diarrhea escmid shea course
TRANSCRIPT

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 1

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 2
¤ C.difficile: Endemic and epidemic ¤ Norovirus Epidemic ¤ Rare:
² Hospital kitchen / visitors ² Salmonella
² Listeria in immunocompromised host (cheese, milk)
² Water supply ² Cryptosporidiosis ² EHEC (tropical countries)
Rupnik M, Widmer A, et al. J Clin Microbiol. 2008 Jun;46(6):2146.
4 6 12 24 36 48 72 hrs 5 7 14 18 21 Tage
S.aureus B.cereus EHEC / ETEC Toxin Salmonellen
Clostridium perfringens Vibrio cholerae Listerien Shigellen Rotavirus Norovirus Campylobacter C.difficile Cyclospora cayetanensis Cryptosporidien Giardia lamblia Listerien /Typhus E.histolytica /Aeromonas

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 3
¤ C. difficile is a gram-‐posiCve, spore-‐forming, obligate anaerobic bacillus that is found in a variety of environmental niche.
¤ Toxigenic (toxin-‐producing) forms of the bacillus are pathogenic for humans.
¤ Spores are very resilient to heat and desiccaCon and can remain viable in the hospital environment for weeks to years.
¤ CDI can range from mild diarrhea, defined as three or more loose stools (those that take the shape of the container) within a 24-‐hour period, to severe life-‐threatening disease . ² Severe forms such as pseudomembranous coliCs, can cause
dehydraCon and tremendous discomfort for the paCent. ² Rarely, toxic megacolon,
² bowel mucosa becomes so inflamed that peristalsis stops, fecal impacCon occurs, and emergent surgery, including colectomy, is required.
ESCMID-SHEA course 2013 24-09-13
Andreas Voss 4
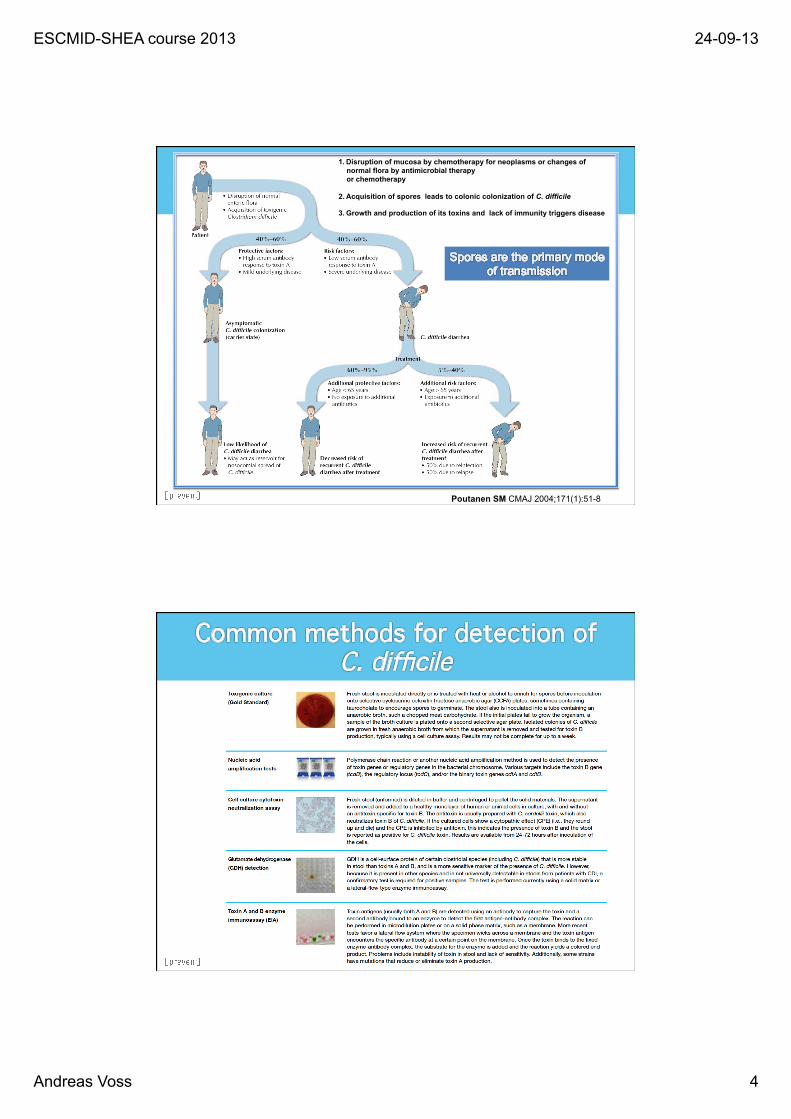
Poutanen SM CMAJ 2004;171(1):51-8
1. Disruption of mucosa by chemotherapy for neoplasms or changes of normal flora by antimicrobial therapy or chemotherapy
2. Acquisition of spores leads to colonic colonization of C. difficile
3. Growth and production of its toxins and lack of immunity triggers disease

