disorders of transepidermal elimination
TRANSCRIPT

Review
Disorders of Transepidermal Elimination
Part 1
THOMAS Y. W O O , M.D., AND IAMES E. RASMUSSEN, M.D.
Transepidermal elimination (TE) is a mechanismwhereby foreign or altered constituents can be re-moved from the dermis. This process involves uniquemorphologic alterations of the epidermis, which formsa channel and thereby facilitates extrusion of thedesired dermal components. The phenomenon of TEmay occur as a primary process characterizing dis-orders, such as elastosis perforans serpiginosa andreactive perforating collagenosis, Occasionally, TEmay occur as a secondary phenomenon. Well-knownexamples are perforating granuloma annuiare andpseudoxanthoma elasticum.
Disorders of Transepidermal Elimination
The human skin is a complex organ in which thedermal and epidermal units function together incomplex cellular interactions in response to variousstimuli. Specifically, many foreign or altered biologicmaterials present in the dermis will incite such Aseries of events aimed at eventual dissolution, isola-tion, or removal of these objects via the epidermis.Dermal "foreign material" may be the consequenceof inflammation, metabolic alterations, neoplastic cells,or external substances.
There are several mechanisms whereby dermalforeign material can be transported to the surface ofthe skin. Mehregan,' a pioneer in this field, differen-tiated three basic categories. In type 1, nonmotilecells such as erythrocytes or small inert particles (eg,hemosiderin) elicit minimal or no dermal reaction.These particles can be trapped between epithelialcells and carried upward to the surface during epi-dermal turnover. In type 2, larger cells, such as motilecells (eg, leukocytes) or organisms such as Treponemapallidum may actively migrate into the epidermal
This is the first in a series of two articles.Address for correspondence: Thomas Y. Woo, M.D., Suite 401,
2681 36th Street, NE, Calgary, Alberta, T1Y 5.53 Canada.
From Ihe Department of Dermatology. Division ofMedicine, University of Calgary I acuity of Medicine,
Calgary, Alberta, Canada and tbe Department ofDermatology, University of Michigan Medical School,
Ann Arbor, Michigan
spaces and hence be carried upward. From the pointof view of the dermis and epidermis, types 1 and 2are relatively passive processes and have been termed"transmigration." This phenomenon is relativelycommon and is often an incidental finding. Once onthe surface, the material is desquamated along withthe adjacent corneocytes.
Type 3, however, involves active epithelial-dermalconnective tissue interaction and is a purposeful,directional mechanism whereby dermal foreign com-ponents are actively eliminated through the epithe-lium. This process was observed by Freudenthai,''who observed small particles of amyloid being ex-pelled through tho epidermis in 1930. Mehreganformulated this phenomenon, termed it "transepi-dermal elimination" (TE), and supported the conceptwith an excellent series of observations of variouspathologic entities.^ He succinctly defined this processas
characterized by varying degrees of pseudoepithplio-matous hyperplasia of the epidermis or follicular epithe-lium. Elongated tongues of newly formed epitheliumextend into the corium surrounding the irritating material.Once the material is partially or completely taken intothe proliferating epithelium, it is slowly moved upwardby the force of maturing keratinocyles and eventuallyeliminated. A continuous flow and elimination of foreignmaterial to the surface will result in formation of multipletransepithelial perforating canals.
The fact that a material was initially present in thedermis and subsequently arrives at the epidermalsurface does not necessarily imply TE. Eor instance,foreign bodies or altered dermal components, whichelicit a strong inflammatory reaction that ultimatelyleads to epithelial necrosis with purulent draining
267

268 INTERNATIONAL lOURNAL OF DERMATOLOGY June 1985 Vol. 24
TABLE 1. Disorders of Tramepidermal Elimination
Disorders in which TE is a constant featureElastosis perforans serpiginosa
PenicillamineOsteogenesis imperfectaMarfan's syndromeEhlers-Danlos syndromeAcrogeriaDown's syndromeCutaneous sclerosis
Reactive perforating collagenosisCollagenome perforant verruciformeChondrodormatrtts noduiaris helicis chronics
Disorders in which TE may occur as a secondary eventGranulomatous disorders
Granuloma annulareNecrobiosis lipoidica diabeticorumRheumatoid noduleSarcoid
Derm<ilnscs wiih calciticatmnPst'udoxdnlhuma elastitumCaktfied tumor of hair follicle originCalcinosis cutisOsteoma cutis
Infectious agentsBotryomycosisSchistosomiasisChromomycosis
OtherLichen nitidusPapuLir mucinosisMelanomaNevo< ellutar nevusPorokeratosis of Mibelli
material through a sinus, does not represent TE. Thesine qua non of this mechanism resides in the factthat the epithelium does not suffer major structuralnitcrations and returns to normal when the processof elimination is temiinated through depletion andexh.iustion of the tiiaterial heing eliminated.
The signal that induces these reactive changes inepidermal architecture is unknown. Both infectiousand noninfectious granulomas, exogenous foreignbodies, and altered dermal components have beenimplicated as ihe inciting event." Regardless of thetype ot material, dose proximity to the epithelium isextremely important; for example, subcutaneousgr.inulomas and deep foreign bodies usually do notinduce epithelial hyperptasia.** This has been dem-onstrated in experitnents by Marks and Schellander,who injected carageenan into different levels of thedermis.'' Material placed below the level oi the hairpapillae did not induce hyperplasia. In contrast,|)la(ement above this zone resulte^d in epidermalproliferation. Thus it appears that in TE elirtiination,the target substance must reside within a certaindermal-epidermal interaction zone.
Diseases that primarily exhibit the phenomenon ofTE are distinct nosologic entities with characteristicclinical morphology, usually an umbilicated papulewith a central core or plug and a unique histologicpresentation. Within the framework of this and asubsequent article, the formulation of this eliminatingmechanism is highlighted and its (haracteristic dis-orders emphasized. Most cogently, elastosis perforansserpiginosa (EPS) and reactive perforating collagenosis(RPC) are elaborated in detail, since these are primarydisorders of TE. In addition, we elaborate on otherentities that secondarily express the phenomenon ofTE, including perforating granuloma annulare; pseu-doxanthoma elasticum; melanoma; nevocellular tie-vus; calcinosis and osteoma cutis; nevus sebaceous;infectious agents, such as botryomycosis, chromo-mycosi5, and schistosomiasis; necrobiosis lipoidica;chondrodermatitis nodularis helicis; papular muci-nosis; tutaneous sclerosis; lichen nitidus; and rheu-matoid nodule (Table I).
Elasfosis Perforans Serpiginosa
History
EPS was initially described by Fisher'' in 1927 in apatient with a circinate papular eruption on the neck.Histopathologic examination revealed a bluish-stainingamorphous plug perforating through the epidermis.At that time, it was thought to be an atypical c:ase ofKyde's disease. Later, Lutz,' in 1953, presented a 21-year-old man with irregulady shaped keratotic ridgescomposecl of closely set nodules present on bothsides of the neck. He assumed the lesions to be ofhair follicle origin and termed them "keratosis follicu-laris serpiginosa."
In 1955, Miescher presented a classical descriptionof EPS located on the neck of a 10-year-old boy."The eruption consisted of closely set keratotic papuleseach with a central plug arranged into hyperkeratoticridges. Individual papules appeared to involute within5 months, but the basic process continued unabatedfortning new lesions. Histologic evaluation revealedacanthosis, hyperkeratosis, and enlargement of theepidermal rete ridges, with interruption of the epi-dermis by a keratotic plug extending from Ihe epi-dermis into the dermis. The plugs consisted of elasticfibers that were histologically well-preserved lowerin the plug, but the higher ascending fibers appearedto lose their staining properties. A homogeneousmass of elastic fibers (elastoma) was present in adja-cent dermal papillae; these papillae were surroundedby epidermal rete ridges that protruded downward,giving the appearance of the epidermis trying loenvelope and eliminate the elastic fibers. Miescher

No. 5 TRANSEPIDERMAL ELIMINATION Wno and Rasmussen 269
interpreted the process to be secondary to poornutrifion, resulting in "necrobiosis" and expulsion ofthe altered elastic tissue. He coined the term "elas-toma intrapapillare perforans verruciforme" to de-scribe this process.^
In the same year, Beening and Ruiter** reported asimilar case in a 13-year-old boy with Down's syn-drome. They considered this to be identical to thecondition described earlier by Lutz^ and termed it"hyperkeratosis folllcularis serpiginosa." This wasprobably the first reported case of EPS appearing inconjunction with a genetic disorder. There are anumber of entities with which EPS has been asso-ciated.
