differences in mood states, health status, and caregiver strain between family caregivers of...
TRANSCRIPT

138 Journal of Pain and Symptom Management Vol. 13 No. 3 March 1997
Original Article
Differences in Mood States, Health Status, and Caregiver Strain Between Family Caregivers of Oncology Outpatients With and Without Cancer-Related Pain Christine Miaskowski, RN, PhD, FAAN, Lisa Kragness, RN, MS, Suzanne Dibble, RN, DNSc, and Margaret Wallhagen, RN, CS, PhD Department of Physiological Nursing, University of California-San Francisco, San Francisco, California, USA
Abstract The purposes of this study were to determine if there are differences in the mood states, health status, and caregiver strain between family caregivers of oncolog 3 outpatients with and without cancer-related pain. a convenience sample of 86family caregivers of patients with cancer-related pain and 42 caregivers of pain-free patients participated in this study. Family caregivers of patients with cancer-related pain scored significantly higher on the tension and depression subscales of the Profile of Mood States and had a significantly higher total mood disturbance score than did caregivers of painzfree patients. Although family caregivers of patients with pain had lower health status scores and higher caregiver strain scores than caregivers of pain-free patients, these differences were not statistically significant. The results of this study suggest that the presence of pain in a cancer patient adversely affects the mood states of J~zmily caregivers, particularly their level of depression and anxiety, and that health care professionals need to assess the psychological needs of family members caring for cancer patients expedencing pain. J Pain Symptom Manage 1997;13:138-14Z © U.S. Cancer Pain Relief Committee, 199Z
Key Words Family caregivers, pain, mood states, health status, caregiver strain
Introduction Cancer treatment is increasingly being pro-
vided in outpatient settings and in patients' homes. The shift from inpatient to outpatient care results in greater caregiving responsibility
Address reprint requests to: Christine Miaskowski, RN, PhD, FAAN, Department of Physiological Nursing, University of California, San Francisco, Box 0610, N 611Y, San Francisco, CA 94143-0610, USA. Accepted for publication:July 23, 1996.
for family members and other informal care- givers. Now, in addition to dealing with the emo- tional, physical, and financial burdens that a diagnosis of cancer has always imposed, family caregivers must play a greater role in assisting patients with the management of disease and treatment-related side effects. The impact of care- giving on the family caregiver is far reaching. Caregiving results in physical and psychological burdens, mood disturbances, and disruption in normal family relationships) '2
© U.S. Cancer Pain Relief Committee, 1997 0885-3924/97/$17.00 Published by Elsevier, New York, New York PII S0885-3924(96)00297-7

Vol. 13 No. 3 March 1997 Family Caregivers of Oncology Outpatients 139
The physical and psychological complica- tions of cancer and its t reatment regimens can be severe sources of stress for patients and their family caregivers. Caregiver stress can be viewed as "a mix of circumstances, experi- ences, responses, and resources that vary con- siderably among caregivers and that, conse- quently, vary in their impact on caregivers' health and behavior. The mix is not stable; a change in 0he of its components can result in the change of others. ''3
Pain is one of the symptoms f requent ly exper ienced by cancer patients. It is a major source of concern for family caregivers. The suffering of the patient leads to family suffer- ing. 4 In one study of nonterminal advanced cancer patients receiving t reatment in outpa- t ient sett ings/ 80% of patients exper ienced pain; 65% of the patients ' caregivers were extremely concerned about the pain. There- fore, it is not surprising that assistance with pain management is frequently identified as a health-care need by cancer patients and their families. 5'6 No study done to date, however, has compared the mood states, health status, and caregiver strain of family caregivers who are caring for ontology outpatients with and without cancer-related pain. Indeed, the litera- ture on the effects of caregiving on family members of oncology outpatients is somewhat limited.
Stresses~Burden of Caregiving A number of studies have investigated the
stresses and burdens related to being a family caregiver of an oncology patient receiving out- patient care. 1'7-11 In one study of 28 family caregivers of oncology outpatients receiving chemotherapy and radiotherapy, 1 81% of the caregivers repor ted increased levels of stress due to their caregiving role. In another study of family caregivers of patients receiving che- mothe rapy , 1° S c h u m a c h e r and co l leagues found that these family caregivers r epor ted higher caregiver strain than a sample of family caregivers caring for elderly patients. 12
Several studies have identified specific stres- sors and burdens exper ienced by family care- givers. 7's'11 In one study, 7 the stressors identi- fied by family caregivers included t reatment uncertainty, role conflict, added responsibili- ties, fear of be ing alone, coping with the
patient situation, guilt, lack of support, lack of satisfaction with the quality of interact ions with the patient, lack of information, and the burden of assisting the patient with activities of daily living. In addit ion, t ranspor ta t ion problems and financial needs were frequently cited stressors. In ano ther study, 8 the most dif- ficult and demanding activity for family care- givers of outpatients receiving chemotherapy was providing emotional support. In a study of spousal caregiver burden, 11 family caregivers (N= 295) caring for a spouse undergoing che- motherapy or radiotherapy repor ted a wide r ange o f b u r d e n s inc lud ing e m p l o y m e n t , physical, social, time, and financial concerns.
