diagnostic accuracy of h&e stained biopsy in ... · diagnostic accuracy of h&e stained...
TRANSCRIPT
Diagnostic Accuracy of H&E stained
Biopsy in Differentiation of
Hydatidiform Mole
Kywe Pyae Wai 1, Saw Wut Hmone 2 , Nyo Me May Thyn 3, Win Naing 4
12 ND Yr M.Med.Sc (Pathology) , Department of Pathology, UMMG
2 Department of Pathology, UM 1
3 Department of Pathology, UM 2
4 Department of Pathology, UMM
Presentation Outlines 1. INTRODUCTION
2. OBJECTIVES
3. MATERIALS AND METHODS
4. RESULTS
5. DICUSSION
6. CONCLUSION
7. RECOMMANDATION
8. REFERENCES
9. ACKNOWLEDGEMENT
14/1/2020 2
INTRODUCTION
Hydatidiform mole
Hydatidiform mole is an abnormal
gestational condition characterized by
significant hydropic enlargement and
variable trophoblastic proliferation
involving part or all of the chorionic villi
(Pirog and Ellenson, 2015).
14/1/2020 3
Histopathological diagnosis and
classification of hydatidiform mole has
become increasingly difficult because
hydatidiform moles are now commonly
evacuated at an earlier stage and do not
satisfy the well-established classic
morphological features (Romaguera et al.,
2004).
14/1/2020 4
Differentiating and classification of
complete mole and partial mole is
important for both clinical practice and
investigational studies because the risk of
choriocarcinoma is higher after complete
mole (Pirog and Ellenson, 2015).
14/1/2020 5
The differentiation between complete
mole and partial mole by this H&E
method alone is not sufficient for some
cases because of inter-observer variability
and suboptimal diagnostic reproducibility
(Romaguera et al., 2004).
14/1/2020 6
Immunohistochemistry is widely used for
confirmation of histological diagnosis
because it is effective, cheaper than other
advanced molecular techniques and with
high accuracy.
14/1/2020 7
Nowadays, the immunostaining of P57
becomes a recognized marker to adjunct the
classification of hydatidiform mole in the
absence of fascilities for genotyping.
P57 immunostaining is an in situ technique
performed on paraffin-embedded tissues and
the results are easy to interpret (Samadder
and Kar, 2015).
14/1/2020 8
The lack of P57 activity can lead to a loss
of cell cycle control, which results
abnormal proliferation and differentiation
of trophoblasts in complete mole.
Therefore, the P57 is not expressed in
complete mole and expressed in partial
mole (Luchini et al., 2016).
14/1/2020 9

The specificity of P57 is 97-100% in
complete hydatidiform mole and 93-95% in
partial hydatidiform mole (Luchini et al.,
2016).
14/1/2020 10
OBJECTIVES
General Objective
To study the diagnostic accuracy of H&E
stained biopsy in differentiation of
Hydatidiform mole
14/1/2020 11
Specific Objectives
1. To differentiate complete and partial hydatidiform mole by H&E-stained biopsy
2. To differentiate complete and partial hydatidiform mole by P57 immunohistochemical marker
3. To compare the diagnostic values of the two methods in differentiation of hydatidiform mole
14/1/2020 12
MATERIALS AND METHODS
Study Design - a cross-sectional, descriptive study.
From July, 2018 to June, 2019
Study Area
1.Gynaecological Units (MRH) and (MTH)
2. Department of Pathology, and (MTH)
3.Common Research Laboratory, UMMG
14/1/2020 13
The sample size was calculated by the
following formula
Sample size n = Z2α/2 p*(1-p*)/d2
(Daniel, 2008)
14/1/2020 14
Fifty-one cases of newly diagnosed cases
of Hydatidiform mole were included
explanation to the patients
taking informed consents
14/1/2020 15
The biopsied samples sent to the Pathology
Department were fixed in 10% buffered
formalin saline.
