distinct features of colorectal cancer in children and adolescents : a population-based study of 159...
TRANSCRIPT

Distinct Features of Colorectal Cancer inChildren and AdolescentsA Population-Based Study of 159 Cases
Iyad Sultan, MD1; Carlos Rodriguez-Galindo, MD2; Hani El-Taani, MD3; Guido Pastore, MD4;
Michela Casanova, MD5; Gianfranco Gallino, MD6; and Andrea Ferrari, MD5
BACKGROUND: Colorectal cancer is exceedingly rare in children and adolescents. Reports from small series indicate
that poor prognostic factors are more common in children than in adults, resulting in worse outcome for the pediatric
population. METHODS: The Surveillance, Epidemiology, and End Results database was searched for records of chil-
dren/adolescents with colorectal cancer, and the features and outcomes were compared with those of adults.
RESULTS: From January 1973 through December 2005, only 159 children/adolescents (ages 4-20 years) were
reported with a diagnosis of colorectal cancer. The most common sites of involvement were the rectum (27%) and
the transverse colon (26%). Adenocarcinoma was the most common histiotype in both adults and pediatric patients;
however, children/adolescents had more unfavorable histiotypes (ie, mucinous adenocarcinoma [22%] and signet ring
cell carcinoma [18%]) when compared with adults (10% and 1%, respectively; P < .001). Poorly differentiated and un-
differentiated tumors (grades III and IV, respectively) and distant stage were more common in children/adolescents
(P < .001). The 5-year relative survival estimates in children/adolescents and adults were 40% � 4.2% and 60% �0.10%, respectively, confirming a worse outcome in the pediatric age group (P < .001). CONCLUSIONS: Children/ado-
lescents represent a minority of patients with colorectal cancer and have high-risk features and worse outcome than
adults. The small number of patients in this age group was an impediment to the development of meaningful clinical
trials. Thus, the principles of management for adult colorectal cancer should be used in the treatment of children and
adolescents. Cancer 2010;116:758–65. VC 2009 American Cancer Society.
KEYWORDS: colorectal cancer, colon, children, adolescents, Surveillance, Epidemiology, and End Results (SEER),
adenocarcinoma.
Colorectal cancer (CRC) is the third most common malignancy in adults worldwide following lung and breast can-cers. There are 945,000 new CRC cases diagnosed each year worldwide (9.4% of cancer cases), and this malignancy is re-sponsible for 492,000 adult cancer deaths yearly (7.9% of total deaths).1 Conversely, CRC is exceedingly rare in thepediatric age group, with an estimated annual incidence of approximately 1 case per million individuals.2 A recent studyof the Italian TREPproject on rare pediatric tumors,3 using data from the Italian network of cancer registries (AIRTum),estimated a CRC incidence rate of 0.09 and 0.72 per million person-years for children ages 10 to 14 years and 15 to 17years, respectively, but recorded no cases in children aged <10 years.4 In the TREPproject, only 6 cases (all aged >10years) were registered between 2000 and 2006, out of 336 patients with rare pediatric tumors.
To better characterize the clinical features and outcomes of CRC in pediatric patients and the differences from theadult form, we performed an analysis of all CRC cases registered on the Surveillance, Epidemiology, and End Results
DOI: 10.1002/cncr.24777, Received: April 3, 2009; Revised: May 22, 2009; Accepted: May 27, 2009, Published online December 2, 2009 in Wiley InterScience
(www.interscience.wiley.com)
Corresponding author: Iyad Sultan, MD, Department of Pediatric Oncology, King Hussein Cancer Center, Queen Rania Al Abdullah Street, PO Box 1269, Amman
11941, Jordan; Fax: (011) 962-6-534-2567; [email protected]
1Department of Pediatric Oncology, King Hussein Cancer Center, Amman, Jordan; 2Department of Pediatric Oncology, St. Jude Children’s Research Hospital, Mem-
phis, Tennessee; 3Department of Internal Medicine, Medical Oncology Section, King Hussein Cancer Center, Amman, Jordan; 4Childhood Cancer Registry of Pied-
mont, Cancer Epidemiology Unit, CPO Piemonte, Center of Experimental Medicine Research, S. Giovanni Hospital, University of Torino, Torino, Italy; 5Pediatric
Oncology Unit, National Cancer Institute, Milan, Italy; 6Colorectal Cancer Surgery Unit, Department of Surgery, National Cancer Institute, Milan, Italy
We thank the King Hussein Cancer Foundation and the American Lebanese Syrian Associated Charities for their support to King Hussein Cancer Center and St.
