division of regulation and...
TRANSCRIPT

CODE OF STATE REGULATIONS 1ROBIN CARNAHAN (7/31/07)Secretary of State
Rules of
Department of Health andSenior Services
Division 30—Division of Regulation and LicensureChapter 40—Comprehensive Emergency Medical
Services Systems Regulations
Title Page
19 CSR 30-40.005 Abbreviations and Definitions Relating to Ambulance Regulations(Rescinded February 28, 1999) .............................................................5
19 CSR 30-40.010 Staffing of Ambulances (Rescinded February 28, 1999) ................................5
19 CSR 30-40.020 Ambulance Vehicle Configuration and Equipment Requirements for Licensure(Rescinded February 28, 1999) .............................................................5
19 CSR 30-40.025 Ambulance Markings (Rescinded February 28, 1999) ...................................5
19 CSR 30-40.030 Insurance Requirements for Ambulance Licensure(Rescinded February 28, 1999) .............................................................5
19 CSR 30-40.035 Reporting Fire and Motor Vehicle Accidents Involving Ambulances(Rescinded February 28, 1999) .............................................................5
19 CSR 30-40.040 Patient Care Equipment (Rescinded February 28, 1999) ................................5
19 CSR 30-40.045 Communicable Disease Policy (Rescinded February 28, 1999) ........................5
19 CSR 30-40.047 Mandatory Notice to Emergency Response Personnel of Possible Exposure to Communicable Diseases ......................................................5
19 CSR 30-40.048 Training for Emergency Response Personnel and Good Samaritans on the Communicable Disease Reporting Regulation(Rescinded February 28, 1999) ............................................................12
19 CSR 30-40.050 Mobile Emergency Medical Technicians (Rescinded February 28, 1999)...........12
19 CSR 30-40.060 Emergency Medical Service Personnel Application(Rescinded February 28, 1999) ............................................................12
19 CSR 30-40.070 Public Convenience and Necessity Hearings (Rescinded February 28, 1999)......12
19 CSR 30-40.080 Records and Forms (Rescinded February 28, 1999) ....................................12

2 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40.090 Examination Procedures (Rescinded February 28, 1999) ..............................12
19 CSR 30-40.100 Relicensure Procedures (Rescinded February 28, 1999) ...............................12
19 CSR 30-40.110 Procedures for EMS Course Approvals (Rescinded February 28, 1999) ............12
19 CSR 30-40.115 Requirements for Mobile Emergency Medical Technician (MEMT) Continuing Education/Quality Improvement (CE/QI) Programs(Rescinded February 28, 1999) ............................................................12
19 CSR 30-40.120 Instructor Qualifications for EMT Courses (Rescinded February 28, 1999) .......12
19 CSR 30-40.130 Use of Obturators by EMTs (Rescinded February 28, 1999)..........................12
19 CSR 30-40.140 Criteria for Revocation, Suspension, Probation and/or Denial of Initial or Renewal Application for Ambulance Attendant, Attendant/Driver and Mobile Emergency Medical Technician Licenses(Rescinded February 28, 1999) ............................................................12
19 CSR 30-40.150 Restriction on Licensure Actions Without Thorough Investigation and Administrative Review (Rescinded February 28, 1999) ..........................12
19 CSR 30-40.152 Criminal Background Checks by Department of Health for Licensure and Renewal Applications (Rescinded February 28, 1999) ..............12
19 CSR 30-40.160 Physician Medical Advisor Required for All Ambulance Services(Rescinded February 28, 1999) ............................................................12
19 CSR 30-40.170 Misrepresenting the Level of Ambulance Service or Training, a Violation of Law (Rescinded February 28, 1999) ....................................13
19 CSR 30-40.175 Minimum Training Level of Personnel Using Emergency Medical Equipment (Rescinded February 28, 1999) ....................13
19 CSR 30-40.180 Use of Pneumatic Counter Pressure Device by EMTs(Rescinded February 28, 1999) ............................................................13
19 CSR 30-40.190 Exceptions to the Requirement for Maintenance of Voice Contact or Telemetry in Regard to Mobile Emergency Medical Technician Advanced Life-Support Procedures (Rescinded February 28, 1999) ................13
19 CSR 30-40.195 Emergency Medical Services (EMS) Personnel Within the Hospital Emergency Department (Rescinded February 28, 1999) ...................13
19 CSR 30-40.200 Definitions Relating to Air Ambulance Services(Rescinded February 28, 1999) ............................................................13
19 CSR 30-40.210 Air Ambulance Regulations for Helicopter (Rescinded February 28, 1999) .......13
19 CSR 30-40.220 Air Ambulance Regulations for Fixed-Wing Aircraft(Rescinded February 28, 1999) ............................................................13

CODE OF STATE REGULATIONS 3ROBIN CARNAHAN (7/31/07)Secretary of State
19 CSR 30-40.302 Emergency Medical Services Regions and Committees ................................13
19 CSR 30-40.303 Medical Director Required for All: Ambulance Services and EmergencyMedical Response Agencies That Provide Advanced Life Support Services,Basic Life Support Services Utilizing Medications or Providing Assistancewith Patients’ Medications, or Basic Life Support Services PerformingInvasive Procedures Including Invasive Airway Procedures; DispatchAgencies Providing Pre-arrival Medical Instructions; andTraining Entities ..............................................................................13
19 CSR 30-40.308 Application and Licensure Requirements Standards for the Licensureand Relicensure of Air Ambulance Services ............................................15
19 CSR 30-40.309 Application and Licensure Requirements Standards for the Licensureand Relicensure of Ground Ambulance Services .......................................17
19 CSR 30-40.331 Application and Accreditation or Certification Requirements for TrainingEntities that Conduct Training for First Responders, Emergency MedicalDispatchers, Emergency Medical Technicians-Basic and EmergencyMedical Technicians-Paramedic ...........................................................19
19 CSR 30-40.333 Application and Licensure Requirements for the Licensure andRelicensure of Emergency Medical Response Agencies ThatProvide Advanced Life Support............................................................22
19 CSR 30-40.340 Initial Emergency Medical Technician Licensure of Mobile EmergencyMedical Technicians, Ambulance Attendants and Ambulance Attendant-DriversWho Have a License with an Expiration Date of August 28, 1998 or Later ......23
19 CSR 30-40.342 Application and Licensure Requirements for the Initial Licensure andRelicensure of Emergency Medical Technician-Basics and EmergencyMedical Technician-Paramedics ...........................................................23
19 CSR 30-40.365 Reasons and Methods the Department Can Use to Take AdministrativeLicensure Actions ............................................................................24
19 CSR 30-40.375 Uniform Data Collection System and Ambulance Reporting Requirementsfor Ambulance Services.....................................................................25
19 CSR 30-40.410 Definitions and Abbreviations Relating to Trauma Centers............................25
19 CSR 30-40.420 Trauma Center Designation Requirements................................................26
19 CSR 30-40.430 Standards for Trauma Center Designation ................................................28
19 CSR 30-40.440 Standards for Pediatric Trauma Center Designation ....................................32
Title 19—DEPARTMENT OFHEALTH AND SENIOR SERVICES
Division 30—Division ofRegulation and Licensure
Chapter 40—ComprehensiveEmergency Medical Services Systems
Regulations
19 CSR 30-40.005 Abbreviations andDefinitions Relating to Ambulance Regula-tions(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.005. Original rule filed March13, 1979, effective June 11, 1979. Amended:Filed Jan. 13, 1990, effective April 26, 1990.Rescinded: Filed Aug. 28, 1998, effectiveFeb. 28, 1999.
19 CSR 30-40.010 Staffing of Ambulances(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.010. Original rule filed Aug. 22,1974, effective Feb. 23, 1975. Amended:Filed Jan. 13, 1990, effective April 26, 1990.Rescinded: Filed Aug. 28, 1998, effectiveFeb. 28, 1999.
19 CSR 30-40.020 Ambulance VehicleConfiguration and Equipment Require-ments for Licensure(Rescinded February 28, 1999)
AUTHORITY: sections 190.115, RSMo 1986and 190.185, RSMo Supp. 1993. This rulewas previously filed as 13 CSR 50-40.020.Original rule filed Aug. 22, 1974, effectiveFeb. 23, 1975. Amended: Filed Oct. 7, 1983,effective Jan. 13, 1984. Rescinded: FiledAug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.025 Ambulance Markings(Rescinded February 28, 1999)
AUTHORITY: sections 190.115.1(4), RSMo1986 and 190.185, RSMo Supp. 1993. Thisrule was previously filed as 13 CSR 50-40.025. Original rule filed Oct. 7, 1983,effective Jan. 13, 1984. Rescinded: FiledAug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.030 Insurance Requirementsfor Ambulance Licensure(Rescinded February 28, 1999)
AUTHORITY: sections 190.120, RSMo 1986,190.185, RSMo Supp. 1993 and 537.610,RSMo Supp. 1989. This rule was previouslyfiled as 13 CSR 50-40.030. Original rulefiled Aug. 22, 1974, effective Feb. 23, 1975.Amended: Filed Oct. 7, 1983, effective Jan.13, 1984. Amended: Filed Nov. 14, 1989,effective Jan. 26, 1990. Rescinded: FiledAug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.035 Reporting Fire andMotor Vehicle Accidents Involving Am-bulances(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. Original rule filed Jan. 18, 1990,effective April 26, 1990. Rescinded: FiledAug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.040 Patient Care Equipment(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.040. Original rule filed Aug. 22,1974, effective Feb. 23, 1975. Amended:Filed Oct. 7, 1983, effective Jan. 13, 1984.Amended: Filed Jan. 13, 1990, effective April26, 1990. Amended: Filed Aug. 26, 1993,effective April 9, 1994. Rescinded: Filed Aug.28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.045 Communicable DiseasePolicy(Rescinded: February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. Original rule filed Jan. 18, 1990,effective April 26, 1990. Amended: FiledAug. 14, 1992, effective Feb. 26, 1993.Rescinded: Filed Aug. 28, 1998, effectiveFeb. 28, 1999.
19 CSR 30-40.047 Mandatory Notice toEmergency Response Personnel of PossibleExposure to Communicable Diseases
PURPOSE: This rule establishes an inquiryand notice procedure to be followed byreceiving medical facility personnel concern-ing the possibility of exposure to communica-ble diseases by emergency response personneland good samaritans.
(1) The following definitions shall be used inthe interpretation of this rule:
(A) Aerosols mean tiny invisible particlesor droplet nuclei usually less than ten (10)micrometers in diameter, which float on aircurrents and are capable of being suspendedin air for a considerable period of time andare not to be confused with droplet as definedin subsection (1)(F) of this rule;
(B) Airborne transmission means person-to-person transmission of infectious organ-isms through the air by means of dropletnuclei;
(C) Bloodborne transmission means per-son-to-person transmission of an infectiousagent through contact with an infected per-son’s blood or other body fluids;
(D) Communicable disease means aninfectious disease transmitted by a significantexposure as defined in subsections (2)(A)—(E) of this rule, and examples of likely com-municable diseases for investigation for pos-sible significant exposures are—
1. Airborne diseases—pulmonary tuber-culosis (Mycobacterium tuberculosis) andmeasles;
2. Bloodborne diseases—Hepatitis Band C and human immunodeficiency virus(HIV) infection including acquired immunod-eficiency syndrome (AIDS);
3. Droplet spread diseases—rubella,Corynebacterium diphtheriae, and Neisseriameningitides; and
4. Uncommon or rare diseases—hemor-rhagic fevers including Lassa, Marburg,Ebola and Congo-Crimean; plague (Yersiniapestis); and rabies;
(E) Designated officer means a city orcounty health department officer, or his/herdesignee, appointed by the director of theDepartment of Health or his/her designee.The designated officer’s designee may be, atlocal option, a person associated with anambulance service, fire department or otherenforcement agency; the designated officermay appoint multiple designees as needed;
(F) Droplets mean large particles of mois-ture that rapidly settle out on horizontal sur-faces and originate from talking, sneezing orcoughing;
(G) Droplet spread means brief passage ofan infectious agent through the air, usuallywithin three feet (3') of the source;
(H) Emergency means a sudden or unfore-seen situation or occurrence that requiresimmediate action to save life or to preventsuffering or disability; the determination ofthe existence of the emergency can be madeeither by the patient/victim or by any emer-gency response personnel (ERP) or goodsamaritan on the scene;
(I) Emergency response personnel (ERP)means firefighters, law enforcement officers,paramedics, emergency medical technicians,
CODE OF STATE REGULATIONS 5ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

first responders and other persons includingemployees of legally organized and recog-nized volunteer organizations—regardless ofwhether the individuals receive compensa-tion—who, in the course of professionalduties, respond to emergencies;
(J) Exposure or significant exposure meansan ERP or good samaritan has experienced apossible risk of becoming infected with acommunicable disease(s) including thoseidentified in paragraphs (1)(D)1.–4. of thisrule by a means identified in subsections(2)(A)–(E) of this rule;
(K) Good samaritans mean individuals thatare not ERPs that provide emergency medicalassistance or aid until ERPs arrive;
(L) Medical facility means a health carefacility licensed under Chapter 197, RSMo ora state medical facility;
(M) Pathogen means any disease-produc-ing microorganism;
(N) Patient means the victim of an emer-gency who has been aided by an ERP or goodsamaritan;
(O) Potentially life-threatening communi-cable disease means an infectious diseasewhich can cause death in a susceptible host;and
(P) Universal precautions means anapproach to infection prevention and controlthat requires all human blood and certainhuman body fluids to be treated as if infec-tious for HIV, hepatitis B virus (HBV), andother bloodborne pathogens.
(2) Means of transmission of communicablediseases are—
(A) Any person-to-person contact in whicha commingling of respiratory secretions (sali-va and sputum) between the patient and ERPor good samaritan may have taken place;
(B) Transmittal of the blood or bloody flu-ids of the patient onto the mucous membranes(mouth, nose or eyes) of the ERP or goodsamaritan or into breaks in the skin of theERP or good samaritan;
(C) Transmittal of other body fluids(semen, vaginal secretions, amniotic fluids,feces, wound drainage or cerebral spinalfluid) onto the mucous membranes or breaksin the skin of the ERP or good samaritan;
(D) Any nonbarrier unprotected contact ofthe ERP or good samaritan with mucousmembranes or nonintact skin of the patient;or
(E) Sharing of airspace by an ERP or agood samaritan with a patient who has beendetermined by the treating facility to have aninfectious disease caused by airbornepathogens.
(3) The designated officer shall have the fol-lowing duties:
(A) Collecting, upon request, facts sur-rounding possible exposure of an ERP orgood samaritan to a communicable disease orinfection;
(B) Contacting facilities that receivedpatients who potentially exposed ERPs orgood samaritans to ascertain if a determina-tion has been made as to whether the patienthas a communicable disease or infection andto ascertain the results of that determination;
(C) Notifying the ERP or good samaritanas to whether s/he has been exposed withinforty-eight (48) hours of receiving thepatient’s diagnosis report, medical informa-tion or necessary test results and providinginformation regarding the exposure, impor-tance of appropriate medical follow-up andconfidentiality; and
(D) Upon request of the receiving medicalfacility or coroner/medical examiner’s office,notifying the ERP or good samaritan ofpotential exposure to a communicable dis-ease.
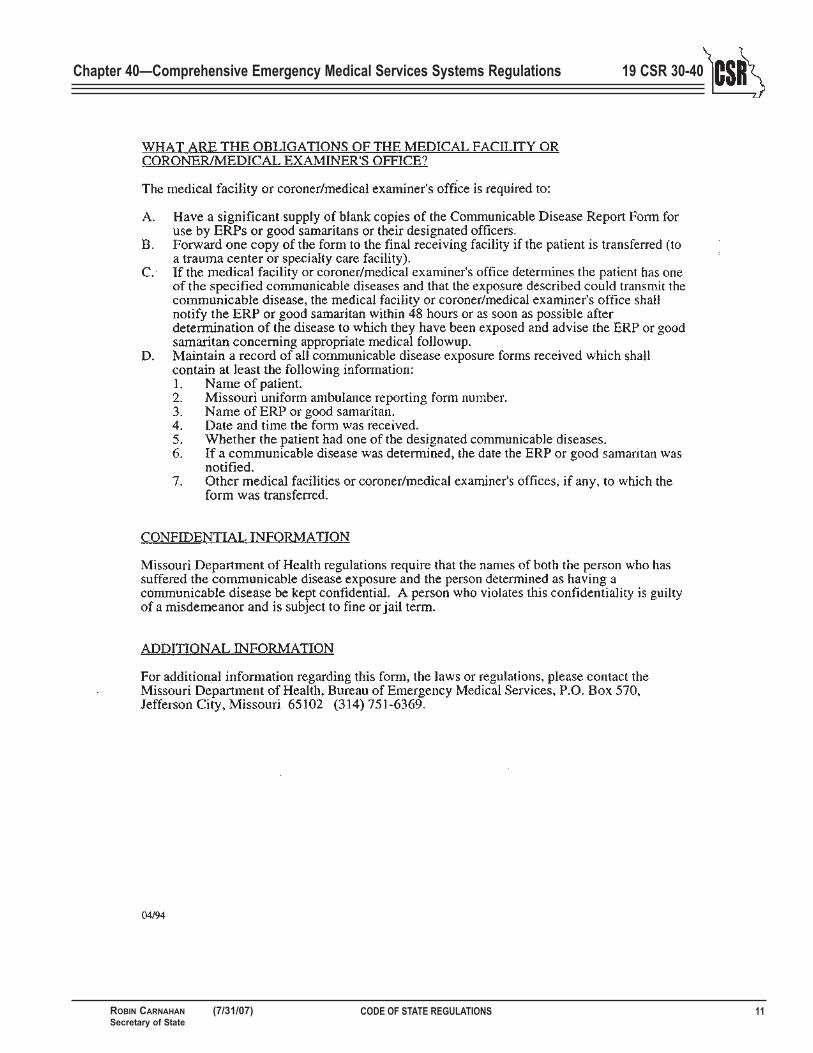
(4) The receiving medical facility personnelshall notify the ERP or good samaritan or theappropriate designated officer as soon asthere has been a determination that there mayhave been a significant exposure—as definedin subsection (1)(J), of this rule—to commu-nicable diseases including those identified inparagraphs (1)(D)1.–4. of this rule, by thosemeans identified in subsections (2)(A)–(E) ofthis rule, thereby creating a risk of infectionfrom a patient transported or assisted duringthe possible time of communicability of theparticular disease. Information provided shallinclude to the extent known the type of dis-ease in question; date, time and place of pos-sible exposure; and recommendations regard-ing appropriate followup. The receiving med-ical facility or coroner/medical examiner’soffice shall make a commitment to faithfullyimplement the procedures provided for bysection (4) of this rule, to assign appropriatepersonnel to investigate cases that appear tohave involved a significant exposure asdefined in subsection (1)(J) of this rule to anERP or good samaritan and to provide thenotification to the ERP or good samaritan ordesignated officer. If the receiving medicalfacility has determined that contacting theappropriate designated officer was better thannotifying the ERP or good samaritan directly,then the designated officer shall employ pre-viously developed policies and proceduresgoverning the dissemination of information tothe ERP or good samaritan and shall directthem to seek appropriate medical care. Noth-ing in this section shall be construed to imply
that a medical facility has absolute knowledgeas to the communicable disease status of allits patients at all times. Neither shall this sec-tion be construed as eliminating or reducingany preexisting duty under the common lawor sections 2681–2690 of the Public HealthService Act (PHS) in 42 U.S.C.A. 300ff-81–300ff-90 to determine the communicabledisease status of any patient.
(5) An ERP or good samaritan may submit arequest for a determination whether s/he hashad a significant exposure to a communicabledisease, preferably within twenty-four (24)hours but as soon as possible.
(A) Upon receipt of a request from a des-ignated officer, an ERP or good samaritan,the medical facility or coroner/medical exam-iner’s office shall evaluate the facts and deter-mine if the ERP or good samaritan may havehad a significant exposure to a communicabledisease.
(B) If a determination is made of a possi-bly significant exposure—as defined in sub-section (1)(J) of this rule—to a communicabledisease(s) including those identified in para-graphs (1)(D)1.–4. of this rule, by a meansidentified in subsections (2)(A)–(E) of thisrule, the ERP or good samaritan shall benotified as soon as possible, but not later thanforty-eight (48) hours after receiving thepatient’s diagnosis report.
(C) If the information provided by theERP, good samaritan or designated officer isinsufficient to make a determination, theERP, good samaritan or designated officershall be notified in writing, by telephone, orby electronic transmission as soon as possiblebut not later than forty-eight (48) hours afterreceiving the initial request.
(D) If the ERP, good samaritan or desig-nated officer receives notice that insufficientinformation was provided, the ERP or goodsamaritan may request the designated officerto evaluate the request and the medical facil-ity’s or coroner/medical examiner’s officeresponse. The designated officer shall thenevaluate the request and the medical facility’sor coroner/medical examiner’s response andreport his/her findings to the ERP or goodsamaritan as soon as possible but not laterthan forty-eight (48) hours after receiving therequest.
1. If the designated officer finds theinformation provided is sufficient to make adetermination of exposure, s/he shall submitthe report to the medical facility or coro-ner/medical examiner’s office.
2. If the designated officer finds theinformation provided was insufficient tomake a determination of exposure, s/he shallcontact the ERP or good samaritan to gather
6 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