After adequate fixation, tissue processing
and proper paraffin wax embedding, all the
tissues sections were stained with
Hematoxylin and Eosin.
14/1/2020 16
Classification of hydatidiform mole was
done according to histological findings
under the ordinary light microscope.
Confirmed cases of hydatidiform mole
were selected and proceeded for
immunohistochemical method.
14/1/2020 17
Then paraffin wax embedded tissue blocks
were proceeded for IHC staining with P57
monoclonal antibody (Mouse monoclonal
antibody for human P57KIP2protein,
Thermoscientific Ltd) by using
Peroxidase-antiperoxidase technique.
14/1/2020 18
Dark brown to black nuclear staining of more
than 10% of villous mesenchyme and
cytotrophoblastic cells were regarded as
positive P57 immunoexpression.
Less than 10% as negative P57
immunoexpression.
14/1/2020 19
Positive control (placenta) and negative
control (without adding primary antibody)
were included in each run.
14/1/2020 20
After getting the results of H&E method
and P57 IHC method, comparison of the
diagnostic values of the two methods in
differentiation of hydatidiform mole were
done and found out the final diagnosis of
hydatidiform mole.
14/1/2020 21
Then the diagnostic accuracy of H&E
stained biopsy was determined in
comparison with P57 IHC method.
14/1/2020 22
RESULTS
0%
5%
10%
15%
20%
25%
30%
35%
under 20years 21-30years 31-40 years over 40 years
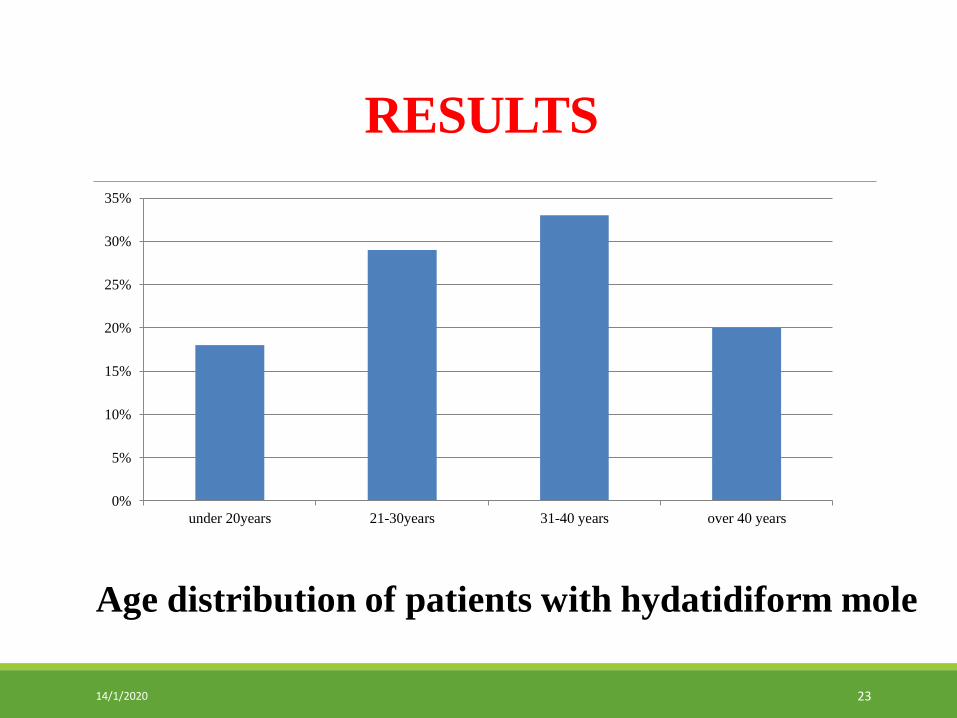
Age distribution of patients with hydatidiform mole
14/1/2020 23
H&E-stained
biopsy Number of
cases
Percentage
%
Complete mole
8 16%
Partial mole 43 84%
Total 51 100%
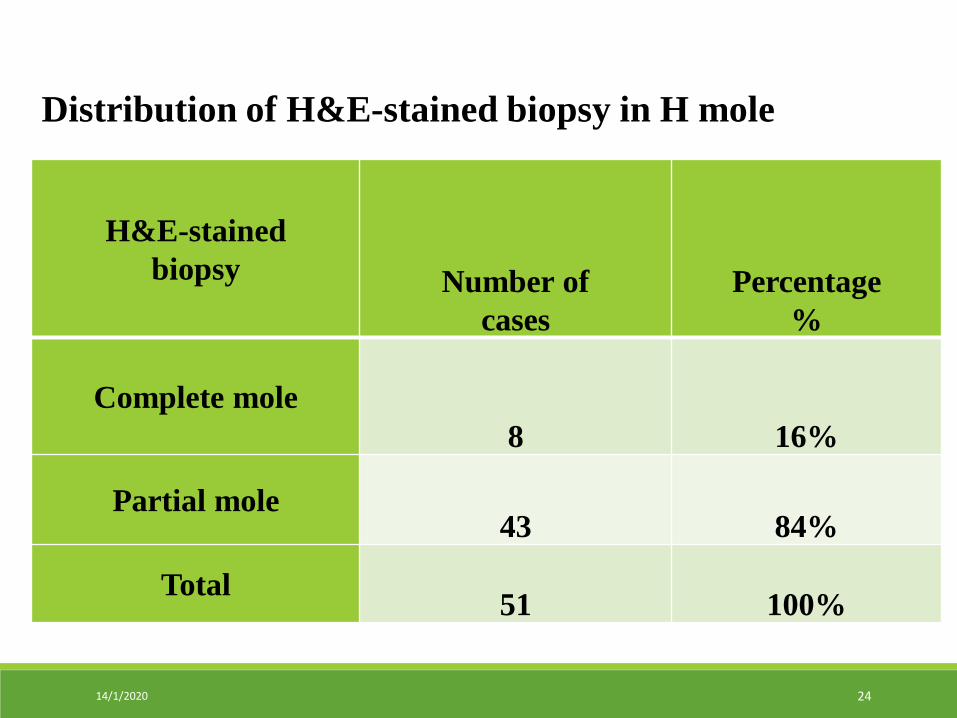
Distribution of H&E-stained biopsy in H mole