Jude Children’s Research Hospital, respectively. We also thank Dr. Najyah Abuirmeileh from King Hussein Cancer Center for reviewing and editing this article.
758 Cancer February 1, 2010
Original Article

(SEER) public-access database collected from various geo-graphic areas in the United States.5 The SEER programcurrently covers approximately 26% of the US popula-tion, and includes 5,306,606 tumors diagnosed between1973 and 2005.
MATERIALS AND METHODS
Study Population
We used the case listing session of the SEER*Stat 6.4.4program5 to identify children/adolescents (aged <20years) with a reported diagnosis of CRC in the SEER 17(available at: http://seer.cancer.gov/data/ accessed on Jan-uary 9, 2009) database based on the International Classifi-cation of Childhood Cancer, version 3,6 group XI(f.2)carcinomas of colon and rectum. The query was set toexclude patients with carcinoid tumors (n ¼ 17), thosewith follow-up in the form of death certificate or autopsyonly (n¼ 0), and those without microscopic confirmationof their disease (n¼ 0).
The survival session of the SEER*Stat software wasused to calculate the relative survival of patients, which isbased on calculated survival of studied patients withadjustment made for expected survival in different agegroups. In addition, the frequency session of the softwarewas used to calculate the frequency of different factors inthe adult population, and the rate session was used to cal-culate the age-adjusted incidence rates.
Statistical Analysis
The histologic types based on the International Classifica-tion of Diseases for Oncology, third edition (ICD-O-3)were grouped under 5 categories: 1) adenocarcinoma, nototherwise specified (NOS); 2) adenocarcinoma in adeno-matous polyp, including cases of adenomatous polyposiscoli (APC); 3) mucinous (including mucin-producing)adenocarcinoma; 4) signet ring cell carcinoma; and 5)others. For tumor staging, we were able to use the histori-cal SEER staging system, which labeled tumors as 1) local-ized tumors (correlating with T1-T3/N0 of the AmericanJoint Committee on Cancer [AJCC] staging system)7; 2)regional (referring to locally advanced tumors invadingthrough serosa/visceral peritoneum, extending to nearbystructures or involving regional lymph nodes and correlat-ing with T4/N1-3); and 3) distant stage (referring to he-matologic spread or distant lymph node involvement,M1).
MedCalc for Windows version 10.0.0 (MedCalcSoftware, Mariakerke, Belgium) was used to perform sta-
tistical calculations on the pediatric population. The chi-square test was used to compare categorical variables. TheKaplan-Meier method was used to calculate survival esti-mates for children/adolescents using all-cause mortality asan endpoint. The log-rank test was used to compare sur-vival curves. Cox proportional hazards regression analysiswas used for multivariate analysis. To compare children/adolescents and adult data, we loaded the numbers gener-ated by the frequency session of the SEER*Stat softwareon the OpenEpi software8 and executed proper statisticaltests to calculate the P values.
RESULTS
Patient CharacteristicsWe identified 550,622 patients with colon cancer whowere diagnosed between January 1973 and December2005 and fulfilled the inclusion criteria. The majority ofpatients (78%) were aged �60 years at diagnosis. Only159 patients (0.03% of the cases) were aged <20 years(median age, 17.5 years) and were selected for the analysisof children/adolescents (among them, only 12 cases wereaged<12 years) (Fig. 1).
Figure 1. A bar histogram is shown demonstrating the fre-quency of colorectal cancer in (A) 550,622 patients withcolorectal cancer diagnosed between 1973 and 2005 and (B)159 children/adolescents diagnosed during the same period.Numbers of patients were extracted from the Surveillance,Epidemiology, and End Results (SEER)*Stat frequency ses-sion and did not include patients with carcinoid tumors.
