division of general internal medicine and geriatrics...
TRANSCRIPT

Division of General Internal Medicine and Geriatrics
Hospital Medicine
Revised 2015

Define Anemia
Describe both kinetic and morphologic approach to determining cause of anemia
Understand pertinent history, physical findings, and indicated studies
Recognize common types of anemia seen in clinical practice
Objectives

Exact cut-off values vary slightly by populations, but in
general, anemia is defined as
Hgb <13.5g/dL or Hct <41% in men
Hgb <12g/dL or Hct <36% in women
Keep in mind that Hgb and Hct are concentrations and dependent on volume status
Anemia

Erythropoiesis takes place within the bone marrow under
the influence of erythropoietin (EPO), a hormone produced in the kidney by cells that sense the adequacy of tissue oxygenation
Immature RBCs (reticulocytes) are formed and typically mature in the marrow for 2-3 days, then are released into the circulation, where they mature for an additional day
RBC circulates for 110-120 days, then is removed by macrophages
Under steady state, RBC production = RBC loss
RBC life cycle
Symptoms are due to decreased Oxygen delivery and, in
the case of acute bleeding, hypovolemia
Primary symptoms: DOE dyspnea at rest
fatigue
palpitations
If severe: lethargy, confusion, high output heart failure, MI
Hypovolemia: dizziness, syncope, shock
Symptoms

Causes of Anemia
Kinetic Approach
Decreased RBC production
Increased RBC destruction
Blood loss
Morphologic Approach
Based on measurement of RBC size Normocytic
Microcytic
Macrocytic
Iron def
Thalassemias
Sideroblastic (congenital, lead, EtOH, drugs)
AOCD
Copper def, Zinc poisoning (rare)
Microcytic (MCV<80)

Acute blood loss
IDA (early)
AOCD (infection, inflammation)
Chronic renal insufficiency
Hypothyroidism
Hypopituitarism
Bone marrow suppression (may also be macrocytic)
Normocytic (MCV 80-100)

Alcohol abuse
B12 deficiency
Folate deficiency
Myelodysplastic syndromes
Reticulocytosis (response to blood loss, hemolysis, etc)
Liver disease
Acute myeloid leukemias
Drug induced (eg, Hydroxyurea, AZT, chemo agents)
Macrocytic (MCV>100)

Take a good history!!
Look for chronic blood loss (dark stools, dyspepsia, abnormal menses, etc)
PMH, signs of infection or inflammatory diseases
Family history of blood disorders, inflamm dz, etc
Medications
Diet, EtOH use, Pica
Neurologic symptoms
Evaluation of the Patient with Anemia

Assess severity and find signs of organ or multisystem
involvement. Tachycardia, Postural hypotension
Dyspnea
Fever
Jaundice
Pallor
Petechiae, ecchymoses
Splenomegaly
Lymphadenopathy
Stool for occult blood
Physical Exam

Laboratory Evaluation
Look at other cell lines (WBC, platelets), RBC indices such as MCV, MCH
Reticulocytes Reticulocyte Production Index of >3 indicates a normal response;
<2 inadequate response
Hemolysis labs: Increased LDH, decreased Haptoglobin, increased indirect bilirubin
Iron studies, B12, Folate, LFTs, Cr, TFTs
Hgb electropheresis
Peripheral blood smear: schistocytes, tear drop cells, look for abnormal WBCs or platelets as well
Bone Marrow bx


Iron is needed in the marrow for heme synthesis RBC
production and maturation
Causes: blood loss (GI, menstrual)
Decreased supply: malnutrition, malabsorption
Increased need (pregnancy)
Microcytosis, anisopoikilocytosis (unequal RBC size, shape)
↓Iron, ↑TIBC (transferrin), ↓Transferrin saturation, and ↓Ferritin (<15)
Treatment: Reverse underlying cause, PO Iron (constipation, dark stools), IV Iron sucrose
Iron Deficiency Anemia (IDA)
Needed for DNA synthesis
Binds to intrinsic factor secreted by gastric parietal cells, then is absorbed in the ileum
Causes:
Malnutrition (alcoholics, vegans, elderly)
Malabsorption: Pernicious anemia (↓IF), sprue, Crohn’s, s/p gastric bypass
Glossitis, neurologic and psychiatric symptoms, sometimes pancytopenia
↓B12 (cobalamin), ↑homocysteine and methylmalonic acid
Hypersegmented neutrophils on smear
Treatment: 1mg B12 IM daily x 7d, then weekly x 4 weeks, then monthly for life if malabsorption (OK to use PO after stores replete in those with normal absorption)
B12 Deficiency

