diabetes recognition program (drp) - ce...
TRANSCRIPT

1
Diabetes Recognition Program (DRP)
A Tool for Improving Quality
Cynthia Martin, ManagerPhysician Recognition Programs, NCQA
Program Overview• NCQA and DRP Overview: Cynthia Martin, Manager, Physician
Recognition Programs, Washington, DC
• Perspectives from a Health Plan: Twyla Johnson, MPH, MBA, M P id Q lit P f M t t Manager, Provider Quality Performance Management, at Highmark, Inc., Pittsburgh, PA
• Perspectives from a Primary Care Practice: Joe Whalen, MD, Mint Hill Family Practice, Medical Director for Disease Management, Southern Piedmont Region of Novant Health, Charlotte, NC
i f d i l i S i h
2
• Perspectives from an Endocrinology Practice: Steven B. Leichter, M.D., F.A.C.P., F.A.C.E, Senior Partner, Endocrine Consultants, PC, The Center for Diabetes and Metabolism, Columbus, GA
• Support provided by Pfizer, Inc.

2
• NCQA Overview
Section Agenda
• NCQA Recognition Programs
• DRP Application & Survey Process
• Benefits of Recognition
3
• NCQA is a private, independent non-profit health care quality oversight organization founded in 1990
• NCQA is committed to measurement transparency and
A Brief Introduction
• NCQA is committed to measurement, transparency, and accountability
• NCQA unites diverse groups around a common goal: improving health care quality
MISSIONTo improve the quality of health care
4
p q y
VISIONTo transform health care through quality measurement, transparency, and accountability

3
NCQA Achieving the Mission• Over 800 plans report HEDIS® data to NCQA
(Commercial, Medicaid, Medicare, HMO/PPO)
• Over 250 commercial MCO plans are accredited by Over 250 commercial MCO plans are accredited by NCQA
• Over 75 Medicaid plans are accredited by NCQA
• Over 100 Medicare Advantage plans are accredited by NCQA (more than any other accrediting body)
O 85 9 illi ti t i t d th h th
5
• Over 85.9 million patients are impacted through the plans NCQA accredits
• Over 14,000 clinicians are recognized nationally by NCQA programs
• Current programs: DRP, HSRP, BPRP, PPC, PCMH• What measures included: Structure, process and
outcomes of excellent care management
NCQA Recognition Programs
outcomes of excellent care management• Where they come from: partnership with leading national
health organizations• Who rewards recognized clinicians: many health plans
and coalitions of employers• Who is recognized: over 14,000 clinicians nationally
6

4
Number of Clinician Recognitions by State
•ME
•VT
•MA•NY
•WA
•OR•WI
•MN
•MI
•MT
•SD
•ND
•ID•NH
as of 7/31/09
•RI
•NJ
•MD
MA
•DE
•AZ
•NV
•NM
•NE
•KS•CO
•IA
•NC
MI
•PA•OH
•VA•MO
•OK
•GA
•SC•TN
•KY
•WV
•AR
•LA
•AL
•IN•IL
•WY
•UT•CA
•CT
•MS• 0 Recognitions
7
•FL
•HI
•TX
•AK
• 101-500 Recognitions
• 26-100 Recognitions
• 1-25 Recognitions
• 501+ Recognitions
What is the DRP applicationand survey process?
8
5
• Developed in partnership with American Diabetes Association (ADA); released in 1997
V l t iti
DRP Basics…
• Voluntary program; non punitive
• Report only clinicians who earn Recognition
• Use nationally recognized reliable, valid measures
9
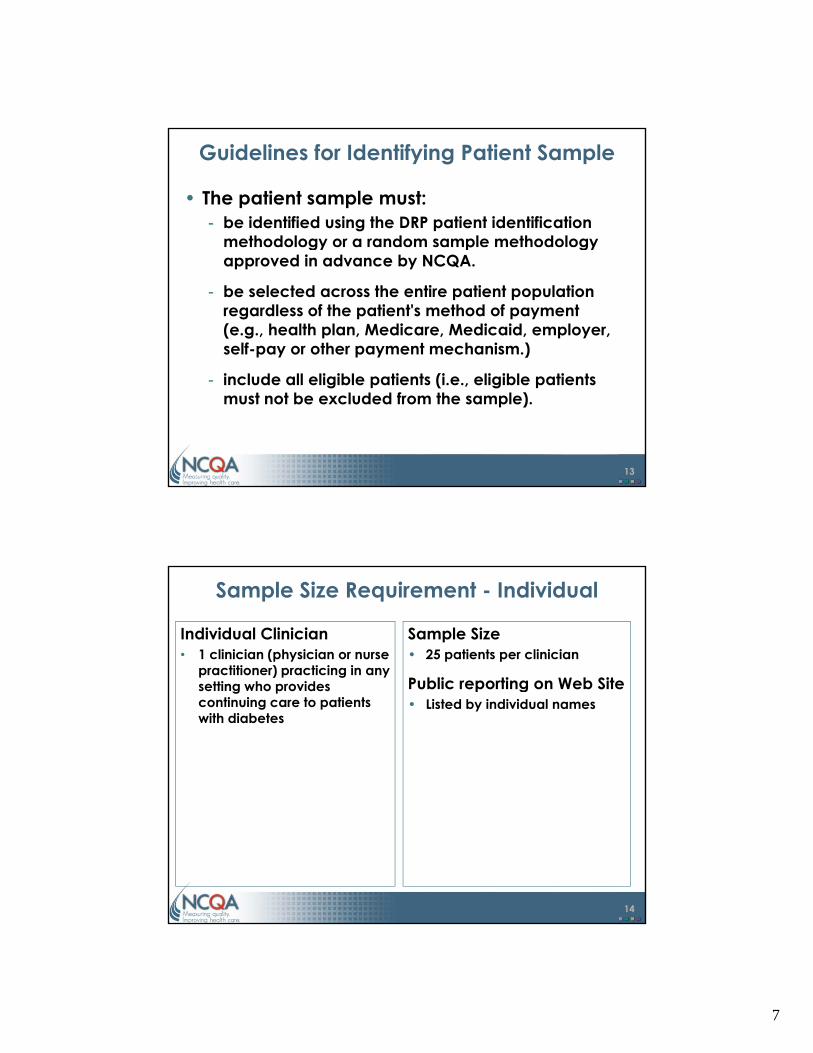
2009 DRP Adult Measures• Outcome Measures
– HbA1c Control >9.0%*– HbA1c Control <8.0%– HbA1c Control <7.0%– Blood Pressure Control ≥140/90 mm Hg*– Blood Pressure Control <130/80 mm Hg– LDL Control ≥130 mg/dl*– LDL Control <100 mg/dl
• Process MeasuresEye Examination
10
– Eye Examination– Foot Examination– Nephropathy Assessment– Smoking Status and Cessation Advice or Treatment
*A measure of poor control