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 5
negative
C. difficile toxin A/B
C. difficile antigen not detected.
C. difficile antigen detected.
C. difficile toxin A/B detected.
C. difficile antigen detected.
C. difficile toxin A/B not detected.
positive C. difficile specific antigen
Interpretation: Absence of C. difficile. No further testing (87.3%)
Interpretation: Toxin-producing C. difficile (4.7%) Interpretation: Non-toxin (1.4%) or toxin-
producing C.difficile (3.3%) or false-positive antigen result (2.7%). Culture should be performed (Called toxigenic culture by repeating toxin test from pos.culture)
Stool specimen for C. difficile testing (n=1,468 consecutive stool samples)
L. Fenner, Widmer AF, Frei R.. J.Clin Microbiol. 2008;46:328-330
positive negative negative
Resultats in <1 hours.
¤ DetecCon of Toxin B, binary Toxin → Typical for 078 plus tcdC-‐DeleCon → NAP1 / PCR Ribotyp 027
I use a “home-‐made” PCR

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 6
Lessa, et al. Clin Infect Dis 2012
2008

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 7
5,77,3 8,2
12,2
16
23,7
0
5
10
15
20
25
1999 2000 2001 2002 2003 2004
Emerg Infect Dis 2007,13:1417-9
per m
illio
n po
pula
tion
www.statistics.gov.uk
ESCMID-SHEA course 2013 24-09-13
Andreas Voss 8
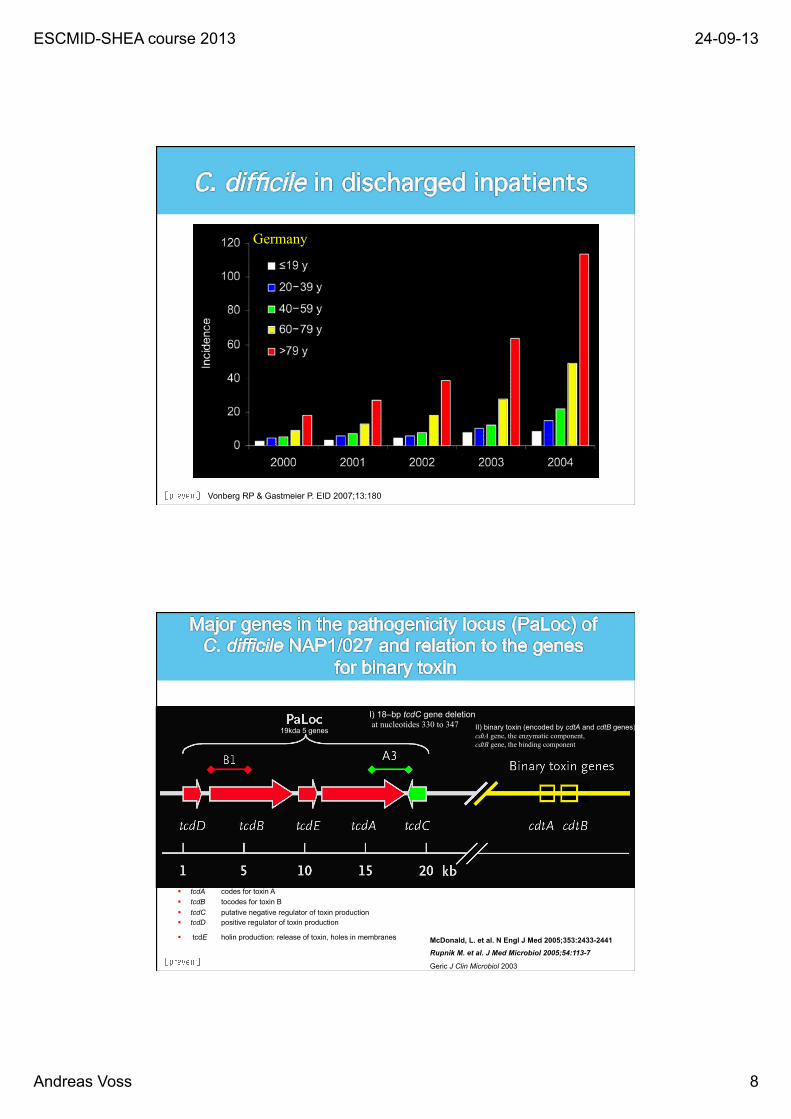
Vonberg RP & Gastmeier P. EID 2007;13:180
Germany
McDonald, L. et al. N Engl J Med 2005;353:2433-2441 Rupnik M. et al. J Med Microbiol 2005;54:113-7
Geric J Clin Microbiol 2003
I) 18–bp tcdC gene deletion at nucleotides 330 to 347 II) binary toxin (encoded by cdtA and cdtB genes)
cdtA gene, the enzymatic component, cdtB gene, the binding component
§ tcdA codes for toxin A § tcdB tocodes for toxin B § tcdC putative negative regulator of toxin production § tcdD positive regulator of toxin production
§ tcdE holin production: release of toxin, holes in membranes
19kda 5 genes