CODE OF STATE REGULATIONS 7ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40
the additional needed information, contactthe medical facility or coroner/medical exam-iner’s office, or both, to collect any addition-al available relevant information. If sufficientfacts are then collected by the medical facili-ty or coroner/medical examiner’s office, theERP or good samaritan shall be notified ofany change in status.
3. If there was not a significant expo-sure, the medical facility, coroner/medicalexaminer’s office or designated officer shallnotify the ERP or good samaritan, or desig-nated officer (who shall notify the ERP orgood samaritan) within forty-eight (48)hours.
(6) If the ERP, good samaritan, designatedofficer and medical facility or coroner/medi-cal examiner’s office are unable to achievesatisfactory resolution to questions or issuesunder the procedures in subsections(5)(A)–(D) of this rule, a request may bemade to the Department of Health, throughits director or the director’s designee, toresolve the issues or questions, preferablywithin seventy-two (72) hours, but as soon aspossible.
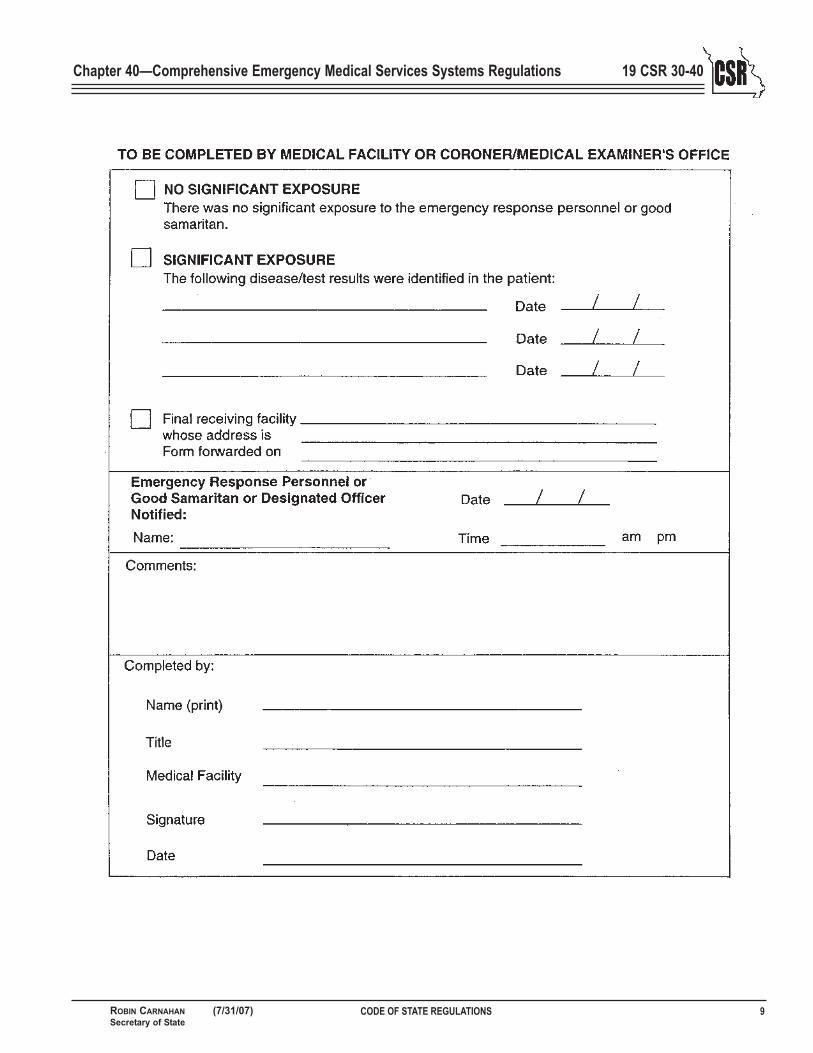
(7) The Department of Health’s Com -municable Disease Exposure Report (formMO 580-1825, 4/94) shall be used by ERPsor good samaritans to notify medical facilitiesor coroners/medical examiner’s office or des-ignated officer regarding suspected exposure.The ERP or good samaritan shall retain acopy of the form and shall send one (1) copyto the designated officer and one (1) copy tothe receiving medical facility orcoroner/medical examiner’s office.
(8) The designated officer and the localhealth department shall assure that an ade-quate supply of reporting forms is provided toall receiving medical facilities orcoroner/medical examiner’s offices withinthe geographic area served.
(9) The notification process established bythe receiving medical facility orcoroner/medical examiner’s office to dealwith reported exposures to ERPs or goodsamaritans shall be as comprehensive as thatfor employees of the medical facility or coro-ner/medical examiner’s office.
(10) Receiving medical facilities or coro-ner/medical examiner’s offices and designat-ed officers with information regarding thesignificant exposure—as defined in subsec-tion (1)(J) of this rule—of an ERP or goodsamaritan to a communicable disease(s)including those identified in paragraphs
(1)(D)1.–4. of this rule by a means identifiedin subsections (2)(A)–(E) of this rule, shallprovide information directly to the affectedERP. In the case of a good samaritan the des-ignated officer or his/her designee shall pro-vide the information directly to the goodsamaritan. All information shall be in a man-ner that protects the identity and confiden-tiality of the possibly infected individual andthe ERP or good samaritan.
(11) A sending medical facility in advance ofthe transfer of a patient to another medicalfacility or back to the patient’s residence shallnotify the ambulance personnel of the exis-tence and nature of any communicable dis-ease(s) including those identified in para-graphs (1)(D)1.–4. of this rule by thosemeans identified in subsections (2)(A)–(E) ofthis rule and appropriate precautions and pro-cedures to follow. If the information suppliedby the sending medical facility is unclear tothe ambulance personnel, the ambulance per-sonnel may make a specific inquiry as towhether there are any known communicabledisease(s) involving a possible significantexposure that might occur during the trans-port of the patient. Nothing in this sectionshall be construed to imply that a medicalfacility has absolute knowledge as to the com-municable disease status of all its patients atall times, but neither shall this section beconstrued to imply that a medical facility hasabsolute knowledge as to the communicabledisease status of all its patients at all times,but neither shall this section be construed aseliminating or reducing any preexisting dutyunder the common law or sections2681–2690 of the PHS Act in 42 U.S.C.A.300ff-81–300ff-90 to determine the commu-nicable disease status of any patient.
AUTHORITY: sections 192.020, RSMo 1986and 192.806.1, RSMo Supp. 1993.* Originalrule filed Feb. 2, 1994, effective Aug. 28,1994.
*Original authority: 192.020, RSMo 1939, amended1945, 1951 and 192.806, RSMo 1992, amended 1993.

8 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure
CODE OF STATE REGULATIONS 9ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

10 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure
CODE OF STATE REGULATIONS 11ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

19 CSR 30-40.048 Training for EmergencyResponse Personnel and Good Samaritanson the Communicable Disease ReportingRegulation (Rescinded February 28, 1999)
AUTHORITY: sections 192.020, RSMo 1986and 192.806.1, RSMo Supp. 1993. Originalrule filed Feb. 2, 1994, effective Aug. 28,1994. Rescinded: Filed Aug. 28, 1998, effec-tive Feb. 28, 1999.
19 CSR 30-40.050 Mobile EmergencyMedical Technicians(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.050. Original rule filed Aug. 22,1974, effective Feb. 23, 1975. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.060 Emergency MedicalService Personnel Application(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo 1994.Original rule filed Sept. 1, 1995, effectiveApril 30, 1996. Rescinded: Filed Aug. 28,1998, effective Feb. 28, 1999.
19 CSR 30-40.070 Public Convenience andNecessity Hearings (Rescinded February 28, 1999)
AUTHORITY: sections 190.125 and 190.185,RSMo 1994. This rule was previously filed as13 CSR 50-40.070. Original rule filed Aug.22, 1974, effective Feb. 23, 1975. Rescindedand readopted: Filed Nov. 16, 1987, effectiveJan. 29, 1988. Amended: Filed April 14,1992, effective Jan. 15, 1993. Emergencyamendment filed May 2, 1994, effective May14, 1994, expired Sept. 10, 1994. Amended:Filed May 2, 1994, effective Oct. 30, 1994.Amended: Filed Nov. 15, 1994, effective May28, 1995. Amended: Filed March 20, 1996,effective Sept. 30, 1996. Rescinded: FiledAug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.080 Records and Forms(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.080. Original rule filed Aug. 22,1974, effective Feb. 23, 1975. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.090 Examination Procedures(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.090. Original rule filed March13, 1979, effective June 11, 1979. Amended:Filed April 14, 1992, effective Jan. 15,1993. Rescinded: Filed Aug. 28, 1998, effec-tive Feb. 28, 1999.
19 CSR 30-40.100 Relicensure Procedures(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.100. Original rule filed March 13,1979, effective June 11, 1979. Amended:Filed June 4, 1990, effective Oct. 31, 1990.Amended: Filed Nov. 9, 1993, effective July10, 1994. Rescinded: Filed Aug. 28, 1998,effective Feb. 28, 1999.
19 CSR 30-40.110 Procedures for EMSCourse Approvals(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.110. Original rule filed March 13,1979, effective June 11, 1979. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.115 Requirements forMobile Emergency Medical Technician(MEMT) Continuing Education/QualityImprovement (CE/QI) Programs (Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. Original rule filed Nov. 9, 1993, effec-tive July 10, 1994. Rescinded: Filed Aug. 28,1998, effective Feb. 28, 1999.
19 CSR 30-40.120 Instructor Qualifi-cations for EMT Courses(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.120. Original rule filed March13, 1979, effective June 11, 1979. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.130 Use of Obturators byEMTs(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.130. Original rule filed March13, 1979, effective June 11, 1979. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.140 Criteria for Revocation,Suspension, Probation and/or Denial ofInitial or Renewal Application forAmbulance At ten dant, Attendant/Driverand Mobile Emergency Medical TechnicianLicenses(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo 1994.This rule was previously filed as 13 CSR 50-40.140. Original rule filed Oct. 7, 1983,effective Jan. 13, 1984. Amended: Filed Sept.1, 1995, effective April 30, 1996. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.150 Restriction on LicensureActions Without Thorough Investigationand Administrative Review(Rescinded February 28, 1999)
AUTHORITY: sections 190.165, RSMo 1986and 190.185, RSMo Supp. 1993. This rulewas previously filed as 13 CSR 50-40.150.Original rule filed Oct. 7, 1983, effectiveJan. 13, 1984. Rescinded: Filed Aug. 28,1998, effective Feb. 28, 1999.
19 CSR 30-40.152 Criminal BackgroundChecks by Department of Health forLicensure and Renewal Applications(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo 1994.Original rule filed Sept. 1, 1995, effectiveApril 30, 1996. Rescinded: Filed Aug. 28,1998, effective Feb. 28, 1999.
19 CSR 30-40.160 Physician MedicalAdvisor Required for All AmbulanceServices(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.160. Original rule filed Oct. 7,1983, effective Jan. 13, 1984. Amended:Filed Jan. 13, 1990, effective April 26, 1990.Amended: Filed Aug. 15, 1994, effective Feb.26, 1995. Rescinded: Filed Aug. 28, 1998,effective Feb. 28, 1999.
12 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure
19 CSR 30-40.170 Misrepresenting theLevel of Ambulance Service or Training, aViolation of Law(Rescinded February 28, 1999)
AUTHORITY: sections 190.185 RSMo Supp.1993 and 570.160, RSMo 1986. This rulewas previously filed as 13 CSR 50-40.170.Original rule filed Oct. 7, 1983, effectiveJan. 13, 1984. Rescinded: Filed Aug. 28,1998, effective Feb. 28, 1999.
19 CSR 30-40.175 Minimum TrainingLevel of Personnel Using EmergencyMedical Equipment(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. Original rule filed Jan. 18, 1990,effective April 26, 1990. Rescinded: FiledAug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.180 Use of PneumaticCounter Pressure Device by EMTs(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.180. Original rule filed Oct. 7,1983, effective Jan. 13, 1984. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.190 Exceptions to the Re-quirement for Maintenance of Voice Con-act or Telemetry in Regard to MobileEmergency Medical Technician AdvancedLife-Support Procedures(Rescinded February 28, 1999)
AUTHORITY: section 190.185, RSMo Supp.1993. This rule was previously filed as 13CSR 50-40.190. Original rule filed Oct. 7,1983, effective Jan. 13, 1984. Rescinded:Filed Aug. 28, 1998, effective Feb. 28, 1999.
19 CSR 30-40.195 Emergency Medical Ser-vice (EMS) Personnel Within the HospitalEmergency Department(Rescinded February 28, 1999)
AUTHORITY: sections 190.140, RSMo Supp.1987 and 190.185, RSMo. Supp. 1993.Original rule filed April 14, 1992, effectiveJan. 15, 1993. Rescinded: Filed Aug. 28,1998, effective Feb. 28, 1999.
19 CSR 30-40.200 Definitions Relating toAir Ambulance Services(Rescinded February 28, 1999)
AUTHORITY: sections 190.125, RSMo 1986and 190.185, RSMo Supp. 1993. Originalrule filed Jan. 5, 1988, effective March 25,1988. Rescinded: Filed Aug. 28, 1998, effec-tive Feb. 28, 1999.
19 CSR 30-40.210 Air Ambulance Regula-tions for Helicopter(Rescinded February 28, 1999)
AUTHORITY: sections 190.100(1) and190.185, RSMo Supp. 1993. Original rulefiled Jan. 5, 1988, effective March 25, 1988.Rescinded: Filed Aug. 28, 1998, effectiveFeb. 28, 1999.
19 CSR 30-40.220 Air Ambulance Regula-tions for Fixed-Wing Aircraft(Rescinded February 28, 1999)
AUTHORITY: sections 190.100(1) and190.185, RSMo Supp. 1993. Original rulefiled Jan. 5, 1988, effective March 25, 1988.Rescinded: Filed Aug. 28, 1998, effectiveFeb. 28, 1999.
19 CSR 30-40.302 Emergency MedicalServices Regions and Committees
PURPOSE: This rule identifies the countiesthat are included in each of the six (6) emer-gency medical services regions and establish-es the requirements for the appointment ofmembers to each of the six (6) regional com-mittees.
(1) The following identifies the counties thatshall be included in each of the six (6) emer-gency medical services (EMS) regions.
(A) The Central EMS region shall includethe counties of Adair, Audrain, Benton,Boone, Callaway, Camden, Chariton, Clark,Cole, Cooper, Dent, Gasconade, Howard,Knox, Lewis, Linn, Macon, Maries, Marion,Miller, Moniteau, Monroe, Montgomery,Morgan, Osage, Pettis, Phelps, Pulaski,Putnam, Ralls, Randolph, Saline, Schuyler,Scotland, Shelby, and Sullivan.
(B) The Kansas City EMS region shallinclude the counties of Bates, Caldwell,Carroll, Cass, Clay, Clinton, Henry, Jackson,Johnson, Lafayette, Platte, and Ray.
(C) The Northwest EMS region shallinclude the counties of Andrew, Atchison,Buchanan, Davies, DeKalb, Gentry, Grundy,
Harrison, Holt, Livingston, Mercer,Nodaway, and Worth.
(D) The St. Louis EMS region shallinclude the counties of Franklin, Jefferson,Lincoln, Pike, St. Charles, St. Louis,Warren, and St. Louis City.
(E) The Southeast EMS region shallinclude the counties of Bollinger, Butler,Cape Girardeau, Carter, Crawford, Dunklin,Iron, Madison, Mississippi, New Madrid,Pemiscot, Perry, Reynolds, Ripley, SaintFrancois, Sainte Genevieve, Scott, Stoddard,Washington, and Wayne.
(F) The Southwest EMS region shallinclude the counties of Barry, Barton, Cedar,Christian, Dade, Dallas, Douglas, Greene,Hickory, Howell, Jasper, Laclede, Lawrence,McDonald, Newton, Oregon, Ozark, Polk,St. Clair, Shannon, Stone, Taney, Texas,Vernon, Webster, and Wright.
(2) Each of the six (6) EMS regional com-mittees shall consist of no more than fifteen(15) members, appointed by the director ofthe Department of Health.
(3) The committees should include represen-tation from emergency medical technicians-basic, emergency medical technicians-paramedic, registered nurses with expertise inemergency medicine, firefighter/emergencymedical technicians, trauma surgeons, physi-cians with expertise in emergency medicine,trauma nurse coordinators from designatedtrauma centers, emergency medical responseagencies, ground ambulance service man-agers, EMS training entities, pediatric hospi-tals or physicians/registered nurses withexpertise in pediatric care, emergency medi-cal dispatchers, air ambulance services,physicians with expertise in EMS medicaldirection, local health departments, hospitaladministrators, medical examiners or coro-ners, and EMS consumers.
AUTHORITY: sections 190.102 and 190.185,RSMo 2000.* Original rule filed Dec. 1,2000, effective May 30, 2001.
*Original authority: 190.102, RSMo 1998; 190.185,RSMo 1973, amended 1989, 1993, 1995, 1998.
19 CSR 30-40.303 Medical DirectorRequired for All: Ambulance Services andEmergency Medical Response AgenciesThat Provide Advanced Life SupportServices, Basic Life Support ServicesUtilizing Medications or Providing Assis-tance With Patients’ Medications, or BasicLife Support Services Performing InvasiveProcedures Including Invasive AirwayProcedures; Dispatch Agencies Providing
CODE OF STATE REGULATIONS 13ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

Pre-arrival Medical Instructions; andTraining Entities
PURPOSE: This rule describes the qualifica-tions and requirements related to medicaldirectors of ambulance services, emergencymedical response agencies, dispatch agen-cies, and training entities.
(1) As used in this rule, the following termsshall have the meanings specified:
(A) ACLS—advanced cardiac life support;(B) ALS—advanced life support;(C) ATLS—advanced trauma life support;(D) BCLS—basic cardiac life support;(E) BLS—basic life support;(F) Board eligibility—a physician who has
applied to a specialty board and has receiveda ruling that s/he has fulfilled the require-ments to take the board examination and theboard certification must be obtained withinfive (5) years of the first appointment;
(G) EMS—emergency medical services;(H) EMT-Basic—emergency medical tech-
nician-basic;(I) EMT-Paramedic—emergency medical
technician-paramedic;(J) PALS—pediatric advanced life support;
and(K) Primary care specialty—family/gener-
al practice, internal medicine, or pediatrics.
(2) Ambulance services that provideadvanced life support services, basic life sup-port services utilizing medications (medica-tions include, but are not limited to, activat-ed charcoal, oral glucose and/or oxygen) orproviding assistance with patients’ medica-tions (patient medications include, but are notlimited, to a prescribed inhaler, nitroglycerinand/or epinephrine), or basic life support ser-vices performing invasive procedures includ-ing invasive airway procedures (invasive air-way procedures include, but are not limitedto, esophageal or endotracheal intubation)shall comply with this section of the regula-tion.
(A) Each licensed ambulance servicewhich provides ALS care shall have a medi-cal director who is licensed as a doctor ofmedicine or a doctor of osteopathy by theMissouri State Board of Registration for theHealing Arts and who has—
1. Board certification in emergencymedicine; or
2. Board certification or board eligibili-ty in a primary care specialty or surgery andhas actively practiced emergency medicineduring the past year and can demonstrate cur-rent course completion or certification inACLS, ATLS and PALS (certification inACLS, ATLS and PALS must be obtained no
later than one (1) year after initial ambulanceservice licensure), or documentation ofequivalent education in cardiac care, traumacare and pediatric care within the past five (5)years; or
3. An active practice in the community,with current course completion or certifica-tion in ACLS and PALS (certifications shallbe obtained no later than one (1) year afterinitial ambulance service licensure), or docu-mented equivalent education in cardiac careand pediatric care within the past five (5)years who develops a written agreement witha physician who meets the requirements stat-ed in (2)(A)1. or (2)(A)2. to review andapprove the processes required in (2)(C),(2)(D), and (2)(E) in order to facilitate themedical direction of the ambulance service.
(B) Each licensed ambulance servicewhich provides only BLS care shall have amedical director who is licensed as a doctorof medicine or a doctor of osteopathy by theMissouri State Board of Registration for theHealing Arts and can demonstrate currentcourse completion or certification in ACLSand PALS (certifications must be obtained nolater than one (1) year after initial ambulanceservice licensure), or can document equiva-lent education in cardiac care and pediatriccare within the past five (5) years.
(C) The medical director, in cooperationwith the ambulance service administrator,shall develop, implement and annually reviewthe following:
1. Medical and treatment protocols formedical, trauma and pediatric patients;
2. Triage and transport protocols;3. Protocols for do-not-resuscitate re-
quests;4. Air ambulance utilization; and5. Medications and medical equipment
to be utilized.(D) The medical director, in cooperation
with the ambulance service administrator,shall ensure that all licensed service person-nel meet the education and skill competenciesrequired for their level of license and patientcare environment. The medical director shallhave the authority to require additional edu-cation and training for any licensed servicepersonnel who fail to meet this requirementand limit the patient care activities of person-nel who deviate from established standards.
(E) The medical director, in cooperationwith the ambulance service administrator,shall develop, implement and annually reviewthe following:
1. Prolonged ambulance scene, responseor transport times;
2. Incomplete run documentation;3. Ambulances that are diverted from
their original destinations;
4. Compliance with adult and pediatrictriage, treatment and transport protocols (orsample thereof);
5. Skills performance (or sample there-of); and
6. Any other activities that the adminis-trator or medical director deem necessary.
(3) Emergency medical response agenciesthat provide advanced life support services,basic life support services utilizing medica-tions (medications include, but are not limit-ed to, activated charcoal, oral glucose and/oroxygen) or providing assistance with patients’medications (patient medications include, butare not limited to, a prescribed inhaler, nitro-glycerin and/or epinephrine), or basic lifesupport services performing invasive proce-dures including invasive airway procedures(invasive airway procedures include, but arenot limited to, esophageal or endotrachealintubation) shall comply with this section ofthe regulation.
(A) Each emergency medical responseagency which provides ALS care shall have amedical director who is licensed as a doctorof medicine or a doctor of osteopathy by theMissouri State Board of Registration for theHealing Arts and who has—
1. Board certification in emergencymedicine; or
2. Board certification or board eligibili-ty in a primary care specialty or surgery andhas actively practiced emergency medicineduring the past year and can demonstrate cur-rent course completion or certification inACLS, ATLS and PALS (certification inACLS, ATLS and PALS must be obtained nolater than one (1) year after initial emergencymedical response agency licensure), or docu-mentation of equivalent education in cardiaccare, trauma care and pediatric care withinthe past five (5) years; or
3. An active practice in the community,with current course completion or certifica-tion in ACLS and PALS (certifications shallbe obtained no later than one (1) year afterinitial emergency medical response agencylicensure), or documented equivalent educa-tion in cardiac care and pediatric care withinthe past five (5) years who develops a writtenagreement with a physician who meets therequirements stated in (3)(A)1. or (3)(A)2. toreview and approve the processes required in(3)(C), (3)(D), and (3)(E) in order to facili-tate the medical direction of the emergencymedical response agency.
(B) Each emergency medical responseagency which provides only BLS care shallhave a medical director who is licensed as adoctor of medicine or a doctor of osteopathyby the Missouri State Board of Registration
14 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

