diagnostic evaluation of the fetal face using 3 ... · diagnostic evaluation of the fetal face...
TRANSCRIPT

Diagnostic Evaluation of the Fetal Face Using3-Dimensional Ultrasound
Gladys A. Ramos, MD,* Marissa V. Ylagan, MD,* Lorene E. Romine, MD,ÞDeborah A. D’Agostini, RDMS,* and Dolores H. Pretorius, MD, FACRÞ
Abstract: Evaluation of the fetal face with 3-dimensional ultra-sound allows for evaluation of the fetal face using surface rendering,multiplanar and multislice displays. Three-dimensional ultrasoundoffers many benefits in evaluating the fetal face because it can berotated into a standard symmetrical orientation and reviewed mil-limeters by millimeters by scrolling through the volumes. Newrendering tools now allow imaging of the hard palate. Clinical ap-plications where 3-dimensional ultrasound adds value as an ad-junct to 2-dimensional ultrasound imaging that are reviewed in thispaper include cleft lip and palate, micrognathia and other profileabnormalities, metopic suture abnormalities, presence and absenceof the nasal bones, orbit abnormalities, and ear abnormalities.In addition, the literature regarding parental bonding to the fetusafter viewing 3-dimensional images of their fetuses is reviewed.
Key Words: fetal face, 3-dimensional ultrasound, fetus,cleft lip, face
(Ultrasound Quarterly 2008;24:215Y223)
LEARNING OBJECTIVES1. Demonstrate how to display a fetal face with 3-dimensional
ultrasound.2. Describe clinical applications where 3-dimensional imag-
ing is a useful adjunct to 2-dimensional ultrasound.3. Identify the literature regarding parental bonding and
3-dimensional images of the fetus.
Evaluation of the fetal face with 3-dimensional (3D) ultra-sound allows the patient and physician to see the forehead,
eyes, nose, lips, and chin in a single frontal rendered image(Fig. 1) that is easy to recognize. Pretty faces are the basisof identification of facial anomalies, both with rendered andmultiplanar imaging. Sonographers, physicians, and otherhealth care providers that perform ultrasound examinationsshould understand the techniques available to examine the fe-tal face with 3D ultrasound (3DUS) as well as 2-dimensional(2D) ultrasound. Rendered images allow the face to be dis-played as a curved structure, whereas multiplanar image dis-plays show 3 perpendicular planar images of the face thatare similar to conventional 2D imaging.
CLEFTING OF THE LIP AND PALATEFetal cleft lip and palate occur in approximately 1 per
1000 infants born in the United States.1 The accurate prenataldiagnosis of this condition can aid with the prognosis andmanagement of this condition. Characterization of the extentof clefting allows for counseling of parents and preparation fora significant anomaly. Conventional (2D ultrasound [2DUS])has been used to make initial diagnosis of cleft lips and pri-mary palate. The detection rate has been reported to rangefrom 20% to 30%.2 However, clefts of the hard or secondarypalate and of the soft palate are difficult to visualize withthis modality. Three-dimensional ultrasound has recently beenused to improve detection of cleft palate. Different renderingtechniques have been proposed to aid in the detection ofclefting particularly of the secondary palate.
PRIMARY PALATEImaging of the lips and primary palate are now com-
monly included in the evaluation of fetal anatomy performedin the midtrimester; the 2007 American Institute of Ultra-sound Medicine Guidelines now recommend that the lipbe evaluated on all fetuses. Conventional 2DUS can detectclefting involving the lips; however, shadowing and artifactcan make detection of associated clefts involving the primarypalate difficult. This is important in regard to managementbecause approximately 80% of clefts of the lip involve theprimary palate.3 Three-dimensional ultrasound has allowedfor improvements in the visualization of the primary palate.Multiplanar reconstruction has allowed for the visualizationof the face in the sagittal, axial, and coronal planes. The ren-dering mode has allowed for the visualization of the softtissues of the face and the bony alveolar ridge. Multislicereconstructions of 3D volumes display data in parallel slicessimilar to magnetic resonance imaging. This modality allows
ORIGINAL RESEARCHCME ARTICLE
Ultrasound Quarterly & Volume 24, Number 4, December 2008 215
Received for publication May 21, 2008; accepted September 7, 2008.*Clinical Fellow (Ramos and Ylagan), Ultrasound Technician (D’Agostini),
Department of Reproductive Medicine, and †Associate Clinical Professorof Radiology (Romine), Professor of Radiology (Pretorius), Departmentof Radiology, University of CaliforniaYSan Diego, San Diego, CA.
Dr Pretorius has disclosed that he received grant/research from GeneralElectric Healthcare and Philips Medical Systems and is a consultant/advisor for Philips Medical Systems.
The remaining authors have disclosed that they have no interests in orsignificant relationships with any commercial companies pertaining tothis educational activity.
All staff members in a position to control the content of this CME activity havedisclosed that they have no financial relationships with, or financialinterests in, any commercial companies pertaining to this educationalactivity.
Lippincott CME Institute, Inc, has identified and resolved all faculty andstaff conflicts of interest regarding this educational activity.
Reprints: Dolores H. Pretorius, MD, FACR, Department of Radiology,University of CaliforniaYSan Diego, 9300 Campus Point Drive, SanDiego, CA 7756 (e-mail: [email protected]).
