diagnosis and management of acute fracture–dislocation of the carpus
TRANSCRIPT

ADVANCED TECHNIQUES IN THE MANAGEMENT OF WRIST TRAUMA 0030-5898/01 $15.00 + .OO
DIAGNOSIS AND MANAGEMENT
DISLOCATION OF THE CARPUS OF ACUTE FRACTURE-
Robert Yaghoubian, MD, Felix Goebel, MD, Douglas S. Musgrave, MD, and Dean G. Sotereanos, MD
Acute fracture-dislocations of the carpus are uncommon inj~ries .~ If treated inadequately, however, these injuries can lead to wrist pain and dysfunction as a result of progressive trau- matic arthritis. Accurate diagnosis and early intervention are essential for excellent results.'
ANATOMY
The wrist joint allows for articulation of the radius and the ulna in the forearm to the metacarpals in the hand. The carpus itself con- sists of 2 transversely oriented rows of bone. The proximal row is made of scaphoid, lu- nate, and triquetrum. The distal row, in turn, consists of trapezoid, trapezium, capitate, and hamate. Extrinsic ligaments stablize the radio- carpal and the ulnocarpal articulations. These ligaments primarily exist on the palmar side of the wrist and include radioscaphocapitate, long radiolunate, short radiolunate, ulnolu- nate, and ulnotriquetral ligaments. The afore- mentioned ligaments form an inverted V on the volar side of the radiocarpal and the ulnocarpal joints (Fig. l).*
Intrinsic ligaments stabilize the midcarpal articulation and the articulations between
osseous structures of the same row. The im- portant intrinsic ligaments include the scaphol- unate, lunotriquetral, scaphocapitate, and triquetrocapitate.
On the palmar side, the lunocapitate articu- lation is devoid of any substantial ligamentous stability. This space is referred to as the space ofPoirier"j and is the primary site of weakness and tear in perilunate fracture-dislocations.
Dorsally the extrinsic and the intrinsic liga- ments are not as distinguishable. They are con- sidered primarily as thickening of the dorsal capsule.
EPIDEMIOLOGY
Acute fracture-dislocations of the carpus can be divided into 2 major categories: (1) per- ilunate fracture-dislocations and (2) axial fracturedislocations of the wrist. Perilunate fracturedislocations represent approximately 5% of wrist fractures and are about twice as common as pure ligamentous dislocations? These specific injuries often can be underdiag- nosed, causing delayed recognition and inter- vention. These injuries usually are due to high- energy trauma that occurs in motor vehicle
From the Division of Hand and Upper Extremity Surgery, Department of Orthopaedic Surgery, University of Pittsburgh, Pittsburgh, Pennsylvania
ORTHOPEDIC CLINICS OF NORTH AMERICA
VOLUME 30 NUMBER 2 APRIL 2001 295

296 YAGHOUBIAN et a1
TT TP CH
Figure 1. Anatomy of the palmar wrist ligaments. R = radius, U = ulna, S = scaphoid, L = lunate, T = tri- quetrum, P = pisiform, Tm = trapezium, Td = trapezoid, C = capitate, H = hamate, RA = radial artery, AIA = an- terior interosseous artery, PRU = palmar radioulnar liga- ment, RSC = radioscaphocapitate, LRL = long radiolunate, SRL = short radiolunate, UL = ulnolunate, UC = ulnocapi- tate, UT = ulnotriquetral, STT = scaphotrapeziotrapezoid, SC = scaphocapitate, TC = triquetrocapitate, TH = tri- quetrohamate, TT = trapeziotrapezoid, TC = trapezocapi- tate, CH = capitohamate. (From Berger RA: The ligaments of the wrist: A current overview of anatomy with consid- erations of their potential functions. Hand Clin 13:63-82, 1997; with permission.)
accidents, falls from a height, or contact sports. The incidence of axial fracture-dislocations of the carpus is less common than perilunate fracture-dislocations and is thought to be ap- proximately 1.5% of all carpal fractures.6 These injuries also are due to high-energy trauma and are associated especially with industrial accidents.6
MECHANISM OF INJURY
Mayfield et al," based on a cadaver model, described the mechanism of injury in perilu- nate dislocations. This injury characteristically forces the wrist into extension, ulnar devi- ation, and intercarpal supination. Based on this model, the wrist goes through 4 stages of instability as the severity of injury increases. In stage I, disruption of the scapholunate interosseous ligament occurs with perilunate dislocations. In the perilunate fracture-
dislocations, there is a scaphoid fracture instead. In stage 11, there is disruption of the dorsal ligamentous attachments to the lunate, and as the force propagates through the space of Poirier, the capitate dislocates away from the lunate. In stage 111, the force of injury progresses to involve the lunotriquetral joint and causes disruption of the lunotriquetral interosseous ligament. In stage IV, the lu- nate completely dislocates from the carpus and is extruded into the carpal tunnel. In the absence of a radial styloid fracture, the radioscaphocapitate ligament usually is torn.
