disclosures crash 2015 pulmonary hypertensive crisis · crash 2015 pulmonary hypertensive crisis...
TRANSCRIPT
CRASH 2015Pulmonary Hypertensive Crisis
Mark Twite MA MB BChir FRCP
Children’s Hospital Colorado & University of ColoradoAnschutz Medical Campus
Disclosures
• No financial disclosures
• Some drugs discussed are an off-label application
2
Objectives
After 30 minutes, understand:
1. Pathophysiology of pulmonary hypertension (PH)
2. Anesthetic management of PH
3. Strategies to prevent and treat a PH crisis
3
Case Scenario
• 18yr old, 70kg female with PH• Requires Broviac® catheter placement and lung biopsy• Last Echocardiogram report
– Tricuspid regurgitant (TR) jet 5m/sec (BP 110/70)– No PFO
• Patient’s medications– Epoprostenol sodium (Flolan®)– Sildenafil (Revatio®)– Bosentan (Tracleer®)– Aspirin– Nifedipine
4
Question
What is the degree of this patient’s PH?
1. Supra-systemic
2. Systemic
3. Sub-systemic
5
Definition: Pulmonary Hypertension
• mPAP ≥ 25 mmHg at rest • Normal mean pulmonary artery pressure (mPAP)≈15mmHg
– independent of age, gender, ethnicity
• During exercise mPAP increases slightly– dependent on age and level of exertion
• PVRI ≥ 3 Wood units m2
• In association with variable degrees of:• Pulmonary vascular remodeling • Vasoconstriction • In-situ thrombosis
6Nef Heart 2010;96:552-559
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis
Case Scenario
• 18yr old, 70kg female with PH• Requires Broviac® catheter placement and lung
biopsy
• Last Echocardiogram report– TR jet 5m/sec (BP 110/45)– No PFO
• Patient’s medications– Epoprostenol sodium (Flolan®)– Sildenafil (Revatio®)– Bosentan (Tracleer®)– Aspirin– Nifedipine
7
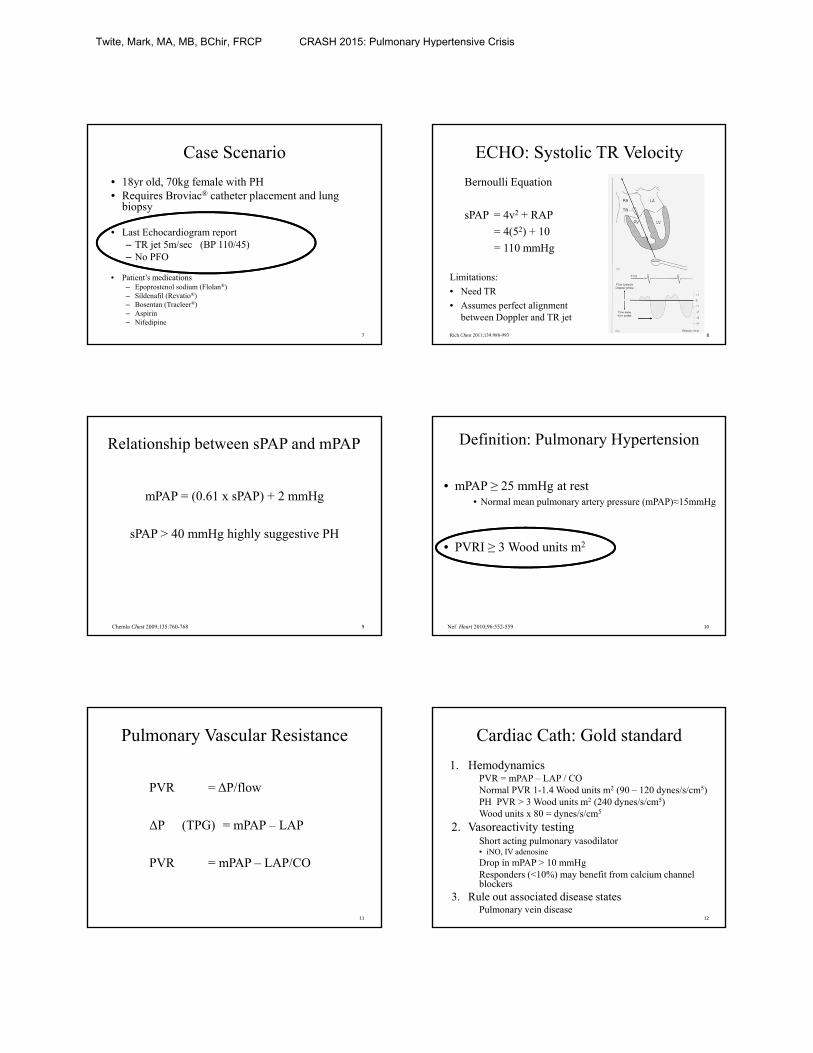
ECHO: Systolic TR Velocity
Bernoulli Equation
sPAP = 4v2 + RAP
= 4(52) + 10
= 110 mmHg
Limitations:
• Need TR
• Assumes perfect alignment between Doppler and TR jet
Rich Chest 2011;139:988-993 8
Relationship between sPAP and mPAP
mPAP = (0.61 x sPAP) + 2 mmHg
sPAP > 40 mmHg highly suggestive PH
9Chemla Chest 2009;135:760-768
Definition: Pulmonary Hypertension
• mPAP ≥ 25 mmHg at rest • Normal mean pulmonary artery pressure (mPAP)≈15mmHg
• PVRI ≥ 3 Wood units m2
10Nef Heart 2010;96:552-559
Pulmonary Vascular Resistance
PVR = ΔP/flow
ΔP (TPG) = mPAP – LAP
PVR = mPAP – LAP/CO
11
Cardiac Cath: Gold standard
1. HemodynamicsPVR = mPAP – LAP / CONormal PVR 1-1.4 Wood units m2 (90 – 120 dynes/s/cm5)PH PVR > 3 Wood units m2 (240 dynes/s/cm5)Wood units x 80 = dynes/s/cm5
2. Vasoreactivity testingShort acting pulmonary vasodilator • iNO, IV adenosine
Drop in mPAP > 10 mmHgResponders (<10%) may benefit from calcium channel blockers
3. Rule out associated disease statesPulmonary vein disease
12
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis
Non-invasively monitor patients with PH?