Copyright * 2008 by Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

clear visualization of the primary palate and distinction fromthe mandible (Fig. 2).4
SECONDARY PALATEComplete evaluation of the palate including both the
primary (alveolar ridge) and the secondary palate (hard andsoft palate) is difficult. The secondary palate has 2 anatomicalcomponents: the hard palate runs posterior and horizontalfrom the alveolar ridge, whereas the soft palate continues
posteriorly and backward in a curved manner ending in theuvula.5 Isolated clefting of the secondary palate have beenreported in 25% to 80% of cases.5 Isolated clefting of eitherof the 2 components can occur. Clefting of the soft palateis easily missed prenatally and even on postnatal evaluation.Several different techniques to improve the visualization ofthese structures have been introduced including the flippedface6 and reverse face view.7
The flipped face technique allows for evaluation of thehard palate by obtaining a volume in the sagittal plane,visualizing a profile, and then flipping that profile on its head.6
The cursor dot is then placed in the palate region, and thepalate is rendered with a thin box. The image displayed is arendered axial image of the primary and secondary palate.This allows for systematic visualization of all components ofthe primary and secondary palate. In our center, we have useda modification of this technique in which the face is keptupright, and a curved thin render box is used to view the hardpalate from the inferior aspect of the maxilla (Figs. 3, 4). Theinitial volume is acquired slightly obliquely from the inferioraspect of the maxilla, pointing upward. We have successfullyimaged the hard palate using this modification that we findmore intuitive because of the upright orientation of the face.
The reverse face view technique developed by Campbellet al7 to evaluate the hard palate entails obtaining a slow 3Dsweep of a fetal profile. This is then rotated 180 degrees to acoronal view, and the volume is then scrolled from back tofront. This allows the secondary palate to be viewed in coronalplane while avoiding shadowing from the maxilla. With thistechnique, 7 cases of clefts were correctly identified; however,1 cleft of the soft palate was missed.7 This technique relies onobtaining optimal fetal profiles because oblique views did notallow for optimal visualization.
Rotten and Levaillant2 took a systematic approach on96 cases of cleft lip and palate, with the hopes of identifying
FIGURE 1. Normal fetal face at 31 weeks. Notice thenormal eyes, nose, and lips. The right forehead is obscuredby overlying placenta.
FIGURE 2. Multislice of the normalorbits, palate, and mandible at30 weeks’ gestational age. Theupper left image is a reference imageof the face in profile. Middle image,upper row, is the mandible (arrows);middle image, middle row, is theprimary palate (double arrows);right image, lower row, is the orbits(open arrows).
Ramos et al Ultrasound Quarterly & Volume 24, Number 4, December 2008
216 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

the anatomical region involved. They noted that imaging themaxilla in the axial view and the lips (anteriorly) andsecondary palate (posteriorly) in the coronal view providedthe diagnosis in 84 cases of cleft lip and palate. In 8 cases(5 of them involving the secondary palate), the diagnosis wasmissed2; 4 false-positive cases were due to artifact, mainlyfrom the maxilla.
Axial imaging of the secondary palate has been furtherinvestigated by Faure et al8 and Pilu and Segata.9 Faure et al8
conducted a prospective study in which ultrasound scans inwhich the anterior axial view of the palate was obtained, andthe 3D underside of the fetal palate was rendered. The palate,and its associated anatomical components, was visualized inall 100 cases at gestational ages ranging from 17, 22, 27, and32 weeks,8 although some patients did have to return for asecond examination. Using tomographic ultrasound imaging,Pilu and Segata9 found that acquiring a volume of the sec-
ondary palate with an angle of insonation of 45 degreesallowed for complete evaluation of the secondary palate. The45-degree insonation was thought to aid in overcoming shad-owing by the alveolar ridge when imaging the secondary pal-ate. Fifteen normal and 1 abnormal fetuses were correctlydiagnosed with this technique. This method, however, is de-pendent on optimal fetal positioning.
Evaluation of the soft palate component of the sec-ondary palate is still limited. Although reports using 3DUSto diagnose isolated soft palate clefts are described,10 there isstill difficulty in consistently imaging this area because of ar-tifact. In our experience, the false-positive rate is high mainlybecause of shadowing.
FACIAL PROFILEThe normal facial profile can be displayed with multi-
planar or rendered display (Fig. 5) by rotating the face into a
FIGURE 4. Cleft of the lip and primary and secondary palate at 19 weeks. A, Rendered image on lower right shows a cleftextending from the alveolar ridge posteriorly through the secondary (hard) palate (arrow). Upper images show upright fetalface in coronal (left) and sagittal (right) planes, both with narrow rendering box overlying palate and green region of interestviewing line slightly curved upward to follow the contour of the palate. Lower left image shows axial plane through the palate.B, Rendered image of the face clearly demonstrates accompanying cleft lip.
FIGURE 3. Evaluation of the palate. A, Normal palate at 29 weeks. Rendered image using a mixture of surface renderingand radiograph light shows both the primary (alveolar ridge, PP) and secondary (hard, HP) palate to be intact. B, Acquisitionof rendered image in A. Upright fetal face in sagittal (upper left image) and coronal (upper right) planes with narrowrendering box overlying palate. Notice that the green region of interest viewing line is curved upward slightly to follow thecontour of the palate. Lower left image shows axial plane through the palate with alveolar ridge displayed. Lower right handimage is the rendered image shown in A.
Ultrasound Quarterly & Volume 24, Number 4, December 2008 Evaluation of Fetal Face Using 3DUS
* 2008 Lippincott Williams & Wilkins 217
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
symmetrical standard orientation. Anomalies involving themandible are associated with at least 100 genetic syndromes.11
Midface hypoplasia is often seen in the setting of skeletaldysplasias such as achondroplasia (Fig. 5) and thanatophoricdysplasia.