Variations of perilunate fracture-disloca- tions can include fractures of the capitate, tri- quetrum, or both and presence or absence of radial or ulnar or both styloid fractures. Other staging systems have been used to accommo- date these variations (Fig. 2).'O A specific varia- tion of the perilunate fracture-dislocation is the scaphocapitate syndrome.4, l3 In this uncom- mon injury, there are fractures of the scaphoid and the capitate. The proximal portion of the capitate usually is rotated 180". The in- jury to the capitate can be missed on plain radiographs.
The mechanism of injury in axial fracture- dislocations is thought to involve dorsopal- mar compression of the wrist, resulting in lon- gitudinal splits of the carpus into 2 or more axial column^.'^ With dorsopalmar compres- sion, there is disruption of the transverse carpal and metacarpal arches, and avulsion of the flexor retinaculum from its peripheral inser- tions. These columnar injuries can involve the radial, ulnar, or both columns of the wrist.
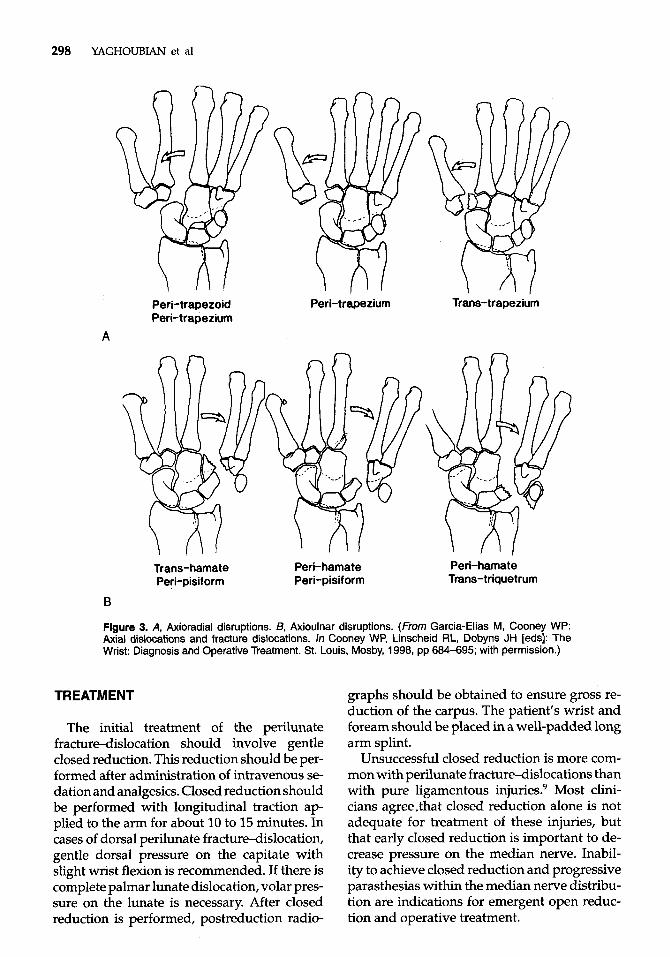
In axial-radial dislocations, the radial col- umn of the carpus is displaced distally and ra- dially. These injuries are divided into 3 groups: peritrapezoid, peritrapezium, and transtrapez- ium. In axial-ulnar dislocations, the ulnar column is displaced proximally and ulnarly. Three groups of the axial-ulnar dislocations include transhamate, perihamate peripisi- form, and perihamate transtriquetrum (Fig. 3A and BL5 .
