diabetes updates, dpp4 inhitors and ramadan and dm
TRANSCRIPT

• Respected audience
• Warm Welcome to you all

• Dr. Rajat SR Biswas, MD
• Resident Physician• CMSOGH, Agrabad• Chittagong

Type 2 Diabetes - Its Managements & Use of DPP-4 inhibitor:
Sitagliptin

History of Diabetes Mellitus
• Coined phrase ‘diabetes mellitus’ from Greek and Latin origins
• 1552 B.C. - Earliest known record of diabetes mentioned on 3rd Dynasty Egyptian papyrus by physician Hesy-Ra; mentions polyuria (frequent urination) as a symptom
• 1869 - Paul Langerhans, a German medical student, announces that the pancreas contains contains two systems of cells. One set secretes the normal pancreatic juice, the function of the other was unknown. These cells are identified as the 'islets of Langerhans.'
• 1921 – Frederick Banting and Charles Best find insulin is secreted from the ‘islets of Langerhans’ of the pancreas.
• 1959 - Two major types of diabetes are recognized: type 1 (insulin-dependent) diabetes and type 2 (non-insulin-dependent) diabetes.

Background
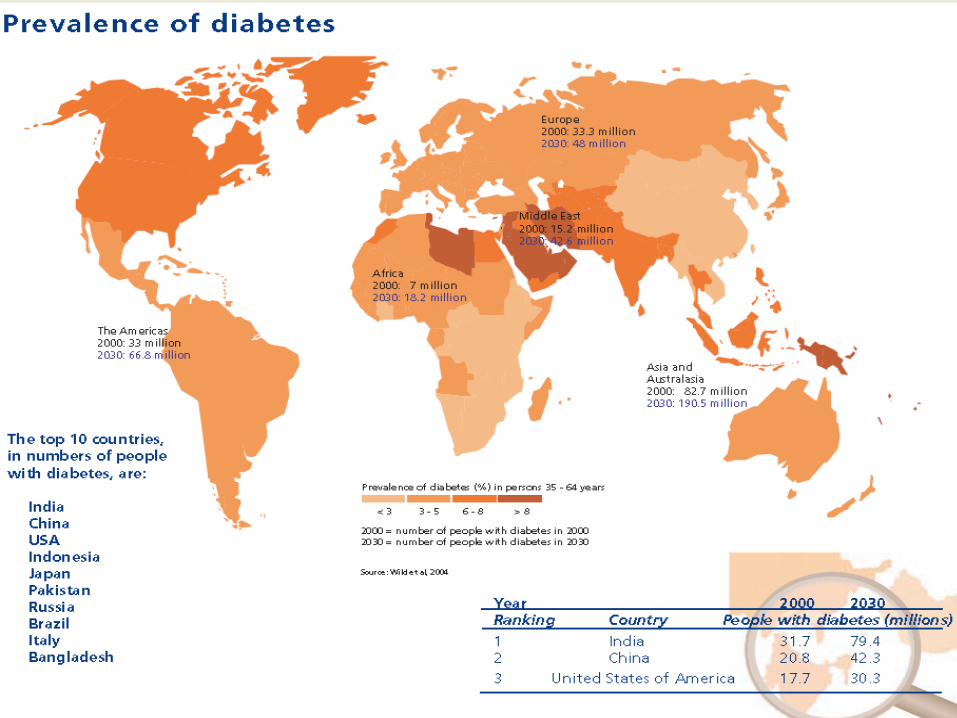

The Diabetes Epidemic: Global Projections, 2010–2030
IDF. Diabetes Atlas 5th Ed. 2011

In Matlab 5% of the young adults (27-50 years) are affected by diabetes
Ref: ICDDR’B annual report 2008
In Bangladesh 5.6 million peoples are diagnosed as diabetic patients, which is 6.1% of total population (age group 20-79 years).
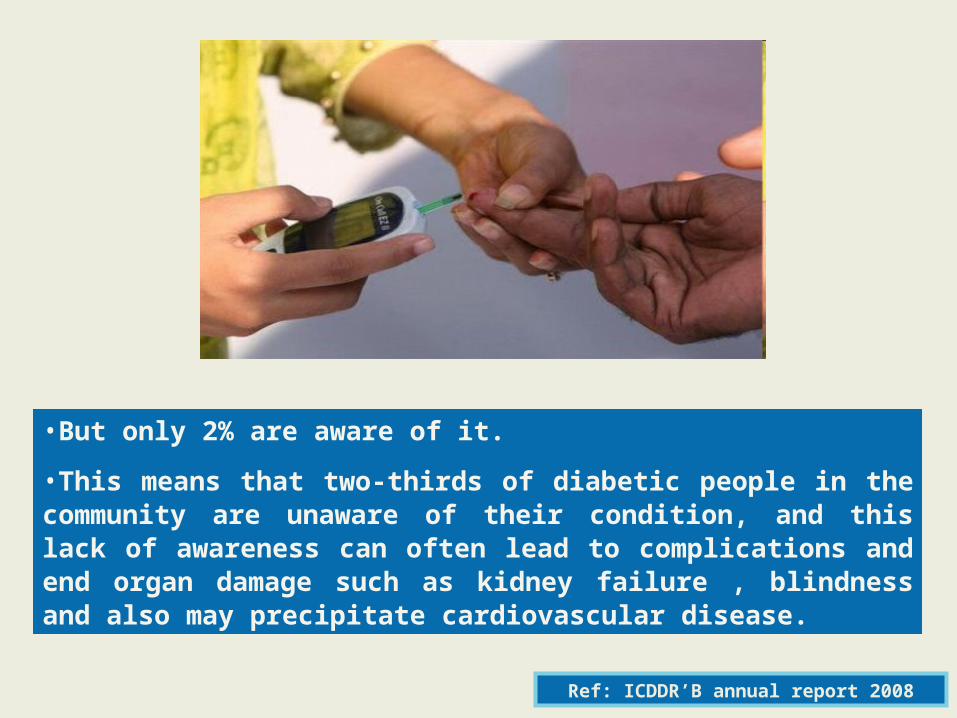
•But only 2% are aware of it.
•This means that two-thirds of diabetic people in the community are unaware of their condition, and this lack of awareness can often lead to complications and end organ damage such as kidney failure , blindness and also may precipitate cardiovascular disease.
Ref: ICDDR’B annual report 2008
Type 2 Diabetes is the main cause of
untreated complications, severe
disabilities and death for an estimated
3 millon people.

Type 2 diabetes increases the Type 2 diabetes increases the risk of serious morbidityrisk of serious morbidity
4.9
3.63.2
2.8 3
11
7
0
2
4
6
8
10
12
Angina Cardiacfailure
Myocardialinfarction
Stroke Renalfailure
Amputation(minor)
Amputation(major)
Rel
ativ
e in
crea
se in
ris
k
Adapted from The Information Centre. National Diabetes Audit, Abridged report for the audit period 2004/2005. London: The Information Centre, 2006.

Carbohydrate
Metabolism
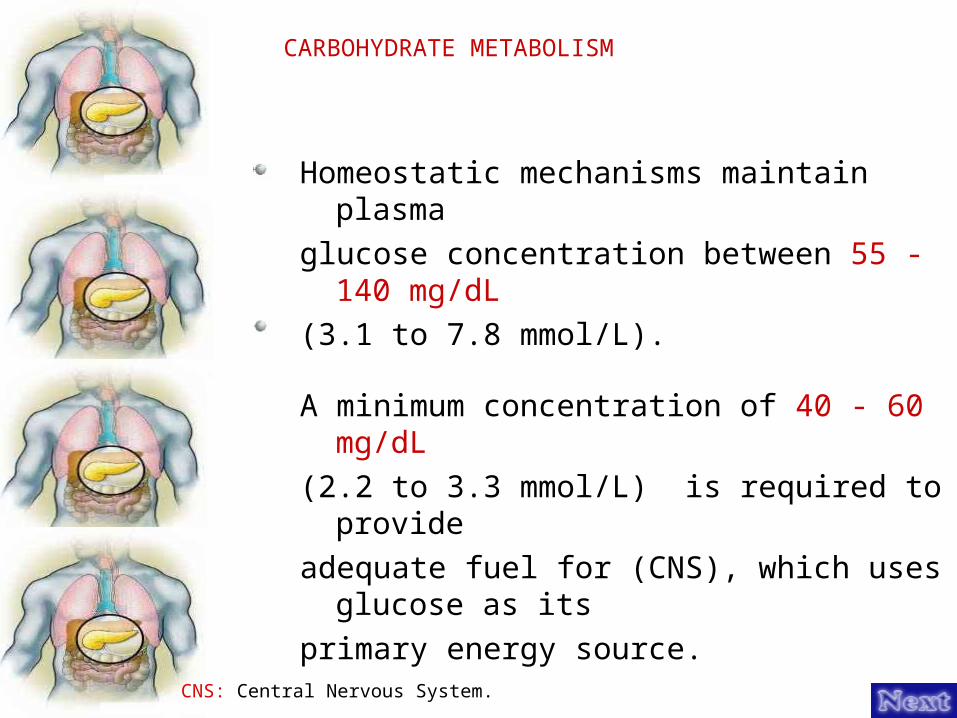
CARBOHYDRATE METABOLISM
Homeostatic mechanisms maintain plasma glucose concentration between 55 - 140 mg/dL(3.1 to 7.8 mmol/L).
A minimum concentration of 40 - 60 mg/dL(2.2 to 3.3 mmol/L) is required to provide adequate fuel for (CNS), which uses glucose as its primary energy source.
CNS: Central Nervous System.

Blood glucose concentration exceed the Re-absorptive capacity of the kidneys( 180 mg/dL ), glucose spills into the urine resulting in a loss of calories and water.
Muscle and fat use glucose as major source of energy, but these tissues require insulin for glucose uptake.
If glucose is unavailable, these tissues are able to use amino acids and fatty acids for fuel.
CARBOHYDRATE METABOLISM – Cont’d

Postprandial Glucose Metabolism in the Nondiabetic Individual
In muscle, insulin promotes the uptake of glucose and its storage as glycogen.
It also stimulate the uptake of amino acid and theirconversion to protein.
In adipose tissue, glucose is converted to free fatty acids and stored as triglycerides.
Insulin prevents a breakdown of these triglycerides to free fatty acids.
The liver doesn't require insulin for glucose transport, but insulin facilitates the conversion of glucose to glycogen and free fatty acids.