• Right ventricle (RV) function– Ability of the RV to cope with progressive increase
in PA pressure
– Determines patient’s functional capacity and survival
• Other ECHO parameters (observer angle dependent):– TAPSE (Tricuspid Annular Plane Systolic Excursion)
– Tei index
13
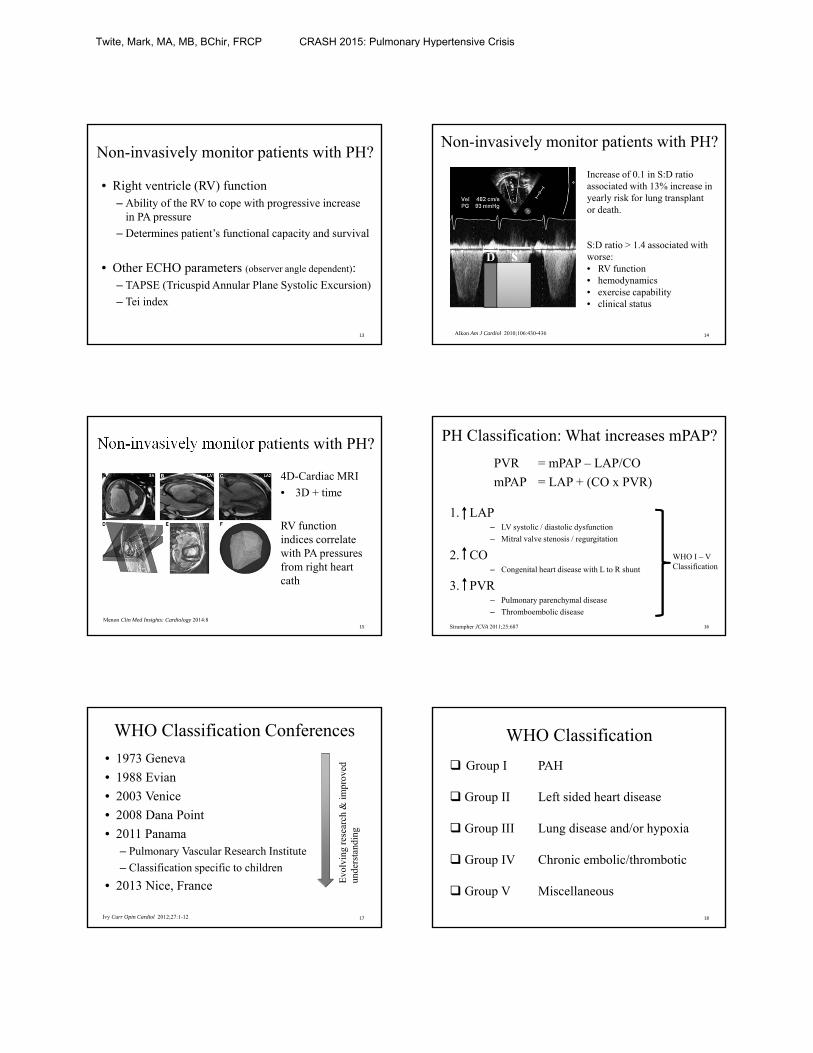
Increase of 0.1 in S:D ratio associated with 13% increase in yearly risk for lung transplant or death.
S:D ratio > 1.4 associated with worse:• RV function• hemodynamics• exercise capability• clinical status
Alkon Am J Cardiol 2010;106:430-436
Non-invasively monitor patients with PH?
14
Non-invasively monitor patients with PH?