6
Who May Apply?
• An individual clinician (i.e., physician or nurse practitioner) or a clinician group
• To be eligible, applicants must:– have a current, non restricted license as a doctor
of medicine (MD) or doctor of osteopathy (DO) or nurse practitioner (NP)
id ti i t ti t ith di b t
11
– provide continuing care to patients with diabetes
– have had face-to-face contact with and submit data on a sample of patients with diabetes
• Review program information - www.ncqa.org/DRP
• Purchase the “2009 DRP Package”- Package contains all the information needed to apply for Recognition
What is the Process?
Package contains all the information needed to apply for Recognition• Review materials & sign Agreement
- DRP Requirements- Recognition Review Agreement and BA Agreement- Data Collection Tool (Web-based)
• Identify the patient sample- Patient sample must be identified using the DRP patient selection
methodology or a random sample methodology approved in advance
12
g gby NCQA
• Abstract medical record data• Enter data in Data Collection Tool• Submit completed materials to NCQA
7
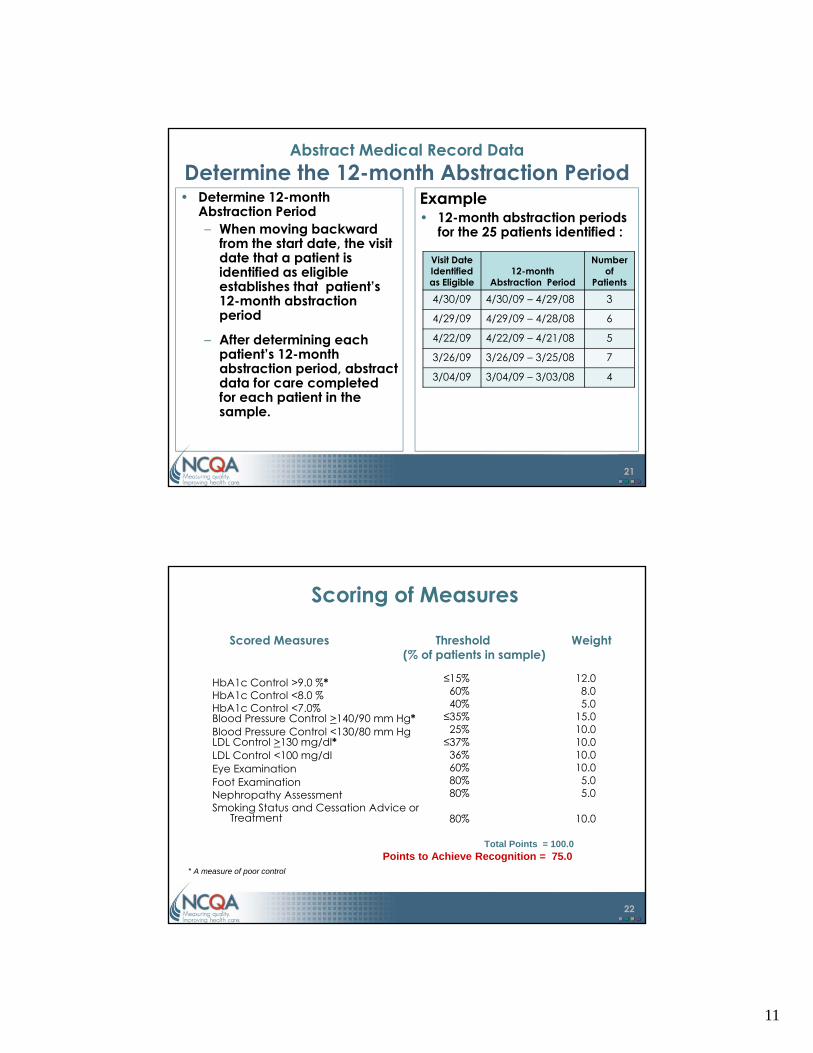
Guidelines for Identifying Patient Sample
• The patient sample must:- be identified using the DRP patient identification
methodology or a random sample methodology gy p gyapproved in advance by NCQA.
- be selected across the entire patient population regardless of the patient's method of payment (e.g., health plan, Medicare, Medicaid, employer, self-pay or other payment mechanism.)
13
- include all eligible patients (i.e., eligible patients must not be excluded from the sample).
Sample Size Requirement - Individual
Individual Clinician • 1 clinician (physician or nurse
practitioner) practicing in any setting who provides
Sample Size• 25 patients per clinician
Public reporting on Web Sitesetting who provides continuing care to patients with diabetes
Public reporting on Web Site• Listed by individual names
14