Dammert and Putkonen"^ were the first to proposethe name "elastosis perforans serpiginosa," in 1958.Their rationale was based on the histologic observa-tion that the elastosis is not necessarily "intrapapillare"nor of follicular origin and that EPS described thesalient histopathologic and clinical features of thedisease in the least number of words.
Clinical Cbaracteristics
In Mehregan's comprehensive review of 101 casesof EPS,"" 90% of patients were younger than 30 yearsold, with the range of 5-84 years. The male to femaleratio was 4:1, with the majority of patients Caucasians.Ninety-four percent of the lesions were on the napeand sides of the neck; 26% on the upper extremities;15% on the face; and occasional lesions on the lowerextremities and trunk.
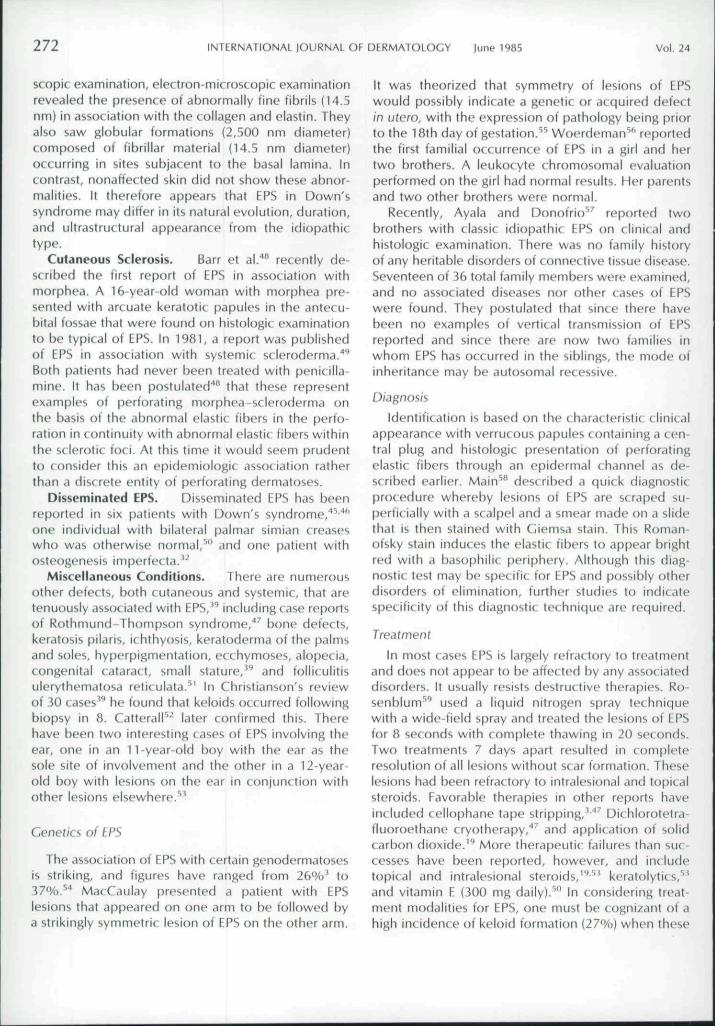
The primary lesion in EPS is an umbilicated dome-or conical-shaped papule that is greyish-yellow incolor and attains 2-3 mm in height and diameter(Eig. 1). Each papule contains a central plug, whichon forcible removal leaves a bleeding crater. Theconfiguration of the papules may be discrete orirregularly arranged into serpiginous outlines, attainingopen or closed rings or even S-shaped figures; how-ever, centrifugal extension of EPS is not a feature ofthe disease. Depigmentation and even atrophy mayexist in the center of these lesions. Eventually, whenresolution occurs, the remaining skin usually appearsnormal but occasionally may have a slight pinkishhue. Nearby hair follicles may or may not be de-stroyed by scarring, and the overlying skin can appearsimilar to an area treated with diathermy." Usuallythis condition is asymptomatic but may be quitepruritic at times.
Histology
EPS has a characteristic appearance when stainedwith hematoxylin and eosin or stains for elastic fibers
FIG, 1. Elastosis perforans serpiginosa (EPS) on the n.ipc nlthe neck of a woman. The serpiginous configuration of umbilicaledpapules is well demonstrated.
(Verhoeff-van Gieson, acid orcein-Giemsa, or alde-hyde fuchsin). The most significant histologic altera-tions include the presence of a canal filled withfibrous material extending from the dermis, throughthe entire epidermis, and communicating to thesurface, where it is at its widest diameter (Fig. 2).The location of the channels may be peri- or trans-follicular." Where the canal crosses a follicle, it tendsto have multiple openings at the surface. Openingsare usually occupied by a plug containing a mixture
FIG. 2. Histopathology of EPS. The epidermal channel can beseen as a spiral in longitudinal section. Within the channel arealtered eosinophilic elastic fibers. (H & E, XlOO)

270 INTERNATIONAL lOURNAL OF DERMATOLOGY |une 1985 Vol. 24
ot keratinous debris and bluish amorphous crust. Theperipheral portion contains keratinous material, anda central portion of dense bluish-staining "necro-biotic" material consists in part of degenerated epi-thelial cells and pyknotic nuclei of inflammatory cells.Also present within the central area are many brightlystaining eosinophilic fibers. The fibrous material oc-cupies a tortuous channel and in cross section mayoccupy small, round, cystic spaces within the epi-dermis that appear to lie above one another, givingthe appearance of a spiral seen in longitudinal sec-tion.'^ These spirals are not epidermal appendages:there are no connections with hair follicles or sweatducts seen on serial section.
The epidermis immediately surrounding the per-forating canal is composed of flattened keratinocytesthat appear to desquamate into the central plug. Thenearby epidermis is acanthotic and produces smallprotruberances of epithelium into the upper dermis.These tongues of epidermis appear pseudoepithe-liomatous and nonpallisading and are without a well-organized basement membrane.
The underlying dermis contains occasional foreignbody granulomas of mononudear phagocytes andmultinucleated giant cells. When perilesional sectionsare stained for elastic fibers, there is a marked increasein the amount and thickness of fibers. Perilesionalelastic fibers are seen extending vertically upwardinto dermal papillae and may lie adjacent to basalcells. In intervening areas between perforating canals,the superficial plexus of elastic fibers is relativelywell-organized and appears normal. As one nears theperforating canals, a stream of connective tissuecontaining many altered elastic fibers is seen to enterthe canals. The perforating elastic fibers extend tothe surface of the lesion, where they can be seenadjacent to the parakeratotic stratum corneum. Thesefibers lose their characteristic staining properties andappear brightly eosinophilic using the acid orcein-Giemsa stain or yellow by the aldehyde fuchsinmethod. In contrast to elastic tissue, the amount ofacid mucopolysaccharide in lesions of EPS is normal.