4D-Cardiac MRI
• 3D + time
RV function indices correlate with PA pressures from right heart cath
15
Menon Clin Med Insights: Cardiology 2014:8
PH Classification: What increases mPAP?
PVR = mPAP – LAP/CO
mPAP = LAP + (CO x PVR)
1. LAP– LV systolic / diastolic dysfunction
– Mitral valve stenosis / regurgitation
2. CO– Congenital heart disease with L to R shunt
3. PVR– Pulmonary parenchymal disease
– Thromboembolic disease
16Strumpher JCVA 2011;25:687
WHO I – VClassification
WHO Classification Conferences
• 1973 Geneva
• 1988 Evian
• 2003 Venice
• 2008 Dana Point
• 2011 Panama– Pulmonary Vascular Research Institute
– Classification specific to children
• 2013 Nice, France Evo
lvin
g re
sear
ch &
impr
oved
un
ders
tand
ing
Ivy Curr Opin Cardiol 2012;27:1-12 17
WHO Classification
Group I PAH
Group II Left sided heart disease
Group III Lung disease and/or hypoxia
Group IV Chronic embolic/thrombotic
Group V Miscellaneous
18
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis
WHO Classification
Group I PAH• Idiopathic
• Heritable: TGF-β Family (BMPR2, ALK-1, Endoglin)
• Drugs: Fenfluramine, methamphetamine
• Herbal supplements: St. John’s Wort
• Associated with: – Congenital heart disease
– Connective tissue disease (SLE)
– HIV
– Chronic hemolytic anemias (Sickle cell disease)
– Schistosomiasis
– Pulmonary veno-occlusive disease (PVOD)19
Group II Left heart disease• Mitral valve disease
Group III Lung disease and/or hypoxia• COPD
• BPD
• Interstitial lung disease
• Sleep-disordered breathing
• High altitude
Group IV Chronic embolic/thrombotic
Group V Miscellaneous• Myeloproliferative disorders
• Metabolic disorders20
Pediatric Pulmonary Hypertension
21
Chromosomal or Genetic
syndrome
Lung development abnormalities
Pathological insults on a
growing lung
PH: Congenital Heart Disease
Biventricular Circulation– mPAP > 25mmHg & PVRI > 3 Wood units m2
– Positive vasodilator response is a fall in mPAP and PVRI by 20% with no change in CO
Univentricular Circulation – following cavopulmonary anastomosis
– PVRI > 3 Wood units m2 or TPG > 6 mmHg
EVEN IF mPAP < 25mmHg
Del Cerro Pulm Circ 2011;1:286-98 22
Adult: Epidemiology & Survival
• Rare disease 5-15 cases / million
• REVEAL– Age of presentation increased from 35yrs in 1980s
to 53yrs
– Male:Female 1:4
– 1yr survival 80-90%
– 3yr survival 60%
23Benza Chest 2012; 142
Pediatric: Epidemiology & Survival
TOPP1
• Global registry
• At diagnosis:– Median age 7yrs
– Dyspnea & fatigue
– 43% other disorders• 85% CHD, 12% BPD
– Chromosome anomalies 13% (Trisomy 21)
REVEAL2
• USA registry
• At diagnosis:– Median age 7yrs
– Dyspnea
– mPAP 56mmHg
– PVRI 17 Wood units m2
– 5yr survival 75%
241Berger Lancet 2012; 379:537-46 2Barst Circulation 2012;125:113-122
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis

Case Scenario
• 18yr old, 70kg female with PH• Requires Broviac® catheter placement and lung biopsy
• Last Echocardiogram report– TR jet 5m/sec (BP 110/45)– No PFO
• Patient’s medications– Epoprostenol sodium (Flolan®)– Sildenafil (Revatio®)– Bosentan (Tracleer®)– Aspirin– Nifedipne
25
Question
Option BP SpO2
1
2
3
4
26
With no PFO on ECHO, what may happen during an acute increase in PVR?