CRC in Children and Adolescents/Sultan et al
Cancer February 1, 2010 759

The age-adjusted incidence rates in children/adoles-cents and adults were 0.38 and 802 per million, respec-tively (both calculated from SEER 9 database and age-adjusted to the 2000 US standard population). There wasno significant change in rates noted over time (1973 to2005).
We compared the distribution of the main clinicalcharacteristics of pediatric patients with those of adults(Table 1). Unlike adults, who had an equal distributionbetween males and females, a higher percentage of males(62%) was found in children/adolescents.
Although adenocarcinoma NOS was the most fre-quently reported histologic subtype in both pediatric andadult groups, a significantly higher percentage of unfavor-able histologies was noted in pediatric cases: mucinousadenocarcinoma and signet ring cell carcinoma repre-sented 22% and 18% of cases, respectively. Adenocarci-noma arising in polyps occurred in 10% of children/adolescents and in 5.6% of patients aged > 20 years (Fig.2A). The most common sites of involvement in children/adolescents were the rectum/anal canal and transversecolon, whereas the rectum/anal canal and ascending
Table 1. Patient Characteristics
Variable Children/Adolescents
Adults P
No. (%) No. (%)
SexMale 99 (62) 277,790 (50) <.001
Female 60 (38) 272,832 (50)
RaceWhite 113 (71) 467,303 (85) <.001
Black 23 (14) 46,916 (8.5)
Others 23 (14) 36,403 (6.6)
SiteAscending colon 27 (17) 148,770 (27) <.001
Transverse colon 41 (26) 72,074 (13)
Descending colon 19 (12) 26,667 (4.8)
Sigmoid colon 23 (14) 125,895 (23)
Rectum/anus 43 (27) 165,087 (30)
Large intestine, NOS 6 (3.8) 12,129 (2.2)
HistologyAdenocarcinoma, NOS 69 (43) 383,267 (70) <.001
Adenocarcinoma in polyp (including APC) 16 (10) 30,984 (5.6)
Mucinous adenocarcinoma 35 (22) 53,297 (10)
Signet ring cell carcinoma 28 (18) 4134 (1)
Others 11 (6.6) 78,940 (14)
GradeWell differentiated; I 15 (9.4) 60,164 (11) <.001
Moderately differentiated; II 54 (34) 296,269 (54)
Poorly differentiated; III 48 (30) 91,329 (17)
Undifferentiated; anaplastic; IV 3 (1.9) 5427 (1)
Unknown 39 (25) 97,433 (18)
StageLocalized 31 (19) 217,549 (40) <.001
Regional 67 (42) 206,952 (38)
Distant 59 (37) 100,945 (18)
Unstaged 2 (1.3) 25,176 (4.6)
Diagnosis era1973-1985 30 (19) 131,484 (24) .049
1986-1995 34 (21) 139,515 (25)
1996-2005 95 (60) 279,623 (51)
NOS indicates not otherwise specified; APC, adenomatous polyposis coli.
Original Article
760 Cancer February 1, 2010
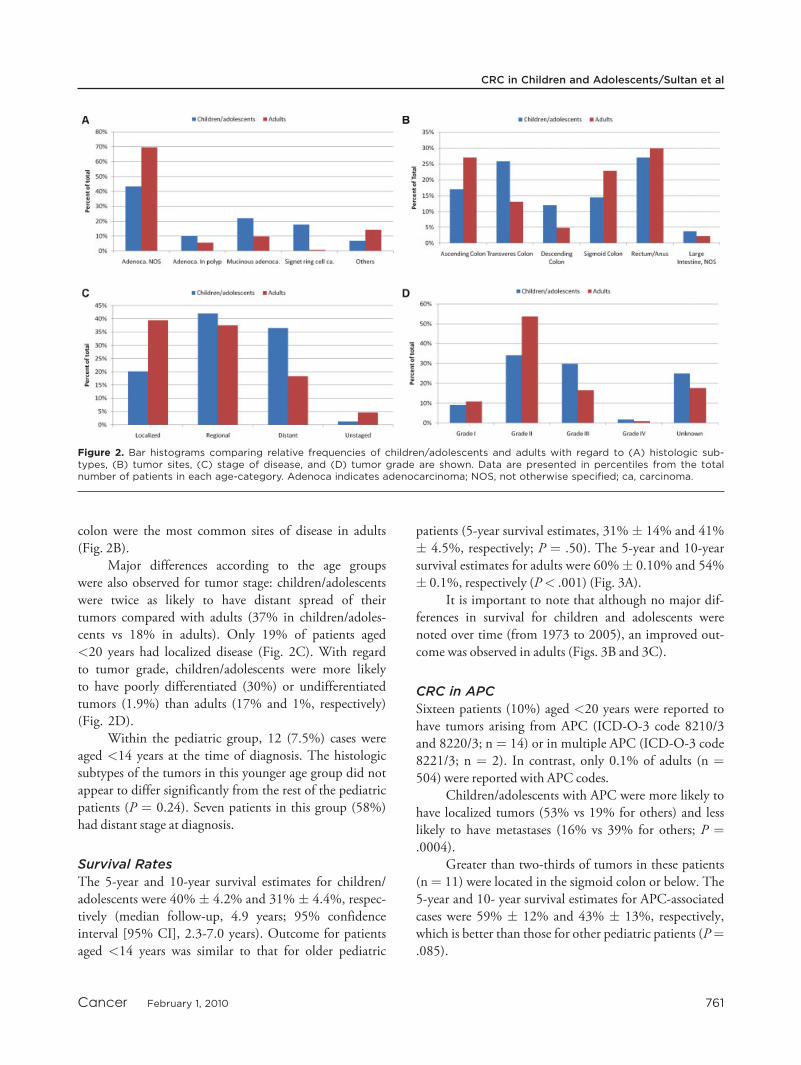
colon were the most common sites of disease in adults(Fig. 2B).