8
Clinician Group• An entity (e.g., group
practice) of 2 or more clinicians:
Sample Size• A maximum of 200 patients as
shown in the table below:
Sample Size Requirement – Group
Number of i i i i
Sample Size i
– who practice at the same site
– who share responsibility for a common panel of patients
clinicians in Group Requirement
2 50
3 75
4 100
5 125
6 150
7 175
8 200
9 or more 200
15
Public reporting on Web Site• Listed by group or site name only
Patient Selection Methodology
• Pick a “Start Date”– The date applicants begin to select the patient sample
• On each day moving backward from the start date, consecutively evaluate the eligibility of each patient seen for an office visit
• Select patients meeting the 3 eligibility criteria until the required sample size is met
16
e equ ed sa p e s e s e – May not go back more than 12 months from the start
date to select patients

9
Eligible Patient Definition
• An eligible patient is one who meets 3 criteria: Is 5 years of age or older
• pediatric patients 5 – 17 years• adult patients 18 – 75 years
– has had a diagnosis of diabetes or notation of prescribed insulin or oral hypoglycemics/antihyperglycemics for at least 12 months
has been under the care of the applicant clinician
17
(or clinician group*) for at least 12 months.
*Does not apply to clinicians seeking individual recognition
Select the Patient SampleStep 1 – Establish a Start Date
Step 1
• Establish a Start DateThe Start Date is the date
Example• You select May 1, 2009
- The Start Date is the date you begin to select the patient sample
AttentionApplicants must submit the
completed DCT and
18
psupporting materials to
NCQA within 180 calendar days of the start date.

10
Select the Patient Sample Step 2 – Identify Eligible Patients
Step 2• Identify eligible patients
– On each day moving backward from the start d t ti l
Example• Moving consecutively
backward from 5/1/09, you identify 25 eligible patients date, consecutively
evaluate the eligibility of each patient seen for an office visit
– Select patients who meet the 3 eligibility criteria
– Identify eligible patients until the required sample i i t
identify 25 eligible patients who had office visits on the following dates:
Visit Date Identified as Eligible
Number of Patients
identified
4/30/09 3
4/29/09 6
19
size is met • May not go back more
than 12 months from the start date to select patients
4/29/09 6
4/22/09 5
3/26/09 7
3/04/09 4
Abstract Medical Record Data
• After selecting the patient sample, abstract data for patient care completed:
– for a12-month period going back from the last visit date that occurred prior to the start date
– from medical record documentation (electronic or paper), administrative data systems or registries
20
11
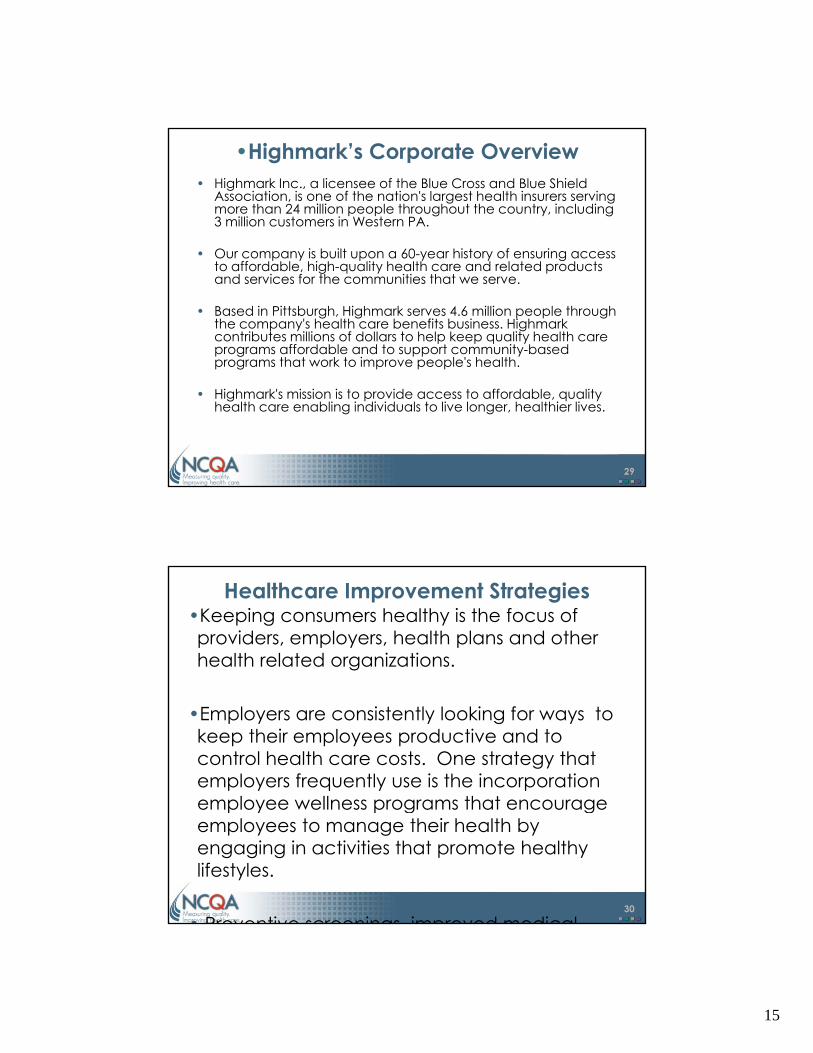
Abstract Medical Record Data Determine the 12-month Abstraction Period
• Determine 12-month Abstraction Period – When moving backward
from the start date, the visit
Example• 12-month abstraction periods
for the 25 patients identified :from the start date, the visit date that a patient is identified as eligible establishes that patient’s 12-month abstraction period
– After determining each patient’s 12-month abstraction period abstract
Visit Date Identified as Eligible
12-month Abstraction Period
Number of
Patients
4/30/09 4/30/09 – 4/29/08 3
4/29/09 4/29/09 – 4/28/08 6
4/22/09 4/22/09 – 4/21/08 5
3/26/09 3/26/09 – 3/25/08 7
21
abstraction period, abstract data for care completed for each patient in the sample.
3/04/09 3/04/09 – 3/03/08 4
Scoring of Measures
Scored Measures Threshold Weight(% of patients in sample)
HbA1c Control >9 0 %* ≤15% 12.0HbA1c Control >9.0 %HbA1c Control <8.0 %HbA1c Control <7.0%Blood Pressure Control >140/90 mm Hg*Blood Pressure Control <130/80 mm Hg LDL Control >130 mg/dl* LDL Control <100 mg/dl Eye Examination Foot Examination Nephropathy Assessment S ki St t d C ti Ad i
60%40%≤35%25%≤37%36%60%80%80%
8.05.0
15.010.010.010.010.05.05.0
22
Smoking Status and Cessation Advice orTreatment
Total Points = 100.0Points to Achieve Recognition = 75.0
* A measure of poor control
80% 10.0