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 9
CDC rapport 2013
¤ Recent anCbioCc exposure
¤ Prolonged length of stay in healthcare facility
¤ Increasing age
¤ Serious underlying illness
¤ Proton pump inhibitors

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 10

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 11
Strength of Recommendation
Hand Hygiene A-II
Contact Precautions a. Glove use b. Gowns
A-I B-III
Private Room or Cohorting C-III
Environmental cleaning, disinfection, or use of disposables a. Disinfect patient rooms and surfaces b. Disinfect equipment between patient use c. Eliminate use of rectal thermometers d. Use of hypochlorite (1000 ppm) for disinfection
B-II C-III B-II B-II
SHEA-CDC-Guideline 2010 (SHEA Guidelines committee (Widmer AF).

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 12

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 13
Culture-negative Patient in
Room for >48h
Asymptomatc CD Patient Carrier in
Room
Patient with CD Diarrhea
in Room 7/88 (8%)
11/38 (29%)
44/90 (49%)
McFarland et al NEJM 1989;320:204

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 14
Riggs MM, et al. Clin Infect dis 2007;45: 992
C.difficile_CID_08 Bobulsky GS et al, Clin Infect Dis 2008;46:447-450
C Of note, the patient had showered 1 h before collection of the culture specimen.
Frequency of acquisition on sterile gloves after contact with skin sites of a
subset of 10 patients
Frequency of Clostridium difficile contamination of skin sites of 27 patients with C. difficile-associated disease (CDAD)

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 15
Shaughnessy et al, ICHE 2011
Intervention Reduction of initial contamination or Incidence of CDAD
References
Unbuffered hypochlorite (500 ppm) Phosphate buffered hypochlorite (1600 ppm pH 7,6)
5 X 100 X
Kaatz, Am J Epidemiol 1988
Unbuffered 1:10 hypochlorite solutions
Before 8.6/1000 pt-d After 3.3/1000 pt-d
Mayfield, CID 2000
Diluted aldehyde-containing disinfectant + other infection control measures
4 X p=0.04 Before 1.5/1000 adm After 0.3/1000 adm
Struelens, Am J Med 1991
Cases with C.difficile:
Disinfection with an active disinfectant against spores necessary
No gluoprotamin (Incidine®) No Quats. No Amines Widmer AF & Frei R.. Infect Control Hosp Epidemiol Nov 2003 Widmer AF & Frei R. Disinfection. Manual of Clinical Microbiology, ASM 2007 /2011

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 16
(gray bars; June 2004 through March 2005) and the intervention period (red bars; June 2005 through March 2006)
Boyce JM et al. ICHE 2008;29:723-9
Inte
rven
tion
perio
d
Inte
rven
tion
perio
d
Inte
rven
tion
perio
d
Inte
rven
tion
perio
d
Inte
rven
tion
perio
d
… in-‐vitro virology versus in-‐vivo infec/on control