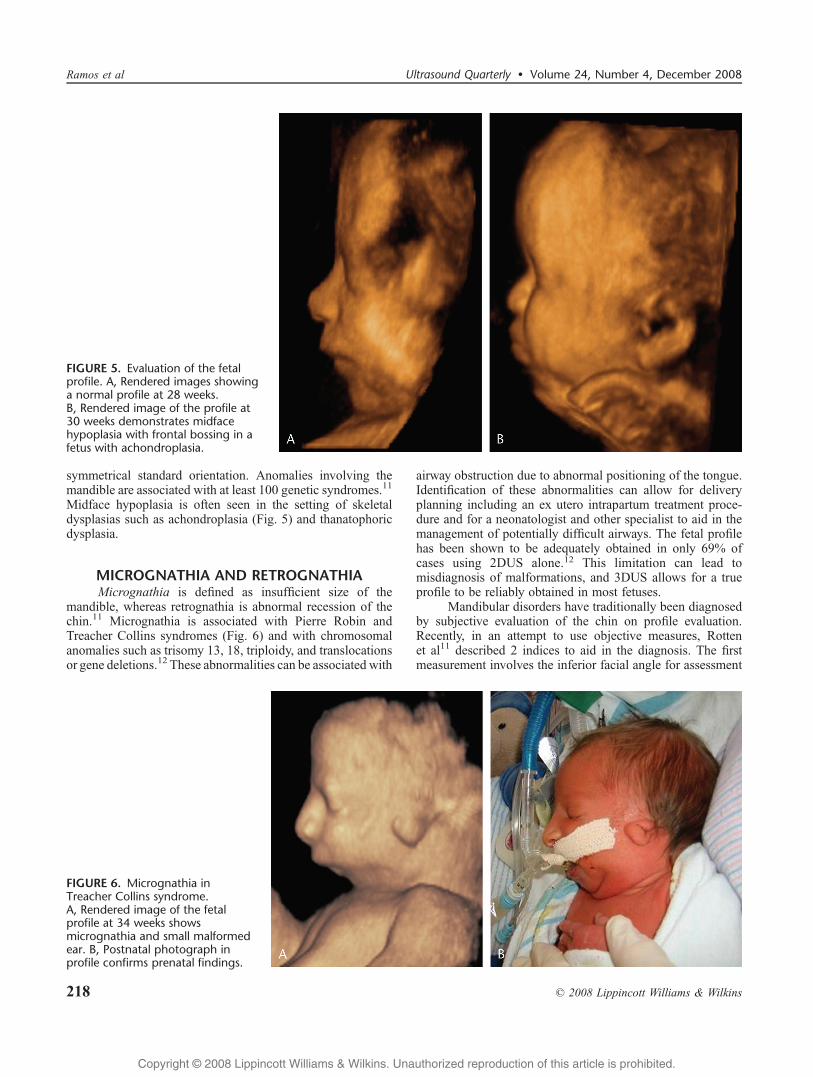
MICROGNATHIA AND RETROGNATHIAMicrognathia is defined as insufficient size of the
mandible, whereas retrognathia is abnormal recession of thechin.11 Micrognathia is associated with Pierre Robin andTreacher Collins syndromes (Fig. 6) and with chromosomalanomalies such as trisomy 13, 18, triploidy, and translocationsor gene deletions.12 These abnormalities can be associated with
airway obstruction due to abnormal positioning of the tongue.Identification of these abnormalities can allow for deliveryplanning including an ex utero intrapartum treatment proce-dure and for a neonatologist and other specialist to aid in themanagement of potentially difficult airways. The fetal profilehas been shown to be adequately obtained in only 69% ofcases using 2DUS alone.12 This limitation can lead tomisdiagnosis of malformations, and 3DUS allows for a trueprofile to be reliably obtained in most fetuses.
Mandibular disorders have traditionally been diagnosedby subjective evaluation of the chin on profile evaluation.Recently, in an attempt to use objective measures, Rottenet al11 described 2 indices to aid in the diagnosis. The firstmeasurement involves the inferior facial angle for assessment
FIGURE 5. Evaluation of the fetalprofile. A, Rendered images showinga normal profile at 28 weeks.B, Rendered image of the profile at30 weeks demonstrates midfacehypoplasia with frontal bossing in afetus with achondroplasia.
FIGURE 6. Micrognathia inTreacher Collins syndrome.A, Rendered image of the fetalprofile at 34 weeks showsmicrognathia and small malformedear. B, Postnatal photograph inprofile confirms prenatal findings.
Ramos et al Ultrasound Quarterly & Volume 24, Number 4, December 2008
218 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

of posterior displacement (retrognathia). The second is the ra-tio of mandible width to maxilla width for assessment of re-striction in size (micrognathia).11 His group found that aninferior facial angle of less than 49.2degrees (mean j 2 SDs)defined retrognathia,11 whereas a mandible width/maxillawidth ratio of less than 0.785 was diagnostic of micro-gnathia.11 Paladini et al13 introduced the measurement ofthe anteroposterior and laterolateral diameter of the mandi-ble to calculate the jaw index to diagnose micrognathia.
METOPIC SUTURESCranial sutures and fontanelles are sites of bone expan-
sion both prenatally and postnatally, allowing for progressivedevelopment of the brain and skull bones.14 Craniosynostosis,or abnormal development of the sutures and fontanelles, maybe an isolated finding but can be associated with various chro-mosomal aberrations or syndromes.15 Historically, prenatalsonographic diagnosis of craniosynostosis has been difficult,with most cases diagnosed in the first year of life.14 Conven-tional 2DUS allows for only limited evaluation of sutures andfontanelles as cross-sectional slices.14,16 Most cases of cranio-synostosis are identified because of an abnormal shape of thehead on 2DUS imaging.
Three-dimensional ultrasound has been shown to reli-ably identify most cranial sutures and fontanelles.14Y16 It isunclear, however, whether craniosynostosis will be identifiedwithout abnormal head shape by only imaging the sutures.Pretorius and Nelson16 suggested in 1994 that 3DUS could beused in evaluating the fetal cranial sutures and fontanelles.Dikkeboom et al15 demonstrated satisfactory visualization ofthe metopic, coronal, squamosal, and lambdoid sutures as wellas anterior, sphenoid, and mastoid fontanelles in 82% to100%of 120 cases. However, they noted that the sagittal suture andposterior fontanelle were more difficult to identify. They alsofound that image quality decreased with advancing gestationalage. Faro et al17 used 3DUS to describe the morphology andnormal development of the fetal frontal bone and metopicsuture between 9 and 34 weeks of gestation. In the first tri-mester, they observed that ossification of the frontal bonesoccurs in medial and lateral directions from a supraorbitalossification center. The frontal bones expand radically in thesecond trimester, delineating the metopic suture in the mid-line (Fig. 7). At approximately 32 weeks of gestation, onsetof closure of the metopic suture was observed, starting inthe supranasal region and extending superiorly toward theanterior fontanelle.
