diagnosis of temporomandibular dysfunction syndrome—image quality at 1.5 and 3.0 tesla magnetic...
TRANSCRIPT

Eur Radiol (2009) 19: 1239–1245DOI 10.1007/s00330-008-1264-7 MAGNETIC RESONANCE
Martina Schmid-SchwapWolfgang DrahanowskyMargit BristelaMichael KundiEva PiehslingerSoraya Robinson
Received: 23 July 2008Revised: 31 October 2008Accepted: 12 November 2008Published online: 10 January 2009# European Society of Radiology 2008
Diagnosis of temporomandibular dysfunction
syndrome—image quality at 1.5 and 3.0 Tesla
magnetic resonance imaging
Abstract The purpose of this studywas to examine the differences inexpert ratings of quality of magneticresonance images (MRI) of the tem-poromandibular joint in 24 patientswith suspected anterior disc displace-ment examined in randomized order at
1.5 and 3.0 T. Parasagittal (closed andopened mouth) and paracoronal sec-tions were performed with a surfacecoil. Two experienced examinersblinded to patient status and type ofMRI diagnosed the images accordingto position of condyle, position andchanges in the signal, and disc shape.In addition, perceptibility of positionand disc shape were assessed. Ahighly significant difference in theperceptibility of disc shape (P<0.001)and position (P<0.001) was obtained.With comparable examination se-quences and identical resolution, the3.0 T MRI of the temporomandibularjoint increases the perceptibility ofjoint structures.
Keywords 3.0 Tesla . Magneticresonance imaging .Temporomandibular joint .Temporomandibular disorders .Clicking
Introduction
Joint disorders are among the most common causes ofillness in the adult population. Patients with disorders ofthe stomatognathic system describe pain and clickingphenomena as primary symptoms. Very frequently theyalso report problems with cervical and neck muscles,limited range of motion, parafunction, headache, andtinnitus. In most cases, anterior disc displacement withinthe joint is identified as the morphological basis forclicking [1–3].
The merits of magnetic resonance imaging (MRI) usingfield strengths of 1.5 T have been well established in thediagnosis of temporomandibular disorders [4, 5]. Absence
of ionizing radiation as well as excellent depiction andvisualization of soft tissue, disc position and morphology,bone marrow changes, and joint effusions are among theadvantages of MRI [6–8]. Katzberg has differentiated thefollowing disc positions: superior or 12-o’clock position(normal position), anterior, anteromedial, and anterolateral[9]. He describes the pathological changes in disc shapefrom the original and normal biconcave shape to abiconvex shape or a shape with obvious deformities orthickening. Intricate structural details of the articular discand the posterior disc attachment may also be depicted andused in the diagnosis of pathological articular changes [5].
High-field MRI with field strengths of more than 2 T hasbeen available for several years and has been increasingly
M. Schmid-Schwap (*) .M. Bristela .E. PiehslingerDepartment of Fixed and RemovableProsthodontics, Bernhard GottliebUniversity Clinic of Dentistry,Währingerstrasse 25a,1090 Vienna, Austriae-mail: [email protected].: +43-4277-67171Fax: +43-4277-67179
M. Bristelae-mail: [email protected]
E. Piehslingere-mail: [email protected]
W. Drahanowsky . S. RobinsonDiagnostic Center Urania,Laurenzerberg 2,1010 Vienna, Austria
W. Drahanowskye-mail: [email protected]
S. Robinsone-mail: [email protected]
M. KundiMedical University of Vienna,Institute of Environmental Health,Center for Public Health,Kinderspitalgasse 15,1090 Vienna, Austriae-mail: [email protected]
used for clinical purposes [10, 11]. While several compar-isons between 1.5 and 3.0 T units with regard to organs andblood vessels have already been performed, only a few 3.0 Tstudies of joints have been reported [12–18]. In a study ofhealthy temporomandibular joints (TMJ), Stehling et al.were able to demonstrate that use of 3.0 T units allowedfor an improved analysis of the small joint structures [19].No studies have yet been reported on the suitability of 3.0T units for the evaluation of temporomandibular dis-orders.