for the Healing Arts and can demonstratecurrent course completion or certification inACLS and PALS, or can document equivalenteducation in cardiac care and pediatric carewithin the past five (5) years.
(C) The medical director, in cooperationwith the emergency medical response agencyadministrator, shall develop, implement andannually review the following:
1. Medical and treatment protocols formedical, trauma and pediatric patients;
2. Triage protocols;3. Protocols for do-not-resuscitate
requests;4. Air ambulance utilization; and5. Medications and medical equipment
to be utilized.(D) The medical director, in cooperation
with the emergency medical response agencyadministrator, shall ensure that all licensedagency personnel meet the education and skillcompetencies required for their level oflicense and patient care environment. Themedical director shall have the authority torequire additional education and training forany licensed agency personnel who fail tomeet this requirement and limit the patientcare activities of personnel who deviate fromestablished standards.
(E) The medical director, in cooperationwith the emergency medical response agencyadministrator, shall develop, implement andannually review the following:
1. Prolonged emergency medical re-sponse agency response times;
2. Incomplete run documentation;3. Compliance with adult and pediatric
triage and treatment protocols (or samplethereof);
4. Skills performance (or sample there-of); and
5. Any other activities that the adminis-trator or medical director deem necessary.
(4) All dispatch agencies which provide pre-arrival medical instructions shall comply withthis section of the regulation.
(A) Each dispatch agency shall have a med-ical director who is licensed as a doctor ofmedicine or a doctor of osteopathy by theMissouri State Board of Registration for theHealing Arts who can demonstrate currentcourse completion or certification in ACLS,or can document equivalent education in car-diac care within the past five (5) years.
(B) The medical director, in cooperationwith the dispatch agency administrator, shalldevelop, implement and annually review thefollowing:
1. Medical pre-arrival instruction proto-cols; and
2. Standards related to the administra-tion of those protocols.
(C) The medical director, in cooperationwith the dispatch agency administrator, shallensure that all dispatch personnel givingmedical pre-arrival instructions meet the edu-cation and skill competencies required fortheir patient care environment. The medicaldirector shall have the authority to requireadditional education and training for any per-sonnel who fail to meet this requirement andlimit the activities related to giving medicalpre-arrival instructions of personnel whodeviate from established standards.
(D) The medical director, in cooperationwith the dispatch agency administrator, shalldevelop, implement and annually review thefollowing:
1. Prolonged ambulance or emergencymedical response agency dispatch times;
2. Compliance with medical pre-arrivalinstruction protocols (or sample thereof); and
3. Any other activities that the adminis-trator or medical director deem necessary.
(5) Training entities shall comply with thissection of the regulation.
(A) Each EMT-Paramedic training entityshall have a medical director who is licensedas a doctor of medicine or a doctor ofosteopathy by the Missouri State Board ofRegistration for the Healing Arts and whohas—
1. Board certification in emergencymedicine; or
2. Board certification or board eligibili-ty in a primary care specialty or surgery andhas actively practiced emergency medicineduring the past year and can demonstrate cur-rent course completion or certification inACLS, ATLS and PALS (certification inACLS, ATLS and PALS must be obtained nolater than one (1) year after initial trainingentity accreditation), or documented equiva-lent education in cardiac care, trauma careand pediatric care within the past five (5)years; or
(B) Each EMT-Basic, continuing educa-tion, first responder or emergency medicaldispatch training entity shall have a medicaldirector who is licensed as a doctor ofmedicine or a doctor of osteopathy by theMissouri State Board of Registration for theHealing Arts and can demonstrate currentcourse completion or certification in ACLSand PALS (certifications must be obtained nolater than one (1) year after initial trainingentity accreditation), or can document equiv-alent education in cardiac care and pediatriccare within the past five (5) years.
(C) Each EMS training entity medicaldirector shall be responsible for ensuring an
accurate and thorough presentation of themedical content of the education and trainingprogram. Ensure that the student has met theeducation and skill competencies based oncurrent national standards and scope of prac-tice for each level of licensure and/or certifi-cation.
AUTHORITY: sections 190.103, 190.108,190.109, 190.131, 190.133, 190.134 and190.185, RSMo Supp. 1998.* Emergencyrule filed Aug. 28, 1998, effective Sept. 7,1998, expired March 5, 1999. Original rulefiled Sept. 1, 1998, effective Feb. 28, 1999.Emergency rescission and rule filed July 30,1999, effective Aug. 9, 1999, expired Feb. 3,2000. Rescinded and readopted: Filed: July30, 1999, effective Jan. 30, 2000.
*Original authority: 190.103, RSMo 1998: 190.108, RSMo1998; 190.109, RSMo 1998; 190.131, RSMo 1998;190.133, RSMo 1998; 190.134, RSMo 1998; and190.185, RSMo 1973, amended 1989, 1993, 1995, 1998.
19 CSR 30-40.308 Application andLicensure Requirements Standards for theLicensure and Relicensure of Air Am-bulance Services
PURPOSE: This rule provides the require-ment and standards related to the licensureand relicensure of air ambulance services.
(1) Application Requirements for AirAmbulance Service Licensure.
(A) Each applicant for ownership of an airambulance service license or relicense shallsubmit an application for licensure to theBureau of Emergency Medical Services(EMS) no less than thirty (30) days or nomore than one hundred and twenty (120) daysprior to their desired date of licensure or reli-censure.
(B) An application shall include the fol-lowing information: type of license appliedfor (rotary wing or fixed wing); trade nameof air ambulance service; location of aircraft;number of aircraft to be used as an air ambu-lance(s); name, address, telephone numbersand e-mail address (if applicable) of operatorof air ambulance service; name of manager;name, address, whether a medical doctor ordoctor of osteopathy, telephone numbers, e-mail address (if applicable), and signature ofmedical director and date signed; certifica-tion by the medical director that they areaware of the qualification requirements andthe responsibilities of an air ambulance ser-vice medical director and agree to serve asmedical director; name, address, telephonenumbers and e-mail address (if applicable) ofproposed licensee of air ambulance service;
CODE OF STATE REGULATIONS 15ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

name of licensee’s chief executive officer; allambulance service licensure and relatedadministrative licensure actions taken againstthe ambulance service or owner by any stateagency in any state; and certification by theapplicant that the application contains nomisrepresentations or falsifications and thatthe information given by them is true andcomplete to the best of their knowledge, andthat the ambulance service has both the inten-tion and the ability to comply with the regu-lations promulgated under the Comprehen-sive Emergency Medical Service SystemsAct, Chapter 190, RSMo Supp. 1998.
(C) Each air ambulance service that meetsthe requirements and standards of the statuteand regulations shall be licensed and reli-censed for a period of five (5) years. Airambulances based inside or outside Missourithat do intra-Missouri transports shall belicensed in the state of Missouri and shall beheld to the same standards.
(D) Air ambulance services which are cur-rently accredited by the Commission on Ac-creditation of Medical Transportation Ser-vices (CAMTS) and have the required liabili-ty insurance coverage shall be considered tobe compliant with the rules for air ambulanceservices. Accredited air ambulance servicesshall attach to their application evidence ofaccreditation and proof of their liability insur-ance coverage. The Bureau of EMS shall con-duct periodic site reviews and inspections ofapplicable records and medical equipment asnecessary to verify compliance.
(E) Fixed wing air ambulances shall meetthe requirements stated in this regulationexcept (2)(E), (4)(A)1., (4)(A)2., (8)(D),(8)(E), and (11).
(2) Air ambulance services shall meet the fol-lowing operation and maintenance standards:
(A) Air ambulance services shall possessor contract for a valid Federal AviationAdministration Title 14 CFR part 135Certificate and if a rotary air ambulance beauthorized to conduct helicopter air ambu-lance operations in accordance with FederalAviation Regulation part 135 and this opera-tions specification;
(B) The air ambulance service shall ensureprompt response to all requests to that servicefor emergency care twenty-four (24) hoursper day, each and every day of the year, andshall provide patients with medically neces-sary care and transportation in accordancewith that air ambulance service’s protocols;
(C) Each air ambulance program shall haveestablished information that is made availableto each emergency service in the area inwhich they operate to include the following:
1. Aircraft capabilities;
2. Appropriate utilization of air ambu-lances;
3. Education and skills of the crew; and4. Safety considerations;
(D) Public liability insurance or proof ofself-insurance, condition to pay losses anddamage caused by or resulting from the neg-ligent operation, maintenance, or use ofambulance services under the service’s oper-ating authority or for loss or damage to prop-erty or others. Documents submitted as proofof insurance shall specify the limits of cover-age and include the ambulance servicelicense number. Public liability coverage forair ambulance services which transportpatients shall meet or exceed:
1. Two hundred fifty thousand dollars($250,000) for bodily injury to, or death of,one (1) person;
2. Five hundred thousand dollars($500,000) for bodily injury to, or death of,all persons injured or killed in any one (1)accident, subject to a minimum of two hun-dred fifty thousand dollars ($250,000) perperson; and
3. One hundred thousand dollars($100,000) for loss or damage to property ofothers in one (1) accident, excluding cargo;and
(E) The aviation crew of an air ambulanceshall meet all requirements of the FederalAviation Administration Title 14 CFR part135.
(3) Each aircraft, when operated as an airambulance, shall meet the following equip-ment requirements:
(A) Documentation that each aircraft isequipped with pediatric and adult medicalsupplies and equipment as required by the airambulance service medical director for thevarious advanced life support procedures orprotocols for the patient care activities in theout-of-hospital setting to which it willrespond. Each service shall be able to pro-duce these records for inspection during nor-mal business hours;
(B) The aircraft will be equipped with allequipment to allow reliable communication,flight following and emergency locator trans-mitter; and
(C) The air ambulance service shall have apolicy and provide for the effective mainte-nance, storage, usage and replacement of itsmedical equipment, devices and medications.
(4) Each aircraft operated as an ambulanceshall meet the following staffing require-ments:
(A) Air medical staff mix shall be selectedby each air ambulance program in accordancewith the medical director’s best judgment as
to what is best for patients transported by theservice, and—
1. On scene flights there shall be at leasttwo (2) air medical crew members. The pri-mary crew member shall be a registerednurse or physician and the secondary crewmember shall be an EMT-Paramedic, regis-tered nurse or physician; and
2. On all transports other than scenes,there shall be at least two (2) air medicalcrew members, one (1) of whom will be aregistered nurse or physician, and a sec-ondary crew member who is approved by themedical director to provide critical care; and
(B) The medical flight crew members willreceive training designed by the medicaldirector and clinical registered nurse supervi-sor to provide knowledge and skills needed tocarry out advanced life support proceduresand written protocols. The unique flight andpre-hospital environment will be addressedduring training.
(5) Each air ambulance service shall maintainaccurate records and forms that include thefollowing:
(A) An air ambulance report to recordinformation on each air ambulance request;
(B) Air ambulance service license;(C) Medical director protocol and policy
authorization;(D) Equipment maintenance records; and(E) Continuing education records.
(6) Each air ambulance service shall havemedical control policies, procedures andstanding orders that have been approved bytheir medical director and clinical registerednurse supervisor—
(A) The protocols will include authoriza-tion for standing orders;
(B) The written protocols will be providedto the Bureau of EMS upon request; and
(C) The medical director will ensure theair medical personnel are provided appropri-ate training to meet standards established bythe program.
(7) Each air ambulance service shall have adesignated medical director, working underan agreement, who is trained and meets therequirements for a medical director in accor-dance with 19 CSR 30-40.303(1).
(A) Medical directors for flight programsshall also demonstrate expertise in advancedtrauma life support, advanced cardiac lifesupport, and in-flight conditions unique tothe air transport of patients.
(B) Medical directors for flight programsmust have a current and valid license to prac-tice medicine in the state of Missouri andshall also maintain staff privileges at a
16 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

Missouri licensed hospital that regularlyreceives patients from the air ambulance pro-gram.
(C) An air ambulance used for transport oftrauma patients must have a medical advisorwho is a trauma surgeon on the staff of a des-ignated trauma center that regularly receivespatients from the air ambulance program andwho will provide expertise in cooperationwith the medical director in the developmentof policies, procedures and quality improve-ment for all trauma related air ambulanceactivities.
(8) Each aircraft operated as an ambulanceshall have the capability to communicate byvoice with local hospital(s), trauma centers,and the service’s own dispatching agency.
(A) Communication specialists shall havethe training commensurate to the scope ofresponsibility in the communication center.
(B) Training shall be provided in aircraftcapabilities, operational limitations, naviga-tion and map coordination.
(C) Information pertinent to each call shallbe logged in order to retrieve complete activ-ity review reports.
(D) Communication specialists shall beresponsible for flight following based onrequirements of the program and FederalAviation Administration Title 14 CFR part135.
(E) A system shall be in place to assureemergency requests are answered, the phonecalls and radio traffic are recorded and aback-up power source is available. The sys-tem shall include means to provide the crewthe ability to communicate by voice withlocal hospitals, trauma centers, police, sher-iff and fire dispatching agencies.
(F) The hospital emergency ambulanceradio system shall not be used for flight fol-lowing.
(9) There shall be an ongoing qualityimprovement program designed to objective-ly and systematically monitor, review andevaluate the quality and appropriateness ofpatient care, pursue opportunities to improvepatient care and resolve identified problems.A safety committee shall be established andshall meet regularly to assess and evaluate thesafety aspects of the operation.
(10) Each air ambulance service shall main-tain policies and procedures that include thefollowing:
(A) Safety program, including infectioncontrol program;
(B) Communications procedures;(C) Ambulance operations procedures;
(D) Standards of clinical care (medicalprotocols);
(E) Equipment maintenance;(F) Disaster/multiple casualty protocols;
and(G) Quality improvement program.
(11) Helicopter visual flight rule programswill adhere to the ceiling and visibility stan-dards of the Federal Aviation Administrationas authorized when conducting helicopter airambulance operations in accordance withFederal Aviation Regulation part 135. Theseoperations specifications will be available forinspection by the Bureau of EMS during nor-mal business hours.
(12) Each ambulance service shall display acopy of their ambulance service license in thepatient care compartment of each ambulanceaircraft operated by the ambulance service.
AUTHORITY: sections 190.103, 190.108,190.120, 190.160, 190.165, 190.175,190.176 and 190.185, RSMo Supp. 1998.*Emergency rule filed Aug. 28, 1998, effectiveSept. 7, 1998, expired March 5, 1999.Original rule filed Sept. 1, 1998, effectiveFeb. 28, 1999.
*Original authority: 190.103, 190.108, RSMo, 1998;190.120, RSMo 1973, amended 1980, 1998; 190.160,RSMo 1973, amended 1998; 190.165, RSMo 1973,amended 1978, 1998; 190.175, RSMo 1973, amended1998; 190.176, RSMo 1998; and 190.185, RSMo 1973,amended 1989, 1993, 1995, 1998.
19 CSR 30-40.309 Application andLicensure Requirements Standards for theLicensure and Relicensure of GroundAmbulance Services
PURPOSE: This rule provides the require-ment and standards related to the licensureand relicensure of ground ambulance ser-vices.
(1) Application Requirements for GroundAmbulance Service Licensure.
(A) Each applicant for ownership of anambulance service license or relicense shallsubmit an application for licensure to theBureau of Emergency Medical Services(EMS) no less than thirty (30) days or nomore than one hundred and twenty (120) daysprior to their desired date of licensure or reli-censure.
(B) An application shall include the fol-lowing information: trade name of the ambu-lance service; location of vehicles; numberof vehicles to be operated by the ambulanceservice; name, address, telephone numbersand e-mail address (if applicable) of operator
of the ambulance service; name of manager;name, address, whether a medical doctor ordoctor of osteopathy, telephone numbers, e-mail address (if applicable), and signature ofmedical director and date signed; certifica-tion by the medical director that they areaware of the qualification requirements andthe responsibilities of an ambulance servicemedical director and agree to serve as medi-cal director; name, address, telephone num-bers and e-mail address (if applicable) ofproposed licensee of the ambulance service;name of licensee’s chief executive officer; allambulance service licensure and relatedadministrative licensure actions taken againstthe ambulance service or owner by any stateagency in any state; and certification by theapplicant that the application contains nomisrepresentations or falsifications and thatthe information given by them is true andcomplete to the best of their knowledge, andthat the ambulance service has both the inten-tion and the ability to comply with the regu-lations promulgated under the Comprehen-sive Emergency Medical Service SystemsAct, Chapter 190, RSMo Supp. 1998.
(C) Each ambulance service that meets therequirements and standards of the statute andregulations shall be licensed and relicensedfor a period of five (5) years.
(D) Ambulance services which are cur-rently accredited by the Commission onAccreditation of Ambulance Services(CAAS) or the Commission on Accreditationof Medical Transportation Services (CAMTS)and have the required liability insurance cov-erage shall be considered to be compliantwith the rules for ambulance services.Accredited ambulance services shall attach totheir application evidence of accreditationand proof of their liability insurance cover-age. The Bureau of EMS may conduct peri-odic site reviews as necessary to verify com-pliance.
(2) Each vehicle operated as an ambulanceshall meet the following vehicle design, spec-ification, operation and maintenance stan-dards:
(A) Vehicle Design and SpecificationStandards. In providing the transportation ofpatients, ambulance services shall utilize onlyvehicles specifically designed, manufacturedand equipped for use as an ambulance andwhich meet current (at date of vehicle manu-facture) U.S. Department of TransportationKKK-A-1822 specifications with exceptionsof the following:
1. Image elements (such as paint) maybe altered to the agency’s preference;
2. Variation of warning lights is allowedfor: type and color of lens, strobe lights in
CODE OF STATE REGULATIONS 17ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

