distribution of misoprostol at antenatal care visits for...
TRANSCRIPT
March 2012
Distribution of Misoprostol at Antenatal Care Visits for Prevention of Postpartum Hemorrhage in Ghana FINAL REPORT
ii
Ghana Health Service (GHS) is the service delivery arm of the Ghana Ministry of Health and is charged with implementing the policies of the Ghana Ministry of Health and providing health care services, with an emphasis on the primary care level, for the people of Ghana.
Venture Strategies Innovations (VSI) is a California-‐based nonprofit organization committed to improving women's health in developing countries by creating access to effective and affordable technologies on a large scale. VSI’s innovative approach involves partnerships that build upon existing infrastructure, resources and markets. VSI focuses on reducing barriers to access and enhancing human capacity to bring about sustainable improvements in health.
Ghana Health Service The Director General Ghana Health Service Private Mail Bag Ministries Post Office Accra, Ghana West Africa Tel: 0302-‐662013 Website: www.ghanahealthservice.org Venture Strategies Innovations 2401 East Katella Avenue, Suite 400 Anaheim, California 92806 USA Tel +1 714 221 2040 Website: www.vsinnovations.org

iii
Foreword
Every 90 seconds, a woman dies in pregnancy or childbirth. This is preventable and unacceptable. In Ghana, maternal health is a priority and Ghana Health Service (GHS) has implemented numerous maternal health initiatives to prevent women from dying during pregnancy and childbirth. Indeed, the GHS Reproductive Health Strategic Plan 2007-‐2011 listed six strategic objectives, the first of which was to reduce maternal mortality and morbidity. Trends indicate that maternal mortality in Ghana has been decreasing; however, progress must be accelerated. Ghana Health Service remains committed to achieving this target and is working diligently with partners to reduce maternal mortality. Hemorrhage is the single largest cause of maternal death in Ghana, causing 24% of all maternal deaths. Misoprostol tablets are a safe, affordable and effective means of preventing postpartum hemorrhage (PPH) and can provide protection to women who do not have access to other interventions for PPH prevention. Due to its ease of use and stability in hot temperatures, misoprostol has the potential to play an important role in the reduction of maternal mortality in Ghana, especially in settings where other uterotonic drugs such as oxytocin may not be feasible. Beginning in 2009, Ghana Health Service and the USA-‐based nongovernmental organization Venture Strategies Innovations collaborated to pilot the distribution of misoprostol to pregnant women at antenatal care visits for prevention of PPH. The success of this project would not have been possible without the dedicated efforts of both organizations. The results demonstrate that scaling up misoprostol distribution in Ghana could substantially increase births protected from PPH and thereby contribute to a reduction in maternal mortality. Dr. Gloria Quansah Asare
Director, Family Health Division Ghana Health Service

iv
Acknowledgements
This project could not have been completed without the contributions of the expert staff and colleagues at Ghana Health Service (GHS) and Venture Strategies Innovations (VSI), whose dedication to this pilot and invaluable contributions to its development led to its successful implementation. Jennet Arcara, former VSI Country Programs Manager, initiated the preliminary work on this pilot project, and oversaw the activities until July 2011. During its implementation, the project benefited from the participation of the GHS District Health Management Teams, including the District Public Health Nurses, who conducted monitoring activities, and Disease Control and Health Information Officers, who played an essential role in data entry and management. Dr. Kwame Amponsa-‐Achiano from GHS expertly managed and analyzed the data for the final report. Bernard E.K. Vikpeh-‐Lartey provided significant support with project monitoring.
The members of the Ministry of Health’s Technical Advisory Group (TAG) reviewed the information, education and communication (IEC) materials and data collection tools, and provided supervision throughout the project.
TAG Members: Prof. S.W.K. Adadevoh, Consultant Obstetrician/Gynecologist Dr. Erasmus E. A. Agongo, Regional Director of Health Service, Eastern Region Health Directorate Abena Amoakohene, Regulatory Officer, Food & Drugs Board Dr. K. Amponsa-‐Achiano, Epidemiologist/Public Health Specialist, Family Health Division, GHS Dr. Gloria Quansah Asare, Director, Family Health Division, GHS Dr. Cynthia Bannerman, Director, Institutional Care Division, GHS Gladys Brew, Safe Motherhood Program Officer, GHS Mimi Deles Darko, Head, Safety Monitoring Department, Food & Drugs Board Dr. Patrick Kuma-‐Aboagye, Deputy Director, Family Health Division, GHS Dr. Frank Nyonator, Director, Policy, Planning, Monitoring & Evaluation Division, GHS Dr. Ali Samba, Obstetrician/Gynecologist, University of Ghana Medical School/Korle Bu Teaching Hospital Samuel Sosi, Municipal Director of Health Service, Elmina Dr. Joe Taylor (deceased October 2011), Consultant Obstetrician/Gynecologist VSI Project Team: Dr. Nuriye Nalan Sahin Hodoglugil, Associate Medical Director Martine Holston, Director, Research and Implementation Molly Moran, Monitoring and Evaluation Specialist Bibiana Irene Bangpuori, Project Coordinator Deborah Koh, Acting Country Programs Manager Emma Nesper Holm, Senior Communications Manager Joanna Ortega, Project Intern Furthermore, the project would not have been possible without the valued contributions of the participating antenatal care providers, community health volunteers and traditional birth attendants.

v
Executive Summary
Ghana signed the United Nations Millennium Declaration and committed to the Millennium Development Goals (MDGs) in September 2000. The fifth MDG aims to reduce the maternal mortality ratio by three-‐quarters, and Ghana Health Service (GHS) has since strategically implemented numerous maternal health initiatives to decrease the country’s maternal mortality. While trends indicate that maternal mortality in Ghana has been decreasing, maternal deaths still occur at a rate of 350 per 100,000 live births, and approximately 24% of these deaths are due to hemorrhage. Postpartum hemorrhage (PPH), or excessive bleeding after delivery, can be prevented using a uterotonic drug as part of the active management of the third stage of labor. Ghana Health Service is committed to ensuring all women receive coverage with a uterotonic drug at the time of delivery to prevent PPH. For facility deliveries, oxytocin is the uterotonic of choice. Misoprostol is a safe, affordable and effective alternative uterotonic drug that can be used to prevent PPH where oxytocin is not feasible or available. It is jointly recommended by the International Federation of Gynecology and Obstetrics and the International Confederation of Midwives as the only available technology to protect against PPH during home births without a skilled attendant. In Ghana, 42% of women deliver at home, yet 95% of women attend at least one antenatal care (ANC) visit with a health care professional during pregnancy. Therefore, ANC represents a key opportunity to reach women with misoprostol and reduce maternal death due to PPH. As part of larger efforts to establish sustainable policies and programs to reduce maternal mortality, the use of misoprostol in obstetrics and gynecology has been integrated into the 2010 Ghana Standard Treatment Guidelines. With support from the USA-‐based nongovernmental organization Venture Strategies Innovations, GHS conducted a pilot project to demonstrate the safety, feasibility and program-‐effectiveness of misoprostol distribution to expectant mothers at ANC visits, in order to increase uterotonic coverage for all women at delivery, as well as to provide evidence to inform policy on the use and expansion of misoprostol for PPH prevention in Ghana. The project was conducted in four districts: Birim South, Komenda-‐Edina-‐Eguafo-‐Abirem (KEEA), Sene and Upper Manya Krobo, so that feasibility issues in different settings could be better understood. The pilot project consisted of two components. The first was a community awareness campaign to ensure that all women were informed on birth preparedness, the importance of facility deliveries, the risk of PPH, and PPH prevention. In support of the community awareness campaign, traditional birth attendants (TBAs) conducted awareness meetings with community leaders and women’s groups as well as one-‐on-‐one information sessions with pregnant women. Community health volunteers (CHVs) received orientation on the project so that they could share these key messages with their communities. The second component of the project was the distribution of misoprostol tablets directly to women who had reached 12 weeks gestation when attending ANC visits. ANC providers trained on the pilot protocol distributed misoprostol, along with a pictorial brochure, to enrolled pregnant women during routine ANC after screening for eligibility and educating them on the use of misoprostol tablets for PPH prevention.

vi
ANC providers began enrolling women in the project in April 2011 and continued through January 2012. In all, providers enrolled 5,345 women who came for ANC, and almost all (99%) took misoprostol tablets home. Follow-‐up was done with 3,615 women after delivery to collect information on their delivery experience and the use of misoprostol. TBAs collected information from 1,456 women on the use of misoprostol at home deliveries they attended. It is important to note that during the course of the pilot, the original batches of misoprostol were recalled due to quality issues and replaced with another brand of misoprostol tablets. This recall took place in July and August 2011, and all tablets were replaced by September 1, 2011. Data was analyzed for Phase 1 (April-‐August 2011) and Phase 2 (September 2011-‐January 2012) to account for the drug recall process during the course of the pilot. Overall, enrollment in the project was about half of all new ANC registrants (47%) when both phases were combined. However, enrollment was lowest during the months of recall, as distribution of tablets was slowed down while tablets were being replaced and staff informed about recall procedures. After the completion of the recall, enrollment gradually increased during Phase 2, reaching 64% of new ANC registrants in December 2011. In line with project goals, uterotonic coverage with misoprostol at home deliveries was very high across all districts, ranging from 88% in KEEA to 96% in Sene. Overall, 93% (n=1,261) of the women who delivered at home swallowed the misoprostol tablets they had with them after delivery. Without misoprostol, these women would not have received any protection from PPH, the leading cause of maternal death. The level of facility where women received misoprostol varied by district, and health centers were the location where the majority (56%) of women enrolled in the pilot received misoprostol. Community-‐based Health Planning and Services (CHPS) compounds were also instrumental for reaching rural women and contributed 23% of all misoprostol distribution, most significantly in Birim South, where they accounted for about half of all distribution (52%). Results of the pilot show that enrolled women used misoprostol correctly and safely. Women reported using misoprostol correctly (correct dose, route and timing) at home deliveries 99% of the time. Further, based on data from home deliveries with TBAs, 95% of women who used misoprostol experienced no side effects due to misoprostol. For the subset of women who enrolled during Phase 2, 364 used misoprostol at a home delivery, and only four (1%) reported excessive bleeding (classified as PPH); none required referral. Women were also very diligent in returning unused misoprostol tablets back to facilities, and retrieval of unused tablets was very high. Overall, among the women in the follow-‐up group who reported taking misoprostol home from ANC (n=3,577), 95% either used the tablets at a home or facility delivery or returned them to the facility, leaving only 5% of women who did not return the tablets.
Findings from this report demonstrate that the distribution of misoprostol to pregnant women at ANC visits has the potential to increase the number of women who receive a uterotonic drug for prevention of PPH at the time of delivery. This finding is particularly pertinent for women who deliver at home and for whom oxytocin is not feasible.
Based on the results of this report, the main recommendation is a phased nationwide scale-‐up of community-‐level distribution of misoprostol for PPH prevention in all districts in Ghana. The findings also indicate that there are some challenges related to the integration of misoprostol distribution at ANC within the current health system, mostly reflected in the enrollment rates. To overcome these

vii
challenges in the scale-‐up phase, it is recommended that all ANC providers, including the lower cadres, be trained to provide information and distribute misoprostol to pregnant women during routine ANC visits. Training additional health providers to educate women and distribute misoprostol for PPH prevention will alleviate the workload of midwives and contribute to all women receiving this important intervention at ANC even in areas where the patient burden is high.
In the scale-‐up phase, community awareness efforts with TBAs and CHVs should continue. TBAs should continue to be informed on the correct use of misoprostol for PPH prevention so they can aid women in taking misoprostol at the home deliveries that they attend.
In addition, to ensure that all women, particularly those who are unable to deliver in a health facility, have access to a uterotonic drug to reduce PPH-‐related maternal mortality, efforts to expand the availability of misoprostol should be undertaken, including registration with Ghana Food and Drugs Board and distribution to all facilities. Scale-‐up of misoprostol for prevention of PPH will complement Ghana’s broader safe motherhood initiatives and serve as a key strategy for reaching the MDG 5 target of reducing maternal mortality by three quarters by the year 2015.

