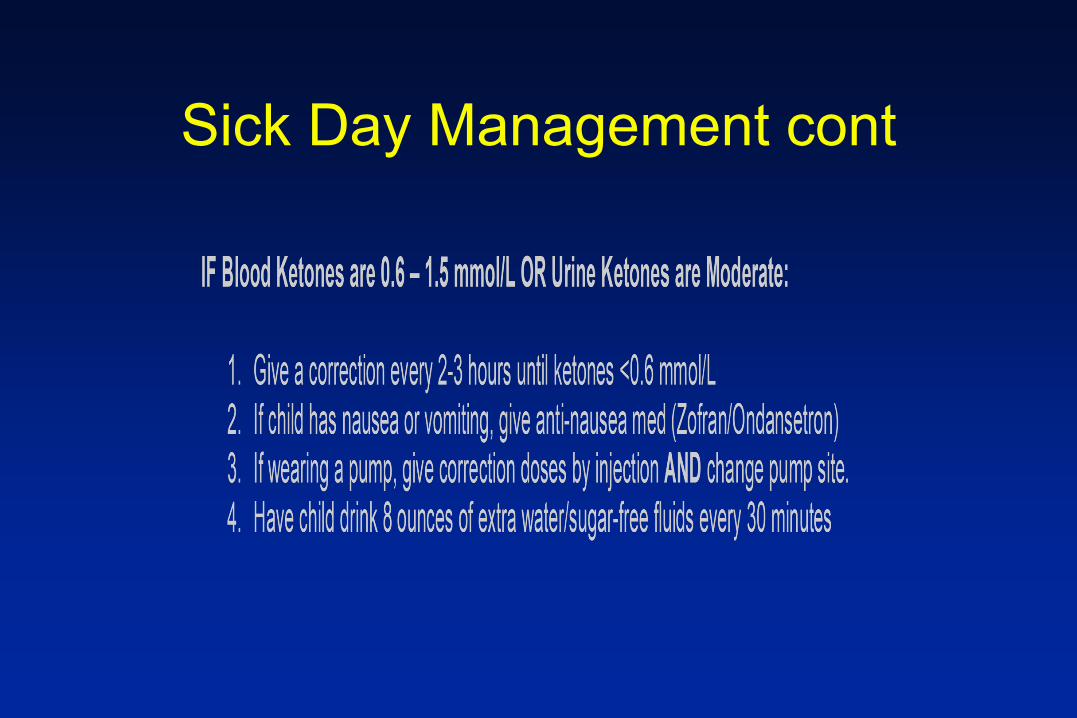
Sick Day Management cont

Sick Day Management cont
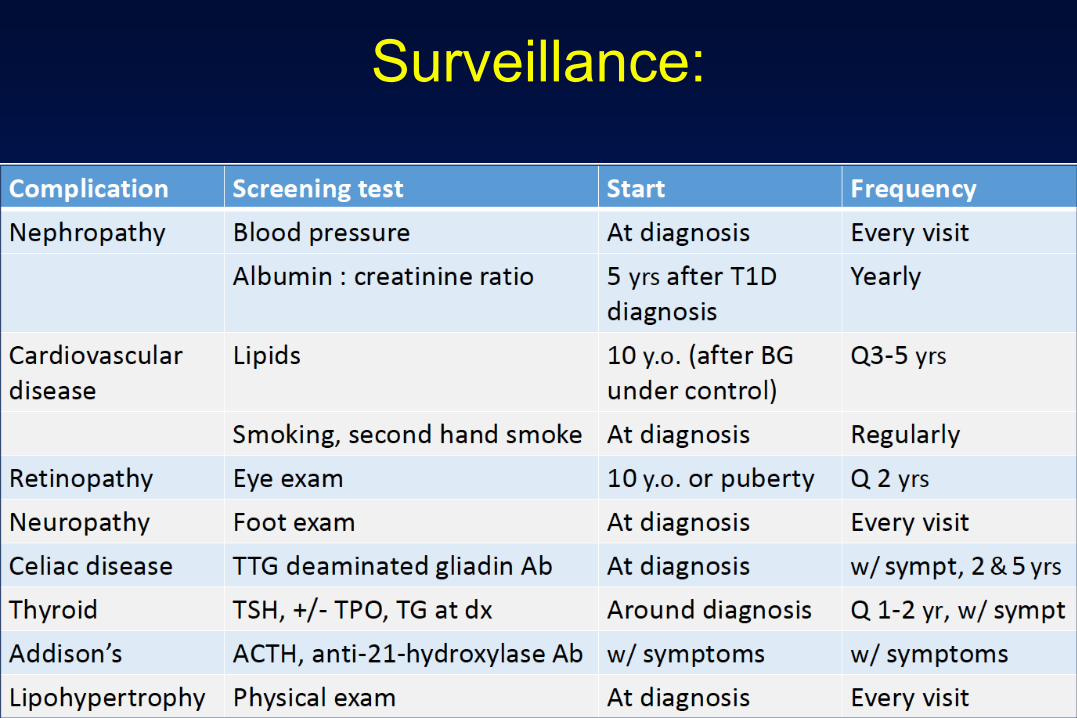
Surveillance:
DIABETES KETOACIDOSIS (DKA)
Missed insulin doses Missed warning signs Triggers: acute illness (URI, gastroenteritis, etc) High metabolic demand, not enough insulin, hyperglycemia, ketones Vomiting, abdominal pain, polyuria, Kussmaul breathing, AMS Dehydration, acidosis, electrolytes imbalance Admission (PICU) Treatment: NPO+IVF + insulin drip
Type 2 DM
Primary defect: – insulin resistance --- hyperglycemia ---
glucose toxicity to beta cells

ß Cell Function
Type 2 Diabetes Random blood sugar over 200 Fasting AM glucose >126 OGTT 2 hour glucose >200 Impaired Glucose Tolerance
Fasting AM glucose 100-126
OGTT 2hr glucose 140-200
The Path to Type 2 Diabetes
Type 2with DKA
↑ Glucose
Obesity-related insulin resistanceGlucose may be normal Asymptomatic
Epidemiology Increasing in incidence, particularly in the teenage years
– Mean age of diagnosis 13.5 yrs– Puberty: peak of insulin resistance
More common in non-Caucasian (African American, Hispanic, Native American)
Stronger (poly)genetic basis than type 1 – Almost 100% concordance in monozygotic twins– >75% of cases in youth have 1st or 2nd degree relative with T2DM
Diagnosis of T2DM Fasting plasma glucose ≥ 126 mg/dl
2-hr oral Glucose tolerance test– 75g glucose load– Plasma glucose 2 hrs later ≥ 200 mg/dl
Symptoms of DM + random plasma glucose ≥ 200 mg/dl – Symptoms: polyuria, polydipsia, weight loss,
glucosuria

Presentation of T2DM in Children Incidental finding Screening due to obesity or family history
of type 2 DM Polydipsia/polyuria Diabetic Ketoacidosis!!!