lieu of halogen lights, additional warninglights beyond the U.S. Department ofTransportation KKK-A-1822 specifications;
3. Power supply and equipment in thepatient compartment may be altered to theagency’s preference; and
4. Other variations may be allowed bythe Bureau of EMS;
(B) Operational Standards.1. Ambulance services shall provide the
quantity of ambulance vehicles, medical sup-plies and personnel to meet the emergencycall volume which can be reasonably antici-pated for their ambulance service area.
2. Ambulance services which are the911 provider or the recognized emergencyprovider shall ensure prompt response to allrequests to that service for emergency careoriginating from their ambulance service areatwenty-four (24) hours per day, each andevery day of the year, and shall providepatients with medically necessary care andtransportation in accordance with that ambu-lance service’s protocols.
3. Public liability insurance or proof ofself-insurance, conditioned to pay losses anddamage caused by or resulting from the neg-ligent operation, maintenance, or use ofambulance services under the service’s oper-ating authority or for loss or damage to prop-erty of others. Documents submitted as proofof insurance shall specify the limits of cover-age and include the ambulance servicelicense number. Public liability coverage forambulance services which transport patientsin the patient compartment of a vehicle shallmeet or exceed—
A. Two hundred fifty thousand dollars($250,000) for bodily injury to, or death of,one (1) person;
B. Five hundred thousand dollars($500,000) for bodily injury to, or death of,all persons injured or killed in any one (1)accident, subject to a minimum of two hun-dred fifty thousand dollars ($250,000) perperson; and
C. One hundred thousand dollars($100,000) for loss or damage to property ofothers in one (1) accident, excluding cargo;and
(C) Maintenance Standards. The ambu-lance service shall have a policy to providefor the effective maintenance of all its ambu-lances and maintain records that demonstratecompliance with such policy.
(3) Each vehicle operated as an ambulanceshall meet the following equipment require-ments:
(A) Documentation that each vehicle isequipped with pediatric and adult medicalsupplies and equipment as required by the
ambulance service medical director for thevarious patient care activities in the out-of-hospital setting to which it will respond. Eachservice shall be able to produce these recordsfor inspection during normal business hours;and
(B) The ambulance service shall have apolicy and provide for the effective mainte-nance, storage, usage and replacement of itsmedical equipment, devices and medications.
(4) Each vehicle operated as an ambulanceshall meet the following staffing require-ments:
(A) When transporting a patient, at leastone (1) licensed EMT, registered nurse, orphysician shall be in attendance with thepatient in the patient compartment at alltimes; and
(B) When an ambulance service providesadvanced life support care under its proto-cols, the patient shall be attended by an EMT-Paramedic, registered nurse or physician.
(5) Each ambulance service shall maintainaccurate records and forms on the following:
(A) An ambulance report to record infor-mation on each emergency request for serviceand each ambulance run;
(B) Ground ambulance service license;(C) Medical director protocol and policy
authorization;(D) Vehicle maintenance records;(E) Vehicle driver education records;(F) Equipment maintenance records; and(G) Records required by other regulatory
agencies.
(6) Each ambulance service shall have a med-ical control plan that has been approved bytheir medical director and service manager.The medical control plan is that portion of themedical protocols which specifically address-es the transfer of patient care between agen-cies.
(7) Each ambulance service that providesadvanced life support services, basic life sup-port services utilizing medications (medica-tions include activated charcoal, oral glucoseand/or oxygen) or providing assistance withpatients’ medications (patient medicationsinclude a prescribed inhaler, nitroglycerinand/or epinephrine), or basic life support ser-vices performing invasive procedures includ-ing invasive airway procedures (invasive air-way procedures include esophageal or endo-tracheal intubation) shall have a designatedmedical director, working under an agree-ment, who is trained and meets the require-ments for a medical director in accordancewith 19 CSR 30-40.303.
(8) Each vehicle operated as an ambulanceshall have the capability to communicate byvoice with local hospital(s), trauma centers,and the service’s own dispatching agency.
(9) There shall be an ongoing qualityimprovement program designed to objective-ly and systematically monitor, review andevaluate the quality and appropriateness ofpatient care, pursue opportunities to improvepatient care and resolve identified problems.
(10) Each ambulance service shall maintainpolicies and procedures that include the fol-lowing:
(A) Safety program, including infectioncontrol program;
(B) Vehicle operations and driving proce-dures;
(C) Communications procedures;(D) Ambulance operations procedures;(E) Standards for clinical care (medical
protocols);(F) Vehicle and equipment maintenance;(G) Disaster/multiple casualty protocols;
and(H) Quality improvement program.
(11) Each ambulance service shall display acopy of their ambulance service license in thepatient care compartment of each ambulancevehicle operated by the ambulance service.
(12) Each ambulance service that held a validambulance vehicle license on August 28,1998, and meets all the legislative and regu-latory requirements for licensure shall beissued an initial license for a period of one tofive (1–5) years. The Bureau of EMS willdetermine the initial licensure period for eachambulance service by randomly selecting anequal number of ambulance services for eachof the five (5) periods of licensure based onthe date the application is received by theBureau of EMS.
(13) An existing ambulance service licenseemay apply for and be granted by Bureau ofEMS a reduction in their primary servicearea if they meet the following requirements:
(A) Submit a completed application forlicensure, requesting a reduction of theirambulance service area and include a detaileddescription of the affected area that will nolonger be included in their primary servicearea; and
(B) Provide written documentation of anagreement with another licensed ambulanceservice, stating the service has agreed to pro-vide ambulance service to the vacated servicearea through an expansion of their services,by either contract or mutual aid agreement orprovide public notice to residents of theaffected area.
18 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

1. Public notice to residents of theaffected area includes:
A. Publishing notice in a newspaperof the largest general circulation, that is pub-lished in the county in the area affected bythe decision to withdraw ambulance cover-age, a minimum of one (1) year in advance ofthe proposed date of discontinuation of ambu-lance services. A completed affidavit of pub-lication and an original clipping of publishednotice must accompany the application forlicensure; and
B. Providing written notice to thecounty commission of any county that as awhole or in part, will be affected by the dis-continuation of services, a minimum of one(1) year in advance of the proposed date ofdiscontinuation of ambulance services.
AUTHORITY: sections 190.103, 190.107,190.176, 190.190, RSMO 2000, 109.105,190.109, 190.120, 190.160, 190.165,190.175, 190.185, RSMo Supp. 2002.*Emergency rule filed Aug. 28, 1998, effectiveSept. 7, 1998, expired March 5, 1999.Original rule filed Sept. 1, 1998, effectiveFeb. 28, 1999. Emergency amendment filedMarch 31, 2003, effective April 14, 2003,expired Oct. 11, 2003. Amended: Filed March31, 2003, effective Sept. 30, 2003.
*Original authority: 190.103, RSMo 1998; 190.105, RSMo1973, amended 1998, 2002; 190.107, RSMo 1998;190.109, RSMo, 1998 amended 2002; 190.120, RSMo1973, amended 1980, 1998, 2002; 190.160, RSMo, 1973,amended 1998, 2002; 190.165, RSMo 1973, amended1978, 1998, 2002; 190.175, RSMo 1973, amended 1998,2002; 190.176, RSMo 1998; 190.185, RSMo 1973,amended 1989, 1993, 1995, 1998, 2002; and 190,190,RSMo 1973, amended 1998.
19 CSR 30-40.331 Application and Ac-creditation or Certification Requirementsfor Training Entities that Conduct Train-ing for First Responders, Emergency Medi-cal Dispatchers, Emergency Medical Tech-nicians-Basic and Emergency MedicalTechnicians-Paramedic
PURPOSE: This rule provides the require-ments for the application and accreditation orcertification of training entities that conductEMS-related training programs.
(1) General Requirements for Certification ofEmergency Medical Technician-Basic (EMT-B) Training Entities, Emergency MedicalTechnician-Paramedic (EMT-P) TrainingEntities, EMT-B Continuing EducationTraining Entities, and EMT-P ContinuingEducation Training Entities.
(A) Each applicant for certification as anemergency medical services (EMS) trainingentity shall make application to the Bureau ofEMS and undergo a review by Bureau ofEMS staff to determine compliance with
these rules. An application shall include:trade name of the training entity; trainingentity business address; daytime telephonenumber of the training entity; type of accred-itation applied for; name, address, telephonenumber and signature of the program direc-tor; name, address, telephone number andsignature of the medical director; and certifi-cation by the applicant that the applicationcontains no misrepresentations or falsifica-tions and that the information given by themis true and complete to the best of theirknowledge, and that the training entity hasboth the intention and the ability to complywith the regulations promulgated under theComprehensive Emergency Medical ServiceSystems Act, Chapter 190, RSMo Supp.1998.
(B) Only certified EMS training entitiesshall be authorized to conduct EMS trainingprograms. Upon receipt of an application forEMS training entity certification, the Bureauof EMS shall cause an inspection of the appli-cant to determine compliance with theserules, and such subsequent inspection as isnecessary or desirable to assure compliancewith these rules. Such inspections shall occurnot less than once every five (5) years.
(C) Each EMS training entity shall demon-strate an organizational structure that assuresresponsibility for the organization, adminis-tration, periodic review, continued develop-ment and effectiveness of all educational pro-grams conducted by the EMS training entity.The EMS training entity shall have an orga-nizational chart and job descriptions for rele-vant positions within the training entity andmake this available to Bureau of EMS per-sonnel on request.
(D) Each EMS training entity shall demon-strate adequate resources for the continuedoperation of all educational programs con-ducted. This shall be available to Bureau ofEMS personnel on request.
(E) Each EMS training entity shall have amedical director who reviews and approvesthe educational content of the program andquality of medical instruction. The medicaldirector for EMS training entities shall meetthe requirements set forth in 19 CSR 30-40.303.
(F) Each EMS training entity shall demon-strate a methodology to evaluate the need fortraining and to assure availability of effectivetraining programs.
(G) Faculty Requirements.1. Each EMS training entity shall have a
qualified faculty. Credentials of faculty shallbe available for review by the Bureau ofEMS.
A. Primary faculty (those who teachtwenty percent (20%) or more of classroom
sessions) shall meet Bureau of EMS require-ments for EMS instructors.
B. The training entity shall describequalifications and training for laboratoryinstructors, where lab instructors are used.
C. The training entity shall describequalifications and training for clinicalinstructors and field preceptors, where clini-cal instructors and field preceptors are used.
2. Qualifications for any adjunct instruc-tors such as physicians, registered nurses,paramedics, clinical specialists or expert lec-turers shall be documented and available forreview by Bureau of EMS.
(H) Physical Facilities.1. Classrooms and laboratories shall
have sufficient space to accommodate themaximum planned number of students andshall be environmentally conducive to pro-viding a quality learning environment. TheBureau of EMS may inspect classroom andlaboratory facilities to determine compliance.
2. Equipment and supplies used in theprovision of instruction shall be available andconsistent with the requirements of the cur-riculum and adequate for the volume of stu-dents enrolled.
A. The Bureau of EMS may periodi-cally inspect such equipment and supplies todetermine compliance with this requirement.
B. The EMS training entity shalldescribe how they will meet this requirementto the Bureau of EMS.
C. The EMS training entity shallassure that the equipment used in its trainingprograms is in proper working order andappropriately cleaned.
3. Training entities that conduct initialcourses of instruction shall make available toall students clearly defined and publishedpolicies and procedures. Such policies andprocedures shall include the following:
A. Admission criteria;B. Student withdrawal and refund of
tuition and/or fees policies;C. Attendance policy;D. Grading and academic criteria;E. Class cancellation policy;F. Appeal and grievance procedures;G. Examination policies;H. Health and safety procedures; andI. Certification requirements of the
National Standard of Emergency MedicalTechnicians.
(I) Program Self-Evaluation.1. Each EMS training entity shall
demonstrate that the programs conductedunder its authority conduct program self-eval-uation. Such evaluation shall include:
A. Evaluation of students shall beconducted and documented on a recurringbasis and with sufficient frequency to provide
CODE OF STATE REGULATIONS 19ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

both the student and program faculty withvalid and timely indicators of each student’sprogress toward and achievement of the com-petencies and objectives stated in the curricu-lum;
B. Test instruments and evaluationmethods shall undergo periodic reviews byappropriate training entity staff and medicaldirector; and
C. Evaluation of the program by thestudents shall be documented and reviewedby the appropriate training entity staff andmedical director.
(J) Record Keeping and Reporting.1. Records shall be maintained for each
student that demonstrate all attendance, clin-ical, practical and written examinationrecords.
2. Records shall be maintained for eachclass session that document name of instruc-tor, title of session, beginning and endingtime of each session, and attendance at thesession.
3. Records shall be maintained for eachinitial course of instruction that documentlocation of course, primary instructor, begin-ning enrollment, drop-out rate, course failrate and number of students successfullycompleting the course.
4. Lesson plans shall be maintained foreach course offered.
5. All records shall be available forreview by Bureau of EMS and kept on file forat least five (5) years.
6. Each EMS training entity shall sub-mit to the Bureau of EMS an annual reportindicating the number, type and location ofcourses offered, the pass/fail rate for eachcourse, and the numbers of students complet-ing training. Each annual report shall containan affidavit that the principal officers andmedical director of the training entity remainthe same as the original application, or shallindicate any change.
7. Certificates of completion shall beissued by the training entity to students, at therequest of the student, after successful com-pletion of the appropriate criteria.
(K) EMS training entities may cooperateand develop satellite programs under theirapproval. In these cases, the EMS trainingentity remains responsible for assuring quali-ty EMS education and compliance withBureau of EMS rules.
(L) Upon EMS training entity approval bythe Bureau of EMS, the Bureau of EMS shallassign an accreditation number to each EMStraining entity. The EMS training entity shallreference this accreditation number on eachcourse completion letter or certificate issuedby the EMS training entity.
(2) Specific Requirements for EMS TrainingEntities Offering Initial EMT-P Courses.
(A) Only EMS training entities certified bythe Bureau of EMS to conduct initial EMT-Pcourses shall offer initial EMT-P courses.
(B) EMT-P students are only authorized toperform the skills and practice in accordancewith the national standard curriculum forEMT-P and approved by the training entitymedical director. The skills and practice per-formed by the student must be under thedirect supervision of a clinical preceptor andcannot be performed while being employed asan EMT-B.
(C) EMS training entities offering initialEMT-P courses shall also be certified to con-duct EMT-B, and/or first responder and/oremergency medical dispatcher, and/or EMScontinuing education programs. If the train-ing entity conducts these programs, the train-ing entity shall also be responsible for assur-ing compliance with the rules set forth forthose programs.
(D) Each EMT-P training entity shall havea formal affiliation with an appropriatelyaccredited university, senior college, commu-nity college, vocational school, technicalschool or an appropriately accredited medicalinstitution with dedication to educationalendeavors. This affiliation shall include thefollowing:
1. Ability for the EMT-P training pro-gram to require prerequisite post-secondaryeducational courses;
2. Responsibility by the accredited post-secondary educational institution and/ormedical institution over the educationalmethodologies used by the EMT-P trainingprogram; and
3. Access by the EMT-P training pro-gram into remedial education as may be nec-essary for the EMT-P training program.
(E) Each EMT-P training program shallhave a designated program director. EachEMT-P course shall have a designated leadinstructor.
(F) Each EMT-P training program shalldemonstrate and document that the EMT-Pcourses taught under its authority meet orexceed the requirements of the national stan-dard curriculum for EMT-P training.
(G) Training entities that provide EMT-Pprograms shall regularly assess the effective-ness of the training program.
(H) Clinical Requirements.1. Each EMS training entity that pro-
vides EMT-P programs shall document anddemonstrate a supervised clinical experiencefor all students.
2. Clinical affiliations shall be estab-lished and confirmed in current written affil-iation agreements with institutions and agen-
cies that provide clinical experience underappropriate medical direction and clinicalsupervision.
3. Students shall be assigned in clinicalsettings where experiences are clinically andeducationally effective in achieving the pro-gram’s objectives.
4. When participating in clinicals, stu-dents will be clearly identified by name andstudent status using nameplate, uniform, orother apparent means to distinguish themfrom other personnel.
5. Field internship shall occur only inassociation with an Advanced Life Supportambulance service which demonstrates medi-cal accountability and employs preceptorswho meet the training entity requirements.
6. The Bureau of EMS will establishminimum standards for clinical experiencesin accordance with current clinical recom-mendations of the national standard curricu-lum for EMT-P training.
(I) Examination Requirements.1. Each EMT-P training entity shall
ensure that graduating students meet entrylevel competence through the use of a finalwritten and practical examination adminis-tered by that training entity.
2. Exam scores for all students shall bemaintained and be made available for reviewby the Bureau of EMS staff.
3. The Bureau of EMS may review theoverall pass rates for these examinations topass rates for examination for licensure (theappropriate National Registry examination).Repeated and disparate differences in theserates from state averages may be ground forreview, recommendation or action by theBureau of EMS on the training entity accred-itation.
(J) Training entities which are currentlyaccredited by the Commission on Accredita-tion of Allied Health Education Programs(CAAHEP) shall be considered to be compli-ant with the rules for training entities thatconduct EMT-Paramedic programs. JointReview Committee accredited programs shallattach to their application evidence of accred-itation. The Bureau of EMS may conductperiodic site reviews as necessary to verifycompliance.
(3) Specific Requirements for EMS TrainingEntities Offering Initial EMT-B Courses.
(A) Only EMS training entities certified bythe Bureau of EMS to conduct initial EMT-Bcourses shall offer initial EMT-B courses.
(B) EMS training entities offering initialEMT-B courses shall also be certified to con-duct first responder, emergency medical dis-patcher, and EMS continuing education pro-grams. If the training entity conducts these
20 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