It has been the goal of this study to evaluate whether theincreased signal-to-noise ratio at 3.0 T can improveradiological confidence in the evaluation of patientswith symptomatic temporomandibular joint disease(TMD).
Materials and methods
Patients
During the period from November 9, 2006 to March 12,2007, 144 patients presented at our Outpatient Unit forFunctional Disorders. Patients with unilateral or bilateralTMJ clicking or clinically suspected anterior disc displace-ment in at least one joint were offered enrolment in thestudy. Exclusion criteria included age younger than18 years, fixed orthodontic device, metallic foreign bodiesin the head region, presence of biostimulators (pacemaker,insulin pump, etc.), claustrophobia, tremor or other form ofmotor unrest, and pregnancy. Thirty patients fulfilled theinclusion criteria; three patients declined participation andtwenty-seven patients were enrolled in the study. Onepatient failed to attend the scheduled visit, one patientwithdrew from the study, and for one patient the imagesobtained were not evaluable because of movementartifacts. Thus, images of 24 patients were available forevaluation.
This study was approved by the Ethics Committee of theMedical University of Vienna and the General Hospital ofthe City of Vienna (EK 404/2006). The experiments wereundertaken after written informed consent was obtainedfrom each patient.
Magnetic resonance imaging
The patients underwent magnetic resonance imaging withclosed and opened mouth both at 1.5 T (Philips Intera 1.5,Philips Medical Systems, The Netherlands) and 3.0 T(Philips Achieva 3.0, Philips Medical Systems, TheNetherlands) in randomized order. For all patients, bothjoints were imaged simultaneously. For both images,Sense-Flex-M surface coils were used. Parasagittal(Figs. 1 and 2) and paracoronal (Fig. 3) slices wereacquired. The MR parameters are shown in Table 1.
Randomization
The sequence of examinations with the 1.5 and 3.0 T unitswas randomized. Randomization was done based on aprepared random list, such that half of the patients
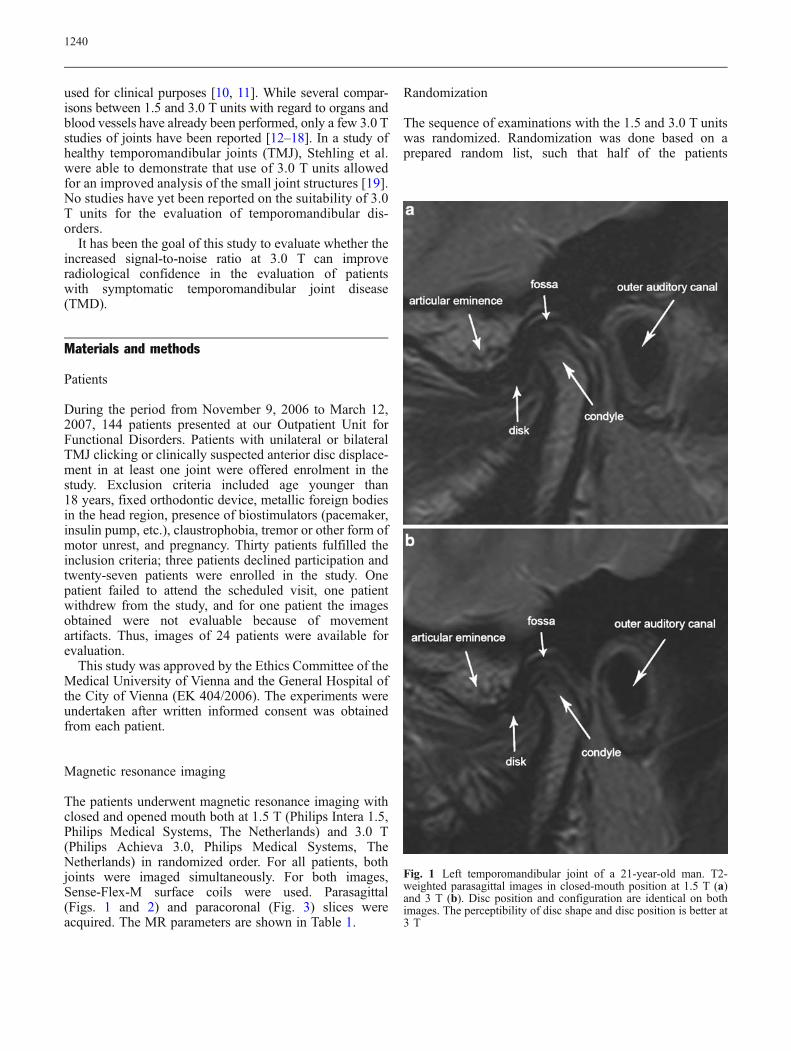
Fig. 1 Left temporomandibular joint of a 21-year-old man. T2-weighted parasagittal images in closed-mouth position at 1.5 T (a)and 3 T (b). Disc position and configuration are identical on bothimages. The perceptibility of disc shape and disc position is better at3 T