viii
Acronyms and Local Terms
ANC Antenatal care
CHN Community Health Nurse; health professionals who provide clinical sessions, including antenatal and postnatal care. CHNs are not trained to perform deliveries.
CHPS Community-‐based Health Planning and Services; a primary health care initiative in Ghana and the name for the primary health care compounds that have been constructed in rural areas.
CHV Community Health Volunteer; this cadre of volunteer was created in conjunction with the Community-‐based Health Planning and Services initiative.
CHW Community Health Worker
DCO Disease Control Officer; heath workers trained in disease surveillance and data management. DCOs form part of the District Health Management Team.
DHMT District Health Management Team; comprised of the District Director, District Public Health Nurse, District Health Information Officer, District Disease Control Officer(s) and/or District Nutrition Officer. This team is responsible for health service delivery at the district level.
Durbar Community meeting
FDB Food and Drugs Board; Ghana’s food and drug regulatory agency
FIGO International Federation of Gynecology and Obstetrics
GHS Ghana Health Service
GSS Ghana Statistical Service
HIO Health Information Officer; health workers trained in health information systems, data management and statistics. HIOs are part of the District Health Management Team.
ICM International Confederation of Midwives
IEC Information, education and communication
PNC Postnatal care
PPH Postpartum hemorrhage; vaginal bleeding in excess of 500 mL during and after delivery
TAG Technical Advisory Group
TBA Traditional birth attendant
VSI Venture Strategies Innovations
WHO World Health Organization

ix
Table of Contents
Foreword ............................................................................................................................................... iii Acknowledgements ............................................................................................................................... iv Executive Summary ................................................................................................................................ v Acronyms and Local Terms .................................................................................................................. viii Table of Contents .................................................................................................................................. ix List of Boxes, Tables and Figures ............................................................................................................ x 1. Introduction ....................................................................................................................................... 1
1.1 Postpartum Hemorrhage in Ghana ............................................................................................................ 1 1.2 Misoprostol for Prevention of PPH ............................................................................................................. 1 1.3 Rationale for Misoprostol Distribution for Prevention of PPH at Home Deliveries .................................... 2 1.4 Misoprostol in Ghana ................................................................................................................................. 2
2. Project Description ............................................................................................................................ 2 2.2 Location and Participants ........................................................................................................................... 3 2.3 Project Timeline .......................................................................................................................................... 5
3. Methods ............................................................................................................................................ 6 3.1 Strategy and Design .................................................................................................................................... 6 3.2 Project Organizational Structure ................................................................................................................ 9 3.3 Project Training .......................................................................................................................................... 9 3.4 Data Collection and Management ............................................................................................................ 10 3.4.1 Data Collection Tools ............................................................................................................................. 10 3.4.2 Data Entry, Management and Analysis ................................................................................................. 11
4. Results ............................................................................................................................................. 11 4.1 Women Reached and Data Used for Analysis .......................................................................................... 11 4.2 Misoprostol Distribution at ANC .............................................................................................................. 11 4.3 Delivery Characteristics and Uterotonic Coverage ................................................................................... 15 4.4 Safety: Correct Use of Misoprostol at Home Deliveries and Return of Unused Misoprostol ................... 17 4.5 Program Effectiveness: Perceived PPH and Referrals .............................................................................. 18 4.6 Home Deliveries with TBAs ...................................................................................................................... 19
5. Major Conclusions and Discussion .................................................................................................. 20 6. Recommendations ........................................................................................................................... 23 7. References ....................................................................................................................................... 25

x
List of Boxes, Tables and Figures
Box 1: Pilot project goals and objectives ................................................................................................ 3 Box 2: Key messages of community awareness campaign ..................................................................... 7 Box 3: Eligibility criteria for the pilot project .......................................................................................... 8 Box 4: Provider perspectives ................................................................................................................ 20 Table 1: Participating pilot project facilities by district .......................................................................... 3 Table 2: Maternal health statistics by project district ............................................................................ 4 Table 3: Health workers trained or oriented during the pilot, by district ............................................ 10 Table 4: Misoprostol distribution data collected ................................................................................. 11 Table 5: Enrollment data ...................................................................................................................... 12 Table 6: Misoprostol distribution at ANC ............................................................................................. 13 Table 7: Delivery characteristics of women who took misoprostol home from ANC ........................... 16 Table 8: Uterotonic drug at delivery .................................................................................................... 16 Table 9: Correct use of misoprostol at home deliveries ....................................................................... 17 Table 10: Deliveries attended by TBAs ................................................................................................. 19 Table 11: Reported experience of side effects among misoprostol users at TBA deliveries ................ 19 Figure 1: Pilot project districts ............................................................................................................... 4 Figure 2: Project timeline ....................................................................................................................... 6 Figure 3: Organizational structure of the project ................................................................................... 9 Figure 4: Proportion of new ANC registrants enrolled over the course of the pilot ............................ 12 Figure 5: Flow chart of women's participation in the pilot project ...................................................... 13 Figure 6: Total number and proportion of women living outside the catchment area by district ....... 14 Figure 7: Location of misoprostol distribution ..................................................................................... 15 Figure 8: Uterotonic coverage at home deliveries ............................................................................... 17 Figure 9: Return of unused misoprostol ............................................................................................... 18

1
1. Introduction
1.1 POSTPARTUM HEMORRHAGE IN GHANA In Ghana, maternal mortality continues to be high at a rate of 350 maternal deaths per 100,000 live births (World Health Organization (WHO), 2010). According to data from 2007, hemorrhage accounts for almost 24% of maternal deaths in Ghana (Ghana Statistical Service (GSS), Ghana Health Service (GHS) and Macro International, 2009a), and the risk of death due to hemorrhage is higher for Ghanaian women living in rural areas (Asamoah et al., 2011). Most often, postpartum hemorrhage (PPH) occurs within a few hours after delivery, and there are no risk factors that consistently predict which women will experience PPH (Prata et al., 2011). Any delay in the management of obstetric emergencies, especially PPH, can have fatal consequences.
However, PPH is both a preventable and treatable condition. The use of a uterotonic drug immediately after the birth of a newborn, as a component of active management of the third stage of labor, is one of the most important interventions that can be used to prevent PPH. Oxytocin is the current recommended uterotonic of choice for preventing and treating PPH, and is administered by a skilled provider to women who deliver in a health facility. However, 41% of all deliveries in Ghana still take place without a skilled provider (GSS, GHS and ICF Macro, 2009b). For these women, oxytocin is not a feasible intervention for preventing PPH, as it requires administration of an injection by a skilled provider and refrigerated storage.
1.2 MISOPROSTOL FOR PREVENTION OF PPH Misoprostol is an important alternative uterotonic drug for prevention and treatment of PPH. Misoprostol is ideal for use at home deliveries because it is administered orally, inexpensive, easy to store, and has an excellent safety profile (Parsons et al., 2007; Derman et al., 2006; Alfirevic et al., 2007; Potts, 2006; USAID, 2011). When used in home deliveries, where no other medicine is available, it is shown to decrease the risk of PPH approximately by half (Derman et al., 2006).
Numerous studies have demonstrated the effectiveness of misoprostol in reducing PPH in community settings (Mobeen et al., 2011; Prata et al., 2009). Research also demonstrates that when educated on the proper use of misoprostol by a community health worker (CHW), women are capable of safely self-‐administering misoprostol at home births (Rajbhandari et al., 2010; Sanghvi et al., 2010). When misoprostol is available at home deliveries, more women receive a uterotonic drug for prevention of PPH, especially lower-‐income women living in remote areas (Rajbhandari et al., 2010; Prata et al., 2012). Moreover, in Afghanistan, births with skilled providers were found to be higher in areas where misoprostol was made available directly to women, likely due to the reinforcement of messages by CHWs of the importance of delivering in a health facility (Sanghvi et al., 2010).
Misoprostol has been recognized by the international community for its potential to reduce PPH at the community level. The International Federation of Gynecology and Obstetrics (FIGO) and the International Confederation of Midwives (ICM) have jointly recommended that in home births without a skilled attendant, misoprostol may be the only available technology to control PPH (ICM/FIGO, 2006). Further, the World Health Organization included misoprostol for prevention of PPH in its Model List of Essential Medicines in May 2011 (WHO, 2011).

2
1.3 RATIONALE FOR MISOPROSTOL DISTRIBUTION FOR PREVENTION OF PPH AT HOME DELIVERIES While all women should ideally deliver in a health facility with a skilled provider, numerous barriers prevent women from delivering in facilities, such as costs, availability of transport, and delays in identifying life-‐threatening complications (Cotter et al., 2006; Amooti-‐Kaguna and Nuwaha, 2000; Duong et al., 2004). Therefore, it is essential to focus on reaching women where they are by linking rural women to life-‐saving maternal health technologies, such as misoprostol.
While almost all women in Ghana (95%) attend at least one antenatal care (ANC) visit, 42% deliver at home (GSS, GHS and ICF Macro, 2009b). Therefore, ANC is a critical point of contact for reaching women with messages about safe motherhood. In addition, it is a key opportunity to distribute misoprostol to pregnant women, thus ensuring that all expectant mothers will receive a uterotonic drug at delivery for PPH prevention regardless of where they deliver. The distribution of misoprostol to pregnant women at ANC, which is referred to as community-‐level distribution because it puts the drug into the hands of women to take home, allows women who deliver at home to have access to a uterotonic drug at birth. In conjunction with the distribution of misoprostol, it is essential to provide education and counseling on safe motherhood, the use of misoprostol for PPH prevention, and the need for skilled attendance at delivery.
1.4 MISOPROSTOL IN GHANA The Ghana Health Service Reproductive Health Strategic Plan 2007-‐2011 lists six strategic objectives, the first of which is to reduce maternal mortality and morbidity. In 2004, misoprostol was included on the Essential Medicines List of Ghana. In 2008, the Ghana Food and Drugs Board (FDB) approved the registration of misoprostol as a program drug to be used in a pilot project to demonstrate the feasibility of misoprostol for prevention of PPH in the Ghanaian context. In May 2009, Ghana Health Service (GHS) and Venture Strategies Innovations (VSI) began planning work to conduct such a pilot project in Ghana to demonstrate the feasibility of the distribution of misoprostol at ANC visits for the prevention of PPH. Misoprostol was incorporated into the 2010 Ghana Standard Treatment Guidelines for obstetric uses, including induced abortion, missed abortion, incomplete abortion, intrauterine fetal death, induction of labor, cervical ripening, and prevention and treatment of PPH. VSI is currently working with GHS and the FDB to register another misoprostol product in the country for obstetric indications.
2. Project Description
In April 2011, GHS and VSI collaboratively launched the implementation of the pilot project in four districts in Ghana to demonstrate the safety, feasibility and program-‐effectiveness of misoprostol distribution to expectant mothers at ANC visits. The pilot project aimed to reach as many women as possible with a uterotonic drug at delivery in order to prevent PPH and associated maternal morbidity and mortality. In addition to employing ANC providers as points of misoprostol distribution, the pilot project involved traditional birth attendants (TBAs) and community health volunteers (CHVs) to disseminate educational messages about safe delivery and misoprostol in order to ensure that women in the community knew about the availability of misoprostol at health facilities.

3
Box 1: Pilot project goals and objectives
The results of the pilot project presented in this report provide GHS with evidence necessary to inform policy on the use of misoprostol for PPH prevention in Ghana. The implementation structure of this project is expected to serve as a model that can be scaled up in Ghana and can be applicable in other settings where many women deliver at home (with or without the presence of a skilled attendant), and where oxytocin may not be feasible.
Institutional Review Board approval for this project was obtained from Ghana Health Service Ethical Review Committee on 25 February 2010, with the ethical clearance ID number: GHS-‐ERC: 01/11/09.
2.2 LOCATION AND PARTICIPANTS All functioning facilities that provide ANC in the four pilot districts (Birim South, KEEA, Upper Manya Krobo and Sene) participated in the project, with the exception of one maternity home in KEEA. In total, 27 Community-‐based Health Planning and Services (CHPS) compounds, 14 health centers, four hospitals and three maternity homes participated in the project (Table 1). CHPS are primary health care compounds that have been constructed in rural areas as part of a primary health care initiative in Ghana. Maternity homes are private facilities where women can receive maternal health services (ANC, delivery, etc.). Project staff recruited TBAs who were previously trained by GHS from across all four districts and oriented them on how to support a delivering woman who had received misoprostol at ANC in using the tablets at delivery. In addition, CHVs were oriented to disseminate messages about the importance of delivering in a health facility, and preparing for a safe delivery, as well as the availability of misoprostol for the prevention of PPH.
Table 1: Participating pilot project facilities by district
Birim South KEEA Sene Upper Manya Krobo Total
CHPS compounds 14 6 5 2 27 Health centers 3 4 3 4 14 Hospitals 0 2 1 1 4 Maternity homes 0 1 0 2 3 Total 17 13 9 9 48
Pilot P rojec t Goals 1) Reduce maternal mortality and morbidity due to postpartum hemorrhage (PPH); 2) Provide empirical evidence to inform policy on misoprostol distribution through
antenatal care (ANC) for the prevention of PPH. Pilot P rojec t Obj ectives 1) Demonstrate that ANC visits are a feasible and effective mechanism for distributing
misoprostol for PPH prevention to women who cannot reach a facility to deliver and give birth at home.
2) Provide evidence that women can safely self-‐administer misoprostol for prevention of PPH at home births after being educated on and receiving the drug at ANC visits.
3) Generate evidence to inform policy in Ghana for a nationwide scale-‐up of misoprostol distribution through ANC.

