disorders of immunity immunodeficiency diseases. objectives. define immunodeficiency. differentiate...
TRANSCRIPT

Disorders of ImmunityDisorders of Immunity
Immunodeficiency DiseasesImmunodeficiency Diseases
Objectives.
• Define immunodeficiency.
• Differentiate between primary and secondary immunodeficiency.
• List and understand the causes of Pr. Immunodeficiency.
• List and understand the causes of Secondary Immunodeficiency.

Origins of Immunodeficiency
Immunodeficiency diseases are conditions where the defense mechanisms of the host are impaired
Primary or Congenital• Inherited genetic defects in immune cell
development or function, or • Inherited deficiency in a particular immune
molecule Secondary or acquired A loss of previously functional immunity due to
infection, toxicity, radiation, splenectomy, aging, malnutrition, etc.
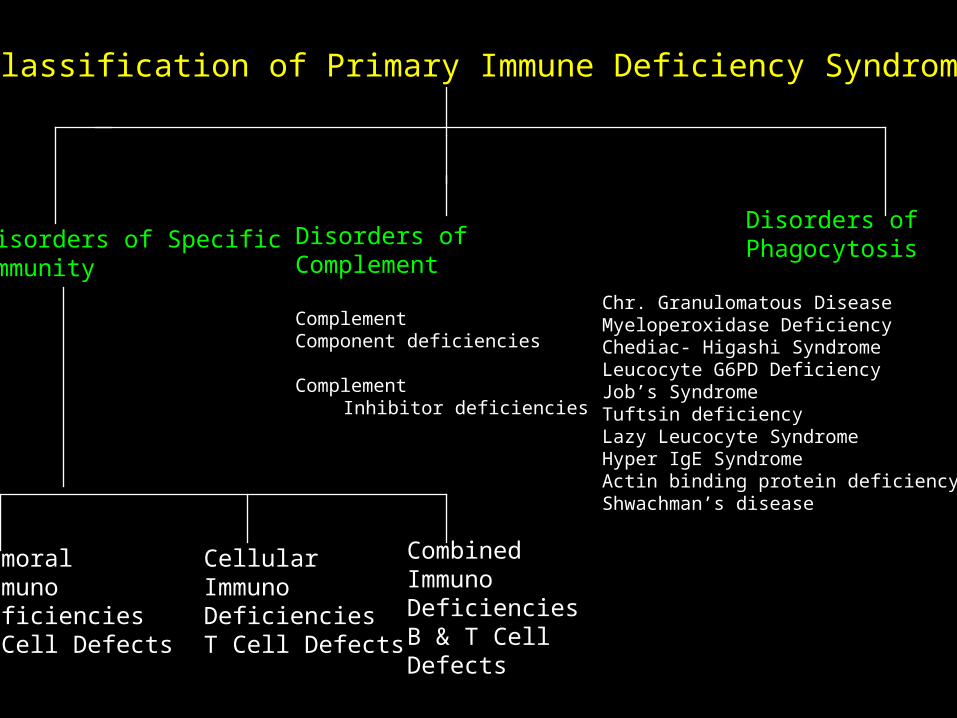
Classification of Primary Immune Deficiency SyndromesClassification of Primary Immune Deficiency Syndromes
Disorders of SpecificImmunity
Disorders ofPhagocytosis
Chr. Granulomatous DiseaseMyeloperoxidase DeficiencyChediac- Higashi SyndromeLeucocyte G6PD DeficiencyJob’s SyndromeTuftsin deficiencyLazy Leucocyte SyndromeHyper IgE SyndromeActin binding protein deficiencyShwachman’s disease
Disorders ofComplement
ComplementComponent deficiencies
Complement Inhibitor deficiencies
HumoralImmunoDeficienciesB Cell Defects
CellularImmunoDeficienciesT Cell Defects
CombinedImmunoDeficienciesB & T CellDefects
Immunodeficiency DiseasesImmunodeficiency Diseases
• Patient unable to fight off infection
• Hall marks– Repeated infections– Opportunistic infections
• Increased susceptibility to tumors

Immunodeficiency DiseasesImmunodeficiency Diseases
• Most are defects in T cells or B cells– T cells, Macrophage defects = Fungal, Viral,
protozoal infections– B cells, Complement defects = Bacterial
infections
Immunodeficiency DiseasesImmunodeficiency Diseases
• Congenital
• Acquired

• These immunodeficiency diseases may involve
Specific immune functions like:• Humoral immunity.• Cell mediated immunity.• Both. OrNon-specific mechanisms like:• Phagocytosis.• Complement.