12
Data Collection Tool
23
Data Submission
Materials to submit:• Signed DRP Recognition Review Agreement (2
copies)p )• Completed Data Collection Tool
– Submitted via secure portal• Application fee
– Payable by check or credit card
24

13
What Happens Next?
• Within 30 - 60 days of receiving all information needed to complete the application, NCQA reviews and makes recognition decisions– 5 percent of applications are selected for
audit
• Clinicians or groups achieving Recognition receive:– letter of recognition– posting to the Recognition Directory
25
posting to the Recognition Directory– certificate of Recognition– media kit/marketing and advertising
guidelines
Benefits of Recognition
• Distinction in provider directories• Receive referrals from ADA’s National Call Center
Establish eligibility for pay for performance rewards or • Establish eligibility for pay-for-performance rewards or differential reimbursement from payers and health plans– For example:
• Bridges to Excellence (BTE)• Physician Quality Reporting Initiative (PQRI)
• Receive credit toward maintenance of board
26
• Receive credit toward maintenance of board certification– For example:
• American Board of Family Medicine (ABFM)• American Board of Internal Medicine (ABIM)

14
• Mailing AddressNCQADiabetes Recognition Program1100 13th Street NW Suite 1000
DRP Contact Information
1100 13th Street, NW, Suite 1000Washington, DC 20005
• Customer Support(questions on DRP in general, purchasing the Data Collection Tool , etc.)
1-888-275-7585
• DRP Staff( ti li th d l t )
27
(questions on sampling methodology, measures, etc.)[email protected]
• Webwww.ncqa.org/DRP
DPRP and Highmark Inc : DPRP and Highmark Inc.: A Health Plan Perspective
Twyla Johnson, ManagerProvider Quality Performance Management, Highmark Inc.
15
•Highmark’s Corporate Overview• Highmark Inc., a licensee of the Blue Cross and Blue Shield
Association, is one of the nation's largest health insurers serving more than 24 million people throughout the country, including 3 million customers in Western PA.
• Our company is built upon a 60-year history of ensuring access to affordable, high-quality health care and related products and services for the communities that we serve.
• Based in Pittsburgh, Highmark serves 4.6 million people through the company's health care benefits business. Highmark contributes millions of dollars to help keep quality health care programs affordable and to support community-based programs that work to improve people's health.
29
p g p p p
• Highmark's mission is to provide access to affordable, quality health care enabling individuals to live longer, healthier lives.
Healthcare Improvement Strategies•Keeping consumers healthy is the focus of providers, employers, health plans and other health related organizations.
•Employers are consistently looking for ways to keep their employees productive and to control health care costs. One strategy that employers frequently use is the incorporation employee wellness programs that encourage
30
employee wellness programs that encourage employees to manage their health by engaging in activities that promote healthy lifestyles.
• Preventive screenings improved medical

16
National Focus on Quality Improvement• Institute for Healthcare Improvement
-100 Thousand and 5 Million Lives Campaign
N ti l Q lit F• National Quality Forum-Measurement Standardization and
Endorsement• Four Cornerstones for Value Driven Healthcare
-Interoperable Health Information Technology
31
Technology-Measure and Publish Quality Information-Measure and Publish Cost Information-Promote Efficiency and Quality through
Incentives
•Highmark’s Commitment to Quality Improvement
• Highmark consistently invests in network providers as a means of building a foundation of high quality cost effective care that enables g q your members to have a greater hand in their health. The following are a few examples of Highmark’s commitment to quality improvement:
• Highmark’s Medical Management Consultant
32
• Highmark s Medical Management Consultant staff provides quality improvement support, education and training to over 3,221 physicians;
• The Highmark Pilot Program for NCQA Ph i i R iti i t h i i th