Fasting Glucose Metabolism in Nondiabetic Individual
As blood glucose concentrations drop toward normal during the fasting state, insulin release is inhibited .
A number of counter regulatory hormonesthat promote an increase in blood sugar are released (e.g., glucagon, epinephrine, growth hormone, glucocorticoides).
Several processes maintain a minimum blood glucose concentration for the CNS.
CNS: Central Nervous System.

Glycogen in the liver glucose.
Amino acids are transported from muscle to liver glucose.
Uptake of glucose by insulin dependent tissues is diminished to conserve glucose for the brain.
Triglycerides are broken down into free fatty acids, which are used as alternative fuel sources.
Fasting Glucose Metabolism in Nondiabetic Individual – Cont’d
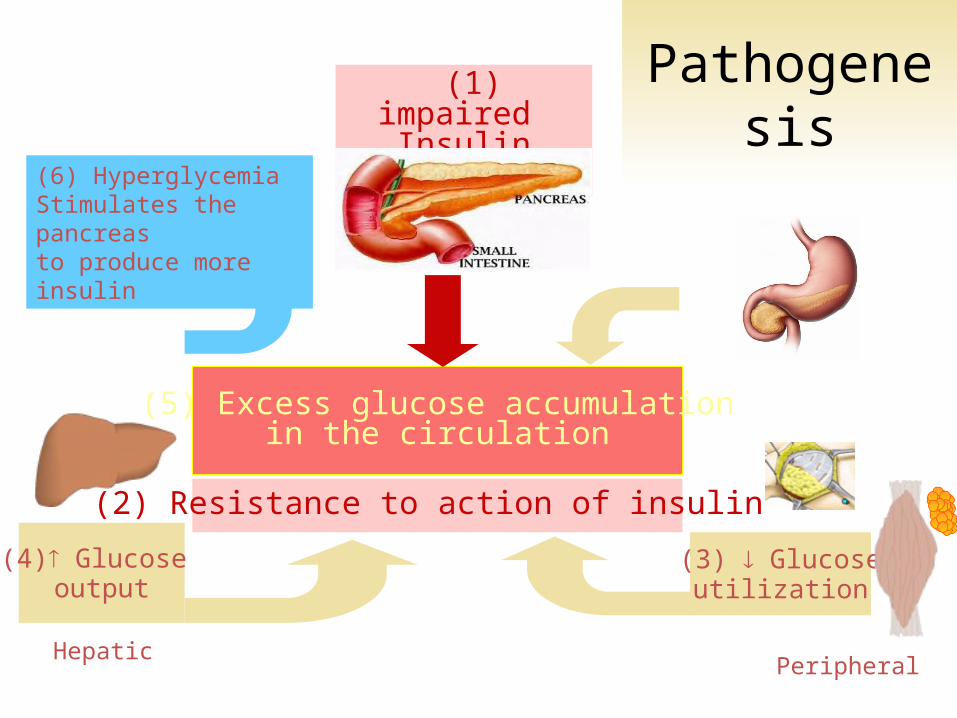
(5) Excess glucose accumulationin the circulation
(2) Resistance to action of insulin
(1) impaired Insulin secretion
(4) Glucose output
HepaticPeripheral
(3) Glucoseutilization
(6) Hyperglycemia Stimulates the pancreas to produce more insulin
Pathogenesis
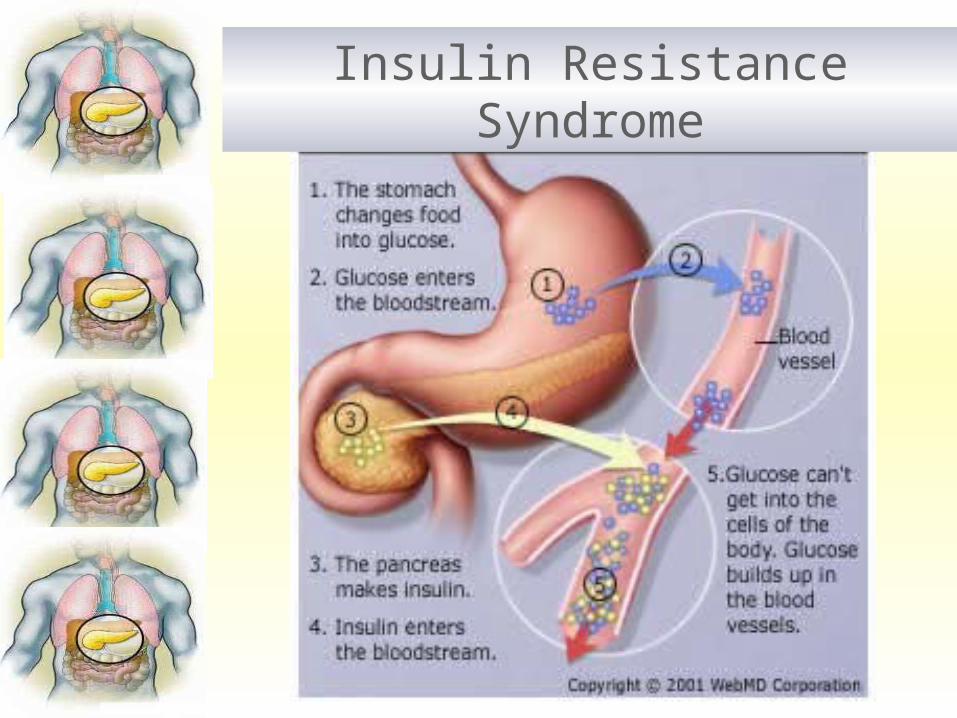
Insulin Resistance Syndrome

Overweight/Obesity - Inactivity.
Hypertension.
A first degree relative with DM
Previous Gestational DM
Coronary Heart Disease
Dyslipidemia
Previously identified impaired fasting glucose (IFG) OR impaired glucose tolerance (IGT).
RISK FACTORS FOR DIABETES INCLUDE:

DIAGNOSIS
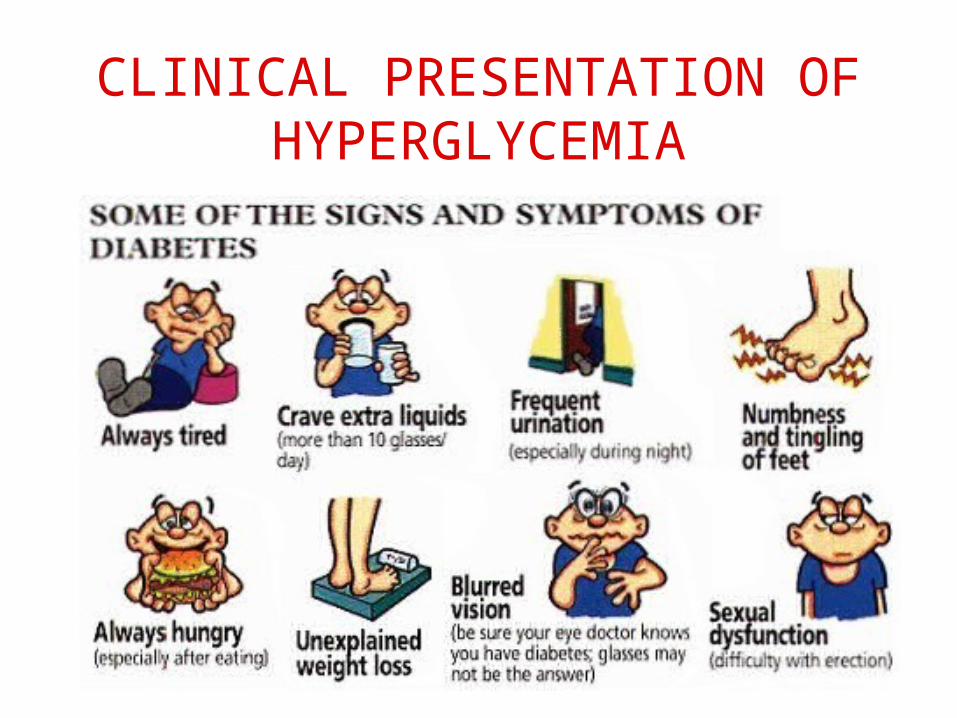
CLINICAL PRESENTATION OF HYPERGLYCEMIA

Screening of asymptomatic individuals at high risk for Type 2 DM should be carried out on an opportunistic basis.
Screening should begin at age 40 years, and be considered at an earlierage (e.g. 30 years) if risk factors for diabetes are present.
Screening should be carried out every 3 years for those with normal glucose tolerance and annually for those with impaired fasting glucose (IFG) or impaired glucose tolerance (IGT).
SCREENING OF ASYMPTOMATIC INDIVIDUALS.

