disease surveillance & registries
TRANSCRIPT

1
นพ.นวนรรน ธีระอัมพรพันธ์ุภาควิชาเวชศาสตร์ชุมชน คณะแพทยศาสตร์ รพ.รามาธิบดี 27 เม.ย. 2559
โอกาสพัฒนาระบบเฝ้าระวังโรคและ Disease Registry
www.SlideShare.net/Nawanan
2
2003 Doctor of Medicine (1st-Class Honors) Ramathibodi
2009 M.S. (Health Informatics) University of Minnesota
2011 Ph.D. (Health Informatics) University of Minnesota
ต ำแหน่งปัจจุบัน• อาจารย์ ภาควิชาเวชศาสตร์ชุมชน
คณะแพทยศาสตร์โรงพยาบาลรามาธิบดีContacts
E-mail [email protected]/NawananFacebook: Informatics RoundLine ID: NawananT
A Brief Introduction
3
• Data Problems in Disease Control• Science of Data & Information• Health IT in Clinical & Public Health Settings• Data Collection & Use• Thailand’s “eHealth” Situation• Creating Health Information Systems of
Tomorrow
Outline
4
คุณเคยเจอปัญหาเหล่านี้บ้างหรือไม่?
5
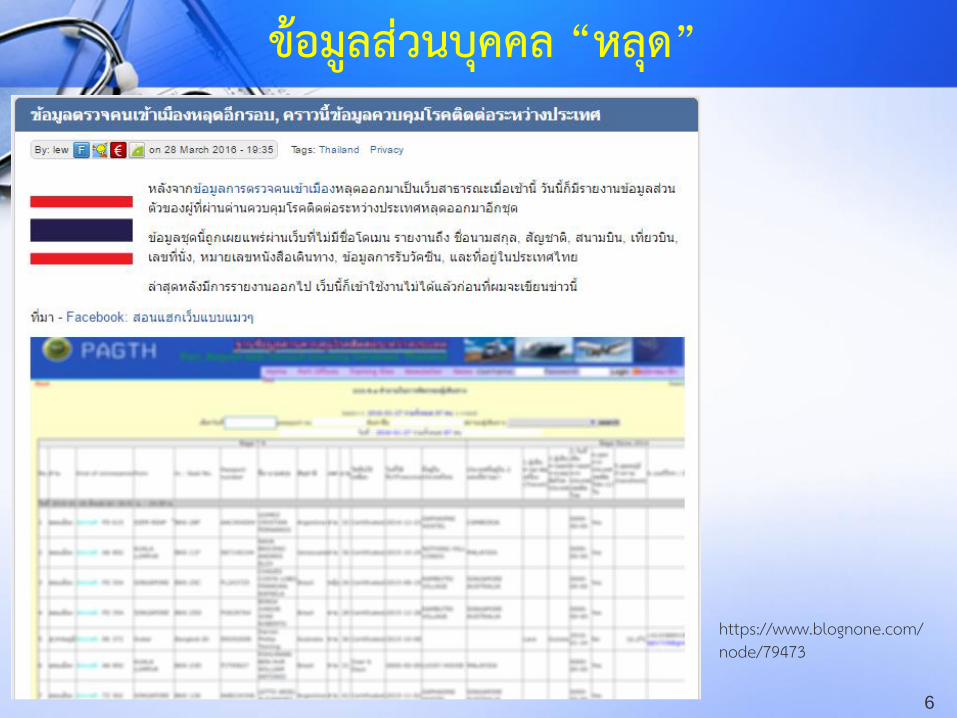
• ผู้บริหารขอรายงานข้อมูลกะทนัหัน• ผู้ใช้งานบ่น ภาระงานเยอะ บันทึกซ้้าซ้อน• Data-rich, information-poor (& wisdom-none)• ข้อมูลจาก 2 แหล่ง ไม่ตรงกัน• 2 โปรแกรมคุยกันไม่รู้เรื่อง• คนถือข้อมูล “หวง” ข้อมูล ไม่ยอมแชร์• ข้อมูลที่แชร์ไปให้หน่วยงานอื่น “หลุด”
คุณเคยเจอปัญหาเหล่านี้บ้างหรือไม่?
6
https://www.blognone.com/node/79473
ข้อมูลส่วนบุคคล “หลุด”
7
• ผู้เกี่ยวข้องเข้าใจ “ศาสตร”์ ของข้อมูลสารสนเทศ
• หลายปัญหามีทางออก แต่ต้องหันหน้าเข้าหากัน– ผู้บริหาร ผู้ใช้ข้อมูล ผู้ถือข้อมูล นักไอที และ
นักวิชาการ
ปัญหาเหล่านี้จะหมดไป ถ้า...

8
• ขาด “การออกแบบ” ระบบข้อมูลที่ดี• ขาดความเข้าใจเรื่อง “ข้อมูล” และ “ระบบ
ข้อมูล/ระบบสารสนเทศ”• ผู้บริหารมองเรื่องนี้เป็นเรื่อง “เทคนิค”• User มองเรื่องนี้เป็นเรื่อง “ไอที” แทนที่จะมอง
เป็นเรื่อง “ข้อมูล” (ในงานของตัวเอง)• ขาด “การจัดการ” ข้อมูลสารสนเทศที่ดี
สาเหตุบางส่วนของปัญหาเหล่านี้

9
“ศาสตร์” ของข้อมูลสารสนเทศ
(Science of Data & Information)

10
• French: informatique = the science and technology of information processing using computers (Greenes & Shortliffe, 1990)
• “[T]he discipline focused on the acquisition, storage, and use of information in a specific setting or domain” (Hersh, 2009)
• “[T]he science of information”(Bernstam et al, 2010)
What is “Informatics”
11
• “Ancient” term
• Being retired
• Future use discouraged by experts
• Only retained in titles of professional organizations
Main Problems
• Medical = Doctor? (e.g. not nursing?)
• Medical informatics vs. Clinical informatics
Medical Informatics

12
• Biomedical informatics• Health informatics• Biomedical and Health informaticsA Few Subtleties• Health informatics suggests the goal is “health”• Health informatics vs. Public health informatics• Health informatics includes Bioinformatics?• No clear winner between
Biomedical informatics vs. Health informatics
Better Terms

13
• Medical computing/computers in medicine?• ‘[R]eferring to biomedical informatics as
“computers in medicine” is like defining cardiology as “stethoscopes in medicine”.’ (Bernstam et al, 2010)
• “[T]he field concerned with the cognitive, information processing, and communication tasks of medical practice, education, and research, including the information science and technology to support these tasks” (Greenes & Shortliffe, 1990)
But What Is M/B/H Informatics Anyway?