Abnormal development of the fetal metopic suture canbe associated with other fetal malformations and numerousgenetic syndromes.17,18 Several studies have used 3DUS inevaluating abnormalities of the metopic suture.18,19 Faro et al19
evaluated the metopic sutures in fetuses with holoprosence-phaly, trisomy 21, and Apert syndrome. Measurements of theheight and gap between the frontal bones were comparedbetween the abnormal and normal fetuses. Holoprosencephalywas associated with accelerated bone development andpremature closure of the metopic suture in the first trimester.20
Fetuses with Apert syndrome were noted to have a wide gapin the metopic suture (15Y23 mm) at 22 to 27 weeks of ges-
tation.21 No differences in development of the frontal bonesandmetopic sutureswere noted between trisomy 21 fetuses andhealthy fetuses in the first trimester.19 In another study, Chaouiet al18 used 3DUS to describe 4 general patterns of abnormaldevelopment of the metopic suture: V- or Y-shape, U-shape,premature closure, and presence of an additional bone. Theyobserved V-, Y-, and U-shaped metopic sutures in fetuses withfacial defects and confirmed previous reports of an associa-tion of premature closure with holoprosencephaly.
NASAL BONEThe fetal nasal bone develops from paired ossification
centers in a membrane that covers the cartilaginous nasalcapsule.22 Absence or hypoplasia of the nasal bone is asso-ciated with an increased risk of Down syndrome. Assessmentof the fetal nasal bone has been performed primarily with2DUS using the facial profile view. This technique, however, istechnically difficult and requires proficiency to obtain a perfectmidsagittal image.23
To overcome the limitations of 2DUS in evaluation ofthe fetal nasal bone, 3-dimensional multiplanar imaging wasproposed as an alternate method. With this technique, Leeet al24 identified 40% to 45% of Down syndrome fetuses in thesecond and early third trimester using absence of the nasalbone as a sonographic marker (Fig. 8). Rembouskos et al25
examined the fetal nasal bone at 11 to 14 weeks’ gestationand found that 3D multiplanar imaging does allow a perfectmidsagittal view of the fetal face to be obtained for assessmentof the nasal bone. However, they noted that the extent to whichthe nasal bone can be demonstrated in the reconstructed imageis dependent on obtaining a good initial 2D view.
FIGURE 7. Evaluation of the metopic suture at 21 weeks.Coronal skeletal-rendered image shows a normal metopicsuture, which separates the 2 frontal bones in the forehead.
Ultrasound Quarterly & Volume 24, Number 4, December 2008 Evaluation of Fetal Face Using 3DUS
* 2008 Lippincott Williams & Wilkins 219
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
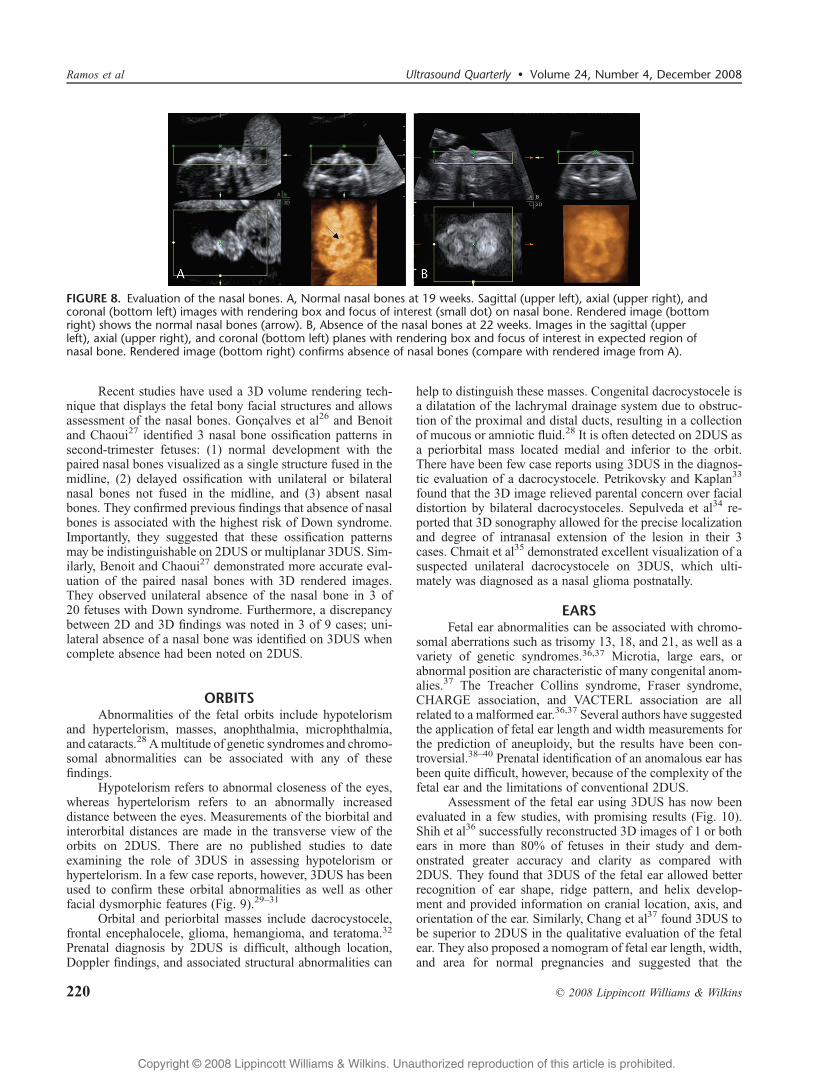
Recent studies have used a 3D volume rendering tech-nique that displays the fetal bony facial structures and allowsassessment of the nasal bones. Gon0alves et al26 and Benoitand Chaoui27 identified 3 nasal bone ossification patterns insecond-trimester fetuses: (1) normal development with thepaired nasal bones visualized as a single structure fused in themidline, (2) delayed ossification with unilateral or bilateralnasal bones not fused in the midline, and (3) absent nasalbones. They confirmed previous findings that absence of nasalbones is associated with the highest risk of Down syndrome.Importantly, they suggested that these ossification patternsmay be indistinguishable on 2DUS or multiplanar 3DUS. Sim-ilarly, Benoit and Chaoui27 demonstrated more accurate eval-uation of the paired nasal bones with 3D rendered images.They observed unilateral absence of the nasal bone in 3 of20 fetuses with Down syndrome. Furthermore, a discrepancybetween 2D and 3D findings was noted in 3 of 9 cases; uni-lateral absence of a nasal bone was identified on 3DUS whencomplete absence had been noted on 2DUS.