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 17
¤ Pro and contra wash ² + Physically removes bacteria and spores ² + effecCve based on good studies ² -‐ Less effecCve against vegetaCve bacteria ² -‐ Poor compliance / Cme consuming
¤ Pro and contra Alcohol ² -‐ No acCvity against spores ² + Enhanced compliance ² + No evidence that washing stops epidemics faster Wash han
ds if vis
ibly soi
led – in
all oth
er case
s just ru
b
Mermel et al, Jt Comm J Qual Patient Saf 2013

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 18
¤ Pre intervenCon ¤ EducaCon & report outcome measures; monitor room cleaning ¤ EducaCon and bleach product use for room cleaning ¤ C. difficile detecCon by PCR ¤ AddiConal cleaning personnel and defined cleaning responsibiliCes ¤ Equipment-‐cleaning training and monitoring.
¤ Enhance discharge room cleaning
¤ Assess need for more housekeeper FTEs to adequately clean rooms
¤ Monitor compliance, report back to Environmental Services unit, infecCon control and hospital administraCon
¤ Single-‐use devices for isolaCon rooms ² blood pressure cuff, thermometer, stethoscope in all isolaCon rooms
² Monitor compliance
¤ Review policies for cleaning of portable equipment ² determine who is responsible for maintaining cleaning and supplies
used for cleaning

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 19
Personal protecCve equipment for isolaCon rooms readily available (gowns, gloves, masks as needed) -‐Easily accessible and readily available -‐Appropriate sizes -‐Easily accessible, frequently empCed hamper bins -‐Monitor compliance and report back to unit, infecCon control and hospital administraCon Robust anCbioCc stewardship program for all hospital units -‐Regularly scheduled prospecCve audits of anCbioCc uClizaCon with direct interacCon and feedback to prescriber -‐Formulary restricCon and pre-‐authorizaCon requirements -‐EducaCon of prescribers
v Develop evidence-‐based pracCce guidelines and incorporate into physician order entry system based on naConal guidelines, local microbiology and hospital anCmicrobial resistance paeerns
v Assist in streamlining, or de-‐escalaCng empiric anCbioCc therapy based on culture results, eliminaCng redundant combinaCon therapy (done in ICUs)
v OpCmizing anCmicrobial dosing based on individual paCent characterisCcs, causaCve organism, site of infecCon, and pharmacokineCc and pharmacodynamic characterisCcs of prescribed drug (done in ICUs)
v Assist in IV to oral conversion of anCbioCcs by developing clinical criteria and guidelines promoCng conversion to use of oral agents (done in ICUs)

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 20
v Audit anCbioCc class and specific anCbioCc use over Cme and report data to CMO
v Assist in narrow spectrum anCbioCc use v Limit quinolone & clindamycin use (done in surgery only) v Monitor process and outcome data, report to infecCon
control, QA, and hospital administraCon v Develop a program to determine paCents at high risk for C.
difficile and automate orders for isolaCon precauCons and C. difficile tesCng along with automated noCficaCon of physician and nursing team caring for individual paCents
v Empower nurses to order C. difficile toxin assay on paCent’s with diarrhea without a doctor’s order
v Improved sensiCvity of C. difficile tesCng and increase frequency of tesCng done by microbiology laboratory
v Develop a medical/surgical guideline for C. difficile management v Incorporate into physician order entry system v Monitor compliance & outcome data, report
v Develop medical/surgical rapid response team for severe C. difficile management v Monitor outcome data, report
v Consider expanding isolaCon precauCons for pts with C. difficile infecCon for duraCon of hospitalizaCon