programs, the training entity shall also beresponsible for assuring compliance with therules set forth for those programs.
(C) Each EMT-B training program shallhave a designated program director. EachEMT-B course shall have a designated leadinstructor.
(D) Each EMT-B training program shalldemonstrate and document that the EMT-Bcourses taught under its authority meet orexceed the requirements of the national stan-dard curriculum for EMT-B training, exceptfor endotracheal intubation which shall not betaught.
(E) Clinical Requirements.1. Each EMS training entity that pro-
vides EMT-B programs shall document anddemonstrate a supervised clinical experiencefor all students.
2. Clinical affiliations shall be estab-lished and confirmed in current written affil-iation agreements with institutions and agen-cies that provide clinical experience underappropriate medical direction and clinicalsupervision.
3. Students shall be assigned in clinicalsettings where experiences are clinically andeducationally effective in achieving the pro-gram’s objectives.
4. When participating in clinicals, stu-dents will be clearly identified by name andstudent status using nameplate, uniform, orother apparent means to distinguish themfrom other personnel.
5. The Bureau of EMS will establishminimum standards for clinical experiencesin accordance with current clinical recom-mendations of the national standard curricu-lum for EMT-B training.
(F) Examination Requirements.1. Each EMT-B training entity shall
ensure that graduating students meet entrylevel competence through the use of a finalwritten and practical examination adminis-tered by that training entity.
2. Exam scores for all students shall bemaintained and be made available for reviewby the Bureau of EMS staff.
3. The Bureau of EMS may review theoverall pass rate for these examinations topass rates for examination for licensure (theappropriate National Registry examination).Repeated and disparate differences in theserates from state averages may be grounds forreview, recommendation or action by theBureau of EMS on the training entity accred-itation.
(4) Specific Requirements for EMS TrainingEntities Offering EMS Continuing Educationfor EMT-B and EMT-P.
(A) EMS training entities offering EMScontinuing education shall be certified to con-duct EMT continuing education and/or firstresponder and/or emergency medical dis-patcher training. If the training entity con-ducts these programs, the training entity shallalso be responsible for assuring complianceto the rules set forth for those programs.
(B) Each EMS continuing education train-ing entity shall have a designated programdirector.
(C) In order for EMS training entities toassign continuing education unit credit for aprogram, the topic must be related to theappropriate national standard curriculum.Improper assignment of continuing educationunits may be grounds for action upon thetraining entity accreditation.
(D) EMS training entities that provide con-tinuing education shall assign continuing edu-cation units according to the formula of fifty(50) minutes training time equals one (1) con-tinuing education unit.
(E) When possible, programs shall beawarded continuing education units accordingto recommendations of the National Registryof EMTs or the Continuing Education Co-ordinating Board for Emergency MedicalServices (CECBEMS).
(F) EMS training entities that provide con-tinuing education may assign continuing edu-cation units for instruction of EMS programsaccording to the formula of fifty (50) minutestraining time equals one (1) continuing edu-cation unit for programs taught at theprovider’s level of licensure or higher.
(G) Accreditation of continuing educationby appropriate recognized national accredit-ing bodies shall constitute approval underBureau of EMS rules.
(5) Specific Requirements for EMS TrainingEntities Offering Emergency MedicalDispatcher Training.
(A) Each training entity offering emergen-cy medical dispatcher training shall demon-strate and document that the emergency med-ical dispatcher courses taught under itsauthority meet or exceed the requirements ofa national standard curriculum for emergencymedical dispatcher training.
(B) Each training entity shall comply withsubsections (1)(A) and (1)(B).
(C) Each training entity shall ensure thatgraduating students meet entry level compe-tence through the use of a final written exam-ination administered by that training entity.
(6) Specific Requirements for EMS TrainingEntities Offering First Responder Training.
(A) Each training entity offering firstresponder training shall demonstrate and doc-
ument that the first responder courses taughtunder its authority meet or exceed therequirements of a national standard curricu-lum for first responder training.
(B) Each training entity shall comply withsubsections (1)(A) and (1)(B).
(C) Each training entity shall ensure thatgraduating students meet entry level compe-tence through the use of a final written andpractical examination administered by thattraining entity.
(7) EMT-B and EMT-P Core ContinuingEducation Requirements.
(A) EMS training entities may offer EMT-B and/or EMT-P core continuing educationprograms by offering a stand-alone program,by attending appropriate sessions of an initialtraining program or through a continuingeducation format.
(B) EMT-B and/or EMT-P core continuingeducation programs shall include a final ormodular evaluation.
(C) The Bureau of EMS will promulgatestandards for offering EMT-B core continu-ing education programs through a continuingeducation format.
(D) The Bureau of EMS will promulgatestandards for offering EMT-P core continuingeducation programs through a continuingeducation format.
(8) Primary Instructor Qualifications.(A) The Bureau of EMS may authorize as
primary instructors for EMS training pro-grams those who can document the follow-ing:
1. Clinical expertise which meets thefollowing:
A. Current licensure and at least two(2) years clinical experience in the level ofcertification instructed or higher; or
B. Credentials as a subject matterexpert as approved by the training entity’smedical director;
2. Instructor training which meets thefollowing:
A. Successful completion of aninstructor training program that meets orexceeds the United States Department ofTransportation EMS instructor curriculum;or
B. Current certification as a MissouriFire Service Instructor I; or
C. Successful completion of a coursefrom an appropriately accredited post-sec-ondary educational institution that is at leastthree (3) credit hours on educational method-ology;
3. EMS instructional experience whichmeets the following:
CODE OF STATE REGULATIONS 21ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40
A. Experience as an AdvancedCardiac Life Support, Basic Cardiac LifeSupport, Basic Trauma Life Support, Pre-Hospital Trauma Life Support, or PediatricAdvanced Life Support instructor; or
B. Experience as a laboratory or guestinstructor with an EMS training entity;
4. Continuing education in instructionaltopics of at least twenty (20) hours over thepast five (5) years; and
5. Competent in adult education theoryand clinical competency consistent with thelevel of curricula that they intend to teach.
AUTHORITY: sections 190.103, 190.131 and190.185, RSMo Supp. 1998.* Emergencyrule filed Aug. 28, 1998, effective Sept. 7,1998, expired March 5, 1999. Original rulefiled Sept. 1, 1998, effective Feb. 28, 1999.
*Original authority: 190.103 and 190.131, RSMo 1998and 190.185, RSMo 1973, amended 1989, 1993, 1995,1998.
19 CSR 30-40.333 Application andLicensure Requirements for the Licensureand Relicensure of Emergency MedicalResponse Agencies That Provide AdvancedLife Support
PURPOSE: This rule provides the require-ment and standards related to the licensureand relicensure of emergency medicalresponse agencies.
(1) Application Requirements for EmergencyMedical Response Agency Licensure.
(A) Each applicant for an emergency med-ical response agency license or relicense shallsubmit an application for licensure to theBureau of Emergency Medical Services(EMS) no less than thirty (30) days or nomore than one hundred twenty (120) daysprior to their desired date of licensure or reli-censure.
(B) An application shall include the fol-lowing information: trade name of the emer-gency medical response agency; location ofvehicles; name, address, telephone numbersand e-mail address (if applicable) of operatorof the emergency medical response agency;name of manager; name, address, whether amedical doctor or doctor of osteopathy, tele-phone numbers, e-mail address (if applica-ble), and signature of medical director anddate signed; certification by the medicaldirector that they are aware of the qualifica-tion requirements and the responsibilities ofan emergency medical response agency med-ical director and agree to serve as medicaldirector; name, address, telephone numbersand e-mail address (if applicable) of proposed
licensee of the emergency medical responseagency; name of licensee’s chief executiveofficer; all emergency medical response agen-cy licensure and related administrative licen-sure actions taken against the emergencymedical response agency or owner by anystate agency in any state; and certification bythe applicant that the application contains nomisrepresentations or falsifications and thatthe information given by them is true andcomplete to the best of their knowledge, andthat the emergency medical response agencyhas both the intention and the ability to com-ply with the regulations promulgated underthe Comprehensive Emergency MedicalService Systems Act, Chapter 190, RSMoSupp. 1998.
(C) Each emergency medical responseagency that meets the requirements and stan-dards of the statute and regulations shall belicensed and relicensed for a period of five(5) years.
(D) A political subdivision or corporationthat is licensed as an ambulance service can-not be licensed as an emergency medicalresponse agency.
(2) Operational Standards.(A) Emergency medical response agencies
shall ensure prompt response to all requeststo that service for emergency care originatingfrom their service area, in accordance with amemorandum of understanding with the localambulance services.
(B) In accordance with the memorandumof understanding with local ambulance ser-vices, emergency medical response agenciesshall provide services, personnel and suppliesto meet the emergency call volume which canbe reasonably anticipated.
(C) The emergency medical response agen-cy shall have a policy and provide for theeffective maintenance, storage, usage andreplacement of its medical equipment,devices and medications.
(3) Each emergency medical response agencyshall maintain accurate records and formsthat include the following:
(A) A report to record information on eachemergency medical call;
(B) Medical director protocol and policyauthorization;
(C) Equipment maintenance records; and(D) Records required by other regulatory
agencies.
(4) Each emergency medical response agen-cy shall have a medical control plan that hasbeen approved by their medical director andagency manager. The medical control plan isthat portion of the medical protocols which
specifically addresses the transfer of patientcare between agencies.
(5) Each emergency medical response agencythat provides advanced life support shall havea designated medical director, working underan agreement, who is trained and meets therequirements for a medical director in accor-dance with 19 CSR 30-40.303.
(6) Each emergency medical response agencyshall have the capability to communicate byvoice with the agency’s own dispatchingagency and when possible, local hospital(s),trauma centers, and local ambulance ser-vices.
(7) Each emergency medical response agencyshall have a memorandum of understandingwith each ambulance service that is a 911provider or recognized emergency provider inareas not covered by 911 ambulance servicesin the agency’s jurisdictional boundaries andwill include the following:
(A) Triage protocols;(B) Do-not-resuscitate requests;(C) Air utilization requests;(D) Medical and trauma treatment proto-
cols;(E) Quality assurance and improvement
program; and(F) Response capabilities of the emergency
medical response agency.
(8) There shall be an ongoing qualityimprovement program designed to objective-ly and systematically monitor, review andevaluate the quality and appropriateness ofpatient care, pursue opportunities to improvepatient care and resolve identified problems.
(9) Each emergency medical response agencyshall maintain policies and procedures thatinclude the following:
(A) Safety program, including infectioncontrol program;
(B) Communications procedures;(C) Standards of clinical care (medical pro-
tocols);(D) Equipment maintenance;(E) Disaster/multiple casualty protocols;
and(F) Quality improvement program.
AUTHORITY: sections 190.103, 190.133,190.160, 190.165, 190.175, 190.176 and190.185, RSMo Supp. 1998.* Emergencyrule filed Aug. 28, 1998, effective Sept. 7,1998, expired March 5, 1999. Original rulefiled Sept. 1, 1998, effective Feb. 28, 1999.
*Original authority: 190.103 and 190.133, RSMo 1998;190.160, RSMo 1973, amended 1998; 190.165, RSMo
22 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

1973, amended 1978, 1998; 190.175, RSMo 1973,amended 1998, 190.176, RSMo 1998; and 190.185, RSMo1973, amended 1989, 1993, 1995, 1998.
19 CSR 30-40.340 Initial EmergencyMedical Technician Licensure of MobileEmergency Medical Technicians, Ambul-ance Attendants and Ambulance Atten-dant-Drivers Who Have a License with anExpiration Date of August 28, 1998 orLater
PURPOSE: This rule provides the require-ments related to the initial emergency medicaltechnician licensure of mobile emergencymedical technicians, ambulance attendantsand ambulance attendant-drivers who have alicense with an expiration date of August 28,1998 or later.
(1) Any person who has a valid mobile emer-gency medical technician, ambulance atten-dant or ambulance attendant-driver licensewith an expiration date of August 28, 1998,or later shall be considered as holding a validinitial license as an emergency medical tech-nician in accordance with section 190.142,RSMo Supp. 1998, after August 28, 1998.
(2) Mobile emergency technicians shall beconsidered as Emergency Medical Techni-cian-Paramedics and ambulance attendantsand ambulance attendant-drivers shall be con-sidered as Emergency Medical Technician-Basics in accordance with section 190.142,RSMo Supp. 1998 after August 28, 1998.
(3) A licensee who has a valid mobile emer-gency medical technician, ambulance atten-dant or ambulance attendant-driver licensewith an expiration date of August 28, 1998 orlater shall be issued upon application areplacement license with an expiration datetwo (2) years from the date of expirationshown on that license.
(4) Each application for an emergency medi-cal technician (EMT) replacement licenseand two (2)-year extension shall include thefollowing: current Missouri EmergencyMedical Services (EMS) license number andexpiration date; applicant’s name, address,date of birth, sex, daytime telephone number,e-mail address (if applicable), and SocialSecurity number; applicant’s signature; and aphotocopy of the applicant’s current license.
AUTHORITY: sections 190.142 and 190.185,RSMo Supp. 1998.* Emergency rule filedAug. 28, 1998, effective Sept. 7, 1998,expired March 5, 1999. Original rule filedSept. 1, 1998, effective Feb. 28, 1999.
*Original authority: 190.142, RSMo 1998 and 190.185,RSMo 1973, amended 1989, 1993, 1995, 1998.
19 CSR 30-40.342 Application andLicensure Requirements for the InitialLicensure and Relicensure of EmergencyMedical Technician-Basics and EmergencyMedical Technician-Paramedics
PURPOSE: This rule provides the require-ments related to the initial licensure and reli-censure of EMT-Basics and EMT-Para-medics.
(1) Application Requirements for EmergencyMedical Technician (EMT) Licensure.
(A) Each applicant for licensure or relicen-sure as an EMT-Basic or EMT-Paramedicshall submit an application for licensure tothe Bureau of Emergency Medical Services(EMS). An applicant for relicensure mustsubmit their application no less than thirty(30) days or no more than one hundred twen-ty (120) days prior to the expiration date oftheir current license.
(B) An application shall include the fol-lowing information: whether an initial licen-sure or relicensure application; if previouslylicensed, their license number and expirationdate; type of license applied for (EMT-Basicor EMT-Paramedic); type of certification oreducation used for licensure or relicensure;applicant’s name, signature, address, date ofbirth, sex, daytime telephone number, e-mailaddress (if applicable), and Social Securitynumber; if applicable, type of present prima-ry EMS affiliation; prior administrativelicensure actions taken against their EMTlicense in Missouri or any other state;whether they have been, during the past five(5) years, finally adjudicated and foundguilty, or entered a plea of guilty or nolo con-tendere, in a criminal prosecution under thelaws of any state or of the United States,whether or not they received a suspendedimposition of sentence for any criminaloffense; if the answer is yes to the precedingstatement they must attach to their applica-tion a certified copy of all charging docu-ments (such as complaints, informations orindictments), judgements and sentencinginformation and any other information theywish considered; certification by the appli-cant that they have the ability to speak, readand write the English language; certificationby the applicant that they do not have a phys-ical or mental impairment which would sub-stantially limit their ability to perform theessential functions of an emergency medicaltechnician position with or without a reason-able accommodation; certification by theapplicant that if relicensing using continuing
education that they have successfully com-pleted the required continuing education inaccordance with state regulations, haveattached a list of these continuing educationunits, and are in possession of documents ofthe required continuing education, and willmake all records available to the Bureau ofEMS upon request under penalty of licenseaction up to and including revocation; certifi-cation by the applicant that the applicationcontains no misrepresentations or falsifica-tions and that the information given by themis true and complete to the best of theirknowledge; certification by the applicant thatthey have the intention and the ability to com-ply with the regulations promulgated underthe Comprehensive Emergency MedicalServices Systems Act, Chapter 190, RSMoSupp. 1998; and certification by the applicantthat they have been a resident of Missouri forfive (5) consecutive years prior to the date ontheir application or have attached to the appli-cation at least two (2) completed fingerprintcards supplied by the Bureau of EMS.
(C) All applicants shall provide theirSocial Security number on their applicationso the Bureau of EMS can perform criminalhistory checks to determine the recency andrelatedness of any criminal convictions priorto the licensure or relicensure of the appli-cant. Criminal history checks that the Bureauof EMS finds not to be relevant to the licen-sure or relicensure of an EMT will not bemaintained in the applicant’s file.
(D) All applicants shall attach to the appli-cation a list of the qualifying continuing edu-cation used for relicensure, as applicable.This list shall include verification by theapplicant’s training officer or medical direc-tor that all core requirements have been met.Receipt of this list does not constituteapproval of continuing education by theBureau of EMS.
(E) An applicant shall provide all informa-tion and certification required on the Bureauof EMS application for EMT licensure.Incomplete or inaccurate information on anapplication shall be cause to deny or takeaction upon a license.
(2) EMT-Basic (EMT-B) Licensure and Re-licensure Requirements.
(A) EMT-Basic (Initial Licensure). Initiallicensure requirements apply to any personwho was not licensed in Missouri prior toAugust 28, 1998, as an attendant or atten-dant-driver by the Bureau of EMS or whoseMissouri license has expired for more thantwo (2) years. The applicant for initial licen-sure shall submit with their license applica-tion to the Bureau of EMS evidence of cur-rent certification with the National Registry
CODE OF STATE REGULATIONS 23ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

of EMTs as an EMT-B, EMT-Intermediate orEMT-Paramedic (EMT-P).
(B) EMT-Basic (Relicensure or Step Downfrom EMT-P).
1. The applicant for relicensure shallsubmit with their license application to theBureau of EMS evidence of current certifica-tion with the National Registry of EMTs as anEMT-Basic, EMT-Intermediate or EMT-Paramedic; or
2. An applicant shall certify to theBureau of EMS:
A. That they have successfully com-pleted one hundred (100) hours of continuingeducation which meet Bureau of EMSapproval criteria under 19 CSR 30-40.331,forty-eight (48) hours of which cover all ele-ments of the EMT-B core continuing educa-tion curriculum and fifty-two (52) hours ofwhich may be elective topics from the EMT-B or EMT-P curriculum;
B. That they are able to produce doc-umentation of the required continuing educa-tion, and will make all records available tothe Bureau of EMS upon request. Licenseesshall maintain such records for a period offive (5) years after the date of relicensure.Failure to obtain and retain complete andaccurate documentation shall be cause fortaking action upon a license; and
C. That they have current basic car-diac life support training (does not counttowards core continuing education curricu-lum).
(3) EMT-Paramedic Licensure and Relicen-sure Requirements.
(A) EMT-Paramedic (Initial Licensure).Initial licensure requirements apply to anyperson who was not licensed in Missouriprior to August 28, 1998 as a mobile emer-gency medical technician by the Bureau ofEMS or whose Missouri license has expiredfor more than two (2) years. The applicant forinitial licensure shall submit with theirlicense application to the Bureau of EMS evi-dence of current certification with theNational Registry of EMTs as an EMT-P.
(B) EMT-Paramedic (Relicensure).1. The applicant for relicensure shall
submit with their license application to theBureau of EMS evidence of current certifica-tion with the National Registry of EMTs as anEMT-P; or
2. An applicant shall certify to theBureau of EMS:
A. That they have successfully com-pleted one hundred and forty-four (144)hours of continuing education which meetBureau of EMS approval criteria under 19CSR 30-40.331, forty-eight (48) hours ofwhich may be elective topics and the remain-
ing ninety-six (96) hours covering all ele-ments of the EMT-P core continuing educa-tion curriculum;
B. That they are able to produce doc-umentation of the required continuing educa-tion, and will make all records available tothe Bureau of EMS upon request. Licenseesshall maintain such records for a period offive (5) years after the date of relicensure.Failure to obtain and retain complete andaccurate documentation shall be cause fortaking action upon a license; and
C. That they have current advancedcardiac life support training (can be countedtowards the refresher requirement).
(4) The Bureau of EMS may select one (1) ormore qualified providers to administer thepractical licensure examination for EMT-Bsand EMT-Ps. The provider shall—
(A) Meet all the requirements of theNational Registry of EMTs;
(B) Make application to the Bureau ofEMS that—
1. Demonstrates necessary expertise,experience and resources needed in adminis-tering EMT practical examinations; and
2. Demonstrates evidence of practicalexaminer training and credentialling;
(C) Operate all tests in accordance with thepolicies and procedures of the NationalRegistry of EMTs and the Bureau of EMS.
AUTHORITY: sections 190.142, 190.160,190.165 and 190.185, RSMo Supp. 1998.*Emergency rule filed Aug. 28, 1998, effectiveSept. 7, 1998, expired March 5, 1999.Original rule filed Sept. 1, 1998, effectiveFeb. 28, 1999.
*Original authority: 190.142, RSMo 1998; 190.160,RSMo 1973, amended 1998; 190.165, RSMo 1973,amended 1998; and 190.185, RSMo 1973, amended 1989,1993, 1995, 1998.
19 CSR 30-40.365 Reasons and Methodsthe Department Can Use to Take Admini-strative Licensure Actions
PURPOSE: This rule provides the reasonsand methods the state can use to take admin-istrative licensure actions.
(1) The department may refuse to issue or maydeny renewal of any certificate, permit orlicense required pursuant to the comprehen-sive emergency medical services systems actfor failure to comply with the provisions of thecomprehensive emergency medical servicessystems act or for any cause listed in section(2) below. The department shall notify theapplicant in writing of the reasons for therefusal or denial and shall advise the appli-
cant of his or her right to file a complaintwith the Administrative Hearing Commissionas provided by Chapter 621, RSMo.
(2) The department may cause a complaint tobe filed with the Administrative HearingCommission as provided by Chapter 621,RSMo, against any holder of any certificate,permit or license required by the comprehen-sive emergency medical services systems actor any person who has failed to renew or hassurrendered his or her certificate, permit orlicense for failure to comply with the provi-sions of the comprehensive emergency medi-cal services systems act or for any of the fol-lowing reasons:
(A) Use or unlawful possession of any con-trolled substance, as defined in Chapter 195,RSMo, or alcoholic beverage to an extent thatsuch use impairs a person’s ability to performthe work of any activity licensed or regulatedby the comprehensive emergency medicalservices systems act;
(B) Being finally adjudicated and foundguilty, or having entered a plea of guilty ornolo contendere, in a criminal prosecutionunder the laws of any state or of the UnitedStates, for any offense reasonably related tothe qualifications, functions or duties of anyactivity licensed or regulated pursuant to thecomprehensive emergency medical servicessystems act, for any offense an essential ele-ment of which is fraud, dishonesty or an actof violence, or for any offense involvingmoral turpitude, whether or not sentence isimposed;
(C) Use of fraud, deception, misrepresen-tation or bribery in securing any certificate,permit or license issued pursuant to the com-prehensive emergency medical services sys-tems act or in obtaining permission to takeany examination given or required pursuantto the comprehensive emergency medical ser-vices systems act;
(D) Obtaining or attempting to obtain anyfee, charge, tuition or other compensation byfraud, deception or misrepresentation;
(E) Incompetency, misconduct, gross neg-ligence, fraud, misrepresentation or dishon-esty in the performance of the functions orduties of any activity licensed or regulated bythe comprehensive emergency medical ser-vices systems act;
(F) Violation of, or assisting or enablingany person to violate, any provision of thecomprehensive emergency medical servicessystems act, or of any lawful rule or regula-tion adopted by the department pursuant tothe comprehensive emergency medical ser-vices systems act;
(G) Impersonation of any person holding acertificate, permit or license or allowing any
24 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