DIAGNOSIS
Patients with perilunate fracture-disloca- tions usually present with wrist pain, swell- ing, and crepitus. There is abnormal wrist

DIAGNOSIS AND MANAGEMENT OF ACUTE FRACTURE-DISLOCATION OF
I I
THE CARPUS 297
/
Stage I Trans-radial styloid Stage 11 Trans-scaphoid Stage 111 Trans-capitate Stage IV Trans-triquetral
Stage V Lunate dislocation
I Short radiolunate jcaphoid \ Lunab ligament
Figure 2. Stages of perilunate fracture dislocations: I = radial styloid, II = scaphoid, 111 = capitate, IV = triquetrum, V = complete h a t e dislocation. (From Kozin SH, Murphy MS, Sooney WP: Perilunate dislo- cations. In Cooney WP, Linscheid RL, Dobyns JH [eds]: The Wrist: Diagnosis and Operative Treatment. St. Louis, Mosby, 1998, pp 632-650; with permission.)
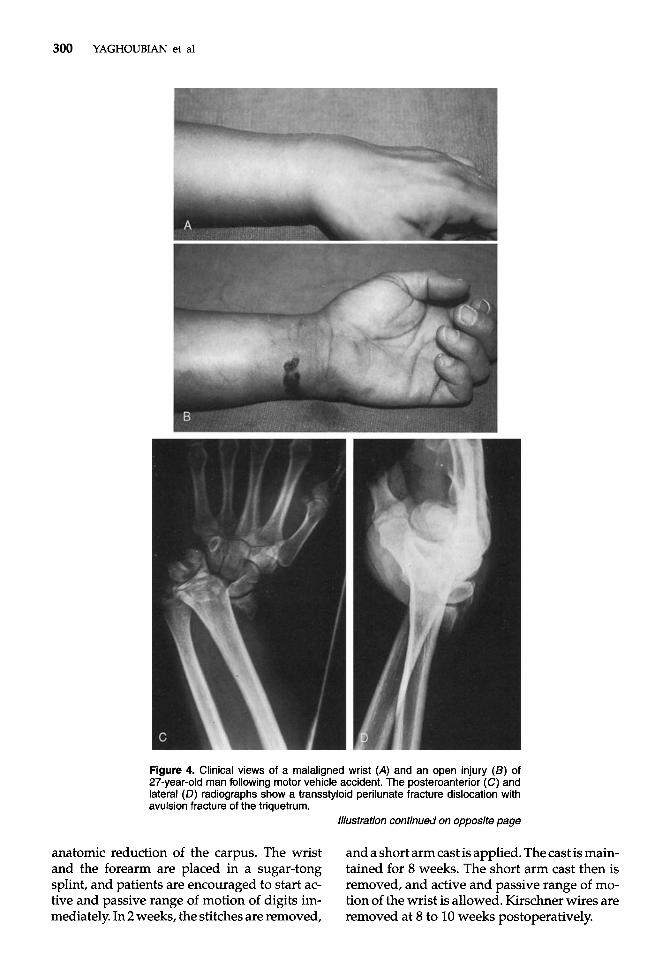
alignment that can be apparent on clinical examination to an experienced eye (Fig. 4A). These patients usually complain of parasthe- sias in the median nerve distribution. The digits usually are kept in a flexed posture, and pas- sive extension can be painful (Fig. 4B).
Radiographic evaluation of these injuries is important. Because about 20% of perilunate in- juries are misdiagnosed with the initial radio- graphic evaluation: posteroanterior and lat- eral radiographs should be obtained in every case. The presence of associated fractures may divert the attention of physicians away from the carpal subluxations or dislocations. True lateral radiographs usually show a loss of col- inearity that exists between the radius, lunate, and capitate. In earlier stages of perilunate fracturedislocation, the lunate remains colin- ear with the radius, as the capitate subluxes dorsally. In stage IV, the capitate remains col- inear with the radius, however, as the lunate is dislocated palmarly (Fig. 5). Distraction ra- diographs can be helpful to delineate any other associated fracture or dislocation that was not
apparent at first glance (see Fig. 4C through E). Additional radiographic studies usually are not necessary in the acute setting. The only ex- ception to this rule is seen in cases of scapho- capitate syndrome. In these injuries, because the capitate fracture may not be obvious on ra- diographs, plain a CT scan or MR imaging scan may be necessary to assess and diagnose the capitate fracture.
Patients with axial fracture-dislocations usually present with associated severe soft tissue injuries, and many are open. There is significant damage to the intrinsic muscula- ture. Associated neurovascular or tendon in- juries can be present. There usually is loss of the metacarpal and carpal arches secondary to a longitudinal split within the hand and thecarpus (Fig. 6).15
Radiographic assessment is crucial in these cases. Axial separation of the carpus and metacarpals is key to the diagnosis. There also can be sagittal fractures of the metacarpals or the carpal bones and rotation deformities of the digits.