Ultrastructural abnormalities of the epidermis arerestricted to the site where TE has occurred.'^ Elec-tron-microscopic examination of the dermis, on theother hand, shows elastic fibers organized into largestrands or as an infiltrating substance interspersedbetween collagen bundles. Ill-defined structures areseen to run parallel to the axis of the elastic fiber,indicating a possible lack of homogenous organization.This is in conjunction with a filamentous material thatappears to be newly assembled elastic fibers. Theelastic fibers in turn are surrounded by tubular-appearing microfibrils. Amino acid analysis revealed
that the amount of elastic tissue in one patient waselevated to 3.5 times that of the control, whereasthe amount of collagen was only minimally elevatedin lesionai skin.'^
In some respects, the lesionai skin of EPS resemblesthat of the newborn or embryonic cutaneous epithe-lium due to several observations. Overall, lesionaielastic tissue appears similar to newly formed elasticfibers. The majority of collagen fibers in EPS are ofsmall diameter and thereby resemble embryonic skin,while EPS lesions contain a similar amount of dermalhydroxylation to the newborn epidermis.'^
Association with Other Disorders
EPS occurs in association with .i number ot con-nective tissue disorders and a wide variety of otherdiseases. In fact, as many as one quarter of all casesof EPS may occur in association with other anomalies.*
Penicillamine-induced EPS. There are at leastnine reported cases'** ^^ of EPS following the admin-istration of therapeutic doses of penicillamine, 1.5-2.0 g daily for up to 6 years.^'-^" In 1972, Guilaine etal.'" described the first case of EPS following penicil-lamine treatment for Wilson's disease (hepatolen-ticular degeneration). Subsequently, seven additionalcases occuring in similar situations have been re-ported.'^ '"̂ The remaining patient developed EPSfollowing penicillamine treatment for cystinuria (con-genital defect of homocystine synthetase)."^"
Clinically, penicillamine-induced EPS appears sim-ilar to primary idiopathic EPS with annular or circinate,keratotic, umbilicated papules on the lower face,sides of neck, axillae, and antecubital fossae; however,one patient had a discoid, firm bordered penile lesionwith a central depressed area within the inner marginof the hyperkeratotic ring.'^
Penicillamine-induced EPS can be differentiatedfrom the idiopathic type by electron-microscopicand, at times, light-microscopic examination. Threemorphologically distinct forms of elastic fibers inpenicillamine-induced EPS may be discerned. First,there are lateral ("lumpy-bumpy") perpendicularbuddings from elastic fibers present in the deepdermis, having the same diameter as the elasticfiber.'"'^'^ Second, Kirsch and Hukill'^ found intenseeosinophilia of the elastic fibers that were penetratingthe epidermis, while those in the reticular dermiswere less eosinophilic or appeared even basophilic.Third, elastic fibers lack the peripheral fibrils and thealternating bands of dense and light layers normallyseen within the cortex.
Hashimoto and others have found the collagenfibers to be abnormal in several cases of penicillamine-

No. 5 TRAN5EPIDERMAL ELIMINATION Woo and Rasmusaen 271
induced EPS.'*-^'"" Fibrils were irregular in diameterand up to five times larger in diameter than normalfibrils, while transverse sections showed the outerlimits of the fibrils to be rather ragged. These collagenabnormalities resemble those found in Ehlers-Danlossyndrome type I and disseminated connective tissuenevi. On this basis, it appears that there is sufficientdifference in the composition and morphology ofelastic and collagen fibers to allow differentiationbetween idiophathic or penicillamine-induced EPS.
Bardach et al."* described a patient who had notonly drug-induced EPS but also a large pulmonary aircyst. Identical light- and electron-microscopic changesin both cutaneous and adjacent pulmonary elastictissue suggested to the authors that the peniciilaminehad induced a disseminated "cutaneo-visceral e!as-tosis."
The pathogenesis of penicillamine-induced EPS inWilson's disease is unknown, but it is tempting tosuggest an etiologic role for peniciilamine in producingrelative local cutaneous deficits in copper and therebyinterfering with normal copper metabolism in theskin.^" More plausible is the theory of Siegal '̂' thatpeniciilamine inhibits lysine-derived polyfunctional,intramolecular, cross-linking formation during elastinsynthesis. Higher doses may also inhibit lysyl oxidase.These changes could conceivably underlie faultyelastin formation with lumpy-bumpy fibers bulging inall directions beyond the confines of the elastic fiber.
Osteogenesis Imperfecta. Osteogenesis imper-fecta (Ol) involves connective tissue componentswith manifestations that include pathologic fracturesand characteristic blue sclera. There are at least sevencases of EPS reported to occur in patients with Ol.Lesions of EPS may occur in localized typical sites,appearing on the neck in five patients^''""' and theantecubital fossa in two.'̂ ^- '̂ Disseminated lesionshave been reported. Kingsley*' described the occur-rence of "extensive and symmetrical" EPS in a 19-year old man with osteogenesis imperfecta. On ex-amination, histologic and ciinicai appearances areidentical to those of the idiopathic variety.
Marfan's Syndrome. There have been reportsof EPS associated with two individuals having Marfan'ssyndrome," and one with a high, arched palate whowas otherwise normal.^''
Ehlers-Danlos Syndrome. In 1958, Meara^^ de-scribed a patient with Ehlers-Danlos syndrome withEPS in the antecubital fossa. Since the initial descrip-tion, four similar cases have been described.̂ ^"^®London^^ presented a case of a 17-year-old man withEPS in conjunction with Ehlers-Danios type IV {Sack-Barabas arterial ecchymotic type). Another case ofEPS has been described by Christianson" in a
4-year-old boy who had a rupture of an anteriorcerebral artery berry aneurysm but was otherwisenormal. Eide"" described EPS in association with fatal,widespread arterial rupture of the aorta, with dissec-tion and elastosis of the endocardium and bronchiolarwalls in a 30-year-old woman who was otherwisenormal. Anning^^ described a similar case in an 18-year-old man with a dissecting aneurysm and EPS. Itis conceivable that Christianson's case and the othersoccurred in individuals with an undiagnosed mild orincomplete form of Ehlers-Danlos type IV, sincethese individuals are prone to arterial rupture andhemorrhage.
Acrogeria. In 1980, Groot et al."" reviewed theliterature on acrogeria and found that 4 patients (allwomen) of a total of 19 (21%) also had EPS. Thesepatients had typical lesions of EPS in both axillae,arms, neck, and thighs. Eurther, two patients hadhigh, arched palates. Superficially, acrogeria may besimilar to Ehlers-Danlos type IV, with conspicuouscutaneous blood vessels and easy bruising, but it isdifferent in that there are neither gross ecchymosesnor intestinal hemorrhage in the former.
Down's Syndrome. Beening and Ruiter,** in 1955,described the first cases of EPS in association withDown's syndrome. Thus far there have been at least15 patients described in the literature.^''•''^'"' Lesionsof EPS in most cases have a similar morphology andappear to occur in similar sites to the idiopathicvariety; however, one of us ().E.R.) has described theoccurrence of atypical EPS in four Down's patients,three boys and one girl.''^ Lesions initially appearedas classical bilateral, hyperkeratotic papules on theneck and upper extremities. Several years later thecircinate papules were replaced with linear and reti-form hypopigmented scars, several of which con-tained a hyperkeratotic papule at one end. Isolatedsingle papules were also seen. Biopsy of a lesion atone end of a scar was consistent with EPS.'*''
Whyte and Winkelmann"^ found the incidence ofEPS in Down's to be 0 among 287 institutionalizedpatients, although our study revealed an incidenceof approximately 1%."^ The chronicity of EPS inDown's can be exemplified by a 21-year follow-upof a patient who was refractory to innumerabletreatments, including both topical and ora! agents."New lesions were still developing while old onesresolved, leaving hyperpigmented scars. This patienthad an episode of scabies; interestingly, all mitesrecovered were within the skin lesions of EPS.
Crotty et al."" studied the biopsy specimens o( EPSfrom the iesional skin on the thigh of a Down'spatient compared with nonaffected buttock skin.Although there were no differences on light-micro-
272 INTERNATIONAL lOURNAL OF DERMATOLOCY |une 1985 Vol. 24
scopic examination, electron-microscopic examinationrevealed the presence ot abnormally fine fibrils (14.5nm) in association with the collagen and elastin. Theyalso saw globular formations {2,500 nm diameter)composed of fibrillar material (14.5 nm diameter)occurring in sites subjacent lo the basal lamina. Incontrast, nonaffected skin did not show these abnor-malities. It therefore appears that EPS in Down'ssyndrome may differ in its natural evolution, duration,and ultrastructurai appearance from the idiopathictype.