DIAGNOSTIC CRITERIA OF TYPE 2 DM
Casual plasma glucose > 200 mg/dl and symptoms of diabetes OR
Fasting Plasma Glucose (FPG) >126 mg/dl OR
Results of a 2-hour 75-g Oral Glucose Tolerance Test (OGTT) > 200 mg/dl
(Non-Pregnant Adults)
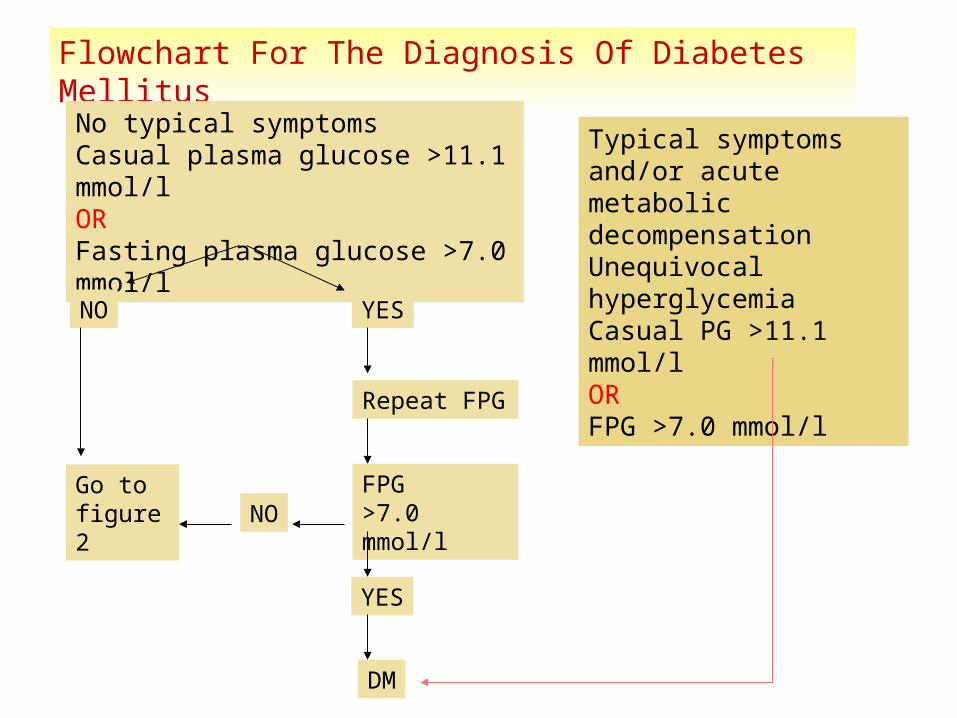
Flowchart For The Diagnosis Of Diabetes Mellitus
No typical symptomsCasual plasma glucose >11.1 mmol/lORFasting plasma glucose >7.0 mmol/l
NO YES
Repeat FPG
FPG >7.0 mmol/l
YES
DM
NOGo tofigure 2
Typical symptoms and/or acute metabolic decompensationUnequivocal hyperglycemiaCasual PG >11.1 mmol/lORFPG >7.0 mmol/l

Flowchart For Individuals Suspected To Have Diabetes But Whose FPG <7.0 Mmol/L
FPG
< 6.0 mmol/l 6.1- 6.9 mmol/l
Oral GlucoseTolerance Test
2- hour post -challenge glucose
<7.8mmol/l
7.8 - 11.0mmol/l
>11.1mmol/l
ImpairedFastingGlycaemia
ImpairedGlucoseTolerance
DiabetesMellitus
NormalFastingGlucose
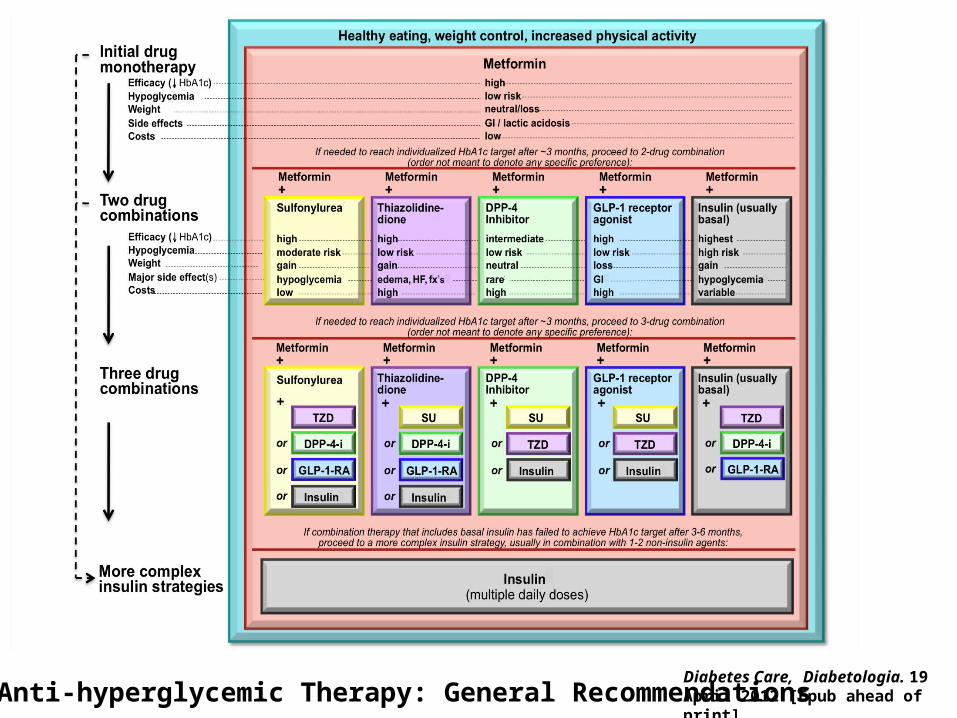
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
•Glycemic targets
- HbA1c < 7.0% (mean PG 150-160 mg/dl [8.3-8.9 mmol/l])
- Pre-prandial PG <130 mg/dl (7.2 mmol/l)
- Post-prandial PG <180 mg/dl (10.0 mmol/l)
- Individualization is key: Tighter targets (6.0 - 6.5%) - younger, healthier Looser targets (7.5 - 8.0%+) - older, comorbidities,
hypoglycemia prone, etc.
- Avoidance of hypoglycemia
PG = plasma glucose Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Figure 1 Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print](Adapted with permission from: Ismail-Beigi F, et al. Ann Intern Med 2011;154:554)
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
ANTI-HYPERGLYCEMIC THERAPY-
•Therapeutic options: Lifestyle
-Weight optimization
-Healthy diet
- Increased activity levelDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
ANTI-HYPERGLYCEMIC THERAPY
• Therapeutic options: Oral agents & non-insulin injectables
- Metformin
- Sulfonylureas
- Thiazolidinediones
- DPP-4 inhibitors
- GLP-1 receptor agonists
- Meglitinides
- -glucosidase inhibitors
- Bile acid sequestrants
- Dopamine-2 agonists
- Amylin mimetics
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
ANTI-HYPERGLYCEMIC THERAPY
•Therapeutic options: Insulin
- Neutral protamine Hagedorn (NPH)
- Regular
- Basal analogues (glargine, detemir)
- Rapid analogues (lispro, aspart, glulisine)
- Pre-mixed varieties
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
Long (Detemir)
Rapid (Lispro, Aspart, Glulisine)
Hours
Long (Glargine)
0 2 4 6 8 10 12 14 16 18 20 22 24
Short (Regular)
Hours after injection
Insu
lin le
vel
ANTI-HYPERGLYCEMIC THERAPY
•Therapeutic options: Insulin
Intermediate (NPH)

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
ANTI-HYPERGLYCEMIC THERAPY
•Implementation strategies:
-Initial therapy
-Advancing to dual combination therapy
-Advancing to triple combination therapy
-Transitions to & titrations of insulin
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

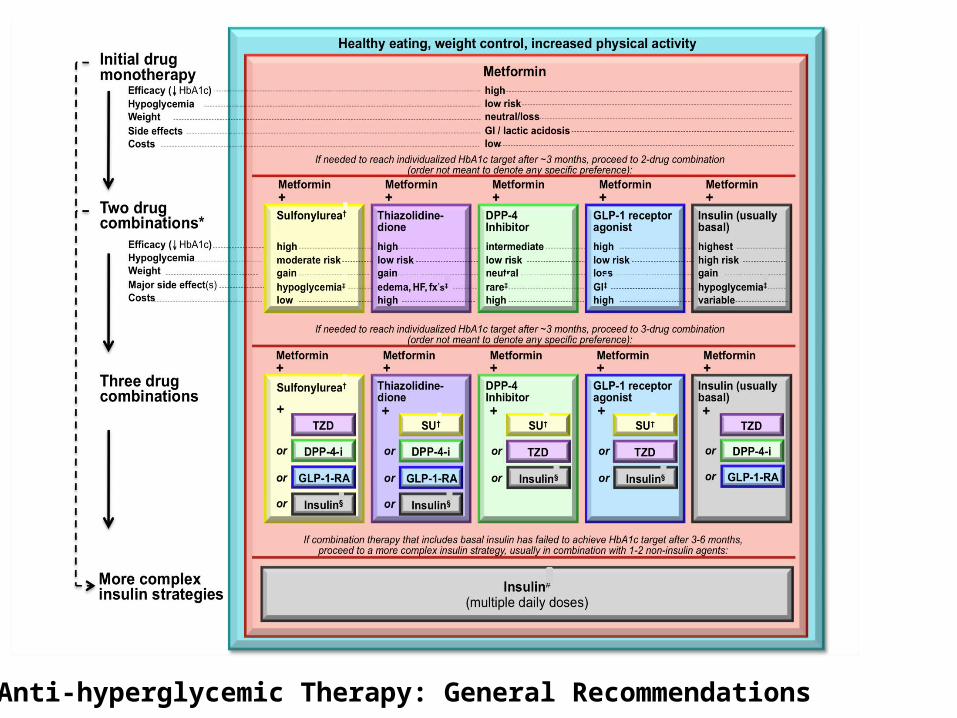
T2DM Antihyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