14
• “[T]he field that is concerned with the optimal use of information, often aided by the use of technology, to improve individual health, health care, public health, and biomedical research” (Hersh, 2009)
• “[T]he application of the science of informationas data plus meaning to problems of biomedical interest” (Bernstam et al, 2010)
More Definitions of M/B/H Informatics
15
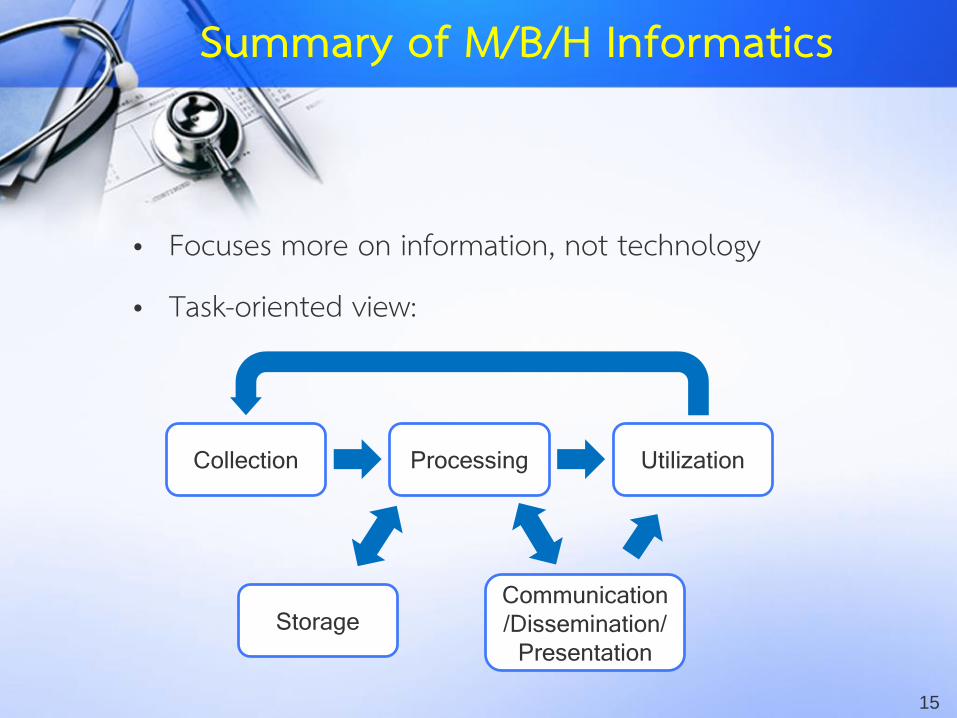
• Focuses more on information, not technology
• Task-oriented view:
Collection Processing
Storage
Utilization
Communication
/Dissemination/
Presentation
Summary of M/B/H Informatics

16
• Health service delivery (health care)– Medical, dental, nursing, pharmacy, etc.– IT management in health care organizations
• Public health– Policy & administration, epidemiology, environmental
health, health services research, etc.• Individual patient/consumer’s health• Education of health professionals• Biomedical research (clinical trials, public health
research, research in biomedical sciences)
Areas Under M/B/H Informatics

17
Data-Information-Knowledge-Wisdom
(DIKW) Pyramid
So What Is Information?
Wisdom
Knowledge
Information
Data

18
Data-Information-Knowledge-Wisdom (DIKW) Pyramid
Contextualization/
Interpretation
Processing/
Synthesis/
Organization
JudgmentWisdom
Knowledge
Information
Data100,000,000
19
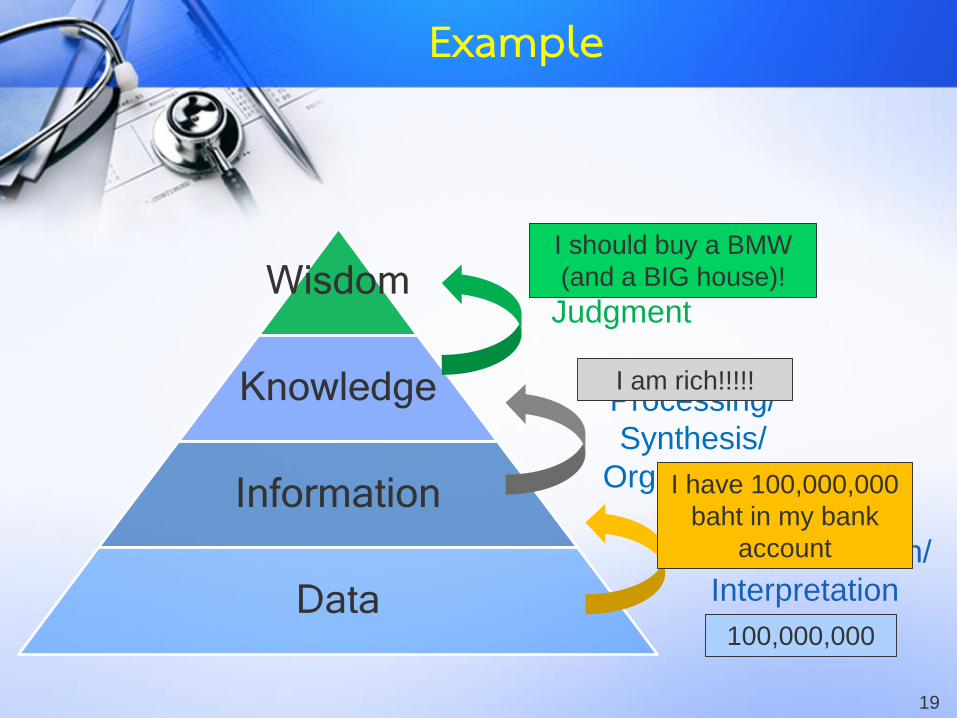
Contextualization/
Interpretation
Processing/
Synthesis/
Organization
JudgmentWisdom
Knowledge
Information
Data100,000,000
I have 100,000,000
baht in my bank
account
I am rich!!!!!
I should buy a BMW
(and a BIG house)!
Example
20
Class Exercise #1