4
The pilot project was conducted in four districts: Birim South and Upper Manya Krobo in the Eastern Region, Komenda-‐Edina-‐Eguafo-‐Abirem (KEEA) in the Central Region and Sene in the Brong Ahafo Region (Figure 1), which have a combined estimated population of approximately 405,890 (Table 2). All districts have fairly high rates of ANC attendance, ranging from 71% in Upper Manya Krobo to 96% in Sene. Table 2 further specifies the population, ANC coverage, facility deliveries and health service providers in each of the project areas.
Figure 1: Pilot project districts
Table 2: Maternal health statistics by project district
Sene KEEA Upper Manya Krobo Birim South
Population (2010) 105,1801 138,4103 92,2256 70,0757 Estimated ANC coverage (2010) 96.3%2 86.3%4 70.7%6 77.2%7 Percentage live births delivered at a health facility8
64.7% 51.7% 59.0% 59.0%
Number of working midwives 31 115 146 97 Number of doctors 11 15 26 07 1 District Profile. Sene District, 2010. 2 Reproductive and Child Health Annual Report. Sene District, 2010. 3 Demographic Data. Komenda-‐Edina-‐Eguafo-‐Abirem District, 2010. 4 Reproductive and Child Health Annual Report. Komenda-‐Edina-‐Eguafo-‐Abirem District, 2010. 5 Half Year Report, Komenda-‐Edina-‐Eguafo-‐Abirem District, 2011 6 Reproductive and Child Health Annual Report. Upper Manya Krobo District, 2010. 7 Reproductive and Child Health Annual Report. Birim South District, 2010 8 Regional estimates (GSS, GHS and ICF Macro, 2009b)
The population of Sene District is sparsely distributed over a large area, and there is only one road that is accessible throughout the year, making delivery of health services difficult. In both Sene and Upper Manya Krobo, a number of communities are located on islands in the Volta Lake and face additional transportation challenges in accessing health services as a result. Both districts in the Eastern Region, Upper Manya Krobo and Birim South, are primarily rural. The majority of the population in Upper Manya Krobo speaks Krobo, Twi and Ewe (District Profile, Upper Manya Krobo District, 2011), while in Birim South an overwhelming majority of the population (90%) is Akan and speaks Twi (District Profile, Birim South District, 2010). The coastal district of KEEA is located in the more urbanized Central Region, and Fante and English are the main languages spoken (Half Year Report, KEEA District, 2011).

5
2.3 PROJECT TIMELINE The planning, implementation and analysis of this project took place over three years (Figure 2). GHS was responsible for the ongoing management and oversight of the project activities. VSI provided financial and technical support to the project, including the development of data collection tools, training materials, monitoring and evaluation design, and assistance with data management and analysis.
The project proposal, community awareness campaign materials, manual of operations and data collection tools were developed and finalized between May 2009 and April 2011. The initial project training for master trainers occurred between September 29 and October 1, 2010, and was followed by trainings of health personnel in the project districts. After the completion of district trainings and finalization of information, education and communication (IEC) materials, distribution of misoprostol to women coming for ANC and data collection began in April 2011 and continued through January 2012. A monitoring visit was done in May 2011 and a rapid assessment of the project was conducted in September 2011 by VSI staff. The findings on these visits were used to address challenges identified and to improve enrollment rates. GHS also paid supportive supervisory visits to project sites. Five Technical Advisory Group (TAG) meetings were held during the course of the pilot, the first one in March 2010 and the last one in October 2011. All of the project activities were reported to the TAG, which provided oversight and recommendations for the continuation of pilot implementation. Data analysis and report writing were completed in February 2012.
SPECIAL CONSIDERATIONS
Tablet Recall The Ghana Food and Drugs Board (FDB) recalled Misotac® brand misoprostol tablets based on information VSI received from partners about drug quality issues which was confirmed by further independent testing of the tablets in July 2011. The tablets were found to have less than the full amount of the active ingredient than indicated in the market approval. With this information, an immediate retrieval of all remaining Misotac® tablets from pilot project health facilities was initiated by FDB and GHS, with support from VSI. With the approval of GHS and the TAG, distribution of misoprostol in the pilot program was continued using Cytotec® brand tablets. It took the months of July and August 2011 to visit all facilities and retrieve all of the tablets, while replacing them with the new tablets. Additionally, women who came to ANC visits and had previously received Misotac® were asked to bring their tablets back to the health facility, where they were replaced with Cytotec®. All pilot facilities were stocked with Cytotec® tablets by September 1, 2011. Recalled tablets were returned to the District Health Management Team and stored under lock and key pending direction from FDB on their proper destruction.
6
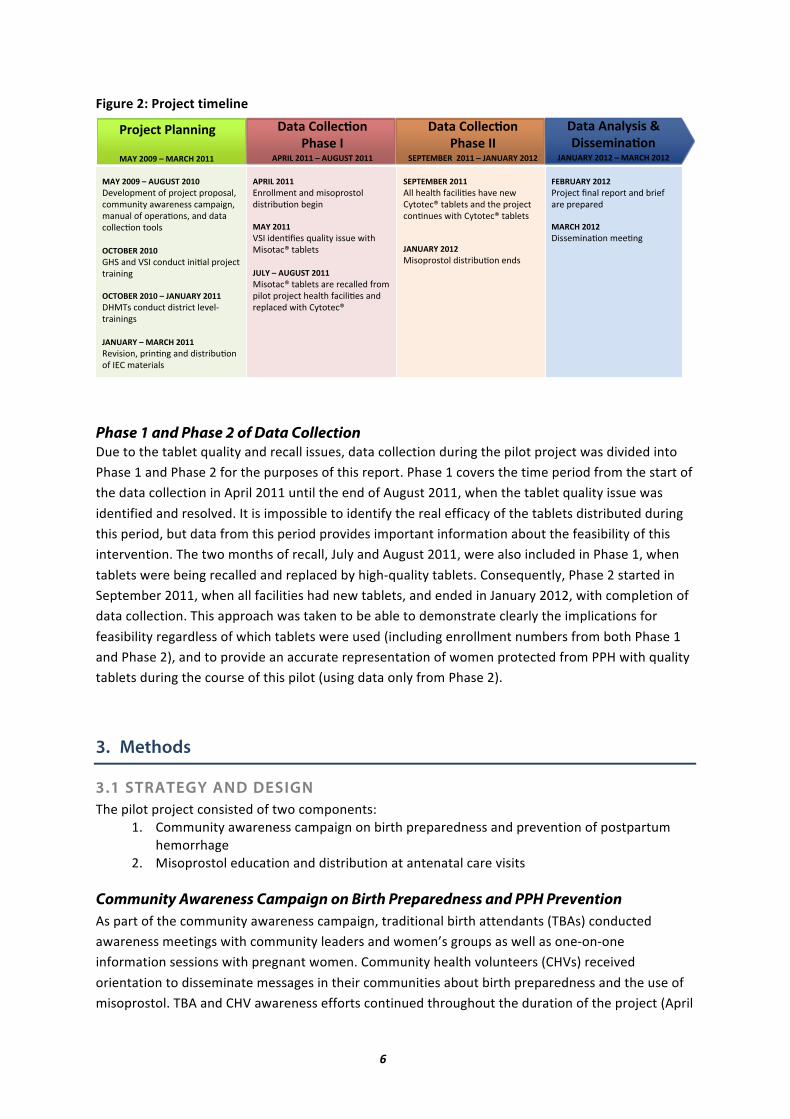
Figure 2: Project timeline
Phase 1 and Phase 2 of Data Collection Due to the tablet quality and recall issues, data collection during the pilot project was divided into Phase 1 and Phase 2 for the purposes of this report. Phase 1 covers the time period from the start of the data collection in April 2011 until the end of August 2011, when the tablet quality issue was identified and resolved. It is impossible to identify the real efficacy of the tablets distributed during this period, but data from this period provides important information about the feasibility of this intervention. The two months of recall, July and August 2011, were also included in Phase 1, when tablets were being recalled and replaced by high-‐quality tablets. Consequently, Phase 2 started in September 2011, when all facilities had new tablets, and ended in January 2012, with completion of data collection. This approach was taken to be able to demonstrate clearly the implications for feasibility regardless of which tablets were used (including enrollment numbers from both Phase 1 and Phase 2), and to provide an accurate representation of women protected from PPH with quality tablets during the course of this pilot (using data only from Phase 2).
3. Methods
3.1 STRATEGY AND DESIGN The pilot project consisted of two components:
1. Community awareness campaign on birth preparedness and prevention of postpartum hemorrhage
2. Misoprostol education and distribution at antenatal care visits Community Awareness Campaign on Birth Preparedness and PPH Prevention As part of the community awareness campaign, traditional birth attendants (TBAs) conducted awareness meetings with community leaders and women’s groups as well as one-‐on-‐one information sessions with pregnant women. Community health volunteers (CHVs) received orientation to disseminate messages in their communities about birth preparedness and the use of misoprostol. TBA and CHV awareness efforts continued throughout the duration of the project (April
!"#"$%&"'()*)$+$$!*)),-*&"./&$
0%12%34$5675$8$9%3:;$5675$
!"#"$:/'',<./&$=>"),$??$
@A=BA9CA3$$5677$8$0%12%34$5675$
!"#"$:/'',<./&$=>"),$?$
%=3?D$5677$8$%2E2@B$5677$
=F/G,<#$='"&&*&H$
9%4$566I$8$9%3:;$5677$
$$
9%4$566I$8$%2E2@B$5676$!"#"$%&'"()*%+*&,%-".)*&,%&%/0$1*.%''2(3)4*050,"("//*.0'&036(1*'0(20$*%+*%&",07%(/1*0(8*80)0*.%$$".7%(*)%%$/**J:BJCA3$5676$9:;*0(8*<;=*.%(82.)*3(370$*&,%-".)*),03(3(6**J:BJCA3$5676$8$0%12%34$5677$!:>?/*.%(82.)*83/),3.)*$"#"$@),03(3(6/**0%12%34$8$9%3:;$5677$A"#3/3%(1*&,3(7(6*0(8*83/),3B27%(*%+*=CD*'0)",30$/**
$
%=3?D$5677$C(,%$$'"()*0(8*'3/%&,%/)%$*83/),3B27%(*B"63(**9%4$5677$<;=*38"(7E"/*F20$3)4*3//2"*53)G*>3/%)0.H*)0B$")/**02D4$8$%2E2@B$5677$>3/%)0.H*)0B$")/*0,"*,".0$$"8*+,%'*&3$%)*&,%-".)*G"0$)G*+0.3$37"/*0(8*,"&$0."8*53)G*D4)%)".H**
$
@A=BA9CA3$5677$I$$*G"0$)G*+0.3$37"/*G0#"*("5*D4)%)".H*)0B$")/*0(8*)G"*&,%-".)*.%(7(2"/*53)G*D4)%)".H*)0B$")/***$0%12%34$5675$>3/%&,%/)%$*83/),3B27%(*"(8/****
$
*
KAC32%34$5675$J,%-".)*E(0$*,"&%,)*0(8*B,3"+*0,"*&,"&0,"8**9%3:;$5675$!3//"'3(07%(*'""7(6*****
$
7
2011 – January 2012). Queen Mothers (traditional female community leaders) were asked to participate in community sensitization efforts because they have a great deal of influence in their communities. In Birim South, for example, Queen Mothers agreed to speak about misoprostol whenever they met with a group of 10 or more women.
The District Health Management Teams (DHMT) undertook additional community awareness activities such as megaphone announcements at markets. Many communities have megaphones that stand elevated on poles in a central area of the community, and announcements were often made between the hours of 5-‐7am and 5-‐7pm. The DHMT, along with individual TBAs and CHVs, also organized durbars, local community meetings, that brought together community members, including the village chiefs and Queen Mothers, with the aim of sharing messages about the availability of misoprostol at health facilities and how misoprostol could be used to prevent excessive bleeding after delivery. Women who had taken misoprostol, along with TBAs who had attended births where misoprostol was taken, were encouraged to speak at these durbars. DHMT members also took advantage of durbars that were already organized to present information on misoprostol. Staff from KEEA arranged for radio announcements about the project on Ahomka FM.
Box 2: Key messages of community awareness campaign
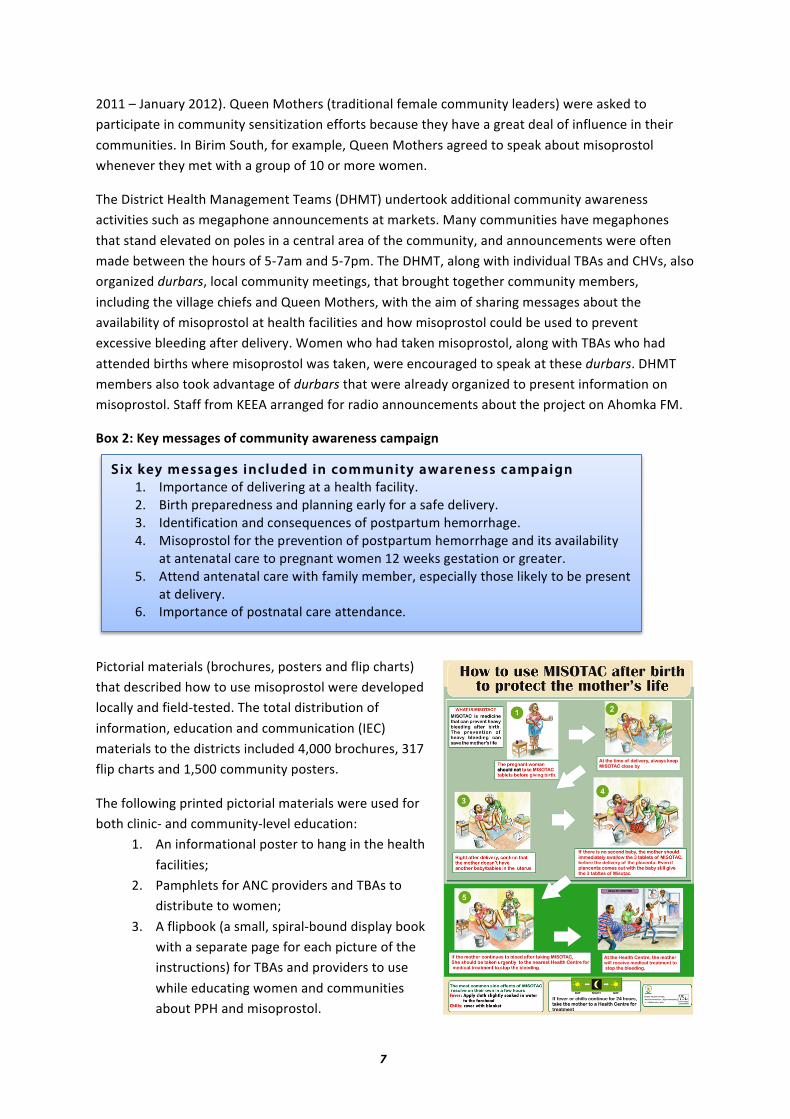
Pictorial materials (brochures, posters and flip charts) that described how to use misoprostol were developed locally and field-‐tested. The total distribution of information, education and communication (IEC) materials to the districts included 4,000 brochures, 317 flip charts and 1,500 community posters.
The following printed pictorial materials were used for both clinic-‐ and community-‐level education:
1. An informational poster to hang in the health facilities;
2. Pamphlets for ANC providers and TBAs to distribute to women;
3. A flipbook (a small, spiral-‐bound display book with a separate page for each picture of the instructions) for TBAs and providers to use while educating women and communities about PPH and misoprostol.
Six key m e ssa ges include d in com munity aware ness c amp aign 1. Importance of delivering at a health facility. 2. Birth preparedness and planning early for a safe delivery. 3. Identification and consequences of postpartum hemorrhage. 4. Misoprostol for the prevention of postpartum hemorrhage and its availability
at antenatal care to pregnant women 12 weeks gestation or greater. 5. Attend antenatal care with family member, especially those likely to be present
at delivery. 6. Importance of postnatal care attendance.