T2DM Antihyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

T2DM Antihyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
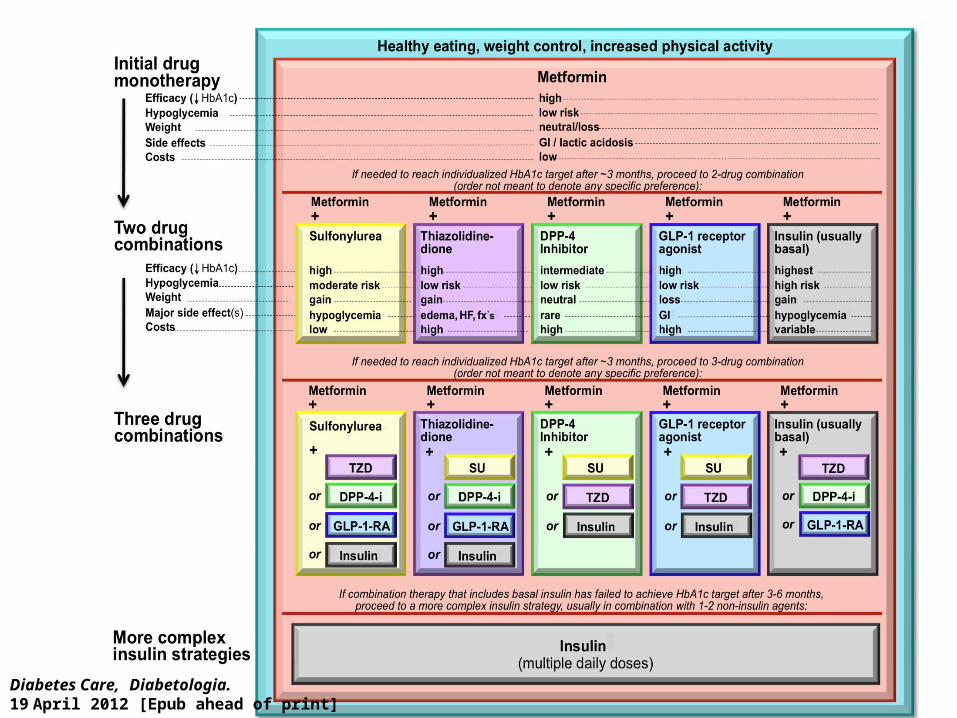
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
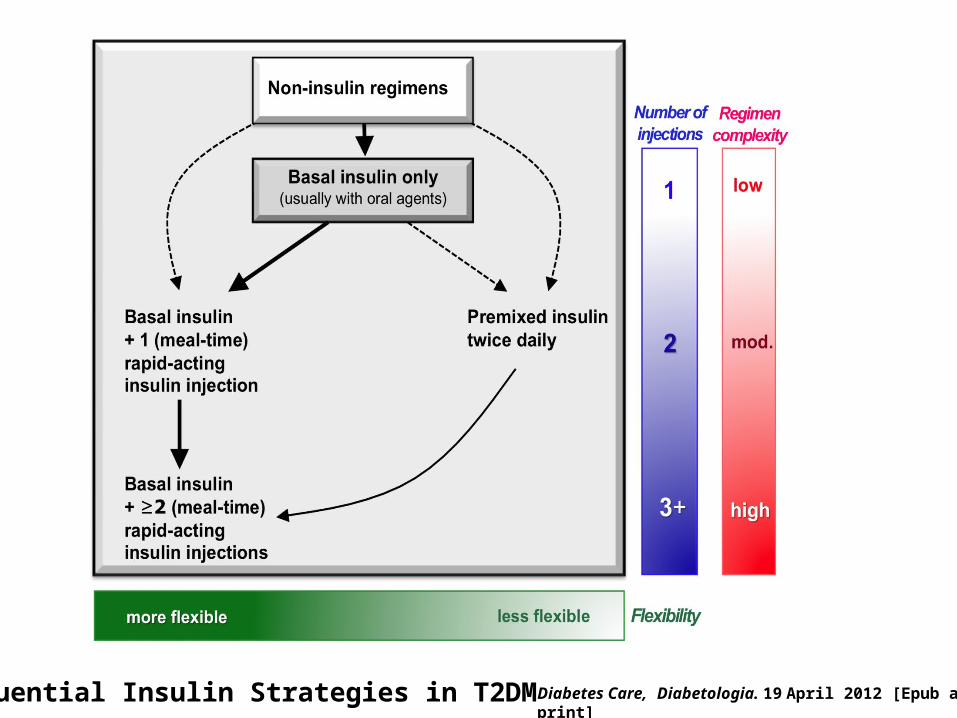
Sequential Insulin Strategies in T2DM Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
4. OTHER CONSIDERATIONS•Age•Weight•Sex / racial / ethnic / genetic differences•Comorbidities
-Coronary artery disease-Heart Failure-Chronic kidney disease-Liver dysfunction-Hypoglycemia
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Age: Older adults
-Reduced life expectancy-Higher CVD burden-Reduced GFR-At risk for adverse events from polypharmacy-More likely to be compromised from hypoglycemia
Less ambitious targetsHbA1c <7.5–8.0% if tighter
targets not easily achievedFocus on drug safety
Less ambitious targetsHbA1c <7.5–8.0% if tighter
targets not easily achievedFocus on drug safety
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Weight
-Majority of T2DM patients overweight / obese-Intensive lifestyle program-Metformin-GLP-1 receptor agonists-? Bariatric surgery
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
T2DM Anti-hyperglycemic Therapy: General RecommendationsDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Adapted Recommendations: When Goal is to Avoid Weight GainDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Sex/ethnic/racial/genetic differences
-Little is known-MODY & other monogenic forms of diabetes-Latinos: more insulin resistance-East Asians: more beta cell dysfunction-Gender may drive concerns about adverse effects
(e.g., bone loss from TZDs)
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Comorbidities
-Coronary Disease
-Heart Failure
-Renal disease
-Liver dysfunction
-Hypoglycemia
Metformin: CVD benefit (UKPDS)
Avoid hypoglycemia ? SUs & ischemic
preconditioning ? Pioglitazone & CVD events ? Effects of incretin-based
therapies
Metformin: CVD benefit (UKPDS)
Avoid hypoglycemia ? SUs & ischemic
preconditioning ? Pioglitazone & CVD events ? Effects of incretin-based
therapies
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Comorbidities
-Coronary Disease
-Heart Failure
-Renal disease
-Liver dysfunction
-Hypoglycemia
Metformin: May use unless condition is unstable or severe
Avoid TZDs ? Effects of incretin-based therapies
Metformin: May use unless condition is unstable or severe
Avoid TZDs ? Effects of incretin-based therapies
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Comorbidities
-Coronary Disease
-Heart Failure
-Renal disease
-Liver dysfunction
-Hypoglycemia
Increased risk of hypoglycemia Metformin & lactic acidosis
US: stop @SCr ≥ 1.5 (1.4 women)
UK: dose @GFR <45 & stop @GFR <30
Caution with SUs (esp. glyburide)
DPP-4-i’s – dose adjust for most
Avoid exenatide if GFR <30
Increased risk of hypoglycemia Metformin & lactic acidosis
US: stop @SCr ≥ 1.5 (1.4 women)
UK: dose @GFR <45 & stop @GFR <30
Caution with SUs (esp. glyburide)
DPP-4-i’s – dose adjust for most
Avoid exenatide if GFR <30Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Comorbidities
-Coronary Disease
-Heart Failure
-Renal disease
-Liver dysfunction
-Hypoglycemia
Most drugs not tested in advanced liver disease
Pioglitazone may help steatosis Insulin best option if disease
severe
Most drugs not tested in advanced liver disease
Pioglitazone may help steatosis Insulin best option if disease
severe
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
OTHER CONSIDERATIONS•Comorbidities
-Coronary Disease
-Heart Failure
-Renal disease
-Liver dysfunction
-Hypoglycemia Emerging concerns regarding association with increased mortality
Proper drug selection in the hypoglycemia prone
Emerging concerns regarding association with increased mortality
Proper drug selection in the hypoglycemia prone
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]
T2DM Anti-hyperglycemic Therapy: General Recommendations

Adapted Recommendations: When Goal is to Avoid Hypoglycemia

Adapted Recommendations: When Goal is to Minimize Costs

Guidelines for Glycemic, BP, & Lipid Control American Diabetes Assoc. Goals
HbA1C < 7.0% (individualization)
Preprandial glucose 70-130 mg/dL (3.9-7.2 mmol/l)
Postprandial glucose < 180 mg/dL
Blood pressure < 140/90 mmHg
Lipids
LDL: < 100 mg/dL (2.59 mmol/l) < 70 mg/dL (1.81 mmol/l) (with overt CVD)HDL: > 40 mg/dL (1.04 mmol/l) > 50 mg/dL (1.30 mmol/l)TG: < 150 mg/dL (1.69 mmol/l)

ADA-EASD Position Statement: Management of Hyperglycemia in T2DM
FUTURE DIRECTIONS / RESEARCH NEEDS
•Comparative effectiveness research Focus on important clinical outcomes
•Contributions of genomic research
•Perpetual need for clinical judgment!
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

The Role of Incretins in The Role of Incretins in Type 2 DiabetesType 2 Diabetes

IncretinsIncretins
Peptides secreted by the intestinal Peptides secreted by the intestinal mucosa in response to food intakemucosa in response to food intake– Glucagon-like peptide-1 (GLP-1)Glucagon-like peptide-1 (GLP-1)– Glucose-dependent insulinotrophic Glucose-dependent insulinotrophic
polypeptide (GIP)polypeptide (GIP)

The incretinsThe incretins
YA
EG
TF
IS
DY
SI
AM
DK
IH
DFVNWLLA
QKGKKNDW
K
H N QTI
GIP: glucose-dependent insulinotropic peptide
HA
EG
TF
TS
DV
SS
YL
EG
QA
AK
EFIAWLVK
GRG
GLP-1: glucagon-like peptide-1
Amino acids shown in gold are homologous with the structure of glucagon