Cutaneous Sclerosis. Barr et al.''" recently de-scribed the first report of EPS in association withmorphea. A 16-year-()ld woman with morphea pre-sented with arcuate keratotic papules in the antecu-bital fossae that were found on histologic examinationto be typical of EPS. In 1981, a report was publishedof EPS in association with systemic scleroderma/''Both patients had never been treated with penicilla-mine. It has been postulated'"' that these representexamples of perforating morphea-scleroderma onthe basis of the abnormal elastic fibers in the perfo-ration in c ontinuity with abnormal elastic fibers withinthe sclerotic foci. At this time it would seem prudentto consider this an epidemiologic association ratherthan a discrete entity of perforating dermatoses.
Disseminated EPS. Disseminated EPS has beenreported in six patients with Down's syndrome,"^**'one individual with bilateral palmar simian creaseswho was otherwise normal/" and one patient withosteogenesis imperfecta." |
Miscellaneous Conditions. There are numerousother detects, both cutaneous and systemic, that aretenuously associated with EPS,'̂ including case reportsof Rothmund-Thompson syndrome,'"' bone defects,keratosis pilaris, ichthyosis, keratoderma of the palmsand soles, hyperpigmentation, ecchymoses, alopecia,congenital cataract, small stature,'" and follicuiitisulerythematosa reticulata.""' In Christianson's reviewof 30 cases*** he found that keloids occurred followingbiopsy in 8. Catterall" later confirmed this. Therehave been two interesting cases of EPS involving theear, one in an 11-year-oid boy with the ear as thesole site of involvement and the other in a 12-year-old boy with lesions on the ear in conjunction withother lesions elsewhere."
Genetics of EPS
The association of EPS with certain genodermatosesis striking, and figures have ranged from 26%' to37%.^"' MacCaulay presented a patient with EPSlesions that appeared on one arm to be followed bya strikingly symmetric lesion of EPS on the other arm.
It was theorized that symmetry of lesions of EPSwouid possibly indicate a genetic or acquired defectin utero, with the expression of pathology being priorto the 1 Bth day of gestation.^^ Woerdeman"''" reportedthe first familial occurrence of EPS in a girl and hertwo brothers. A leukocyte chromosomal evaluationperformed on the girl had normal results. Her parentsand two other brothers were normal.
Recently, Ayala and Donofrio" reported twobrothers with classic idiopathic EPS on clinical andhistoiogic examination. There was no family historyof any heritable disorders of connective tissue disease.Seventeen of 36 total family members were examined,and no associated diseases nor other cases of EPSwere found. They postulated that since there havebeen no examples of vertical transmission of EPSreported and since there are now two families inwhom EPS has occurred in the siblings, the mode ofinheritance may be autosomal recessive.
Diagnosis
Identification is based on the characteristic clinicalappearance with verrucous papules containing a cen-tral plug and histologic presentation of perforatingelastic fibers through an epidermal channel as de-scribed earlier. Main''" described a quick diagnosticprocedure whereby lesions of EPS are scraped su-perficially with a scalpel and a smear made on a slidethat is then stained with Giemsa stain. This Roman-ofsky stain induces the elastic fibers to appear brightred with a basophilic periphery. Although this diag-nostic test may be specific for EPS and possibly otherdisorders of elimination, further studies to indicatespecificity of this diagnostic technique are required.
Treatment
In most cases EPS is largely refractory to treatmentand does not appear to be affected tiy any associateddisorders. It usually resists destructive therapies. Ro-senblum" used a liquid nitrogen spray techniquewith a wide-field spray and treated the lesions of EPSfor 8 seconds with complete thawing in 20 seconds.Two treatments 7 days apart resulted in completeresolution of all lesions without scar formation. Theselesions had been refractory to intralesional .ind t()|)icalsteroids. Eavorable therapies in other reports haveint luded cellophane tape stripping,•'•'^ Dichlorott'tra-fluoroethane cryotherapy,''^ and application of solidcarbon dioxide.'"* More therapeutic failures than suc-cesses have been reported, however, and includetopical and intralesional steroids,'''''' keratolytics,"'and vitamin E (300 mg daily).^ '̂ In considering treat-ment modalities for EPS, one must be cognizant of ahigh incidence of keloid formation (27%) when these

No. 5 TRANSEPIDERMAL ELIMINATION Woo and Rasmussen 273
have biopsy specimens taken.'^ Unfortu-nately, the incidence of keloids following treatmentattempts is unknown. On the whole, most indivulualsmust iotirn to live a peaceful coexistence with theirlesions until the lesions resolve spontaneously dueto some unknown stimulus.
Reactive Perforating CollagenosisHistory
Reactive perforating collagenosis was first describedin an excellent succinct report in 1967 by Mehregan.'''*His patient was a 6-year-old girl with an unusualepithelial response to superficial trauma. At 9 monthsof age, she experienced numerous discrete papuleslocated over the extremities, many in a linear distri-bution, suggesting Koebnerization of the lesions. His-tologic observations led Mehregan^'' to suggest thename "reactive perforating collagenosis" (RPC).
Clinical Characteristics
Clinically, RPC starts as a 1 -mm papule that evolvesover 3-4 weeks to 6 mm in si/e and occurs often insites exposed to trauma (Fig. JJ. The papules becomeumbilicated and contain a central plug of hornymaterial that can be removed with a curette onlywith some difficulty, often leaving a bleeding crater.With time the central umbilication becomes shallowerand the plug is eliminated. By 2 months, the lesionsdisappear completely, leaving a scar or area of hy-popigmentation, Although each individual lesion hasa finite life span, a person may have recurrent lesionsthai eru[)t over time, persisting for as long as 37years.*'"'
A total of 47 patients with RPC have been described{Table 2). Approximately 56% were male patientsand 44% were female patients. Onset (wben indi-cated) was prior to 1 year of age in 18% and duringchildhood in 58%. Only 10 patients were reportedwith an onset during adulthood (older than 18 yearsof age), and tbey appear to constitute a separategroup. The extremities are involved in 100% ofreported cases, predominantly on the extensor as-pects. Specific sites include the extensors of the handin 58% of patients, the trunk in 40%, and the facein 27"/.). The vast majority (66%) of patients relatedonset of the lesions to trauma, usually insect bitesand scratches, although precif)itation from acne le-sions*'' or even corporal punishment''^ have beenreported. Only two patients specifically denied rela-tionship to trauma.''••'̂ ^
Lesions of RPC can be induced experimentally andmay be site-dependent (extensor aspect preferred).Bovenmeyer" first reported successfully inducing le-sions in a 4-year-old girl. Using the extensor surface
of tbe left forearm, he was able to produce lesionsby scratching the skin with a 25-gauge needle. Neithera tongue blade nor a needle prick was effec tive ininducing lesions in a similar site. Since then, severalauthors^'"'' ''̂ have been able to induce lesions inthe presacral area, upper back, and extensors of thewrist, forearm, and fingers using a variety of methods,including pinprick, scratch, and superficial abrasionwith a 4-mm punch. Sites wbere lesions could notbe produced in experiments are the upper tbigh,*^scapula,*''' and flexor forearm.''' Cold has been re-p<Kted to exacerbate the total number of lesions infour patients,""*''''''" and four patients reported "intol-erance" to cold.*''' One patient/'"' how(»ver, reportedworsening of the eruption in spring.
Histology
Tbe histopathology of RPC varies with the age ofthe lesions, and step sections must be performed onall specimens to document the presence of TE ofcollagen." Sections of early nonumbilicated lesionsshow perilesional epidermis to be acanthotic. In thecenter there is a widened dermal papillae containingbluish connective tissue confined to the upper dermis.There is no underlying inflammatory infiltrate, whilethe overlying epidermis is thinned and tbe stratumcorneum has a thin layer of parakeratosis.