17
•Highmark’s Engagement Philosophy
•Highmark - Healthcare Provider-Account-Member Collaboration
•
•15 Dedicated •Medical Management
Consultants
•Dedicated Medical Directors
•2 Clinical Pharmacists
•20 Network Provider •Relations Representatives
33
•Improved Health Status – Patients; Shared Savings and Efficiencies
•Evidence Based Care Tools, Best Practices and Information
•Network, Peer, Customized Data, Trends Reports, Action Plans,
Performance Targets
•
•Accounts, Clients• Members
Medical Management Consultant Processes
• Assess where the practice lies against quality performance criteria - the Quality Improvement Roadmap to Success
• Evaluate the practice office operations to determine process improvement opportunities - Clinical Office Process Evaluation Key Questions Questions
• Meet with the physicians and staff to provide feedback and recommend a course of action to improve clinical quality and office operations
• Collaborate with the physicians and staff to create a work plan that:
- defines the problem; - establishes baseline measures; - specifies action steps; - designates responsible team member;
34
designates responsible team member; - establishes a timeline for expected outcomes; and - incorporates a control mechanism to ensure the operations don’t
falter.
• Scheduled meetings to monitor and report on the practice’s performance against their clinical quality and process improvement activities

18
•Why Is the NCQA Pilot Program Important to Highmark?
• The NCQA program was implemented as a strategic initiative that supports Highmark’s strategy of working collaboratively with strategy of working collaboratively with network providers to improve care to our members.
• It is also intended to meet Highmark employer account and member expectations of attracting and retaining a
35
p g gnetwork of high performing, efficient and effective primary care providers and specialists who are recognized locally and nationally as the premier providers of quality care.
•Highmark Pilot Program for NCQA Physician Recognition: Diabetes
• The program provides administrative and financial support to Primary Care Physicians (PCP) and Endocrinologists who are attempting to gain NCQA recognition by providing documentation of their patient’s care against nationally recognized evidence based medical guidelines.
• The first phase of the program began in Western PA in Jan ‘07 and ended in Dec ‘07
36
Western PA in Jan 07 and ended in Dec 07. The second phase of the program is currently underway in Central PA and will continue until 2009.
• The pilot program is divided into three distinct levels. This enables the staff to measure

19
•Highmark Program Planning Phase• Prior to implementation, Highmark worked
closely with the NCQA staff to develop processes and procedures for carrying out specific phases of the program.
• Staff training: NCQA staff provided on-line training on the DPRP guidelines to the Highmark team via webinar. This was
37
conducted to allow the MMC staff to gain complete knowledge of the NCQA requirements prior to educating the physicians.
•Highmark Pilot Program Western PA •Diabetes Results
• Five hundred and thirty nine (539) physicians • Five hundred and thirty nine (539) physicians applied to participate in the Diabetes program. Fifty percent (50%) or 271 physicians from 93 practices were selected to participate.
38
• 143 or 53% of the physicians specialize in Family Practice, 98 or 36% of the physicians specialize in Internal Medicine, 29 or 11% of the physicians practice in multi-specialty practices and only 1 – less than 1% of the

20
•Highmark Pilot Program Western PA •Diabetes Results
100% 100%90% 90% 86%
Percent of Physicians Completing the Diabetes Program
90% 90% 86% 80%
20%
40%
60%
80%
100%
% o
f Ach
ieve
men
t
39
0%
20%%
Level 1 Level 2 Level 3
Percent of Physicians Goal
•Highmark Pilot Program Western PA •Diabetes Results
•The clinical results of the Diabetes program showed marked improvement across several measures. The following table shows the percent improvement of physician practices between the pre-survey and post survey.
Diabetes Program Measures Criteria Pre-Survey Post-Survey % Change
HbA1c Poor Control >9.0% <=15% of patients 78% 91% 17%
HbA1c Control <7.0% 40% of patients 72% 92% 27%
Blood Pressure >=140/90 mm Hg <=35% of patients 96% 97% 2%
Blood Pressure Control <130/80 mm Hg 25% of patients 56% 85% 51%
Retinal Screening 60% of patients 38% 48% 25%
Smoking Status & Cessation Advice 80% of patients 93% 99% 7%
LDL >=130 <=37% of patients 97% 99% 2%
40
LDL > 130 < 37% of patients 97% 99% 2%
LDL <100 36% of patients 89% 97% 9%
Nephropathy Assessment 80% of patients 50% 64% 28%
Foot Examination 80% of patients 59% 77% 32%
TOTAL (Score=100) 9% 32% 276%
TOTAL (Score= 75 - 100) 63% 97% 55%
•Note: The pre-survey is based on 2,355 patients and the post survey reflects 4,653 patients. • Based on an 81% return rate of physicians in 75 out of 93 practices.

21
•Recognition of Physician Participants
41
•
•Recognition of Physician Participants
• •Cynthia Ayers, MD, left, displays her NCQA Recognition
•Michael Madden, MD, left, Highmark medical director, Medical Performance •Management talks with Mina
•Sandra Tomlinson, senior vice president, Provider Services, and Ken Melani, MD, Highmark president and
42
Award with Renee Reynolds.Management, talks with Mina
Harkins, center, assistant vice president, Physician Recognition Programs, NCQA and Bruce Bagley, Medical Director for Quality Improvement, American Academy for Family Physicians.
, g pCEO, both congratulated providers on NCQA recognition.