L-Cell(ileum)
Proglucagon
GLP-1 [7–37]
GLP-1 [7–36 NH2]
K-Cell(jejunum)
ProGIP
GIP [1–42]
GIP=glucose-dependent insulinotropic peptide; GLP-1=glucagon-like peptide-1 Adapted from Drucker DJ. Diabetes Care. 2003; 26: 2929–2940.
GLP-1 and GIP are synthesized and secreted GLP-1 and GIP are synthesized and secreted from the Gut in Response to food intakefrom the Gut in Response to food intake
59
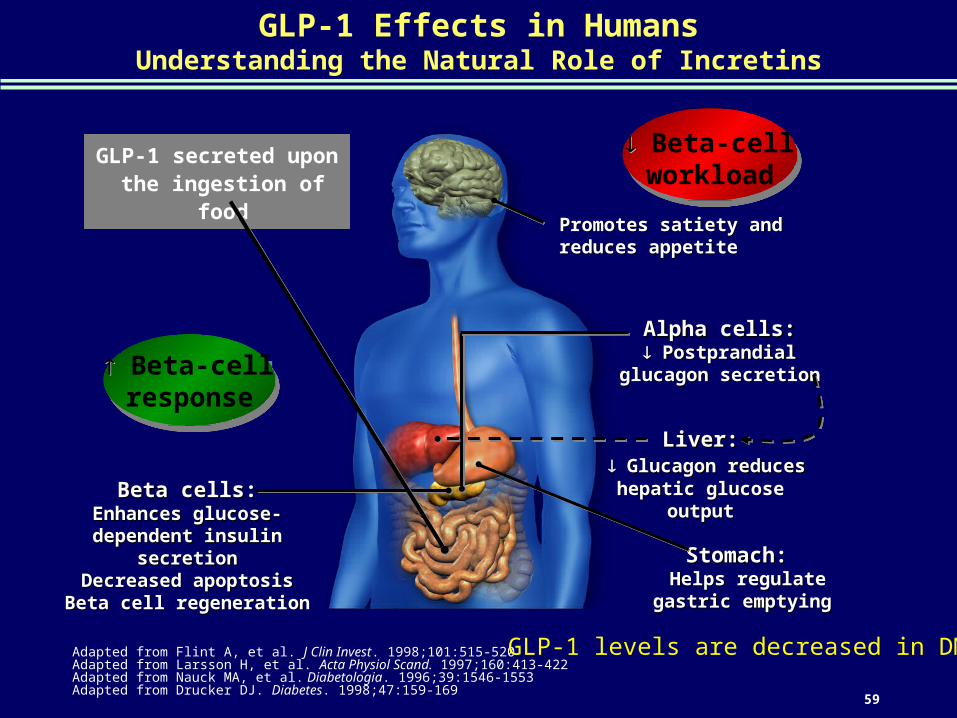
GLP-1 Effects in HumansUnderstanding the Natural Role of Incretins
Adapted from Flint A, et al. J Clin Invest. 1998;101:515-520Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160:413-422Adapted from Nauck MA, et al. Diabetologia. 1996;39:1546-1553Adapted from Drucker DJ. Diabetes. 1998;47:159-169
Stomach:Stomach: Helps regulate Helps regulate
gastric emptyinggastric emptying
Promotes satiety and Promotes satiety and reduces appetitereduces appetite
Liver:Liver: Glucagon reduces Glucagon reduces
hepatic glucose outputhepatic glucose outputBeta cells:Beta cells:Enhances glucose-Enhances glucose-
dependent insulin secretiondependent insulin secretionDecreased apoptosisDecreased apoptosisBeta cell regenerationBeta cell regeneration
Alpha cells:Alpha cells: PostprandialPostprandial
glucagon secretionglucagon secretion
GLP-1 secreted upon the ingestion of food
Beta-cellworkload
Beta-cellworkload
Beta-cellresponse
Beta-cellresponse
GLP-1 levels are decreased in DM 2
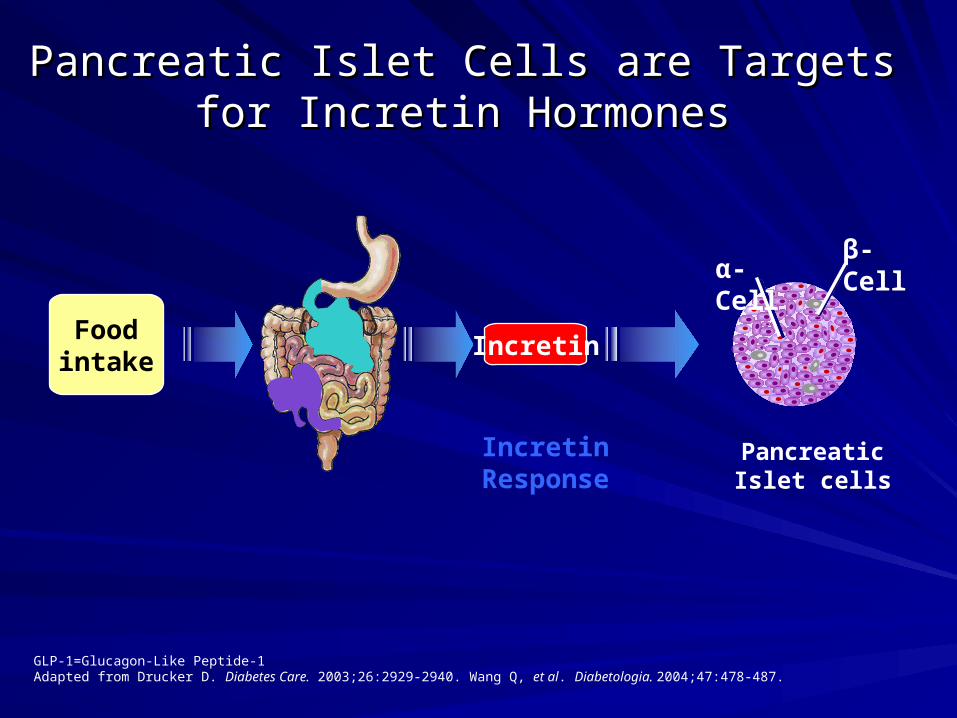
Pancreatic Islet Cells are Targets for Incretin Pancreatic Islet Cells are Targets for Incretin HormonesHormones
GLP-1=Glucagon-Like Peptide-1Adapted from Drucker D. Diabetes Care. 2003;26:2929-2940. Wang Q, et al. Diabetologia. 2004;47:478-487.
Incretin Response
Foodintake
α-Cellβ-Cell
Pancreatic Islet cells
Incretin
DPP 4
GLP-1 and GIP are inactivated by dipeptidyl peptidase-4 (DPP-4) - this enzyme inactivates the incretin molecules by removing two amino acids from the N-terminal ends of the GLP-1 and GIP peptide chains.
As a result of DPP-4 activity, intact, biologically active GLP-1 represents only 10-20% of total plasma GLP-1.
GLP-1 Inactive metabolites
Dipeptidyl peptidase-IV (DPP-IV)
62
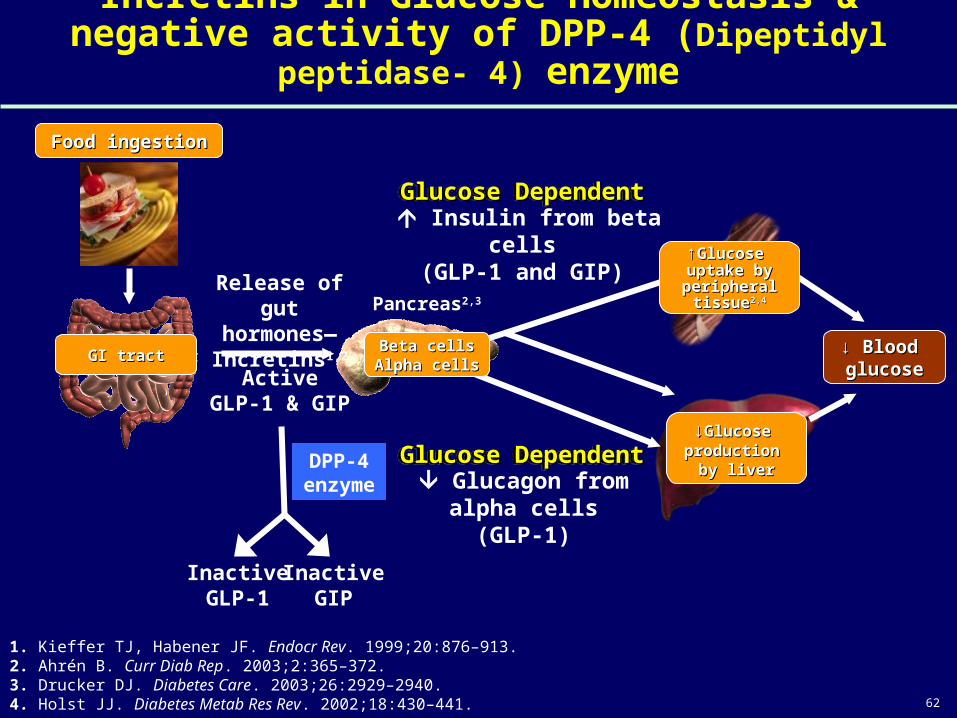
Incretins in Glucose Homeostasis & negative activity of DPP-4 (Dipeptidyl peptidase- 4) enzyme
1. Kieffer TJ, Habener JF. Endocr Rev. 1999;20:876–913. 2. Ahrén B. Curr Diab Rep. 2003;2:365–372.3. Drucker DJ. Diabetes Care. 2003;26:2929–2940. 4. Holst JJ. Diabetes Metab Res Rev. 2002;18:430–441.
Insulin from beta cells(GLP-1 and GIP)
Glucagon fromalpha cells
(GLP-1)
Release of gut hormones— Incretins1,2
Pancreas2,3
Glucose DependentGlucose DependentGlucose DependentGlucose Dependent
ActiveGLP-1 & GIP
DPP-4 enzyme
InactiveGIP
InactiveGLP-1
Glucose DependentGlucose DependentGlucose DependentGlucose Dependent
↓ ↓ Blood Blood glucoseglucose
GI tractGI tract
↓↓Glucose Glucose production production
by liverby liver
Food ingestionFood ingestion
↑↑Glucose Glucose uptake by uptake by peripheral peripheral
tissuetissue2,42,4
Beta cellsBeta cellsAlpha cellsAlpha cells
63
New treatment options for Type 2 Diabetes
1) Amylin analog 2) GLP-1 analogs3) DPP-IV inhibitors
Clinical Diabetes. VA Fonseca. Saunders, 2006, p.395-416.