Physiology of Pulmonary Circulation
• Pulmonary vascular bed is a high-flow low-pressure circulation system
• Large cross sectional area
• High compliance arterioles with thin walls (less smooth muscle cells)
• Pressure and resistance are 10% of systemic circulation
• Sympathetic nervous system innervation
• Pulmonary arteries• Constrict with hypoxia (Euler-Liljestrand reflex) and relax with
hyperoxia
• Respond to changes in cardiac output and airway pressure
27
8mm ≈ 1 x R 4mm ≈ 16 x R 2mm ≈ 256 x R
Pathophysiology of Pulmonary Circulation
FIXED Structural changes decrease X-sectional area
REACTIVE Vascular smooth muscle contraction
Poiseuille’s Law R = π r4 p / 8nl
28
PH: Pathology
A. Vasculopathy of the pulmonary arteriole cells1. Endothelial
Intimal hyperplasia
2. Smooth muscle cell (SMC)Medial hypertrophy
3. AdventitialProliferation
B. Vasoconstriction
C. Thrombosis
29
Les
s di
sten
sibl
e ve
ssel
Fixe
d vs
. Rea
ctiv
e
PH: PathologyPlexiform lesion
Normal30
Cool Chest 2005;128:656-571
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis
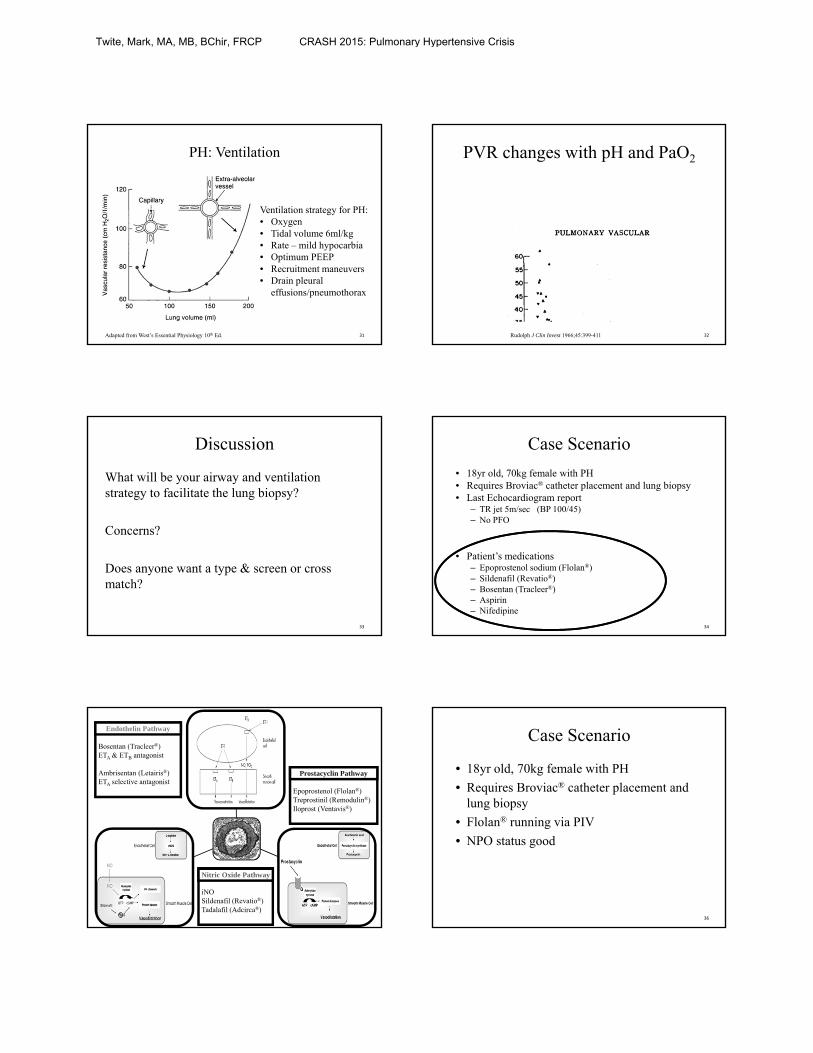
PH: Ventilation
31Adapted from West’s Essential Physiology 10th Ed.
Ventilation strategy for PH:• Oxygen• Tidal volume 6ml/kg• Rate – mild hypocarbia• Optimum PEEP• Recruitment maneuvers• Drain pleural
effusions/pneumothorax
PVR changes with pH and PaO2
32Rudolph J Clin Invest 1966;45:399-411
Discussion
What will be your airway and ventilation strategy to facilitate the lung biopsy?
Concerns?
Does anyone want a type & screen or cross match?