1240

underwent the 1.5 T examination first, while the other halfunderwent the 3.0 T examination first.
Ratings of images
Two experienced examiners (one radiologist specialized inhead and neck imaging for 17 years and one dentist
specialized in TMJ dysfunction syndrome for 13 years)were blinded to patient identity, clinical findings, and typeof MRI. They assessed the images independently of eachother in randomized order on the same day on differentmachines in separate rooms. The two exams on eachpatient were presented at the same time. Using a dedicatedMR work station, the examiners evaluated the closed
Fig. 2 Right temporomandibular joint of a 31-year-old man. T2-weighted parasagittal images in closed-mouth position at 1.5 T (a)and 3 T (b). The disc is far better delineated at 3T than at 1.5 T
Fig. 3 Paracoronal sections of the same joint as in Fig. 1 at 1.5 T (a)and 3 T (b). Note the better delineation especially of the lateralportion of the disc
1241

images for (1) perceptibility of disc position/delineation tosurrounding tissue (delineation of the disc to fossaand condyle), (2) disc shape, using a five-point scale (1=excellent delineation with defined sharply bounded lines,5=insufficient delineation, structures not circumscribable),(3) changes in the signal (evenly dark, central brightening,focal brightening, disc residues), and (4) shape of the disc(biconcave, flattened, biconvex, deformed). In addition, (5)location and position of condyle (normal, retral, anterior,lateral, compression, distraction) and (6) disc (anteriordislocation with reposition, without reposition) were alsoassessed.
Statistical evaluation
Statistical evaluation of disc shape and position by the raterswas done by two-factorial analysis of variance for repeatedmeasurements with raters and type of MRI as factors.
Normality of residuals was assessed by Kolmogorov-Smirnov tests.
Interobserver agreement was tested by weighted Kappacoefficients. For all statistical tests, P values below 0.05were considered significant.
Results
Forty-eight TMJ images of 24 patients were evaluated.Five of the patients were male, and 19 were female. Theaverage age was 35.5±13.0 years.