On examination ot older umbilicated lesions, acup-shaped crater containing a plug, wbich is para-keratotic, with degenerated collagen and numerousexocytic inflammatory cells is visible. Masson's tri-chrome and phospbotungstic acid-hematoxylin stainsfor collagen reveal that the central plug consists ofretractile hyalinized and altered collagen that is elim-inated in a transepidermal fashion. Since the directionof elimination is pcrpendic ular to the epidermi'^, thecollagen fibers can be e.ibily seen within the plugand in numerous small perforations within the un-dedying epidermis. The epidermis of the lateral wallot the crater is slightly acanthotic with hypergranulosisand hyperkeratosis. The upper dermis sbows a mini-mal phagocytic and lympbocytic infiltrate with a slightincrease in vascularity,^'' and some authors havereported tbe additional presence of reactive granu-lation tissue.*"'
On examination of resolving lesions of RPC," amuch smaller, shallower crater containing predomi-nantly parakeratotic keratin with only small foci ofdegenerated collagen is visible. At the base of theplug, the epidermis is almost regenerated. Here tbemalpighian cells appear to contain abundant cyto-plasm with a large amount of glycogen in larger cells;however, tbe granular layer is absent and the basal

274 INTERNATIONAL JOURNAL OF DERMATOLOGY June 1985 Vol. 24
TABLE 2. Reactive Perforating Co!lagenosi%: Reported Cases
CaseNo.
1
2
3
4
5
6
7
8
<•}
10
11
12
13
14
15
16
17
18
19
20
21
22
2.1
24252&27
28
29
30
31
32
33
Author
Kanan"'
Kanan"
Kanan'-^
Kanan"^
Kanan'-^
Kanan"''
Kanan"
Mehregan*"
|. Weiner"
I. Weiner"
Mehregan'
Mehregan'
Mehregan'
Mehregan'(siblings)
Mehregan'
Mehregan'(siblings)
Mehregan'
Mehregan'
Mehregan'(siblings)
Mehregan'
Sovenmyi-r"
A. Weiner*''
A. Weiner*'
Mohri*-'Shitara"Miwa'*Nair*"
Nair"'(father)
Nair"*(children)
Nair*°(children)
Nair"*(children)
Fretzin"
jillson**(siblings)
Sex
M
F
M
M
M
M
F
F
F
M
NS
NS
NS
NS
NS
NS
NS
NS
NS
NS
F
M
f
M
NS
NS
M
M
F
F
M
F
M
Age atPresentation
farly chldhd
Early chldhd
Farty chldhd
Early chldhd
Early chldhd
Early chldhd
Early chldhd
9 months
Farly infancy
Early infancy
Chldhd
Chtdhd
Adult
Chldhd
Chldhd
Chldhd
Chldhd
Chldhd
Chidhd
Chldhd
4 years
1 year
18 mnths
20
NS
NS
10
3
3
5
NS
s
1
Age atOnset(Years)
26
28
20
40
32
32
24
6
11
6
Adult
Chldhd
Adult
Chldhd
Chldhd
Chldhd
Chldhd
Adult
Chldhd
Chidhd
f>
6 on oneoccasion
8
20
AdullAdull
51
40
12
10
1'/;
24
1
Type of Trauma
Scratches andabrasions
Scratches andabrasions
Scratches andabrasions
Scratches andabrasions
Scratches andabrasions
Scratches andabrasions
Scratches, abrasions.& mosquilo bites
Superficial scratcheselbows, knees
Superficial scratchesarms and legs
Superficial scratchesarms, legs, and face
Superficial scratcheslegs, scalp, trunk
Superficial scratchesscalp, trunk
Superficial scratchesscalp, trunk
Scratches andmosquilo bites
Scratches andmosquito bites
Scratches .indmosquito bites
Scratches andmosquiro biles
Scratches andmosquito bites
Scralches andmosquito bites
Cat scratches, insectbites
Sites of corporalpunishment
Nol constantlyobtained
NoneNSNSNS
NS
NS
NS
NS
Insect bites, acnepapules
NS
Parental Affected Sites
Face, hands (dorsa), feet
Face, bands, feet (dorsa)
Hands & feet
Hands & feet
Hands & feet
Hands & feet
Hands & legs
Dorsa of hands, forearms
Scalp, hands (dorsa)
Scalp, hands (dorsa)
Hands (dorsa), arms
Hands (dorsa), arms, legs
Hands (dorsa), arms, legs
Hands (dorsa). arms, legsbites
Hands (dorsal, arms, andlegs
Hands (dorsa). arms &legs bites
Hands (dorsa). arms &legs
Scalp, hands (dorsa).arms, legs, trunk
Hands (dorsal, arms, legsbites
Hands (dorsa), arms, legs
Face, exiensof legs.forearms, butiocks
Face, exiremities, trunk
Face, extremities, trunk
Elbows, nol linearNSHands, elbows, buttocksExtensor extremities wilh
KoebnerDofsa hands, extensor
extremities face, scalp.palms, soles (all over)
Extensor extremities andtrunk
NS.
Extremities
Arms, legs
Back of hands, arms.elbows, knees
Unaffected Areas
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Trunk, palms, soles
Palms, soles
Palms, soles
Palms, soles
Trunk, plams, soles
Trunk, palms, soles
Palms, soles.upper thighs
Palms, soles
Palms, soles
Trunk, palms, soles
Trunk, palms, soles
Palms, soles.upper thighs
Pdlms. soles
Palms, soles
Rest of bodyNSPalms, solesTrunk, palms, soles
Mucosrfl
NS
NS
N&
NS
Trunk, palms, soles
Consanguinity
Positive
Positive
Positive
Positive
Positive
Positive
Positive
NS
NS
NS
NS
NS
NS
NS
Negative
NS
NS
NS
NS
NS
Negative
NS
NS
NS
NS
NS
Negative
NS
Positive
Positive
Positive
NS
NS

No. 5 TRANSEPIDERMAL ELIMINATION Woo atid Rasmusien 275
TABLE 2. Continued
C.iseNo.
14
.it.
37
30
39
4041
42
43
44
4(1
A?
NS.
Aulhdf
lillson"'
Poliak'*Poliak"*
Poiidk'*
Puliak'*
Poliak**
Poli.ik**Cdthran"'Cochrdn'*
Cullen"'
Pai.firh.i'*Bingul"
Nyfors"(Siblings)
Nyfors"
no! '.ignific.int.
Sex
M
FF
M
F
M
MFF
F
M
F
M
M
Age .llPresentation
1
BUck adultBlack adult
Bl<i(.k adull
Hispanicadull
Hispanicadult
Bl,ick adullBldck adullBlack adull
Bbckchldhd
33
1 month
5
Age atOnsel(Years)
4
4151
80
57
77
654136
19
2311
3
7
Type of Trauma
NS
NS (on dialysis)NS
Scratch (on dialysis)
Scratch (on dialysis)
NS
Scralch (on dialysis)NS (on dialysis)NS (on dialysis)
Insect bile, scratch
NSCat scratch
Tree scratches
NS
Parental Affected Sites
Back of hands, arms,elbows, knees
Extensor extremitiesExtensor extremities,
Irunk, faceExtensor extremities.
trunk, faceExtensor extremities.
trunk, faceExtensor extremities.
trunk, faceExtensor extremitiesTrunk, arms, central barkExtensor arms, upper
backDorsa hands, extensor
ft»rearms, trunk, thighsFxtensor extremitiesDorsa hands, extremities.
extensors, flexorsBegin on trunk, then
face, extremities.dorsa hands
Extremities, face, dorsahands
Unaffected Areas
Trunk, palms, soles
Trunk, palms, solesPalms, soles
Palms, soles
Palms, soles
Palms, soles
Trunk, palms, solesPalms, solesPalms, soles
Palms, soles
Trunk, palms, solesTrunk, palms, soles
Palms, soles
Trunk, palms, soles
Consanguinity
NS
NSNS
NS
NS
NS
NSNS
NS
NS
NSNS
NS
NS
eel! layer appears to be incompletely developed withd partially organized basement membrane. The re-maining altered dermal collagen is eliminated througha narrow tunnel within the epidermis in the centerof the lesion, the lining epithelium of the tunnelbeing well-organized. The underlying dermis showsslight vascularity and minimal inflammatory infiltrate.
Stains for calcium, elastic tissue, and acid muco-polysaccharide are negative in the plug and exhibitno increase in the dermal papillae at any stage.Similar light-microscopic features are seen in bothnaturally occurring lesions of RPC and experimentallyinduced lesions.*"'
Electron-microscopic examination of the epidermisin early lesions shows complete disappearance of thebasal lamina. Desmosomes are intact, but bundles ofnormal-appearing collagen fibers appear interspersedwithin widened intercellular spaces.™ Mohri**^ studiedthe dermis of a regressing lesion and found that thecollagen was disrupted by large masses of fine fila-mentous material, accumulations of small vesicularbodies, and phagocytes.