33
Case Scenario
• 18yr old, 70kg female with PH• Requires Broviac® catheter placement and lung biopsy• Last Echocardiogram report
– TR jet 5m/sec (BP 100/45)– No PFO
• Patient’s medications– Epoprostenol sodium (Flolan®)– Sildenafil (Revatio®)– Bosentan (Tracleer®)– Aspirin– Nifedipine
34
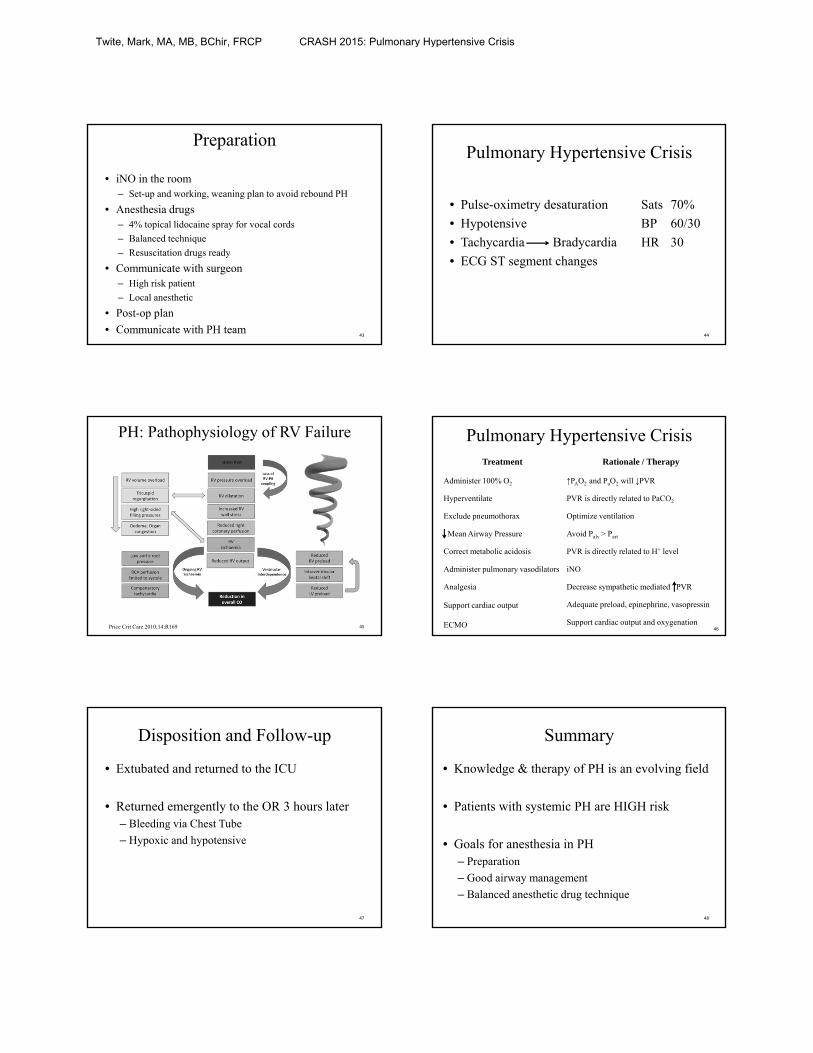
35
Bosentan (Tracleer®) ETA & ETB antagonist
Ambrisentan (Letairis®) ETA selective antagonist
Epoprostenol (Flolan®)Treprostinil (Remodulin®)Iloprost (Ventavis®)
iNOSildenafil (Revatio®)Tadalafil (Adcirca®)
Nitric Oxide Pathway
Prostacyclin Pathway
Endothelin Pathway Case Scenario
• 18yr old, 70kg female with PH
• Requires Broviac® catheter placement and lung biopsy
• Flolan® running via PIV
• NPO status good
36
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis
Question
What is this patient’s risk of cardiac arrest under general anesthesia?
1. 10 times LESS
2. SAME
3. 10 times GREATER
4. 40 times GREATER
37
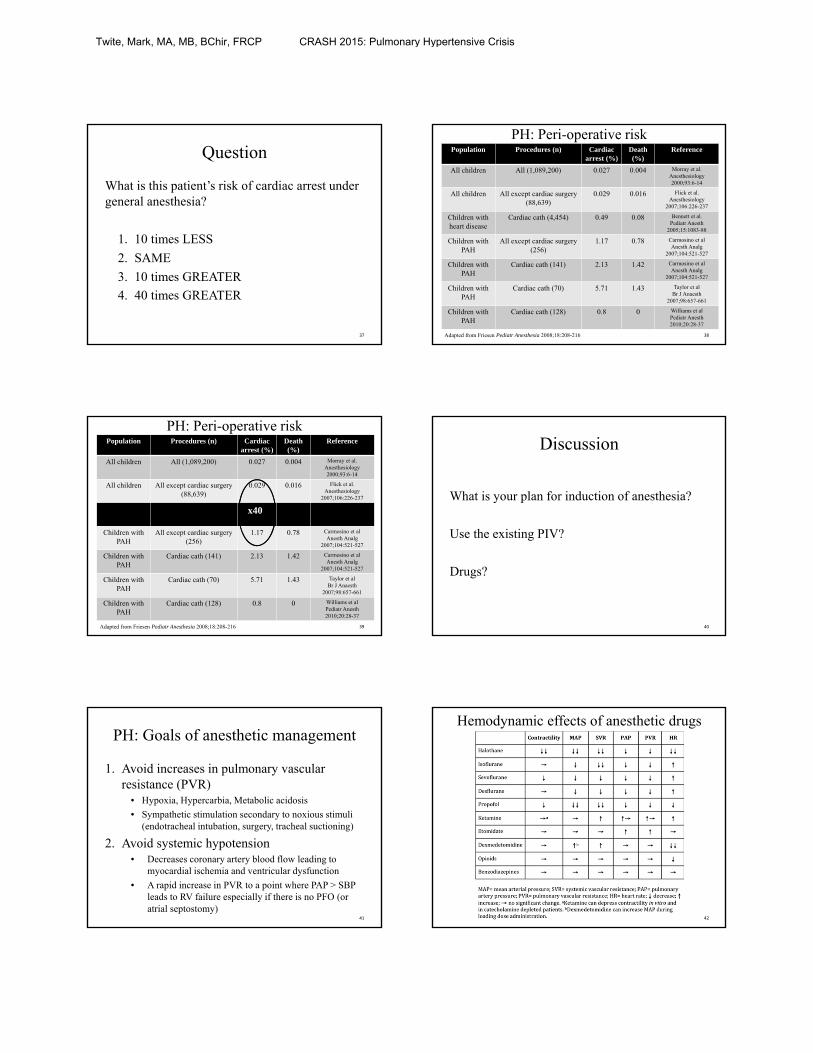
PH: Peri-operative riskPopulation Procedures (n) Cardiac
arrest (%)Death (%)
Reference
All children All (1,089,200) 0.027 0.004 Morray et al. Anesthesiology 2000;93:6-14
All children All except cardiac surgery (88,639)
0.029 0.016 Flick et al. Anesthesiology
2007;106:226-237
Children with heart disease
Cardiac cath (4,454) 0.49 0.08 Bennett et al. Pediatr Anesth
2005;15:1083-88
Children with PAH
All except cardiac surgery (256)
1.17 0.78 Carmosino et alAnesth Analg
2007;104:521-527
Children with PAH
Cardiac cath (141) 2.13 1.42 Carmosino et alAnesth Analg
2007;104:521-527
Children with PAH
Cardiac cath (70) 5.71 1.43 Taylor et alBr J Anaesth
2007;98:657-661
Children with PAH
Cardiac cath (128) 0.8 0 Williams et alPediatr Anesth2010;20:28-37
38Adapted from Friesen Pediatr Anesthesia 2008;18:208-216
PH: Peri-operative riskPopulation Procedures (n) Cardiac
arrest (%)Death (%)
Reference
All children All (1,089,200) 0.027 0.004 Morray et al. Anesthesiology 2000;93:6-14
All children All except cardiac surgery (88,639)
0.029 0.016 Flick et al. Anesthesiology
2007;106:226-237
Children with heart disease
Cardiac cath (4,454) x409 0.08 Bennett et al. Pediatr Anesth
2005;15:1083-88
Children with PAH
All except cardiac surgery (256)
1.17 0.78 Carmosino et alAnesth Analg
2007;104:521-527
Children with PAH
Cardiac cath (141) 2.13 1.42 Carmosino et alAnesth Analg
2007;104:521-527