person to use his or her certificate, permit,license or diploma from any school;
(H) Disciplinary action against the holderof a license or other right to practice anyactivity regulated by the comprehensiveemergency medical services systems actgranted by another state, territory, federalagency or country upon grounds for whichrevocation or suspension is authorized in thisstate;
(I) Being finally adjudged insane or incom-petent by a court of competent jurisdiction;
(J) Assisting or enabling any person topractice or offer to practice any activitylicensed or regulated by the comprehensiveemergency medical services systems act whois not licensed and currently eligible to prac-tice pursuant to the comprehensive emergen-cy medical services systems act;
(K) Issuance of a certificate, permit orlicense based upon a material mistake of fact;
(L) Violation of any professional trust orconfidence;
(M) Use of any advertisement or solicita-tion which is false, misleading or deceptive tothe general public or persons to whom theadvertisement or solicitation is primarilydirected; and
(N) Violation of the drug laws or rules andregulations of this state, any other state or thefederal government.
(3) The Department of Health may suspendany certificate, permit or license requiredpursuant to the comprehensive emergencymedical services systems act simultaneouslywith the filing of the complaint with theAdministrative Hearing Commission, if thedepartment finds that there is an imminentthreat to the public health. The notice of sus-pension shall include the basis of the suspen-sion and notice of the right to appeal suchsuspension. The licensee may appeal thedecision to suspend the license, certificate orpermit to the department. The appeal shallbe filed within ten (10) days from the date ofthe filing of the complaint. A hearing shallbe conducted by the department within ten(10) days from the date the appeal is filed.The suspension shall continue in effect untilthe conclusion of the proceedings, includingreview thereof, unless sooner withdrawn bythe department, dissolved by a court of com-petent jurisdiction or stayed by theAdministrative Hearing Commission.
AUTHORITY: sections 190.165 and 190.185,RSMo Supp. 1998.* Emergency rule filedJan. 14, 1999, effective Jan. 24, 1999,expired July 22, 1999. Original rule filedJan. 14, 1999, effective June 30, 1999.
*Original authority: 190.165, RSMo 1973, amended1978, 1998 and 190.185, RSMo 1973, amended 1984,1993, 1995, 1998.
19 CSR 30-40.375 Uniform Data Collec-tion System and Ambulance ReportingRequirements for Ambulance Services
PURPOSE: This rule provides the require-ments for an ambulance service to report cer-tain information on each ambulance run andto submit certain data to the department.
(1) An ambulance report or an electronicambulance reporting system shall be used byan ambulance service to record informationon each ambulance run and shall be subject toapproval by the department.
(2) A copy of all emergency life threateningruns as described in section (4) shall be sentto the department at least quarterly no laterthan thirty (30) days after the end of eachquarter.
(3) Each ambulance service shall report tothe department the total number of emergen-cy life threatening runs, emergency urgentruns, emergency dry runs, non-emergencylife threatening runs, non-emergency urgent,and non-emergency dry runs no later thanthirty (30) days after the end of each calendaryear.
(4) Each ambulance report shall include, butnot be limited to, the following information:run report number; date of run; ambulanceservice number, vehicle identification num-ber; state of pickup; county of pickup; type ofrun to scene; type of run from scene; timesdispatched, enroute, arrive scene, departscene, and arrive destination; place of inci-dent; patient destination; personnel licensenumbers; systolic blood pressure; respiratoryrate; glasgow coma score; protective equip-ment used; factors affecting emergency med-ical services (EMS); treatment authorization;trauma assessments; cause of injury; illnessassessment; destination determination;patient name, address, date of birth, race, andsex; and treatment administered. The ambu-lance service shall keep a copy of this infor-mation for at least five (5) years.
AUTHORITY: sections 190.175 and 190.185,RSMo Supp. 1998.* Emergency rule filedAug. 28, 1998, effective Sept. 7, 1998,expired March 5, 1999. Original rule filedSept. 1, 1998, effective Feb. 28, 1999.
*Original authority: 190.175, RSMo 1973; amended 1998and 190.185, RSMo 1973, amended 1989, 1993, 1995,1998.
19 CSR 30-40.410 Definitions andAbbreviations Relating to Trauma Centers
PURPOSE: This rule defines terminologyrelated to trauma centers.
(1) The following definitions and abbrevia-tions shall be used in the interpretation of therules in 19 CSR 30-40.400 to 19 CSR 30-40.450:
(A) Advanced cardiac life support (ACLS)certified means that an individual has suc-cessfully completed a course of training inadvanced cardiac life-support techniques cer-tified by the American Heart Association andthat certification is maintained;
(B) Anesthesiologist assistant (AA) meansa person who meets each of the followingconditions:
1. Has graduated from an anesthesiolo-gist assistant program accredited by theAmerican Medical Association’s Committeeon Allied Health Education and Accreditationor by its successor agency;
2. Has passed the certifying examinationadministered by the National Commission onCertification of Anesthesiologist Assistants;
3. Has active certification by theNational Commission on Certification ofAnesthesiologist Assistants;
4. Is currently licensed as an anesthesi-ologist assistant in the state of Missouri; and
5. Provides health care services delegat-ed by a licensed anesthesiologist. For the pur-poses of subsection (1)(B), the licensed anes-thesiologist shall be “immediately available”as this term is defined in section 334.400,RSMo.
(C) ATLS course means the advanced trau-ma life support course approved by theAmerican College of Surgeons whenrequired, certification shall be maintained;
(D) Bureau of EMS means the MissouriDepartment of Health and Senior Services’Bureau of Emergency Medical Services;
(E) Board-admissible means that a physi-cian has applied to a specialty board and hasreceived a ruling that s/he has fulfilled therequirements to take the examinations. Boardcertification must be obtained within five (5)years of the first appointment;
(F) Board-certified means that a physicianhas fulfilled all requirements, has satisfacto-rily completed the written and oral examina-tions, and has been awarded a board diplomain a specialty field;
(G) Certified registered nurse anesthetist(CRNA) means a registered nurse who hasgraduated from a school of nurse anesthesiaaccredited by the Council on Accreditation ofEducational Programs of Nurse Anesthesia orits predecessor and who has been certified as
CODE OF STATE REGULATIONS 25ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

a nurse anesthetist by the Council onCertification of Nurse Anesthetists;
(H) CME means continuing medical edu-cation and refers to the highest level of con-tinuing education approved by the MissouriState Medical Association, the MissouriAssociation of Osteopathic Physicians andSurgeons, The American Osteopathic As-sociation or the Accreditation Council forContinuing Medical Education;
(I) Continuing nursing education meanseducation approved or recognized by anational nurses’ organization and/or traumamedical director;
(J) Credentialed or credentialing is a hos-pital-specific system of documenting and rec-ognizing the qualifications of medical staffand nurses and authorizing the performanceof certain procedures in the hospital setting;
(K) Glasgow coma scale is a scoring sys-tem for assessing a patient’s level of con-sciousness utilizing a point system whichmeasures eye opening, verbal response andmotor response. The higher the total score,the better the patient’s neurological status;
(L) Immediately available (IA) meansbeing present at the time of the patient’sarrival at the hospital when prior notificationis possible and no more than twenty (20) min-utes from the hospital under normal drivingand weather conditions;
(M) In-house (IH) means being on the hos-pital premises twenty-four (24) hours a day;
(N) Major pediatric trauma case means apatient fifteen (15) years of age or under witha revised trauma score of 11 or less;
(O) Major trauma case is a patient with aninjury severity score of more than fifteen(15), using the scoring method described inthe article “The Injury Severity Score,”pages 187-196 of The Journal of Trauma,Vol. 14, No. 3, 1974;
(P) Major trauma patient means a traumapatient with cardiopulmonary arrest, unstableblunt or penetrating chest or abdominalinjury, airway compromise, systolic bloodpressure less than ninety (90) millimeters ofmercury, pulse less than sixty (60) or greaterthan one hundred (100) per minute with clin-ical signs of shock, severe neurologicalinjuries or signs of deteriorating neurologicalstatus, or prolonged loss of consciousness;
(Q) Missouri trauma registry is a statewidedata collection system to compile and main-tain statistics on mortality and morbidity oftrauma victims, using a reporting form pro-vided by the Missouri Department of Healthand Senior Services;
(R) Multidisciplinary trauma conferencemeans a meeting of members of the traumateam and other appropriate hospital personnel
to review the care of trauma patients at thehospital;
(S) PALS means pediatric advanced lifesupport, a course of training availablethrough the American Heart Associationwhen required, certification shall be main-tained;
(T) Physician advisory group is two (2) ormore physicians who collectively assume therole of a medical advisor;
(U) Promptly available (PA) means arrivalat the hospital within thirty (30) minutes afternotification of a patient’s arrival at the hospi-tal;
(V) R is a symbol to indicate that a stan-dard is a requirement for trauma center des-ignation at a particular level;
(W) Revised trauma score (RTS) is anumerical methodology for categorizing thephysiological status of trauma patients;
(X) Review is the inspection of hospitals todetermine compliance with the rules of thischapter. There are four (4) types of reviews:the initial review of hospitals never beforedesignated as trauma centers or hospitalsnever before reviewed for compliance withthe rules of this chapter or hospitals applyingfor a new level of trauma center designation;the verification review to evaluate the correc-tion of any deficiencies noted in a previousreview; and the validation review, which shalloccur every five (5) years to assure continuedcompliance with the rules of this chapter, anda focus review to allow review of substantialdeficiencies by a review team;
(Y) Senior resident is a physician in at leastthe third post-graduate year of study;
(Z) Severely injured patient is an injuredpatient with a glasgow coma score less thanthirteen (13) or a systolic blood pressure lessthan ninety (90) millimeters of mercury orrespirations less than ten (10) per minute ormore than twenty-nine (29) per minute;
(AA) Surgical trauma call roster is a hos-pital-specific list of surgeons assigned to trau-ma care, including date(s) of coverage andback-up surgeons;
(BB) Trauma center is a hospital that hasbeen designated in accordance with the rulesin this chapter to provide systematized medi-cal and nursing care to trauma patients. LevelI is the highest level of designation, usuallyrepresenting a large urban hospital with auniversity affiliation. Level II is the nexthighest level of designation and is usually alarge community hospital dealing with largevolumes of serious trauma in a geographicarea lacking a hospital with resources of levelI. Level III is the next level and usually rep-resents a small rural hospital with a commit-ment to trauma care that is commensuratewith limited resources;
(CC) Trauma medical director is a surgeondesignated by the hospital who is responsiblefor the trauma service and quality assuranceprograms related to trauma care;
(DD) Trauma nurse coordinator is a regis-tered nurse designated by the hospital withresponsibility for monitoring and evaluatingthe nursing care of trauma patients and thecoordination of quality assurance programsfor the trauma center;
(EE) Trauma nursing course is an educa-tion program in nursing care of traumapatients;
(FF) Trauma service is an organizationalcomponent of the hospital specializing in thecare of injured patients;
(GG) Trauma team is a team consisting ofthe emergency physician, physicians on thesurgical trauma call roster, appropriate anes-thesiology staff, nursing and other supportstaff as needed;
(HH) Trauma team activation protocol is ahospital document outlining the criteria usedto identify major trauma patients and the pro-cedures for notification of trauma team mem-bers and indicating surgical and non-surgicalspecialty response times acceptable for treat-ing major trauma patients; and
(II) Trauma triage is an estimation ofinjury severity at the scene of an accident.
AUTHORITY: sections 190.185, RSMo Supp.2006 and 190.241, RSMo 2000.* Emergencyrule filed Aug. 28, 1998, effective Sept. 7,1998, expired March 5, 1999. Original rulefiled Sept. 1, 1998, effective Feb. 28, 1999.Amended: Filed Jan. 16, 2007, effective Aug.30, 2007.
*Original authority: 190.185, RSMo 1973, amended1989, 1993, 1995, 1998, 2002 and 190.241, RSMo 1987,amended 1998.
19 CSR 30-40.420 Trauma CenterDesignation Requirements
PURPOSE: This rule establishes the require-ments for participation in Missouri’s traumacenter program.
(1) Participation in Missouri’s trauma centerprogram is voluntary and no hospital shall berequired to participate. No hospital shall inany way indicate to the public that it is a trau-ma center unless that hospital has been des-ignated as such by the Bureau of EmergencyMedical Services (EMS). Hospitals desiringtrauma center designation shall apply to theBureau of EMS. Only those hospitals foundby review to be in compliance with therequirements of the rules in this chapter shallbe designated by Bureau of EMS as traumacenters.
26 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

(2) The application required for trauma cen-ter designation shall be made upon forms pre-pared or prescribed by the Bureau of EMSand shall contain information the Bureau ofEMS deems necessary to make a fair deter-mination of eligibility for review and desig-nation in accordance with the rules of thischapter.
(A) An application shall include the fol-lowing information: designation levelrequested; name, address and telephone num-ber of hospital; name of chief executive offi-cer, chairman/president of board of trustees,surgeon in charge of trauma care, traumanurse coordinator, director of emergencymedicine, and director of trauma intensivecare; number of emergency department trau-ma caseload, trauma team activations, com-puterized tomography scan capability, mag-netic resonance imaging capability, operatingrooms, intensive care unit/critical care unitbeds, burn beds, rehabilitation beds, traumasurgeons, neurosurgeons, orthopedists, emer-gency department physicians, anesthesiolo-gists, certified registered nurse anesthetists,pediatricians, and pediatric surgeons; date ofapplication; and signatures of the chair-man/president of board of trustees, hospitalchief executive officer, surgeon in charge oftrauma, and director of emergency medicine.
(B) The Bureau of EMS shall notify thehospital of any apparent omissions or errorsin the completion of the application and shallcontact the hospital to arrange a date for thereview.
(C) Failure of a hospital to cooperate inarranging for a mutually suitable date forreview shall constitute forfeiture of applica-tion when a hospital’s initial review is pend-ing or suspension of designation when a hos-pital’s verification or validation review ispending.
(D) Hospitals designated as trauma centersunder the previous designation system shallmaintain their designation until a review isconducted using the rules of this chapter.
(3) The review of hospitals for trauma centerdesignation shall include interviews with des-ignated hospital staff, a review of the physi-cal plant and equipment, and a review ofrecords and documents as deemed necessaryto assure compliance with the requirementsof the rules of this chapter. The cost of anyand all site reviews shall be paid by eachapplicant hospital or renewing trauma centerunless adequate funding is available toBureau of EMS to pay for reviews.
(A) For the purpose of reviewing traumacenters and hospitals applying for traumacenter designation, the Bureau of EMS shalluse review teams consisting of two (2) sur-
geons, one (1) emergency physician and one(1) registered nurse who are experts in trau-ma care, experienced in trauma center reviewand disinterested politically and financially inthe hospitals to be reviewed. Out-of-statereview teams shall conduct levels I and IIreviews. In-state reviewers may conduct levelIII reviews.
(B) Any substantial deficiencies cited inthe initial review or the validation reviewregarding patient care issues, especially thoserelated to delivery of timely surgical inter-vention, shall require a focused review to beconducted. When deficiencies involve docu-mentation or policy or equipment, the hospi-tal’s plan of correction shall be submitted toBureau of EMS and verified by Bureau ofEMS personnel.
(C) The verification review shall be con-ducted in the same manner and detail as ini-tial and validation reviews. A review of thephysical plant will not be necessary unless adeficiency was cited in the physical plant inthe preceding initial or validation review. Ifdeficiencies relate only to a limited numberof areas of hospital operations, a focusedreview shall be conducted. The review teamfor a focused review shall be comprised ofreview team members with the requiredexpertise to evaluate corrections in the speci-fied deficiency area.
(D) Validation reviews shall occur everyfive (5) years. Level I and II trauma centersundergoing American College of Surgeonsreverification review at shorter intervals mayincorporate Bureau of EMS personnel inthese reviews and, if they successfully passreverification and meet all requirements here-in, submit that review for Bureau EMS rever-ification.
(E) Upon completion of a review, thereviewers shall submit a report of their find-ings to the Bureau of EMS. If this is also anAmerican College of Surgeons (ACS) verifi-cation or reverification, the hospital shallrequest a copy of the report be sent directlyto the Bureau of EMS from the ACS verifica-tion committee. The report shall statewhether the specific standards for traumacenter designation have or have not been met;if not met, in what way they were not met.The report shall include the patient chartaudits and a narrative summary to includepre-hospital, hospital, trauma service, emer-gency department, operating room, recoveryroom, clinical lab, intensive care unit, bloodbank, rehabilitation, quality improvement,education, outreach, research, chart review,and interviews. The Bureau of EMS has finalauthority to determine compliance with therules of this chapter.
(F) Within thirty (30) days after receivinga review report, the Bureau of EMS shallreturn a copy of the report in whole to thechief executive officer of the hospitalreviewed. Included with the report shall benotification indicating that the hospital hasmet the criteria for trauma center designationor has failed to meet the criteria for the des-ignation level for which it applied and optionsthe hospital may pursue.
(G) If a verification review is required, thehospital shall be allowed a period of up toeight (8) months to correct deficiencies. Aplan of correction form shall be provided bythe Bureau of EMS and shall be completed bythe hospital and returned to the Bureau ofEMS within sixty (60) days after notificationof review findings.
(H) Once a review is completed, a finalreport shall be prepared by the Bureau ofEMS. The final report shall be public recordand shall disclose the standards by which thereviews were conducted and whether the stan-dards were met. The reports filed by thereviewers shall be held confidential and shallbe disclosed only to the hospital’s chief exec-utive officer or an authorized representative.
(4) The Bureau of EMS shall have the author-ity to put on probation, suspend, revoke ordeny trauma center designation if there is rea-sonable cause to believe that there has been asubstantial failure to comply with the require-ments of the rules in this chapter. Once des-ignated as a trauma center, a hospital mayvoluntarily surrender the designation at anytime without giving cause, by contacting theBureau of EMS. In these cases, the applica-tion and review process shall be completedagain before the designation may be reinstat-ed.
(A) Trauma center designation shall bevalid for a period of five (5) years from thedate the trauma center is designated.Expiration of the designation shall occurunless the trauma center applies for valida-tion review within this five (5)-year period.
(B) The Bureau of EMS shall investigatecomplaints against trauma centers. Failure ofthe hospital to cooperate in providing docu-mentation and interviews with appropriatestaff may result in revocation of trauma cen-ter designation. Any hospital which takesadverse action toward an employee for coop-erating with the Bureau of EMS regarding acomplaint is subject to revocation of traumacenter designation.
AUTHORITY: sections 190.185 and 190.241,RSMo Supp. 1998.* Emergency rule filedAug. 28, 1998, effective Sept. 7, 1998,expired March 5, 1999. Original rule filedSept. 1, 1998, effective Feb. 28, 1999.
CODE OF STATE REGULATIONS 27ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