8
Misoprostol Education and Distribution at ANC All women attending ANC were educated on birth preparedness and PPH prevention, using the six messages of the awareness campaign. Most ANC providers led group education sessions for women. Providers also spoke with women individually to ask if they would like to enroll in the pilot project and to explain the informed consent. If a woman agreed to enroll in the project, she was required to sign the informed consent form. Enrolled women were then provided more in-‐depth information on misoprostol, screened for medical eligibility, and if eligible (see Box 3), offered misoprostol tablets to take with them for use at home births if they were unable to return to the facility for delivery. Based on the project protocol, women could receive the tablets at an ANC visit once they had reached 12 weeks gestation. ANC providers gave eligible expectant mothers three (3) tablets of misoprostol in special envelopes or medicine sachets, with a pictorial brochure explaining how to take the tablets.
Box 3: Eligibility criteria for the pilot project
All pilot project participants were encouraged to come back for a postnatal care (PNC) visit after their delivery. At the PNC visit, providers asked women about their delivery experience, and whether or not they had used the misoprostol tablets provided to them. While it was difficult to collect follow-‐up information at PNC visits because many women who enrolled in the pilot live in very remote, rural villages and do not often come to facilities to receive PNC, the project management put strategies in place during the pilot to ensure that as many women as possible returned for a PNC visit for follow-‐up. The following strategies were utilized to encourage follow-‐up at PNC: radio announcements, megaphone announcements on market days, and providers and CHVs visiting women’s homes to provide PNC and to collect follow-‐up information. PNC forms were also completed for some clients prior to discharge from the facility after delivery, especially for women who were not likely to return for PNC.
Distribution of misoprostol tablets to district health facilities
The number of misoprostol tablets per district was estimated and allocated based on client load. Taking this into account, each district determined how many tablets would be required for each of its facilities during the pilot project.
Each district collected its allocation from the Central Medical Stores and stored it in
district pharmacies. Each facility subsequently collected tablets as needed.
Participants in the pilot project were pregnant women who attended ANC and for whom the ANC provider anticipated a vaginal delivery. Enrollment in the project was voluntary, but subject to the following eligibility criteria (determined by the ANC provider):
1. Ability to give informed consent (written or oral depending on woman’s literacy level). 2. Anticipation of an uncomplicated vaginal delivery. 3. Anticipation of a home delivery. 4. Not allergic to prostaglandins. 5. Did not have a high-‐risk pregnancy or other chronic disease (e.g. high blood pressure,
diabetes, cardiac disease, or other chronic conditions).

9
3.2 PROJECT ORGANIZATIONAL STRUCTURE Dr. Gloria Quansah Asare, Director of the Family Health Division of Ghana Health Service, served as the Advisory Principal Investigator for this project, and was responsible for the oversight of implementation of the project and compliance with project protocols. VSI staff in Ghana and California, USA assisted in the development, coordination and organization of project training, implementation and data collection. The VSI-‐Ghana Project Coordinator, assisted by the Monitoring Supervisor, oversaw the day-‐to-‐day implementation of the project, including training, monitoring, and data collection and management. Each district had a District Health Management Team that oversaw ANC providers. In turn, ANC providers were responsible for the supervision of the TBAs associated with their catchment area (Figure 3). The reporting structure for the providers in this project followed the existing structure of supervision. Figure 3: Organizational structure of the project
3.3 PROJECT TRAINING VSI and GHS led the initial training of trainers in October 2010. The DHMTs conducted district-‐level trainings and orientations between October 2010 and January 2011. ANC providers received training on misoprostol for PPH prevention, meaning that after the training they were able to distribute misoprostol directly to women for use for PPH prevention at home births. In the context of this pilot project, “oriented” was used to refer to TBAs and CHVs who were familiarized with the procedures of the pilot project, but not able to actually provide the intervention (misoprostol for PPH prevention). Thus, TBAs and CHVs were able to inform their communities about the use of misoprostol for prevention of PPH, but were not allowed to administer misoprostol to women at delivery. In total, 208 ANC providers were trained, while 311 TBAs and 255 CHVs were oriented to the project (Table 3).
!"#$#%&'#()"%*'+,-.'%
/'0-1$#(%211+3-$#)1+%4/56!78&895%
:-;)+-.)%&'#()"%%<#$#0'='$)%>'#=%
*?6?%
%862%@+1,-3'+;%
/'0-1$#(%211+3-$#)1+%2?6>/8A%
:-;)+-.)%&'#()"%%<#$#0'='$)%>'#=%
B??8%
%862%@+1,-3'+;%
/'0-1$#(%211+3-$#)1+%?8*>?/6%
:-;)+-.)%&'#()"%%<#$#0'='$)%>'#=%
C@@?/%<86D8%B/545%
%862%@+1,-3'+;%
:-;)+-.)%&'#()"%%<#$#0'='$)%>'#=%
4E/E<%*5C>&%
%862%@+1,-3'+;%
@+1F'.)%211+3-$#)1+%GH*EI%<1$-)1+-$0%*JK'+,-;1+%GH*EI%
:#)#%<#$#0'+%G!&*I%
83,-;1+;%G!&*I%83,-;1+;%GH*EI%

10
Table 3: Health workers trained or oriented during the pilot, by district
Birim South KEEA Sene
Upper Manya Krobo
Total
Trained to distribute misoprostol Antenatal care providers 57 76 26 49 208
Oriented to inform women about the project Traditional birth attendants 19 148 75 69 311 Community health volunteers 34 31 50 140 255 Other health workers 15 19 32 9 75
Throughout the course of the project, some trained providers were transferred to different facilities with new providers replacing them. These new providers were given on-‐the-‐job training about the ongoing misoprostol pilot project, conducted either by a member of the DHMT team, the VSI-‐Ghana Project Coordinator, or by a trained provider working at the facility.
3.4 DATA COLLECTION AND MANAGEMENT
3.4.1 DATA COLLECTION TOOLS Data was collected from women who gave consent and were enrolled in the project both before they delivered (during their ANC visit, when they were given misoprostol) and after they delivered. Three different data collection forms were used:
1) ANC Misoprostol Addendum: Antenatal care providers completed the ANC Misoprostol Addendum for every woman who enrolled in the project at an ANC visit. During enrollment, ANC providers asked women for their permission to collect information on their delivery experience. All women who took misoprostol home were advised to come back to the facility to deliver, and if not, to come back to the facility after delivery for postnatal care and to report on their delivery experience and the use of misoprostol.
2) Postnatal Follow-‐up Form: Providers completed the Postnatal Follow-‐up Form in the facilities for women who took misoprostol and then delivered at the facility and/or came back later for a postnatal visit. It could be completed at the time of delivery, or at a later postnatal visit. This form provided information on participants’ delivery information and whether and when they used misoprostol.
3) TBA Delivery Form: Because home deliveries with TBAs are common in the pilot districts, and it was possible that women who received misoprostol tablets from ANC would deliver at home with a TBA, another simplified form with pictorials, the TBA Delivery Form, was provided to TBAs in the pilot districts. TBAs were trained to complete the form for all enrolled women1 they assisted in delivery. For TBAs who were illiterate, providers and CHVs assisted them in completing the forms. The TBA Delivery Form included information on both delivery and the immediate postpartum period, to capture the information on whether or not misoprostol was used at delivery as well as perceived blood loss and referrals.
It should be noted that data from these forms is presented separately in the following sections. Women captured with the Postnatal Follow-‐up Form are not completely exclusive from women
1 Women enrolled at ANC had a large red “M” (standing for misoprostol) written on their Ghana Health Service ANC Record Book. This alerted TBAs to the fact that these women were enrolled in the project.