Humoral immunodeficiencies – B cell defects.
• X- linked agammaglobulinemia.
• Transient hypogammaglobulinemia of infancy.
• Common variable immunodeficiency.
• Selective immunoglobulin deficiencies.
• Immunodeficiency with hyper IgM.
• Transcobalamin II Deficiency.
Cellular immunodeficiency – T cell defects.
• Thymic hypoplasia – DiGeorges Syndrome.
• Purine nucleoside phosphorylase (PNP) deficiency.

Combined immunodeficiency – Both B cell and T cell defects.)
• Cellular immunodeficiency with abnormal immunoglobulin synthesis – (Nezelof’s syndrome.)
• Ataxia telangiectasia.• Wiskott- Aldrich Syndrome.• Immunodeficiency with Thymoma.• Severe combined immunodeficiency.• MHC Class II deficiency.
Disorders of Complement.
• Complement component deficiencies.
• Complement inhibitor deficiencies.

Disorders of Phagocytosis.
• Chronic granulomatous disease.
• Myeloperoxidase deficiency.
• Chediak-Higashi syndrome.
• Leucocyte G-6-PD deficiency.

B- CELL DEFECIENCYX-Linked Agammaglobulinemia – Bruton’s
disease.• First immunodeficiency disease to be
recognised.• A.k.a Bruton’s disease.• Basic defect is in failure of pre-B cells to
differentiate into B cells.• All classes of immunoglobulins are grossly
depleted in the serum.• B-cells in circulation decreased.

• Tonsils, adenoids, lymph nodes are atrophic.• Manifestations are not apparent till 6 months of
age - ???• Patients suffer from recurrent infections with
pyogenic bacteria – Pneumococci, Streptococci, meningococci, Pseudomonas and Hemophilus influenzae.
• T cells are normal hence can handle Viral, fungal and protozoal diseases.

Common variable immunodefeciency.
• A.k.a LATE ONSET HYPOGAMMAGLOBULINEMIA.
• Seen between 15-35 yrs of age.• Characterized by recurrent pyogenic infections.• B-cells normal in number but defective in function.• Increased suppressor T cell and decreased
Helper T cell activity.

Selective Immunoglobulin deficiency.
• Selective deficiency of one or more immunoglobulin class.
• Other classes normal.Selective IgA deficiency:• Total absence of serum and secretory IgA.• Increased susceptibility to respiratory and GIT Infections.• Anti-IgA antibodies are found.Selective IgM deficiency:• Assos with septicemia with meningococci and Gram
Negative bacteria.
Immunodeficiency with Hyper IgM.
• Low levels of IgA, IgG with elevated IgM.
• X-Linked or autosomal reccessive.
• Patients are susceptible to infections and autoimmune disorders such as thrombocytopenia, neutropenia and hemolytic anemia--??
Cellular Immunodeficiency – T cell defects.
• Thymic Hypoplasia – DiGeorges Syndrome.• Developmental defect of the 3rd and 4th pharyngeal
pouches.• Aplasia or hypoplasia of thymus and parathyroid glands.• T-cells are deficient or absent in circulation.• Humoral immunity –normal.• Patients show enhanced susceptibility to viral, fungal
and bacterial infections.• Delayed hypersensitivity and graft rejection are
depressed.

Combined immunodeficiencyBoth B cell and T cell deficincies.
Nezelof’s Syndrome- Cellular immunodeficiency withabnormal immunoglobulin synthesis.• Depressed CMI.• Selectively elevated, decreased or normal
immunoglobulins.• Pts susceptible to viral, fungal and bacterial infections.• Thymus is small and peripheral lymphoid tissues are
atrophic.• Autoimmune conditions like hemolytic anemia are
common.

ATAXIA TELANGIECTASIA
• Autosomal recessive genetic disorder.• Defeciency of cellular and humoral mechanisms.• Assos. With cerebellar ataxia and dilated capillaries
(telagiectasia), ovarian dysgenesis and chromosomal abnormalities.
• Most patients lack IgA and IgE.• Death occurs due to sino-pulmonary infection in early life
or malignancy in the 3rd decade.??• There is impairment of delayed hypersensitivity and graft
rejection.