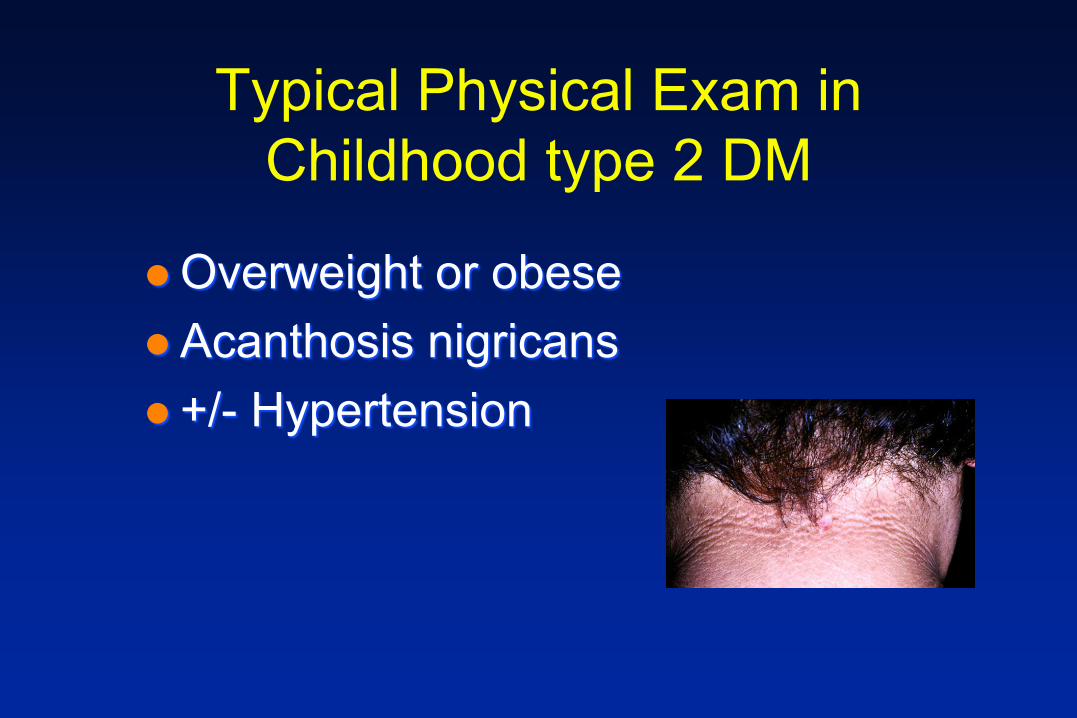
Typical Physical Exam in Childhood type 2 DM
Overweight or obeseAcanthosis nigricans +/- Hypertension

Management
Promote lifestyle changes – Weight loss, increased exercise
Oral hypoglycemic agents– Metformin
Insulin may be necessary – High doses needed due to insulin resistance
Goal for home glucose monitoring
Check at least twice a day– Morning and 1-2 hours after a meal– Check more often if on insulin– Check during symptoms of low blood sugar
The insulin resistance syndrome
Type II Diabetes Obesity Nephropathy Hypertension Dyslipidemia Polycystic Ovary Syndrome Non-alcoholic fatty liver disease Systemic inflammation
Metformin
Insulin sensitizer– Liver: ↓ gluconeogenesis ↓ hepatic
glucose production– muscle, fat tissue: ↑ glucose uptake– May help with ovulatory abnormalities in
girls with PCOS
Metformin: side effects
GI– Abdominal pain, diarrhea, nausea– Slow dosage titration over 3-4 weeks
• 500 mg daily 1000 mg bid
Lactic acidosis: extremely rare– Don’t use in renal impairment, liver
disease, cardiac/respiratory insufficiency
Insulin
Ketosis/ketoacidosis Oral agents inadequate (persistently
elevated HbA1c despite oral therapy) May be able to use Lantus only
Surveillance:
At diagnosis and yearly:- Lipids- Urine Alb/creatinine ratio- Dilated eye exam- Periodontal examination- Foot examination- Depression screening- BP every visit
15-25% of newly diagnosed T1DM may be obese
Many children with T2DM have ketonuria or DKA at diagnosis
Type 1 vs Type 2 DM: not always easy
Distinguishing Type 1 from Type 2
May be clinically obvious