11
captured with the TBA Delivery Form, as the same woman who delivered at home with a TBA (and had a TBA Delivery Form completed for her), could go to a health facility and have a Postnatal Follow-‐up Form completed for her during her postnatal care visit.
3.4.2 DATA ENTRY, MANAGEMENT AND ANALYSIS Health Information Officers (HIOs) and Disease Control Officers (DCOs) working for GHS entered the data from project forms using EpiInfo 6 throughout the project. While collecting data during routine supervisory visits, the team addressed any challenges arising in the data collection and proper documentation. Once entered, the HIOs and DCOs sent the data to the Data Manager based in Accra at GHS and the data was analyzed in Stata 10 in February 2012.
4. Results
4.1 WOMEN REACHED AND DATA FOR ANALYSIS During the project time period (April 1, 2011 through January 31, 2012), 11,328 women were registered as “new ANC registrants2” in the four pilot project districts (as reported by the District Health Management Teams) (Table 4). A total of 5,345 (47%) of these women were enrolled in the pilot project by ANC providers over both phases of the data collection. Follow-‐up data was collected at postnatal care visits on the delivery experiences of 68% of enrolled women.
Table 4: Misoprostol distribution data collected
Birim South KEEA Sene
Upper Manya Krobo
Total
Number of new ANC registrants^ 2,070 3,687 3,582 1,989 11,328 Number of women enrolled (of new ANC registrants)
1,359 (65.7%)
1,408 (38.2%)
1,755 (49.0%)
823 (41.4%)
5,345 (47.2%)
Follow-‐up data collected at a postnatal care visit (of enrolled women)
907 (66.7%)
1,319 (93.7%)
1,098 (62.6%)
291 (35.4%)
3,615 (67.6%)
^District Health Management Team ANC Records
4.2 MISOPROSTOL DISTRIBUTION AT ANC One measure of the feasibility of introducing misoprostol distribution at ANC is the ability of providers to enroll women in the project. While the enrollment rate was 41.6% for the first phase, it was 52.4% for the second phase, after the recall. Taken together, overall enrollment in the project was about half of all new ANC registrants (47%)(Table 5).3
2 In the context of the Ghanaian health system “new ANC registrant” is a term used to identify a pregnant woman who reports for antenatal care at a health facility for the first time and is registered and given an ANC card. 3 For the purposes of determining the feasibility of this pilot project, new ANC registrants were used as the denominator for determining the proportion of women enrolled in the pilot. However, it should be noted that new ANC registrants do not capture all women who may have been eligible to receive misoprostol. For example, some women may have become new ANC registrants months before the pilot began, and then come to ANC during the pilot and been eligible to receive misoprostol.
12
Table 5: Enrollment data
Phase 1: April 1 – August 31, 2011
Phase 2: Sept 1 – January 31, 2012 Total
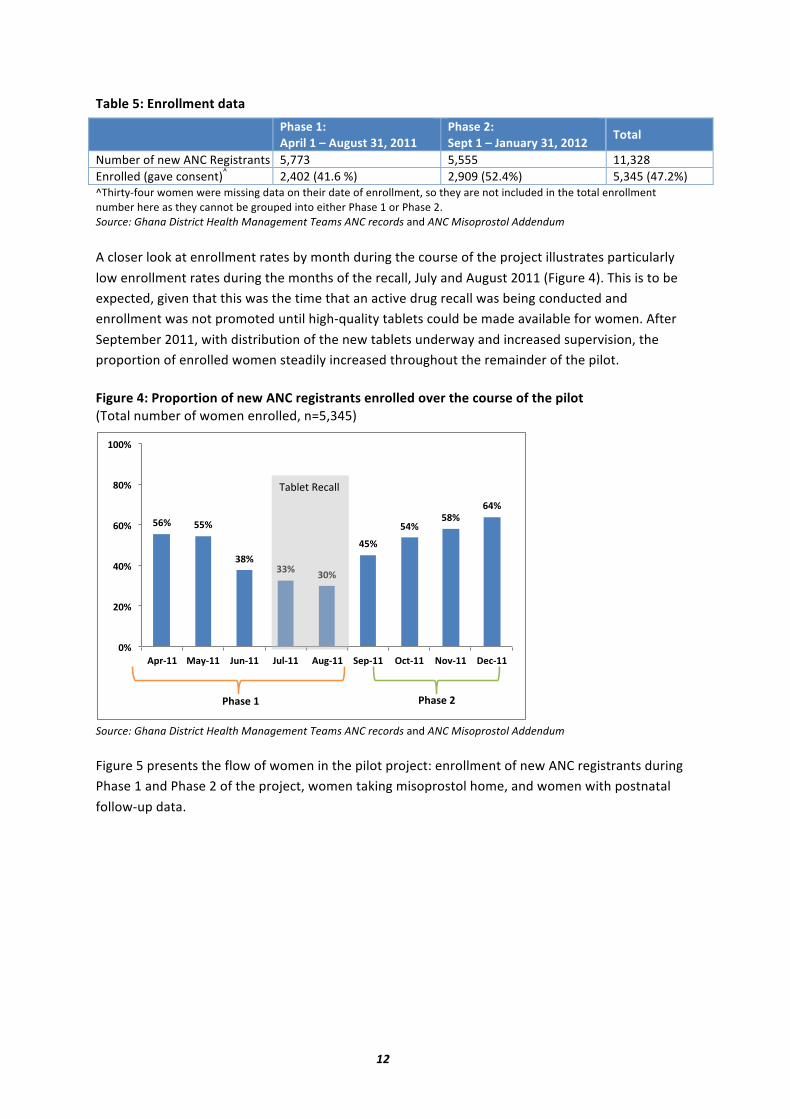
Number of new ANC Registrants 5,773 5,555 11,328 Enrolled (gave consent)^ 2,402 (41.6 %) 2,909 (52.4%) 5,345 (47.2%) ^Thirty-‐four women were missing data on their date of enrollment, so they are not included in the total enrollment number here as they cannot be grouped into either Phase 1 or Phase 2. Source: Ghana District Health Management Teams ANC records and ANC Misoprostol Addendum A closer look at enrollment rates by month during the course of the project illustrates particularly low enrollment rates during the months of the recall, July and August 2011 (Figure 4). This is to be expected, given that this was the time that an active drug recall was being conducted and enrollment was not promoted until high-‐quality tablets could be made available for women. After September 2011, with distribution of the new tablets underway and increased supervision, the proportion of enrolled women steadily increased throughout the remainder of the pilot. Figure 4: Proportion of new ANC registrants enrolled over the course of the pilot (Total number of women enrolled, n=5,345)
Source: Ghana District Health Management Teams ANC records and ANC Misoprostol Addendum Figure 5 presents the flow of women in the pilot project: enrollment of new ANC registrants during Phase 1 and Phase 2 of the project, women taking misoprostol home, and women with postnatal follow-‐up data.
!"#$ !!#$
%&#$%%#$ %'#$
(!#$
!(#$!&#$
"(#$
'#$
)'#$
('#$
"'#$
&'#$
*''#$
+,-.**$ /01.**$ 234.**$ 235.**$ +36.**$ 78,.**$ 9:;.**$ <=>.**$ ?8:.**$
!"#$%&'(%)"$$'
@A0B8$*$ @A0B8$)$

13
Figure 5: Flow chart of women's participation in the pilot project
^Thirty-‐four women were missing data on their date of enrollment and 48 were missing the date they took the misoprostol home.
The overwhelming majority of women who enrolled in the project took misoprostol home with them from ANC (99%)(Table 6). Of the 31 women who were enrolled and did not take misoprostol home, half were not eligible (n=16). Six women said that they wanted to accept misoprostol at a later ANC visit, and five said that misoprostol was not currently available at the facility; however, these 11 women did not return to receive misoprostol at a subsequent visit. Of the remaining enrolled women who gave a reason for not taking misoprostol home, two said that they did not have enough information on misoprostol; one said that she needed to get permission from her husband/relative; one wanted to discuss it with a friend/husband/relative; and one wanted to think about it. Two women did not give a response (data not shown). On average, women enrolled in the project were 25.9 weeks pregnant. The project protocol stipulated that only women who had reached 12 weeks gestation could take misoprostol home; however, 61 women (1%) were given misoprostol to take home before they had reached 12 weeks gestation. It is noteworthy that most women received misoprostol after their second ANC visit, when they were in their second trimester. Table 6: Misoprostol distribution at ANC
Birim South (n=1,359 )
KEEA (n=1,408 )
Sene (n=1,755 )
Upper Manya Krobo (n=823 )
Total (n=5,345 )
Enrolled (gave consent) 1,359 1,408 1,755 823 5,345
Took misoprostol home (% of those enrolled)
1,357 (99.9%)
1,389 (98.7%)
1,747 (99.5%) 821 (99.8%) 5,314 (99.4%)
Average gestational age in weeks at receipt of misoprostol (min; max) 25.5 (4; 40) 27.4 (6; 40) 24.7 (3; 40) 26.6 (6; 40) 25.9 (4; 40)
Source: ANC Misoprostol Addendum
!"#$%!&$'"()*+,-.+*$!"#$%&'&#()&!"#$%&*&
+,-./0&*1''&2&3#(4#.5&*1'*6&78''9:*;&
/.,011"2$!"#$%&'&
&+,-./0&2&,4<4$=&*1''6&(8&*9>1*&
/.,011"2$!"#$%&*&
+?%-=%@A%.&*1''&2&3#(4#.5&*1'*6&(8&*9B1B&
30+-1$40*+.-+-1$50110#678$50,9*$(8:9C'D&
30+-1$.79:",$0;$#09".$#<0$+00=$9)*08,0*+01$<09"$
(8D9:'>&

14
Overall, 643 (12%) of the total 5,314 women who took misoprostol home were living outside of the catchment area of the pilot project facilities (Figure 6). These women came to the pilot project facilities and were enrolled and given misoprostol tablets, according to the protocol. Living outside the catchment area had implications for the ability of providers to follow up with these women after delivery, as they probably live further away than other enrolled women and may not have returned to the facility for a postnatal care visit. Thus, the large number of women living outside the facility catchment area is one of the reasons why the postnatal follow-‐up in this project was relatively low. Approximately one out of five women from Upper Manya Krobo and Sene districts did not live in the catchment area. This is not surprising, as both of these districts serve clients who live on islands in the Volta Lake, and who come in to access health services at facilities in Sene and Upper Manya Krobo on market days. Figure 6: Total number and proportion of women living outside the catchment area by district (Total number of women who took misoprostol home, n=5,314)
Source: ANC Misoprostol Addendum Four levels of health facilities were involved in this project: Community-‐based Health Planning and Services (CHPS) compounds, health centers, hospitals and maternity homes. Health centers distributed misoprostol to the largest number of women enrolled in the project (56%)(Figure 7). It is notable that CHPS compounds in Birim South were the most prominent distribution point for misoprostol in the district, with over half of all women reporting them as the facility level where they were given misoprostol. Overall, almost one out of four women received misoprostol from a CHPS compound, highlighting the importance of these low-‐level facilities as misoprostol distribution points. Very few women received misoprostol from maternity homes (2% overall).