298 YAGHOUBIAN et a1
Peri-trapezoid Peri-trapezium Peri-trapezium
Trans-trapezium
A
Trans-hamate Peri-hamate Peri-hamate Peri-pisiform Peri-pisiform Trans-triquetrum
B
Figure 3. A, Axioradial disruptions. 6, Axioulnar disruptions. (From Garcia-Elias M, Cooney WP: Axial dislocations and fracture dislocations. In Cooney WP, Linscheid RL, Dobyns JH [eds]: The Wrist: Diagnosis and Operative Treatment. St. Louis, Mosby, 1998, pp 684-695; with permission.)
TREATMENT
The initial treatment of the perilunate fracture-dislocation should involve gentle closed reduction. This reduction should be per- formed after administration of intravenous se- dation and analgesics. Closed reduction should be performed with longitudinal traction ap- plied to the arm for about 10 to 15 minutes. In cases of dorsal perilunate fracture-dislocation, gentle dorsal pressure on the capitate with slight wrist flexion is recommended. If there is complete palmar lunate dislocation, volar pres- sure on the lunate is necessary. After closed reduction is performed, postreduction radio-
graphs should be obtained to ensure gross re- duction of the carpus. The patient’s wrist and foream should be placed in a well-padded long arm splint.
Unsuccessful closed reduction is more com- mon with perilunate fracturedislocations than with pure ligamentous injuries? Most clini- cians agree.that closed reduction alone is not adequate for treatment of these injuries, but that early closed reduction is important to de- crease pressure on the median nerve. Inabil- ity to achieve closed reduction and progressive parasthesias within the median nerve distribu- tion are indications for emergent open reduc- tion and operative treatment.

DIAGNOSIS AND MANAGEMENT OF ACUTE FRACTURE-DISLOCATION OF THE CARPUS 299
Operative treatments of this problem include closed reduction and pin fixation versus open reduction and internal fixation and direct re- pair of torn ligaments. For percutaneous pin fixation to be successful, the closed reduction has to be perfect. Slight malalignment of the carpus is unacceptable because this can lead to chronic wrist instability and SLAC wrist. Per- fect closed reduction of these injuries may be impossible to achieve, however, as is explained by Mayfield's paradox." Although the ideal position for rotatory scapholunate dissociation or scaphoid fracture would be wrist extension, maintenance of a position of wrist extension would be detrimental to healing of torn palmar ligaments. For transscaphoid variants of per- ilunate dislocations, the paradox is solved by using a compression screw to treat the scaphoid fracture.
Open reduction, internal fixation, and anato- mic ligamentous repair have become the main- stay of treatment all perilunate inj~ries. '~, '~ Different surgical approaches have been de- scribed to address this injury. It has become clear, however, that combined volar and dor- sal approaches provide the most reliable means for anatomic repair.I8 A palmar approach usu- ally is needed to repair the rent in the volar capsule at the lunocapitate joint and release the carpal tunnel. It can be difficult to fix the scaphoid fracture adequately through this ap- proach, however. The dorsal approach usu- ally is needed to fix the scaphoid fracture or repair the torn scapholunate interosseous ligament.
The authors' preferred approach is a com- bined volar and dorsal approach. A standard carpal'tunnel incision is made to release the flexor retinaculum. The lunate is reduced in the lunate fossa so that on the lateral radiograph there is colinear alignment of the radius and the lunate. Provisional pin fixation is made from the radius into the lunate.
A longitudinal midline incision is made dorsally. The extensor retinaculum is divided between the third and fourth compartments. The extensor pollicis longus is released and retracted radially. The dorsal wrist capsule is isolated and opened through a longitudinal in- cision. Reduction of the lunate then is checked dorsally. The scaphoid fracture, if present, is reduced and stabilized provisionally using a 0.045-inch Kirschner wire. A compression
screw of choice is used to provide permanent fixation of this fracture. Anatomic fixation of this fracture is ensured using intraoperative fluoroscopy.