In addition to the specific burdens identi- fied by family caregivers, factors that impact the level of strain among family caregivers have also been identified, a-l° Three studies 8-1° have found that caregiver burden increases with i nc rea s ing p a t i e n t d e p e n d e n c y and impaired levels of patient functioning. Oberst and colleagues v also r epo r t ed that b u rden increased with the length of time the patient was on t reatment and that caregivers with few material and personal resources, poor health, a n d / o r limited educat ion may be the most likely to consider the caregiving situation as harmful and threatening. In addition, social background and context (such as age and gen- der of the caregiver and the patient, and the patient 's point in the disease trajectory) have been shown to explain the degree of caregiver strain e x p e r i e n c e d by family caregivers of oncology outpatients, l° Strain exper ienced by family caregivers was greater when the patient was younger. Gender was also a factor in the level of caregiver strain. Higher levels of care- giver strain were associated with caring for male patients and male caregivers exper ienced more strain than did female caregivers. Care- giver strain was found to be greater for care- givers of patients with nonrecur ren t disease than for caregivers of patients with recur ren t disease) °
The findings of these studies demonstrate that family caregivers of oncolog T outpatients experi- ence increased levels of strain from a number of different stressors. An increase in the impair- ment and dependency of the patient is one of the factors that can cause an increase in the level of strain experienced by family caregivers. None of the studies done to date, however, have evalu-

140 Miaskowski et al. Vot. 13 No. 3 March 1997
ated differences in the level of cai~egiver strain experienced by family caregivers who are caring for oncology outpatients with and without cancer-related pain.
Family Caregiver Mood and Mental Health Status
The mood and mental health status of fam- ily caregivers of oncology outpatients has been investigated. 1's'1°'13 Several studies have found little m o o d dis turbance and relatively low depression scores s'~°'15'16 among family care- givers of oncology outpatients. In fact, the psy- chological status of the family members of oncology outpatients has been reported to coincide with that of the general public. ~3 In the only longitudinal study done to date, 16 the total mood disturbance of the family caregiv- ers of oncology outpatients did not change over three cycles of chemotherapy, but family caregivers reported more depression and anxi- ety than did the patients.
In contrast , several studies 1,l~A4A7 have determined that family caregivers of oncology patients experience changes in their mood states, pa r t i cu la r ly when pa t ien ts are in advanced stages of the disease. Perry and Roades de Meneses I reported that all 28 of the family caregivers of non-terminal advanced cancer patients receiving treatment in outpa- tient settings acknowledged experiencing a change in their emotional state. Anxiety and fear were the emot ions mos t f r equen t ly expressed. Inability to cope, difficulty sleep- ing, emotional withdrawal, and increased cry- ing were also reported by a large percentage of caregivers. Given and Given 14 found that family caregivers of patients with recurrent breast cancer were more depressed than the caregivers of newly diagnosed patients. Six months latex, both groups of family caregivers reported increases in their level of depression with the caregivers of recurrent breast cancer patients experiencing the larger increase.
Kurtz and colleagues 17 also found that care- giver depression increased significantly with the stage of the patient's illness. Family care- givers of patients who died within 6 months after being enrolled in the study were more depressed than family caregivers of patients who survived for greater than 6 months. In another study, 13 the psychological well-being
of spouses and o ther close relatives of a sample of oncology outpatients was found to be significantly correlated with the patient's treatment status (that is, follow-up care, active treatment, or palliative treatment). Relatives of patients receiving palliative care displayed the highest anxiety, the greatest mood distur- bance, and the poorest mental health.
Although the data are somewhat conflicting, these studies suggest that family caregivers of oncology patients experience changes in their mood, particularly related to depression and anxiety. No study done to date, however, has evaluated changes in mood states in family care- givers who are caring for oncology outpatients with and without cancer-related pain.
Family Caregiver Physical Health Status
Very little research has been done on the physical health status of family caregivers of oncology outpatients. One study is found that spouse-caregivers of cancer patients reported s ignif icant ly be t t e r h e a l t h t h a n s p o u s e - caregivers of Alzheimer's patients. In another study, ~5 the perceived impact of caregiving on family members' health was found to be rela- tively small. The level of optimism of family caregivers was found to be an important pre- dictor of variations in their perceptions of the impact of the caregiving experience on their health (that is, family caregivers who were more optimistic reported that their health was less affected by caregiving than those who were less optimistic). In addition, higher levels of depression in the cancer patients were asso- ciated with a greater negative impact on the health of the caregiver. Two additional stud- ies 14'17 have reported that family caregivers experience significant negative consequences on their health status as the stage of the can- cer patient's illness progresses.
The literature presents a conflicting picture of the effect of caregiving on the health status of family caregivers. In general, the effect appears to be minimal, but, as with changes in mood states, there is a significant negative impact with disease progression. Additional research is needed to clarify the impact of care- giving on the health stares of the family care- giver.

Vol. 13 No. 3 March 1997 Family Caregivers of Oncology Outpatients 141
Family Caregivers of Patients in Pain
Research on the family caregiver's experi- ence and response to cancer pain is limited.
Early work by Hinds 19 demonstrated that 30% of family members reported difficulty dealing with the patient's pain problem. In addition, work by Ferrell and colleagues 2'4'~ demonstrated that family members were negatively impacted by the patient's pain experience.
In one qualitative study, 4 the family care- giver's experience of caring for a patient in pa in was ca tegor ized in to th ree gene ra l response categories: helplessness, coping by denying feelings, and a wish for death. Terms such as "heartbreaking," "frustrating," and "helplessness" were used by the caregivers to describe how they were affected by witnessing the pain of their family member. The manage- ment of a cancer patient's pain was described as a caregiver burden.
The results of a quantitative evaluation 2 f o u n d that family caregivers of oncology patients rated the patient's pain as extremely distressing to both themselves and the patient. In add i t ion , family caregivers r a t ed the patient's pain intensity higher than did the patients. Research by Yeager and colleagues 2° also demonstrated that family caregivers tend to overestimate their family member 's pain.