As to the pathogenesis of this disorder, RPC lesionsare almost always invoked by some sort of superficialtrauma, although interestingly deeper wounds, suchas surgical incisions, do not induce lesions.*"' The
pathogenetic effects can be constructed as follows.In response to trauma, injury to dermal connectivetissue occurs, resulting in alteration ot papillary col-lagen. Reactive epithelial hyperplasia in the adjacentepidermis occurs, while the directly overlying epi-dermis becomes thin and shows multiple foci ofdisruption through which altered collagen and sparseinflammatory cells are eliminated. As underlying der-mal material is transferred from the dermis to thesurface, the epidermis sinks into this area, which wasformerly occupied. The process of TE continuesunabated until the entire supply of altered collagen
Fit,. 3. Linear Koebner phenumpnon in lesion ot reactiveperforating coilagenosis (RPC). Individual morphology of RPCconsists of umbilicated papules in a linear arrangement on thedorsa of the extremities. (Courtesy of Scott W. Bronslein, M.D.)
276 INTERNATIONAL )OURNAL OF DERMATOLOGY |une 1985 Vol. 24
TABLE 3. Cases of RPC with Adull Onsef
Author
Mehregan'Mohri"'
Poliak* '̂
Cochran""
Onset
Adult20 yrs.
AduitAdultAdultAdultAdultAdult41 yrs.36 yrs.
Sex
—
FFMFMMFF
Diabetes
.
—
YesYesYesYesYesYesYesYes
Nephropathy
Yes—
Y«sYesYesYes——YesYes
Dialysis
Yes—
YesNoYesNoNoYesYesYes
Retinoptithy
—
YesYesYesYesYesYesYes
—
Pruritus
.
—
YesYesYesYesYesYesYesYes
Other
Wegener'sgranulomatosis
RPC cleared with UVBRPC treated with UVB
is exhausted. At this point, a repair phenomenonoccurs in which epidermal reconstitution closes offthe eliminating channels. The keratotic plug at thosurface gradually sloughs off via normal epidermalturnover, leaving minimal or no scarring.
A5_soc(d(/on with Other Disorders
Conditions associated with RPC include; ricketts,^'ricketts-like bone* changes,'"'' bilateral coxa vera,''^Wegener's granulomatosus,*'^ lichen amyloidosus,''^rheumatoid arthritis,'''' and Henoch-Schonlein pur-pura.'''
There appears to be a specialized subset of RPC,defined by adult onset and the presence of diabetesmellitus. These cases are summari;!ed in Table 3. Tencases of RPC with onset in adulthood (older than 18years of age) were recorded in the literature.'•''"'''^''•''•'Of these 10 patients, 8 had diabetes mellitus (7 ofthe 8 had diabetic nephropathy), 1 had chronic renaldisease and was on dialysis (it was not stated whetherdiabetes was present),' and 1 had Wegener's granu-lomatosis.''' Of all the patients with diabetes and RPC(a total of nine),^"''*"^'' eight lall into the group definedabove (with onset of RPC in adulthood), while thesole diabetic with onset al 10 years of age had only"mild" diabetes. Thus using the criteria of onset ofRPC in adult years, the physician must be alert tothe concomitant presence of diabetes mellitus, which,if present, may be severe with diabetic nephropathy.Patients with diabetes and RPC had lesions resemblingclassical RPC in all aspects, except tor .lgc of onsetand a tendency to be pruritic although dialysis-induced pruritus may be responsible In some cases.Cuilen*'" w.is able to treat the pruritus successfullywith UVB light. Poiiak''' was able to induce skinlesions experimentally in two of his patients withdiabetic adult onset RPC, Lesions of RPC differ from
so-called Kyrle's disease on the basis of many criterttT(discussed below), such as the presence of linearKoebnerization, the tendency to remain discrete, andthe presence of TE of collagen.
Cenet;cs of RPC
There were 25 patients (52%) with RPC who hadaffected family members (mostly siblings). Of these25 patients, 10 had a history of parental consanguinity.Considering this genetic background, the evidenceleads us to postulate an autosomal recessive modeof inheritance, although further genetic studies arenecessary to delineate more clearly the mechani'<mof transmission.
Treatment
Treatment of this disorder is often frustrating andunrewarding. Recently Cullen*"" treated a 25-year-oldwoman with tretinoin 0.1% cream, which decreasedthe total number from 12-21 to 0-2 lesions. Oralforms of treatment have included: antibiotics,'""*''''''"such as erythromycin and tetracycline; oval vitaminA 100,000 Units daily''^'^''; oral prednisone 20 50mg/day''^; methotrexate, with some response*"'; andoral proteolytic enzyme Ananase^*^, 200 mg tid.*'''Other agents have included topical keratolytics"^^'topical steroids with or without occ lusion'"''; intrale-sional steroids^''; and ultraviolet light B in diabeticpatients on renal dialysis.'''' Isotretinoin undoubtedlywould be of some benefit, espe< iaily sine e it atfectskeratinization and prior responses to topical tretinoinhave been encouraging.
Collagenome Perforant Verruciforme
Collagenome perforant verruciforme (CPV) wasfirst described by Woringer and Laugier in 196.3."""'

No. 5 TRAN5EP1DERMAL ELIMINATION Woo and Ra^mussen 277
A 19-yearoId man had numerous cuts and lacerationsafter falling through a glass roof. Three weeks later,flesh-colored hyperkoratotic papules developed inthe sites of lacerations consisting of 2-3 mm erythe-matOLis papules arranged in linear or grouped config-urations. Remission was evident without treatmentwithin i months, with almost complete disappearanceof the lesions. Histologic examination showed papil-lomatosis and hyperkeratosis with a channel disruptingthe epidermis. Within this space were basophilicnonelastir collagen bundles extruding from the dermisto the surface of the skin. Later, Delacretaz andCattlen"' des{ ribed another case of CPV in a 6 yearold boy who sustained trauma to his right thigh.Three weeks later, a 2 X 4.5-cm plaque appeared atthe site of injury, consisting of 10 40 papules, eachwith a central keratinous plug. The plaque resolvedwithin i months. They presented two other atypicalcases—a 12-year-old boy following injection of acorticosteroid and a 30-year-old woman followingremoval of a mote—calling these examples of TE oftraumatically altered collagen.
Although CPV and RPC are similar in many aspects,(hey differ in several ways.*^ CPV evolves in a singleepisode, without reported familial background (al-though the number of reported cases is extremelysmall). RPC does not always have a history of specificimmediate trauma, appears mostly on the dorsa ofthe fingers, and has onset in childhood or in adultdiabetics and can continue up to .37 years {althoughindividual lesions resolve in 1-2 months).*"" Until thenumber of reported cases of CPV has increased, onecannot generalize about the true nature of this entityand probably best regard it as a separate but veryclosely related entity to RPC.
Chondrodermatitis Nndularis Helicis Chronica
Chondrodermatitis noduiaris helicis chronica(CNHC) probably represents a distinct separate entitywith TE as the primary pathologic event. In 1980,Goette^* and Cruz^'' independently proposed thatthe pathogenesis of CNHC was due to this form ofelimination. CNHC almost exclusively affects Cauca-sian males in their middle years. Typical appearanceis a well-defined V -̂cm nodule that appears pink topearly-grey. The lesions apfjear most often on thehelix and rarely on the anthelix (Fig. 4). There is anadherent central crust that, on removal, will reveal asmall erosion or cup-shaped depression with a pin-point channel. These lesions may be bilateral andcan be quite tender, especially with pressure.