*Original authority: 190.185, RSMo, 1973, amended1989, 1993, 1995, 1998 and 190.241, RSMo 1987,amended 1998.
19 CSR 30-40.430 Standards for TraumaCenter Designation
PURPOSE: This rule establishes standardsfor level I, II and III trauma center designa-tion.
EDITOR’S NOTE: I-R, II-R or III-R after astandard indicates a requirement for level I,II or III trauma center respectively. I-IH,II-IH or III-IH after a standard indicates anin-house requirement for level I, II or IIItrauma center respectively. I-IA, II-IA orIII-IA indicates an immediately availablerequirement for level I, II or III trauma cen-ter respectively. I-PA, II-PA or III-PA indi-cates a promptly available requirement forlevel I, II or III trauma center respectively.
(1) General Standards for Trauma CenterDesignation.
(A) The hospital board of directors, admin-istration, medical staff and nursing staff shalldemonstrate a commitment to quality traumacare. Methods of demonstrating the commit-ment shall include, but not be limited to, aboard resolution that the hospital governingbody agrees to establish policy and proce-dures for the maintenance of services essen-tial for a trauma center; assure that all trau-ma patients will receive medical care at thelevel of the hospital’s designation; committhe institution’s financial, human and physi-cal resources as needed for the trauma pro-gram; and establish a priority admission forthe trauma patient to the full services of theinstitution. (I-R, II-R, III-R)
(B) Trauma centers shall agree to accept alltrauma victims appropriate for the level ofcare provided at the hospital, regardless ofrace, sex, creed or ability to pay. (I-R, II-R,III-R)
(C) The hospital shall demonstrate evi-dence of a trauma program that provides thetrauma team with appropriate experience tomaintain skill and proficiency in the care oftrauma patients. Such evidence shall include,meeting of continuing education unit require-ments by all professional staff, documentedregular attendance at trauma quality improve-ment meetings, documentation of continuedexperience in management of sufficient num-bers of severe trauma patients to maintainskill levels, and outcome data on quality ofpatient care.
(D) There shall be a lighted designatedhelicopter landing area at the trauma center
to accommodate incoming medical heli-copters. (I-R, II-R, III-R)
1. The landing area shall serve solely asthe receiving and take-off area for medicalhelicopters and shall be cordoned off at alltimes from the general public to assure itscontinual availability and safe operation.(I-R, II-R, III-R)
2. The landing area shall be on the hos-pital premises no more than three (3) minutesfrom the emergency room. (I-R, II-R, III-R)
(E) The hospital shall appoint a board-cer-tified surgeon to serve as the trauma medicaldirector. (I-R, II-R, III-R)
1. There shall be a job description andorganization chart depicting the relationshipbetween the trauma medical director andother services. (I-R, II-R, III-R)
2. The trauma medical director shall bea member of the surgical trauma call roster.(I-R, II-R, III-R)
3. The trauma medical director shall beresponsible for the education and training ofthe medical and nursing staff in trauma care.(I-R, II-R, III-R)
4. The trauma medical director shalldocument a minimum average of sixteen (16)hours of continuing medical education(CME) in trauma care every year. (I-R, II-R,III-R)
5. The trauma medical director shallparticipate in the trauma center’s researchand publication projects. (I-R)
(F) There shall be a trauma nurse coordi-nator. (I-R, II-R, III-R)
1. There shall be a job description andorganization chart depicting the relationshipbetween the trauma nurse coordinator andother services. (I-R, II-R, III-R)
2. The trauma nurse coordinator shalldocument a minimum average of twenty-four(24) hours of continuing nursing education intrauma care every year. (I-R, II-R, III-R)
(G) By the time of the initial review, allmembers of the surgical trauma call rostershall have successfully completed or be reg-istered for a provider Advanced Trauma LifeSupport (ATLS) course. (I-R, II-R, III-R)
(H) All members of the surgical traumacall roster and anesthesiology, neurosurgeryand orthopedic surgery shall document aminimum average of eight (8) hours of CMEin trauma care every year. In hospitals desig-nated as adult/pediatric trauma centers, anadditional six (6) hours per year of pediatrictrauma education must be maintained by trau-ma surgeons caring for pediatric patients.(I-R, II-R, III-R)
(I) The hospital shall demonstrate thatthere is adequate post-discharge follow-up ontrauma patients, including rehabilitationresults where applicable. This shall include
identification of members of the rehabilitationteam, discharge summary of trauma care tothe patient’s private physician and documen-tation in the patient’s medical record of thepost-discharge plan. (I-R, II-R, III-R)
(J) A Missouri trauma registry shall becompleted on each of the following traumapatients: any patient who is admitted and hasa length of stay of twenty-four (24) hours ormore; any patient who is transferred to oradmitted from another acute care hospital;any patient who dies in the hospital; and anypatient who is admitted to the intensive careunit (ICU) at any time during the hospitalstay. The registry form shall include the fol-lowing items: hospital identification numberand hospital medical record number; patientname and address, Social Security number,date of birth, sex and race; if minor (undereighteen (18) years) name of parent orguardian; date of injury; time of injury;external cause of injury (E code); scene ofinjury; place of injury; protective equipmentused; mode of arrival; ambulance servicenumber; ambulance report number; ambu-lance times; if transfer in, name of sendinghospital, city located, date and time patientarrived at sending hospital; date and time ofarrival in emergency department; glasgowcoma score, systolic blood pressure and res-piratory rate at arrival in the emergencydepartment; time sent to computerizedtomography (ct); time of call and arrival inemergency department of the trauma surgeonand neurosurgeon; time of discharge fromemergency department; blood alcohol con-centration (mg/dl); drugs detected as result oftoxicology test; admitting service; emergencydepartment disposition; if transferred out,name and location of receiving hospital; dateand time of arrival in operating room; oper-ating room procedures ranked by apparentseverity; final diagnoses ranked by apparentseverity; date and time admitted; date andtime discharged; total ICU days; dispositionat discharge; degree of disability and disabil-ity related to; billed hospital charges; andexpected main source of payment. The reg-istry forms for patients discharged during anyone (1) month shall be completed and sent tothe Department of Health by the last day ofthe following month. The registry may besubmitted electronically in a format definedby the Department of Health. Electronic datashall be submitted quarterly, ninety (90) daysafter the quarter ends. The trauma registrymust be current and complete. A patient logwith admission date, patient name, andinjuries must be available for use during thesite review process. Information provided byhospitals on the trauma registry shall be sub-ject to the same confidentiality requirements
28 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure
and procedures contained in section 192.067,RSMo. (I-R, II-R, III-R)
(K) The hospital shall have a trauma teamactivation protocol that establishes the crite-ria used to rank trauma patients according tothe severity and type of injury and identifiesthe persons authorized to notify trauma teammembers when a major trauma patient is enroute or has arrived at the trauma center.(I-R, II-R, III-R)
1. The trauma team activation protocolshall provide for immediate notification andrapid response requirements for trauma teammembers when a major trauma patient is enroute to the trauma center. (I-R, II-R, III-R)
(L) The hospital shall have a plan to notifyan organ or tissue procurement organizationand cooperate in the procurement of anatom-ical gifts in accordance with the provisions insection 194.233, RSMo. (I-R, II-R, III-R)
(M) There shall be no level III trauma cen-ters designated within fifteen (15) miles ofany Missouri level I or II trauma center.Hospitals which have continually been levelIII trauma centers since January 1, 1989, andwhich are within fifteen (15) miles of aMissouri level I or II trauma center may con-tinue as level III trauma centers, providedthey continue to meet standards for level IIItrauma centers.
(2) Hospital Organization Standards forTrauma Center Designation.
(A) There shall be a delineation of privi-leges for the trauma service staff made by themedical staff credentialing committee. (I-R,II-R, III-R)
(B) All members of the surgical traumacall roster shall comply with the availabilityand response requirements in subsection(2)(D) of this rule. If not on the hospitalpremises, trauma team members who areimmediately available shall carry electronicpaging devices at all times to permit contactby the hospital and shall respond immediate-ly to a contact by the hospital. (I-R, II-R,III-R)
(C) Physicians who are board-certified orboard-admissible in the following specialtiesand who are credentialed by the hospital fortrauma care shall be on the trauma centerstaff:
1. Cardiac surgery—I-R;2. General surgery—I-R, II-R, III-R;3. Neurologic surgery—I-R, II-R;4. Obstetric-gynecologic surgery—I-R,
II-R;5. Ophthalmic surgery—I-R, II-R;6. Dental surgery—I-R;7. Orthopedic surgery—I-R, II-R;8. Otorhinolaryngologic surgery—I-R,
II-R;
9. Pediatric surgery—I-R;10. Plastic, oral and maxillofacial
surgery—I-R, II-R;11. Thoracic surgery—I-R, II-R; and12. Urologic surgery—I-R, II-R.
(D) The following specialists who are cre-dentialed by the hospital for trauma care shallbe available to the patient as indicated:
1. General surgery—I-IH, II-IA, III-PA.A. The general surgery staffing
requirement may be fulfilled by senior resi-dents credentialed in general surgery, includ-ing trauma care, and capable of assessingemergent situations in general surgery.
B. The trauma surgeon shall be imme-diately available and be in attendance with thepatient when a senior surgical resident is ful-filling availability requirements;
2. Neurologic surgery—I-IH, II-IA.A. The neurologic surgery staffing
requirement may be fulfilled by a surgeonwho has been approved by the chief of neu-rosurgery for care of patients with neuraltrauma.
B. The surgeon shall be capable ofinitiating measures toward stabilizing thepatient and performing diagnostic proce-dures.
3. Cardiac surgery—I-PA;4. Obstetric-gynecologic surgery—I-PA,
II-PA;5. Ophthalmic surgery—I-PA, II-PA;6. Orthopedic surgery—I-PA, II-PA;7. Otorhinolaryngologic surgery—I-PA,
II-PA;8. Pediatric surgery—I-PA;9. Plastic and maxillofacial surgery—
I-PA, II-PA;10. Thoracic surgery—I-PA, II-PA;11. Urologic surgery—I-PA, II-PA;12. Emergency medicine—I-IH, II-IH,
III-IH;13. Anesthesiology—I-IH, II-IA, III-PA.
A. In a level I or II trauma center,anesthesiology staffing requirements may befulfilled by anesthesiology residents capableof assessing emergent situations in traumapatients and of providing any indicated treat-ment. When anesthesiology residents areused to fulfill availability requirements, thestaff anesthesiologist on call will be advisedand promptly available.
B. In a level II trauma center, anes-thesiology staffing requirements may be ful-filled when the staff anesthesiologist ispromptly available and an in-house certifiedregistered nurse anesthetist (CRNA) capableof assessing emergent situations in traumapatients and of initiating and providing anyindicated treatment is available.
C. In a level III trauma center, anes-thesiology requirements may be fulfilled by
either a CRNA with physician supervision oran anesthesiologist assistant with anesthesiol-ogist supervision in accordance with sections334.400 to 334.430, RSMo;
14. Cardiology—I-PA, II-PA;15. Chest medicine—I-PA;16. Gastroenterology—I-PA;17. Hematology—I-PA, II-PA;18. Infectious diseases—I-PA;19. Internal medicine—I-PA, II-PA,
III-PA;20. Nephrology—I-PA, II-PA;21. Pathology—I-PA, II-PA;22. Pediatrics—I-PA, II-PA;23. Psychiatry—I-PA, II-PA; and24. Radiology—I-PA, II-PA.
(3) Standards for Special Facilities/Re-sources/Capabilities for Trauma CenterDesignation.
(A) The hospital shall meet emergencydepartment standards for trauma center des-ignation.
1. The emergency department staffingshall ensure immediate and appropriate careof the trauma patient. (I-R, II-R, III-R)
A. The physician director of theemergency department shall be board-certi-fied or board-admissible in emergencymedicine. (I-R, II-R)
B. There shall be a physician compe-tent in the care of the critically injured in theemergency department twenty-four (24)hours a day. (I-R, II-R, III-R)
(I) All emergency departmentphysicians shall be currently certified inATLS and advanced cardiac life support(ACLS). (I-R, II-R, III-R)
(II) The emergency departmentphysician shall be a designated member of thetrauma team, and shall document a minimumaverage of sixteen (16) hours of trauma edu-cation per year. (I-R, II-R, III-R)
C. There shall be written protocolsdefining the relationship of the emergencydepartment physicians to other physicianmembers of the trauma team. (I-R, II-R,III-R)
D. The emergency department shallemploy a trauma utilization assessment sys-tem which predicts the number of registerednurses needed to provide adequate care andresuscitation of trauma patients. There shallbe no fewer than one (1) registered nurse pershift credentialed in trauma nursing on dutyin the emergency department. (I-R, II-R,III-R)
E. All registered nurses regularlyassigned to the emergency department shallbe credentialed in trauma nursing by the hos-pital within one (1) year of assignment. (I-R,II-R, III-R)
CODE OF STATE REGULATIONS 29ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

(I) Registered nurses credentialedin trauma nursing shall document a minimumof eight (8) hours of trauma-related continu-ing nursing education per year. (I-R, II-R,III-R)
(II) By the time of the initialreview, all registered nurses assigned to theemergency department shall have successful-ly completed or be registered for a providerACLS course. (I-R, II-R, III-R)
2. Equipment for resuscitation and lifesupport for the critically or seriously injuredshall include the following:
A. Airway control and ventilationequipment including laryngoscopes, endotra-cheal tubes, bag-mask resuscitator, sources ofoxygen and mechanical ventilator, includingpediatric sizes—I-R, II-R, III-R;
B. Suction devices, including pedi-atric sizes—I-R, II-R, III-R;
C. Electrocardiograph, oscilloscopeand defibrillator, including pediatric capabil-ity—I-R, II-R, III-R;
D. Central line insertion equipment—I-R, II-R, III-R;
E. All standard intravenous fluids andadministration devices and intravenouscatheters, including pediatric sizes—I-R,II-R, III-R;
F. Sterile surgical sets for proceduresstandard for the emergency department,including pediatric sizes—I-R, II-R, III-R;
G. Gastric lavage equipment, includ-ing pediatric sizes—I-R, II-R, III-R;
H. Drugs and supplies necessary foremergency care, including pediatricdosages—I-R, II-R, III-R;
I. Two-way radio linked with emer-gency medical service (EMS) vehicles—I-R,II-R, III-R;
J. End-tidal carbon dioxide monitor—I-R, II-R, III-R and mechanical ventilators,including pediatric capability—I-R, II-R;
K. Skeletal tongs—I-R, II-R, III-R;L. Temperature control devices for
patient, parenteral fluids and blood—I-R,II-R, III-R; and
M. Rapid infusion system for par-enteral infusion—I-R, II-R, III-R.
3. There shall be documentation that allequipment is checked according to the hospi-tal preventive maintenance schedule. (I-R,II-R, III-R)
4. There shall be a designated traumaresuscitation area in the emergency depart-ment. (I-R, II-R)
5. There shall be X-ray capability withtwenty-four (24)-hour coverage by techni-cians. (I-IH, II-IH, III-IA)
6. Nursing documentation for the trau-ma patient shall be on a trauma flow sheet.(I-R, II-R, III-R)
(B) The hospital shall meet intensive careunit (ICU) standards for trauma center desig-nation.
1. There shall be a designated surgeonmedical director for the ICU. (I-R, II-R,III-R)
2. A physician who is not the emergen-cy department physician shall be on duty inthe ICU or available in-house twenty-four(24) hours a day in a level I trauma center andshall be on call and available within twenty(20) minutes in a level II trauma center.
3. The ICU shall utilize a patient classi-fication system which defines the severity ofinjury and indicates the number of registerednurses needed to staff the unit. The minimumregistered nurse/trauma patient ratio usedshall be one to two (1:2). (I-R, II-R, III-R)
4. Registered nurses shall be creden-tialed in trauma care within one (1) year ofassignment, documenting a minimum of eight(8) hours of trauma-related continuing nurs-ing education per year. (I-R, II-R, III-R)
5. Nursing care documentation shall beon a twenty-four (24)-hour patient flow sheet.(I-R, II-R, III-R)
6. At the time of the initial review, nurs-es assigned to ICU shall have successfullycompleted or be registered for a providerACLS course. (I-R, II-R, III-R)
7. There shall be beds for traumapatients or comparable care provided untilspace is available in ICU. (I-R, II-R, III-R)
8. Equipment for resuscitation and toprovide life support for the critically or seri-ously injured shall include, but not be limit-ed to:
A. Airway control and ventilationequipment including laryngoscopes, endotra-cheal tubes, bag-mask resuscitator, and amechanical ventilator, including pediatricsizes—I-R, II-R, III-R;
B. Oxygen source with concentrationcontrols—I-R, II-R, III-R;
C. Cardiac emergency cart, includingpediatric cardiac equipment and medica-tions—I-R, II-R, III-R;
D. Temporary transvenous pacemak-ers, including pediatric sizes—I-R, II-R,III-R;
E. Electrocardiograph, oscilloscopeand defibrillator, including pediatric sizes—I-R, II-R, III-R;
F. Cardiac output monitoring—I-R,II-R;
G. Electronic pressure monitoringand pulse oximetry—I-R, II-R;
H. End tidal carbon dioxide monitorand mechanical ventilators, including pedi-atric capability—I-R, II-R, III-R;
I. Patient weighing devices, includingpediatric scales—I-R, II-R, III-R;
J. Pulmonary function measuringdevices, including pediatric capability—I-R,II-R, III-R;
K. Temperature control devices foradult and pediatric patients—I-R, II-R, III-R;
L. Drugs, intravenous fluids and sup-plies for adult and pediatric patients—I-R,II-R, III-R; and
M. Intracranial pressure monitoringdevices—I-R, II-R.
9. There shall be documentation that allequipment is checked according to the hospi-tal preventive maintenance schedule. (I-R,II-R, III-R)
10. There shall be separate pediatric andadult ICUs or a combined ICU with nursestrained in pediatric intensive care. (I-R)
(C) The hospital shall meet post-anesthesiarecovery room (PAR) standards for traumacenter designation.
1. Registered nurses and other essentialpersonnel who are not on duty shall be oncall and available within twenty (20) minutes.(I-R, II-R, III-R)
2. Equipment for resuscitation and toprovide life support for the critically or seri-ously injured shall include, but not be limit-ed to:
A. Airway control and ventilationequipment including laryngoscopes, endotra-cheal tubes of all sizes, bag-mask resuscita-tor, sources of oxygen and mechanical venti-lator—I-R, II-R, III-R;
B. Suction devices—I-R, II-R, III-R;C. Electrocardiograph, oscilloscope
and defibrillator—I-R, II-R, III-R;D. Apparatus to establish central
venous pressure monitoring—I-R, II-R;E. All standard intravenous fluids
and administration devices, including intra-venous catheters—I-R, II-R, III-R;
F. Sterile surgical set for emergencyprocedures—I-R, II-R, III-R;
G. Drugs and supplies necessary foremergency care—I-R, II-R, III-R;
H. Temperature control devices forthe patient, for parenteral fluids and forblood—I-R, II-R, III-R;
I. Intracranial pressure monitoringdevices—I-R, II-R;
J. Temporary pacemaker—I-R, II-R,III-R;
K. Electronic pressure monitoring—I-R, II-R; and
L. Pulmonary function measuringdevices—I-R, II-R, III-R.
(D) The hospital shall have acutehemodialysis capability or a written transferagreement. (I-R, II-R, III-R)
(E) The hospital shall have a physi-cian-directed burn unit or a written transferagreement. (I-R, II-R, III-R)
30 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

(F) The hospital shall have injury rehabili-tation and spinal cord injury rehabilitationcapability or a written transfer agreement.(I-R, II-R, III-R)
(G) The hospital shall have pediatric trau-ma management capability or a written trans-fer agreement. (I-R, II-R, III-R)
(H) Radiological capabilities for traumacenter designation shall include:
1. Angiography of all types—I-R, II-R;2. Sonography available twenty-four
(24) hours a day with a thirty (30)-minutemaximum response time—I-R;
3. Nuclear scanning availabletwenty-four (24) hours a day with a thirty(30)-minute maximum response time—I-R;
4. Resuscitation equipment available tothe radiology department—I-R, II-R, III-R;
5. Adequate physician and nursing per-sonnel present with monitoring equipment tofully support the trauma patient and providedocumentation of care during the time thepatient is physically present in the radiologydepartment and during transportation to andfrom the radiology department—I-R, II-R,III-R;
6. In-house computerized tomography(Mobile computerized tomography services,contracts for those services with other insti-tutions or computerized tomography inremote areas of a hospital requiring trans-portation from the main hospital buildingshall not be considered in-house.)—I-R, II-R;and
7. Computerized tomography techni-cian—I-IH, II-IA.
(I) There shall be documentation of ade-quate support services in assisting thepatient’s family from the time of entry intothe facility to the time of discharge. (I-R,II-R, III-R)
(J) Medical surgical floors of a designatedtrauma center shall have the following per-sonnel and equipment:
1. Registered nurses and other essentialpersonnel on duty twenty-four (24) hours aday—I-R, II-R, III-R;
2. Equipment for resuscitation and toprovide support for the injured patient includ-ing, but not limited to:
A. Airway control and ventilationequipment including laryngoscopes, endotra-cheal tubes of all sizes, bag-mask resuscitatorand sources of oxygen—I-R, II-R, III-R;
B. Suction devices—I-R, II-R, III-R;C. Electrocardiograph, oscilloscope
and defibrillator—I-R, II-R, III-R;D. All standard intravenous fluids and
administration devices and intravenouscatheters—I-R, II-R, III-R; and
E. Drugs and supplies necessary foremergency care—I-R, II-R, III-R; and
3. Documentation that all equipment ischecked according to the hospital preventivemaintenance schedule—I-R, II-R, III-R.
(K) The operating room personnel, equip-ment and procedures of a trauma center shallinclude, but not be limited to:
1. An operating room adequately staffedin-house twenty-four (24) hours a day—I-R,II-R;
2. Equipment for resuscitation and toprovide life support for the critically or seri-ously injured, including, but not limited to:
A. Cardiopulmonary bypass capabili-ty—I-R;
B. Operating microscope—I-R;C. Thermal control equipment for
patient, parenteral fluids and blood—I-R,II-R, III-R;
D. X-ray capability—I-R, II-R,III-R;
E. Endoscopes, all varieties—I-R,II-R, III-R;
F. Instruments necessary to performan open craniotomy—I-R; II-R; and
G. Monitoring equipment—I-R,II-R, III-R;
3. Documentation that all equipment ischecked according to the hospital preventivemaintenance schedule—I-R, II-R, III-R; and
4. Documentation that any certified reg-istered nurse anesthetist (CRNA) participat-ing in care of trauma patients completes aminimum average of eight (8) hours of trau-ma-related continuing nursing educationevery year—I-R, II-R, III-R;
(L) The following clinical laboratory ser-vices shall be available twenty-four (24)hours a day:
1. Standard analyses of blood, urine andother body fluids—I-R, II-R, III-R;
2. Blood typing and cross-matching—I-R, II-R, III-R;
3. Coagulation studies—I-R, II-R, III-R;4. Comprehensive blood bank or access
to a community central blood bank and ade-quate hospital blood storage facilities—I-R,II-R, III-R;
5. Blood gases and pH determinations—I-R, II-R, III-R;
6. Serum and urine osmolality—I-R,II-R;
7. Microbiology—I-R, II-R, III-R;8. Drug and alcohol screening—I-R,
II-R, III-R; and9. A written protocol that the trauma
patient receives priority—I-R, II-R, III-R.
(4) Standards for Programs in QualityAssurance, Outreach, Public Education andTraining for Trauma Center Designation.
(A) There shall be an ongoing qualityassurance program designed to objectively
and systematically monitor, review and evalu-ate the quality and appropriateness of patientcare, pursue opportunities to improve patientcare and resolve identified problems. (I-R,II-R, III-R)
(B) The following additional quality assur-ance measures shall be required:
1. Regular reviews of all trauma-relateddeaths that are within seven (7) days ofadmission to the trauma center—I-R, II-R,III-R;
2. A regular morbidity and mortalityreview—I-R, II-R, III-R;
3. A regular multidisciplinary traumaconference that includes all members of thetrauma team, with minutes of the conferencesto include attendance, individual casesreviewed and findings—I-R, II-R, III-R;
4. Regular medical nursing audits, uti-lization reviews and tissue reviews—I-R,II-R, III-R;
5. Regular reviews of the reports gener-ated by the Department of Health from theMissouri trauma registry and the head andspinal cord injury registry—I-R, II-R, III-R;
6. Regular reviews of pre-hospital andregional systems of trauma care—I-R, II-R,III-R; and
7. In trauma centers using CRNAs tofulfill any part of the anesthesiology staffingrequirements, a separate quality assuranceprogram to assure ongoing review by thephysician(s) responsible for the anesthesiolo-gy service.
(C) An outreach program shall be estab-lished to assure twenty-four (24)-hour avail-ability of telephone consultation with physi-cians in the outlying region. (I-R)
(D) A public education program shall beestablished to promote injury prevention andstandard first aid and to resolve problemsconfronting the public, medical professionand hospitals regarding optimal care for theinjured. (I-R, II-R)
(E) The hospital shall document existing orplanned programs to increase public aware-ness of trauma prevention. These programsmay be collectively presented with other hos-pitals and organizations. (I-R, II-R)
(F) The hospital shall be actively involvedin local and regional emergency medical ser-vices systems by providing training and clini-cal resources. (I-R, II-R, III-R)
(G) There shall be a hospital-approved pro-cedure for credentialing nurses in traumacare. (I-R, II-R, III-R)
1. All nurses regularly assigned to theemergency department or ICU shall completea minimum of sixteen (16) hours of traumanursing courses to become credentialed intrauma care. (I-R, II-R, III-R)
CODE OF STATE REGULATIONS 31ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