For 15 TMJs, normal position of condyle was seen, 10showed a retral position, 5 lateral position, 2 compression,and 3 distraction; 13 joints showed combinations. In sevenpatients, the disc showed bilateral displacement withreposition upon mouth opening, and two patients showeda bilateral anterior disc displacement without reposition.Eight patients showed a unilateral disc displacement with
Table 1 Magnetic resonance parameters of the sequences at 1.5 and 3.0 T
T2w-TSE sequence T1w-TSE sequence PDw-TSE sequence
Parasagittal closed mouth Paracoronal closed mouth Parasagittal opened mouth
1.5 T 3.0 T 1.5 T 3.0 T 1.5 T 3.0 T
FOV (mm) 150 150 130 130 150 150
Slices 15 15 8 8 15 15
Slice thickness (mm) 2 2 2 2 2 2
TSE factor 14 14 4 6 6 6
TR (ms) 4,823 4,147 550 551 2,451 2,375
TE (ms) 80 80 13.9 8.4 20 20
Flip angle (°) 90 90 90 90 90 90
NSA 4 2 3 4 4 2
Scan duration (min) 3:56 3:27 3:39 4:06 4:10 4:35
Measured voxel size (mm) 0.55/0.71/2.00 0.55/0.71/2.00 0.54/0.68/2.00 0.54/0.68/2.00 0.55/0.79/2.00 0.55/0.79/2.00
Reconstructed voxel size (mm) 0.29/0.29/2.00 0.29/0.29/2.00 0.51/0.50/2.00 0.51/0.50/2.00 0.29/0.29/2.00 0.29/0.29/2.00
Table 2 Assessment of disc shape and signal intensity by examiner and unit (1.5 T, 3 T) in percentage of joints (n=48)
Assessment of Category 1.5 T 3 T
Examiner 1 Examiner 2 Examiner 1 Examiner 2
Disc shape Biconcave 75 62 70 64
Flat 8 17 10 18
Deformed 17 21 20 18
Signal intensity Evenly dark 79 77 56 54
Central brightening 13 15 14 16
Focal brightening 4 4 22 22
Residues 4 4 8 8
1242

reposition and four patients a combination of discdisplacement with or without reposition on the differentsides. In three patients MRI failed to show any discdisplacement. The assessment did not reveal any inter-observer differences with the disc position in one jointbeing not clearly evaluable in the 1.5 T image for bothobservers. In addition, disc shape and signal intensity werealso assessed. The individual percentage ratings are shownin Table 2 with a biconvex disc being found in none of thepatients.
In Table 3 the results of the ratings for perceptibility ofdisc shape and disc position have been listed separatelyfor the two units. The 3.0 T unit consistently providedbetter results than the 1.5 T unit. This difference wasindependent of disc pathologies (displacement, position ofcondyle).
The difference between the two units was highly signif-icant for left and right sides with regard to perceptibility ofshape as well as position, while no significant differencebetween raters was found (Table 4).
Interobserver agreement was assessed with respect totwo different aspects: (1) perceptibility of disc shape andposition and (2) assessment of pathology of disc shape andsignal intensity. Raters showed only low to moderateagreement in their assessment of the perceptibility of shape(0.334 for 1.5 T and 0.488 for 3 T) and position (0.450 for1.5 T and 0.384 for 3 T). The assessment of pathologies indisc shape and signal intensity showed good to excellentconsistency between observers (disc shape: 0.728 for 1.5 T
and 0.764 for 3 T, signal intensity: 0.639 for 1.5 T and0.969 for 3 T) that was consistently higher at 3 T(statistically significant for signal intensity).
Discussion
Temporomandibular dysfunction syndrome ranks third infrequency among orofacial disorders [20]. A higherprevalence in female patients is a well known phenomenonwith some authors having described more than 80%females [21, 22], which is in accordance with a rate ofabout 80% females in the present study. The average age of35.5 years of the patients enrolled in the study is similar tothe results of other authors [22, 23].
The importance of MRI in the diagnosis of TMD hasbeen confirmed in numerous studies [4, 5, 7, 8].Improvement of the quality of TMJ MRI could be achievedwith the use of higher field strengths [24] as a result of theirhigher signal-to-noise ratios [11]. The benefits of higherfield strengths have already been shown for the examina-tions of various joints. In comparative studies of smallerjoints, field strengths of 3.0 T provided for superior qualityversus a field strength of 1.5 T [13, 19].
Precise visibility and clear evaluability of joint structuresis of major importance for the diagnostic assessment ofabnormalities. As clinical diagnosis does not alwaysprovide a complete image of joint structures [4, 25–28],accurate diagnostic assessment with MRI is indispensable.