ORBITSAbnormalities of the fetal orbits include hypotelorism
and hypertelorism, masses, anophthalmia, microphthalmia,and cataracts.28 Amultitude of genetic syndromes and chromo-somal abnormalities can be associated with any of thesefindings.
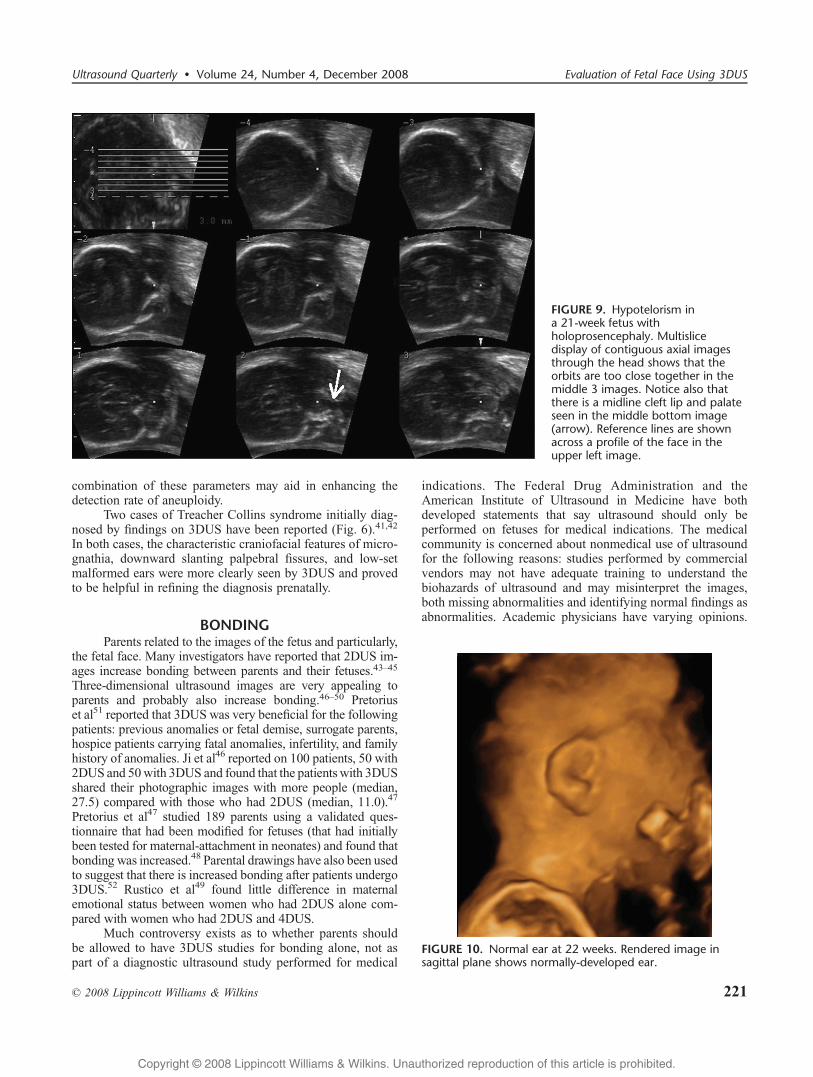
Hypotelorism refers to abnormal closeness of the eyes,whereas hypertelorism refers to an abnormally increaseddistance between the eyes. Measurements of the biorbital andinterorbital distances are made in the transverse view of theorbits on 2DUS. There are no published studies to dateexamining the role of 3DUS in assessing hypotelorism orhypertelorism. In a few case reports, however, 3DUS has beenused to confirm these orbital abnormalities as well as otherfacial dysmorphic features (Fig. 9).29Y31
Orbital and periorbital masses include dacrocystocele,frontal encephalocele, glioma, hemangioma, and teratoma.32
Prenatal diagnosis by 2DUS is difficult, although location,Doppler findings, and associated structural abnormalities can
help to distinguish these masses. Congenital dacrocystocele isa dilatation of the lachrymal drainage system due to obstruc-tion of the proximal and distal ducts, resulting in a collectionof mucous or amniotic fluid.28 It is often detected on 2DUS asa periorbital mass located medial and inferior to the orbit.There have been few case reports using 3DUS in the diagnos-tic evaluation of a dacrocystocele. Petrikovsky and Kaplan33
found that the 3D image relieved parental concern over facialdistortion by bilateral dacrocystoceles. Sepulveda et al34 re-ported that 3D sonography allowed for the precise localizationand degree of intranasal extension of the lesion in their 3cases. Chmait et al35 demonstrated excellent visualization of asuspected unilateral dacrocystocele on 3DUS, which ulti-mately was diagnosed as a nasal glioma postnatally.
EARSFetal ear abnormalities can be associated with chromo-
somal aberrations such as trisomy 13, 18, and 21, as well as avariety of genetic syndromes.36,37 Microtia, large ears, orabnormal position are characteristic of many congenital anom-alies.37 The Treacher Collins syndrome, Fraser syndrome,CHARGE association, and VACTERL association are allrelated to a malformed ear.36,37 Several authors have suggestedthe application of fetal ear length and width measurements forthe prediction of aneuploidy, but the results have been con-troversial.38Y40 Prenatal identification of an anomalous ear hasbeen quite difficult, however, because of the complexity of thefetal ear and the limitations of conventional 2DUS.