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 21
Equipment Cleaning Chart
Equipment / Item LocaCon Frequency Responsibility Daily Room Cleaning Product
Daily IsolaCon Room Cleaning
Product Discharge Room Cleaning Product Monitoring
Automated external defibrillator (a@er use)
Units & hospital-‐wide As needed CSD* Disinfectant wipes N/A N/A CSD
Bathroom PaCent room Daily & discharge EVS† Dimension 11 Dispatch disinfectant
Dispatch disinfectant EVS
Bed/chair alarm PaCent room Daily & discharge EVS Dimension 11 Dispatch disinfectant
Dispatch disinfectant Nursing
Beds (remains in room) PaCent room Daily & discharge EVS Dimension 11 Dispatch
disinfectant Dispatch
disinfectant EVS
Bedside and overbed table PaCent room Daily & discharge EVS Dimension 11 Dispatch
disinfectant Dispatch
disinfectant EVS
Blood pressure cuffs in the room PaCent room Daily & discharge Nursing Dimension 11 Dispatch
disinfectant Dispatch
disinfectant Nursing
Call bell/control PaCent room Daily & discharge EVS Dimension 11 Dispatch disinfectant
Dispatch disinfectant Nursing
Cardiac monitors telemetry & lead
wire PaCent room Daily & discharge Nursing Disinfectant wipes Disinfectant wipes Disinfectant wipes Nursing
Chair scale PaCent room Amer use & between
paCents or send to CSD
Nursing Disinfectant wipes Disinfectant wipes N/A Nursing
Commode PaCent room Amer use & Between PaCents
Nursing Dispatch disinfectant
Dispatch disinfectant Nursing
Computer PaCent room Daily & as needed Nursing Disinfectant wipes Disinfectant wipes N/A EVS
Computer in nurses’ sta/on
Nursing staCon
Daily & as needed Unit secretary Disinfectant wipes Disinfectant wipes N/A Nursing
Computer on wheels Unit Daily & as needed Nursing Disinfectant wipes Disinfectant wipes N/A Nursing
Cooling Blanket PaCent room Amer use & between
paCents or send to CSD
Nursing Disinfectant wipes Disinfectant wipes Return to CSD Nursing
Con/nuous passive mo/on machine for
knee PaCent room
Amer use & between paCents
Nursing Disinfectant wipes Disinfectant wipes Return to CSD Nursing
Reduce “floaCng” responsibiliCes
EM Norovirus

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 22
¤ Short incubaCon (15–48 h) ¤ Illness duraCon 12–60 h ¤ VomiCng in > 50% symptomaCc paCents ¤ PaCents and staff both affected ¤ No bacterial pathogen in stool culture
Management of hospital outbreaks of gastro-enteritis due to small round structured viruses. REPORT OF THE PUBLIC HEALTH LABORATORY SERVICE VIRAL GASTRO ENTERITIS WORKING GROUP J. Hosp Infect 2000

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 23
Turcios RM. Clinical Infectious Diseases 2006; 42:964–9
Type Year Level of Detection
Sensitivity
Specificity
EM 1972 ~ 106-7 ? ?
Antigen detection ELISA
IDEIA NLV kit Dako Cytomation, Ltd. (Ely, UK), SRSV(II)-AD kit Denka Seiken Co., Ltd. (Tokyo, Japan), RIDASCREEN norovirus (R-Biopharm AG, Darmstadt,Germany
1995 104-6 60-80% 60-80%
RT-PCR 1992 ~ 102-4 90% 99%
Immuno-PCR 2005 ~ 101-3 >95% 99%
Culture 7/2005 ? Asanaka M. PNASJuly 19,
2005;102:10327–10332
? ?
Glass et al, JID 2000;181 (Suppl 2):256 Okitsu-Negishi S. JJ. Clin Microbiol Oct. 2006, p. 3784–3786 De Bruin. J Virol Meth 2006; 137, November 2006, Pages 259-264

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 24
Burton-MacLeod JA. J Clin Microbiol 2004;42:2587–2595 Okitsu-Negishi S. JJ. Clin Microbiol Oct. 2006, p. 3784–3786
RIDA GI 50% NA Screen GII 84% NA
Both 76% 95% 90%
JID 2000;181 (Suppl 2):259
Other 3%
Oyster consumption
6% Vacation settings (including cruise ships) 11%
Schools and day care centers 11%
Restaurants and catered meals 26%
Nursing homes and hospitals 43%
Settings and presumptive modes of transmission for 90 outbreaks of gastroenteritis in the United States, January 1996 to June 1997