Additional work by Ferrell and colleagues 6 demonstrated that family caregivers of cancer patients in pain described both the sense of joy in caregiving and also the intensity of the physical and psychological burdens resulting from caregiving. The burdens identified were self-sacrifice, feeling inadequate and helpless, feeling alone, worrying about the future, and the burden of the patient. The caregivers were found to participate in the patients' pain by analogy of experience and to, thereby, experi- ence their own emotional and spiritual pain.
In another study, m family caregivers' ethical conflicts associated with pain m a n a g e m e n t were evaluated. The most frequent decisions and conflicts that caregivers experienced were related to medications, including decisions about what medication to give, how much to give, and when to give it. Other conflicts and decisions had to do with balancing dichoto- mies (for example, how much cont ro l to assume versus how much to surrender to the
pa t ien t or nurse) , t r e a t m e n t / i n t e r v e n t i o n decisions (for example, whether or not to con- sent to medical interventions that may cause s y m p t o m dis t ress for the p a t i e n t ) , a n d spiritual/existential conflict (for example, why is the patient suffering so much?).
The literature review clearly indicates that family caregivers of cancer patients experience strain, are burdened by caregiving, and find pain a significant burden. Although there is some conflicting information related to family caregivers ' m o o d , it, too, appears to be impacted by the role of caregiver, particularly in later stages of the disease. The impact of caregiving on physical health is less clear, but it also appears to be negatively affected by dis- ease progression. Although the literature does indicate that pain results in fear and suffering for family caregivers and is very distressing to them, the exact role pain plays in caregiver burden and its effect on health status and mood states of family caregivers needs to be determined.
Therefore, the purposes of this study are (a) to determine if there are differences in mood states between family caregivers of oncology outpatients with and without cancer-related pain; (b) to determine if there are differences in health status between family caregivers of oncology outpatients with and without cancer- related pain; and (c) to determine if there are differences in caregiver strain between family caregivers of ontology outpatients with and without cancer-related pain.
Methods
Design and Setting This descriptive study used self-report ques-
tionnaires to obtain information from the fam- ily caregivers of oncology outpatients. Sixteen ambula tory care sites that are part of the Oncology Nursing Research Network partici- pated in this study. The 16 sites are located throughout the state of California (N = 15) and in Montana (N = 1). Four of the sites are affiliated with university medical centers and 12 are community-based practices. Two sites provide outpatient radiation therapy services, ten sites provide outpat ient chemotherapy, and four sites provide both radiation and che- motherapy services.

142 Miaskowski et al. Vol. 13 No. 3 March 1997
Sample Family caregivers were ident i f ied by the
pat ients as the individual most involved in their care. A convenience sample of 128 fam- ily caregivers of onco logy ou tpa t i en t s was recruited. The family caregivers were willing to participate in the study, were age 18 years or older, were able to read and write English, and gave in fo rmed consent.
I n s t r u m e n t s
The study ins t ruments inc luded a demo- graphic questionnaire, the short fo rm of the Profile of Mood States (POMS), 22 the Care- giver Strain Index (CSI), 12 and the 20-item Medical Outcomes Study Short-Form General Heal th Survey (MOS-SF 20).23
The d e m o g r a p h i c quest ionnaire ob ta ined informat ion on age, gender, relat ionship of the family caregiver to the patient, marital sta- tus, educat ional background, ethnicity, and e m p l o y m e n t status. The ques t ionna i re was developed by a panel of experts in oncology nursing and has been used in previous studies.
The shor t f o r m of the Profile o f Mood States (POMS) (37 items) was developed by Shacham. 22 The shor t form, based on the original 65-item quest ionnaire developed by McNair et al., 24 contains six subscales measur- ing tension, depression, anger, fatigue, confu- sion, and vigor. A total m o o d d is turbance (TMD) score is also calculated. The TMD score is a s um m ary measure of distress with higher scores indicating increased m o o d dis- turbance. Individual items of the POMS are scored on a five-point Likert scale ranging f rom 0 (not at all) to 4 (extremely). The TMD score is calculated by summing each of the individual scores with vigor weighted nega- tively. Shacham, 22 in a study of 83 cancer patients, r e p o r t e d that the in te rna l consis- tency scores of the POMS subscales ranged f rom 0.80 to 0.91 and that the corre la t ion coefficients between the short and long ver- sions of the subscales were all above 0.95. The reliability coefficients for the POMS subscales for this study ranged f rom 0.83 to 0.95.
The MOS-SF 2023 is a 20-item ins t rument developed to measure general functional sta- tus and well-being. The items relate to six heal th concepts that are cons ide red to be impor tan t to any individual: physical function- ing, role functioning, social functioning, men-
tal heal th , hea l th pe rcep t ions , a n d bodi ly pain. Scores for each health concep t range f rom 0 to 100, with higher scores indicating b e t t e r h e a l t h . S t e w a r t a n d c o l l e a g u e s 23 repor ted that the internal consistency reliabil- ity coefficients for the MOS-SF 20 range f rom 0.81 to 0.88. In this study, the reliability coeffi- cients for the MOS-SF 20 subscales r anged f rom 0.85 to 0.87.