Look for markers of islet cell autoimmunity– 80% - Anti GAD (glutamic acid decarboxylase) Ab– Islet cell antibodies– 5-10% of adults with Type 2 have one or more positive
antibody
Look for residual islet cell function– Serum insulin or C-peptide
Look at subsequent clinical course on insulin– Type 1 kids -“honeymoon” period– Type 2 kids- larger per kg insulin doses
Distinguishing Type 1 from Type 2

Presentation of Type 1 vs. Type 2
Type 1 Slender Weight loss Almost always symptomatic School age Caucasian No acanthosis nigricans Ketonuria usual Often presents with ketoacidosis
Type 2 Obese Often no weight loss Often asymptomatic Unusual in preteen Non-Caucasian Acanthosis nigricans Ketonuria less typical Ketoacidosis less frequent

Summary Type 1 and type 2 DM increasing in
incidence Helpful to distinguish between the two If ketonuria admit to the hospital and
start insulin If obese or signs of insulin resistance
lifestyle modification and metformin Monitor for comorbidities
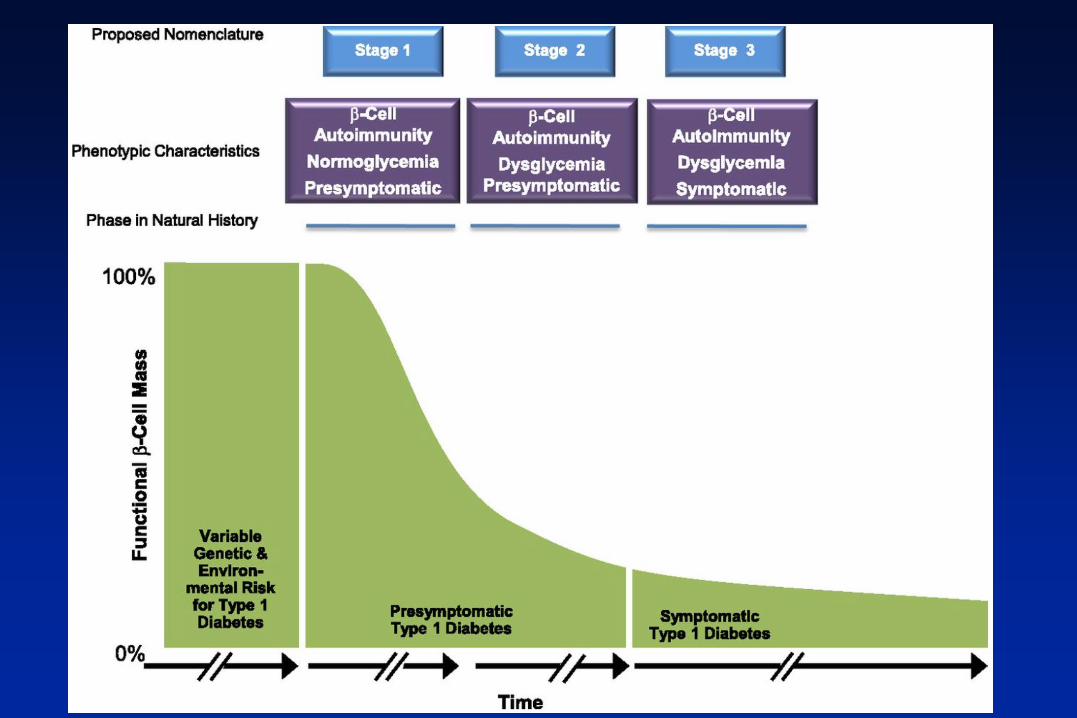
References Insel RA et al. Staging Presymptomatic Type 1 Diabetes: A Scientific Statement of
JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care 2015 Oct; 38(10):1964-1974
Standards of medical care in Diabetes 2019. ADA Chaing JL et al. Type 1 Diabetes in Children and Adolescents: A Position Statement
by the American Diabetes Association. Diabetes Care 2018 Sept; 41(9): 2026-2044 Arslanian S. Evaluation and Management of Youth-Onset Type 2 Diabetes: A
Position Statement by the American Diabetes Association. Diabetes Care 2018 Dec; 41(12): 2648-2668