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 25
JID 2000;181 (Suppl 2):259
No data 43%
Foodborne 21%
Unknown 16%
Waterborne 3%
Oyster consumption 6%
Person-to-person 11%
Settings and presumptive modes of transmission for 90 outbreaks of gastroenteritis in the United States, January 1996 to June 1997
Viral Shedding (via RT-‐PCR):
¤ Day 1 78% ¤ Day 8 45% ¤ Day 15 35% ¤ Day 22 26%
B Rockx; Clin Infect Dis 2002, 35: 246-53
ESCMID-SHEA course 2013 24-09-13
Andreas Voss 26
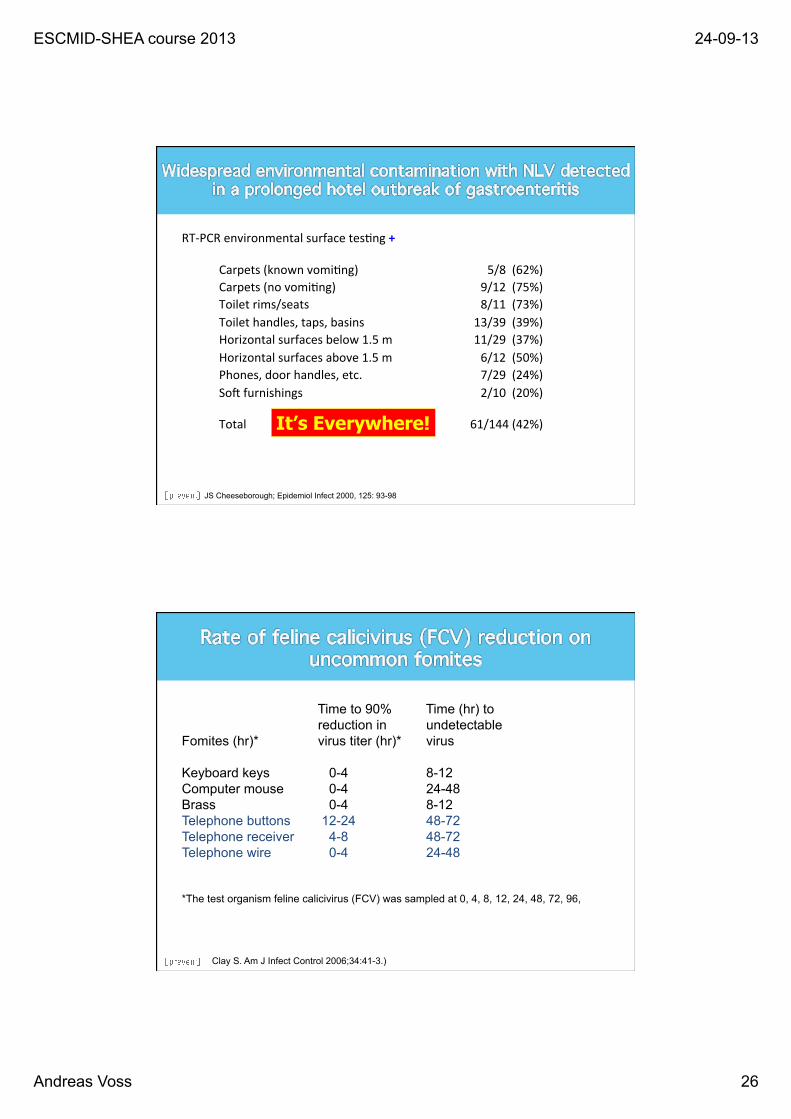
RT-‐PCR environmental surface tesCng +
Carpets (known vomiCng) 5/8 (62%) Carpets (no vomiCng) 9/12 (75%) Toilet rims/seats 8/11 (73%) Toilet handles, taps, basins 13/39 (39%) Horizontal surfaces below 1.5 m 11/29 (37%) Horizontal surfaces above 1.5 m 6/12 (50%) Phones, door handles, etc. 7/29 (24%) Som furnishings 2/10 (20%) Total 61/144 (42%) It’s Everywhere!
JS Cheeseborough; Epidemiol Infect 2000, 125: 93-98
Time to 90% Time (hr) to reduction in undetectable
Fomites (hr)* virus titer (hr)* virus Keyboard keys 0-4 8-12 Computer mouse 0-4 24-48 Brass 0-4 8-12 Telephone buttons 12-24 48-72 Telephone receiver 4-8 48-72 Telephone wire 0-4 24-48
*The test organism feline calicivirus (FCV) was sampled at 0, 4, 8, 12, 24, 48, 72, 96,
Clay S. Am J Infect Control 2006;34:41-3.)