T h e Caregiver Strain I n d e x (CSI) 12 is a 13-item ins t rument that identifies strain per- ceived by informal caregivers. The items on the questionnaire reflect 13 stressors identi- fied in an earlier study 25 and th rough a review of the l i terature. The caregiver supplies a "yes" or " n o " response to each i tem indicat- ing whether the s ta tement applies to him or her. The CSI score, ranging f rom 0 to 13, is compu ted by summing the n u m b e r of "yes" responses. Robinson 12 r epo r t ed an in ternal consistency score of 0.86 and de t e rmined con- struct validity in three areas: pat ient character- istics, caregiver's subjective percept ions of the caregiving relationship, and physical and emo- tional status of the caregiver. The reliability and validity of the CSI have been tested and established in two studies. 12'25 The internal consistency reliability coefficient of the CSI in this study was 0.79.
D a t a Collection Procedures
The proposal was approved by the Commit- tee on H u m a n Research at the University of California, San Francisco and by the H u m a n Research C o m m i t t e e s at the var ious sites. Nurses at the 16 sites were t rained in the data collection procedures by the project director. After in formed consent was obtained, family caregivers were asked to comple te the study questionnaires.
D a t a Ana lys i s
Data were analyzed using the CRUNCH® statistical software package. Descriptive staffs- tics and frequency distributions were gener- ated. In order to de te rmine if there were dif- f e r e n c e s in d e m o g r a p h i c c h a r a c t e r i s t i c s between family caregivers of oncology outpa- tients with and without cancer-related pain, independen t Student 's t tests and chi-square analyses were p e r f o r m e d . To d e t e r m i n e if there were differences in m o o d states between the two groups of family caregivers, indepen-
Vol. 13 No. 3 March 1997 Family Caregivers of Oncology Outpatients 143
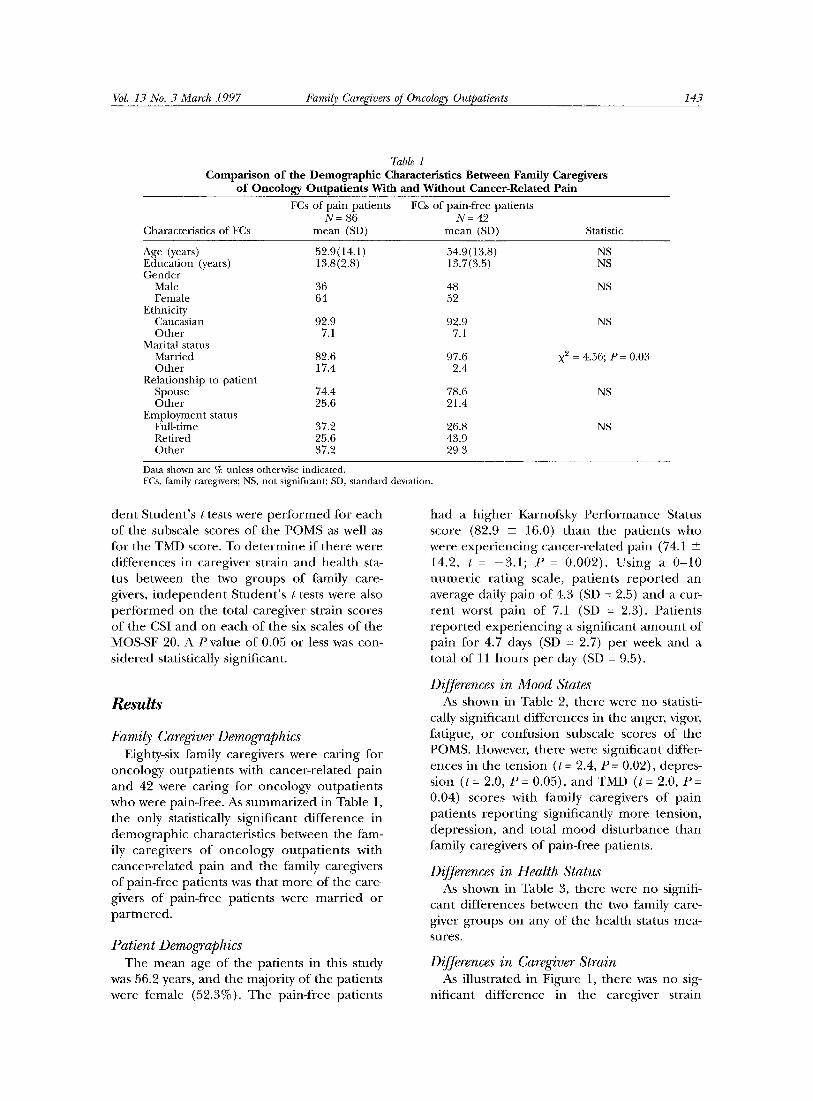
7"able 1 Comparison of file Demographic Characteristics Between Family Caregivers
of Oncology Outpatients With and Without Cancer-Related Pain FCs of pain patients FCs of pain-free patients
N = 86 N = 42 Characteristics of FCs mean (SD) mean (SD) Statistic
Age (years) 52.9(14.1) 54.9(13.8) NS Education (years) 13.8(2.8) 13.7(3.5) NS Gender
Male 36 48 NS Female 64 52
Ethnicity Caucasian 92.9 92.9 NS Other 7.1 7.1
Marital status Married 82.6 97.6 X 2 = 4.56; P = 0.03 Other 17.4 2.4
Relationship to patient Spouse 74.4 78.6 NS Other 25.6 21.4
Employment status Full-time 37.2 26.8 NS Retired 25.6 43.9 Other 37.2 29.3
Data shown are % unless otherwise indicated. FCs, family caregivers; NS, not significant; SD, standard deviation.
d e n t S t u d e n t ' s t tests were p e r f o r m e d fo r each o f the subscale scores o f the P O M S as well as for the TMD score. To d e t e r m i n e i f t h e r e were d i f f e rences in ca reg iver s t ra in a n d h e a l t h sta- tus be tween the two g r o u p s o f fami ly care- givers, i n d e p e n d e n t S t u d e n t ' s t tests were also p e r f o r m e d on the to ta l ca reg iver s t ra in scores o f the CSI a n d on each o f the six scales o f the MOS-SF 20. A P va lue o f 0.05 o r less was con- s i d e r e d statist ically s ignif icant .