"̂̂ reviewed 24 cases in which the adjacent
Ftc. 4. A painfut nodule with a rentral plug is prest'ni on Ihehelix of the ear. consUlf^nl wilh i.hondroderm,iriris noHuliiris hclicisrhronica (CNHC). (Courli-sy of Dt'tlof K. Goetle. M.I.).)
epidermis was acanthotic or exhibited pseudoepithe-iiomatous hyperplasia with a central crater-like(iepression and channel (Fig. 5). The underlying dermiscontained a homogeneous fibrinoid maleri.il in amilieu of altered dermal collagen. The collagen bun-dles were swollen and intensely eosinophilic. Elasticfibers often showed degeneration where dermalchanges were most prominent. Granulation tissue, acbronic granulomalous and inflammatory infiltrate,telangiectasias, and solar elastosis could be seen inthe maiority of spet imens. There was evidence ofunderlying perichondritis. Changes in the cartilagewere found by Bard"^ to be inconsistent, whereasGoette*" found 10 of 17 biopsy specimens to contain"degenerated" cartilage. Abnormal collagen may bethe inciting factor in the pathogenesis. It has been
Fic. 5. Hislopalholojiy of CNHC demonsirating (ransepidermalc'iiminaiion TE of altered dermal collagen. (xlOO) (Courtesy ofDetlef K. Goette, M.D.)
278 INTERNATIONAL lOURNAL OF DERMATOLOGY June 1985 Vol. 24
proposed that CNHC is a primary disorder of TE,representing a perforating actinic granuloma."' Anatomy, vast ul.ir deticiency, trauma, and actinic damagemay also be important in the pathogenesis.
Drug Names
isotretinoin: AccutanepeniciHatnine: Cuprimine, Depentrelinopn: Retin-A
Acknowledgment
Drs. R. ). Barr, M. G. Wood, K. Hashimoto, D. A. Weigand,C. A. Parra, S. W. Bronslein, D. L Ciomons, D. K. Goette. H.Bdrda(h, ). W. B.vd. P. B. Hukill, D. Vnlpin, and A. H. MehreRanprovided phuIoKraphs. Dt. Amir H. Mehregan made helpful sug-gestions .ind provided editorial review.
References
1. Mehregan AH. Transepithelial elimination. Curr Probl Dermatol.I970;3:124- 147.
2. Freudenthal W. Amyloid in der Hdut. Arch Dermatol Syphil.1930;162:40 94.
3. Mehregan AH. Elastosis perforans serpiginosa: a review of theliteftiture and report of t ) cases. Arch Dermatol. 1968;97:381 393.
4. Batres E, Kiima M, Tschen J. Transepithelial elimination incutaneous sarcoidosis. ) Cutan Pathol. 1982;9;50 54.
5. Marks R. Schellander F. The epid4>rmal response in subepi-dermal mtlammation. Br 1 Dermatol. 1973;83:363 376.
6. Fischer E. Eigenartiger analomischer Befund bei einer Haul-krankheil Zbt: Herz uni Gefass. Krankh. I927;22:599-160.
7. Lutz W. Keratosis follicularis serpjginosa. Dermatologica.1953;106:318-320.
8. Miescher VG. Flastoma inlrapapillare perforans verrut iforme.Dermatologica. 1955;110:254 266.
9. Becning GW, Ruiter M. Keratusis follicularis serpiginosa (Lutz)Dermatologica. Basel. 1955;nO:175.
10. Dammert K, Putkonen T. Keratosis follicularis serpiginosa Lutz.Dermatologica. 1958:116:143-155.
11. Wilkinson DS. Keratosis fciilicularis serpiginosa (Lutz). Br JIVrmatol. 1959,71:77-78.
12. Hashimoto K, Hill WR. Elastosis perforans serpiginosa: a casereport with histochemicai and enzyme digestion studies. )Invest Dermatol. 1960;35:7-14,
13. Volpin 0, Pasquali-Ronchetti I, et al. Ultrastructural andbiochemical studies on a case of elastosis perforans serpi-ginosa. Dermatologica. 197a;156:209-223.
14. Guilaine I, Benhamon |P, Molas G. Elastome perforant verru-ciforme chez un malade traile par penicillamine pourmaladie de Wilson. Societe Francaise de Dermatologiqueet de Syphiligraphie. 1972:79:450 453.
15. Koblenzer C. Elastosis perforans serpiginosa, secondary toprolonged treatment with penicillamine tor Wilson's disease.Int ) Dermatol. 1982:21:283 284.
16. Pass F, Gotdfischer S, Sternlieb I, et al. Elastosis perforansserpiginosa during penicillamine therapy for Wilson's dis-ease. Arch Dermatol. I973;10«:713 715.
17. Kirsth N, Hukill PB. Elastosis perforans serpiginosa inducedby penicitlamine. Arch Dermatol. 1977,113:630-635.
18. Bardach H, Gebhart W, Niebauer G. "Lumpy-bumpy" elasticfibers in the skin and lungs of a patient with peni< ilLimine-induced elastosis perforans serpiginosa. I Cutan Biol. 1979;6:243-252.
19. Rosenblum GA. Liquid nitrogen cryotherapy in a case ofelastosis perforans serpiginosa. | Am Acad Dermatol. 1983;8;718-721.
20. Abel M. Etastosis perforans serpiginosa associated with peni-cillamine. Arch Dermatol. 1977; 113:1303.
21. Hashimolo K, M( Fvoy B, Belcher R. Ultrastructure of penicil-lamine-induced ".kin lesions. I Am Acad Dfrmatoi. 1981,4:300-315.
22. Keymond |L, Stoebner P, Zambetli I', ct al. Peni( ilUmineinduced elastosis perforans serpiginosa: an ullrastru(turalstudy of two cases. I Cutan Pathol. 1982;9:352 357.
23. Levy RS, Fisher M, Atter |. Penicillamine: review and cutaneousmanifestations. I Am Atad Dermatol. 1983,8:548 558.
24. Sternlieb I, Fisher M, Scheinberg IF) Penicillamine-inducedskin lesions. | Rbeumatol. 1981;8{suppl 7):149-1.54.
25. Cohen AS, Hashimoto K. Electron microscopic observationson the lesions of elastosis perforans serpiginosa. 1 InvesIDermatol. 1960,35:15-19.
26. Siegal RC. Collagen cross-linking: effect of D-penitillamine oncross-linking in vitro. 1 Biol Chem. 1977;252:254-259,
27. Carey TD. Elaslosis perforans serpiginosa. Arch Dermatol.1977:113:1444-1445.
28. Relias A, Sakellarlou G, Tsoitis G, et al. Elastose perforanleserpigineuse de lutz-Miescher et osteogenesis imperfecta.Ann Dermatol Sypbilol. 1968,95:491-504.
29. lones PE, Smith DC. Porokeratosis. Arch Dermatol. 1947;56:425-436.
30. Hitch |M, Lund HZ. Elastosis perforans serpiginosa. ArchDermatol. 1959:79:407 421.
31. Reed WB, Pidgeon |W. Elastosis perforans serpiginosa withosteogenesis imperfecli. Arch Dermatoi. 1964,89:342-344.
32. Kingsley H|. Elastosis perforans serpiginosa with osteogenesisimperfecti. Arch Dermatol. 1964:90:453.
33. Anning ST. Elasloma intrapapillare perforans verruciforme(Miescber). Proc R Soc Med. 1958,51:932.
34. Empson CL, lacobs DS. Elastosis perforans serpiginosa andhigh arched palate. Laryngoscope. 1969:79:368 374.
35. Meara RH. Ehlers Danios syndrome and ^ elastoma verruci-forme perforans (Miescher). Trans St. John (losp Derm S(K:.1958:40:72.
36. London ID, Girhan EG, Garrick I, et al. Elastosis perforansserpiginosa with systemic involvement. South Mod |.1974,67:225-227.
37. Zambal Z. Sind hyperkeratosis follicularis in tutem pcnelransund elastoma intrapapillare perforans verriu iforme identisth?Haularzt. 1958;9:304-.3n.
38. Korting GW. Elastosis perforans serpiginosa als ektodermalesrandsymptom bei Cutis Laxa. Arch Klin Exp Dermatol.1966,224:437 446.
39. Christianson HB. Elastosis perforans serpiginosa: associationwith congenital abnormalities: report of Iwo cases. SouthMed |. 1966:59:15-19.
40. Eide I. Elastosis perforans serpiginosa with widespread arteriallesions: a case report. Acta Derm Venereol (Stockh). 1977;57:533-537.