Major differences according to the age groupswere also observed for tumor stage: children/adolescentswere twice as likely to have distant spread of theirtumors compared with adults (37% in children/adoles-cents vs 18% in adults). Only 19% of patients aged<20 years had localized disease (Fig. 2C). With regardto tumor grade, children/adolescents were more likelyto have poorly differentiated (30%) or undifferentiatedtumors (1.9%) than adults (17% and 1%, respectively)(Fig. 2D).
Within the pediatric group, 12 (7.5%) cases wereaged <14 years at the time of diagnosis. The histologicsubtypes of the tumors in this younger age group did notappear to differ significantly from the rest of the pediatricpatients (P ¼ 0.24). Seven patients in this group (58%)had distant stage at diagnosis.
Survival Rates
The 5-year and 10-year survival estimates for children/adolescents were 40% � 4.2% and 31% � 4.4%, respec-tively (median follow-up, 4.9 years; 95% confidenceinterval [95% CI], 2.3-7.0 years). Outcome for patientsaged <14 years was similar to that for older pediatric
patients (5-year survival estimates, 31% � 14% and 41%� 4.5%, respectively; P ¼ .50). The 5-year and 10-yearsurvival estimates for adults were 60%� 0.10% and 54%� 0.1%, respectively (P< .001) (Fig. 3A).
It is important to note that although no major dif-ferences in survival for children and adolescents werenoted over time (from 1973 to 2005), an improved out-come was observed in adults (Figs. 3B and 3C).
CRC in APC
Sixteen patients (10%) aged <20 years were reported tohave tumors arising from APC (ICD-O-3 code 8210/3and 8220/3; n ¼ 14) or in multiple APC (ICD-O-3 code8221/3; n ¼ 2). In contrast, only 0.1% of adults (n ¼504) were reported with APC codes.
Children/adolescents with APC were more likely tohave localized tumors (53% vs 19% for others) and lesslikely to have metastases (16% vs 39% for others; P ¼.0004).
Greater than two-thirds of tumors in these patients(n¼ 11) were located in the sigmoid colon or below. The5-year and 10- year survival estimates for APC-associatedcases were 59% � 12% and 43% � 13%, respectively,which is better than those for other pediatric patients (P¼.085).
Figure 2. Bar histograms comparing relative frequencies of children/adolescents and adults with regard to (A) histologic sub-types, (B) tumor sites, (C) stage of disease, and (D) tumor grade are shown. Data are presented in percentiles from the totalnumber of patients in each age-category. Adenoca indicates adenocarcinoma; NOS, not otherwise specified; ca, carcinoma.