21
• Patient A is allergic to penicillin. He was recently prescribed amoxicillin for his sore throat.
• What are data, information, knowledge, and wisdom?
Class Exercise #1: Case A

22
• Hospital B received complaints from many patients about poor service of providers in the OPD.
• What kind of data & information do you need, and for what knowledge & wisdom?
Class Exercise #1: Case B

23
http://www.nationtv.tv/main/content/social/378498782/
Class Exercise #1: Case C
• As a disease control officer responsible for rabies, what data & information do you need? Why? What knowledge & wisdom do you wish to have?

24
• Patient A is allergic to penicillin. He was recently prescribed amoxicillin for his sore throat.
• What are data, information, knowledge, and wisdom?
Class Exercise #1: Case A

25
• Patient A is allergic to penicillin. He was recently prescribed amoxicillin for his sore throat.
• Data: Penicillin, amoxicillin, sore throat
• Information:– Patient A has penicillin allergy
– Patient A was prescribed amoxicillin for his sore throat
• Knowledge:– Patient A may have allergic reaction to his prescription
• Wisdom:– Patient A should not take amoxicillin!!!
Class Exercise #1: Case A

26
• Hospital B received complaints from many patients about poor service of providers in the OPD.
• What kind of data & information do you need, and for what knowledge & wisdom?
Class Exercise #1: Case B

27
http://www.nationtv.tv/main/content/social/378498782/
Class Exercise #1: Case C
• As a disease control officer responsible for rabies, what data & information do you need? Why? What knowledge & wisdom do you wish to have?

28
• “[T]he field that is concerned with the optimal use of information, often aided by the use of technology, to improve individual health, health care, public health, and biomedical research” (Hersh, 2009)
• “[T]he application of the science of informationas data plus meaning to problems of biomedical interest” (Bernstam et al, 2010)
Back to the Definitions
Informatics focuses on “I”, not “T”
29
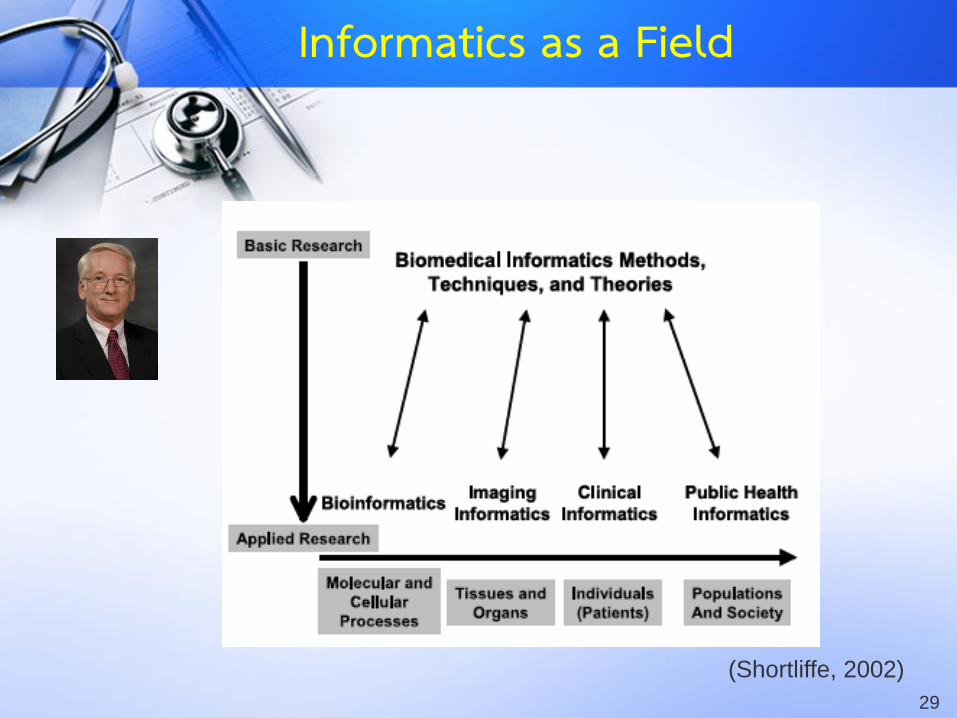
(Shortliffe, 2002)
Informatics as a Field

30
(Hersh, 2009)
Informatics as a Field

31
Biomedical/Health
Informatics
Computer & Information
Science
Engineering
Cognitive & Decision Science
Social Sciences
(Psychology, Sociology, Linguistics,
Law & Ethics)
Statistics & Research Methods
Medical Sciences &
Public Health
Management
Library Science,
Information Retrieval,
KM
And More!
Informatics and Other Fields
32
(Theera-Ampornpunt, 2015)
Informatics as a Field
tmi.or.th/jtmi/

33
Health IT in Clinical & Public Health Settings

34
To treat & to care for their patients to their best abilities,given limited time & resources
Image Source: http://en.wikipedia.org/wiki/File:Newborn_Examination_1967.jpg (Nevit Dilmen)
What Clinicians Want