In cases of perilunate injury without scap- hoid fracture, it is essential to repair the scapholunate interosseous ligament. This re- pair can be done either by using bone anchor in the scaphoid because the ligament usually avulases off of the scaphoid or by making drill holes through the scaphoid. Before the ligament repair, the scapholunate joint should be reduced anatomically using a 0.045-inch Kirschner wire in the scaphoid as a joystick. The scapholunate joint is stabilized using a 0.062-inch Kirschner wire from radial to ulnar, and intraoperative fluoroscopy should be used to check this reduction. On the lateral projec- tion, the angle between the scaphoid and the lunate should be 45" to 60".
The other 2 intercarpal articulations with the lunate need to be addressed next. The capitate is reduced to the lunate first. This reduction should be checked radiographically. On the lateral projection, there should be a colinear relationship between the capitate, the lunate, and the radius. It is crucial that lunate not be in dorsiflexion or palmar flexion. After attain- ing an anatomic reduction of the capitate, an- other 0.062-inch Kirschner wire is placed from scaphoid into the capitate. The triquetrum is reduced to the lunate and stabilized with an- other 0.062-inch Kirschner wire. At this time, the rent in the volar capsule at the level of the lunocapitate joint is repaired with nonab- sorbable suture. In stage IV perilunate injuries, in which the radioscaphocapitate or long radi- olunate ligaments (or both) have avulsed off of the radial styloid, they can be repaired to the radius using bone anchors.
In the case of a scaphocapitate syndrome, the capitate is addressed through the dorsal approach. Usually the proximal portion of the capitate is rotated 180", this needs to be reduced anatomically and stabilized using a compres- sion screw. The tip of this screw, similar to any other screw within the carpus, should be buried under the proximal articular surface. In cases in which there is a styloid fracture, it can be fixed through the dorsal approach using a compres- sion screw or Kirschner wires.
At the conclusion of the case, intraopera- tive radiographs should be obtained to ensure
300 YAGHOUBIAN et a1
Figure 4. Clinical views of a malaligned wrist (A) and an open injury (B) of 27-year-old man following motor vehicle accident. The posteroanterior (C) and lateral (D) radiographs show a transstyloid perilunate fracture dislocation with avulsion fracture of the triquetrum.
Illustration continued on opposite page
anatomic reduction of the carpus. The wrist and the forearm are placed in a sugar-tong splint, and patients are encouraged to start ac- tive and passive range of motion of digits im- mediately. In 2 weeks, the stitches are removed,
and a short arm cast is applied. The cast is main- tained for 8 weeks. The short arm cast then is removed, and active and passive range of mo- tion of the wrist is allowed. Kirschner wires are removed at 8 to 10 weeks postoperatively.

DIAGNOSIS AND MANAGEMENT OF ACUTE FRACTURE-DISLOCATION OF THE CARPUS 301
Figure 4 (Continued). €, A distraction radiograph was then obtained to assess the injury further. Fand G, Postoperative radiographs show the realignment of the carpus.
Axial fracture-dislocations usually are open injuries and are associated with severe soft tissue damage, including neurovascular and tendinous injuries. In these instances, imme- diate irrigation and dkbridement is performed, and bone stability is restored by open reduction and internal fixation of fracture-dislocations. Usually, Kirschner wire fixation is sufficient to stabilize osseous injuries; however, compres- sion screws can be used as needed to aug- ment fixation. Appropriate primary repair or grafting of associated neurovascular or tendi- nous injuries is performed next. In cases of closed injuries, if anatomic reduction can be
attained, percutaneous fixation may be suffi- cient to maintain the reduction. The wrist is immobilized with a short arm cast for about 8 weeks. At 10 to 12 weeks, the Kirschner wires are removed. Occupational therapy is begun for wrist range of motion and strengthening.
RESULTS
Perilunate injuries of the carpus can be dis- abling. Despite excellent radiographic results, patients may end up with significant loss of motion and grip strength.* The outcome of these injuries not only depends on the severity

302 YAGHOUBIAN et a1
Figure 5. Transstyloid, transscaphoid lunate dislocation in a 34-year-old man following a biking accident. The scaphoid is fractured at its waist. There is also a mildly displaced radial styloid fracture (A). B, The lunate is rotated and dislocated into the carpal tunnel. C, The median nerve was compressed by the dislocated lunate.
of the initial trauma, but also on many other factors along the course of treatment. Delay in treatment can be associated with irreversible injuries to the median nerve and with increased difficulty in attaining an anatomic reduction. Results are correlated closely with obtaining an accurate anatomic reduction of the fractures and dislocations of the carpus.” l2 Failure to restore wrist alignment can lead to develop- ment of early arthritis and SLAC wrist. Irre- versible damage or loss of the articular surfaces cannot be corrected surgically and is associ- ated with chronic wrist pain. In these instances, salvage procedures might involve proximal
row carpectomy, or partial or complete wrist arthrodesis.