CRC in Children and Adolescents/Sultan et al
Cancer February 1, 2010 761

Patients With Multiple Primary Tumors
Sixteen patients (10%) aged<20 years had multiple regis-tered primary tumors. Four of them were reported withAPC codes. The first primary tumors were CRC in 10cases, and other malignancies in 6, in whom CRCoccurred as a second malignancy. Seven patients had >2malignancies. In 8 patients, >1 record of CRC was regis-tered as a primary tumor; these were not recurrent tumorsbut rather a new primary tumor that appeared at a differ-ent site, with a different histology, or both. Among thenon-CRC primary tumors, there were 7 brain tumors, 3sarcomas, 1 chronic myelogenous leukemia, 1 transitionalrenal cell carcinoma, and 1 case of follicular non-Hodgkinlymphoma.
In the adult group, 25% of cases had �2 primarytumors registered (n ¼ 139,309). When cases of multipleCRC primary tumors were excluded, the percentagedropped to 14% (n¼ 79,848).
Prognostic Factors in Children/Adolescents
When we investigated the association of different clinicalfactors with outcome using univariate analysis, sex, race,and primary tumor site did not appear to affect survival.
Conversely, tumor grade (P¼ .003) (Fig. 4A), pathologicsubtype (P ¼ .0008) (Fig. 4B), and tumor stage (P <
.001) (Fig. 4C) were found to be significantly associatedwith survival. The histologic subtypes found to be associ-ated with worse survival were mucinous adenocarcinoma(5-year survival rate, 27% � 8.1%) and signet ring cellcarcinoma (5-year survival rate, 13%� 7.0%).
When these factors, stage, grade, and histology, werecompared in a multivariate model using Cox proportionalhazards regression analysis, regional/distant stages had thehighest hazards ratio (HR) (HR, 3.15; 95% CI, 1.06-9.31[P ¼ .039]). Unfavorable grades (grades III and IV) werefound to be associated with an HR of 1.87 (95% CI,1.11-3.14; P¼ .019), whereas unfavorable histologic sub-types (mucinous adenocarcinoma and signet ring cell car-cinoma) lost significance (HR, 1.58; 95% CI, 0.94-2.65[P¼ .086]).
DISCUSSIONGiven the scant data on pediatric CRC available in the lit-erature, the possibility of performing a population-basedstudy using the SEER database offered a unique
Figure 3. Graphs demonstrating survival estimates comparing (A) children/adolescents and adults (P < .001, log-rank test), (B)only children/adolescents, and (C) adults during 3 arbitrarily defined periods are shown. The estimates in B and C were directlyderived from the Surveillance, Epidemiology, and End Results (SEER)*Stat survival session and were not compared directly usinga log-rank test, resulting in the lack of P values.
Original Article
762 Cancer February 1, 2010

opportunity to collect data on a large series of cases and tocompare clinical findings and outcomes with thoseobserved in adults. As may happen for other retrospectivepopulation-based studies, this analysis had some limita-tions (ie, the lack of pathologic review, the possibleunder–reporting of hereditary nonpolyposis colorectalcancer [HNPCC], the use of the less-accurate SEER stag-ing system instead of the Dukes classification or the AJCCstaging system [which has been documented in the SEERdatabase only since 2004], and the very limited treatment
data). Despite these limitations, our analysis reports someinteresting findings.
First, this series highlights the extreme rarity ofCRC in pediatric patients; in particular, this tumor wasfound to be an absolute exception in the prepubertal agegroup (the vast majority of the SEER cases occurred inadolescents).
As already documented by other authors,9-38 thecurrent analysis confirms that advanced stage at diagnosis,high occurrence of aggressive histologic subtypes (poorlydifferentiated, signet ring, and mucinous adenocarci-noma), and poor survival are the hallmarks of pediatricCRC.
Moreover, whereas improvement in outcome overthe period of analysis was noted in adults,39 no differencesin survival rates were documented for the group of chil-dren and adolescents included in the SEER database dur-ing the same period.
Several factors may contribute to the unsatisfactoryoutcome of children/adolescents with CRC. It is possiblethat the limited experience of pediatric oncologists andsurgeons may have a role; data from adult series indicatethat the experience and the level of specialization of thesurgeons was a prognostic variable.40-42 The SEER data-base does not provide adequate data regarding treatmentmodalities; therefore, any discussion on CRC therapy isbeyond the aims of the current study.