Children with PAH
Cardiac cath (70) 5.71 1.43 Taylor et alBr J Anaesth
2007;98:657-661
Children with PAH
Cardiac cath (128) 0.8 0 Williams et alPediatr Anesth2010;20:28-37
39Adapted from Friesen Pediatr Anesthesia 2008;18:208-216
Discussion
What is your plan for induction of anesthesia?
Use the existing PIV?
Drugs?
40
PH: Goals of anesthetic management
1. Avoid increases in pulmonary vascular resistance (PVR)
• Hypoxia, Hypercarbia, Metabolic acidosis
• Sympathetic stimulation secondary to noxious stimuli (endotracheal intubation, surgery, tracheal suctioning)
2. Avoid systemic hypotension • Decreases coronary artery blood flow leading to
myocardial ischemia and ventricular dysfunction
• A rapid increase in PVR to a point where PAP > SBP leads to RV failure especially if there is no PFO (or atrial septostomy)
41
Hemodynamic effects of anesthetic drugs
42
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis
Preparation
• iNO in the room– Set-up and working, weaning plan to avoid rebound PH
• Anesthesia drugs– 4% topical lidocaine spray for vocal cords
– Balanced technique
– Resuscitation drugs ready
• Communicate with surgeon– High risk patient
– Local anesthetic
• Post-op plan
• Communicate with PH team43
Pulmonary Hypertensive Crisis
• Pulse-oximetry desaturation Sats 70%
• Hypotensive BP 60/30
• Tachycardia Bradycardia HR 30
• ECG ST segment changes
44
PH: Pathophysiology of RV Failure
45Price Crit Care 2010;14:R169
Pulmonary Hypertensive CrisisTreatment
Administer 100% O2
Hyperventilate
Exclude pneumothorax
Mean Airway Pressure
Correct metabolic acidosis
Administer pulmonary vasodilators
Analgesia
Support cardiac output
ECMO
Rationale / Therapy
↑PAO2 and PaO2 will ↓PVR
PVR is directly related to PaCO2
Optimize ventilation
Avoid Palv > Part
PVR is directly related to H+ level
iNO
Decrease sympathetic mediated PVR
Adequate preload, epinephrine, vasopressin
Support cardiac output and oxygenation46
Disposition and Follow-up
• Extubated and returned to the ICU
• Returned emergently to the OR 3 hours later– Bleeding via Chest Tube
– Hypoxic and hypotensive
47
Summary
• Knowledge & therapy of PH is an evolving field
• Patients with systemic PH are HIGH risk
• Goals for anesthesia in PH– Preparation
– Good airway management
– Balanced anesthetic drug technique
48
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis

Thankyou!