15
Figure 7: Location of misoprostol distribution (Total number of women who took misoprostol home, n=5,314)^
Source: ANC Misoprostol Addendum ^Information was missing on the type of facility where misoprostol was received for 83 women.
4 .3 DELIVERY CHARACTERISTICS AND UTEROTONIC COVERAGE Of those women who took misoprostol home from ANC and for whom postpartum data was collected using the Postnatal Follow-‐up Form, location of delivery varied across districts (Table 7); home delivery ranged from 23% in KEEA to 48% in Birim South. All districts had fairly low rates of delivery at CHPS compounds, with the exception of Birim South, where 30% of facility deliveries took place at this facility level. While the majority of women in KEEA who delivered at a facility delivered at health centers (93%), far fewer women delivered in health centers in the other districts (19-‐48%). Delivery in a hospital ranged from 7% in KEEA to 56% in Sene. Over half (53%) of all women delivered with a nurse/midwife, while only 2.6% of women delivered with a doctor. In Sene District, 167 (15%) of women delivered with a ward assistant. Ward assistants are people with minimal education who have been given health care training and on-‐the-‐job training to assist in clinical care. TBAs attended around one-‐third of deliveries in Birim South, Sene and Upper Manya Krobo, and 22% of deliveries in KEEA. It should be noted that because of the varying rate of follow-‐up in this pilot project (ranging from 35% of enrolled women in Upper Manya Krobo to 94% of women in KEEA) (Table 4), the data on location of delivery and attendant at delivery cannot be understood as being representative of the true distribution of location/attendance at delivery in the population.
52%
6% 21%
11% 23%
48%
87% 53%
28%
56%
0% 5%
26%
54%
19%
0% 2% 2% 7% 2%
0%
20%
40%
60%
80%
100%
Birim South KEEA Sene Upper Manya Krobo
Total
CHPS compound Health center Hospital Maternity home

16
Table 7: Delivery characteristics of women who took misoprostol home from ANC
Birim South (n=907)
KEEA (n=1,319)
Sene (n=1,098)
Upper Manya Krobo (n=291)
Total (n=3,615)
Location of delivery^ Home 431 (47.5%) 307 (23.3%) 501 (45.6%) 116 (39.9%) 1,355 (37.5%) Facility 476 (52.5%) 1,003 (76.0%) 595 (54.2%) 148 (50.9%) 2,222 (61.5%) CHPS compound 141 (29.6%) 2 (0.2%) 10 (1.7%) 7 (4.0%) 160 (7.2%) Health center 229 (48.1%) 928 (92.5%) 242 (40.4%) 33 (18.8%) 1,432 (64.4%) Hospital 105 (22.1%) 72 (7.1%) 338 (56.4%) 75 (42.6%) 590 (26.6%) Maternity home 1 (0.2%) 1 (0.1%) 5 (0.8%) 33 (18.8%) 40 (1.8%)
Attendant at delivery* Doctor 29 (3.2%) 21 (1.6%) 38 (3.5%) 7 (2.4%) 95 (2.6%) Nurse/midwife 443 (48.8%) 958 (72.6%) 387 (35.3%) 134 (46.0%) 1922 (53.2%) Ward assistant 0 0 167 (15.2%) 0 167 (4.6%) TBA 315 (34.7%) 294 (22.3%) 363 (33.1%) 110 (37.8%) 1082 (29.9%) Friend/relative 120 (13.2%) 42 (3.2%) 143 (13.0%) 34 (11.7%) 339 (9.4%)
Source: Postnatal Follow-‐Up Form ^Thirty-‐eight women gave no response for delivery location * No response from 10 women. Among women who participated in the pilot, uterotonic coverage at home deliveries was very high across all districts, ranging from 88% in KEEA and UMK to 96% in Sene (Table 8). Overall, 93% of the women who delivered at home and completed the Postnatal Follow-‐up Form took misoprostol at delivery. Only 7% of the women who delivered at home did not take misoprostol. Of these women, 75 said that they forgot or could not find the tablets; 14 said that they did not want to take the misoprostol; and five said that they did not take misoprostol home from ANC (data not shown; women could select more than one reason). The majority of women who delivered in a health facility received oxytocin (82%); however, it is notable that in Sene District, 30% of women delivering in a health facility received misoprostol at delivery. This occurred because the ward assistants in Sene were not authorized to use oxytocin at deliveries. Table 8: Uterotonic drug at delivery^
Birim South (n=907)
KEEA (n=1,319)
Sene (n=1,098)
Upper Manya Krobo (n=291)
Total (n=3,615)
Home delivery1 ^ 431 (47.5%) 307 (23.3%) 501 (45.6%) 116 (39.9%) 1,355 (37.5%) Misoprostol 407 (94.4%) 270 (88.0%) 482 (96.2%) 102 (87.9%) 1,261 (93.1%) No uterotonic 24 (5.6%) 35 (11.4%) 18 (3.59%) 12 (10.3%) 89 (6.6%)
Facility delivery 476 (52.5%) 1,003 (76.0%) 595 (54.2%) 148 (50.9%) 2,222 (61.5%) Misoprostol 23 (4.8%) 55 (5.5%) 180 (30.3%) 19 (12.8%) 277 (12.5%) Oxytocin 440 (92.4%) 924 (92.1%) 344 (57.8%) 121 (81.8%) 1,829 (82.3%) No information* 13 24 71 8 116 (5.2%)
1Includes births en route to the health facility ^Thirty-‐eight women provided no response for delivery location. ^^Five women who delivered at home were missing data on uterotonic drug at delivery; these women may or may not have taken misoprostol at delivery. *One hundred and sixteen women who delivered at a facility had no data for uterotonic drug used at facility; these women may or may not have received a uterotonic at delivery. Source: Postnatal Follow-‐Up Form
17
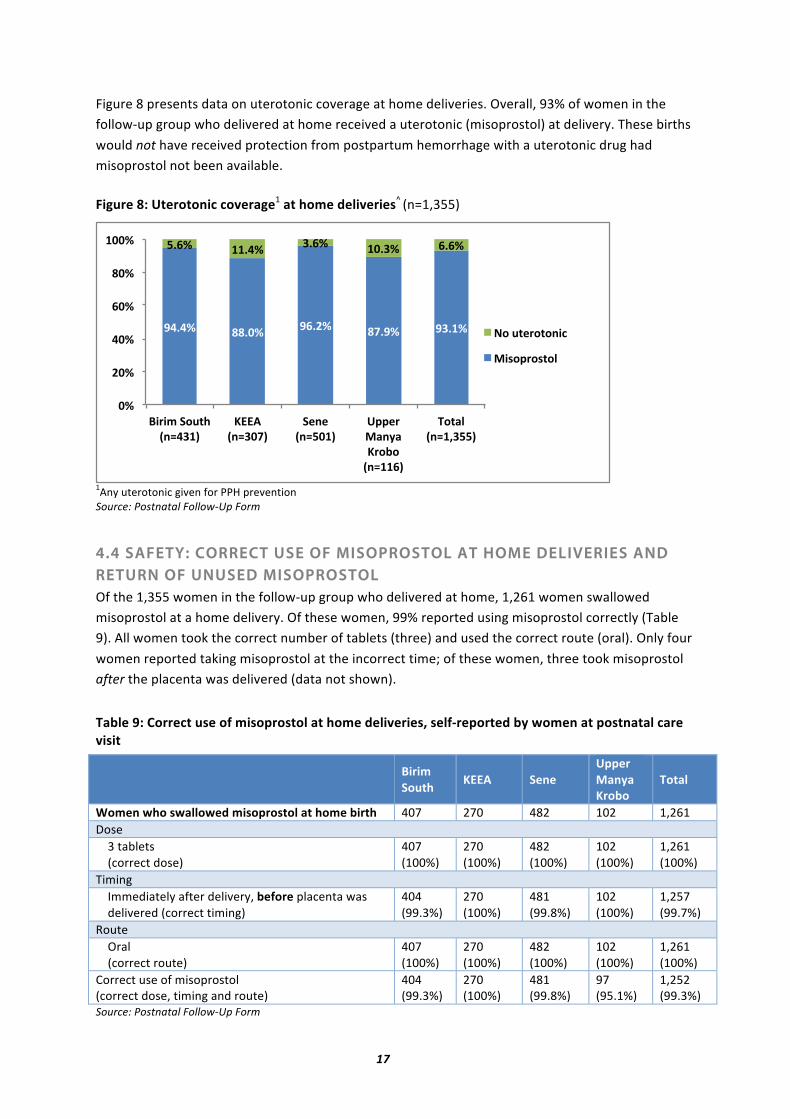
Figure 8 presents data on uterotonic coverage at home deliveries. Overall, 93% of women in the follow-‐up group who delivered at home received a uterotonic (misoprostol) at delivery. These births would not have received protection from postpartum hemorrhage with a uterotonic drug had misoprostol not been available. Figure 8: Uterotonic coverage1 at home deliveries^ (n=1,355)
1Any uterotonic given for PPH prevention Source: Postnatal Follow-‐Up Form
4.4 SAFETY: CORRECT USE OF MISOPROSTOL AT HOME DELIVERIES AND RETURN OF UNUSED MISOPROSTOL Of the 1,355 women in the follow-‐up group who delivered at home, 1,261 women swallowed misoprostol at a home delivery. Of these women, 99% reported using misoprostol correctly (Table 9). All women took the correct number of tablets (three) and used the correct route (oral). Only four women reported taking misoprostol at the incorrect time; of these women, three took misoprostol after the placenta was delivered (data not shown).
Table 9: Correct use of misoprostol at home deliveries, self-‐reported by women at postnatal care visit
Birim South KEEA Sene
Upper Manya Krobo
Total
Women who swallowed misoprostol at home birth 407 270 482 102 1,261 Dose 3 tablets (correct dose)
407 (100%)
270 (100%)
482 (100%)
102 (100%)
1,261 (100%)
Timing Immediately after delivery, before placenta was delivered (correct timing)
404 (99.3%)
270 (100%)
481 (99.8%)
102 (100%)
1,257 (99.7%)
Route Oral (correct route)
407 (100%)
270 (100%)
482 (100%)
102 (100%)
1,261 (100%)
Correct use of misoprostol (correct dose, timing and route)
404 (99.3%)
270 (100%)
481 (99.8%)
97 (95.1%)
1,252 (99.3%)
Source: Postnatal Follow-‐Up Form
!"#"$% &&#'$% !(#)$% &*#!$% !+#,$%
-#($% ,,#"$% +#($% ,'#+$% (#($%
'$%
)'$%
"'$%
('$%
&'$%
,''$%
./0/1%23456%%%%%%%%%%%%%%%%%%%%789"+,:%
;<<=%%%%%%%%%%%%%%%789+'*:%
2>8>%%%%%%%%%%%%%%%%%789-',:%
?@@>0%AB8CB%;03D3%%%%%%%789,,(:%
E35BF%%%%%%789,G+--:%
H3%45>03538/I%
A/J3@03J53F%

18
Of the women who took misoprostol home from ANC and did not use it at a home delivery, the vast majority (83%) returned the misoprostol to the facility, as they had been instructed to do by the ANC provider who initially gave them the misoprostol (Figure 9). The proportion returning misoprostol was also high for facility deliveries, with 92% of women who delivered at a facility and did not use misoprostol returning the drug. Of all the misoprostol distributed to women, only 5% (n=164) of women who received misoprostol at ANC did not return the misoprostol (data not shown). Unused misoprostol tablets were returned to the District Health Management Team where they were stored under lock and key pending direction from the Food & Drugs Board for their proper destruction.
Figure 9: Return of unused misoprostol (n=3,577)^
^38 women gave no response for delivery location. Five women who delivered at home were missing data on uterotonic at delivery. Source: Postnatal Follow-‐Up Form
4.5 PROGRAM EFFECTIVENESS: PERCEIVED PPH AND REFERRALS During the PNC visit, providers asked women how much blood they lost after delivery and whether they had been referred. From the subset of 978 women who enrolled during Phase 2 (after September 1, 2011), 364 used misoprostol at a home delivery. Of these women, only four perceived PPH, and none were referred. Of the women who delivered at home and did not receive a uterotonic drug, one perceived PPH; she also did not need to be referred (data not shown).
During this pilot, two maternal deaths were reported (one in Birim South and one in KEEA). In both cases, further inquiry was conducted as to the cause of death, and both were found to be unrelated to the project or taking misoprostol. According to an account from the Birim South DHMT, the deceased experienced bleeding during pregnancy. She was treated for antepartum hemorrhage, but died of unknown causes three days after being discharged from the hospital. In KEEA, the Municipal Public Health Nurse reported that after delivering at the Health Center, the deceased experienced postpartum hemorrhage that was unresponsive to oxytocin. She was referred to the Regional Hospital where she developed complications and died.