Children and adolescents with CRC presentedwith more advanced disease than their adult counter-parts. Whether the more advanced presentation isrelated to a delay in diagnosis or to an intrinsically moreaggressive behavior of the disease in younger ages isunclear. Although the latter variable is out of the physi-cian’s control, every effort should be made to improveearly diagnosis. Several studies have reported longerdiagnostic delays for children with CRC.9,11,12,15,17,22
Presenting signs and symptoms are often vague and non-specific (mild abdominal pain, constipation or diarrhea,hematochezia, weight loss), and might be underesti-mated. Thus, an effort must be made to educate healthproviders in the early recognition of this malignancy inchildren.35
At the current time, considerations of a differentbiology and pathogenesis of pediatric CRC are purelyspeculative. However, the high incidence of unfavorablehistologic subtypes, and the documentation of uniquemicrosatellite instability in younger patients,24,43 wouldsuggest some differences in pathogenesis. The biology ofCRC in adults is well known and its multistep process
Figure 4. Kaplan-Meier curves demonstrating survival esti-mates of children/adolescents compared according to (A) tu-mor grade, (B) histologic subtype, and (C) stage of diseaseare shown. All-cause mortality was used as an endpoint, andthe log-rank test was used to compare the curves with P val-ues shown on each panel. Adenoca indicates adenocarci-noma; NOS, not otherwise specified; ca, carcinoma.
CRC in Children and Adolescents/Sultan et al
Cancer February 1, 2010 763
(which is considered to evolve over approximately 10years) as well as the familial nature of early-onset tumorshave been widely described.43-47 In contrast, the tumori-genesis of childhood CRC, which necessarily occurs overa shorter period, is still unclear and most likely evolvesthrough different steps.24
The SEER database is not adequate to investigatefamily history and the association of neoplasms with he-reditary conditions. In this regard, no data were availableregarding an HNPCC association and molecular charac-terizations (APC gene, mismatch repair genes MLH1 andMSH2), and 10% of children and adolescent patientswere reported to have the APC codes, compared with only0.1% of adults.
Further studies are necessary to investigate thebiology of pediatric CRC. A better understanding ofthe molecular mechanisms underlying CRC may pavethe way to the development of new therapeuticapproaches. Given the extreme rarity of this tumor inthe pediatric age group, it will be only through collabo-rative efforts between clinicians and biologists, betweenthe different groups dedicated to pediatric rare tumors,3
and, more importantly, between the pediatric and adultoncologists and surgeons that advances will be made.Finally, it is our responsibility to improve awarenessand early referral to expert professionals, a measure thatmay result in an immediate favorable impact on theoutcome of these children.
CONFLICT OF INTEREST DISCLOSURESThe authors made no disclosures.
REFERENCES1. Parkin DM. Global cancer statistics in the year 2000. Lancet
Oncol. 2001;2:533-543.2. Pappo AS, Furman WL. Management of infrequent cancers
in childhood. In: Pizzo PA, Poplack DC, eds. Principlesand Practice of Pediatric Oncology. 5th ed. Philadelphia:Lippincott Williams & Wilkins; 2006:1172-1200.
3. Ferrari A, Bisogno G, De Salvo GL, Indolfi P, Perilongo G,Cecchetto G. The challenge of very rare tumours in child-hood: the Italian TREP project. Eur J Cancer. 2007;43:654-659.
4. Pastore G, De Salvo GL, Bisogno G, et al. Evaluating theaccess to pediatric cancer care centres of children and ado-lescents with rare tumors in Italy: the TREP project. PediatrBlood Cancer. 2009;53:152-155.
5. Surveillance, Epidemiology, and End Results (SEER) Pro-gram SEER*Stat Database: Incidence-SEER 17 Regs Lim-ited-Use þ Hurricane Katrina Impacted Louisiana Cases,Nov 2007 Submission (1973-2005 varying)-Linked To
County Attributes-Total U.S., 1969-2005 Counties. Be-thesda, Md: National Cancer Institute, Division of CancerControl and Population Sciences, Surveillance Research Pro-gram, Cancer Statistics Branch, 2008. Available at: http://www.seer.cancer.gov. Accessed January 9, 2009.