49
Bibliography
1. Alkon J, Humpl T, Manlhiot C, McCrindle BW, Reyes JT, Friedberg MK. Usefulness of the right ventricular systolic to diastolic duration ratio to predict functional capacity and survival in children with pulmonary arterial hypertension. The American journal of cardiology. Aug 1 2010;106(3):430‐436.
2. Alswang M, Friesen RH, Bangert P. Effect of preanesthetic medication on carbon dioxide tension in children with congenital heart disease. Journal of cardiothoracic and vascular anesthesia. Aug 1994;8(4):415‐419.
3. Archer SL, Weir EK, Wilkins MR. Basic science of pulmonary arterial hypertension for clinicians: new concepts and experimental therapies. Circulation. May 11 2010;121(18):2045‐2066.
4. Barst RJ, McGoonMD, Elliott CG, Foreman AJ, Miller DP, Ivy DD. Survival in childhood pulmonary arterial hypertension: insights from the registry to evaluate early and long‐term pulmonary arterial hypertension disease management. Circulation. Jan 3 2012;125(1):113‐122.
5. Bennett D, Marcus R, Stokes M. Incidents and complications during pediatric cardiac catheterization. Paediatric anaesthesia. Dec 2005;15(12):1083‐1088.
6. Berger RM, Beghetti M, Humpl T, et al. Clinical features of paediatric pulmonary hypertension: a registry study. Lancet. Feb 11 2012;379(9815):537‐546.
7. Berger S, Konduri GG. Pulmonary hypertension in children: the twenty‐first century. Pediatric clinics of North America. Oct 2006;53(5):961‐987, x.
8. Blaise G, LanglebenD, Hubert B. Pulmonary arterial hypertension: pathophysiology and anesthetic approach. Anesthesiology. Dec 2003;99(6):1415‐1432.
9. Budhiraja R, Tuder RM, Hassoun PM. Endothelial dysfunction in pulmonary hypertension. Circulation. Jan 20 2004;109(2):159‐165.
10. Carmosino MJ, Friesen RH, Doran A, Ivy DD. Perioperative complications in children with pulmonary hypertension undergoing noncardiac surgery or cardiac catheterization. Anesthesia and analgesia. Mar 2007;104(3):521‐527.
11. Cerro MJ, Abman S, Diaz G, et al. A consensus approach to the classification of pediatric pulmonary hypertensive vascular disease: Report from the PVRI Pediatric Taskforce, Panama 2011. Pulmonary circulation. 2011;1(2):286‐298.
12. Chemla D, Castelain V, Provencher S, HumbertM, Simonneau G, Herve P. Evaluation of various empirical formulas for estimating mean pulmonary artery pressure by using systolic pulmonary artery pressure in adults. Chest. Mar 2009;135(3):760‐768.
50
13. Cool CD, Groshong SD, Oakey J, Voelkel NF. Pulmonary hypertension: cellular and molecular mechanisms. Chest. Dec 2005;128(6 Suppl):565S‐571S.
14. Farber HW, Loscalzo J. Pulmonary arterial hypertension. The New England journal of medicine. Oct 14 2004;351(16):1655‐1665.
15. Fischer LG, Van Aken H, Burkle H. Management of pulmonary hypertension: physiological and pharmacological considerations for anesthesiologists. Anesthesia and analgesia. Jun 2003;96(6):1603‐1616.
16. Flick RP, Sprung J, Harrison TE, et al. Perioperative cardiac arrests in children between 1988 and 2005 at a tertiary referral center: a study of 92,881 patients. Anesthesiology. Feb 2007;106(2):226‐237; quiz 413‐224.
17. Friesen RH, Williams GD. Anesthetic management of children with pulmonary arterial hypertension. Paediatric anaesthesia. Mar 2008;18(3):208‐216.
18. Haworth SG. The management of pulmonary hypertension in children. Archives of disease in childhood. Jul 2008;93(7):620‐625.
19. Heath D, Edwards JE. The pathology of hypertensive pulmonary vascular disease; a description of six grades of structural changes inthe pulmonary arteries with special reference to congenital cardiac septal defects. Circulation. Oct 1958;18(4 Part 1):533‐547.
20. Hickey PR, Hansen DD, Cramolini GM, Vincent RN, Lang P. Pulmonary and systemic hemodynamic responses to ketamine in infants with normal and elevated pulmonary vascular resistance. Anesthesiology. Mar 1985;62(3):287‐293.
21. Hickey PR, Hansen DD, Strafford M, Thompson JE, Jonas RE, Mayer JE. Pulmonary and systemic hemodynamic effects of nitrous oxide in infants with normal and elevated pulmonary vascular resistance. Anesthesiology. Oct 1986;65(4):374‐378.
22. Hickey PR, Hansen DD, Wessel DL, Lang P, Jonas RA. Pulmonary and systemic hemodynamic responses to fentanyl in infants. Anesthesia and analgesia. May 1985;64(5):483‐486.