Results
Family Caregiver Demographics Eighty-six fami ly caregivers were ca r ing for
o n c o l o g y ou tpa t i en t s with c a n c e r - r e l a t e d p a i n a n d 42 were ca r ing for o n c o l o g y o u t p a t i e n t s who were pain-f ree . As s u m m a r i z e d in Table 1, the only statist ically s ign i f ican t d i f f e r e n c e in d e m o g r a p h i c charac te r i s t i cs b e t w e e n the fam- ily ca r eg ive r s o f o n c o l o g y o u t p a t i e n t s wi th cance r - r e l a t ed p a i n a n d the fami ly caregivers o f pa in- f ree pa t ien t s was tha t m o r e o f the care- givers o f pa in- f ree pa t i en t s were m a r r i e d o r p a r t n e r e d .
Patient Demographics T h e m e a n age o f the pa t i en t s in this s tudy
was 56.2 years, a n d the ma jo r i ty o f the pa t i en t s were f ema le (52.3%). T h e pa in - f ree pa t i en t s
h a d a h i g h e r Karnofsky P e r f o r m a n c e Status score (82.9 + 16.0) t h a n the pa t i en t s who were e x p e r i e n c i n g cance r - r e l a t ed pa in (74.1 _+ 14.2, t = - 3 . 1 ; P = 0 .002) . U s i n g a 0 - 1 0 n u m e r i c r a t i n g scale , p a t i e n t s r e p o r t e d a n average dai ly pa in o f 4.3 (SD -- 2.5) a n d a cur- r e n t wors t p a i n o f 7.1 (SD = 2.3). Pa t i en t s r e p o r t e d e x p e r i e n c i n g a s igni f icant a m o u n t o f pa in for 4.7 days (SD = 2.7) p e r week a n d a to ta l o f 11 h o u r s p e r day (SD = 9.5).
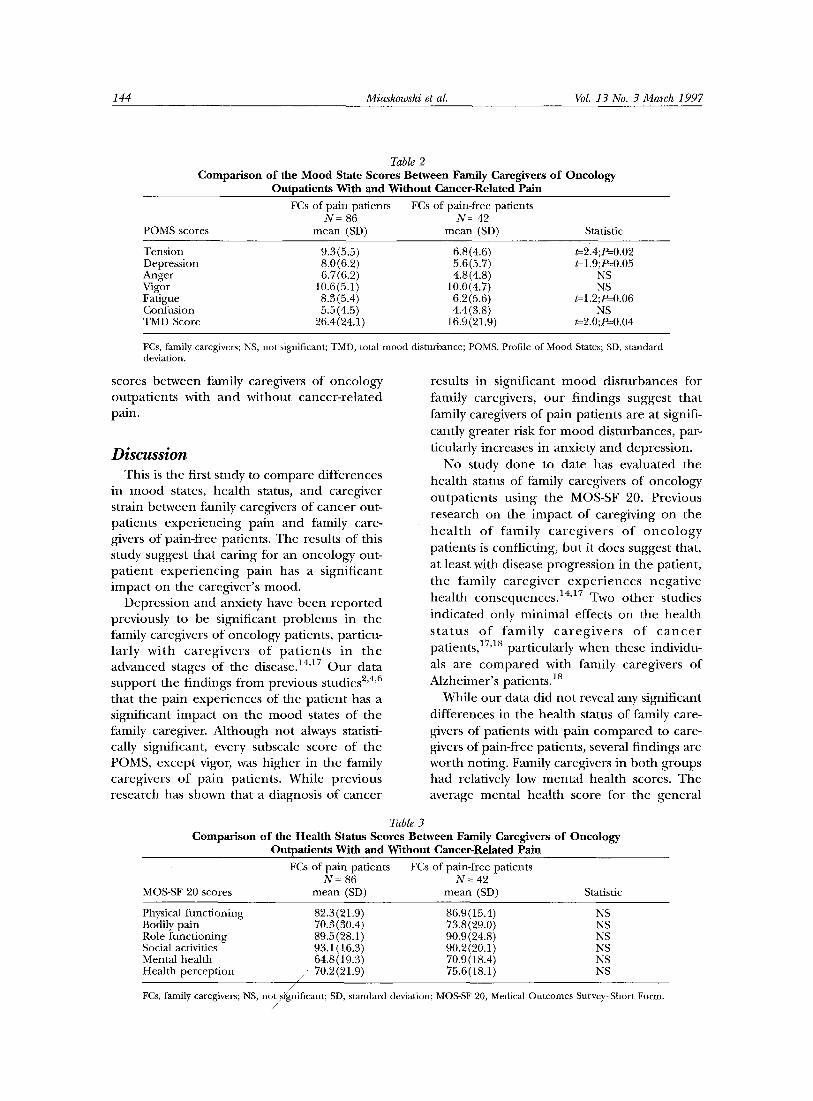
Differences in Mood States As shown in Table 2, t h e r e were no statisti-
cally s ign i f ican t d i f f e r ences in the anger , vigor, fa t igue , o r c o n f u s i o n subsca le scores o f the POMS. However , t h e r e were s igni f icant differ- ences in the t ens ion (t = 2.4, P = 0.02), depres - s ion (t = 2.0, P = 0.05), a n d TMD (t = 2.0, P = 0.04) scores wi th f ami ly ca reg ive r s o f p a i n pa t i en t s r e p o r t i n g s ignif icant ly m o r e tens ion , dep re s s ion , a n d to ta l m o o d d i s t u r b a n c e t han fami ly caregivers o f pa in - f ree pat ients .