64
New oral hypoglycaemic
DPP 4 Inhibitors
65
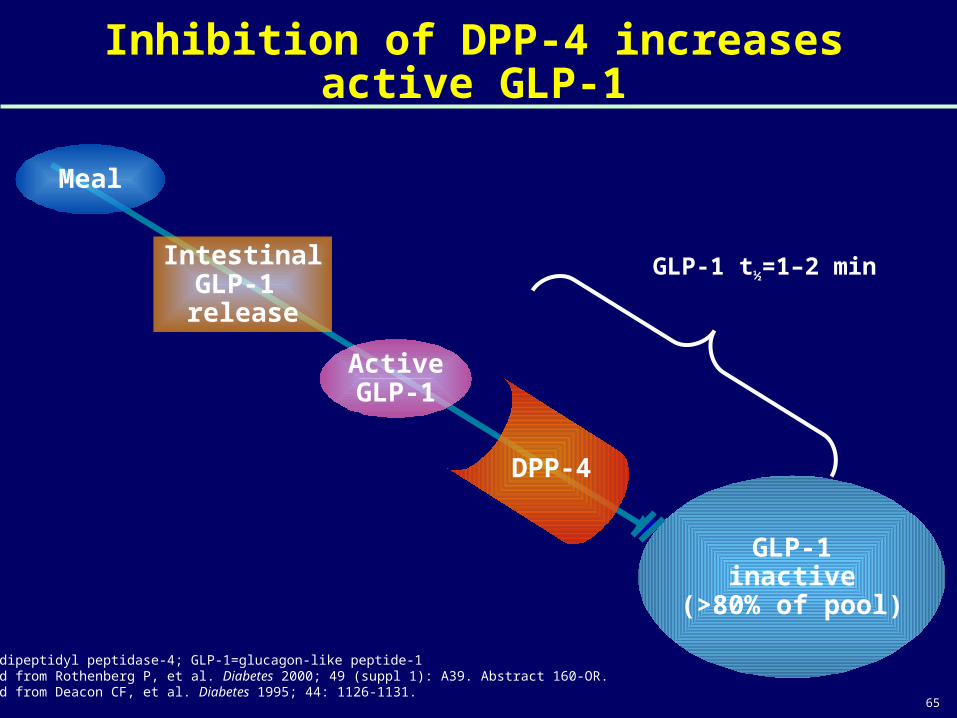
Inhibition of DPP-4 increases active GLP-1
GLP-1inactive
(>80% of pool)
ActiveGLP-1
Meal
DPP-4
IntestinalGLP-1 release
GLP-1 t½=1–2 min
DPP-4=dipeptidyl peptidase-4; GLP-1=glucagon-like peptide-1Adapted from Rothenberg P, et al. Diabetes 2000; 49 (suppl 1): A39. Abstract 160-OR.Adapted from Deacon CF, et al. Diabetes 1995; 44: 1126-1131.
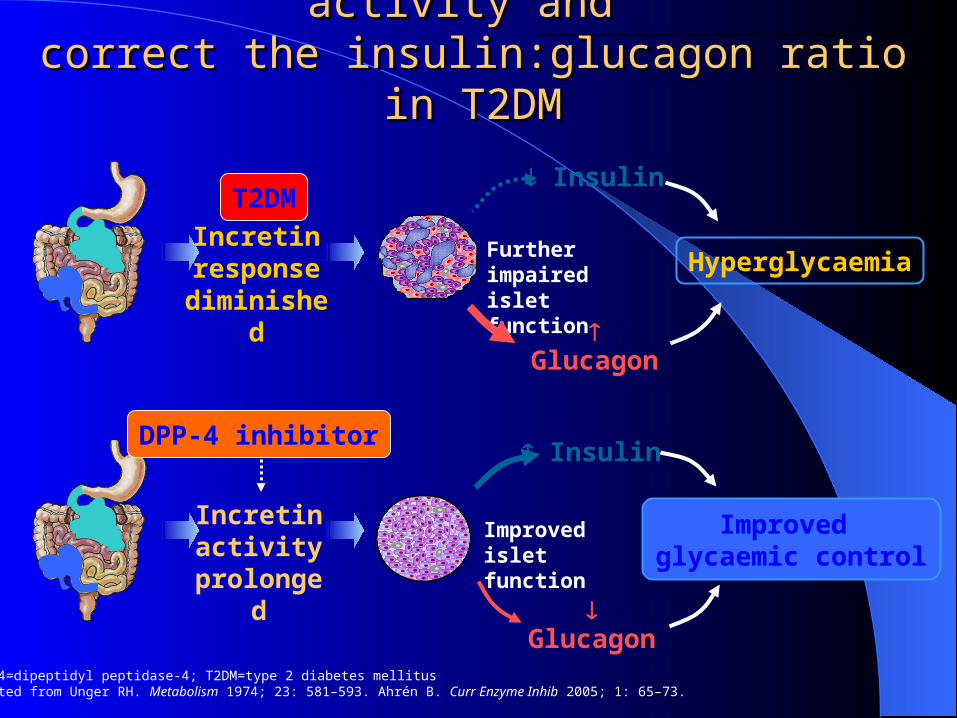
DPP-4=dipeptidyl peptidase-4; T2DM=type 2 diabetes mellitus Adapted from Unger RH. Metabolism 1974; 23: 581–593. Ahrén B. Curr Enzyme Inhib 2005; 1: 65–73.
Insulin
Glucagon
Improved glycaemic control
Incretin activity
prolonged
Improved islet function
DPP-4 inhibitor
Insulin
Glucagon
HyperglycaemiaIncretin
response diminished
Further impaired islet function
T2DM
Blocking DPP-4 can improve incretin activity and Blocking DPP-4 can improve incretin activity and
correct the insulin:glucagon ratio in T2DMcorrect the insulin:glucagon ratio in T2DM
Beyond insulin targeted therapyBeyond insulin targeted therapy
Most therapeutic options for diabetes are focused on abnormal insulin secretion and action and do not address the role of other glucoregulatory hormones.
Also current intensive treatment of diabetes have some shortcomings, like weight gain, oedema, increased risk of hypoglycemia and inability to suppress marked day to day glucose fluctuation.
Clinical Diabetes. VA Fonseca. Saunders, 2006, p.395-416.

New treatment options for Type 2 New treatment options for Type 2 DiabetesDiabetes
1) Amylin analog 2) GLP-1 analogs3) DPP-IV inhibitors
Clinical Diabetes. VA Fonseca. Saunders, 2006, p.395-416.

DPP-4 inhibitor: sitagliptin (GLIPITA)

DPP-IV inhibitor: Sitagliptin DPP-IV inhibitor: Sitagliptin (GLIPITA)
Sitagliptin (Glipita): tab 50, 100 mg
FDA approved in Oct 2006.

Pharmacokinetic studyPharmacokinetic study
Following a single oral 100 mg dose to healtly volunteers:
AUC: 8.52 µM.hr; it increased in a dose-proportional manner. Cmax: 950 nM. Bioavailability: 87 % Absorbed within 1-4 hours of oral intake
Because coadministration of a high-fat meal with Sitagliptin had no effecton the pharmacokinetics, it may be administered with or without food.

Pharmacokinetic dataPharmacokinetic data
Protein binding: 38% T1/2: 12.4 hours Duration of action 18-24 hrs
Metabolism: Hepatic (CYP3A4 and CYP2C8) , nominal.
Excretion: Renal (80%)
Elimination occours primarily unchanged via active tubular secretion by OAT3
Renal clearanceRenal clearance: 350 ml/min

DoseDose100 mg orally once daily in the morningNot influenced by food. If CCR <30 ml/min/1.73m2 then 25 mg
dailyIf CCR 30-50 ml/min/1.73m2 then 50 mg
dailyCan be used in mild to moderate
impairment of liver function.
IndicationIndication
Used as monotherapy or add-on with MTF /TZD in inadequately controlled T2DM.
Can be used with any other class of oral agent or insulin.
Not to be used in T1DM and DKASuitable for obese and overweight patients.
Side EffectsSide Effects
Nasopharyngitis and upper RTIHeadacheNausea, stomach pain, diarrhoea ( less
common)Allergy including anaphylaxis (rarely)Exfoliative skin lesion (rarely)

Precautions Precautions
Before starting sitagliptin, take history ofAllergyPancreatitisCKDHeart disease

Stop the drugStop the drug
In case ofPancreatitisFever, sore throat, headacheSevere blistering, peeling, red skin rashAllergic reactions
Drug InteractionsDrug Interactions
No significant interactions
Dose adjustment required with digoxin
Use in Special situationsUse in Special situations
Pregnancy- Category B drug in all trimesters. No harm to fetus in animal studies. Inadequate studies in pregnant women.
Breastfeeding- No studiesPaediatrics- Use not established

Clinical trial

Clinical trial:phase IIIClinical trial:phase III
Following a single oral 100 mg dose to healtly volunteers:
AUC: 8.52 µM.hr; it increased in a dose-proportional manner. Cmax: 950 nM. T1/2: 12.4 hours. Bioavailability: 87 %
Because coadministration of a high-fat meal with Sitagliptin had no effecton the pharmacokinetics, it may be administered with or without food.
Aims/hypothesis:
1. to assess the efficacy and safety of sitagliptin as monotherapy.
2. to assess the inadequate glycaemic control (HbA1c ≥7% and ≤10%) on exercise and diet.
• Methods: a total of 521 patients aged 27-76 years with main baseline HbA1c of 8.1% were randomised in a 1:2:2 ratio to treatment with:
1. Placebo2. Sitagliptin 100mg once daily3. Sitagliptin 200mg once daily For 18 weeks.
Aims/hypothesis:
1. to assess the efficacy and safety of sitagliptin as monotherapy.
2. to assess the inadequate glycaemic control (HbA1c ≥7% and ≤10%) on exercise and diet.
• Methods: a total of 521 patients aged 27-76 years with main baseline HbA1c of 8.1% were randomised in a 1:2:2 ratio to treatment with:
1. Placebo2. Sitagliptin 100mg once daily3. Sitagliptin 200mg once daily For 18 weeks.
The American Journal of Medicine (2010) 123. S38-S48