WISKOTT-ALDRICH SYNDROME
• X-linked reccessive disease.
• Characterised by eczema(elevated IgE), bleeding(thrombocytopenia) and recurrent infections.
• Most affected children die due to bleeding, infection or lymphoreticular malignancy.

SCID --Severe combined immunodeficiency diseases.
• These include many syndromes with severe combined deficiency of both humoral and CMI.
• They are inherited as AUTOSOMAL RECESSIVE MODE.
• There are 3 types of SCID

Swiss type of agammaglobulinemia.• Cause is lymphoid stem cell defects.• Absent humoral and CMI.• Agammaglobulinemia and lymphocytopenia.Reticular dysgenesis.• Most serious type of SCID.• Defect at the level of multi-potent stem cell of bone
marrow.• Failure of myelopoeisis.• Neutropenia, thrombocytopenia, anemia and bone
marrow aplasia.• Fatal in 1st week of life.

Adenosine deaminase deficiency:• In these pts ADA is deficient in all tissues
including RBC’s.• ADA deficiency leads to accumulation of
adenosine and deoxy adenosine triphosphate which are toxic to lymphocytes especially T cells.
• Great loss of T cell function as compared to B cell function.
• Vulnerable to all types of infections.

Complement deficiencies.
• Usually due to genetic abnormalities:
• C3 Def – pyogenic infections.
• C6, C7, C8 – Neisserial infections.
• COMPLEMENT INHIBITOR DEFICIENCY:
• C1 Inhibitor deficiency – hereditary angioneurotic edema.

Phagocyte Deficiencies
• Chronic Granulomatous Disease
– NADPH oxidase defect
• Chediak -Higashi Syndrome
– Abnormal lysosome formation
• Leukocyte Adhesion Deficiency
– Absence of leukocyte adhesion molecules

Immunodeficiency
• Primary Immunodeficiency– Neutrophil defects: CGD
– Humoral: B cell defects
– Humoral: Complement
– Cell-mediated: T cells
– Severe combined immunodeficiency
• Secondary Immunodeficiency– AIDS
– Neutropenia• Post-transplant
• BMT
• chemotherapy
– Splenectomised patient
– Malnutrition.
– Anti-cancer chemotherapy.
– Radiation therapy.

Primary ImmunodeficiencyPathogens
• Humoral defects– Capsulated bacteria
• S. pneumoniae
• H. influenzae
• N. meningitidis
• S. aureus
– Enteroviruses
– mycoplasma
• Cell-mediated– intracellular bacteria
• Mycobacteria, Salmonella, Listeria, Legionella
– Viruses• Herpes, Respiratory &
Enteric viruses
– Fungi & protozoa• Candida, Aspergillus,
Pneumocystis, Cryptococcus, Cryptosporidium, Toxoplasma
• Neutrophil defects– S. aureus, Candida,
Aspergillus

Immune Deficiency TherapiesImmune Deficiency Therapies
• B-cell deficiency : Gamma globulin
• SCID : Bone marrow transplant, enzyme replacement
• DiGeorge’s Syndrome : Fetal thymus transplant
• Gene therapy

Inherited Functional DisordersInherited Functional Disorders
• Disorders of Granulocyte Function– Job’s syndrome – directional motility is
impaired – recurrent boils and abscesses– Lazy Leukocyte Syndrome – random and
directed movement are defective – cells fail to respond to inflammatory stimuli – mild symptoms of low grade fever, recurrent infections (gums, mouth, ears)
– Chediak-Higashi – abnormal granule release

Inherited Functional DisordersInherited Functional Disorders
• Congenital C3 deficiency – inability to ingest microorganisms- repeated severe infections with encapsulated bacteria
• Chronic Granulomatous Disease – inability to kill catalase positive organisms – recurrent pyogenic infection
• Leukocyte Glucose-6-Phosphate Dehydrogenase Deficiency – similar to CGD Myeloperoxidase Deficiency-benign – slow bacterial killing, but complete

Monocyte-Macrophage DisordersMonocyte-Macrophage Disorders
• Mucopolysaccharidoses – deficiencies in specific enzymes to degrade mucopolysaccharides (Hurley syndrome, Hunter syndrome: gargoylism)
• Lipidoses: lipid storage diseases – macrophages become overloaded with lipids (Gaucher, Niemann-Pick, Tay-Sachs)