2. The content and format of any traumanursing courses developed and offered by ahospital shall be developed in cooperationwith the trauma medical director. A copy ofthe course curriculum used shall be filed withthe Bureau of EMS. (I-R, II-R, III-R)
3. Trauma nursing courses offered byinstitutions of higher education in Missourior the Trauma Nurse Core curriculum offeredby the Emergency Nurses’ Association maybe used to fulfill this requirement. To receivecredit for this course, a nurse shall obtainadvance approval for the course from thetrauma medical director and trauma nursecoordinator and shall present evidence of sat-isfactory completion of the course. (I-R,II-R, III-R)
(H) Hospital diversion information must bemaintained to include date, length of time andreason for diversion. This must be monitoredas a part of the quality improvement processand available when the hospital is sitereviewed.
(5) Standards for the Programs in TraumaResearch for Trauma Center Designation.
(A) The hospital and its staff shall docu-ment a research program in trauma. (I-R)
(B) The hospital shall agree to cooperateand participate with the Bureau of EMS inconducting epidemiological studies and indi-vidual case studies for the purpose of devel-oping injury control and prevention pro-grams. (I-R, II-R, III-R)
AUTHORITY: sections 190.185, RSMo Supp.2006 and 190.241, RSMo 2000.* Emergencyrule filed Aug. 28, 1998, effective Sept. 7,1998, expired March 5, 1999. Original rulefiled Sept. 1, 1998, effective Feb. 28, 1999.Amended: Filed Jan. 16, 2007, effective Aug.30, 2007.
*Original authority: 190.185, RSMo 1973, amended1989, 1993, 1995, 1998, 2002 and 190.241, RSMo 1987,amended 1998.
19 CSR 30-40.440 Standards for PediatricTrauma Center Designation
PURPOSE: This rule establishes standardsfor pediatric trauma center designation.
(1) General Standards for Pediatric TraumaCenter Designation.
(A) The pediatric trauma center shall belocated in a children’s hospital or in a level Itrauma center.
(B) The hospital board of directors, admin-istration, medical staff and nursing staff shalldemonstrate a commitment to quality pedi-atric trauma care and shall treat any pediatric
trauma patient presented to the facility forcare. Methods of demonstrating the commit-ment shall include, but not be limited to, aboard resolution that the hospital governingbody agrees to establish policies and proce-dures for the maintenance of the servicesessential to a pediatric trauma center; assurethat all pediatric trauma patients will receivemedical care that meets the standards of thisrule; commit the institution’s financial,human and physical resources as needed forthe trauma program; and establish a priorityfor the pediatric trauma patient to the full ser-vices of the institution.
(C) The hospital shall demonstrate evi-dence of a pediatric trauma program that pro-vides the trauma team with appropriate expe-rience to maintain skill and proficiency in thecare of pediatric trauma patients.
(D) The hospital shall have a pediatrictrauma team activation protocol that estab-lishes the criteria used to rank trauma victimsaccording to the severity and type of injuryand identifies the persons authorized to noti-fy trauma team members when a major pedi-atric trauma patient is en route or has arrivedat the pediatric trauma center. That protocolshall provide for immediate notification andrapid response requirements for trauma teammembers.
(E) There shall be a lighted helipad on thehospital premises no more than three (3) min-utes from the emergency department.
(F) The hospital shall appoint a board-cer-tified pediatric surgeon to serve as pediatrictrauma medical director.
1. The pediatric trauma medical directorshall document a minimum average of sixteen(16) hours of trauma-related continuing med-ical education (CME) every year.
2. There shall be a job description andorganizational chart depicting the relationshipbetween the pediatric trauma program direc-tor and other services.
(G) A registered nurse shall be appointedto serve as the pediatric trauma nurse coordi-nator.
1. The pediatric trauma nurse coordina-tor shall document a minimum average oftwenty-four (24) hours of trauma-related con-tinuing nursing education every year.
2. There shall be a job description andorganization chart depicting the relationshipbetween the pediatric trauma nurse coordina-tor and other services.
(H) By the time of the initial review, pedi-atric surgeons who comprise the pediatricsurgical trauma call roster shall have success-fully completed or be registered for aprovider advanced trauma life support(ATLS) course.
(I) All members of the pediatric surgicaltrauma call roster, including anesthesiology,shall document a minimum average of eight(8) hours of trauma-related CME every year.
(J) The hospital shall be able to documentactive involvement in local and regionalemergency medical services (EMS) systems.The hospital can demonstrate involvement inthe local and regional EMS programs by par-ticipating in EMS training programs and jointeducational programs regarding the pediatricpatient; providing appropriate clinical experi-ence and EMS system quality assessment andquality assurance mechanisms; and assistingin the development of regional policies andprocedures.
(K) The hospital shall have a plan to noti-fy an organ or tissue procurement organiza-tion and cooperate in the procurement ofanatomical gifts in accordance with the pro-visions in section 194.233, RSMo.
(L) All pediatric trauma centers shall sup-port and fully participate in the Missouritrauma registry and shall belong to theMissouri poison control network.
(2) Hospital Organization Standards forPediatric Trauma Center Designation.
(A) Pediatric specialists representing thefollowing specialties shall be on staff at thecenter and shall be board-certified orboard-admissible and credentialed in traumacare: cardiac surgery, neurologic surgery,ophthalmic surgery, oral surgery-dental,orthopedic surgery, otorhinolaryngologicsurgery, pediatric surgery; plastic and max-illofacial surgery, thoracic surgery and uro-logic surgery. Obstetric and gynecologic sur-geons shall be available on a consultant basis.
(B) The emergency department staffingshall ensure immediate and appropriate careof the pediatric trauma patient. The emergen-cy department pediatrician shall be board cer-tified/eligible in pediatric medicine and shallfunction as a designated member of the pedi-atric trauma team. All emergency departmentphysicians shall have successfully completedand be current in ATLS and pediatricadvanced life support (PALS) course prior tothe initial review and shall document a mini-mum average of sixteen (16) hours of CME intrauma care every year. There shall be writ-ten protocols to clearly establish responsibil-ities and define the relationship between theemergency department pediatricians andother physician members of the pediatrictrauma team.
(C) The pediatric trauma surgeon on callshall be physically present in-housetwenty-four (24) hours a day and shall meetall major trauma patients in the emergencydepartment at the time of the patient’s arrival.
32 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure

This requirement may be fulfilled by seniorresidents in general surgery who areATLS-certified and able to deliver surgicaltreatment immediately and provide controland leadership for care of the pediatric trau-ma patient. When senior residents are used tofulfill availability requirements, the pediatrictrauma surgeon shall be immediately avail-able.
(D) A neurosurgeon shall be availablein-house and dedicated to the hospital’s pedi-atric trauma service. The neurosurgeonrequirement may be fulfilled by a surgeonexperienced in the care of pediatric patientswith neural trauma and able to deliver surgi-cal treatment immediately and provide con-trol and leadership for the care of the pedi-atric patient with neural trauma.
(E) Pediatric specialists representing thefollowing specialties shall be on call andpromptly available: cardiac surgery, micro-surgery, hand surgery, ophthalmic surgery,oral surgery-dental, orthopedic surgery,otorhinolaryngologic surgery, pediatricsurgery, plastic and maxillofacial surgery,thoracic surgery and urologic surgery.
(F) A board-certified or board-admissiblepediatrician credentialed in emergency careshall be available in the emergency depart-ment twenty-four (24) hours a day. Thisrequirement may be fulfilled by a physicianwho is board-certified or board-admissible inemergency medicine who demonstrates com-mitment by engaging in the exclusive practiceof pediatric emergency medicine a minimumof one hundred (100) hours per month or hasan additional year of training in pediatricemergency medicine.
(G) A board-certified or board-admissibleanesthesiologist credentialed in pediatric careshall be available in-house twenty-four (24)hours a day. Senior anesthesiology residentsor anesthesiologists not credentialed in pedi-atric care may fulfill the in-house require-ment if the credentialed pediatric anesthesiol-ogist is on call and promptly available.
(H) A pediatric radiologist shall bepromptly available twenty-four (24) hours aday.
(I) Pediatric specialists representing thefollowing non-surgical specialties shall be oncall and available: cardiology, chestmedicine, gastroenterology, hematology,infectious diseases, nephrology, neurology,pathology, psychiatry and neonatology.
(3) Standards for Special Facilities/Re-sources/Capabilities for Pediatric TraumaCenter Designation.
(A) Hospitals shall meet emergencydepartment standards for pediatric traumacenter designation.
1. There shall be a minimum of two (2)registered nurses per shift specializing inpediatric trauma care assigned to the emer-gency department.
A. All registered nurses regularlyassigned to pediatric care in the emergencydepartment shall document a minimum ofeight (8) hours per year of continuing nursingeducation on care of the pediatric traumapatient.
B. All registered nurses regularlyassigned to pediatric care in the emergencydepartment shall be PALS certified withinone (1) year of assignment to the unit andshall maintain a current PALS certification.
2. Respiratory therapy technicians whowork with pediatric trauma patients in theemergency department shall be experiencedin pediatric respiratory therapy techniques.
3. There shall be a designated traumaresuscitation area in the emergency depart-ment equipped for pediatric patients.Equipment to be immediately accessible forresuscitation and to provide life support forthe seriously injured pediatric patient shallinclude, but not be limited to:
A. Airway control and ventilationequipment for all size patients, includinglaryngoscopes, assorted blades, airways,endotracheal tubes and bag-mask resuscita-tor;
B. Oxygen, air and suction devices;C. Electrocardiograph, monitor and
defibrillator to include internal and externalpediatric paddles;
D. Apparatus to establish centralvenous pressure monitoring and arterial mon-itoring;
E. All standard intravenous fluids andadministration devices, including intravenouscatheters designed for delivering IV fluidsand medications at rates and in amountsappropriate for pediatric patients;
F. Sterile surgical sets for standardprocedures for the emergency department;
G. Gastric lavage equipment;H. Drugs and supplies necessary for
emergency care;I. Two-way radio linked with EMS
vehicles; J. Equipment for spinal stabilization
for all age groups; K. Temperature control devices for
patients, parenteral fluids and blood;L. Blood pressure cuffs, chest tubes,
nasogastric tubes and urinary drainage appa-ratus for the pediatric patient; and
M. Patient weighing devices.(B) The hospital shall meet radiological
capabilities for pediatric trauma center desig-nation.
1. There shall be X-ray capability withtwenty-four (24)-hour coverage by in-housetechnicians.
2. There shall be radiological capabili-ties promptly available, including general,peripheral and cerebrovascular angiography,sonography and nuclear scanning.
3. Adequate physician and nursing per-sonnel shall be present with monitoringequipment to fully support the trauma patientand provide documentation of care during thetime that the patient is physically present inthe radiology department and during trans-portation to and from the radiology depart-ment.
4. There shall be in-house computerizedtomography with a technician availablein-house twenty-four (24) hours a day.Mobile computerized tomography services,contracts for those services with other insti-tutions or computerized tomography inremote areas of a hospital requiring trans-portation from the main hospital buildingshall not be considered in-house.
5. The pediatric trauma surgeon, neuro-surgeon and emergency pediatrician shalleach have the authority to initiate computer-ized tomography.
6. There shall be a continuing review ofthe availability of computerized tomographyservices for the pediatric trauma patient.
7. There shall be adequate resuscitationequipment available to the radiology depart-ment.
(C) The hospital shall meet pediatric inten-sive care unit standards for trauma centerdesignation.
1. The medical director for the pediatricintensive care unit (PICU) shall be board-cer-tified or board-eligible in pediatric criticalcare.
2. There shall be a pediatrician or seniorpediatric resident on duty in the PICU twen-ty-four (24) hours a day or available frominside the hospital. This physician shall main-tain a current PALS certification. The physi-cian on duty in the PICU shall not be theemergency department pediatrician or theon-call trauma surgeon.
3. The PICU patient shall have nursingcare by a registered nurse who is regularlyassigned to pediatric intensive care.
4. The PICU shall utilize a patient clas-sification system which defines the severity ofinjury and indicates the number of registerednurses needed to staff the unit. The minimumregistered nurse/trauma patient ratio usedshall be one to two (1:2).
CODE OF STATE REGULATIONS 33ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40

34 CODE OF STATE REGULATIONS (7/31/07) ROBIN CARNAHAN
Secretary of State
19 CSR 30-40—DEPARTMENT OF HEALTHAND SENIOR SERVICES Division 30—Division of Regulation and Licensure
5. All registered nurses regularlyassigned to the PICU shall document a mini-mum of eight (8) hours per year of continu-ing nursing education on care of the pediatrictrauma patient.
6. Within one (1) year of assignment, allregistered nurses regularly assigned to PICUshall be PALS-certified. Registered nurses inpediatric trauma centers designated beforeJanuary 1, 1989 shall have successfully com-pleted or be registered for a PALS course byJanuary 1, 1991.
7. There shall be immediate access toclinical laboratory services.
8. Equipment to be immediately acces-sible for resuscitation and life support forseriously injured pediatric patients shallinclude, but not be limited to:
A. Airway control and ventilationequipment for all size patients includinglaryngoscopes, assorted blades, endotrachealtubes, bag-mask resuscitator and mechanicalventilator;
B. Oxygen and suction devices; C. Electrocardiograph, monitor and
defibrillator, including internal and externalpediatric paddles;
D. Apparatus to establish invasivehemodynamic monitoring, end tidal carbondioxide monitoring and pulse oximetry;
E. All standard intravenous fluids andadministration devices, including intravenouscatheters designed for delivering IV fluidsand medications at rates and in amountsappropriate for pediatric patients;
F. Gastric lavage equipment;G. Drugs and supplies necessary for
emergency care;H. Temporary transvenous pacemak-
er;I. Patient weighing devices;J. Cardiac output monitoring devices; K. Pulmonary function measuring
devices;L. Temperature control devices for
the patient, parenteral fluids and blood;M. Intracranial pressure monitoring
devices; N. Appropriate emergency surgical
trays; and O. Blood pressure cuffs, chest tubes,
nasogastric tubes and urinary drainage appa-ratus for the pediatric patient.
(D) The hospital shall meet post-anesthesiarecovery room (PAR) standards for pediatrictrauma center designation. Unless the hospi-tal uses PICU to recover pediatric traumapatients, the following PAR standards apply:
1. The post-anesthesia recovery roomshall be staffed with registered nurses regu-larly assigned to pediatric care and other
essential personnel on call and availabletwenty-four (24) hours a day; and
2. Equipment to be accessible for resus-citation and life support for the seriouslyinjured pediatric patient shall include, but notbe limited to:
A. Airway control and ventilationequipment for all size patients includinglaryngoscopes, assorted blades, airways,endotracheal tubes and bag-mask resuscita-tor;
B. Oxygen and suction devices; C. Electrocardiograph, monitor and
defibrillator, including internal and externalpediatric paddles;
D. Apparatus to establish and main-tain hemodynamic monitoring;
E. All standard intravenous fluids andadministration devices, including intravenouscatheters designed for delivering IV fluidsand medications at rates and in amountsappropriate for pediatric patients;
F. Sterile surgical sets for emergencyprocedures;
G. Drugs and supplies necessary foremergency care;
H. Temperature control devices forthe patient, parenteral fluids and blood;
I. Temporary transvenous pacemaker;and
J. Electronic pressure monitoring. (E) The pediatric trauma center shall have
hemodialysis capability.(F) The pediatric trauma center shall have
organized burn care or a written transferagreement.
(G) The pediatric trauma center shall havespinal cord injury management capability ora written transfer agreement.
(H) There shall be documentation of ade-quate support services in assisting thepatient’s family from the time of entry intothe facility to the time of discharge.
(I) There shall be an operating room ade-quately staffed in-house and available twen-ty-four (24) hours a day with a back-up oper-ating room staff on call and promptly avail-able. Equipment for resuscitation and to pro-vide life support for the critically or serious-ly injured pediatric patient shall include, butnot be limited to:
1. Cardiopulmonary bypass capability;2. Operating microscope;3. Thermal control equipment for
patient, parenteral fluids and blood; 4. Endoscopes, all varieties; 5. Instruments necessary to perform an
open craniotomy; 6. Invasive and noninvasive monitoring
equipment; 7. Pediatric anesthesia equipment; 8. Cardiac output equipment;
9. Defibrillator and monitor, includinginternal and external pediatric paddles; and
10. Blood pressure cuffs, chest tubes,nasogastric tubes and urinary drainage appa-ratus for the pediatric patient.
(J) Clinical laboratory services shall beavailable twenty-four (24) hours a day. Thereshall be a comprehensive blood bank andaccess to a community central blood bankand adequate hospital storage facilities. Thereshall be provisions to provide and receive thefollowing laboratory test results twenty-four(24) hours a day:
1. Microbiology; 2. Standard analyses of blood, urine and
other body fluids; 3. Blood typing and cross-matching; 4. Coagulation studies; 5. Blood gases and pH determinations; 6. Serum and urine osmolality; and 7. Drug and alcohol screening.
(4) Standards for Programs in QualityAssurance, Outreach, Public Education andTraining for Pediatric Trauma CenterDesignation.
(A) There shall be a special audit of alltrauma-related deaths. There shall be a mech-anism in place to review all deaths and iden-tify primary admitted patients versus trans-ferred patients. Transferred patients shall befurther identified as transferred after stabiliz-ing treatment or direct admission after pro-longed treatment.
(B) There shall be a morbidity and mortal-ity review.
(C) There shall be a regular multidisci-plinary trauma conference that includes allmembers of the trauma team. Minutes of theconference shall include attendance, individ-ual cases reviewed and findings.
(D) There shall be a medical and nursingquality assessment program and utilizationreviews and tissue reviews on a regular basis.Documentation of quality assurance shallinclude problem identification, analysis,action plan, documentation and location ofaction, implementation and reevaluation.
(E) There shall be twenty-four (24)-houravailability of telephone consultation withphysicians in the outlying areas.
(F) The hospital shall demonstrate leader-ship in injury prevention in infants and chil-dren.
(G) The hospital and its staff shall docu-ment a research program in pediatric trauma.
(H) There shall be formal continuing edu-cation programs in pediatric trauma and reha-bilitation provided by the hospital for staffphysicians and nurses.
(I) The hospital shall provide programs incontinuing education for the area physicians,

CODE OF STATE REGULATIONS 35ROBIN CARNAHAN (7/31/07)Secretary of State
Chapter 40—Comprehensive Emergency Medical Services Systems Regulations 19 CSR 30-40
registered nurses and emergency medical ser-vice providers concerning the treatment of thepediatric trauma patient.
(5) Standards for the Programs in TraumaRehabilitation for Pediatric Trauma CenterDesignation.
(A) The hospital shall have a rehabilitationfacility or a written transfer agreement with arehabilitation center which is specificallyequipped for the care of children.
(B) The pediatric trauma rehabilitationteam shall develop and implement a proce-dure for discharge planning for the pediatrictrauma patient.
(C) The pediatric trauma rehabilitationplan developed for the pediatric traumapatient shall be under the direction of a physi-atrist or a physician with experience in pedi-atric trauma rehabilitation.
(D) The hospital shall develop a plan todocument that there is adequate post-dis-charge follow-up on pediatric traumapatients, including rehabilitation resultswhere applicable. This shall include identifi-cation of members of the rehabilitation team,discharge summary of trauma care to thepatient’s private physician and documentationthe patient’s medical record of the post-dis-charge plan.
AUTHORITY: sections 190.185 and 190.241,RSMo Supp. 1998.* Emergency rule filedAug. 28, 1998, effective Sept. 7, 1998,expired March 5, 1999. Original rule filedSept. 1, 1998, effective Feb. 28, 1999.
*Original authority: 190.185, RSMo 1973, amended1989, 1993, 1995, 1998 and 190.241, RSMo 1987,amended 1998.