Clinical trial:phase IIIClinical trial:phase IIIClinical trial:phase IIIClinical trial:phase III
HbA1c was significantly reduced with Sitagliptin 100 mg and 200 mg compared with placebo.
HbA1c was significantly reduced with Sitagliptin 100 mg and 200 mg compared with placebo.
Results: : after 18 weeksResults: : after 18 weeks
Mean HbA1c over time for placebo, once-daily sitagliptin 100mg and once-daily sitagliptin 200mg groups.Mean HbA1c over time for placebo, once-daily sitagliptin 100mg and once-daily sitagliptin 200mg groups.
The American Journal of Medicine (2010) 123. S38-S48
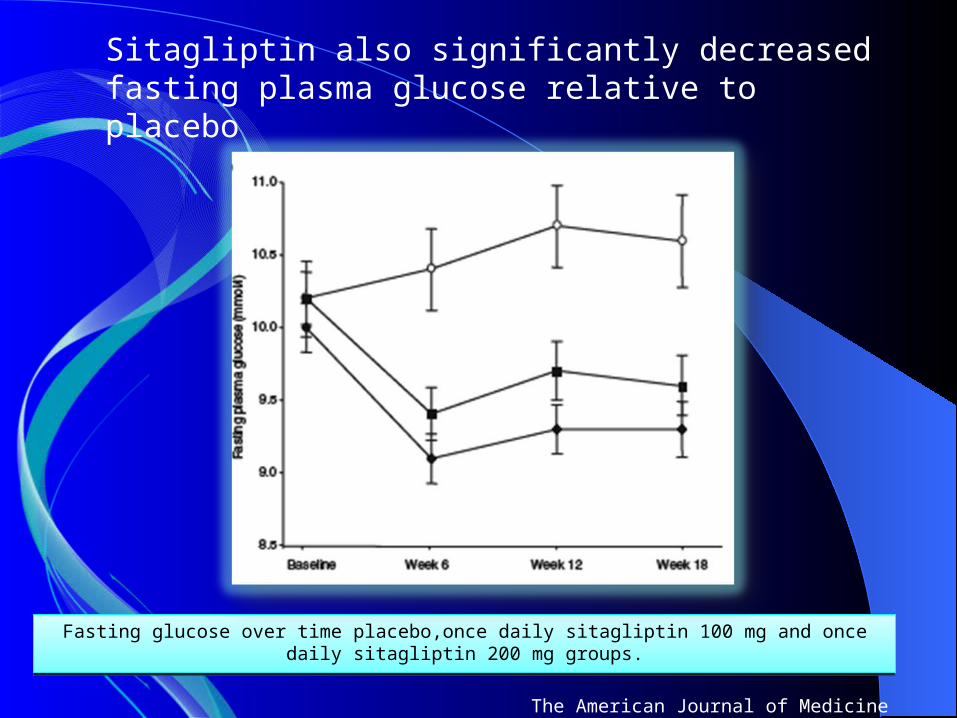
Fasting glucose over time placebo,once daily sitagliptin 100 mg and once daily sitagliptin 200 mg groups.
Fasting glucose over time placebo,once daily sitagliptin 100 mg and once daily sitagliptin 200 mg groups.
The American Journal of Medicine (2010) 123. S38-S48
Sitagliptin also significantly decreased fasting plasma glucose relative to placebo

Insulin:glucagon ratio, markers of insulin secretion and beta cell function, were significantly improved with sitaglipin.
HbA1c was reduced by 0.7 to 0.8 % over 24-52 wks. Fasting blood sugar was reduced by 1-1.5mmole/L. Postprandial blood sugar was reduced by 3 mmole/L.
Insulin:glucagon ratio, markers of insulin secretion and beta cell function, were significantly improved with sitaglipin.
HbA1c was reduced by 0.7 to 0.8 % over 24-52 wks. Fasting blood sugar was reduced by 1-1.5mmole/L. Postprandial blood sugar was reduced by 3 mmole/L.
The incidence of hypoglycaemia and gastrointestinal adverse experiences was not signicantly different between sitagliptin and placebo.
Sitagliptin had a neutral effect on body weight.

• Conclusion/interpretation: Sitagliptin significantly improved glycaemic control and was well
tolerated in patients with type 2 diabetes mellitus who had inadequate glycaemic control on exercise and diet.
• Conclusion/interpretation: Sitagliptin significantly improved glycaemic control and was well
tolerated in patients with type 2 diabetes mellitus who had inadequate glycaemic control on exercise and diet.
Sitagliptin is also well-tolerated at doses of 100 mg once daily in combination with metformin or pioglitazone, without significant hypoglicemia or weight gain.
The American Journal of Medicine (2010) 123. S38-S48
Clinical Trial
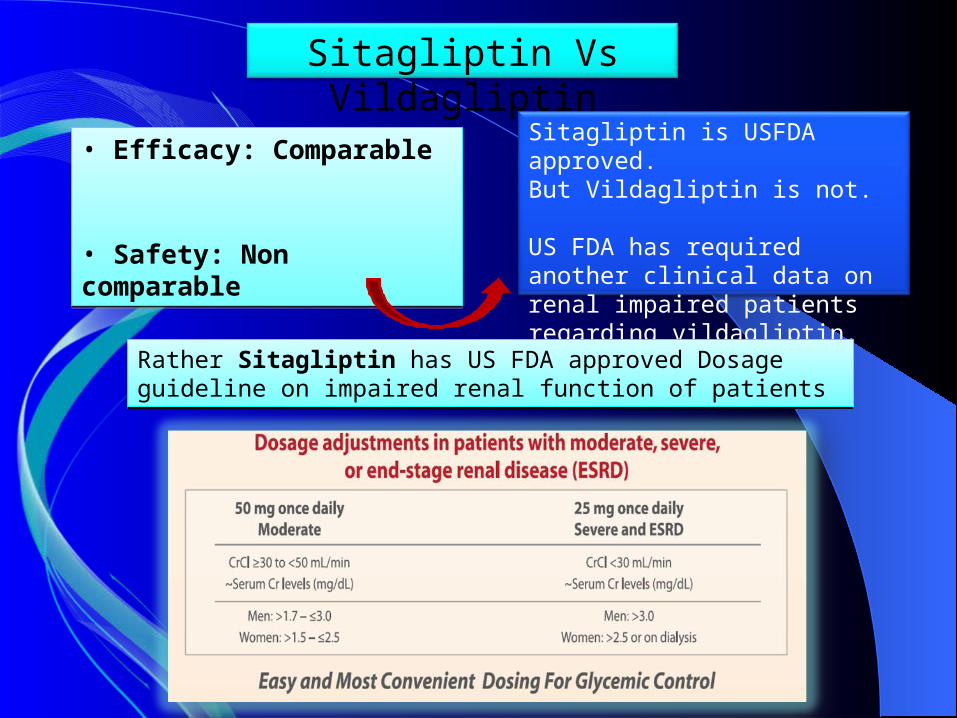
Sitagliptin Vs Vildagliptin
• Efficacy: Comparable
• Safety: Non comparable
• Efficacy: Comparable
• Safety: Non comparable
Sitagliptin is USFDA approved. But Vildagliptin is not.
US FDA has required another clinical data on renal impaired patients regarding vildagliptin.
Rather Sitagliptin has US FDA approved Dosage guideline on impaired renal function of patientsRather Sitagliptin has US FDA approved Dosage guideline on impaired renal function of patients

Sitagliptin can be used in mild to moderate impairment of liver function.
Vildagliptin is contraindicated when ALT or AST >3times the upper limit of normal.
Vildagliptin also requires monitoring of LFT during treatment.
• Sitagliptin 100 mg/day was found well tolerated in clinical trials up to 2 years in duration.
• Insignificant side effects such as Nausea/Vomiting, Nasal/Sinus Congestion, and Headache were observed.
• Treatment with Sitagliptin does not cause hypoglycemia
• Treatment with Sitagliptin does not cause weight gain
• An effective choice in diabetic with renal insufficiency
• Sitagliptin 100 mg/day was found well tolerated in clinical trials up to 2 years in duration.
• Insignificant side effects such as Nausea/Vomiting, Nasal/Sinus Congestion, and Headache were observed.
• Treatment with Sitagliptin does not cause hypoglycemia
• Treatment with Sitagliptin does not cause weight gain
• An effective choice in diabetic with renal insufficiency
The American Journal of Medicine (2010) 123. S38-S48
Summary of clinical trial

Risks associated with FASTING in Risks associated with FASTING in patients with diabetespatients with diabetes
Hypoglycemia
HyperglycemiaHyperglycemia
Diabetic ketoacidosisDiabetic ketoacidosis
Dehydration and thrombosisDehydration and thrombosis
Patient Queries
•Should I fast?
•What dose adjustment to be done?
•How often should I monitor blood glucose?
•What to do if I develop hypoglycemia?
Physician Queries
•Is fasting safe in diabetics?
•How should fasting patients with type 2 DM be managed?
• How should fasting patients with type 1DM be managed?
•Is it safe for pregnant women with DM?
•Absolute contraindications of fasting ?
Physician Queries
•Which OHA is safe and superior?
•Is insulin safe? If yes, which insulin and which regimen?
•What are the dose adjustment in Ramadan?