35
• Safe
• Timely
• Effective
• Patient-Centered
• Efficient
• Equitable
Institute of Medicine, Committee on Quality of Health Care in America. Crossing the quality
chasm: a new health system for the 21st century. Washington, DC: National Academy
Press; 2001. 337 p.
High Quality Care
36
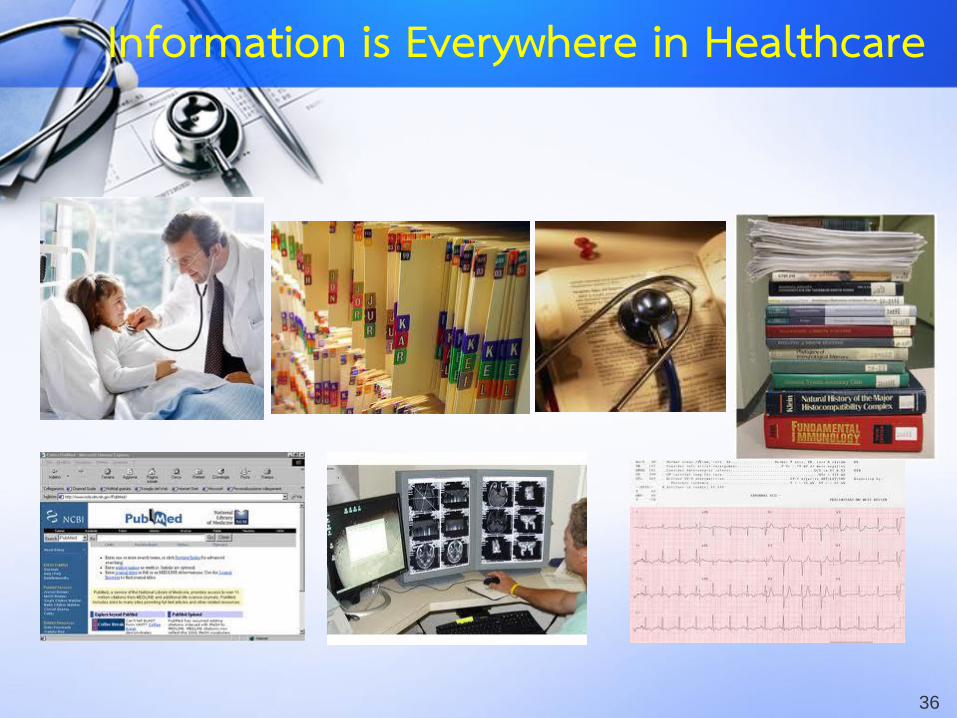
Information is Everywhere in Healthcare

37
Shortliffe EH. Biomedical informatics in the education of physicians. JAMA.
2010 Sep 15;304(11):1227-8.
“Information” in Medicine
38
38
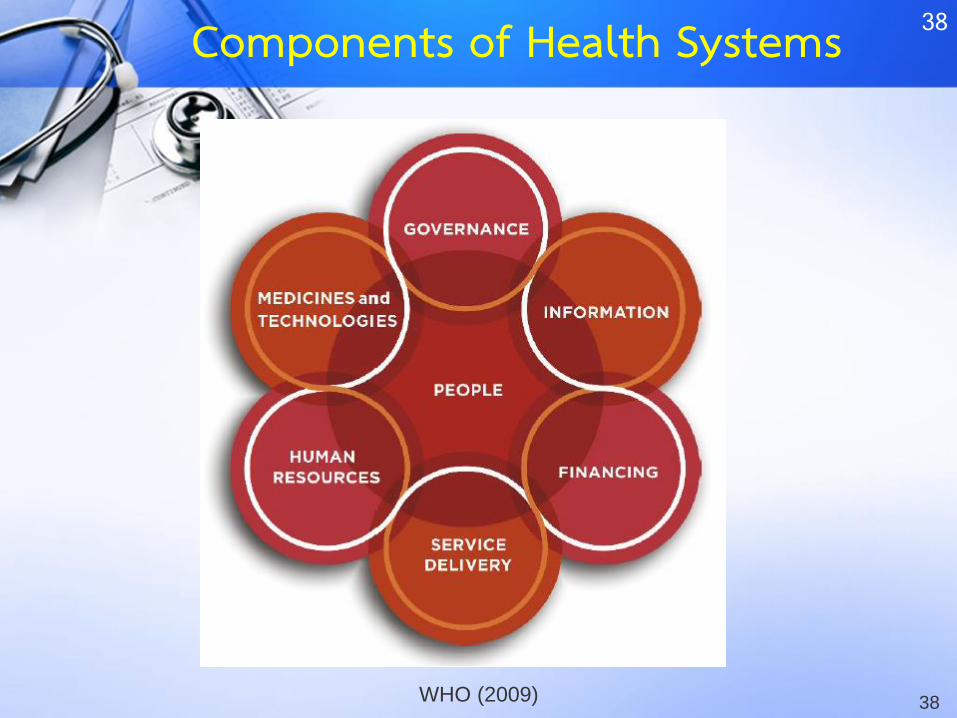
WHO (2009)
Components of Health Systems
39
39
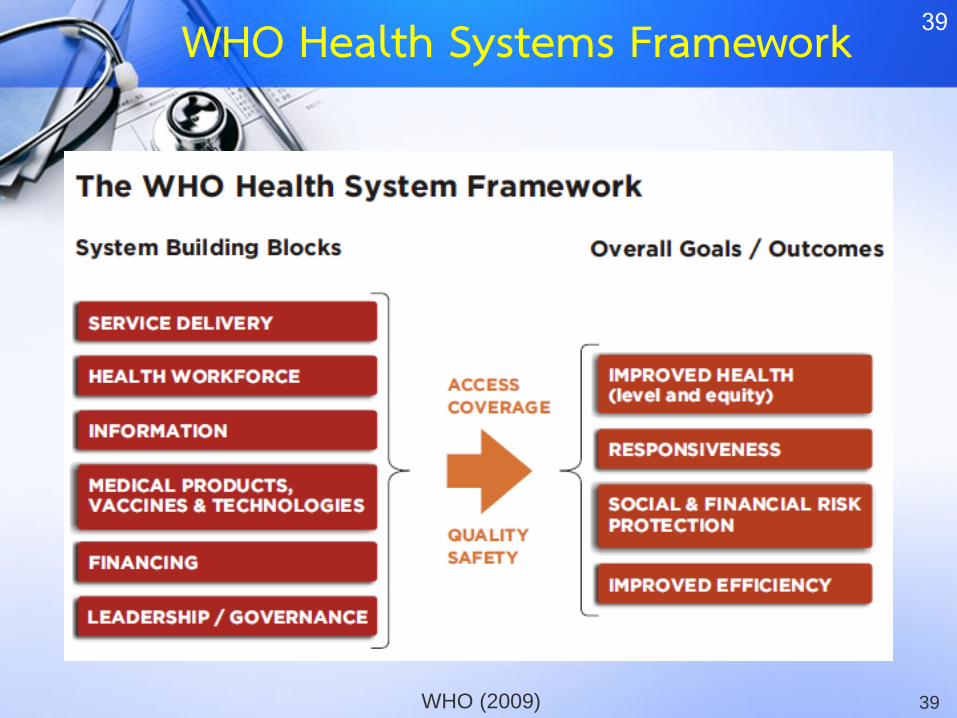
WHO (2009)
WHO Health Systems Framework