Table 3 Average grading (1=excellent to 5=very poor/insufficient) by examiner and unit (1.5, 3 T) of perceptibility of disc position anddisc shape across joints (n=48)
Perceptibility of 1.5 T 3 T
Examiner 1 Examiner 2 Examiner 1 Examiner 2
Disc shape Mean 2.61 2.79 1.62 1.58
SD 0.95 0.95 0.57 0.70
Position Mean 2.44 2.69 1.58 1.44
SD 0.86 1.00 0.58 0.71
Table 4 P values from analysis of variance for comparison of units (1.5, 3 T), raters, and interaction between units and raters for theassessment of perceptibility of disc shape and position for left and right joints and for both joints combined
Perceptibility of Joint Comparison
Unit (1.5, 3 T) Rater Interaction
Disc shape Left <0.001** 0.135 0.133
Right <0.001** 0.588 0.56
Both <0.001** 0.16 0.159
Disc position Left <0.001** 0.149 0.005**
Right <0.001** 0.207 0.604
Both <0.001** 0.092 0.009**
**Statistically significant (multiply P values by two to obtain multiple-endpoint-adjusted figures)
1243

A statistically significant correlation between an increasedsignal on T2-weighted images in the posterior discattachment and the presence of pain has been demonstrated[29]. The more precise the detailed rendition, the higherwill be the potential for diagnosing characteristic progres-sive changes. The present study was designed to determinewhether MRI of symptomatic TMJ at a higher fieldstrength of 3.0 T as compared to 1.5 T provides for betterperceptibility of disc shape and disc position as well as forassessment of shape and signal intensity. For this purpose,comparable examination sequences were selected for bothfield strengths to identify potential benefits of the 3.0 T unitin routine clinical practice. It showed that the 3.0 T unit atthe same resolution yielded better results for perceptibilityof joint structures without increasing the time needed forthe procedure. This correlated with the results of Stehling etal. who noted a better visualization of the smaller TMJstructures at 3.0 T [19]. Improved detail delineationfacilitates diagnosis of joint pathologies and progressivechanges [5]. Precise evaluation of even small changes indisc position, shape, and signal intensity is of utmostimportance for optimum therapy planning [30]. MRI isvery useful in the control of splint therapy [31]; in this caseexact diagnosis of small changes in the disc position is veryimportant [32].
The consistency between the two raters in the assess-ment of perceptibility of position and shape was fair tomoderate. For the assessment of disc shape goodconsistency was found at both field strengths, andagreement between raters in the assessment of signalintensity of the disc was good at 1.5 T and excellent at 3.0T. Comparable results were reported by Saupe et al. who
noted a fair interobserver agreement for 1.5 T and a goodinterobserver agreement for 3.0 T in their examinations ofcadaveric wrists [33].
Some limitations of the present study should not gounmentioned. For the images with the jaw in open positionwe used a standard splint with a height of 30 mm. Thus,possible repositions in excess of 30 mm may have goneunnoted. Disc position, mobility, and condyle positionwere identical with both examiners and both fieldstrengths. However, the disc was not assessable in onepatient in the 1.5 T images, while it was in the 3.0 T imagesof the same patient. In addition, different examiners mayassess the 3.0 T images as distinctly superior to 1.5 Timages as indicated by a significant interaction betweenexaminer and unit in our study.
Another limitation is the fact that for the 3.0 T unit used,no specific TMJ coil is available. Therefore, we used asimilar surface coil as for the 1.5 T unit. This coil has notbeen optimized for TMJ examinations but was selected toensure better comparability. Likely, an optimized TMJ coilwill even further improve the perceptibility of the differentanatomical structures.
The contrast parameter deviated slightly between thetwo units as a result of the different gradient systems andthe required field-strength-related adjustments. For thesame reasons and under the premises of an essentiallysimilar contrast behavior, measuring times could also onlybe kept roughly, but not exactly, identical.
In conclusion, the 3 T unit delivers images of betterquality as regards evaluability of disc position and shape ascompared to 1.5 T MR and thus provides added diagnosticassurance that is critical for therapeutic decisions.