Differences in Health Status As shown in Table 3, t h e r e were n o signifi-
c an t d i f f e rences b e t w e e n the two fami ly care- giver g r o u p s on any o f the hea l th status mea- sures.
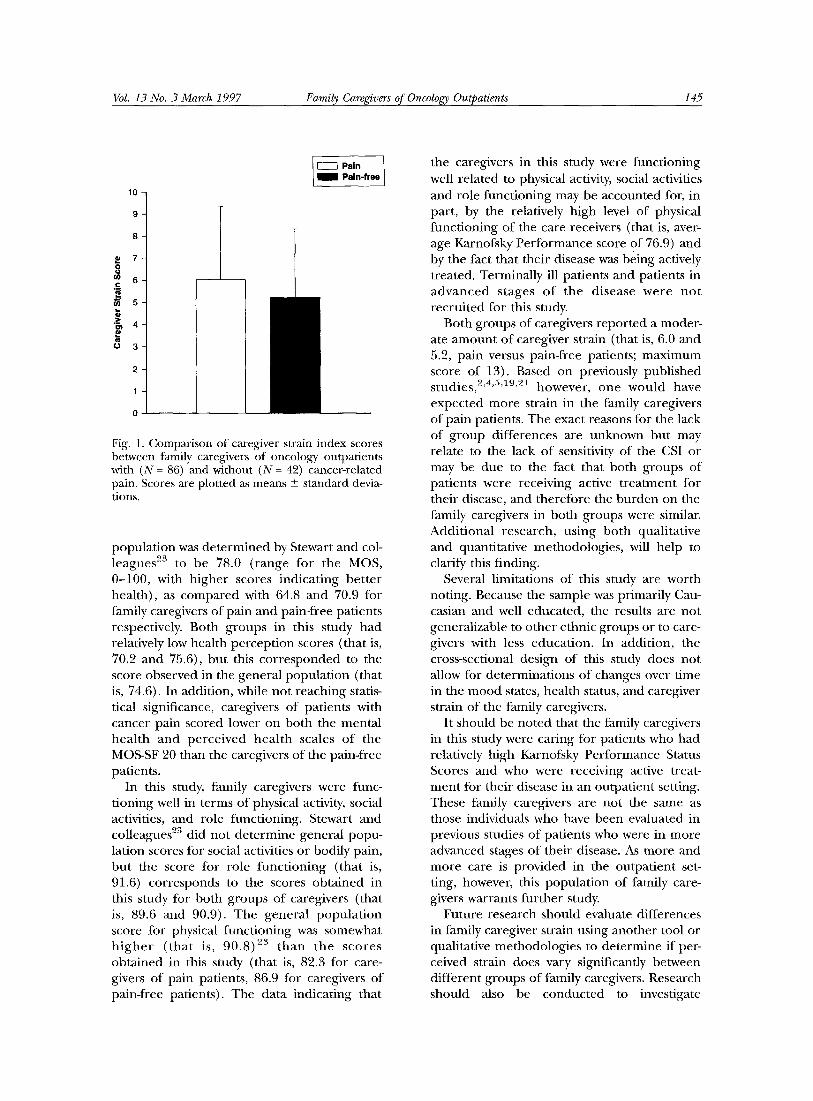
Differences in Caregiver Strain As i l lus t ra ted in F igu re 1, t he re was n o sig-
n i f i can t d i f f e r e nc e in the careg iver s t ra in
144 Miaskowski et al. Vol. 13 No. 3 March 1997
Table 2 Comparison of the Mood State Scores Between Family Caregivers of Oncology
Outpatients With and Without Cancer-Related Pain FCs of pain patients FCs of pain-free patients
N = 86 N = 42 POMS scores mean (SD) mean (SD) Statistic
Tension 9.3(5.5) 6.8(4.6) t=2.4;P=-0.02 Depression 8.0(6.2) 5.6(5.7) t=l.9;P=0.05 Anger 6.7 (6.2) 4.8 (4.8) NS Vigor 10.6(5.1) 10.0(4.7) NS Fatigue 8.3 (5.4) 6.2 (5.6) t=1.2;P=-0.06 Confusion 5.5(4.5) 4.4(3.8) NS TMD Score 26.4(24.1) 16.9(21.9) t=2.0;P=0.04
FCs, family caregivers; NS, not significant; TMD, total mood disturbance; POMS, Profile of Mood States; SD, standard deviation.
scores between family caregivers of oncology outpatients with and without cancer-related pain.
Discussion This is the first study to compare differences
in mood states, health status, and caregiver strain between family caregivers of cancer out- patients experiencing pain and family care- givers of pain-free patients. The results of this study suggest that caring for an oncology out- patient experiencing pain has a significant impact on the caregiver's mood.
Depression and anxiety have been reported previously to be significant problems in the family caregivers of oncology patients, particu- larly with caregivers of pat ients in the advanced stages of the disease. 14'17 Our data support the findings from previous studies 2'4'6 that the pain experiences of the patient has a significant impact on the mood states of the family caregiver. Although not always statisti- cally significant, every subscale score of the POMS, except vigor, was higher in the family caregivers of pain patients. While previous research has shown that a diagnosis of cancer
results in significant mood disturbances for family caregivers, our findings suggest that family caregivers of pain patients are at signifi- cantly greater risk for mood disturbances, par- ticularly increases in anxiety and depression.