22
Recognition in Highmark Marketing & Communications Products
43
•Recognition in Highmark Marketing & Communications Products
44

23
Recognition in Highmark’s QualityBLUE Physician Pay For Performance Program• QualityBLUE is available in 49 counties with more than 5,000 physicians from
1,500 practices eligible to participate.
• The program aligns a portion of provider reimbursement with performance on clinical quality measures generic prescribing member access electronic clinical quality measures, generic prescribing, member access, electronic prescribing, utilization of electronic health record and implementation of office based best practices.
• The Best Practice component of QualityBLUE requires physicians to conduct innovative practice improvement studies focusing on medical management and clinical quality issues that are not a part of the clinical quality measures within the QualityBLUE program.
• It reinforces and teaches the continuous quality improvement model for primary care practices, while encouraging innovation and core problem
45
primary care practices, while encouraging innovation and core problem solving.
• Physicians are also able to earn points for professional certification or recognition activities from NCQA and other national organizations as a part of the Best Practice component of QualityBLUE.
Recognition in Highmark’s Provider Directory
The Provider Directory publishes physician demographic information on Highmarkbcbs.com based on a physician practice questionnaire that can be updated at any time via NaviNetR. This information is available on the Internet.
i
46
•Highmarkbcbs.com
•330,000 hits/month•Provider Directory page
visited most often
24
Summary
• Committed to Quality• Expanding program to Central PA• Looking for opportunities to address other
clinical areas
47
Joseph B Whalen MD
DPRP and Novant Health:A Primary Care Perspective
Joseph B. Whalen, MDNovant Health, Charlotte, NC

25
NCQADiabetes Physician Recognition Program
• About Novant Health• Trends in Health CareTrends in Health Care• Benefits of DPRP Participation• Costs/Barriers of Participation in DPRP• Outcomes of Our Participation in DPRP
49
About NOVANT HEALTH
• NOVANT HEALTH is a not-for profit, integrated health care system in North Carolina serving more than 4 million people reaching from southern Virginia to p p g gnorthern South Carolina
• Mission: to improve the health of communities, one person
at a time
Inpatient Facilities: 9 (Licensed Beds: 2,650)
50
p ( , )Plus Partnership Hospitals: 7
Long-terms Care Facilities: 2 (Licensed Beds: 351)Medical Group Physicians: 882 (269 clinic locations) Physician Medical Group Visits: 3,193,309 (2007)
26
Novant Medical Group Disease Management
• NCQA Program Participation– Diabetes Physician Recognition Program y g g
• (65-70% of eligible Novant Medical Group physicians recognized)
– Heart & Stroke Recognition Program • (55-60% of eligible Novant Medical Group physicians
recognized)
• Corporate Sponsorship
51
Co po a e Spo so s p– Executive support– Physician champions established– Dedicated staff (8 RNs/analysts)
Trends in Health Care
• Quality Overview • Reimbursement Trends
• Pay for Performance (P4P)• Physician Quality Reporting Initiative (PQRI)• Nonpayment for Nonperformance
• Quality Organizations
52

27
8 Points of Quality Care1. Everyone wants high-quality healthcare – patients, doctors, employers
and payers.2. High-quality is delivering the right amount of healthcare at the right time
to improve the health of your patients without providing unnecessary treatment that can increase the cost and risk to your patients.
3 M j h ll f t d ’ h lth i l d d fi i d li i 3. Major challenges for today’s healthcare include defining, delivering, measuring and reimbursing high-quality healthcare.
4. Physicians will increasingly be graded and ranked according to the measured quality of care they deliver.
5. Adhering to basic quality guidelines is not too difficult as long as the right systems are in place.
6. There is emerging evidence that performance measurement, monitoring and recognition of excellence improves care and lowers costs.
53
7. Quality measurement is here to stay and the trend toward paying providers based on their quality of care will accelerate in the coming years.
8. Physicians who accept and embrace these challenges stand the best chance of surviving and prospering.
Trends in Health Care
• Quality Overview • Reimbursement Trends
• Pay for Performance (P4P)• Physician Quality Reporting Initiative (PQRI)• Nonpayment for Nonperformance
• Quality Organizations
54

28
Benefits of DPRP Participation For Clinicians and Health Plans
• Program designed in partnership with American Diabetes Association
d i C /Q li f C• Improved Patient Care/Quality of Care• Reduction in Healthcare Costs• Improved Reimbursement• Attract/Recruit New Patients and New
E l G
55
Employer Groups• ABFM Maintenance of Certification
– Part IV-Performance in Practice Module (PPM)
Benefits of DPRP Participation for Clinicians and Health Plans
• Improved Patient Care/Quality of Care:Decreases and prevents long term diabetes – Decreases and prevents long-term diabetes complications.
– Promotes early treatment of diabetes and its co-morbid conditions.
– Provides evidence-based decision making– Supports delivery of consistent high quality patient
care
56
care