14/1/2020 24
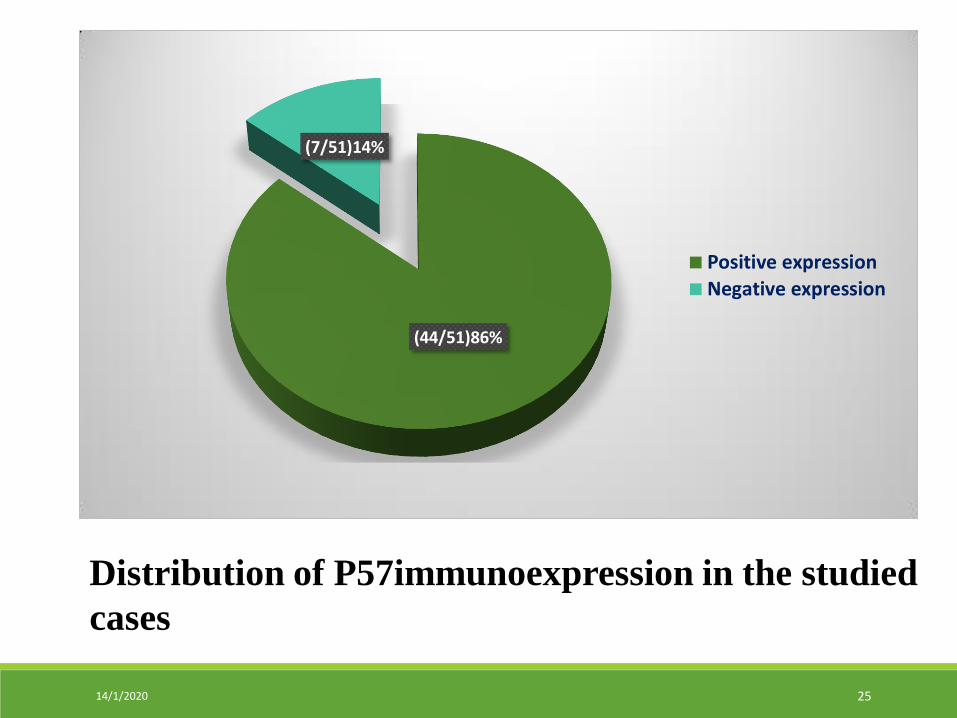
Distribution of P57immunoexpression in the studied
cases
(44/51)86%
(7/51)14%
Positive expression
Negative expression
14/1/2020 25
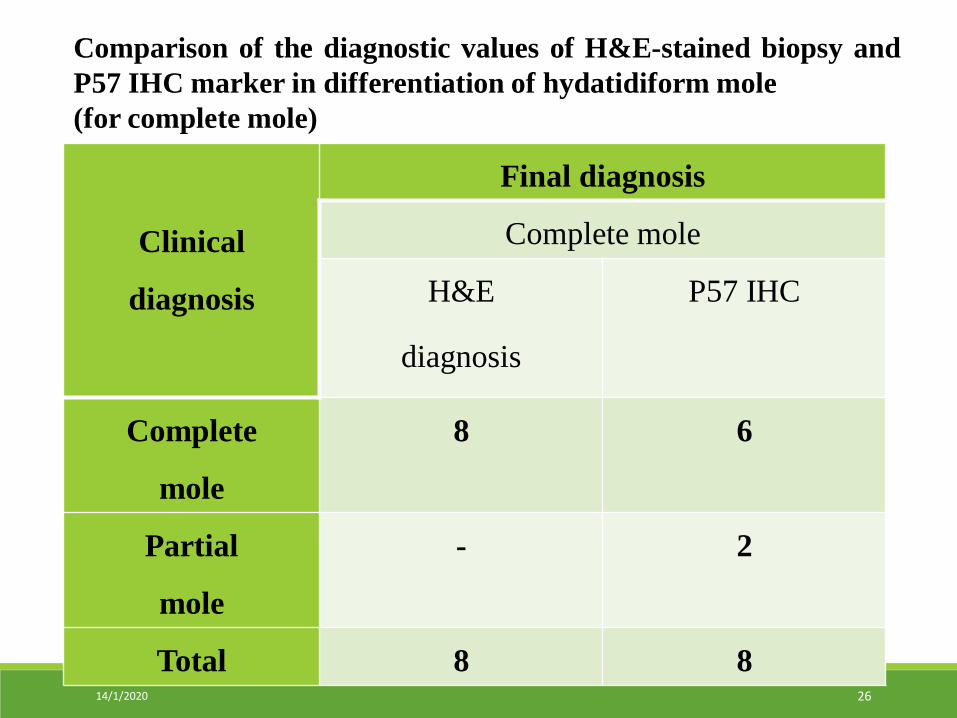
Clinical
diagnosis
Final diagnosis
Complete mole
H&E
diagnosis
P57 IHC
Complete
mole
8 6
Partial
mole
- 2
Total 8 8
Comparison of the diagnostic values of H&E-stained biopsy and
P57 IHC marker in differentiation of hydatidiform mole
(for complete mole)
14/1/2020 26

Clinical
diagnosis
Final diagnosis
Partial mole
H&E
diagnosis
P57 IHC
Complete
mole
- 1
Partial mole 43 42
Total 43 43
Comparison of the diagnostic values of H&E-stained biopsy and
P57 IHC marker in differentiation of hydatidiform mole
(for partial mole)
14/1/2020 27
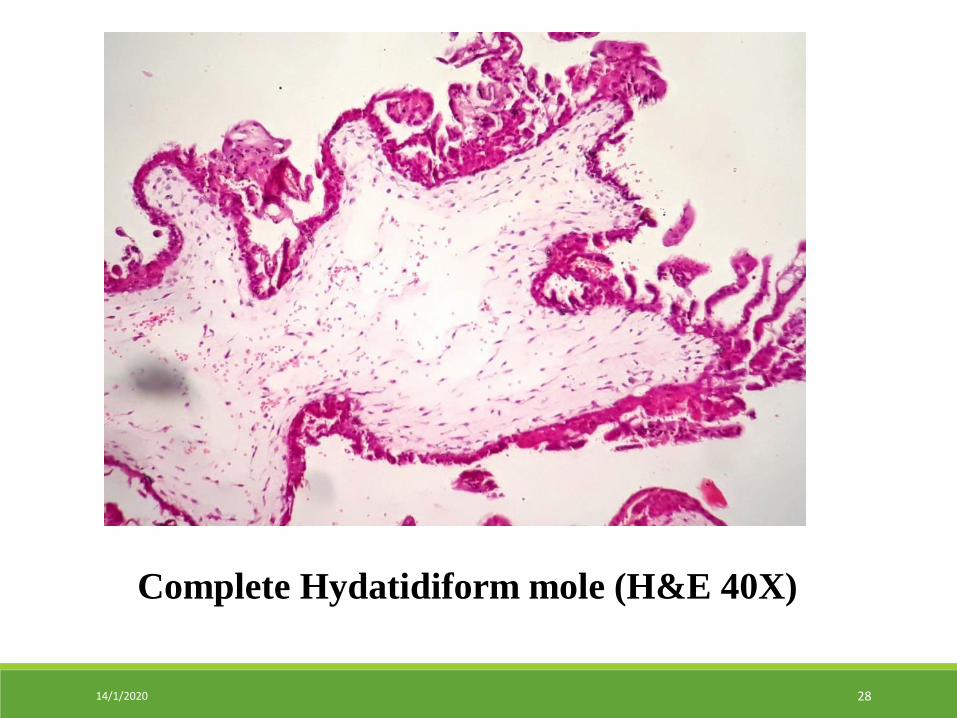
Complete Hydatidiform mole (H&E 40X)
14/1/2020 28