40
(IOM, 2001)(IOM, 2000) (IOM, 2011)
Landmark Institute of Medicine Reports

41
• To Err is Human (IOM, 2000) reported that:
– 44,000 to 98,000 people die in U.S. hospitals each year as a result of preventable medical mistakes
– Mistakes cost U.S. hospitals $17 billion to $29 billion yearly
– Individual errors are not the main problem
– Faulty systems, processes, and other conditions lead to preventable errors
Health IT Workforce Curriculum Version
3.0/Spring 2012 Introduction to Healthcare and Public Health in the US: Regulating Healthcare - Lecture d
Patient Safety
42
• Humans are not perfect and are bound to make errors
• Highlight problems in U.S. health care system that systematically contributes to medical errors and poor quality
• Recommends reform
• Health IT plays a role in improving patient safety
Institute of Medicine Reports Summary
43Image Source: (Left) http://docwhisperer.wordpress.com/2007/05/31/sleepy-heads/
(Right) http://graphics8.nytimes.com/images/2008/12/05/health/chen_600.jpg
To Err is Human 1: Attention

44Image Source: Suthan Srisangkaew, Department of Pathology, Facutly of Medicine Ramathibodi Hospital
To Err is Human 2: Memory
45
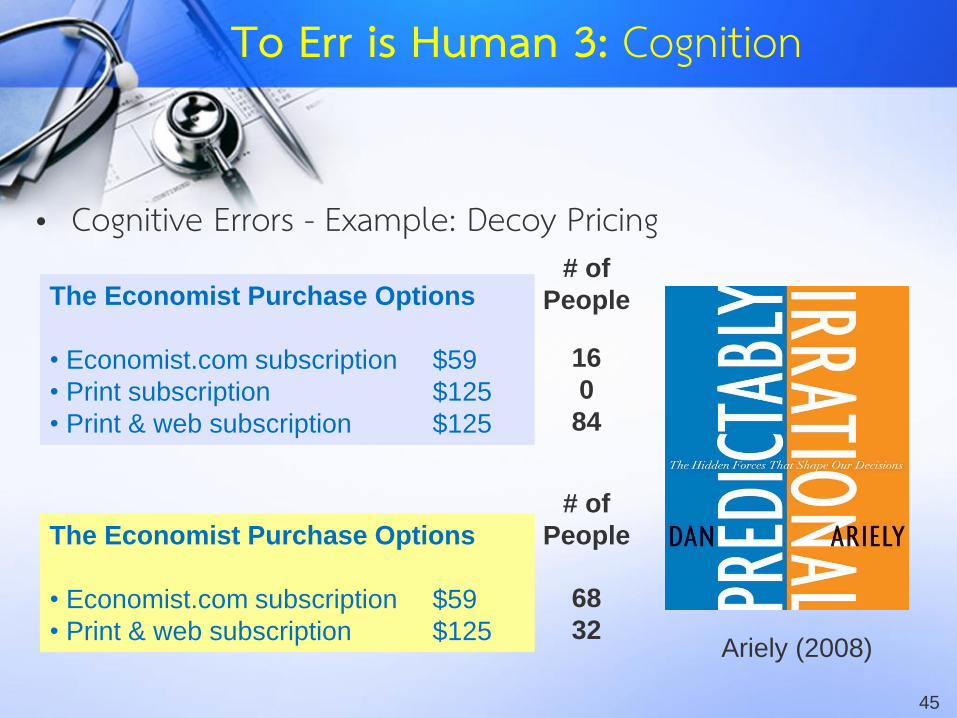
• Cognitive Errors - Example: Decoy Pricing
The Economist Purchase Options
• Economist.com subscription $59
• Print subscription $125
• Print & web subscription $125
Ariely (2008)
16
0
84
The Economist Purchase Options
• Economist.com subscription $59
• Print & web subscription $125
68
32
# of
People
# of
People
To Err is Human 3: Cognition

46
• It already happens....(Mamede et al., 2010; Croskerry, 2003; Klein, 2005; Croskerry, 2013)
What If This Happens in Healthcare?