The outcome of axial fracture-dislocations of the carpus depends on associated soft tissue injuries. Based on a series of patients treated at the Mayo Clinic, nerve injury was associ- ated especially with poor result^.^ Patients with ulnar axial fracture-dislocations had a 3 times increased incidence of nerve injury than pa- tients with similar injuries on the radial side. In cases in which there is no concomitant neu- rovascular or tendinous injury, an anatomic re- duction usually is associated with satisfactory outcome.

DIAGNOSIS AND MANAGEMENT OF ACUTE FRACTURE-DISLOCATION OF THE CARPUS 303
Figure 6. Radiographs of the wrist of a 36-year-old man after crush injury to the wrist. The patient sustained a combined axial and perilunate fracture dislocation. A and 6, Associated injuries included ulnar artery, ulnar nerve, flexor tendon lacerations, and comminuted fracture of the small finger middle phalanx. Cand D, Postoperative radiographs show realignment of the carpus and reduction of the base of the ring finger metacarpal to the hamate.
304 YAGHOUBIAN et a1
COMPLICATIONS
Complications of perilunate injuries include missed diagnosis, median neuropathy, resid- ual or chronic carpal instability, nonunion or malunion of fractures, avascular necrosis of the scaphoid or the lunate, arthrosis, and pro- gressive posttraumatic arthritis. Inaccurate or missed diagnosis can lead to chronic perilunate instability and severe degenerative arthriti~.~, Thorough clinical and radiographic evalua- tions are important and are essential for pre- vention of this complication. .
Median nerve paresthesia usually is related to the initial injury. The subluxed or dislo- cated lunate may encroach on the carpal tun- nel and cause pressure on the median nerve. Early closed reduction and decompression of the carpal tunnel during surgical treatment is recommended. In cases of closed injuries, in- ability to obtain closed reduction and progres- sive median nerve neuropathy are indications for emergent operative intervention.
Avascular necrosis of the scaphoid occurs infrequently after transscaphoid perilunate injuries and can be lessened with rigid in- ternal fixation of the scaphoid. Treatment of ischemic necrosis of the scaphoid includes re- vision open reduction and internal fixation. Supplementary bone graft usually is necessary to increase the success of this procedure. Vas- cularized distal radius autograft might be a consideration, however, the intial trauma may injured the blood supply to the appropriate portion of the distal radius. Avascular necro- sis of the lunate, although rare, if present, is usually a transient phenomenon. This en- tity should not be confused with Kienbock’s disease.’’ The diagnosis can be suspected based on plain radiographs, when the lunate is radio- paque compared with adjacent carpal bones. Treatment of transient ischemia of the lunate usually is observation.
Nonunion of the scaphoid, if not treated, can lead to avascular necrosis of the proximal pole of the scaphoid or scaphoid nonunion ad- vanced collapse. This complication usually is treated with revision open reduction, internal fixation, and supplemental bone grafting.
In cases of scaphoid malunion, the normal articulation between the radial styloid and the scaphoid is lost. A dorsal humpback deformity of the scaphoid is shown on lateral films or CT
scan. To prevent progressive arthritis, open re- duction of the scaphoid with a wedge of iliac crest autograft may be necessary.
Residual and chronic perilunate instability is a challenging dilemma for an experienced ~1inician.I~ This instability could be of a dis- sociative pattern; that is, it could involve scapholunate or lunotriquetral ligament dis- ruption. It also can be of a nondissociative pattern, in which there is an instability of the midcarpal or radiocarpal joints. Radiocarpal instability is evident by translocation of the en- tire carpus on the radius, usually in an ulnar direction.