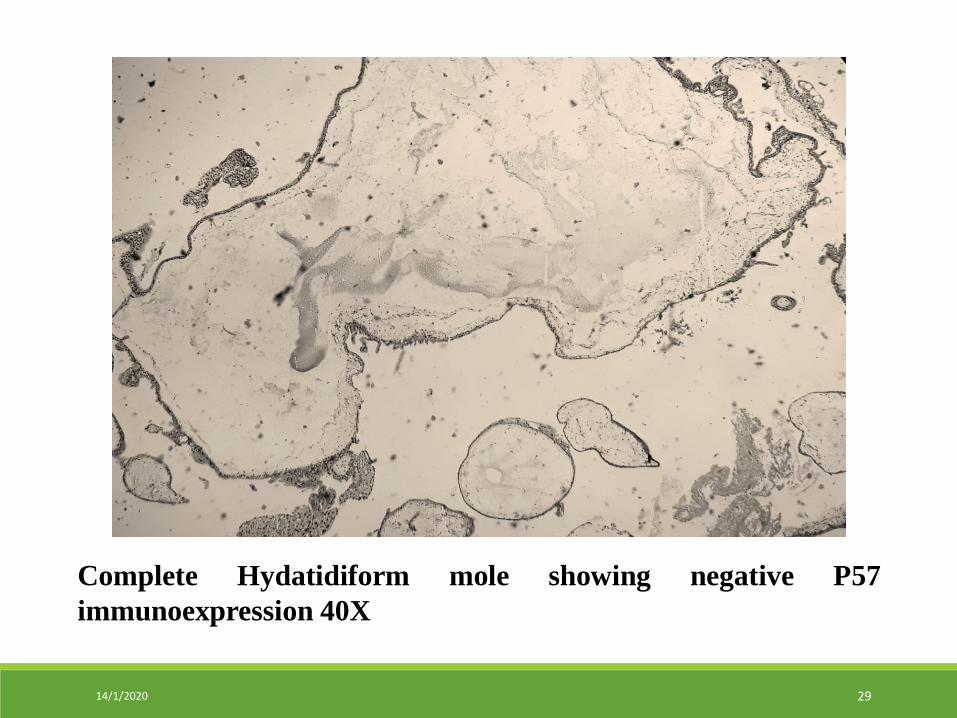
Complete Hydatidiform mole showing negative P57
immunoexpression 40X
14/1/2020 29
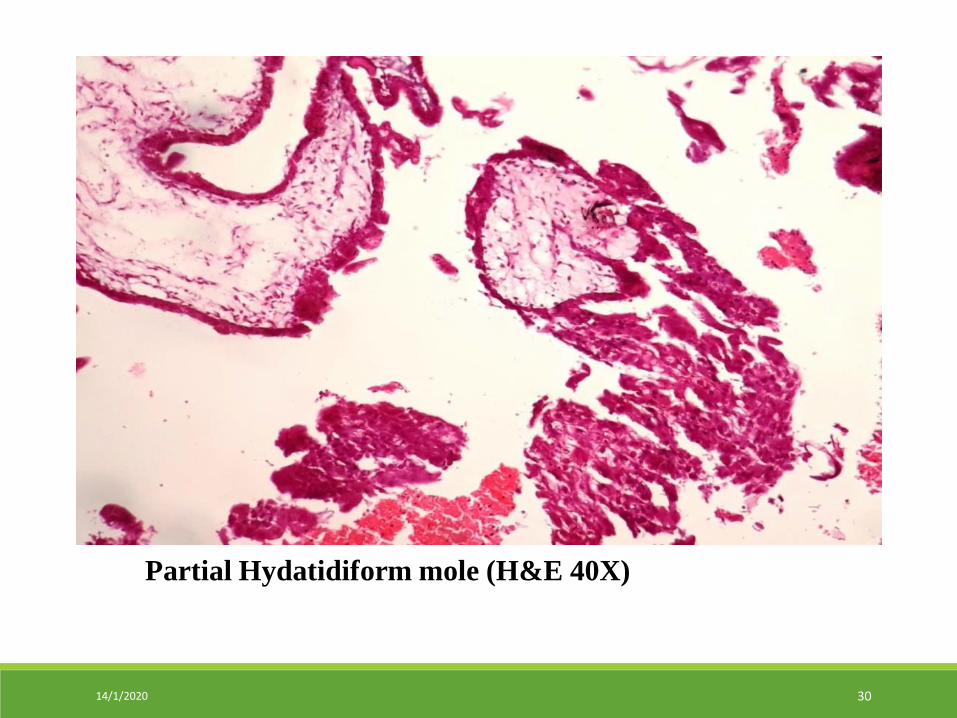
Partial Hydatidiform mole (H&E 40X)
14/1/2020 30
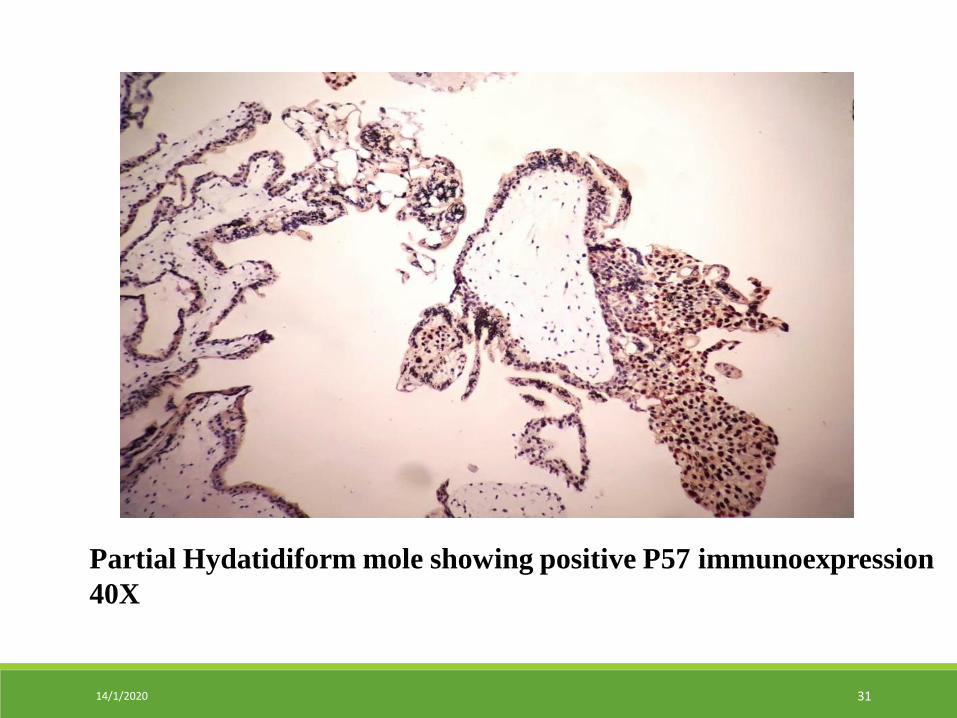
Partial Hydatidiform mole showing positive P57 immunoexpression
40X
14/1/2020 31
DICUSSION
Histological morphology yields an
accurate diagnosis in the majority of
hydatidiform mole by routine H&E
sections.
14/1/2020 32
However, sometimes making a diagnosis
can be problematic based on morphology alone, when distinguishing between complete mole and partial mole.
14/1/2020 33
P57 immunohistochemical detection of
nuclear staining of cytotrophoblasts and
villous mesenchymal cells was an effective
method for differentiation and accurate
diagnosis.
14/1/2020 34
In this study, among 51 cases of