23. Hickey PR, Hansen DD, Wessel DL, Lang P, Jonas RA, Elixson EM. Blunting of stress responses in the pulmonary circulation of infants by fentanyl. Anesthesia and analgesia. Dec 1985;64(12):1137‐1142.
24. HumbertM, Morrell NW, Archer SL, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. Journal of the American College of Cardiology. Jun 16 2004;43(12 Suppl S):13S‐24S.
25. HumbertM, Sitbon O, SimonneauG. Treatment of pulmonary arterial hypertension. The New England journal of medicine. Sep 30 2004;351(14):1425‐1436.
26. Ivy D. Advances in pediatric pulmonary arterial hypertension. Current opinion in cardiology. Mar 2012;27(2):70‐81.
27. MacKnight B, Martinez EA, Simon BA. Anesthetic management of patients with pulmonary hypertension. Seminars in cardiothoracic and vascular anesthesia. Jun 2008;12(2):91‐96.
28. MacNee W. Pathophysiology of cor pulmonale in chronic obstructive pulmonary disease. Part two. American journal of respiratory and critical care medicine. Oct 1994;150(4):1158‐1168.
29. MacNee W. Pathophysiology of cor pulmonale in chronic obstructive pulmonary disease. Part One. American journal of respiratory and critical care medicine. Sep 1994;150(3):833‐852.
51
30. McLaughlin VV, McGoonMD. Pulmonary arterial hypertension. Circulation. Sep 26 2006;114(13):1417‐1431.
31. Morray JP, Geiduschek JM, Ramamoorthy C, et al. Anesthesia‐related cardiac arrest in children: initial findings of the Pediatric Perioperative Cardiac Arrest (POCA) Registry. Anesthesiology. Jul 2000;93(1):6‐14.
32. Nef HM, MollmannH, Hamm C, Grimminger F, Ghofrani HA. Pulmonary hypertension: updated classification and management of pulmonary hypertension. Heart. Apr 2010;96(7):552‐559.
33. Penaloza D, Arias‐Stella J. The heart and pulmonary circulation at high altitudes: healthy highlanders and chronic mountain sickness. Circulation. Mar 6 2007;115(9):1132‐1146.
34. Price LC, Wort SJ, Finney SJ, Marino PS, Brett SJ. Pulmonary vascular and right ventricular dysfunction in adult critical care: current and emerging options for management: a systematic literature review. Crit Care. 2010;14(5):R169.
35. Rashid A, Ivy D. Severe paediatric pulmonary hypertension: new management strategies. Archives of disease in childhood. Jan 2005;90(1):92‐98.
36. Rich JD, Shah SJ, Swamy RS, Kamp A, Rich S. Inaccuracy of Doppler echocardiographic estimates of pulmonary artery pressures in patients with pulmonary hypertension: implications for clinical practice. Chest. May 2011;139(5):988‐993.
37. Rudolph AM, Yuan S. Response of the pulmonary vasculature to hypoxia and H+ ion concentration changes. The Journal of clinical investigation. Mar 1966;45(3):399‐411.
38. Shukla AC, AlmodovarMC. Anesthesia considerations for children with pulmonary hypertension. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.Mar 2010;11(2 Suppl):S70‐73.
39. Strumpher J, Jacobsohn E. Pulmonary hypertension and right ventricular dysfunction: physiology and perioperative management. Journal of cardiothoracic and vascular anesthesia. Aug 2011;25(4):687‐704.
40. Taylor CJ, Derrick G, McEwan A, Haworth SG, SuryMR. Risk of cardiac catheterization under anaesthesia in children with pulmonary hypertension. British journal of anaesthesia. May 2007;98(5):657‐661.
41. Williams GD, Jones TK, Hanson KA, Morray JP. The hemodynamic effects of propofol in children with congenital heart disease. Anesthesia and analgesia. Dec 1999;89(6):1411‐1416.
42. Williams GD, Maan H, Ramamoorthy C, et al. Perioperative complications in children with pulmonary hypertension undergoing general anesthesia with ketamine. Paediatric anaesthesia. Jan 2010;20(1):28‐37.
43. Williams GD, Philip BM, Chu LF, et al. Ketamine does not increase pulmonary vascular resistance in children with pulmonary hypertension undergoing sevoflurane anesthesia and spontaneous ventilation. Anesthesia and analgesia. Dec 2007;105(6):1578‐1584, table of contents.
44. Wolfe RR, Loehr JP, Schaffer MS, Wiggins JW, Jr. Hemodynamic effects of ketamine, hypoxia and hyperoxia in children with surgically treated congenital heart disease residing greater than or equal to 1,200 meters above sea level. The American journal of cardiology. Jan 1 1991;67(1):84‐87.
52
Twite, Mark, MA, MB, BChir, FRCP CRASH 2015: Pulmonary Hypertensive Crisis