Small stores of folate in body, thus you can become deficient
relatively quickly (but can also be repleted quickly)
Causes:
Malnutrition, EtOH abuse, pregnancy, malabsporption, chronic hemolysis
Drugs: TMP, phenytoin, MTX
↓Folate, normal MMA, ↑homocysteine
It is reasonable to treat empirically with PO Folic Acid 1mg/day
Exclude B12 Deficiency before starting treatment as neurologic symptoms will progress
Folate Deficiency

Chronic infections, malignancy, collagen vascular diseases, HIV
Inflammatory cytokines decreases iron absorption and impairs iron utilization
Relative decrease in EPO production in response to low Hct
↓Transferrin (TIBC), ↓ or normal Iron, ↓ or normal %sat, ↑or normal Ferritin
Treatment:
Make sure iron stores replete
Can use ESA for goal Hgb 10-12g/dL (caution in malignancy)
Treat underlying disease
Anemia of chronic inflammation

Decreased renal cortical mass , decreased erythropoetin
Normochromic/normocytic
Peripheral smear may show Burr cells
ESA to achieve target Hbg levels 10 – 12
ESA can lead to HTN, Thrombosis, MI, CVA
Iron stores improve efficacy, Ferritin > 100
Anemia of Kidney Disease
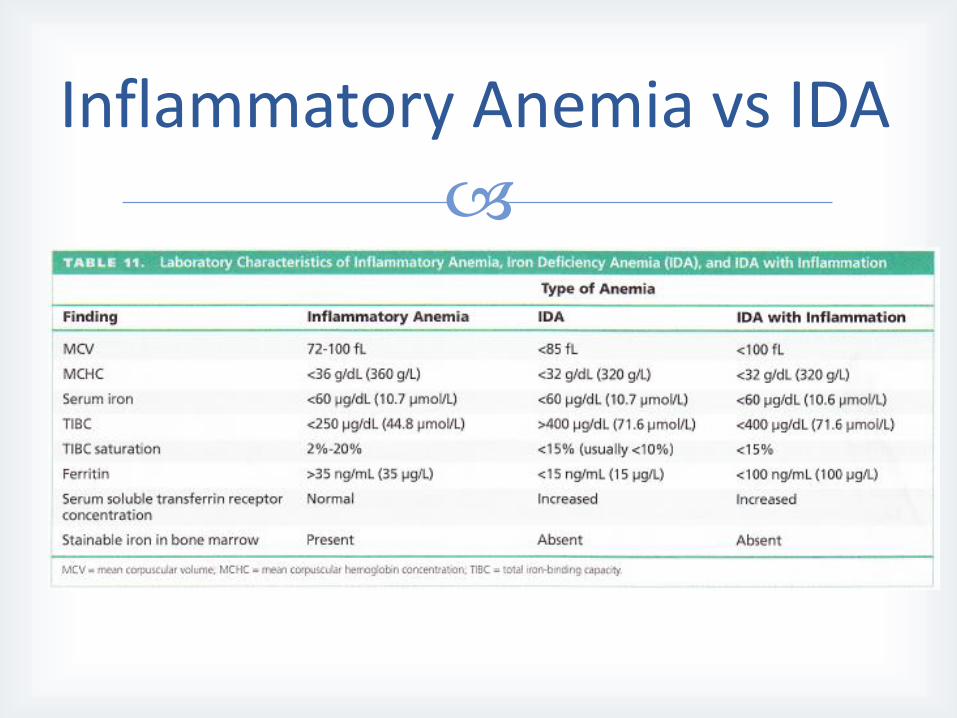
Inflammatory Anemia vs IDA

Apply your understanding of clinical history and physical
exam before ordering extensive laboratory studies
Evaluating the blood smear will always provide important information
Anemia is never normal
Key Messages

MKSAP 16, Hematology and Oncology, pp 18 – 35.
Up to Date; Approach to the adult patient with Anemia; Schrier, Stanley, Jan 2013.
ESRD Network II, Medical Review Committee 2011 goals.
Pocket Medicine, 3rd ed. Edited by Marc Sabatine, 2008.
References

Original Version: Pam Charity, MD 2013
Revised 6/11/2015: Stefanie Erway, MD
Revision History