6. Steliarova-Foucher E, Stiller C, Lacour B, Kaatsch P. Inter-national Classification of Childhood Cancer, third edition.Cancer. 2005;103:1457-1467.
7. Greene F, Page D, Fleming I, et al. AJCC Cancer StagingHandbook. 6th ed. New York: Springer; 2002.
8. Dean AG, Sullivan KM, Soe MM. OpenEpi: Open SourceEpidemiologic Statistics for Public Health, Version. Avail-able at: www.OpenEpi.com, updated October 26, 2008.Accessed January 11, 2009.
9. Brown RA, Rode H, Millar AJ, Sinclair-Smith C, Cywes S.Colorectal carcinoma in children. J Pediatr Surg. 1992;27:919-921.
10. Cozart DT, Lang NP, Hauer-Jensen M. Colorectal cancerin patients under 30 years of age. Contributors to theSouthwestern Surgical Congress Unusual Case Registry. AmJ Surg. 1993;166:764-767.
11. Karnak I, Ciftci AO, Senocak ME, Buyukpamukcu N.Colorectal carcinoma in children. J Pediatr Surg. 1999;34:1499-1504.
12. Lamego CM, Torloni H. Colorectal adenocarcinoma inchildhood and adolescent. Report of 11 cases and review ofthe literature. Pediatr Radiol. 1989;19:504-508.
13. LaQuaglia MP, Heller G, Filippa DA, et al. Prognostic fac-tors and outcome in patients 21 years and under with colo-rectal carcinoma. J Pediatr Surg. 1992;27:1085-1089;discussion 1089-1090.
14. Pratt CB, Rao BN, Merchant TE, et al. Treatment ofcolorectal carcinoma in adolescents and young adultswith surgery, 5-fluorouracil/leucovorin/interferon-alpha 2aand radiation therapy. Med Pediatr Oncol. 1999;32:459-460.
15. Rao BN, Pratt CB, Fleming ID, Dilawari RA, Green AA,Austin BA. Colon carcinoma in children and adolescents. Areview of 30 cases. Cancer. 1985;55:1322-1326.
16. Rodriguez-Bigas MA, Mahoney MC, Weber TK, PetrelliNJ. Colorectal cancer in patients aged 30 years or younger.Surg Oncol. 1996;5:189-194.
17. Sebbag G, Lantsberg L, Arish A, Levi I, Hoda J. Colon car-cinoma in the adolescent. Pediatr Surg Int. 1997;12:446-448.
18. Shahrudin MD, Noori SM. Cancer of the colon and rectumin the first three decades of life. Hepatogastroenterology.1997;44:441-444.
19. Taguchi T, Suita S, Hirata Y, Ishii E, Ueda K. Carcinomaof the colon in children: a case report and review of 41Japanese cases. J Pediatr Gastroenterol Nutr. 1991;12:394-399.
20. Andersson A, Bergdahl L. Carcinoma of the colon in chil-dren: a report of six new cases and a review of the literature.J Pediatr Surg. 1976;11:967-971.
21. Bhatia S, Pratt CB, Sharp GB, Robison LL. Family historyof cancer in children and young adults with colorectal can-cer. Med Pediatr Oncol. 1999;33:470-475.
22. Chantada GL, Perelli VB, Lombardi MG, et al. Colorectalcarcinoma in children, adolescents, and young adults.J Pediatr Hematol Oncol. 2005;27:39-41.
23. Chen LK, Hwang SJ, Li AF, Lin JK, Wu TC. Colorectalcancer in patients 20 years old or less in Taiwan. South MedJ. 2001;94:1202-1205.
Original Article
764 Cancer February 1, 2010

24. Durno C, Aronson M, Bapat B, Cohen Z, Gallinger S.Family history and molecular features of children, adoles-cents, and young adults with colorectal carcinoma. Gut.2005;54:1146-1150.
25. Endreseth BH, Romundstad P, Myrvold HE, Hestvik UE,Bjerkeset T, Wibe A. Rectal cancer in the young patient.Dis Colon Rectum. 2006;49:993-1001.