hydatidiform mole, distribution of H&E-
stained biopsy shows 8 cases (16%) were
complete mole and 43 cases (84%) were
partial mole.
14/1/2020 35
Immunoexpression of P57 in complete
mole were 14% (7/51) and in partial mole
were 86% (44/51).
14/1/2020 36
Among 8 cases of complete mole
diagnosed by H&E staining, 6 cases were
confirmed by negative staining of P57
(75% (6/8)) but 2 cases were found to be
P57 positive, the final diagnosis became
partial mole.
14/1/2020 37
The study done by Diwa et al in 2016, P57
immunoexpression was observed in only 1
(2%) of the 54 cases diagnosed as partial
mole.
All 68 (100%) cases diagnosed as
complete mole were negative for P57
immunoexpression (Diwa et al., 2016).
14/1/2020 38
Out of 43 cases of partial mole diagnosed
by H&E staining, 42 cases were confirmed
by positive staining of P57 (98% (42/43))
but only 1 case showed P57 negative
staining and final diagnosis was found to
be a complete mole (p<0.0001).
14/1/2020 39
CONCLUSION
According to the findings in this study, P57
IHC is likely to be useful in differentiating
complete mole from partial mole.
14/1/2020 40
Therefore, P57 is a sensitive and specific
IHC marker which should be used to
differentiate complete mole and partial
mole in problematic cases.
14/1/2020 41
RECOMMANDATION
The results from the present study may
help for further studies, and prospective
study with longer study period and larger
population of patients are suggested to get
more clinically useful data.
14/1/2020 42
Furthermore, cytogenetic studies and
molecular studies on hydatidiform mole
should be introduced in Myanmar to get
better diagnosis and better management of
hydatidiform mole cases.