Assessment of the fetal ear using 3DUS has now beenevaluated in a few studies, with promising results (Fig. 10).Shih et al36 successfully reconstructed 3D images of 1 or bothears in more than 80% of fetuses in their study and dem-onstrated greater accuracy and clarity as compared with2DUS. They found that 3DUS of the fetal ear allowed betterrecognition of ear shape, ridge pattern, and helix develop-ment and provided information on cranial location, axis, andorientation of the ear. Similarly, Chang et al37 found 3DUS tobe superior to 2DUS in the qualitative evaluation of the fetalear. They also proposed a nomogram of fetal ear length, width,and area for normal pregnancies and suggested that the
FIGURE 8. Evaluation of the nasal bones. A, Normal nasal bones at 19 weeks. Sagittal (upper left), axial (upper right), andcoronal (bottom left) images with rendering box and focus of interest (small dot) on nasal bone. Rendered image (bottomright) shows the normal nasal bones (arrow). B, Absence of the nasal bones at 22 weeks. Images in the sagittal (upperleft), axial (upper right), and coronal (bottom left) planes with rendering box and focus of interest in expected region ofnasal bone. Rendered image (bottom right) confirms absence of nasal bones (compare with rendered image from A).
Ramos et al Ultrasound Quarterly & Volume 24, Number 4, December 2008
220 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
combination of these parameters may aid in enhancing thedetection rate of aneuploidy.
Two cases of Treacher Collins syndrome initially diag-nosed by findings on 3DUS have been reported (Fig. 6).41,42
In both cases, the characteristic craniofacial features of micro-gnathia, downward slanting palpebral fissures, and low-setmalformed ears were more clearly seen by 3DUS and provedto be helpful in refining the diagnosis prenatally.
BONDINGParents related to the images of the fetus and particularly,
the fetal face. Many investigators have reported that 2DUS im-ages increase bonding between parents and their fetuses.43Y45
Three-dimensional ultrasound images are very appealing toparents and probably also increase bonding.46Y50 Pretoriuset al51 reported that 3DUS was very beneficial for the followingpatients: previous anomalies or fetal demise, surrogate parents,hospice patients carrying fatal anomalies, infertility, and familyhistory of anomalies. Ji et al46 reported on 100 patients, 50 with2DUS and 50with 3DUS and found that the patientswith 3DUSshared their photographic images with more people (median,27.5) compared with those who had 2DUS (median, 11.0).47
Pretorius et al47 studied 189 parents using a validated ques-tionnaire that had been modified for fetuses (that had initiallybeen tested for maternal-attachment in neonates) and found thatbonding was increased.48 Parental drawings have also been usedto suggest that there is increased bonding after patients undergo3DUS.52 Rustico et al49 found little difference in maternalemotional status between women who had 2DUS alone com-pared with women who had 2DUS and 4DUS.
Much controversy exists as to whether parents shouldbe allowed to have 3DUS studies for bonding alone, not aspart of a diagnostic ultrasound study performed for medical
indications. The Federal Drug Administration and theAmerican Institute of Ultrasound in Medicine have bothdeveloped statements that say ultrasound should only beperformed on fetuses for medical indications. The medicalcommunity is concerned about nonmedical use of ultrasoundfor the following reasons: studies performed by commercialvendors may not have adequate training to understand thebiohazards of ultrasound and may misinterpret the images,both missing abnormalities and identifying normal findings asabnormalities. Academic physicians have varying opinions.
FIGURE 9. Hypotelorism ina 21-week fetus withholoprosencephaly. Multislicedisplay of contiguous axial imagesthrough the head shows that theorbits are too close together in themiddle 3 images. Notice also thatthere is a midline cleft lip and palateseen in the middle bottom image(arrow). Reference lines are shownacross a profile of the face in theupper left image.
FIGURE 10. Normal ear at 22 weeks. Rendered image insagittal plane shows normally-developed ear.
Ultrasound Quarterly & Volume 24, Number 4, December 2008 Evaluation of Fetal Face Using 3DUS
* 2008 Lippincott Williams & Wilkins 221
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Doubilet50 wrote in an editorial that many instruments beganas single-use devices and, only later, were used for manydifferent reasons (eg, computer, microscope, and camera). Hesuggests that to ban or condemn use of ultrasound forentertainment is wholly inconsistent with our acceptance ofmany other goods and services that provide enjoyment, whilecarrying a small potential risk.50
TECHNICAL POINTSCurrently in our laboratory, we perform 3-dimensional
ultrasound (3DUS) evaluation of the fetal face when it aidsin the diagnosis of a suspected anomaly on 2DUS or if it isrequested by referring physicians for diagnostic purposes. Thetiming of the evaluation is typically optimal at 22 weeks;however, with the rising rates of first trimester screening, wenow are able to perform 3DUS of the face as early as 12 weeks;in patients at risk for cleft lip and palate, we generally do ourfirst examination at 18 weeks, although we have seen ab-normal faces as early as 12 weeks. Minimum requirements toperform 3DUS, include multiplanar display, rendered display,3DUS, and 4-dimensional ultrasound (4DUS). Presets forsurface rendering and skeletal display are also used. Four-dimensional ultrasound aids in rendering and movement,whereas 3DUS allows for improved multiplanar and multislicerendering. Typically, our examinations are scheduled for 60minutes. If upon examining the fetal face we note that fetalpositioning is not optimal, we have the mother perform toetouches, walk around, or empty her bladder. If diagnosticevaluation is still not possible, we may need to rescheduleher visit.