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 27
Hos
pita
l Epi
info
rmed
No
adm
issi
on to
war
d x
Norovirus Epidemic Dec 2002
0 2 4 6 8
10 12 14 16 18
8.11
10.1
1 12
.11
14.1
1 16
.11
18.1
1 20
.11
22.1
1 24
.11
26.1
1 28
.11
30.1
1 2.
12
4.12
6.12
8.12
10.1
2 12
.12
14.1
2 16
.12
18.1
2 20
.12
22.1
2 24
.12
26.1
2 28
.12
30.1
2
Inci
denc
e
Personal Patienten
>100 HCWs working days lost
Norovirus outbreaks: Always patients & HCWs
Khanna N & Widmer AF. J Hosp Infection 2003
¤ Cohort nurse or isolate symptomaCc individuals (Category II) ¤ Wear gloves and apron for contact with
an affected paCent or environment always when entering the pa/ent room wearing a mask (Category II)
¤ Wash hands with soap and water amer contact with an affected paCent or environment, amer removing gloves and apron Use an alcoholic hand-‐rub containing >95% Ethanol, unless hands are visibly soiled (Category I)
¤ Remove exposed food such as fruit (No Category)
¤ Consider use of anCemeCcs for paCents with vomiCng (No Category)
¤ Exclude affected staff from the ward immediately and unCl 48 h symptom-‐free unCl 24hrs symptom-‐free (Category II)
¤ Close the ward to prevent the introducCon of new suscepCbles.
¤ Avoid transfer to unaffected wards or departments (unless medically urgent and amer consultaCon with infecCon control staff). The priority is to stop spread of the virus to other areas (Category II).
¤ Exclude non-‐essenCal personnel from the ward (Category II)
Chadwick Journal of Hospital Infection (2000) 45: 1–10
ESCMID-SHEA course 2013 24-09-13
Andreas Voss 28
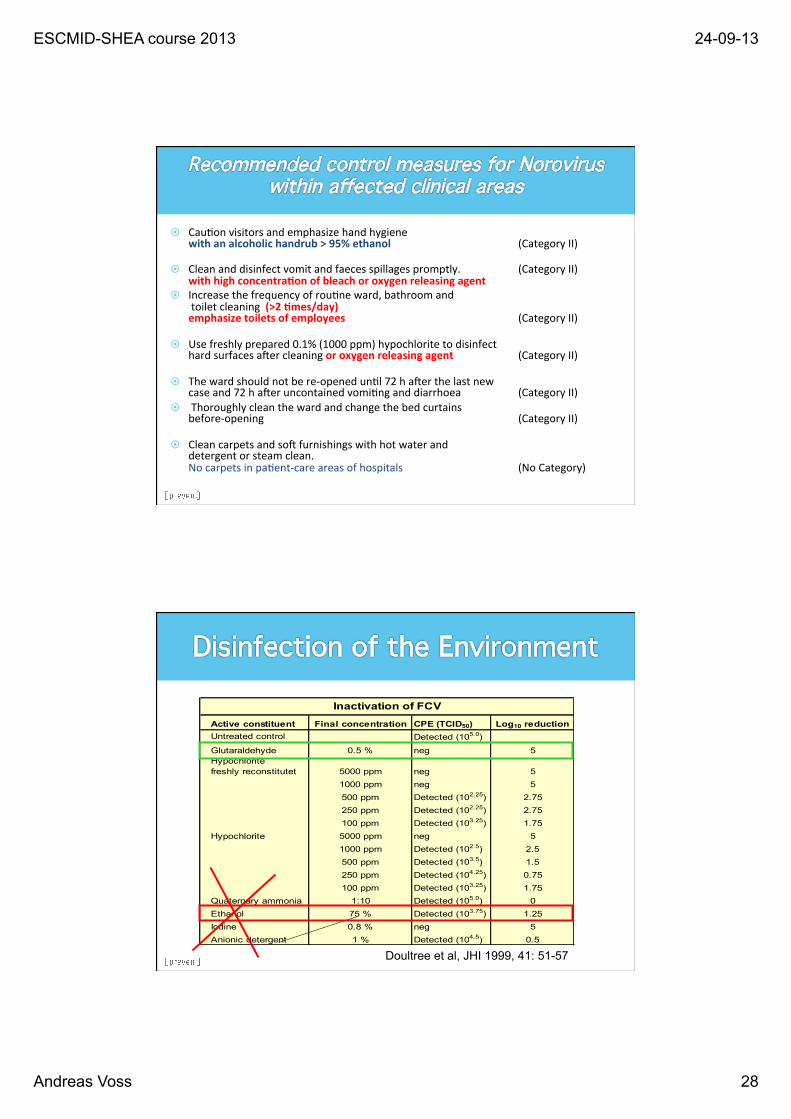
¤ CauCon visitors and emphasize hand hygiene with an alcoholic handrub > 95% ethanol (Category II)
¤ Clean and disinfect vomit and faeces spillages promptly. (Category II) with high concentra/on of bleach or oxygen releasing agent
¤ Increase the frequency of rouCne ward, bathroom and toilet cleaning (>2 /mes/day) emphasize toilets of employees (Category II)
¤ Use freshly prepared 0.1% (1000 ppm) hypochlorite to disinfect hard surfaces amer cleaning or oxygen releasing agent (Category II)
¤ The ward should not be re-‐opened unCl 72 h amer the last new case and 72 h amer uncontained vomiCng and diarrhoea (Category II)
¤ Thoroughly clean the ward and change the bed curtains before-‐opening (Category II)
¤ Clean carpets and som furnishings with hot water and detergent or steam clean. No carpets in paCent-‐care areas of hospitals (No Category)
Chadwick Journal of Hospital Infection (2000) 45: 1–10 Khanna & Widmer : J Hosp Infect 2003
Active constituent Final concentration CPE (TCID50) Log10 reductionUntreated control Detected (105.0)
Glutaraldehyde 0.5 % neg 5Hypochloritefreshly reconstitutet 5000 ppm neg 5
1000 ppm neg 5500 ppm Detected (102.25) 2.75250 ppm Detected (102.25) 2.75100 ppm Detected (103.25) 1.75
Hypochlorite 5000 ppm neg 51000 ppm Detected (102.5) 2.5500 ppm Detected (103.5) 1.5250 ppm Detected (104.25) 0.75100 ppm Detected (103.25) 1.75
Quaternary ammonia 1:10 Detected (105.0) 0Ethanol 75 % Detected (103.75) 1.25Iodine 0.8 % neg 5Anionic detergent 1 % Detected (104.5) 0.5
Inactivation of FCV
Doultree et al, JHI 1999, 41: 51-57