47
Mamede S, van Gog T, van den Berge K, Rikers RM, van Saase JL, van Guldener C,
Schmidt HG. Effect of availability bias and reflective reasoning on diagnostic accuracy
among internal medicine residents. JAMA. 2010 Sep 15;304(11):1198-203.
Cognitive Biases in Healthcare

48
Croskerry P. The importance of cognitive errors in diagnosis and strategies to minimize them.
Acad Med. 2003 Aug;78(8):775-80.
Cognitive Biases in Healthcare
49
Klein JG. Five pitfalls in decisions about diagnosis and prescribing. BMJ. 2005 Apr
2;330(7494):781-3.
“Everyone makes mistakes. But our reliance on cognitive processes prone to bias makes treatment
errors more likely than we think”
Cognitive Biases in Healthcare
50
• Medication Errors
– Drug Allergies
– Drug Interactions
• Ineffective or inappropriate treatment
• Redundant orders
• Failure to follow clinical practice guidelines
Common Errors in Clinical Practice

51
Why We Need ICT
in Healthcare?
#1: Because information is
everywhere in healthcare

52
Why We Need ICT
in Healthcare?
#2: Because healthcare is
error-prone and technology
can help

53
Why We Need ICT
in Healthcare?
#3: Because access to
high-quality patient
information improves care

54
Why We Need ICT
in Healthcare?
#4: Because healthcare at all
levels is fragmented &
in need of process improvement

55
Health
Information
Technology
Goal
Value-Add
Tools
Health IT: What’s in a Word?

56
Hospital A Hospital B
Clinic C
Government
Lab Patient at Home
Health Information Exchange
57
• Health IT for Consumers/Patients– Personal Health Records
– Telemedicine
– Web Sites for Patient Education & Engagement
– mHealth & Social Media
Images from HealthVault.com, American Telecare, Inc. & WHO
Health IT Beyond Hospitals & Clinics

58
• eHealth & mHealth– mHealth in disaster management: #ThaiFlood
• Data reporting to government agencies– Claims & reimbursements– Diseases– Utilization statistics– Quality measures– Such as MoPH’s Health Data Centers (HDC) reports
• Biosurveillance / Disease Surveillance (active vs. passive; case reporting vs. predictive)
• Epidemiologic & health services research
Other IT for Public Health
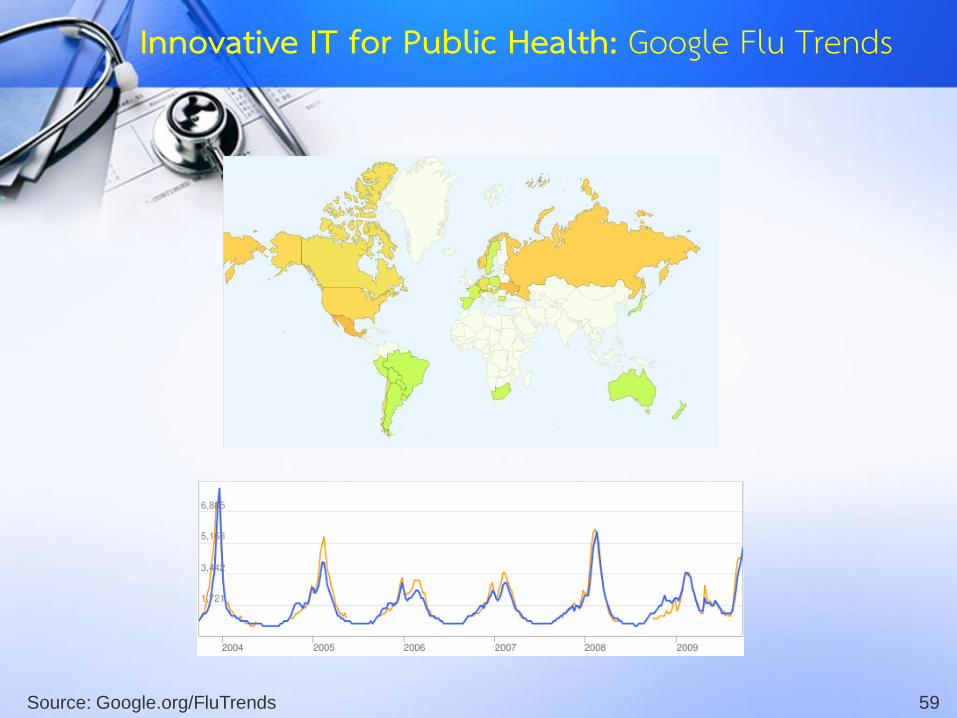
59Source: Google.org/FluTrends
Innovative IT for Public Health: Google Flu Trends

60Source: www.biophics.org
Thailand’s Disease Surveillance

61Image Source: https://en.wikipedia.org/wiki/United_Nations_Security_Council_Resolution_1540
Credits: Wikimedia Commons, User:Andux, User;Vardion, and Simon Eugster
Global Threats: Bioterrorism
62
• eHealth & mHealth– mHealth in disaster management: #ThaiFlood
• Data reporting to government agencies– Claims & reimbursements– Diseases– Utilization statistics– Quality measures– Such as MoPH’s Health Data Centers (HDC) reports
• Biosurveillance / Disease Surveillance (active vs. passive; case reporting vs. predictive)
• Epidemiologic & health services research
Other IT for Public Health

63
IT for Public Health
Shortliffe EH, Cimino JJ, editors. Biomedical Informatics: Computer Applications in Health Care and Biomedicine. 3rd ed. New York: Springer; 2006. 1037 p.
http://www.amazon.com/Biomedical-Informatics-Computer-Applications-Biomedicine/dp/0387289860/

64
IT for Public Health
Shortliffe EH, Cimino JJ, editors. Biomedical Informatics: Computer Applications in Health Care and Biomedicine. 3rd ed. New York: Springer; 2006. 1037 p.
http://www.amazon.com/Biomedical-Informatics-Computer-Applications-Biomedicine/dp/0387289860/
Disease Surveillance & Registries
Consumer Health IT, Websites, mHealth, Social Media
Data Reporting for
Planning & Evaluation

65
• Key Issues– Interdisciplinary Communications– Organizational and Collaborative Issues– Funding and Sustainability– System Design
Example: Immunization Registries
66
Data Collection & Use

67
Quantitative Data/Information/Knowledge
Qualitative Data/Information/Knowledge
Types of Data/Information/Knowledge
68
Use of data for the purpose originally intended when collecting data, such as Use of hospital’s patient data for treatment &
patient care
Use of disease surveillance data for outbreak monitoring, investigation & control
Use of research data for analysis & reporting
Primary Use of Data
69
Use of data for other purposes other than primary use, such as
Use of patient care data for education & research
Use of hospital’s patient data for reimbursements, quality improvement, or other management activities
Use of patient care data for public health activities (disease surveillance, evaluation, policy-making, regulation/auditing, etc.)
Use of research data collected in one study for other studies
Secondary Use of Data