SUMMARYThree-dimensional ultrasound has become an important
tool as an adjunct to 2DUS in the evaluation of the fetal face. Itallows for better characterization of the normal anatomy of thefetal face and has increased the diagnostic accuracy of anom-alies. Three-dimensional ultrasound can also enhance parents’understanding of the anomalies and may allow for earlierbonding with their fetuses. It is important for sonologists andsonographers to have an understanding of how to evaluate thefetal face with 3DUS.
ACKNOWLEDGMENTSThe authors thank Philips Medical Systems and General
Electric Healthcare for equipment loan. The authors alsothank Vivian Cohen for manuscript assistance.
REFERENCES1. Lee W, Kirk J, Shaheen K, et al. Fetal cleft lip and palate detection by
three-dimensional ultrasonography. Ultrasound Obstet Gynecol.2000;16:314Y320.
2. Rotten D, Levaillant J. Two- and three-dimensional sonographicassessment of the fetal face. 2. Analysis of cleft lip, alveolus and palate.Ultrasound Obstet Gynecol. 2004;24:402Y411.
3. Johnson D, Pretorius D, Budorick N, et al. Fetal lip and primary palate:three-dimensional versus two-dimensional US. Radiology. 2000;217:236Y239.
4. McGahan MC, Ramos GA, Landry C, et al. Multislice display of the fetalface using 3-dimensional ultrasonography. J Ultrasound Med. 2008;27(11):1573Y1581.
5. Campbell S. Prenatal ultrasound examination of the secondary palate.Ultrasound Obstet Gynecol. 2007;29(2):124Y127.
6. Platt L, Devore G, Pretorius D. Improving cleft palate/cleft lip antenataldiagnosis by 3-dimensional sonography: the Bflipped face[ view.J Ultrasound Med. 2006;25:1423Y1430.
7. Campbell S, Lees C, Moscoso G, et al. Ultrasound antenatal diagnosis ofcleft palate by a new technique: the 3D Breverse face[ view. UltrasoundObstet Gynecol. 2005;25:12Y18.
8. Faure J, Captier G, Baumeler M, et al. Sonographic assessment ofnormal fetal palate using three-dimensional imaging: a new technique.Ultrasound Obstet Gynecol. 2007;29:159Y165.
9. Pilu G, Segata M. A novel technique for visualization of the normaland cleft fetal secondary palate: angled insonation and three-dimensionalultrasound. Ultrasound Obstet Gynecol. 2007;29:166Y169.
10. Benacerraf B, Sadow P, Barnewolt C, et al. Cleft of the secondary palatewithout cleft lip diagnosed with three-dimensional ultrasound andmagnetic resonance imaging in a fetus with Fryns’ syndrome.Ultrasound Obstet Gynecol. 2006;27:566Y570.
11. Rotten D, Levaillant J, Martinez H, et al. The fetal mandible: a 2D and3D sonographic approach to the diagnosis of retrognathia andmicrognathia. Ultrasound Obstet Gynecol. 2002;19(2):122Y130.
12. Kurjak A, Azumendi G, Andonotopo W, et al. Three- andfour-dimensional ultrasonography for the structural and functionalevaluation of the fetal face. Am J Obstet Gynecol. 2007;196(1):16Y28.
13. Paladini D, Morra T, Teodoro A, et al. Objective diagnosis ofmicrognathia in the fetus: the jaw index. Obstet Gynecol.1999;93(3):382Y386.
14. Ginath S, Debby A, Malinger G. Demonstration of cranial sutures andfontanelles at 15 to 16 weeks of gestation: a comparison betweentwo-dimensional and three-dimensional ultrasonography. Prenat Diagn.2004;24(10):812Y815.
15. Dikkeboom C, Roelfsema N, Van Adrichem L, et al. The role ofthree-dimensional ultrasound in visualizing the fetal cranial sutures andfontanels during the second half of pregnancy. Ultrasound ObstetGynecol. 2004;24(4):412Y416.
16. Pretorius D, Nelson T. Prenatal visualization of cranial sutures andfontanelles with three-dimensional ultrasonography. J Ultrasound Med.1994;13(11):871Y876.
17. Faro C, Benoit B, Wegrzyn P, et al. Three-dimensional sonographicdescription of the fetal frontal bones and metopic suture. UltrasoundObstet Gynecol. 2005;26:618Y621.
18. Chaoui R, Levaillant J, Benoit B, et al. Three-dimensional sonographicdescription of abnormal metopic suture in second- and third-trimesterfetuses. Ultrasound Obstet Gynecol. 2005;26:761Y764.
19. Faro C, Wegrzyn P, Benoit B, et al. Metopic suture in fetuses withholoprosencephaly at 11 + 0 to 13 + 6 weeks of gestation. UltrasoundObstet Gynecol. 2006;27:162Y166.
20. Faro C, Wegrzyn P, Benoit B, et al. Metopic suture in fetuses withtrisomy 21 at 11 + 0 to 13 + 6 weeks of gestation. Ultrasound ObstetGynecol. 2006;27:286Y289.
21. Faro C, Chaoui R, Wegrzyn P, et al. Metopic suture in fetuses withApert syndrome at 22-27 weeks of gestation. Ultrasound ObstetGynecol. 2006;27:28Y33.
22. Sandikcioglu M, MLlsted K, Kjaer I. The prenatal development of thehuman nasal and vomeral bones. J Craniofac Genet Dev Biol.1994;14:124Y234.
23. Cicero S, Dezerega V, Andrade E, et al. Learning curve for sonographicexamination of the fetal nasal bone at 11Y14 weeks. Ultrasound ObstetGynecol. 2003;22:135Y137.
24. Lee W, DeVore G, Comstock C, et al. Nasal bone evaluation in fetuseswith Down syndrome during the second and third trimesters of pregnancy.J Ultrasound Med. 2003;22:55Y60.
25. Rembouskos G, Cicero S, Longo D, et al. Assessment of the fetal nasalbone at 11Y14 weeks of gestation by three-dimensional ultrasound.Ultrasound Obstet Gynecol. 2004;23:232Y236.