No study done to date has evaluated the health status of family caregivers of oncology outpatients using the MOS-SF 20. Previous research on the impact of caregiving on the heal th of family caregivers of oncology patients is conflicting, but it does suggest that, at least with disease progression in the patient, the family caregiver experiences negative health consequences. 14'17 Two other studies indicated only minimal effects on the health s ta tus of fami ly caregivers of c ance r patients, 17'a8 particularly when these individu- als are compared with family caregivers of Alzheirner's patients. 18
While our data did not reveal any significant differences in the health status of family care- givers of patients with pain compared to care- givers of pain-free patients, several findings are worth noting. Family caregivers in both groups had relatively low mental health scores. The average mental health score for the general
Table 3 Comparison of the Health Status Scores Between Family Caregivers of Oncology
Outpatients With and Without Cancer-Related Pain FCs of pain patients FCs of pain-free patients
N = 86 N = 42 MOS-SF 20 scores mean (SD) mean (SD) Statistic
Physical functioning 82.3(21.9) 86.9(15.4) NS Bodily pain 70.3(30.4) 73.8(29.0) NS Role functioning 89.5 (28.1) 90.9 (24.8) NS Social activities 93.1 (16.3) 90.2(20.1) NS Mental health 64.8(19.3) 70.9(18.4) NS Health perception / / 70.2(21.9) 75.6(18.1) NS
FCs, family caregivers; NS, no~'g~nificant; SD, standard deviation; MOS-SF 20, Medical Outcomes Survey-Short Form.
Vol. 13 No. 3 March 1997 Family Caregivers of Oncology Outpatients 145
1 I--'--1 Pain 1 Pain-free 10
8
i
Fig. 1. Comparison of caregiver strain index scores between family caregivers of oncology outpatients with (N = 86) and without (N = 42) cancer-related pain. Scores are plotted as means _+ standard devia- tions.
populat ion was de termined by Stewart and col- leagues 2s to be 78.0 (range for the MOS, 0-100, with higher scores indicating bet ter health), as compared with 64.8 and 70.9 for thmily caregivers of pain and pain-free patients respectively. Both groups in this study had relatively low health percept ion scores (that is, 70.2 and 75.6), but this cor responded to the score observed in the general populat ion (that is, 74.6). In addition, while not reaching statis- tical significance, caregivers of patients with cancer pain scored lower on both the mental hea l th and perce ived heal th scales of the MOS-SF 20 than the caregivers of the pain-free patients.
In this study, t~tmily caregivers were func- tioning well in terms of physical activity, social activities, and role functioning. Stewart and colleagues 2s did not determine general popu- lation scores for social activities or bodily pain, bu t the score for role funct ioning (that is, 91.6) corresponds to the scores obtained in this study for both groups of caregivers (that is, 89.6 and 90.9). The general popula t ion score for physical functioning was somewhat h i g h e r ( tha t is, 90.8) 23 t han the scores obtained in this study (that is, 82.3 for care- givers of pain patients, 86.9 for caregivers of pain-free patients). The data indicating that
the caregivers in this study were functioning well related to physical activity, social activities and role functioning may be accounted for, in part, by the relatively high level of physical functioning of the care receivers (that is, aver- age Karnofsky Performance score of 76.9) and by the fact that their disease was being actively treated. Terminally ill patients and patients in advanced stages o f the disease were no t recrui ted for this study.
Both groups of caregivers repor ted a moder- ate amount of caregiver strain (that is, 6.0 and 5.2, pain versus pain-free patients; maximum score of 13). Based on previously published studies, 2'4'5'19'21 however, one would have expected more strain in the family caregivers of pain patients. The exact reasons for the lack of group differences are unknown but may relate to the lack of sensitivity of the CSI or may be due to the fact that both groups of patients were receiving active t reatment for their disease, and therefore the burden on the family caregivers in both groups were similar. Addit ional research, using both qualitative and quantitative methodologies, will help to clarify this finding.
Several limitations of this study are worth noting. Because the sample was primarily Cau- casian and well educated, the results are not generalizable to other ethnic groups or to care- givers with less education. In addition, the cross-sectional design of this study does not allow for determinations of changes over time in the mood states, health status, and caregiver strain of the family caregivers.
It should be noted that the family caregivers in this study were caring for patients who had relatively high Karnofsky Performance Status Scores and who were receiving active treat- ment for their disease in an outpatient setting. These family caregivers are not the same as those individuals who have been evaluated in previous studies of patients who were in more advanced stages of their disease. As more and more care is provided in the outpatient set- ring, however, this populat ion of family care- givers warrants fur ther study.
Future research should evaluate differences in family caregiver strain using another tool or qualitative methodologies to determine if per- ceived strain does vary significantly between different groups of family caregivers. Research should also be conducted to investigate

146 Miaskowski et al. Vol. 13 No. 3 March 1997
whethe r strain a nd m o o d states vary over t ime and if they vary based on severity o f pain o r o the r pa t ien t or caregiver characteristics. Lon- gi tudinal studies with family are part icular ly i m p o r t a n t because onco logy patients are living longe r with their chron ic illness. Future stud- ies cou ld also evaluate what caregiver charac- teristics (for example, gende r o r re la t ionship to the pat ient) inf luence caregiver ou tcomes . In te rven t ions to min imize the negative impac t o f the pa t i en t ' s pa in u p o n the ca reg ive r ' s m o o d shou ld also be deve loped and tested.