19
4.6 HOME DELIVERIES WITH TBAS A TBA Delivery Form was used to collect data on women who took misoprostol home from ANC and delivered with a TBA. TBAs were oriented to understand and help administer misoprostol to women whose deliveries they attended. Over the course of the project, 1,456 TBAs filled out TBA Delivery Forms for women enrolled in the pilot (Table 10). Of these women, 97% swallowed misoprostol at delivery with a TBA and TBAs reported that almost all (99%) took the correct dose of misoprostol. TBAs reported that only seven women (0.5%) took the incorrect dose of misoprostol. Further, TBAs reported that 99% of women (n=1,450) whose deliveries they attended were in good condition when the TBA left after delivery; only three women were sick when the TBA left. Table 10: Deliveries attended by TBAs
Birim South (n=438)
KEEA (n=272)
Sene (n=673)
Upper Manya Krobo (n=73)
Total (n=1,456)
Delivered with TBA 438 272 673 73 1,456
Took misoprostol home from ANC 437 (99.8%)
271 (99.6%)
670 (99.6%)
72 (98.6%)
1,450 (99.6%)
Took misoprostol at delivery with TBA^ 425 (97.3%)
252 (93.0%)
668 (99.7%)
68 (94.4%)
1,413 (97.4%)
Took correct dose of misoprostol (3 tablets)
423 (99.5%)
249 (98.8%)
665 (99.6%)
68 (100.0%)
1,406 (99.5%)
Took incorrect dose 2 (4.7%) 3 (1.2%) 2 (3.0%) 0 7 (0.5%) Condition when TBA left woman
Good 435 (99.3%)
270 (99.3%)
672 (99.9%)
73 (100%)
1,450 (99.6%)
Sick 2 (0.5%) 0 1 (0.2%) 0 3 (0.2%) ^Three women were missing data on whether they had used misoprostol at delivery with a TBA. Source: TBA Delivery Form The majority (95%) of women who delivered with a TBA and for whom a TBA Delivery Form was filled out reported no side effects related to the use of misoprostol (Table 11). Of those who did report side effects, the most common was shivering (4%). It is important to note that data from the TBA Delivery Form did not contain information on the date that the woman received the misoprostol tablets, i.e. whether it was before or after the recall.
Table 11: Reported experience of side effects among misoprostol users at TBA deliveries
Birim South (n=425)
KEEA (n=252)
Sene (n=668)
Upper Manya Krobo (n=68)
Total (n=1,413)
None 407 (95.8%)
235 (93.3%)
634 (94.9%)
63 (92.7%)
1,339 (94.8%)
Shivering 11 (2.6%) 10 (4.0%) 25 (3.7%) 3 (4.4%) 49 (3.5%) Nausea/vomiting 3 (0.7%) 1 (0.4%) 4 (0.6%) 1 (1.5%) 9 (0.6%) Watery stools 0 2 (0.8%) 1 (0.2%) 0 3 (0.2%) Temperature increase 1 (0.2%) 2 (0.8%) 4 (0.6%) 0 7 (0.5%) Source: TBA Delivery Form

20
Box 4: Provider perspectives
5. Major Conclusions and Discussion
This pilot project provides evidence for the feasibility and safety of misoprostol distribution through antenatal care (ANC) visits for prevention of postpartum hemorrhage at home births. Facility use of misoprostol was also important in cases where oxytocin was not consistently available. The following are additional important discussion points based on the results.
MISOPROSTOL DISTRIBUTION AT ANC GREATLY INCREASES UTEROTONIC COVERAGE AT HOME DELIVERIES The pilot project results demonstrate that approximately 93% of the women who delivered at home and returned for postnatal care (PNC) during this pilot received uterotonic coverage from misoprostol. Without the availability of misoprostol, those women would have had no protection from postpartum hemorrhage (PPH). In addition, in Upper Manya Krobo and Sene districts, approximately one out of five women who enrolled did not live in the catchment area, as both of these districts serve clients living on islands in the Volta Lake. This illustrates that misoprostol distribution at ANC can successfully offer uterotonic protection to women who access health services on a limited basis or who cannot make it to a health facility for delivery.
TRADITIONAL BIRTH ATTENDANTS AND WOMEN BOTH REPORT THAT MISOPROSTOL WAS USED CORRECTLY For those women who accepted misoprostol at ANC, usage was reported as very high and overwhelmingly correct, with 99% of women reporting at their PNC visit that they correctly used misoprostol at a home delivery. Traditional birth attendants (TBAs) also collected information on
“Before (the misoprostol pilot project) women would deliver and sometimes they would bleed and continue to bleed. Many women had bleeding that did not stop. I would send them to the health facility when this happened. With misoprostol, some women will bleed small, but bleeding always stops.”
Traditional birth attendant, Tator Bator (Sene District)
“Many of the women who come (to ANC) are from far away and they cannot go to the health center to deliver. Maybe if they try, they will deliver in the car. If there is no car to go, they cannot walk. The misoprostol is helping them a lot, and it is also helping us (providers) because there are fewer complications (referrals).”
Community Health Nurse, Kokobeng CHPS (Birim South District)
“It (misoprostol) has been very good for us (the providers). It has increased our ANC attendance, and more women are now coming to deliver at the facility. It is very important for the women who deliver with the TBAs, for the women who live far away and cannot come to the facilities for delivery. Before, PPH was our biggest problem, and when women delivered far away and had PPH, many women died before they arrived at the facility. We are so happy with the misoprostol because we see that it is saving women’s lives.”
Comfort, District Public Health Nurse (Birim South District)
21
correct use of misoprostol at home deliveries and reported that 99% of women took the correct dose of misoprostol for prevention of PPH.
WOMEN RETURN UNUSED MISOPROSTOL TO FACILITIES Overall, almost all (95%) of the misoprostol tablets that were distributed were used at delivery or returned to a facility, according to data collected from those who attended PNC. Of the women who did not use misoprostol at delivery and returned for a PNC visit, 83% of those who delivered at home and 92% of those who delivered at a facility returned unused misoprostol to a facility. This is a key point, as it is critical to track drugs that are introduced at the community level. Women demonstrated that they could be held accountable for the misoprostol that they took home from ANC and that they could be trusted to return unused misoprostol.
MISOPROSTOL DISTRIBUTION AT LOWEST LEVEL FACILITIES (CHPS COMPOUNDS) IS CRITICAL TO REACHING WOMEN WHERE THEY ARE It is important to note that CHPS compounds were the source of misoprostol distribution for 23% of enrolled women in this pilot. This was most significant in Birim South, where about half of all distribution (52%) occurred at CHPS compounds. In order to achieve maximum uterotonic coverage, all facility levels should be able to distribute misoprostol to pregnant women for PPH prevention.
COMMUNITY HEALTH VOLUNTEERS AND TBAS ARE ESSENTIAL FOR COMMUNITY AWARENESS EFFORTS Over 300 TBAs and 200 community health volunteers (CHVs) were oriented to this pilot project and trained to educate women about the use of misoprostol and safe delivery. TBAs and CHVs both reported during supervisory visits that women and community members responded positively to their messages, and that women appreciated having messages about safe motherhood brought to them by fellow members of their community. Both TBAs and CHVs reported to VSI staff during monitoring visits that they felt capable of teaching women about misoprostol and how to correctly take the tablets.
GHANA IS AMONG A GROUP OF COUNTRIES TO DEMONSTRATE FEASIBILITY OF COMMUNITY-LEVEL DISTRIBUTION OF MISOPROSTOL FOR PPH PREVENTION Since 2008, VSI has collaborated with ministries of health and local implementing partners in seven countries to develop evidence for the feasibility of use of misoprostol at the community level for prevention of postpartum hemorrhage. Building on the health infrastructure in each country, particularly by engaging the health workers closest to women at the community level, the partners have adapted the distribution mechanism to maximize uterotonic coverage in each setting. Among these countries, six have successfully demonstrated that ANC is an effective and feasible channel for distributing misoprostol for PPH prevention, including Tanzania, Zambia, Kenya, Mozambique, Bangladesh and now, Ghana. In addition, in Bangladesh, Kenya, Nigeria and Mozambique, community-‐level providers including trained birth attendants, community midwives and traditional birth attendants safely provided misoprostol to women at home deliveries. In these pilot programs, the proportion of births protected against PPH with any uterotonic drug increased through the introduction of misoprostol for use among those who are unable to deliver in a health facility (Venture Strategies Innovations et al., 2010, 2011).
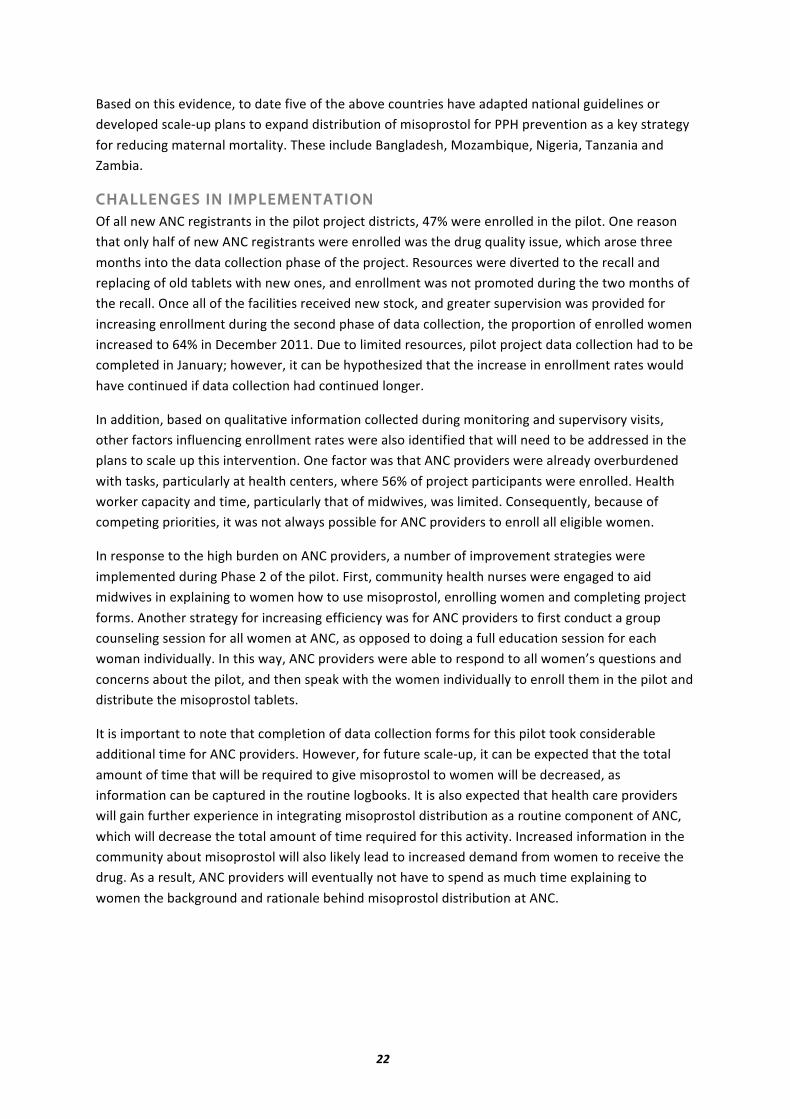
22
Based on this evidence, to date five of the above countries have adapted national guidelines or developed scale-‐up plans to expand distribution of misoprostol for PPH prevention as a key strategy for reducing maternal mortality. These include Bangladesh, Mozambique, Nigeria, Tanzania and Zambia.
CHALLENGES IN IMPLEMENTATION Of all new ANC registrants in the pilot project districts, 47% were enrolled in the pilot. One reason that only half of new ANC registrants were enrolled was the drug quality issue, which arose three months into the data collection phase of the project. Resources were diverted to the recall and replacing of old tablets with new ones, and enrollment was not promoted during the two months of the recall. Once all of the facilities received new stock, and greater supervision was provided for increasing enrollment during the second phase of data collection, the proportion of enrolled women increased to 64% in December 2011. Due to limited resources, pilot project data collection had to be completed in January; however, it can be hypothesized that the increase in enrollment rates would have continued if data collection had continued longer.
In addition, based on qualitative information collected during monitoring and supervisory visits, other factors influencing enrollment rates were also identified that will need to be addressed in the plans to scale up this intervention. One factor was that ANC providers were already overburdened with tasks, particularly at health centers, where 56% of project participants were enrolled. Health worker capacity and time, particularly that of midwives, was limited. Consequently, because of competing priorities, it was not always possible for ANC providers to enroll all eligible women.
In response to the high burden on ANC providers, a number of improvement strategies were implemented during Phase 2 of the pilot. First, community health nurses were engaged to aid midwives in explaining to women how to use misoprostol, enrolling women and completing project forms. Another strategy for increasing efficiency was for ANC providers to first conduct a group counseling session for all women at ANC, as opposed to doing a full education session for each woman individually. In this way, ANC providers were able to respond to all women’s questions and concerns about the pilot, and then speak with the women individually to enroll them in the pilot and distribute the misoprostol tablets.
It is important to note that completion of data collection forms for this pilot took considerable additional time for ANC providers. However, for future scale-‐up, it can be expected that the total amount of time that will be required to give misoprostol to women will be decreased, as information can be captured in the routine logbooks. It is also expected that health care providers will gain further experience in integrating misoprostol distribution as a routine component of ANC, which will decrease the total amount of time required for this activity. Increased information in the community about misoprostol will also likely lead to increased demand from women to receive the drug. As a result, ANC providers will eventually not have to spend as much time explaining to women the background and rationale behind misoprostol distribution at ANC.