26. Gon0alves L, Espinoza J, Lee W, et al. Phenotypic characteristics ofabsent and hypoplastic nasal bones in fetuses with Down syndrome:description by 3-dimensional ultrasonography and clinical significance.J Ultrasound Med. 2004;23:1619Y1627.
27. Benoit B, Chaoui R. Three-dimensional ultrasound with maximal moderendering: a novel technique for the diagnosis of bilateral or unilateral
Ramos et al Ultrasound Quarterly & Volume 24, Number 4, December 2008
222 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

absence or hypoplasia of nasal bones in second-trimester screening forDown syndrome. Ultrasound Obstet Gynecol. 2005;25:19Y24.
28. Benacerraf B, Nyberg D. The face and neck. In: Nyberg D, McGahan J,Pretorius D, Pilu G, eds. Diagnostic Imaging of Fetal Anomalies.Philadelphia, PA: Lippincott Williams & Wilkins; 2003:335Y379.
29. Tonni G, Ventura A, Centini G, et al. First trimester three-dimensionaltransvaginal imaging of alobar holoprosencephaly associated withproboscis and hypotelorism (ethmocephaly) in a 46,XX fetus. CongenitAnom (Kyoto). 2008;48(1):51Y55.
30. Sase M, Hasegawa K, Honda R, et al. Ultrasonographic findings of facialdysmorphism in Wolf-Hirschhorn syndrome. Am J Perinatal.2005;22(2):99Y102.
31. Lee G, Hur S, Shin J, et al. Prenatal diagnosis of holoprosencephaly withethmocephaly via 3-dimensional sonography. J Clin Ultrasound.2006;34(6):306Y308.
32. Mernagh JR, Mohide PT, Lappalainen RE, et al. US assessment of thefetal head and neck: a state-of-the-art pictorial review. Radiographics.1999;19:S229YS241.
33. Petrikovsky B, Kaplan G. Fetal dacryocystocele: comparing 2D and 3Dimaging. Pediatr Radiol. 2003;33:582Y583.
34. Sepulveda W, Wojakowski A, Elias D, et al. Congenital dacryocystocele:prenatal 2- and 3-dimensional sonographic findings. J Ultrasound Med.2005;24:225Y230.
35. Chmait R, Pretorius D, Hull A. Nasal glioma.Ultrasound Obstet Gynecol.2002;20:417Y418.
36. Shih J, Shyu M, Lee C, et al. Antenatal depiction of the fetal ear withthree-dimensional ultrasonography. Obstet Gynecol. 1998;91:500Y505.
37. Chang C, Chang F, Yu C, et al. Fetal ear assessment and prenatal detectionof aneuploidy by the quantitative three-dimensional ultrasonography.Ultrasound Med Biol. 2000;26:743Y749.
38. Awwad J, Azar G, Karam K, et al. Ear length: a potential sonographicmarker for Down syndrome. Int J Gynecol Obstet. 1994;44:233Y238.
39. Birnholz J, Farrell E. Fetal ear length. Pediatrics. 1988;81:555Y558.40. Gill P, Vanhook J, Fitzsimmons J, et al. Fetal ear measurements in
the prenatal detection of trisomy 21. Prenat Diagn. 1994;14(8):739Y743.41. Hsu TYHJ, Chang SY, Chang MS. Prenatal three-dimensional
sonographic images associated with Treacher Collins syndrome.Ultrasound Obstet Gynecol. 2002;19(4):413Y422.
42. Tanaka YKK, Tanaka H, Yanagihara T, et al. Antenatal three-dimensionalsonographic features of Treacher Collins syndrome. Ultrasound ObstetGynecol. 2002;19(4):414Y415.
43. Whynes D. Receipt of information and women’s attitudes towardsultrasound scanning during pregnancy. Ultrasound Obstet Gynecol.2002;19(1):7Y12.
44. Zechmeister I. Foetal images: the power of visual technology in antenatalcare and the implications for women’s reproductive freedom. HealthCare Anal. 2001;9(4):387Y400.
45. Campbell S, Reading A, Coxs D, et al. Ultrasound scanning in pregnancy:the short term psychological effects of early real time scanning.J Psychosom Obstet Gyn. 1982;1:57Y61.
46. Ji E, Pretorius D, Newton R, et al. Effects of ultrasound on maternal-fetalbonding: a comparison of 2-dimensional vs. 3-dimensional imaging.Ultrasound Obstet Gynecol. 2005;25:473Y477.
47. Pretorius D, Hearon H, Hollenbach K, et al. Parental artistic drawings ofthe fetus pre and post 3 / 4 dimensional ultrasound examination.J Ultrasound Med. 2007;26:301Y308.
48. Pretorius D, Gattu S, Ji E, et al. Preexamination and postexaminationassessment of parental-fetal bonding in patients undergoing3-/4-dimensional obstetric ultrasonography. J Ultrasound Med.2006;25(11):1411Y1421.
49. Rustico MAMC, Grigio M, Maggioni C, et al. Two-dimensional vs.two- plus four-dimensional ultrasound in pregnancy and the effect onmaternal emotional status: a randomized study. Ultrasound ObstetGynecol. 2005;25(5):468Y472.
50. Doubilet P. Entertainment ultrasound. J Ultrasound Med.2005;24(2):251Y253.
51. Pretorius D, Hull A, Newton R, et al. Impact of patient initiated3-dimensional ultrasound examination. Ultrasound Obstet Gynecol.2000;16(suppl 1):94.
52. Maier B, Steiner H, Wienerroither H, et al. The psychologicalimpact of three-dimensional fetal imaging on the fetomaternalrelationship. In: Baba K, Jurkovic D, eds. Three-DimensionalUltrasound in Obstetrics and Gynecology. New York, NY:Parthenon; 1997:67Y74.
Ultrasound Quarterly & Volume 24, Number 4, December 2008 Evaluation of Fetal Face Using 3DUS
* 2008 Lippincott Williams & Wilkins 223
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.