A dynamic dissociative pattern is shown by lack of carpal bone malalignment on plain ra- diographs and presence of widening of the scapholunate or lunotriquetral intervals on stress radiographs. The treatment for dynamic scapholunate or lunotriquetral instability is lig- ament reconstruction and dorsal capsulode- sis. Chronic nondissociative instability or static dissociative patterns usually are treated with a salvage procedure of choice. These procedures, which include proximal row carpectomy and limited or complete wrist fusion, also are ap- propriate surgical treatments for progressive wrist arthritis. Complications seen with axial fracturedislocations include adhesion of re- paired nerves or tendons, progressive arthritis, and first web space ~ontracture.~
SUMMARY
Perilunate dislocations and fracture-dislo- cations of the carpus are devastating injuries. To minimize morbidity, an early and accu- rate diagnosis is essential. Although an early closed reduction is recommended, understand- ing wrist kinematics has allowed clinicians to realize that anatomic open reduction, inter- nal fixation, and ligamentous repair are vi- tal for optimal functional results. This repair is achieved best using a combined volar and dorsal approach. Outcome is correlated with the magnitude of the initial trauma and accu- racy of the reduction. Associated injuries in the axial fracturedislocations usually dictate the outcome. Repair of these associated injuries and anatomic reduction and fixation of frac- ture-dislocations are important for excellent results.
DIAGNOSIS AND MANAGEMENT OF ACUTE FRACTURE-DISLOCATION OF THE CARPUS 305
References
1. Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their po- tential functions. Hand Clin 13:63-82,1997
2. Cooney WP, Bussey R, Dobyns JH, et a1 Difficult wrist fractures: Perilunate fracture dislocations of the wrist. Clin Orthop 214:13&147,1987
3. Cooney WP, Linscheid RL, Dobyns JH: Fractures and dislocations of the wrist. In Rockwood CA Jr, Green DP, Bucholtz RW (eds): Fractures in Adults, ed 3. Philadel- phia, JB Lippincott, 1991, pp 563-678
4. Fenton RL The naviculo-capitate fracture syndrome. J Bone Joint Surg Am 38:681-684,1956
5. Garcia-Elias M, Cooney WP: Axial dislocations and fracture dislocations. In Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist Diagnosis and Operative Treatment. St Louis, Mosby, 1998, pp 684-695
6. Garcia-Elias M, Dobyns JH, Cooney WP 111, et al: Trau- matic axial dislocations of the carpus. J Hand Surg Am 14446457,1989
7. Green DP, OBrien ET Open reduction of carpal dislo- cations: Indications and operative techniques. J Hand Surg Am 3:250-265,1978
8. Herzberg G, Comtet JJ, Linscheid RL, et a1 Perilu- nate dislocation and fracture dislocations: A multicen- ter study. J Hand Surg Am 18:768-779,1993
9. Jasmine MS, Packer JW, Edwards GS Jr: Irreducible transscaphoid perilunate dislocation. J Hand Surg Am
10. Kozin SH, Murphy MS, Cooney WP: Perilunate dis- locations. In Cooney WP, Linscheid RL, Dobyns JH
13:212-215,1988
(eds): The Wrist: Diagnosis and Operative Treatment. St Louis, Mosby, 1998, pp 632-650
11. Mayfield JK, Johnson RP, Kilcoyne RK Carpal dislo- cations: Pathomechanics and progressive perilunar in- stability. J Hand Surg Am 5:226-241,1980
12. Minami A, Ogino T, Ohshio I, et al: Correlation between clinical results and carpal instabilities in patients after reduction of lunate and perilunar dislocations. J Hand Surg Br 11:213-220,1986
13. Monahan PR, Galasko CS: The scapho-capitate fracture syndrome: A mechanism of injury. J Bone Joint Surg Br
14. Moneim MS, Hofammann KE 111, Omer GE: Transs- caphoid perilunate fracture-dislocation: Results of open reduction and pin fixation. Clin Orthop 190:227- 235,1984
15. Norbeck DE Jr, Larson 8, Blair SJ, et a1 Traumatic lon- gitudinal disruption of the carpus. J Hand Surg Am
16. Poirier P, Charpy A: Traite danatomie humaine, ed 3. Paris, Masson, 1911
17. Siegert JJ, Frassica FJ, Amadio PC: Treatment of chronic perilunate dislocations. J Hand Surg Am 13:20&212, 1988
18. Sotereanos DG, Mitsionis GJ, Giannakopoulos GN, et al: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 22:49-56,1997
19. White RE Jr, Omer GE Jr: Transient vascular compro- mise of the lunate after fracture-dislocation or dis- location of the carpus. J Hand Surg Am 9:181-184, 1984
54: 122-1 24,1972
12:509-514,1987
Address reprint requests to
Dean G. Sotereanos, MD Division of Hand and Upper Extremity Surgery
Department of Orthopaedic Surgery Kaufmann-Building, Suit 911
Fifth Avenue Pittsburgh, PA 15213