T h e results o f this study suggest tha t the presence o f pain in a cancer pa t ien t adversely affects the m o o d states o f family caregivers, part icularly their level o f depress ion and anxi- ety. Heal th-care professionals n e e d to assess the psychological needs o f family caregivers, pay ing pa r t i cu l a r a t t en t ion to those family m e m b e r s c a r i n g fo r pa t ien ts e x p e r i e n c i n g pain. Des ign ing in t e rven t ions for b o t h the patients and the family caregivers in this h igh risk g r o u p will be an impor t an t step in improv- ing the e m o t i o n a l wel l -be ing o f b o t h the pa t ien t and their family caregiver.
Acknowledgment This s tudy was f u n d e d by grants f r o m the
Cance r Research Coord ina t ing Commi t t ee o f the University o f California and the O n c o l o g y Nurs ing Founda t ion .
R e f e r e n c e s
1. Perry GR, Roades de Meneses M. Cancer patients at home: needs and coping styles of pri- mary caregivers. Home Healthcare Nurse 1989;7: 27-30.
2. Ferrell BR, Ferrell BA, Rhiner M, Grant M. Family factors influencing cancer pain manage- ment. Postgrad MedJ 1991;67(suppl 2):$64-$69.
3. Pear|in LI, Mu JT, Semple SJ, Skaff MM. Care- giving and tile stress process: An overview of concepts and their measures. Gerontologist 1990;30:583-594.
4. Ferrell BR, Rhiner M, Cohen MZ, Grant M. Pain as a metaphor for illness, part I: impact of can- cer pain on family caregivers. Oncol Nurs Forum 1991;18:1303-1309.
5. Ferrell BR, Cohen MZ, Rhiner M, Rozek A. Pain as a metaphor for illness, part II: family care- givers' management of pain. Oncol Nuts Forum 1991;18:1315-1321.
6. Ferrell BR, Taylor EJ, Grant M, Fowler M, Corbisi-
ero RM. Pain management at home: struggle, com- fort, and mission. Cancer Nuts 1993;16:169-178.
7. BlankJJ, Clark L, Longman AJ, AtwoodJR. Per- ceived home care needs of cancer patients and their caregivers. Cancer Nurs 1989;12:78-84.
8. Carey PJ, Oberst MT, McCubbin MA, Huges SH. Appraisal and caregiving burden in family members caring tot patients receiving chemo- therapy. Oncol Nurs Forum 1991;18:1341-1348.
9. Oberst MT, Thomas SE, Gass KA, Ward SE. Caregiving demands and appraisal of stress among family caregivers. Cancer Nuts 1989;12:209-215.
10. Schumacher KL, Dodd MJ, Paul SM. The stress process in family caregivers of persons receiving chemotherapy. Res Nurs Health 1993;16:395-404.
11. Siegel K, Raveis VII, Mor V, Houts P. The rela- tionship of spousal caregiver burden to patient dis- ease and treatment-related conditions. Ann Oncol 1991;2:511-516.
12. Robinson BC. Validation of a caregiver strain index. J Gerontol 1983;38:344-348.
13. Cassileth BR, Lusk EJ, Strouse TB, Miller DS, Brown LL, Cross PA. A psychological analysis of can- cer patients and their next-of-kin. Cancer 1985;55:72- 76.
14. Given B, Given CW. Patient and family care- giver reaction to new and recurrent breast cancer. J Am Med Wom Assoc 1992;47:201-212.
15. Given CW, Stommel M, Given B, OsuchJ, Kurtz ME, Kurtz JC. The influence of cancer patients' symptoms and functional states on patients' depres- sion and family caregivers' reaction and depression. Health Psychol 1993;12:277-285.
16. Musci EC, Dodd MJ. Predicting self-care with patients and family members' affective states and family functioning. Oncol Nurs Forum 1990;17: 394-400.
17. Kurtz ME, Given B, Kurtz JC, Given CW. The interaction of age, symptoms, and survival status on physical and mental health of patients with cancer and their families. Cancer 1994;74:2071-2078.
18. Clipp EC, George LK. Dementia and cancer: a comparison of spouse caregivers. Gerontologist 1993;33:534-541.
19. Hinds C. The needs of families who care for patients with cancer at home: are we meeting them? J Adv Nuts 1985;10:575-581.
20. Yeager KA, Miaskowski C, Dibble SL, Wallhagen M. Differences in pain knowledge and perception of the pain experience between outpatients with cancer and their family caregivers. Oncol Nurs Forum 1995;22:1235-1241.
21. Taylor EJ, Ferrell BR, Grant M, Cheyney L. Man- aging cancer pain at home: the decisions and ethical conflicts of patients, family caregivers, and homecare nurses. Oncol Nurs Forum 1993;20:919-926.
22. Shacham S. A shortened version of the Profile

Vol. 13 No. 3 March 1997 Family Careg~vers of Oncology Outpatients 147
of Mood States. J Pers Assess 1983;47:305-306.
23. Stewart AL, Greenfield S, Hays RD, et al. Func- tional status and well-being of patients with chronic condit ions: results from the Medical Outcomes Study. JAMA 1989;262:907-913.
24. McNair DM, Lorr M, Droppleman LE ETIS
manual for the Profile of Mood States. San Diego, CA: Educational and Industrial Testing Service, 1971.
25. Robinson B, Thurnher M. Taking care of aged parents: a family cycle transition. Gerontologist 1979;19:586-593.
26. CRUNCH ® Software, Berkeley, CA.