29
Benefits of DPRP Participation for Clinicians and Health Plans
• Improved Patient Care/Quality of Care:– Allows for feedback to physicians on performance p y p
and patient population– Identifies opportunities for incorporating
improvement strategies– Supports IT Utilization
57
Benefits of DPRP Participation for Clinicians and Health Plans
Reducing risk of long-term complications• One point reduction in A1c reduces risk of
microvascular diabetic complications by 40%microvascular diabetic complications by 40%• 10 mm Hg reduction in systolic blood pressure
reduces diabetes complication risk by 12%• Improved control of cholesterol and lipids can
reduce cardiovascular complications by 20-50%
58
50%•Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2005.•http://www.cdc.gov/diabetes/pubs/factsheet05.htm (Accessed December 1, 2009).
30
Benefits of DPRP Participation for Clinicians and Health Plans
Reducing risk of long-term complications• Detection of diabetic eye disease and
treatment can reduce development of severe treatment can reduce development of severe vision loss by estimated 50-60%
• Comprehensive foot programs can reduce amputation rates by 45-85%
• Detection and treatment of early diabetic kidney disease can reduce the development of
l f il b 30 70%
59
renal failure by 30-70%•Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2005.•http://www.cdc.gov/diabetes/pubs/factsheet05.htm (Accessed December 1, 2009).
Benefits of DPRP Participation for Clinicians and Health Plans
• Reduction in Health Care Costs
• Improved Reimbursement:– Pay-for-Performance (P4P) Participation– Contract negotiations with Health Plans
60

31
Benefits of DPRP Participation for Clinicians and Health Plans
• Attract/Recruit New Patients and Employer Groups:– Health Plan Network designation Health Plan Network designation – NCQA Seal of Quality– Listing on NCQA’s Recognized Physician Directory
Website– Advertising and media opportunities
• ABFM Maintenance of Certification (Physicians):
61
( y )– Module IV
• PQRI
Costs/Barriers to DPRP Participation
• Time/Cost of Data Collection– Data Collection– Submission process
A li ti f– Application fee• MD/Staff Resistance to Change
– Personal delusions of good care– Incomplete documentation– Change to routine– Measuring Quality is too difficult
L k f S t St ff
62
• Lack of Support Staff• Lack of Financial Incentive
32
Novant Outcomes of DPRP Participation
• Documented Improvement in Diabetes Care• Improved Reimbursement Contracts• P4P ParticipationP4P Participation
– Charlotte Healthcare Collaborative– Bridges to Excellence– PQRI
• Physician buy-in/acceptance– Continue to demonstrate high quality care
63
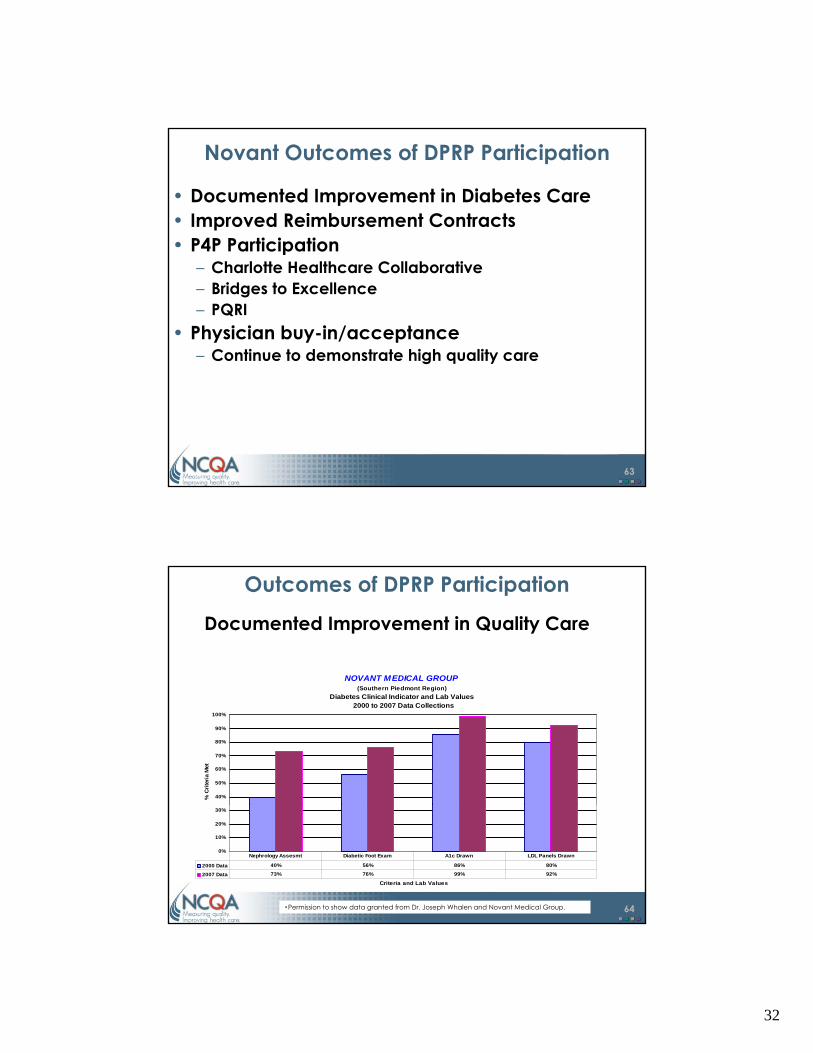
Outcomes of DPRP Participation
Documented Improvement in Quality Care
NOVANT MEDICAL GROUP(Southern Piedmont Region)
Diabetes Clinical Indicator and Lab Values 2000 to 2007 Data Collections
40%
50%
60%
70%
80%
90%
100%
% C
riter
ia M
et
64
0%
10%
20%
30%
Criteria and Lab Values
2000 Data 40% 56% 86% 80%
2007 Data 73% 76% 99% 92%
Nephrology Assesmt Diabetic Foot Exam A1c Drawn LDL Panels Drawn
•Permission to show data granted from Dr. Joseph Whalen and Novant Medical Group.