70
• Operational Information System– Clinical: Hospital Information Systems, Electronic Medical
Records, Health Information Exchange (HIE), etc.
– Public Health: Disease Surveillance, Disease Registries, HIE
• Management Information Systems– Clinical: Hospital’s Data Warehouse & Reporting Systems
– Public Health: Disease Surveillance, Disease Registries, Data Warehouse & Reporting Systems & Business Intelligence
Types of Health Information Systems

71
Inefficiencies: Costs, time & effort associated with primary data collection
Data Quality: Duplicated & inconsistent data
Burden on data informants/custodians
Primary Use of Data: Issues

72
Privacy: Is sharing/disclosure/reuse of data originally collected for other purposes allowed/appropriate/legal? (“หวงข้อมูล”, “ละเมิดสิทธิ”)
Changes in context -> unaware changes in meaning -> incorrect interpretation of data
Obtaining data & integrating data from multiple sources
Data standardization
Secondary Use of Data: Issues
73
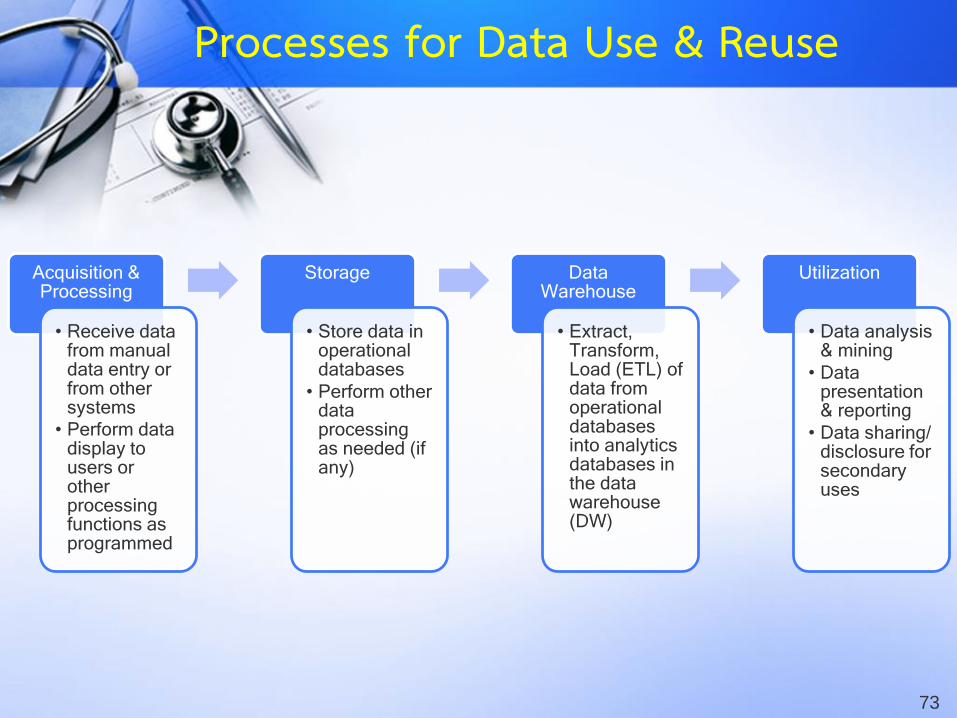
Acquisition & Processing
• Receive data from manual data entry or from other systems
• Perform data display to users or other processing functions as programmed
Storage
• Store data in operational databases
• Perform other data processing as needed (if any)
Data Warehouse
• Extract, Transform, Load (ETL) of data from operational databases into analytics databases in the data warehouse (DW)
Utilization
• Data analysis & mining
• Data presentation & reporting
• Data sharing/disclosure for secondary uses
Processes for Data Use & Reuse

74Image Source: http://www.hiso.or.th/dashboard/
Data Reporting Systems

75Image Source: http://www.inetsoft.com/business/solutions/applying_business_intelligence_to_manufacturing/
Business Intelligence
76Image Source: https://www.sas.com/technologies/bi/entbiserver/
Business Dashboards

77
Practical Guides on Data Management &
Reporting
78
What?
Where?
From Whom?
How?
Action!
Now What?
Guides for Data Collection & Use
79
Step 1: Identify data elements needed for a specific project (“What?”)What are data, information, knowledge & wisdom we
want from the project?
What is the scope (geographic location, timeframe, population, disease, clinical setting, etc.)?
Guides for Data Collection & Use

80
Step 2: Identify potential sources for needed data (“Where?”)
Data quality: completeness, accuracy, validity & reliability
Data quality closer to the source generally has better quality
Collecting primary data is more expensive
Two copies of data will often lead to inconsistencies
Are these sources manual or electronic data? What are pros & cons for each source?
Sometimes, paper records can’t be avoided (don’t aim for paperless, but rather less paper)
Guides for Data Collection & Use

81
Validity & Reliability
Image Source: https://commons.wikimedia.org/wiki/File:Reliability_and_validity.svg (© Nevit Dilmen)

82
Systematic Errors (Biases) Selection Bias
Information Bias / Misclassification
Confounding
Threats to Validity
83
Random Errors Sampling Errors
Random measurement errors
Threats to Reliability

84
Step 3: Determine if primary or secondary use of data is more feasible & appropriate (“From Whom?”) Check if there are legal, privacy, policy & technical concerns
for obtaining data for secondary uses
Management/administrative data should ideally be by-product of well-designed operational/clinical data
Be aware of context/meaning when data were collected (loss of context and potential misinterpretations are easy if attention is not paid to context)
Guides for Data Collection & Use