26. Jerkic S, Rosewich H, Scharf JG, et al. Colorectal cancer intwo pre-teenage siblings with familial adenomatous polypo-sis. Eur J Pediatr. 2005;164:306-310.
27. Kam MH, Eu KW, Barben CP, Seow-Choen F. Colorectalcancer in the young: a 12-year review of patients 30 yearsor less. Colorectal Dis. 2004;6:191-194.
28. Lee PY, Fletcher WS, Sullivan ES, Vetto JT. Colorectal can-cer in young patients: characteristics and outcome. Am Surg.1994;60:607-612.
29. Minardi AJ Jr, Sittig KM, Zibari GB, McDonald JC. Colo-rectal cancer in the young patient. Am Surg. 1998;64:849-853.
30. Radhakrishnan CN, Bruce J. Colorectal cancers in childrenwithout any predisposing factors. A report of eight cases andreview of the literature. Eur J Pediatr Surg. 2003; 13:66-68.
31. Stones DK, McGill N. Colon carcinoma in African chil-dren. Med Pediatr Oncol. 2003;40:410-411.
32. Sule AZ, Mandong BM. Malignant colorectal tumours inpatients 30 years and below: a review of 35 cases. Cent Afr JMed. 1999;45:209-212.
33. Toki A, Todani T, Watanabe Y, Ogura K, Miyauchi A,Agatsuma Y. Carcinoma of the colon in childhood; reportof 2 cases expressing p53 without K-ras mutation. Eur JPediatr Surg. 1997;7:315-317.
34. Vastyan AM, Walker J, Pinter AB, Gerrard M, Kajtar P.Colorectal carcinoma in children and adolescents—a reportof seven cases. Eur J Pediatr Surg. 2001;11:338-341.
35. Ferrari A, Rognone A, Casanova M, et al. Colorectal carci-noma in children and adolescents: the experience of the Isti-tuto Nazionale Tumori of Milan, Italy. Pediatr BloodCancer. 2008;50:588-593.
36. Kravarusic D, Feigin E, Dlugy E, et al. Colorectal carci-noma in childhood: a retrospective multicenter study.J Pediatr Gastroenterol Nutr. 2007;44:209-211.
37. Goldthorn JF, Powars D, Hays DM. Adenocarcinoma ofthe colon and rectum in the adolescent. Surgery. 1983;93:409-414.
38. Chung YF, Eu KW, Machin D, et al. Young age is not apoor prognostic marker in colorectal cancer. Br J Surg.1998;85:1255-1259.
39. Mitry E, Bouvier AM, Esteve J, Faivre J. Improvement incolorectal cancer survival: a population-based study. Eur JCancer. 2005;41:2297-2303.
40. Goligher J. Colorectal surgery as a specialty. Dis Colon Rec-tum. 1997;40:733-735.
41. Simons AJ, Ker R, Groshen S, et al. Variations in treatmentof rectal cancer: the influence of hospital type and caseload.Dis Colon Rectum. 1997;40:641-646.
42. Porter GA, Soskolne CL, Yakimets WW, Newman SC. Sur-geon-related factors and outcome in rectal cancer. Ann Surg.1998;227:157-167.
43. Kim HC, Kim CN, Yu CS, Roh SA, Kim JC. Methylationof the hMLH1 and hMSH2 promoter in early-onset spo-radic colorectal carcinomas with microsatellite instability. IntJ Colorectal Dis. 2003;18:196-202.
44. Fearon ER. Human cancer syndromes: clues to the originand nature of cancer. Science. 1997;278:1043-1050.
45. Lynch HT, Smyrk T, Lynch J. An update of HNPCC(Lynch syndrome). Cancer Genet Cytogenet. 1997;93:84-99.
46. Leppert M, Dobbs M, Scambler P, et al. The gene for fami-lial polyposis coli maps to the long arm of chromosome 5.Science. 1987;238:1411-1413.
47. Losi L, Di Gregorio C, Pedroni M, et al. Molecular geneticalterations and clinical features in early-onset colorectal carci-nomas and their role for the recognition of hereditary cancersyndromes. Am J Gastroenterol. 2005;100:2280-2287.
CRC in Children and Adolescents/Sultan et al
Cancer February 1, 2010 765