23
6. Recommendations
This pilot project provides evidence that can inform the scale-‐up of community-‐level distribution of misoprostol to all eligible women in Ghana, with the goal of ensuring all women receive a uterotonic drug, regardless of where they deliver. Such a strategy will be significant in addressing maternal mortality due to postpartum hemorrhage, particularly in low-‐resource settings and at home deliveries where oxytocin is not feasible. The following are recommendations for a successful scale-‐up based on pilot project results.
TRAIN ALL ANC PROVIDERS TO DISTRIBUTE MISOPROSTOL All ANC providers should be trained to distribute misoprostol to pregnant women during routine ANC care. In this pilot, women who received misoprostol at an ANC visit and delivered at home used misoprostol correctly almost universally, indicating the high quality of education they received from ANC providers. Regular trainings should be organized for new ANC providers to ensure that all facility providers have the skills to educate on and distribute misoprostol to eligible women; refresher trainings for existing providers should be conducted as well. Additionally, lower-‐level providers should also be trained on misoprostol, in order to assist ANC providers with the necessary documentation related to misoprostol distribution. Midwives are often extremely busy providing routine ANC services, and training community health nurses to educate about and distribute misoprostol will be essential to ensuring that busy health centers and hospitals have the capability to distribute misoprostol to all eligible women at ANC. Group counseling to women about misoprostol is recommended as an effective and time-‐efficient means of educating women at ANC, as opposed to one-‐on-‐one counseling. Given the many languages that are spoken in Ghana, it is important to encourage providers to use pictorial information, education and communication (IEC) materials to explain misoprostol to women, especially since some providers mentioned that language could be a barrier to communicating with women about misoprostol.
ORIENT TBAS TO AID WOMEN IN TAKING MISOPROSTOL AT DELIVERY All TBAs should be oriented on misoprostol in order to support women who have taken misoprostol home from ANC and deliver with a TBA. TBAs effectively reported on the deliveries they attended with women who had received misoprostol, and almost all women who delivered with TBAs used misoprostol correctly. TBAs should also be encouraged to use pictorial IEC materials to explain to women how to correctly use misoprostol.
CONTINUE COMMUNITY-LEVEL AWARENESS EFFORTS WITH TBAS AND CHVS TBAs and CHVs should continue community awareness efforts and incorporate stories from women who have taken misoprostol into these efforts. Community leaders should also be encouraged to hold durbars to discuss misoprostol, and district-‐level health workers should continue to facilitate other promotional activities such as megaphone announcements in villages. Continued collaboration with village leaders and Queen Mothers should also be maintained and strengthened. Ensuring that communities understand the benefits of misoprostol for reducing PPH at home births will be essential to increasing enrollment at ANC when this project is scaled up in Ghana.

24
MAKE MISOPROSTOL AVAILABLE AT ALL ANC AND DELIVERY FACILITIES To ensure that providers have all the tools available to them to help prevent PPH, both misoprostol and oxytocin should be available in delivery rooms. There are situations where oxytocin may not be available due to stock-‐outs, improper storage or drug expiration. For this reason, we recommend that all facilities where deliveries take place and where women access antenatal care consistently stock misoprostol to increase the likelihood that a woman will receive a uterotonic at delivery.
DEVELOP STRATEGIES FOR SECURING CONSISTENT AVAILABILITY OF HIGH-QUALITY MISOPROSTOL TABLETS It is important to have multiple misoprostol products registered in Ghana in order to ensure the continual availability of high-‐quality misoprostol. This can be achieved through registration of misoprostol for specific obstetric indications, an effort currently being pursued by GHS and the Food and Drugs Board. Availability of at least two different products will provide a supply cushion in the event of any future problems with drug quality, while at the same time increasing availability of the drug in the country through various distribution networks. It is also important to engage the private sector during the registration process, in order to extend the range of outlets where high-‐quality registered tablets can be made available to women.
INCORPORATE MISOPROSTOL DISTRIBUTION AND POSTNATAL FOLLOW-UP INTO EXISTING OUTREACH ACTIVITIES AND FACILITY FORMS To ensure that misoprostol reaches women in rural areas and to maximize follow-‐up coverage, misoprostol distribution and early postnatal follow-‐up efforts should be incorporated into existing outreach activities, which include vaccination campaigns and general health outreach visits to rural villages to support maternal and newborn health. These visits provide an ideal opportunity to educate and provide rural women with misoprostol. Further, as opposed to having separate forms for enrolling women in the project, data on misoprostol distribution and follow-‐up should be collected using existing facility logbooks, which can be revised to capture misoprostol-‐related data.
ADDITIONAL RECOMMENDATIONS FROM NATIONAL DISSEMINATION MEETING IN ACCRA ON MARCH 19, 2012 On the occasion of the meeting to disseminate the results of this pilot project, Ghana Health Service and key maternal health stakeholders echoed the recommendation of scaling up the distribution of misoprostol at ANC for prevention of postpartum hemorrhage at home deliveries in Ghana. Meeting participants developed the following additional recommendations:
-‐ Equip community health volunteers to conduct postnatal follow-‐up in hard-‐to reach areas. -‐ Develop a feasible system to record the return and destruction of unused tablets. -‐ Include misoprostol in a free maternal health package.
The project partners and key stakeholders recommend a phased scale-‐up of misoprostol distribution at ANC as a strategy for increasing the number of women who receive a uterotonic drug at the time of delivery, and to thereby contribute to a reduction in the burden of PPH and maternal mortality in Ghana for years to come.
25
7. References
Alfirevic Z, Blum J, Walraven G et al. Prevention of postpartum hemorrhage with misoprostol. International Journal of Gynecology and Obstetrics 2007;99:S198-‐S201.
Amooti-‐Kagunaa B, Nuwahab F. Factors influencing choice of delivery sites in Rakai district of Uganda. Social Science and Medicine 2000;50:203-‐13.
Asamoah BO, Moussa KM, Stafstrom M, et al. Distribution of causes of maternal mortality among different socio-‐demographic groups in Ghana; a descriptive study. BMC Public Health 2011;159 (11) doi: 1471-‐2458-‐11-‐159
Cotter K, Hawken M, Temmerman M. Low use of skilled attendants’ delivery services in rural Kenya. Journal of Health, Population, and Nutrition 2006;24 (4):467-‐71.
Demographic Data. Komenda-‐Edina-‐Eguafo-‐Abirem District, 2010.
Derman R, Kodkany B, Goudar S et al. Oral misoprostol in preventing postpartum haemorrhage in resource-‐poor communities: a randomised controlled trial. Lancet 2006;368 (9543):1248-‐53. District Profile. Sene District, 2010.
District Profile. Birim South District, 2010.
Duong DV, Binns CW, Lee AH. Utilization of delivery services at the primary health care level in rural Vietnam. Social Science & Medicine 2004;59:25-‐2595.
Ethiopia Federal Ministry of Health, Venture Strategies for Health and Development, DKT-‐Ethiopia. Community Level Prevention of Postpartum Hemorrhage: The Role of Misoprostol. Final Report, May 2008.
Ghana Health Service, Reproductive and Child Health Department. Ghana Health Service Strategic Plan 2007-‐2011. April 2007.
Ghana Ministry of Health. Ghana Standard Treatment Guidelines, Sixth Edition. Accra, Ghana: Ghana National Drugs Programme, 2010.
Ghana Statistical Service (GSS), Ghana Health Service (GHS) and Macro International. Ghana maternal health survey 2007. Calverton, Maryland, USA: GSS, GHS, and Macro International, 2009a.
Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF Macro. Ghana demographic and health survey 2008. Accra, Ghana: GSS, GHS, and ICF Macro, 2009b.
Half Year Report. Komenda-‐Edina-‐Eguafo-‐Abirem District, 2011.
International Confederation of Midwives (ICM)/International Federation of Obstetricians and Gynecologists (FIGO). Prevention and treatment of post-‐partum haemorrhage: New advances for low resource settings. ICM-‐FIGO Joint Statement. ICM/FIGO, 2006.
Mobeen N, Durocher J, Zuberi N et al. Administration of misoprostol by trained traditional birth attendants to prevent postpartum haemorrhage in homebirths in Pakistan: a randomized placebo-‐controlled trial. British Journal of Obstetrics & Gynaecology 2011;118 (3):353-‐61.
Parsons SM, Walley RL, Crane JM et al. Rectal misoprostol versus oxytocin in the management of the third stage of labour. Journal of Obstetrics and Gynaecology Canada 2007;29 (9):711-‐8.

26
Potts M. Misoprostol in Practice. A Textbook of Postpartum Hemorrhage. Duncow, Kirkmahoe, Dumfrieshire, UK: Sapiens Publishing, 2006; 178-‐179
Prata N, Ejembi C, Fraser A et al. Community mobilization to reduce postpartum hemorrhage in home births in northern Nigeria. Social Science & Medicine 2012;74:1288-‐96.
Prata N, Hamza S, Bell S et al. Inability to predict postpartum hemorrhage: insights from Egyptian intervention data. BMC Pregnancy and Childbirth 2011;11:97-‐106.
Prata N, Gessessew A, Abraha AK et al. Prevention of postpartum hemorrhage: options for home births in rural Ethiopia. African Journal of Reproductive Health 2009;13 (2):87-‐95.
Rajbhandari S, Hodgins S, Sanghvi H et al. Expanding uterotonic protection following childbirth through community-‐based distribution of misoprostol: operations research study in Nepal. International Journal of Gynaecology and Obstetrics 2010;108 (3):282-‐8.
Reproductive and Child Health Annual Report. Birim South District, 2010.
Reproductive and Child Health Annual Report. Komenda-‐Edina-‐Eguafo-‐Abirem District, 2010.
Reproductive and Child Health Annual Report. Sene District, 2010.
Reproductive and Child Health Annual Report. Upper Manya Krobo District, 2010.
Sanghvi H, Ansari N, Prata N et al. Prevention of postpartum hemorrhage at home birth in Afghanistan. International Journal of Gynaecology and Obstetrics 2010;108 (3):276-‐81.
United States Agency for International Development (USAID). Postpartum hemorrhage: Prevention and management: Technical brief. USAID, 2011. Accessed online 24 February 2012 at http://www.k4health.org/system/files/PPH%20TechBrief%20nov2011%20v2.pdf
Venture Strategies Innovations, Associação Moçambicana de Obstetras e Ginecologistas, PSI/Mozambique, Bixby Center for Population, Health and Sustainability. Community-‐based Prevention of Postpartum Hemorrhage with Misoprostol in Mozambique. Final Report, May 2011d.
Venture Strategies Innovations, ICDDR,B, RDRS Bangladesh, Bixby Center for Population, Health and Sustainability. Scaling Up of Misoprostol for Prevention of Postpartum Hemorrhage in 29 Upazilas of Bangladesh. Final Report, May 2011c.
Venture Strategies Innovations, Ministry of Health, Zambia, Bixby Center for Population, Health and Sustainability. Misoprostol Distribution at Antenatal Care Visits for Prevention of Postpartum Hemorrhage. Final Report, December 2010b. Venture Strategies Innovations, Ministry of Health and Social Welfare, Tanzania, Ifakara Health Institute, Bixby Center for Population, Health and Sustainability, PSI/Tanzania. Prevention of Postpartum Hemorrhage at Home Births: Misoprostol Distribution during Antenatal Care Visits in Tanzania. Final Report, February 2011b.
Venture Strategies Innovations, Ministry of Public Health and Sanitation, Kenya, Kenya Obstetrical and Gynaecological Society. Introduction of Misoprostol for Prevention of Postpartum Hemorrhage at the Community Level in Kenya. Final Report, March 2011a.
Venture Strategies Innovations, Population and Reproductive Health Partnership, Ahmadu Bello University, Bixby Center for Population, Health and Sustainability. Prevention of Postpartum

27
Hemorrhage at Home Births in Five Communities around Zaria, Kaduna State, Nigeria. Final Report, June 2010a.
World Health Organization (WHO). Trends in maternal mortality: 1990 to 2008 estimates developed by WHO, UNICEF, UNFPA and The World Bank. Geneva: WHO, 2010. Accessed online 20 January 2012 at http://whqlibdoc.who.int/publications/2010/9789241500265_eng.pdf
World Health Organization. WHO Model List of Essential Medicines. 16th list (updated) March 2010. Accessed online 23 April 2011 at: http://www.who.int/selection_medicines/committees/expert/17/sixteenth_adult_list_en.pdf