14/1/2020 43
REFERENCES
1. Diwa, M. H., Kim, M. A., Avila, J. M. C., Pedroza, D.G. and Michelle, A.
M. (2016) Utility of P57KIP2 and Her-2 Fluorescence in Situ
Hybridization in Differentiating Partial from CopleteHydatidiform Mole.
ACTA MEDICA PHILIPPINA.50(4), pp.318-325.
2. IHC World (2012) Introduction to IHC technique[online].Online
information Center For Immunohistochemistory. Available from
:http://www.ihcworld.com/ Introduction.hmt [Accessed on 9th June
2017].
3. Lee, C., Smith, H. O. and Kim, S. J. (2009). Epidemiology, In: Hancock,
B. W, Berkowitz, R. S, Seckl, M, Cole, L. A (eds). Gestational
trophoblastic disease 3rd ed. International Society for the study of
Trophoblastic Disease, Sheffield, pp.49-96.
14/1/2020 44
REFERENCES
4.Lelic, M., Fatusic, Z., Iijazovic, E., Ramic, S., Markovic, S.,
Alicelebic, S. (2017), Challenges in the Routine Praxis Diagnosis of
Hydatidiform Mole; a Tertiary Health Center Experience, MED
ARCH.2017 AUG; 71 (4) pp.256-260.
5. Madi, J. M, Braga, A. R., Paganella, M. P., Litvin, I. E., and
Wendland, E. M. D. R., (2016), Accuracy of p57 KIP2compared with
genotyping for the diagnosis of complete hydatidiform mole;
protocol for a systematic review and meta-analysis, Systematic
Reviews (2016) 5:169, pp 1-6.
6. Pirog, E. C. and Ellenson, L. H. (2015) Gestational Trophoblastic
Disease. In:Kumar,V., Abbas, A.K. and Aster, J.C. (eds.) Robbins
and Cotran Pathologic Basis of Disease. 9thedn. Philadelphia:
Elsevier, pp.1039-1042.
14/1/2020 45
REFERENCES
7. Romaguera, R. L, Maria, M., Rodriguez Jocelyn, H. Bruce, Zuluaga,
T.,Viciana, A., Manuel, A.Penalver and Nadji, M. (2004) Molar
Gestations and Hydropic Abortions Differentiated by P57
Immunostaining,Fetal and Pediatric Pathology, pp.1-11.
8. Rosai, J (2011) Female Reproductive System (pregnancy, trophoblastic
disease and placenta). Rosai and Ackerman’s Surgical Pathology,
10thedn. St. Louis: Mosby, pp.1639-1641.
9. Samadder, A. and Kar, R. (2015) Utility of P57 immunohistochemistry
in differentiating between complete mole, partial mole & non-molar
or hydropic abortus.Indian J Med Res 145, January 2017, pp.133-
137.
14/1/2020 46
REFERENCES
10. Su-Thandar-Han (2011) Outcome of Women who had Hydatidiform
Mole after Surgical Evacuation in Central Women's Hospital
(Yangon); M.Med.Sc (OG) Dissertaion, University of Medicine (1),
Yangon.
11. Toe-Toe-Win (2005) A study of Risk Factors for Hydatidiform Mole
in North Okkalapa General Hospital: M.Med.Sc (OG)
Dissertation,University of Medicine (2), Yangon.
12. Yi-Yi-Lwin (2014) Clinical Profile Of Hydatidiform Mole In
Teaching Hospitals Of University Of Medicine, Magway: M.Med.Sc
(OG) Dissertation,University Of Medicine, Magway.
14/1/2020 47
ACKNOWLEDGEMENT
Rector Prof Dr Htay Hla (Rector,
University of Medicine, Magway)
Prof Dr Nwe Mar Tun (Professor and
Head, Department of Obstetrics and
Gynaecology, UM1)
Department of Medical Research
(External Grant) for Financial Support
14/1/2020 48
THANK YOU VERY MUCH FOR YOUR KIND ATTENTION
? ? Any Questions
14/1/2020 49