41. DeCroot WP, Tafclkruyer |, Woerdman M|. Familial acrogeria(Gotlron) Br | Dermatol. I98O;1O3:213 223.
42. Woerdman M), Scott FP. Keratosis follicularis serpiginosa (Lutz).Dermatologica. 1959:118:18-26.
43. Tschen E, Head E. Elastosis perforans serpiginosa and othercomplications. Arcb Dermatol 1980:116:1348.
44. Crotty C, Bell M, Ester SA, et al. Cytologic features of elastosisperforans serpiginosa (EPS) associated with Down's syn-drome. I Am Acad Dermalol. 1983:8:25.5-256.
45. Rasmussen |E. Disseminated elastosis perforans serpiginosa infouf mongoioids. Br | Dermarol. 1972:86:2-13.
46. Ritchie EB. Elastosis perforans serpiginosa. Arch Dermatol.1960:82:178-181.
47. Whyte H), Winkelmann RK. Elastosis perforans (perforatingelastosis): the association of congenital anomalies, salientfacts in the histology, studies of enzyme digestion and areport of necropsy in a case. ) Invest Dermatol. 1960;35:113-122.

No. 5 TRANSEPIDERMAL ELIMINATION Woo and Rasmussen 279
48. Barr RS, Siegal )M, Graham )H. Elastosis perforans serpiginos.iassociated with morphea. ) Am Acad Dermatol. I980;3:19-22.
49. May NC, Lester KS. EUistosis perforans serpiginosa associatedwith systemic sclerosis. J Am Acad Dermarol. 1982;6:945.
50. Pedro SD, Garcia RL. Disseminate eiastosis perforans serpigi-nosa. Arch Dermatol. I974;109:84-85.
51. Dogos R, Touraine R, Balaith S, et al. Elastome perforaniverruciforme de Lutz-Miescher associe a une atrophodfrmievermiculee. Reunion de la societe francaise de dermatologiea Mars. 1967;406-407.
52. Catterall MD, Padley NR. Elastosis perforans serpiginosa. ClinExp Dermatol, 1979;4:n9-122.
53. Weidman Al, Allen B. Elastosis perforans serpiginosa: twocases involving the ear. Arch Dermatol. 1971;103:324-327.
54. Smilh EW, Malak )A, Goodman RM. et al. Reactive perforatingelastosis: a feature of certain genetic disorders. )ohns Hop-kins Med ). 1962;111:235-251.
55. MacCauley WL. Symmetry in elastosis perforans serpiginosa:its significance. Arch Dormatol. 1963;88:21 5-217.
56. Woerdman M). Bour D)H. BijUma |B. Elastosis perforansserpiginosa: report of a family with chromosomal investi-gation. Arch Dermatol. 1965;92:559-560.
57. Ayala F, Dnnolrio P. Elastosis perforans serpiginosa: report ofa family. Dermatologica. 1983;166:32-37.
.58. Main RA, Dave VK, Carr A]. Elastosis perforans serpiginosa: adiagnostic measure. Br I Dermatol. 1971;85:195-19b,
59. Mehregan AH, Schwartz OD, Livingood CS. Reactive perforatingcollagenosis. Arch Dermatol. t967;96:277-282.
60. Nair BKH, Sarojini PA, Basheer AM, et al. Reactive perforatingcollagenosis. Br J Dermatol. 1974;91:399-403.
61. Eretzin DF. Reactive perforating collageneosis. Arch Dermatol.1974:109:750.
62. Weiner AL. Reactive perforating collagenosis. Arch Dermatol.1970;102:540-544.
63. Mohri S, Sano T, Fukuda. An adult case of reactive perforatingcoliagenosis. | Dermatol (Tokyo). 1980;7:363-369.
64. Bovenmyer DA. Reactive perforating collagenosis, experimentalproduction of the lesion. Arch Dermalol. 197O;1()2:313-317.
6.5. Kanan MW. Familial reactive perforating collagenosis andintolerance to cold. Br I Dermatol. 1974;91:4O5-414.
66. Poliak SC, Lebwohl MG, Parris A. et al. Reactive perforatingcnllagenosis associated with diabetes mellitus. N Engl IMed. 1982:306:81-84.
67. Cullen SI, Successful treatment of reactive perforating colla-genosis with Iretinoin. Cutis. 1979:23:87-193.
68. Pasricha |S, Girgia HS, Kandhari KC. Reactive perforatingcollagenosis. Dermatologica. 1971;143:353-356.
69. Jillson OF. Reactive perforating collagenosis. Arch Dermatol.1973;107:4M-465.
70. Fretzin DF, Beai DW. |ao W. Light and ultrastructural studyof reactive perforating collagenosis. Arch Dermatol.1980:116:1054-1058.
71. Bingal O. Hyperkeratosis follicuJaris and parafollicularis incutem penetrans. (Kyrle's disease) in a child. Turk I Pedi.ili.1965;7:143-I49.
72. Nyfors A, Mehregan AH. Reactive perforating collagenosis.Acta Derm Venereol (Stockh). 1973:53:375-380.
73. Shitara A, Nitto H, Nakajima H. Lichen myxedematous .mdreactive perforalJng collagenosis in a patient with diabetesmellitus. Clin Dermatol. 1975:29:749-754.
74. Miwa T, Yamada K, Mori S. A tasi' of reactive perforatingcollagenosis observed in a patient with rheumatoid arlhrilis.Clin Dermatol. 1978:32:439-444.
75. Bronstein S. Reactive perforating collagenosis in a patient withHenoch-Schonlein purpura. Presented at American Acad-emy of Dermatology Meeting, New Orleans, December1903.
76. Cochran R], Rucker SB, Wilkin |K. Reactive perforating colla-genosis of diabetes and renal failure. Cutis. 1983;31:55-58.
77. Cochran R), Tucker SB, Wilkin JK. Reactive perforating colla-genosis and diabetes melitisand renal failure. Cutis, 1983:31:55-58.
78. Mehregan AH. Perforating dermatoses: .i t linicopathologicreview. Int i Dermatol. 1977:16:19-27.
79. Weiner |. Kyrle's disease: hyperkeralosis follicularis et para-foliicularis in cutem penetrans in siblings. Arch Dermatol1967:95:329-330.
80. Woringer F, Laugier P. Collagenoma perforans verruciforme.Derm Wo< henschr. 1963:147:64-68.
81. Laugier P, Woringer F. Reflexions au sujet d'un collagenomeperforant verruciforme. Ann Dermatol Syphilol. 1963:90-29-36.
82. Deiacretaz, Gattlen |M. Transepidermal elimination of trau-matically altered collagen. Dermalologica. 1976:1 52:6.'S-71.
83. Goette DK. Chondrodermatitis nodularis chronica helicis: aperforating necrobiotic granuloma. | Am Acad Dermatol.1980:2:148-154.
84. Santa Cruz DJ. Chondrodermatitis nodularis helicis: a trans-epidermal perforating disorder. J Cutan Pathol. 1980:7:70-76.
85. Bard JW. Chondrodermatitis nodularis chronica helicis. Der-matologita. 1981:163:376-384.
Phototherapy
Phototherapy has lately resumed a respectability lacking since the turn of the century and thedays of Finsen. In medicine, phototherapy and phot(K hemotherapy are routinely used in certainskin diseases and neonatal jaundice, and there is much interest in the use of lasers with porphyrinfor the phototherapy of internal neoplasia. In the cosmetic sector, solaria are in vogue for skintanning (the UK Health and Safety Executive has issued a guidance note for operators); andwhite-skinned people continue to expose their bodies to natural sunlight despite the correlationbetween solar exposure and skin cancer. Holiday resorts in Britain have examined the potentialof large solaria—airhouses accommodating 20 or tnore persons in which the concave innersut̂ ace provides a diffuse reflecting surface—to compensate for sunless summers. Most tanningfacilities, however, are made for individual use. The lamps may emit much more spectral powerthan the equivalent wavebands of the solar spectrum; consequently, the risk of burning andphotosensitisation is higher than with sunlight, especially as satisfactory radiometry is difficultwith tnultitube arrays.—Skin photohiology. Lancet. 1983:1:566.