Pre-Ramadan medical assessment & educational counseling

• Plan at least 3 months before
• Education of diabetic patients and their families
• Must focus on: - The situations contraindicating fasting - Treatment of diabetes and it’s modification: Meal planning physical activities medication

• Importance and tool of self monitoring skills and adjustment
• Must insist on: - The risk of acute complication and means to
prevent them
Dietary guidelines
Divide your food in to 2-3 meal – - Iftaar, Dinner & Sahur/predawn.Limit the amount of sweet food taken at iftaar – - Jelapi, Laddoo, burfi, Sweets, sugar containing sarbatLimit fried food- - Samosas , Pakoras, puri, parata, fried kababsChoose sugar free type drinks and drink plenty water

• Slow energy release foods ( such as wheat, semolina, beans, rice) should be taken before fasting, whereas foods high in saturated fat ( such as ghee, samosas, pakoras) should be minimized
• Advise to use small amount of monounsaturated oils in cooking
• Before and after fasting include high fibre foods such as whole grain cereals, brown rice, beans and pulses, fruits vegetables and salad

Exercise
-Maintain normal level of physical activity
-Excessive physical activity: increased risk of hypoglycemia (especially before Iftaar)
-Physical exercise can be performed about one hour after Iftaar.
-Taraweih are to be considered as part of the daily exercise

Management of patients with type 2 diabetes
The choice of treatment options should be
individualizedindividualized

Recommended changes to treatment regimen in patients with type 2 DM who fast during Ramadan(ADA Position Statement on Ramadan )Before Ramadan During Ramadan
Patients controled on diet and exercise
No change needed (modify time and intensity of exercise), ensure adequate fluid intake

Patients on oral agents
Before Ramadan During Ramadan
Biguanide, metformin 500 mg three times a day, or sustained release metformin
Metformin, 1,000 mg at the sunset meal (Iftaar), 500 mg at the predawn meal (Sahur)
TZDsAcarbose
No change needed

Patients on oral agents
Before Ramadan During Ramadan
Sulfonylureas once daily dose Glimepiride, gliclazide MR,
Dose should be given at Iftaar
Sulfonylureas BID dose Gliclazide, Glipizide
Full morning dose at the Iftaar and half of the usual evening dose at Sahur/Pre-dawn

Patients on oral agents
Before Ramadan During Ramadan
Glinides: Prandial regulators : Repaglinide, Nateglinide
These are quick acting tablet might be more suitable for taking when fasting
DPP-4 inhibitors Keep same dose as before
Liraglutide keep the same dose anytime but preferably during iftaar.

Patients on insulinBasal-Bolus
Bolus -Morning Insulin Dose –Full dose at Iftaar-Lunch dose – keep same dose if dinner is taken-Evening Insulin Dose – reduce 50% at Sahur Basal-If on intermediate acting -reduce 50% of intermediate acting Insulin at sahur -If on analogue - keep same dose at same time as before.
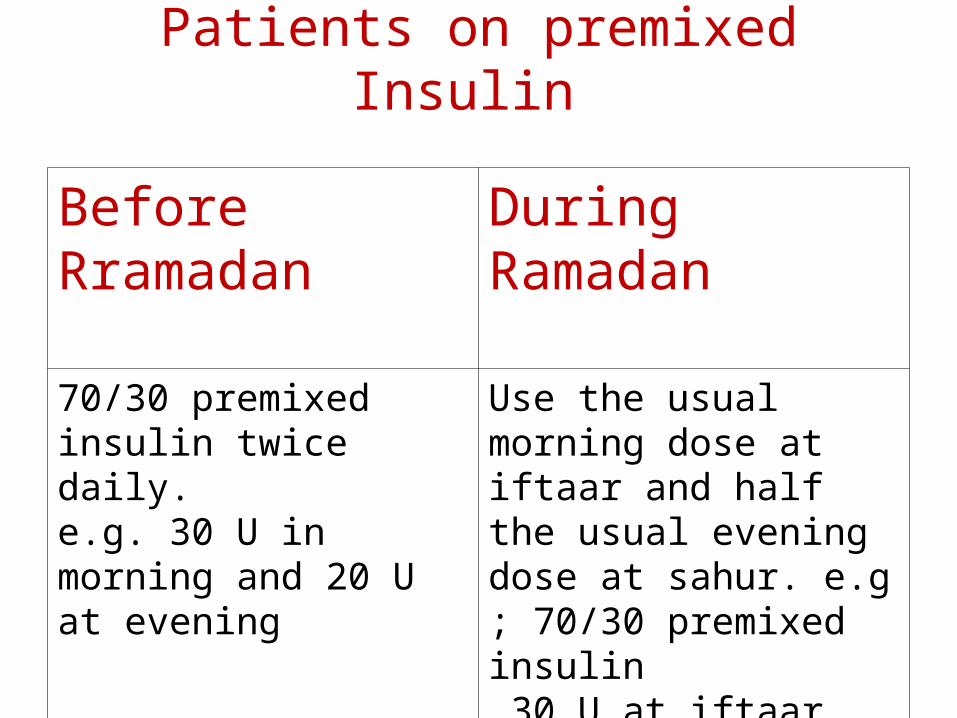
Patients on premixed Insulin
Before Rramadan During Ramadan
70/30 premixed insulin twice daily.e.g. 30 U in morning and 20 U at evening
Use the usual morning dose at iftaar and half the usual evening dose at sahur. e.g ; 70/30 premixed insulin 30 U at iftaar and 10 U at suhur

On premixed insulin + Metformin
Give Iftaar as same as for breakfast premixed dose but
Take Metformin at Sahur and Iftaar and patient may be okay and may not require premixed at Sahur
But if midday blood sugar control not good, add premixed 50% of normal evening dose at Sahur
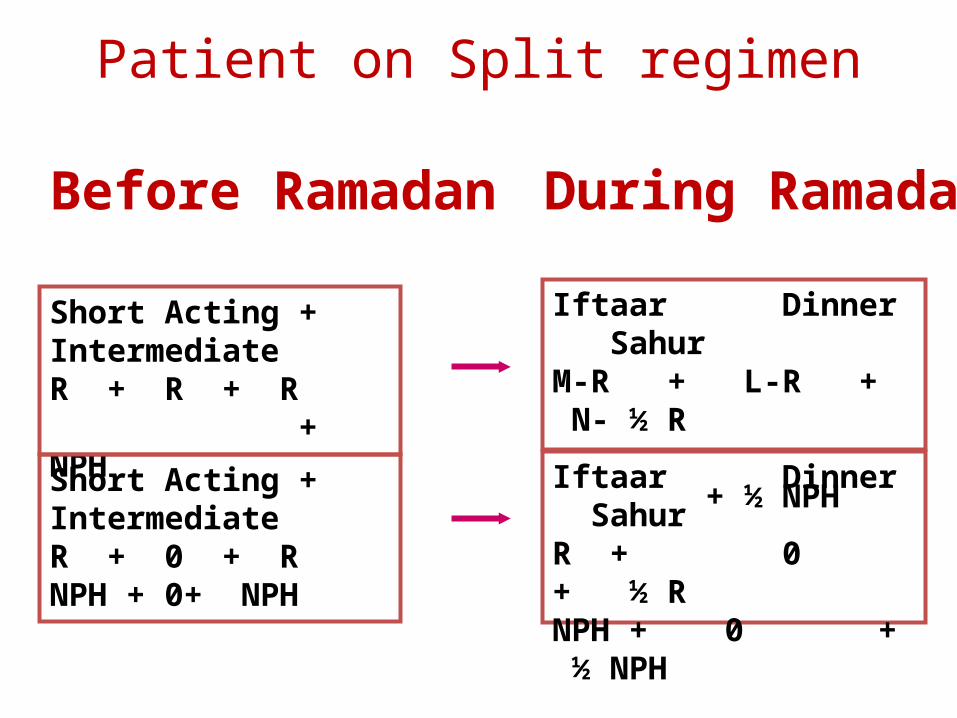
Before Ramadan
Short Acting + IntermediateR + R + R + NPH
During Ramadan
Short Acting + IntermediateR + 0 + RNPH + 0+ NPH
Iftaar Dinner SahurR + 0 + ½ RNPH + 0 + ½ NPH
Iftaar Dinner SahurM-R + L-R + N- ½ R + ½ NPH
Patient on Split regimen

Patients on combination of OHA and GLP-1 analogue
• Keep same dose of Liraglutide preferably during iftaar.
• Keep same dose of Metformin and
• Dose and time schedule of secretagogues should be reduced according to the treatment guideline of OHA during Ramadan.

Patients on combination basal insulin and GLP-1 analogue
• Keep the same dose of Liraglutide preferably during iftaar
• Basal insulin dose should be same at bed time
Monitoring during Ramadan
To recognize subclinical hypo and hyperglycemia
2hour post Suhur and one/half hour pre Iftaar - to pick subclinical hypoglycemia
2 hour post Iftar/ Dinner - to pick sub clinical hyperglycemia Adjust insulin dose 3 days interval
Pre-iftaar- Adjust Detemir/GlarginMid day-Adjust NPH2 h Post iftaar-Adjust iftaar bolus dose2 h Post dinner- Adjust dinner bolus dose2 h Post sahur-Adjust sahur bolus dose

Breaking the fast- Immediately if hypoglycemia occurs
(BG<60mg/dL, 3.3 mmol/L)
- If BG<70mg/dL, 3.9 mmol/L in the few hours after the start of the fast
- If BG exceeds 300 mg/dL (16.7 mmol/L) ketones in urine should be checked, medical advice sought
- Sick days
Pregnancy and fasting during RAMADAN• Pregnancy is a state of increased insulin resistance
• Elevated BG & HbA1c levels are associated with increased risk of major congenital malformations
• Should be strongly advised not to fast
• Ideally, patients should be managed by a team -Obstetrician, Endocrinologist, a Nutritionist and Diabetes Nurse Educators
• The management of pregnant patients during RAMADAN is based on appropriate diet and intensive insulin therapy
CONCLUSION
• Type 2 diabetes is largely asymptomatic and the treatments are inconvenient, impose on daily life and employment
• Lifestyle change is the most important but the most difficult to achieve
• In insulin-treated patients, hypoglycaemia is a major risk, especially in the young, elderly and long-standing Type 1 patients
• Monitor diabetes complications• Ensure older people are actively involved in
setting goals for their diabetes management

-Majority of uncomplicated type 2 diabetic patients can fast during
Ramadan safely though fasting during Ramadan for patients with
diabetes carries a risk of complications
-Type 1 diabetic patients should be strongly advised not to fast
(hypo- hyperglycemia)
-Type 2 diabetic patients, who fast during Ramadan, are at relatively
lower risk of hypo- hyperglycemia
-Pre-Ramadan medical assessment, education and motivation are
very important to prevent diabetes related complication
-Management plan must be highly individualized
-
Conclusion(Contd.)
• Thank you all