33
Outcomes of DPRP Participation
• National Recognition:– VHA Leadership Awards, 2003– North Carolina Alliance for Healthy Communities North Carolina Alliance for Healthy Communities,
Honorable Mention, 2005– North Carolina Alliance for Health Communities,
Eagle Award, 2006– AMGA Best Practice in Diabetes Learning
Collaborative, 2005
65
Summary
• Quality measurement is here to stay and the trend toward paying providers based on their quality of care will accelerate in the coming years.
• Physicians and Health Plans who accept and embrace these challenges (understand what is being measured, how to provide the data, and when and how to change what you’re doing) stand the best chance of surviving and prospering.
• NCQA’s DPRP is a great way to get started measuring
66
quality.

34
DPRP and Endocrine Consultants PC: DPRP and Endocrine Consultants, PC: An Endocrine Practice Perspective
Steven B. Leichter, MD, FACP, FACESenior Partner, Endocrine Consultants, PC
h C t f i b t d t b liThe Center for Diabetes and MetabolismColumbus, Georgia
Why Support NCQA Measures?
• Provides a reasonable framework for the process of patient care
• Provides guidance for the organization of • Provides guidance for the organization of assessments and charting
• Prepare physicians for reviews of their care insurers are currently requiring
• Is the preferred model for “pay-for-performance”
68
performance

35
Pay-for-Performance (PfP) is Coming…NCQA Recognition is Consistent with
Physician Care Patterns
Why Support NCQA Recognition as a “PfP” Model for Diabetes?
• A substantial percentage of the recognition scoring is based on physician care and not
ti t lipatient compliance• Patient outcome standards are reasonable• The measures are supported by most major
health organizations, including the American Diabetes Association
70

36
The NCQA Measures Incorporate the Relevant Clinical Standards of Care in
Diabetes
• Care guidelines of the ADAg• Lipid guidelines of the NCEP (ATP III)• Hypertension guidelines (JNC7)
71
Alternative PfP ModelsAre based solely on clinical outcomes

37
How Does NCQA RecognitionHow Does NCQA RecognitionBenefit an Endocrine Practice?
Benefits to Endocrine Practice Organization
• Prioritizes the foci of care for diabetic patients• Facilitates the organization of the clinical chart
to demonstrate the organization of careto demonstrate the organization of care• Enhances the application of best clinical
practices in the care of each patient
74
38
Reasons for a Practice to Participate in DPRP
• NCQA Recognition is a Seal of Approval that the practice can market to its patients as a mark of its excellencemark of its excellence
• Insurers, upon learning that a physician is “recognized”, may market that to their diabetic clients
• Referring physicians recognize the excellence associated with recognition
75
associated with recognition
Benefits to Relations With Insurers
• Insurers refer diabetic patients desiring specialty care to recognized physicians
• Insurers tend to be more supportive to • Insurers tend to be more supportive to recognized practices
• Insurers may exempt recognized physicians from duplicating charts for external review of the quality of diabetes care
76

39
Possible Financial Benefits
• Some insurers may support the fees for NCQA Recognition
• Some insurers pay a one time bonus to • Some insurers pay a one-time bonus to physicians upon recognition
• In 2009 Medicare began PQRI rewards
77
The Benefits of RecognitionThe Benefits of RecognitionTo Endocrine Consultants

40
Benefits:1. Organization of Care
• Streamlined the processing of diabetic patients to focus efficiently on the aspects of care advocated by the NCQA measuresadvocated by the NCQA measures
• Encouraged us to establish chart forms, which facilitated appropriate routine testing protocols for patients
• Encouraged us to analyze “noncompliance” in detail to obtain better patient outcomes
79
detail to obtain better patient outcomes
Benefits:2. Decisions About Treatment
• NCQA measures encouraged us to consider the total treatment package for every patient in terms of affordability ease every patient in terms of affordability, ease of use and conformity to the formulary available to the patient
• Encouraged drug regimens, which required fewer pills per dayE d t t ti t f di t
80
• Encouraged support to patients for dietary and diabetes self-care tasks

41
Benefits:3. Relationship with Insurers
• We were exempted from required chart audits• At least 100 patients were referred to us based
on our NCQA Recognition by Georgia insurers on our NCQA Recognition by Georgia insurers and Medicare!
• We found that we had “more clout” when negotiating treatment issues with prior authorization groups in insurers.
81
Current Initiatives in Georgia
• Insurers currently requesting HEDIS®
medical information for any patient diagnosed with diabetes to confirm that diagnosed with diabetes to confirm that care is by NCQA measures
• The same insurers and Medicaid plans are considering a PfP model for diabetes care
82
•Healthcare Effectiveness Data Information Set (HEDIS) is a registered trademark of the National Committee for Quality Assurance (NCQA).

42
Models of The Center For Health Transformation
• Three models of implementation of Bridges to Excellence in Atlanta, Savannah and Columbus
• Models engage physicians in enhanced provider status, prescribing, and better market position
83
• Acceptance is growing
The Columbus Project
• Three components: physician recognized; community awareness;
l tievaluation• Of 81 physicians identified to be eligible
for recognition, 51 are recognized or in the process after only 12 months
• Recognized clinicians will be marketed by
84
employers and insurers to the public
43
Pa for Performance Pay-for-Performance is coming.
85
Thank You
Please click the ‘Main Menu’ button or proceed to the Post-Test/Evaluation.
Main Menu Post-Test/Evaluation
86