85
Step 4: Plan how to collect data (“How?”) Primary Data: Plan procedures & resources needed for data collection
Secondary Data: Discuss with data custodian & make arrangements for obtaining data (if necessary, go back to Steps 2-3)
Use standard data format if possible, especially if integrating data from multiple sources
If multiple sources are available on same data, choose best one
Document the data collection process, technical procedures, and relevant metadata (data about data)
Guides for Data Collection & Use
86
Step 5: Collect data & perform data analysis/use (“Action!”) Data validation, cleaning, preparation & transformation
Executive data collection as planned
Revisit previous steps if facing challenges in data collection
Perform analysis/use & verify/validate results
Interpret data/information to yield knowledge
What’s Next: Convert knowledge into wisdom & actions
Guides for Data Collection & Use

87
Step 6: Maintenance (“Now What?”) Pay attention to security, privacy, and disclosure for data in custody
Data custodian is legally responsible for unauthorized access, disclosure, and use
Once project is over and data no longer need to be maintained, destroy them securely
For long-term or ongoing data uses, consider implementing DW, BI, or other appropriate tools Expertise & technical knowledge required
Guides for Data Collection & Use

88
Step 6 (Continued): Periodically check for following changes to determine if changes/updates
are necessary Business processes IT environment Data structure Collection processes Context & meaning Data needs Etc.
Evaluation & continuing improvements
Guides for Data Collection & Use
89
Thailand’s eHealth Situation

90
WHO ITU. National eHealth strategy toolkit. Geneva, Switzerland: 2012.
Components of eHealth (WHO-ITU)
91
Kijsanayotin B, Kasitipradith N, Pannarunothai S. eHealth in Thailand:
the current status. Stud Health Technol Inform. 2010;160(Pt 1):376-80.
Thailand’s eHealth: 2010

92
Str
ate
gy &
In
ve
stm
en
t
Standards & Interoperability
Infrastructure
Services, Applications
Software
Leadership & governance
Le
gis
latio
n, p
olic
y &
co
mp
lian
ce
Wo
rkfo
rce
Thailand’s eHealth: Unbalanced Development
Slide courtesy of Dr. Boonchai Kijsanayotin

93
eHealth Applications
Enabling Policies and Strategies
Foundation Policies and Strategies
Thailand’s eHealth: Shaky Foundations
Slide courtesy of Dr. Boonchai Kijsanayotin

94
ความส้าคัญล้าดับต้นของการพัฒนาระบบข้อมูลข่าวสารสุขภาพ1. มีหน่วยงานระดับประเทศเพื่อวางนโยบาย และก้ากับดูแลการพัฒนา
ระบบข้อมูลข่าวสารสุขภาพของประเทศ2. วางรากฐานด้านมาตรฐานข้อมูลสุขภาพ เพื่อบูรณาการระบบข้อมูล
และเกิดการใช้ และการแลกเปลี่ยนข้อมูลอย่างกว้างขวาง3. มีกฎหมายและระเบียบเกี่ยวกับระบบข้อมูลสุขภาพโดยเฉพาะ4. มีการผลิต และพัฒนาบุคลากรด้านระบบข้อมูลสุขภาพอย่างเป็น
ระบบและเพียงพอ
ข้อเสนอการพัฒนา
Kijsanayotin B, Kasitipradith N, Pannarunothai S. eHealth in Thailand:
the current status. Stud Health Technol Inform. 2010;160(Pt 1):376-80.

95
eHealth Governance
96
Creating Health Information Systems of Tomorrow

97
Winchester Mystery House
Image Source: https://en.wikipedia.org/wiki/Winchester_Mystery_House (© Ben Franske)
98
Winchester Mystery House
https://en.wikipedia.org/wiki/Winchester_Mystery_House
• A mansion in San Jose, California which was once the personal residence of Sarah Winchester, the widow of gun magnate William Wirt Winchester.
• It is privately owned and serves as a tourist attraction.• Renowned for its size & its architectural curiosities.• Construction commenced in 1884

99
Winchester Mystery House
https://en.wikipedia.org/wiki/Winchester_Mystery_House
• Carpenters were hired and worked on the house day and night until it became a 7-story mansion.
• Home contains numerous oddities such as doors and stairs that go nowhere, windows overlooking other rooms and stairs with odd-sized risers.
• No architect was used. Building was added on in a haphazard fashion.
• There was a lack of any master building plan.
100
Architecture
https://en.wikipedia.org/wiki/Winchester_Mystery_House
• มีอะไรใน IT ขององค์กร (หรือของระบบสุขภาพ) ที่คล้ายคลึงกับ Winchester Mystery House หรือไม่?
• เราจะป้องกันปัญหานี้ได้อย่างไร
101
Enterprise Architecture
Federation of EA Professional Organizations, Common Perspectives on Enterprise Architecture, Architecture and Governance Magazine,
Issue 9-4, November 2013 (2013). Retrieved on November 19, 2013. via https://en.wikipedia.org/wiki/Enterprise_architecture
• สถาปัตยกรรมองค์กร (EA) is "a well-defined practice for conducting enterprise analysis, design, planning, and implementation, using a holistic approach at all times, for the successful development and execution of strategy. Enterprise architecture applies architecture principles and practices to guide organizations through the business, information, process, and technology changes necessary to execute their strategies..."

102
• ผู้บริหารขอรายงานข้อมูลกะทนัหัน• ผู้ใช้งานบ่น ภาระงานเยอะ บันทึกซ้้าซ้อน• Data-rich, information-poor (& wisdom-none)• ข้อมูลจาก 2 แหล่ง ไม่ตรงกัน• 2 โปรแกรมคุยกันไม่รู้เรื่อง• คนถือข้อมูล “หวง” ข้อมูล ไม่ยอมแชร์• ข้อมูลที่แชร์ไปให้หน่วยงานอื่น “หลุด”
Enterprise Architecture จะแก้ปัญหาเหล่านี้

103
WHO ITU. National eHealth strategy toolkit. Geneva, Switzerland: 2012.
Components of eHealth (WHO-ITU)

104
Message for LDC Participants
• Focus on the I, not the T, in the word “IT”• Use data to produce value-add (information, knowledge,
wisdom & action!)• There is a science (and experts) of information in health• Various IT applications in clinical & public Health settings• Answers are in the WHO-ITU eHealth model• DDC needs to work with others to “reform” Thailand’s
eHealth