References
1. Farrar WB (1978) Characteristics of thecondylar path in internal derangementsof the TMJ. J Prosthet Dent 39:319–323
2. McCarty W (1980) Diagnosis andtreatment of internal derangements ofthe articular disc and mandible condyle.In: Solberg W, Clark G (eds) Tempo-romandibular joint problems. Quintes-sence, Chicago, pp 145–164
3. Clark GT (1984) A critical evaluationof orthopedic interocclusal appliancetherapy: effectiveness for specificsymptoms. J Am Dent Assoc 108:364–368
4. Limchaichana N, Nilsson H, EkbergEC, Nilner M, Petersson A (2007)Clinical diagnoses and MRI findings inpatients with TMD pain. J Oral Rehabil34:237–245
5. Katzberg RW, Tallents RH (2005)Normal and abnormal temporomandib-ular joint disc and posterior attachmentas depicted by magnetic resonanceimaging in symptomatic and asymp-tomatic subjects. J Oral MaxillofacSurg 63:1155–1161
6. Piehslinger E, Schimmerl S, Celar A,Crowley C, Imhof H (1995) Compari-son of magnetic resonance tomographywith computerized axiography in diag-nosis of temporomandibular joint dis-orders. Int J Oral Maxillofac Surg24:13–19
7. Puelacher W (1998) Funktionelle Kie-fergelenkschirurgie. In: Schroll K,Watzek G (eds) Zahnärztliche Chirur-gie, Band III. Verlag Wilhelm Maud-rich, Wien, pp 167–207
8. Sonnabend E, Benz C (1997) Rönt-gentechnik in der Zahnheilkunde.Urban & Schwarzenberg, München
9. Katzberg RW (1989) Temporomandib-ular joint imaging. Radiology 170:297–307
10. Schild H (2005) Klinische Hochfeld-MRT. Fortschr Röntgenstr 177:621–631
11. Trattnig S, Pinker K, Ba-Ssalamah A,Nöbauer-Huhmann IM (2006) The op-timal contrast agents at high field MRI.Eur Radiol 16:1280–1287
12. Glaser C, Horng A, Mendilik T,Weckbach S, Hoffmann RT, Wagner S,Raya JG, Horger W, Reiser M (2007)T2 relaxation time in patellar cartilage-global and regional reproducibility at1.5 Tesla and 3 Tesla. Rofo 179:146–152
1244

13. Wieners G, Detert J, Streitparth F, PechM, Fischbach F, Burmester G, Ricke J,Backhaus M, Bruhn H (2007) High-resolution MRI of the wrist and fingerjoints in patients with rheumatoid ar-thritis: comparison of 1.5 Tesla and 3.0Tesla. Eur Radiol 17:2176–2182
14. Lutterbey G, Behrends K, FalkenhausenMV, Wattjes MP, Morakkabati N, Gie-seke J, Schild H (2004) Is the body-coilat 3 Tesla feasable for the MRI evalua-tion of the painful knee? A comparativestudy. Eur Radiol 17:503–508
15. Eckstein F, Hudelmaier M, Wirth W,Kiefer B, Jackson R, Yu J, Eaton CB,Schneider E (2006) Double echo steadystate magnetic resonance imaging ofknee articular cartilage at 3 Tesla: apilot study for the Osteoarthritis In-itiative. Ann Rheum Dis 65:433–441
16. Weckbach S, Mendlik T, Horger W,Wagner S, Reiser MF, Glaser C (2006)Quantitative assessment of patellarcartilage volume and thickness at 3.0Tesla comparing a 3D-fast low angleshot versus a 3D-true fast imaging withsteady-state precession sequence forreproducibility. Invest Radiol 41:189–197
17. Lee KY, Masi JN, Sell CA, Schier R,Link TM, Steinbach LS, Safran M,Majumdar S (2005) Computer-aidedquantification of focal cartilage lesionsusing MRI: accuracy and initial ar-throscopic comparison. OsteoarthritisCartilage 13:728–737