ESCMID-SHEA course 2013 24-09-13
Andreas Voss 29
Präparat Amphisept E Sterillium Virugard Sterillium Sterillium pure
Wirksamkeit
bakterizid, fungizid, tuberkulozid,
HBV/HIV, BVDV, Herpes, Rota,
Adeno, Vaccinia
bakterizid, fungizid,
tuberkulozid, Polio,
Adeno,Papova, Vaccinia, HBV, HIV,
BVDV, Herpes, Rota
bakterizid, fungizid,
tuberkulozid, HBV, BVDV, HIV,Herpes, Influenza A,
Rota, Vaccinia, Papova
bakterizid, fungizid,tuberkulozid,
HBV/HIV,BVDV, Herpes,
Papova,Rota, Vaccinia
Tuberkulose 60 Sek. 60 Sek. 60 Sek. 60 Sek.MRSA/EHEC/VRE 30 Sek. 30 Sek. 30 Sek. 30 Sek.Listerien/Salmonellen 30 Sek. 15 Sek. 30 Sek. 30 Sek.DVV Adeno 5 Min. 2 Min. / / Papova / 2 Min. 5 Min. 5. Min. Polio
o.B./m.B./ 1 Min. / /
Vaccinia 30 Sek. 15 Sek. 30 Sek. 1 Min.Sonstige HBV o.B./m.B. 30 Sek. 30 Sek. 30 Sek. 30 Sek. HCV (BVDV) 30 Sek. 30 Sek. 30 Sek. 30 Sek.
Norwalk (Calici)o.B./m.B. / 2 Min. (RKI) / /HIV 30 Sek. 30 Sek. 30 Sek. 30 Sek.Herpes 30 Sek. 15 Sek. 30 Sek. 30 Sek.Influenza / / 15 Sek. /Rota 30 Sek. 15 Sek. 30 Sek. 30 Sek.
Farbe/Duftstoffe ( + / + ) ( - / - ) ( + / + ) ( - / - )Flammpunkt 19,5° C 0° C 23° C 22,5° C
¤ Be prepared for Norovirus: you ALWAYS will be (too) late ¤ Organize a rapid informaCon system ¤ Have a wrieen plan with
² designated laboratory (and forms filled in) ² Restricted paCent move during outbreaks ² Hand rub with high-‐ethanol content stored in the hospital ready to use. ² Surface disinfectants on stock acCve against Norovirus ² Trained health care personel ² Trained cleaning personell
¤ Contact IsolaCon (& droplet precauCons, especially if vomiCng or cleaning bedpans)
¤ Send infected HCWs home at least as long as they are sick (48hrs amer recovery necessary ?)