18. Saupe N, Prüssmann KP, Luechinger R,Bösiger P, Marincek B, Weishaupt D(2005) MR imaging of the wrist: com-parison between 1,5- and 3-T MRimaging - preliminary experience. Ra-diology 234:256–264
19. Stehling C, Vieth V, Bachmann R,Nassenstein I, Kugel H, Kooijman H,Heindel W, Fischbach R (2007) High-resolution magnetic resonance imagingof the temporomandibular joint: imagequality at 1.5 and 3.0 Tesla in volun-teers. Invest Radiol 42:428–434
20. Diedrichs G, Bockholt R (1990) Funk-tionsstörungen des Kausystems. Eineretrospektive Studie an 1778 Patientender Westdeutschen Kieferklinik. ZWR2:96–101
21. Wilkes C (1989) Internal derangementsof the temporomandibular joint. Patho-logical variations. Arch OtolaryngolHead Neck Surg 115:469–447
22. Ozawa S, Tanne K (1997) Diagnosticaccuracy of sagittal condylar movementpatterns for identifying internal de-rangement of the temporomandibularjoint. J Orofac Pain 11:222–231
23. List T, Helkimo M, Andersson S,Carlsson GE (1992) Acupuncture andocclusal splint therapy in the treatmentof craniomandibular disorders. Part I. Acomparative study. Swed Dent J16:125–141
24. Hansson LG, Westesson PL, KatzbergRW, Tallents RH, Kurita K, Holtas,Svensson SA, Eriksson L, Johansen CC(1989) MR imaging of the temporo-mandibular joint: comparison of imagesof autopsy specimens made at 0.3 T and1.5 T with anatomic cryosections. Am JRoentgenol 152:1241–1244
25. Schmid-Schwap M, Briedl JG, Robin-son S, Piehslinger E (2005) Correlationbetween disk morphology in MRT andtime curves in electronic axiography inpatients with anterior disk displacementwith reposition. Cranio 23:1–8
26. Emshoff R, Rudisch A (2001) Validityof clinical diagnostic criteria for tempo-romandibular disorders: clinical versusmagnetic resonance imaging diagnosisof temporomandibular joint derange-ment and osteoarthrosis. Oral Surg OralMed Oral Pathol Oral Radiol Endod91:50–55
27. Rudisch A, Innerhofer K, Bertram S,Emshoff R (2001) Magnetic resonanceimaging findings of internal derange-ment and effusion in patients withunilateral temporomandibular jointpain. Oral Surg Oral Med Oral PatholOral Radiol Endod 92:566–571
28. Tognini F, Manfredini D, MontagnaniG, Bosco M (2004) Is clinical assess-ment valid for the diagnosis of tempo-romandibular disc displacement?Minerva Stomatol 53:439–448
29. Sano T, Westesson PL (1995) Internalderangement related to osteoarthrosis intemporomandibular joint. Increased T2signal in the retrodiskal tissue in painfuljoints. Oral Surg Oral Med Oral PatholOral Radiol Endod 79:511–516
30. Eberhard D, Bantleon HP, Steger W(2002) The efficacy of anterior reposi-tioning splint therapy studied by mag-netic resonance imaging. Eur J Orthodont24:343–352
31. Ohnuki T, Fukuda M, Nakata A, NagaiH, Takahashi T, Sasano T, Miyamoto Y(2006) Evaluation of the position, mo-bility and morphology of the disc byMRI before and after four differenttreatments for temporomandibular jointdisorders. Dentomaxillofac Radiol35:103–109
32. Fayed MM, El-Mangoury NH, El-Bokle DN, Belai AI (2004) Occlusalsplint therapy and magnetic resonanceimaging. World Orthodont 5:133–140
33. Saupe N, Pfirrmann CWA, SchmidMR, Schartler T, Manestar W,Weishaupt D (2007) MR imaging ofcartilage in cadaveric wrists: compari-son between imaging at 1.5 and 3.0 Tand gross pathologic inspection. Radi-ology 243:180–187
1245